Update on 8 th Edition Cutaneous AJCC Staging of Primary Cutaneous Melanoma. Michael T. Tetzlaff MD, PhD
|
|
|
- Cameron Warren Lewis
- 5 years ago
- Views:
Transcription
 and Translational and Molecular Pathology Director, Pathology Imaging Laboratory The University of Texas MD")
1 Update on 8 th Edition Cutaneous AJCC Staging of Primary Cutaneous Melanoma Michael T. Tetzlaff MD, PhD Associate Professor Departments of Pathology (Dermatopathology) and Translational and Molecular Pathology Director, Pathology Imaging Laboratory The University of Texas MD Anderson Cancer Center Executive Officer Translational Research Program The Alliance for Clinical Trials
2 Disclosures Seattle Genetics, Advisory Board Myriad Genetics, Advisory Board Novartis LLC, Advisory Board None related to topics presented






3 Update on 8 th Edition AJCC staging: Primary cutaneous melanoma Does not apply to melanomas of the conjunctiva, uvea, or mucosal melanomas of the head/neck, vulva/vaginal, or anorectum. Conjunctival Anorectal Urothelial Vulvar

4 Performing the biopsy and sending the requisition: Help us help you
5 Pathologic reporting for primary cutaneous melanoma * (A) RIGHT SHOULDER, SKIN PUNCH BIOPSY: * * * * * * * * * * MELANOMA, INVASIVE, SUPERFICIAL SPREADING TYPE CLARK LEVEL, IV BRESLOW THICKNESS, 2.25 MM RADIAL (NON-TUMORIGENIC) GROWTH PHASE, PRESENT VERTICAL (TUMORIGENIC) GROWTH PHASE, PRESENT MITOTIC FIGURES/MM 2, 6 ULCERATION, PRESENT (3.2 MM) REGRESSION, PRESENT VASCULAR INVASION, PRESENT PERINEURAL INVASION, PRESENT MICROSCOPIC SATELLITOSIS, PRESENT (3 X 2 MM) TUMOR-INFILTRATING LYMPHOCYTES, NON-BRISK ASSOCIATED MELANOCYTIC NEVUS, PRESENT INTRADERMAL) PREDOMINANT CYTOLOGY, EPITHELIOID SURGICAL MARGINS: INVASIVE MELANOMA PRESENT AT PERIPHERAL TISSUE EDGES * Required by CAP * Required by AJCC * Recommended by AJCC



6 T-category determined by Breslow thickness and ulceration Breslow (Tumor) thickness Ulceration Mitotic figures

7 T-category determined by Breslow thickness and ulceration All principle T-category ranges are preserved in the 8 th Edition AJCC Major differences: Definition of pt1b Breslow reported to 0.1 mm
8 7 th vs 8 th Edition AJCC staging of primary cutaneous melanoma Most significant change affects definition of pt1 melanomas pt1a pt1b 1.00 mm 1.00 mm 7 th Edition pt1 NO ulceration and mitotic rate <1/mm 2 With ulceration or mitotic rate>1/mm 2 8 th Edition pt1 pt1a <0.8 mm NON-ulcerated pt1b mm NON-ulcerated pt1b 1.0 mm With ulceration Major differences: Mitotic rate no longer contributes to the determination of pt1b Breslow thickness 0.8 mm major determinant of pt1b along with ulceration Breslow reported to 0.1 mm




9 Basis for the 0.8 mm cut-off among pt1 melanomas Tumor thickness 0.75 mm among the most influential Tumor thickness > 0.78 mm represented a natural cut-point


10 Basis for the 0.8 mm cut-off among pt1 melanomas N=6263 patients with thin melanomas Tumor thickness 0.80 mm was a natural and significant cut-point distinguishing particularly adverse 10 year survival.
 top of granular layer or (2) base of the ulcer to the deepest point of")
11 T-category determined by Breslow thickness and ulceration Breslow thickness Breslow thickness: Measured from: (1) top of granular layer or (2) base of the ulcer to the deepest point of invasion



 Biopsy specimen 1")
12 Additional changes to the Breslow thickness measurements Breslow thickness for pathologic staging Includes: Thickness measured in the biopsy OR Biopsy specimen 2 If the biopsy is transected, Breslow thickness is recorded as AT LEAST Thickness measured in the excision WHICHEVER IS GREATEST (NOT ADDITIVE) Biopsy specimen 1 Biopsy specimen BT1 + BT2 BT3
13 Additional changes to the Breslow thickness measurements Breslow thickness for pathologic staging Includes: Thickness measured in the biopsy OR If the biopsy is transected, Breslow thickness is recorded as AT LEAST Thickness measured in the excision WHICHEVER IS GREATEST (NOT ADDITIVE) Tumor thickness now recorded to the nearest 0.1 mm (instead of the nearest 0.01 mm) Due to impracticality and imprecision of 0.01 mm measurements particularly for tumors > 1 mm Important pathologic staging implications: 0.75 mm to 0.84 mm now recorded as 0.8 mm (pt1b) 0.95 mm to 1.04 mm now recorded as 1.0 mm (pt1b)




14 Important pitfalls in measuring Breslow thickness Avoid measuring around adnexal structrues Compared 257 patients with periadnexal involvement to 514 patients without. Breslow thickness did not include periadnexal extension. No difference in DSS, OSS Slightly more frequent SLN metastases


15 T-category determined by Breslow thickness and ulceration Clarification on ptis, pt0 and ptx ptis: Melanoma in situ pt0: No evidence of primary tumor ( melanoma of unknown primary ) ptx: Tumor thickness cannot be determined Tangential sectioning or the epidermis is not visualized

16 T-category determined by Breslow thickness and ulceration Ulceration Absence of intact epidermis with accompanying host reaction overlying invasive melanoma : Fibrin deposition with neutrophil scale/serum crust Based on microscopic examination Must be distinguished from artifactual or traumatic disruption
17 T-category defines prognosis among node-negative patients pt1a/b pt2a pt2b/3a pt3b/4a pt4b N0 N0




18 Mitotic figures are still important prognostic indicators Hotspot method. AJCC still strongly recommends a careful tabulation of the mitotic rate. NOT BINARY (0 vs 1) NOT IHC assisted. Mart-1/PHH3 cn0
 Tumor infiltrating lymphocytes (TILs) recorded as:")

 Best identified at the periphery of the tumor")
19 Additional factors of the primary tumor recommended for clinical care Clark level (II, III, IV, V) Tumor infiltrating lymphocytes (TILs) recorded as: Absent Non-Brisk Brisk Lymphovascular invasion IHC aided detection may assist in the detection Neurotropism Defined as melanoma cells abutting nerve sheaths, usually circumferentially (perineural invasion) or within nerves (intraneural invasion) Best identified at the periphery of the tumor MiTF/D2-40
20 Melanoma of unknown primary origin: pt0 Patient presents with a lymph node or distant visceral metastasis but no known primary melanoma. Iatrogenic or non-iatrogenic procedures caused regression Spontaneously regressed primary melanoma Patients with metastases restricted to lymph node should be considered as regional stage III disease. Such patients have a prognosis and natural history similar to if not MORE FAVORABLE than those same staging characteristics from a known primary cutaneous melanoma
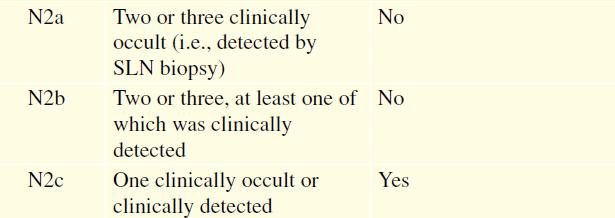
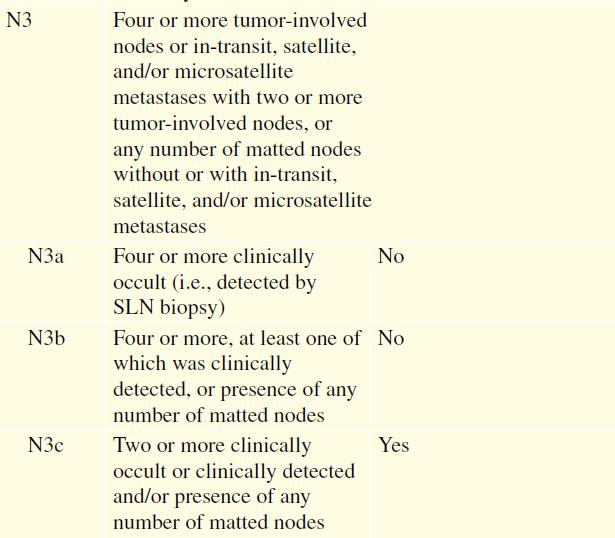
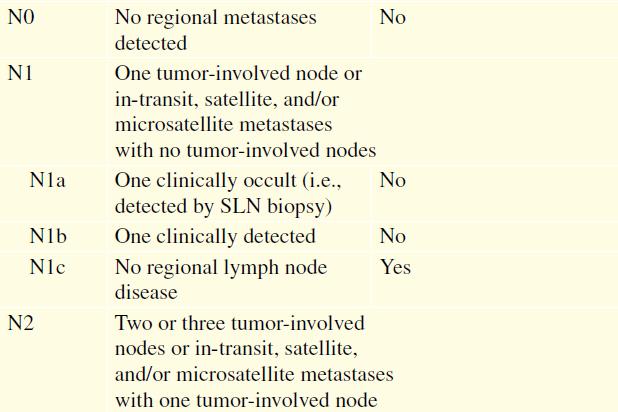
21 N-category determined by number and extent of nodal disease and satellites Major modifications: Clinically occult replaces microscopic [pnxa] Clinically evident replaces macroscopic [pnxb] Microsatellite, satellite or in-transit metastasis [pnxc]
22

23 N-category determined by number and extent of nodal disease and satellites N1a N2a N3a Clinically occult Lymph node N1b N2b N3b Clinically evident Lymph node N1c N2c N3c Microsatellite Satellite In-transit met

24 N-category determined by sentinel node evaluation in most cases Most lymph node metastases are detected by examination of the sentinel lymph node. Sentinel lymph nodes in melanoma About 20% positive 16% initial H&E 4% additional sections/ihc <5% with extracapsular extension

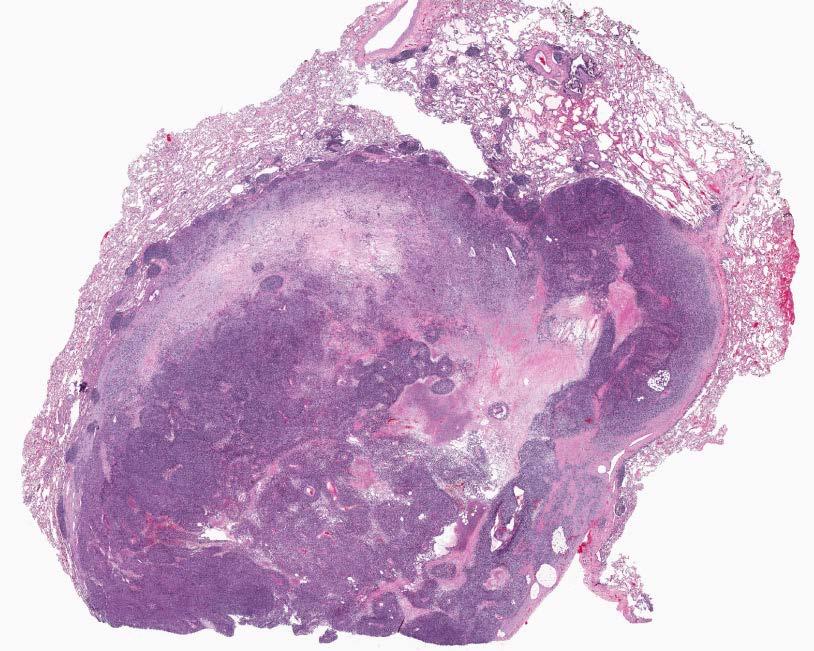
25 Subcapsular cluster of cells in the lymph node

 No unequivocal evidence for a minimum size threshold of microscopic tumor burden that is applied to define node")
26 Isolated cells in the SLN are significant Criteria for positive lymph node: Any tumor deposit size Isolated IHC+ tumor cell acceptable H&E confirmation not required Positive for at least one melanocytic marker (HMB45, Melan-A/Mart-1, Sox- 10, MITF, S100) Cells have malignant morphology (similar to primary tumor) and in the correct location (subcapsular versus intracapsular) No unequivocal evidence for a minimum size threshold of microscopic tumor burden that is applied to define node positive disease.
 Anatomic location of the SLN deposit Subcapsular Intraparenchymal Both")
27 N-category and capturing the extent of SNL disease burden Extent of sentinel lymph node disease burden correlates with non-sentinel lymph node positivity and predicts survival. Number of positive SLNs Size of the largest discrete deposit (at least one dimension) Anatomic location of the SLN deposit Subcapsular Intraparenchymal Both

28 Extracapsular extension Defined as the presence of nodal metastasis extending through the lymph node capsule into adjacent tissues usually seen as microscopic extension of metastatic melanoma into the perinodal adipose tissue.
29 Microsatellites, Satellites and In-transit metastases Each represents a discrete deposit of melanoma separated from the primary melanoma by normal tissue and each considered to represent lymphatic spread of tumor. 8 th Edition AJCC does not require minimum size threshold or minimum distance from the primary lesion. Microsatellites situated close to the primary lesion should be subjected to additional sections to exclude a connection.
 focus of metastatic melanoma in skin/subcutis adjacent or deep to the primary melanoma.")
 Detected during examination of the primary")
30 Microsatellites, Satellites and In-transit metastases Microsatellite: clinically occult (microscopic) focus of metastatic melanoma in skin/subcutis adjacent or deep to the primary melanoma. The tumor cells are discontinuous from the primary tumor and separated from the primary lesion by normal tissue (rather than fibrosis or inflammation) Detected during examination of the primary resection specimen.


31 Microsatellites, Satellites and In-transit metastases Satellite: clinically evident focus of metastatic melanoma in the skin or subcutis within 2 cm but discontinuous from the primary tumor. In transit metastasis: clinically evident metastasis in the skin or subcutis located > 2 cm from the primary tumor in the region between the tumor and the regional lymph node basin.
32 Microsatellites, Satellites and In-transit metastases Satellite: clinically evident focus of metastatic melanoma in the skin or subcutis within 2 cm but discontinuous from the primary tumor. In transit metastasis: clinically evident metastasis in the skin or subcutis located > 2 cm from the primary tumor in the region between the tumor and the regional lymph node basin. In transit Metastasis Microsatellite Satellite Primary Melanoma

33 8 th Edition AJCC primary cutaneous melanoma Stage III groups robustly stratify survival

34 Melanoma staging M-category: site and LDH



35 Thank you Section of Dermatopathology, UTMDACC: Victor G. Prieto MD, PhD Jonathan L. Curry MD Carlos A. Torres-Cabala MD Priya Nagarajan MD, PhD Phyu Aung MD, PhD Doina Ivan MD Departments of Melanoma Medical and Surgical Oncology, UTMDACC: Jeff Gershenwald MD Michael A. Davies MD, PhD
36
Michael T. Tetzlaff MD, PhD
 Update on American Joint Cancer Committee (AJCC) staging system for primary cutaneous melanoma Emphasis on concise and accurate reporting of primary and metastatic melanoma for effective risk stratification
Update on American Joint Cancer Committee (AJCC) staging system for primary cutaneous melanoma Emphasis on concise and accurate reporting of primary and metastatic melanoma for effective risk stratification
Michael T. Tetzlaff MD, PhD
 American Joint Cancer Committee (AJCC) staging system for primary cutaneous melanoma (8 th Edition) and principles of sentinel lymph node evaluation Emphasis on concise and accurate reporting of primary
American Joint Cancer Committee (AJCC) staging system for primary cutaneous melanoma (8 th Edition) and principles of sentinel lymph node evaluation Emphasis on concise and accurate reporting of primary
Melanoma Update: 8th Edition of AJCC Staging System
 Melanoma Update: 8th Edition of AJCC Staging System Rosalie Elenitsas, M.D. Professor of Dermatology Director, Dermatopathology University of Pennsylvania DISCLOSURE OF RELATIONSHIPS WITH INDUSTRY None
Melanoma Update: 8th Edition of AJCC Staging System Rosalie Elenitsas, M.D. Professor of Dermatology Director, Dermatopathology University of Pennsylvania DISCLOSURE OF RELATIONSHIPS WITH INDUSTRY None
Protocol applies to melanoma of cutaneous surfaces only.
 Melanoma of the Skin Protocol applies to melanoma of cutaneous surfaces only. Procedures Biopsy (No Accompanying Checklist) Excision Re-excision Protocol revision date: January 2005 Based on AJCC/UICC
Melanoma of the Skin Protocol applies to melanoma of cutaneous surfaces only. Procedures Biopsy (No Accompanying Checklist) Excision Re-excision Protocol revision date: January 2005 Based on AJCC/UICC
Primary Cutaneous Melanoma Pathology Reporting Proforma DD MM YYYY. *Tumour site. *Specimen laterality. *Specimen type
 Primary Cutaneous Melanoma Pathology Reporting Proforma Includes the International Collaboration on Cancer reporting dataset denoted by * Family name Given name(s) Date of birth DD MM YYYY Sex Male Female
Primary Cutaneous Melanoma Pathology Reporting Proforma Includes the International Collaboration on Cancer reporting dataset denoted by * Family name Given name(s) Date of birth DD MM YYYY Sex Male Female
47. Melanoma of the Skin
 1 Terms of Use The cancer staging form is a specific document in the patient record; it is not a substitute for documentation of history, physical examination, and staging evaluation, or for documenting
1 Terms of Use The cancer staging form is a specific document in the patient record; it is not a substitute for documentation of history, physical examination, and staging evaluation, or for documenting
Malignant tumors of melanocytes : Part 3. Deba P Sarma, MD., Omaha
 Malignant tumors of melanocytes : Part 3 Deba P Sarma, MD., Omaha Let s go over one case of melanoma using the following worksheet. Of the various essential information that needs to be included in the
Malignant tumors of melanocytes : Part 3 Deba P Sarma, MD., Omaha Let s go over one case of melanoma using the following worksheet. Of the various essential information that needs to be included in the
Protocol for the Examination of Specimens From Patients With Melanoma of the Skin
 Protocol for the Examination of Specimens From Patients With Melanoma of the Skin Version: Protocol Posting Date: June 2017 Includes ptnm requirements from the 8 th Edition, AJCC Staging Manual For accreditation
Protocol for the Examination of Specimens From Patients With Melanoma of the Skin Version: Protocol Posting Date: June 2017 Includes ptnm requirements from the 8 th Edition, AJCC Staging Manual For accreditation
Case Scenario 1 Worksheet. Primary Site C44.4 Morphology 8743/3 Laterality 0 Stage/ Prognostic Factors
 CASE SCENARIO 1 9/10/13 HISTORY: Patient is a 67-year-old white male and presents with lesion located 4-5cm above his right ear. The lesion has been present for years. No lymphadenopathy. 9/10/13 anterior
CASE SCENARIO 1 9/10/13 HISTORY: Patient is a 67-year-old white male and presents with lesion located 4-5cm above his right ear. The lesion has been present for years. No lymphadenopathy. 9/10/13 anterior
Michael T. Tetzlaff MD, PhD
 Molecular alterations informing the diagnosis of melanocytic tumors Michael T. Tetzlaff MD, PhD Associate Professor Department of Pathology, Section of Dermatopathology Department of Translational and
Molecular alterations informing the diagnosis of melanocytic tumors Michael T. Tetzlaff MD, PhD Associate Professor Department of Pathology, Section of Dermatopathology Department of Translational and
Cutaneous Melanoma: Epidemiology (USA) The Sentinel Node in Head and Neck Melanoma. Cutaneous Melanoma: Epidemiology (USA)
 The Sentinel Node in Head and Neck Melanoma. Cutaneous Melanoma: Epidemiology (USA)") The Sentinel Node in Head and Neck Melanoma Cutaneous Melanoma: Epidemiology (USA) 6 th leading cause of cancer among men and women 68,720 new cases of invasive melanoma in 2009 8,650 deaths from melanoma
The Sentinel Node in Head and Neck Melanoma Cutaneous Melanoma: Epidemiology (USA) 6 th leading cause of cancer among men and women 68,720 new cases of invasive melanoma in 2009 8,650 deaths from melanoma
Melanoma and the genes: Molecular alterations informing the diagnosis of melanocytic tumors
 Melanoma and the genes: Molecular alterations informing the diagnosis of melanocytic tumors Michael T. Tetzlaff MD, PhD Associate Professor Department of Pathology, Section of Dermatopathology Department
Melanoma and the genes: Molecular alterations informing the diagnosis of melanocytic tumors Michael T. Tetzlaff MD, PhD Associate Professor Department of Pathology, Section of Dermatopathology Department
Update on Merkel cell carcinoma
 Merkel cell carcinoma: Diagnosis, staging, sentinel lymph node biopsy and prognostic markers Michael T. Tetzlaff MD, PhD Associate Professor Departments of Pathology (Dermatopathology) and Translational
Merkel cell carcinoma: Diagnosis, staging, sentinel lymph node biopsy and prognostic markers Michael T. Tetzlaff MD, PhD Associate Professor Departments of Pathology (Dermatopathology) and Translational
Merkel cell carcinoma: Diagnosis, staging, sentinel lymph node biopsy and prognostic markers
 Merkel cell carcinoma: Diagnosis, staging, sentinel lymph node biopsy and prognostic markers Michael T. Tetzlaff MD, PhD Associate Professor Departments of Pathology (Dermatopathology) and Translational
Merkel cell carcinoma: Diagnosis, staging, sentinel lymph node biopsy and prognostic markers Michael T. Tetzlaff MD, PhD Associate Professor Departments of Pathology (Dermatopathology) and Translational
Melanoma-Back to Basics I Thought I Knew Ya! Paul K. Shitabata, M.D. Dermatopathologist APMG
 Melanoma-Back to Basics I Thought I Knew Ya! Paul K. Shitabata, M.D. Dermatopathologist APMG At tumor board, a surgeon insists that all level II melanomas are invasive since they have broken through the
Melanoma-Back to Basics I Thought I Knew Ya! Paul K. Shitabata, M.D. Dermatopathologist APMG At tumor board, a surgeon insists that all level II melanomas are invasive since they have broken through the
Impact of Prognostic Factors
 Melanoma Prognostic Factors: where we started, where are we going? Impact of Prognostic Factors Staging Management Surgical intervention Adjuvant treatment Suraj Venna, MD Assistant Clinical Professor,
Melanoma Prognostic Factors: where we started, where are we going? Impact of Prognostic Factors Staging Management Surgical intervention Adjuvant treatment Suraj Venna, MD Assistant Clinical Professor,
Surgery for Melanoma and What s on the Horizon
 and What s on the Horizon Giorgos C. Karakousis, M.D. Assistant Professor of Surgery Perelman School of Medicine at the University of Pennsylvania Background/Overview 76,870 cases of melanoma estimated
and What s on the Horizon Giorgos C. Karakousis, M.D. Assistant Professor of Surgery Perelman School of Medicine at the University of Pennsylvania Background/Overview 76,870 cases of melanoma estimated
AJCC 8 Implementation January 1, 2018 Melanoma of the Skin. Suraj Venna
 AJCC 8 Implementation January 1, 2018 Melanoma of the Skin Suraj Venna Personalized Medicine AJCC 8 th Edition This Time It s Personal Traditional AJCC (TNM) population-based analyses of large databases
AJCC 8 Implementation January 1, 2018 Melanoma of the Skin Suraj Venna Personalized Medicine AJCC 8 th Edition This Time It s Personal Traditional AJCC (TNM) population-based analyses of large databases
Sentinel Node Alphabet Soup: MSLT-1, DeCOG-SLT, MSLT-2, UNC
 Sentinel Node Alphabet Soup: MSLT-1, DeCOG-SLT, MSLT-2, UNC David W. Ollila MD James and Jesse Millis Professor of Surgery University of North Carolina, Chapel Hill Disclosures: None July 15, 2018 AJCC
Sentinel Node Alphabet Soup: MSLT-1, DeCOG-SLT, MSLT-2, UNC David W. Ollila MD James and Jesse Millis Professor of Surgery University of North Carolina, Chapel Hill Disclosures: None July 15, 2018 AJCC
Melanoma Underwriting Presented at 2018 AHOU Conference. Hank George FALU
 Melanoma Underwriting Presented at 2018 AHOU Conference Hank George FALU MELANOMA EPIDEMIOLOGY 70-80,000 American cases annually Majority are in situ or thin > 20% are diagnosed age 45 8-9,000 melanoma
Melanoma Underwriting Presented at 2018 AHOU Conference Hank George FALU MELANOMA EPIDEMIOLOGY 70-80,000 American cases annually Majority are in situ or thin > 20% are diagnosed age 45 8-9,000 melanoma
Update on Spitzoid and Blue nevus-like melanocytic lesions Emphasis on molecular studies informing diagnosis, prognosis and therapy
 Update on Spitzoid and Blue nevus-like melanocytic lesions Emphasis on molecular studies informing diagnosis, prognosis and therapy Michael T. Tetzlaff MD, PhD Associate Professor Department of Pathology,
Update on Spitzoid and Blue nevus-like melanocytic lesions Emphasis on molecular studies informing diagnosis, prognosis and therapy Michael T. Tetzlaff MD, PhD Associate Professor Department of Pathology,
Translating Evidence into Practice: Primary Cutaneous Melanoma Guidelines. Sentinel Lymph Node Biopsy
 American Academy of Dermatology 2018 Annual Meeting San Diego, CA, February 17, 2018 Translating Evidence into Practice: Primary Cutaneous Melanoma Guidelines. Sentinel Lymph Node Biopsy Christopher Bichakjian,
American Academy of Dermatology 2018 Annual Meeting San Diego, CA, February 17, 2018 Translating Evidence into Practice: Primary Cutaneous Melanoma Guidelines. Sentinel Lymph Node Biopsy Christopher Bichakjian,
Seventh Edition Staging 2017 Melanoma. Overview. This webinar is sponsored by. the Centers for Disease Control and Prevention.
 Seventh Edition Staging 2017 Melanoma Donna M. Gress, RHIT, CTR Validating science. Improving patient care. No materials in this presentation may be repurposed in print or online without the express written
Seventh Edition Staging 2017 Melanoma Donna M. Gress, RHIT, CTR Validating science. Improving patient care. No materials in this presentation may be repurposed in print or online without the express written
Melanoma Case Scenario 1
 Melanoma Case Scenario 1 History and physical 11/5/16 Patient is a single, 48-year-old male in good health who presented to his primary physician for a yearly physical exam during which a 3.4 x 2.8 x 1.5
Melanoma Case Scenario 1 History and physical 11/5/16 Patient is a single, 48-year-old male in good health who presented to his primary physician for a yearly physical exam during which a 3.4 x 2.8 x 1.5
Protocol for the Examination of Specimens From Patients With Merkel Cell Carcinoma of the Skin
 Protocol for the Examination of Specimens From Patients With Merkel Cell Carcinoma of the Skin Version: Protocol Posting Date: June 2017 Includes ptnm requirements from the 8 th Edition, AJCC Staging Manual
Protocol for the Examination of Specimens From Patients With Merkel Cell Carcinoma of the Skin Version: Protocol Posting Date: June 2017 Includes ptnm requirements from the 8 th Edition, AJCC Staging Manual
Melanoma Case Scenario 1
 Melanoma Case Scenario 1 History and physical 11/5/16 Patient is a single, 48-year-old male in good health who presented to his primary physician for a yearly physical exam during which a 3.4 x 2.8 x 1.5
Melanoma Case Scenario 1 History and physical 11/5/16 Patient is a single, 48-year-old male in good health who presented to his primary physician for a yearly physical exam during which a 3.4 x 2.8 x 1.5
Precision Surgery for Melanoma
 Precision Surgery for Melanoma Giorgos C. Karakousis, M.D. Assistant Professor of Surgery Perelman School of Medicine at the University of Pennsylvania Background 87,110 cases of melanoma estimated in
Precision Surgery for Melanoma Giorgos C. Karakousis, M.D. Assistant Professor of Surgery Perelman School of Medicine at the University of Pennsylvania Background 87,110 cases of melanoma estimated in
Collaborative Stage for TNM 7 - Revised 07/14/2009 [ Schema ]
![Collaborative Stage for TNM 7 - Revised 07/14/2009 [ Schema ]](/thumbs/71/65936251.jpg "Collaborative Stage for TNM 7 - Revised 07/14/2009 [ Schema ]") MelanomaSkin CS Tumor Size Collaborative Stage for TNM 7 - Revised 07/14/2009 [ Schema ] Code 000 No mass/tumor found Description 001-988 001-988 millimeters (code exact size in millimeters) 989 989 millimeters
MelanomaSkin CS Tumor Size Collaborative Stage for TNM 7 - Revised 07/14/2009 [ Schema ] Code 000 No mass/tumor found Description 001-988 001-988 millimeters (code exact size in millimeters) 989 989 millimeters
Melanoma Quality Reporting
 Melanoma Quality Reporting September 1, 2013 December 31, 2016 Laurence McCahill, MD Surgical Oncologist Metro Health Surgical Oncology Metro Health Professional Building 2122 Health Drive SW Wyoming,
Melanoma Quality Reporting September 1, 2013 December 31, 2016 Laurence McCahill, MD Surgical Oncologist Metro Health Surgical Oncology Metro Health Professional Building 2122 Health Drive SW Wyoming,
Desmoplastic Melanoma R/O BCC. Clinical Information. 74 y.o. man with lesion on left side of neck r/o BCC
 R/O BCC Sabine Kohler, M.D. Professor of Pathology and Dermatology Dermatopathology Service Stanford University School of Medicine Clinical Information 74 y.o. man with lesion on left side of neck r/o
R/O BCC Sabine Kohler, M.D. Professor of Pathology and Dermatology Dermatopathology Service Stanford University School of Medicine Clinical Information 74 y.o. man with lesion on left side of neck r/o
WHAT DOES THE PATHOLOGY REPORT MEAN?
 Melanoma WHAT IS MELANOMA? Melanoma is a type of cancer that affects cells called melanocytes. These cells are found mainly in skin but also in the lining of other areas such as nose and rectum, and also
Melanoma WHAT IS MELANOMA? Melanoma is a type of cancer that affects cells called melanocytes. These cells are found mainly in skin but also in the lining of other areas such as nose and rectum, and also
Melanoma. Kaushik Mukherjee MD A. Scott Pearson MD
 Melanoma Kaushik Mukherjee MD A. Scott Pearson MD Disclosures You still have to study Not all inclusive No Western blots Extensive use of Google Image Search and Sabiston Melanoma Basics 8 th most common
Melanoma Kaushik Mukherjee MD A. Scott Pearson MD Disclosures You still have to study Not all inclusive No Western blots Extensive use of Google Image Search and Sabiston Melanoma Basics 8 th most common
3/23/2017. Disclosure of Relevant Financial Relationships. Pathologic Staging Updates in Breast Cancer. Pathologic Staging Updates Breast Cancer
 Pathologic Staging Updates in Breast Cancer Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position to influence or control the content of CME
Pathologic Staging Updates in Breast Cancer Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position to influence or control the content of CME
NAACCR Webinar Series 1
 Collecting Cancer Data: Melanoma 2013 2014 NAACCR Webinar Series April 3, 2014 Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching
Collecting Cancer Data: Melanoma 2013 2014 NAACCR Webinar Series April 3, 2014 Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching
What are the new AJCC Staging System changes, and how will they affect my patients?
 What are the new AJCC Staging System changes, and how will they affect my patients? Emily Y. Chu, M.D., Ph.D. Assistant Professor of Dermatology & Pathology and Laboratory Medicine University of Pennsylvania
What are the new AJCC Staging System changes, and how will they affect my patients? Emily Y. Chu, M.D., Ph.D. Assistant Professor of Dermatology & Pathology and Laboratory Medicine University of Pennsylvania
Melanoma Surgery Update James R. Ouellette, DO FACS Premier Health Cancer Institute Wright State University Chief, Surgical Oncology Division
 Melanoma Surgery Update 2018 James R. Ouellette, DO FACS Premier Health Cancer Institute Wright State University Chief, Surgical Oncology Division Surgery for Melanoma Mainstay of treatment for potentially
Melanoma Surgery Update 2018 James R. Ouellette, DO FACS Premier Health Cancer Institute Wright State University Chief, Surgical Oncology Division Surgery for Melanoma Mainstay of treatment for potentially
Collaborative Stage for TNM 7 - Revised 12/02/2009 [ Schema ]
![Collaborative Stage for TNM 7 - Revised 12/02/2009 [ Schema ]](/thumbs/82/86783199.jpg "Collaborative Stage for TNM 7 - Revised 12/02/2009 [ Schema ]") CS Tumor Size Collaborative Stage for TNM 7 - Revised 12/02/2009 [ Schema ] Note: the specific tumor size as documented in the medical record. If the ONLY information regarding tumor size is the physician's
CS Tumor Size Collaborative Stage for TNM 7 - Revised 12/02/2009 [ Schema ] Note: the specific tumor size as documented in the medical record. If the ONLY information regarding tumor size is the physician's
Patient age and cutaneous malignant melanoma: Elderly patients are likely to have more aggressive histological features and poorer survival
 MOLECULAR AND CLINICAL ONCOLOGY 7: 1083-1088, 2017 Patient age and cutaneous malignant melanoma: Elderly patients are likely to have more aggressive histological features and poorer survival FARUK TAS
MOLECULAR AND CLINICAL ONCOLOGY 7: 1083-1088, 2017 Patient age and cutaneous malignant melanoma: Elderly patients are likely to have more aggressive histological features and poorer survival FARUK TAS
Colon and Rectum. Protocol revision date: January 2005 Based on AJCC/UICC TNM, 6th edition
 Colon and Rectum Protocol applies to all invasive carcinomas of the colon and rectum. Carcinoid tumors, lymphomas, sarcomas, and tumors of the vermiform appendix are excluded. Protocol revision date: January
Colon and Rectum Protocol applies to all invasive carcinomas of the colon and rectum. Carcinoid tumors, lymphomas, sarcomas, and tumors of the vermiform appendix are excluded. Protocol revision date: January
A PRACTICAL APPROACH TO ATYPICAL MELANOCYTIC LESIONS BIJAN HAGHIGHI M.D, DIRECTOR OF DERMATOPATHOLOGY, ST. JOSEPH HOSPITAL
 A PRACTICAL APPROACH TO ATYPICAL MELANOCYTIC LESIONS BIJAN HAGHIGHI M.D, DIRECTOR OF DERMATOPATHOLOGY, ST. JOSEPH HOSPITAL OBJECTIVES Discuss current trends and changing concepts in our understanding of
A PRACTICAL APPROACH TO ATYPICAL MELANOCYTIC LESIONS BIJAN HAGHIGHI M.D, DIRECTOR OF DERMATOPATHOLOGY, ST. JOSEPH HOSPITAL OBJECTIVES Discuss current trends and changing concepts in our understanding of
Talk to Your Doctor. Fact Sheet
 Talk to Your Doctor Hearing the words you have skin cancer is overwhelming and would leave anyone with a lot of questions. If you have been diagnosed with Stage I or II cutaneous melanoma with no apparent
Talk to Your Doctor Hearing the words you have skin cancer is overwhelming and would leave anyone with a lot of questions. If you have been diagnosed with Stage I or II cutaneous melanoma with no apparent
46. Merkel Cell Carcinoma
 1 Terms of Use The cancer staging form is a specific document in the patient record; it is not a substitute for documentation of history, physical examination, and staging evaluation, or for documenting
1 Terms of Use The cancer staging form is a specific document in the patient record; it is not a substitute for documentation of history, physical examination, and staging evaluation, or for documenting
Uveal Melanoma. Protocol applies to malignant melanoma of the uvea.
 Uveal Melanoma Protocol applies to malignant melanoma of the uvea. Protocol revision date: January 2005 Based on AJCC/UICC TNM, 6 th edition Procedures Cytology (No Accompanying Checklist) Biopsy (No Accompanying
Uveal Melanoma Protocol applies to malignant melanoma of the uvea. Protocol revision date: January 2005 Based on AJCC/UICC TNM, 6 th edition Procedures Cytology (No Accompanying Checklist) Biopsy (No Accompanying
Protocol for the Examination of Specimens From Patients With Merkel Cell Carcinoma of the Skin
 Protocol for the Examination of Specimens From Patients With Merkel Cell Carcinoma of the Skin Protocol applies to Merkel cell carcinoma of cutaneous surfaces only. Based on AJCC/UICC TNM, 7th edition
Protocol for the Examination of Specimens From Patients With Merkel Cell Carcinoma of the Skin Protocol applies to Merkel cell carcinoma of cutaneous surfaces only. Based on AJCC/UICC TNM, 7th edition
Tracking skin cancers and melanoma at the microscopic level
 Tracking skin cancers and melanoma at the microscopic level Rosalie Elenitsas, M.D. Professor of Dermatology Director of Dermatopathology Hospital of the University of Pennsylvania May 12, 2017 Outline
Tracking skin cancers and melanoma at the microscopic level Rosalie Elenitsas, M.D. Professor of Dermatology Director of Dermatopathology Hospital of the University of Pennsylvania May 12, 2017 Outline
Rebecca Vogel, PGY-4 March 5, 2012
 Rebecca Vogel, PGY-4 March 5, 2012 Historical Perspective Changes In The Staging System Studies That Started The Talk Where We Go From Here Cutaneous melanoma has become an increasingly growing problem,
Rebecca Vogel, PGY-4 March 5, 2012 Historical Perspective Changes In The Staging System Studies That Started The Talk Where We Go From Here Cutaneous melanoma has become an increasingly growing problem,
Melanocytic Lesions: Use of Immunohistochemistry and Special Studies Napa Valley 2018
 Melanocytic Lesions: Use of Immunohistochemistry and Special Studies Napa Valley 2018 Victor G. Prieto, MD, PhD Professor Depts. of Pathology and Dermatology University of Texas - MD Anderson Cancer Center
Melanocytic Lesions: Use of Immunohistochemistry and Special Studies Napa Valley 2018 Victor G. Prieto, MD, PhD Professor Depts. of Pathology and Dermatology University of Texas - MD Anderson Cancer Center
NAACCR Webinar Series 1
 Collecting Cancer Data: Skin Malignancies 2/4/2010 NAACCR 2009 2010 Webinar Series Questions Please use the Q&A panel to submit your questions Send questions to All Panelist Collecting Cancer Data: Skin
Collecting Cancer Data: Skin Malignancies 2/4/2010 NAACCR 2009 2010 Webinar Series Questions Please use the Q&A panel to submit your questions Send questions to All Panelist Collecting Cancer Data: Skin
Protocol for the Examination of Specimens From Patients With Melanoma of the Skin
 Protocol for the Examination of Specimens From Patients With Melanoma of the Skin Protocol applies to melanoma of cutaneous surfaces only. Based on AJCC/UICC TNM, 7th edition Protocol web posting date:
Protocol for the Examination of Specimens From Patients With Melanoma of the Skin Protocol applies to melanoma of cutaneous surfaces only. Based on AJCC/UICC TNM, 7th edition Protocol web posting date:
Epithelial Cancer- NMSC & Melanoma
 Epithelial Cancer- NMSC & Melanoma David Chin MB, BCh, BAO, LRCP, LRCS (Ireland) MCh(MD), PhD (UQ), FRCS, FRACS (Plast) Plastic & Reconstructive Surgeon Visiting Scientist Melanoma Genomic Group & Drug
Epithelial Cancer- NMSC & Melanoma David Chin MB, BCh, BAO, LRCP, LRCS (Ireland) MCh(MD), PhD (UQ), FRCS, FRACS (Plast) Plastic & Reconstructive Surgeon Visiting Scientist Melanoma Genomic Group & Drug
Staging Challenges in Lower GI Cancers. Disclosure of Relevant Financial Relationships. AJCC 8 th edition and CAP protocol updates
 Staging Challenges in Lower GI Cancers Sanjay Kakar, MD University of California, San Francisco March 05, 2017 Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education
Staging Challenges in Lower GI Cancers Sanjay Kakar, MD University of California, San Francisco March 05, 2017 Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education
6. Cervical Lymph Nodes and Unknown Primary Tumors of the Head and Neck
 1 Terms of Use The cancer staging form is a specific document in the patient record; it is not a substitute for documentation of history, physical examination, and staging evaluation, or for documenting
1 Terms of Use The cancer staging form is a specific document in the patient record; it is not a substitute for documentation of history, physical examination, and staging evaluation, or for documenting
Topics for Discussion. Malignant Melanoma. Surgical Treatment. Current Treatment of Cutaneous Melanoma 5/17/2013. Lymph Regional nodes:
 Topics for Discussion What is a sentinel lymph node (SLN)? Utility of sentinel lymph biopsies: therapeutic or staging? Current Treatment of Cutaneous Melanoma Carlos Corvera, M.D. Associate Professor of
Topics for Discussion What is a sentinel lymph node (SLN)? Utility of sentinel lymph biopsies: therapeutic or staging? Current Treatment of Cutaneous Melanoma Carlos Corvera, M.D. Associate Professor of
Biomarkers in melanoma: staging, prognosis and detection of early metastases
 Review CONTENTS Staging of melanoma Prognostic biomarkers for Stage I & II melanoma Individualized prognosis for Stage I & II melanoma patients Detection of metastasis in Stage I III melanoma Expert opinion
Review CONTENTS Staging of melanoma Prognostic biomarkers for Stage I & II melanoma Individualized prognosis for Stage I & II melanoma patients Detection of metastasis in Stage I III melanoma Expert opinion
Molecular Enhancement of Sentinel Node Evaluation
 Cochran Illustrations 060104 Molecular Enhancement of Sentinel Node Evaluation Alistair Cochran, MD and Rong Huang MD Departments of Pathology and Laboratory Medicine and Surgery, David Geffen School of
Cochran Illustrations 060104 Molecular Enhancement of Sentinel Node Evaluation Alistair Cochran, MD and Rong Huang MD Departments of Pathology and Laboratory Medicine and Surgery, David Geffen School of
Updates on Melanoma: Are You Following the Latest Guidelines of Care? Jerry Brewer, MD
 Updates on Melanoma: Are You Following the Latest Guidelines of Care? Jerry Brewer, MD Disclosure Statement Update on Melanoma Are You Following the Latest Guidelines of Care? I, Jerry D. Brewer, MD, do
Updates on Melanoma: Are You Following the Latest Guidelines of Care? Jerry Brewer, MD Disclosure Statement Update on Melanoma Are You Following the Latest Guidelines of Care? I, Jerry D. Brewer, MD, do
Definition of Synoptic Reporting
 Definition of Synoptic Reporting The CAP has developed this list of specific features that define synoptic reporting formatting: 1. All required cancer data from an applicable cancer protocol that are
Definition of Synoptic Reporting The CAP has developed this list of specific features that define synoptic reporting formatting: 1. All required cancer data from an applicable cancer protocol that are
Clinical Pathological Conference. Malignant Melanoma of the Vulva
 Clinical Pathological Conference Malignant Melanoma of the Vulva History F/48 Chinese Married Para 1 Presented in September 2004 Vulval mass for 2 months Associated with watery and blood stained discharge
Clinical Pathological Conference Malignant Melanoma of the Vulva History F/48 Chinese Married Para 1 Presented in September 2004 Vulval mass for 2 months Associated with watery and blood stained discharge
Morphological characteristics of the primary tumor and micrometastases in sentinel lymph nodes as a predictor of melanoma progression
 Morphological characteristics of the primary tumor and micrometastases in sentinel lymph nodes as a predictor of melanoma progression M.N. Kukushkina, S.I. Korovin, O.I. Solodyannikova, G.G. Sukach, A.Yu.
Morphological characteristics of the primary tumor and micrometastases in sentinel lymph nodes as a predictor of melanoma progression M.N. Kukushkina, S.I. Korovin, O.I. Solodyannikova, G.G. Sukach, A.Yu.
Genetic Testing: When should it be ordered? Julie Schloemer, MD Dermatology
 Genetic Testing: When should it be ordered? Julie Schloemer, MD Dermatology Outline Germline testing CDKN2A BRCA2 BAP1 Somatic testing Gene expression profiling (GEP) BRAF Germline vs Somatic testing
Genetic Testing: When should it be ordered? Julie Schloemer, MD Dermatology Outline Germline testing CDKN2A BRCA2 BAP1 Somatic testing Gene expression profiling (GEP) BRAF Germline vs Somatic testing
Head & Neck Squamous Carcinoma: Artifacts, Challenges, and Controversies. Agenda
 Head & Neck Squamous Carcinoma: Artifacts, Challenges, and Controversies Jennifer L. Hunt, MD, MEd Aubrey J. Hough Jr, MD, Endowed Professor of Pathology Chair of Pathology and Laboratory Medicine University
Head & Neck Squamous Carcinoma: Artifacts, Challenges, and Controversies Jennifer L. Hunt, MD, MEd Aubrey J. Hough Jr, MD, Endowed Professor of Pathology Chair of Pathology and Laboratory Medicine University
Surgical Issues in Melanoma
 Surgical Issues in Melanoma Mark B. Faries, MD, FACS Director, Donald L. Morton Melanoma Research Program Director, Surgical Oncology Training Program Professor of Surgery John Wayne Cancer Institute Surgical
Surgical Issues in Melanoma Mark B. Faries, MD, FACS Director, Donald L. Morton Melanoma Research Program Director, Surgical Oncology Training Program Professor of Surgery John Wayne Cancer Institute Surgical
You Are Going to Cut How Much Skin? Locoregional Surgical Treatment. Justin Rivard MD, MSc, FRCSC September 21, 2018
 You Are Going to Cut How Much Skin? Locoregional Surgical Treatment Justin Rivard MD, MSc, FRCSC September 21, 2018 Presenter Disclosure Faculty/Speaker: Justin Rivard Relationships with financial sponsors:
You Are Going to Cut How Much Skin? Locoregional Surgical Treatment Justin Rivard MD, MSc, FRCSC September 21, 2018 Presenter Disclosure Faculty/Speaker: Justin Rivard Relationships with financial sponsors:
Dr Rosalie Stephens. Mr Richard Martin. Medical Oncologist Auckland City Hospital Auckland
 Dr Rosalie Stephens Medical Oncologist Auckland City Hospital Auckland Mr Richard Martin General Surgeon Melanoma Unit Team Waitemata District Health Board Auckland 8:30-9:25 WS #99: Interactive Case Studies
Dr Rosalie Stephens Medical Oncologist Auckland City Hospital Auckland Mr Richard Martin General Surgeon Melanoma Unit Team Waitemata District Health Board Auckland 8:30-9:25 WS #99: Interactive Case Studies
NEW SURGICAL APPROACHES TO MELANOMA THERAPY
 NEW SURGICAL APPROACHES TO MELANOMA THERAPY Melanoma 2003: New Insights Into Therapy & Treatment Douglas L. Fraker, M.D. University of Pennsylvania Surgical Treatment of Melanoma Primary resection margins
NEW SURGICAL APPROACHES TO MELANOMA THERAPY Melanoma 2003: New Insights Into Therapy & Treatment Douglas L. Fraker, M.D. University of Pennsylvania Surgical Treatment of Melanoma Primary resection margins
This form may provide more data elements than required for collection by standard setters such as NCI SEER, CDC NPCR, and CoC NCDB.
 1 Terms of Use The cancer staging form is a specific document in the patient record; it is not a substitute for documentation of history, physical examination, and staging evaluation, or for documenting
1 Terms of Use The cancer staging form is a specific document in the patient record; it is not a substitute for documentation of history, physical examination, and staging evaluation, or for documenting
Disclosures. Outline. What IS tumor budding?? Tumor Budding in Colorectal Carcinoma: What, Why, and How. I have nothing to disclose
 Tumor Budding in Colorectal Carcinoma: What, Why, and How Disclosures I have nothing to disclose Soo-Jin Cho, MD, PhD Assistant Professor UCSF Dept of Pathology Current Issues in Anatomic Pathology 2017
Tumor Budding in Colorectal Carcinoma: What, Why, and How Disclosures I have nothing to disclose Soo-Jin Cho, MD, PhD Assistant Professor UCSF Dept of Pathology Current Issues in Anatomic Pathology 2017
VULVAR CARCINOMA. Page 1 of 5
 VULVAR CARCINOMA EXAMPLE OF A VULVAR CARCINOMA USING PROPOSED TEMPLATE Case: Invasive squamous cell carcinoma arising in D-VIN Tumor in left labia major Left partial vaginectomy and sentinel lymph node
VULVAR CARCINOMA EXAMPLE OF A VULVAR CARCINOMA USING PROPOSED TEMPLATE Case: Invasive squamous cell carcinoma arising in D-VIN Tumor in left labia major Left partial vaginectomy and sentinel lymph node
Radionuclide detection of sentinel lymph node
 Radionuclide detection of sentinel lymph node Sophia I. Koukouraki Assoc. Professor Department of Nuclear Medicine Medicine School, University of Crete 1 BACKGROUND The prognosis of malignant disease is
Radionuclide detection of sentinel lymph node Sophia I. Koukouraki Assoc. Professor Department of Nuclear Medicine Medicine School, University of Crete 1 BACKGROUND The prognosis of malignant disease is
Springer Healthcare. Staging and Diagnosing Cutaneous Melanoma. Concise Reference. Dirk Schadendorf, Corinna Kochs, Elisabeth Livingstone
 Concise Reference Staging and Diagnosing Cutaneous Melanoma Dirk Schadendorf, Corinna Kochs, Elisabeth Livingstone Extracted from Handbook of Cutaneous Melanoma: A Guide to Diagnosis and Treatment Published
Concise Reference Staging and Diagnosing Cutaneous Melanoma Dirk Schadendorf, Corinna Kochs, Elisabeth Livingstone Extracted from Handbook of Cutaneous Melanoma: A Guide to Diagnosis and Treatment Published
Controversies and Questions in the Surgical Treatment of Melanoma
 Controversies and Questions in the Surgical Treatment of Melanoma Giorgos C. Karakousis, M.D. Assistant Professor of Surgery Division of Endocrine and Oncologic Surgery University of Pennsylvania School
Controversies and Questions in the Surgical Treatment of Melanoma Giorgos C. Karakousis, M.D. Assistant Professor of Surgery Division of Endocrine and Oncologic Surgery University of Pennsylvania School
Vernon K. Sondak. Department of Cutaneous Oncology Moffitt Cancer Center Tampa, Florida
 Vernon K. Sondak Department of Cutaneous Oncology Moffitt Cancer Center Tampa, Florida Australasian Melanoma Conference 2016 Sydney, NSW, Australia October 29, 2016 Disclosures Dr. Sondak is a compensated
Vernon K. Sondak Department of Cutaneous Oncology Moffitt Cancer Center Tampa, Florida Australasian Melanoma Conference 2016 Sydney, NSW, Australia October 29, 2016 Disclosures Dr. Sondak is a compensated
World Articles of Ear, Nose and Throat Page 1
 World Articles of Ear, Nose and Throat ---------------------Page 1 Primary Malignant Melanoma of the Tongue: A Case Report Authors: Nanayakkara PR*, Arudchelvam JD** Ariyaratne JC*, Mendis K*, Jayasekera
World Articles of Ear, Nose and Throat ---------------------Page 1 Primary Malignant Melanoma of the Tongue: A Case Report Authors: Nanayakkara PR*, Arudchelvam JD** Ariyaratne JC*, Mendis K*, Jayasekera
David B. Troxel, MD. Common Medicolegal Situations: Misdiagnosis of Melanoma
 Common Medicolegal Situations: Misdiagnosis of Melanoma David B. Troxel, MD Medical Director, The Doctors Company, Napa, California Clinical Professor Emeritus, University of California at Berkeley Past
Common Medicolegal Situations: Misdiagnosis of Melanoma David B. Troxel, MD Medical Director, The Doctors Company, Napa, California Clinical Professor Emeritus, University of California at Berkeley Past
Predictive Factors for the Positivity of the Sentinel Lymph Node in Malignant Melanoma
 ORIGINAL RESEARCH SURGERY // ANATOMO-PATHOLOGY Predictive Factors for the Positivity of the Sentinel Lymph Node in Malignant Melanoma Călin Crăciun, Orsolya Hankó- Bauer, Zalán Benedek, Sorin Sorlea, Marius
ORIGINAL RESEARCH SURGERY // ANATOMO-PATHOLOGY Predictive Factors for the Positivity of the Sentinel Lymph Node in Malignant Melanoma Călin Crăciun, Orsolya Hankó- Bauer, Zalán Benedek, Sorin Sorlea, Marius
Dermatopathology: The tumor is composed of keratinocytes which show atypia, increase mitoses and abnormal mitoses.
 Squamous cell carcinoma (SCC): A common malignant tumor of keratinocytes arising in the epidermis, usually from a precancerous condition: 1- UV induced actinic keratosis, usually of low grade malignancy.
Squamous cell carcinoma (SCC): A common malignant tumor of keratinocytes arising in the epidermis, usually from a precancerous condition: 1- UV induced actinic keratosis, usually of low grade malignancy.
Chapter 2 Staging of Breast Cancer
 Chapter 2 Staging of Breast Cancer Zeynep Ozsaran and Senem Demirci Alanyalı 2.1 Introduction Five decades ago, Denoix et al. proposed classification system (tumor node metastasis [TNM]) based on the dissemination
Chapter 2 Staging of Breast Cancer Zeynep Ozsaran and Senem Demirci Alanyalı 2.1 Introduction Five decades ago, Denoix et al. proposed classification system (tumor node metastasis [TNM]) based on the dissemination
category cm0. Category will ensure it T1 melanoma. 68 Retinoblastoma
 AJCC 8 th Edition Chapter 1 Principles of Cancer Staging: Node Status Not Required in Rare Circumstances Clinical Staging, cn Category For some cancer sites in which lymph node involvement is rare, patients
AJCC 8 th Edition Chapter 1 Principles of Cancer Staging: Node Status Not Required in Rare Circumstances Clinical Staging, cn Category For some cancer sites in which lymph node involvement is rare, patients
NAACCR Hospital Registry Webinar Series
 NAACCR Hospital Registry Webinar Series October 4, 2007 Abstracting Melanoma Cancer Incidence and Treatment Data Image source: commons.wikimedia.org/wiki/image.melanoma.jpg Sites include Melanoma Skin
NAACCR Hospital Registry Webinar Series October 4, 2007 Abstracting Melanoma Cancer Incidence and Treatment Data Image source: commons.wikimedia.org/wiki/image.melanoma.jpg Sites include Melanoma Skin
Original Articles Primary orbital melanoma in association with cellular blue nevus
 Original Articles Primary orbital melanoma in association with cellular blue nevus Tarek El-Sawy, MD, PhD, a Mathieu F. Bakhoum, PhD, a Michael Tetzlaff, MD, PhD, b Qasiem J. Nasser, MD, a Victor G. Prieto,
Original Articles Primary orbital melanoma in association with cellular blue nevus Tarek El-Sawy, MD, PhD, a Mathieu F. Bakhoum, PhD, a Michael Tetzlaff, MD, PhD, b Qasiem J. Nasser, MD, a Victor G. Prieto,
STAGE CATEGORY DEFINITIONS
 CLINICAL Extent of disease before any treatment y clinical staging completed after neoadjuvant therapy but before subsequent surgery TX Tis Tis (DCIS) Tis (LCIS) Tis (Paget s) T1 T1mi T1a T1b T1c a b c
CLINICAL Extent of disease before any treatment y clinical staging completed after neoadjuvant therapy but before subsequent surgery TX Tis Tis (DCIS) Tis (LCIS) Tis (Paget s) T1 T1mi T1a T1b T1c a b c
The New AJCC: 8 th Edition and Beyond. 8th Edition AJCC Melanoma Staging System. Jeffrey E. Gershenwald, MD, FACS. AJCC Physician to Physician
 AJCC Physician to Physician 8th Edition AJCC Melanoma Staging System Jeffrey E. Gershenwald, MD, FACS Dr. John M. Skibber Professor, Department of Surgical Oncology Professor, Department of Cancer Biology
AJCC Physician to Physician 8th Edition AJCC Melanoma Staging System Jeffrey E. Gershenwald, MD, FACS Dr. John M. Skibber Professor, Department of Surgical Oncology Professor, Department of Cancer Biology
Update on staging colorectal carcinoma, the 8 th edition AJCC. General overview of staging. When is staging required? 11/1/2017
 Update on staging colorectal carcinoma, the 8 th edition AJCC Dale C. Snover, MD November 3, 2017 General overview of staging Reason for uniform staging Requirements to use AJCC manual and/or CAP protocols
Update on staging colorectal carcinoma, the 8 th edition AJCC Dale C. Snover, MD November 3, 2017 General overview of staging Reason for uniform staging Requirements to use AJCC manual and/or CAP protocols
Polypoid Melanoma, A Virulent Variant of the Nodular Growth Pattern
 Polypoid Melanoma, A Virulent Variant of the Nodular Growth Pattern ELIZABETH A. MANCI, M.D., CHARLES M. BALCH, M.D..TARIQ M. MURAD, M.D., PH.D., AND SENG/JAW SOONG, PH.D. Manci, Elizabeth A., Balch, Charles
Polypoid Melanoma, A Virulent Variant of the Nodular Growth Pattern ELIZABETH A. MANCI, M.D., CHARLES M. BALCH, M.D..TARIQ M. MURAD, M.D., PH.D., AND SENG/JAW SOONG, PH.D. Manci, Elizabeth A., Balch, Charles
Quality ID #397: Melanoma Reporting National Quality Strategy Domain: Communication and Care Coordination
 Quality ID #397: Melanoma Reporting National Quality Strategy Domain: Communication and Care Coordination 2018 OPTIONS FOR INDIVIDUAL MEASURES: CLAIMS ONLY MEASURE TYPE: Outcome DESCRIPTION: Pathology
Quality ID #397: Melanoma Reporting National Quality Strategy Domain: Communication and Care Coordination 2018 OPTIONS FOR INDIVIDUAL MEASURES: CLAIMS ONLY MEASURE TYPE: Outcome DESCRIPTION: Pathology
AJCC Staging of Head & Neck Cancer (7 th edition, 2010) -LIP & ORAL CAVITY-
 -LIP & ORAL CAVITY-") TX: primary tumor cannot be assessed T0: no evidence of primary tumor Tis: carcinoma in situ. T1: tumor is 2 cm or smaller AJCC Staging of Head & Neck Cancer (7 th edition, 2010) -LIP & ORAL CAVITY- T2:
TX: primary tumor cannot be assessed T0: no evidence of primary tumor Tis: carcinoma in situ. T1: tumor is 2 cm or smaller AJCC Staging of Head & Neck Cancer (7 th edition, 2010) -LIP & ORAL CAVITY- T2:
Case #1: 75 y/o Male (treated and followed by prostate cancer oncology specialist ).
.") SOLID TUMORS WORKSHOP Cases for review Prostate Cancer Case #1: 75 y/o Male (treated and followed by prostate cancer oncology specialist ). January 2009 PSA 4.4, 20% free; August 2009 PSA 5.2; Sept 2009
SOLID TUMORS WORKSHOP Cases for review Prostate Cancer Case #1: 75 y/o Male (treated and followed by prostate cancer oncology specialist ). January 2009 PSA 4.4, 20% free; August 2009 PSA 5.2; Sept 2009
Staging for Residents, Nurses, and Multidisciplinary Health Care Team
 Staging for Residents, Nurses, and Multidisciplinary Health Care Team Donna M. Gress, RHIT, CTR Validating science. Improving patient care. Learning Objectives Introduce the concept and history of stage
Staging for Residents, Nurses, and Multidisciplinary Health Care Team Donna M. Gress, RHIT, CTR Validating science. Improving patient care. Learning Objectives Introduce the concept and history of stage
Standards and datasets for reporting cancers. Dataset for histopathological reporting of primary cutaneous malignant.
 Standards and datasets for reporting cancers Dataset for histopathological reporting of primary cutaneous malignant melanoma and regional lymph nodes February 2019 Authors: Dr David Slater, Chesterfield
Standards and datasets for reporting cancers Dataset for histopathological reporting of primary cutaneous malignant melanoma and regional lymph nodes February 2019 Authors: Dr David Slater, Chesterfield
Printed by Martina Huckova on 10/3/2011 3:04:54 PM. For personal use only. Not approved for distribution. Copyright 2011 National Comprehensive
 Table of Contents NCCN Categories of Evidence and Consensus Category 1: Based upon high-level evidence, there is uniform NCCN consensus that the intervention is appropriate. Category 2A: Based upon lower-level
Table of Contents NCCN Categories of Evidence and Consensus Category 1: Based upon high-level evidence, there is uniform NCCN consensus that the intervention is appropriate. Category 2A: Based upon lower-level
12. Malignant Melanoma of Skin
 KEY FACTS 12. Malignant Melanoma of Skin ICD-9 172 On average 160 melanomas of the skin were registered per year. Twice as common in females than in males. Higher than expected numbers in Southern Board
KEY FACTS 12. Malignant Melanoma of Skin ICD-9 172 On average 160 melanomas of the skin were registered per year. Twice as common in females than in males. Higher than expected numbers in Southern Board
Sentinel Node in Malignant Melanoma The Pathologist s Point of View
 Sentinel Node in Malignant Melanoma The Pathologist s Point of View S.J. Diaz-Cano Department of Pathology, Barts and The London School of Medicine, University of London, Barts and The London NHS Trust,
Sentinel Node in Malignant Melanoma The Pathologist s Point of View S.J. Diaz-Cano Department of Pathology, Barts and The London School of Medicine, University of London, Barts and The London NHS Trust,
11/21/13 CEA: 1.7 WNL
 Case Scenario 1 A 70 year-old white male presented to his primary care physician with a recent history of rectal bleeding. He was referred for imaging and a colonoscopy and was found to have adenocarcinoma.
Case Scenario 1 A 70 year-old white male presented to his primary care physician with a recent history of rectal bleeding. He was referred for imaging and a colonoscopy and was found to have adenocarcinoma.
Update on SLN and Melanoma: DECOG and MSLT-II. Gordon H. Hafner, MD, FACS
 Update on SLN and Melanoma: DECOG and MSLT-II Gordon H. Hafner, MD, FACS No disclosures The surgery of malignant disease is not the surgery of organs, it is of the lymphatic system. Lord Moynihan Lymph
Update on SLN and Melanoma: DECOG and MSLT-II Gordon H. Hafner, MD, FACS No disclosures The surgery of malignant disease is not the surgery of organs, it is of the lymphatic system. Lord Moynihan Lymph
Skin lesions suspicious for melanoma: New Zealand excision margin guidelines in practice
 Skin lesions suspicious for melanoma: excision margin guidelines in practice Tess Brian MBBS; 1 Michael B. Jameson MBChB, FRACP, FRCP, PhD 2,3 1 Department of Plastic and Reconstructive Surgery, Waikato
Skin lesions suspicious for melanoma: excision margin guidelines in practice Tess Brian MBBS; 1 Michael B. Jameson MBChB, FRACP, FRCP, PhD 2,3 1 Department of Plastic and Reconstructive Surgery, Waikato
Research Article Prediction of Sentinel Node Status and Clinical Outcome in a Melanoma Centre
 Skin Cancer Volume 2013, Article ID 904701, 7 pages http://dx.doi.org/10.1155/2013/904701 Research Article Prediction of Sentinel Node Status and Clinical Outcome in a Melanoma Centre Vera Teixeira, 1
Skin Cancer Volume 2013, Article ID 904701, 7 pages http://dx.doi.org/10.1155/2013/904701 Research Article Prediction of Sentinel Node Status and Clinical Outcome in a Melanoma Centre Vera Teixeira, 1
Disclosures. SLNB for Melanoma 25/02/2014 SENTINEL LYMPH NODE BIOPSY FOR MELANOMA: CURRENT GUIDELINES AND THEIR CLINICAL APPLICATION
 8 th Canadian Melanoma Conference February 22, 2014 Rimrock Resort Hotel, Banff, Alberta SENTINEL LYMPH NODE BIOPSY FOR MELANOMA: CURRENT GUIDELINES AND THEIR CLINICAL APPLICATION Christopher Bichakjian,
8 th Canadian Melanoma Conference February 22, 2014 Rimrock Resort Hotel, Banff, Alberta SENTINEL LYMPH NODE BIOPSY FOR MELANOMA: CURRENT GUIDELINES AND THEIR CLINICAL APPLICATION Christopher Bichakjian,
The pathology of bladder cancer
 1 The pathology of bladder cancer Charles Jameson Introduction Carcinoma of the bladder is the seventh most common cancer worldwide [1]. It comprises 3.2% of all cancers, with an estimated 260 000 new
1 The pathology of bladder cancer Charles Jameson Introduction Carcinoma of the bladder is the seventh most common cancer worldwide [1]. It comprises 3.2% of all cancers, with an estimated 260 000 new
Descriptor Definition Author s notes TNM descriptors Required only if applicable; select all that apply multiple foci of invasive carcinoma
 S5.01 The tumour stage and stage grouping must be recorded to the extent possible, based on the AJCC Cancer Staging Manual (7 th Edition). 11 (See Tables S5.01a and S5.01b below.) Table S5.01a AJCC breast
S5.01 The tumour stage and stage grouping must be recorded to the extent possible, based on the AJCC Cancer Staging Manual (7 th Edition). 11 (See Tables S5.01a and S5.01b below.) Table S5.01a AJCC breast
Directly Coded Summary Stage Melanoma
 Directly Coded Summary Stage Melanoma National Center for Chronic Disease Prevention and Health Promotion Division of Cancer Prevention and Control, National Program of Cancer Registries Directly Coded
Directly Coded Summary Stage Melanoma National Center for Chronic Disease Prevention and Health Promotion Division of Cancer Prevention and Control, National Program of Cancer Registries Directly Coded