What the surgeon wants from the radiologist before breast cancer surgery. Erica Patocskai Isabelle Trop
|
|
|
- Evan Kennedy
- 5 years ago
- Views:
Transcription

1 What the surgeon wants from the radiologist before breast cancer surgery Erica Patocskai Isabelle Trop Centre Hospitalier de l université de Montréal CAR, April 2013
2 Plan What is the role of MRI for breast cancer preoperative evaluation? How can radiology help in the evaluation of women treated with neoadjuvant chemotherapy? In the post-z0011 era, does it remain relevant to evaluate the axillary region?
3 A few facts Mastectomy = local excision + radiation for lesions < 2cm YES, in terms of mortality at 20 years: 41.7% local excision vs 41.2% mastectomy NO, in terms of local recurrence: 30/352 (8.5%) local excision vs 8/349 (2.3%) mastectomy (p<0.001) Ø Prognosis worse in women with late recurrence Fisher, NEJM 2002 Veronesi, NEJM 2002 Strive for complete excision of tumor with clean margins The local recurrence rate after conservative surgery is significantly lower than the rate of additional disease at MRI 10-20% additional disease vs 1.8-4% recurrence rate at 8 years Solin. JCO 2008; 26:386. Hwang. Ann Surg Oncol 2009; 16:3000.
4 A few more facts Positive margins Not uncommon Frequency depends on definition % positive margins 17% close (< 1 mm) margins 17% re-excision 33% residual tumor Kurniawan, Ann Surg Oncol 2008 With positive margins, odds of local recurrence 2.4 X é (p<0.01) Houssami. EJC 2010; 46:3219. Strive for fewer interventions with positive margins and fewer re-excisions
5 Lancet 2010 First randomized prospective study evaluating preop breast MRI 1623 women eligible for breast-conserving surgery after triple assessment (clinical, mammo and US workup) 45 centers in the United Kingdom MRI group n = 816 No MRI group n = 807 First-intention mastectomy 58 (7%) 10 (1%) Repeat tumorectomy within 6 mos 85 (10%) 90 (11 %) Overall mastectomy rate 106 (13%) 71 (9%) Overall reoperation rate at 6 mos 153 (19%) 156 (19%)
6 1. In COMICE, 38% of recommended mastectomies were false+ Suspicious lesions at MRI were not evaluated prior to surgery, surgery was widened without pathologic proof of disease. 2. The rate of re-intervention for + margins (10%) is quite low Wider surgeries were performed, diminishing the potential benefit of MRI in precisely delineating multifocal disease % of women were menopausal and 77% were 50 yo Likelihood of added benefit of MRI over MG-US is lower. 4. Radiologist-surgeon expertise issue 14% of surgeons enrolled 1-2 patients per year Rate of controlat cancer detection: 1.6%, half of expected value. Long-term benefits on recurrence rate and mortality were not evaluated Sardanelli: These results only reveal the performance of suboptimal MRI!
 Preop MRI no MRI Adjusted OR TOTAL n=3112 Initial mastectomy 16.4% 8.")
 Inf Lobular CA n=766 Initial Mastectomy 31.1% 24.9% 2.12 (p=0.008) Re-excision rate 10.9% 18.0% 0.56 (p=0.")
7 Preoperative Magnetic Resonance Imaging in Breast Cancer: Meta-Analysis of Surgical Outcomes Annals of Surgery: February : studies (2 randomized trials, 7 cohorts) Preop MRI no MRI Adjusted OR TOTAL n=3112 Initial mastectomy 16.4% 8.1% 3.06 (p<0.001) Re-excision rate 11.6% 11.4% 0.95 (p=0.71) Overall mastectomy 25.5% 18.2% 1.51 (p<0.001) Inf Lobular CA n=766 Initial Mastectomy 31.1% 24.9% 2.12 (p=0.008) Re-excision rate 10.9% 18.0% 0.56 (p=0.09) Overall mastectomy 43.0% 40.2% 1.64 (p=0.034)
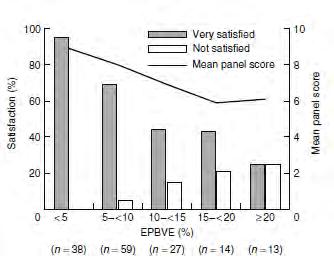
8 Optimizing use of preop MRI Added value in women with dense breast parenchyma 7% re-excision rate with preop MR vs 26% without 17% positive margins with MRI vs 53% without Added value in women yo Re-excision rates were halved from 60% to 30% with MRI Philpotts, RSNA 2011
 62 (44%) were pathology-proven malignant 81 women had Unidentified Bright Objects without correlation at ultrasound (11.")
 No malignancies after mean follow-up of 57.")
9 Prospective study of 690 women undergoing breast MRI prior to surgery 141 additional lesions in 121 women (17.5%) 62 (44%) were pathology-proven malignant 81 women had Unidentified Bright Objects without correlation at ultrasound (11.7% of population) If within 3cm of the index cancer, margins were widened 77.5% at surgery were malignant If multicentric or contralateral, MRI follow-up (n=44) No malignancies after mean follow-up of 57.1 months No change in surgical management should occur without pathologic proof Elshof, Br Ca Res Tr 2010
10 Optimizing use of preop MRI At the CHUM, preoperative MRI for Clinico-radio-path discordance Young women Dense breast parenchyma Strong family Hx Candidates for neoadjuvant chemotherapy Second-look ultrasounds/mag views as needed MRI-guided biopsies in 2012, 88 lesions/1800 MRI (4.9%)
 1985 CBC after first breast cancer EAPC = -3.07%/yr (95% CI, -3.")
 Decrease in incidence of controlateral cancer since mid-80s Decrease in locoregional recurrence with targeted")
11 Shift in breast cancer A Hazard Rate (% per year) 1985 marks introduction of Tamoxifen EAPC = 0.27%/yr (range, -0.4 to 0.9) 1985 CBC after first breast cancer EAPC = -3.07%/yr (95% CI, -3.5 to -2.7) Decrease in incidence of controlateral cancer since mid-80s Decrease in locoregional recurrence with targeted therapies Introduction of Herceptin Year of Diagnosis for First Breast Cancer Kiess. Cancer 2012; 118:1982.
12 Shift in breast cancer management Morrow. RSNA The era of effective multimodality therapy obviates the need to surgically eradicate all microscopic disease in both the breast and the axillary nodes. Outcome is largely determined by biology and the availability of targeted therapy.
13 Neoadjuvant chemotherapy HOW CAN RADIOLOGY HELP THIS SUBGROUP OF WOMEN IN THE EVALUATION OF TREATMENT RESPONSE AND SURGICAL PLANNING?
14 Neoadjuvant chemotherapy Neoadjuvant chemotherapy is used increasingly preoperatively for women with breast cancer With similar locoregional control and survival, decrease tumor bulk to allow for conservative surgery. More protocols are available Not generally recommended for tumors <2cm, strongly expressing hormonal receptors, or of low-grade. Not for ILC, DCIS Rate of complete pathologic response As high as 40-67% in her2+ subpopulations De Los Santos et al. Cancer 2013
15 Evaluation of tumor response Complete pathologic response = no residual invasive CA (+- DCIS) Must be able to correctly assess response to treatment, including DCIS, to limit the extent of surgery Clinical exam, mammo and US are imperfect for tumor assessment Ultrasound still best for lymph node evaluation Radiologic evaluation is opportunity to deploy clip at cancer site Local control 98.6% with clip, vs 91.7% without Highest sensitivity is MRI, but with limitations Oh et al. Cancer 110:
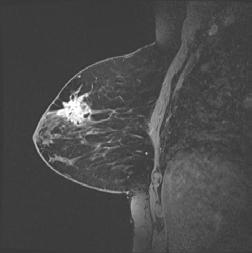
16 Assessing chemotherapy response at MRI Pre-treatment 62 yo woman. 6.1 X 5.8 cm high-grade infiltrating ductal carcinoma with 5.5 cm axillary metastasis ER- PR- her2- (Triple negative tumor). Taxol X 12; FEC X 4

.")

17 Pre-treatment Assessing chemotherapy response at MRI Partial response to treatment, with size decrease (4.6 down to 2.7 cm) for intramammary tumor, and axillary metastasis (5.8 down to 3 cm). Surgery: partial mastectomy and axillary dissection - T2 N1 disease. Post-treatment MRI correlates well with pathology size for enhancing masses. MRI s ability to evaluate for complete response better for high grade lesions

 T1 gado before treatment")
18 Assessing chemotherapy response at MRI 30 yo woman, no family history Multifocal Grade 2 infiltrating ductal carcinoma ER+ PR+ Her2- (Luminal A subtype ) T1 gado before treatment Taxol X 12; FEC X 4



19 Assessing chemotherapy response at MRI T1 gado before treatment MRI often underestimates residual disease when dealing with non-mass enhancement. T1 post chemo T1 gado post chemo Clinically, residual 3.1 X 2.6 cm mass; no palp node. At MRI: enhancing masses have resolved, spiculated mass and distortion remain. Surgery: modified radical mastectomy with skin preservation and DIEP flap. Surgical pathology revealed partial response, with discontinuous residual disease (largest IDC measuring 2 cm); 7/12 nodes +.

 Treated with AC X 4,")



20 Pre-treatment Assessing chemotherapy response at MRI 43 yo woman with 3.5 x 1.3 cm Grade 3 IDC; ER+ PR- Her2+ (Her2-enriched tumor ) Treated with AC X 4, T + H Post-treatment MRI reveals no residual enhancement, suggestive of complete response. Partial mastectomy and sentinel node performed. Final pathology revealed 2 mm residual focus of ductal carcinoma in situ, 0/3 lymph nodes MRI is limited in cases of DCIS, and for multifocal disease
21 MRI as predictor of tumor response MRI s predictive ability depends on cancer subtype, reflecting Type and Frequency of response to chemotherapy MRI appearance of tumour Radiologic complete response for NME and low-grade cancers should be interpreted with caution Management changes based on MRI will require further improvements in our ability to correctly assess for pathologic complete response at imaging Diffusion-weighted imaging Tumour bed biopsy? Sens Spec NPV PPV Accuracy Total 83% 47% 47% 83% 74% 567 women, reported by De Los Santos et al. Cancer 2013.
22 Once Imaging Complete Individualizing surgery for each woman Optimal Lumpectomy Candidates: Tumors < 5 cm, limited to one quadrant Breast size/tumor size ratio permitting lumpectomy with acceptable cosmetic result No contraindications to breast XRT Spear SL, et al. Plast Reconstr Surg 2009 Golshan M. Diseases of the Breast 2009

23
24 Surgical considerations after partial mastectomy Which women are candidates for oncoplastic reconstruction: Excision of more than 20% of breast volume Non favorable localisation (central, inferior, medial) Large breasts or important ptosis and desire reduction

25 When more than 20% excised The goal is to obliterate the residual cavity to avoid a seroma by remodeling with displacement of adjacent breast tissue Undermining of skin and separation of breast tissue from pectoral muscle & reapproximation of breast tissue

26 Musculocutaneous flap post partial mastectomy If not enough residual breast tissue available a musculocutaneous flap may be used Latissimus dorsi most frequent Preoperative imaging essential because if positive margins.very difficult problem


27 Non favorable location (Inferior)



28 Non favorable location (Inferior)



29 Partial mastectomy with reduction Images from S. Willey



30 Partial mastectomy with reduction Images from S. Willey

31 Immediate Reconstruction post Mastectomy With or without neoadjuvant chemotherapy Delayed Reconstruction

32 Immediate Reconstruction post Mastectomy The main advantage is skin preservation Delayed Reconstruction Immediate Reconstruction



33 Skin sparing mastectomy & Immediate reconstruction with expander

34 Preservation of the nipple-areola complex is becoming more widespread
35 Nipple Sparing Criteria Not Typicaly Performed after Neoadjuvant Chemotherapy Optimal Nipple-sparing mastectomy Candidates: Tumor < 3 cm Tumour at least 2 cm from the nipple-areola complex Absence of multicentricity No malignant calcifications extending to nipple-areola complex Negative intraoperative biopsy of nipple-areola complex Spear SL, et al. Plast Reconstr Surg 2009 Golshan M. Diseases of the Breast 2009
36 Axillary evaluation prior to surgery Does it remain relevant to evaluate the axillary region after the results from the ACOSOG Z11 trial have been released?
37 Until recently... Abnormal lymph node on U/S FNA & axillary dissection if + Normal lymph nodes on U/S dissection if + sentinel lymph node biopsy & axillary
38 Now Radiologists not sure when to biopsy abnormal lymph nodes Surgeons not sure when to ask for a frozen section and when to do axillary dissection Radio-oncologists now see patients with positive sentinel nodes without dissections Patients have to make important decisions based on a widely criticised trial

39 ACOSOG Z0011 Phase 3 non-inferiority trial conducted at 115 sites
40 ACOSOG Z0011 Eligible Clinical T1 T2 N0 breast cancer H&E-detected metastases in SN Lumpectomy with whole breast irradiation Adjuvant systemic therapy by choice Ineligible Clinical N1 or T3 Extracapsular extension Bilateral breast cancer Total mastectomy Preoperative chemotherapy Nodal irradiation or PBI Metastases in SN detected by IHC
41 Patient Characteristics Z11 Median age: 55 years 70% T1 tumors HR (+) >80% in both groups Equal number of patients with systemic therapy (96-7%) 58 % chemotherapy & 46% hormone therapy
42 Patient Characteristics Z11 70% had only one positive node 40% with micrometastases and 60% macrometastases
43 Results No significant difference in Locoregional Recurrence between patients treated with SLN (2.8%) or ALND (4.1%) No significant difference in Disease-Free Survival between patients treated with SLN (83.9%) or ALND (82.2%) No significant difference in Overall Survival between patients treated with SLN (92.5%) or ALND (91.8%)
44 Criticisms Mainly older ER positive patients with very favorable prognosis (how many 5 cm tumors?) 70% had only one + lymph node Don t know HER 2 status of patients How many patients HER 2+ or triple which confer a worse prognosis?
45 Methodological Shortcomings Targeted enrollment of 1900 with final analysis after 500 deaths 891 (47%) patients accrued Trial closed early because mortality rate (94 deaths) lower than expected Protocol violations (no radiotherapy in 11%, no lymph node metastasis (7% vs 11 % in SNB only) ) Analysis based on intent to treat in a trial of noninferiority
46 Methodological Shortcomings Missing data Histological grade 25% Lymphovascular invasion 25% Size of metastasis 15% Hormone receptor status 9% Lost to followup 19% (22% vs 17%)
47 Radiotherapy Details of the radiation not in database The degree to which the radiation oncologists biased the field edge superiorly to cover more of the axilla is currently undocumented It is probable that the majority of patients received adequate dose to the Level I and a portion of Level II to control microscopic disease
48 Conclusions of INESS (Institute of Excellence in Health and Social Services) Z11 does not provide sound statistical proof that omission of axillary dissection after positive sentinel node biopsy is not inferior to axillary dissection Prudence has to be applied when applying the results to patients with a more aggressive tumor who are underrepresented in z11 Young patients T2 More than 1 LN with a macrometastasis Grade 3 HER 2+ or triple
49 What we do in the CHUM (mostly)
50 Should radiologists continue to perform FNA of suspicious nodes? Yes, almost all of the time to avoid SNB Not only for T3 or N1 How do you know if the surgeon will use z11 criteria? How do you predict that patient will not request or require mastectomy (if additional foci found)? How do you predict whether the patient will not receive preoperative chemotherapy?
51 Always Follow Z11 Criteria Axillary dissection: Total mastectomy Neoadjuvant chemotherapy Partial breast radiotherapy
52 We often follow Z11 Criteria No dissection: T1/T2 One or two positive SLNs without extracapsular extension Whole-breast radiotherapy Receiving systemic therapy *Almost always when older patient with hormone receptor + disease

53 In the CHUM In patients at higher risk of locoregional recurrence the complexities of z11 are explained and informed decision is obtained «Risk-benefit ratio is patient specific»
54 What about regional node irradiation?? TRADING ONE TREATMENT FOR ANOTHER
55 What happens to all these patients that we don t dissect?? Radiooncologists generally include level 1 and 2 in their fields of treatment if no axillary dissection

56 Suggested Approach for Radiation Field with SN + but no Axillary Dissection Haffty B et al. JCO 29, 34, 2011 MD Anderson, Dana Farber, Cancer Institute of New Jersey
57 AMAROS EORTC (After Mapping of the Axilla Radiotherapy or Surgery) 4827 Total Patients Tumor < 5 cm Mastectomy or BCS Opened in 2001-ongoing SLN-Positive randomized to RT vs ALND Main objective: prove equivalent locoregional control and reduced morbidity for ART Straver et al. Ann Surg Onc & J Clin Onc 2010
58 New Trials?Abandoning SLN Sentinel node vs. Observation after axillary UltrasouND (SOUND) N=1,560 European Institute of Oncology, Milan Eligibility: <2 cm, negative preop axillary US, breast conservation Gentilini & Veronesi, Breast 2012


59 Photomosaic of 32,000 Barbies Chris Jordan, «Close encounters: facing the future» Katzen art centre, Massachusetts.
Implications of ACOSOG Z11 for Clinical Practice: Surgical Perspective
 :$;7)#*8'-87*4BCD'E7)F'31$4.$&'G$H'E7)F&'GE'>??ID >?,"'@4,$)4*,#74*8'!74/)$++'74',"$'A.,.)$'7%'()$*+,'!*42$)!7)74*67&'!3 6 August 2011 Implications of ACOSOG Z11 for Clinical
:$;7)#*8'-87*4BCD'E7)F'31$4.$&'G$H'E7)F&'GE'>??ID >?,"'@4,$)4*,#74*8'!74/)$++'74',"$'A.,.)$'7%'()$*+,'!*42$)!7)74*67&'!3 6 August 2011 Implications of ACOSOG Z11 for Clinical
Implications of ACOSOG Z11 for Clinical Practice: Surgical Perspective
 Memorial Sloan-Kettering Cancer Center 1275 York Avenue, New York, NY 10065 10th International Congress on the Future of Breast Cancer Coronado, CA 6 August 2011 Implications of ACOSOG Z11 for Clinical
Memorial Sloan-Kettering Cancer Center 1275 York Avenue, New York, NY 10065 10th International Congress on the Future of Breast Cancer Coronado, CA 6 August 2011 Implications of ACOSOG Z11 for Clinical
Why Do Axillary Dissection? Nodal Treatment and Survival NSABP B04. Revisiting Axillary Dissection for SN Positive Patients
 Memorial Sloan-Kettering Cancer Center 1275 York Avenue, New York, NY 10065 10th International Congress on the Future of Breast Cancer Coronado, CA Why Do Axillary Dissection? 6 August 2011 Implications
Memorial Sloan-Kettering Cancer Center 1275 York Avenue, New York, NY 10065 10th International Congress on the Future of Breast Cancer Coronado, CA Why Do Axillary Dissection? 6 August 2011 Implications
Surgical Therapy: Sentinel Node Biopsy and Breast Conservation
 Surgical Therapy: Sentinel Node Biopsy and Breast Conservation Stephen B. Edge, MD Professor of Surgery and Oncology Roswell Park Cancer Institute University at Buffalo Dr. Roswell Park: Tradition in Cancer
Surgical Therapy: Sentinel Node Biopsy and Breast Conservation Stephen B. Edge, MD Professor of Surgery and Oncology Roswell Park Cancer Institute University at Buffalo Dr. Roswell Park: Tradition in Cancer
Breast Imaging: Multidisciplinary Approach. Madelene Lewis, MD Assistant Professor Associate Program Director Medical University of South Carolina
 Breast Imaging: Multidisciplinary Approach Madelene Lewis, MD Assistant Professor Associate Program Director Medical University of South Carolina No Disclosures Objectives Discuss a multidisciplinary breast
Breast Imaging: Multidisciplinary Approach Madelene Lewis, MD Assistant Professor Associate Program Director Medical University of South Carolina No Disclosures Objectives Discuss a multidisciplinary breast
Debate Axillary dissection - con. Prof. Dr. Rodica Anghel Institute of Oncology Bucharest
 Debate Axillary dissection - con Prof. Dr. Rodica Anghel Institute of Oncology Bucharest Summer School of Oncology, third edition Updated Oncology 2015: State of the Art News & Challenging Topics Bucharest,
Debate Axillary dissection - con Prof. Dr. Rodica Anghel Institute of Oncology Bucharest Summer School of Oncology, third edition Updated Oncology 2015: State of the Art News & Challenging Topics Bucharest,
Breast Surgery When Less is More and More is Less. E MacIntosh, MD June 6, 2015
 Breast Surgery When Less is More and More is Less E MacIntosh, MD June 6, 2015 Presenter Disclosure Faculty: E. MacIntosh Relationships with commercial interests: None Mitigating Potential Bias Not applicable
Breast Surgery When Less is More and More is Less E MacIntosh, MD June 6, 2015 Presenter Disclosure Faculty: E. MacIntosh Relationships with commercial interests: None Mitigating Potential Bias Not applicable
16/09/2015. ACOSOG Z011 changing practice. Presentation outline. Nodal mets #1 prognostic tool. Less surgery no change in oncologic outcomes
 ACOSOG Z011 changing practice The end of axillary US/FNA? Preoperative staging of the axilla in the era of Z011 Adena S Scheer MD MSc FRCSC Surgical Oncologist, St. Michael s Hospital Assistant Professor,
ACOSOG Z011 changing practice The end of axillary US/FNA? Preoperative staging of the axilla in the era of Z011 Adena S Scheer MD MSc FRCSC Surgical Oncologist, St. Michael s Hospital Assistant Professor,
BREAST MRI. Elizabeth A. Rafferty, M.D. Avon Comprehensive Breast Center Massachusetts General Hospital Harvard Medical School
 BREAST MRI Elizabeth A. Rafferty, M.D. Avon Comprehensive Breast Center Massachusetts General Hospital Harvard Medical School BREAST MRI Any assessment of the breast parenchyma requires the administration
BREAST MRI Elizabeth A. Rafferty, M.D. Avon Comprehensive Breast Center Massachusetts General Hospital Harvard Medical School BREAST MRI Any assessment of the breast parenchyma requires the administration
The Role of Sentinel Lymph Node Biopsy and Axillary Dissection
 The Role of Sentinel Lymph Node Biopsy and Axillary Dissection Henry Mark Kuerer, MD, PhD, FACS Department of Surgical Oncology University of Texas MD Anderson Cancer Center SLN Biopsy Revolutionized surgical
The Role of Sentinel Lymph Node Biopsy and Axillary Dissection Henry Mark Kuerer, MD, PhD, FACS Department of Surgical Oncology University of Texas MD Anderson Cancer Center SLN Biopsy Revolutionized surgical
Radiotherapy Implications of ACOSOG Z-11 for Clinical Practice. Julia White, MD Professor of Radiation Oncology Medical College of Wisconsin
 1 Radiotherapy Implications of ACOSOG Z-11 for Clinical Practice Julia White, MD Professor of Radiation Oncology Medical College of Wisconsin Disclosures: none Agenda 1. ACOSOG Z-11: Another perspective
1 Radiotherapy Implications of ACOSOG Z-11 for Clinical Practice Julia White, MD Professor of Radiation Oncology Medical College of Wisconsin Disclosures: none Agenda 1. ACOSOG Z-11: Another perspective
Recent Update in Surgery for the Management of Breast Cancer
 Recent Update in Surgery for the Management of Breast Cancer Wonshik Han, MD, PhD Professor, Department of Surgery, Seoul National University College of Medicine Chief of Breast Care Center, Seoul National
Recent Update in Surgery for the Management of Breast Cancer Wonshik Han, MD, PhD Professor, Department of Surgery, Seoul National University College of Medicine Chief of Breast Care Center, Seoul National
BREAST MRI. Elizabeth A. Rafferty, M.D. Avon Comprehensive Breast Center Massachusetts General Hospital Harvard Medical School
 BREAST MRI Elizabeth A. Rafferty, M.D. Avon Comprehensive Breast Center Massachusetts General Hospital Harvard Medical School BREAST MRI Any assessment of the breast parenchyma requires the administration
BREAST MRI Elizabeth A. Rafferty, M.D. Avon Comprehensive Breast Center Massachusetts General Hospital Harvard Medical School BREAST MRI Any assessment of the breast parenchyma requires the administration
Advances in Breast Surgery. Catherine Campo, D.O. Breast Surgeon Meridian Health System April 17, 2015
 Advances in Breast Surgery Catherine Campo, D.O. Breast Surgeon Meridian Health System April 17, 2015 Objectives Understand the surgical treatment of breast cancer Be able to determine when a lumpectomy
Advances in Breast Surgery Catherine Campo, D.O. Breast Surgeon Meridian Health System April 17, 2015 Objectives Understand the surgical treatment of breast cancer Be able to determine when a lumpectomy
When do you need PET/CT or MRI in early breast cancer?
 When do you need PET/CT or MRI in early breast cancer? Elizabeth A. Morris MD FACR Chief, Breast Imaging Service Memorial Sloan-Kettering Cancer Center NY, NY Objectives What is the role of MRI in initial
When do you need PET/CT or MRI in early breast cancer? Elizabeth A. Morris MD FACR Chief, Breast Imaging Service Memorial Sloan-Kettering Cancer Center NY, NY Objectives What is the role of MRI in initial
Surgical Advances in the Treatment of Breast Cancer. Laura Kruper, MD, MSCE Chief, Breast Surgery
 Surgical Advances in the Treatment of Breast Cancer Laura Kruper, MD, MSCE Chief, Breast Surgery Nothing to disclose DISCLOSURE LESS IS MORE Radiation Lymph nodes Reconstruction Less is More! Radiation
Surgical Advances in the Treatment of Breast Cancer Laura Kruper, MD, MSCE Chief, Breast Surgery Nothing to disclose DISCLOSURE LESS IS MORE Radiation Lymph nodes Reconstruction Less is More! Radiation
Advances in Localized Breast Cancer
 Advances in Localized Breast Cancer Melissa Camp, MD, MPH and Fariba Asrari, MD June 18, 2018 Moderated by Elissa Bantug 1 Advances in Surgery for Breast Cancer Melissa Camp, MD June 18, 2018 2 Historical
Advances in Localized Breast Cancer Melissa Camp, MD, MPH and Fariba Asrari, MD June 18, 2018 Moderated by Elissa Bantug 1 Advances in Surgery for Breast Cancer Melissa Camp, MD June 18, 2018 2 Historical
Position Statement on Management of the Axilla in Patients with Invasive Breast Cancer
 - Official Statement - Position Statement on Management of the Axilla in Patients with Invasive Breast Cancer Sentinel lymph node (SLN) biopsy has replaced axillary lymph node dissection (ALND) for the
- Official Statement - Position Statement on Management of the Axilla in Patients with Invasive Breast Cancer Sentinel lymph node (SLN) biopsy has replaced axillary lymph node dissection (ALND) for the
Results of the ACOSOG Z0011 Trial
 DCIS and Early Breast Cancer Symposium JUNE 15-17 2012 CAPPADOCIA Results of the ACOSOG Z0011 Trial Kelly K. Hunt, M.D. Professor of Surgery Axillary Node Dissection Staging, Regional control, Survival
DCIS and Early Breast Cancer Symposium JUNE 15-17 2012 CAPPADOCIA Results of the ACOSOG Z0011 Trial Kelly K. Hunt, M.D. Professor of Surgery Axillary Node Dissection Staging, Regional control, Survival
Sentinel Lymph Node Biopsy for Breast Cancer
 Sentinel Lymph Node Biopsy for Breast Cancer Registrar Tutorial Adam Cichowitz Surgical Registrar The Royal Melbourne Hospital Sentinel Lymph Node Biopsy Axillary LN status important prognostic factor
Sentinel Lymph Node Biopsy for Breast Cancer Registrar Tutorial Adam Cichowitz Surgical Registrar The Royal Melbourne Hospital Sentinel Lymph Node Biopsy Axillary LN status important prognostic factor
Ductal Carcinoma-in-Situ: New Concepts and Controversies
 Ductal Carcinoma-in-Situ: New Concepts and Controversies James J. Stark, MD, FACP Medical Director, Cancer Program and Palliative Care Maryview Medical Center Professor of Medicine, EVMS Case Presentation
Ductal Carcinoma-in-Situ: New Concepts and Controversies James J. Stark, MD, FACP Medical Director, Cancer Program and Palliative Care Maryview Medical Center Professor of Medicine, EVMS Case Presentation
Surgical Issues in Neoadjuvant Chemotherapy
 14 th Bossche Mamma Congress Ruwenbergstraat 7 5271 AG Sint Michielsgestel June 14, 2016 Surgical Issues in Neoadjuvant Chemotherapy Tari A. King MD FACS Chief, Breast Surgery Dana Farber/Brigham and Women
14 th Bossche Mamma Congress Ruwenbergstraat 7 5271 AG Sint Michielsgestel June 14, 2016 Surgical Issues in Neoadjuvant Chemotherapy Tari A. King MD FACS Chief, Breast Surgery Dana Farber/Brigham and Women
Breast Cancer. Most common cancer among women in the US. 2nd leading cause of death in women. Mortality rates though have declined
 Breast Cancer Most common cancer among women in the US 2nd leading cause of death in women Mortality rates though have declined 1 in 8 women will develop breast cancer Breast Cancer Breast cancer increases
Breast Cancer Most common cancer among women in the US 2nd leading cause of death in women Mortality rates though have declined 1 in 8 women will develop breast cancer Breast Cancer Breast cancer increases
How to Use MRI Following Neoadjuvant Chemotherapy (NAC) in Locally Advanced Breast Cancer
 in Locally Advanced Breast Cancer") Global Breast Cancer Conference 2016 & 5 th International Breast Cancer Symposium April 29 th 2016, 09:40-10:50 How to Use MRI Following Neoadjuvant Chemotherapy (NAC) in Locally Advanced Breast Cancer
Global Breast Cancer Conference 2016 & 5 th International Breast Cancer Symposium April 29 th 2016, 09:40-10:50 How to Use MRI Following Neoadjuvant Chemotherapy (NAC) in Locally Advanced Breast Cancer
Breast Cancer. Saima Saeed MD
 Breast Cancer Saima Saeed MD Breast Cancer Most common cancer among women in the US 2nd leading cause of death in women 1 in 8 women will develop breast cancer Incidence/mortality rates have declined Breast
Breast Cancer Saima Saeed MD Breast Cancer Most common cancer among women in the US 2nd leading cause of death in women 1 in 8 women will develop breast cancer Incidence/mortality rates have declined Breast
Surgical Considerations in Breast Cancer treated with Neoadjuvant Therapy
 Surgical Considerations in Breast Cancer treated with Neoadjuvant Therapy Rebecca Warburton MD Department of Surgery, University of British Columbia Mount Saint Joseph Hospital, Providence Health Care
Surgical Considerations in Breast Cancer treated with Neoadjuvant Therapy Rebecca Warburton MD Department of Surgery, University of British Columbia Mount Saint Joseph Hospital, Providence Health Care
Breast Cancer: Management of the Axilla in Greg McKinnon MD FRCSC SON Vancouver Oct 2016
 Breast Cancer: Management of the Axilla in 2016 Greg McKinnon MD FRCSC SON Vancouver Oct 2016 No Disclosures Principle #1 There is no point talking about surgical therapy in isolation. From a patient
Breast Cancer: Management of the Axilla in 2016 Greg McKinnon MD FRCSC SON Vancouver Oct 2016 No Disclosures Principle #1 There is no point talking about surgical therapy in isolation. From a patient
ANNEX 1 OBJECTIVES. At the completion of the training period, the fellow should be able to:
 1 ANNEX 1 OBJECTIVES At the completion of the training period, the fellow should be able to: 1. Breast Surgery Evaluate and manage common benign and malignant breast conditions. Assess the indications
1 ANNEX 1 OBJECTIVES At the completion of the training period, the fellow should be able to: 1. Breast Surgery Evaluate and manage common benign and malignant breast conditions. Assess the indications
Sentinel Node Biopsy. Is There Any Role for Axillary Dissection? JCCNB Nov 20, Stephen B. Edge, MD
 Sentinel Node Biopsy Is There Any Role for Axillary Dissection? JCCNB Nov 20, 2010 Tokyo, Japan Stephen B. Edge, MD Roswell Park Cancer Institute University at Buffalo Buffalo, NY USA SNB with Clinically
Sentinel Node Biopsy Is There Any Role for Axillary Dissection? JCCNB Nov 20, 2010 Tokyo, Japan Stephen B. Edge, MD Roswell Park Cancer Institute University at Buffalo Buffalo, NY USA SNB with Clinically
Evolution of Breast Surgery
 Evolution of Breast Surgery Natasha Rueth MD Surgical Oncologist Piper Breast Center and Alina Health Surgical Specialists Minneapolis, MN Definitions Radical Mastectomy: Removal of breast, chest muscles,
Evolution of Breast Surgery Natasha Rueth MD Surgical Oncologist Piper Breast Center and Alina Health Surgical Specialists Minneapolis, MN Definitions Radical Mastectomy: Removal of breast, chest muscles,
Page 1. AHN-JHU Breast Cancer Symposium. Novel Local Regional Clinical Trials. Background. Neoadjuvant Chemotherapy Benefit.
 AHN-JHU Breast Cancer Symposium Novel Local Regional Clinical Trials March 22, 2019 Thomas B. Julian, MD, FACS Associate Medical Director, Cancer Program Development, ANH Cancer Institute Background In
AHN-JHU Breast Cancer Symposium Novel Local Regional Clinical Trials March 22, 2019 Thomas B. Julian, MD, FACS Associate Medical Director, Cancer Program Development, ANH Cancer Institute Background In
Neoadjuvant Treatment of. of Radiotherapy
 Neoadjuvant Treatment of Breast Cancer: Role of Radiotherapy Neoadjuvant Chemotherapy Many new questions for radiation oncology? lack of path stage to guide indications should treatment response affect
Neoadjuvant Treatment of Breast Cancer: Role of Radiotherapy Neoadjuvant Chemotherapy Many new questions for radiation oncology? lack of path stage to guide indications should treatment response affect
Ultrasound or FNA for Predicting Node Positive in Breast Cancer
 Ultrasound or FNA for Predicting Node Positive in Breast Cancer Chiun Sheng Huang, MD, PhD, MPH Professor and Chairman Department of Surgery Director of Breast Care Center National Taiwan University Hospital
Ultrasound or FNA for Predicting Node Positive in Breast Cancer Chiun Sheng Huang, MD, PhD, MPH Professor and Chairman Department of Surgery Director of Breast Care Center National Taiwan University Hospital
The Challenge of Individualizing Loco-Regional Treatments for Patients with Localized Breast Cancer
 The Challenge of Individualizing Loco-Regional Treatments for Patients with Localized Breast Cancer Le défi des traitements locorégionaux individualisés pour les patientes présentant un cancer du sein
The Challenge of Individualizing Loco-Regional Treatments for Patients with Localized Breast Cancer Le défi des traitements locorégionaux individualisés pour les patientes présentant un cancer du sein
Evaluation of the Axilla Post Z-0011 Trial New Paradigm
 Evaluation of the Axilla Post Z-0011 Trial New Paradigm Belinda Curpen, MD, FRCPC; Tetyana Dushenkovska; Mia Skarpathiotakis MD, FRCPC; Carrie Betel, MD, FRCPC; Kalesha Hack, MD, FRCPC; Lara Richmond,
Evaluation of the Axilla Post Z-0011 Trial New Paradigm Belinda Curpen, MD, FRCPC; Tetyana Dushenkovska; Mia Skarpathiotakis MD, FRCPC; Carrie Betel, MD, FRCPC; Kalesha Hack, MD, FRCPC; Lara Richmond,
Case Scenario 1 History and Physical 3/15/13 Imaging Pathology
 Case Scenario 1 History and Physical 3/15/13 The patient is an 84 year old white female who presented with an abnormal mammogram. The patient has a five year history of refractory anemia with ringed sideroblasts
Case Scenario 1 History and Physical 3/15/13 The patient is an 84 year old white female who presented with an abnormal mammogram. The patient has a five year history of refractory anemia with ringed sideroblasts
Radiotherapy Management of Breast Cancer Treated with Neoadjuvant Chemotherapy. Julia White MD Professor, Radiation Oncology
 Radiotherapy Management of Breast Cancer Treated with Neoadjuvant Chemotherapy Julia White MD Professor, Radiation Oncology Agenda Efficacy of radiotherapy in the management of breast cancer in the Adjuvant
Radiotherapy Management of Breast Cancer Treated with Neoadjuvant Chemotherapy Julia White MD Professor, Radiation Oncology Agenda Efficacy of radiotherapy in the management of breast cancer in the Adjuvant
Evaluating the Z011 study and how local-regional therapy for early breast cancer may change
 Evaluating the Z011 study and how local-regional therapy for early breast cancer may change Karen Hoffman, M.D., M.H.Sc., M.P.H. Dept of Radiation Oncology The University of Texas MD Anderson Cancer Center
Evaluating the Z011 study and how local-regional therapy for early breast cancer may change Karen Hoffman, M.D., M.H.Sc., M.P.H. Dept of Radiation Oncology The University of Texas MD Anderson Cancer Center
Balancing Evidence and Clinical Practice in the Treatment of Localized Breast Cancer May 5, 2006
 Balancing Evidence and Clinical Practice in the Treatment of Localized Breast Cancer May 5, 2006 Deborah Hamolsky MS, RN : DCIS Carol Franc Buck Breast Care Center UCSF Comprehensive Cancer Center Jane
Balancing Evidence and Clinical Practice in the Treatment of Localized Breast Cancer May 5, 2006 Deborah Hamolsky MS, RN : DCIS Carol Franc Buck Breast Care Center UCSF Comprehensive Cancer Center Jane
Targeting Surgery for Known Axillary Disease. Abigail Caudle, MD Henry Kuerer, MD PhD Dept. Surgical Oncology MD Anderson Cancer Center
 Targeting Surgery for Known Axillary Disease Abigail Caudle, MD Henry Kuerer, MD PhD Dept. Surgical Oncology MD Anderson Cancer Center Nodal Ultrasound at Diagnosis Whole breast and draining lymphatic
Targeting Surgery for Known Axillary Disease Abigail Caudle, MD Henry Kuerer, MD PhD Dept. Surgical Oncology MD Anderson Cancer Center Nodal Ultrasound at Diagnosis Whole breast and draining lymphatic
CURRENT CONTROVERSIES IN BREAST CANCER SURGERY Less or more!?
 CURRENT CONTROVERSIES IN BREAST CANCER SURGERY Less or more!? I have no Disclosures Wolfgang Gatzemeier Breast Unit Milan, Italy 17th ESO-ESMO- EONS Masterclass in Clinical Oncology 24-29 MARCH 2018 Optimal
CURRENT CONTROVERSIES IN BREAST CANCER SURGERY Less or more!? I have no Disclosures Wolfgang Gatzemeier Breast Unit Milan, Italy 17th ESO-ESMO- EONS Masterclass in Clinical Oncology 24-29 MARCH 2018 Optimal
Is Complete Axillary Dissection Needed Following Mastectomy and Sentinel Node Biopsy for N1 disease?
 Is Complete Axillary Dissection Needed Following Mastectomy and Sentinel Node Biopsy for N1 disease? Mylin A. Torres, MD Director, Glenn Family Breast Center Louis and Rand Glenn Family Chair in Breast
Is Complete Axillary Dissection Needed Following Mastectomy and Sentinel Node Biopsy for N1 disease? Mylin A. Torres, MD Director, Glenn Family Breast Center Louis and Rand Glenn Family Chair in Breast
EVALUATION OF AXILLARY LYMPH NODES AFTER NEOADJUVANT SYSTEMIC THERAPY KIM, MIN JUNG SEVERANCE HOSPITAL, YONSEI UNIVERSITY
 EVALUATION OF AXILLARY LYMPH NODES AFTER NEOADJUVANT SYSTEMIC THERAPY KIM, MIN JUNG SEVERANCE HOSPITAL, YONSEI UNIVERSITY AXILLARY LYMPH NODE METASTASIS Axillary lymph node metastasis is one of the most
EVALUATION OF AXILLARY LYMPH NODES AFTER NEOADJUVANT SYSTEMIC THERAPY KIM, MIN JUNG SEVERANCE HOSPITAL, YONSEI UNIVERSITY AXILLARY LYMPH NODE METASTASIS Axillary lymph node metastasis is one of the most
Oncoplastic breast surgery in a Danish perspective II: Reconstructive strategy in oncoplastic breast surgery
 Oncoplastic breast surgery in a Danish perspective II: Reconstructive strategy in oncoplastic breast surgery Michael Rose, MD Department of Surgery and Plastic Surgery, Hospital of Southwest Jutland, Denmark
Oncoplastic breast surgery in a Danish perspective II: Reconstructive strategy in oncoplastic breast surgery Michael Rose, MD Department of Surgery and Plastic Surgery, Hospital of Southwest Jutland, Denmark
Prophylactic Mastectomy State of the Art
 Memorial Sloan-Kettering Cancer Center 1275 York Avenue, New York, NY 10065 6 th Brazilian Breast Cancer Conference Sao Paulo, Brazil 9 March 2012 Prophylactic Mastectomy State of the Art Monica Morrow
Memorial Sloan-Kettering Cancer Center 1275 York Avenue, New York, NY 10065 6 th Brazilian Breast Cancer Conference Sao Paulo, Brazil 9 March 2012 Prophylactic Mastectomy State of the Art Monica Morrow
Surgical Management of the Axilla
 Surgical Management of the Axilla Jean-Francois Boileau, MD, MSc, FRCSC Surgical Oncologist, Montreal Jewish General Hospital Segal Cancer Centre Associate Member, Department of Oncology, McGill University
Surgical Management of the Axilla Jean-Francois Boileau, MD, MSc, FRCSC Surgical Oncologist, Montreal Jewish General Hospital Segal Cancer Centre Associate Member, Department of Oncology, McGill University
Evolution of Regional Nodal Management of Breast Cancer
 Evolution of Regional Nodal Management of Breast Cancer Bruce G. Haffty, MD Director (Interim) Rutgers Cancer Institute of New Jersey Professor and Chair Department of Radiation Oncology Rutgers, The State
Evolution of Regional Nodal Management of Breast Cancer Bruce G. Haffty, MD Director (Interim) Rutgers Cancer Institute of New Jersey Professor and Chair Department of Radiation Oncology Rutgers, The State
Breast Cancer. Dr. Andres Wiernik 2017
 Breast Cancer Dr. Andres Wiernik 2017 Agenda: The Facts! (Epidemiology/Risk Factors) Biological Classification/Phenotypes of Breast Cancer Treatment approach Local Systemic Agenda: The Facts! (Epidemiology/Risk
Breast Cancer Dr. Andres Wiernik 2017 Agenda: The Facts! (Epidemiology/Risk Factors) Biological Classification/Phenotypes of Breast Cancer Treatment approach Local Systemic Agenda: The Facts! (Epidemiology/Risk
Principles of breast radiation therapy
 ANZ 1601/BIG 16-02 EXPERT ESMO Preceptorship Program 2017 Principles of breast radiation therapy Boon H Chua Professor Director of Cancer and Haematology Services UNSW Sydney and Prince of Wales Hospital
ANZ 1601/BIG 16-02 EXPERT ESMO Preceptorship Program 2017 Principles of breast radiation therapy Boon H Chua Professor Director of Cancer and Haematology Services UNSW Sydney and Prince of Wales Hospital
BREAST CONSERVATION TREATMENT IN EARLY STAGE DISEASE AND DCIS LAWRENCE J. SOLIN, MD, FACR, FASTRO
 BREAST CONSERVATION TREATMENT IN EARLY STAGE DISEASE AND DCIS LAWRENCE J. SOLIN, MD, FACR, FASTRO Chairman Department of Radiation Oncology Albert Einstein Medical Center Philadelphia, PA Professor (Adjunct)
BREAST CONSERVATION TREATMENT IN EARLY STAGE DISEASE AND DCIS LAWRENCE J. SOLIN, MD, FACR, FASTRO Chairman Department of Radiation Oncology Albert Einstein Medical Center Philadelphia, PA Professor (Adjunct)
The Case FOR Oncoplastic Surgery in Small Breasts. Barbara L. Smith, MD, PhD Massachusetts General Hospital Harvard Medical School Boston, MA USA
 The Case FOR Oncoplastic Surgery in Small Breasts Barbara L. Smith, MD, PhD Massachusetts General Hospital Harvard Medical School Boston, MA USA Changing issues in breast cancer management Early detection
The Case FOR Oncoplastic Surgery in Small Breasts Barbara L. Smith, MD, PhD Massachusetts General Hospital Harvard Medical School Boston, MA USA Changing issues in breast cancer management Early detection
Surgery for Breast Cancer
 Surgery for Breast Cancer 1750 Mastectomy - Petit 1894 Radical mastectomy Halsted Extended, Super radical mastectomy 1948 Modified radical mastectomy Patey 1950-60 WLE & RT Baclesse, Mustakallio 1981-85
Surgery for Breast Cancer 1750 Mastectomy - Petit 1894 Radical mastectomy Halsted Extended, Super radical mastectomy 1948 Modified radical mastectomy Patey 1950-60 WLE & RT Baclesse, Mustakallio 1981-85
Practice of Axilla Surgery
 Summer School of Breast Disease 2016 Practice of Axilla Surgery Axillary Lymph Node Dissection & Sentinel Lymph Node Biopsy 연세의대외과 박세호 Contents Anatomy of the axilla Axillary lymph node dissection (ALND)
Summer School of Breast Disease 2016 Practice of Axilla Surgery Axillary Lymph Node Dissection & Sentinel Lymph Node Biopsy 연세의대외과 박세호 Contents Anatomy of the axilla Axillary lymph node dissection (ALND)
Relevance. Axillary Node Recurrence. Purpose. Case Presentation: Is axillary staging required? Two trends have emerged:
 Axillary Node Recurrence N.L. Davis Associate Professor of Surgery, UBC Head of Surgical Oncology, BCCA Relevance In an attempt to minimize long term complications and to maximize cancer control, the management
Axillary Node Recurrence N.L. Davis Associate Professor of Surgery, UBC Head of Surgical Oncology, BCCA Relevance In an attempt to minimize long term complications and to maximize cancer control, the management
ROLE OF MRI IN SCREENING, DIAGNOSIS AND MANAGEMENT OF BREAST CANCER. B.Zandi Professor of Radiology
 ROLE OF MRI IN SCREENING, DIAGNOSIS AND MANAGEMENT OF BREAST CANCER B.Zandi Professor of Radiology Introduction In the USA, Breast Cancer is : The Most Common Non-Skin Cancer The Second Leading cause of
ROLE OF MRI IN SCREENING, DIAGNOSIS AND MANAGEMENT OF BREAST CANCER B.Zandi Professor of Radiology Introduction In the USA, Breast Cancer is : The Most Common Non-Skin Cancer The Second Leading cause of
Breast cancer reconstruction surgery (immediate and delayed) across Ontario: Patient indications and appropriate surgical options
 across Ontario: Patient indications and appropriate surgical options") A Quality Initiative of the Program in Evidence-Based Care (PEBC), Cancer Care Ontario (CCO) Breast cancer reconstruction surgery (immediate and delayed) across Ontario: Patient indications and appropriate
A Quality Initiative of the Program in Evidence-Based Care (PEBC), Cancer Care Ontario (CCO) Breast cancer reconstruction surgery (immediate and delayed) across Ontario: Patient indications and appropriate
BREAST CANCER SURGERY. Dr. John H. Donohue
 Dr. John H. Donohue HISTORY References to breast surgery in ancient Egypt (ca 3000 BCE) Mastectomy described in numerous medieval texts Petit formulated organized approach in 18 th Century Improvements
Dr. John H. Donohue HISTORY References to breast surgery in ancient Egypt (ca 3000 BCE) Mastectomy described in numerous medieval texts Petit formulated organized approach in 18 th Century Improvements
Case Scenario 1. 2/15/2011 The patient received IMRT 45 Gy at 1.8 Gy per fraction for 25 fractions.
 Case Scenario 1 1/3/11 A 57 year old white female presents for her annual mammogram and is found to have a suspicious area of calcification, spread out over at least 4 centimeters. She is scheduled to
Case Scenario 1 1/3/11 A 57 year old white female presents for her annual mammogram and is found to have a suspicious area of calcification, spread out over at least 4 centimeters. She is scheduled to
Breast Health. Program Objectives. Facts About Breast Cancer in the United States
 Breast Health Meridian Cancer Care Yolanda Tammaro, M.D. Meridian Medical Group- Specialty Care Breast Surgery, Ocean Medical Center Program Objectives Participants will: Learn some basic breast cancer
Breast Health Meridian Cancer Care Yolanda Tammaro, M.D. Meridian Medical Group- Specialty Care Breast Surgery, Ocean Medical Center Program Objectives Participants will: Learn some basic breast cancer
Resection Margins in Breast Conserving Surgery. Alberto Costa, MD Canton Ticino Breast Unit Lugano, Switzerland
 Resection Margins in Breast Conserving Surgery Alberto Costa, MD Canton Ticino Breast Unit Lugano, Switzerland Breast Conserving Surgery 1 Probably one of the most important innovation in cancer surgery
Resection Margins in Breast Conserving Surgery Alberto Costa, MD Canton Ticino Breast Unit Lugano, Switzerland Breast Conserving Surgery 1 Probably one of the most important innovation in cancer surgery
BREAST CONSERVATION TREATMENT IN EARLY STAGE DISEASE AND DCIS LAWRENCE J. SOLIN, MD, FACR, FASTRO
 BREAST CONSERVATION TREATMENT IN EARLY STAGE DISEASE AND DCIS LAWRENCE J. SOLIN, MD, FACR, FASTRO Chairman Department of Radiation Oncology Albert Einstein Healthcare Network Philadelphia, PA Professor
BREAST CONSERVATION TREATMENT IN EARLY STAGE DISEASE AND DCIS LAWRENCE J. SOLIN, MD, FACR, FASTRO Chairman Department of Radiation Oncology Albert Einstein Healthcare Network Philadelphia, PA Professor
M D..,., M. M P.. P H., H, F. F A.. A C..S..
 Implications of NSABP B-32 and Loco-Regional Therapy Considerations After Neoadjuvant Chemotherapy Terry Mamounas, M.D., M.P.H, F.A.C.S. Professor of Surgery Northeastern Ohio Medical University Medical
Implications of NSABP B-32 and Loco-Regional Therapy Considerations After Neoadjuvant Chemotherapy Terry Mamounas, M.D., M.P.H, F.A.C.S. Professor of Surgery Northeastern Ohio Medical University Medical
Surgical Considera0ons with Neoadjuvant Treatment in Breast Cancer
 Surgical Considera0ons with Neoadjuvant Treatment in Breast Cancer David R McCready MD MSc FRCSC FACS GaAuso Chair in Breast Surgical Oncology Professor of Surgery, University of Toronto Princess Margaret
Surgical Considera0ons with Neoadjuvant Treatment in Breast Cancer David R McCready MD MSc FRCSC FACS GaAuso Chair in Breast Surgical Oncology Professor of Surgery, University of Toronto Princess Margaret
What is Cancer? Petra Ketterl, MD Medical Oncology and Functional Medicine
 What is Cancer? Petra Ketterl, MD Medical Oncology and Functional Medicine What is Cancer? Layman s terms: cancer starts when cells grow out of control (in any place in the body) and crowd out normal cells
What is Cancer? Petra Ketterl, MD Medical Oncology and Functional Medicine What is Cancer? Layman s terms: cancer starts when cells grow out of control (in any place in the body) and crowd out normal cells
Feasibility of Preoperative Axillary Lymph Node Marking with a Clip in Breast Cancer Patients before Neoadjuvant Chemotherapy: A Preliminary Study
 [ABS-0078] GBCC 2018 Feasibility of Preoperative Axillary Lymph Node Marking with a Clip in Breast Cancer Patients before Neoadjuvant Chemotherapy: A Preliminary Study Eun Young Kim 1, Kwan Ho Lee 1, Yong
[ABS-0078] GBCC 2018 Feasibility of Preoperative Axillary Lymph Node Marking with a Clip in Breast Cancer Patients before Neoadjuvant Chemotherapy: A Preliminary Study Eun Young Kim 1, Kwan Ho Lee 1, Yong
RADIOTHERAPY IN BREAST CANCER :
 RADIOTHERAPY IN BREAST CANCER : PAST, PRESENT, FUTURE Dr Jyotirup Goswami Consultant Radiation Oncologist Narayana Cancer Institute Narayana Superspecialty Hospital Breast cancer is the classic paradigm
RADIOTHERAPY IN BREAST CANCER : PAST, PRESENT, FUTURE Dr Jyotirup Goswami Consultant Radiation Oncologist Narayana Cancer Institute Narayana Superspecialty Hospital Breast cancer is the classic paradigm
Lessons Learnt from Neoadjuvant Hormone Therapy. 10 Lessons Learnt from Neoadjuvant Endocrine Therapy. Lesson 1
 Lessons Learnt from Neoadjuvant Hormone Therapy Mike Dixon Clinical Director Breakthrough Research Unit Edinburgh 10 Lessons Learnt from Neoadjuvant Endocrine Therapy 10 Lessons Learnt from Neoadjuvant
Lessons Learnt from Neoadjuvant Hormone Therapy Mike Dixon Clinical Director Breakthrough Research Unit Edinburgh 10 Lessons Learnt from Neoadjuvant Endocrine Therapy 10 Lessons Learnt from Neoadjuvant
Lessons Learnt from Neoadjuvant Hormone Therapy. Mike Dixon Clinical Director Breakthrough Research Unit Edinburgh
 Lessons Learnt from Neoadjuvant Hormone Therapy Mike Dixon Clinical Director Breakthrough Research Unit Edinburgh 10 Lessons Learnt from Neoadjuvant Endocrine Therapy 10 Lessons Learnt from Neoadjuvant
Lessons Learnt from Neoadjuvant Hormone Therapy Mike Dixon Clinical Director Breakthrough Research Unit Edinburgh 10 Lessons Learnt from Neoadjuvant Endocrine Therapy 10 Lessons Learnt from Neoadjuvant
How can surgeons help the Radiation Oncologists?
 How can surgeons help the Radiation Oncologists? Lorna Weir BC Surgical Oncology fall breast cancer update Oct 24, 2009 Disclosure no conflict of interest Outline Introduction OR reports Marking of surgical
How can surgeons help the Radiation Oncologists? Lorna Weir BC Surgical Oncology fall breast cancer update Oct 24, 2009 Disclosure no conflict of interest Outline Introduction OR reports Marking of surgical
Recurrence following Treatment of Ductal Carcinoma in Situ with Skin-Sparing Mastectomy and Immediate Breast Reconstruction
 Recurrence following Treatment of Ductal Carcinoma in Situ with Skin-Sparing Mastectomy and Immediate Breast Reconstruction Aldona J. Spiegel, M.D., and Charles E. Butler, M.D. Houston, Texas Skin-sparing
Recurrence following Treatment of Ductal Carcinoma in Situ with Skin-Sparing Mastectomy and Immediate Breast Reconstruction Aldona J. Spiegel, M.D., and Charles E. Butler, M.D. Houston, Texas Skin-sparing
Applicability of the ACOSOG Z0011 Criteria in Women with High-Risk Node-Positive Breast Cancer Undergoing Breast Conserving Surgery
 Ann Surg Oncol (2015) 22:1128 1132 DOI 10.1245/s10434-014-4090-y ORIGINAL ARTICLE BREAST ONCOLOGY Applicability of the ACOSOG Z0011 Criteria in Women with High-Risk Node-Positive Breast Cancer Undergoing
Ann Surg Oncol (2015) 22:1128 1132 DOI 10.1245/s10434-014-4090-y ORIGINAL ARTICLE BREAST ONCOLOGY Applicability of the ACOSOG Z0011 Criteria in Women with High-Risk Node-Positive Breast Cancer Undergoing
Repeating Conservative Surgery after Ipsilateral Breast Tumor Reappearance: Criteria for Selecting the Best Candidates
 Ann Surg Oncol (2012) 19:3771 3776 DOI 10.1245/s10434-012-2404-5 ORIGINAL ARTICLE BREAST ONCOLOGY Repeating Conservative Surgery after Ipsilateral Breast Tumor Reappearance: Criteria for Selecting the
Ann Surg Oncol (2012) 19:3771 3776 DOI 10.1245/s10434-012-2404-5 ORIGINAL ARTICLE BREAST ONCOLOGY Repeating Conservative Surgery after Ipsilateral Breast Tumor Reappearance: Criteria for Selecting the
Loco-Regional Management After Neoadjuvant Chemotherapy
 1 Loco-Regional Management After Neoadjuvant Chemotherapy Terry Mamounas, M.D., M.P.H., F.A.C.S. Medical Director, Comprehensive Breast Program UF Health Cancer Center at Orlando Health Professor of Surgery,
1 Loco-Regional Management After Neoadjuvant Chemotherapy Terry Mamounas, M.D., M.P.H., F.A.C.S. Medical Director, Comprehensive Breast Program UF Health Cancer Center at Orlando Health Professor of Surgery,
Conservative Surgery and Radiation Stage I and II Breast Cancer
 Conservative Surgery and Radiation Stage I and II Breast Cancer Variant 1: Premenopausal 41-year-old woman, 1.1-cm GII IDC, upper outer quadrant (UOQ), ER/PR ( ), HER2 ( ), primary excised with lumpectomy,
Conservative Surgery and Radiation Stage I and II Breast Cancer Variant 1: Premenopausal 41-year-old woman, 1.1-cm GII IDC, upper outer quadrant (UOQ), ER/PR ( ), HER2 ( ), primary excised with lumpectomy,
ARROCase - April 2017
 ARROCase - April 2017 Radiation Indications in the setting of Neoadjuvant chemotherapy for Breast Cancer Lauren Colbert, MD, MSCR Faculty Mentor: Benjamin Smith, MD UT MD Anderson Cancer Center 37 year
ARROCase - April 2017 Radiation Indications in the setting of Neoadjuvant chemotherapy for Breast Cancer Lauren Colbert, MD, MSCR Faculty Mentor: Benjamin Smith, MD UT MD Anderson Cancer Center 37 year
Prediction of Postoperative Tumor Size in Breast Cancer Patients by Clinical Assessment, Mammography and Ultrasonography
 Prediction of Postoperative Tumor Size in Breast Cancer Patients by Clinical Assessment, Mammography and Ultrasonography Eyad Fawzi AlSaeed 1 and Mutahir A. Tunio 2* 1 Consultant Radiation Oncology, Chairman
Prediction of Postoperative Tumor Size in Breast Cancer Patients by Clinical Assessment, Mammography and Ultrasonography Eyad Fawzi AlSaeed 1 and Mutahir A. Tunio 2* 1 Consultant Radiation Oncology, Chairman
03/14/2019. Postmastectomy radiotherapy; the meta-analyses, and the paradigm change to altered fractionation Mark Trombetta M.D.
 radiotherapy; the meta-analyses, and the paradigm change to altered fractionation Mark Trombetta M.D. Division of Radiation Oncology Allegheny Health Network Cancer Institute Professor of Radiation Oncology
radiotherapy; the meta-analyses, and the paradigm change to altered fractionation Mark Trombetta M.D. Division of Radiation Oncology Allegheny Health Network Cancer Institute Professor of Radiation Oncology
Ductal Carcinoma in Situ (DCIS)
") Diagnosis and Treatment of Patients with Primary and Metastatic Breast Cancer Ductal Carcinoma in Situ (DCIS) Ductal Carcinoma in Situ DCIS Versions 2002 2017: Audretsch / Blohmer / Brunnert / Budach /
Diagnosis and Treatment of Patients with Primary and Metastatic Breast Cancer Ductal Carcinoma in Situ (DCIS) Ductal Carcinoma in Situ DCIS Versions 2002 2017: Audretsch / Blohmer / Brunnert / Budach /
Maria João Cardoso, MD, PhD
 Locally Advanced Breast Cancer Specific Issues in LocorregionalTreatment Surgery, MD, PhD Head Breast Surgeon Breast Unit, Champalimaud Foundation Lisbon, Portugal 1 Conflict of Interest Disclosure No
Locally Advanced Breast Cancer Specific Issues in LocorregionalTreatment Surgery, MD, PhD Head Breast Surgeon Breast Unit, Champalimaud Foundation Lisbon, Portugal 1 Conflict of Interest Disclosure No
Newly Diagnosed Breast Cancer: Preoperative Imaging and Localization
 Newly Diagnosed Breast Cancer: Preoperative Imaging and Localization Debra Monticciolo, MD Professor of Radiology Texas A&M University no disclosures Debra Monticciolo, MD Professor of Radiology Texas
Newly Diagnosed Breast Cancer: Preoperative Imaging and Localization Debra Monticciolo, MD Professor of Radiology Texas A&M University no disclosures Debra Monticciolo, MD Professor of Radiology Texas
Updates in Breast Care. Truth or Hype. History of Breast Cancer Surgery. Dr Karen Barbosa 5/3/2017 4/20/2017
 Updates in Breast Care Dr Karen Barbosa 4/20/2017 Truth or Hype Princess Bust Developer Sears, Roebuck and Co. 1897 Promised to make the breast round, firm and beautiful History of Breast Cancer Surgery
Updates in Breast Care Dr Karen Barbosa 4/20/2017 Truth or Hype Princess Bust Developer Sears, Roebuck and Co. 1897 Promised to make the breast round, firm and beautiful History of Breast Cancer Surgery
Intraoperative. Radiotherapy
 Intraoperative Radiotherapy ROBERTO ORECCHIA UNIVERSITY of MILAN & EUROPEAN INSTITUTE of ONCOLOGY & CNAO FOUNDATION Breast Cancer Brescia, 30th September 2011 IORT, very selective technique to intensify
Intraoperative Radiotherapy ROBERTO ORECCHIA UNIVERSITY of MILAN & EUROPEAN INSTITUTE of ONCOLOGY & CNAO FOUNDATION Breast Cancer Brescia, 30th September 2011 IORT, very selective technique to intensify
Breast Cancer Earlier Disease. Stefan Aebi Luzerner Kantonsspital
 Breast Cancer Earlier Disease Stefan Aebi Luzerner Kantonsspital stefan.aebi@onkologie.ch Switzerland Breast Cancer Earlier Disease Diagnosis and Prognosis Local Therapy Surgery Radiation therapy Adjuvant
Breast Cancer Earlier Disease Stefan Aebi Luzerner Kantonsspital stefan.aebi@onkologie.ch Switzerland Breast Cancer Earlier Disease Diagnosis and Prognosis Local Therapy Surgery Radiation therapy Adjuvant
Updates on management of the axilla in breast cancer the surgical point of view
 Updates on management of the axilla in breast cancer the surgical point of view Edwige Bourstyn Centre des maladies du sein Hôpital Saint Louis Paris Sentinel lymph node biopsy (SLNB) is the standard of
Updates on management of the axilla in breast cancer the surgical point of view Edwige Bourstyn Centre des maladies du sein Hôpital Saint Louis Paris Sentinel lymph node biopsy (SLNB) is the standard of
Savitri Krishnamurthy, MD 1
 EVOLVING TRENDS IN PATHOLOGIC EVALUATION OF AXILLARY LYMPH NODES IN BREAST CANCER Savitri Krishnamurthy, M.D. Professor Department of Pathology University of Texas M. D. Anderson Cancer Center AXILLARY
EVOLVING TRENDS IN PATHOLOGIC EVALUATION OF AXILLARY LYMPH NODES IN BREAST CANCER Savitri Krishnamurthy, M.D. Professor Department of Pathology University of Texas M. D. Anderson Cancer Center AXILLARY
What are Adequate Margins of Resection for Breast-Conserving Therapy?
 What are Adequate Margins of Resection for Breast-Conserving Therapy? Jay R. Harris Dana-Farber Cancer Institute (DFCI) Brigham and Women s Hospital (BWH) Harvard Medical School What are Adequate Margins
What are Adequate Margins of Resection for Breast-Conserving Therapy? Jay R. Harris Dana-Farber Cancer Institute (DFCI) Brigham and Women s Hospital (BWH) Harvard Medical School What are Adequate Margins
Breast Cancer Diagnosis, Treatment and Follow-up
 Breast Cancer Diagnosis, Treatment and Follow-up What is breast cancer? Each of the body s organs, including the breast, is made up of many types of cells. Normally, healthy cells grow and divide to produce
Breast Cancer Diagnosis, Treatment and Follow-up What is breast cancer? Each of the body s organs, including the breast, is made up of many types of cells. Normally, healthy cells grow and divide to produce
Image guided core biopsies:
 Recommendations on the Surgical, Radiologic and Pathologic Approaches to Breast Disease: Using best practices based on multidisciplinary methodologies developed through the Allina Breast Committee. Image
Recommendations on the Surgical, Radiologic and Pathologic Approaches to Breast Disease: Using best practices based on multidisciplinary methodologies developed through the Allina Breast Committee. Image
EDITORIAL. Ann Surg Oncol (2011) 18: DOI /s
 18: DOI /s") Ann Surg Oncol (2011) 18:2407 2412 DOI 10.1245/s10434-011-1593-7 EDITORIAL Multidisciplinary Considerations in the Implementation of the Findings from the American College of Surgeons Oncology Group (ACOSOG)
Ann Surg Oncol (2011) 18:2407 2412 DOI 10.1245/s10434-011-1593-7 EDITORIAL Multidisciplinary Considerations in the Implementation of the Findings from the American College of Surgeons Oncology Group (ACOSOG)
ACRIN 6666 Therapeutic Surgery Form
 S1 ACRIN 6666 Therapeutic Surgery Form 6666 Instructions: Complete a separate S1 form for each separate area of each breast excised with the intent to treat a cancer (e.g. each lumpectomy or mastectomy).
S1 ACRIN 6666 Therapeutic Surgery Form 6666 Instructions: Complete a separate S1 form for each separate area of each breast excised with the intent to treat a cancer (e.g. each lumpectomy or mastectomy).
Outcomes of patients with inflammatory breast cancer treated by breast-conserving surgery
 Breast Cancer Res Treat (2016) 160:387 391 DOI 10.1007/s10549-016-4017-3 EDITORIAL Outcomes of patients with inflammatory breast cancer treated by breast-conserving surgery Monika Brzezinska 1 Linda J.
Breast Cancer Res Treat (2016) 160:387 391 DOI 10.1007/s10549-016-4017-3 EDITORIAL Outcomes of patients with inflammatory breast cancer treated by breast-conserving surgery Monika Brzezinska 1 Linda J.
UK Interdisciplinary Breast Cancer Symposium. Should lobular phenotype be considered when deciding treatment? Michael J Kerin
 UK Interdisciplinary Breast Cancer Symposium Should lobular phenotype be considered when deciding treatment? Michael J Kerin Professor of Surgery National University of Ireland, Galway and Galway University
UK Interdisciplinary Breast Cancer Symposium Should lobular phenotype be considered when deciding treatment? Michael J Kerin Professor of Surgery National University of Ireland, Galway and Galway University
Evaluation of Pathologic Response in Breast Cancer Treated with Primary Systemic Therapy
 Evaluation of Pathologic Response in Breast Cancer Treated with Primary Systemic Therapy Eun Yoon Cho, MD, PhD Department of Pathology and Translational Genomics Samsung Medical Center Sungkyunkwan University
Evaluation of Pathologic Response in Breast Cancer Treated with Primary Systemic Therapy Eun Yoon Cho, MD, PhD Department of Pathology and Translational Genomics Samsung Medical Center Sungkyunkwan University
Indications and Technical Considerations for Adjuvant Radiation after Neoadjuvant Chemotherapy in Breast Cancer
 Indications and Technical Considerations for Adjuvant Radiation after Neoadjuvant Chemotherapy in Breast Cancer Wendy A. Woodward, M.D. Ph.D. A sociate Profesor Section Chief, Breast Radiation Oncology
Indications and Technical Considerations for Adjuvant Radiation after Neoadjuvant Chemotherapy in Breast Cancer Wendy A. Woodward, M.D. Ph.D. A sociate Profesor Section Chief, Breast Radiation Oncology
Recent Updates in Surgical Management of Breast Cancer Asian Patient's Perspective
 Recent Updates in Surgical Management of Breast Cancer Asian Patient's Perspective Tokyo-West Tokushukai Hospital Department of Breast Oncology Tokyo-West Tokushukai Hospital, Tokyo, Japan Kaz Sato, MD,
Recent Updates in Surgical Management of Breast Cancer Asian Patient's Perspective Tokyo-West Tokushukai Hospital Department of Breast Oncology Tokyo-West Tokushukai Hospital, Tokyo, Japan Kaz Sato, MD,
Post-Mastectomy RT after Neoadjuvant Chemotherapy (NAC)
") Post-Mastectomy RT after Neoadjuvant Chemotherapy (NAC) Jay R. Harris, M.D. Dana-Farber Cancer Institute Brigham and Women s Hospital Harvard Medical School Conclusions When considering PMRT, use both
Post-Mastectomy RT after Neoadjuvant Chemotherapy (NAC) Jay R. Harris, M.D. Dana-Farber Cancer Institute Brigham and Women s Hospital Harvard Medical School Conclusions When considering PMRT, use both
Contralateral Prophylactic Mastectomy with Immediate Reconstruction: Added Benefits, Added Risks
 Contralateral Prophylactic Mastectomy with Immediate Reconstruction: Added Benefits, Added Risks Grant W. Carlson Wadley R. Glenn Professor of Surgery Divisions of Plastic Surgery & Surgical Oncology Emory
Contralateral Prophylactic Mastectomy with Immediate Reconstruction: Added Benefits, Added Risks Grant W. Carlson Wadley R. Glenn Professor of Surgery Divisions of Plastic Surgery & Surgical Oncology Emory
Loco-Regional Management After Neoadjuvant Chemotherapy
 1 Loco-Regional Management After Neoadjuvant Chemotherapy Terry Mamounas, M.D., M.P.H., F.A.C.S. Medical Director, Comprehensive Breast Program UF Health Cancer Center at Orlando Health Professor of Surgery,
1 Loco-Regional Management After Neoadjuvant Chemotherapy Terry Mamounas, M.D., M.P.H., F.A.C.S. Medical Director, Comprehensive Breast Program UF Health Cancer Center at Orlando Health Professor of Surgery,
What is an Adequate Lumpectomy Margin in 2018?
 What is an Adequate Lumpectomy Margin in 2018? Stuart J. Schnitt, M.D. Brigham and Women s Hospital, Dana-Farber Cancer Institute, and Harvard Medical School Boston, MA None Disclosures Topics Current
What is an Adequate Lumpectomy Margin in 2018? Stuart J. Schnitt, M.D. Brigham and Women s Hospital, Dana-Farber Cancer Institute, and Harvard Medical School Boston, MA None Disclosures Topics Current
Cryoablation in the Management of Early Stage Breast Cancer
 13 th Annual Pacific Northwest Breast and Gynecologic Care Conference Cryoablation in the Management of Early Stage Breast Cancer Dennis R. Holmes, M.D., Inc. Int. Director, Margie Peterson Breast Center
13 th Annual Pacific Northwest Breast and Gynecologic Care Conference Cryoablation in the Management of Early Stage Breast Cancer Dennis R. Holmes, M.D., Inc. Int. Director, Margie Peterson Breast Center