Thomas Gernon, MD Otolaryngology THE EVOLVING TREATMENT OF SCCA OF THE OROPHARYNX
|
|
|
- April Gordon
- 5 years ago
- Views:
Transcription



1 Thomas Gernon, MD Otolaryngology THE EVOLVING TREATMENT OF SCCA OF THE OROPHARYNX
2 Disclosures I have nothing to disclose.



3 3




4 Changing Role of Surgery N=42,688 Chen Ay et al. Larygoscope. 2007; 117:16-21
5 RCT S: A SHIFT TOWARDS ORGAN-PRESERVING NON- SURGICAL TREATMENT Veterans Affairs Laryngeal Cancer Study Group Arm 1: Induction chemotherapy Responders: proceed to XRT Non-responders: proceed with surgery + post-op XRT Arm 2: Surgery + post-op XRT No difference in 5-yr overall survival The Department of Veterans Affairs Laryngeal Cancer Study Group. Induction chemotherapy plus radiation compared with surgery plus radiation in patients with advanced laryngeal cancer. N Engl J Med 1991;324:
6 RCT S CONTINUED EORTC Head and Neck Cancer Cooperative Group Similar to VA trial design: Stage III/IV pyriform sinus CA Long-term survival rates were similar in the laryngectomy and induction chemotherapy groups Lefebvre JL, Chevalier D, Luboinski B et al. Larynx preservation in pyriform sinus cancer: preliminary results of a European Organization for Research and Treatment of Cancer phase III trial. EORTC Head and Neck Cancer Cooperative Group. J Natl Cancer Inst 1996;88: Intergroup Similar to VA trial, except showed that chemotherapy given CONCURRENTLY with XRT provided better local control than induction chemotx followed by XRT Forastiere AA, Goepfert H, Maor M et al. Concurrent chemotherapy and radiotherapy for organ preservation in advanced laryngeal cancer. N Engl J Med 2003;349: EORTC #22931 and RTOG #9501 In the post-operative operati e management of patients with advanced anced head and neck cancer with high-risk features, adjuvant chemotherapy-enhanced radiation therapy (CERT) was shown to be more efficacious than radiotherapy alone in terms of locoregional control and disease-free survival. Bernier J, Domenge C, Ozsahin M, et al. Postoperative Irradiation with or without Concomitant Chemotherapy for Locally Advanced, g,, p py y Head and Neck Cancer. The New England journal of medicine 2004;350: Cooper JS, Pajak TF, Forastiere AA, et al. Postoperative Concurrent Radiotherapy and Chemotherapy for High-Risk Squamous-Cell Carcinoma of the Head and Neck. The New England journal of medicine 2004;350:
7 SCCA OF THE OROPHARYNX SURGERY, RADIATION OR BOTH Parsons et al Review of 51 studies 6400 patients (tonsil SCCA and tongue base) Surgery with or without RT RT with or without necks dissection Results: Base of Tongue Local control 79% vs 76% (P=0.087) Local-regional control 60% vs 69% (P=0.009) 5 year survival 49% vs 52% 5 yr cause specific survival 62% and 63% (P=0.4)
8 SCCA OF THE OROPHARYNX SURGERY, RADIATION, OR BOTH Results: Tonsil Local control 70% vs 68% (P=0.2) Local-Regional Control 65% vs 69% (P=0.1) 5 year survival 47% vs 43% (P=0.2) 5 year cause specific survival 57% vs 59% (p=0.3) Complications Base of Tongue Severe 32% vs 3.8% (P<0.001) 001) Fatal complication 3.5% vs.4% (P<0.001) Tonsillar region Severe 23% vs 6% (P<0.001) Fatal complication (P<0.001)
9 Furthermore, available data on the functional consequences of ftreatment t tsuggest tthe superiority it of frt +/- ND. The authors conclude that RT +/-ND is preferable for the majority of patients with SCC of the oropharynx. Cancer 2002;94:


 pts : 99 / 230")
10 Long-term Toxicity of Radiation Machtay et al. JCO 2008 Long-term morbidity from RT, chemort in three prospective clinical trials 99 / 230 (43%) pts : 99 / 230 (43%) pts : severe late toxicity
11 CHANGING TRENDS IN HNSCC
12 HPV PREVALENCE Gillison et al 2012 Prevalence of infection pts aged % HPV type 16 infection was 1.0% Bimodal age distribution Peak prevalence age yrs (7.3%) and yrs (11.4%) Men higher prevalence than women for oral HPV infection 10.1% vs 3.6% Infection less common among those without a hx of sexual contact vs. those with a hx of sexual contact 0.9% vs 7.5% Prevalence increases with greater number of sexual partners and with cigarette smoking The incidence of HPV+ OPSCCA is currently 2.6 per 100,000.
13 Phenotypically Favorable Perfect set up for TOS Smaller primary tumors Accessible Better prognosis Live longer Avoid CRT in younger patients Lewis et al. Oncology, 2015.
14 HPV+ OPSCC Clinical Presentation Earlier T-stage Advanced N-Stage Cystic appearing nodes Indication for tonsillectomy and base of tongue biopsies in unknown primary Histology Non-Keratinizing Poorly differentiated




15 Histology HPV+ vs HPV- SCCA 15
16 Risk Stratification Two Different Cancers? Ang et al. N Engl J Med. 2010
17 HPV+ vs HPV- Overall survival Horne et al, 2016
18 Head and Neck Cancer in 2016 HPV+ OPSCC Excellent survival What is the next step to improve treatment? Speech and swallow reducing long term complications Transoral endoscopic-assisted surgery: preserving function and healing by 1) minimizing size of resection and 2) nerve preservation Transoral laser microresection (TLM) Transoral robotic-assisted surgery (TORS)
19 Surgery Adoption of a New Treatment Can it be done safely? Is it oncologically sound? How does it compare functionally to the current standard?


20 History of Transoral Surgery TOS first described in 1951 Practiced selectively at some institutions in 1980s-90s TLM developed in 1990s in Germany Steiner et al. Arch Otolaryngol Head Neck Surg, 2003.
21 Transoral endoscopic- assisted surgery: Steiner revolution Endoscopic microresection of laryngeal tumors achieved equivalent local control to open surgical approaches Superior functional outcome








22 da Vinci Robotic Surgery Laryngoscope Jul;115(7): Three dimensional visualization Tremor filtration Wristed instrumentation
23
24








25 FK retractor
26







27
28 Potential Patient Benefits In comparison to other surgical approaches Avoidance of disfiguring mandibulotomy Avoidance of tracheostomy Quicker return to normal speech and swallowing Significantly less pain Less Blood loss Less risk of wound infection Shorter hospital stay Shorter recovery time Minimal scarring
29 Specific Contraindications to TORS Mandibular invasion Tongue base involvement requiring resection of > 50% of the tongue base Pharyngeal wall involvement necessitating resection of >50% of the posterior pharyngeal wall Radiologic confirmation of carotid artery involvement Fixation of tumor to prevertebral fascia Involvement of the pterygoids
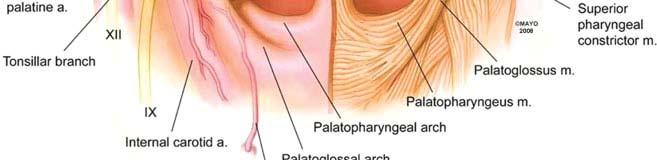
30 TORS applications Oropharnx and skull base Tonsil Tongue base Palate Pharyngeal wall Parapharyngeal Space Larynx and hypopharynx Supraglottis Glottis Pyriform sinus Pharyngeal wall


31 TORS Radical Tonsillectomy
 Blood Loss Weinstein et al 189 mls (range 0-500 mls) Moore et al 12.")
32 Operative Findings Operative time Weinstein et al 1hr43mins (range, 26 mins-3 hrs 53mins) Moore et al 71.3 minute Positioning Time Weinstein et al 9 min (range, 2-22 minutes) Blood Loss Weinstein et al 189 mls (range mls) Moore et al 12.6 ml (range, 0-50 ml) Surgical margins Weinstein et al 25/27 patients(93%) negative
33 PEG Dependence Postoperative Swallowing Weinstein et al: 26/27 (96%) pts w/out gastrostomy Moore et al: 0/45 pts with gastrostomy 48.9% with temporary DHT palces Avg duration 12.5 days (range, 2-41 days) Ozer et al: 11/56 Gtube placement during RT 0 pts with long term PEG dependence Genden et al 0 cases of long term PEG dependence Literature reports 5-10% of CRT patients PEG dependent > 2 years after treatment
34 Trach Dependence Tracheostomy Dependence Weinstein et al: 1/27 pts trach dependent Moore et al: 0/45 pts trach dependent 13.1% had temporary tracheostomy tube placement Ozer et al: 0/56 pts trach dependent Hospital stay Moore et al: 3.8 days
35 FUNCTIONAL RESULTS OF TLMS AND TORS Hinni et al,
36 WHICH MODALITY IS BETTER? ORGAN PRESERVATION? Survival Worden et al. JCO 2008 Fakhry et al. JNCI

37 WHICH MODALITY IS BETTER? SURGERY? Cohen et al, 2011 Haughey et al,
38 HPV+ LITERATURE REVIEW N T3 4% HPV+ OS for Surv Rec LR DM HPV+ Worden % Ang % 13% 8.7% Posner % 13% 5% Haughey % 6.8% 6% Cohen % 0 5.4% Moore % 5% 1.6% 38
39
40 Conclusions for TOS Can Trans Oral Surgery be performed safely? Is TOS oncologically sound? TOS is equivalent to organ preservation protocols in the treatment of OPSCCA How does TOS compare functionally? TOS demonstrates functional outcomes as good as nonsurgical therapy 40
41 Question? What prognostic factors are important in treatment of HPV+ disease How can those factors be used to modify treatment in the future?
42 Are typical High Risk features important in surgically treated HPV+ OPSCCA? RTOG 9501 and EORTC High-risk i features = improved survival with cisplatin-based CRT High-risk path Positive margins ECE 2 or more nodes Level 4/5 nodes Perineural/vascular invasion Combined analysis positive margins and ECE Bernier. Head Neck, 2005.

43 T Stage 43
44 44
45 PROGNOSTIC FACTORS Margin Status Positive margins associated with reduced DFS Close margins (<5mm) on primary specimen with additional negative frozen sections is sufficient Without additional negative pathologic prognosticators radiation to the primary site may not be needed Prognostic Impact of Adjuvant Therapy Chemotherapy did not demonstrate survival or recurrence advantage in comparison to those receiving RT alone 45 Haughey et al, 2012
46 Prgonostic factors Presence of Angioinvasion Prognostic for DSS Greater rates of recurrence and death due to disease Increased likelihood of distant metastases

 Sinha, Haughey et al.")
47 Number of Nodes More Important than ECE Wash U 220 patients with HPV+OPC Surgical resection (TLM or TORS) Sinha, Haughey et al. Oral Oncol 2015
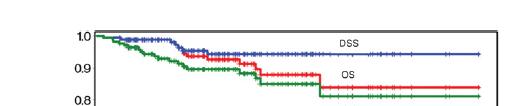
48 Number of nodes and DSS <5 LN >/=5 LN + LN <5 No benefit from adjuvant therapy in regards to DSS +LN >/= 5 CRT and RT equal Sinha, Haughey et al. Oral Oncol 2015
49
50 De-intensification is the Future



51 De-escalation Many Ways to Skin a Sheep Improved survival irrespective treatment modality Radiation Dose Volume Use CRT Selective use Surgery TOS Lewis et al. Oncology, 2015.
52 Single Modality Treatment 30 patients TORS + ND only No HPV data Majority T1/T2 1/3 Node positive Follow up >18 months Local control 97% Locoregional control 90% Distant disease 0% Weinstein, Arch Otolaryngol Head Neck Surg 2012.
53 Surgery as a Single Modality Limited to early stage tumors (T1-2, N0-1) Decreased morbidity Radiation for treatment of recurrence
54 asdf
55 Is HPV+ OPSCC staged correctly?
56 OS for HPV + OPSCCA based on stage per AJCC staging system (7 th edition)
57 Out with the Old in with the New
58 What about the Treatment Failure?


59 Immunotherapy for HNSCC HNSCC associated with immune suppressive state Altered lymphocyte homeostasis CD4+, CD3+, CD8+ PD-1 or PD-L1 routinely expressed in HNSCC Prevents T-cell activation and allows tumor escape




60 Immunotherapy for Head and Neck SCCA Pembrolizumab (Keytruda) Seiwert et al
61 Pembrolizumab Approved Aug 5,2016 by FDA For treatment of patients with recurrent or metastatic HNSCC With disease progression on or after platinum containing therapy Pembrolizumab 10 mg/kg every 2 weeks 174 pts Objective response rate 16% Range of duration of response 2.4 months-27.7 months 28 responding patients» 23 (82%) had responses of longer than 6 months


62 Base of tongue tumor: T2N0 vs. N1




63 Base of tongue tumor




64 Base of tongue tumor
65 Base of tongue tumor Pathology report: 2.2 cm moderately differentiated invasive carcinoma. Negative margins Staged neck dissection: 0/22 positive lymph nodes Pathologic Stage II: no adjuvant treatment recommended

66 Base of tongue tumor: postoperative healing 3 months



67 Questions? s
68 Surgical Margins asdf Hinni. Head and Neck, 2013.

69 69
70 SMOKING STATUS Nonsurgically treated patients Smokers with HPV positive OPSCC cancers reported Poorer survival both overall and disease specific Greater risk of recurrence Distant metastases Surgically treated patients Smokers had worse OS than never smokers On multivariate analysis neither current smoking history alone or tobacco exposure (>10 and >20 pack years) demonstrated an increased hazard of poorer DSS Would expect smokers to have worse OS given poorer general health Haughey et al,
71 FUTURE DIRECTIONS FOR HPV + OPSCCA Is there a role for further de-escalation of therapy in P16 positive oropharynx tumors? Do patients need treatment to Gy in post-surgical settings? Is chemotherapy necessary in post-operative treatment of HPV + OPSCCA? 71
72 OBJECTIVES Describe the epidemiology and demographics of HPV+ SCCA Prevalence Clinical Presentation History Outcomes Surgical Non-Surgical Prognostic factors in surgically treated HPV+ OPSCC
73 Margins No universal definition of inadequate margins No RCTs comparing margins Improvement in LR and survival in later studies Better assessment? Tumor shrinkage? 20-25% Better adjuvant therapy? HPV factor? Close Margins now generally accepted for OPC
74 Surgical Intensification in HPV-Negative, For Comparison
75 HPV AND HNSCC Gillison et al Assayed HNSCC tumor specimens from 253 pts HPV detected in 25% of cases HPV16 detected in 90% of HPV positive tumors HPV + oropharyngeal tumors less likely to have TP53 mutations 2009 Klussman et al Compared 28 HPV+ tumors to 32 HPV unrelated tumors HPV- tumors Increased chromosomal alterations Fewer 16q losses» Greater 16q loss associated with better overall survival and disease free survival
76 DEMOGRAPHICS HPV+ OPSCCA HPV- OPSCCA Caucasian - Older age (60) Middle aged (40-60) Low SES High SES M:F = 3:2 M:F = 3:1 Tobacco/ Alcohol Sexual
77 Hinne et al

78 78
Transoral Robotic Surgery (TORS) for Oropharyngeal Cancer
 for Oropharyngeal Cancer") Transoral Robotic Surgery (TORS) for Oropharyngeal Cancer Ellie Maghami, MD, FACS Professor of Otolaryngology / Head and Neck Surgery Chief, Division of Head and Neck Surgery Norman and Sadie Lee Professor
Transoral Robotic Surgery (TORS) for Oropharyngeal Cancer Ellie Maghami, MD, FACS Professor of Otolaryngology / Head and Neck Surgery Chief, Division of Head and Neck Surgery Norman and Sadie Lee Professor
Disclosure. Access 10/4/2013. The emerging role of TransOralRobotic Surgery (TORS) Organ preservation in the management of head and neck cancer
 Organ preservation in the management of head and neck cancer") Disclosure The emerging role of TransOralRobotic Surgery (TORS) Intuitive Surgical, Inc. Proctor/Honoraria Eddie Méndez, MD, MS, FACS Associate Professor, Department of Otolaryngology: Head & Neck Surgery
Disclosure The emerging role of TransOralRobotic Surgery (TORS) Intuitive Surgical, Inc. Proctor/Honoraria Eddie Méndez, MD, MS, FACS Associate Professor, Department of Otolaryngology: Head & Neck Surgery
Locally advanced head and neck cancer
 Locally advanced head and neck cancer Radiation Oncology Perspective Petek Erpolat, MD Gazi University, Turkey Definition and Management of LAHNC Stage III or IV cancers generally include larger primary
Locally advanced head and neck cancer Radiation Oncology Perspective Petek Erpolat, MD Gazi University, Turkey Definition and Management of LAHNC Stage III or IV cancers generally include larger primary
Indications and techniques of surgery for the primary treatment of HNSCC
 Prof. Christian Simon Chef-de-service Service d ORL et chirurgie cervico-faciale Centre Hospitalier Universitaire Vaudois (CHUV) Université de Lausanne Lausanne, Suisse Indications and techniques of surgery
Prof. Christian Simon Chef-de-service Service d ORL et chirurgie cervico-faciale Centre Hospitalier Universitaire Vaudois (CHUV) Université de Lausanne Lausanne, Suisse Indications and techniques of surgery
De-Escalate Trial for the Head and neck NSSG. Dr Eleanor Aynsley Consultant Clinical Oncologist
 De-Escalate Trial for the Head and neck NSSG Dr Eleanor Aynsley Consultant Clinical Oncologist 3 HPV+ H&N A distinct disease entity Leemans et al., Nature Reviews, 2011 4 Good news Improved response to
De-Escalate Trial for the Head and neck NSSG Dr Eleanor Aynsley Consultant Clinical Oncologist 3 HPV+ H&N A distinct disease entity Leemans et al., Nature Reviews, 2011 4 Good news Improved response to
Laryngeal Preservation Using Radiation Therapy. Chemotherapy and Organ Preservation
 1 Laryngeal Preservation Using Radiation Therapy 1903: Schepegrell was the first to perform radiation therapy for the treatment of laryngeal cancer Conventional external beam radiation produced disappointing
1 Laryngeal Preservation Using Radiation Therapy 1903: Schepegrell was the first to perform radiation therapy for the treatment of laryngeal cancer Conventional external beam radiation produced disappointing
Clinical Trials in Transoral Endoscopic Head &Neck Surgery ECOG3311 and RTOG1221. Chris Holsinger, MD, FACS Bob Ferris, MD, PhD, FACS
 Clinical Trials in Transoral Endoscopic Head &Neck Surgery ECOG3311 and RTOG1221 Chris Holsinger, MD, FACS Bob Ferris, MD, PhD, FACS 1 Disclosure I have no conflicts of interest to disclose 2 Robotic H&N
Clinical Trials in Transoral Endoscopic Head &Neck Surgery ECOG3311 and RTOG1221 Chris Holsinger, MD, FACS Bob Ferris, MD, PhD, FACS 1 Disclosure I have no conflicts of interest to disclose 2 Robotic H&N
Self-Assessment Module 2016 Annual Refresher Course
 LS16031305 The Management of s With r. Lin Learning Objectives: 1. To understand the changing demographics of oropharynx cancer, and the impact of human papillomavirus on overall survival and the patterns
LS16031305 The Management of s With r. Lin Learning Objectives: 1. To understand the changing demographics of oropharynx cancer, and the impact of human papillomavirus on overall survival and the patterns
HPV INDUCED OROPHARYNGEAL CARCINOMA radiation-oncologist point of view. Prof. dr. Sandra Nuyts Dep. Radiation-Oncology UH Leuven Belgium
 HPV INDUCED OROPHARYNGEAL CARCINOMA radiation-oncologist point of view Prof. dr. Sandra Nuyts Dep. Radiation-Oncology UH Leuven Belgium DISCLOSURE OF INTEREST Nothing to declare HEAD AND NECK CANCER -HPV
HPV INDUCED OROPHARYNGEAL CARCINOMA radiation-oncologist point of view Prof. dr. Sandra Nuyts Dep. Radiation-Oncology UH Leuven Belgium DISCLOSURE OF INTEREST Nothing to declare HEAD AND NECK CANCER -HPV
Organ-Preservation Strategies in head and neck cancer. Teresa Bonfill Abella Oncologia Mèdica Parc Taulí Sabadell. Hospital Universitari
 Organ-Preservation Strategies in head and neck cancer Teresa Bonfill Abella Oncologia Mèdica Parc Taulí Sabadell. Hospital Universitari Larynx Hypopharynx The goal of treatment is to achieve larynx preservation
Organ-Preservation Strategies in head and neck cancer Teresa Bonfill Abella Oncologia Mèdica Parc Taulí Sabadell. Hospital Universitari Larynx Hypopharynx The goal of treatment is to achieve larynx preservation
Surgical Margins in Transoral Robotic Surgery for Oropharyngeal Squamous Cell Carcinoma
 Surgical Margins in Transoral Robotic Surgery for Oropharyngeal Squamous Cell Carcinoma Consensus update and recommendations, 2018 Head and Neck Steering Committee P. Gorphe *, F. Nguyen, Y. Tao, P. Blanchard,
Surgical Margins in Transoral Robotic Surgery for Oropharyngeal Squamous Cell Carcinoma Consensus update and recommendations, 2018 Head and Neck Steering Committee P. Gorphe *, F. Nguyen, Y. Tao, P. Blanchard,
New Paradigms for Treatment of. Erminia Massarelli, MD, PHD, MS Clinical Associate Professor
 New Paradigms for Treatment of Head and Neck cancers Erminia Massarelli, MD, PHD, MS Clinical Associate Professor City of Hope Disclosure Statement Grant/Research Support frommerck Bristol Grant/Research
New Paradigms for Treatment of Head and Neck cancers Erminia Massarelli, MD, PHD, MS Clinical Associate Professor City of Hope Disclosure Statement Grant/Research Support frommerck Bristol Grant/Research
Triple-Modality Treatment in Patients With Advanced Stage Tonsil Cancer
 Triple-Modality Treatment in Patients With Advanced Stage Tonsil Cancer Dylan F. Roden, MD, MPH 1,2 ; David Schreiber, MD 2,3 ; and Babak Givi, MD 1,2 BACKGROUND: Concurrent chemoradiation (CCRT) and upfront
Triple-Modality Treatment in Patients With Advanced Stage Tonsil Cancer Dylan F. Roden, MD, MPH 1,2 ; David Schreiber, MD 2,3 ; and Babak Givi, MD 1,2 BACKGROUND: Concurrent chemoradiation (CCRT) and upfront
Accepted 28 April 2005 Published online 13 September 2005 in Wiley InterScience ( DOI: /hed.
 DEFINING RISK LEVELS IN LOCALLY ADVANCED HEAD AND NECK CANCERS: A COMPARATIVE ANALYSIS OF CONCURRENT POSTOPERATIVE RADIATION PLUS CHEMOTHERAPY TRIALS OF THE EORTC (#22931) AND RTOG (#9501) Jacques Bernier,
DEFINING RISK LEVELS IN LOCALLY ADVANCED HEAD AND NECK CANCERS: A COMPARATIVE ANALYSIS OF CONCURRENT POSTOPERATIVE RADIATION PLUS CHEMOTHERAPY TRIALS OF THE EORTC (#22931) AND RTOG (#9501) Jacques Bernier,
Simultaneous Integrated Boost or Sequential Boost in the Setting of Standard Dose or Dose De-escalation for HPV- Associated Oropharyngeal Cancer
 Simultaneous Integrated Boost or Sequential Boost in the Setting of Standard Dose or Dose De-escalation for HPV- Associated Oropharyngeal Cancer Dawn Gintz, CMD, RTT Dosimetry Coordinator of Research and
Simultaneous Integrated Boost or Sequential Boost in the Setting of Standard Dose or Dose De-escalation for HPV- Associated Oropharyngeal Cancer Dawn Gintz, CMD, RTT Dosimetry Coordinator of Research and
Laryngeal Conservation
 Laryngeal Conservation Sarah Rodriguez, MD Faculty Advisor: Shawn Newlands, MD, PhD The University of Texas Medical Branch Department of Otolaryngolgy Grand Rounds Presentation February 2005 Introduction
Laryngeal Conservation Sarah Rodriguez, MD Faculty Advisor: Shawn Newlands, MD, PhD The University of Texas Medical Branch Department of Otolaryngolgy Grand Rounds Presentation February 2005 Introduction
T1/T2 LARYNX CANCER. Click to edit Master Presentation Date. Thomas J Gernon, MD Otolaryngology-Head and Neck Surgery
 ADVANCES IN TREATMENT OF T1/T2 LARYNX CANCER Click to edit Master Presentation Date Thomas J Gernon, MD Otolaryngology-Head and Neck Surgery I have nothing to disclose CHANGING TRENDS IN HNSCC GLOTTIC
ADVANCES IN TREATMENT OF T1/T2 LARYNX CANCER Click to edit Master Presentation Date Thomas J Gernon, MD Otolaryngology-Head and Neck Surgery I have nothing to disclose CHANGING TRENDS IN HNSCC GLOTTIC
Emerging Role of Immunotherapy in Head and Neck Cancer
 Emerging Role of Immunotherapy in Head and Neck Cancer Jared Weiss, MD Associate Professor of Medicine and Section Chief of Thoracic and Head/Neck Oncology UNC Lineberger Comprehensive Cancer Center Copyright
Emerging Role of Immunotherapy in Head and Neck Cancer Jared Weiss, MD Associate Professor of Medicine and Section Chief of Thoracic and Head/Neck Oncology UNC Lineberger Comprehensive Cancer Center Copyright
Pre- Versus Post-operative Radiotherapy
 Postoperative Radiation and Chemoradiation: Indications and Optimization of Practice Dislosures Clinical trial support from Genentech Inc. Sue S. Yom, MD, PhD Associate Professor UCSF Radiation Oncology
Postoperative Radiation and Chemoradiation: Indications and Optimization of Practice Dislosures Clinical trial support from Genentech Inc. Sue S. Yom, MD, PhD Associate Professor UCSF Radiation Oncology
Head and Neck Cancer:
 Head and Neck Cancer: Robert Haddad M.D. Clinical Director Head and Neck Oncology Program Dana Farber Cancer Institute Boston, MA Predictive Biomarkers: HPV Abstract 6003: Survival Outcomes By HPV Status
Head and Neck Cancer: Robert Haddad M.D. Clinical Director Head and Neck Oncology Program Dana Farber Cancer Institute Boston, MA Predictive Biomarkers: HPV Abstract 6003: Survival Outcomes By HPV Status
Adjuvant Therapy in Locally Advanced Head and Neck Cancer. Ezra EW Cohen University of Chicago. Financial Support
 Adjuvant Therapy in Locally Advanced Head and Neck Cancer Ezra EW Cohen University of Chicago Financial Support This program is made possible by an educational grant from Eli Lilly Oncology, who had no
Adjuvant Therapy in Locally Advanced Head and Neck Cancer Ezra EW Cohen University of Chicago Financial Support This program is made possible by an educational grant from Eli Lilly Oncology, who had no
HPV-Related Head and Neck Squamous Cancers
 2015 Wisconsin Comprehensive Cancer Control Summit Aligning Partners, Priorities, and the Plan HPV-Related Head and Neck Squamous Cancers MCW Department of Otolaryngology and Communication Sciences MCW
2015 Wisconsin Comprehensive Cancer Control Summit Aligning Partners, Priorities, and the Plan HPV-Related Head and Neck Squamous Cancers MCW Department of Otolaryngology and Communication Sciences MCW
The International Federation of Head and Neck Oncologic Societies. Current Concepts in Head and Neck Surgery and Oncology
 The International Federation of Head and Neck Oncologic Societies Current Concepts in Head and Neck Surgery and Oncology www.ifhnos.net The International Federation of Head and Neck Oncologic Societies
The International Federation of Head and Neck Oncologic Societies Current Concepts in Head and Neck Surgery and Oncology www.ifhnos.net The International Federation of Head and Neck Oncologic Societies
MANAGEMENT OF CA HYPOPHARYNX
 MANAGEMENT OF CA HYPOPHARYNX GENERAL TREATMENT RECOMMENDATIONS BASED ON HYPOPHARYNX TUMOR STAGE For patients presenting with early-stage definitive radiotherapy alone or voice-preserving surgery are viable
MANAGEMENT OF CA HYPOPHARYNX GENERAL TREATMENT RECOMMENDATIONS BASED ON HYPOPHARYNX TUMOR STAGE For patients presenting with early-stage definitive radiotherapy alone or voice-preserving surgery are viable
Squamous Cell Carcinoma of the Oral Cavity: Radio therapeutic Considerations
 Squamous Cell Carcinoma of the Oral Cavity: Radio therapeutic Considerations Troy G. Scroggins Jr. MD Chairman, Department of Radiation Oncology Ochsner Health Systems 1 Association of Postoperative Radiotherapy
Squamous Cell Carcinoma of the Oral Cavity: Radio therapeutic Considerations Troy G. Scroggins Jr. MD Chairman, Department of Radiation Oncology Ochsner Health Systems 1 Association of Postoperative Radiotherapy
Larynx Hypopharynx. Therapy algorithms. Why larynx preservation at all? State of the art Jean Louis Lefebvre,Lille Jan Klozar,Prague
 Larynx Hypopharynx Moderation Rainald Knecht,Hamburg State of the art Jean Louis Lefebvre,Lille Debate pro CRT Jan Klozar,Prague contra CRT Marshall Posner,Boston Clinical cases all Therapy algorithms
Larynx Hypopharynx Moderation Rainald Knecht,Hamburg State of the art Jean Louis Lefebvre,Lille Debate pro CRT Jan Klozar,Prague contra CRT Marshall Posner,Boston Clinical cases all Therapy algorithms
Protocol of Radiotherapy for Head and Neck Cancer
 106 年 12 月修訂 Protocol of Radiotherapy for Head and Neck Cancer Indication of radiotherapy Indication of definitive radiotherapy with or without chemotherapy (1) Resectable, but medically unfit, or high
106 年 12 月修訂 Protocol of Radiotherapy for Head and Neck Cancer Indication of radiotherapy Indication of definitive radiotherapy with or without chemotherapy (1) Resectable, but medically unfit, or high
MANAGEMENT OF LOCALLY ADVANCED OROPHARYNGEAL CANER: HPV AND NON-HPV MEDIATED CANCERS
 MANAGEMENT OF LOCALLY ADVANCED OROPHARYNGEAL CANER: HPV AND NON-HPV MEDIATED CANCERS Kyle Arneson, MD PhD Avera Medical Group Radiation Oncology Avera Cancer Institute 16 th Annual Oncology Symposium September
MANAGEMENT OF LOCALLY ADVANCED OROPHARYNGEAL CANER: HPV AND NON-HPV MEDIATED CANCERS Kyle Arneson, MD PhD Avera Medical Group Radiation Oncology Avera Cancer Institute 16 th Annual Oncology Symposium September
11/7/2014. Disclosure Dr. Walvekar, I have the following relationship(s) with commercial interests.
 with commercial interests.") TORS & Supraglottic Laryngectomy Disclosure Dr. Walvekar, I have the following relationship(s) with commercial interests. Hood Laboratories Rec. Royalties Cook Industries Rec. Honoraria Medtronic Rec.
TORS & Supraglottic Laryngectomy Disclosure Dr. Walvekar, I have the following relationship(s) with commercial interests. Hood Laboratories Rec. Royalties Cook Industries Rec. Honoraria Medtronic Rec.
Treatment for Supraglottic Ca History: : Total Laryngectomy y was routine until early 50 s, when XRT was developed Ogura and Som developed the one-sta
 Role of Laser Therapy in Laryngeal Cancer Khalid Hussain AL-Qahtani MD,MSc,FRCS(c) MSc Assistant Professor Consultant of Otolaryngology Advance Head & Neck Oncology, Thyroid & Parathyroid,Microvascular
Role of Laser Therapy in Laryngeal Cancer Khalid Hussain AL-Qahtani MD,MSc,FRCS(c) MSc Assistant Professor Consultant of Otolaryngology Advance Head & Neck Oncology, Thyroid & Parathyroid,Microvascular
Head and Neck cancer
 Head and Neck cancer Medical Oncologist s Role in Multidisciplinary Teams - Focus on Adjuvant & Neo-adjuvant Therapy - Hye Ryun Kim, M.D. Yonsei Cancer Center, Medical Oncology Contents I. Introduction
Head and Neck cancer Medical Oncologist s Role in Multidisciplinary Teams - Focus on Adjuvant & Neo-adjuvant Therapy - Hye Ryun Kim, M.D. Yonsei Cancer Center, Medical Oncology Contents I. Introduction
HPV and Head and Neck Cancer: What it means for you and your patients
 HPV and Head and Neck Cancer: What it means for you and your patients Financial Disclosure: None November 8, 2013 Steven J. Wang, MD Associate Professor Department of Otolaryngology-Head and Neck Surgery
HPV and Head and Neck Cancer: What it means for you and your patients Financial Disclosure: None November 8, 2013 Steven J. Wang, MD Associate Professor Department of Otolaryngology-Head and Neck Surgery
HPV POSITIVE OROPHARYNGEAL CARCINOMA the radiation oncologist point of view. Prof. dr. Sandra Nuyts Dep. Radiation-Oncology UH Leuven Belgium
 HPV POSITIVE OROPHARYNGEAL CARCINOMA the radiation oncologist point of view Prof. dr. Sandra Nuyts Dep. Radiation-Oncology UH Leuven Belgium HEAD AND NECK CANCER -HPV Change in incidence: HEAD AND NECK
HPV POSITIVE OROPHARYNGEAL CARCINOMA the radiation oncologist point of view Prof. dr. Sandra Nuyts Dep. Radiation-Oncology UH Leuven Belgium HEAD AND NECK CANCER -HPV Change in incidence: HEAD AND NECK
OROPHARYNX CANCER. Anthony Zeitouni, MD, FRCSC. Co-Lead, Head Neck Cancer Rossy Cancer Network
 OROPHARYNX CANCER Anthony Zeitouni, MD, FRCSC Co-Lead, Head Neck Cancer Rossy Cancer Network CFPC CoI Templates: Slide 1 FACULTY/PRESENTER DISCLOSURE Faculty: Dr Anthony Zeitouni Relationships with commercial
OROPHARYNX CANCER Anthony Zeitouni, MD, FRCSC Co-Lead, Head Neck Cancer Rossy Cancer Network CFPC CoI Templates: Slide 1 FACULTY/PRESENTER DISCLOSURE Faculty: Dr Anthony Zeitouni Relationships with commercial
Neoplasie del laringe Diagnosi e trattamento
 Neoplasie del laringe Diagnosi e trattamento Venerdì 22 maggio 2015 Alessandria Trattamenti non chirurgici: Preservazione d organo, malattia localmente avanzata Marco C Merlano A.O. S.Croce e Carle, Ospedale
Neoplasie del laringe Diagnosi e trattamento Venerdì 22 maggio 2015 Alessandria Trattamenti non chirurgici: Preservazione d organo, malattia localmente avanzata Marco C Merlano A.O. S.Croce e Carle, Ospedale
ACR Appropriateness Criteria Adjuvant Therapy for Resected Squamous Cell Carcinoma of the Head and Neck EVIDENCE TABLE
 1. Johnson JT, Barnes EL, Myers EN, Schramm VL, Jr., Borochovitz D, Sigler BA. The extracapsular spread of tumors in cervical node metastasis. Arch Otolaryngol 1981; 107(1):75-79.. Snow GB, Annyas AA,
1. Johnson JT, Barnes EL, Myers EN, Schramm VL, Jr., Borochovitz D, Sigler BA. The extracapsular spread of tumors in cervical node metastasis. Arch Otolaryngol 1981; 107(1):75-79.. Snow GB, Annyas AA,
Oral Cavity Cancer Combined modality therapy
 Oral Cavity Cancer Combined modality therapy Dr. Christos CHRISTOPOULOS Radiation Oncologist Head and Neck Cancers Centre Hospitalier Universitaire (C.H.U.) de Limoges, France Disclosure slide I have no
Oral Cavity Cancer Combined modality therapy Dr. Christos CHRISTOPOULOS Radiation Oncologist Head and Neck Cancers Centre Hospitalier Universitaire (C.H.U.) de Limoges, France Disclosure slide I have no
Head and Neck Cancer in FA: Risks, Prevention, Screening, & Treatment Options David I. Kutler, M.D., F.A.C.S.
 Head and Neck Cancer in FA: Risks, Prevention, Screening, & Treatment Options David I. Kutler, M.D., F.A.C.S. Associate Professor Division of Head and Neck Surgery Department of Otolaryngology-Head and
Head and Neck Cancer in FA: Risks, Prevention, Screening, & Treatment Options David I. Kutler, M.D., F.A.C.S. Associate Professor Division of Head and Neck Surgery Department of Otolaryngology-Head and
Title. CitationInternational Journal of Clinical Oncology, 20(6): 1. Issue Date Doc URL. Rights. Type. File Information
: 1. Issue Date Doc URL. Rights. Type. File Information") Title Clinical outcomes of weekly cisplatin chemoradiother Sakashita, Tomohiro; Homma, Akihiro; Hatakeyama, Hir Author(s) Takatsugu; Iizuka, Satoshi; Onimaru, Rikiya; Tsuchiy CitationInternational Journal
Title Clinical outcomes of weekly cisplatin chemoradiother Sakashita, Tomohiro; Homma, Akihiro; Hatakeyama, Hir Author(s) Takatsugu; Iizuka, Satoshi; Onimaru, Rikiya; Tsuchiy CitationInternational Journal
Case Scenario. 7/13/12 Anterior floor of mouth biopsy: Infiltrating squamous cell carcinoma, not completely excised.
 Case Scenario 7/5/12 History A 51 year old white female presents with a sore area on the floor of her mouth. She claims the area has been sore for several months. She is a current smoker and user of alcohol.
Case Scenario 7/5/12 History A 51 year old white female presents with a sore area on the floor of her mouth. She claims the area has been sore for several months. She is a current smoker and user of alcohol.
Benefits of Genomic Medicine: What to Tell the Patient
 Benefits of Genomic Medicine: What to Tell the Patient Christine H. Chung, M.D. Associate Professor of Oncology Director, HNC Therapeutics Program Johns Hopkins University No Conflict of Interest to Disclose
Benefits of Genomic Medicine: What to Tell the Patient Christine H. Chung, M.D. Associate Professor of Oncology Director, HNC Therapeutics Program Johns Hopkins University No Conflict of Interest to Disclose
Head and Neck Reirradiation: Perils and Practice
 Head and Neck Reirradiation: Perils and Practice David J. Sher, MD, MPH Department of Radiation Oncology Dana-Farber Cancer Institute/ Brigham and Women s Hospital Conflicts of Interest No conflicts of
Head and Neck Reirradiation: Perils and Practice David J. Sher, MD, MPH Department of Radiation Oncology Dana-Farber Cancer Institute/ Brigham and Women s Hospital Conflicts of Interest No conflicts of
Sequencing Chemo with Radiation therapy Locally Advanced Head and Neck Cancer. Dr P Vijay Anand Reddy Director Apollo Cancer Hospital
 Sequencing Chemo with Radiation therapy Locally Advanced Head and Neck Cancer Dr P Vijay Anand Reddy Director Apollo Cancer Hospital H&N Ca - Disease Burden 15-20% of all cancers in India, 8% worldwide
Sequencing Chemo with Radiation therapy Locally Advanced Head and Neck Cancer Dr P Vijay Anand Reddy Director Apollo Cancer Hospital H&N Ca - Disease Burden 15-20% of all cancers in India, 8% worldwide
Early adoption of transoral robotic surgical program: preliminary outcomes.
 Thomas Jefferson University Jefferson Digital Commons Department of Otolaryngology - Head and Neck Surgery Faculty Papers Department of Otolaryngology - Head and Neck Surgery 9-1-2012 Early adoption of
Thomas Jefferson University Jefferson Digital Commons Department of Otolaryngology - Head and Neck Surgery Faculty Papers Department of Otolaryngology - Head and Neck Surgery 9-1-2012 Early adoption of
The International Federation of Head and Neck Oncologic Societies. Current Concepts in Head and Neck Surgery and Oncology
 The International Federation of Head and Neck Oncologic Societies Current Concepts in Head and Neck Surgery and Oncology 2018 www.ifhnos.net The International Federation of Head and Neck Oncologic Societies
The International Federation of Head and Neck Oncologic Societies Current Concepts in Head and Neck Surgery and Oncology 2018 www.ifhnos.net The International Federation of Head and Neck Oncologic Societies
The management of advanced supraglottic and
 ORIGINAL ARTICLE ORGAN PRESERVATION FOR ADVANCED LARYNGEAL CARCINOMA Robert L. Foote, MD, 1 R. Tyler Foote, 1 Paul D. Brown, MD, 1 Yolanda I. Garces, MD, 1 Scott H. Okuno, MD, 2 Scott E. Strome, MD 3 1
ORIGINAL ARTICLE ORGAN PRESERVATION FOR ADVANCED LARYNGEAL CARCINOMA Robert L. Foote, MD, 1 R. Tyler Foote, 1 Paul D. Brown, MD, 1 Yolanda I. Garces, MD, 1 Scott H. Okuno, MD, 2 Scott E. Strome, MD 3 1
Case Scenario 1. 7/13/12 Anterior floor of mouth biopsy: Infiltrating squamous cell carcinoma, not completely excised.
 Case Scenario 1 7/5/12 History A 51 year old white female presents with a sore area on the floor of her mouth. She claims the area has been sore for several months. She is a current smoker and user of
Case Scenario 1 7/5/12 History A 51 year old white female presents with a sore area on the floor of her mouth. She claims the area has been sore for several months. She is a current smoker and user of
Immunotherapy for the Treatment of Head and Neck Cancers. Robert F. Taylor, MD Aurora Health Care
 Immunotherapy for the Treatment of Head and Neck Cancers Robert F. Taylor, MD Aurora Health Care Disclosures No relevant financial relationships to disclose I will be discussing non-fda approved indications
Immunotherapy for the Treatment of Head and Neck Cancers Robert F. Taylor, MD Aurora Health Care Disclosures No relevant financial relationships to disclose I will be discussing non-fda approved indications
Lymph node ratio as a prognostic factor in head and neck cancer patients
 Chen et al. Radiation Oncology (2015) 10:181 DOI 10.1186/s13014-015-0490-9 RESEARCH Open Access Lymph node ratio as a prognostic factor in head and neck cancer patients Chien-Chih Chen 1*, Jin-Ching Lin
Chen et al. Radiation Oncology (2015) 10:181 DOI 10.1186/s13014-015-0490-9 RESEARCH Open Access Lymph node ratio as a prognostic factor in head and neck cancer patients Chien-Chih Chen 1*, Jin-Ching Lin
TREATMENT TIME & TOBACCO: TWIN TERRORS Of H&N Therapy
 TREATMENT TIME & TOBACCO: TWIN TERRORS Of H&N Therapy Anurag K. Singh, MD Professor of Medicine University at Buffalo School of Medicine Professor of Oncology Director of Radiation Research Roswell Park
TREATMENT TIME & TOBACCO: TWIN TERRORS Of H&N Therapy Anurag K. Singh, MD Professor of Medicine University at Buffalo School of Medicine Professor of Oncology Director of Radiation Research Roswell Park
Piero Nicolai SURGERY FOR THE TREATMENT OF OROPHARYNGEAL CARCINOMA: STATE OF ART. Department of Otorhinolaryngology University of Brescia
 Biology and technology contribution to clinical advancement: the case of oropharyngeal cancer Brescia May 8 th, 2009 SURGERY FOR THE TREATMENT OF OROPHARYNGEAL CARCINOMA: STATE OF ART Piero Nicolai Department
Biology and technology contribution to clinical advancement: the case of oropharyngeal cancer Brescia May 8 th, 2009 SURGERY FOR THE TREATMENT OF OROPHARYNGEAL CARCINOMA: STATE OF ART Piero Nicolai Department
SAMO MASTERCLASS HEAD & NECK CANCER. Nicolas Mach, PD Geneva University Hospital
 SAMO MASTERCLASS HEAD & NECK CANCER Nicolas Mach, PD Geneva University Hospital Epidemiology Prevention Best treatment for localized disease Best treatment for relapsed or metastatic disease Introduction
SAMO MASTERCLASS HEAD & NECK CANCER Nicolas Mach, PD Geneva University Hospital Epidemiology Prevention Best treatment for localized disease Best treatment for relapsed or metastatic disease Introduction
ORIGINAL ARTICLE. Salvage Surgery After Failure of Nonsurgical Therapy for Carcinoma of the Larynx and Hypopharynx
 ORIGINAL ARTICLE Salvage Surgery After Failure of Nonsurgical Therapy for Carcinoma of the Larynx and Hypopharynx Sandro J. Stoeckli, MD; Andreas B. Pawlik, MD; Margareta Lipp, MD; Alexander Huber, MD;
ORIGINAL ARTICLE Salvage Surgery After Failure of Nonsurgical Therapy for Carcinoma of the Larynx and Hypopharynx Sandro J. Stoeckli, MD; Andreas B. Pawlik, MD; Margareta Lipp, MD; Alexander Huber, MD;
Use of Larynx-Preservation Strategies in the Treatment of Laryngeal Cancer. American Society of Clinical Oncology Clinical Practice Guideline
 Use of Larynx-Preservation Strategies in the Treatment of Laryngeal Cancer American Society of Clinical Oncology Clinical Practice Guideline Introduction ASCO convened an Expert Panel to develop recommendations
Use of Larynx-Preservation Strategies in the Treatment of Laryngeal Cancer American Society of Clinical Oncology Clinical Practice Guideline Introduction ASCO convened an Expert Panel to develop recommendations
Persistent tracheostomy after primary chemoradiation for advanced laryngeal or hypopharyngeal cancer
 ORIGINAL ARTICLE Persistent tracheostomy after primary chemoradiation for advanced laryngeal or hypopharyngeal cancer Paul A. Tennant, MD, * Elizabeth Cash, PhD, Jeffrey M. Bumpous, MD, Kevin L. Potts,
ORIGINAL ARTICLE Persistent tracheostomy after primary chemoradiation for advanced laryngeal or hypopharyngeal cancer Paul A. Tennant, MD, * Elizabeth Cash, PhD, Jeffrey M. Bumpous, MD, Kevin L. Potts,
Persistent Tracheostomy after Organ Preservation Protocol in Patients Treated for Larynx and Hypopharynx Cancer
 THIEME Original Research 377 Persistent Tracheostomy after Organ Preservation Protocol in Patients Treated for Larynx and Hypopharynx Cancer Carlos Miguel Chiesa Estomba Frank Alberto Betances Reinoso
THIEME Original Research 377 Persistent Tracheostomy after Organ Preservation Protocol in Patients Treated for Larynx and Hypopharynx Cancer Carlos Miguel Chiesa Estomba Frank Alberto Betances Reinoso
RADIO- AND RADIOCHEMOTHERAPY OF HEAD AND NECK TUMORS. Zoltán Takácsi-Nagy PhD Department of Radiotherapy National Institute of Oncology, Budapest 1.
 RADIO- AND RADIOCHEMOTHERAPY OF HEAD AND NECK TUMORS Zoltán Takácsi-Nagy PhD Department of Radiotherapy National Institute of Oncology, Budapest 1. 550 000 NEW PATIENTS/YEAR WITH HEAD AND NECK CANCER ALL
RADIO- AND RADIOCHEMOTHERAPY OF HEAD AND NECK TUMORS Zoltán Takácsi-Nagy PhD Department of Radiotherapy National Institute of Oncology, Budapest 1. 550 000 NEW PATIENTS/YEAR WITH HEAD AND NECK CANCER ALL
Human Papillomavirus and Head and Neck Cancer. Ed Stelow, MD
 Human Papillomavirus and Head and Neck Cancer Ed Stelow, MD No conflict of interest Declaration Cancer 1974 Lancet Oncol 2016; 17: e477-8 JAMA 1984; 252: 1857 JAMA 1988;259(13):1943-1944 Clin Cancer Res
Human Papillomavirus and Head and Neck Cancer Ed Stelow, MD No conflict of interest Declaration Cancer 1974 Lancet Oncol 2016; 17: e477-8 JAMA 1984; 252: 1857 JAMA 1988;259(13):1943-1944 Clin Cancer Res
Oral cancer: Prognosis & Treatment. Dr. Hani Al Sheikh Radhi
 Oral cancer: Prognosis & Treatment Dr. Hani Al Sheikh Radhi Prognostic factors in Oral caner TNM staging T stage N stage M stage Site Histological Factors Vascular & Perineural Invasion Surgical Margins
Oral cancer: Prognosis & Treatment Dr. Hani Al Sheikh Radhi Prognostic factors in Oral caner TNM staging T stage N stage M stage Site Histological Factors Vascular & Perineural Invasion Surgical Margins
CURRENT STANDARD OF CARE IN NASOPHARYNGEAL CANCER
 CURRENT STANDARD OF CARE IN NASOPHARYNGEAL CANCER Jean-Pascal Machiels Department of medical oncology Institut I Roi Albert II Cliniques universitaires Saint-Luc Université catholique de Louvain, Brussels,
CURRENT STANDARD OF CARE IN NASOPHARYNGEAL CANCER Jean-Pascal Machiels Department of medical oncology Institut I Roi Albert II Cliniques universitaires Saint-Luc Université catholique de Louvain, Brussels,
Cetuximab/cisplatin and radiotherapy in HNSCC: is there a favorite choice?
 Cent. Eur. J. Med. 9(2) 2014 279-284 DOI: 10.2478/s11536-013-0154-9 Central European Journal of Medicine Cetuximab/cisplatin and radiotherapy in HNSCC: is there a favorite choice? Jacopo Giuliani* 1, Marina
Cent. Eur. J. Med. 9(2) 2014 279-284 DOI: 10.2478/s11536-013-0154-9 Central European Journal of Medicine Cetuximab/cisplatin and radiotherapy in HNSCC: is there a favorite choice? Jacopo Giuliani* 1, Marina
Case Scenario 1. Pathology: Specimen type: Incisional biopsy of the glottis Histology: Moderately differentiated squamous cell carcinoma
 Case Scenario 1 History A 52 year old male with a 20 pack year smoking history presented with about a 6 month history of persistent hoarseness. The patient had a squamous cell carcinoma of the lip removed
Case Scenario 1 History A 52 year old male with a 20 pack year smoking history presented with about a 6 month history of persistent hoarseness. The patient had a squamous cell carcinoma of the lip removed
Anatomy of Head of Neck Cancer
 Anatomy of Head of Neck Cancer J. Robert Newman, MD The ENT Center of Central GA H&N Cancer Overview Most categories of cancer are represented in the H&N Squamous cell carcinoma most common mucosal cancer
Anatomy of Head of Neck Cancer J. Robert Newman, MD The ENT Center of Central GA H&N Cancer Overview Most categories of cancer are represented in the H&N Squamous cell carcinoma most common mucosal cancer
Head and Neck Cancer Update Sandro V Porceddu
 Head and Neck Cancer Update Sandro V Porceddu Director, Radiation Oncology Research Princess Alexandra Hospital, Brisbane Associate Professor, University of Queensland President, Trans Tasman Radiation
Head and Neck Cancer Update Sandro V Porceddu Director, Radiation Oncology Research Princess Alexandra Hospital, Brisbane Associate Professor, University of Queensland President, Trans Tasman Radiation
Comparing Alternative treatment Regimens for intermediate and high risk oropharyngeal cancer CompARE. Prof. Hisham Mehanna.
 Comparing Alternative treatment Regimens for intermediate and high risk oropharyngeal cancer CompARE Prof. Hisham Mehanna Chief investigator: Hisham Mehanna Arm 1: Mehmet Sen Arm2: John Chester/Martin
Comparing Alternative treatment Regimens for intermediate and high risk oropharyngeal cancer CompARE Prof. Hisham Mehanna Chief investigator: Hisham Mehanna Arm 1: Mehmet Sen Arm2: John Chester/Martin
HPV-RELATED HEAD AND NECK CANCER
 WINTER REFRESHER COURSE FOR FAMILY MEDICINE HPV-RELATED HEAD AND NECK CANCER DISCLOSURES MCW Department of Otolaryngology and Communication Sciences MCW Institute for Health and Society (Center for Bioethics
WINTER REFRESHER COURSE FOR FAMILY MEDICINE HPV-RELATED HEAD AND NECK CANCER DISCLOSURES MCW Department of Otolaryngology and Communication Sciences MCW Institute for Health and Society (Center for Bioethics
3/12/2018. Head & Neck Cancer Review INTRODUCTION
 Head & Neck Cancer Review Joseph Rosales, MD March 12, 2018 INTRODUCTION Epidemiology/Risk Factors Anatomy Presentation/Workup Treatment Surgery vs Radiation Chemotherapy Side effects Special circumstances
Head & Neck Cancer Review Joseph Rosales, MD March 12, 2018 INTRODUCTION Epidemiology/Risk Factors Anatomy Presentation/Workup Treatment Surgery vs Radiation Chemotherapy Side effects Special circumstances
Head & Neck Cancer: When to Irradiate
 Head & Neck Cancer: When to Irradiate ESO-ESMO Latin-America 2018 Talented students colleagues 1 > 15 different diseases for RT strategies NC NP OC OP H L 2 HPV Prognostic Marker >2010 Trial Cases Marker
Head & Neck Cancer: When to Irradiate ESO-ESMO Latin-America 2018 Talented students colleagues 1 > 15 different diseases for RT strategies NC NP OC OP H L 2 HPV Prognostic Marker >2010 Trial Cases Marker
QUIZZES WITH ANSWERS FOR COLLECTING CANCER DATA: PHARYNX
 QUIZZES WITH ANSWERS FOR COLLECTING CANCER DATA: PHARYNX MP/H Quiz 1. A patient presented with a prior history of squamous cell carcinoma of the base of the tongue. The malignancy was originally diagnosed
QUIZZES WITH ANSWERS FOR COLLECTING CANCER DATA: PHARYNX MP/H Quiz 1. A patient presented with a prior history of squamous cell carcinoma of the base of the tongue. The malignancy was originally diagnosed
Head and Neck Cancer Service
 Dr Hoda Al Booz. MMedSci, MD, FFRRCSI, FRCR. Head and Neck Cancer Service Dr Hoda Al Booz Consultant in Clinical Oncology Bristol Cancer Institute Dr Hoda Al Booz. MMedSci, MD, FFRRCSI, FRCR. documents/
Dr Hoda Al Booz. MMedSci, MD, FFRRCSI, FRCR. Head and Neck Cancer Service Dr Hoda Al Booz Consultant in Clinical Oncology Bristol Cancer Institute Dr Hoda Al Booz. MMedSci, MD, FFRRCSI, FRCR. documents/
JOSE FRANCISCO GALLEGOS HERNANDEZ Hospital de Oncología, CMN SXXI. IMSS México City.
 JOSE FRANCISCO GALLEGOS HERNANDEZ Hospital de Oncología, CMN SXXI. IMSS México City. HNSCC with a global incidence of over 500,000 cases and 200,000 deaths annually is the leading cause of mortality and
JOSE FRANCISCO GALLEGOS HERNANDEZ Hospital de Oncología, CMN SXXI. IMSS México City. HNSCC with a global incidence of over 500,000 cases and 200,000 deaths annually is the leading cause of mortality and
ESMO Perceptorship H&N cancer Epidemiology, Anatomy and Workup 16 March 2018
 ESMO Perceptorship H&N cancer Epidemiology, Anatomy and Workup 16 March 2018 Dr. Victor Ho-Fun Lee MBBS, MD, FRCR, FHKCR, FHKAM (Radiology) Clinical Associate Professor Department of Clinical Oncology
ESMO Perceptorship H&N cancer Epidemiology, Anatomy and Workup 16 March 2018 Dr. Victor Ho-Fun Lee MBBS, MD, FRCR, FHKCR, FHKAM (Radiology) Clinical Associate Professor Department of Clinical Oncology
Cancer of the Head and Neck and. HPV Infection. Andrew Urquhart MD, FACS Dept. Otolaryngology/Head and Neck Surgery Marshfield Clinic
 Cancer of the Head and Neck and HPV Infection Andrew Urquhart MD, FACS Dept. Otolaryngology/Head and Neck Surgery Marshfield Clinic Disclaimer I have no relevant financial relationships with the manufacturer(s)
Cancer of the Head and Neck and HPV Infection Andrew Urquhart MD, FACS Dept. Otolaryngology/Head and Neck Surgery Marshfield Clinic Disclaimer I have no relevant financial relationships with the manufacturer(s)
Outcomes in Oncology
 Outcomes in Oncology Ochsner Cancer Institute s Report to Physicians May 2014 ochsner.org/cancer Head and Neck Cancer Update: New Strategies for the Treatment of Oropharyngeal Cancer Dear Physicians, In
Outcomes in Oncology Ochsner Cancer Institute s Report to Physicians May 2014 ochsner.org/cancer Head and Neck Cancer Update: New Strategies for the Treatment of Oropharyngeal Cancer Dear Physicians, In
FRCS Otolarynoglogy VIVA Course Dundee Guidelines. Andrew Kinshuck ST-8 ENT Aintree University Hospital, Liverpool
 FRCS Otolarynoglogy VIVA Course Dundee www.frcsentvivacourse.co.uk Guidelines Andrew Kinshuck ST-8 ENT Aintree University Hospital, Liverpool Marking Descriptors Available from JCIE website if search for
FRCS Otolarynoglogy VIVA Course Dundee www.frcsentvivacourse.co.uk Guidelines Andrew Kinshuck ST-8 ENT Aintree University Hospital, Liverpool Marking Descriptors Available from JCIE website if search for
FINE NEEDLE ASPIRATION OF ENLARGED LYMPH NODE: Metastatic squamous cell carcinoma
 Case Scenario 1 HNP: A 70 year old white male presents with dysphagia. The patient is a current smoker, current user of alcohol and is HPV positive. A CT of the Neck showed mass in the left pyriform sinus.
Case Scenario 1 HNP: A 70 year old white male presents with dysphagia. The patient is a current smoker, current user of alcohol and is HPV positive. A CT of the Neck showed mass in the left pyriform sinus.
Clinical Discussion. Dr Pankaj Chaturvedi. Professor and Surgeon Tata Memorial Hospital
 Clinical Discussion Dr Pankaj Chaturvedi Professor and Surgeon Tata Memorial Hospital chaturvedi.pankaj@gmail.com 47/M/smoker Hopkins : Transglottic lesion No cartilage infiltration but sclerosis Left
Clinical Discussion Dr Pankaj Chaturvedi Professor and Surgeon Tata Memorial Hospital chaturvedi.pankaj@gmail.com 47/M/smoker Hopkins : Transglottic lesion No cartilage infiltration but sclerosis Left
RESEARCH ARTICLE. Salvage Transoral Robotic Surgery for Recurrent or Residual Head and Neck Squamous Cell Carcinoma: A Single Institution Experience
 DOI:http://dx.doi.org/10.7314/APJCP.2015.16.17.7627 Salvage TORS for Recurrent or Residual Head Neck Cancer RESEARCH ARTICLE Salvage Transoral Robotic Surgery for Recurrent or Residual Head and Neck Squamous
DOI:http://dx.doi.org/10.7314/APJCP.2015.16.17.7627 Salvage TORS for Recurrent or Residual Head Neck Cancer RESEARCH ARTICLE Salvage Transoral Robotic Surgery for Recurrent or Residual Head and Neck Squamous
QUIZZES WITH ANSWERS FOR COLLECTING CANCER DATA: PHARYNX
 QUIZZES WITH ANSWERS FOR COLLECTING CANCER DATA: PHARYNX MP/H Quiz 1. A patient presented with a prior history of squamous cell carcinoma of the base of the tongue. The malignancy was originally diagnosed
QUIZZES WITH ANSWERS FOR COLLECTING CANCER DATA: PHARYNX MP/H Quiz 1. A patient presented with a prior history of squamous cell carcinoma of the base of the tongue. The malignancy was originally diagnosed
Lymph node density as an independent prognostic factor in node-positive patients with tonsillar cancer
 ORIGINAL ARTICLE Lymph node density as an independent prognostic factor in node-positive patients with tonsillar cancer Jun-Ook Park, MD, PhD, 1 Young-Hoon Joo, MD, PhD, 2 Kwang-Jae Cho, MD, PhD, 2 Min-Sik
ORIGINAL ARTICLE Lymph node density as an independent prognostic factor in node-positive patients with tonsillar cancer Jun-Ook Park, MD, PhD, 1 Young-Hoon Joo, MD, PhD, 2 Kwang-Jae Cho, MD, PhD, 2 Min-Sik
Non-surgical treatment for locally advanced head and neck squamous cell carcinoma: beyond the upper limit
 Editorial Non-surgical treatment for locally advanced head and neck squamous cell carcinoma: beyond the upper limit Hiroto Ishiki, Satoru Iwase Department of Palliative Medicine, The Institute of Medical
Editorial Non-surgical treatment for locally advanced head and neck squamous cell carcinoma: beyond the upper limit Hiroto Ishiki, Satoru Iwase Department of Palliative Medicine, The Institute of Medical
3/8/2014. Case Presentation. Primary Treatment of Anal Cancer. Anatomy. Overview. March 6, 2014
 Case Presentation Primary Treatment of Anal Cancer 65 year old female presents with perianal pain, lower GI bleeding, and anemia with Hb of 7. On exam 6 cm mass protruding through the anus with bulky R
Case Presentation Primary Treatment of Anal Cancer 65 year old female presents with perianal pain, lower GI bleeding, and anemia with Hb of 7. On exam 6 cm mass protruding through the anus with bulky R
Transoral Laser Microsurgery (TLM) Adjuvant Therapy for Advanced Stage Oropharyngeal Cancer: Outcomes and Prognostic Factors
 Adjuvant Therapy for Advanced Stage Oropharyngeal Cancer: Outcomes and Prognostic Factors") The Laryngoscope VC 2009 The American Laryngological, Rhinological and Otological Society, Inc. Transoral Laser Microsurgery (TLM) Adjuvant Therapy for Advanced Stage Oropharyngeal Cancer: Outcomes and
The Laryngoscope VC 2009 The American Laryngological, Rhinological and Otological Society, Inc. Transoral Laser Microsurgery (TLM) Adjuvant Therapy for Advanced Stage Oropharyngeal Cancer: Outcomes and
Mini J.Elnaggar M.D. Radiation Oncology Ochsner Medical Center 9/23/2016. Background
 Mini J.Elnaggar M.D. Radiation Oncology Ochsner Medical Center 9/23/2016 Background Mostly adenocarcinoma (scc possible, but treated like anal cancer) 39, 220 cases annually Primary treatment: surgery
Mini J.Elnaggar M.D. Radiation Oncology Ochsner Medical Center 9/23/2016 Background Mostly adenocarcinoma (scc possible, but treated like anal cancer) 39, 220 cases annually Primary treatment: surgery
Disclosures. Immunotherapyin Head & NeckCancer. Actual landscape of systemic treatment in HNSCC. Head andneckcanceris an immunogeneic tumor
 Immunotherapyin Head & NeckCancer Disclosures Astra-Zeneca/medimmune: clinical trial BMS: advisory board, clinical trial Merck: advisory board, clinical trial, research funding Carla van Herpen Medical
Immunotherapyin Head & NeckCancer Disclosures Astra-Zeneca/medimmune: clinical trial BMS: advisory board, clinical trial Merck: advisory board, clinical trial, research funding Carla van Herpen Medical
Oral cavity cancer Post-operative treatment
 Oral cavity cancer Post-operative treatment Dr. Christos CHRISTOPOULOS Radiation Oncologist Centre Hospitalier Universitaire (C.H.U.) de Limoges, France Important issues RT -techniques Patient selection
Oral cavity cancer Post-operative treatment Dr. Christos CHRISTOPOULOS Radiation Oncologist Centre Hospitalier Universitaire (C.H.U.) de Limoges, France Important issues RT -techniques Patient selection
Concurrent Chemo- and Radiotherapy for Ororpharynx Cancer
 Concurrent Chemo- and Radiotherapy for Ororpharynx Cancer Faye Johnson MD, PhD Associate Professor Thoracic/Head and Neck Medical Oncology August 2017 Objectives Review data that support concurrent chemo-
Concurrent Chemo- and Radiotherapy for Ororpharynx Cancer Faye Johnson MD, PhD Associate Professor Thoracic/Head and Neck Medical Oncology August 2017 Objectives Review data that support concurrent chemo-
CANCERS of OROPHARYNX and HYPOPHARYNX. STAGING and TREATMENT
 1 CANCERS of OROPHARYNX and HYPOPHARYNX STAGING and TREATMENT 2 1. Staging 2. General Principles of Treatment 3. Site Specific Treatment Guidelines 4. Selected Abstracts from Relevant Studies 3 1. Staging
1 CANCERS of OROPHARYNX and HYPOPHARYNX STAGING and TREATMENT 2 1. Staging 2. General Principles of Treatment 3. Site Specific Treatment Guidelines 4. Selected Abstracts from Relevant Studies 3 1. Staging
Management of Salivary Gland Malignancies. No Disclosures or Conflicts of Interest. Anatomy 10/4/2013
 Management of Salivary Gland Malignancies Daniel G. Deschler, MD Director: Division of Head and Neck Surgery Massachusetts Eye & Ear Infirmary Massachusetts General Hospital Professor Harvard Medical School
Management of Salivary Gland Malignancies Daniel G. Deschler, MD Director: Division of Head and Neck Surgery Massachusetts Eye & Ear Infirmary Massachusetts General Hospital Professor Harvard Medical School
JOURNAL SCAN FOR IJHNS
 JOURNAL SCAN FOR IJHNS IJHNS Journal Scan for IJHNS Meta-analysis of Chemotherapy in Head and Neck Cancer (MACH-NC): An Update on 93 Randomized Trials and 17,346 Patients Jean-Pierre Pignon A, Aurélie
JOURNAL SCAN FOR IJHNS IJHNS Journal Scan for IJHNS Meta-analysis of Chemotherapy in Head and Neck Cancer (MACH-NC): An Update on 93 Randomized Trials and 17,346 Patients Jean-Pierre Pignon A, Aurélie
AJCC Cancer Staging 8 th edition. Lip and Oral Cavity Oropharynx (p16 -) and Hypopharynx Larynx
 and Hypopharynx Larynx") AJCC Cancer Staging 8 th edition Lip and Oral Cavity Oropharynx (p16 -) and Hypopharynx Larynx AJCC 7 th edition Lip and Oral cavity Pharynx Larynx KEY CHANGES Skin of head and neck (Vermilion of the lip)
AJCC Cancer Staging 8 th edition Lip and Oral Cavity Oropharynx (p16 -) and Hypopharynx Larynx AJCC 7 th edition Lip and Oral cavity Pharynx Larynx KEY CHANGES Skin of head and neck (Vermilion of the lip)
Service Line: Rapid Response Service Version: 1.0 Publication Date: Month XX, 2017 Report Length: 79 Pages
 CADTH RAPID RESPONSE REPORT: SYSTEMATIC REVIEW Treatments for Locally Advanced Oropharyngeal Cancer: A Systematic Review of Clinical Effectiveness and Cost- Effectiveness Service Line: Rapid Response Service
CADTH RAPID RESPONSE REPORT: SYSTEMATIC REVIEW Treatments for Locally Advanced Oropharyngeal Cancer: A Systematic Review of Clinical Effectiveness and Cost- Effectiveness Service Line: Rapid Response Service
Katsuro Sato. Department of Speech, Language and Hearing Sciences, Niigata University of Health and Welfare, Niigata, Japan
 Report Niigata Journal of Health and Welfare Vol. 12, No. 1 Retrospective analysis of head and neck cancer cases from the database of the Niigata Prefecture Head and Neck Malignant Tumor Registration Committee
Report Niigata Journal of Health and Welfare Vol. 12, No. 1 Retrospective analysis of head and neck cancer cases from the database of the Niigata Prefecture Head and Neck Malignant Tumor Registration Committee
Treatment and prognosis of patients with recurrent laryngeal carcinoma: a retrospective study
 Page 1 of 7 Treatment and prognosis of patients with recurrent laryngeal carcinoma: a retrospective study T Jin 1, H Lin 2,3, HX Lin 2,3, XY Cai 2,3, HZ Wang 2,3, WH Hu 2,3, LB Guo 4, JZ Zhao 5 * Abstract
Page 1 of 7 Treatment and prognosis of patients with recurrent laryngeal carcinoma: a retrospective study T Jin 1, H Lin 2,3, HX Lin 2,3, XY Cai 2,3, HZ Wang 2,3, WH Hu 2,3, LB Guo 4, JZ Zhao 5 * Abstract
Head and Neck SCC. HPV in Tumors of the Head and Neck. Overview. Role of HPV in Pathogenesis of Head & Neck Tumors
 HPV in Tumors of the Head and Neck Christina Kong, M.D. Associate Professor, Stanford Dept of Pathology Director, Cytopathology Laboratory & Cytopathology Fellowship ckong@stanford.edu Head and Neck SCC
HPV in Tumors of the Head and Neck Christina Kong, M.D. Associate Professor, Stanford Dept of Pathology Director, Cytopathology Laboratory & Cytopathology Fellowship ckong@stanford.edu Head and Neck SCC
NICE guideline Published: 10 February 2016 nice.org.uk/guidance/ng36
 Cancer of the upper aerodigestive e tract: assessment and management in people aged 16 and over NICE guideline Published: 10 February 2016 nice.org.uk/guidance/ng36 NICE 2018. All rights reserved. Subject
Cancer of the upper aerodigestive e tract: assessment and management in people aged 16 and over NICE guideline Published: 10 February 2016 nice.org.uk/guidance/ng36 NICE 2018. All rights reserved. Subject
Nasopharynx Cancer. 1 Feb Presenters: Dr Raghav Murali-Ganesh (Radiation Oncology Registrar) Dr Peter Luk (Pathology Registrar)
 Dr Peter Luk (Pathology Registrar)") Nasopharynx Cancer 1 Feb 2016 Presenters: Dr Raghav Murali-Ganesh (Radiation Oncology Registrar) Dr Peter Luk (Pathology Registrar) Expert Panels Prof Mo Mo Tin Prof Michael Boyer Dr Raewyn Campbell Prof
Nasopharynx Cancer 1 Feb 2016 Presenters: Dr Raghav Murali-Ganesh (Radiation Oncology Registrar) Dr Peter Luk (Pathology Registrar) Expert Panels Prof Mo Mo Tin Prof Michael Boyer Dr Raewyn Campbell Prof
First of all, the pathophysiology
 Welcome. My name is Eric Sturgis and I m a Professor in Head and Neck Surgery with a joint appointment in the Department of Epidemiology at The University of Texas MD Anderson Cancer Center. And today
Welcome. My name is Eric Sturgis and I m a Professor in Head and Neck Surgery with a joint appointment in the Department of Epidemiology at The University of Texas MD Anderson Cancer Center. And today
Hypopharynx. 1. Introduction. 1.1 General Information and Aetiology
 Hypopharynx 1. Introduction 1.1 General Information and Aetiology The human pharynx is the part of the throat situated between the nasal cavity and the esophagus and can be divided into three parts: the
Hypopharynx 1. Introduction 1.1 General Information and Aetiology The human pharynx is the part of the throat situated between the nasal cavity and the esophagus and can be divided into three parts: the
Wojciech K. Mydlarz, M.D. Pharyngocutaneous Fistulas after Salvage Laryngectomy: Need for Vascularized Tissue
 Wojciech K. Mydlarz, M.D. Pharyngocutaneous Fistulas after Salvage Laryngectomy: Need for Vascularized Tissue Disclosures No Relevant Financial Relationships or Commercial Interests Educational Objectives
Wojciech K. Mydlarz, M.D. Pharyngocutaneous Fistulas after Salvage Laryngectomy: Need for Vascularized Tissue Disclosures No Relevant Financial Relationships or Commercial Interests Educational Objectives