Prostate cancer staging and datasets: The Nitty-Gritty. What determines our pathological reports? 06/07/2018. Dan Berney Maastricht 2018
|
|
|
- Kerry Conley
- 5 years ago
- Views:
Transcription
1 Prostate cancer staging and datasets: The Nitty-Gritty What determines our pathological reports? Dan Berney Maastricht 2018 Biopsy reporting. How not to do it. The TNM 8 th edition. Changes good and bad Some philosophy. 1
.")
mm (spanning 4mm) 2.5 (2+0.")
 mm corresponding to to approximately 75%, 50%, and 25% of the areas studied in each core")





2 Left base: Five disrupted prostate cores, three of which contain a moderately to poorly differentiated adenocarcinoma of the prostate gland, Gleason grade 3+4 (=score 7). The approximate ratio of Gleason pattern 3 to 4 is 95:5. The tumour occupies discontinuous lengths of 3 ( )mm (spanning 4mm) 2.5 (2+0.5) mm (spanning 3mm) and 2 ( ) mm corresponding to to approximately 75%, 50%, and 25% of the areas studied in each core respectively. There is perineural invasion in one core, but no evidence of acute inflammation, high grade PIN, or extraprostatic extension. Conclusion Gleason grade 3+4 Grade Group 2 No of involved cores 18 Total tumour length 85mm Total length of all cores studied: 191mm % of tumour length in all cores 5% Maximum tumour length: 13mm Tumour Laterality: Bilateral Left base: Five disrupted prostate cores, three of which contain a moderately to poorly differentiated adenocarcinoma of the prostate gland, Gleason grade 3+4 (=score 7). The approximate ratio of Gleason pattern 3 to 4 is 95:5. The tumour occupies discontinuous lengths of 3 ( )mm (spanning 4mm) 2.5 (2+0.5) mm (spanning 3mm) and 2 ( ) mm corresponding to to approximately 75%, 50%, and 25% of the areas studied in each core respectively. There is perineural invasion in one core, but no evidence of acute inflammation, high grade PIN, or extraprostatic extension. Conclusion Gleason grade 3+4 Grade Group 2 No of involved cores 18 Total tumour length 85mm Total length of all cores studied: 191mm % of tumour length in all cores 5% Maximum tumour length: 13mm Tumour Laterality: Bilateral 2
 11 10 13 14 12 11 Adenocarcinoma Yes Yes Yes Yes No No present?")

3 Biopsy site (Modified Barzell Zone) 1 Left anterior apex 2 3 Left anterior Right base anterior apex 4 Right anterior base 5 Midline apex 6 Midline base Block number A B C D E F NSNumber of cores Longest core (mm) Adenocarcinoma Yes Yes Yes Yes No No present? Number of cores involved Largest cancer focus (mm) Total core length (mm) Total cancer length (mm) % cancer in sample Gleason 3+3=6 3+4=7 3+4=7 3+4=7 - - Perineural invasion No No No Yes No No High grade PIN in 1 core? No No No No No No Left Base: 3/5 prostate cores show adenocarcinoma, Gleason score 3+4=7 without cribriform areas, (5% grade 4) (3mm 75%, 3mm 50%, 2mm 25% discontinuously) Perineural invasion seen. Conclusion: prostatic adenocarcinoma, Gleason score 3+4=7, Grade Group 2 in 18/25 cores, Perineural invasion seen. IS THERE CANCER? TYPE IT GRADE IT MEASURE IT OTHER FACTORS PNI, LVI, ECE etc 3
 11 (46) 41 (40) mm each core 21 (27) 2 (8) 23 (22) Maximum mm in a core 37 (47) 11 (46) 48 (47) Aggregate mm 12 (15) 3 (13) 15 (15) Which % linear extent do you use?")
 Surgeon Oncologist Total Here is a prostate cancer with 60% core involvement. Which tumour extent parameter do you use?")
4 What do clinicians really (really) want? Which mm linear extent do you use? Surg Onc Both Don't use 30 (38) 11 (46) 41 (40) mm each core 21 (27) 2 (8) 23 (22) Maximum mm in a core 37 (47) 11 (46) 48 (47) Aggregate mm 12 (15) 3 (13) 15 (15) Which % linear extent do you use? Don't use 24 (30) 3 (12) 27 (26) % each core 20 (25) 7 (27) 27 (26) maximum % in a core 25 (32) 8 (31) 33 (31) Aggregate % 33 (42) 10 (38) 43 (41) Other 0 (0) 2 (8) 2 (2) Survey Question Responses (percentage) Surgeon Oncologist Total Here is a prostate cancer with 60% core involvement. Which tumour extent parameter do you use? Number (+) cores 77 (97) 20 (83) 97 (94) Number (+) cores each side 35 (44) 8 (33) 43 (42) % number of cores 73 (92) 24 (100) 97 (94) mm linear extent 49 (62) 13 (54) 62 (60) And here is one with 20% core involvement! % linear extent 64 (81) 23 (96) 87 (84) 4

5 Percentages are determined by the amount of benign tissue biopsied! Precise measurements are pointless Different levels?! How long is a stromal gap and on which level? Biopsy measurement in age of mpmri Targeted Biased samples Should we be counting per SITE 5



6 Peri-Neural Invasion Is it worth the bother! Neurosafe Are we serving the patients, the clinicians or ourselves? TNM AJCC/UICC Editions Edition Publication Dates for cancer diagnosis 1st nd rd Is the data we provide of patient benefit? 4 th thy th th th




7 Changes in 7 th edition Which? Microscopic bladder neck invasion downstaged from pt4 to pt3a Gleason score recognised as preferred grading method Prognostic factors: Gleason and PSA incorporated into prognostic stage groups Changes in AJCC 8 th edition Pathologically organ confined disease no longer subclassified Gleason score by 2014 criteria and grade group given AJCC prognostic stage 3 includes some organ confined tumours based on PSA and grade Statistical prediction models included 7
8 Clinical ct category Which Errata? Tx T0 T1 T1a T1b T1c Primary tumour cannot be assessed No evidence of primary tumour Clinically inapparent tumour which is non palpable Incidental finding in 5% or less of tissue resected Incidental finding in more than 5% of the tissue resected Tumour found by needle biopsy but impalpable Present the changes in AJCC TNM 8 th edition Critically look at the evidence base Examine areas of doubt Potential for further refinements T2 T2a T2b T2c T3 T3a T3b T4 Tumour is palpable and confined within the prostate Tumour occupies 1 half of one side or less Tumour involves more than one half of one side but not both sides Tumour involves both sides Extra-prostatic tumour that is not fixed or does not invade adjacent structures Extra-prostatic extension Seminal vesicle invasion Fixed or invades other structures other than SVs (rectum, muscles, pelvic wall) 8

9 Do not use.. MRI CT Biopsy information on laterality Staging of TURP Chips T1a 5% involvement T1b More than 5% Cantrell BB et al. Pathological factors that influence prognosis in stage A prostatic cancer: the influence of extent versus grade. J Urol. 1981;125: patients followed for 2 to 15 years In 14 patients (12%) extensive local (2) or metastatic (12) disease developed. Extent and grade of disease accurately predicted progression. No patient with Gleason 2 to 4 had progression Patients with <5 % cancer; 2% had progression. Patients >5 % cancer; 32% had progression 9
10 How do you measure % involvement? 1. Estimate of area involved overall. 2. Count positive and negative chippings. Conclusions Preoperative ct staging by TNM still has huge variability as it uses low level technology and some historic data. Survival from prostate cancer (%) HR=2.08, 95% CI= P < Time since entry (years) cancerous chips <= 10% cancerous chips >10-25% cancerous chips >25-75% cancerous chips >75% pt staging Applicable only to men who have had a radical prostatectomy. Not WW, AM, RT, Brachytherapy, hormones etc etc! Rajab R et al. An improved prognostic model for stage T1a and T1b prostate cancer by assessments of cancer extent. Mod Pathol Jan;24(1):58-63 (Fig. 1). 10



11 PATHOLOGIC STAGE T2 T3 T4 T3a T3b Organ Confined CRITERIA Extraprostatic extension Extraprostatic extension (unilateral or bilateral) or microscopic invasion of bladder neck Tumour invades seminal vesicles Tumour is fixed or invades adjacent structures other than seminal vesicles such as external sphincter, rectum, bladder, levator muscles and/or pelvic wall 2a 2c 2b 11


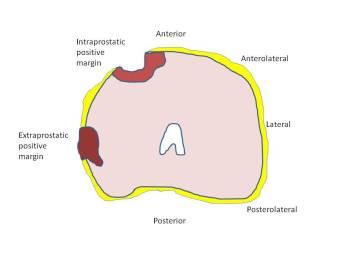
12 = pt2b What s also not there Tumour volume Extent of extra-prostatic extension Surgical margin assessment The prostatic capsule A condensed fibromusculr layer of prostatic stroma Well formed; Posterolateral Poorly seen Apex, anteriorly, bladder neck 12

 beyond the boundary of the")

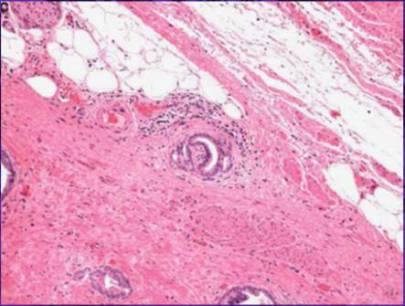
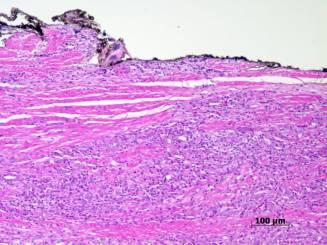
13 EPE The presence of neoplastic glands abutting on or within periprostatic fat or beyond the adjacent fat plane in situations where no fat is present in the immediate area of interest (most useful at the lateral, posterolateral and posterior aspects of the prostate) Neoplastic glands surrounding nerves in the neurovascular bundle (posterolaterally) beyond the boundary of the normal prostatic glandular tissue. A nodular extension of tumour bulging beyond the periphery of the prostate or beyond the compressed fibromuscular prostatic stroma at the outer edge of the gland. T3a 13

14 T2 or T3a? 14




15 Subclassification of pt3a disease Tumour is found outside the prostate to a depth of <1 high-power field in 1-2 Sections F-EPE a few neoplastic glands outside the prostate on 1-2 slides 15

16 Other TNM changes 16

17 Conclusions We need to lead and be better in biopsy reporting with education of clinicians and pathologists. TNM Improved from previous but still crude. Much further work is necessary to catch up with other organ risk prediction models Risk assessment tools 15 multivariate models assessed Only 2 models on metastatic disease from large Phase 3 studies accepted All OC models rejected! 17
I have no financial relationships to disclose. I WILL NOT include discussion of investigational or off-label use of a product in my presentation.
 Prostate t Cancer MR Report Disclosure Information Vikas Kundra, M.D, Ph.D. I have no financial relationships to disclose. I WILL NOT include discussion of investigational or off-label use of a g product
Prostate t Cancer MR Report Disclosure Information Vikas Kundra, M.D, Ph.D. I have no financial relationships to disclose. I WILL NOT include discussion of investigational or off-label use of a g product
3/23/2017. Significant Changes in Prostate Cancer Classification, Grading, Staging and Reporting. Disclosure of Relevant Financial Relationships
 Disclosure of Relevant Financial Relationships Staging and Reporting of Prostate Cancer: Major Changes in 8 th Edition AJCC Staging and CAP Cancer Checklists USCAP requires that all planners (Education
Disclosure of Relevant Financial Relationships Staging and Reporting of Prostate Cancer: Major Changes in 8 th Edition AJCC Staging and CAP Cancer Checklists USCAP requires that all planners (Education
S1.04 Principal clinician. G1.01 Comments. G2.01 *Specimen dimensions (prostate) S2.02 *Seminal vesicles
 S2.02 *Seminal vesicles") Prostate Cancer Histopathology Reporting Proforma (Radical Prostatectomy) Includes the International Collaboration on Cancer reporting dataset denoted by * Family name Given name(s) Date of birth Sex Male
Prostate Cancer Histopathology Reporting Proforma (Radical Prostatectomy) Includes the International Collaboration on Cancer reporting dataset denoted by * Family name Given name(s) Date of birth Sex Male
S1.04 PRINCIPAL CLINICIAN G1.01 COMMENTS S2.01 SPECIMEN LABELLED AS G2.01 *SPECIMEN DIMENSIONS (PROSTATE) S2.03 *SEMINAL VESICLES
 S2.03 *SEMINAL VESICLES") Prostate Cancer Histopathology Reporting Proforma (Radical Prostatectomy) Includes the International Collaboration on Cancer reporting dataset denoted by * Family name Given name(s) Date of birth Indigenous
Prostate Cancer Histopathology Reporting Proforma (Radical Prostatectomy) Includes the International Collaboration on Cancer reporting dataset denoted by * Family name Given name(s) Date of birth Indigenous
Prostate cancer ~ diagnosis and impact of pathology on prognosis ESMO 2017
 Prostate cancer ~ diagnosis and impact of pathology on prognosis ESMO 2017 Dr Puay Hoon Tan Division of Pathology Singapore General Hospital Prostate cancer (acinar adenocarcinoma) Invasive carcinoma composed
Prostate cancer ~ diagnosis and impact of pathology on prognosis ESMO 2017 Dr Puay Hoon Tan Division of Pathology Singapore General Hospital Prostate cancer (acinar adenocarcinoma) Invasive carcinoma composed
A schematic of the rectal probe in contact with the prostate is show in this diagram.
 Hello. My name is William Osai. I am a nurse practitioner in the GU Medical Oncology Department at The University of Texas MD Anderson Cancer Center in Houston. Today s presentation is Part 2 of the Overview
Hello. My name is William Osai. I am a nurse practitioner in the GU Medical Oncology Department at The University of Texas MD Anderson Cancer Center in Houston. Today s presentation is Part 2 of the Overview
Procedures Needle Biopsy Transurethral Prostatic Resection Suprapubic or Retropubic Enucleation (Subtotal Prostatectomy) Radical Prostatectomy
 Radical Prostatectomy") Prostate Gland Protocol applies to invasive carcinomas of the prostate gland. Protocol web posting date: July 2006 Protocol effective date: April 2007 Based on AJCC/UICC TNM, 6 th edition Procedures Needle
Prostate Gland Protocol applies to invasive carcinomas of the prostate gland. Protocol web posting date: July 2006 Protocol effective date: April 2007 Based on AJCC/UICC TNM, 6 th edition Procedures Needle
GUIDELINES ON PROSTATE CANCER
 10 G. Aus (chairman), C. Abbou, M. Bolla, A. Heidenreich, H-P. Schmid, H. van Poppel, J. Wolff, F. Zattoni Eur Urol 2001;40:97-101 Introduction Cancer of the prostate is now recognized as one of the principal
10 G. Aus (chairman), C. Abbou, M. Bolla, A. Heidenreich, H-P. Schmid, H. van Poppel, J. Wolff, F. Zattoni Eur Urol 2001;40:97-101 Introduction Cancer of the prostate is now recognized as one of the principal
AJCC Cancer Staging 8 th Edition. Prostate Chapter 58. Executive Committee, AJCC. Professor and Director, Duke Prostate Center
 AJCC Cancer Staging 8 th Edition Prostate Chapter 58 Judd W Moul, MD, FACS Executive Committee, AJCC Professor and Director, Duke Prostate Center Duke University Durham, North Carolina Validating science.
AJCC Cancer Staging 8 th Edition Prostate Chapter 58 Judd W Moul, MD, FACS Executive Committee, AJCC Professor and Director, Duke Prostate Center Duke University Durham, North Carolina Validating science.
Prostate Cancer Grading, Staging and Reporting: An Update Cristina Magi-Galluzzi, MD, PhD
 Prostate Cancer Grading, Staging and Reporting: An Update Cristina Magi-Galluzzi, MD, PhD Director, Genitourinary Pathology R.J. Tomsich Pathology & Laboratory Medicine Institute Professor of Pathology,
Prostate Cancer Grading, Staging and Reporting: An Update Cristina Magi-Galluzzi, MD, PhD Director, Genitourinary Pathology R.J. Tomsich Pathology & Laboratory Medicine Institute Professor of Pathology,
Protocol for the Examination of Specimens From Patients With Carcinoma of the Prostate Gland
 Protocol for the Examination of Specimens From Patients With Carcinoma of the Prostate Gland Version: Protocol Posting Date: June 2017 Includes ptnm requirements from the 8 th Edition, AJCC Staging Manual
Protocol for the Examination of Specimens From Patients With Carcinoma of the Prostate Gland Version: Protocol Posting Date: June 2017 Includes ptnm requirements from the 8 th Edition, AJCC Staging Manual
TOPICS FOR DISCUSSION
 INTERNATIONAL SOCIETY OF UROLOGIC PATHOLOGY PATHOLOGIC STAGING OF SELECT UROLOGIC MALIGNANCIES Mahul B. Amin, MD Professor and Chairman Pathology and Laboratory Medicine Cedars-Sinai Medical Center Los
INTERNATIONAL SOCIETY OF UROLOGIC PATHOLOGY PATHOLOGIC STAGING OF SELECT UROLOGIC MALIGNANCIES Mahul B. Amin, MD Professor and Chairman Pathology and Laboratory Medicine Cedars-Sinai Medical Center Los
GUIDELINEs ON PROSTATE CANCER
 GUIDELINEs ON PROSTATE CANCER (Text update March 2005: an update is foreseen for publication in 2010. Readers are kindly advised to consult the 2009 full text print of the PCa guidelines for the most recent
GUIDELINEs ON PROSTATE CANCER (Text update March 2005: an update is foreseen for publication in 2010. Readers are kindly advised to consult the 2009 full text print of the PCa guidelines for the most recent
A215- Urinary bladder cancer tissues
 A215- Urinary bladder cancer tissues (formalin fixed) For research use only Specifications: No. of cases: 45 Tissue type: Urinary bladder cancer tissues No. of spots: 2 spots from each cancer case (90
A215- Urinary bladder cancer tissues (formalin fixed) For research use only Specifications: No. of cases: 45 Tissue type: Urinary bladder cancer tissues No. of spots: 2 spots from each cancer case (90
Diagnosis, pathology and prognosis including variant pathology
 PROSTATE CANCER Diagnosis, pathology and prognosis including variant pathology No Conflict of Interest Universitat Autónoma de Barcelona F.Algaba Section of Pathology PROSTATE CANCER Diagnosis, pathology
PROSTATE CANCER Diagnosis, pathology and prognosis including variant pathology No Conflict of Interest Universitat Autónoma de Barcelona F.Algaba Section of Pathology PROSTATE CANCER Diagnosis, pathology
Collaborative Staging
 Slide 1 Collaborative Staging Site-Specific Instructions Prostate 1 In this presentation, we are going to take a closer look at the collaborative staging data items for the prostate primary site. Because
Slide 1 Collaborative Staging Site-Specific Instructions Prostate 1 In this presentation, we are going to take a closer look at the collaborative staging data items for the prostate primary site. Because
Q&A. Overview. Collecting Cancer Data: Prostate. Collecting Cancer Data: Prostate 5/5/2011. NAACCR Webinar Series 1
 Collecting Cancer Data: Prostate NAACCR 2010-2011 Webinar Series May 5, 2011 Q&A Please submit all questions concerning webinar content through the Q&A panel Overview NAACCR 2010-2011 Webinar Series 1
Collecting Cancer Data: Prostate NAACCR 2010-2011 Webinar Series May 5, 2011 Q&A Please submit all questions concerning webinar content through the Q&A panel Overview NAACCR 2010-2011 Webinar Series 1
Prostate Case Scenario 1
 Prostate Case Scenario 1 H&P 5/12/16: A 57-year-old Hispanic male presents with frequency of micturition, urinary urgency, and hesitancy associated with a weak stream. Over the past several weeks, he has
Prostate Case Scenario 1 H&P 5/12/16: A 57-year-old Hispanic male presents with frequency of micturition, urinary urgency, and hesitancy associated with a weak stream. Over the past several weeks, he has
Prostate MRI. Overview. Introduction 2/20/2015. Prostate cancer is most frequently diagnosed noncutaneous cancer in males (25%)
") Prostate MRI John Bell, MD Introduction Prostate Cancer Screening Staging Anatomy Prostate MRI overview Functional MRI Multiparametric Approach Indications Example Cases Overview Introduction Prostate
Prostate MRI John Bell, MD Introduction Prostate Cancer Screening Staging Anatomy Prostate MRI overview Functional MRI Multiparametric Approach Indications Example Cases Overview Introduction Prostate
Case Scenario 1. 4/19/13 Bone Scan: No scintigraphic findings to suggest skeletal metastases.
 Case Scenario 1 3/8/13 H&P 68 YR W/M presents w/elevated PSA. Patient is a non-smoker, current alcohol use. Physical Exam: On digital rectal exam the sphincter tone is normal and there is a 1 cm nodule
Case Scenario 1 3/8/13 H&P 68 YR W/M presents w/elevated PSA. Patient is a non-smoker, current alcohol use. Physical Exam: On digital rectal exam the sphincter tone is normal and there is a 1 cm nodule
Supplemental Information
 Supplemental Information Prediction of Prostate Cancer Recurrence using Quantitative Phase Imaging Shamira Sridharan 1, Virgilia Macias 2, Krishnarao Tangella 3, André Kajdacsy-Balla 2 and Gabriel Popescu
Supplemental Information Prediction of Prostate Cancer Recurrence using Quantitative Phase Imaging Shamira Sridharan 1, Virgilia Macias 2, Krishnarao Tangella 3, André Kajdacsy-Balla 2 and Gabriel Popescu
Collecting Cancer Data: Prostate Q&A. Overview. NAACCR Webinar Series June 11, 2009
 Collecting Cancer Data: Prostate NAACCR 2008-2009 Webinar Series June 11, 2009 Q&A Please submit all questions concerning webinar content through the Q&A panel Overview 2008-2009 NAACCR Webinar Series
Collecting Cancer Data: Prostate NAACCR 2008-2009 Webinar Series June 11, 2009 Q&A Please submit all questions concerning webinar content through the Q&A panel Overview 2008-2009 NAACCR Webinar Series
Chapter 2. Understanding My Diagnosis
 Chapter 2. Understanding My Diagnosis With contributions from Nancy L. Brown, Ph.D.,Palo Alto Medical Foundation Research Institute; and Patrick Swift, M.D., Alta Bates Comprehensive Cancer Program o Facts
Chapter 2. Understanding My Diagnosis With contributions from Nancy L. Brown, Ph.D.,Palo Alto Medical Foundation Research Institute; and Patrick Swift, M.D., Alta Bates Comprehensive Cancer Program o Facts
Recommendations for the Reporting of Prostate Carcinoma
 Recommendations for the Reporting of Prostate Carcinoma Association of Directors of Anatomic and Surgical Pathology * ADASP Reporting Guidelines It has been evident for decades that pathology reports are
Recommendations for the Reporting of Prostate Carcinoma Association of Directors of Anatomic and Surgical Pathology * ADASP Reporting Guidelines It has been evident for decades that pathology reports are
6/5/2010. Renal vein invasion & Capsule Penetration (T3a) Adrenal Gland involvement (T4 vs. M1) Beyond Gerota s Fascia? (?T4).
 Adrenal Gland involvement (T4 vs. M1) Beyond Gerota s Fascia? (?T4).") GU Cancer Staging: Updates and Challenging Areas 13 th Current Issues in Surgical Pathology San Francisco, CA June 5, 2010 Jeffry P. Simko, PhD, MD Associate Professor Departments of Urology and Anatomic
GU Cancer Staging: Updates and Challenging Areas 13 th Current Issues in Surgical Pathology San Francisco, CA June 5, 2010 Jeffry P. Simko, PhD, MD Associate Professor Departments of Urology and Anatomic
Large blocks in prostate and bladder pathology
 Large blocks in prostate and bladder pathology Farkas Sükösd Department of Pathology, University of Szeged The history of the large block technique in radical prostatectomy and cystectomy The first large
Large blocks in prostate and bladder pathology Farkas Sükösd Department of Pathology, University of Szeged The history of the large block technique in radical prostatectomy and cystectomy The first large
Comparative Analysis Research of Robotic Assisted Laparoscopic Prostatectomy
 Comparative Analysis Research of Robotic Assisted Laparoscopic Prostatectomy By: Jonathan Barlaan; Huy Nguyen Mentor: Julio Powsang, MD Reader: Richard Wilder, MD May 2, 211 Abstract Introduction: The
Comparative Analysis Research of Robotic Assisted Laparoscopic Prostatectomy By: Jonathan Barlaan; Huy Nguyen Mentor: Julio Powsang, MD Reader: Richard Wilder, MD May 2, 211 Abstract Introduction: The
Neoplasms of the Prostate and Bladder
 Neoplasms of the Prostate and Bladder 2015-2016 FCDS Educational Webcast Series Steven Peace, BS, CTR September 19, 2015 2015 Focus o Anatomy o SSS 2000 o MPH Rules o AJCC TNM 1 CDC & Florida DOH Attribution
Neoplasms of the Prostate and Bladder 2015-2016 FCDS Educational Webcast Series Steven Peace, BS, CTR September 19, 2015 2015 Focus o Anatomy o SSS 2000 o MPH Rules o AJCC TNM 1 CDC & Florida DOH Attribution
The Depth of Tumor Invasion is Superior to 8 th AJCC/UICC Staging System to Predict Patients Outcome in Radical Cystectomy.
 30 th Congress of the European Society of Pathology Tuesday, September 11, 2018 The Depth of Tumor Invasion is Superior to 8 th AJCC/UICC Staging System to Predict Patients Outcome in Radical Cystectomy.
30 th Congress of the European Society of Pathology Tuesday, September 11, 2018 The Depth of Tumor Invasion is Superior to 8 th AJCC/UICC Staging System to Predict Patients Outcome in Radical Cystectomy.
INTRADUCTAL LESIONS OF THE PROSTATE. Jonathan I. Epstein
 INTRADUCTAL LESIONS OF THE PROSTATE Jonathan I. Epstein Topics Prostatic intraepithelial neoplasia (PIN) Intraductal adenocarcinoma (IDC-P) Intraductal urothelial carcinoma Ductal adenocarcinoma High Prostatic
INTRADUCTAL LESIONS OF THE PROSTATE Jonathan I. Epstein Topics Prostatic intraepithelial neoplasia (PIN) Intraductal adenocarcinoma (IDC-P) Intraductal urothelial carcinoma Ductal adenocarcinoma High Prostatic
Update on Reporting Prostate Cancer Pathology
 Update on Reporting Prostate Cancer Pathology Dr. Andrew J. Evans MD, PhD, FACP, FRCPC Consultant in Genitourinary Pathology University Health Network, Toronto, ON None Disclosures Learning Objectives
Update on Reporting Prostate Cancer Pathology Dr. Andrew J. Evans MD, PhD, FACP, FRCPC Consultant in Genitourinary Pathology University Health Network, Toronto, ON None Disclosures Learning Objectives
New research in prostate brachytherapy
 New research in prostate brachytherapy Dr Ann Henry Associate Professor in Clinical Oncology University of Leeds and Leeds Cancer Centre PIVOTAL boost opening 2017 To evaluate - The benefits of pelvic
New research in prostate brachytherapy Dr Ann Henry Associate Professor in Clinical Oncology University of Leeds and Leeds Cancer Centre PIVOTAL boost opening 2017 To evaluate - The benefits of pelvic
ADENOCARCINOMA OF THE PROSTATE
 Ref : ADENOCARCINOMA OF THE PROSTATE Div. of Urology, Dept. Surgery Medical Faculty, University of Sumatera Utara Clinical Manual of Urology, (Philip M. Hanno et al eds), McGraw-Hill Int ed, 3 rd ed, 2001
Ref : ADENOCARCINOMA OF THE PROSTATE Div. of Urology, Dept. Surgery Medical Faculty, University of Sumatera Utara Clinical Manual of Urology, (Philip M. Hanno et al eds), McGraw-Hill Int ed, 3 rd ed, 2001
Diagnosis of prostate cancer
 Diagnosis of prostate cancer Epidemiology Prostate cancer (PC) is the most common cancer in men and the 2 nd cause of cancer death in the developed world. Incidence with age, reaching 80% at age 80 (at
Diagnosis of prostate cancer Epidemiology Prostate cancer (PC) is the most common cancer in men and the 2 nd cause of cancer death in the developed world. Incidence with age, reaching 80% at age 80 (at
20 Prostate Cancer Dan Ash
 20 Prostate Cancer Dan Ash 1 Introduction Prostate cancer is a disease of ageing men for which the aetiology remains unknown. The incidence rises up to 30 to 40% in men over 80. The symptoms of localised
20 Prostate Cancer Dan Ash 1 Introduction Prostate cancer is a disease of ageing men for which the aetiology remains unknown. The incidence rises up to 30 to 40% in men over 80. The symptoms of localised
SEER Summary Stage Still Here!
 SEER Summary Stage Still Here! CCRA NORTHERN REGION STAGING SYMPOSIUM SEPTEMBER 20, 2017 SEER Summary Stage Timeframe: includes all information available through completion of surgery(ies) in the first
SEER Summary Stage Still Here! CCRA NORTHERN REGION STAGING SYMPOSIUM SEPTEMBER 20, 2017 SEER Summary Stage Timeframe: includes all information available through completion of surgery(ies) in the first
Prostate Cancer Case Study 1. Medical Student Case-Based Learning
 Prostate Cancer Case Study 1 Medical Student Case-Based Learning The Case of Mr. Powers Prostatic Nodule The effervescent Mr. Powers is found by his primary care provider to have a prostatic nodule. You
Prostate Cancer Case Study 1 Medical Student Case-Based Learning The Case of Mr. Powers Prostatic Nodule The effervescent Mr. Powers is found by his primary care provider to have a prostatic nodule. You
Standards and Datasets for Reporting Cancers. Dataset for histopathology reports for prostatic carcinoma (2 nd edition) October 2009
 October 2009") Standards and Datasets for Reporting Cancers Dataset for histopathology reports for prostatic carcinoma (2 nd edition) October 2009 Unique document number Document name G084 Dataset for histopathology
Standards and Datasets for Reporting Cancers Dataset for histopathology reports for prostatic carcinoma (2 nd edition) October 2009 Unique document number Document name G084 Dataset for histopathology
11/10/2015. Prostate cancer in the U.S. Multi-parametric MRI of Prostate Diagnosis and Treatment Planning. NIH estimates for 2015.
 Multi-parametric MRI of Prostate Diagnosis and Treatment Planning Temel Tirkes, M.D. Associate Professor of Radiology Director, Genitourinary Radiology Indiana University School of Medicine Department
Multi-parametric MRI of Prostate Diagnosis and Treatment Planning Temel Tirkes, M.D. Associate Professor of Radiology Director, Genitourinary Radiology Indiana University School of Medicine Department
When to worry, when to test?
 Focus on CME at the University of Calgary Prostate Cancer: When to worry, when to test? Bryan J. Donnelly, MSc, MCh, FRCSI, FRCSC Presented at a Canadian College of Family Practitioner s conference (October
Focus on CME at the University of Calgary Prostate Cancer: When to worry, when to test? Bryan J. Donnelly, MSc, MCh, FRCSI, FRCSC Presented at a Canadian College of Family Practitioner s conference (October
Boot Camp Case Scenarios
 Boot Camp Case Scenarios Case Scenario 1 Patient is a 69-year-old white female. She presents with dyspnea on exertion, cough, and right rib pain. Patient is a smoker. 9/21/12 CT Chest FINDINGS: There is
Boot Camp Case Scenarios Case Scenario 1 Patient is a 69-year-old white female. She presents with dyspnea on exertion, cough, and right rib pain. Patient is a smoker. 9/21/12 CT Chest FINDINGS: There is
Prostate MRI for local staging and surgical planning in prostate cancer
 Prostate MRI for local staging and surgical planning in prostate cancer 15th Annual Floyd A. Fried Advances in Urology Symposium June 23, 2017 Ray Tan, MD, MSHPM Assistant Professor Disclosures None Objectives
Prostate MRI for local staging and surgical planning in prostate cancer 15th Annual Floyd A. Fried Advances in Urology Symposium June 23, 2017 Ray Tan, MD, MSHPM Assistant Professor Disclosures None Objectives
Are Prostate Carcinoma Clinical Stages T1c and T2 Similar?
 Clinical Urology Are Clinical Stages T1c and T2 Similar? International Braz J Urol Vol. 32 (2): 165-171, March - April, 2006 Are Prostate Carcinoma Clinical Stages T1c and T2 Similar? Athanase Billis,
Clinical Urology Are Clinical Stages T1c and T2 Similar? International Braz J Urol Vol. 32 (2): 165-171, March - April, 2006 Are Prostate Carcinoma Clinical Stages T1c and T2 Similar? Athanase Billis,
PSA. HMCK, p63, Racemase. HMCK, p63, Racemase
 Case 1 67 year old male presented with gross hematuria H/o acute prostatitis & BPH Urethroscopy: small, polypoid growth with a broad base emanating from the left side of the verumontanum Serum PSA :7 ng/ml
Case 1 67 year old male presented with gross hematuria H/o acute prostatitis & BPH Urethroscopy: small, polypoid growth with a broad base emanating from the left side of the verumontanum Serum PSA :7 ng/ml
Outline (1) Outline (2) Concepts in Prostate Pathology. Peculiarities of Prostate Cancer. Peculiarities of Prostate Cancer
 Outline (2) Concepts in Prostate Pathology. Peculiarities of Prostate Cancer. Peculiarities of Prostate Cancer") Concepts in Prostate Pathology Murali Varma Cardiff, UK wptmv@cf.ac.uk Sarajevo Nov 2013 Outline (1) Peculiarities of prostate cancer Peculiarities of prostate needle biopsy Needle bx vs. TURP Prostate
Concepts in Prostate Pathology Murali Varma Cardiff, UK wptmv@cf.ac.uk Sarajevo Nov 2013 Outline (1) Peculiarities of prostate cancer Peculiarities of prostate needle biopsy Needle bx vs. TURP Prostate
Case #1: 75 y/o Male (treated and followed by prostate cancer oncology specialist ).
.") SOLID TUMORS WORKSHOP Cases for review Prostate Cancer Case #1: 75 y/o Male (treated and followed by prostate cancer oncology specialist ). January 2009 PSA 4.4, 20% free; August 2009 PSA 5.2; Sept 2009
SOLID TUMORS WORKSHOP Cases for review Prostate Cancer Case #1: 75 y/o Male (treated and followed by prostate cancer oncology specialist ). January 2009 PSA 4.4, 20% free; August 2009 PSA 5.2; Sept 2009
Genitourinary Neoplasms Updated for 2012 Requirements and CSv02.04
 Presentation Outline Genitourinary Neoplasms Updated for 2012 Requirements and CSv02.04 X:\FCDS_PUB\wwwroot\downloads\Teleconfere nces\2013 FCDS Educational Webcast Series February 28, 2013 General Information
Presentation Outline Genitourinary Neoplasms Updated for 2012 Requirements and CSv02.04 X:\FCDS_PUB\wwwroot\downloads\Teleconfere nces\2013 FCDS Educational Webcast Series February 28, 2013 General Information
Genitourinary Neoplasms Updated for 2012 Requirements and CSv02.04
 Genitourinary Neoplasms Updated for 2012 Requirements and CSv02.04 X:\FCDS_PUB\wwwroot\downloads\Teleconfere nces\2013 FCDS Educational Webcast Series February 28, 2013 1 Steven Peace, BS, CTR Susan Smith
Genitourinary Neoplasms Updated for 2012 Requirements and CSv02.04 X:\FCDS_PUB\wwwroot\downloads\Teleconfere nces\2013 FCDS Educational Webcast Series February 28, 2013 1 Steven Peace, BS, CTR Susan Smith
Case Discussions: Prostate Cancer
 Case Discussions: Prostate Cancer Andrew J. Stephenson, MD FRCSC FACS Chief, Urologic Oncology Glickman Urological and Kidney Institute Cleveland Clinic Elevated PSA 1 54 yo, healthy male, family Hx of
Case Discussions: Prostate Cancer Andrew J. Stephenson, MD FRCSC FACS Chief, Urologic Oncology Glickman Urological and Kidney Institute Cleveland Clinic Elevated PSA 1 54 yo, healthy male, family Hx of
25 TH ICRO DEHRADUN STAGING OF GENITOURINARY MALIGNANCIES
 25 TH ICRO DEHRADUN STAGING OF GENITOURINARY MALIGNANCIES SPEAKER DR DEEPAK ABROL CLINICAL ONCOLOGIST JAND K HEALTH SERVICES CONSULTANT ONCOLOGIST MAHARISHI DAYANAND HOSPITAL AND MEDICAL RESEARCH CENTER
25 TH ICRO DEHRADUN STAGING OF GENITOURINARY MALIGNANCIES SPEAKER DR DEEPAK ABROL CLINICAL ONCOLOGIST JAND K HEALTH SERVICES CONSULTANT ONCOLOGIST MAHARISHI DAYANAND HOSPITAL AND MEDICAL RESEARCH CENTER
Prostate Pathology: Prostate Carcinoma, variants and Gleason Grading (Part 1)
") Prostate Pathology: Prostate Carcinoma, variants and Gleason Grading (Part 1) Jae Y. Ro, MD, PhD June 7, 2012 Ten Leading Cancer Types for the Estimated New Cancer Cases and Deaths By Sex, United States,
Prostate Pathology: Prostate Carcinoma, variants and Gleason Grading (Part 1) Jae Y. Ro, MD, PhD June 7, 2012 Ten Leading Cancer Types for the Estimated New Cancer Cases and Deaths By Sex, United States,
A re-audit of Prostate biopsies from January to December 2010 and 2013.
 A re-audit of Prostate biopsies from January to December 2010 and 2013. Dr. M S Siddiqui Consultant Histopathologist University Hospital of North Tees Stockton on Tees. Objectives To assess and compare
A re-audit of Prostate biopsies from January to December 2010 and 2013. Dr. M S Siddiqui Consultant Histopathologist University Hospital of North Tees Stockton on Tees. Objectives To assess and compare
Magnetic resonance imaging predictors of extracapsular extension of prostate cancer: Do they accurately reflect pt3 staging?
 Magnetic resonance imaging predictors of extracapsular extension of prostate cancer: Do they accurately reflect pt3 staging? Poster No.: C-1399 Congress: ECR 2010 Type: Scientific Exhibit Topic: Genitourinary
Magnetic resonance imaging predictors of extracapsular extension of prostate cancer: Do they accurately reflect pt3 staging? Poster No.: C-1399 Congress: ECR 2010 Type: Scientific Exhibit Topic: Genitourinary
da Vinci Prostatectomy
 da Vinci Prostatectomy Justin T. Lee MD Director of Robotic Surgery Urology Associates of North Texas (UANT) USMD Prostate Cancer Center (www.usmdpcc.com) Prostate Cancer Facts Prostate cancer Leading
da Vinci Prostatectomy Justin T. Lee MD Director of Robotic Surgery Urology Associates of North Texas (UANT) USMD Prostate Cancer Center (www.usmdpcc.com) Prostate Cancer Facts Prostate cancer Leading
Clinical Case Conference
 Clinical Case Conference Intermediate-risk prostate cancer 08/06/2014 Long Pham Clinical Case 64 yo man was found to have elevated PSA of 8.65. TRUS-biopies were negative. Surveillance PSA was 7.2 in 3
Clinical Case Conference Intermediate-risk prostate cancer 08/06/2014 Long Pham Clinical Case 64 yo man was found to have elevated PSA of 8.65. TRUS-biopies were negative. Surveillance PSA was 7.2 in 3
RECTAL CARCINOMA: A DISTANCE APPROACH. Stephanie Nougaret
 RECTAL CARCINOMA: A DISTANCE APPROACH Stephanie Nougaret stephanienougaret@free.fr Despite the major improvements that have been made due to total mesorectal excision (TME) management of rectal cancer
RECTAL CARCINOMA: A DISTANCE APPROACH Stephanie Nougaret stephanienougaret@free.fr Despite the major improvements that have been made due to total mesorectal excision (TME) management of rectal cancer
Case Scenario 1 Worksheet. Primary Site C44.4 Morphology 8743/3 Laterality 0 Stage/ Prognostic Factors
 CASE SCENARIO 1 9/10/13 HISTORY: Patient is a 67-year-old white male and presents with lesion located 4-5cm above his right ear. The lesion has been present for years. No lymphadenopathy. 9/10/13 anterior
CASE SCENARIO 1 9/10/13 HISTORY: Patient is a 67-year-old white male and presents with lesion located 4-5cm above his right ear. The lesion has been present for years. No lymphadenopathy. 9/10/13 anterior
Update on staging colorectal carcinoma, the 8 th edition AJCC. General overview of staging. When is staging required? 11/1/2017
 Update on staging colorectal carcinoma, the 8 th edition AJCC Dale C. Snover, MD November 3, 2017 General overview of staging Reason for uniform staging Requirements to use AJCC manual and/or CAP protocols
Update on staging colorectal carcinoma, the 8 th edition AJCC Dale C. Snover, MD November 3, 2017 General overview of staging Reason for uniform staging Requirements to use AJCC manual and/or CAP protocols
Localized at a focus, central point or locus. Localized finding distinct from neighboring tissues, not a threedimensional
 LEXICON ABNORMALITY Focal abnormality Focus Index Lesion Lesion Localized at a focus, central point or locus Localized finding distinct from neighboring tissues, not a threedimensional space occupying
LEXICON ABNORMALITY Focal abnormality Focus Index Lesion Lesion Localized at a focus, central point or locus Localized finding distinct from neighboring tissues, not a threedimensional space occupying
ACOS Inquiry and Response Selected Inquires CS Tumor Size/Extension Evaluation, CS Lymph Nodes Evaluation, CS Metastasis at Diagnosis Evaluation *
 ACOS Inquiry and Response Selected Inquires CS Tumor Size/Extension Evaluation, CS Lymph Nodes Evaluation, CS Metastasis at Diagnosis Evaluation * CS Tumor Size/Extension Evaluation 24842 12/11/2007: Q:
ACOS Inquiry and Response Selected Inquires CS Tumor Size/Extension Evaluation, CS Lymph Nodes Evaluation, CS Metastasis at Diagnosis Evaluation * CS Tumor Size/Extension Evaluation 24842 12/11/2007: Q:
Carcinoma of the Urinary Bladder Histopathology
 Carcinoma of the Urinary Bladder Histopathology Reporting Proforma (Radical & Partial Cystectomy, Cystoprostatectomy) Includes the International Collaboration on Cancer reporting dataset denoted by * Family
Carcinoma of the Urinary Bladder Histopathology Reporting Proforma (Radical & Partial Cystectomy, Cystoprostatectomy) Includes the International Collaboration on Cancer reporting dataset denoted by * Family
Prostate MRI: Who needs it?
 Prostate MRI: Who needs it? Fergus Coakley MD, Professor of Radiology and Urology, Vice Chair for Clinical Services, Chief of Abdominal Imaging, UCSF Abdominal Imaging Magnetic Resonance Science Center
Prostate MRI: Who needs it? Fergus Coakley MD, Professor of Radiology and Urology, Vice Chair for Clinical Services, Chief of Abdominal Imaging, UCSF Abdominal Imaging Magnetic Resonance Science Center
ACCME/Disclosures. Cribriform Lesions of the Prostate. Case
 Cribriform Lesions of the Prostate Ming Zhou, MD, PhD Departments of Pathology and Urology New York University Langone Medical Center New York, NY Ming.Zhou@NYUMC.ORG ACCME/Disclosures The USCAP requires
Cribriform Lesions of the Prostate Ming Zhou, MD, PhD Departments of Pathology and Urology New York University Langone Medical Center New York, NY Ming.Zhou@NYUMC.ORG ACCME/Disclosures The USCAP requires
The importance of maximal restoration of peri-prostatic support
 Providing the best evidence for each surgical option in organ confined prostate cancer The importance of maximal restoration of peri-prostatic support A. Mottrie ORSI-Academy Melle Belgium OLV Hospital
Providing the best evidence for each surgical option in organ confined prostate cancer The importance of maximal restoration of peri-prostatic support A. Mottrie ORSI-Academy Melle Belgium OLV Hospital
Uropathology January Jon Oxley
 Uropathology January 2012 Jon Oxley Background to seminar These slides were available to view via the web from scanned slides The junior pathologists answered questions on them via the web The answers
Uropathology January 2012 Jon Oxley Background to seminar These slides were available to view via the web from scanned slides The junior pathologists answered questions on them via the web The answers
Quality ID #250 (NQF 1853): Radical Prostatectomy Pathology Reporting National Quality Strategy Domain: Effective Clinical Care
: Radical Prostatectomy Pathology Reporting National Quality Strategy Domain: Effective Clinical Care") Quality ID #250 (NQF 1853): Radical Prostatectomy Pathology Reporting National Quality Strategy Domain: Effective Clinical Care 2018 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY MEASURE TYPE: Process
Quality ID #250 (NQF 1853): Radical Prostatectomy Pathology Reporting National Quality Strategy Domain: Effective Clinical Care 2018 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY MEASURE TYPE: Process
Evaluation of the 7th American Joint Committee on Cancer TNM Staging System for Prostate Cancer in Point of Classification of Bladder Neck Invasion
 Jpn J Clin Oncol 2013;43(2)184 188 doi:10.1093/jjco/hys196 Advance Access Publication 5 December 2012 Evaluation of the 7th American Joint Committee on Cancer TNM Staging System for Prostate Cancer in
Jpn J Clin Oncol 2013;43(2)184 188 doi:10.1093/jjco/hys196 Advance Access Publication 5 December 2012 Evaluation of the 7th American Joint Committee on Cancer TNM Staging System for Prostate Cancer in
Some prostatic diseases
 Some prostatic diseases Benign Prostatic Hyperplasia (Nodular Hyperplasia) Extremely common Present in a significant number of men by the age of 40 & its frequency rises progressively with age, reaching
Some prostatic diseases Benign Prostatic Hyperplasia (Nodular Hyperplasia) Extremely common Present in a significant number of men by the age of 40 & its frequency rises progressively with age, reaching
Aram Kim 4, Myong Kim 1, Se Un Jeong 2, Cheryn Song 1, Yong Mee Cho 2, Jae Yoon Ro 3 and Hanjong Ahn 1*
 Kim et al. BMC Urology (2018) 18:7 DOI 10.1186/s12894-018-0321-z RESEARCH ARTICLE Open Access Level of invasion into fibromuscular band is an independent factor for positive surgical margin and biochemical
Kim et al. BMC Urology (2018) 18:7 DOI 10.1186/s12894-018-0321-z RESEARCH ARTICLE Open Access Level of invasion into fibromuscular band is an independent factor for positive surgical margin and biochemical
Pathologic Assessment of Invasion in TUR Specimens. A. Lopez-Beltran. T1 (ct1)
") Pathologic Assessment of Invasion in TUR Specimens A. Lopez-Beltran T1 (ct1) 1 Prognostic factors for progression/invasive disease Ta,T1,CIS- NMIBC :TNM 2017 ESSENTIAL: Grade T stage CIS Number of lesions
Pathologic Assessment of Invasion in TUR Specimens A. Lopez-Beltran T1 (ct1) 1 Prognostic factors for progression/invasive disease Ta,T1,CIS- NMIBC :TNM 2017 ESSENTIAL: Grade T stage CIS Number of lesions
UICC TNM 8 th Edition Errata
 UICC TNM 8 th Edition Errata ions are in italics Head and Neck Tumours Pages 20, p27, p34, p38, p41, and p49 ly pn2a Metastasis in a single ipsilateral lymph node, less than 3cm in greatest dimension with
UICC TNM 8 th Edition Errata ions are in italics Head and Neck Tumours Pages 20, p27, p34, p38, p41, and p49 ly pn2a Metastasis in a single ipsilateral lymph node, less than 3cm in greatest dimension with
The Role of the Pathologist Active Surveillance for Prostate Cancer
 The Role of the Pathologist Active Surveillance for Prostate Cancer Thomas M. Wheeler, M.D. W. L. Moody, Jr., Professor and Chair Department of Pathology & Immunology Baylor College of Medicine Houston,
The Role of the Pathologist Active Surveillance for Prostate Cancer Thomas M. Wheeler, M.D. W. L. Moody, Jr., Professor and Chair Department of Pathology & Immunology Baylor College of Medicine Houston,
Prostatectomy as salvage therapy. Cases. Paul Cathcart - Guy s & St Thomas NHS Trust, London
 Prostatectomy as salvage therapy Cases Paul Cathcart - Guy s & St Thomas NHS Trust, London Attributes of brachytherapy appeal to young men who place high utility on genitourinary function At risk of
Prostatectomy as salvage therapy Cases Paul Cathcart - Guy s & St Thomas NHS Trust, London Attributes of brachytherapy appeal to young men who place high utility on genitourinary function At risk of
CONTEMPORARY UPDATE OF PROSTATE CANCER STAGING NOMOGRAMS (PARTIN TABLES) FOR THE NEW MILLENNIUM
 FOR THE NEW MILLENNIUM") RAPID COMMUNICATION CME ARTICLE CONTEMPORARY UPDATE OF PROSTATE CANCER STAGING NOMOGRAMS (PARTIN TABLES) FOR THE NEW MILLENNIUM ALAN W. PARTIN, LESLIE A. MANGOLD, DANA M. LAMM, PATRICK C. WALSH, JONATHAN
RAPID COMMUNICATION CME ARTICLE CONTEMPORARY UPDATE OF PROSTATE CANCER STAGING NOMOGRAMS (PARTIN TABLES) FOR THE NEW MILLENNIUM ALAN W. PARTIN, LESLIE A. MANGOLD, DANA M. LAMM, PATRICK C. WALSH, JONATHAN
Prostate Cancer: Screening, Treatment, and Survivorship
 Prostate Cancer: Screening, Treatment, and Survivorship Timothy C. Brand, MD, FACS LTC(P), MC, USA Urology Residency Director Associate Professor of Surgery, USUHS Madigan Army Medical Center No Disclosures
Prostate Cancer: Screening, Treatment, and Survivorship Timothy C. Brand, MD, FACS LTC(P), MC, USA Urology Residency Director Associate Professor of Surgery, USUHS Madigan Army Medical Center No Disclosures
Protocol for the Examination of Specimens from Patients with Carcinoma of the Prostate Gland
 Protocol for the Examination of Specimens from Patients with Carcinoma of the Prostate Gland Protocol applies to invasive carcinomas of the prostate gland. This modified NB CAP version has not been reviewed,
Protocol for the Examination of Specimens from Patients with Carcinoma of the Prostate Gland Protocol applies to invasive carcinomas of the prostate gland. This modified NB CAP version has not been reviewed,
S Crouzet, O Rouvière, JY Chapelon, F Mege, X martin, A Gelet
 S Crouzet, O Rouvière, JY Chapelon, F Mege, X martin, A Gelet Why HIFU? Efficacy demonstrated Real time control of the target Early control of the necrosis area is possible with MRI or TRUS using contrast
S Crouzet, O Rouvière, JY Chapelon, F Mege, X martin, A Gelet Why HIFU? Efficacy demonstrated Real time control of the target Early control of the necrosis area is possible with MRI or TRUS using contrast
UICC TNM 8 th Edition Errata
 UICC TNM 8 th Edition Errata ions are in italics Page 28 Oropharynx p16 positive Pathological Stage II,T2 N2 M0 T3 N0,N1 M0 Stage II,T2 N2 M0 T3,T4 N0,N1 M0 Page 61 Oesophagus Adenocarcinoma Pathological
UICC TNM 8 th Edition Errata ions are in italics Page 28 Oropharynx p16 positive Pathological Stage II,T2 N2 M0 T3 N0,N1 M0 Stage II,T2 N2 M0 T3,T4 N0,N1 M0 Page 61 Oesophagus Adenocarcinoma Pathological
Radical prostatectomy as radical cure of prostate cancer in a high risk group: A single-institution experience
 MOLECULAR AND CLINICAL ONCOLOGY 1: 337-342, 2013 Radical prostatectomy as radical cure of prostate cancer in a high risk group: A single-institution experience NOBUKI FURUBAYASHI 1, MOTONOBU NAKAMURA 1,
MOLECULAR AND CLINICAL ONCOLOGY 1: 337-342, 2013 Radical prostatectomy as radical cure of prostate cancer in a high risk group: A single-institution experience NOBUKI FURUBAYASHI 1, MOTONOBU NAKAMURA 1,
B REAST STAGING FORM. PATHOLOGIC Extent of disease through completion of definitive surgery. CLINICAL Extent of disease before any treatment
 B REAST STAGING FORM CLINICAL Extent of disease before any treatment y clinical staging completed after neoadjuvant therapy but before subsequent surgery (DCIS) (LCIS) (Paget s) mi c a b c d TUMOR SIZE:
B REAST STAGING FORM CLINICAL Extent of disease before any treatment y clinical staging completed after neoadjuvant therapy but before subsequent surgery (DCIS) (LCIS) (Paget s) mi c a b c d TUMOR SIZE:
Anatomic distribution and pathologic characterization of small-volume prostate cancer (o0.5 ml) in whole-mount prostatectomy specimens
 in whole-mount prostatectomy specimens") & 2005 USCAP, Inc All rights reserved 0893-3952/05 $30.00 www.modernpathology.org Anatomic distribution and pathologic characterization of small-volume prostate cancer (o0.5 ml) in whole-mount prostatectomy
& 2005 USCAP, Inc All rights reserved 0893-3952/05 $30.00 www.modernpathology.org Anatomic distribution and pathologic characterization of small-volume prostate cancer (o0.5 ml) in whole-mount prostatectomy
B REAST STAGING FORM. PATHOLOGIC Extent of disease through completion of definitive surgery. CLINICAL Extent of disease before any treatment
 B REAST STAGING FORM Extent of disease before any treatment y clinical staging completed after neoadjuvant therapy but before subsequent surgery (DCIS) (LCIS) (Paget s) mi a b c a b c d TUMOR SIZE: S TAGE
B REAST STAGING FORM Extent of disease before any treatment y clinical staging completed after neoadjuvant therapy but before subsequent surgery (DCIS) (LCIS) (Paget s) mi a b c a b c d TUMOR SIZE: S TAGE
PLACE LABEL HERE. ACRIN 6659 Registration/Eligibility Institution
 A0 ACRIN 6659 Registration/Eligibility No Case No Instructions: For potential study participants, Part 2 must be completed before Part 1 If any of the answers, for Part 2, vary from the prompts provided
A0 ACRIN 6659 Registration/Eligibility No Case No Instructions: For potential study participants, Part 2 must be completed before Part 1 If any of the answers, for Part 2, vary from the prompts provided
Definition of Synoptic Reporting
 Definition of Synoptic Reporting The CAP has developed this list of specific features that define synoptic reporting formatting: 1. All required cancer data from an applicable cancer protocol that are
Definition of Synoptic Reporting The CAP has developed this list of specific features that define synoptic reporting formatting: 1. All required cancer data from an applicable cancer protocol that are
Prognostic value of the Gleason score in prostate cancer
 BJU International (22), 89, 538 542 Prognostic value of the Gleason score in prostate cancer L. EGEVAD, T. GRANFORS*, L. KARLBERG*, A. BERGH and P. STATTIN Department of Pathology and Cytology, Karolinska
BJU International (22), 89, 538 542 Prognostic value of the Gleason score in prostate cancer L. EGEVAD, T. GRANFORS*, L. KARLBERG*, A. BERGH and P. STATTIN Department of Pathology and Cytology, Karolinska
Prognostic Value of Surgical Margin Status for Biochemical Recurrence Following Radical Prostatectomy
 Original Article Japanese Journal of Clinical Oncology Advance Access published January 17, 2008 Jpn J Clin Oncol doi:10.1093/jjco/hym135 Prognostic Value of Surgical Margin Status for Biochemical Recurrence
Original Article Japanese Journal of Clinical Oncology Advance Access published January 17, 2008 Jpn J Clin Oncol doi:10.1093/jjco/hym135 Prognostic Value of Surgical Margin Status for Biochemical Recurrence
Catholic University of Louvain, St - Luc University Hospital Head and Neck Oncology Programme. Anatomopathology. Pathology 1 Sept.
 Anatomopathology Pathology 1 Anatomopathology Biopsies Frozen section Surgical specimen Peculiarities for various tumor site References Pathology 2 Biopsies Minimum data, which should be given by the pathologist
Anatomopathology Pathology 1 Anatomopathology Biopsies Frozen section Surgical specimen Peculiarities for various tumor site References Pathology 2 Biopsies Minimum data, which should be given by the pathologist
1/25/13 Right partial nephrectomy followed by completion right radical nephrectomy.
 History and Physical Case Scenario 1 45 year old white male presents with complaints of nausea, weight loss, and back pain. A CT of the chest, abdomen and pelvis was done on 12/8/12 that revealed a 12
History and Physical Case Scenario 1 45 year old white male presents with complaints of nausea, weight loss, and back pain. A CT of the chest, abdomen and pelvis was done on 12/8/12 that revealed a 12
Gross appearance of nodular hyperplasia in material obtained from suprapubic prostatectomy. Note the multinodular appearance and the admixture of
 Tiền liệt tuyến Tiền liệt tuyến Gross appearance of nodular hyperplasia in material obtained from suprapubic prostatectomy. Note the multinodular appearance and the admixture of solid and microcystic areas.
Tiền liệt tuyến Tiền liệt tuyến Gross appearance of nodular hyperplasia in material obtained from suprapubic prostatectomy. Note the multinodular appearance and the admixture of solid and microcystic areas.
Prognostic factors of genitourinary tumors: Do we have to care?
 Prognostic factors of genitourinary tumors: Do we have to care? Jae Y. Ro, MD, PhD Professor and Director of Surgical Pathology The Methodist Hospital, Weill Medical College of Cornell University, Houston,
Prognostic factors of genitourinary tumors: Do we have to care? Jae Y. Ro, MD, PhD Professor and Director of Surgical Pathology The Methodist Hospital, Weill Medical College of Cornell University, Houston,
Adenocarcinoma of the Prostate Part II: Tissue Prognosticators
 ANATOMIC PATHOLOGY Review Article Adenocarcinoma of the Prostate Part II: Tissue Prognosticators PETER A. HUMPHREY, MD, PHD,* AND PHILIP J. WALTHER, MD, PHDf In this second review article of a two-part
ANATOMIC PATHOLOGY Review Article Adenocarcinoma of the Prostate Part II: Tissue Prognosticators PETER A. HUMPHREY, MD, PHD,* AND PHILIP J. WALTHER, MD, PHDf In this second review article of a two-part
MUSCLE - INVASIVE AND METASTATIC BLADDER CANCER
 10 MUSCLE - INVASIVE AND METASTATIC BLADDER CANCER Recommendations from the EAU Working Party on Muscle Invasive and Metastatic Bladder Cancer G. Jakse (chairman), F. Algaba, S. Fossa, A. Stenzl, C. Sternberg
10 MUSCLE - INVASIVE AND METASTATIC BLADDER CANCER Recommendations from the EAU Working Party on Muscle Invasive and Metastatic Bladder Cancer G. Jakse (chairman), F. Algaba, S. Fossa, A. Stenzl, C. Sternberg
OMPRN Pathology Matters Meeting 2017
 OMPRN Pathology Matters Meeting 2017 Pathology of Aggressive Prostate Cancer Intraductal Carcinoma and Cribriform Carcinoma Dr. Michelle Downes, Staff Urologic Pathologist Sunnybrook Health Sciences Centre,
OMPRN Pathology Matters Meeting 2017 Pathology of Aggressive Prostate Cancer Intraductal Carcinoma and Cribriform Carcinoma Dr. Michelle Downes, Staff Urologic Pathologist Sunnybrook Health Sciences Centre,
David Gillatt Bristol Urological Institute. David Gillatt Bristol UK
 David Gillatt Bristol Urological Institute David Gillatt Bristol UK Prostate Problems The prostate grows with age - >80% men over 60 have benign enlargement As it grows it can obstruct the flow of urine
David Gillatt Bristol Urological Institute David Gillatt Bristol UK Prostate Problems The prostate grows with age - >80% men over 60 have benign enlargement As it grows it can obstruct the flow of urine
Prostate Cancer MRI. Accurate Diagnosis and Treatment. PSA to Prostate MRI. for patients and curious doctors
 6 Prostate Cancer MRI Accurate Diagnosis and Treatment PSA to Prostate MRI for patients and curious doctors Samuel Aronson, M.D. Vincent Pelsser, M.D. Franck Bladou, M.D. Armen Aprikian, M.D. & Marc Emberton,
6 Prostate Cancer MRI Accurate Diagnosis and Treatment PSA to Prostate MRI for patients and curious doctors Samuel Aronson, M.D. Vincent Pelsser, M.D. Franck Bladou, M.D. Armen Aprikian, M.D. & Marc Emberton,
What Is Prostate Cancer? Prostate cancer is the development of cancer cells in the prostate gland (a gland that produces fluid for semen).
.") What Is Prostate Cancer? Prostate cancer is the development of cancer cells in the prostate gland (a gland that produces fluid for semen). It is a very common cancer in men; some cancers grow very slowly,
What Is Prostate Cancer? Prostate cancer is the development of cancer cells in the prostate gland (a gland that produces fluid for semen). It is a very common cancer in men; some cancers grow very slowly,
Disease-specific death and metastasis do not occur in patients with Gleason score 6 at radical prostatectomy
 Disease-specific death and metastasis do not occur in patients with at radical prostatectomy Charlotte F. Kweldam, Mark F. Wildhagen*, Chris H. Bangma* and Geert J.L.H. van Leenders Departments of Pathology,
Disease-specific death and metastasis do not occur in patients with at radical prostatectomy Charlotte F. Kweldam, Mark F. Wildhagen*, Chris H. Bangma* and Geert J.L.H. van Leenders Departments of Pathology,
Procedures Needle Biopsy Transurethral Prostatic Resection Suprapubic or Retropubic Enucleation (Subtotal Prostatectomy) Radical Prostatectomy
 Radical Prostatectomy") Prostate Gland Protocol applies to invasive carcinomas of the prostate gland. Protocol web posting date: July 2006 Protocol effective date: April 2007 Based on AJCC/UICC TNM, 6 th edition Procedures Needle
Prostate Gland Protocol applies to invasive carcinomas of the prostate gland. Protocol web posting date: July 2006 Protocol effective date: April 2007 Based on AJCC/UICC TNM, 6 th edition Procedures Needle
Multiparametric MR Imaging of the Prostate after Treatment of Prostate Cancer
 Multiparametric MR Imaging of the Prostate after Treatment of Prostate Cancer RadioGraphics 2018; 38:437 449 Pritesh Patel, MD Melvy S. Mathew, MD Igor Trilisky, MD Aytekin Oto, MD, MBA Jeffrey S. Klein,
Multiparametric MR Imaging of the Prostate after Treatment of Prostate Cancer RadioGraphics 2018; 38:437 449 Pritesh Patel, MD Melvy S. Mathew, MD Igor Trilisky, MD Aytekin Oto, MD, MBA Jeffrey S. Klein,