Update on staging colorectal carcinoma, the 8 th edition AJCC. General overview of staging. When is staging required? 11/1/2017
|
|
|
- Sabrina Leonard
- 6 years ago
- Views:
Transcription
1 Update on staging colorectal carcinoma, the 8 th edition AJCC Dale C. Snover, MD November 3, 2017 General overview of staging Reason for uniform staging Requirements to use AJCC manual and/or CAP protocols CAP accreditation American college of surgeons program standards Differences between AJCC manual and CAP protocols Who decides what is in the AJCC manual and CAP protocols When is staging required? Colon/rectal resection (segmental, partial, total, low anterior or AP resection) For all carcinomas including small and large cell high grade NE carcinomas Not for low grade NE tumors, sarcomas or lymphomas Not required for Primary resection specimens with no residual cancer (e.g. following neoadjuvant therapy) Polypectomies/excisional biopsies Local submucosal (anal disc) excisions Cytology specimens 1
2 Differences between AJCC and CAP protocols AJCC revised about every 7 years CAP revised more frequently Even for the 8 th edition, some minor differences exist AJCC list of histopathological type does not include several subtypes including micropapillary and serrated adenocarcinomas Grading of specific subtypes (medullary, signet ring) are not directly addressed Generally the CAP protocols seem more complete Basic principles of staging TMN stages Global stage Required elements Optional elements Issues with TNM staging TNM results in a global stage for a tumor but does not include all relevant prognostic information Generally covered under Additional factors recommended for clinical care This can result in undertreatment (i.e. all Stage II colon carcinoma is not the same) This has resulted in some unusual staging decisions, like N1c 2
3 Required elements Required by AJCC and CAP to be included in every report Which implies general consensus on the clinical significance of these findings Optional elements Used at the discretion or the pathologist or as driven by local clinical requests Some elements that most authorities consider prognostically important are not included as required elements, most notably tumor budding pt-categories Areas of controversy or 8 th edition change in red ptx primary tumor cannot be assessed pt0 no evidence of primary tumor ptis intramucosal carcinoma (so why is it still called is?) pt1 - invasion into submucosa pt2 invasion into muscularis propria pt3 invasion through muscularis propria pt4 invasion into visceral peritoneum (pt4a) or adjacent structures (pt4b) 3
4 pn-categories Areas of controversy or 8 th edition change in red pnx cannot be assessed pn0 no regional node metastases pn0(i+) metastases <0.2 mm pn1a one metastasis > 0.2 mm pn1b 2-3 metastases pn1c non-nodal tumor deposits without identified LN metastases pn2a 4 6 metastases pn2b 7 or more metastases pm-categories Areas of controversy or 8 th edition change in red Note that there is no pmx M0 No distant metastases by imaging (not assigned by pathologist) M1 Metastasis to one or more distant site M1a metastasis to one site/organ without peritoneal involvement M1b metastases to two or more sites/organs without peritoneal involvement M1c peritoneal involvement regardless of other organ involvement Controversies and 8 th edition changes T-stage What constitutes invasion Definition of pt4a N-stage What to do with non-nodal tumor deposits What to do with isolated tumor cells Ancillary issues What to do with tumor budding Grading non-conventional pattern carcinomas Deletion of histological features suggesting microsatellite instability Use of molecular markers 4
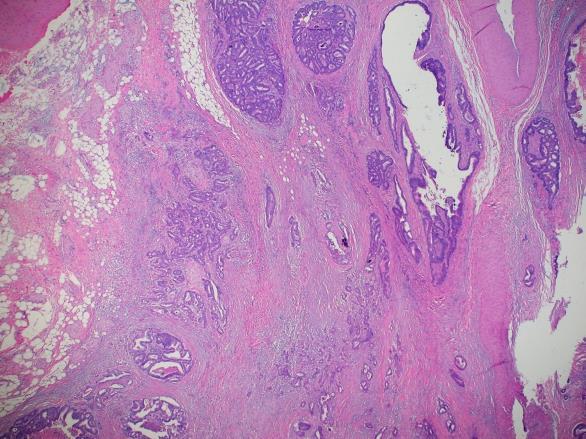
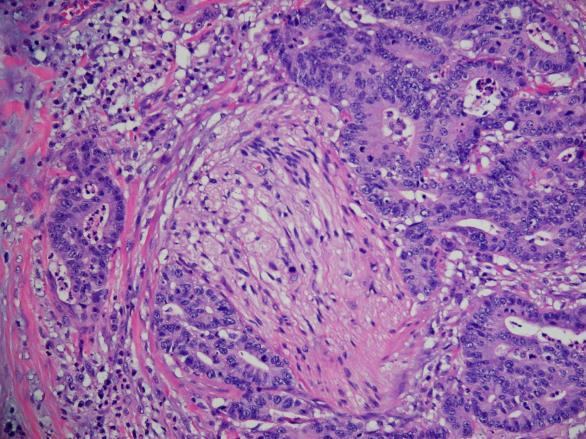
5 What constitutes invasion In the 6 th and 7 th edition of AJCC, invasion was defined by invasion into the submucosa Tis tumor limited to lamina propria above muscularis mucosa (included both non-invasive high grade dysplasia and intramucosal invasion) T1 tumor invading through muscularis mucosa into submucosa So, what to do with tumors into but not through the muscularis mucosa? What is the significance of the MM in terms of invasion The existing dogma is that tumors that have not invaded through the MM do not have access to lymphatics and do not metastasize However, it is clear that lymphatics do exist in the lamina propria, especially in neoplastic polyps and cancers and lymph node metastases can occur Into the MM A not uncommon problem in polyps In neoplastic polyps, the MM is often splayed and thickened, making determination of invasion through the MM difficult 5
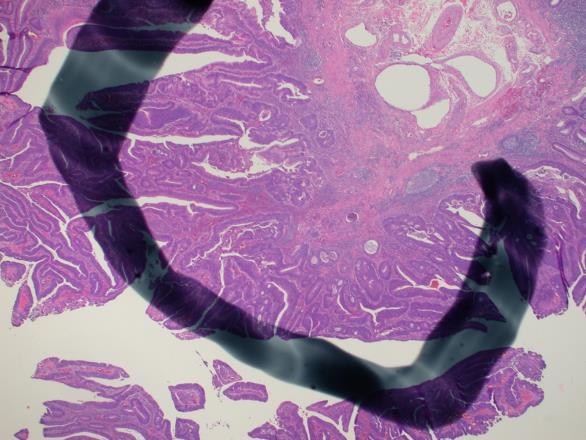
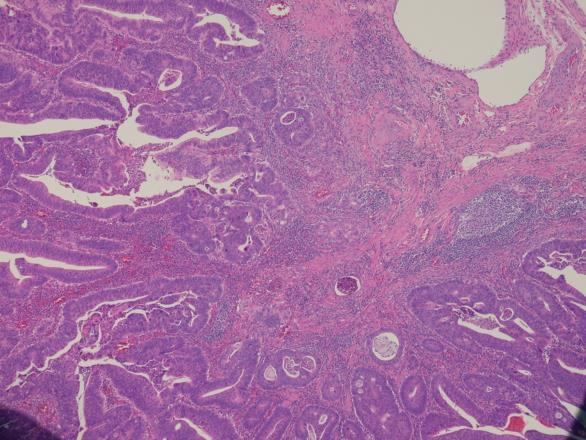
6 6


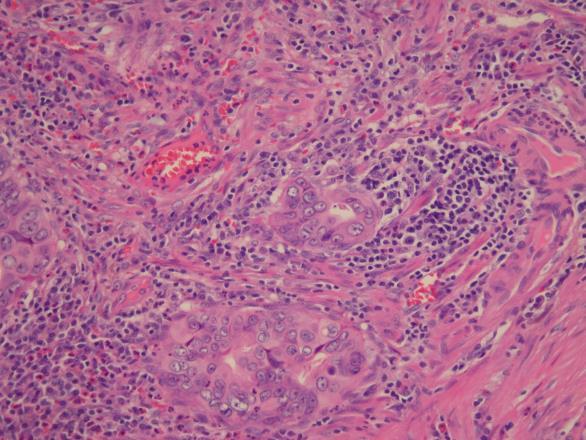
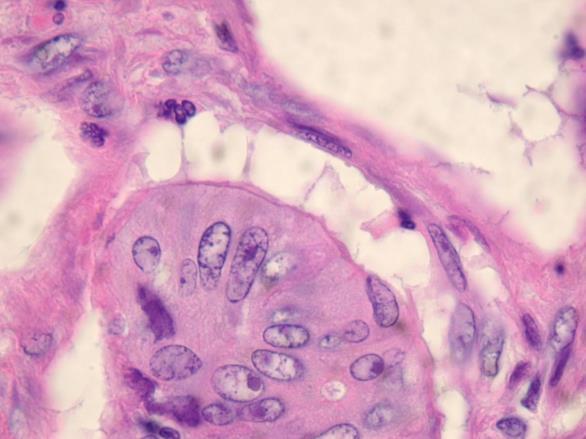
7 D2-40 So Tumors invading into the muscularis mucosa do have some capacity for lymph node metastasis 7
8 8 th edition revision of definition of invasion In the 8 th edition the definition of invasion and the difference between Tis and T1 has been clarified High grade dysplasia is no longer considered Tis Tis refers to intramucosal invasion and also invasion into but not through the muscularis mucosae So why is it still called is???? T1 is defined by invasion into the submucosa This distinction is probably more important in polyps with focal invasive carcinoma T4a vs 4b What are the issues? Which is worse, 4a or 4b? What constitutes peritoneal surface involvement Including new definition for 8 th edition Definitions of T4a and T4b 6 th edition T4a: tumor invading adjacent organs directly T4b: tumor involving the free peritoneal surface 7 th and 8 th edition (as well as the last CAP revision of the 6 th edition) T4a: tumor involving free peritoneal surface T4b: tumor invading adjacent organs 8

9 Why the change? 6 th edition decision based study by Shepard et al demonstrating worse prognosis for surface involvement than invasion of adjacent organs Why? Perhaps because invasion of adjacent organs is confined disease and can be resected 7 th and 8 th edition decision based on large analysis of SEER data showing just the opposite But, is SEER data really better just because the study is larger? After all, there is no quality control for pathology in the SEER data, and the data analyzed was from , when different criteria were used for peritoneal involvement What constitutes surface involvement anyway? 5 th edition Tumor on surface, ulceration of tumor on surface, and desmoplastic reaction to tumor involving surface 6th and 7 th editions Only tumor on surface or ulceration of tumor on surface T4a 9


10 Not T4a Not T4a but deserves additional sampling or levels New to the 8 th edition Surface involvement is considered present if there is perforation of tumor into inflammatory debris on the external surface of the colon 10


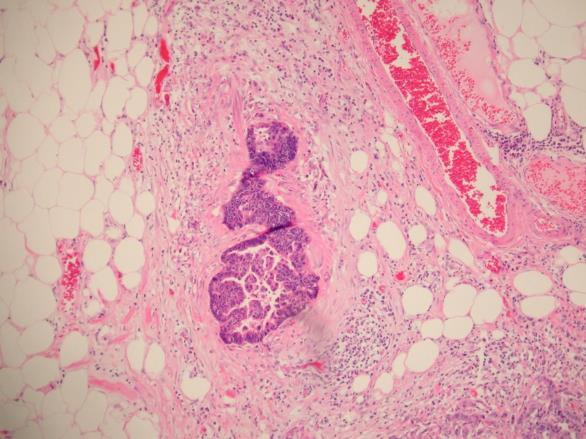
11 T4a by virtue of tumor cells in the inflammatory cap Issues involving lymph nodes Tumor deposits AKA non-nodal tumor deposits, previously also known as discontinuous extramural extension Isolated tumor cells (pn0(i+)) Surprisingly, ITCs have been part of the lexicon of colon cancer since the 5 th edition, although most pathologists were not aware of ITCs except in breast carcinoma 11

12 The history of N1c and non-nodal tumor deposits Non-nodal tumor deposits are nodules of tumor in the fat surrounding the colon that are not obviously associated with a lymph node They are clearly recognized as having prognostic significance greater than that of lymph node metastases, but have suffered from varying definitions and reporting requirements The history of N1c and non-nodal tumor deposits 5 th edition defined by size < 3mm = discontinous extramural extension considered part of T-category (T3) >3mm = replaced lymph node Counted with lymph nodes 6 th edition defined by shape Round contour resembling node = replaced lymph node (pn) Irregular contour = discontinuous extramural extension (i.e. non-nodal tumor deposit) Considered to be vascular invasion (pv) 12
13 The history of N1c and non-nodal tumor deposits 7 th edition still defined by shape as in 6 th However, any non-nodal tumor deposit is included in the N category, but only if there are no other positive nodes Reported as pn1c Otherwise, not part of N but are to be reported separately as a required element 8 th edition Defined as discreet tumor nodules within the lymph drainage are of the primary carcinoma without identifiable lymph node and without vascular or neural structure i.e. shape, contour and size are no longer considered If one can identify clearcut vascular or perineural invasion, they are not considered non-nodal tumor deposits but rather simply as vascular or perineural invasion (at least 40% (AJCP 2010; 133: ). 13
14 14
15 The history of N1c and non-nodal tumor deposits So why in the 7 th edition were non-nodal deposits moved to the N category Not sure, but if not included as N and there were no clear nodes involved, the case would be considered Stage II and may not receive adjuvant chemotherapy (and this really happens) So, cookbooks may be bad for your health, and this is an attempt to cook the cookbook As a practical matter, however, with the new definition of tumor deposit, many of these cases will be reverting to N0 with LVI and will be considered Stage II. Isolated tumor cells in lymph nodes in colon carcinoma Surprisingly to many, ITCs in colon are defined and treated like ITCs in breast carcinoma (< 0.2 mm) In the 5 th edition of AJCC, there was a general statement that ITCs were N0 regardless of the organ system In the 6 th and 7 th editions they were more organ specific but somewhat hidden In the 8 th edition, questions are arising in regard to colon but they are still considered pn0(i+) Why might ITCs in colon cancer be of more significance than ITCs in breast? In breast, sentinel nodes are very carefully examined with multiple levels, and if a met is <0.2 mm, that is probably the maximum size of the met In colon cancer, ITCs are being discovered in single sections of random nodes, and may well be only the tip of the iceberg if additional levels of the nodes were cut 15
16 8 th edition and ITCs Despite mounting evidence that they may have some prognostic significance, ITCs in the 8 th edition are still considered N0(i+) However, it might be worthwhile doing additional levels of nodes with ITCs if there are no truly positive nodes to avoid understaging Changes in the M-category A new category of M1c, peritoneal involvement, was added to reflect the known poor prognosis of these patients Given that peritoneal surface involvement (e.g. pt4a) is associated with the development of peritoneal carcinomatosis, this is a subtle admission (perhaps) that T4a might be prognostically worse than p4b Other changes and issues Grading of carcinoma Tumor budding 16
17 Grading of Adenocarcinoma NOS In the 6 th and 7 th editions a simplified grading system was recommended Low grade - > 50% glands High grade - < 50% glands In the 8 th edition, reversion to a 4 grade system is recommended (without a really good reason) GX cannot be assessed G1 well differentiated (>95% glands) G2 moderately differentiated (50 95% glands) G3 poorly differentiated ( < 50% glands) G4 undifferentiated (no glands, no mucin, no squamous or NE differentiation) Grading of colon carcinoma variants NOS Graded by gland percentage Always low grade Medullary carcinoma Always high grade Signet ring carcinoma Undifferentiated carcinoma (G4) Clear cell and sarcomatoid carcinoma What to do with mucinous carcinoma? Mucinous carcinoma grading Dependent on MSI status MSS are considered high grade MSI are considered low grade 17

18 Other histological subtypes with prognostic significance Micropapillary pattern >5% is associated with lymph node metastases Serrated adenocarcinoma may have worse prognosis But this is complicated by MSI status and presence or absence of mucinous carcinoma pattern Illustrate micropapillary and serrated patterns 18

19 19

20 Optional elements At the users discretion However, some elements that most authorities consider prognostically important are not included as required elements, most notably tumor budding A brief history of tumor budding and its significance Definition of a tumor bud A single cell or collection of less than 5 cells Usually seen at the leading edge of tumors, but also may be intratumoral Significance of tumor budding When present in significant amount (i.e. a high degree of tumor budding ) is associated with lymph node metastases and poorer prognosis In malignant polyps, tumor budding has similar significance and may affect management of polyps 20


21 What is the data for this association? Essentially every publication that has evaluated tumor budding, regardless of methodology, has found it to be significant, often more significant that other factors like lymphatic invasion or perineural invasion See Mitrovic et all (including Dr. Riddell) Mod Pathol 2012: 25: for one of many supportive editorials So, why is it not a required element 21
22 Why is not a required element? Not being a CAP/AJCC insider, I don t know However, the usual criticisms revolves around Lack of consensus on how to evaluate tumor budding and Lack of consensus on if it can be evaluated by H and E or needs cytokeratin staining Methods of evaluation Range from the Ueno hot spot method to complicated methods involving analysis of multiple fields May or may not recommend cytokeratin staining Ueno method Histopathology 2002; 40: Identify the area of tumor with the most evident tumor budding Count the number of buds per 20X high power field (technically per mm 2 ) Report the number of buds CAP recommends reporting as low (0 4), intermediate (5 9) or high (10 or more) CAP recommends reporting for all polyps and for Stage I and II cancers but does not require it 22
23 Cytokeratin or H and E alone There is no question that use of cytokeratin stain allows easier identification of tumor buds resulting in greater numbers of tumors with a high degree of tumor budding Studies using cytokeratin have found results similar to H and E However, only one study directly compared H and E and cytokeratin and in multivariate analysis only H and E identified buds had prognostic significance. In the end, given the extra expense and time of CK staining and the lack of proof that the results are more meaningful than H and E, I would not recommend using CK as a routine but may be useful if tumor buds are obscured by inflammation and the CAP also does not suggest using CK. Summary of changes in the 8 th edition Revision of grading of colon carcinoma 4 grades instead of 2 Definition of invasion High grade dysplasia is not included in Tis Into but not through muscularis mucosa is included as Tis Definition of T4a Tumor with perforation and tumor within inflammatory debris extending to surface is T4a Redefinition of non-nodal tumor deposits If vascular or perineural invasion present these are not considered non-nodal tumor deposits and are not included in pn1c New category of distant metastasis M1c, peritoneal carcinomatosis Web site for CAP protocol =/UCMCon/Contribution%20Folders/WebCont ent/pdf/cp-colon-17protocol-4001.pdf 23
Staging Challenges in Lower GI Cancers. Disclosure of Relevant Financial Relationships. AJCC 8 th edition and CAP protocol updates
 Staging Challenges in Lower GI Cancers Sanjay Kakar, MD University of California, San Francisco March 05, 2017 Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education
Staging Challenges in Lower GI Cancers Sanjay Kakar, MD University of California, San Francisco March 05, 2017 Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education
LOINC. Clinical information. RCPA code. Record if different to report header Operating surgeon name and contact details. Absent.
 Complete as narrative or use the structured format below 55752-0 17.02.28593 Clinical information 22027-7 17.02.30001 Record if different to report header Operating surgeon name and contact details 52101004
Complete as narrative or use the structured format below 55752-0 17.02.28593 Clinical information 22027-7 17.02.30001 Record if different to report header Operating surgeon name and contact details 52101004
Colorectal Cancer Structured Pathology Reporting Proforma DD MM YYYY
 Colorectal Cancer Structured Pathology Reporting Proforma Mandatory questions (i.e. protocol standards) are in bold (e.g. S1.03). Family name Given name(s) Date of birth DD MM YYYY S1.02 Clinical details
Colorectal Cancer Structured Pathology Reporting Proforma Mandatory questions (i.e. protocol standards) are in bold (e.g. S1.03). Family name Given name(s) Date of birth DD MM YYYY S1.02 Clinical details
Disclosures. Outline. What IS tumor budding?? Tumor Budding in Colorectal Carcinoma: What, Why, and How. I have nothing to disclose
 Tumor Budding in Colorectal Carcinoma: What, Why, and How Disclosures I have nothing to disclose Soo-Jin Cho, MD, PhD Assistant Professor UCSF Dept of Pathology Current Issues in Anatomic Pathology 2017
Tumor Budding in Colorectal Carcinoma: What, Why, and How Disclosures I have nothing to disclose Soo-Jin Cho, MD, PhD Assistant Professor UCSF Dept of Pathology Current Issues in Anatomic Pathology 2017
Colon and Rectum. Protocol revision date: January 2005 Based on AJCC/UICC TNM, 6th edition
 Colon and Rectum Protocol applies to all invasive carcinomas of the colon and rectum. Carcinoid tumors, lymphomas, sarcomas, and tumors of the vermiform appendix are excluded. Protocol revision date: January
Colon and Rectum Protocol applies to all invasive carcinomas of the colon and rectum. Carcinoid tumors, lymphomas, sarcomas, and tumors of the vermiform appendix are excluded. Protocol revision date: January
Small Intestine. Protocol revision date: January 2005 Based on AJCC/UICC TNM, 6 th edition
 Small Intestine Protocol applies to all invasive carcinomas of the small intestine, including those with focal endocrine differentiation. Excludes carcinoid tumors, lymphomas, and stromal tumors (sarcomas).
Small Intestine Protocol applies to all invasive carcinomas of the small intestine, including those with focal endocrine differentiation. Excludes carcinoid tumors, lymphomas, and stromal tumors (sarcomas).
Greater Manchester & Cheshire Guidelines for Pathology Reporting for Oesophageal and Gastric Malignancy
 Greater Manchester & Cheshire Guidelines for Pathology Reporting for Oesophageal and Gastric Malignancy Authors: Dr Gordon Armstrong, Dr Sue Pritchard 1. General Comments 1.1 Cancer reporting: Biopsies
Greater Manchester & Cheshire Guidelines for Pathology Reporting for Oesophageal and Gastric Malignancy Authors: Dr Gordon Armstrong, Dr Sue Pritchard 1. General Comments 1.1 Cancer reporting: Biopsies
Gastric Cancer Staging AJCC eighth edition. Duncan McLeod Westmead Hospital, NSW
 Gastric Cancer Staging AJCC eighth edition Duncan McLeod Westmead Hospital, NSW Summary of changes New clinical stage prognostic groups, ctnm Postneoadjuvant therapy pathologic stage groupings, yptnm -
Gastric Cancer Staging AJCC eighth edition Duncan McLeod Westmead Hospital, NSW Summary of changes New clinical stage prognostic groups, ctnm Postneoadjuvant therapy pathologic stage groupings, yptnm -
Nodal staging of colorectal cancer, TNM and practical issues
 Nodal staging of colorectal cancer, TNM and practical issues Gábor Cserni 1. Bács-Kiskun County Teaching Hospital, Kecskemét 2. University of Szeged, Szeged Different staging systems: A,B,C,(D) Same letters
Nodal staging of colorectal cancer, TNM and practical issues Gábor Cserni 1. Bács-Kiskun County Teaching Hospital, Kecskemét 2. University of Szeged, Szeged Different staging systems: A,B,C,(D) Same letters
A916: rectum: adenocarcinoma
 General facts of colorectal cancer The colon has cecum, ascending, transverse, descending and sigmoid colon sections. Cancer can start in any of the r sections or in the rectum. The wall of each of these
General facts of colorectal cancer The colon has cecum, ascending, transverse, descending and sigmoid colon sections. Cancer can start in any of the r sections or in the rectum. The wall of each of these
Early colorectal cancer Quality and rules for a good pathology report Histoprognostic factors
 Early colorectal cancer Quality and rules for a good pathology report Histoprognostic factors Frédéric Bibeau, MD, PhD Pathology department Biopathology unit Institut du Cancer de Montpellier France Quality
Early colorectal cancer Quality and rules for a good pathology report Histoprognostic factors Frédéric Bibeau, MD, PhD Pathology department Biopathology unit Institut du Cancer de Montpellier France Quality
Gastric Cancer Histopathology Reporting Proforma
 Gastric Cancer Histopathology Reporting Proforma Mandatory questions (i.e. protocol standards) are in bold (e.g. S1.01). S1.01 Identification Family name Given name(s) Date of birth Sex Male Female Intersex/indeterminate
Gastric Cancer Histopathology Reporting Proforma Mandatory questions (i.e. protocol standards) are in bold (e.g. S1.01). S1.01 Identification Family name Given name(s) Date of birth Sex Male Female Intersex/indeterminate
malignant polyp Daily Challenges in Digestive Endoscopy for Endoscopists and Endoscopy Nurses BSGIE Annual Meeting 18/09/2014 Mechelen
 Plan Incidental finding of a malignant polyp 1. What is a polyp malignant? 2. Role of the pathologist and the endoscopist 3. Quantitative and qualitative risk assessment 4. How to decide what to do? Hubert
Plan Incidental finding of a malignant polyp 1. What is a polyp malignant? 2. Role of the pathologist and the endoscopist 3. Quantitative and qualitative risk assessment 4. How to decide what to do? Hubert
AJCC Cancer Staging 8 th Edition
 AJCC Cancer Staging 8 th Edition Colon and Rectal Cancer Staging Update Webinar George J Chang, MD, MS Deputy Chair, Department of Surgical Oncology Chief, Colon and Rectal Surgery Professor of Surgical
AJCC Cancer Staging 8 th Edition Colon and Rectal Cancer Staging Update Webinar George J Chang, MD, MS Deputy Chair, Department of Surgical Oncology Chief, Colon and Rectal Surgery Professor of Surgical
11/21/13 CEA: 1.7 WNL
 Case Scenario 1 A 70 year-old white male presented to his primary care physician with a recent history of rectal bleeding. He was referred for imaging and a colonoscopy and was found to have adenocarcinoma.
Case Scenario 1 A 70 year-old white male presented to his primary care physician with a recent history of rectal bleeding. He was referred for imaging and a colonoscopy and was found to have adenocarcinoma.
Greater Manchester & Cheshire Guidelines for Pathology Reporting of Oesophageal and Gastric Malignancy
 Greater Manchester & Cheshire Guidelines for Pathology Reporting of Oesophageal and Gastric Malignancy Authors: Dr Stephen Hayes, Dr David Bisset, Dr Gordon Armstrong, Dr Sue Pritchard 1. General Comments
Greater Manchester & Cheshire Guidelines for Pathology Reporting of Oesophageal and Gastric Malignancy Authors: Dr Stephen Hayes, Dr David Bisset, Dr Gordon Armstrong, Dr Sue Pritchard 1. General Comments
SEER EOD AND SUMMARY STAGE ABSTRACTORS TRAINING
 SEER EOD AND SUMMARY STAGE ABSTRACTORS TRAINING OVERVIEW What is SEER EOD Ambiguous Terminology General Guidelines EOD Primary Tumor EOD Regional Nodes EOD Mets Site Specific Data Items (SSDI) SEER Summary
SEER EOD AND SUMMARY STAGE ABSTRACTORS TRAINING OVERVIEW What is SEER EOD Ambiguous Terminology General Guidelines EOD Primary Tumor EOD Regional Nodes EOD Mets Site Specific Data Items (SSDI) SEER Summary
Diagnostic Difficulties Encountered Among Colorectal Polyps
 Diagnostic Difficulties Encountered Among Colorectal Polyps Rhonda K. Yantiss, M.D. Professor of Pathology and Laboratory Medicine Department of Pathology and Laboratory Medicine Weill Cornell Medical
Diagnostic Difficulties Encountered Among Colorectal Polyps Rhonda K. Yantiss, M.D. Professor of Pathology and Laboratory Medicine Department of Pathology and Laboratory Medicine Weill Cornell Medical
6/5/2010. Renal vein invasion & Capsule Penetration (T3a) Adrenal Gland involvement (T4 vs. M1) Beyond Gerota s Fascia? (?T4).
 Adrenal Gland involvement (T4 vs. M1) Beyond Gerota s Fascia? (?T4).") GU Cancer Staging: Updates and Challenging Areas 13 th Current Issues in Surgical Pathology San Francisco, CA June 5, 2010 Jeffry P. Simko, PhD, MD Associate Professor Departments of Urology and Anatomic
GU Cancer Staging: Updates and Challenging Areas 13 th Current Issues in Surgical Pathology San Francisco, CA June 5, 2010 Jeffry P. Simko, PhD, MD Associate Professor Departments of Urology and Anatomic
Definition of Synoptic Reporting
 Definition of Synoptic Reporting The CAP has developed this list of specific features that define synoptic reporting formatting: 1. All required cancer data from an applicable cancer protocol that are
Definition of Synoptic Reporting The CAP has developed this list of specific features that define synoptic reporting formatting: 1. All required cancer data from an applicable cancer protocol that are
LUNG STAGING FORM LATERALITY: LEFT RIGHT BILATERAL
 LUNG STAGING FORM LATERALITY: LEFT RIGHT BILATERAL ( ) Tx Primary tumor cannot be assessed, or tumor proven by the presence of malignant cells in sputum or bronchial washings but not visualized by imaging
LUNG STAGING FORM LATERALITY: LEFT RIGHT BILATERAL ( ) Tx Primary tumor cannot be assessed, or tumor proven by the presence of malignant cells in sputum or bronchial washings but not visualized by imaging
Staging for Residents, Nurses, and Multidisciplinary Health Care Team
 Staging for Residents, Nurses, and Multidisciplinary Health Care Team Donna M. Gress, RHIT, CTR Validating science. Improving patient care. Learning Objectives Introduce the concept and history of stage
Staging for Residents, Nurses, and Multidisciplinary Health Care Team Donna M. Gress, RHIT, CTR Validating science. Improving patient care. Learning Objectives Introduce the concept and history of stage
Rectal Cancer Cookbook Update. A. JOURET-MOURIN with the collaboration of A Hoorens,P Demetter, G De Hertogh,C Cuvelier and C Sempoux
 Rectal Cancer Cookbook Update A. JOURET-MOURIN with the collaboration of A Hoorens,P Demetter, G De Hertogh,C Cuvelier and C Sempoux Prof Dr A Jouret-Mourin, Department of Pathology, UCL, St Luc, Brussels
Rectal Cancer Cookbook Update A. JOURET-MOURIN with the collaboration of A Hoorens,P Demetter, G De Hertogh,C Cuvelier and C Sempoux Prof Dr A Jouret-Mourin, Department of Pathology, UCL, St Luc, Brussels
Tumours of the Oesophagus & Gastro-Oesophageal Junction Histopathology Reporting Proforma
 Tumours of the Oesophagus & Gastro-Oesophageal Junction Histopathology Reporting Proforma Mandatory questions (i.e. protocol standards) are in bold (e.g. S1.01). S1.01 Identification Family name Given
Tumours of the Oesophagus & Gastro-Oesophageal Junction Histopathology Reporting Proforma Mandatory questions (i.e. protocol standards) are in bold (e.g. S1.01). S1.01 Identification Family name Given
STAGE CATEGORY DEFINITIONS
 CLINICAL Extent of disease before any treatment y clinical staging completed after neoadjuvant therapy but before subsequent surgery TX Tis Tis (DCIS) Tis (LCIS) Tis (Paget s) T1 T1mi T1a T1b T1c a b c
CLINICAL Extent of disease before any treatment y clinical staging completed after neoadjuvant therapy but before subsequent surgery TX Tis Tis (DCIS) Tis (LCIS) Tis (Paget s) T1 T1mi T1a T1b T1c a b c
Joseph Misdraji, M.D. GI pathology Unit Massachusetts General Hospital
 Joseph Misdraji, M.D. GI pathology Unit Massachusetts General Hospital jmisdraji@partners.org Low-grade appendiceal mucinous neoplasm (LAMN) High-grade appendiceal mucinous neoplasm (HAMN) Adenocarcinoma
Joseph Misdraji, M.D. GI pathology Unit Massachusetts General Hospital jmisdraji@partners.org Low-grade appendiceal mucinous neoplasm (LAMN) High-grade appendiceal mucinous neoplasm (HAMN) Adenocarcinoma
ACRIN 6666 Therapeutic Surgery Form
 S1 ACRIN 6666 Therapeutic Surgery Form 6666 Instructions: Complete a separate S1 form for each separate area of each breast excised with the intent to treat a cancer (e.g. each lumpectomy or mastectomy).
S1 ACRIN 6666 Therapeutic Surgery Form 6666 Instructions: Complete a separate S1 form for each separate area of each breast excised with the intent to treat a cancer (e.g. each lumpectomy or mastectomy).
Carcinoma of the Renal Pelvis and Ureter Histopathology
 Carcinoma of the Renal Pelvis and Ureter Histopathology Reporting Proforma (NEPHROURETERECTOMY AND URETERECTOMY) Includes the International Collaboration on Cancer reporting dataset denoted by * Family
Carcinoma of the Renal Pelvis and Ureter Histopathology Reporting Proforma (NEPHROURETERECTOMY AND URETERECTOMY) Includes the International Collaboration on Cancer reporting dataset denoted by * Family
Imaging in gastric cancer
 Imaging in gastric cancer Gastric cancer remains a deadly disease because of late diagnosis. Adenocarcinoma represents 90% of malignant tumors. Diagnosis is based on endoscopic examination with biopsies.
Imaging in gastric cancer Gastric cancer remains a deadly disease because of late diagnosis. Adenocarcinoma represents 90% of malignant tumors. Diagnosis is based on endoscopic examination with biopsies.
NUMERATOR: Reports that include the pt category, the pn category and the histologic grade
 Quality ID #100 (NQF 0392): Colorectal Cancer Resection Pathology Reporting: pt Category (Primary Tumor) and pn Category (Regional Lymph Nodes) with Histologic Grade National Quality Strategy Domain: Effective
Quality ID #100 (NQF 0392): Colorectal Cancer Resection Pathology Reporting: pt Category (Primary Tumor) and pn Category (Regional Lymph Nodes) with Histologic Grade National Quality Strategy Domain: Effective
A215- Urinary bladder cancer tissues
 A215- Urinary bladder cancer tissues (formalin fixed) For research use only Specifications: No. of cases: 45 Tissue type: Urinary bladder cancer tissues No. of spots: 2 spots from each cancer case (90
A215- Urinary bladder cancer tissues (formalin fixed) For research use only Specifications: No. of cases: 45 Tissue type: Urinary bladder cancer tissues No. of spots: 2 spots from each cancer case (90
NUMERATOR: Reports that include the pt category, the pn category and the histologic grade
 Quality ID #100 (NQF 0392): Colorectal Cancer Resection Pathology Reporting: pt Category (Primary Tumor) and pn Category (Regional Lymph Nodes) with Histologic Grade National Quality Strategy Domain: Effective
Quality ID #100 (NQF 0392): Colorectal Cancer Resection Pathology Reporting: pt Category (Primary Tumor) and pn Category (Regional Lymph Nodes) with Histologic Grade National Quality Strategy Domain: Effective
Interactive Staging Bee
 Interactive Staging Bee ROBIN BILLET, MA, CTR GA/SC REGIONAL CONFERENCE NOVEMBER 6, 2018? Clinical Staging includes any information obtained about the extent of cancer obtained before initiation of treatment
Interactive Staging Bee ROBIN BILLET, MA, CTR GA/SC REGIONAL CONFERENCE NOVEMBER 6, 2018? Clinical Staging includes any information obtained about the extent of cancer obtained before initiation of treatment
Protocol applies to melanoma of cutaneous surfaces only.
 Melanoma of the Skin Protocol applies to melanoma of cutaneous surfaces only. Procedures Biopsy (No Accompanying Checklist) Excision Re-excision Protocol revision date: January 2005 Based on AJCC/UICC
Melanoma of the Skin Protocol applies to melanoma of cutaneous surfaces only. Procedures Biopsy (No Accompanying Checklist) Excision Re-excision Protocol revision date: January 2005 Based on AJCC/UICC
8. The polyp in the illustration can be described as (circle all that apply) a. Exophytic b. Pedunculated c. Sessile d. Frank
 a. Exophytic b. Pedunculated c. Sessile d. Frank") Quiz 1 Overview 1. Beginning with the cecum, which is the correct sequence of colon subsites? a. Cecum, ascending, splenic flexure, transverse, hepatic flexure, descending, sigmoid. b. Cecum, ascending,
Quiz 1 Overview 1. Beginning with the cecum, which is the correct sequence of colon subsites? a. Cecum, ascending, splenic flexure, transverse, hepatic flexure, descending, sigmoid. b. Cecum, ascending,
WHAT SHOULD WE DO WITH TUMOUR BUDDING IN EARLY COLORECTAL CANCER?
 CANCER STAGING TNM and prognosis in CRC WHAT SHOULD WE DO WITH TUMOUR BUDDING IN EARLY COLORECTAL CANCER? Alessandro Lugli, MD Institute of Pathology University of Bern Switzerland Maastricht, June 19
CANCER STAGING TNM and prognosis in CRC WHAT SHOULD WE DO WITH TUMOUR BUDDING IN EARLY COLORECTAL CANCER? Alessandro Lugli, MD Institute of Pathology University of Bern Switzerland Maastricht, June 19
S1.04 Principal clinician. G1.01 Comments. G2.01 *Specimen dimensions (prostate) S2.02 *Seminal vesicles
 S2.02 *Seminal vesicles") Prostate Cancer Histopathology Reporting Proforma (Radical Prostatectomy) Includes the International Collaboration on Cancer reporting dataset denoted by * Family name Given name(s) Date of birth Sex Male
Prostate Cancer Histopathology Reporting Proforma (Radical Prostatectomy) Includes the International Collaboration on Cancer reporting dataset denoted by * Family name Given name(s) Date of birth Sex Male
The pathology of bladder cancer
 1 The pathology of bladder cancer Charles Jameson Introduction Carcinoma of the bladder is the seventh most common cancer worldwide [1]. It comprises 3.2% of all cancers, with an estimated 260 000 new
1 The pathology of bladder cancer Charles Jameson Introduction Carcinoma of the bladder is the seventh most common cancer worldwide [1]. It comprises 3.2% of all cancers, with an estimated 260 000 new
Collaborative Stage for TNM 7 - Revised 06/30/2008 [ Schema ]
![Collaborative Stage for TNM 7 - Revised 06/30/2008 [ Schema ]](/thumbs/82/86264030.jpg "Collaborative Stage for TNM 7 - Revised 06/30/2008 [ Schema ]") Collaborative Stage for TNM 7 - Revised 06/30/2008 [ Schema ] CS Tumor Size 000 No mass/tumor found 001-988 001-988 millimeters (code exact size in millimeters) 989 989 millimeters or larger 990 Microscopic
Collaborative Stage for TNM 7 - Revised 06/30/2008 [ Schema ] CS Tumor Size 000 No mass/tumor found 001-988 001-988 millimeters (code exact size in millimeters) 989 989 millimeters or larger 990 Microscopic
Urinary Bladder: WHO Classification and AJCC Staging Update 2017
 Urinary Bladder: WHO Classification and AJCC Staging Update 2017 Houston Society of Clinical Pathologists 58 th Annual Spring Symposium Houston, TX April 8, 2017 Jesse K. McKenney, MD Classification
Urinary Bladder: WHO Classification and AJCC Staging Update 2017 Houston Society of Clinical Pathologists 58 th Annual Spring Symposium Houston, TX April 8, 2017 Jesse K. McKenney, MD Classification
This form may provide more data elements than required for collection by standard setters such as NCI SEER, CDC NPCR, and CoC NCDB.
 1 Terms of Use The cancer staging form is a specific document in the patient record; it is not a substitute for documentation of history, physical examination, and staging evaluation, or for documenting
1 Terms of Use The cancer staging form is a specific document in the patient record; it is not a substitute for documentation of history, physical examination, and staging evaluation, or for documenting
Expert panel observations
 Expert panel observations Professor Neil A Shepherd Gloucester and Cheltenham, UK Gloucestershire Cellular Pathology Laboratory Three big issues in BCSP pathology serrated pathology & what do we do about
Expert panel observations Professor Neil A Shepherd Gloucester and Cheltenham, UK Gloucestershire Cellular Pathology Laboratory Three big issues in BCSP pathology serrated pathology & what do we do about
Chapter 2 Staging of Breast Cancer
 Chapter 2 Staging of Breast Cancer Zeynep Ozsaran and Senem Demirci Alanyalı 2.1 Introduction Five decades ago, Denoix et al. proposed classification system (tumor node metastasis [TNM]) based on the dissemination
Chapter 2 Staging of Breast Cancer Zeynep Ozsaran and Senem Demirci Alanyalı 2.1 Introduction Five decades ago, Denoix et al. proposed classification system (tumor node metastasis [TNM]) based on the dissemination
3/23/2017. Disclosure of Relevant Financial Relationships. Pathologic Staging Updates in Breast Cancer. Pathologic Staging Updates Breast Cancer
 Pathologic Staging Updates in Breast Cancer Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position to influence or control the content of CME
Pathologic Staging Updates in Breast Cancer Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position to influence or control the content of CME
Carcinoma of the Urinary Bladder Histopathology
 Carcinoma of the Urinary Bladder Histopathology Reporting Proforma (Radical & Partial Cystectomy, Cystoprostatectomy) Includes the International Collaboration on Cancer reporting dataset denoted by * Family
Carcinoma of the Urinary Bladder Histopathology Reporting Proforma (Radical & Partial Cystectomy, Cystoprostatectomy) Includes the International Collaboration on Cancer reporting dataset denoted by * Family
Colon and Rectum. Protocol revision date: January 2005 Based on AJCC/UICC TNM, 6th edition
 Colon and Rectum Protocol applies to all invasive carcinomas of the colon and rectum. Carcinoid tumors, lymphomas, sarcomas, and tumors of the vermiform appendix are excluded. Protocol revision date: January
Colon and Rectum Protocol applies to all invasive carcinomas of the colon and rectum. Carcinoid tumors, lymphomas, sarcomas, and tumors of the vermiform appendix are excluded. Protocol revision date: January
Pancreas (Exocrine) Protocol applies to all carcinomas of the exocrine pancreas.
 Protocol applies to all carcinomas of the exocrine pancreas.") Pancreas (Exocrine) Protocol applies to all carcinomas of the exocrine pancreas. Protocol revision date: January 2005 Based on AJCC/UICC TNM, 6 th edition Procedures Cytology (No Accompanying Checklist)
Pancreas (Exocrine) Protocol applies to all carcinomas of the exocrine pancreas. Protocol revision date: January 2005 Based on AJCC/UICC TNM, 6 th edition Procedures Cytology (No Accompanying Checklist)
Urinary Bladder, Ureter, and Renal Pelvis
 Urinary Bladder, Ureter, and Renal Pelvis Protocol applies to all carcinomas of the urinary bladder, ureter, and renal pelvis. Protocol revision date: January 2005 Based on AJCC/UICC TNM, 6th edition Procedures
Urinary Bladder, Ureter, and Renal Pelvis Protocol applies to all carcinomas of the urinary bladder, ureter, and renal pelvis. Protocol revision date: January 2005 Based on AJCC/UICC TNM, 6th edition Procedures
Overview. Collecting Cancer Data: Colon 11/5/2009. Collecting Cancer Data: NAACCR Webinar Series 1. Agenda NAACCR WEBINAR SERIES
 Collecting Cancer Data: Colon 11/5/2009 Collecting Cancer Data: Colon/Rectum/Appendix NAACCR 2009 2010 WEBINAR SERIES Agenda Overview Treatment MP/H Rules CSv2 2 Overview Colon/Rectum/Appendix 2009 2010
Collecting Cancer Data: Colon 11/5/2009 Collecting Cancer Data: Colon/Rectum/Appendix NAACCR 2009 2010 WEBINAR SERIES Agenda Overview Treatment MP/H Rules CSv2 2 Overview Colon/Rectum/Appendix 2009 2010
BLADDER CANCER EPIDEMIOLOGY
 BLADDER CANCER WHAT IS NEW AND CLINICALLY RELEVANT Canadian Geese - Geist Reservoir (my backyard), Indianapolis, USA BLADDER CANCER EPIDEMIOLOGY Urinary bladder 17,960 2% Urinary bladder 4,390 1.6% Siegel
BLADDER CANCER WHAT IS NEW AND CLINICALLY RELEVANT Canadian Geese - Geist Reservoir (my backyard), Indianapolis, USA BLADDER CANCER EPIDEMIOLOGY Urinary bladder 17,960 2% Urinary bladder 4,390 1.6% Siegel
COLLECTING CANCER DATA: STOMACH AND ESOPHAGUS
 COLLECTING CANCER DATA: STOMACH AND ESOPHAGUS 2017 2018 NAACCR WEBINAR SERIES Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching
COLLECTING CANCER DATA: STOMACH AND ESOPHAGUS 2017 2018 NAACCR WEBINAR SERIES Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching
Question: If in a particular case, there is doubt about the correct T, N or M category, what do you do?
 Exercise 1 Question: If in a particular case, there is doubt about the correct T, N or M category, what do you do? : 1. I mention both categories that are in consideration, e.g. pt1-2 2. I classify as
Exercise 1 Question: If in a particular case, there is doubt about the correct T, N or M category, what do you do? : 1. I mention both categories that are in consideration, e.g. pt1-2 2. I classify as
Peritoneal Involvement in Stage II Colon Cancer
 Anatomic Pathology / PERITONEAL INVOLVEMENT IN STAGE II COLON CANCER Peritoneal Involvement in Stage II Colon Cancer A.M. Lennon, MB, MRCPI, H.E. Mulcahy, MD, MRCPI, J.M.P. Hyland, MCh, FRCS, FRCSI, C.
Anatomic Pathology / PERITONEAL INVOLVEMENT IN STAGE II COLON CANCER Peritoneal Involvement in Stage II Colon Cancer A.M. Lennon, MB, MRCPI, H.E. Mulcahy, MD, MRCPI, J.M.P. Hyland, MCh, FRCS, FRCSI, C.
2014/2015 FCDS Educational Webcast Series
 2014/2015 FCDS Educational Webcast Series February 19, 2015 Steven Peace, CTR 2015 Update; Background, Anatomy, Risk Factors, Screening Guidelines, MPH Rules Review AJCC TNM 7 th ed, SS2000, CSv02.05 and
2014/2015 FCDS Educational Webcast Series February 19, 2015 Steven Peace, CTR 2015 Update; Background, Anatomy, Risk Factors, Screening Guidelines, MPH Rules Review AJCC TNM 7 th ed, SS2000, CSv02.05 and
Ritu Nayar, MD Professor and Vice Chair of Pathology Northwestern University, Feinberg School of Medicine Chicago, IL
 Ritu Nayar, MD Professor and Vice Chair of Pathology Northwestern University, Feinberg School of Medicine Chicago, IL email: r-nayar@northwestern.edu Nothing to disclose College of American Pathologists
Ritu Nayar, MD Professor and Vice Chair of Pathology Northwestern University, Feinberg School of Medicine Chicago, IL email: r-nayar@northwestern.edu Nothing to disclose College of American Pathologists
Colon and Rectum: 2018 Solid Tumor Rules
 2018 SEER Solid Tumor Manual 2018 KCR SPRING TRAINING Colon and Rectum: 2018 Solid Tumor Rules 1 Colon and Rectum Solid Tumor Rules Separate sections for: Introduction Changes from 2007 MP/H rules Equivalent
2018 SEER Solid Tumor Manual 2018 KCR SPRING TRAINING Colon and Rectum: 2018 Solid Tumor Rules 1 Colon and Rectum Solid Tumor Rules Separate sections for: Introduction Changes from 2007 MP/H rules Equivalent
Seventh Edition Staging 2017 Colorectum. Overview. This webinar is sponsored by. the Centers for Disease Control and Prevention.
 Seventh Edition Staging 2017 Colorectum Donna M. Gress, RHIT, CTR Validating science. Improving patient care. No materials in this presentation may be repurposed in print or online without the express
Seventh Edition Staging 2017 Colorectum Donna M. Gress, RHIT, CTR Validating science. Improving patient care. No materials in this presentation may be repurposed in print or online without the express
Completing the Puzzle AJCC TNM Staging Breast. Nicole Catlett, CTR 2017 Kentucky Cancer Registry Fall Conference, September 21 & 22, 2017
 Completing the Puzzle AJCC TNM Staging Breast Nicole Catlett, CTR 2017 Kentucky Cancer Registry Fall Conference, September 21 & 22, 2017 OBJECTIVES Understanding of Breast TNM staging Identify clinical
Completing the Puzzle AJCC TNM Staging Breast Nicole Catlett, CTR 2017 Kentucky Cancer Registry Fall Conference, September 21 & 22, 2017 OBJECTIVES Understanding of Breast TNM staging Identify clinical
Prostate cancer staging and datasets: The Nitty-Gritty. What determines our pathological reports? 06/07/2018. Dan Berney Maastricht 2018
 Prostate cancer staging and datasets: The Nitty-Gritty What determines our pathological reports? Dan Berney Maastricht 2018 Biopsy reporting. How not to do it. The TNM 8 th edition. Changes good and bad
Prostate cancer staging and datasets: The Nitty-Gritty What determines our pathological reports? Dan Berney Maastricht 2018 Biopsy reporting. How not to do it. The TNM 8 th edition. Changes good and bad
COLON AND RECTUM SOLID TUMOR RULES ABSTRACTORS TRAINING
 COLON AND RECTUM SOLID TUMOR RULES ABSTRACTORS TRAINING COLON AND RECTUM SOLID TUMOR RULES Separate sections for: Introduction Changes from 2007 MP/H rules Equivalent Terms Terms that are NOT Equivalent
COLON AND RECTUM SOLID TUMOR RULES ABSTRACTORS TRAINING COLON AND RECTUM SOLID TUMOR RULES Separate sections for: Introduction Changes from 2007 MP/H rules Equivalent Terms Terms that are NOT Equivalent
Case Scenario 1 Worksheet. Primary Site C44.4 Morphology 8743/3 Laterality 0 Stage/ Prognostic Factors
 CASE SCENARIO 1 9/10/13 HISTORY: Patient is a 67-year-old white male and presents with lesion located 4-5cm above his right ear. The lesion has been present for years. No lymphadenopathy. 9/10/13 anterior
CASE SCENARIO 1 9/10/13 HISTORY: Patient is a 67-year-old white male and presents with lesion located 4-5cm above his right ear. The lesion has been present for years. No lymphadenopathy. 9/10/13 anterior
Alison Douglass Gillian Lieberman, MD. November. Colon Cancer. Alison Douglass, Harvard Medical School Year III Gillian Lieberman, MD
 November Colon Cancer Alison Douglass, Harvard Medical School Year III Our Patient Mr. K. is a 67 year old man with no prior medical problems other than hemorrhoids which have caused occasional rectal
November Colon Cancer Alison Douglass, Harvard Medical School Year III Our Patient Mr. K. is a 67 year old man with no prior medical problems other than hemorrhoids which have caused occasional rectal
Uterine Cervix. Protocol applies to all invasive carcinomas of the cervix.
 Uterine Cervix Protocol applies to all invasive carcinomas of the cervix. Protocol revision date: January 2005 Based on AJCC/UICC TNM, 6 th edition and FIGO 2001 Annual Report Procedures Cytology (No Accompanying
Uterine Cervix Protocol applies to all invasive carcinomas of the cervix. Protocol revision date: January 2005 Based on AJCC/UICC TNM, 6 th edition and FIGO 2001 Annual Report Procedures Cytology (No Accompanying
Oesophagus and Stomach update dysplasia and early cancer
 Oesophagus and Stomach update dysplasia and early cancer Dr Tim Bracey STR teaching 13/4/16 Please check pathkids.com for previous talks One of the biggest units in the country (100 major resections per
Oesophagus and Stomach update dysplasia and early cancer Dr Tim Bracey STR teaching 13/4/16 Please check pathkids.com for previous talks One of the biggest units in the country (100 major resections per
Descriptor Definition Author s notes TNM descriptors Required only if applicable; select all that apply multiple foci of invasive carcinoma
 S5.01 The tumour stage and stage grouping must be recorded to the extent possible, based on the AJCC Cancer Staging Manual (7 th Edition). 11 (See Tables S5.01a and S5.01b below.) Table S5.01a AJCC breast
S5.01 The tumour stage and stage grouping must be recorded to the extent possible, based on the AJCC Cancer Staging Manual (7 th Edition). 11 (See Tables S5.01a and S5.01b below.) Table S5.01a AJCC breast
Thyroid Gland. Protocol applies to all malignant tumors of the thyroid gland, except lymphomas.
 Thyroid Gland Protocol applies to all malignant tumors of the thyroid gland, except lymphomas. Procedures Cytology (No Accompanying Checklist) Partial Thyroidectomy Total Thyroidectomy With/Without Lymph
Thyroid Gland Protocol applies to all malignant tumors of the thyroid gland, except lymphomas. Procedures Cytology (No Accompanying Checklist) Partial Thyroidectomy Total Thyroidectomy With/Without Lymph
VULVAR CARCINOMA. Page 1 of 5
 VULVAR CARCINOMA EXAMPLE OF A VULVAR CARCINOMA USING PROPOSED TEMPLATE Case: Invasive squamous cell carcinoma arising in D-VIN Tumor in left labia major Left partial vaginectomy and sentinel lymph node
VULVAR CARCINOMA EXAMPLE OF A VULVAR CARCINOMA USING PROPOSED TEMPLATE Case: Invasive squamous cell carcinoma arising in D-VIN Tumor in left labia major Left partial vaginectomy and sentinel lymph node
Procedures Needle Biopsy Transurethral Prostatic Resection Suprapubic or Retropubic Enucleation (Subtotal Prostatectomy) Radical Prostatectomy
 Radical Prostatectomy") Prostate Gland Protocol applies to invasive carcinomas of the prostate gland. Protocol web posting date: July 2006 Protocol effective date: April 2007 Based on AJCC/UICC TNM, 6 th edition Procedures Needle
Prostate Gland Protocol applies to invasive carcinomas of the prostate gland. Protocol web posting date: July 2006 Protocol effective date: April 2007 Based on AJCC/UICC TNM, 6 th edition Procedures Needle
Protocol for the Examination of Specimens From Patients With Primary Carcinoma of the Colon and Rectum
 Protocol for the Examination of Specimens From Patients With Primary Carcinoma of the Colon and Rectum Well-differentiated neuroendocrine neoplasms (carcinoid tumors) are not included. Based on AJCC/UICC
Protocol for the Examination of Specimens From Patients With Primary Carcinoma of the Colon and Rectum Well-differentiated neuroendocrine neoplasms (carcinoid tumors) are not included. Based on AJCC/UICC
Protocol for the Examination of Specimens From Patients With Carcinoma of the Stomach
 Protocol for the Examination of Specimens From Patients With Carcinoma of the Stomach Version: Protocol Posting Date: June 2017 Includes ptnm requirements from the 8 th Edition, AJCC Staging Manual For
Protocol for the Examination of Specimens From Patients With Carcinoma of the Stomach Version: Protocol Posting Date: June 2017 Includes ptnm requirements from the 8 th Edition, AJCC Staging Manual For
High risk stage II colon cancer
 High risk stage II colon cancer Joel Gingerich, MD, FRCPC Assistant Professor Medical Oncologist University of Manitoba CancerCare Manitoba Disclaimer No conflict of interests 16 October 2010 Overview
High risk stage II colon cancer Joel Gingerich, MD, FRCPC Assistant Professor Medical Oncologist University of Manitoba CancerCare Manitoba Disclaimer No conflict of interests 16 October 2010 Overview
4/10/2018. SEER EOD and Summary Stage. Overview KCR 2018 SPRING TRAINING. What is SEER EOD? Ambiguous Terminology General Guidelines
 SEER EOD and Summary Stage KCR 2018 SPRING TRAINING Overview What is SEER EOD Ambiguous Terminology General Guidelines EOD Primary Tumor EOD Regional Nodes EOD Mets SEER Summary Stage 2018 Site Specific
SEER EOD and Summary Stage KCR 2018 SPRING TRAINING Overview What is SEER EOD Ambiguous Terminology General Guidelines EOD Primary Tumor EOD Regional Nodes EOD Mets SEER Summary Stage 2018 Site Specific
S1.04 PRINCIPAL CLINICIAN G1.01 COMMENTS S2.01 SPECIMEN LABELLED AS G2.01 *SPECIMEN DIMENSIONS (PROSTATE) S2.03 *SEMINAL VESICLES
 S2.03 *SEMINAL VESICLES") Prostate Cancer Histopathology Reporting Proforma (Radical Prostatectomy) Includes the International Collaboration on Cancer reporting dataset denoted by * Family name Given name(s) Date of birth Indigenous
Prostate Cancer Histopathology Reporting Proforma (Radical Prostatectomy) Includes the International Collaboration on Cancer reporting dataset denoted by * Family name Given name(s) Date of birth Indigenous
What Pathology can tell us in the approach of localized colorectal cancer
 What Pathology can tell us in the approach of localized colorectal cancer A/Prof Tony Lim Kiat Hon Department of Anatomical Pathology Singapore General Hospital ESMO 2017 Singapore Nov 1 2 Do we still
What Pathology can tell us in the approach of localized colorectal cancer A/Prof Tony Lim Kiat Hon Department of Anatomical Pathology Singapore General Hospital ESMO 2017 Singapore Nov 1 2 Do we still
Papillary Lesions of the Breast: WHO Update
 Papillary Lesions of the Breast: WHO Update Stuart J. Schnitt, M.D. Department of Pathology Beth Israel Deaconess Medical Center and Harvard Medical School Boston, MA, USA Papillary Lesions of the Breast
Papillary Lesions of the Breast: WHO Update Stuart J. Schnitt, M.D. Department of Pathology Beth Israel Deaconess Medical Center and Harvard Medical School Boston, MA, USA Papillary Lesions of the Breast
SEER Summary Stage Still Here!
 SEER Summary Stage Still Here! CCRA NORTHERN REGION STAGING SYMPOSIUM SEPTEMBER 20, 2017 SEER Summary Stage Timeframe: includes all information available through completion of surgery(ies) in the first
SEER Summary Stage Still Here! CCRA NORTHERN REGION STAGING SYMPOSIUM SEPTEMBER 20, 2017 SEER Summary Stage Timeframe: includes all information available through completion of surgery(ies) in the first
Small Intestine. Protocol revision date: January 2005 Based on AJCC/UICC TNM, 6 th edition
 Small Intestine Protocol applies to all invasive carcinomas of the small intestine, including those with focal endocrine differentiation. Excludes carcinoid tumors, lymphomas, and stromal tumors (sarcomas).
Small Intestine Protocol applies to all invasive carcinomas of the small intestine, including those with focal endocrine differentiation. Excludes carcinoid tumors, lymphomas, and stromal tumors (sarcomas).
Neoplasms of the Colon and of the Rectum
 Neoplasms of the Colon and of the Rectum 2 0 1 5-2 0 1 6 F C D S E D U C A T I O N A L W E B C A S T S E R I E S S T E V E N P E A C E, B S, C T R F E B R U A R Y 1 8, 2 0 1 6 2016 Focus o Anatomy o SS
Neoplasms of the Colon and of the Rectum 2 0 1 5-2 0 1 6 F C D S E D U C A T I O N A L W E B C A S T S E R I E S S T E V E N P E A C E, B S, C T R F E B R U A R Y 1 8, 2 0 1 6 2016 Focus o Anatomy o SS
3/23/2017. Disclaimer. Common Changes in TNM Staging. Overview. Overview. Understanding Terminology. Overview
 Common Changes in TNM Staging Understanding the General Rules of Cancer Staging Thomas P. Baker, MD FCAP March 5, 2017 Disclaimer The identification of specific products or scientific instrumentation is
Common Changes in TNM Staging Understanding the General Rules of Cancer Staging Thomas P. Baker, MD FCAP March 5, 2017 Disclaimer The identification of specific products or scientific instrumentation is
This form may provide more data elements than required for collection by standard setters such as NCI SEER, CDC NPCR, and CoC NCDB.
 1 Terms of Use The cancer staging form is a specific document in the patient record; it is not a substitute for documentation of history, physical examination, and staging evaluation, or for documenting
1 Terms of Use The cancer staging form is a specific document in the patient record; it is not a substitute for documentation of history, physical examination, and staging evaluation, or for documenting
Exercise 15: CSv2 Data Item Coding Instructions ANSWERS
 Exercise 15: CSv2 Data Item Coding Instructions ANSWERS CS Tumor Size Tumor size is the diameter of the tumor, not the depth or thickness of the tumor. Chest x-ray shows 3.5 cm mass; the pathology report
Exercise 15: CSv2 Data Item Coding Instructions ANSWERS CS Tumor Size Tumor size is the diameter of the tumor, not the depth or thickness of the tumor. Chest x-ray shows 3.5 cm mass; the pathology report
Protocol for the Examination of Specimens from Patients with Primary Carcinomas of the Colon and Rectum
 Protocol for the Examination of Specimens from Patients with Primary Carcinomas of the Colon and Rectum Well differentiated neuroendocrine neoplasms (carcinoid tumors) are not included. Based on AJCC/UICC
Protocol for the Examination of Specimens from Patients with Primary Carcinomas of the Colon and Rectum Well differentiated neuroendocrine neoplasms (carcinoid tumors) are not included. Based on AJCC/UICC
Kidney Case 1 SURGICAL PATHOLOGY REPORT
 Kidney Case 1 Surgical Pathology Report February 9, 2007 Clinical History: This 45 year old woman was found to have a left renal mass. CT urography with reconstruction revealed a 2 cm medial mass which
Kidney Case 1 Surgical Pathology Report February 9, 2007 Clinical History: This 45 year old woman was found to have a left renal mass. CT urography with reconstruction revealed a 2 cm medial mass which
Protocol for the Examination of Specimens from Patients with Primary Carcinoma of the Colon and Rectum
 Protocol for the Examination of Specimens from Patients with Primary Carcinoma of the Colon and Rectum Well-differentiated neuroendocrine neoplasms (carcinoid tumors) are not included. This modified NB
Protocol for the Examination of Specimens from Patients with Primary Carcinoma of the Colon and Rectum Well-differentiated neuroendocrine neoplasms (carcinoid tumors) are not included. This modified NB
Histo-prognostic factors what histopathology has to offer for clinical decision making
 Histo-prognostic factors what histopathology has to offer for clinical decision making Daniela E. Aust Institute for Pathology, University Hospital Dresden, Germany Center for Molecular Tumor Diagnostics
Histo-prognostic factors what histopathology has to offer for clinical decision making Daniela E. Aust Institute for Pathology, University Hospital Dresden, Germany Center for Molecular Tumor Diagnostics
The International Association for the Study of Lung Cancer (IASLC) Lung Cancer Staging Project, Data Elements
 Lung Cancer Staging Project, Data Elements") Page 1 Contents 1.1. Registration... 2 1.2. Patient Characteristics... 3 1.3. Laboratory Values at Diagnosis... 5 1.4. Lung Cancers with Multiple Lesions... 6 1.5. Primary Tumour Description... 10 1.6.
Page 1 Contents 1.1. Registration... 2 1.2. Patient Characteristics... 3 1.3. Laboratory Values at Diagnosis... 5 1.4. Lung Cancers with Multiple Lesions... 6 1.5. Primary Tumour Description... 10 1.6.
Head & Neck Squamous Carcinoma: Artifacts, Challenges, and Controversies. Agenda
 Head & Neck Squamous Carcinoma: Artifacts, Challenges, and Controversies Jennifer L. Hunt, MD, MEd Aubrey J. Hough Jr, MD, Endowed Professor of Pathology Chair of Pathology and Laboratory Medicine University
Head & Neck Squamous Carcinoma: Artifacts, Challenges, and Controversies Jennifer L. Hunt, MD, MEd Aubrey J. Hough Jr, MD, Endowed Professor of Pathology Chair of Pathology and Laboratory Medicine University
Seventh Edition Staging 2017 Breast
 Seventh Edition Staging 2017 Breast Donna M. Gress, RHIT, CTR Validating science. Improving patient care. No materials in this presentation may be repurposed in print or online without the express written
Seventh Edition Staging 2017 Breast Donna M. Gress, RHIT, CTR Validating science. Improving patient care. No materials in this presentation may be repurposed in print or online without the express written
Clinical, Pathologic and Molecular Updates
 Colorectal Cancer: Clinical, Pathologic and Molecular Updates Joanna A. Gibson, M.D./Ph.D. Yale University School of Medicine/Yale New Haven Hospital, Department of Pathology Gastrointestinal, Pancreaticobiliary
Colorectal Cancer: Clinical, Pathologic and Molecular Updates Joanna A. Gibson, M.D./Ph.D. Yale University School of Medicine/Yale New Haven Hospital, Department of Pathology Gastrointestinal, Pancreaticobiliary
Local staging of colon cancer: the current role of CT
 Local staging of colon cancer: the current role of CT Poster No.: C-2699 Congress: ECR 2018 Type: Authors: Keywords: DOI: Educational Exhibit A. P. Pissarra, R. R. Domingues Madaleno, C. Sanches, L. Curvo-
Local staging of colon cancer: the current role of CT Poster No.: C-2699 Congress: ECR 2018 Type: Authors: Keywords: DOI: Educational Exhibit A. P. Pissarra, R. R. Domingues Madaleno, C. Sanches, L. Curvo-
A Comparative Study of Rectal and Colonic Carcinoma: Demographic, Pathologic and TNM Staging Analysis
 Journal of the Egyptian Nat. Cancer Inst., Vol. 18, 3, September: 2-263, 2006 A Comparative Study of Rectal and ic Carcinoma: Demographic, Pathologic and TNM Staging Analysis TAREK N. EL-BOLKAINY, M.D.;
Journal of the Egyptian Nat. Cancer Inst., Vol. 18, 3, September: 2-263, 2006 A Comparative Study of Rectal and ic Carcinoma: Demographic, Pathologic and TNM Staging Analysis TAREK N. EL-BOLKAINY, M.D.;
Protocol for the Examination of Specimens From Patients With Primary Carcinoma of the Colon and Rectum
 Protocol for the Examination of Specimens From Patients With Primary Carcinoma of the Colon and Rectum Well-differentiated neuroendocrine neoplasms (carcinoid tumors) are not included. Based on AJCC/UICC
Protocol for the Examination of Specimens From Patients With Primary Carcinoma of the Colon and Rectum Well-differentiated neuroendocrine neoplasms (carcinoid tumors) are not included. Based on AJCC/UICC
NPQR Quality Payment Program (QPP) Measures 21_18247_LS.
 Measures 21_18247_LS.") NPQR Quality Payment Program (QPP) Measures 21_18247_LS MEASURE ID: QPP 99 MEASURE TITLE: Breast Cancer Resection Pathology Reporting pt Category (Primary Tumor) and pn Category (Regional Lymph Nodes)
NPQR Quality Payment Program (QPP) Measures 21_18247_LS MEASURE ID: QPP 99 MEASURE TITLE: Breast Cancer Resection Pathology Reporting pt Category (Primary Tumor) and pn Category (Regional Lymph Nodes)
Greater Manchester and Cheshire HPB Unit Guidelines for the Assessment & Management of Hepatobiliary and Pancreatic Disease Chapter 14
 Greater Manchester and Cheshire HPB Unit Guidelines for the Assessment & Management of Hepatobiliary and Pancreatic Disease Chapter 14 Contents 14. Neuroendocrine Tumours 161 14.1. Diagnostic algorithm
Greater Manchester and Cheshire HPB Unit Guidelines for the Assessment & Management of Hepatobiliary and Pancreatic Disease Chapter 14 Contents 14. Neuroendocrine Tumours 161 14.1. Diagnostic algorithm
Wendy L Frankel. Chair and Distinguished Professor
 1 Wendy L Frankel Chair and Distinguished Professor Case 1 59 y/o woman Abdominal pain No personal or family history of cancer History of colon polyps Colonoscopy Polypoid rectosigmoid mass Biopsy 3 4
1 Wendy L Frankel Chair and Distinguished Professor Case 1 59 y/o woman Abdominal pain No personal or family history of cancer History of colon polyps Colonoscopy Polypoid rectosigmoid mass Biopsy 3 4
Case presentation. Eran Zittan. MD Mount Sinai Hospital, Toronto, Canada. Emek Medical Center, Afula, Israel. March, 2016
 Case presentation Eran Zittan. MD Mount Sinai Hospital, Toronto, Canada. Emek Medical Center, Afula, Israel. March, 2016 60 y/o man with long standing UC+PSC. Last 10 years on clinical and endoscopic remission.
Case presentation Eran Zittan. MD Mount Sinai Hospital, Toronto, Canada. Emek Medical Center, Afula, Israel. March, 2016 60 y/o man with long standing UC+PSC. Last 10 years on clinical and endoscopic remission.
UICC TNM 8 th Edition Errata
 UICC TNM 8 th Edition Errata ions are in italics Head and Neck Tumours Pages 20, p27, p34, p38, p41, and p49 ly pn2a Metastasis in a single ipsilateral lymph node, less than 3cm in greatest dimension with
UICC TNM 8 th Edition Errata ions are in italics Head and Neck Tumours Pages 20, p27, p34, p38, p41, and p49 ly pn2a Metastasis in a single ipsilateral lymph node, less than 3cm in greatest dimension with
2018 Updates for Neoplasms of the Appendix, Colon, Rectum and GI NETs
 2018 Updates for Neoplasms of the Appendix, Colon, Rectum and GI NETs 1 2018-2019 FCDS WEBCAST SERIES 10/18/2018 STEVEN PEACE, CTR CDC & Florida DOH Attribution 2 Funding for this conference was made possible
2018 Updates for Neoplasms of the Appendix, Colon, Rectum and GI NETs 1 2018-2019 FCDS WEBCAST SERIES 10/18/2018 STEVEN PEACE, CTR CDC & Florida DOH Attribution 2 Funding for this conference was made possible
AJCC 7 th Edition Staging Disease Site Webinar Colorectum
 AJCC 7 th Edition Staging Disease Site Webinar Colorectum Donna M. Gress, RHIT, CTR Validating science. Improving patient care. This presentation was supported by the Cooperative Agreement Number DP13-1310
AJCC 7 th Edition Staging Disease Site Webinar Colorectum Donna M. Gress, RHIT, CTR Validating science. Improving patient care. This presentation was supported by the Cooperative Agreement Number DP13-1310