|
|
|
- Julian Johnston
- 5 years ago
- Views:
Transcription


1 Lya Crichlow, MD Kings County Hospital Center September 3, 2009 Morbidity and Mortality Conference
2 Case presentation 56 year old male who presented with 1 week history of dysphagia Unable to tolerate solids but able to tolerate soft diet and liquids PMHx: Denies PSHx: L humeral ORIF Meds: None
3 Case presentation Social Hx 40 pack year smoking history Alcohol abuse (1 pint of vodka per day/10 years) Review of systems: 10 pound weight iht loss over 2 weeks Physical exam: Cachetic No diffuse lymphadenopathy


4


5




6



7




8



9
10 Case Presentation CT chest 6/12/09 Marked thickening of the middle third of the esophagus with distension of the esophagus proximal to this point R hilar lymph node approximately 10 mm EGD 6/16/09 Large ulcerated, circumferential, partially obstructing mass at 28 cm from the gums, extending for approximately 6 cm Stomach and duodenum were unremarkable Unable to pass adult scope due to stricture Pathology Moderately differentiated squamous cell carcinoma
11 Case Presentation Barium swallow 6/15/2009 Infiltrating lesion midthoracic esophagus approximately 9 cm in length extending just below carina Tight stricture at central portion of the lesion, <5mm at most narrow point








12
13 Case Presentation PET SCAN 6/19/09 Neoplastic range metabolic FDG uptake in middle third of the esophagus (SUV 16.4) Pulmonary Function tests FEV1 66 % of normal ABG 7.42/42/93/27/98%/3.1





14
15 Surgery Procedure 6/25/09 Bronchoscopy Laparotomy Splenectomy Pyloroplasty Feeding jejunostomy Right thoracotomy Esophagectomy Left neck exploration Cervical esophagogastric anastamosis
16 Pathology 4 x 2.5 cm fungating mass invading muscular wall Moderately differentiated squamous cell carcinoma Negative margins 8 lymph nodes negative for tumor Stage T2NOMx
17 Postoperative Course POD # 4: Remained mechanically ventilated, febrile to 102. Bilateral pleural effusions POD # 5: Septic shock. Febrile bil to POD # 5: CT chest/abdomen/pelvis Bilateral l pneumonia No evidence of abscess in abdomen/pelvis




18
19 PostOperative Course Sputum culture from POD # 5: Hemophilus parainfluenzae POD # 6: Barium swallow: No evidence of leak





20
21 Postoperative Course Sputum culture from POD # 5: Hemophilus parainfluenzae POD # 6: Barium swallow: No evidence of leak POD # 18: Tracheostomy POD # 29: Bradycardia di progressing to full cardiac arrest. ACLS protocol performed for 10 minutes then patient was resuscitated. Responsive to painful stimuli
22 Postoperative Course POD # 29: Pt witnessed to have seizure activity after the code. Head CT showed no acute pathology POD # 35: Repeat head CT: Diffuse axonal injury Neurology consulted. EEG performed showing no correlation between disorganized movements therefore no evidence of seizure activity Unable to control movements with benzodiazapenes, clonopin or depakote POD # 67: Discharge to skilled nursing facility
23
24 Epidemiology Incidence in the United States is 20 per 100, 000 Worldwide incidence: 160 per 100, : ~ 14, 300 deaths 2 major histological types: Squamous cell carcinoma Adenocarcinoma
25 SQUAMOUS CELL CARCINOMA 70 % found in upper & middle 1/3 rd of esophagus Most common form of esophageal cancer worldwide Risk factors Smoking Alcohol Food additives eg nitrosamines (smoked food) ADENOCARCINOMA Distal 1/3 rd and at the GE junction Most common subtype in the US and Western world Risk factors Barrett s esophagus GERD Obesity
26 Presentation Asymptomatic Dysphagia especially to solids (60 % of the lumen must be occluded) d) Retrosternal pain Decreased parenteral intake Weight loss Hoarseness Aspiration pneumonia
27 Diagnosis Esophagram Recommended for any patient presenting with dysphagia Differentiate intramural vs intraluminal lesions Differentiate intrinsic vs extrinsic compression Endoscopy Visualize the lesion Location Biopsy
28 Staging 2 Classification systems exist: TNM system T tumor depth N Involvement of regional lymph nodes M Disease to nonregional lymph nodes & distant sites WNM system (Ellis system) W Wall penetration N number of positive lymph nodes M Distant disease



29 TNM staging Townsend: Sabiston Textbook of Surgery 18 th Edition 2007
30 Comparison of TNM & WNM staging systems Townsend: Sabiston Textbook of Surgery 18 th Edition 2007
31 Staging: CT Chest/Abdomen/Pelvis Length of the tumor Esophageal thickness and thickness of the stomach Regional lymph node status Distant metastasis
32 Staging: PET scan Uptake of fluorodeoxyglucose Evaluate primary mass, regional lymph nodes and distant disease Detection of metastatic disease: Sensitivity 88 %, Specificity 93 % Rizk et al 2006 examined if SUV levels can predict survival after esophagectomy. Pts with SUV < 4.5 more likely to have early stage disease and less lymph node involvement. Overall survival better than in high SUV group
33 Overall survival of all patients based on maximum SUV Conclusion PET SUV could predict clinical/pathologic stage and overall survival in pts with esophageal cancer Rizk et al Preoperative 18[F]-fluorodeoxyglucose positron emission tomograpy standardized uptake values predict survival after esophageal adenocarcinoma resection Ann Thorac Surg 2006: 81 (3)
34 Staging: Endoscopic Ultrasound Determine depth of tumor Status of regional lymph nodes Able to biopsy regional lymph nodes Disadvantage: Tends to overstage T status Understage N status Zuccaro et al 2006 compared EUS staging vs pathology after esophagectomy in 266 patients. T2 tumors only identified correctly in 42 % of patients by EUS, 54 % of cases they were overstaged as T3
35 Townsend: Sabiston Textbook of Surgery 18 th Edition 2007
36 History of esophageal resection Czerny st esophageal resection. Cervical tumor Torek 1911 Resection of thoracic esophagus. Pt had cervical esophagostomy & gastrostomy. External rubber tube connected the 2. Pt lived for 10 years Turner 1933 Transhiatal esophagectomy Oshawa 1933 Thoracic resection with anastomosis Ivor Lewis 1946 Described Ivor Lewis esophagectomy
37 Surgical Therapy Modified McKeown/Triincisional Technique Transhiatal Esophagectomy Ivor Lewis Esophagectomy En Bloc Resection Left thoracoabdominal approach
38 Transhiatal Esophagectomy Better surgical option for patients with poor pulmonary function i.e. FEV1 < 800 Contraindications: i Severe CAD or valvular disease Bulky tumors of midesophagus difficult to dissect



39 Transhiatal Esophagectomy ACS Principles & Practice of Surgery 2009


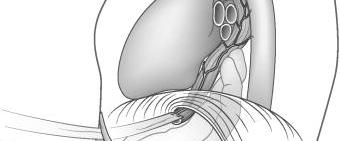


40 Transhiatal Esophagectomy Selke: Sabiston & Spencer Surgery of the Chest; 7 th Edition 2005







41 Transhiatal Esophagectomy ACS Principles & Practice of Surgery 2009





42 Transhiatal Esophagectomy ACS Principles & Practice of Surgery 2009
43 Modified McKeown/Triincisional Technique Combination of Ivor Lewis and transhiatal approaches Useful for tumors at any level of the esophagus Consists of: Laparotomy with construction of gastric neoesophagus Right thoracotomy Cervical anastomosis
44 Ivor Lewis Esophagectomy Contraindications Tumors in upper 1/3 rd of esophagus Long segment Barrett s esophagus with extension into cervical esophagus Technique Laparotomy R thoracotomy Anastomosis is made in the chest




45 Ivor Lewis Esophagectomy ACS Principles & Practice of Surgery 2009






46 Ivor Lewis Esophagectomy ACS Principles & Practice of Surgery 2009
47 En Bloc Resection Advocated by some surgeons as there are some studies which show removal of lymph nodes improves survival Technique Triincisional Ligation of azygos, hemiazygos, intercostal veins Removal of mediastinal lymph nodes Excision of rim of diaphragm Removal of paracardial, left gastric, portal, common hepatic, celiac, splenic lymph nodes Cervical esophagogastric anastomosis
48 Complications of Esophagectomy Mortality Historically % Experienced centers: 3 4 % Advances in ICU care have improved mortality significantly Anastomotic leak Ivor Lewis: Mediastinitis t s Cervical leaks can be drained
49 Complications of Esophagectomy Anastomotic Stricture Recurrent Laryngeal Nerve Injury Respiratory Incidence reported 2 47 % Hemorrhage Delayed emptying of the conduit
50 Chemotherapy & Radiation Radiation as a sole therapy mainly for poor sugical candidates or those in need of palliation RTOG study Randomized control trial over 5 years Radiation (64 Gy) vs radiation (50 Gy) plus chemotherapy (cisplatin, fluorouracil) T1 3N0 1M0 At 5 years, survival for combination therapy group was 26 % vs 0 % for radiation alone
51 Does chemotherapy followed by surgery offer any benefit? American Intergroup 0113 trial Randomized control study Compared surgery alone vs preoperative chemotherapy followed by surgery No significant difference between 2 groups in terms of survival Meta analyses have shown a some survival benefit to preoperative chemotherapy
52 What is the role of chemoradiation? 2 most important prognostic factors: Tumor invasion Lymph node metastasis T stage Chemoradiotherapy for T2 lesions or above (some surgeons advocate en bloc resection has as good results as chemoradiotherapy for T2 lesions) Chemoradiotherapy for any evidence of lymph node disease
53 Conclusion Improvements in surgical critical care, resection technique and multimodal therapy have improved the survival of esophageal cancer Surgery remains a crucial element in the treatment of the disease Current studies show that lymph node status and depth of tumor invasion are the most important prognostic factors
54 References Rizk et al Preoperative 18[F] fluorodeoxyglucose positron emission tomograpy standardized uptake values predict survival after esophageal adenocarcinoma resection Ann Thorac Surg 2006: 81 (3) Zuccaro et al Endoscopic ultrasound errors in esophageal caner Am J Gastroenterol 2005; 100 (3): Selke: Sabiston & Spencer Surgery of the Chest: 7 th Edition Townsend: Sabiston Textbook of Surgery: 18 th Edition Cooper et al Chemoradiatotherapy of locally advanced esophageal cancer: long term follow up of a prospective randominzed trial (RTOG 85 01). Radiation Therapy Oncology Group JAMA 1999; 281 (17): Kelsen et al Chemotherapy followed by surgery compared with surgery alone for localized esophageal cancer. N Engl J Med 1998; 339 (27): Dubecz et al Modern Surgery for Esophageal Cancer Gastroenterol t Clin N Am 37 (2008) Quiros et al Multidisciplinary Approach to Esophageal and Gastric Cancer Surg Clin N Am 89 (2009) 79 96
Aliu Sanni MD SUNY Downstate Medical Center August 16, 2012
 Aliu Sanni MD SUNY Downstate Medical Center August 16, 2012 Case Presentation 60yr old AAF with PMH of CAD s/p PCI 1983, CVA, GERD, HTN presented with retrosternal chest pain on 06/12 Associated dysphagia
Aliu Sanni MD SUNY Downstate Medical Center August 16, 2012 Case Presentation 60yr old AAF with PMH of CAD s/p PCI 1983, CVA, GERD, HTN presented with retrosternal chest pain on 06/12 Associated dysphagia
Management of Esophageal Cancer: Evidence Based Review of Current Guidelines. Madhuri Rao, MD PGY-5 SUNY Downstate Medical Center
 Management of Esophageal Cancer: Evidence Based Review of Current Guidelines Madhuri Rao, MD PGY-5 SUNY Downstate Medical Center Case Presentation 68 y/o male PMH: NIDDM, HTN, hyperlipidemia, CAD s/p stents,
Management of Esophageal Cancer: Evidence Based Review of Current Guidelines Madhuri Rao, MD PGY-5 SUNY Downstate Medical Center Case Presentation 68 y/o male PMH: NIDDM, HTN, hyperlipidemia, CAD s/p stents,
SETTING Fudan University Shanghai Cancer Center. RESPONSIBLE PARTY Haiquan Chen MD.
 OFFICIAL TITLE A Phase Ⅲ Study of Left Side Thoracotomy Approach (SweetProcedure) Versus Right Side Thoracotomy Plus Midline Laparotomy Approach (Ivor-Lewis Procedure) Esophagectomy in Middle or Lower
OFFICIAL TITLE A Phase Ⅲ Study of Left Side Thoracotomy Approach (SweetProcedure) Versus Right Side Thoracotomy Plus Midline Laparotomy Approach (Ivor-Lewis Procedure) Esophagectomy in Middle or Lower
Quiz Adenocarcinoma of the distal stomach has been increasing in the last 20 years. a. True b. False
 Quiz 1 1. Which of the following are risk factors for esophagus cancer. a. Obesity b. Gastroesophageal reflux c. Smoking and Alcohol d. All of the above 2. Adenocarcinoma of the distal stomach has been
Quiz 1 1. Which of the following are risk factors for esophagus cancer. a. Obesity b. Gastroesophageal reflux c. Smoking and Alcohol d. All of the above 2. Adenocarcinoma of the distal stomach has been
Case Scenario year-old white male presented to personal physician with dyspepsia with reflux.
 Case Scenario 1 57-year-old white male presented to personal physician with dyspepsia with reflux. 7/12 EGD: In the gastroesophageal junction we found an exophytic tumor. The tumor occupies approximately
Case Scenario 1 57-year-old white male presented to personal physician with dyspepsia with reflux. 7/12 EGD: In the gastroesophageal junction we found an exophytic tumor. The tumor occupies approximately
 Surgical Management of Esophageal Cancer Sophia L Fu, MD Long Island College Hospital SUNY Downstate Medical Center, Brooklyn, NY 03/27/2009 Questions The T and N status of esophageal carcinoma is most
Surgical Management of Esophageal Cancer Sophia L Fu, MD Long Island College Hospital SUNY Downstate Medical Center, Brooklyn, NY 03/27/2009 Questions The T and N status of esophageal carcinoma is most
Controversies in management of squamous esophageal cancer
 2015.06.12 12.47.48 Page 4(1) IS-1 Controversies in management of squamous esophageal cancer C S Pramesh Thoracic Surgery, Department of Surgical Oncology, Tata Memorial Centre, India In Asia, squamous
2015.06.12 12.47.48 Page 4(1) IS-1 Controversies in management of squamous esophageal cancer C S Pramesh Thoracic Surgery, Department of Surgical Oncology, Tata Memorial Centre, India In Asia, squamous
Determining the Optimal Surgical Approach to Esophageal Cancer
 Determining the Optimal Surgical Approach to Esophageal Cancer Amit Bhargava, MD Attending Thoracic Surgeon Department of Cardiovascular and Thoracic Surgery Open Esophagectomy versus Minimally Invasive
Determining the Optimal Surgical Approach to Esophageal Cancer Amit Bhargava, MD Attending Thoracic Surgeon Department of Cardiovascular and Thoracic Surgery Open Esophagectomy versus Minimally Invasive
Case Scenario 1. The patient has now completed his neoadjuvant chemoradiation and has been cleared for surgery.
 Case Scenario 1 July 10, 2010 A 67-year-old male with squamous cell carcinoma of the mid thoracic esophagus presents for surgical resection. The patient has completed preoperative chemoradiation. This
Case Scenario 1 July 10, 2010 A 67-year-old male with squamous cell carcinoma of the mid thoracic esophagus presents for surgical resection. The patient has completed preoperative chemoradiation. This
Minimally Invasive Esophagectomy- Valuable. Jayer Chung, MD University of Colorado Health Sciences Center December 11, 2006
 Minimally Invasive Esophagectomy- Valuable Jayer Chung, MD University of Colorado Health Sciences Center December 11, 2006 Overview Esophageal carcinoma What is minimally invasive esophagectomy (MIE)?
Minimally Invasive Esophagectomy- Valuable Jayer Chung, MD University of Colorado Health Sciences Center December 11, 2006 Overview Esophageal carcinoma What is minimally invasive esophagectomy (MIE)?
ESOPHAGEAL CANCER. Dr. Paul Gardiner December 17, 2002 Discipline of Surgery Rounds
 ESOPHAGEAL CANCER Dr. Paul Gardiner December 17, 2002 Discipline of Surgery Rounds ESOPHAGEAL CANCER I. EPIDEMIOLOGY INCIDENCE, DIAGNOSIS & STAGING II. TREATMENT OPTIONS Current role of induction therapies
ESOPHAGEAL CANCER Dr. Paul Gardiner December 17, 2002 Discipline of Surgery Rounds ESOPHAGEAL CANCER I. EPIDEMIOLOGY INCIDENCE, DIAGNOSIS & STAGING II. TREATMENT OPTIONS Current role of induction therapies
Robotic Surgery for Esophageal Cancer
 Robotic Surgery for Esophageal Cancer Kemp H. Kernstine, MD PhD Division of Thoracic Surgery City of Hope Medical Center and Beckman Research Institute May 1, 2010 Esophageal Cancer on the Rise JNCI 2005,
Robotic Surgery for Esophageal Cancer Kemp H. Kernstine, MD PhD Division of Thoracic Surgery City of Hope Medical Center and Beckman Research Institute May 1, 2010 Esophageal Cancer on the Rise JNCI 2005,
Surgical strategies in esophageal cancer
 Gastro-Conference Berlin 2005 October 1-2, 2005 Surgical strategies in esophageal cancer J. Rüdiger Siewert Department of Surgery, Klinikum rechts der Isar Technische Universität München Esophageal Cancer
Gastro-Conference Berlin 2005 October 1-2, 2005 Surgical strategies in esophageal cancer J. Rüdiger Siewert Department of Surgery, Klinikum rechts der Isar Technische Universität München Esophageal Cancer
The Learning Curve for Minimally Invasive Esophagectomy
 The Learning Curve for Minimally Invasive Esophagectomy AATS Focus on Thoracic Surgery Mastering Surgical Innovation Las Vegas Nevada Oct. 27-28 2017 Scott J Swanson, M.D. Professor of Surgery Harvard
The Learning Curve for Minimally Invasive Esophagectomy AATS Focus on Thoracic Surgery Mastering Surgical Innovation Las Vegas Nevada Oct. 27-28 2017 Scott J Swanson, M.D. Professor of Surgery Harvard
ESOPHAGEAL CANCER AND GERD. Prof Salman Guraya FRCS, Masters MedEd
 ESOPHAGEAL CANCER AND GERD Prof Salman Guraya FRCS, Masters MedEd Learning objectives Esophagus anatomy and physiology Esophageal cancer Causes, presentations of esophageal cancer Diagnosis and management
ESOPHAGEAL CANCER AND GERD Prof Salman Guraya FRCS, Masters MedEd Learning objectives Esophagus anatomy and physiology Esophageal cancer Causes, presentations of esophageal cancer Diagnosis and management
7/20/2017. Esophageal Cancer: A Less Common But Deadly Cancer. Objectives. Disclosure Statement NYNPA Conference October Saratoga New York
 Esophageal Cancer: A Less Common But Deadly Cancer 2017 NYNPA Conference October 18-22 Saratoga New York Mary McGreal DNP, RN, ANP-C, CCRN, CMC, Adjunct Professor at Stony Brook University School of Nursing
Esophageal Cancer: A Less Common But Deadly Cancer 2017 NYNPA Conference October 18-22 Saratoga New York Mary McGreal DNP, RN, ANP-C, CCRN, CMC, Adjunct Professor at Stony Brook University School of Nursing
Oesophageal Cancer: The Image after Surgery
 Oesophageal Cancer: The Image after Surgery Poster No.: C-2253 Congress: ECR 2014 Type: Educational Exhibit Authors: A. Loureiro, N. V. V. B. Marques, M. Palmeiro, P. Pereira, 1 1 1 1 2 1 1 2 1 R. Gil,
Oesophageal Cancer: The Image after Surgery Poster No.: C-2253 Congress: ECR 2014 Type: Educational Exhibit Authors: A. Loureiro, N. V. V. B. Marques, M. Palmeiro, P. Pereira, 1 1 1 1 2 1 1 2 1 R. Gil,
Oesophageal Cancer: The Image after Surgery
 Oesophageal Cancer: The Image after Surgery Poster No.: C-2253 Congress: ECR 2014 Type: Educational Exhibit Authors: A. Loureiro, N. V. V. B. Marques, M. Palmeiro, P. Pereira, 1 1 1 1 2 1 1 2 1 R. Gil,
Oesophageal Cancer: The Image after Surgery Poster No.: C-2253 Congress: ECR 2014 Type: Educational Exhibit Authors: A. Loureiro, N. V. V. B. Marques, M. Palmeiro, P. Pereira, 1 1 1 1 2 1 1 2 1 R. Gil,
Esophageal cancer: Biology, natural history, staging and therapeutic options
 EGEUS 2nd Meeting Esophageal cancer: Biology, natural history, staging and therapeutic options Michael Bau Mortensen MD, Ph.D. Associate Professor of Surgery Centre for Surgical Ultrasound, Upper GI Section,
EGEUS 2nd Meeting Esophageal cancer: Biology, natural history, staging and therapeutic options Michael Bau Mortensen MD, Ph.D. Associate Professor of Surgery Centre for Surgical Ultrasound, Upper GI Section,
Esophageal Cancer. Wesley A. Papenfuss MD FACS Surgical Oncology Aurora Cancer Care. David Demos MD Thoracic Surgery Aurora Cancer Care
 Esophageal Cancer Wesley A. Papenfuss MD FACS Surgical Oncology Aurora Cancer Care David Demos MD Thoracic Surgery Aurora Cancer Care No Disclosures Learning Objectives Review the classification scheme
Esophageal Cancer Wesley A. Papenfuss MD FACS Surgical Oncology Aurora Cancer Care David Demos MD Thoracic Surgery Aurora Cancer Care No Disclosures Learning Objectives Review the classification scheme
CASE REPORTS. Giant Esophagus. An Unusual Case of Massive Idiopathic Hypertrophy
 CASE REPORTS An Unusual Case of Massive Idiopathic Hypertrophy and Dilatation of the Esophagus and Proximal Stomach Mark H. Wall, M.D., Epifanio E. Espinas, M.D., Arthur W. Silver, M.D., and Francis X.
CASE REPORTS An Unusual Case of Massive Idiopathic Hypertrophy and Dilatation of the Esophagus and Proximal Stomach Mark H. Wall, M.D., Epifanio E. Espinas, M.D., Arthur W. Silver, M.D., and Francis X.
1. Epidemiology of Esophageal Cancer 2. Operative Strategies 3. Minimally Invasive Esophagectomy 4. Video
 Minimally Invasive Esophagectomy Guilherme M Campos, MD, FACS Assistant Professor of Surgery Director G.I. Motility Center Director Bariatric Surgery Program University of California San Francisco ESOPHAGEAL
Minimally Invasive Esophagectomy Guilherme M Campos, MD, FACS Assistant Professor of Surgery Director G.I. Motility Center Director Bariatric Surgery Program University of California San Francisco ESOPHAGEAL
RTC Dec Felicitas Koller and Eric Grogan
 RTC Dec 11 2009 Felicitas Koller and Eric Grogan Cancer Statistics, United States Number of patients 200000 150000 100000 50000 0 Lung Breast New Cases Deaths Esophageal Colorectal Prostate http://www.cancer.org/statistics
RTC Dec 11 2009 Felicitas Koller and Eric Grogan Cancer Statistics, United States Number of patients 200000 150000 100000 50000 0 Lung Breast New Cases Deaths Esophageal Colorectal Prostate http://www.cancer.org/statistics
A 16 yr old boy with aggressive ca esophagus. DR Ayunga A.O Physician-Garisa PGH Associate Faculty Lecturer-UON Afya Bora Fellow in Global Health
 A 16 yr old boy with aggressive ca esophagus DR Ayunga A.O Physician-Garisa PGH Associate Faculty Lecturer-UON Afya Bora Fellow in Global Health Cancer of esophagus in a 16yr old Y.N 16 yr old boy unwell
A 16 yr old boy with aggressive ca esophagus DR Ayunga A.O Physician-Garisa PGH Associate Faculty Lecturer-UON Afya Bora Fellow in Global Health Cancer of esophagus in a 16yr old Y.N 16 yr old boy unwell
MINIMALLY INVASIVE ESOPHAGECTOMY FOR CANCER: where do we stand?
 MINIMALLY INVASIVE ESOPHAGECTOMY FOR CANCER: where do we stand? Ph Nafteux, MD Copenhagen, Nov 3rd 2011 Department of Thoracic Surgery, University Hospitals Leuven, Belgium W. Coosemans, H. Decaluwé, Ph.
MINIMALLY INVASIVE ESOPHAGECTOMY FOR CANCER: where do we stand? Ph Nafteux, MD Copenhagen, Nov 3rd 2011 Department of Thoracic Surgery, University Hospitals Leuven, Belgium W. Coosemans, H. Decaluwé, Ph.
Transhiatal Esophagectomy: Lower Mortality, Diminished Morbidity, Equal Effectiveness
 Transhiatal Esophagectomy: Lower Mortality, Diminished Morbidity, Equal Effectiveness Sunil Malhotra, M.D. Department of Surgery University of Colorado Resident Debate April 30, 2007 Esophageal Cancer
Transhiatal Esophagectomy: Lower Mortality, Diminished Morbidity, Equal Effectiveness Sunil Malhotra, M.D. Department of Surgery University of Colorado Resident Debate April 30, 2007 Esophageal Cancer
Determining Resectability and Appropriate Surgery for Esophageal Cancer
 Determining Resectability and Appropriate Surgery for Esophageal Cancer Peter Baik, DO, FACOS Thoracic Surgery Cancer Treatment Centers of America 1 Esophageal and Esophagogastric Junction Cancers Siewert
Determining Resectability and Appropriate Surgery for Esophageal Cancer Peter Baik, DO, FACOS Thoracic Surgery Cancer Treatment Centers of America 1 Esophageal and Esophagogastric Junction Cancers Siewert
Surgical Problems in Proximal GI Cancer Management Cardia Tumours Question #1: What are cardia tumours?
 Surgical Problems in Proximal GI Cancer Management Cardia Tumours Question #1: What are cardia tumours? Question #2: How are cardia tumours managed? Michael F. Humer December 3, 2005 Vancouver, BC Case
Surgical Problems in Proximal GI Cancer Management Cardia Tumours Question #1: What are cardia tumours? Question #2: How are cardia tumours managed? Michael F. Humer December 3, 2005 Vancouver, BC Case
AATS Focus on Thoracic Surgery: Minimally Invasive Esophagectomy: Are We Still Getting Better in 2017?
 AATS Focus on Thoracic Surgery: Mastering Surgical Innovation Las Vegas, NV October 28, 2017 Session VIII: Video Session Minimally Invasive Esophagectomy: Are We Still Getting Better in 2017? James D.
AATS Focus on Thoracic Surgery: Mastering Surgical Innovation Las Vegas, NV October 28, 2017 Session VIII: Video Session Minimally Invasive Esophagectomy: Are We Still Getting Better in 2017? James D.
Imaging in gastric cancer
 Imaging in gastric cancer Gastric cancer remains a deadly disease because of late diagnosis. Adenocarcinoma represents 90% of malignant tumors. Diagnosis is based on endoscopic examination with biopsies.
Imaging in gastric cancer Gastric cancer remains a deadly disease because of late diagnosis. Adenocarcinoma represents 90% of malignant tumors. Diagnosis is based on endoscopic examination with biopsies.
Thymic Tumors. Feiran Lou MD. MS. Kings County Hospital Department of Surgery
 Thymic Tumors Feiran Lou MD. MS. Kings County Hospital Department of Surgery Case HPI 53 yo man referred from OSH for anterior mediastinal mass. Initially presented with leg weakness and back pain for
Thymic Tumors Feiran Lou MD. MS. Kings County Hospital Department of Surgery Case HPI 53 yo man referred from OSH for anterior mediastinal mass. Initially presented with leg weakness and back pain for
Minimally Invasive Esophagectomy
 Minimally Invasive Esophagectomy M A R K B E R R Y, M D A S S O C I AT E P R O F E S S O R D E PA R T M E N T OF C A R D I O T H O R A C I C S U R G E R Y S TA N F O R D U N I V E R S I T Y S E P T E M
Minimally Invasive Esophagectomy M A R K B E R R Y, M D A S S O C I AT E P R O F E S S O R D E PA R T M E N T OF C A R D I O T H O R A C I C S U R G E R Y S TA N F O R D U N I V E R S I T Y S E P T E M
Limited en bloc Resection of the Gastroesophageal Junction with Isoperistaltic Jejunal Interposition
 22 Limited en bloc Resection of the Gastroesophageal Junction with Isoperistaltic Jejunal Interposition J.R. Izbicki, W.T. Knoefel, D. C. Broering ] Indications Severe dysplasia in the distal esophagus
22 Limited en bloc Resection of the Gastroesophageal Junction with Isoperistaltic Jejunal Interposition J.R. Izbicki, W.T. Knoefel, D. C. Broering ] Indications Severe dysplasia in the distal esophagus
Case Scenario 1. The patient agreed to a CT guided biopsy of the left upper lobe mass. This was performed and confirmed non-small cell carcinoma.
 Case Scenario 1 An 89 year old male patient presented with a progressive cough for approximately six weeks for which he received approximately three rounds of antibiotic therapy without response. A chest
Case Scenario 1 An 89 year old male patient presented with a progressive cough for approximately six weeks for which he received approximately three rounds of antibiotic therapy without response. A chest
COLLECTING CANCER DATA: STOMACH AND ESOPHAGUS
 COLLECTING CANCER DATA: STOMACH AND ESOPHAGUS 2017 2018 NAACCR WEBINAR SERIES Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching
COLLECTING CANCER DATA: STOMACH AND ESOPHAGUS 2017 2018 NAACCR WEBINAR SERIES Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching
Mediastinal Staging. Samer Kanaan, M.D.
 Mediastinal Staging Samer Kanaan, M.D. Overview Importance of accurate nodal staging Accuracy of radiographic staging Mediastinoscopy EUS EBUS Staging TNM Definitions T Stage Size of the Primary Tumor
Mediastinal Staging Samer Kanaan, M.D. Overview Importance of accurate nodal staging Accuracy of radiographic staging Mediastinoscopy EUS EBUS Staging TNM Definitions T Stage Size of the Primary Tumor
UCLA General Surgery Residency Program Rotation Educational Policy Goals and Objectives
 UPDATED: July 2009 ROTATION: THORACIC SURGERY UCLA General Surgery Residency Program ROTATION DIRECTOR: Mary Maish, M.D. CHIEF OF CARDIAC SURGERY: Robert Cameron, M.D. SITES: UCLA Medical Center - Westwood
UPDATED: July 2009 ROTATION: THORACIC SURGERY UCLA General Surgery Residency Program ROTATION DIRECTOR: Mary Maish, M.D. CHIEF OF CARDIAC SURGERY: Robert Cameron, M.D. SITES: UCLA Medical Center - Westwood
Minimally Invasive Esophagectomy
 American Association of Thoracic Surgery (AATS) 95 th Annual Meeting Seattle, WA April 29, 2015 General Thoracic Masters of Surgery Video Session Minimally Invasive Esophagectomy James D. Luketich MD,
American Association of Thoracic Surgery (AATS) 95 th Annual Meeting Seattle, WA April 29, 2015 General Thoracic Masters of Surgery Video Session Minimally Invasive Esophagectomy James D. Luketich MD,
Minimally Invasive Esophagectomy: OVERRATED!!! Sagar Damle UCHSC December 11, 2006
 Minimally Invasive Esophagectomy: OVERRATED!!! Sagar Damle UCHSC December 11, 2006 Esophageal Cancer - Est. 15,000 cases in 2006 - Est. 14,000 deaths - Overall 5-year survival: 15.6% - 33.6 % for local
Minimally Invasive Esophagectomy: OVERRATED!!! Sagar Damle UCHSC December 11, 2006 Esophageal Cancer - Est. 15,000 cases in 2006 - Est. 14,000 deaths - Overall 5-year survival: 15.6% - 33.6 % for local
A Proposed Strategy for Treatment of Superficial Carcinoma. in the Thoracic Esophagus Based on an Analysis. of Lymph Node Metastasis
 Kitakanto Med J 2002 ; 52 : 189-193 189 A Proposed Strategy for Treatment of Superficial Carcinoma in the Thoracic Esophagus Based on an Analysis of Lymph Node Metastasis Susumu Kawate,' Susumu Ohwada,'
Kitakanto Med J 2002 ; 52 : 189-193 189 A Proposed Strategy for Treatment of Superficial Carcinoma in the Thoracic Esophagus Based on an Analysis of Lymph Node Metastasis Susumu Kawate,' Susumu Ohwada,'
Abstracting Upper GI Cancer Incidence and Treatment Data Quiz 1 Multiple Primary and Histologies Case 1 Final Pathology:
 Abstracting Upper GI Cancer Incidence and Treatment Data Quiz 1 Multiple Primary and Histologies Case 1 A 74 year old male with a history of GERD presents complaining of dysphagia. An esophagogastroduodenoscopy
Abstracting Upper GI Cancer Incidence and Treatment Data Quiz 1 Multiple Primary and Histologies Case 1 A 74 year old male with a history of GERD presents complaining of dysphagia. An esophagogastroduodenoscopy
Larry Tan, MD Thoracic Surgery, HSC. Community Cancer Care Educational Conference October 27, 2017
 Larry Tan, MD Thoracic Surgery, HSC Community Cancer Care Educational Conference October 27, 2017 To describe patient referral & triage for the patient with suspected lung cancer To describe the initial
Larry Tan, MD Thoracic Surgery, HSC Community Cancer Care Educational Conference October 27, 2017 To describe patient referral & triage for the patient with suspected lung cancer To describe the initial
Slide 1. Slide 2. Slide 3. Investigation and management of lung cancer Robert Rintoul. Epidemiology. Risk factors/aetiology
 Slide 1 Investigation and management of lung cancer Robert Rintoul Department of Thoracic Oncology Papworth Hospital Slide 2 Epidemiology Second most common cancer in the UK (after breast). 38 000 new
Slide 1 Investigation and management of lung cancer Robert Rintoul Department of Thoracic Oncology Papworth Hospital Slide 2 Epidemiology Second most common cancer in the UK (after breast). 38 000 new
MEDIASTINAL STAGING surgical pro
 MEDIASTINAL STAGING surgical pro Paul E. Van Schil, MD, PhD Department of Thoracic and Vascular Surgery University of Antwerp, Belgium Mediastinal staging Invasive techniques lymph node mapping cervical
MEDIASTINAL STAGING surgical pro Paul E. Van Schil, MD, PhD Department of Thoracic and Vascular Surgery University of Antwerp, Belgium Mediastinal staging Invasive techniques lymph node mapping cervical
National Oesophago-Gastric Cancer Audit New Patient Registration sheet Patients with Oesophageal High Grade Glandular Dysplasia
 National Oesophago-Gastric Cancer Audit New Patient Registration sheet Patients with Oesophageal High Grade Glandular Dysplasia Patient Details Surname: NHS number: Forename: Postcode: Sex: Male Female
National Oesophago-Gastric Cancer Audit New Patient Registration sheet Patients with Oesophageal High Grade Glandular Dysplasia Patient Details Surname: NHS number: Forename: Postcode: Sex: Male Female
Index. Surg Oncol Clin N Am 16 (2007) Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type.") Surg Oncol Clin N Am 16 (2007) 465 469 Index Note: Page numbers of article titles are in boldface type. A Adjuvant therapy, preoperative for gastric cancer, staging and, 339 B Breast cancer, metabolic
Surg Oncol Clin N Am 16 (2007) 465 469 Index Note: Page numbers of article titles are in boldface type. A Adjuvant therapy, preoperative for gastric cancer, staging and, 339 B Breast cancer, metabolic
Clinical study on postoperative recurrence in patients with pn0 esophageal squamous cell carcinoma
 Guo et al. Journal of Cardiothoracic Surgery 2014, 9:150 RESEARCH ARTICLE Open Access Clinical study on postoperative recurrence in patients with pn0 esophageal squamous cell carcinoma Xu-feng Guo, Teng
Guo et al. Journal of Cardiothoracic Surgery 2014, 9:150 RESEARCH ARTICLE Open Access Clinical study on postoperative recurrence in patients with pn0 esophageal squamous cell carcinoma Xu-feng Guo, Teng
Gastroesophageal reflux disease Principles of GERD treatment Treatment of reflux diseases GERD
 Esophagus Anatomy/Physiology Gastroesophageal reflux disease Principles of GERD treatment Treatment of reflux diseases GERD Manometry Question 50 years old female with chest pain and dysphagia. Manometry
Esophagus Anatomy/Physiology Gastroesophageal reflux disease Principles of GERD treatment Treatment of reflux diseases GERD Manometry Question 50 years old female with chest pain and dysphagia. Manometry
Robotic-assisted McKeown esophagectomy
 Case Report Page 1 of 8 Robotic-assisted McKeown esophagectomy Dingpei Han, Su Yang, Wei Guo, Runsen Jin, Yajie Zhang, Xingshi Chen, Han Wu, Hailei Du, Kai Chen, Jie Xiang, Hecheng Li Department of Thoracic
Case Report Page 1 of 8 Robotic-assisted McKeown esophagectomy Dingpei Han, Su Yang, Wei Guo, Runsen Jin, Yajie Zhang, Xingshi Chen, Han Wu, Hailei Du, Kai Chen, Jie Xiang, Hecheng Li Department of Thoracic
Case Scenario 1. Pathology report Specimen from mediastinoscopy Final Diagnosis : Metastatic small cell carcinoma with residual lymphatic tissue
 Case Scenario 1 Oncology Consult: Patient is a 51-year-old male with history of T4N3 squamous cell carcinoma of tonsil status post concurrent chemoradiation finished in October two years ago. He was hospitalized
Case Scenario 1 Oncology Consult: Patient is a 51-year-old male with history of T4N3 squamous cell carcinoma of tonsil status post concurrent chemoradiation finished in October two years ago. He was hospitalized
Surgery for Gastric and Oesophageal Cancer
 Surgery for Gastric and Oesophageal Cancer Trends in cancer mortality, England and Wales SMR base 1980 Oesophago-Gastric Cancer The National Problem 5 th commonest malignancy 4 th commonest cause of death
Surgery for Gastric and Oesophageal Cancer Trends in cancer mortality, England and Wales SMR base 1980 Oesophago-Gastric Cancer The National Problem 5 th commonest malignancy 4 th commonest cause of death
Esophageal Cancer. What is esophageal cancer?
 Scan for mobile link. Esophageal Cancer Esophageal cancer occurs when cancer cells develop in the esophagus. The two main types are squamous cell carcinoma and adenocarcinoma. Esophageal cancer may not
Scan for mobile link. Esophageal Cancer Esophageal cancer occurs when cancer cells develop in the esophagus. The two main types are squamous cell carcinoma and adenocarcinoma. Esophageal cancer may not
Esophageal Cancer. Source: National Cancer Institute
 Esophageal Cancer Esophageal cancer forms in the tissues that line the esophagus, or the long, hollow tube that connects the mouth and stomach. Food and drink pass through the esophagus to be digested.
Esophageal Cancer Esophageal cancer forms in the tissues that line the esophagus, or the long, hollow tube that connects the mouth and stomach. Food and drink pass through the esophagus to be digested.
FTS Oesophagectomy: minimal research to date 3,4
 Fast Track Programme in patients undergoing Oesophagectomy: A Single Centre 5 year experience Sullivan J, McHugh S, Myers E, Broe P Department of Upper Gastrointestinal Surgery Beaumont Hospital Dublin,
Fast Track Programme in patients undergoing Oesophagectomy: A Single Centre 5 year experience Sullivan J, McHugh S, Myers E, Broe P Department of Upper Gastrointestinal Surgery Beaumont Hospital Dublin,
WHO BENEFITS FROM ADJUVANT CHEMOTHERAPY RADIATION CHEMORADIATION? Dr. Paul Gardiner April 23, 2001 Discipline of Surgery Grand Rounds
 WHO BENEFITS FROM ADJUVANT CHEMOTHERAPY RADIATION CHEMORADIATION? Dr. Paul Gardiner April 23, 2001 Discipline of Surgery Grand Rounds LUNG Dr. Greenland ESOPHAGUS Dr. Gardiner ESOPHAGEAL CANCER 1200 new
WHO BENEFITS FROM ADJUVANT CHEMOTHERAPY RADIATION CHEMORADIATION? Dr. Paul Gardiner April 23, 2001 Discipline of Surgery Grand Rounds LUNG Dr. Greenland ESOPHAGUS Dr. Gardiner ESOPHAGEAL CANCER 1200 new
Esophageal Cancer Staging Essentials: The New TNM Staging System (7th edition) and Clinicoradiologic Implications
 and Clinicoradiologic Implications") Esophageal Cancer Staging Essentials: The New TNM Staging System (7th edition) and Clinicoradiologic Implications Poster No.: E-0060 Congress: ESTI 2012 Type: Scientific Exhibit Authors: K. Lee, T. J.
Esophageal Cancer Staging Essentials: The New TNM Staging System (7th edition) and Clinicoradiologic Implications Poster No.: E-0060 Congress: ESTI 2012 Type: Scientific Exhibit Authors: K. Lee, T. J.
Esophageal cancer. What is esophageal cancer? Esophageal cancer is a disease in which malignant (cancer) cells form in the tissues of the esophagus.
 cells form in the tissues of the esophagus.") Esophageal Cancer Esophageal cancer What is esophageal cancer? What are risk factors? Signs and symptoms Tests for esophageal cancer Stages of esophageal cancer Treatment options What is esophageal cancer?
Esophageal Cancer Esophageal cancer What is esophageal cancer? What are risk factors? Signs and symptoms Tests for esophageal cancer Stages of esophageal cancer Treatment options What is esophageal cancer?
Bronchogenic Carcinoma
 A 55-year-old construction worker has smoked 2 packs of ciggarettes daily for the past 25 years. He notes swelling in his upper extremity & face, along with dilated veins in this region. What is the most
A 55-year-old construction worker has smoked 2 packs of ciggarettes daily for the past 25 years. He notes swelling in his upper extremity & face, along with dilated veins in this region. What is the most
Appendix 1: Regional Lymph Node Stations for Staging Esophageal Cancer
 Appendix 1: Regional Lymph Node Stations for Staging Esophageal Cancer Locoregional (N stage) disease was redefined in the seventh edition of the AJCC Cancer Staging Manual as any periesophageal lymph
Appendix 1: Regional Lymph Node Stations for Staging Esophageal Cancer Locoregional (N stage) disease was redefined in the seventh edition of the AJCC Cancer Staging Manual as any periesophageal lymph
Lymph node metastasis is one of the most important prognostic
 ORIGINAL ARTICLE Comparison of Survival and Recurrence Pattern Between Two-Field and Three-Field Lymph Node Dissections for Upper Thoracic Esophageal Squamous Cell Carcinoma Young Mog Shim, MD, Hong Kwan
ORIGINAL ARTICLE Comparison of Survival and Recurrence Pattern Between Two-Field and Three-Field Lymph Node Dissections for Upper Thoracic Esophageal Squamous Cell Carcinoma Young Mog Shim, MD, Hong Kwan
9/18/2015. Disclosures. Objectives. Dysphagia Sherri Ekobena PA-C. I have no relevant financial interests to disclose I have no conflicts of interest
 Dysphagia Sherri Ekobena PA-C Disclosures I have no relevant financial interests to disclose I have no conflicts of interest Objectives Define what dysphagia is Define types of dysphagia Define studies
Dysphagia Sherri Ekobena PA-C Disclosures I have no relevant financial interests to disclose I have no conflicts of interest Objectives Define what dysphagia is Define types of dysphagia Define studies
North of Scotland Cancer Network Clinical Management Guideline for Non Small Cell Lung Cancer
 THIS DOCUMENT IS North of Scotland Cancer Network Clinical Management Guideline for Non Small Cell Lung Cancer [Based on WOSCAN NSCLC CMG with further extensive consultation within NOSCAN] UNCONTROLLED
THIS DOCUMENT IS North of Scotland Cancer Network Clinical Management Guideline for Non Small Cell Lung Cancer [Based on WOSCAN NSCLC CMG with further extensive consultation within NOSCAN] UNCONTROLLED
Esophageal Cancer Initially Thought to be Accompanied by a Solitary Metastasis to an Intrathoracic Paraaortic Lymph Node
 2012 66 5 417 421 Esophageal Cancer Initially Thought to be Accompanied by a Solitary Metastasis to an Intrathoracic Paraaortic Lymph Node a b* a a a a a a a b ʼ 418 Horio et al. Acta Med. Okayama Vol.
2012 66 5 417 421 Esophageal Cancer Initially Thought to be Accompanied by a Solitary Metastasis to an Intrathoracic Paraaortic Lymph Node a b* a a a a a a a b ʼ 418 Horio et al. Acta Med. Okayama Vol.
An Update: Lung Cancer
 An Update: Lung Cancer Andy Barlow Consultant in Respiratory Medicine Lead Clinician for Lung Cancer (West Herts Hospitals NHS Trust) Lead for EBUS-Harefield Hospital (RB&HFT) Summary Lung cancer epidemiology
An Update: Lung Cancer Andy Barlow Consultant in Respiratory Medicine Lead Clinician for Lung Cancer (West Herts Hospitals NHS Trust) Lead for EBUS-Harefield Hospital (RB&HFT) Summary Lung cancer epidemiology
Diagnosis and Surgical Outcomes for Primary Malignant Melanoma of the Esophagus: A Single-Center Experience
 Diagnosis and Surgical Outcomes for Primary Malignant Melanoma of the Esophagus: A Single-Center Experience Shaohua Wang, MD, Yuji Tachimori, MD, Nobukazu Hokamura, MD, Hiroyasu Igaki, MD, Takayoshi Kishino,
Diagnosis and Surgical Outcomes for Primary Malignant Melanoma of the Esophagus: A Single-Center Experience Shaohua Wang, MD, Yuji Tachimori, MD, Nobukazu Hokamura, MD, Hiroyasu Igaki, MD, Takayoshi Kishino,
Uniportal video-assisted thoracic surgery for esophageal cancer
 Surgical Technique on Esophageal Surgery Uniportal video-assisted thoracic surgery for esophageal cancer Hasan F. Batirel Thoracic Surgery Department, Marmara University Hospital, Istanbul, Turkey Correspondence
Surgical Technique on Esophageal Surgery Uniportal video-assisted thoracic surgery for esophageal cancer Hasan F. Batirel Thoracic Surgery Department, Marmara University Hospital, Istanbul, Turkey Correspondence
A Multidisciplinary Approach to Esophageal Dysphagia: Role of the SLP. Darlene Graner, M.A., CCC-SLP, BRS-S Sharon Burton, M.D.
 A Multidisciplinary Approach to Esophageal Dysphagia: Role of the SLP Darlene Graner, M.A., CCC-SLP, BRS-S Sharon Burton, M.D. What is the role of the SLP? Historically SLPs the preferred providers for
A Multidisciplinary Approach to Esophageal Dysphagia: Role of the SLP Darlene Graner, M.A., CCC-SLP, BRS-S Sharon Burton, M.D. What is the role of the SLP? Historically SLPs the preferred providers for
Index. Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type. A Adenocarcinoma, pancreatic ductal, laparoscopic distal pancreatectomy for, 61 Adrenal cortical carcinoma, laparoscopic adrenalectomy for, 114
Note: Page numbers of article titles are in boldface type. A Adenocarcinoma, pancreatic ductal, laparoscopic distal pancreatectomy for, 61 Adrenal cortical carcinoma, laparoscopic adrenalectomy for, 114
FINE NEEDLE ASPIRATION OF ENLARGED LYMPH NODE: Metastatic squamous cell carcinoma
 Case Scenario 1 HNP: A 70 year old white male presents with dysphagia. The patient is a current smoker, current user of alcohol and is HPV positive. A CT of the Neck showed mass in the left pyriform sinus.
Case Scenario 1 HNP: A 70 year old white male presents with dysphagia. The patient is a current smoker, current user of alcohol and is HPV positive. A CT of the Neck showed mass in the left pyriform sinus.
01/26/2010 GENERAL SURGERY ABSITE ANATOMY ANATOMY. Yvonne M. Carter, MD Georgetown University Medical Center. Layers. mucosa. squamous epithelium
 GENERAL SURGERY ABSITE REVIEW: ESOPHAGUS Yvonne M. Carter, MD Georgetown University Medical Center ANATOMY Layers mucosa muscle squamous epithelium columnar epithelium (distal 2cm) inner = circular outer
GENERAL SURGERY ABSITE REVIEW: ESOPHAGUS Yvonne M. Carter, MD Georgetown University Medical Center ANATOMY Layers mucosa muscle squamous epithelium columnar epithelium (distal 2cm) inner = circular outer
BRANDON REGIONAL HEALTH CENTER; WHIPPLE S PROCEDURE AND ESOPHAGECTOMY AUDIT
 BRANDON REGIONAL HEALTH CENTER; WHIPPLE S PROCEDURE AND ESOPHAGECTOMY AUDIT By: Amy Cisyk Home for the Summer Program July, 2016 Brandon, Manitoba Supervisor: Dr. Marvin Goossen Whipple s Procedure Audit
BRANDON REGIONAL HEALTH CENTER; WHIPPLE S PROCEDURE AND ESOPHAGECTOMY AUDIT By: Amy Cisyk Home for the Summer Program July, 2016 Brandon, Manitoba Supervisor: Dr. Marvin Goossen Whipple s Procedure Audit
Educational Objectives. Managing Lung Cancer From the Solitary Pulmonary Nodule to Complex Cases: A Multidisciplinary Approach.
 Managing Lung Cancer From the Solitary Pulmonary Nodule to Complex Cases: A Multidisciplinary Approach Robert A. Meguid, MD, MPH, FACS Assistant Professor of Cardiothoracic Surgery Surgical Director, Surgical
Managing Lung Cancer From the Solitary Pulmonary Nodule to Complex Cases: A Multidisciplinary Approach Robert A. Meguid, MD, MPH, FACS Assistant Professor of Cardiothoracic Surgery Surgical Director, Surgical
Hong Kong Society of Upper Gastrointestinal Surgeons CLINICAL MEETING 29 NOV 2012
 Hong Kong Society of Upper Gastrointestinal Surgeons CLINICAL MEETING 29 NOV 2012 Esophageal Leiomyoma Introduction Case presentation Operative video Discussion Esophageal Leiomyoma Benign tumors of the
Hong Kong Society of Upper Gastrointestinal Surgeons CLINICAL MEETING 29 NOV 2012 Esophageal Leiomyoma Introduction Case presentation Operative video Discussion Esophageal Leiomyoma Benign tumors of the
POSTOPERATIVE COMPLICATIONS OF TRANSTHORACIC ESOPHAGECTOMY FOR ESOPHAGEAL CARCINOMA
 International International Multidisciplinary Multidisciplinary e Journal/ e-journal Dr. A. Razaque Shaikh, Dr. Khenpal Das, Dr Shahida Khatoon ISSN 2277. (133-140) - 4262 POSTOPERATIVE COMPLICATIONS OF
International International Multidisciplinary Multidisciplinary e Journal/ e-journal Dr. A. Razaque Shaikh, Dr. Khenpal Das, Dr Shahida Khatoon ISSN 2277. (133-140) - 4262 POSTOPERATIVE COMPLICATIONS OF
Medicinae Doctoris. One university. Many futures.
 Medicinae Doctoris The Before and The After: Can chemotherapy revise the trajectory of gastric and esophageal cancers? Dr. David Dawe MD, FRCPC Medical Oncologist Assistant Professor Disclosures None All
Medicinae Doctoris The Before and The After: Can chemotherapy revise the trajectory of gastric and esophageal cancers? Dr. David Dawe MD, FRCPC Medical Oncologist Assistant Professor Disclosures None All
Case Scenario 1. Pathology: Specimen type: Incisional biopsy of the glottis Histology: Moderately differentiated squamous cell carcinoma
 Case Scenario 1 History A 52 year old male with a 20 pack year smoking history presented with about a 6 month history of persistent hoarseness. The patient had a squamous cell carcinoma of the lip removed
Case Scenario 1 History A 52 year old male with a 20 pack year smoking history presented with about a 6 month history of persistent hoarseness. The patient had a squamous cell carcinoma of the lip removed
Pancreas Case Scenario #1
 Pancreas Case Scenario #1 An 85 year old white female presented to her primary care physician with increasing abdominal pain. On 8/19 she had a CT scan of the abdomen and pelvis. This showed a 4.6 cm mass
Pancreas Case Scenario #1 An 85 year old white female presented to her primary care physician with increasing abdominal pain. On 8/19 she had a CT scan of the abdomen and pelvis. This showed a 4.6 cm mass
UNIVERSITY OF MEDICINE AND PHARMACY CRAIOVA DOCTORAL SCHOOL DOCTORAL THESIS THE ROLE OF NON-INVASIVE EXPLORATIONS IN THE
 UNIVERSITY OF MEDICINE AND PHARMACY CRAIOVA DOCTORAL SCHOOL DOCTORAL THESIS THE ROLE OF NON-INVASIVE EXPLORATIONS IN THE DIAGNOSIS AND STAGING OF ESOPHAGEAL CANCER THESIS COORDINATOR: Prof.univ.dr. Rogoveanu
UNIVERSITY OF MEDICINE AND PHARMACY CRAIOVA DOCTORAL SCHOOL DOCTORAL THESIS THE ROLE OF NON-INVASIVE EXPLORATIONS IN THE DIAGNOSIS AND STAGING OF ESOPHAGEAL CANCER THESIS COORDINATOR: Prof.univ.dr. Rogoveanu
Part II. A randomized trial
 77 Part II A randomized trial 78 79 Chapter 5 Preliminary experience of minimally invasive esophagectomy for cancer. Maas KW Biere SSAY Gisbertz SS van der Peet DL M.A. Cuesta Submitted 80 Chapter 5 ABSTRACT
77 Part II A randomized trial 78 79 Chapter 5 Preliminary experience of minimally invasive esophagectomy for cancer. Maas KW Biere SSAY Gisbertz SS van der Peet DL M.A. Cuesta Submitted 80 Chapter 5 ABSTRACT
Oesophagogastric Cancer The Patient s Pathway
 National helpline: 0121 704 9860 V1 Oesophagogastric Cancer The Patient s Pathway {Based on The St Thomas Hospital Pathway} Registered Charity No. 1062461 Contents Introduction 3-5 Curative pathway 5-7
National helpline: 0121 704 9860 V1 Oesophagogastric Cancer The Patient s Pathway {Based on The St Thomas Hospital Pathway} Registered Charity No. 1062461 Contents Introduction 3-5 Curative pathway 5-7
Esophageal Perforation
 Esophageal Perforation Dr. Carmine Simone Thoracic Surgeon, Division of General Surgery Head, Division of Critical Care May 15, 2006 Overview Case presentation Radiology Pre-operative management Operative
Esophageal Perforation Dr. Carmine Simone Thoracic Surgeon, Division of General Surgery Head, Division of Critical Care May 15, 2006 Overview Case presentation Radiology Pre-operative management Operative
Clinicopathologic and prognostic factors of young and elderly patients with esophageal adenocarcinoma: is there really a difference?
 Diseases of the Esophagus (2008) 21, 596 600 DOI: 10.1111/j.1442-2050.2008.00817.x Original article Clinicopathologic and prognostic factors of young and elderly patients with esophageal adenocarcinoma:
Diseases of the Esophagus (2008) 21, 596 600 DOI: 10.1111/j.1442-2050.2008.00817.x Original article Clinicopathologic and prognostic factors of young and elderly patients with esophageal adenocarcinoma:
Jejunostomy after oesophagectomy, how and why I do it
 Jejunostomy after oesophagectomy, how and why I do it Graeme Couper. Consultant Oesophago-gastric Surgeon, The Royal Infirmary of Edinburgh BAPEN Conference 2010 2nd & 3rd November Harrogate International
Jejunostomy after oesophagectomy, how and why I do it Graeme Couper. Consultant Oesophago-gastric Surgeon, The Royal Infirmary of Edinburgh BAPEN Conference 2010 2nd & 3rd November Harrogate International
Lymph node invasion might have more prognostic impact than R status in advanced esophageal adenocarcinoma
 The American Journal of Surgery (2013) 205, 711-717 Clinical Surgery Lymph node invasion might have more prognostic impact than R status in advanced esophageal adenocarcinoma Magali Cabau, M.D. a, Guillaume
The American Journal of Surgery (2013) 205, 711-717 Clinical Surgery Lymph node invasion might have more prognostic impact than R status in advanced esophageal adenocarcinoma Magali Cabau, M.D. a, Guillaume
Case Scenario 1 Worksheet. Primary Site C44.4 Morphology 8743/3 Laterality 0 Stage/ Prognostic Factors
 CASE SCENARIO 1 9/10/13 HISTORY: Patient is a 67-year-old white male and presents with lesion located 4-5cm above his right ear. The lesion has been present for years. No lymphadenopathy. 9/10/13 anterior
CASE SCENARIO 1 9/10/13 HISTORY: Patient is a 67-year-old white male and presents with lesion located 4-5cm above his right ear. The lesion has been present for years. No lymphadenopathy. 9/10/13 anterior
Newly Diagnosed Cases Cancer Related Death NCI 2006 Data
 Multi-Disciplinary Management of Esophageal Cancer: Surgical and Medical Steps Forward Alarming Thoracic Twin Towers 200000 150000 UCSF UCD Thoracic Oncology Conference November 21, 2009 100000 50000 0
Multi-Disciplinary Management of Esophageal Cancer: Surgical and Medical Steps Forward Alarming Thoracic Twin Towers 200000 150000 UCSF UCD Thoracic Oncology Conference November 21, 2009 100000 50000 0
THORACIC MALIGNANCIES
 THORACIC MALIGNANCIES Summary for Malignant Malignancies. Lung Ca 1 Lung Cancer Non-Small Cell Lung Cancer Diagnostic Evaluation for Non-Small Lung Cancer 1. History and Physical examination. 2. CBCDE,
THORACIC MALIGNANCIES Summary for Malignant Malignancies. Lung Ca 1 Lung Cancer Non-Small Cell Lung Cancer Diagnostic Evaluation for Non-Small Lung Cancer 1. History and Physical examination. 2. CBCDE,
Adam J. Hansen, MD UHC Thoracic Surgery
 Adam J. Hansen, MD UHC Thoracic Surgery Sometimes seen on Chest X-ray (CXR) Common incidental findings on computed tomography (CT) chest and abdomen done for other reasons Most lung cancers discovered
Adam J. Hansen, MD UHC Thoracic Surgery Sometimes seen on Chest X-ray (CXR) Common incidental findings on computed tomography (CT) chest and abdomen done for other reasons Most lung cancers discovered
OCCULT CERVICAL NODAL METASTASIS IN ESOPHAGEAL CANCER: PRELIMINARY RESULTS OF THREE-FIELD LYMPHADENECTOMY
 OCCULT CERVICAL NODAL METASTASIS IN ESOPHAGEAL CANCER: PRELIMINARY RESULTS OF THREE-FIELD LYMPHADENECTOMY Nasser K. Altorki, MD David B. Skinner, MD The extent of lymphadenectomy for carcinoma of the thoracic
OCCULT CERVICAL NODAL METASTASIS IN ESOPHAGEAL CANCER: PRELIMINARY RESULTS OF THREE-FIELD LYMPHADENECTOMY Nasser K. Altorki, MD David B. Skinner, MD The extent of lymphadenectomy for carcinoma of the thoracic
Lung. 10/24/13 Chest X-ray: 2.9 cm mass like density in the inferior lingular segment worrisome for neoplasm. Malignancy cannot be excluded.
 Lung Case Scenario 1 A 54 year white male presents with a recent abnormal CT of the chest. The patient has a history of melanoma, kidney, and prostate cancers. 10/24/13 Chest X-ray: 2.9 cm mass like density
Lung Case Scenario 1 A 54 year white male presents with a recent abnormal CT of the chest. The patient has a history of melanoma, kidney, and prostate cancers. 10/24/13 Chest X-ray: 2.9 cm mass like density
Physical Exam. Vitals stable on room air Abdomen soft, non-distented Normal external genitalia Patent anus No limb anomalies
 Case Presentation 1 day-old full-term baby girl noted to have drooling of saliva and increased secretions at birth Fetal US @32wks had shown polyhydramnios Birth weight 3515g Apgar 7@1min and 8@5min Unable
Case Presentation 1 day-old full-term baby girl noted to have drooling of saliva and increased secretions at birth Fetal US @32wks had shown polyhydramnios Birth weight 3515g Apgar 7@1min and 8@5min Unable
Adenocarcinoma of gastro-esophageal junction - Case report
 Case Report denocarcinoma of gastro-esophageal junction - Case report nupsingh Dhakre 1*, Ibethoi Yengkhom 2, Harshin Nagori 1, nup Kurele 1, Shreedevi. Patel 3 1 2 nd year Resident, 2 3rd year Resident,
Case Report denocarcinoma of gastro-esophageal junction - Case report nupsingh Dhakre 1*, Ibethoi Yengkhom 2, Harshin Nagori 1, nup Kurele 1, Shreedevi. Patel 3 1 2 nd year Resident, 2 3rd year Resident,
PLACE LABEL HERE. Radiation Therapy Oncology Group Phase II - SBRT - Medically Inoperable I /II NSCLC Follow-up Form. RTOG Study No.
 Radiation Therapy Oncology Group Phase II - SBRT - Medically Inoperable I /II NSCLC Follow-up Form RTOG Study No. 0813 Case # Name RTOG Patient ID INSTRUCTIONS: Submit this form at the appropriate followup
Radiation Therapy Oncology Group Phase II - SBRT - Medically Inoperable I /II NSCLC Follow-up Form RTOG Study No. 0813 Case # Name RTOG Patient ID INSTRUCTIONS: Submit this form at the appropriate followup
Boot Camp Case Scenarios
 Boot Camp Case Scenarios Case Scenario 1 Patient is a 69-year-old white female. She presents with dyspnea on exertion, cough, and right rib pain. Patient is a smoker. 9/21/12 CT Chest FINDINGS: There is
Boot Camp Case Scenarios Case Scenario 1 Patient is a 69-year-old white female. She presents with dyspnea on exertion, cough, and right rib pain. Patient is a smoker. 9/21/12 CT Chest FINDINGS: There is
Rescue for Complications After Esophagectomy The role of early diagnosis and intervention
 Rescue for Complications After Esophagectomy The role of early diagnosis and intervention Andrew C Chang, MD AATS/STS Postgraduate Symposium General Thoracic Surgery April 26, 2015 Disclosures Ethicon
Rescue for Complications After Esophagectomy The role of early diagnosis and intervention Andrew C Chang, MD AATS/STS Postgraduate Symposium General Thoracic Surgery April 26, 2015 Disclosures Ethicon
Preoperative Workup for Pulmonary Resection. Kristen Bridges, M.D. Richmond University Medical Center January 21, 2016
 Preoperative Workup for Pulmonary Resection Kristen Bridges, M.D. Richmond University Medical Center January 21, 2016 Patient Presentation 50 yo male with 70 pack year smoking history Large R hilar lung
Preoperative Workup for Pulmonary Resection Kristen Bridges, M.D. Richmond University Medical Center January 21, 2016 Patient Presentation 50 yo male with 70 pack year smoking history Large R hilar lung
Free Esophageal Perforation Following Hybrid Visceral Debranching and Distal Endograft Extension to Repair a Ruptured Thoracoabdominal Aortic
 Free Esophageal Perforation Following Hybrid Visceral Debranching and Distal Endograft Extension to Repair a Ruptured Thoracoabdominal Aortic Aneurysm History A 56-year-old gentleman, who had been referred
Free Esophageal Perforation Following Hybrid Visceral Debranching and Distal Endograft Extension to Repair a Ruptured Thoracoabdominal Aortic Aneurysm History A 56-year-old gentleman, who had been referred
Thoracic Surgery; An Overview
 Thoracic Surgery What we see Thoracic Surgery; An Overview James P. Locher, Jr, MD Methodist Cardiovascular and Thoracic Surgery Lung cancer Mets Fungus and TB Lung abcess and empyema Pleural based disease
Thoracic Surgery What we see Thoracic Surgery; An Overview James P. Locher, Jr, MD Methodist Cardiovascular and Thoracic Surgery Lung cancer Mets Fungus and TB Lung abcess and empyema Pleural based disease
Case Scenario #1 Larynx
 Case Scenario #1 Larynx 56 year old white female who presented with a 2 month history of hoarseness treated with antibiotics, but with no improvement. In the last 3 weeks, she has had a 15 lb weight loss,
Case Scenario #1 Larynx 56 year old white female who presented with a 2 month history of hoarseness treated with antibiotics, but with no improvement. In the last 3 weeks, she has had a 15 lb weight loss,
The incidence of adenocarcinoma of the esophagus
 GENERAL THORACIC A Retrospective Analysis of Locally Advanced Esophageal Cancer Patients Treated With Neoadjuvant Chemoradiation Therapy Followed by or Alone Kenneth A. Kesler, MD, Paul R. Helft, MD, Elizabeth
GENERAL THORACIC A Retrospective Analysis of Locally Advanced Esophageal Cancer Patients Treated With Neoadjuvant Chemoradiation Therapy Followed by or Alone Kenneth A. Kesler, MD, Paul R. Helft, MD, Elizabeth