An update on lipidology and cardiovascular risk management. Lipids, Metabolism & Vascular Risk Section - Royal Society of Medicine
|
|
|
- Benedict Byrd
- 5 years ago
- Views:
Transcription


 London, UK,")
1 An update on lipidology and cardiovascular risk management Lipids, Metabolism & Vascular Risk Section - Royal Society of Medicine National and international lipid modification guidelines: A critical appraisal Claudia STEFANUTTI (Rome, Italy, EU) London, UK, September 9, 6
2 Guidelines: why? The guidelines nowadays represent an evidence-based consensus The guidelines have been developed to support healthcare professionals communicating with individuals about their cardiovascular (CV) risk and the benefits of a healthy lifestyle and early modification of their CV risk In addition, the guidelines provide tools for healthcare professionals to promote population-based strategies and integrate these into international, national or regional prevention frameworks and to translate these in locally delivered healthcare services This is in line with the recommendations of the World Health Organization (WHO) global status report on non-communicable diseases.

3 Health impact pyramid. Alberico L. Catapano et al. Eur Heart J 6;eurheartj.ehw7 6 European Society of Cardiology and European Atherosclerosis Association. All rights reserved. For permissions please journals.permissions@oup.com.
4 Problems with Guidelines Institutional conflicts Inter-relationship between related diseases Commercial funding Personal conflicts Personal stakes Academic stakes Government conflicts Cost containment Priorities in healthcare Courtesy of Dr. Handrean Soran


5 The US guidelines for the treatment of dyslipidemia
6 Backframe
7 Similarities between the ACC/AHA Guidelines and the NLA Recommendations Lipid screening for primary prevention is recommended at -year intervals Lifestyle therapy is supported as first step in all treatment algorithms ASCVD (*) risk reduction is the goal of therapy Moderate- or high-intensity statin therapy is the central focus of pharmacotherapy Patient- MD (provider) discussion of risk/benefit ratio precedes all decisions on drug treatment Regular lipid and lipoprotein FU is necessary to assess adherence to therapy (*): Atherosclerotic Cardio- Vascular Disease

8 Evidence base ACC/AHA RCT(s) with ASCVD outcomes Meta-analyses of RCT NLA RCT(s) with ASCVD outcomes Meta-analyses of RCT Selected post-hoc analyses of RCT Observational epidemiologic studies Genetic studies Metabolic studies Mechanistic studies
9 Genetic Studies Genetic epidemiology reduces the likelihood of confounding by focusing on single variables: genetic mutations Identification of specific mutations may serve to generate hypotheses for other types of trials Often limited in patient selection and costly

10 Data Demonstrating Genetic Variants affecting ASCVD Risk Loss of function mutations in the gene encoding for PCSK9 are associated in Black subjects with 8% LDL-C reduction and 88% CHD relative risk reduction Loss of function mutations in the gene encoding for NPCL are associated with mg/dl reduction in LDL-C and a % CHD relative risk reduction Cohen JC, et al: Sequence variations in PCSK9, low LDL, and protection against coronary heart disease. N Engl J Med. 6 Mar ;():6-7. Myocardial Infarction Genetics Consortium Investigators: Inactivating mutations in NPCL and protection from coronary heart disease. N Engl J Med. Nov 7;7():7-8.
11 Risk Calculator ACC/AHA supports use of pooled Cohort risk calculator as initial step in non-hispanic white and African-American non-diabetics, age - 79, with no ASCVD and with LDL-C 7-89 mg/dl to assess statin benefit; consider using long-term risk assessment in -9 year-old individuals not in high-risk groups NLA recommends risk factors counting and assessment of other ASCVD risk indicators first, with optional use of any of risk calculators in patients with major risk factors to aid in clinical decision-making
12 ACC/AHA Guideline Additional Markers of Increased ASCVD Risk Consider for additional measurement of ASCVD risk in patients who do not fall into one of the statin benefit groups (-7.% year risk) LDL-C 6mg/dL Family history of premature ASCVD CAC score Agatston units or 7%th-ile Hs-CRP mg/l Ankle-brachial index <.9 High lifetime -9
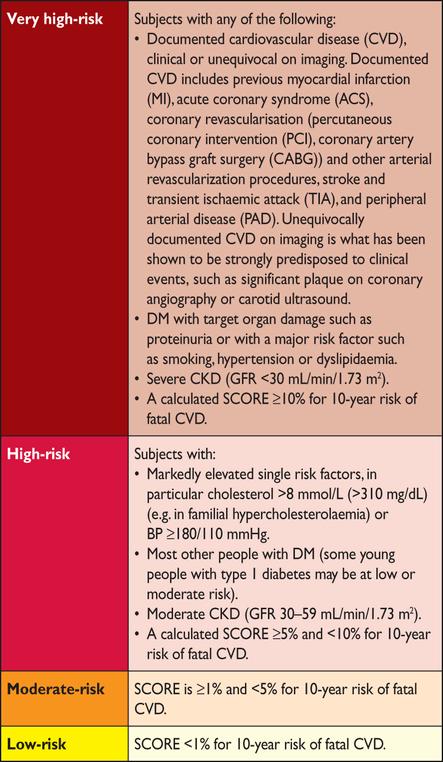
13 European Heart Journal (), SCORE chart: year risk of fatal cardiovascular disease (CVD) in populations at low CVD risk % and over %-% %-9% %-% % % < % SCORE -year risk of fatal CVD in populations at Low CVD risk Non-smoker Smoker Women Systolic blood pressure (mmhg) Cholesterol (mmol/l) Age 6 6 Non-smoker Smoker Men mg/dl Note: the SCORE chart is for use in people without overt CVD, diabetes, chronic kidney disease, or very high levels of individual risk factors because such people are ALREADY at HIGH RISK and need INTENSIVE RISK FACTOR ADVICE
14 ACC/AHA Statin Benefit Groups H: High intensity statin M: Moderate intensity statin Clinically ASCVD (H preferred; M if age > 7 or if not candidate for H Primary elevations of LDL-C 9 mg/dl (H preferred; M if not candidate for H) Age -7 years with diabetes, and LDL-C 7-89 mg/dl, no clinical ASCVD (M if -year risk < 7.%; H if 7.%) Age -7 years, no clinical ASCVD or diabetes, LDL-C 7-89 mg/dl, and estimated -year ASCVD risk 7.% using Pooled Cohort Equations (M or H)
15 High- and Moderate-Intensity Daily Statin Therapy High intensity (Lowers Moderate Intensity (Lowers LDL-C %) LDL-C -%) Atorvastatin -8 mg Rosuvastatin - mg Bold= Tested in RCT and reviewed by Expert Panel Yellow= Not tested in RCT s reviewed by Expert Panel Atorvastatin () mg Fluvastatin XL 8 mg Fluvastatin mg x/day Lovastatin mg Pitavastatin - mg Pravastatin (8) mg Rosuvastatin () mg Simvastatin - mg Simvastatin 8 mg* *Although simvastatin 8 mg was evaluated in RCTs, initiation of simvastatin 8 mg or titration to 8 mg is not recommended by the FDA due to the increased risk of myopathy, including rhabdomyolysis

16 ACC/AHA Perspective on Statin Therapy Statin intensity trial showed clear benefit of high-intensity vs moderate intensity statins Because fixed doses, no dosage titrations, were employed, one should not assume that a dosage titration strategy is correct or that addition of non-statins to achieve low LDL-C is indicated ACC/AHA Perspective on Non-statin Lipid Drug Therapy Non-statin therapies, as compared to statin therapy, do not provide acceptable ASCVD risk reduction benefits relative to their potential for adverse effects in the routine prevention of ASCVD Niacin in AIM-HIGH and HPS- THRIVE Fibrates in ACCORD-Lipids and FIELD
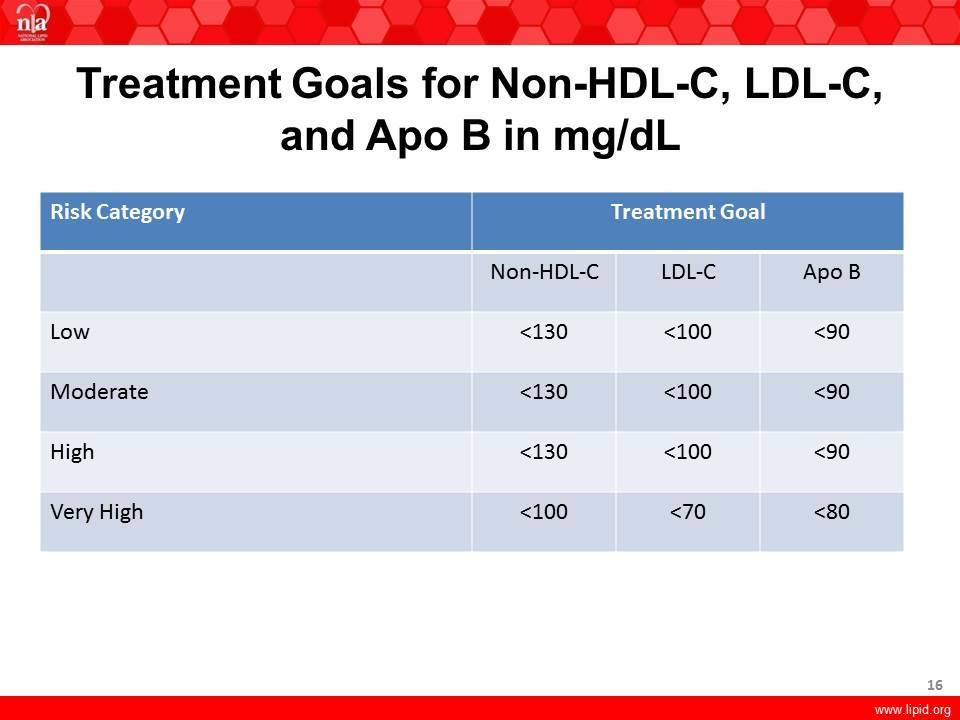
17 Overview of the NLA Recommendations. All preventive therapy begins with risk assessment and a provider (Specialist MD is supposed!)-patient discussion of the pros and cons of therapy. Life-style therapy is the first step in all ASCVD preventive recommendations, regardless of baseline risk. Judicious use of evidence-based drug therapy, particularly M- and H-dose statins, is associated with optimal ASCVD risk reduction. When excessive circulating atherogenic cholesterol (non-hdl-c [primary target] and LDL-C) persists after appropriate lifestyle and statin therapy, the use of non-statin therapy should be considered. Long-term follow-up fostered by provider -patient communication is essential for optimal ASCVD prevention

:7-88.")
18 What is the advantage of Non-HDL-C over LDL-C in Assessing ASCVD RISK? Non-HDL-C is more predictive of ASCVD risk than LDL-C in observational studies. The same is true for on-treatment levels in clinical trials of statin therapy When Non-HDL-C and LDL-C are discordant, risk follows Non-HDL-C Non-HDL-C testing is universally available, requires no additional cost, and accurate values may be obtained in the non-fasting state Boekholdt SM, et al: Lipid-related markers and cardiovascular disease prediction. JAMA. Jun ;7():99-6. Jacobson TA, et al: National Lipid Association recommendations for patient-centered management of dyslipidemia: part - executive summary. J Clin Lipidol. Sep-Oct;8():7-88. Robinson JG, Wang S, Smith BJ, Jacobson TA. Meta-analysis of the relationship between non-high-density lipoprotein cholesterol reduction and coronary heart disease risk. J Am Coll Cardiol. 9 Jan 7;():6-.
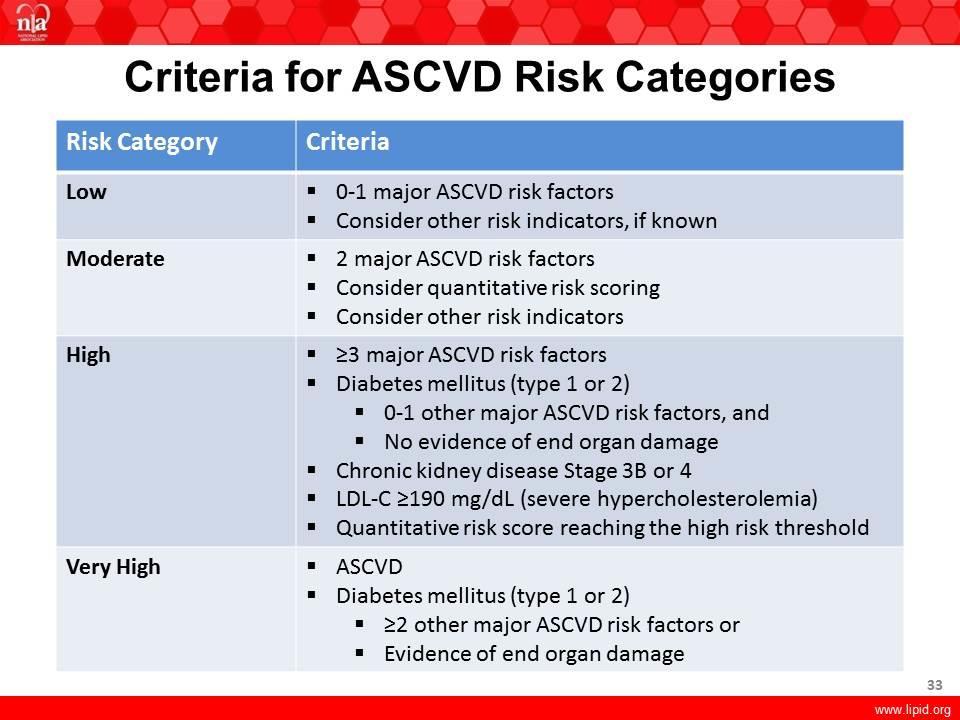
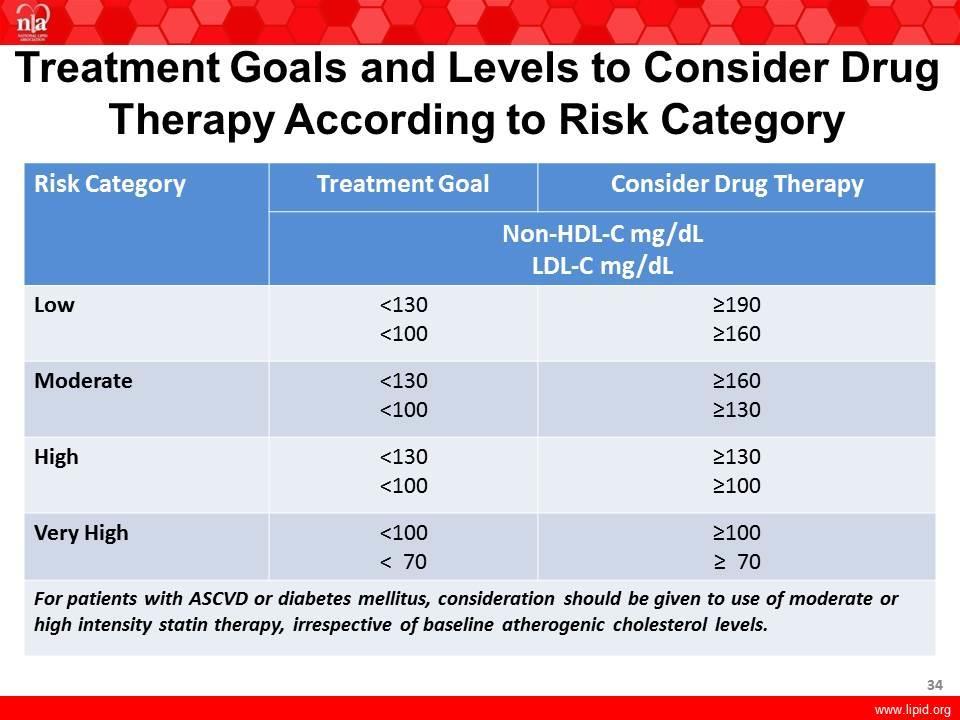
19 NLA Recommendations: Stepwise Approach to Risk Assessment. Identify the highest ASCVD risk category that applies to the patient. If very high risk, begin with moderate- or high-intensity statin with non- HDL-C and LDL-C goals < and < 7 mg/dl, respectively. In remaining patients count number of major risk factors and treat to goals for non-hdl-c < and LDL-C < mg/dl, respectively Further Risk Assessment in Patients with Two Major Risk Factors Key Clinical Criteria: multipack/day cigarette smoking; strong family history of premature CHD; non-hdl-c > 9 mg/dl or LDL-C > 6 mg/dl High Risk Quantitative Scoring: -year FRS %; ACC/AHA -year risk %; lifetime risk % High Risk Biomarkers: CAC score Agatston units or 7th%-ile; hscrp. mg/l; Lp(a) mg/dl (protein; isoform insensitive assay); or urine albumine/creatinine ratio mg/g
20 Joint British Societies- non-hdl-c (TC minus HDL-c=non-HDL-c) to replace LDL-C professional lifestyle support to improve lipid profiles. Cholesterol lowering drug therapy is recommended in: Patients with established CVD Individuals at high risk of CVD: diabetes age > years, patients with CKD stages, or FH Individuals with high -year CVD risk (defined by NICE guidance) Individuals with high lifetime CVD risk estimated from heart age and other JBS calculator metrics, in whom lifestyle changes alone are considered insufficient JBS- board; Heart ; ii : -67 Courtesy of Dr. Handrean Soran
21
22
23
24 Recommendations for treatment targets for LDL-C Recommendations Class Level In patients at VERY HIGH CV risk (established CVD, type diabetes, type diabetes with target organ damage, moderate to severe CKD or a SCORE level %) the LDL-C goal is <.8 mmol/l (less than ~ 7 mg/dl) and/or % LDL-C reduction when target level cannot be reached. I A In patients at HIGH CV risk (markedly elevated single risk factors, a SCORE level to < %) an LDL-C goal <. mmol/l (less than ~ mg/dl) should be considered. IIa A In subjects at MODERATE risk (SCORE level > to %) an LDL-C goal <. mmol/l (less than ~ mg/dl) should be considered. IIa C European Heart Journal (),
25


26 Intervention strategies as a function of total CV risk and LDL-C level Total CV risk (SCORE) % < 7 mg/dl <.8 mmol/l 7 to < mg/dl.8 to <. mmol/l LDL-C levels to < mg/dl. to <. mmol/l to < 9 mg/dl. to <.9 mmol/l < No lipid intervention No lipid intervention Lifestyle intervention Lifestyle intervention > 9 mg/dl >.9 mmol/l Lifestyle intervention, consider drug if uncontrolled Class/Level I/C I/C I/C I/C IIa/A to < Lifestyle intervention Lifestyle intervention Lifestyle intervention, consider drug if uncontrolled Lifestyle intervention, consider drug if uncontrolled Lifestyle intervention, consider drug if uncontrolled Class/Level I/C I/C IIa/A IIa/A I/A > to <, or high risk Lifestyle intervention consider drug* Lifestyle intervention consider drug* Lifestyle intervention and immediate drug intervention Lifestyle intervention and immediate drug intervention Lifestyle intervention and immediate drug intervention Class/Level IIa/A IIa/A IIa/A I/A I/A or very high risk Lifestyle intervention consider drug* Lifestyle intervention and immediate drug intervention Lifestyle intervention and immediate drug intervention Lifestyle intervention and immediate drug intervention Lifestyle intervention and immediate drug intervention Class/Level IIa/A IIa/A I/A I/A I/A European Heart Journal (),
27
28

29 NLA Perspective on Statin Therapy Statin therapy is the most potent and evidence-based approach to lowering non-hdl-c and LDL-C and reduces ASCVD events Statin intensity trial showed clear benefit for high-intensity vs moderate-intensity statins Broad-based evidence supports «lower is better» concept. Clinicians should address residual risk by appropriately-dosed statin therapy
30 Efficacy of Intensive Lowering LDL-C in Subjects with Low Baseline LDL-C Meta-analysis of RCT of > participants and years treatment duration or more vs less intense statin trials involving 69,8 subjects The major vascular event (MVE) reduction, among in those with baseline LDL-C < 77 mg/dl per further 9 mg/dl reduction was 9%; in those with baseline LDL-C < 7 mg/dl, similar reduction in LDL-C continued to demonstrate MVE reduction Cholesterol Treatment Trialists (CTT) Collaboration: Efficacy and safety of more intensive lowering of LDL cholesterol: a meta-analysis of data from 7, participants in 6 randomised trials. Lancet. Nov ;76(97):67-8.
31 Joint British Societies- Statins are recommended They are highly effective at reducing CVD events Benefit to LDL-c levels < mmol/l so intensive non-hdl- C lowering required. Statins are safe There is a small increase in risk of developing diabetes The benefits of cholesterol lowering greatly exceed any risk associated with diabetes. If statin intolerance develops use a stepwise strategy switch agents and re-challenge dosing. Low HDL-C values contributes to CVD risk, Drug therapy to raise HDL-c no effect on CVD risk Drug therapy for HDL-C is not currently indicated. JBS- board; Heart ; ii : -67 Courtesy of Dr. Handrean Soran
32 NLA Perspective on Non-Statin Lipid Drug Therapy If non-hdl-c and LDL-C goals are not achieved with statin therapy, the addition of evidence-based non-statin therapy should be considered to lower atherogenic cholesterol level and to achieve goals Ezetimibe is a safe, evidence-based non-statin therapy that may be considered in post MI patients and selected other patients with elevated non-hdl-c and/or LDL-C Resins or Niacin can be considered in selected patients Meta-analyses of Fibrate therapy in subgroups with atherogenic dyslipidemia suggest ASCVD risk reduction
33

34
35
36 Central Focus of Guidelines: Summary ACC/AHA define statin benefit groups; risk-benefit discussion; use moderate- or high-intensity statin therapy with life-style change as background therapy; generally avoid non-statin drug therapy; no lipid goals NLA identify ASCVD risk level; risk-benefit discussion; emphasize healthy life-style; use moderate- or high-intensity statin therapy, and under appropriate circumstances, adjunctive non-statin therapy, to lower atherogenic cholesterol; maintain lipid goals (non-hdl-c is favored lipoprotein lipid target)



37 The differences Evidence base Central focus Lipid and lipoprotein goals Non-statin therapies Risk estimation (calculator) ACC/AHA NLA
38 TAKE HOME MESSAGE Major advances have been made in the clinical management of LDL-C. Many RCTs in the past decades have shown that LDL-C lowering therapy reduces the risk for ASCVD Despite advances made on different international guidelines and clinical recommendations, the real world management remains far from what is recommended in these guidelines, in terms of best practice for both lifestyle and drug intervention In addition, significant ASCVD risk persists despite the use of current lipid lowering standard of care, like the available therapies and treatment targets for patients at high ASCVD risk, HeFH, HoFH, statin intolerant patients, as well as HyperLp(a)lipoproteinaemic subjects (Isolated and Combined forms) Use careful clinical judgement when treat dyslipidaemia and/or any metabolic disorder predictive of ASCVD risk
Dyslipidemia in the light of Current Guidelines - Do we change our Practice?
 Dyslipidemia in the light of Current Guidelines - Do we change our Practice? Dato Dr. David Chew Soon Ping Senior Consultant Cardiologist Institut Jantung Negara Atherosclerotic Cardiovascular Disease
Dyslipidemia in the light of Current Guidelines - Do we change our Practice? Dato Dr. David Chew Soon Ping Senior Consultant Cardiologist Institut Jantung Negara Atherosclerotic Cardiovascular Disease
New Guidelines in Dyslipidemia Management
 The Fourth IAS-OSLA Course on Lipid Metabolism and Cardiovascular Risk Muscat, Oman, February 2018 New Guidelines in Dyslipidemia Management Dr. Khalid Al-Waili, MD, FRCPC, DABCL Senior Consultant Medical
The Fourth IAS-OSLA Course on Lipid Metabolism and Cardiovascular Risk Muscat, Oman, February 2018 New Guidelines in Dyslipidemia Management Dr. Khalid Al-Waili, MD, FRCPC, DABCL Senior Consultant Medical
New Guidelines in Dyslipidemia Management
 The Third IAS-OSLA Course on Lipid Metabolism and Cardiovascular Risk Muscat, Oman, February 2017 New Guidelines in Dyslipidemia Management Dr. Khalid Al-Waili, MD, FRCPC, DABCL Senior Consultant Medical
The Third IAS-OSLA Course on Lipid Metabolism and Cardiovascular Risk Muscat, Oman, February 2017 New Guidelines in Dyslipidemia Management Dr. Khalid Al-Waili, MD, FRCPC, DABCL Senior Consultant Medical
What do the guidelines say about combination therapy?
 What do the guidelines say about combination therapy? Christie M. Ballantyne, MD Center for Cardiovascular Disease Prevention Methodist DeBakey Heart & Vascular Center Baylor College of Medicine Houston,
What do the guidelines say about combination therapy? Christie M. Ballantyne, MD Center for Cardiovascular Disease Prevention Methodist DeBakey Heart & Vascular Center Baylor College of Medicine Houston,
HYPERLIPIDEMIA IN THE OLDER POPULATION NICOLE SLATER, PHARMD, BCACP AUBURN UNIVERSITY, HARRISON SCHOOL OF PHARMACY JULY 16, 2016
 HYPERLIPIDEMIA IN THE OLDER POPULATION NICOLE SLATER, PHARMD, BCACP AUBURN UNIVERSITY, HARRISON SCHOOL OF PHARMACY JULY 16, 2016 NOTHING TO DISCLOSE I, Nicole Slater, have no actual or potential conflict
HYPERLIPIDEMIA IN THE OLDER POPULATION NICOLE SLATER, PHARMD, BCACP AUBURN UNIVERSITY, HARRISON SCHOOL OF PHARMACY JULY 16, 2016 NOTHING TO DISCLOSE I, Nicole Slater, have no actual or potential conflict
Dyslipidemia and Combination Therapy: A Framework for Clinical Decision Making
 Dyslipidemia and Combination Therapy: A Framework for Clinical Decision Making Shashank Sinha, MD Pamela B. Morris, MD, FACC 8 October 2016 Mexico City Introduction: Pamela B. Morris, MD, FACC COMING TO
Dyslipidemia and Combination Therapy: A Framework for Clinical Decision Making Shashank Sinha, MD Pamela B. Morris, MD, FACC 8 October 2016 Mexico City Introduction: Pamela B. Morris, MD, FACC COMING TO
A Systemic Approach to Lipid Management Making Sense of the Fatty Debate
 A Systemic Approach to Lipid Management Making Sense of the Fatty Debate M Ranu Muttreja MD Aria Jefferson Health October 8, 2017 Historical Perspective Lipid Hypothesis Early 1900 s Anitschkow fed rabbits
A Systemic Approach to Lipid Management Making Sense of the Fatty Debate M Ranu Muttreja MD Aria Jefferson Health October 8, 2017 Historical Perspective Lipid Hypothesis Early 1900 s Anitschkow fed rabbits
Managing Dyslipidemia and ASCVD Risk: Confusion, Controversy Consensus
 Managing Dyslipidemia and ASCVD Risk: Confusion, Controversy Consensus Pamela B. Morris, MD, FACC, FAHA, FASPC, FNLA Chair, ACC Prevention of Cardiovascular Disease Council and Section The Medical University
Managing Dyslipidemia and ASCVD Risk: Confusion, Controversy Consensus Pamela B. Morris, MD, FACC, FAHA, FASPC, FNLA Chair, ACC Prevention of Cardiovascular Disease Council and Section The Medical University
2/10/2016. Patient-Centered Management of Dyslipidemia. No disclosures. What is Patient-Centered Management?
 Patient-Centered Management of Dyslipidemia Carl E. Orringer, MD, FACC, FNLA Associate Professor of Medicine University of Miami Miller School of Medicine President, National Lipid Association 1 No disclosures
Patient-Centered Management of Dyslipidemia Carl E. Orringer, MD, FACC, FNLA Associate Professor of Medicine University of Miami Miller School of Medicine President, National Lipid Association 1 No disclosures
Considerations and Controversies in the Management of Dyslipidemia for ASCVD Risk Reduction
 Considerations and Controversies in the Management of Dyslipidemia for ASCVD Risk Reduction Pamela B. Morris, MD, FACC, FAHA, FASCP, FNLA Chair, ACC Prevention of Cardiovascular Disease Council The Medical
Considerations and Controversies in the Management of Dyslipidemia for ASCVD Risk Reduction Pamela B. Morris, MD, FACC, FAHA, FASCP, FNLA Chair, ACC Prevention of Cardiovascular Disease Council The Medical
Nicole Ciffone, MS, ANP-C, AACC Clinical Lipid Specialist
 1 Nicole Ciffone, MS, ANP-C, AACC Clinical Lipid Specialist New Cardiovascular Horizons Multidisciplinary Strategies for Optimal Cardiovascular Care February 7, 2015 2 Objectives After participating in
1 Nicole Ciffone, MS, ANP-C, AACC Clinical Lipid Specialist New Cardiovascular Horizons Multidisciplinary Strategies for Optimal Cardiovascular Care February 7, 2015 2 Objectives After participating in
Review of guidelines for management of dyslipidemia in diabetic patients
 2012 international Conference on Diabetes and metabolism (ICDM) Review of guidelines for management of dyslipidemia in diabetic patients Nan Hee Kim, MD, PhD Department of Internal Medicine, Korea University
2012 international Conference on Diabetes and metabolism (ICDM) Review of guidelines for management of dyslipidemia in diabetic patients Nan Hee Kim, MD, PhD Department of Internal Medicine, Korea University
David Y. Gaitonde, MD, FACP Endocrinology DDEAMC, Fort Gordon
 David Y. Gaitonde, MD, FACP Endocrinology DDEAMC, Fort Gordon I have no actual or potential conflicts of interest in relation to this program or presentation. Raphael School of Athens, 1509-1511 Apply
David Y. Gaitonde, MD, FACP Endocrinology DDEAMC, Fort Gordon I have no actual or potential conflicts of interest in relation to this program or presentation. Raphael School of Athens, 1509-1511 Apply
Lipid Panel Management Refresher Course for the Family Physician
 Lipid Panel Management Refresher Course for the Family Physician Objectives Understand the evidence that was evaluated to develop the 2013 ACC/AHA guidelines Discuss the utility and accuracy of the new
Lipid Panel Management Refresher Course for the Family Physician Objectives Understand the evidence that was evaluated to develop the 2013 ACC/AHA guidelines Discuss the utility and accuracy of the new
No relevant financial relationships
 MANAGEMENT OF LIPID DISORDERS Balancing Benefits and harms Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial relationships baron@medicine.ucsf.edu
MANAGEMENT OF LIPID DISORDERS Balancing Benefits and harms Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial relationships baron@medicine.ucsf.edu
Confusion about guidelines: How should we treat lipids?
 Confusion about guidelines: How should we treat lipids? Anne Carol Goldberg, MD, FACP, FAHA, FNLA Professor of Medicine Washington University School of Medicine American College of Physicians Missouri
Confusion about guidelines: How should we treat lipids? Anne Carol Goldberg, MD, FACP, FAHA, FNLA Professor of Medicine Washington University School of Medicine American College of Physicians Missouri
Update on Lipid Management in Cardiovascular Disease: How to Understand and Implement the New ACC/AHA Guidelines
 Update on Lipid Management in Cardiovascular Disease: How to Understand and Implement the New ACC/AHA Guidelines Paul Mahoney, MD Sentara Cardiology Specialists Lipid Management in Cardiovascular Disease
Update on Lipid Management in Cardiovascular Disease: How to Understand and Implement the New ACC/AHA Guidelines Paul Mahoney, MD Sentara Cardiology Specialists Lipid Management in Cardiovascular Disease
THE ESC/EAS LIPID GUIDELINES IN THE ELDERLY
 THE ESC/EAS LIPID GUIDELINES IN THE ELDERLY Alberico L. Catapano alberico.catapano@unimi.it Alberico L. Catapano Potential Conflict Of Interest Prof. Catapano has received honoraria, lecture fees, or research
THE ESC/EAS LIPID GUIDELINES IN THE ELDERLY Alberico L. Catapano alberico.catapano@unimi.it Alberico L. Catapano Potential Conflict Of Interest Prof. Catapano has received honoraria, lecture fees, or research
Disclosure. No relevant financial relationships. Placebo-Controlled Statin Trials
 MANAGEMENT OF HYPERLIPIDEMIA AND CARDIOVASCULAR RISK IN WOMEN: Balancing Benefits and Harms Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial
MANAGEMENT OF HYPERLIPIDEMIA AND CARDIOVASCULAR RISK IN WOMEN: Balancing Benefits and Harms Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial
2013 ACC AHA LIPID GUIDELINE JAY S. FONTE, MD
 2013 ACC AHA LIPID GUIDELINE JAY S. FONTE, MD How do you interpret my blood test results? What are our targets for these tests? Before the ACC/AHA Lipid Guidelines A1c:
2013 ACC AHA LIPID GUIDELINE JAY S. FONTE, MD How do you interpret my blood test results? What are our targets for these tests? Before the ACC/AHA Lipid Guidelines A1c:
No relevant financial relationships
 MANAGEMENT OF LIPID DISORDERS: WHERE DO WE STAND WITH THE NEW PRACTICE GUIDELINES? Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Disclosure No relevant financial relationships
MANAGEMENT OF LIPID DISORDERS: WHERE DO WE STAND WITH THE NEW PRACTICE GUIDELINES? Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Disclosure No relevant financial relationships
Cholesterol Management Roy Gandolfi, MD
 Cholesterol Management 2017 Roy Gandolfi, MD Goals Interpreting cholesterol guidelines Cholesterol treatment in diabetics Statin use and side effects therapy Reporting- Comparison data among physicians
Cholesterol Management 2017 Roy Gandolfi, MD Goals Interpreting cholesterol guidelines Cholesterol treatment in diabetics Statin use and side effects therapy Reporting- Comparison data among physicians
Observations on US CVD Prevention Guidelines. Donald M. Lloyd-Jones, MD ScM FACC FAHA
 Observations on US CVD Prevention Guidelines Donald M. Lloyd-Jones, MD ScM FACC FAHA What are Guidelines? Evidence Base for Guidelines Tricoci, JAMA 2009 Evidence Base for Guidelines Tricoci, JAMA 2009
Observations on US CVD Prevention Guidelines Donald M. Lloyd-Jones, MD ScM FACC FAHA What are Guidelines? Evidence Base for Guidelines Tricoci, JAMA 2009 Evidence Base for Guidelines Tricoci, JAMA 2009
Learning Objectives. Patient Case
 Joseph Saseen, Pharm.D., FASHP, FCCP, BCPS Professor and Vice Chair, Department of Clinical Pharmacy University of Colorado Anschutz Medical Campus Learning Objectives Identify the 4 patient populations
Joseph Saseen, Pharm.D., FASHP, FCCP, BCPS Professor and Vice Chair, Department of Clinical Pharmacy University of Colorado Anschutz Medical Campus Learning Objectives Identify the 4 patient populations
Introduction. Objective. Critical Questions Addressed
 Introduction Objective To provide a strong evidence-based foundation for the treatment of cholesterol for the primary and secondary prevention of ASCVD in women and men Critical Questions Addressed CQ1:
Introduction Objective To provide a strong evidence-based foundation for the treatment of cholesterol for the primary and secondary prevention of ASCVD in women and men Critical Questions Addressed CQ1:
2013 Cholesterol Guidelines. Anna Broz MSN, RN, CNP, AACC Adult Certified Nurse Practitioner North Ohio Heart, Inc.
 2013 Cholesterol Guidelines Anna Broz MSN, RN, CNP, AACC Adult Certified Nurse Practitioner North Ohio Heart, Inc. Disclosures Speaker Gilead Sciences NHLBI Charge to the Expert Panel Evaluate higher quality
2013 Cholesterol Guidelines Anna Broz MSN, RN, CNP, AACC Adult Certified Nurse Practitioner North Ohio Heart, Inc. Disclosures Speaker Gilead Sciences NHLBI Charge to the Expert Panel Evaluate higher quality
Latest Guidelines for Lipid Management
 Latest Guidelines for Lipid Management Goals Recognize the differences between different guidelines Understand the effective strategies to tailor lipid lowering therapies based on evidence and guideline
Latest Guidelines for Lipid Management Goals Recognize the differences between different guidelines Understand the effective strategies to tailor lipid lowering therapies based on evidence and guideline
LDL How Low can (should) you Go and be Safe
 you Go and be Safe") LDL How Low can (should) you Go and be Safe Edward Shahady MD, FAAFP, ABCL Clinical Professor Family Medicine Medical Director Diabetes Master Clinician Program Definition of Low LDL National Health and
LDL How Low can (should) you Go and be Safe Edward Shahady MD, FAAFP, ABCL Clinical Professor Family Medicine Medical Director Diabetes Master Clinician Program Definition of Low LDL National Health and
Lipid Management 2013 Statin Benefit Groups
 Clinical Integration Steering Committee Clinical Integration Chronic Disease Management Work Group Lipid Management 2013 Statin Benefit Groups Approved by Board Chair Signature Name (Please Print) Date
Clinical Integration Steering Committee Clinical Integration Chronic Disease Management Work Group Lipid Management 2013 Statin Benefit Groups Approved by Board Chair Signature Name (Please Print) Date
Lipid Management C. Samuel Ledford, MD Interventional Cardiology Chattanooga Heart Institute
 Lipid Management 2018 C. Samuel Ledford, MD Interventional Cardiology Chattanooga Heart Institute Disclosures No Financial Disclosures Disclosures I am an Interventional Cardiologist I put STENTS in for
Lipid Management 2018 C. Samuel Ledford, MD Interventional Cardiology Chattanooga Heart Institute Disclosures No Financial Disclosures Disclosures I am an Interventional Cardiologist I put STENTS in for
Prevention of Heart Disease: The New Guidelines
 Prevention of Heart Disease: The New Guidelines Nisha I. Parikh MD MPH Assistant Professor of Medicine Division of Cardiology Department of Medicine University of California San Francisco May 18 th 2015
Prevention of Heart Disease: The New Guidelines Nisha I. Parikh MD MPH Assistant Professor of Medicine Division of Cardiology Department of Medicine University of California San Francisco May 18 th 2015
Acute Coronary Syndromes (ACS)
") Sally A. Arif, Pharm.D., BCPS (AQ Cardiology) Assistant Professor of Pharmacy Practice Midwestern University, Chicago College of Pharmacy Cardiology Clinical Specialist, Rush University Medical Center
Sally A. Arif, Pharm.D., BCPS (AQ Cardiology) Assistant Professor of Pharmacy Practice Midwestern University, Chicago College of Pharmacy Cardiology Clinical Specialist, Rush University Medical Center
New Cholesterol Guidelines What the LDL are we supposed to do now?!
 New Cholesterol Guidelines What the LDL are we supposed to do now?! Michael D. Shapiro Assistant Professor of Medicine and Radiology Knight Cardiovascular Institute Oregon Health & Science University 2013
New Cholesterol Guidelines What the LDL are we supposed to do now?! Michael D. Shapiro Assistant Professor of Medicine and Radiology Knight Cardiovascular Institute Oregon Health & Science University 2013
Prevention Updates and Paradigm Shifts
 Prevention Updates and Paradigm Shifts Andrew Freeman, MD, FACC Director of Clinical Cardiology and Operations National Jewish Health Assistant Professor of Medicine National Jewish Health and University
Prevention Updates and Paradigm Shifts Andrew Freeman, MD, FACC Director of Clinical Cardiology and Operations National Jewish Health Assistant Professor of Medicine National Jewish Health and University
Disclosures No relationships (not even to an employer) No off-label uses. Cholesterol Lowering Guidelines: What now?
 No off-label uses. Cholesterol Lowering Guidelines: What now?") Disclosures No relationships (not even to an employer) No off-label uses Cholesterol Lowering Guidelines: What now?, FACP 1 2 65-year-old white woman Total cholesterol 175mg/dL HDL 54 mg/dl LDL 96 mg/dl
Disclosures No relationships (not even to an employer) No off-label uses Cholesterol Lowering Guidelines: What now?, FACP 1 2 65-year-old white woman Total cholesterol 175mg/dL HDL 54 mg/dl LDL 96 mg/dl
Lipid Management: The Next Level How Will the New ACC/AHA Guidelines Change My Practice
 Lipid Management: The Next Level How Will the New ACC/AHA Guidelines Change My Practice Vera Bittner, MD, MSPH Professor of Medicine Section Head, Preventive Cardiology Medical Director, Cardiac Rehabilitation
Lipid Management: The Next Level How Will the New ACC/AHA Guidelines Change My Practice Vera Bittner, MD, MSPH Professor of Medicine Section Head, Preventive Cardiology Medical Director, Cardiac Rehabilitation
Disclosures. Prevention of Heart Disease: The New Guidelines. Summary of Talk. Four guidelines. No relevant disclosures.
 Disclosures Prevention of Heart Disease: The New Guidelines No relevant disclosures Nisha I. Parikh MD MPH Assistant Professor of Medicine Division of Cardiology Department of Medicine University of California
Disclosures Prevention of Heart Disease: The New Guidelines No relevant disclosures Nisha I. Parikh MD MPH Assistant Professor of Medicine Division of Cardiology Department of Medicine University of California
What have We Learned in Dyslipidemia Management Since the Publication of the 2013 ACC/AHA Guideline?
 What have We Learned in Dyslipidemia Management Since the Publication of the 2013 ACC/AHA Guideline? Salim S. Virani, MD, PhD, FACC, FAHA Associate Professor, Section of Cardiovascular Research Baylor
What have We Learned in Dyslipidemia Management Since the Publication of the 2013 ACC/AHA Guideline? Salim S. Virani, MD, PhD, FACC, FAHA Associate Professor, Section of Cardiovascular Research Baylor
Conflict of Interest Disclosure. Learning Objectives. Learning Objectives. Guidelines. Update on Lifestyle Guidelines
 Conflict of Interest Disclosure Updates for the Ambulatory Care Pharmacist: Dyslipidemia and CV Risk Assessment No conflicts of interest to disclose 2014 Updates to the Updates in Ambulatory Care Pharmacy
Conflict of Interest Disclosure Updates for the Ambulatory Care Pharmacist: Dyslipidemia and CV Risk Assessment No conflicts of interest to disclose 2014 Updates to the Updates in Ambulatory Care Pharmacy
New ACC/AHA Guidelines on Lipids: Are PCSK9 Inhibitors Poised for a Breakthrough?
 New ACC/AHA Guidelines on Lipids: Are PCSK9 Inhibitors Poised for a Breakthrough? Sidney C. Smith, Jr. MD, FACC, FAHA Professor of Medicine/Cardiology University of North Carolina at Chapel Hill Immediate
New ACC/AHA Guidelines on Lipids: Are PCSK9 Inhibitors Poised for a Breakthrough? Sidney C. Smith, Jr. MD, FACC, FAHA Professor of Medicine/Cardiology University of North Carolina at Chapel Hill Immediate
ATP IV: Predicting Guideline Updates
 Disclosures ATP IV: Predicting Guideline Updates Daniel M. Riche, Pharm.D., BCPS, CDE Speaker s Bureau Merck Janssen Boehringer-Ingelheim Learning Objectives Describe at least two evidence-based recommendations
Disclosures ATP IV: Predicting Guideline Updates Daniel M. Riche, Pharm.D., BCPS, CDE Speaker s Bureau Merck Janssen Boehringer-Ingelheim Learning Objectives Describe at least two evidence-based recommendations
How would you manage Ms. Gold
 How would you manage Ms. Gold 32 yo Asian woman with dyslipidemia Current medications: Simvastatin 20mg QD Most recent lipid profile: TC = 246, TG = 100, LDL = 176, HDL = 50 What about Mr. Williams? 56
How would you manage Ms. Gold 32 yo Asian woman with dyslipidemia Current medications: Simvastatin 20mg QD Most recent lipid profile: TC = 246, TG = 100, LDL = 176, HDL = 50 What about Mr. Williams? 56
4 th and Goal To Go How Low Should We Go? :
 4 th and Goal To Go How Low Should We Go? : Evaluating New Lipid Lowering Therapies Catherine Bourg Rebitch, PharmD, BCACP Clinical Associate Professor Disclosure The presenter has nothing to disclose
4 th and Goal To Go How Low Should We Go? : Evaluating New Lipid Lowering Therapies Catherine Bourg Rebitch, PharmD, BCACP Clinical Associate Professor Disclosure The presenter has nothing to disclose
Pharmacy Drug Class Review
 Pharmacy Drug Class Review January 22, 2014 Authored By: Christina Manciocchi, Pharm.D. BCACP Disclaimer: Specific agents may have variations Edited By: Richard J. Kraft, Pharm.D.BCPS NEW CHOLESTEROL GUIDELINES
Pharmacy Drug Class Review January 22, 2014 Authored By: Christina Manciocchi, Pharm.D. BCACP Disclaimer: Specific agents may have variations Edited By: Richard J. Kraft, Pharm.D.BCPS NEW CHOLESTEROL GUIDELINES
PCSK9 Agents Drug Class Prior Authorization Protocol
 PCSK9 Agents Drug Class Prior Authorization Protocol Line of Business: Medicaid P & T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has been developed through review of medical
PCSK9 Agents Drug Class Prior Authorization Protocol Line of Business: Medicaid P & T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has been developed through review of medical
A New Age of Dyslipidemia Treatment: Role of Non- Statin Therapies
 A New Age of Dyslipidemia Treatment: Role of Non- Statin Therapies BRODY MAACK, PHARMD, BCACP, CTTS Objectives 1. Review current guidelines regarding use of statin medications in the treatment and prevention
A New Age of Dyslipidemia Treatment: Role of Non- Statin Therapies BRODY MAACK, PHARMD, BCACP, CTTS Objectives 1. Review current guidelines regarding use of statin medications in the treatment and prevention
When Statins Aren t Enough: Appropriate Therapies for High-Risk Patients with Diabetes
 When Statins Aren t Enough: Appropriate Therapies for High-Risk Patients with Diabetes Kim K. Birtcher, MS, PharmD, AACC, FNLA, CLS, BCPS (AQ-Cardiology), CDE Clinical Professor University of Houston College
When Statins Aren t Enough: Appropriate Therapies for High-Risk Patients with Diabetes Kim K. Birtcher, MS, PharmD, AACC, FNLA, CLS, BCPS (AQ-Cardiology), CDE Clinical Professor University of Houston College
DYSLIPIDEMIA TREATMENT: HYBRIDIZING CLINICAL PRACTICE GUIDELINES
 DYSLIPIDEMIA TREATMENT: HYBRIDIZING CLINICAL PRACTICE GUIDELINES SATURDAY/4:30-5:30PM ACPE UAN: 0107-9999-17-249-L01-P 0.1 CEU/1.0 hr Activity Type: Knowledge-Based Learning Objectives for Pharmacists:
DYSLIPIDEMIA TREATMENT: HYBRIDIZING CLINICAL PRACTICE GUIDELINES SATURDAY/4:30-5:30PM ACPE UAN: 0107-9999-17-249-L01-P 0.1 CEU/1.0 hr Activity Type: Knowledge-Based Learning Objectives for Pharmacists:
Deep Dive into Contemporary Cholesterol Management. Kim Allan Williams, Sr., MD, FACC Pamela B. Morris, MD, FACC 7 October 2016 Mexico City
 Deep Dive into Contemporary Cholesterol Management Kim Allan Williams, Sr., MD, FACC Pamela B. Morris, MD, FACC 7 October 2016 Mexico City Introduction: Pamela B. Morris, MD, FACC COMING TO CONSENSUS IN
Deep Dive into Contemporary Cholesterol Management Kim Allan Williams, Sr., MD, FACC Pamela B. Morris, MD, FACC 7 October 2016 Mexico City Introduction: Pamela B. Morris, MD, FACC COMING TO CONSENSUS IN
Clinical Policy: Lomitapide (Juxtapid) Reference Number: ERX.SPA.170 Effective Date:
 Reference Number: ERX.SPA.170 Effective Date:") Clinical Policy: (Juxtapid) Reference Number: ERX.SPA.170 Effective Date: 01.11.17 Last Review Date: 11.17 Revision Log See Important Reminder at the end of this policy for important regulatory and legal
Clinical Policy: (Juxtapid) Reference Number: ERX.SPA.170 Effective Date: 01.11.17 Last Review Date: 11.17 Revision Log See Important Reminder at the end of this policy for important regulatory and legal
2013 Cholesterol Guidelines. Anna Broz MSN, RN, CNP, AACC Cer=fied Adult Nurse Prac==oner North Ohio Heart, Inc.
 2013 Cholesterol Guidelines Anna Broz MSN, RN, CNP, AACC Cer=fied Adult Nurse Prac==oner North Ohio Heart, Inc. Disclosures Speaker Gilead Sciences NHLBI Charge to the Expert Panel Evaluate higher quality
2013 Cholesterol Guidelines Anna Broz MSN, RN, CNP, AACC Cer=fied Adult Nurse Prac==oner North Ohio Heart, Inc. Disclosures Speaker Gilead Sciences NHLBI Charge to the Expert Panel Evaluate higher quality
2013 ACC/AHA Guidelines on the Assessment of Atherosclerotic Cardiovascular Risk: Overview and Commentary
 2013 ACC/AHA Guidelines on the Assessment of Atherosclerotic Cardiovascular Risk: Overview and Commentary The Johns Hopkins Ciccarone Center for the Prevention of Heart Disease Becky McKibben, MPH; Seth
2013 ACC/AHA Guidelines on the Assessment of Atherosclerotic Cardiovascular Risk: Overview and Commentary The Johns Hopkins Ciccarone Center for the Prevention of Heart Disease Becky McKibben, MPH; Seth
CLINICAL OUTCOME Vs SURROGATE MARKER
 CLINICAL OUTCOME Vs SURROGATE MARKER Statin Real Experience Dr. Mostafa Sherif Senior Medical Manager Pfizer Egypt & Sudan Objective Difference between Clinical outcome and surrogate marker Proper Clinical
CLINICAL OUTCOME Vs SURROGATE MARKER Statin Real Experience Dr. Mostafa Sherif Senior Medical Manager Pfizer Egypt & Sudan Objective Difference between Clinical outcome and surrogate marker Proper Clinical
ACC/AHA GUIDELINES ON LIPIDS AND PCSK9 INHIBITORS
 ACC/AHA GUIDELINES ON LIPIDS AND PCSK9 INHIBITORS Ziyad Ghazzal MD, FACC, FSCAI Professor of Medicine Deputy Vice President/Dean Associate Dean for Clinical Affairs American University of Beirut Adjunct
ACC/AHA GUIDELINES ON LIPIDS AND PCSK9 INHIBITORS Ziyad Ghazzal MD, FACC, FSCAI Professor of Medicine Deputy Vice President/Dean Associate Dean for Clinical Affairs American University of Beirut Adjunct
PCSK9 Inhibitors: Promise or Pitfall?
 PCSK9 Inhibitors: Promise or Pitfall? Tracy Harlan, PharmD PGY2 Ambulatory Care Resident University of Iowa Hospitals and Clinics tracy harlan@uiowa.edu Tracy Harlan does not have any actual or potential
PCSK9 Inhibitors: Promise or Pitfall? Tracy Harlan, PharmD PGY2 Ambulatory Care Resident University of Iowa Hospitals and Clinics tracy harlan@uiowa.edu Tracy Harlan does not have any actual or potential
Is Lower Better for LDL or is there a Sweet Spot
 Is Lower Better for LDL or is there a Sweet Spot ALAN S BROWN MD, FACC FNLA FAHA FASPC DIRECTOR, DIVISION OF CARDIOLOGY ADVOCATE LUTHERAN GENERAL HOSPITAL, PARK RIDGE, ILLINOIS DIRECTOR OF CARDIOLOGY,
Is Lower Better for LDL or is there a Sweet Spot ALAN S BROWN MD, FACC FNLA FAHA FASPC DIRECTOR, DIVISION OF CARDIOLOGY ADVOCATE LUTHERAN GENERAL HOSPITAL, PARK RIDGE, ILLINOIS DIRECTOR OF CARDIOLOGY,
Disclosure. No relevant financial relationships. Placebo-Controlled Statin Trials
 PREVENTING CARDIOVASCULAR DISEASE IN WOMEN: Current Guidelines for Hypertension, Lipids and Aspirin Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial
PREVENTING CARDIOVASCULAR DISEASE IN WOMEN: Current Guidelines for Hypertension, Lipids and Aspirin Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial
Dyslipedemia New Guidelines
 Dyslipedemia New Guidelines New ACC/AHA Prevention Guidelines on Blood Cholesterol November 12, 2013 Mohammed M Abd El Ghany Professor of Cardiology Cairo Universlty 1 1 0 Cholesterol Management Pharmacotherapy
Dyslipedemia New Guidelines New ACC/AHA Prevention Guidelines on Blood Cholesterol November 12, 2013 Mohammed M Abd El Ghany Professor of Cardiology Cairo Universlty 1 1 0 Cholesterol Management Pharmacotherapy
Placebo-Controlled Statin Trials EXPLAINING THE DECREASE IN DEATHS FROM CHD! PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN EXPLAINING THE DECREASE IN
 PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest EXPLAINING THE DECREASE
PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest EXPLAINING THE DECREASE
Update on Cholesterol Management: The 2013 ACC/AHA Guidelines
 Update on Cholesterol Management: The 2013 ACC/AHA Guidelines Ola Akinboboye MD MPH MBA Medical Director, Queens Heart institute Rosedale. Associate Professor of Clinical Medicine, Weill Medical College
Update on Cholesterol Management: The 2013 ACC/AHA Guidelines Ola Akinboboye MD MPH MBA Medical Director, Queens Heart institute Rosedale. Associate Professor of Clinical Medicine, Weill Medical College
UPDATES IN LIPID MANAGEMENT
 UPDATES IN LIPID 2017 Cardiovascular Symposium MANAGEMENT SUDHA RAVILLA, MD, DIPLOMATE, ABCL MEDICAL DIRECTOR CLINICAL LIPIDOLOGY TMHPP METABOLIC HEALTH CENTER INTRODUCTION CVD is STILL the No. 1 cause
UPDATES IN LIPID 2017 Cardiovascular Symposium MANAGEMENT SUDHA RAVILLA, MD, DIPLOMATE, ABCL MEDICAL DIRECTOR CLINICAL LIPIDOLOGY TMHPP METABOLIC HEALTH CENTER INTRODUCTION CVD is STILL the No. 1 cause
PCSK9 Inhibitors Praluent (Alirocumab) and Repatha (Evolocumab) For the Treatment of Familial Hypercholesterolemia
 and Repatha (Evolocumab) For the Treatment of Familial Hypercholesterolemia") PCSK9 Inhibitors Praluent (Alirocumab) and Repatha (Evolocumab) For the Treatment of Familial Hypercholesterolemia Policy Number: Original Effective Date: MM.04.037 08/01/2016 Line(s) of Business: HMO;
PCSK9 Inhibitors Praluent (Alirocumab) and Repatha (Evolocumab) For the Treatment of Familial Hypercholesterolemia Policy Number: Original Effective Date: MM.04.037 08/01/2016 Line(s) of Business: HMO;
Sanger Heart & Vascular Institute Symposium 2015
 Sanger Heart & Vascular Institute Symposium 2015 Cardiovascular Update For Primary Care Physicians William E. Downey, MD FACC FSCAI Medical Director, Interventional Cardiology Sanger Heart & Vascular Institute
Sanger Heart & Vascular Institute Symposium 2015 Cardiovascular Update For Primary Care Physicians William E. Downey, MD FACC FSCAI Medical Director, Interventional Cardiology Sanger Heart & Vascular Institute
UnitedHealthcare Pharmacy Clinical Pharmacy Programs
 UnitedHealthcare Pharmacy Clinical Pharmacy Programs Program Number 2017 P 2063-8 Program Prior Authorization/Medical Necessity Medication Repatha (evolocumab) P&T Approval Date 5/2015, 9/2015, 11/2015,
UnitedHealthcare Pharmacy Clinical Pharmacy Programs Program Number 2017 P 2063-8 Program Prior Authorization/Medical Necessity Medication Repatha (evolocumab) P&T Approval Date 5/2015, 9/2015, 11/2015,
Drug Class Monograph
 Drug Class Monograph Class: Proprotein Convertase Subtilisin/Kexin Type 9 (PCSK9) Inhibitor Drugs: Praluent (alirocumab), Repatha (evolocumab) Line of Business: Medi-Cal Effective Date: February 17, 2016
Drug Class Monograph Class: Proprotein Convertase Subtilisin/Kexin Type 9 (PCSK9) Inhibitor Drugs: Praluent (alirocumab), Repatha (evolocumab) Line of Business: Medi-Cal Effective Date: February 17, 2016
Lipid Control Today: Management within the Context of other Cardiovascular Risk Factors
 Best Practices Lipid Control Today: Management within the Context of other Cardiovascular Risk Factors James A. Underberg, MD, MS, FACPM, FACP, FASH, FNLA, FASPC Lipidology & Cardiovascular Disease Prevention
Best Practices Lipid Control Today: Management within the Context of other Cardiovascular Risk Factors James A. Underberg, MD, MS, FACPM, FACP, FASH, FNLA, FASPC Lipidology & Cardiovascular Disease Prevention
Lipids & Hypertension Update
 Lipids & Hypertension Update No financial disclosures Michael W. Cullen, MD, FACC Senior Associate Consultant, Assistant Professor of Medicine Mayo Clinic Department of Cardiovascular Diseases 34 th Annual
Lipids & Hypertension Update No financial disclosures Michael W. Cullen, MD, FACC Senior Associate Consultant, Assistant Professor of Medicine Mayo Clinic Department of Cardiovascular Diseases 34 th Annual
Approach to Dyslipidemia among diabetic patients
 Approach to Dyslipidemia among diabetic patients Farzad Hadaegh, MD, Professor of Internal Medicine & Endocrinology Prevention of Metabolic Disorders Research Center, Research Institute for Endocrine Sciences
Approach to Dyslipidemia among diabetic patients Farzad Hadaegh, MD, Professor of Internal Medicine & Endocrinology Prevention of Metabolic Disorders Research Center, Research Institute for Endocrine Sciences
2017 Cardiovascular Summit for Primary Care Thursday 30th & Friday 31st March Crowne Plaza, Dublin
 2017 Cardiovascular Summit for Primary Care Thursday 30th & Friday 31st March 2017 - Crowne Plaza, Dublin 2016 ESC Guidelines on Cardiovascular Risk and elevated lipids Carlos Brotons Sardenya Primary
2017 Cardiovascular Summit for Primary Care Thursday 30th & Friday 31st March 2017 - Crowne Plaza, Dublin 2016 ESC Guidelines on Cardiovascular Risk and elevated lipids Carlos Brotons Sardenya Primary
Novel PCSK9 Outcomes. in Perspective: Lessons from FOURIER & ODYSSEY LDL-C. ASCVD Risk. Suboptimal Statin Therapy
 LDL-C Novel PCSK9 Outcomes Suboptimal Statin Therapy ASCVD Risk in Perspective: Lessons from FOURIER & ODYSSEY Jennifer G. Robinson, MD, MPH Professor, Departments of Epidemiology & Medicine Director,
LDL-C Novel PCSK9 Outcomes Suboptimal Statin Therapy ASCVD Risk in Perspective: Lessons from FOURIER & ODYSSEY Jennifer G. Robinson, MD, MPH Professor, Departments of Epidemiology & Medicine Director,
Young high risk patients the role of statins Dr. Mohamed Jeilan
 Young high risk patients the role of statins Dr. Mohamed Jeilan KCS Congress: Impact through collaboration CONTACT: Tel. +254 735 833 803 Email: kcardiacs@gmail.com Web: www.kenyacardiacs.org Disclosures
Young high risk patients the role of statins Dr. Mohamed Jeilan KCS Congress: Impact through collaboration CONTACT: Tel. +254 735 833 803 Email: kcardiacs@gmail.com Web: www.kenyacardiacs.org Disclosures
4/7/ The stats on heart disease. + Deaths & Age-Adjusted Death Rates for
 + Update on Lipid Management Stacey Gardiner, MD Assistant Professor Division of Cardiovascular Medicine Medical College of Wisconsin + The stats on heart disease Over the past 10 years for which statistics
+ Update on Lipid Management Stacey Gardiner, MD Assistant Professor Division of Cardiovascular Medicine Medical College of Wisconsin + The stats on heart disease Over the past 10 years for which statistics
Disclosures. Choosing a Statin/New Therapies. Case. How else would you do to treat him? LDL-C Reduction with Different Statin Strategies
 Disclosures I have no disclosures relevant to this talk Choosing a Statin/New Therapies Aryan Aiyer, MD Assistant Professor of Medicine University of Pittsburgh School of Medicine UPMC Heart and Vascular
Disclosures I have no disclosures relevant to this talk Choosing a Statin/New Therapies Aryan Aiyer, MD Assistant Professor of Medicine University of Pittsburgh School of Medicine UPMC Heart and Vascular
Placebo-Controlled Statin Trials MANAGEMENT OF HIGH BLOOD CHOLESTEROL MANAGEMENT OF HIGH BLOOD CHOLESTEROL: IMPLICATIONS OF THE NEW GUIDELINES
 MANAGEMENT OF HIGH BLOOD CHOLESTEROL: IMPLICATIONS OF THE NEW GUIDELINES Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest
MANAGEMENT OF HIGH BLOOD CHOLESTEROL: IMPLICATIONS OF THE NEW GUIDELINES Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest
Lipid Therapy: Statins and Beyond. Ivan Anderson, MD RIHVH Cardiology
 Lipid Therapy: Statins and Beyond Ivan Anderson, MD RIHVH Cardiology Outline The cholesterol hypothesis and lipid metabolism The Guidelines 4 Groups that Benefit from Lipid therapy Initiation and monitoring
Lipid Therapy: Statins and Beyond Ivan Anderson, MD RIHVH Cardiology Outline The cholesterol hypothesis and lipid metabolism The Guidelines 4 Groups that Benefit from Lipid therapy Initiation and monitoring
Index. cardiology.theclinics.com. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A ACC/AHA. See American College of Cardiology/ ACE inhibitors. See Angiotensin-converting enzyme (ACE) inhibitors American College of Cardiology/American
Index Note: Page numbers of article titles are in boldface type. A ACC/AHA. See American College of Cardiology/ ACE inhibitors. See Angiotensin-converting enzyme (ACE) inhibitors American College of Cardiology/American
This is a lipid lowering drug strategy which should only be used within an overall lifestyle and clinical management strategy.
 Treatment Guideline Statin Prescribing Objective These guidelines represent the views of the Gloucestershire Hospitals NHS Foundation Trust, which were arrived at after consideration of the available evidence
Treatment Guideline Statin Prescribing Objective These guidelines represent the views of the Gloucestershire Hospitals NHS Foundation Trust, which were arrived at after consideration of the available evidence
Highlights of the new blood pressure and cholesterol guidelines: A whole new philosophy. Jeremy L. Johnson, PharmD, BCACP, CDE, BC-ADM
 Highlights of the new blood pressure and cholesterol guidelines: A whole new philosophy Jeremy L. Johnson, PharmD, BCACP, CDE, BC-ADM OSHP 2014 Annual Meeting Oklahoma City, OK April 4, 2014 1 Objectives
Highlights of the new blood pressure and cholesterol guidelines: A whole new philosophy Jeremy L. Johnson, PharmD, BCACP, CDE, BC-ADM OSHP 2014 Annual Meeting Oklahoma City, OK April 4, 2014 1 Objectives
Placebo-Controlled Statin Trials Prevention Of CVD in Women"
 MANAGEMENT OF HIGH BLOOD CHOLESTEROL: IMPLICATIONS OF THE NEW GUIDELINES Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest
MANAGEMENT OF HIGH BLOOD CHOLESTEROL: IMPLICATIONS OF THE NEW GUIDELINES Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest
Achieving Cholesterol Management Goals: Identifying Clinician-Centered Challenges to Optimal Patient Care
 Achieving Cholesterol Management Goals: Identifying Clinician-Centered Challenges to Optimal Patient Care Purpose Explore the adherence rates to cholesterol treatment targets among patients who seek care
Achieving Cholesterol Management Goals: Identifying Clinician-Centered Challenges to Optimal Patient Care Purpose Explore the adherence rates to cholesterol treatment targets among patients who seek care
Pharmacy Management Drug Policy
 SUBJECT: ; Praluent (alirocumab), Repatha (evolocumab) POLICY NUMBER: Pharmacy-61 EFFECTIVE DATE: 8/15 LAST REVIEW DATE: 9/22/2017 If the member s subscriber contract excludes coverage for a specific service
SUBJECT: ; Praluent (alirocumab), Repatha (evolocumab) POLICY NUMBER: Pharmacy-61 EFFECTIVE DATE: 8/15 LAST REVIEW DATE: 9/22/2017 If the member s subscriber contract excludes coverage for a specific service
New Lipid Guidelines. PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN: Implications of the New Guidelines for Hypertension and Lipids.
 PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN: Implications of the New Guidelines for Hypertension and Lipids Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Disclosure No relevant
PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN: Implications of the New Guidelines for Hypertension and Lipids Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Disclosure No relevant
Andrew Cohen, MD and Neil S. Skolnik, MD INTRODUCTION
 2 Hyperlipidemia Andrew Cohen, MD and Neil S. Skolnik, MD CONTENTS INTRODUCTION RISK CATEGORIES AND TARGET LDL-CHOLESTEROL TREATMENT OF LDL-CHOLESTEROL SPECIAL CONSIDERATIONS OLDER AND YOUNGER ADULTS ADDITIONAL
2 Hyperlipidemia Andrew Cohen, MD and Neil S. Skolnik, MD CONTENTS INTRODUCTION RISK CATEGORIES AND TARGET LDL-CHOLESTEROL TREATMENT OF LDL-CHOLESTEROL SPECIAL CONSIDERATIONS OLDER AND YOUNGER ADULTS ADDITIONAL
THE 2013 ACC/AHA GUIDELINES ON THE TREATMENT OF BLOOD CHOLESTEROL
 THE 2013 ACC/AHA GUIDELINES ON THE TREATMENT OF BLOOD CHOLESTEROL Anne Carol Goldberg, MD, FACP, FAHA, FNLA Associate Professor of Medicine Washington University School of Medicine National Lipid Association
THE 2013 ACC/AHA GUIDELINES ON THE TREATMENT OF BLOOD CHOLESTEROL Anne Carol Goldberg, MD, FACP, FAHA, FNLA Associate Professor of Medicine Washington University School of Medicine National Lipid Association
UnitedHealthcare Pharmacy Clinical Pharmacy Programs
 UnitedHealthcare Pharmacy Clinical Pharmacy Programs Program Number 2017 P 2062-8 Program Prior Authorization/Medical Necessity Medication Praluent (alirocumab) P&T Approval Date 5/2015, 8/2015, 9/2015,
UnitedHealthcare Pharmacy Clinical Pharmacy Programs Program Number 2017 P 2062-8 Program Prior Authorization/Medical Necessity Medication Praluent (alirocumab) P&T Approval Date 5/2015, 8/2015, 9/2015,
Medical Policy An independent licensee of the Blue Cross Blue Shield Association
 Statin Therapy Page 1 of 10 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: Statin Therapy Prime Therapeutics will review Prior Authorization requests. Prior Authorization
Statin Therapy Page 1 of 10 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: Statin Therapy Prime Therapeutics will review Prior Authorization requests. Prior Authorization
2013 ACC/AHA CHOLESTEROL GUIDELINES TO REDUCE ASCVD RISK 1/7/2018. Disclosures
 Unblurring the Lines of Statin Use in Primary and Secondary Prevention of Cardiovascular Disease Disclosures Teryn J. Bibb reports she has no actual or potential conflict of interest in relation to this
Unblurring the Lines of Statin Use in Primary and Secondary Prevention of Cardiovascular Disease Disclosures Teryn J. Bibb reports she has no actual or potential conflict of interest in relation to this
JUPITER NEJM Poll. Panel Discussion: Literature that Should Have an Impact on our Practice: The JUPITER Study
 Panel Discussion: Literature that Should Have an Impact on our Practice: The Study Kaiser COAST 11 th Annual Conference Maui, August 2009 Robert Blumberg, MD, FACC Ralph Brindis, MD, MPH, FACC Primary
Panel Discussion: Literature that Should Have an Impact on our Practice: The Study Kaiser COAST 11 th Annual Conference Maui, August 2009 Robert Blumberg, MD, FACC Ralph Brindis, MD, MPH, FACC Primary
Guidelines for Management of Dyslipidemia and Prevention of Cardiovascular Disease
 AMERICAN ASSOCIATION OF CLINICAL ENDOCRINOLOGISTS AMERICAN COLLEGE OF ENDOCRINOLOGY Guidelines for Management of Dyslipidemia and Prevention of Cardiovascular Disease Writing Committee Chair: Paul S. Jellinger,
AMERICAN ASSOCIATION OF CLINICAL ENDOCRINOLOGISTS AMERICAN COLLEGE OF ENDOCRINOLOGY Guidelines for Management of Dyslipidemia and Prevention of Cardiovascular Disease Writing Committee Chair: Paul S. Jellinger,
2013 ACC/AHA Cholesterol Guidelines JULIE HAMMOND, D.O. PGY-2 MATTHEW PAOLI, D.O. PGY-2
 2013 ACC/AHA Cholesterol Guidelines JULIE HAMMOND, D.O. PGY-2 MATTHEW PAOLI, D.O. PGY-2 GOALS ACC/AHA as publisher of guidelines Determining which patients are appropriate for statin therapy The treatment
2013 ACC/AHA Cholesterol Guidelines JULIE HAMMOND, D.O. PGY-2 MATTHEW PAOLI, D.O. PGY-2 GOALS ACC/AHA as publisher of guidelines Determining which patients are appropriate for statin therapy The treatment
See Important Reminder at the end of this policy for important regulatory and legal information.
 Clinical Policy: (Repatha) Reference Number: HIM.PA.SP46 Effective Date: 01.01.18 Last Review Date: Line of Business: Health Insurance Marketplace Revision Log See Important Reminder at the end of this
Clinical Policy: (Repatha) Reference Number: HIM.PA.SP46 Effective Date: 01.01.18 Last Review Date: Line of Business: Health Insurance Marketplace Revision Log See Important Reminder at the end of this
Diabetes: Use of Adjunctive Therapy ACEs, ARBs, ASA & STATINs --Oh My! Veronica J. Brady, PhD, FNP-BC, BC-ADM, CDE Project ECHO April 19, 2018
 Diabetes: Use of Adjunctive Therapy ACEs, ARBs, ASA & STATINs --Oh My! Veronica J. Brady, PhD, FNP-BC, BC-ADM, CDE Project ECHO April 19, 2018 Points to Ponder ASCVD is the leading cause of morbidity
Diabetes: Use of Adjunctive Therapy ACEs, ARBs, ASA & STATINs --Oh My! Veronica J. Brady, PhD, FNP-BC, BC-ADM, CDE Project ECHO April 19, 2018 Points to Ponder ASCVD is the leading cause of morbidity
Management of Lipid Disorders and Hypertension: Implications of the New Guidelines
 Management of Lipid Disorders and Hypertension Management of Lipid Disorders and Hypertension: Implications of the New Guidelines Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine
Management of Lipid Disorders and Hypertension Management of Lipid Disorders and Hypertension: Implications of the New Guidelines Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine
What Role do the New PCSK9 Inhibitors Have in Lipid Lowering Treatment?
 What Role do the New PCSK9 Inhibitors Have in Lipid Lowering Treatment? Jennifer G. Robinson, MD, MPH Professor, Departments of Epidemiology & Medicine Director, Prevention Intervention Center University
What Role do the New PCSK9 Inhibitors Have in Lipid Lowering Treatment? Jennifer G. Robinson, MD, MPH Professor, Departments of Epidemiology & Medicine Director, Prevention Intervention Center University
Hyperlipidemia: Past and Present. Rebecca Khaimova, PharmD The Brooklyn Hospital Center
 Hyperlipidemia: Past and Present Rebecca Khaimova, PharmD The Brooklyn Hospital Center Rkhaimova@tbh.org Conflicts of Interest None to disclose Learning Objectives for Pharmacist Describe the pathophysiology
Hyperlipidemia: Past and Present Rebecca Khaimova, PharmD The Brooklyn Hospital Center Rkhaimova@tbh.org Conflicts of Interest None to disclose Learning Objectives for Pharmacist Describe the pathophysiology
Is it an era for statin for life?
 Is it an era for statin for life? Mohamed Abdel Ghany Professor of Cardiology Cairo University Cardiovascular Disease (CVD) is the leading global cause of death 1 Dyslipidemia as a main Risk Factor for
Is it an era for statin for life? Mohamed Abdel Ghany Professor of Cardiology Cairo University Cardiovascular Disease (CVD) is the leading global cause of death 1 Dyslipidemia as a main Risk Factor for
Accelerated atherosclerosis begins years prior to the diagnosis of diabetes
 Joslin Diabetes Forum 211: Optimizing Care for the Practicing Clinician Risk for atherosclerosis is 2 4 times greater in patients with diabetes CVD accounts for 65% of diabetic mortality >5% of patients
Joslin Diabetes Forum 211: Optimizing Care for the Practicing Clinician Risk for atherosclerosis is 2 4 times greater in patients with diabetes CVD accounts for 65% of diabetic mortality >5% of patients
Review current guideline recommendations for lipid-lowering therapy
 Breakout Session #3 New Paradigms in the Management of Dyslipidemia Review current guideline recommendations for lipid-lowering therapy Dr Meral KAYIKCIOGLU Ege University Medical School, Cardiology Dept,
Breakout Session #3 New Paradigms in the Management of Dyslipidemia Review current guideline recommendations for lipid-lowering therapy Dr Meral KAYIKCIOGLU Ege University Medical School, Cardiology Dept,
Understanding US Lipid Guidelines-2013:
 Presentation to NLA Symposium: May 3 2014 Understanding US Lipid Guidelines-2013: Neil J. Stone MD, MACP, FACC Bonow Professor of Medicine Feinberg School of Medicine Northwestern University Chicago, Il
Presentation to NLA Symposium: May 3 2014 Understanding US Lipid Guidelines-2013: Neil J. Stone MD, MACP, FACC Bonow Professor of Medicine Feinberg School of Medicine Northwestern University Chicago, Il
Case Studies The Role of Non-Statin Therapies for LDL-C Lowering in the Management of ASCVD Risk
 Case Studies The Role of Non-Statin Therapies for LDL-C Lowering in the Management of ASCVD Risk Kim K. Birtcher, PharmD, MS, AACC Clinical Professor University of Houston College of Pharmacy Houston,
Case Studies The Role of Non-Statin Therapies for LDL-C Lowering in the Management of ASCVD Risk Kim K. Birtcher, PharmD, MS, AACC Clinical Professor University of Houston College of Pharmacy Houston,