New Guidelines in Dyslipidemia Management
|
|
|
- Teresa Cook
- 5 years ago
- Views:
Transcription



1 The Third IAS-OSLA Course on Lipid Metabolism and Cardiovascular Risk Muscat, Oman, February 2017 New Guidelines in Dyslipidemia Management Dr. Khalid Al-Waili, MD, FRCPC, DABCL Senior Consultant Medical Biochemist & Lipidologist Sultan Qaboos University Hospital
2 Outline History of U.S. Dyslipidaemia Guideline Development New ACC/AHA cholesterol treatment guideline published Nov 2013 New NICE Guidelines 2014 Guidelines for Patients with CKD New ESC/EAS Guidelines 2016 New Middle East Guidelines 2016
3 History of U.S. Dyslipidemia Guideline Development ATP I 1 ATP II 2 ATP III 3 ATP III Update 4 ACC/AHA Guidelines 5 Exclusive focus on LDL-C Risk assessment guides therapy Lower LDL-C threshold for therapy initiation in high risk patients Lower LDL-C threshold for therapy initiation in very high risk patients Use of moderate- or high-intensity statin therapy for patients across 4 major groups at risk for ASCVD* *ASCVD, Atherosclerotic Cardiovascular Disease 1. NCEP. Arch Intern Med.1988;148: NCEP ATP II. Circulation.1994;89: NCEP ATP III. Circulation. 2002;106: Grundy SM, et al. Circulation. 2004;110: Stone NJ, et al. J Am Coll Cardiol. 2013: doi: /j.jacc Available at: Accessed November 13, 2013.
4 NCEP ATP III Updated Report: Risk Categories Increasing Risk Lower Risk Moderate Risk Moderately High-Risk High-Risk Very High-Risk 0-1 risk factor 2+ risk factors 10-year risk <10% 2+ risk factors 10-year risk 10-20% CHD CHD risk equivalents 10-year risk >20% Established CVD plus: - Multiple major risk factors - Severe and poorly controlled risk factors - Multiple risk factors of metabolic syndrome - ACS ACS=acute coronary syndromes; CHD=coronary heart disease; CVD=cardiovascular disease. Grundy et al. Circulation. 2004;110:
5 NCEP ATP III Updated Report: LDL-C Goals Based on Risk Category Increasing Risk Lower Risk Moderate Risk Moderately High-Risk High-Risk Very High-Risk LDL-C Goal <160 mg/dl LDL-C Goal <130 mg/dl LDL-C Goal <130 mg/dl LDL-C Goal <100 mg/dl LDL-C Goal <100 mg/dl Optional Goal <100 mg/dl Optional Goal <70 mg/dl Grundy et al. Circulation. 2004;110:


6 New ACC/AHA cholesterol treatment guideline published Nov 2013 AHA, American Heart Association ACC, American College of Cardiology
7 What is new in the 2013 Guideline? Identification of 4 major statin benefit groups Shift away from treat to target approach Definitions of statin intensity provided New global risk assessment tool for primary prevention Addition of non-statin drug therapy to statins to further decrease ASCVD risk addressed Stone NJ, et al. J Am Coll Cardiol. 2013: doi: /j.jacc Available at: Accessed November 13, 2013.
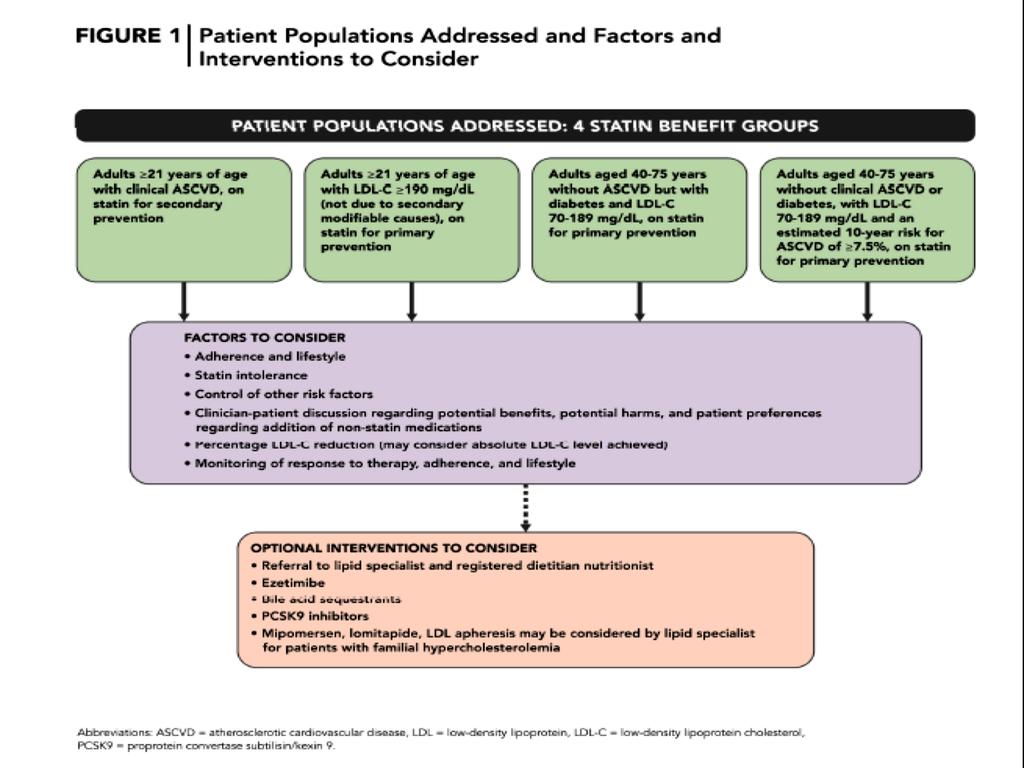
8 Major Statin Benefit Groups ASCVD LDL (mg/dl) DM (40 75 years) 10 year risk ASCVD 7.5 % 1 Yes > No Yes - 4 No No Yes ASCVD, Atherosclerotic Cardiovascular Disease
9 Group 1: Patients with clinical ASCVD Guideline Direction High-intensity statin therapy should be initiated or continued as first-line therapy in women and men 75 years of age who have clinical ASCVD, unless contraindicated. * *ACC/AHA Guideline 2013/p 22/secondary prevention #1
10 Group 2: Patients with primary elevations of LDL C 190 mg/dl ( 4.9 mmol/l) Guideline Direction Adults 21 years of age with primary LDL C 190 mg/dl ( 4.9 mmol/l) should be treated with statin therapy (10-year ASCVD risk estimation is not required): Use high-intensity statin therapy unless contraindicated. * *ACC/AHA Guideline 2013/p 22/primary prevention 21/#2
11 Group 3: Patients with diabetes aged years with LDL mg/dl ( mmol/l) and without clinical ASCVD Guideline Direction Moderate-intensity statin therapy should be initiated or continued for adults 40 to 75 years of age with diabetes mellitus. High-intensity statin therapy is reasonable for adults 40 to 75 years of age with diabetes mellitus with a 7.5% estimated 10-year ASCVD risk unless contraindicated. * *ACC/AHA Guideline 2013/p 23/primary prevention with diabetes/# 1,2
12 Group 3: Patients with diabetes aged years with LDL mg/dl ( mmol/l) and without clinical ASCVD Type 1 or 2 diabetes Age years Yes No Consider statin individually Estimate 10-year ASCVD risk with Pooled Cohort Equations ASCVD risk 7.5% ASCVD risk <7.5% High-intensity statin* Moderate-intensity statin *Expected to reduce LDL-C by 50% Expected to reduce LDL-C by 30 to <50% Stone NJ, et al. J Am Coll Cardiol 2013 Nov 7. Epub ahead of print
13 Group 4: Patients without clinical ASCVD or diabetes with LDL C 70 to 189 mg/dl (1.8 to 4.9 mmol/l) and estimated 10-year ASCVD risk 7.5% Guideline Direction Adults 40 to 75 years of age with LDL C 70 to 189 mg/dl (1.8 to 4.9 mmol/l), without clinical ASCVD or diabetes and an estimated 10-year ASCVD risk 7.5% should be treated with moderate- to high-intensity statin therapy. * *ACC/AHA Guideline 2013/p 23/Primary Prevention w/o Diabetes/#2
14 Major Statin Benefit Groups ASCVD LDL (mg/dl) DM (40 75 yrs) 10 year risk ASCVD 7.5 % Statin 1 Yes < 75 yrs High Intensity > 75 yrs Moderate Intensity 2 - > High Intensity 3a No Yes - Moderate Intensity 3b No Yes 7.5 % High Intensity 4 No No 7.5 % Moderate to High Intensity No No % Moderate Intensity No No < 5 % The potential for an ASCVD risk reduction benefit clearly exceeds the potential for adverse effects in adults within the 4 major statin groups.
15 Guidelines use new ASCVD risk calculator 10-year risk (%) of ASCVD (non-fatal MI, CHD death, or fatal/non-fatal stroke) is calculated from simple parameters: Risk factor Sex (male or female) Age (years) Race (African-American or White/other) Total cholesterol (mg/dl) HDL-C (mg/dl) SBP (mmhg) Treatment for high BP (yes or no) Diabetes (yes or no) Smoker (yes or no) 10 year risk and Lifetime Risk BP, blood pressure HDL-C, high density lipoprotein-cholesterol SBP, Systolic blood pressure Goff DC Jr, et al. J Am Coll Cardiol 2013 Nov 7. Epub ahead of print
16 Guidelines specify statin doses High-intensity LDL-C by 50% Moderate-intensity LDL-C by 30 50% Atorvastatin (40) 80 mg mg Rosuvastatin mg 5 10 mg Simvastatin mg 10 mg Low-intensity LDL-C by <30%* Pravastatin mg mg Lovastatin 40 mg 20 mg Fluvastatin XL 80 mg Fluvastatin 40 mg bid mg Pitvastatin 2 4 mg 1 mg Bold: Statins and doses evaluated in RCTs Italics: Statins and doses approved by US FDA but not tested in RCTs reviewed *Should be used in patients unable to tolerate moderate-to high-intensity therapy Asian ancestry may modify the statin dose prescribed Stone NJ, et al. J Am Coll Cardiol 2013 Nov 7. Epub ahead of print Reproduced with kind permission from American College of Cardiology Jan 2014
17 Patients outside the four benefit groups: Consider statin therapy individually Statins can be considered for patients with 10-year ASCVD risk <7.5% based on additional factors 1 Elevated lifetime ASCVD risk 1 LDL-C >160 mg/dl (~4.0 mmol/l) Other genetic hyperlipidemias 1 Family history of ASCVD 1 C-reactive protein >2 mg/l (~19 nmol/l) Ankle-brachial index <0.9 High coronary artery calcium (CAC) score 1 Carotid intimal-medial thickness not recommended 2 Exceptions: 1 NYHA class II IV HF or maintenance hemodialysis insufficient evidence HF, heart failure Individual discussion of benefits and risks 1 1. Stone NJ, et al. J Am Coll Cardiol 2013 Nov 7. Epub ahead of print 2. Goff DC Jr, et al. J Am Coll Cardiol 2013 Nov 7. Epub ahead of print
18 A New Perspective on LDL C and/or Non-HDL C Treatment Goals Lack of RCT evidence to support continued use of specific LDL C and/or non-hdl C treatment targets No recommendations for or against specific LDL-C and non-hdl-c goals for primary or secondary prevention Stone NJ, et al. J Am CollCardiol. 2013: doi: /j.jacc Available at: Accessed November 13, 2013.
19 Summary: 2013 Guideline Recommendations for Statin Therapy ASCVD Statin Benefit Groups Heart healthy lifestyle habits are the foundation of ASCVD prevention Clinical ASCVD LDL-C 190 mg/dl Diabetes; age years* Estimated 10-yr ASCVD risk 7.5% ; age years* High-Intensity statin (age 75 years) Moderate-intensity statin if >75 years or not a candidate for high-intensity statin High-intensity statin Moderate-intensity statin if not a candidate for highintensity statin Moderate-intensity statin High-intensity statin if estimated 10 year ASCVD risk 7.5% Moderate- to high-intensity statin ASCVD prevention benefit of statin therapy may be less clear in other groups. Consider additional factors influencing ASCVD risk, potential ASCVD risk benefits and adverse effects, drug-drug interactions, and patient preferences for statin treatment. * With LDL-C of mg/dl Estimated using the Pooled Cohort Risk Assessment Equations Stone NJ, et al. J Am CollCardiol. 2013: doi: /j.jacc Available at: Accessed November 13, 2013.
20 Safety Considerations Creatinine Kinase (CK) Routine monitoring of CK not recommended Measurement may be useful at baseline in those at increased risk of muscle events and in patients with muscle symptoms Guideline provides recommendations for management of muscle symptoms Alanine Transaminase (ALT) Baseline measurement recommended Routine hepatic monitoring not recommended unless symptoms suggesting hepatotoxicity are present Type-2 Diabetes Statins modestly increase risk of type-ii diabetes in patients with risk factors for diabetes Potential for ASCVD risk reduction benefit outweighs risk of diabetes in all but lowest risk individuals Evaluate for new onset diabetes according to current diabetes screening guidelines Stone NJ, et al. J Am Coll Cardiol. J Am Coll Cardiol. 2013: doi: /j.jacc Available at: Accessed November 13, 2013.
21 Recommendations for Non-statin Therapies * No data supporting the routine use of non-statin drugs combined with statin therapy to further decrease ASCVD events * In high-risk patients who have an insufficient response to statin therapy, or who are unable to tolerate either a statin or the recommended statin intensity, addition of a non-statin cholesterol-lowering therapy can be considered Stone NJ, et al. J Am Coll Cardiol. 2013: doi: /j.jacc Available at: Accessed November 13, 2013.
22
23 2016 ACC Expert Consensus Decision Pathway on the Role of Non-Statin Therapies for LDL-Cholesterol Lowering in the Management of Atherosclerotic Cardiovascular Disease Risk * Since the publication of the 2013 ACC/AHA cholesterol guidelines, RCTs evaluating the safety and efficacy of non-statin therapies have provided important information regarding the potential benefits and harms of these agents in ASCVD risk reduction when used in combination with evidencebased statin therapy * In addition, the approval of 2 PCSK9 inhibitors for LDL-C lowering in specific high-risk patients has resulted in gaps in expert guidance regarding the role of available non-statin therapies
24 2016 ACC Expert Consensus Decision Pathway on the Role of Non-Statin Therapies for LDL-Cholesterol Lowering in the Management of Atherosclerotic Cardiovascular Disease Risk * This Expert Consensus Decision Pathway addresses current gaps in care for LDL-C lowering to reduce ASCVD risk and recommendations build on the evidence base established by the 2013 ACC/AHA cholesterol guideline * Recommendations attempt to provide practical guidance for clinicians and patients regarding the use of non-statin therapies to further reduce ASCVD risk in situations not covered by the guideline until such time as the scientific evidence base expands and cardiovascular outcomes trials are completed with new agents for ASCVD risk reduction
25
26
27
28 NICE July 2014
29 Key priorities for implementation NICE 2014 Identifying and assessing cardiovascular disease (CVD) risk * For the primary prevention of CVD in primary care, use a systematic strategy to identify people who are likely to be at high risk. [2008, amended 2014] * Prioritize people for a full formal risk assessment if their estimated 10-year risk of CVD is 10% or more. [2008, amended 2014] * Use the QRISK2 risk assessment tool to assess CVD risk for the primary prevention of CVD in people up to and including age 84 years. [new 2014] * Do not use a risk assessment tool to assess CVD risk in people with an estimated glomerular filtration rate (egfr) less than 60 ml/min/1.73 m2 and/or albuminuria. These people are at increased risk of CVD. [new 2014]
30 Key priorities for implementation Lipid modification therapy for the primary and secondary prevention of CVD * Before starting lipid modification therapy for the primary prevention of CVD, take at least 1 lipid sample to measure a full lipid profile. This should include measurement of TC, HDL, non- HDL and triglyceride concentrations. A fasting sample is not needed. [new 2014] * Offer atorvastatin 20 mg for the primary prevention of CVD to people who have a 10% or greater 10-year risk of developing CVD. Estimate the level of risk using the QRISK2 assessment tool. [new 2014] * Start statin treatment in people with CVD with atorvastatin 80 mg. Use a lower dose of atorvastatin if any of the following apply: * potential drug interactions * high risk of adverse effects * patient preference [new 2014]
31 Key priorities for implementation Lipid modification therapy for the primary and secondary prevention of CVD * Measure TC, HDL and non-hdl in all people who have been started on high-intensity statin treatment at 3 months of treatment and aim for > 40% reduction in non-hdl cholesterol. If a greater than 40% reduction in non-hdl cholesterol is not achieved: * discuss adherence and timing of dose * optimize adherence to diet and lifestyle measures * consider increasing dose if started on less than atorvastatin 80 mg and the person is judged to be at higher risk because of comorbidities, risk score or using clinical judgment. [new 2014]
32 Grouping of Statins as per NICE Reduction in LDL-C Dose (mg/day) Fluvastatin 21% 1 27% 1 33% 2 Pravastatin 20% 1 24% 1 29% 1 Simvastatin 27% 1 32% 2 37% 2 42% 3,4 Atorvastatin 37% 2 43% 3 49% 3 55% 3 Rosuvastatin 38% 2 43% 3 48% 3 53% % 30%: low intensity. 2 31% 40%: medium intensity. 3 Above 40%: high intensity. 4 Advice from the MHRA: there is an increased risk of myopathy associated with high-dose (80 mg) simvastatin. The 80 mg dose should be considered only in patients with severe hypercholesterolaemia and high risk of cardiovascular complications who have not achieved their treatment goals on lower doses, when the benefits are expected to outweigh the potential risks.
33 Be Aware
34 NICE Do not delay in 2ndary prevention
35 NICE NODM
36 NICE T1DM
37 NICE T2DM
38 NICE Fibrates / Nicotinic Acid / Bile acid sequestrants / Omega 3 Fatty Acids
39 Guidelines for Patients with CKD * ACC/AHA did not address specific recommendations for patients with CKD * Appendix of Evidence Statements includes the following statement regarding use of atorvastatin for secondary prevention in patients with CKD, based on results of TNT: In adults with CHD/CVD and chronic kidney disease (CKD) (excluding hemodialysis), fixed high-intensity statin treatment (atorvastatin 80 mg) that achieved a mean LDL C of 79 mg/dl reduced CHD/CVD events more than fixed lower-dose statin treatment that achieved a mean LDL C of 99 mg/dl (2.6 mmol/l). In this trial, the mean LDL C levels achieved differed by 20 mg/dl (0.52 mmol/l), or 20% between the 2 groups. * However, KDIGO (Kidney Disease Improving Global Outcomes) 2013 guidelines recommend statin therapy for CKD patients 50 years of age and patients years of age with known coronary disease, diabetes, prior ischemic stroke, or 10-year CHD risk >10% * Once appropriate therapy has been selected, measuring LDL-C is not recommended unless results would change management * Escalation to reach specific LDL-C goals is no longer recommended
40 NICE CKD

41 Adapted from reference : National Kidney Foundation. KDOQI clinical practice guidelines and clinical practice recommendations for diabetes and chronic kidney disease. Am J Kidney Dis. 2007;49(suppl 2);S1-S179.
42
43 Table 5 Very high-risk High-risk Moderate risk Risk categories Low-risk SCORE <1%. Subjects with any of the following: Documented CVD, clinical or unequivocal on imaging. Documented clinical CVD includes previous AMI, ACS, coronary revascularization and other arterial revascularization procedures, stroke and TIA, aortic aneurysm and PAD. Unequivocally documented CVD on imaging includes plaque on coronary angiography or carotid ultrasound. It does NOT include some increase in continuous imaging parameters such as intima media thickness of the carotid artery. DM with target organ damage such as proteinuria or with a major risk factor such as smoking or marked hypercholesterolaemia or marked hypertension. Severe CKD (GFR <30 ml/min/1.73 m2). A calculated SCORE 10%. Subjects with: Markedly elevated single risk factors, in particular cholesterol >8 mmol/l (>310 mg/dl) (e.g. in familial hypercholesterolaemia) or BP 180/110 mmhg. Most other people with DM (with the exception of young people with type 1 DM and without major risk factors that may be at low or moderate risk). Moderate CKD (GFR ml/min/1.73 m 2 ). A calculated SCORE 5% and <10%. SCORE is 1% and <5% at 10 years. Many middleaged subjects belong to this category European Guidelines on cardiovascular disease prevention in clinical practice The Sixth Joint Task Force of the European Society of Cardiology and Other Societies on Cardiovascular Disease Prevention in Clinical Practice (constituted by representatives of 10 societies and by invited experts) Developed with the special contribution of the European Association Recommendations for lipid control Recommendations d e Class a Level b Ref c In patients at VERY HIGH CV risk, an LDL-C goal <1.8 mmol/l (<70 mg/dl), or a reduction of at least 50% if the baseline is between 1.8 and 3.5 mmol/l (70 and 135 mg/ dl) is recommended. f In patients at HIGH CV risk, an LDL-C goal <2.6 mmol/l (<100 mg/dl), or a reduction of at least 50% if the baseline is between 2.6 and 5.1 mmol/l (100 and 200 mg/dl) is recommended. In the remaining patients on LDL-C lowering treatment, an LDL-C goal <3.0 mmol/l (<115 mg/dl) should be considered. I B I B IIa C ¼ ¼ ¼ Piepoli et al. European Heart Journal doi: /eurheartj/ehw106 ¼ ¼ 43
44
45
46
47
48
49
50
51 Conclusions It has been proven in many large clinical trials that reducing level of LDL cholesterol reduces the risk of having a cardiovascular event. The benefit is proportional to the CVD risk. More intensive treatments are more effective in preventing clinical events Low LDL-C is safe Statins are the cornerstone of LDL-C lowering Addition of ezetimibe to a statin reduces ASCVD events (IMPROVE-IT trial) Large clinical ASCVD outcomes trials of PCSK9 inhibitors are ongoing. However, there are some preliminary, post-hoc shorter-term CV data available suggesting that these agents may reduce ASCVD risk.
52 *Questions???? Thank you
New Guidelines in Dyslipidemia Management
 The Fourth IAS-OSLA Course on Lipid Metabolism and Cardiovascular Risk Muscat, Oman, February 2018 New Guidelines in Dyslipidemia Management Dr. Khalid Al-Waili, MD, FRCPC, DABCL Senior Consultant Medical
The Fourth IAS-OSLA Course on Lipid Metabolism and Cardiovascular Risk Muscat, Oman, February 2018 New Guidelines in Dyslipidemia Management Dr. Khalid Al-Waili, MD, FRCPC, DABCL Senior Consultant Medical
2013 ACC AHA LIPID GUIDELINE JAY S. FONTE, MD
 2013 ACC AHA LIPID GUIDELINE JAY S. FONTE, MD How do you interpret my blood test results? What are our targets for these tests? Before the ACC/AHA Lipid Guidelines A1c:
2013 ACC AHA LIPID GUIDELINE JAY S. FONTE, MD How do you interpret my blood test results? What are our targets for these tests? Before the ACC/AHA Lipid Guidelines A1c:
Dyslipidemia in the light of Current Guidelines - Do we change our Practice?
 Dyslipidemia in the light of Current Guidelines - Do we change our Practice? Dato Dr. David Chew Soon Ping Senior Consultant Cardiologist Institut Jantung Negara Atherosclerotic Cardiovascular Disease
Dyslipidemia in the light of Current Guidelines - Do we change our Practice? Dato Dr. David Chew Soon Ping Senior Consultant Cardiologist Institut Jantung Negara Atherosclerotic Cardiovascular Disease
What do the guidelines say about combination therapy?
 What do the guidelines say about combination therapy? Christie M. Ballantyne, MD Center for Cardiovascular Disease Prevention Methodist DeBakey Heart & Vascular Center Baylor College of Medicine Houston,
What do the guidelines say about combination therapy? Christie M. Ballantyne, MD Center for Cardiovascular Disease Prevention Methodist DeBakey Heart & Vascular Center Baylor College of Medicine Houston,
Latest Guidelines for Lipid Management
 Latest Guidelines for Lipid Management Goals Recognize the differences between different guidelines Understand the effective strategies to tailor lipid lowering therapies based on evidence and guideline
Latest Guidelines for Lipid Management Goals Recognize the differences between different guidelines Understand the effective strategies to tailor lipid lowering therapies based on evidence and guideline
Learning Objectives. Patient Case
 Joseph Saseen, Pharm.D., FASHP, FCCP, BCPS Professor and Vice Chair, Department of Clinical Pharmacy University of Colorado Anschutz Medical Campus Learning Objectives Identify the 4 patient populations
Joseph Saseen, Pharm.D., FASHP, FCCP, BCPS Professor and Vice Chair, Department of Clinical Pharmacy University of Colorado Anschutz Medical Campus Learning Objectives Identify the 4 patient populations
Long-Term Complications of Diabetes Mellitus Macrovascular Complication
 Long-Term Complications of Diabetes Mellitus Macrovascular Complication Sung Hee Choi MD, PhD Professor, Seoul National University College of Medicine, SNUBH, Bundang Hospital Diabetes = CVD equivalent
Long-Term Complications of Diabetes Mellitus Macrovascular Complication Sung Hee Choi MD, PhD Professor, Seoul National University College of Medicine, SNUBH, Bundang Hospital Diabetes = CVD equivalent
Acute Coronary Syndromes (ACS)
") Sally A. Arif, Pharm.D., BCPS (AQ Cardiology) Assistant Professor of Pharmacy Practice Midwestern University, Chicago College of Pharmacy Cardiology Clinical Specialist, Rush University Medical Center
Sally A. Arif, Pharm.D., BCPS (AQ Cardiology) Assistant Professor of Pharmacy Practice Midwestern University, Chicago College of Pharmacy Cardiology Clinical Specialist, Rush University Medical Center
An update on lipidology and cardiovascular risk management. Lipids, Metabolism & Vascular Risk Section - Royal Society of Medicine
 An update on lipidology and cardiovascular risk management Lipids, Metabolism & Vascular Risk Section - Royal Society of Medicine National and international lipid modification guidelines: A critical appraisal
An update on lipidology and cardiovascular risk management Lipids, Metabolism & Vascular Risk Section - Royal Society of Medicine National and international lipid modification guidelines: A critical appraisal
Pharmacy Drug Class Review
 Pharmacy Drug Class Review January 22, 2014 Authored By: Christina Manciocchi, Pharm.D. BCACP Disclaimer: Specific agents may have variations Edited By: Richard J. Kraft, Pharm.D.BCPS NEW CHOLESTEROL GUIDELINES
Pharmacy Drug Class Review January 22, 2014 Authored By: Christina Manciocchi, Pharm.D. BCACP Disclaimer: Specific agents may have variations Edited By: Richard J. Kraft, Pharm.D.BCPS NEW CHOLESTEROL GUIDELINES
4/7/ The stats on heart disease. + Deaths & Age-Adjusted Death Rates for
 + Update on Lipid Management Stacey Gardiner, MD Assistant Professor Division of Cardiovascular Medicine Medical College of Wisconsin + The stats on heart disease Over the past 10 years for which statistics
+ Update on Lipid Management Stacey Gardiner, MD Assistant Professor Division of Cardiovascular Medicine Medical College of Wisconsin + The stats on heart disease Over the past 10 years for which statistics
Introduction. Objective. Critical Questions Addressed
 Introduction Objective To provide a strong evidence-based foundation for the treatment of cholesterol for the primary and secondary prevention of ASCVD in women and men Critical Questions Addressed CQ1:
Introduction Objective To provide a strong evidence-based foundation for the treatment of cholesterol for the primary and secondary prevention of ASCVD in women and men Critical Questions Addressed CQ1:
Conflict of Interest Disclosure. Learning Objectives. Learning Objectives. Guidelines. Update on Lifestyle Guidelines
 Conflict of Interest Disclosure Updates for the Ambulatory Care Pharmacist: Dyslipidemia and CV Risk Assessment No conflicts of interest to disclose 2014 Updates to the Updates in Ambulatory Care Pharmacy
Conflict of Interest Disclosure Updates for the Ambulatory Care Pharmacist: Dyslipidemia and CV Risk Assessment No conflicts of interest to disclose 2014 Updates to the Updates in Ambulatory Care Pharmacy
Review current guideline recommendations for lipid-lowering therapy
 Breakout Session #3 New Paradigms in the Management of Dyslipidemia Review current guideline recommendations for lipid-lowering therapy Dr Meral KAYIKCIOGLU Ege University Medical School, Cardiology Dept,
Breakout Session #3 New Paradigms in the Management of Dyslipidemia Review current guideline recommendations for lipid-lowering therapy Dr Meral KAYIKCIOGLU Ege University Medical School, Cardiology Dept,
CLINICAL OUTCOME Vs SURROGATE MARKER
 CLINICAL OUTCOME Vs SURROGATE MARKER Statin Real Experience Dr. Mostafa Sherif Senior Medical Manager Pfizer Egypt & Sudan Objective Difference between Clinical outcome and surrogate marker Proper Clinical
CLINICAL OUTCOME Vs SURROGATE MARKER Statin Real Experience Dr. Mostafa Sherif Senior Medical Manager Pfizer Egypt & Sudan Objective Difference between Clinical outcome and surrogate marker Proper Clinical
Update on Lipid Management in Cardiovascular Disease: How to Understand and Implement the New ACC/AHA Guidelines
 Update on Lipid Management in Cardiovascular Disease: How to Understand and Implement the New ACC/AHA Guidelines Paul Mahoney, MD Sentara Cardiology Specialists Lipid Management in Cardiovascular Disease
Update on Lipid Management in Cardiovascular Disease: How to Understand and Implement the New ACC/AHA Guidelines Paul Mahoney, MD Sentara Cardiology Specialists Lipid Management in Cardiovascular Disease
Primary Prevention Patients aged 85yrs and over
 Rotherham Guideline for the management of Non-Familial Hypercholesterolaemia Type 1 Diabetes Offer lifestyle advice Over 40yrs of age? Diabetic for more than 10 years? Established nephropathy? Other CVD
Rotherham Guideline for the management of Non-Familial Hypercholesterolaemia Type 1 Diabetes Offer lifestyle advice Over 40yrs of age? Diabetic for more than 10 years? Established nephropathy? Other CVD
Lipid Management: The Next Level How Will the New ACC/AHA Guidelines Change My Practice
 Lipid Management: The Next Level How Will the New ACC/AHA Guidelines Change My Practice Vera Bittner, MD, MSPH Professor of Medicine Section Head, Preventive Cardiology Medical Director, Cardiac Rehabilitation
Lipid Management: The Next Level How Will the New ACC/AHA Guidelines Change My Practice Vera Bittner, MD, MSPH Professor of Medicine Section Head, Preventive Cardiology Medical Director, Cardiac Rehabilitation
Lipid Management 2013 Statin Benefit Groups
 Clinical Integration Steering Committee Clinical Integration Chronic Disease Management Work Group Lipid Management 2013 Statin Benefit Groups Approved by Board Chair Signature Name (Please Print) Date
Clinical Integration Steering Committee Clinical Integration Chronic Disease Management Work Group Lipid Management 2013 Statin Benefit Groups Approved by Board Chair Signature Name (Please Print) Date
No relevant financial relationships
 MANAGEMENT OF LIPID DISORDERS Balancing Benefits and harms Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial relationships baron@medicine.ucsf.edu
MANAGEMENT OF LIPID DISORDERS Balancing Benefits and harms Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial relationships baron@medicine.ucsf.edu
Prevention of Heart Disease: The New Guidelines
 Prevention of Heart Disease: The New Guidelines Nisha I. Parikh MD MPH Assistant Professor of Medicine Division of Cardiology Department of Medicine University of California San Francisco May 18 th 2015
Prevention of Heart Disease: The New Guidelines Nisha I. Parikh MD MPH Assistant Professor of Medicine Division of Cardiology Department of Medicine University of California San Francisco May 18 th 2015
How would you manage Ms. Gold
 How would you manage Ms. Gold 32 yo Asian woman with dyslipidemia Current medications: Simvastatin 20mg QD Most recent lipid profile: TC = 246, TG = 100, LDL = 176, HDL = 50 What about Mr. Williams? 56
How would you manage Ms. Gold 32 yo Asian woman with dyslipidemia Current medications: Simvastatin 20mg QD Most recent lipid profile: TC = 246, TG = 100, LDL = 176, HDL = 50 What about Mr. Williams? 56
Dyslipedemia New Guidelines
 Dyslipedemia New Guidelines New ACC/AHA Prevention Guidelines on Blood Cholesterol November 12, 2013 Mohammed M Abd El Ghany Professor of Cardiology Cairo Universlty 1 1 0 Cholesterol Management Pharmacotherapy
Dyslipedemia New Guidelines New ACC/AHA Prevention Guidelines on Blood Cholesterol November 12, 2013 Mohammed M Abd El Ghany Professor of Cardiology Cairo Universlty 1 1 0 Cholesterol Management Pharmacotherapy
Review of guidelines for management of dyslipidemia in diabetic patients
 2012 international Conference on Diabetes and metabolism (ICDM) Review of guidelines for management of dyslipidemia in diabetic patients Nan Hee Kim, MD, PhD Department of Internal Medicine, Korea University
2012 international Conference on Diabetes and metabolism (ICDM) Review of guidelines for management of dyslipidemia in diabetic patients Nan Hee Kim, MD, PhD Department of Internal Medicine, Korea University
2013 Cholesterol Guidelines. Anna Broz MSN, RN, CNP, AACC Adult Certified Nurse Practitioner North Ohio Heart, Inc.
 2013 Cholesterol Guidelines Anna Broz MSN, RN, CNP, AACC Adult Certified Nurse Practitioner North Ohio Heart, Inc. Disclosures Speaker Gilead Sciences NHLBI Charge to the Expert Panel Evaluate higher quality
2013 Cholesterol Guidelines Anna Broz MSN, RN, CNP, AACC Adult Certified Nurse Practitioner North Ohio Heart, Inc. Disclosures Speaker Gilead Sciences NHLBI Charge to the Expert Panel Evaluate higher quality
Lipid Panel Management Refresher Course for the Family Physician
 Lipid Panel Management Refresher Course for the Family Physician Objectives Understand the evidence that was evaluated to develop the 2013 ACC/AHA guidelines Discuss the utility and accuracy of the new
Lipid Panel Management Refresher Course for the Family Physician Objectives Understand the evidence that was evaluated to develop the 2013 ACC/AHA guidelines Discuss the utility and accuracy of the new
4/24/15. AHA/ACC 2013 Guideline Key Points
 Review of the ACC/AHA 2013 Guidelines Anita Ralstin, MS, CNS, CNP Next Step Health Consultant, LLC 1! Discuss the rationale for the change in lipid guidelines and how that affects the decision to implement
Review of the ACC/AHA 2013 Guidelines Anita Ralstin, MS, CNS, CNP Next Step Health Consultant, LLC 1! Discuss the rationale for the change in lipid guidelines and how that affects the decision to implement
2013 Cholesterol Guidelines. Anna Broz MSN, RN, CNP, AACC Cer=fied Adult Nurse Prac==oner North Ohio Heart, Inc.
 2013 Cholesterol Guidelines Anna Broz MSN, RN, CNP, AACC Cer=fied Adult Nurse Prac==oner North Ohio Heart, Inc. Disclosures Speaker Gilead Sciences NHLBI Charge to the Expert Panel Evaluate higher quality
2013 Cholesterol Guidelines Anna Broz MSN, RN, CNP, AACC Cer=fied Adult Nurse Prac==oner North Ohio Heart, Inc. Disclosures Speaker Gilead Sciences NHLBI Charge to the Expert Panel Evaluate higher quality
2013 ACC/AHA Cholesterol Guidelines JULIE HAMMOND, D.O. PGY-2 MATTHEW PAOLI, D.O. PGY-2
 2013 ACC/AHA Cholesterol Guidelines JULIE HAMMOND, D.O. PGY-2 MATTHEW PAOLI, D.O. PGY-2 GOALS ACC/AHA as publisher of guidelines Determining which patients are appropriate for statin therapy The treatment
2013 ACC/AHA Cholesterol Guidelines JULIE HAMMOND, D.O. PGY-2 MATTHEW PAOLI, D.O. PGY-2 GOALS ACC/AHA as publisher of guidelines Determining which patients are appropriate for statin therapy The treatment
Highlights of the new blood pressure and cholesterol guidelines: A whole new philosophy. Jeremy L. Johnson, PharmD, BCACP, CDE, BC-ADM
 Highlights of the new blood pressure and cholesterol guidelines: A whole new philosophy Jeremy L. Johnson, PharmD, BCACP, CDE, BC-ADM OSHP 2014 Annual Meeting Oklahoma City, OK April 4, 2014 1 Objectives
Highlights of the new blood pressure and cholesterol guidelines: A whole new philosophy Jeremy L. Johnson, PharmD, BCACP, CDE, BC-ADM OSHP 2014 Annual Meeting Oklahoma City, OK April 4, 2014 1 Objectives
CVD risk assessment using risk scores in primary and secondary prevention
 CVD risk assessment using risk scores in primary and secondary prevention Raul D. Santos MD, PhD Heart Institute-InCor University of Sao Paulo Brazil Disclosure Honoraria for consulting and speaker activities
CVD risk assessment using risk scores in primary and secondary prevention Raul D. Santos MD, PhD Heart Institute-InCor University of Sao Paulo Brazil Disclosure Honoraria for consulting and speaker activities
Disclosures. Prevention of Heart Disease: The New Guidelines. Summary of Talk. Four guidelines. No relevant disclosures.
 Disclosures Prevention of Heart Disease: The New Guidelines No relevant disclosures Nisha I. Parikh MD MPH Assistant Professor of Medicine Division of Cardiology Department of Medicine University of California
Disclosures Prevention of Heart Disease: The New Guidelines No relevant disclosures Nisha I. Parikh MD MPH Assistant Professor of Medicine Division of Cardiology Department of Medicine University of California
Lipid Therapy: Statins and Beyond. Ivan Anderson, MD RIHVH Cardiology
 Lipid Therapy: Statins and Beyond Ivan Anderson, MD RIHVH Cardiology Outline The cholesterol hypothesis and lipid metabolism The Guidelines 4 Groups that Benefit from Lipid therapy Initiation and monitoring
Lipid Therapy: Statins and Beyond Ivan Anderson, MD RIHVH Cardiology Outline The cholesterol hypothesis and lipid metabolism The Guidelines 4 Groups that Benefit from Lipid therapy Initiation and monitoring
Disclosure. No relevant financial relationships. Placebo-Controlled Statin Trials
 MANAGEMENT OF HYPERLIPIDEMIA AND CARDIOVASCULAR RISK IN WOMEN: Balancing Benefits and Harms Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial
MANAGEMENT OF HYPERLIPIDEMIA AND CARDIOVASCULAR RISK IN WOMEN: Balancing Benefits and Harms Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial
Cholesterol Management Roy Gandolfi, MD
 Cholesterol Management 2017 Roy Gandolfi, MD Goals Interpreting cholesterol guidelines Cholesterol treatment in diabetics Statin use and side effects therapy Reporting- Comparison data among physicians
Cholesterol Management 2017 Roy Gandolfi, MD Goals Interpreting cholesterol guidelines Cholesterol treatment in diabetics Statin use and side effects therapy Reporting- Comparison data among physicians
New Cholesterol Guidelines What the LDL are we supposed to do now?!
 New Cholesterol Guidelines What the LDL are we supposed to do now?! Michael D. Shapiro Assistant Professor of Medicine and Radiology Knight Cardiovascular Institute Oregon Health & Science University 2013
New Cholesterol Guidelines What the LDL are we supposed to do now?! Michael D. Shapiro Assistant Professor of Medicine and Radiology Knight Cardiovascular Institute Oregon Health & Science University 2013
ATP IV: Predicting Guideline Updates
 Disclosures ATP IV: Predicting Guideline Updates Daniel M. Riche, Pharm.D., BCPS, CDE Speaker s Bureau Merck Janssen Boehringer-Ingelheim Learning Objectives Describe at least two evidence-based recommendations
Disclosures ATP IV: Predicting Guideline Updates Daniel M. Riche, Pharm.D., BCPS, CDE Speaker s Bureau Merck Janssen Boehringer-Ingelheim Learning Objectives Describe at least two evidence-based recommendations
FORTH VALLEY. LIPID LOWERING GUIDELINE v5 2016
 FORTH VALLEY LIPID LOWERING GUIDELINE v5 2016 This guideline applies to people over 16 years of age. This guideline is not intended to serve as a standard of medical care or be applicable in every situation.
FORTH VALLEY LIPID LOWERING GUIDELINE v5 2016 This guideline applies to people over 16 years of age. This guideline is not intended to serve as a standard of medical care or be applicable in every situation.
Prevention Updates and Paradigm Shifts
 Prevention Updates and Paradigm Shifts Andrew Freeman, MD, FACC Director of Clinical Cardiology and Operations National Jewish Health Assistant Professor of Medicine National Jewish Health and University
Prevention Updates and Paradigm Shifts Andrew Freeman, MD, FACC Director of Clinical Cardiology and Operations National Jewish Health Assistant Professor of Medicine National Jewish Health and University
Dyslipidemia and Combination Therapy: A Framework for Clinical Decision Making
 Dyslipidemia and Combination Therapy: A Framework for Clinical Decision Making Shashank Sinha, MD Pamela B. Morris, MD, FACC 8 October 2016 Mexico City Introduction: Pamela B. Morris, MD, FACC COMING TO
Dyslipidemia and Combination Therapy: A Framework for Clinical Decision Making Shashank Sinha, MD Pamela B. Morris, MD, FACC 8 October 2016 Mexico City Introduction: Pamela B. Morris, MD, FACC COMING TO
Disclosures. Overview 9/30/ ACC/AHA Guidelines on the Treatment of Blood Cholesterol to Reduce Atherosclerotic Cardiovascular Risk in Adults
 2013 ACC/AHA Guidelines on the Treatment of Blood Cholesterol to Reduce Atherosclerotic Cardiovascular Risk in Adults 2014 AAHP Fall Seminar Sherry Myatt, PharmD, BCPS Assistant Director of Pharmacy for
2013 ACC/AHA Guidelines on the Treatment of Blood Cholesterol to Reduce Atherosclerotic Cardiovascular Risk in Adults 2014 AAHP Fall Seminar Sherry Myatt, PharmD, BCPS Assistant Director of Pharmacy for
Disclosures No relationships (not even to an employer) No off-label uses. Cholesterol Lowering Guidelines: What now?
 No off-label uses. Cholesterol Lowering Guidelines: What now?") Disclosures No relationships (not even to an employer) No off-label uses Cholesterol Lowering Guidelines: What now?, FACP 1 2 65-year-old white woman Total cholesterol 175mg/dL HDL 54 mg/dl LDL 96 mg/dl
Disclosures No relationships (not even to an employer) No off-label uses Cholesterol Lowering Guidelines: What now?, FACP 1 2 65-year-old white woman Total cholesterol 175mg/dL HDL 54 mg/dl LDL 96 mg/dl
HYPERLIPIDEMIA IN THE OLDER POPULATION NICOLE SLATER, PHARMD, BCACP AUBURN UNIVERSITY, HARRISON SCHOOL OF PHARMACY JULY 16, 2016
 HYPERLIPIDEMIA IN THE OLDER POPULATION NICOLE SLATER, PHARMD, BCACP AUBURN UNIVERSITY, HARRISON SCHOOL OF PHARMACY JULY 16, 2016 NOTHING TO DISCLOSE I, Nicole Slater, have no actual or potential conflict
HYPERLIPIDEMIA IN THE OLDER POPULATION NICOLE SLATER, PHARMD, BCACP AUBURN UNIVERSITY, HARRISON SCHOOL OF PHARMACY JULY 16, 2016 NOTHING TO DISCLOSE I, Nicole Slater, have no actual or potential conflict
Disclosure. No relevant financial relationships. Placebo-Controlled Statin Trials
 PREVENTING CARDIOVASCULAR DISEASE IN WOMEN: Current Guidelines for Hypertension, Lipids and Aspirin Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial
PREVENTING CARDIOVASCULAR DISEASE IN WOMEN: Current Guidelines for Hypertension, Lipids and Aspirin Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial
Prevention of Cardiovascular Disease
 Save Thais from Heart Diseases 2019 Prevention of Cardiovascular Disease Orawan Anupraiwan, MD. Central Chest Institute of Thailand ASCVD Prevention Pyramid Risk categories Very high-risk High-risk Documented
Save Thais from Heart Diseases 2019 Prevention of Cardiovascular Disease Orawan Anupraiwan, MD. Central Chest Institute of Thailand ASCVD Prevention Pyramid Risk categories Very high-risk High-risk Documented
NEW GUIDELINES FOR CHOLESTEROL
 NEW GUIDELINES FOR CHOLESTEROL NEW CHOLESTEROL GUIDELINES 2013 Recently updated guidelines for the treatment of high blood cholesterol levels is a major update since 2002. The news media have trumpeted
NEW GUIDELINES FOR CHOLESTEROL NEW CHOLESTEROL GUIDELINES 2013 Recently updated guidelines for the treatment of high blood cholesterol levels is a major update since 2002. The news media have trumpeted
2016 EUROPEAN GUIDELINES ON CVD PREVENTION IN CLINICAL PRACTICE
 2016 EUROPEAN GUIDELINES ON CVD PREVENTION IN CLINICAL PRACTICE Massimo F Piepoli, MD, PhD, FESC, Piacenza, Italy on behalf of the 6 th Joint Task Force 2 3 Guidelines still based upon the principles of
2016 EUROPEAN GUIDELINES ON CVD PREVENTION IN CLINICAL PRACTICE Massimo F Piepoli, MD, PhD, FESC, Piacenza, Italy on behalf of the 6 th Joint Task Force 2 3 Guidelines still based upon the principles of
Cardiovascular Risk and Dyslipidemia Management Clinician Guide SEPTEMBER 2017
 Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Cardiovascular Risk and Dyslipidemia Management Clinician Guide SEPTEMBER 2017 Introduction This Clinician Guide is based on the 2017 KP National
Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Cardiovascular Risk and Dyslipidemia Management Clinician Guide SEPTEMBER 2017 Introduction This Clinician Guide is based on the 2017 KP National
Placebo-Controlled Statin Trials EXPLAINING THE DECREASE IN DEATHS FROM CHD! PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN EXPLAINING THE DECREASE IN
 PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest EXPLAINING THE DECREASE
PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest EXPLAINING THE DECREASE
No relevant financial relationships
 MANAGEMENT OF LIPID DISORDERS: WHERE DO WE STAND WITH THE NEW PRACTICE GUIDELINES? Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Disclosure No relevant financial relationships
MANAGEMENT OF LIPID DISORDERS: WHERE DO WE STAND WITH THE NEW PRACTICE GUIDELINES? Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Disclosure No relevant financial relationships
Deep Dive into Contemporary Cholesterol Management. Kim Allan Williams, Sr., MD, FACC Pamela B. Morris, MD, FACC 7 October 2016 Mexico City
 Deep Dive into Contemporary Cholesterol Management Kim Allan Williams, Sr., MD, FACC Pamela B. Morris, MD, FACC 7 October 2016 Mexico City Introduction: Pamela B. Morris, MD, FACC COMING TO CONSENSUS IN
Deep Dive into Contemporary Cholesterol Management Kim Allan Williams, Sr., MD, FACC Pamela B. Morris, MD, FACC 7 October 2016 Mexico City Introduction: Pamela B. Morris, MD, FACC COMING TO CONSENSUS IN
Considerations and Controversies in the Management of Dyslipidemia for ASCVD Risk Reduction
 Considerations and Controversies in the Management of Dyslipidemia for ASCVD Risk Reduction Pamela B. Morris, MD, FACC, FAHA, FASCP, FNLA Chair, ACC Prevention of Cardiovascular Disease Council The Medical
Considerations and Controversies in the Management of Dyslipidemia for ASCVD Risk Reduction Pamela B. Morris, MD, FACC, FAHA, FASCP, FNLA Chair, ACC Prevention of Cardiovascular Disease Council The Medical
2.3 CONTACT HOURS. Managing. By Kristine Anne Scordo, PhD, RN, ACNP-BC, FAANP
 2.3 CONTACT HOURS 2.3 CONTACT HOURS Managing hyperlipidemia The updated cholesterol treatment guidelines Abstract: The ACC/AHA 2013 cholesterol treatment guidelines focus on lowering the risk of heart
2.3 CONTACT HOURS 2.3 CONTACT HOURS Managing hyperlipidemia The updated cholesterol treatment guidelines Abstract: The ACC/AHA 2013 cholesterol treatment guidelines focus on lowering the risk of heart
ACC/AHA GUIDELINES ON LIPIDS AND PCSK9 INHIBITORS
 ACC/AHA GUIDELINES ON LIPIDS AND PCSK9 INHIBITORS Ziyad Ghazzal MD, FACC, FSCAI Professor of Medicine Deputy Vice President/Dean Associate Dean for Clinical Affairs American University of Beirut Adjunct
ACC/AHA GUIDELINES ON LIPIDS AND PCSK9 INHIBITORS Ziyad Ghazzal MD, FACC, FSCAI Professor of Medicine Deputy Vice President/Dean Associate Dean for Clinical Affairs American University of Beirut Adjunct
Andrew Cohen, MD and Neil S. Skolnik, MD INTRODUCTION
 2 Hyperlipidemia Andrew Cohen, MD and Neil S. Skolnik, MD CONTENTS INTRODUCTION RISK CATEGORIES AND TARGET LDL-CHOLESTEROL TREATMENT OF LDL-CHOLESTEROL SPECIAL CONSIDERATIONS OLDER AND YOUNGER ADULTS ADDITIONAL
2 Hyperlipidemia Andrew Cohen, MD and Neil S. Skolnik, MD CONTENTS INTRODUCTION RISK CATEGORIES AND TARGET LDL-CHOLESTEROL TREATMENT OF LDL-CHOLESTEROL SPECIAL CONSIDERATIONS OLDER AND YOUNGER ADULTS ADDITIONAL
Update on Cholesterol Management: The 2013 ACC/AHA Guidelines
 Update on Cholesterol Management: The 2013 ACC/AHA Guidelines Ola Akinboboye MD MPH MBA Medical Director, Queens Heart institute Rosedale. Associate Professor of Clinical Medicine, Weill Medical College
Update on Cholesterol Management: The 2013 ACC/AHA Guidelines Ola Akinboboye MD MPH MBA Medical Director, Queens Heart institute Rosedale. Associate Professor of Clinical Medicine, Weill Medical College
Applying the Intricacies of the New Hypertension and Lipid Guidelines to Your Patients
 Applying the Intricacies of the New Hypertension and Lipid Guidelines to Your Patients Joe Anderson, PharmD, PhC, BCPS James Nawarskas, PharmD, PhC, BCPS Gretchen Ray, PharmD, PhC, BCACP University of
Applying the Intricacies of the New Hypertension and Lipid Guidelines to Your Patients Joe Anderson, PharmD, PhC, BCPS James Nawarskas, PharmD, PhC, BCPS Gretchen Ray, PharmD, PhC, BCACP University of
4 th and Goal To Go How Low Should We Go? :
 4 th and Goal To Go How Low Should We Go? : Evaluating New Lipid Lowering Therapies Catherine Bourg Rebitch, PharmD, BCACP Clinical Associate Professor Disclosure The presenter has nothing to disclose
4 th and Goal To Go How Low Should We Go? : Evaluating New Lipid Lowering Therapies Catherine Bourg Rebitch, PharmD, BCACP Clinical Associate Professor Disclosure The presenter has nothing to disclose
THE ESC/EAS LIPID GUIDELINES IN THE ELDERLY
 THE ESC/EAS LIPID GUIDELINES IN THE ELDERLY Alberico L. Catapano alberico.catapano@unimi.it Alberico L. Catapano Potential Conflict Of Interest Prof. Catapano has received honoraria, lecture fees, or research
THE ESC/EAS LIPID GUIDELINES IN THE ELDERLY Alberico L. Catapano alberico.catapano@unimi.it Alberico L. Catapano Potential Conflict Of Interest Prof. Catapano has received honoraria, lecture fees, or research
Management of Post-transplant hyperlipidemia
 Management of Post-transplant hyperlipidemia B. Gisella Carranza Leon, MD Assistant Professor of Medicine Lipid Clinic - Vanderbilt Heart and Vascular Institute Division of Diabetes, Endocrinology and
Management of Post-transplant hyperlipidemia B. Gisella Carranza Leon, MD Assistant Professor of Medicine Lipid Clinic - Vanderbilt Heart and Vascular Institute Division of Diabetes, Endocrinology and
Sanger Heart & Vascular Institute Symposium 2015
 Sanger Heart & Vascular Institute Symposium 2015 Cardiovascular Update For Primary Care Physicians William E. Downey, MD FACC FSCAI Medical Director, Interventional Cardiology Sanger Heart & Vascular Institute
Sanger Heart & Vascular Institute Symposium 2015 Cardiovascular Update For Primary Care Physicians William E. Downey, MD FACC FSCAI Medical Director, Interventional Cardiology Sanger Heart & Vascular Institute
PCSK9 Agents Drug Class Prior Authorization Protocol
 PCSK9 Agents Drug Class Prior Authorization Protocol Line of Business: Medicaid P & T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has been developed through review of medical
PCSK9 Agents Drug Class Prior Authorization Protocol Line of Business: Medicaid P & T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has been developed through review of medical
Young high risk patients the role of statins Dr. Mohamed Jeilan
 Young high risk patients the role of statins Dr. Mohamed Jeilan KCS Congress: Impact through collaboration CONTACT: Tel. +254 735 833 803 Email: kcardiacs@gmail.com Web: www.kenyacardiacs.org Disclosures
Young high risk patients the role of statins Dr. Mohamed Jeilan KCS Congress: Impact through collaboration CONTACT: Tel. +254 735 833 803 Email: kcardiacs@gmail.com Web: www.kenyacardiacs.org Disclosures
MOLINA HEALTHCARE OF CALIFORNIA
 MOLINA HEALTHCARE OF CALIFORNIA HIGH BLOOD CHOLESTEROL IN ADULTS GUIDELINE Molina Healthcare of California has adopted the Third Report of the National Cholesterol Education Program (NCEP) Expert Panel
MOLINA HEALTHCARE OF CALIFORNIA HIGH BLOOD CHOLESTEROL IN ADULTS GUIDELINE Molina Healthcare of California has adopted the Third Report of the National Cholesterol Education Program (NCEP) Expert Panel
CVD Risk Assessment. Michal Vrablík Charles University, Prague Czech Republic
 CVD Risk Assessment Michal Vrablík Charles University, Prague Czech Republic What is Risk? A cumulative probability of an event, usually expressed as percentage e.g.: 5 CV events in 00 pts = 5% risk This
CVD Risk Assessment Michal Vrablík Charles University, Prague Czech Republic What is Risk? A cumulative probability of an event, usually expressed as percentage e.g.: 5 CV events in 00 pts = 5% risk This
Hypertension Guidelines: JNC- Late, JNC- 8, or JNC- Fake?
 Hypertension Guidelines: JNC- Late, JNC- 8, or JNC- Fake? Brian G. Choi, MD, MBA, FACC Associate Professor of Medicine Co-Director, Advanced Cardiac Imaging November 14, 2014 Washington, DC Disclosures
Hypertension Guidelines: JNC- Late, JNC- 8, or JNC- Fake? Brian G. Choi, MD, MBA, FACC Associate Professor of Medicine Co-Director, Advanced Cardiac Imaging November 14, 2014 Washington, DC Disclosures
American Diabetes Association 2018 Guidelines Important Notable Points
 American Diabetes Association 2018 Guidelines Important Notable Points The Standards of Medical Care in Diabetes-2018 by ADA include the most current evidencebased recommendations for diagnosing and treating
American Diabetes Association 2018 Guidelines Important Notable Points The Standards of Medical Care in Diabetes-2018 by ADA include the most current evidencebased recommendations for diagnosing and treating
PIEDMONT ACCESS TO HEALTH SERVICES, INC. Guidelines for Screening and Management of Dyslipidemia
 PIEDMONT ACCESS TO HEALTH SERVICES, INC. Policy Number: 01-09-021 SUBJECT: Guidelines for Screening and Management of Dyslipidemia EFFECTIVE DATE: 04/2008 REVIEWED/REVISED: 04/12/10, 03/17/2011, 4/10/2012,
PIEDMONT ACCESS TO HEALTH SERVICES, INC. Policy Number: 01-09-021 SUBJECT: Guidelines for Screening and Management of Dyslipidemia EFFECTIVE DATE: 04/2008 REVIEWED/REVISED: 04/12/10, 03/17/2011, 4/10/2012,
PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN
 PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest EXPLAINING THE DECREASE
PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest EXPLAINING THE DECREASE
Conflicts of interest. What's the Skinny on the Lipid Guidelines? Key Differences. Are you applying the new ACC/AHA Lipid guidelines in your practice?
 Conflicts of interest What's the Skinny on the Lipid Guidelines? The presenter has no relevant conflicts of interest to disclose. Kathleen Vest, PharmD, CDE, BCACP At the end of this presentation, pharmacist
Conflicts of interest What's the Skinny on the Lipid Guidelines? The presenter has no relevant conflicts of interest to disclose. Kathleen Vest, PharmD, CDE, BCACP At the end of this presentation, pharmacist
Diabetes: Use of Adjunctive Therapy ACEs, ARBs, ASA & STATINs --Oh My! Veronica J. Brady, PhD, FNP-BC, BC-ADM, CDE Project ECHO April 19, 2018
 Diabetes: Use of Adjunctive Therapy ACEs, ARBs, ASA & STATINs --Oh My! Veronica J. Brady, PhD, FNP-BC, BC-ADM, CDE Project ECHO April 19, 2018 Points to Ponder ASCVD is the leading cause of morbidity
Diabetes: Use of Adjunctive Therapy ACEs, ARBs, ASA & STATINs --Oh My! Veronica J. Brady, PhD, FNP-BC, BC-ADM, CDE Project ECHO April 19, 2018 Points to Ponder ASCVD is the leading cause of morbidity
When Statins Aren t Enough: Appropriate Therapies for High-Risk Patients with Diabetes
 When Statins Aren t Enough: Appropriate Therapies for High-Risk Patients with Diabetes Kim K. Birtcher, MS, PharmD, AACC, FNLA, CLS, BCPS (AQ-Cardiology), CDE Clinical Professor University of Houston College
When Statins Aren t Enough: Appropriate Therapies for High-Risk Patients with Diabetes Kim K. Birtcher, MS, PharmD, AACC, FNLA, CLS, BCPS (AQ-Cardiology), CDE Clinical Professor University of Houston College
Copyright 2017 by Sea Courses Inc.
 Diabetes and Lipids Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any means graphic, electronic, or
Diabetes and Lipids Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any means graphic, electronic, or
Speaker Disclosure. Pharmacist Objectives. Path to New Hypertension (HTN) Guidelines. Overview of New HTN Guidelines 8/21/2014
 Guidelines. Overview of New HTN Guidelines 8/21/2014") Speaker Disclosure Erica Pearce, Pharm.D. declares no conflicts of interest, real or apparent, and no financial interests in any company, product, or service mentioned in this program, including grants,
Speaker Disclosure Erica Pearce, Pharm.D. declares no conflicts of interest, real or apparent, and no financial interests in any company, product, or service mentioned in this program, including grants,
Clinical Policy: Lomitapide (Juxtapid) Reference Number: ERX.SPA.170 Effective Date:
 Reference Number: ERX.SPA.170 Effective Date:") Clinical Policy: (Juxtapid) Reference Number: ERX.SPA.170 Effective Date: 01.11.17 Last Review Date: 11.17 Revision Log See Important Reminder at the end of this policy for important regulatory and legal
Clinical Policy: (Juxtapid) Reference Number: ERX.SPA.170 Effective Date: 01.11.17 Last Review Date: 11.17 Revision Log See Important Reminder at the end of this policy for important regulatory and legal
CPE Session 7. Update on Clinical Practice Guidelines and Best Evidence in the Management of Hyperlipidemia and Cardiovascular Risk Reduction
 CPE Session 7 Update on Clinical Practice Guidelines and Best Evidence in the Management of Hyperlipidemia and Cardiovascular Risk Reduction Saturday, April 25, 2015 ACPE UAN 0128-0000-15-027-L01-P 1.0
CPE Session 7 Update on Clinical Practice Guidelines and Best Evidence in the Management of Hyperlipidemia and Cardiovascular Risk Reduction Saturday, April 25, 2015 ACPE UAN 0128-0000-15-027-L01-P 1.0
Vincent J. Caracciolo, MD FACC FOMA May 2014
 Vincent J. Caracciolo, MD FACC FOMA May 2014 Goals of the Guidelines National Heart, lung and Blood Institute ( NHLBI) collaborated with ACC/AHA to develop guidelines a.) assess CV risk, b.) lifestyle
Vincent J. Caracciolo, MD FACC FOMA May 2014 Goals of the Guidelines National Heart, lung and Blood Institute ( NHLBI) collaborated with ACC/AHA to develop guidelines a.) assess CV risk, b.) lifestyle
DYSLIPIDEMIA TREATMENT: HYBRIDIZING CLINICAL PRACTICE GUIDELINES
 DYSLIPIDEMIA TREATMENT: HYBRIDIZING CLINICAL PRACTICE GUIDELINES SATURDAY/4:30-5:30PM ACPE UAN: 0107-9999-17-249-L01-P 0.1 CEU/1.0 hr Activity Type: Knowledge-Based Learning Objectives for Pharmacists:
DYSLIPIDEMIA TREATMENT: HYBRIDIZING CLINICAL PRACTICE GUIDELINES SATURDAY/4:30-5:30PM ACPE UAN: 0107-9999-17-249-L01-P 0.1 CEU/1.0 hr Activity Type: Knowledge-Based Learning Objectives for Pharmacists:
Pharmaceutical Help to Control Cholesterol
 Pharmaceutical Help to Control Cholesterol Catherine E. Cooke, PharmD, BCPS, PAHM President, PosiHealth, Inc. Clinical Associate Professor, Univ. of Maryland This program has been brought to you by PharmCon
Pharmaceutical Help to Control Cholesterol Catherine E. Cooke, PharmD, BCPS, PAHM President, PosiHealth, Inc. Clinical Associate Professor, Univ. of Maryland This program has been brought to you by PharmCon
Coronary Heart Disease and Stroke, Primary and Secondary Prevention Guidelines (Cholesterol)
") CLINICAL GUIDELINE Coronary Heart Disease and Stroke, Primary and Secondary Prevention Guidelines (Cholesterol) A guideline is intended to assist healthcare professionals in the choice of disease-specific
CLINICAL GUIDELINE Coronary Heart Disease and Stroke, Primary and Secondary Prevention Guidelines (Cholesterol) A guideline is intended to assist healthcare professionals in the choice of disease-specific
Disclosure. A New Partnership. Objectives 03/27/2014. What is the main way you have obtained information about the 2013 ACC/AHA Cholesterol Guideline?
 Disclosure Lindsey Clark, PharmD, BCPS Cardiology-Medicine Pharmacy Specialist University of Cincinnati Medical Center April 10, 2014 I, Lindsey Clark, do not have a financial interest or affiliation with
Disclosure Lindsey Clark, PharmD, BCPS Cardiology-Medicine Pharmacy Specialist University of Cincinnati Medical Center April 10, 2014 I, Lindsey Clark, do not have a financial interest or affiliation with
Royal Wolverhampton Hospital Adult Lipid Lowering Therapy Guidelines Lipid Lowering Therapy for the Prevention of Cardiovascular Disease
 Royal Wolverhampton Hospital Adult Lipid Lowering Therapy Guidelines 1 This guideline is intended to assist rational and cost-effective prescribing of lipid regulating medications across both primary and
Royal Wolverhampton Hospital Adult Lipid Lowering Therapy Guidelines 1 This guideline is intended to assist rational and cost-effective prescribing of lipid regulating medications across both primary and
Lipids & Hypertension Update
 Lipids & Hypertension Update No financial disclosures Michael W. Cullen, MD, FACC Senior Associate Consultant, Assistant Professor of Medicine Mayo Clinic Department of Cardiovascular Diseases 34 th Annual
Lipids & Hypertension Update No financial disclosures Michael W. Cullen, MD, FACC Senior Associate Consultant, Assistant Professor of Medicine Mayo Clinic Department of Cardiovascular Diseases 34 th Annual
2/10/2016. Perspectives on the 2013 ACC/AHA Cholesterol Guidelines. Disclosures. ATP-III Update 2004
 Perspectives on the 2013 ACC/AHA Cholesterol Guidelines Donald M. Lloyd-Jones, MD ScM Senior Associate Dean Chair and Professor of Preventive Medicine Northwestern Feinberg School of Medicine Disclosures
Perspectives on the 2013 ACC/AHA Cholesterol Guidelines Donald M. Lloyd-Jones, MD ScM Senior Associate Dean Chair and Professor of Preventive Medicine Northwestern Feinberg School of Medicine Disclosures
Management of Lipid Disorders and Hypertension: Implications of the New Guidelines
 Management of Lipid Disorders and Hypertension Management of Lipid Disorders and Hypertension: Implications of the New Guidelines Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine
Management of Lipid Disorders and Hypertension Management of Lipid Disorders and Hypertension: Implications of the New Guidelines Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine
Death is inevitable but premature death is not. Sir Richard Doll
 Welcome to the Diabetes Care for You webinar Please log onto the conference call so you can hear our presenter From any SCFT Cisco phone dial 800800 From a mobile phone or any other phone dial 01273 242
Welcome to the Diabetes Care for You webinar Please log onto the conference call so you can hear our presenter From any SCFT Cisco phone dial 800800 From a mobile phone or any other phone dial 01273 242
Chapter 2: Pharmacological cholesterol-lowering treatment in adults Kidney International Supplements (2013) 3, ; doi: /kisup.2013.
 3, ; doi: /kisup.2013.") http://www.kidney-international.org chapter & 3 KDIGO Chapter : Pharmacological cholesterol-lowering treatment in adults Kidney International Supplements (3) 3, 7 79; doi:.38/kisup.3.34 INTRODUCTION Therapeutic
http://www.kidney-international.org chapter & 3 KDIGO Chapter : Pharmacological cholesterol-lowering treatment in adults Kidney International Supplements (3) 3, 7 79; doi:.38/kisup.3.34 INTRODUCTION Therapeutic
Placebo-Controlled Statin Trials Prevention Of CVD in Women"
 MANAGEMENT OF HIGH BLOOD CHOLESTEROL: IMPLICATIONS OF THE NEW GUIDELINES Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest
MANAGEMENT OF HIGH BLOOD CHOLESTEROL: IMPLICATIONS OF THE NEW GUIDELINES Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest
Placebo-Controlled Statin Trials
 PREVENTION OF CHD WITH LIPID MANAGEMENT AND ASPIRIN: MATCHING TREATMENT TO RISK Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of
PREVENTION OF CHD WITH LIPID MANAGEMENT AND ASPIRIN: MATCHING TREATMENT TO RISK Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of
APPENDIX 2F Management of Cholesterol
 Patients with established CVD: Coronary heart disease Cerebrovascular disease Peripheral vascular disease APPEDIX 2F Management of Cholesterol Patients at high risk of cardiovascular events: Chronic kidney
Patients with established CVD: Coronary heart disease Cerebrovascular disease Peripheral vascular disease APPEDIX 2F Management of Cholesterol Patients at high risk of cardiovascular events: Chronic kidney
Placebo-Controlled Statin Trials MANAGEMENT OF HIGH BLOOD CHOLESTEROL MANAGEMENT OF HIGH BLOOD CHOLESTEROL: IMPLICATIONS OF THE NEW GUIDELINES
 MANAGEMENT OF HIGH BLOOD CHOLESTEROL: IMPLICATIONS OF THE NEW GUIDELINES Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest
MANAGEMENT OF HIGH BLOOD CHOLESTEROL: IMPLICATIONS OF THE NEW GUIDELINES Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest
Landmesser U et al. Eur Heart J 2017; https://doi.org/ /eurheartj/ehx549
 2017 Update of ESC/EAS Task Force on Practical Clinical Guidance for PCSK9 inhibition in Patients with Atherosclerotic Cardiovascular Disease or in Familial Hypercholesterolaemia Cardiovascular Outcomes
2017 Update of ESC/EAS Task Force on Practical Clinical Guidance for PCSK9 inhibition in Patients with Atherosclerotic Cardiovascular Disease or in Familial Hypercholesterolaemia Cardiovascular Outcomes
See Important Reminder at the end of this policy for important regulatory and legal information.
 Clinical Policy: (Repatha) Reference Number: HIM.PA.SP46 Effective Date: 01.01.18 Last Review Date: Line of Business: Health Insurance Marketplace Revision Log See Important Reminder at the end of this
Clinical Policy: (Repatha) Reference Number: HIM.PA.SP46 Effective Date: 01.01.18 Last Review Date: Line of Business: Health Insurance Marketplace Revision Log See Important Reminder at the end of this
Supplementary Online Content
 Supplementary Online Content Kavousi M, Leening MJG, Nanchen D, et al. Comparison of application of the ACC/AHA guidelines, Adult Treatment Panel III guidelines, and European Society of Cardiology guidelines
Supplementary Online Content Kavousi M, Leening MJG, Nanchen D, et al. Comparison of application of the ACC/AHA guidelines, Adult Treatment Panel III guidelines, and European Society of Cardiology guidelines
Implementation of CV Risk and. Dyslipidemia Guidelines. Impact on Americans 11/25/2014. Summary Implementing new. Dyslipidemia Guidelines
 Summary Implementing new Dyslipidemia Guidelines Implementation of CV Risk and Dyslipidemia Guidelines Ronald D. Scott, MD Regional KPSC CVD Co-Lead Family Medicine and Lipidology, WLA ASCVD (Atherosclerotic
Summary Implementing new Dyslipidemia Guidelines Implementation of CV Risk and Dyslipidemia Guidelines Ronald D. Scott, MD Regional KPSC CVD Co-Lead Family Medicine and Lipidology, WLA ASCVD (Atherosclerotic
Disclosures. Diabetes and Cardiovascular Risk Management. Learning Objectives. Atherosclerotic Cardiovascular Disease
 Disclosures Diabetes and Cardiovascular Risk Management Tony Hampton, MD, MBA Medical Director Advocate Aurora Operating System Advocate Aurora Healthcare Downers Grove, IL No conflicts or disclosures
Disclosures Diabetes and Cardiovascular Risk Management Tony Hampton, MD, MBA Medical Director Advocate Aurora Operating System Advocate Aurora Healthcare Downers Grove, IL No conflicts or disclosures
Approach to Dyslipidemia among diabetic patients
 Approach to Dyslipidemia among diabetic patients Farzad Hadaegh, MD, Professor of Internal Medicine & Endocrinology Prevention of Metabolic Disorders Research Center, Research Institute for Endocrine Sciences
Approach to Dyslipidemia among diabetic patients Farzad Hadaegh, MD, Professor of Internal Medicine & Endocrinology Prevention of Metabolic Disorders Research Center, Research Institute for Endocrine Sciences
PCSK9 Inhibitors Praluent (Alirocumab) and Repatha (Evolocumab) For the Treatment of Familial Hypercholesterolemia
 and Repatha (Evolocumab) For the Treatment of Familial Hypercholesterolemia") PCSK9 Inhibitors Praluent (Alirocumab) and Repatha (Evolocumab) For the Treatment of Familial Hypercholesterolemia Policy Number: Original Effective Date: MM.04.037 08/01/2016 Line(s) of Business: HMO;
PCSK9 Inhibitors Praluent (Alirocumab) and Repatha (Evolocumab) For the Treatment of Familial Hypercholesterolemia Policy Number: Original Effective Date: MM.04.037 08/01/2016 Line(s) of Business: HMO;
What have We Learned in Dyslipidemia Management Since the Publication of the 2013 ACC/AHA Guideline?
 What have We Learned in Dyslipidemia Management Since the Publication of the 2013 ACC/AHA Guideline? Salim S. Virani, MD, PhD, FACC, FAHA Associate Professor, Section of Cardiovascular Research Baylor
What have We Learned in Dyslipidemia Management Since the Publication of the 2013 ACC/AHA Guideline? Salim S. Virani, MD, PhD, FACC, FAHA Associate Professor, Section of Cardiovascular Research Baylor
Pamela B. Morris, MD, FACC, FAHA, FASPC, FNLA
 2017 Focused Update of the 2016 ACC Expert Consensus Decision Pathway on the Role of Non-statin Therapies for LDL-C Lowering in the Management of ASCVD Risk Pamela B. Morris, MD, FACC, FAHA, FASPC, FNLA
2017 Focused Update of the 2016 ACC Expert Consensus Decision Pathway on the Role of Non-statin Therapies for LDL-C Lowering in the Management of ASCVD Risk Pamela B. Morris, MD, FACC, FAHA, FASPC, FNLA