Identification and management of familial hypercholesterolaemia (FH) - An overview
|
|
|
- Shannon Cook
- 6 years ago
- Views:
Transcription
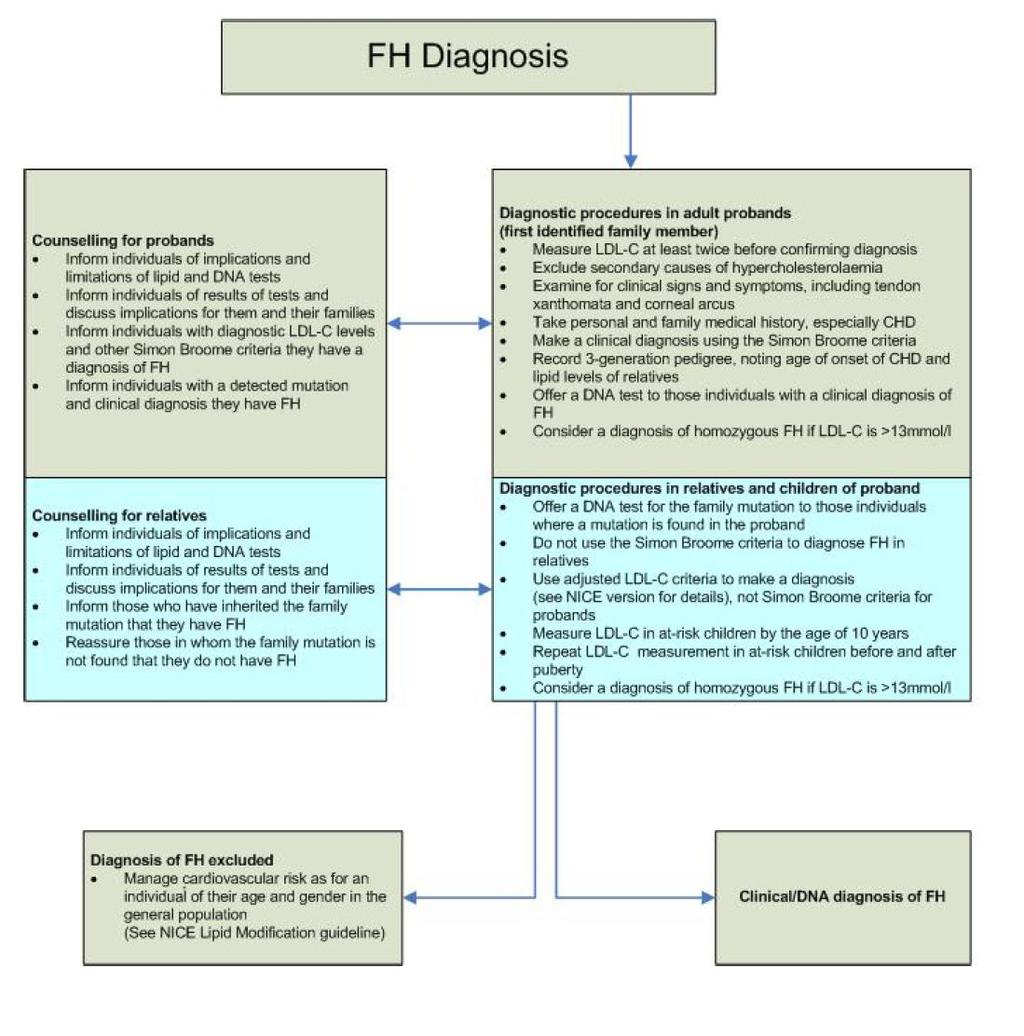
1 Identification and management of familial hypercholesterolaemia (FH) - An overview National Collaborating Centre for Primary Care and Royal College of General Practitioners NICE Guideline CG 71 (August 2008)
2 Prevalence of Primary Dyslipidaemias Hypercholesterolaemia Familial (approx. 1 in 500) Polygenic (common, 1 in 50) Hypertriglyceridaemia Familial lipoprotein lipase deficiency (approx. 1 in 1,000,000) Familial apolipoprotein CII deficiency (approx. 1 in 1,000,000) Familial Hypertriglyceridaemia (approx. 1 in 100) Combined Hyperlipidaemia Familial combined hyperlipidaemia (approx. 1 in 100) Familial Type III (Remnant) Hyperlipidaemia (approx. 1 in 5,000)
3 Family History 1990 I II 10.3 Index Case?chol III 25 yrs? chol 27 yrs? chol
4 Second Degree Relatives of FH Proband LDL Cholesterol Distribution

5 Corneal Arcus Lipidus

6 Achilles Tendon Xanthoma

7 The LDL-receptor pathway Soutar, A Nat Clin Pract Cardiovasc Med 2006; 4:214
8 LDLR gene mutations Soutar, A Nat Clin Pract Cardiovasc Med 2006; 4:214
9 Family History Revisited 2007 I II III TC 8.9 (mmol/l) 10.3 Index Case APOB R3527Q TC 9.9 (mmol/l) CABG age 44?chol
10 Identification and Management of Familial Hypercholesterolaemia the NICE Guidance 1.1 Diagnosis 13 recommendations 1.2 Identifying individuals with FH using cascade testing 8 recommendations 1.3 Management 56 recommendations 1.4 Information needs and support 14 recommendations 1.5 Ongoing Assessment and Monitoring 8 recommendations A total of 99 recommendations
11 Simon Broome diagnostic criteria for probands Definite familial hypercholesterolaemia is defined as: total cholesterol above 6.7mmol/l or LDL cholesterol above 4.0mmol/l in a child aged under 16 years or total cholesterol above 7.5mmol/l or LDL cholesterol above 4.9mmol/l in an adult (levels either pretreatment or highest on treatment) plus tendon xanthomas in patient, or in 1st degree relative (parent, sibling, child), or in 2nd degree relative (grandparent, uncle, aunt) or DNA-based evidence of an LDL receptor mutation, familial defective apo B-100, or a PCSK9 mutation. Possible familial hypercholesterolaemia is defined as above plus one of the criteria below: family history of myocardial infarction: below age of 50 years in 2nd degree relative or below age 60 years in 1st degree relative family history of raised total cholesterol: above 7.5mmol/l in adult 1st or 2nd degree relative or above 6.7mmol/l in child or sibling aged under 16 years.
12 Key priorities for implementation (1) Diagnosis A family history should always be obtained from an individual being investigated for FH to determine if a dominant pattern of inheritance is present. [1.1.6] In children at risk of FH because of an affected parent, LDL-C concentrations should usually be measured by the age of ten years. This measurement should be repeated after puberty before a diagnosis of FH can be excluded. [1.1.8] Individuals with FH are at a very high risk of coronary heart disease. Risk estimation tools such as those based on the Framingham algorithm should not be used to assess their risk. [1.1.10]
13 Key priorities for implementation (2) Identifying individuals with FH using cascade testing All individuals with FH should be referred to a specialist with expertise in FH for confirmation of diagnosis and initiation of cascade testing. [1.2.2] Cascade testing using a combination of lipid concentration measurement and DNA testing should be used to identify relatives of index cases with a clinical diagnosis of FH. [1.2.4] The establishment and use of a nationwide family based follow-up system is recommended to enable comprehensive identification of affected individuals. [1.2.8]
14 Key priorities for implementation (3) Management Adults - Prescription of a potent statin should usually be considered when trying to achieve a reduction of LDL-C concentrations of greater than 50% (from baseline). [ ] Children - Children and young people diagnosed with, or being investigated for a diagnosis of, FH should be referred to a specialist with expertise in FH in an appropriate child focused setting. [ ] Women and girls - When lipid modifying medication is first considered for girls and women, risks to the pregnancy and the fetus while taking lipid modifying medication should be discussed. This discussion should be regularly revisited. [ ] Ongoing assessment and monitoring Review - All treated individuals with FH should have a regular structured review carried out at least annually. [ ]
15 Important points on diagnosis Individuals with a clinical diagnosis of FH should be offered a DNA test to increase the certainty of their diagnosis and to aid diagnosis amongst their relatives. [1.1.11] Individuals with a clinical diagnosis of FH and their relatives who have a detected mutation should be informed they have an unequivocal diagnosis of FH. [1.1.12] In families in which a mutation has been identified, the mutation should be used to identify affected relatives. [1.2.5] In the absence of a DNA diagnosis, cascade testing using lipid measurements should be undertaken.[1.2.6] To diagnose FH in relatives, the gender and age-specific probabilities based on LDL cholesterol concentrations in appendix E should be used. Simon Broome LDL-C criteria should not be used. [1.2.7]
16 Simon Broome diagnostic criteria for probands Definite familial hypercholesterolaemia is defined as: total cholesterol above 6.7mmol/l or LDL cholesterol above 4.0mmol/l in a child aged under 16 years or total cholesterol above 7.5mmol/l or LDL cholesterol above 4.9mmol/l in an adult (levels either pretreatment or highest on treatment) plus tendon xanthomas in patient, or in 1st degree relative (parent, sibling, child), or in 2nd degree relative (grandparent, uncle, aunt) or DNA-based evidence of an LDL receptor mutation, familial defective apo B-100, or a PCSK9 mutation. Possible familial hypercholesterolaemia is defined as above plus one of the criteria below: family history of myocardial infarction: below age of 50 years in 2nd degree relative or below age 60 years in 1st degree relative family history of raised total cholesterol: above 7.5mmol/l in adult 1st or 2nd degree relative or above 6.7mmol/l in child or sibling aged under 16 years.
17
18 LDL-C Diagnostic Tables for 1º relatives Age
19 Important points on management Statins should be the initial treatment for all adults with FH. [ ] Adults - Prescription of a potent statin should usually be considered when trying to achieve a reduction of LDL-C concentrations of greater than 50% (from baseline). [ ] Ezetimibe recommendations for use as monotherapy and in combination with statins as per with TA132 [ ] Individuals not achieving a reduction in LDL-C concentrations of greater than 50% from baseline should be referred to a specialist with expertise in FH. [ ] Individuals with intolerance or contraindications to statins or ezetimibe should be referred to a specialist with expertise in FH for consideration for treatment with either a bile acid sequestrant (resin), nicotinic acid, or a fibrate to reduce LDL-C concentrations. [ ]
20 Referral to Specialists (1) 1. A clinical diagnosis of homozygous FH should be considered in individuals with LDL-C concentrations greater than 13mmol/l and they should be referred to a specialist centre. [1.1.2] 2. All individuals with FH should be referred to a specialist with expertise in FH for confirmation of diagnosis and initiation of cascade testing. [1.2.2 ] 3. Individuals not achieving a reduction in LDL-C concentrations of greater than 50% from baseline should be referred to a specialist with expertise in FH.[ ] 4. Individuals with FH should be referred to a specialist with expertise in FH if they are assessed to be at high risk, that is, they have - established coronary heart disease; or a family history of premature coronary heart disease; or two or more other cardiovascular risk factors (for example, smoking, hypertension, diabetes, male sex). [ ] 5. Individuals with intolerance or contraindications to statins or ezetimibe should be referred to a specialist [ ]
21 Referral to Specialists (2) 6. Children and young people diagnosed with, or being investigated for a diagnosis of, FH should be referred to a specialist with expertise in FH in an appropriate child focused setting. [ ] 7. Individuals experiencing unusual side effects should be referred to a specialist with expertise in FH. [ ] 8. All individuals and families with FH should be offered individualised nutritional advice from a healthcare professional with specific expertise in nutrition. [ ] 9. A specialist with expertise in FH should provide information to individuals with FH on their specific level of risk of coronary heart disease, its implications for them and their families, lifestyle advice and treatment options. [ ] 10.Individuals with FH should be referred urgently to a specialist with expertise in cardiology for evaluation if they have signs or symptoms of possible coronary heart disease. [ ]
22 LDL-lowering apheresis Specialist treatment Adults and children with clinical homozygous FH should be considered for apheresis. The timing of initiation of apheresis will depend on other factors, such as response to lipid modifying medication and presence of coronary heart disease. [ ] In exceptional cases, individuals with heterozygous FH with progressive, symptomatic CHD, despite maximal tolerated lipid modifying medication and optimal medical therapy, should be considered for apheresis. This should be undertaken in a specialist centre on a case by case basis and data collected into an appropriate registry. [ ] Liver transplantation Individuals with homozygous FH should be offered liver transplantation as an option following failure of medication and apheresis. [ ]
23 Who are the Specialists? Specialist One who has expertise in a particular field of medicine by virtue of additional training and experience. For this guideline, we use specialist to refer to a healthcare professional with an expertise in FH. Specialist centre The definition of a specialist centre is not rigid and is based on a combination of patient treatment services, numbers and ages of individuals attending there, the presence of a multi-disciplinary team (which may include for example, physicians, lipidologists, specialist nurses, dieticians), the ability to manage the more unusual manifestations of the condition and the additional functions such as research, education and standard setting. Care is supervised by expert healthcare professionals but shared with local hospitals and primary care teams. Whilst details of the model may vary between patients and areas, the key is that specialist supervision oversees local provision with the patient seen at diagnosis for initial assessment and then at minimum, annually for review.
24 4. Research recommendations 4.1 Identification using clinical registers What is the clinical and cost-effectiveness of identifying an FH patient (defined by DNA testing) from GP registers and from secondary care registers? 4.2 Lipid-modifying therapy in children What is the clinical effectiveness and safety of differing doses of lipid modifying therapy in children with FH? 4.3 Apheresis for people with heterozygous FH What are the appropriate indications, effectiveness, and safety of apheresis in heterozygous FH patients? 4.4 Pregnancy in women with FH What are the implications of FH for the safety of a mother during pregnancy and what are the risks of fetal malformations attributable to pharmacological therapies? 4.5 Cardiovascular evaluation for people with FH What is the utility of routine cardiovascular evaluation for asymptomatic people with familial hypercholesterolaemia?
25 Conclusions Full Implementation of the Lipid Modification Guideline will dramatically increase the number of patients receiving lipid lowering treatment for primary prevention Extension of cardiovascular risk assessment will lead to identification of new cases of primary hyperlipidaemia Full implementation of Familial Hypercholesterolaemia Guideline will require a major increase in the activity of secondary care based specialist lipid and clinical genetics services and an expansion of laboratory facilities for molecular diagnosis of FH Establishment of new apheresis centres will be required to deliver specialist treatment to eligible FH heterozygotes A national FH database program will be required to support the development of a Lipid Clinic network for the efficient delivery of cascade screening nationwide.

26 Model 1 Genetics Centre Based

27 Model 2 Outreach Service
28 Pathway for Cascade Testing of Relatives 1 Proband s Mutation Identified Proband Referred to Genetics Appointment with proband to compile pedigree Relatives within Region Reply slips given to proband to pass on, or sent direct with letter inviting them to appointment Relatives out of Region Letter sent direct, or given to proband to pass on, to recommend GP check cholesterol
29 Pathway for Cascade Testing of Relatives 2 Pathway following DNA Mutation Analysis Mutation Negative DNA Mutation Positive Result Cholesterol normal (Green Zone) Cholesterol high (Grey / Red Zone) FH Excluded Refer to Lipid Clinic Letter to inform patient and GP, cc Lead Consultant, Lipid Clinic No further action. Letter to inform patient. Letter to GP, recommending referral to Lipid Clinic. cc to Lead Consultant, Lipid Clinic
Appendix F Simon Broome Diagnostic criteria for index individuals and relatives
 Appendix F Simon Broome Diagnostic criteria for index individuals and relatives 1 SIMON BROOME DIAGNOSTIC CRITERIA FOR INDEX INDIVIDUALS (PROBANDS) 2 2 GENDER- AND AGE-SPECIFIC LDL-C CRITERIA FOR THE DIAGNOSIS
Appendix F Simon Broome Diagnostic criteria for index individuals and relatives 1 SIMON BROOME DIAGNOSTIC CRITERIA FOR INDEX INDIVIDUALS (PROBANDS) 2 2 GENDER- AND AGE-SPECIFIC LDL-C CRITERIA FOR THE DIAGNOSIS
Familial hypercholesterolaemia
 Familial hypercholesterolaemia Jaimini Cegla MRCP FRCPath PhD Consultant in Chemical Pathology and Metabolic Medicine Hammersmith Hospital Lipid Clinic 20 April 2017 An unrecognised, potentially fatal,
Familial hypercholesterolaemia Jaimini Cegla MRCP FRCPath PhD Consultant in Chemical Pathology and Metabolic Medicine Hammersmith Hospital Lipid Clinic 20 April 2017 An unrecognised, potentially fatal,
Royal Wolverhampton Hospital Adult Lipid Lowering Therapy Guidelines Lipid Lowering Therapy for the Prevention of Cardiovascular Disease
 Royal Wolverhampton Hospital Adult Lipid Lowering Therapy Guidelines 1 This guideline is intended to assist rational and cost-effective prescribing of lipid regulating medications across both primary and
Royal Wolverhampton Hospital Adult Lipid Lowering Therapy Guidelines 1 This guideline is intended to assist rational and cost-effective prescribing of lipid regulating medications across both primary and
The identification and management of heterozygous familial hypercholesterolaemia in adults, young people and children (QS41)
") QS 41 The identification and management of heterozygous familial hypercholesterolaemia in adults, young people and children (QS41) NICE provided the content for this booklet which is independent of any
QS 41 The identification and management of heterozygous familial hypercholesterolaemia in adults, young people and children (QS41) NICE provided the content for this booklet which is independent of any
Proprotein Convertase Subtilisin/Kexin type 9(PCSK9) Inhibitors Prior Authorization with Quantity Limit Program Summary
 Inhibitors Prior Authorization with Quantity Limit Program Summary") Proprotein Convertase Subtilisin/Kexin type 9(PCSK9) Inhibitors Prior Authorization with Quantity Limit Program Summary Proprotein Convertase Subtilisin/Kexin type 9(PCSK9) Inhibitors Prior Authorization
Proprotein Convertase Subtilisin/Kexin type 9(PCSK9) Inhibitors Prior Authorization with Quantity Limit Program Summary Proprotein Convertase Subtilisin/Kexin type 9(PCSK9) Inhibitors Prior Authorization
West Midlands Familial Hypercholesterolaemia Service
 Elaine George WMFHS Clinical Programme Manager West Midlands Familial Hypercholesterolaemia Service Elaine George WMFHS Clinical Programme Manager PCCS Conference November 2018 1 Presentation Objectives
Elaine George WMFHS Clinical Programme Manager West Midlands Familial Hypercholesterolaemia Service Elaine George WMFHS Clinical Programme Manager PCCS Conference November 2018 1 Presentation Objectives
Volume 2; Number 11 July 2008
 Volume 2; Number 11 July 2008 CONTENTS Page 1 NICE Clinical Guideline 67: Lipid Modification (May 2008) Page 7 NICE Technology Appraisal 132: Ezetimibe for the treatment of primary (heterozygous familial
Volume 2; Number 11 July 2008 CONTENTS Page 1 NICE Clinical Guideline 67: Lipid Modification (May 2008) Page 7 NICE Technology Appraisal 132: Ezetimibe for the treatment of primary (heterozygous familial
Cost effectiveness of cascade testing for FH:
 Cost effectiveness of cascade testing for FH: Background In 2008, NICE published evidence-based guidelines for identification and management of FH Updated 2017 Recommended all Clinical FH DNA test to confirm
Cost effectiveness of cascade testing for FH: Background In 2008, NICE published evidence-based guidelines for identification and management of FH Updated 2017 Recommended all Clinical FH DNA test to confirm
Primary Prevention Patients aged 85yrs and over
 Rotherham Guideline for the management of Non-Familial Hypercholesterolaemia Type 1 Diabetes Offer lifestyle advice Over 40yrs of age? Diabetic for more than 10 years? Established nephropathy? Other CVD
Rotherham Guideline for the management of Non-Familial Hypercholesterolaemia Type 1 Diabetes Offer lifestyle advice Over 40yrs of age? Diabetic for more than 10 years? Established nephropathy? Other CVD
Focus on FH (Familial Hypercholesterolemia) Joshua W. Knowles, MD PhD for PCNA May, 2013
 Joshua W. Knowles, MD PhD for PCNA May, 2013") Focus on FH (Familial Hypercholesterolemia) Joshua W. Knowles, MD PhD for PCNA May, 2013 Conflicts CMO for The FH Foundation Pre-talk quiz What is cascade screening? 1. screening all family members 2.
Focus on FH (Familial Hypercholesterolemia) Joshua W. Knowles, MD PhD for PCNA May, 2013 Conflicts CMO for The FH Foundation Pre-talk quiz What is cascade screening? 1. screening all family members 2.
REPATHA (PCSK9 INHIBITORS)
") REPATHA (PCSK9 INHIBITS) Indications: PCSK9 Inhibitors are indicated for treatment of adults with heterozygous familial hypercholesterolemia (HeFH) or clinical atherosclerotic cardiovascular disease as
REPATHA (PCSK9 INHIBITS) Indications: PCSK9 Inhibitors are indicated for treatment of adults with heterozygous familial hypercholesterolemia (HeFH) or clinical atherosclerotic cardiovascular disease as
Guidelines for the Diagnosis and Management of Familial Hypercholesterolaemia
 The Cardiac Society of Australia and New Zealand Guidelines for the Diagnosis and Management of Familial Hypercholesterolaemia This guideline was originally developed by David Sullivan, Gerard Watts, Ian
The Cardiac Society of Australia and New Zealand Guidelines for the Diagnosis and Management of Familial Hypercholesterolaemia This guideline was originally developed by David Sullivan, Gerard Watts, Ian
APPENDIX 2F Management of Cholesterol
 Patients with established CVD: Coronary heart disease Cerebrovascular disease Peripheral vascular disease APPEDIX 2F Management of Cholesterol Patients at high risk of cardiovascular events: Chronic kidney
Patients with established CVD: Coronary heart disease Cerebrovascular disease Peripheral vascular disease APPEDIX 2F Management of Cholesterol Patients at high risk of cardiovascular events: Chronic kidney
Southern Derbyshire Shared Care Pathology Guidelines. Dyslipidaemia
 Southern Derbyshire Shared Care Pathology Guidelines Dyslipidaemia This guideline applies to patients with significantly abnormal lipid profiles, which may be primary (genetic), secondary to other diseases
Southern Derbyshire Shared Care Pathology Guidelines Dyslipidaemia This guideline applies to patients with significantly abnormal lipid profiles, which may be primary (genetic), secondary to other diseases
SECONDARY PREVENTION OF CORONARY HEART DISEASE AND ISCHAEMIC STROKE/TIA
 PRIMARY PREVENTION OF CHD AND STROKE IN HIGH RISK PATIENTS Random non fasting test for total cholesterol, HDL cholesterol (TC:HDL ratio) and LFTs If cholesterol > 7.5 mmol/l or LDL C 5mmol/l exclude secondary
PRIMARY PREVENTION OF CHD AND STROKE IN HIGH RISK PATIENTS Random non fasting test for total cholesterol, HDL cholesterol (TC:HDL ratio) and LFTs If cholesterol > 7.5 mmol/l or LDL C 5mmol/l exclude secondary
Identification and management of familial hypercholesterolaemia (FH) Full guideline draft version. February 2008
 Full guideline draft version. February 2008") Identification and management of familial hypercholesterolaemia (FH) Full guideline draft version February 00 National Collaborating Centre for Primary Care 0 Page of Citation DeMott K, Nherera L, Humphries
Identification and management of familial hypercholesterolaemia (FH) Full guideline draft version February 00 National Collaborating Centre for Primary Care 0 Page of Citation DeMott K, Nherera L, Humphries
Familial Hypercholesterolemia What a cardiologist should know
 Institut für Klinische Chemie Arnold von Eckardstein Familial Hypercholesterolemia What a cardiologist should know Etiology of Hypercholesterolemia monogenic: (rare): e.g. familial hypercholesterolemia
Institut für Klinische Chemie Arnold von Eckardstein Familial Hypercholesterolemia What a cardiologist should know Etiology of Hypercholesterolemia monogenic: (rare): e.g. familial hypercholesterolemia
PCSK9 Inhibitors Praluent (Alirocumab) and Repatha (Evolocumab) For the Treatment of Familial Hypercholesterolemia
 and Repatha (Evolocumab) For the Treatment of Familial Hypercholesterolemia") PCSK9 Inhibitors Praluent (Alirocumab) and Repatha (Evolocumab) For the Treatment of Familial Hypercholesterolemia Policy Number: Original Effective Date: MM.04.037 08/01/2016 Line(s) of Business: HMO;
PCSK9 Inhibitors Praluent (Alirocumab) and Repatha (Evolocumab) For the Treatment of Familial Hypercholesterolemia Policy Number: Original Effective Date: MM.04.037 08/01/2016 Line(s) of Business: HMO;
In 2008 NICE issued guidelines on lipid modification. Key points are summarised below.
 Hyperlipidaemia: management In 2008 NICE issued guidelines on lipid modification. Key points are summarised below. Primary prevention A systematic strategy should be used to identify people aged 40-74
Hyperlipidaemia: management In 2008 NICE issued guidelines on lipid modification. Key points are summarised below. Primary prevention A systematic strategy should be used to identify people aged 40-74
Familial Hypercholeterolaemia
 Familial Hypercholeterolaemia Is it all about statins? Gerald F Watts DSc PhD MD FRACP FRCP Professor and Head, Cardiometabolic Service, Department of Cardiology, Royal Perth Hospital School of Medicine,
Familial Hypercholeterolaemia Is it all about statins? Gerald F Watts DSc PhD MD FRACP FRCP Professor and Head, Cardiometabolic Service, Department of Cardiology, Royal Perth Hospital School of Medicine,
Drug Class Prior Authorization Criteria PCSK9 Inhibitors
 Drug Class Prior Authorization Criteria PCSK9 Inhibitors Line of Business: Medicaid P & T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has been developed through review of
Drug Class Prior Authorization Criteria PCSK9 Inhibitors Line of Business: Medicaid P & T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has been developed through review of
ADMINISTRATIVE POLICY AND PROCEDURE
 ADMINISTRATIVE POLICY PROCEDURE Policy #: Subject: PCSK9 INHIBITS (ex: Repatha) Section: Care Management Effective Date: January 1, 2015 Revision Date(s): NA Review Date(s): NA Responsible Parties: Patryce
ADMINISTRATIVE POLICY PROCEDURE Policy #: Subject: PCSK9 INHIBITS (ex: Repatha) Section: Care Management Effective Date: January 1, 2015 Revision Date(s): NA Review Date(s): NA Responsible Parties: Patryce
Request for Prior Authorization for PCSK9 inhibitor therapy Website Form Submit request via: Fax
 Request for Prior Authorization for PCSK9 inhibitor therapy Website Form www.highmarkhealthoptions.com Submit request via: Fax - 1-855-476-4158 PCSK9 is a protein that reduces the hepatic removal of low-density
Request for Prior Authorization for PCSK9 inhibitor therapy Website Form www.highmarkhealthoptions.com Submit request via: Fax - 1-855-476-4158 PCSK9 is a protein that reduces the hepatic removal of low-density
Appendix E Health Economic modelling
 Appendix E Health Economic modelling Appendix E: Health economic modelling Page 1 of 55 1 Use of high intensity statin compared to low intensity statin in the management of FH patients 1.1 Introduction
Appendix E Health Economic modelling Appendix E: Health economic modelling Page 1 of 55 1 Use of high intensity statin compared to low intensity statin in the management of FH patients 1.1 Introduction
Drug Prior Authorization Guideline PCSK9 Inhibitors -
 Drug Prior Authorization Guideline PCSK9 Inhibitors - REPATHA (evolocumab) PRALUENT (alirocumab) PA9911 Covered Service: Yes when meets criteria below Prior Authorization Required: Yes-as shown below Additional
Drug Prior Authorization Guideline PCSK9 Inhibitors - REPATHA (evolocumab) PRALUENT (alirocumab) PA9911 Covered Service: Yes when meets criteria below Prior Authorization Required: Yes-as shown below Additional
Prevalence of hypercholesterolaemia in young Afrikaners with myocardial infarction. Ischaemic heart disease risk factors.
 AFRICA CARDIOVASCULAR JOURNAL OF AFRICA Vol 20, No 1, January/February 2009 17 Cardiovascular historical Review topics Article S Afr Med J. 1987 Feb 7;71(3):139-42. Prevalence of hypercholesterolaemia
AFRICA CARDIOVASCULAR JOURNAL OF AFRICA Vol 20, No 1, January/February 2009 17 Cardiovascular historical Review topics Article S Afr Med J. 1987 Feb 7;71(3):139-42. Prevalence of hypercholesterolaemia
Lipids What s new (and what s not)
") Lipids What s new (and what s not) Overview Background evidence Obesity Guidelines Treatment options Pragmatic lipidology Side effects Familial Hypercholesterolaemia Cases Summary Background evidence CHD
Lipids What s new (and what s not) Overview Background evidence Obesity Guidelines Treatment options Pragmatic lipidology Side effects Familial Hypercholesterolaemia Cases Summary Background evidence CHD
FORTH VALLEY. LIPID LOWERING GUIDELINE v5 2016
 FORTH VALLEY LIPID LOWERING GUIDELINE v5 2016 This guideline applies to people over 16 years of age. This guideline is not intended to serve as a standard of medical care or be applicable in every situation.
FORTH VALLEY LIPID LOWERING GUIDELINE v5 2016 This guideline applies to people over 16 years of age. This guideline is not intended to serve as a standard of medical care or be applicable in every situation.
Repatha. Repatha (evolocumab) Description
 Description") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.40.08 Subject: Repatha Page: 1 of 8 Last Review Date: December 2, 2016 Repatha Description Repatha (evolocumab)
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.40.08 Subject: Repatha Page: 1 of 8 Last Review Date: December 2, 2016 Repatha Description Repatha (evolocumab)
Medical Policy An independent licensee of the Blue Cross Blue Shield Association
 Proprotein Convertase Subtilisin/kexin type 9 Page 1 of 24 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: Proprotein Convertase Subtilisin/kexin type 9 (PCSK9)
Proprotein Convertase Subtilisin/kexin type 9 Page 1 of 24 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: Proprotein Convertase Subtilisin/kexin type 9 (PCSK9)
Repatha. Repatha (evolocumab) Description
 Description") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.16.08 Subject: Repatha Page: 1 of 8 Last Review Date: September 18, 2015 Repatha Description Repatha
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.16.08 Subject: Repatha Page: 1 of 8 Last Review Date: September 18, 2015 Repatha Description Repatha
Helen Williams Consultant Pharmacist for CV Disease - South London
 Helen Williams Consultant Pharmacist for CV Disease - South London CVD remains the leading cause of death in the UK Accounts for a third of all deaths 46,000 deaths in people < 75 years (70% of these
Helen Williams Consultant Pharmacist for CV Disease - South London CVD remains the leading cause of death in the UK Accounts for a third of all deaths 46,000 deaths in people < 75 years (70% of these
Familial Hypercholesterolemia
 Familial Hypercholesterolemia Dr.Ramzi Al-Mohammadi Assistant Professor of Medicine Interventional Cardiologist, Advanced HF and Transplant Consultant Classification of Hyperlipedemia Primary hyperlipedemia:
Familial Hypercholesterolemia Dr.Ramzi Al-Mohammadi Assistant Professor of Medicine Interventional Cardiologist, Advanced HF and Transplant Consultant Classification of Hyperlipedemia Primary hyperlipedemia:
Case Discussions: Treatment Strategies for High Risk Populations. Most Common Reasons for Referral to the Baylor Lipid Clinic
 Case Discussions: Treatment Strategies for High Risk Populations Peter H. Jones MD, FNLA Associate Professor Methodist DeBakey Heart and Vascular Center Baylor College of Medicine Most Common Reasons for
Case Discussions: Treatment Strategies for High Risk Populations Peter H. Jones MD, FNLA Associate Professor Methodist DeBakey Heart and Vascular Center Baylor College of Medicine Most Common Reasons for
Role of Genetic Counseling in FH: What Referring Physicians Need to Know. Amy C. Sturm, MS, CGC September 21, 2013
 Role of Genetic Counseling in FH: What Referring Physicians Need to Know Amy C. Sturm, MS, CGC September 21, 2013 Disclosures Nothing to disclose. 2 Introduction to the topic Who are genetic counselors?
Role of Genetic Counseling in FH: What Referring Physicians Need to Know Amy C. Sturm, MS, CGC September 21, 2013 Disclosures Nothing to disclose. 2 Introduction to the topic Who are genetic counselors?
Prescribing Policy: Lipid Modification - Primary Prevention
 Prescribing Policy: Lipid Modification - Primary Prevention Policy Statement: Date of Approval: 11 th February 2010 This policy defines the decision made by the NHS Western Cheshire Clinical Commissioning
Prescribing Policy: Lipid Modification - Primary Prevention Policy Statement: Date of Approval: 11 th February 2010 This policy defines the decision made by the NHS Western Cheshire Clinical Commissioning
Juxtapid and Kynamro
 DRUG POLICY Juxtapid and Kynamro BENEFIT APPLICATION Benefit determinations are based on the applicable contract language in effect at the time the services were rendered. Exclusions, limitations or exceptions
DRUG POLICY Juxtapid and Kynamro BENEFIT APPLICATION Benefit determinations are based on the applicable contract language in effect at the time the services were rendered. Exclusions, limitations or exceptions
WORKSHOP 1. Management of Patients with Familial Hypercholesterolemia
 WORKSHOP 1 Management of Patients with Familial Hypercholesterolemia Tutors: Manal Al-Kindi (Oman)/ Gilles Lambert (France) (Case 1) Zuhier Awan (KSA)/ Raul Santos (Brazil) (Case 2) Khalid Al-Waili (Oman)/
WORKSHOP 1 Management of Patients with Familial Hypercholesterolemia Tutors: Manal Al-Kindi (Oman)/ Gilles Lambert (France) (Case 1) Zuhier Awan (KSA)/ Raul Santos (Brazil) (Case 2) Khalid Al-Waili (Oman)/
Coronary Heart Disease and Stroke, Primary and Secondary Prevention Guidelines (Cholesterol)
") CLINICAL GUIDELINE Coronary Heart Disease and Stroke, Primary and Secondary Prevention Guidelines (Cholesterol) A guideline is intended to assist healthcare professionals in the choice of disease-specific
CLINICAL GUIDELINE Coronary Heart Disease and Stroke, Primary and Secondary Prevention Guidelines (Cholesterol) A guideline is intended to assist healthcare professionals in the choice of disease-specific
HoFH presents with a wide spectrum of LDL-C levels in a genetically confirmed cohort of patients
 HoFH presents with a wide spectrum of LDL-C levels in a genetically confirmed cohort of patients Claudia Stefanutti Department of Molecular Medicine, Sapienza University Rome, Italy HoFH, homozygous familial
HoFH presents with a wide spectrum of LDL-C levels in a genetically confirmed cohort of patients Claudia Stefanutti Department of Molecular Medicine, Sapienza University Rome, Italy HoFH, homozygous familial
Clinical Policy: Evolocumab (Repatha) Reference Number: ERX.SPA.169 Effective Date:
 Reference Number: ERX.SPA.169 Effective Date:") Clinical Policy: (Repatha) Reference Number: ERX.SPA.169 Effective Date: 01.11.17 Last Review Date: 11.17 Revision Log See Important Reminder at the end of this policy for important regulatory and legal
Clinical Policy: (Repatha) Reference Number: ERX.SPA.169 Effective Date: 01.11.17 Last Review Date: 11.17 Revision Log See Important Reminder at the end of this policy for important regulatory and legal
ESC/EAS Guidelines for the Management of Dyslipidaemias
 ESC/EAS Guidelines for the Management of Dyslipidaemias Professor Željko Reiner, MD, PhD, FRCP(Lond), FESC, FACC University Hospital Center Zagreb School of Medicine, University of Zagreb, Croatia Declaration
ESC/EAS Guidelines for the Management of Dyslipidaemias Professor Željko Reiner, MD, PhD, FRCP(Lond), FESC, FACC University Hospital Center Zagreb School of Medicine, University of Zagreb, Croatia Declaration
2017 Cardiovascular Summit for Primary Care Thursday 30th & Friday 31st March Crowne Plaza, Dublin
 2017 Cardiovascular Summit for Primary Care Thursday 30th & Friday 31st March 2017 - Crowne Plaza, Dublin 2016 ESC Guidelines on Cardiovascular Risk and elevated lipids Carlos Brotons Sardenya Primary
2017 Cardiovascular Summit for Primary Care Thursday 30th & Friday 31st March 2017 - Crowne Plaza, Dublin 2016 ESC Guidelines on Cardiovascular Risk and elevated lipids Carlos Brotons Sardenya Primary
PROPROTEIN CONVERTASE SUBTILISIN KEXIN 9 (PCSK9) INHIBITORS Praluent (alirocumab) Repatha (evolocumab)
 INHIBITORS Praluent (alirocumab) Repatha (evolocumab)") PROPROTEIN CONVERTASE SUBTILISIN KEXIN 9 (PCSK9) INHIBITORS Praluent (alirocumab) Repatha (evolocumab) Non-Discrimination Statement and Multi-Language Interpreter Services information are located at the
PROPROTEIN CONVERTASE SUBTILISIN KEXIN 9 (PCSK9) INHIBITORS Praluent (alirocumab) Repatha (evolocumab) Non-Discrimination Statement and Multi-Language Interpreter Services information are located at the
Medical Policy An independent licensee of the Blue Cross Blue Shield Association
 Proprotein Convertase Subtilisin/kexin type 9 Page 1 of 22 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: Proprotein Convertase Subtilisin/kexin type 9 (PCSK9)
Proprotein Convertase Subtilisin/kexin type 9 Page 1 of 22 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: Proprotein Convertase Subtilisin/kexin type 9 (PCSK9)
Index. cardiology.theclinics.com. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A ACC/AHA. See American College of Cardiology/ ACE inhibitors. See Angiotensin-converting enzyme (ACE) inhibitors American College of Cardiology/American
Index Note: Page numbers of article titles are in boldface type. A ACC/AHA. See American College of Cardiology/ ACE inhibitors. See Angiotensin-converting enzyme (ACE) inhibitors American College of Cardiology/American
Saving Lives, Saving Families: The health, social and economic advantages of detecting and treating familial hypercholesterolaemia (FH)
") 1 Saving Lives, Saving Families: The health, social and economic advantages of detecting and treating familial hypercholesterolaemia (FH) Economics Chapter: Estimating the benefits from treatment and increasing
1 Saving Lives, Saving Families: The health, social and economic advantages of detecting and treating familial hypercholesterolaemia (FH) Economics Chapter: Estimating the benefits from treatment and increasing
Dyslipidaemia. Dr NM Oosthuizen Dept of Chemical Pathology SA
 Dyslipidaemia Dr NM Oosthuizen Dept of Chemical Pathology SA13 2014 Endogenous and exogenous pathways Endogenous Exogenous Reverse cholesterol transport Dyslipidaemias Causes can be primary or secondary
Dyslipidaemia Dr NM Oosthuizen Dept of Chemical Pathology SA13 2014 Endogenous and exogenous pathways Endogenous Exogenous Reverse cholesterol transport Dyslipidaemias Causes can be primary or secondary
Pharmacy Policy Bulletin
 Pharmacy Policy Bulletin Title: Policy #: PCSK9 inhibitors Rx.01.170 Application of pharmacy policy is determined by benefits and contracts. Benefits may vary based on product line, group, or contract.
Pharmacy Policy Bulletin Title: Policy #: PCSK9 inhibitors Rx.01.170 Application of pharmacy policy is determined by benefits and contracts. Benefits may vary based on product line, group, or contract.
NICE QIPP about Lipitor. Robert Trotter. Clinical Effectiveness Consultant
 NICE QIPP about Lipitor Robert Trotter Clinical Effectiveness Consultant LIP2894c Date of preparation: April 2009 Prescribing information for atorvastatin is available on the last slide Roadmap Background
NICE QIPP about Lipitor Robert Trotter Clinical Effectiveness Consultant LIP2894c Date of preparation: April 2009 Prescribing information for atorvastatin is available on the last slide Roadmap Background
Hyperlipidaemia, dyslipidaemia and hypercholesterolaemia
 Medicine > Cardiology > Hyperlipidaemia, dyslipidaemia and Background information Patient information including patient decision aid Key messages for this pathway FH specialist nurse contact details Local
Medicine > Cardiology > Hyperlipidaemia, dyslipidaemia and Background information Patient information including patient decision aid Key messages for this pathway FH specialist nurse contact details Local
Appendix E Health Economic modelling
 Appendix E Health Economic modelling Page 1 of 56 1 Use of high intensity statin compared to low intensity statin in the management of FH patients 1.1 Introduction Familial hypercholesterolemia (FH) is
Appendix E Health Economic modelling Page 1 of 56 1 Use of high intensity statin compared to low intensity statin in the management of FH patients 1.1 Introduction Familial hypercholesterolemia (FH) is
Elements for a public summary
 VI.2 Elements for a public summary VI.2.1 Overview of disease epidemiology Cardiovascular disease (CVD) is responsible for one-third of global deaths and is a leading and increasing contributor to the
VI.2 Elements for a public summary VI.2.1 Overview of disease epidemiology Cardiovascular disease (CVD) is responsible for one-third of global deaths and is a leading and increasing contributor to the
DYSLIPIDEMIA. Michael Brändle, Stefan Bilz
 DYSLIPIDEMIA Michael Brändle, Stefan Bilz Cardiovascular risk in patients with DM Current guidelines with emphasis on patients with DM Familial Hypercholesterolemia PCSK9-inhibitors Primary Prevention
DYSLIPIDEMIA Michael Brändle, Stefan Bilz Cardiovascular risk in patients with DM Current guidelines with emphasis on patients with DM Familial Hypercholesterolemia PCSK9-inhibitors Primary Prevention
Pharmacy Management Drug Policy
 SUBJECT: ; Praluent (alirocumab), Repatha (evolocumab) POLICY NUMBER: Pharmacy-61 EFFECTIVE DATE: 8/15 LAST REVIEW DATE: 9/22/2017 If the member s subscriber contract excludes coverage for a specific service
SUBJECT: ; Praluent (alirocumab), Repatha (evolocumab) POLICY NUMBER: Pharmacy-61 EFFECTIVE DATE: 8/15 LAST REVIEW DATE: 9/22/2017 If the member s subscriber contract excludes coverage for a specific service
Repatha. Repatha (evolocumab) Description
 Description") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.40.08 Subject: Repatha Page: 1 of 9 Last Review Date: September 15, 2017 Repatha Description Repatha
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.40.08 Subject: Repatha Page: 1 of 9 Last Review Date: September 15, 2017 Repatha Description Repatha
Repatha. Repatha (evolocumab) Description
 Description") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.40.08 Subject: Repatha Page: 1 of 9 Last Review Date: November 30, 2018 Repatha Description Repatha (evolocumab)
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.40.08 Subject: Repatha Page: 1 of 9 Last Review Date: November 30, 2018 Repatha Description Repatha (evolocumab)
Proprotein Convertase Subtilisin Kexin 9 (PCSK9) Inhibitors: PRALUENT (alirocumab) subcutaneous injection REPATHA (evolocumab) subcutaneous injection
 Inhibitors: PRALUENT (alirocumab) subcutaneous injection REPATHA (evolocumab) subcutaneous injection") REPATHA (evolocumab) subcutaneous injection Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific benefit plan. This Pharmacy
REPATHA (evolocumab) subcutaneous injection Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific benefit plan. This Pharmacy
QUANTITY LIMIT TARGET DRUGS- RECOMMENDED LIMITS Brand (generic) GPI Multisource Code Quantity Limit
 GPI Multisource Code Quantity Limit") Proprotein Convertase Subtilisin/Kexin type 9(PCSK9) Inhibitors Prior Authorization with Quantity Limit Criteria- Through Preferred Agent(s) Program Summary This program applies to Commercial, Netresults
Proprotein Convertase Subtilisin/Kexin type 9(PCSK9) Inhibitors Prior Authorization with Quantity Limit Criteria- Through Preferred Agent(s) Program Summary This program applies to Commercial, Netresults
An update on lipidology and cardiovascular risk management. Lipids, Metabolism & Vascular Risk Section - Royal Society of Medicine
 An update on lipidology and cardiovascular risk management Lipids, Metabolism & Vascular Risk Section - Royal Society of Medicine National and international lipid modification guidelines: A critical appraisal
An update on lipidology and cardiovascular risk management Lipids, Metabolism & Vascular Risk Section - Royal Society of Medicine National and international lipid modification guidelines: A critical appraisal
Comprehensive Treatment for Dyslipidemias. Eric L. Pacini, MD Oregon Cardiology 2012 Cardiovascular Symposium
 Comprehensive Treatment for Dyslipidemias Eric L. Pacini, MD Oregon Cardiology 2012 Cardiovascular Symposium Primary Prevention 41 y/o healthy male No Medications Normal BP, Glucose and BMI Social History:
Comprehensive Treatment for Dyslipidemias Eric L. Pacini, MD Oregon Cardiology 2012 Cardiovascular Symposium Primary Prevention 41 y/o healthy male No Medications Normal BP, Glucose and BMI Social History:
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE
 NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE QUALITY AND OUTCOMES FRAMEWORK (QOF) INDICATOR DEVELOPMENT PROGRAMME Briefing paper QOF indicator area: Peripheral arterial disease Potential output:
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE QUALITY AND OUTCOMES FRAMEWORK (QOF) INDICATOR DEVELOPMENT PROGRAMME Briefing paper QOF indicator area: Peripheral arterial disease Potential output:
Mortality and cardiovascular morbidity in patients with familial hypercholesterolemia
 Mortality and cardiovascular morbidity in patients with familial hypercholesterolemia PhD Thesis Liv J Mundal UNIVERSITY OF OSLO 2016 Liv J Mundal, 2016 Series of dissertations submitted to the Faculty
Mortality and cardiovascular morbidity in patients with familial hypercholesterolemia PhD Thesis Liv J Mundal UNIVERSITY OF OSLO 2016 Liv J Mundal, 2016 Series of dissertations submitted to the Faculty
Developing General Practice and Web-Based Toolkits for the Familial Hypercholesterolaemia (FH) Case Ascertainment Tool (FAMCAT)
 Case Ascertainment Tool (FAMCAT)") Developing General Practice and Web-Based Toolkits for the Familial Hypercholesterolaemia (FH) Case Ascertainment Tool (FAMCAT) Dr Stephen Weng NIHR Research Fellow NIHR School for Primary Care Research
Developing General Practice and Web-Based Toolkits for the Familial Hypercholesterolaemia (FH) Case Ascertainment Tool (FAMCAT) Dr Stephen Weng NIHR Research Fellow NIHR School for Primary Care Research
Russian research program evaluating the extent of underdiagnosed and undertreated of familial hypercholesterolaemia in the population.
 Russian research program evaluating the extent of underdiagnosed and undertreated of familial hypercholesterolaemia in the population. Grant ID number 11532493 Main collaborators: 1. Russian National Atherosclerosis
Russian research program evaluating the extent of underdiagnosed and undertreated of familial hypercholesterolaemia in the population. Grant ID number 11532493 Main collaborators: 1. Russian National Atherosclerosis
Common Repatha Documentation Requirements for Patients With Primary Hyperlipidemia and Established CVD 1,2
 Established CVD Common Repatha Documentation Requirements for Patients With Primary Hyperlipidemia and Established CVD 1,2 Primary and Secondary Diagnosis Codes Primary Diagnosis: Primary hyperlipidemia
Established CVD Common Repatha Documentation Requirements for Patients With Primary Hyperlipidemia and Established CVD 1,2 Primary and Secondary Diagnosis Codes Primary Diagnosis: Primary hyperlipidemia
Nephrologisches Zentrum Göttingen GbR Priv. Doz. Dr. med. V. Schettler
 Therapeutic algorithm for Patients with severe Hypercholesterolemia or isolated Lipoprotein(a)-Hyperlipoproteinemia with progressive cardiovascular disease: PCSK9- Inhibitors, Lipoprotein Apheresis or
Therapeutic algorithm for Patients with severe Hypercholesterolemia or isolated Lipoprotein(a)-Hyperlipoproteinemia with progressive cardiovascular disease: PCSK9- Inhibitors, Lipoprotein Apheresis or
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE
 NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE QUALITY AND OUTCOMES FRAMEWORK (QOF) INDICATOR DEVELOPMENT PROGRAMME Briefing paper QOF indicator area: Primary prevention of CVD Potential output:
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE QUALITY AND OUTCOMES FRAMEWORK (QOF) INDICATOR DEVELOPMENT PROGRAMME Briefing paper QOF indicator area: Primary prevention of CVD Potential output:
UnitedHealthcare Pharmacy Clinical Pharmacy Programs
 UnitedHealthcare Pharmacy Clinical Pharmacy Programs Program Number 2017 P 2063-8 Program Prior Authorization/Medical Necessity Medication Repatha (evolocumab) P&T Approval Date 5/2015, 9/2015, 11/2015,
UnitedHealthcare Pharmacy Clinical Pharmacy Programs Program Number 2017 P 2063-8 Program Prior Authorization/Medical Necessity Medication Repatha (evolocumab) P&T Approval Date 5/2015, 9/2015, 11/2015,
Low-density lipoproteins cause atherosclerotic cardiovascular disease (ASCVD) 1. Evidence from genetic, epidemiologic and clinical studies
 1. Evidence from genetic, epidemiologic and clinical studies") Low-density lipoproteins cause atherosclerotic cardiovascular disease (ASCVD) 1. Evidence from genetic, epidemiologic and clinical studies A Consensus Statement from the European Atherosclerosis Society
Low-density lipoproteins cause atherosclerotic cardiovascular disease (ASCVD) 1. Evidence from genetic, epidemiologic and clinical studies A Consensus Statement from the European Atherosclerosis Society
Need Help.. 4. Resources Abbreviations used in the FH Registry Eligibility Criteria for Inclusion in the FH Registry..
 The purpose of the National Familial Hypercholesterolaemia Registry is to collate data to facilitate clinical service planning and to inform clinical best practice. The Registry will also enable research
The purpose of the National Familial Hypercholesterolaemia Registry is to collate data to facilitate clinical service planning and to inform clinical best practice. The Registry will also enable research
Evolocumab for the treatment of primary hypercholesterolaemia and mixed dyslipidaemia
 Evolocumab for the treatment of primary hypercholesterolaemia and mixed dyslipidaemia Lead author: Nancy Kane Regional Drug & Therapeutics Centre (Newcastle) November 2015 2015 Summary Evolocumab (Repatha,
Evolocumab for the treatment of primary hypercholesterolaemia and mixed dyslipidaemia Lead author: Nancy Kane Regional Drug & Therapeutics Centre (Newcastle) November 2015 2015 Summary Evolocumab (Repatha,
Familial Hypercholesterolaemia: Finding FH and Primary Prevention. Rob Gingell FH Specialist Nurse (North Wales)
") Familial Hypercholesterolaemia: Finding FH and Primary Prevention Rob Gingell FH Specialist Nurse (North Wales) robert.gingell@wales.nhs.uk (Relatively) Simple Genetics! Familial Hypercholesterolaemia
Familial Hypercholesterolaemia: Finding FH and Primary Prevention Rob Gingell FH Specialist Nurse (North Wales) robert.gingell@wales.nhs.uk (Relatively) Simple Genetics! Familial Hypercholesterolaemia
THE ESC/EAS LIPID GUIDELINES IN THE ELDERLY
 THE ESC/EAS LIPID GUIDELINES IN THE ELDERLY Alberico L. Catapano alberico.catapano@unimi.it Alberico L. Catapano Potential Conflict Of Interest Prof. Catapano has received honoraria, lecture fees, or research
THE ESC/EAS LIPID GUIDELINES IN THE ELDERLY Alberico L. Catapano alberico.catapano@unimi.it Alberico L. Catapano Potential Conflict Of Interest Prof. Catapano has received honoraria, lecture fees, or research
The Addition of Ezetimibe to Statin therapy in. Patients with Homozygous Familial. Hypercholesterolaemia
 The Addition of Ezetimibe to Statin therapy in Patients with Homozygous Familial Hypercholesterolaemia Submitted in fulfilment with the requirements for the degree Master in Medicine (MMed) Dr Adriano
The Addition of Ezetimibe to Statin therapy in Patients with Homozygous Familial Hypercholesterolaemia Submitted in fulfilment with the requirements for the degree Master in Medicine (MMed) Dr Adriano
New Guidelines in Dyslipidemia Management
 The Fourth IAS-OSLA Course on Lipid Metabolism and Cardiovascular Risk Muscat, Oman, February 2018 New Guidelines in Dyslipidemia Management Dr. Khalid Al-Waili, MD, FRCPC, DABCL Senior Consultant Medical
The Fourth IAS-OSLA Course on Lipid Metabolism and Cardiovascular Risk Muscat, Oman, February 2018 New Guidelines in Dyslipidemia Management Dr. Khalid Al-Waili, MD, FRCPC, DABCL Senior Consultant Medical
Lipids explained. 1 Patient understanding. Time out. Abstract
 Lipids explained PHC774 Edwards R (2013) Lipids explained. Primary Health Care. 23, 1, 32-38. Date of acceptance: October 23 2012. Rhiannon Edwards is British Heart Foundation familial hypercholesterolaemia
Lipids explained PHC774 Edwards R (2013) Lipids explained. Primary Health Care. 23, 1, 32-38. Date of acceptance: October 23 2012. Rhiannon Edwards is British Heart Foundation familial hypercholesterolaemia
The overall frequency of major
 Basia M. Hamata, MD, Gordon A. Francis, MD, FRCPC When are your patients abnormal lipid levels not their fault? Lipid-lowering lifestyle behaviors alone will not usually reduce the risk of premature heart
Basia M. Hamata, MD, Gordon A. Francis, MD, FRCPC When are your patients abnormal lipid levels not their fault? Lipid-lowering lifestyle behaviors alone will not usually reduce the risk of premature heart
Cholesterol (blood, plasma, serum)
") 1 Cholesterol (blood, plasma, serum) 1 Name and description of analyte 1.1 Name of analyte Cholesterol (plasma; also blood, serum) 1.2 Alternative names 2,15-dimethyl-14-(1,5-dimethylhexyl)tetracyclo[8.7.0.0
1 Cholesterol (blood, plasma, serum) 1 Name and description of analyte 1.1 Name of analyte Cholesterol (plasma; also blood, serum) 1.2 Alternative names 2,15-dimethyl-14-(1,5-dimethylhexyl)tetracyclo[8.7.0.0
Kynamro (mipomersen)
") Kynamro (mipomersen) Line(s) of Business: HMO; PPO; QUEST Integration Original Effective Date: 10/01/2015 Current Effective Date: 01/01/201803/01/2019 POLICY A. INDICATIONS The indications below including
Kynamro (mipomersen) Line(s) of Business: HMO; PPO; QUEST Integration Original Effective Date: 10/01/2015 Current Effective Date: 01/01/201803/01/2019 POLICY A. INDICATIONS The indications below including
DIAGNOSIS AND TREATMENT OF FH CHILDREN. O. GUARDAMAGNA Dipartimento di Scienze della Sanità Pubblica e Pediatriche UNIVERSITA DI TORINO
 DIAGNOSIS AND TREATMENT OF FH CHILDREN O. GUARDAMAGNA Dipartimento di Scienze della Sanità Pubblica e Pediatriche UNIVERSITA DI TORINO DISCLOSURES Kowa MSD Pfizer Astrazeneca Synageva/Alexion OUTLINE Background
DIAGNOSIS AND TREATMENT OF FH CHILDREN O. GUARDAMAGNA Dipartimento di Scienze della Sanità Pubblica e Pediatriche UNIVERSITA DI TORINO DISCLOSURES Kowa MSD Pfizer Astrazeneca Synageva/Alexion OUTLINE Background
Death is inevitable but premature death is not. Sir Richard Doll
 Welcome to the Diabetes Care for You webinar Please log onto the conference call so you can hear our presenter From any SCFT Cisco phone dial 800800 From a mobile phone or any other phone dial 01273 242
Welcome to the Diabetes Care for You webinar Please log onto the conference call so you can hear our presenter From any SCFT Cisco phone dial 800800 From a mobile phone or any other phone dial 01273 242
Praluent. Praluent (alirocumab) Description
 Description") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.40.06 Subject: Praluent Page: 1 of 10 Last Review Date: September 20, 2018 Praluent Description Praluent
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.40.06 Subject: Praluent Page: 1 of 10 Last Review Date: September 20, 2018 Praluent Description Praluent
UNIVERSITA DI PISA CHIMICA E TECNOLOGIE FARMACEUTICHE FAMILIAL HYPERCHOLESTEROLEMIA DIPARTIMENTO DI FARMACIA GENETIC CAUSES AND THERAPY
 UNIVERSITA DI PISA DIPARTIMENTO DI FARMACIA CHIMICA E TECNOLOGIE FARMACEUTICHE CORSO DI BASI BIOCHIMICHE DELL AZIONE DEI FARMACI FAMILIAL HYPERCHOLESTEROLEMIA GENETIC CAUSES AND THERAPY ERIKA ROSARIA PACCIOLLA
UNIVERSITA DI PISA DIPARTIMENTO DI FARMACIA CHIMICA E TECNOLOGIE FARMACEUTICHE CORSO DI BASI BIOCHIMICHE DELL AZIONE DEI FARMACI FAMILIAL HYPERCHOLESTEROLEMIA GENETIC CAUSES AND THERAPY ERIKA ROSARIA PACCIOLLA
Genetic Dyslipidemia and Cardiovascular Diseases
 Sultan Qaboos University Genetic Dyslipidemia and Cardiovascular Diseases Fahad AL Zadjali, PhD Fahadz@squ.edu.om We care 1 2/14/18 DISCLOSURE OF CONFLICT No financial relationships with commercial interests
Sultan Qaboos University Genetic Dyslipidemia and Cardiovascular Diseases Fahad AL Zadjali, PhD Fahadz@squ.edu.om We care 1 2/14/18 DISCLOSURE OF CONFLICT No financial relationships with commercial interests
Fa m i l i a l hy p e rc h o l e s te ro l a e m i a
 Me d i c i n et o d a y PEER REVIEWED ARTICLE POINTS: 2 CPD/ PDP Fa m i l i a l hy p e rc h o l e s te ro l a e m i a wa lking time bombs and digging for gold Treatment of familial hypercholesterolaemia,
Me d i c i n et o d a y PEER REVIEWED ARTICLE POINTS: 2 CPD/ PDP Fa m i l i a l hy p e rc h o l e s te ro l a e m i a wa lking time bombs and digging for gold Treatment of familial hypercholesterolaemia,
THE CLINICAL BIOCHEMISTRY OF LIPID DISORDERS
 THE CLINICAL BIOCHEMISTRY OF LIPID DISORDERS Hormonal regulation INSULIN lipid synthesis, lipolysis CORTISOL lipolysis GLUCAGON lipolysis GROWTH HORMONE lipolysis CATECHOLAMINES lipolysis LEPTIN catabolism
THE CLINICAL BIOCHEMISTRY OF LIPID DISORDERS Hormonal regulation INSULIN lipid synthesis, lipolysis CORTISOL lipolysis GLUCAGON lipolysis GROWTH HORMONE lipolysis CATECHOLAMINES lipolysis LEPTIN catabolism
Subject: Repatha (evolocumab) Original Effective Date: 09/28/2015. Policy Number: MCP-258 Revision Date(s): 5/4/16; 4/17/17
 Original Effective Date: 09/28/2015. Policy Number: MCP-258 Revision Date(s): 5/4/16; 4/17/17") Subject: Repatha (evolocumab) Original Effective Date: 09/28/2015 Policy Number: MCP-258 Revision Date(s): 5/4/16; 4/17/17 Review Date(s): 5/4/2016, 4/17/2017, 7/10/2018 DISCLAIMER This Medical Policy
Subject: Repatha (evolocumab) Original Effective Date: 09/28/2015 Policy Number: MCP-258 Revision Date(s): 5/4/16; 4/17/17 Review Date(s): 5/4/2016, 4/17/2017, 7/10/2018 DISCLAIMER This Medical Policy
Andrew Cohen, MD and Neil S. Skolnik, MD INTRODUCTION
 2 Hyperlipidemia Andrew Cohen, MD and Neil S. Skolnik, MD CONTENTS INTRODUCTION RISK CATEGORIES AND TARGET LDL-CHOLESTEROL TREATMENT OF LDL-CHOLESTEROL SPECIAL CONSIDERATIONS OLDER AND YOUNGER ADULTS ADDITIONAL
2 Hyperlipidemia Andrew Cohen, MD and Neil S. Skolnik, MD CONTENTS INTRODUCTION RISK CATEGORIES AND TARGET LDL-CHOLESTEROL TREATMENT OF LDL-CHOLESTEROL SPECIAL CONSIDERATIONS OLDER AND YOUNGER ADULTS ADDITIONAL
SIGN 149 Risk estimation and the prevention of cardiovascular disease. Quick Reference Guide July Evidence
 SIGN 149 Risk estimation and the prevention of cardiovascular disease Quick Reference Guide July 2017 Evidence ESTIMATING CARDIOVASCULAR RISK R Individuals with the following risk factors should be considered
SIGN 149 Risk estimation and the prevention of cardiovascular disease Quick Reference Guide July 2017 Evidence ESTIMATING CARDIOVASCULAR RISK R Individuals with the following risk factors should be considered
Proposals regarding the Cholesterol Lowering Pharmaceuticals Atorvastatin and Ezetimibe
 26 April 2010 Proposals regarding the Cholesterol Lowering Pharmaceuticals Atorvastatin and Ezetimibe PHARMAC is seeking feedback on the following proposals relating to the cholesterol lowering pharmaceuticals
26 April 2010 Proposals regarding the Cholesterol Lowering Pharmaceuticals Atorvastatin and Ezetimibe PHARMAC is seeking feedback on the following proposals relating to the cholesterol lowering pharmaceuticals
Lipid Lowering in patients with High Risk of Cardiovascular Disease (Primary Prevention)
") Lipid Lowering in patients with High Risk of Cardiovascular Disease (Primary Prevention) Policy Statement: October 2010 This policy defines the decision made by NHS Wirral following an evidence review
Lipid Lowering in patients with High Risk of Cardiovascular Disease (Primary Prevention) Policy Statement: October 2010 This policy defines the decision made by NHS Wirral following an evidence review
Cascade Screening for FH: the U.S. experience
 Cascade Screening for FH: the U.S. experience Paul N. Hopkins, MD, MSPH Professor of Internal Medicine Cardiovascular Genetics University of Utah Disclosures Consultant Genzyme, Amgen, Regeneron Research
Cascade Screening for FH: the U.S. experience Paul N. Hopkins, MD, MSPH Professor of Internal Medicine Cardiovascular Genetics University of Utah Disclosures Consultant Genzyme, Amgen, Regeneron Research
Repeat ischaemic heart disease audit of primary care patients ( ): Comparisons by age, sex and ethnic group
: Comparisons by age, sex and ethnic group") Repeat ischaemic heart disease audit of primary care patients (2002-2003): Comparisons by age, sex and ethnic group Baseline-repeat ischaemic heart disease audit of primary care patients: a comparison
Repeat ischaemic heart disease audit of primary care patients (2002-2003): Comparisons by age, sex and ethnic group Baseline-repeat ischaemic heart disease audit of primary care patients: a comparison
If yes, continue to #2. If no, do not approve. DENIAL TEXT: See the initial denial text at the end of the guideline.
 Generic Brand HICL GCN Exception/Other LOMITAPIDE JUXTAPID 39883 This drug requires a written request for prior authorization. All requests for Juxtapid (lomitapide) require review by a pharmacist prior
Generic Brand HICL GCN Exception/Other LOMITAPIDE JUXTAPID 39883 This drug requires a written request for prior authorization. All requests for Juxtapid (lomitapide) require review by a pharmacist prior
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE. Overview
 NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE Overview Ezetimibe for the treatment of primary (heterozygous familial and non-familial) hypercholesterolaemia The overview is written by members of
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE Overview Ezetimibe for the treatment of primary (heterozygous familial and non-familial) hypercholesterolaemia The overview is written by members of
Proprotein Convertase Subtilisin Kexin 9 (PCSK9) Inhibitors: PRALUENT (alirocumab) subcutaneous injection REPATHA (evolocumab) subcutaneous injection
 Inhibitors: PRALUENT (alirocumab) subcutaneous injection REPATHA (evolocumab) subcutaneous injection") REPATHA (evolocumab) subcutaneous injection Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific benefit plan. This Pharmacy
REPATHA (evolocumab) subcutaneous injection Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific benefit plan. This Pharmacy
How would you manage Ms. Gold
 How would you manage Ms. Gold 32 yo Asian woman with dyslipidemia Current medications: Simvastatin 20mg QD Most recent lipid profile: TC = 246, TG = 100, LDL = 176, HDL = 50 What about Mr. Williams? 56
How would you manage Ms. Gold 32 yo Asian woman with dyslipidemia Current medications: Simvastatin 20mg QD Most recent lipid profile: TC = 246, TG = 100, LDL = 176, HDL = 50 What about Mr. Williams? 56
Familial hypercholesterolaemia Your quick guide
 Familial hypercholesterolaemia Your quick guide Coronary heart disease is the UK s single biggest killer. For over 50 years we ve pioneered research that s transformed the lives of people living with heart
Familial hypercholesterolaemia Your quick guide Coronary heart disease is the UK s single biggest killer. For over 50 years we ve pioneered research that s transformed the lives of people living with heart