King s Research Portal
|
|
|
- Ashlynn Eaton
- 5 years ago
- Views:
Transcription
.")

1 King s Research Portal DOI: /j.chest Document Version Peer reviewed version Link to publication record in King's Research Portal Citation for published version (APA): Azoulay, E., Knoebl, P., Garnacho-Montero, J., Rusinova, K., Galstian, G., Eggimann, P.,... Scully, M. (2017). Expert statements on the standard of care in critically ill adult patients with atypical haemolytic uraemic syndrome. DOI: /j.chest Citing this paper Please note that where the full-text provided on King's Research Portal is the Author Accepted Manuscript or Post-Print version this may differ from the final Published version. If citing, it is advised that you check and use the publisher's definitive version for pagination, volume/issue, and date of publication details. And where the final published version is provided on the Research Portal, if citing you are again advised to check the publisher's website for any subsequent corrections. General rights Copyright and moral rights for the publications made accessible in the Research Portal are retained by the authors and/or other copyright owners and it is a condition of accessing publications that users recognize and abide by the legal requirements associated with these rights. Users may download and print one copy of any publication from the Research Portal for the purpose of private study or research. You may not further distribute the material or use it for any profit-making activity or commercial gain You may freely distribute the URL identifying the publication in the Research Portal Take down policy If you believe that this document breaches copyright please contact librarypure@kcl.ac.uk providing details, and we will remove access to the work immediately and investigate your claim. Download date: 22. Dec. 2018

2 Accepted Manuscript Expert statements on the standard of care in critically ill adult patients with atypical haemolytic uraemic syndrome Elie Azoulay, MD, PhD, Paul Knoebl, MD, José Garnacho-Montero, MD, PhD, Katerina Rusinova, MD, PhD, Gennadii Galstian, MD, PhD, Philippe Eggimann, MD, PhD, Fekri Abroug, MD, PhD, Dominique Benoit, MD, PhD, Michael von Bergwelt- Baildon, MD, PhD, Julia Wendon, MD, Marie Scully, MD PII: S (17) DOI: /j.chest Reference: CHEST 1069 To appear in: CHEST Received Date: 31 January 2017 Revised Date: 1 March 2017 Accepted Date: 31 March 2017 Please cite this article as: Azoulay E, Knoebl P, Garnacho-Montero J, Rusinova K, Galstian G, Eggimann P, Abroug F, Benoit D, von Bergwelt-Baildon M, Wendon J, Scully M, Expert statements on the standard of care in critically ill adult patients with atypical haemolytic uraemic syndrome, CHEST (2017), doi: /j.chest This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
3 Expert statements on the standard of care in critically ill adult patients with atypical haemolytic uraemic syndrome Elie Azoulay, MD, PhD; Paul Knoebl MD; José Garnacho-Montero, MD, PhD; Katerina Rusinova, MD, PhD; Gennadii Galstian, MD, PhD; Philippe Eggimann, MD, PhD; Fekri Abroug, MD, PhD; Dominique Benoit, MD, PhD; Michael von Bergwelt-Baildon, MD, PhD; Julia Wendon, MD; Marie Scully, MD. Author for Correspondence: Elie Azoulay, Medical Intensive Care Unit, Hôpital Saint-Louis, ECSTRA team, and clinical epidemiology, UMR 1153 (Center of Epidemiology and Biostatistics Sorbonne Paris Cité, CRESS), INSERM, Paris Diderot Sorbonne University Tel: Fax: Page 1 of 35
4 List of abbreviations: ahus: atypical haemolytic uraemic syndrome ICU: Intensive Care Unit TTP: thrombotic thrombocytopenic purpura TMA: thrombotic microangiopathy DIC: disseminated intravascular coagulation STEC: Shiga toxin-producing Escherichia coli Page 2 of 35
5 Competing interests This review article is an independent piece of work from the signing authors. This group of experts met at an advisory board to discuss thrombotic microangiopathies in critically ill patients. Together, they defined the content of this article, the scope of the systematic review, the elements needed to make this review didactical and thoughtful for the readers, as well as to select the content of each tables and figures. Senior authors have drafted the review and all authors have added their contribution and suggested changes. A medical writer has edited the sentences where needed and improved the language. Before submission, the paper circulated several times within authors and each single suggestion has been taken into account. Alexion has paid the travels and the hotel (for one night) to make the meeting happen. Alexion also paid the medical writer. The generation of this work was an offshoot from the medical attendees and not in any way directed by Alexion. Authors do not believe that industry could possibly benefit from the content of this review. In addition: Elie Azoulay is part of the board of Gilead France, and has received fees for lectures from Alexion and Astellas. His institution has received grants from Fisher & Payckle, Pfizer and Cubist. Gennadii Galstian have received lecture honoraria from Alexion PHARMA INTERNATIONAL Sàrl and Alexion Pharma LLC, Russia Paul Knoebl has served as an advisory board member, speaker and consultant for Alexion, Ablynx and Baxalta (now Shire). Dominique Benoit has received speaker s honoraria from Pfizer and MSD. Marie Scully has received advisory board and speaker s honoraria for Alexion, Ablyn, Baxalta and Novartis. Page 3 of 35
6 ACKNOWLEDGEMENTS All authors were involved in drafting and critical revision of the manuscript. Medical writing and editorial assistance were provided by Kate Kavanagh and Lindsay Napier at Darwin Healthcare Communications which was funded by Alexion Pharma GmbH. Page 4 of 35
7 Author affiliations: Fekri Abroug, Fattouma Bourguiba Teaching Hospital Monastir, Tunisia Dominique Benoit, Ghent University Hospital, Ghent, Belgium Michael von Bergwelt-Baildon, Uniklinik, Cologne, Germany Philippe Eggimann, University Hospital of Lausanne, Switzerland Gennadii Galstian, National Research Center for Hematology, Russia José Garnacho-Montero, Virgen de Macarena University Hospital, Seville, Spain Paul Knoebl, Medical University of Vienna, Vienna General Hospital, Austria Katerina Rusinova, University Hospital, 1 st Faculty of Medicine, Charles University in Prague, Czech Republic Marie Scully, University College London, United Kingdom Julia Wendon, King s College Hospital, London, United Kingdom Page 5 of 35
8 Keywords: Atypical haemolytic uraemic syndrome, thrombocytopenia, thrombotic microangiopathy, organ failure, plasma exchange, eculizumab Page 6 of 35
9 Abstract Background: Atypical haemolytic uraemic syndrome (ahus) presents similarly to thrombotic thrombocytopenic purpura (TTP), and other causes or conditions with thrombotic microangiopathy (TMA) such as DIC or sepsis. Similarity in clinical presentation may hinder diagnosis and optimal treatment selection in the urgent setting in the ICU. However, there is currently no consensus on the diagnosis or treatment of ahus for ICU specialists. This review aims to summarise available data on the diagnosis and treatment strategies of ahus in the ICU in order to enhance the understanding of ahus diagnosis and outcomes in patients managed in the ICU. Methods: A review of the recent literature (January 2009 March 2016) was performed to select the most relevant articles for ICU physicians. Results: Based on the paucity of adult ahus cases overall and within the ICU, no specific recommendations could be formally graded for the critical care setting. However, the expert panel recognises a core set of skills required by intensivists for diagnosing and managing patients with ahus: recognising thrombotic microangiopathies, differentiating ahus from related conditions, recognising involvement of other organ systems, understanding the pathophysiology of ahus, knowing the diagnostic workup and relevant outcomes in critically ill ahus patients, and knowing the standard of care for patients with ahus based on available data and guidelines. Conclusions: Managing critically ill patients with ahus requires basic skills that, in the absence of sufficient data from patients treated within the ICU, can be gleaned from an increasingly relevant literature outside the ICU. More data on critically ill patients with ahus are needed to validate these conclusions within the ICU setting. Page 7 of 35
10 INTRODUCTION Thrombotic microangiopathies (TMAs) are a group of disorders characterised by thrombocytopenia, microangiopathic haemolytic anaemia and organ dysfunction in which ischaemic organ injury can occur to the brain, kidneys, heart, pancreas, liver, lungs, eyes and skin. Conditions with TMAs include the haemolytic uraemic syndromes (HUSs) and thrombotic thrombocytopenic purpura (TTP), as well as a number of differential diagnoses that must also be excluded (Figure 1). These conditions have a similar clinical presentation of consumptive thrombocytopenia, mechanical haemolysis and organ failure, although with distinct causes, and are typically associated with thickening and inflammation of arterioles and capillaries, detachment and swelling of endothelial cells, subendothelial widening, accumulation of proteins and cellular debris, or platelet thrombi that obstruct the vascular lumen. 1,2 Herein, we will focus on one of these conditions, atypical haemolytic uraemic syndrome (ahus). ahus is a rare but life-threatening condition that affects both children and adults. It accounts for approximately 10% of cases of HUS in children but the majority of HUS cases in adults. 3 The annual incidence of ahus is thought to be around 1 2 per million in adults, 4 although epidemiological data are limited. 5 ahus is distinct from typical, or diarrhoea associated-hus, now commonly called STEC-HUS, which is typically caused by shiga-toxin due to bacterial infection and often associated with bloody diarrhoea. In most cases, ahus is caused by the uncontrolled activation of the complement system, which leads to platelet, leucocyte and endothelial cell activation and TMA, 1,6-8 ultimately causing thrombosis and organ dysfunction. 8,9 Accordingly, it may be unmasked by conditions with enhanced complement activation, such as systemic lupus erythematosus, pregnancy, malignant hypertension, and hematopoietic stem cell transplantation. Page 8 of 35
11 Genetic abnormalities have been found in approximately 50 70% of patients with ahus, 4,10 and a wide variety of mutations are associated with the condition. 4,8 Although gene mutations increase the risk of ahus, they may not be sufficient to cause overt symptoms without additional environmental triggers. These include infections, pregnancy, certain medications, malignancy, sepsis, bone marrow transplantation and connective tissue disorders. 2,9,11 Consequently, genetic testing is currently not useful for the acute diagnosis of ahus, e.g. in the intensive care unit (ICU) setting, but it can provide diagnostic confirmation, prognostic value and information on long-term treatment. Furthermore, owing to the severe nature of the condition, the time delay in obtaining genetic results is not consistent with the need for rapid initiation of therapy. In the absence of any fast, specific diagnostic tests for ahus, the condition can only be diagnosed after exclusion of TTP 12 and related TMAs. Previously, ahus and TTP have been managed in the same way, as the conditions are difficult to differentiate and only one treatment option, plasma therapy (plasma infusion or plasma exchange), was available. 1,4 The benefits of plasma exchange, although not evaluated in prospective studies, include the removal of pathological substances from the blood and the replacement of deficient plasma components. 13 However, although plasma therapy has improved outcomes considerably in TTP, reducing the mortality rate from 90% to 10 20%, 14 more than 50% of patients with ahus proceed to end stage renal disease or death despite plasma therapy. 8,12 Consequently, specific, urgent and interdisciplinary management is paramount in the treatment of patients with ahus owing to both the severity of the illness and the potential development of irreversible complications of organ involvement. 1 Eculizumab, approved in 2011, is the first treatment for ahus with proven efficacy and safety in prospective clinical trials. 6 This monoclonal antibody targets the complement system by blocking the cleavage of C5, avoiding the production of cleavage products C5a Page 9 of 35
12 and C5b; 15 evidence suggests that early initiation can improve renal and non-renal recovery. 16,17 In many cases, the ICU is the only clinical environment in which such specialised, urgent care can be effectively provided at any time. Based on the experience of the panel, physicians in the ICU see an average of three patients with TMA per year, many of whom are not diagnosed at the time of admission. Although treatment guidelines for ahus are available for nephrology, 14,18-20 there is currently no consensus on the diagnosis or treatment of ahus for ICU specialists. This review aims to summarise available data on the diagnosis and treatment of ahus in the ICU with the goal of enhancing the understanding of ahus diagnosis and outcomes in patients managed in the ICU. Page 10 of 35
13 RESEARCH DESIGN AND METHODS The need for this manuscript was identified by a multidisciplinary multinational expert panel of 11 members (nine intensive care physicians and two haematologists), who met in September 2015 to define unmet needs and skill priorities for ICU clinicians managing critically ill patients with ahus and to evaluate existing recommendations outside critical care. A literature search was conducted in the National Library of Medicine database (PubMed; looking for articles published between January 2009 and March 2016, using the search terms atypical haemolytic uraemic syndrome or atypical hemolytic uremic syndrome or diarrhoea negative haemolytic uraemic syndrome or diarrhea negative hemolytic uremic syndrome or ahus or D-HUS with search filters of humans and English language. Additional relevant articles were also included from internet searches using the same search terms. Articles were reviewed manually for relevance by the authors; studies concerning both transplant and native kidney patients with ahus were permitted in this study, as well as systematic literature reviews and specialist review articles. In total, 539 articles were identified, of which 56 were considered relevant (included diagnosis and/or treatment of adult patients with ahus). Page 11 of 35
14 DIAGNOSIS OF PATIENTS WITH ahus Diagnosis of ahus typically commences with the broad diagnosis of TMA (Figure 2, Table 1) and implicates the involvement of not only the ICU physician but also other specialists, notably haematologists and nephrologists. Clinical suspicion of a TMA is based on clinical findings, including microangiopathic haemolytic anaemia, thrombocytopenia, low haptoglobin, elevated lactate dehydrogenase, elevated reticulocytes, fragmented red cells and schistocytes on peripheral blood smear. Acute kidney injury is common in ahus, but other organ involvement, including cardiac, gastrointestinal or neurological damage, may be present and can dominate the clinical picture 1,5,21-24 (Figure 2, Table 1). Once a suspicion of TMA has been established, further investigations, including a full patient medical and family history, are required to exclude other potential causes of TMA, including TTP, shiga-toxin associated HUS (STEC-HUS) or TMA as a transient manifestation of another condition (e.g. malignancy or autoimmune disease) or adverse drug effect, although identification of one of these modulating factors does not preclude development of ahus in individuals with a genetic predisposition. Additionally, an HIV test and a pregnancy test in women of childbearing age should be performed to account for these potential triggers. 25 Differential diagnosis Distinguishing ahus from TTP ADAMTS13 activity The most critical and urgent differential diagnosis is to differentiate TTP from ahus owing to the urgency of specific treatment. Testing for ADAMTS13 (a disintegrin and metalloproteinase with thrombospondin motifs 13) activity is recommended to differentiate between TTP and ahus, 23 and sampling must take place prior to administration of plasma therapy. ADAMTS13 deficiency is characteristic of TTP, with levels < 10% widely Page 12 of 35
15 considered to be diagnostic for the condition. 12,14,23,26-29 ADAMTS13, also known as vwf cleavage protease, acts by cleavage of vwf into smaller, less thrombotic fragments, thereby reducing platelet aggregation. Conversely, in TTP, reduced activity of ADAMTS13 results in platelet hyperadhesiveness and clumping within the microvasculature. 23,30 Somewhat reduced ADAMTS13-activity levels (> 10% of normal) may also occur in ahus, but such levels are sufficient to exclude TTP. While results from the ADAMTS13 assay are typically available within a few hours when the assay is established in the local laboratory, they may take some days when the sample has to be shipped, meaning that treatment decisions may need to be made prior to receiving the results of the test. If ADAMTS13 tests are not available within a few hours, a diagnostic algorithm developed by Coppo et al. in which TTP is suggested by low platelet count (< /L), mildly elevated serum creatinine ( 200 µmol/l) and detectable antinuclear antibodies could help form an initial differential diagnosis. 31 In the interim, until TTP has been excluded, patients should receive plasma exchange. Organ involvement The presence of associated organ involvement may be included within the diagnostic workup to provide evidence for differentiation of ahus from TTP, but it is not conclusive. Renal impairment is the most common complication in ahus (Figure 3), but renal function may be preserved in up to 20% of cases. Acute kidney injury may be seen in TTP but is typically reversible with therapy 32 The need for renal support, such as haemodialysis, is not a common feature of TTP, but it can be seen in progressive disease with multiorgan involvement. Neurological signs (e.g. confusion, focal cerebral abnormalities and seizures) and cardiovascular signs (e.g. cardiomyopathy, myocardial infarction, myocarditis and heart failure) occur in 10 48% and 10% of ahus cases, respectively; 9 however, these signs tend to Page 13 of 35
16 be more frequent in TTP. 14,33 Tsai 34 reported that complications of abnormal vascular permeability (including brain oedema, pleural or pericardial effusions, pulmonary oedema from oliguria or cardiac insufficiency, and ascites) may be used to differentiate TTP from ahus as they are thought to occur rarely in TTP without comorbidity. ahus is also occasionally associated with large artery obstruction. 35 Arterial hypertension may be present, while pulmonary involvement is frequent in untreated ahus but rarely associated with other TMAs. 23 Complement protein level testing Complement factor testing for complement components 3 and 4 (C3 and C4, respectively), complement factor H, complement factor I and antibodies against complement components can detect protein deficiencies due to genetic mutations but cannot differentiate between normal protein and normal levels of functionally ineffective protein. 28 C4 levels are usually normal, but C3 levels are low (normal range mg/dl in males and mg/dl in females 36 ) in up to 40% of patients with ahus. 22,37 Many functional complement tests are very sensitive to preanalytical errors. Therefore, complement testing may help to confirm suspected ahus, but it is not useful as a diagnostic test by itself. Genetic testing Genetic abnormalities in the complement system proteins have been documented, 38 and assessment of these mutations may be used to confirm a diagnosis. Mutations in complement factor H account for ~25% of ahus cases, membrane cofactor protein for ~10%, complement factor I for 5 10% and thrombomodulin for up to 5% of cases, 39 although no known mutations are identified in 30 50% of patients. 4,10 Other genetic variants include gainof-function mutations in the genes coding for complement factor B and C3, and anticomplement factor H antibodies associated with homozygous complement factor H-related Page 14 of 35
17 1 3 deletion. 4,8 The parameters associated with clinical ahus onset are yet to be wholly elucidated. The current hypothesis is a two-hit model: 1) pre-existing genetic susceptibility factors that are capable of stimulating endothelial cell activation/damage and/or platelet aggregation; and 2) modulating factors, encompassing a variety of conditions that can be infectious, inflammatory or related to pregnancy, drugs or stress and are linked epidemiologically to both TTP and ahus. 23 Mutations confer a genetic predisposition, so although a positive result is compatible with the diagnosis, a negative result does not necessarily exclude ahus. Additionally, the results from such tests may take weeks, which is not compatible with the urgent care setting of the ICU, where rapid treatment decisions and administration of urgent therapy are necessities. Page 15 of 35
18 Distinguishing ahus from STEC-HUS and pneumococcal HUS Culture-based assays (serology or polymerase chain reaction, PCR) for Shiga toxinproducing Escherichia coli (STEC), using a stool or rectal swab, in patients with diarrhoea can diagnose STEC-HUS and clearly differentiate it from ahus. Although E. coli is not the only source of Shiga toxin, STEC-HUS, previously referred to as typical HUS or diarrhoeapositive HUS, is the most commonly used terminology today and is used here to refer to this subset of HUS. The presence of diarrhoea alone has been used in the past to differentiate between the conditions; however, this cannot be relied upon as up to one-third of ahus cases also involve diarrhoea, so the presence of Shiga toxin must be analysed in patients with diarrhoea. 23 Pneumococcal HUS is linked to the evidence of invasive pneumococcal infection. Bacterial culture from sterile bodily fluids is required for confirmation of pneumococcal infection and pneumococcal HUS is in contrast to ahus and TTP often associated with a positive Coombs test. 25 Page 16 of 35
19 Further tests to consider in the workup of a patient presenting with TMA Patients presenting with TMA may require further testing to rule out additional associated conditions. Disseminated intravascular coagulopathy and sepsis may present with TMA features but can be ruled out by measuring coagulation parameters, which are all normal in ahus and TTP. 14 Pregnancy can result in complications of TMAs; TMA often leads to fetal death and TMA therapy may have an influence on the fetus. Therefore, a pregnancy test should be performed in women of childbearing age. 40 Viral infections, including HIV, hepatitis B virus, hepatitis C virus, cytomegalovirus and Epstein Barr virus, can also cause TMA and so must be investigated. 1,40 Serology tests, such as antinuclear antibodies and anti- DNA-antibodies to neutrophil cytoplasmic antigens, must be considered to rule out systemic diseases, 1 and basal organ testing, including a brain and lung CT scan, troponin levels, blood glucose levels and serum lipase levels, is also recommended. 40 While a negative direct antiglobulin test (Coombs test) can confirm TMA, a positive result may be indicative of autoimmune haemolytic anaemia, Evans syndrome (when in conjunction with immunemediated thrombocytopenia) or pneumococcal HUS. A full medical history should be acquired to determine underlying conditions, such as malignancies, and drug- or medicationassociated TMAs, 1,40 for example heparin-induced thrombocytopenia (HIT). 41 Family history of TMA or renal injury should also be evaluated considering the important genetic component of ahus. Page 17 of 35
20 Diagnosing ahus in the ICU setting Data on the clinical presentation and diagnosis of ahus, particularly in the ICU setting, are limited by the small number of patients with this condition reported in ICU literature 28 Furthermore, findings relating to ahus are mostly published in nephrology and haematology journals, with limited reach to the ICU specialist. An industry-supported global ahus registry was initiated in 2012, and data on the baseline demographics and clinical characteristics of 516 patients with ahus were recently published. 42 A review of the available case studies relevant to the ICU setting revealed that the initial diagnostic workup was similar for all patients, regardless of the presenting symptoms. It is notable that a variety of approaches were taken for progression beyond the TMA diagnosis, with most patients receiving initial plasma exchange while undergoing further investigations, including ADAMTS13 activity, Shiga toxin testing, kidney biopsy if feasible in critically ill patients and genetic screening. Together, information from these case studies can inform an appropriate workup relevant to patients presenting with ahus symptoms within the ICU. A summary of the key considerations for the differential diagnosis of ahus in the ICU setting is presented in Table 1. Page 18 of 35
21 TREATMENT OF PATIENTS WITH ahus IN THE ICU Knowing the standard of care for patients with ahus, based on available guidelines and expert suggestions on best practice in the treatment of critically ill patients with ahus, is a skill we consider necessary within the ICU. No published guidelines or recommendations focus on the management of patients in the ICU; however, there are no differences in treatment requirements between settings, and published treatment guidelines from other clinical settings apply. Immediate ICU management The critical nature of acute TMA means that a high proportion of patients may be admitted to the ICU at presentation. Owing to the severity of the progression of ahus and other TMAs, a suspected diagnosis should be treated as a medical emergency, and initial supportive measures should be introduced with urgency. The British Committee for Standards in Haematology guidelines suggest that appropriate treatment should be initiated within 4 8 h from diagnosis, as delays are associated with increased morbidity and mortality. 14 While plasma exchange has greatly improved the survival of patients with TTP, 12 it is not considered the most effective therapy for ahus as the majority of patients will die or require long-term renal replacement therapy despite this treatment. 4,12,37 However, owing to the difficulty in differentiating between ahus and TTP, initiation of plasma exchange is often necessary while laboratory results are being determined. 43 Exceptions include patients with metastatic cancer with bone marrow involvement for which plasma exchange would not improve the situation. Plasma exchange requires careful monitoring of organ function, platelet counts and the presence of infections, which can arise from central venous lines and Page 19 of 35
22 other sources related to medical interventions. Platelet concentrates should be avoided during initial therapy as they may aggravate platelet aggregation. 40 Specific management of ahus Once ADAMTS13 is proven detectable (> 10% activity) the probability of a diagnosis of ahus is high, and more specific therapy can be applied. This can be confirmed with a negative test for STEC, once laboratory results have been received. Treatment options for ahus were limited to plasma exchange, dialysis for renal failure and kidney transplantation until 2011, when eculizumab, a recombinant, humanised, monoclonal antibody was approved for use in patients with ahus. 12,43 Eculizumab selectively targets and inhibits the terminal complement protein C5, thereby inhibiting the terminal complement activation. 44 Eculizumab has been demonstrated to be effective and well tolerated in four prospective phase II trials in patients with ahus These trials were however not carried out in the critical care setting. In these trials, terminal complement inhibition with eculizumab was associated with inhibition of further TMA progression, increased platelet count and significant improvement in renal function, including discontinuation of dialysis in 80% of patients on dialysis at initiation of treatment and prevention of recurrence after transplantation. 6 Based on these results, eculizumab was included in a 2015 update to the clinical guidelines 1 and in an international consensus for the treatment of ahus in children in In addition, a number of reviews on the management of patients with ahus recommend the use of eculizumab. 14,20,25,28,43,48,49 However, eculizumab is contraindicated in patients with unresolved Neisserial infection, e.g. Neisseria meningitidis, and in unvaccinated individuals owing to the role of terminal complement in the prevention of Neisserial infection, unless the benefits of treatment outweigh the risks of contracting the infection. 50 Vaccination against Neisseria meningitidis serotypes A, C, Y and W135 and meningococcus Page 20 of 35
23 Type B should be administered at least 2 weeks prior to initiation of eculizumab. If eculizumab treatment needs to be initiated immediately in a critically ill patient, prophylactic antibiotics should be given at the start of therapy and maintained for a minimum of 2 weeks 51 or as specified in individual country guidelines. Management should also include supportive measures aimed at managing the risks and consequences of ahus, such as hypertension, anaemia, thrombocytopenia, acute renal failure and infections, particularly in patients not receiving specific targeted treatment, e.g. eculizumab. Hypertension is common in patients presenting with ahus and should be managed with appropriate medications (angiotensin converting enzyme inhibitors or angiotensin receptor blockers), while red blood cell transfusion may be considered for patients with anaemia, noting that platelet infusions are contraindicated unless the patient is bleeding or at high risk of haemorrhage (i.e. at-risk surgical procedure) or severely thrombocytopenic (platelet count <30,000/mm 3 ). Due to the risk of relapse triggered by infections, physicians should be vigilant for signs of infection, initiating appropriate treatment where necessary. 1,3 Recommendations for standard of care for patients with ahus in the ICU Using published recommendations 1 and expert opinions of the panel, recommendations for the standard of care for adult patients with ahus in the ICU are outlined in Table 3. Page 21 of 35
24 OUTCOMES OF CRITICALLY ILL PATIENTS WITH ahus Data regarding the outcomes of adult patients with ahus are sparse owing to the rarity of the disorder, and data relating to the treatment of such patients in the ICU are rarer still. However, existing studies agree that the prognosis of patients with ahus is poor, with around 50% of patients requiring dialysis, suffering permanent kidney damage or dying within 1 year of first occurrence despite plasma therapy. 4,10,52 In an Italian cohort, mortality after the first episode was 2% in adults; this was markedly lower than the 12% mortality rate reported in children in the same study. Furthermore, 32% of survivors never recovered renal function. 10 Despite plasma therapy, at 3 5 years after onset, 67% of adults with ahus had either died or reached end-stage renal failure. 10 Kidney transplantation, while cited as a treatment option for ahus, was, in fact, rarely considered because of an overall risk of recurrence after transplantation of 50%, with a high risk of graft rejection (up to 100%) in those with recurrence. 3 The risk of post-transplant recurrence varies according to the genetic mutation present and ranges from 0 to 30% in patients with membrane cofactor protein mutation, 40 to 70% with C3 mutation, 45 to 80% with complement factor I mutation, 75 to 90% with complement factor H mutation and up to 100% with complement factor B mutation. 3,10,17,53 Owing to the high risk of graft rejection, living-donor transplantation is not recommended, particularly from living relations owing to the increased risk of the donor subsequently developing ahus. 3 Since the approval of eculizumab, outcomes of patients with ahus have improved significantly, causing a paradigm shift in the management of these patients. 19,47 Notably, 80% of patients on dialysis at baseline could discontinue dialysis with eculizumab. 25,45 A 2-year extension of a phase II study with eculizumab found that haematological normalisation was achieved by 13 of 17 patients after 26 weeks and by 15 patients at both years 1 and 2. In a Page 22 of 35
25 retrospective study of 19 cases of ahus in adults, all with acute kidney injury, nine had normal kidney function after 3 months treatment with eculizumab. 54 Page 23 of 35
26 Conclusion This review is the first of its kind to outline the standard of care in critically ill adult patients with ahus in the ICU. ahus is defined by thrombocytopenia, non-immune haemolytic anaemia and acute kidney injury, and often presents with associated organ dysfunction. Although TTP is fairly well recognised by critical care specialists, ahus remains a diagnostic challenge owing to the rarity of the disease. As there are no specific tests and ahus is diagnosed by exclusion, diagnosis should be oriented towards ahus if disseminated intravascular coagulation is ruled out, STEC test is negative and plasma activity of ADAMTS13 is > 10%. For optimal patient outcomes, early recognition and appropriate treatment are critical to reduce the risk of irreversible organ damage or death. This review suggests initiating plasma therapy within 4 8 h of TMA diagnosis and switching to eculizumab treatment as early as possible after a confirmed ahus diagnosis (ADAMTS13 > 10% and a negative STEC test). Page 24 of 35
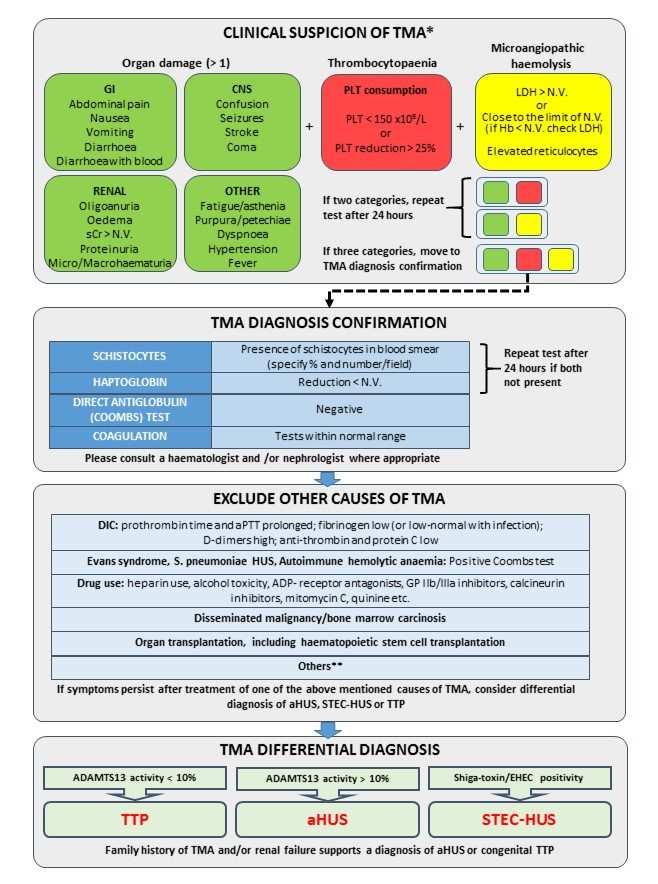
27 Figure legends Fig. 1. Pathophysiology of TMAs. 1 ADAMTS13, a disintegrin and metalloproteinase with thrombospondin motifs 13; ahus, atypical haemolytic uraemic syndrome; C3, complement component 3; CMV, cytomegalovirus; EBV, Epstein Barr virus; FB, complement factor B; FH, complement factor H; FI, complement factor I; HELLP, Haemolysis, Elevated Liver enzymes, Low Platelet count; MCP, membrane cofactor protein; THBD, thrombomodulin; TMA, thrombotic microangiopathy; TTP, thrombotic thrombocytopenic purpura. Fig. 2. Algorithm for the differential diagnosis of ahus in the ICU. 1,12,14,25,40,55,56 *If two categories of clinical findings are present (organ damage and/or thrombocytopaenia and/or microangiopathic haemolysis), repeat tests after 24 hours. If three categories of clinical findings are present, move to TMA diagnosis confirmation. **Others include acute viraemia (CMV, HIV, EBV), pregnancy-associated complications (HELLP, pre-eclampsia), malignant hypertension, catastrophic antiphospholipid antibody syndrome and severe, systemic autoimmune diseases. This list is not exhaustive. ADAMTS13, a disintegrin and metalloproteinase with thrombospondin motifs 13; ADP, adenosine diphosphate; ahus, atypical haemolytic uraemic syndrome; aptt, activated partial thromboplastin time; CMV, cytomegalovirus; CNS, central nervous system; DIC, disseminated intravascular coagulation; EBV, Epstein Barr virus; EHEC, enterohaemorrhagic Escherichia coli; GI, gastrointestinal; GP, glycoprotein; Hb, haemoglobin; HELLP, Haemolysis, Elevated Liver enzymes, Low Platelet count; LDH, lactate dehydrogenase; N.V. normal value; PLT, platelet; scr, serum creatinine; STEC, Shiga toxin-producing Escherichia coli; TMA, thrombotic microangiopathy; TTP, thrombotic thrombocytopenic purpura. Fig. 3. Frequency of organ involvement in atypical haemolytic uraemic syndrome. 9 CNS, central nervous system; GI, gastrointestinal. Page 25 of 35
28 Table 1. Recommended tests for the differential diagnosis of ahus. 1,12,14,25,40,55,56 Identify TMA Test Outcome in ahus In alternative diagnosis Reticulocyte counts Increased Free serum haemoglobin Increased LDH Increased Haptoglobin Decreased Often decreased in TMAs, normal in DIC and sepsis Schistocytes Present Can be present in all TMAs Platelet count Decreased (most of the time) Can be reduced in all TMAs Haemoglobin Decreased Can be decreased in all TMAs Serum creatinine Increased (most of the time) Can be increased in all TMAs Haematuria and proteinuria Present (most of the time) Can be present in all TMAs Kidney biopsy a Often arteriolar and/or glomerular intracapillary thrombosis if kidney affected Additional tests to perform to advise on other possible causes of TMA Direct antiglobulin test (Coombs test) Negative Positive in autoimmune haemolytic anaemias, Evans syndrome and pneumococcal HUS Fibrinogen Normal Reduced fibrinogen and elevated fibrinogen degradation products in DIC aptt, PT Normal Prolonged in DIC Plasma coagulation tests Normal Reduced in DIC D-dimer Normal (can be elevated) Elevated D-dimer in DIC or TMA Liver enzyme levels Normal (can be elevated if liver is Elevated in HELLP syndrome involved) Viral infections, including HIV, HBV, HCV, and H1N1 Can be a precipitant of ahus Known external precipitant of TMA Pregnancy test (where Pregnancy-triggered TMA caused Pregnancy-triggered TMA caused appropriate) by ahus usually presents in late pregnancy or post partum by TTP usually presents during pregnancy Antibody testing, including Negative Positive in systemic diseases like antinuclear antibody, lupus SLE, CAPS; 30% of TTP have anticoagulant, antiphospholipid positive ANA antibodies Rule out TTP and STEC-HUS STEC infection: faecal sample or Negative Positive in STEC-HUS rectal swab test for E. coli and/or PCR for Shiga toxin, and serology of LPS of common Shiga toxinproducing strains ADAMTS13 > 10% activity < 10% activity in TTP a Kidney biopsies are rarely performed as little information can be obtained above that from laboratory results; kidney biopsy in critically ill patients with low platelet counts should not be performed owing to bleeding risk. This is not an exhaustive list, but a suggestion. Further tests for conditions that can mimic TMA, such as malaria, babesiosis and vitamin deficiency, may be warranted. ADAMTS13, a disintegrin and metalloproteinase with thrombospondin motifs 13; ahus, atypical haemolytic uraemic syndrome; aptt, activated partial thromboplastin time; CAPS, cryopyrin-associated autoinflammatory syndrome; DIC, disseminated intravascular coagulation; HBV, hepatitis B virus; Page 26 of 35
29 HCV, hepatitis C virus; HELLP, Haemolysis, Elevated Liver enzymes, Low Platelet count; LDH, lactate dehydrogenase; LPS, lipopolysaccharide; MAHA, microangiopathic haemolytic anaemia; PCR, polymerase chain reaction; PT, prothrombin time; SLE, systemic lupus erythematosus; STEC, Shiga toxin-producing Escherichia coli; TMA, thrombotic microangiopathy; TTP, thrombotic thrombocytopenic purpura. Page 27 of 35
30 Table 2. Key considerations for differential diagnosis of ahus in the ICU. 1. Microangiopathic haemolytic anaemia, thrombocytopenia and organ impairment should be recognised as being suggestive of TMA 2. A full medical history should be taken to exclude or identify other causes, e.g. previous TMA episodes, pregnancy, prior malignancies, drug use, etc. 3. Disseminated intravascular coagulation and sepsis should be ruled out by clinical picture, microbiological testing and assessment of coagulation screen 4. TTP and STEC-HUS should be ruled out with ADAMTS13 activity (before initiation of plasma therapy) and Shiga tests; if ADAMTS13-activity test is not available, the Coppo algorithm 31 to assess serum creatinine and platelet count may be considered 5. If TMA persists upon specific treatment of associated condition (Fig 1), differential diagnosis for ahus should be considered ADAMTS13, a disintegrin and metalloproteinase with thrombospondin motifs 13; ahus, atypical haemolytic uraemic syndrome; ICU, intensive care unit; STEC, Shiga toxinproducing Escherichia coli; TMA, thrombotic microangiopathy; TTP, thrombotic thrombocytopenic purpura. Page 28 of 35
31 Table 3. Recommendations for management of adult patients with suspected ahus in the ICU. 1. Obtain adequate diagnostic samples before plasma therapy 2. Make use of multidisciplinary care, including nephrologists and haematologists 3. Initiate plasma therapy within 4 8 h of admission or diagnosis of TMA. For patients with an initial presentation of TMA, switch to eculizumab as soon as a diagnosis of ahus is confirmed (ADAMTS13 > 10% and STEC negative); for patients with a history of previous ahus, initiate eculizumab immediately upon admission to the ICU 4. Careful ICU monitoring should be offered as organ dysfunction may appear or worsen until remission 5. Owing to the increased risk of Neisseria meningitidis infection with eculizumab treatment, patients should be vaccinated against serotypes A, C, Y and W135 and subtype B 2 weeks before eculizumab is initiated; unvaccinated individuals should receive prophylactic antibiotics upon eculizumab initiation until at least 2 weeks after Neisseria meningitidis vaccination (please refer to country-specific guidelines). ADAMTS13, a disintegrin and metalloproteinase with thrombospondin motifs 13; ahus, atypical haemolytic uraemic syndrome; ICU, intensive care unit; STEC, Shiga toxinproducing Escherichia coli; TMA, thrombotic microangiopathy. Page 29 of 35
32 REFERENCES 1. Campistol JM, Arias M, Ariceta G et al. An update for atypical haemolytic uraemic syndrome: Diagnosis and treatment. A consensus document. Nefrologia. 2015;35(5): Franchini M. Atypical hemolytic uremic syndrome: from diagnosis to treatment. Clin Chem Lab Med. 2015;53(11): Loirat C, Fremeaux-Bacchi V. Atypical hemolytic uremic syndrome. Orphanet J Rare Dis. 2011;6: Fremeaux-Bacchi V, Fakhouri F, Garnier A et al. Genetics and outcome of atypical hemolytic uremic syndrome: a nationwide French series comparing children and adults. Clin J Am Soc Nephrol. 2013;8(4): Mele C, Remuzzi G, Noris M. Hemolytic uremic syndrome. Semin Immunopathol. 2014;36(4): Legendre CM, Licht C, Loirat C. Eculizumab in atypical hemolytic-uremic syndrome. N Engl J Med. 2013;369(14): Riedl M, Fakhouri F, Le Quintrec M et al. Spectrum of complement-mediated thrombotic microangiopathies: pathogenetic insights identifying novel treatment approaches. Semin Thromb Hemost. 2014;40(4): Noris M, Mele C, Remuzzi G. Podocyte dysfunction in atypical haemolytic uraemic syndrome. Nat Rev Nephrol. 2015;11(4): Hofer J, Rosales A, Fischer C, Giner T. Extra-renal manifestations of complementmediated thrombotic microangiopathies. Front Pediatr. 2014;2: Noris M, Caprioli J, Bresin E et al. Relative role of genetic complement abnormalities in sporadic and familial ahus and their impact on clinical phenotype. Clin J Am Soc Nephrol. 2010;5(10): Page 30 of 35
33 11. Mannucci PM. Understanding organ dysfunction in thrombotic thrombocytopenic purpura. Intensive Care Med. 2015;41(4): Scully M, Goodship T. How I treat thrombotic thrombocytopenic purpura and atypical haemolytic uraemic syndrome. Br J Haematol. 2014;164(6): Reeves HM, Winters JL. The mechanisms of action of plasma exchange. Br J Haematol. 2014;164(3): Scully M, Hunt BJ, Benjamin S et al. Guidelines on the diagnosis and management of thrombotic thrombocytopenic purpura and other thrombotic microangiopathies. Br J Haematol. 2012;158(3): Cofiell R, Kukreja A, Bedard K et al. Eculizumab reduces complement activation, inflammation, endothelial damage, thrombosis, and renal injury markers in ahus. Blood. 2015;125(21): Walle JV, Delmas Y, Ardissino G, Wang J, Kincaid JF, Haller H. Improved renal recovery in patients with atypical hemolytic uremic syndrome following rapid initiation of eculizumab treatment. J Nephrol Zuber J, Le QM, Sberro-Soussan R, Loirat C, Fremeaux-Bacchi V, Legendre C. New insights into postrenal transplant hemolytic uremic syndrome. Nat Rev Nephrol. 2011;7(1): Sawai T, Nangaku M, Ashida A et al. Diagnostic criteria for atypical hemolytic uremic syndrome proposed by the Joint Committee of the Japanese Society of Nephrology and the Japan Pediatric Society. Pediatr Int. 2014;56(1): Loirat C, Fakhouri F, Ariceta G et al. An international consensus approach to the management of atypical hemolytic uremic syndrome in children. Pediatr Nephrol. 2016;31(1): Nester CM. Managing atypical hemolytic uremic syndrome: chapter 2. Kidney Int. 2015;87(5): Sallee M, Ismail K, Fakhouri F et al. Thrombocytopenia is not mandatory to diagnose haemolytic and uremic syndrome. BMC Nephrol. 2013;14:3. Page 31 of 35
34 22. Nester CM, Barbour T, de Cordoba SR et al. Atypical ahus: State of the art. Mol Immunol. 2015;67(1): Laurence J. Atypical hemolytic uremic syndrome (ahus): making the diagnosis. Clin Adv Hematol Oncol. 2012;10(10 Suppl 17): Shenkman B, Einav Y. Thrombotic thrombocytopenic purpura and other thrombotic microangiopathic hemolytic anemias: diagnosis and classification. Autoimmun Rev. 2014;13(4-5): Loirat C, Saland J, Bitzan M. Management of hemolytic uremic syndrome. Presse Med. 2012;41(3 Pt 2):e115-e Feng S, Eyler SJ, Zhang Y et al. Partial ADAMTS13 deficiency in atypical hemolytic uremic syndrome. Blood. 2013;122(8): Campistol JM, Arias M, Ariceta G et al. An update for atypical haemolytic uraemic syndrome: diagnosis and treatment. A consensus document. Nefrologia. 2013;33(1): Nester CM, Thomas CP. Atypical hemolytic uremic syndrome: what is it, how is it diagnosed, and how is it treated? Hematology Am Soc Hematol Educ Program. 2012;2012: Contreras E, de la Rubia J, Del Rio-Garma J, Diaz-Ricart M, Garcia-Gala JM, Lozano M. [Diagnostic and therapeutic guidelines of thrombotic microangiopathies of the Spanish Apheresis Group]. Med Clin (Barc ). 2015;144(7): Tsai HM. Untying the knot of thrombotic thrombocytopenic purpura and atypical hemolytic uremic syndrome. Am J Med. 2013;126(3): Coppo P, Schwarzinger M, Buffet M et al. Predictive features of severe acquired ADAMTS13 deficiency in idiopathic thrombotic microangiopathies: the French TMA reference center experience. PLoS One. 2010;5(4):e Zafrani L, Mariotte E, Darmon M et al. Acute renal failure is prevalent in patients with thrombotic thrombocytopenic purpura associated with low plasma ADAMTS13 activity. J Thromb Haemost. 2015;13(3): Page 32 of 35
35 33. Noris M, Remuzzi G. Cardiovascular complications in atypical haemolytic uraemic syndrome. Nat Rev Nephrol. 2014;10(3): Tsai HM. Thrombotic thrombocytopenic purpura and the atypical hemolytic uremic syndrome: an update. Hematol Oncol Clin North Am. 2013;27(3): Rosove MH. Thrombotic microangiopathies. Semin Arthritis Rheum. 2014;43(6): Caliskan Y, Ozluk Y, Celik D et al. The Clinical Significance of Uric Acid and Complement Activation in the Progression of IgA Nephropathy. Kidney Blood Press Res. 2016;41(2): Taylor CM, Machin S, Wigmore SJ, Goodship TH. Clinical practice guidelines for the management of atypical haemolytic uraemic syndrome in the United Kingdom. Br J Haematol. 2010;148(1): Noris M, Remuzzi G. Atypical hemolytic-uremic syndrome. N Engl J Med. 2009;361(17): Kavanagh D, Goodship TH, Richards A. Atypical hemolytic uremic syndrome. Semin Nephrol. 2013;33(6): Knobl PN. Treatment of thrombotic microangiopathy with a focus on new treatment options. Hamostaseologie. 2013;33(2): Studt JD, Binet I, Nair G, Schanz U. Heparin-induced thrombocytopenia associated with thrombotic microangiopathy. Hamostaseologie. 2013;33(2): Licht C, Ardissino G, Ariceta G et al. The global ahus registry: methodology and initial patient characteristics. BMC Nephrol. 2015;16: Cataland SR, Wu HM. How I treat: the clinical differentiation and initial treatment of adult patients with atypical hemolytic uremic syndrome. Blood. 2014;123(16): Legendre CM, Licht C, Muus P et al. Terminal complement inhibitor eculizumab in atypical hemolytic-uremic syndrome. N Engl J Med. 2013;368(23): Page 33 of 35
36 45. Licht C, Greenbaum LA, Muus P et al. Efficacy and safety of eculizumab in atypical hemolytic uremic syndrome from 2-year extensions of phase 2 studies. Kidney Int. 2015;87(5): Greenbaum LA, Fila M, Ardissino G et al. Eculizumab is a safe and effective treatment in pediatric patients with atypical hemolytic uremic syndrome. Kidney Int. 2016;89(3): Fakhouri F, Hourmant M, Campistol JM et al. Terminal Complement Inhibitor Eculizumab in Adult Patients With Atypical Hemolytic Uremic Syndrome: A Single- Arm, Open-Label Trial. Am J Kidney Dis Picard C, Burtey S, Bornet C, Curti C, Montana M, Vanelle P. Pathophysiology and treatment of typical and atypical hemolytic uremic syndrome. Pathol Biol (Paris). 2015;63(3): Schmidtko J, Peine S, El-Housseini Y, Pascual M, Meier P. Treatment of atypical hemolytic uremic syndrome and thrombotic microangiopathies: a focus on eculizumab. Am J Kidney Dis. 2013;61(2): Alexion. Soliris Summary of Product Characteristics Bouts A, Monnens L, Davin JC, Struijk G, Spanjaard L. Insufficient protection by Neisseria meningitidis vaccination alone during eculizumab therapy. Pediatr Nephrol. 2011;26(10): Caprioli J, Noris M, Brioschi S et al. Genetics of HUS: the impact of MCP, CFH, and IF mutations on clinical presentation, response to treatment, and outcome. Blood. 2006;108(4): Fremeaux-Bacchi V, Miller EC, Liszewski MK et al. Mutations in complement C3 predispose to development of atypical hemolytic uremic syndrome. Blood. 2008;112(13): Fakhouri F, Delmas Y, Provot F et al. Insights from the use in clinical practice of eculizumab in adult patients with atypical hemolytic uremic syndrome affecting the native kidneys: an analysis of 19 cases. Am J Kidney Dis. 2014;63(1): Page 34 of 35
37 55. Greenbaum LA. Atypical hemolytic Uremic Syndrome. 2014: Hunt BJ. Bleeding and coagulopathies in critical care. N Engl J Med. 2014;370(22):2153. Page 35 of 35

38
39

40
Atypical Hemolytic Uremic Syndrome: When the Environment and Mutations Affect Organ Systems. A Case Report with Review of Literature
 Atypical Hemolytic Uremic Syndrome: When the Environment and Mutations Affect Organ Systems. A Case Report with Review of Literature Mouhanna Abu Ghanimeh 1, Omar Abughanimeh 1, Ayman Qasrawi 1, Abdulraheem
Atypical Hemolytic Uremic Syndrome: When the Environment and Mutations Affect Organ Systems. A Case Report with Review of Literature Mouhanna Abu Ghanimeh 1, Omar Abughanimeh 1, Ayman Qasrawi 1, Abdulraheem
When a patient presents with TMA, identify the underlying cause for the appropriate diagnosis... IS IT TTP OR IS IT ahus?
 When a patient presents with TMA, identify the underlying cause for the appropriate diagnosis... IS IT TTP OR IS IT ahus? ADAMTS13 activity >5% RULES OUT a diagnosis of severe ADAMTS13 deficiency (TTP)
When a patient presents with TMA, identify the underlying cause for the appropriate diagnosis... IS IT TTP OR IS IT ahus? ADAMTS13 activity >5% RULES OUT a diagnosis of severe ADAMTS13 deficiency (TTP)
Hemolytic uremic syndrome: Investigations and management
 Hemolytic uremic syndrome: Investigations and management SAWAI Toshihiro M.D., Ph.D. Department of Pediatrics, Shiga University of Medical Science Otsu, JAPAN AGENDA TMA; Thrombotic micro angiopathy STEC-HUS;
Hemolytic uremic syndrome: Investigations and management SAWAI Toshihiro M.D., Ph.D. Department of Pediatrics, Shiga University of Medical Science Otsu, JAPAN AGENDA TMA; Thrombotic micro angiopathy STEC-HUS;
DRUG NAME: Eculizumab Brand(s): Soliris DOSAGE FORM/ STRENGTH: 10 mg/ml (300 mg per vial)
: Soliris DOSAGE FORM/ STRENGTH: 10 mg/ml (300 mg per vial)") Preamble: A confirmed diagnosis of atypical hemolytic uremic syndrome (ahus) is required for eculizumab funding. The information below is to provide clinicians with context for how a diagnosis of ahus
Preamble: A confirmed diagnosis of atypical hemolytic uremic syndrome (ahus) is required for eculizumab funding. The information below is to provide clinicians with context for how a diagnosis of ahus
ahus A PATIENT S GUIDE To learn more about ahus, visit Copyright 2011, Alexion Pharmaceuticals, Inc. All rights reserved.
 To learn more about ahus, visit www.ahussource.com ahus A PATIENT S GUIDE Copyright 2011, Alexion Pharmaceuticals, Inc. All rights reserved. SOL 1169 BECOME EMPOWERED By learning more and taking control
To learn more about ahus, visit www.ahussource.com ahus A PATIENT S GUIDE Copyright 2011, Alexion Pharmaceuticals, Inc. All rights reserved. SOL 1169 BECOME EMPOWERED By learning more and taking control
Soliris and You. Your Guide To Living With ahus. INDICATION & IMPORTANT SAFETY INFORMATION FOR SOLIRIS (eculizumab)
") INDICATION & IMPORTANT SAFETY INFORMATION FOR SOLIRIS (eculizumab) INDICATION What is SOLIRIS? SOLIRIS is a prescription medicine called a monoclonal antibody. SOLIRIS is used to treat: adults and children
INDICATION & IMPORTANT SAFETY INFORMATION FOR SOLIRIS (eculizumab) INDICATION What is SOLIRIS? SOLIRIS is a prescription medicine called a monoclonal antibody. SOLIRIS is used to treat: adults and children
Recent advances in pathogenesis & treatment of ahus
 Recent advances in pathogenesis & treatment of ahus Miquel Blasco Pelicano Nephrology and Kidney Transplant Unit Hospital Clínic, Barcelona Atypical Hemolytic Uremic Syndrome (ahus) Ultra-rare disease:
Recent advances in pathogenesis & treatment of ahus Miquel Blasco Pelicano Nephrology and Kidney Transplant Unit Hospital Clínic, Barcelona Atypical Hemolytic Uremic Syndrome (ahus) Ultra-rare disease:
Safety and Efficacy of Eculizumab in Pediatric Patients With ahus, With or Without Baseline Dialysis
 SA-PO546 Safety and Efficacy of Eculizumab in Pediatric Patients With ahus, With or Without Baseline Johan Vande Walle, 1 Larry A. Greenbaum, 2 Camille L. Bedrosian, 3 Masayo Ogawa, 3 John F. Kincaid,
SA-PO546 Safety and Efficacy of Eculizumab in Pediatric Patients With ahus, With or Without Baseline Johan Vande Walle, 1 Larry A. Greenbaum, 2 Camille L. Bedrosian, 3 Masayo Ogawa, 3 John F. Kincaid,
New insights in thrombotic microangiopathies : TTP and ahus
 New insights in thrombotic microangiopathies : TTP and ahus Dr Catherine LAMBERT Hematology Cliniques universitaires Saint-Luc Catherine.lambert@uclouvain.be New insights in thrombotic microangiopathies
New insights in thrombotic microangiopathies : TTP and ahus Dr Catherine LAMBERT Hematology Cliniques universitaires Saint-Luc Catherine.lambert@uclouvain.be New insights in thrombotic microangiopathies
Soliris (eculizumab) DRUG.00050
 DRUG.00050") Market DC Soliris (eculizumab) DRUG.00050 Override(s) Prior Authorization Approval Duration 1 year Medications Soliris (eculizumab) APPROVAL CRITERIA Paroxysmal Nocturnal Hemoglobinuria I. Initiation of
Market DC Soliris (eculizumab) DRUG.00050 Override(s) Prior Authorization Approval Duration 1 year Medications Soliris (eculizumab) APPROVAL CRITERIA Paroxysmal Nocturnal Hemoglobinuria I. Initiation of
Beyond Plasma Exchange: Targeted Therapy for Thrombotic Thrombocytopenic Purpura
 Beyond Plasma Exchange: Targeted Therapy for Thrombotic Thrombocytopenic Purpura Kristen Knoph, PharmD, BCPS PGY2 Pharmacotherapy Resident Pharmacy Grand Rounds April 25, 2017 2016 MFMER slide-1 Objectives
Beyond Plasma Exchange: Targeted Therapy for Thrombotic Thrombocytopenic Purpura Kristen Knoph, PharmD, BCPS PGY2 Pharmacotherapy Resident Pharmacy Grand Rounds April 25, 2017 2016 MFMER slide-1 Objectives
Safety and Efficacy of Eculizumab in Pediatric Patients With ahus, With or Without Baseline Dialysis
 SP281 Safety and Efficacy of Eculizumab in Pediatric Patients With ahus, With or Without Baseline Johan Vande Walle, 1 Larry A. Greenbaum, 2 Camille L. Bedrosian, 3 Masayo Ogawa, 3 John F. Kincaid, 3 Chantal
SP281 Safety and Efficacy of Eculizumab in Pediatric Patients With ahus, With or Without Baseline Johan Vande Walle, 1 Larry A. Greenbaum, 2 Camille L. Bedrosian, 3 Masayo Ogawa, 3 John F. Kincaid, 3 Chantal
What is meant by Thrombotic Microangiopathy (TMA)?
?") What is meant by Thrombotic Microangiopathy (TMA)? Thrombotic Microangiopathy (TMA) is a group of disorders characterized by injured endothelial cells, microangiopathic hemolytic anemia (MAHA), with its
What is meant by Thrombotic Microangiopathy (TMA)? Thrombotic Microangiopathy (TMA) is a group of disorders characterized by injured endothelial cells, microangiopathic hemolytic anemia (MAHA), with its
Specialised Services Policy: CP98 Eculizumab for Atypical Haemolytic Uraemic Syndrome (ahus)
") Specialised Services Policy: CP98 Eculizumab for Atypical Haemolytic Uraemic Syndrome (ahus) Document Author: Assistant Director for Evidence, Evaluation and Effectiveness Executive Lead: Medical Director
Specialised Services Policy: CP98 Eculizumab for Atypical Haemolytic Uraemic Syndrome (ahus) Document Author: Assistant Director for Evidence, Evaluation and Effectiveness Executive Lead: Medical Director
Accepted Manuscript. No more thrombotic thrombocytopenic purpura/hemolytic uremic syndrome please. Yeong-Hau H. Lien MD, PhD S (18)
") Accepted Manuscript No more thrombotic thrombocytopenic purpura/hemolytic uremic syndrome please Yeong-Hau H. Lien MD, PhD PII: S0002-9343(18)30965-3 DOI: https://doi.org/10.1016/j.amjmed.2018.10.009 Reference:
Accepted Manuscript No more thrombotic thrombocytopenic purpura/hemolytic uremic syndrome please Yeong-Hau H. Lien MD, PhD PII: S0002-9343(18)30965-3 DOI: https://doi.org/10.1016/j.amjmed.2018.10.009 Reference:
Risk factors of chronic renal failure after atypical Hemolytic Uremic Syndrome under plasmatherapy
 Risk factors of chronic renal failure after atypical Hemolytic Uremic Syndrome under plasmatherapy Professeur Eric Rondeau Urgences néphrologiques et Transplantation rénale Hôpital Tenon, Paris WWA SFH
Risk factors of chronic renal failure after atypical Hemolytic Uremic Syndrome under plasmatherapy Professeur Eric Rondeau Urgences néphrologiques et Transplantation rénale Hôpital Tenon, Paris WWA SFH
M.Weitz has documented that he has no relevant financial relationships to disclose or conflict of interest to resolve.
 M.Weitz has documented that he has no relevant financial relationships to disclose or conflict of interest to resolve. Prophylactic eculizumab prior to kidney transplantation for atypical hemolytic uremic
M.Weitz has documented that he has no relevant financial relationships to disclose or conflict of interest to resolve. Prophylactic eculizumab prior to kidney transplantation for atypical hemolytic uremic
TMA in HUS and TTP: new insights
 TMA in HUS and TTP: new insights Daan Dierickx University Hospitals Leuven, Department of Hematology, Belgium 20th Annual Meeting Belgian Society on Thrombosis and Haemostatis Antwerpen, 22 th November
TMA in HUS and TTP: new insights Daan Dierickx University Hospitals Leuven, Department of Hematology, Belgium 20th Annual Meeting Belgian Society on Thrombosis and Haemostatis Antwerpen, 22 th November
DR V PHILIP CLINICAL HAEMATOLOGY UNIT CHRIS HANI BARAGWANATH ACADEMIC HOSPITAL
 DR V PHILIP CLINICAL HAEMATOLOGY UNIT CHRIS HANI BARAGWANATH ACADEMIC HOSPITAL Rare but fatal disease if unrecognized and untreated Incidence about 1: 1 million in the USA Female preponderance of 2:1 Part
DR V PHILIP CLINICAL HAEMATOLOGY UNIT CHRIS HANI BARAGWANATH ACADEMIC HOSPITAL Rare but fatal disease if unrecognized and untreated Incidence about 1: 1 million in the USA Female preponderance of 2:1 Part
Introduction to pathogenesis and treatment of thrombotic microangiopathies (TMA)
") Introduction to pathogenesis and treatment of thrombotic microangiopathies (TMA) JM.Campistol, Nephrology and Renal Transplant Department, Hospital Clinic, University of Barcelona, Barcelona, Spain. jmcampis@clinic.cat
Introduction to pathogenesis and treatment of thrombotic microangiopathies (TMA) JM.Campistol, Nephrology and Renal Transplant Department, Hospital Clinic, University of Barcelona, Barcelona, Spain. jmcampis@clinic.cat
Hemolytic uremic syndrome
 Hemolytic uremic syndrome Doyeun Oh Department of Internal Medicine CHA University School of Medicine Disclosures for Doyeun Oh Research Support/P.I. Employee Consultant Major Stockholder Speakers Bureau
Hemolytic uremic syndrome Doyeun Oh Department of Internal Medicine CHA University School of Medicine Disclosures for Doyeun Oh Research Support/P.I. Employee Consultant Major Stockholder Speakers Bureau
Soliris (eculizumab) Inhibits TMA and Improves Renal Function in Pediatric and Adult Patients with atypical Hemolytic Uremic Syndrome (ahus)
 Inhibits TMA and Improves Renal Function in Pediatric and Adult Patients with atypical Hemolytic Uremic Syndrome (ahus)") Soliris (eculizumab) Inhibits TMA and Improves Renal Function in Pediatric and Adult Patients with atypical Hemolytic Uremic Syndrome (ahus) New Data from the Largest Prospective Trial of Adult Patients
Soliris (eculizumab) Inhibits TMA and Improves Renal Function in Pediatric and Adult Patients with atypical Hemolytic Uremic Syndrome (ahus) New Data from the Largest Prospective Trial of Adult Patients
DIAGNOSTIC CHALLENGES IN THROMBOTIC MICROANGIOPATHIES
 DIAGNOSTIC CHALLENGES IN THROMBOTIC MICROANGIOPATHIES Summary of Presentations from the Alexion-Sponsored Symposium, held at the 51 st ERA EDTA Congress, Amsterdam, the Netherlands, on 1 st June 2014 Chairperson
DIAGNOSTIC CHALLENGES IN THROMBOTIC MICROANGIOPATHIES Summary of Presentations from the Alexion-Sponsored Symposium, held at the 51 st ERA EDTA Congress, Amsterdam, the Netherlands, on 1 st June 2014 Chairperson
Supplementary Appendix
 Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Lapeyraque A-L, Malina M, Fremeaux-Bacchi V, et al. Eculizumab
Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Lapeyraque A-L, Malina M, Fremeaux-Bacchi V, et al. Eculizumab
HUS and TTP Testing. Kenneth D. Friedman, M.D. Director, Hemostasis Reference Lab BloodCenter of Wisconsin, Milwaukee WI
 HUS and TTP Testing Kenneth D. Friedman, M.D. Director, Hemostasis Reference Lab BloodCenter of Wisconsin, Milwaukee WI Disclosures Relevant Financial Relationships Consultant: Ablynx, Bayer, CSL Behring,
HUS and TTP Testing Kenneth D. Friedman, M.D. Director, Hemostasis Reference Lab BloodCenter of Wisconsin, Milwaukee WI Disclosures Relevant Financial Relationships Consultant: Ablynx, Bayer, CSL Behring,
THROMBOTIC MICROANGIOPATHY. Jun-Ki Park 7/19/11
 THROMBOTIC MICROANGIOPATHY Jun-Ki Park 7/19/11 TMAs are microvascular occlusive disorders characterized by systemic or intrarenal aggregation of platelets, thrombocytopenia, and mechanical injury to erythrocytes.
THROMBOTIC MICROANGIOPATHY Jun-Ki Park 7/19/11 TMAs are microvascular occlusive disorders characterized by systemic or intrarenal aggregation of platelets, thrombocytopenia, and mechanical injury to erythrocytes.
Thrombotic Microangiopathies (TMA) / TTP/HUS/αHUS Pathology & Molecular. Genetics
 / TTP/HUS/αHUS Pathology & Molecular. Genetics") Thrombotic Microangiopathies (TMA) / TTP/HUS/αHUS Pathology & Molecular Genetics Helen Liapis, M.D. Senior Consultant Arkana Labs Professor of Pathology & Immunology. retired Washington University School
Thrombotic Microangiopathies (TMA) / TTP/HUS/αHUS Pathology & Molecular Genetics Helen Liapis, M.D. Senior Consultant Arkana Labs Professor of Pathology & Immunology. retired Washington University School
Initial management of TMA syndromes
 Initial management of TMA syndromes Elie Azoulay, Saint-Louis Hospital, Medical Intensive Care Unit Paris Diderot Sorbonne University Groupe de Recherche Respiratoire en Réanimation Onco-Hématologique
Initial management of TMA syndromes Elie Azoulay, Saint-Louis Hospital, Medical Intensive Care Unit Paris Diderot Sorbonne University Groupe de Recherche Respiratoire en Réanimation Onco-Hématologique
THE MULTIPLE FACETS OF THROMBOTIC MICROANGIOPATHIES
 THE MULTIPLE FACETS OF THROMBOTIC MICROANGIOPATHIES Summary of Presentations from the Alexion-Sponsored Symposium, held at the 19 th EHA Congress, Milan, Italy, on 12 th June 2014 Chairperson Pier Mannuccio
THE MULTIPLE FACETS OF THROMBOTIC MICROANGIOPATHIES Summary of Presentations from the Alexion-Sponsored Symposium, held at the 19 th EHA Congress, Milan, Italy, on 12 th June 2014 Chairperson Pier Mannuccio
Soliris (eculizumab, rmc) Section 100 Restriction Criteria
 Section 100 Restriction Criteria") Soliris (eculizumab, rmc) Section 100 Restriction Criteria A guide to initiation and ongoing access to (Section 100) funded Soliris for the treatment of patients with atypical Haemolytic Uraemic Syndrome
Soliris (eculizumab, rmc) Section 100 Restriction Criteria A guide to initiation and ongoing access to (Section 100) funded Soliris for the treatment of patients with atypical Haemolytic Uraemic Syndrome
Corporate Medical Policy
 Corporate Medical Policy File Name: Origination: Last CAP Review: Next CAP Review: Last Review: eculizumab_soliris 8/2014 4/2018 4/2019 4/2018 Description of Procedure or Service Paroxysmal nocturnal hemoglobinuria
Corporate Medical Policy File Name: Origination: Last CAP Review: Next CAP Review: Last Review: eculizumab_soliris 8/2014 4/2018 4/2019 4/2018 Description of Procedure or Service Paroxysmal nocturnal hemoglobinuria
Thrombotic Thrombocytopenic Purpura and the Role of ADAMTS-13
 Thrombotic Thrombocytopenic Purpura and the Role of ADAMTS-13 Mark Cunningham,MD Director, Hematology Laboratory Department of Pathology University of Kansas Medical Center College of American Pathologists
Thrombotic Thrombocytopenic Purpura and the Role of ADAMTS-13 Mark Cunningham,MD Director, Hematology Laboratory Department of Pathology University of Kansas Medical Center College of American Pathologists
Most Common Hemostasis Consults: Thrombocytopenia
 Most Common Hemostasis Consults: Thrombocytopenia Cindy Neunert, MS MSCS Assistant Professor, Pediatrics CUMC Columbia University TSHNA Meeting, April 15, 2016 Financial Disclosures No relevant financial
Most Common Hemostasis Consults: Thrombocytopenia Cindy Neunert, MS MSCS Assistant Professor, Pediatrics CUMC Columbia University TSHNA Meeting, April 15, 2016 Financial Disclosures No relevant financial
Medical Policy. MP Eculizumab (Soliris) Related Policies None. Last Review: 01/24/2019 Effective Date: 04/25/2019 Section: Prescription Drug
 Related Policies None. Last Review: 01/24/2019 Effective Date: 04/25/2019 Section: Prescription Drug") Medical Policy Last Review: 01/24/2019 Effective Date: 04/25/2019 Section: Prescription Drug Related Policies None DISCLAIMER Our medical policies are designed for informational purposes only and are not
Medical Policy Last Review: 01/24/2019 Effective Date: 04/25/2019 Section: Prescription Drug Related Policies None DISCLAIMER Our medical policies are designed for informational purposes only and are not
A PATIENT S JOURNEY. Learning about atypical hemolytic uremic syndrome (ahus)
") A PATIENT S JOURNEY Learning about atypical hemolytic uremic syndrome (ahus) Begin your path to empowerment Being diagnosed with ahus can be overwhelming. You may have many questions: What is ahus? How
A PATIENT S JOURNEY Learning about atypical hemolytic uremic syndrome (ahus) Begin your path to empowerment Being diagnosed with ahus can be overwhelming. You may have many questions: What is ahus? How
Thrombotic thrombocytopenic purpura: a look at the future
 Thrombotic thrombocytopenic purpura: a look at the future Andrea Artoni, MD Ph.D. Angelo Bianchi Bonomi Hemophilia and Thrombosis Center IRCCS Ca Granda Ospedale Maggiore Policlinico Milan, Italy andrea.artoni@policlinico.mi.it
Thrombotic thrombocytopenic purpura: a look at the future Andrea Artoni, MD Ph.D. Angelo Bianchi Bonomi Hemophilia and Thrombosis Center IRCCS Ca Granda Ospedale Maggiore Policlinico Milan, Italy andrea.artoni@policlinico.mi.it
Primary causes: Complement dysregulation (50% of non-shiga toxin-producing E. coli ) Secondary causes:
 Secondary causes:") General department INTRODUCTION The hemolytic uremic syndrome (HUS): microangiopathic hemolytic anemia, thrombocytopenia, and acute kidney injury One of the main causes of acute kidney injury in children
General department INTRODUCTION The hemolytic uremic syndrome (HUS): microangiopathic hemolytic anemia, thrombocytopenia, and acute kidney injury One of the main causes of acute kidney injury in children
R. Coward has documented that he has received cooperative grants from Takeda and Novo Nordisk
 R. Coward has documented that he has received cooperative grants from Takeda and Novo Nordisk Advances in our understanding of the pathogenesis of glomerular thrombotic microangiopathy Lindsay Keir Richard
R. Coward has documented that he has received cooperative grants from Takeda and Novo Nordisk Advances in our understanding of the pathogenesis of glomerular thrombotic microangiopathy Lindsay Keir Richard
Clinical Study Eculizumab Therapy Leads to Rapid Resolution of Thrombocytopenia in Atypical Hemolytic Uremic Syndrome
 Hindawi Publishing Corporation Advances in Hematology Volume 214, Article ID 295323, 7 pages http://dx.doi.org/1.1155/214/295323 Clinical Study Therapy Leads to Rapid Resolution of Thrombocytopenia in
Hindawi Publishing Corporation Advances in Hematology Volume 214, Article ID 295323, 7 pages http://dx.doi.org/1.1155/214/295323 Clinical Study Therapy Leads to Rapid Resolution of Thrombocytopenia in
A CAREGIVER S JOURNEY
 A CAREGIVER S JOURNEY Learning about atypical hemolytic uremic syndrome (ahus) Begin your path to effective advocacy and support Caring for someone who is diagnosed with ahus can be overwhelming. You may
A CAREGIVER S JOURNEY Learning about atypical hemolytic uremic syndrome (ahus) Begin your path to effective advocacy and support Caring for someone who is diagnosed with ahus can be overwhelming. You may
Things to never miss in the office. Brett Houston MD FRCPC (PYG-5, hematology) Leonard Minuk MD FRCPC
 Leonard Minuk MD FRCPC") Things to never miss in the office Brett Houston MD FRCPC (PYG-5, hematology) Leonard Minuk MD FRCPC Presenter Disclosure Faculty / Speaker s name: Brett Houston / Leonard Minuk Relationships with commercial
Things to never miss in the office Brett Houston MD FRCPC (PYG-5, hematology) Leonard Minuk MD FRCPC Presenter Disclosure Faculty / Speaker s name: Brett Houston / Leonard Minuk Relationships with commercial
Haemolytic uraemic syndrome the story of a whodunit
 Haemolytic uraemic syndrome the story of a whodunit Paul Warwicker Lancashire Teaching Hospitals NHS Trust RCP Kidney for the General Physician Conference Nov 17 Renal thrombotic microangiopathy (TMA)
Haemolytic uraemic syndrome the story of a whodunit Paul Warwicker Lancashire Teaching Hospitals NHS Trust RCP Kidney for the General Physician Conference Nov 17 Renal thrombotic microangiopathy (TMA)
TMA CASE STUDY. Pamela Harmon, RN & Keturah Tomlin, RN Toronto General Hospital Apheresis Unit
 TMA CASE STUDY Pamela Harmon, RN & Keturah Tomlin, RN Toronto General Hospital Apheresis Unit Cumulative fraction of patients free of events ahus is a catastrophic disease that can result in sudden & progressive
TMA CASE STUDY Pamela Harmon, RN & Keturah Tomlin, RN Toronto General Hospital Apheresis Unit Cumulative fraction of patients free of events ahus is a catastrophic disease that can result in sudden & progressive
Guideline. Abstract. Key words
 bs_bs_banner Pediatrics International (2014) 56, 1 5 doi: 10.1111/ped.12274 Guideline Diagnostic criteria for atypical hemolytic uremic syndrome proposed by the Joint Committee of the Japanese Society
bs_bs_banner Pediatrics International (2014) 56, 1 5 doi: 10.1111/ped.12274 Guideline Diagnostic criteria for atypical hemolytic uremic syndrome proposed by the Joint Committee of the Japanese Society
Soliris Medical Policy Prior Authorization Program Summary
 Soliris Medical Policy Prior Authorization Program Summary Precertification/Prior Authorization may be required under certain plans. Please verify each member s benefits. OBJECTIVE The intent of the Soliris
Soliris Medical Policy Prior Authorization Program Summary Precertification/Prior Authorization may be required under certain plans. Please verify each member s benefits. OBJECTIVE The intent of the Soliris
Heme (Bleeding and Coagulopathies) in the ICU
 in the ICU") Heme (Bleeding and Coagulopathies) in the ICU General Topics To Discuss Transfusions DIC Thrombocytopenia Liver and renal disease related bleeding Lack of evidence in managing critical illness related
Heme (Bleeding and Coagulopathies) in the ICU General Topics To Discuss Transfusions DIC Thrombocytopenia Liver and renal disease related bleeding Lack of evidence in managing critical illness related
The utility of ADAMTS13 in differentiating TTP from other acute thrombotic microangiopathies: results from the UK TTP Registry
 research paper The utility of ADAMTS13 in differentiating TTP from other acute thrombotic microangiopathies: results from the UK TTP Registry Sevda Hassan, 1 John-Paul Westwood, 2 Debra Ellis, 2 Chris
research paper The utility of ADAMTS13 in differentiating TTP from other acute thrombotic microangiopathies: results from the UK TTP Registry Sevda Hassan, 1 John-Paul Westwood, 2 Debra Ellis, 2 Chris
ISTITUTO DI RICERCHE FARMACOLOGICHE MARIO NEGRI CLINICAL RESEARCH CENTER ALDO E FOR CELE RARE DACCO DISEASES ALDO E CELE DACCO
 ISTITUTO DI RICERCHE FARMACOLOGICHE MARIO NEGRI CENTRO MARIO DI NEGRI RICERCHE INSTITUTE CLINICHE FOR PHARMACOLOGICAL PER LE MALATTIE RESEARCH RARE CLINICAL RESEARCH CENTER ALDO E FOR CELE RARE DACCO DISEASES
ISTITUTO DI RICERCHE FARMACOLOGICHE MARIO NEGRI CENTRO MARIO DI NEGRI RICERCHE INSTITUTE CLINICHE FOR PHARMACOLOGICAL PER LE MALATTIE RESEARCH RARE CLINICAL RESEARCH CENTER ALDO E FOR CELE RARE DACCO DISEASES
Dr. E.SUDHA (Fellow in Pediatric Nephrology) DEPT OF PEDIATRIC NEPHROLOGY & DIALYSIS Dr.MEHTA CHILDRENS HOSPITAL
 DEPT OF PEDIATRIC NEPHROLOGY & DIALYSIS Dr.MEHTA CHILDRENS HOSPITAL") Dr. E.SUDHA (Fellow in Pediatric Nephrology) DEPT OF PEDIATRIC NEPHROLOGY & DIALYSIS Dr.MEHTA CHILDRENS HOSPITAL CASE HISTORY 4 yrs old previously well boy Born to 2 nd degree consanguinity Fever x 5 days
Dr. E.SUDHA (Fellow in Pediatric Nephrology) DEPT OF PEDIATRIC NEPHROLOGY & DIALYSIS Dr.MEHTA CHILDRENS HOSPITAL CASE HISTORY 4 yrs old previously well boy Born to 2 nd degree consanguinity Fever x 5 days
Medication Prior Authorization Form
 Policy Number: 1054 Policy History Approve Date: 06/01/2018 Effective Date: 06/01/2018 Preauthorization All Plans Benefit plans vary in coverage and some plans may not provide coverage for certain service(s)
Policy Number: 1054 Policy History Approve Date: 06/01/2018 Effective Date: 06/01/2018 Preauthorization All Plans Benefit plans vary in coverage and some plans may not provide coverage for certain service(s)
* Renal insufficiencies
 Thrombotic Thrombocytopenic Purpura Behzad Poopak, DCLS PhD. Tehran medical Branch Islamic Azad university bpoopak@yahoo.com Case Summary Ms. X, a 35-year year-old woman Complained of weakness, low grade
Thrombotic Thrombocytopenic Purpura Behzad Poopak, DCLS PhD. Tehran medical Branch Islamic Azad university bpoopak@yahoo.com Case Summary Ms. X, a 35-year year-old woman Complained of weakness, low grade
Spectrum of complement-mediated thrombotic microangiopathies after kidney transplantation
 Spectrum of complement-mediated thrombotic microangiopathies after kidney transplantation Marius Miglinas Vilnius university hospital: Nephrology center, Center of Rare Kidney Diseases Vilnius university
Spectrum of complement-mediated thrombotic microangiopathies after kidney transplantation Marius Miglinas Vilnius university hospital: Nephrology center, Center of Rare Kidney Diseases Vilnius university
Untying the Knot of Thrombotic Thrombocytopenic Purpura and Atypical Hemolytic Uremic Syndrome
 REVIEW Untying the Knot of Thrombotic Thrombocytopenic Purpura and Atypical Hemolytic Uremic Syndrome Han-Mou Tsai, MD imah Hematology Associates, New Hyde Park, NY. ABSTRACT Patients presenting with microangiopathic
REVIEW Untying the Knot of Thrombotic Thrombocytopenic Purpura and Atypical Hemolytic Uremic Syndrome Han-Mou Tsai, MD imah Hematology Associates, New Hyde Park, NY. ABSTRACT Patients presenting with microangiopathic
Approccio morfologico alle microangiopatie trombotiche
 Approccio morfologico alle microangiopatie trombotiche Gina Zini Polo Oncologia e Ematologia Policlinico A. Gemelli Università Cattolica S. Cuore - Roma 1 Thrombotic microangiopathies Occlusive microangiopathic
Approccio morfologico alle microangiopatie trombotiche Gina Zini Polo Oncologia e Ematologia Policlinico A. Gemelli Università Cattolica S. Cuore - Roma 1 Thrombotic microangiopathies Occlusive microangiopathic
Microangiopatia trombotica (MAT) e Sindrome emolitico-uremica atipica (SEUa): Basi patogenetiche, inquadramento diagnostico e principi del
 e Sindrome emolitico-uremica atipica (SEUa): Basi patogenetiche, inquadramento diagnostico e principi del") Microangiopatia trombotica (MAT) e Sindrome emolitico-uremica atipica (SEUa): Basi patogenetiche, inquadramento diagnostico e principi del trattamento Vincenzo Montinaro U.O. Nefrologia Azienda Ospedaliera
Microangiopatia trombotica (MAT) e Sindrome emolitico-uremica atipica (SEUa): Basi patogenetiche, inquadramento diagnostico e principi del trattamento Vincenzo Montinaro U.O. Nefrologia Azienda Ospedaliera
Year 2004 Paper one: Questions supplied by Megan
 QUESTION 53 Endothelial cell pathology on renal biopsy is most characteristic of which one of the following diagnoses? A. Pre-eclampsia B. Haemolytic uraemic syndrome C. Lupus nephritis D. Immunoglobulin
QUESTION 53 Endothelial cell pathology on renal biopsy is most characteristic of which one of the following diagnoses? A. Pre-eclampsia B. Haemolytic uraemic syndrome C. Lupus nephritis D. Immunoglobulin
Paolo Gresele Dipartimento di Medicina, Sezione di Medicina Interna e Cardiovascolare, Università di Perugia
 Le sindromi trombotiche microangiopatiche: il ruolo del laboratorio Paolo Gresele Dipartimento di Medicina, Sezione di Medicina Interna e Cardiovascolare, Università di Perugia Microangiopatie trombotiche:
Le sindromi trombotiche microangiopatiche: il ruolo del laboratorio Paolo Gresele Dipartimento di Medicina, Sezione di Medicina Interna e Cardiovascolare, Università di Perugia Microangiopatie trombotiche:
Renal failure and thrombocytopaenia? Don t forget TTP/HUS. Jonathan Wala Nephrologist
 Renal failure and thrombocytopaenia? Don t forget TTP/HUS Jonathan Wala Nephrologist Thrombotic microangiopathies Disorders characterized by: thrombocytopaenia microangiopathic haemolytic anaemia (MAHA)
Renal failure and thrombocytopaenia? Don t forget TTP/HUS Jonathan Wala Nephrologist Thrombotic microangiopathies Disorders characterized by: thrombocytopaenia microangiopathic haemolytic anaemia (MAHA)
Let`s go for the diagnosis! Yazeed Toukan, MD Pediatric Pulmonary Institute, Ruth Rappaport Children`s Hospital July 2016
 Let`s go for the diagnosis! Yazeed Toukan, MD Pediatric Pulmonary Institute, Ruth Rappaport Children`s Hospital July 2016 Case report 20 months old girl Israeli Arab Muslim family, consanguineous marriage
Let`s go for the diagnosis! Yazeed Toukan, MD Pediatric Pulmonary Institute, Ruth Rappaport Children`s Hospital July 2016 Case report 20 months old girl Israeli Arab Muslim family, consanguineous marriage
Extrarenal involvement in pediatric ahus Kosan C et al
 Case Report J Ped. Nephrology 2014;2(4):154-157 http://journals.sbmu.ac.ir/jpn Atypical Hemolytic Uremic Syndrome with Severe Extrarenal Manifestations: a Case Report How to Cite This Article: KOŞAN C,
Case Report J Ped. Nephrology 2014;2(4):154-157 http://journals.sbmu.ac.ir/jpn Atypical Hemolytic Uremic Syndrome with Severe Extrarenal Manifestations: a Case Report How to Cite This Article: KOŞAN C,
Thrombotic microangiopathies and antineoplastic agents
 Thrombotic microangiopathies and antineoplastic agents Paul Coppo paul.coppo@aphp.fr Service d Hématologie - Hôpital Saint-Antoine AP-HP et Université Pierre & Marie Curie Centre de Référence des Microangiopathies
Thrombotic microangiopathies and antineoplastic agents Paul Coppo paul.coppo@aphp.fr Service d Hématologie - Hôpital Saint-Antoine AP-HP et Université Pierre & Marie Curie Centre de Référence des Microangiopathies
HEME 10 Bleeding Disorders
 HEME 10 Bleeding Disorders When injury occurs, three mechanisms occur Blood vessels Primary hemostasis Secondary hemostasis Diseases of the blood vessels Platelet disorders Thrombocytopenia Functional
HEME 10 Bleeding Disorders When injury occurs, three mechanisms occur Blood vessels Primary hemostasis Secondary hemostasis Diseases of the blood vessels Platelet disorders Thrombocytopenia Functional
Introduction. Arif Asif 1 Ali Nayer 2 Christian S. Haas 3
 J Nephrol (2017) 30:347 362 DOI 10.1007/s40620-016-0357-7 REVIEW Atypical hemolytic uremic syndrome in the setting of complement-amplifying conditions: case reports and a review of the evidence for treatment
J Nephrol (2017) 30:347 362 DOI 10.1007/s40620-016-0357-7 REVIEW Atypical hemolytic uremic syndrome in the setting of complement-amplifying conditions: case reports and a review of the evidence for treatment
Approach to disseminated intravascular coagulation
 Approach to disseminated intravascular coagulation Khaire Ananta Shankarrao 1, Anil Burley 2, Deshmukh 3 1.MD Scholar, [kayachikitsa] 2.Professor,MD kayachikitsa. 3.Professor and HOD,Kayachikitsa. CSMSS
Approach to disseminated intravascular coagulation Khaire Ananta Shankarrao 1, Anil Burley 2, Deshmukh 3 1.MD Scholar, [kayachikitsa] 2.Professor,MD kayachikitsa. 3.Professor and HOD,Kayachikitsa. CSMSS
ahus: recent insights and management
 ahus: recent insights and management Steven Van Laecke MD, PhD Renal Division, Ghent University Hospital, Belgium 13 th BANTAO Sarajevo October 8 2017 The complement is everywhere I could benefit from
ahus: recent insights and management Steven Van Laecke MD, PhD Renal Division, Ghent University Hospital, Belgium 13 th BANTAO Sarajevo October 8 2017 The complement is everywhere I could benefit from
1. INSTRUCTIONS 2. DEFINITION OF HUS
 CQ_IBK_aHUS_01 / version 25/11/09 European Paediatric Research Group for HUS and related disorders Case questionnaire for diarrhoea negative/vtec (STEC) negative cases acute phase 1. INSTRUCTIONS Please
CQ_IBK_aHUS_01 / version 25/11/09 European Paediatric Research Group for HUS and related disorders Case questionnaire for diarrhoea negative/vtec (STEC) negative cases acute phase 1. INSTRUCTIONS Please
Eculizumab as Prophylactic Therapy in Atypical Hemolytic Uremic Syndrome in Adult Living-Related Kidney Transplantation
 Anti-C5 as Prophylactic Therapy in Atypical Hemolytic Uremic Syndrome in Living- Related Kidney Transplantation Authors: Miquel Blasco 1, Santiago Rodríguez de Córdoba 2, Fritz Diekmann 1, Mercedes Saiz
Anti-C5 as Prophylactic Therapy in Atypical Hemolytic Uremic Syndrome in Living- Related Kidney Transplantation Authors: Miquel Blasco 1, Santiago Rodríguez de Córdoba 2, Fritz Diekmann 1, Mercedes Saiz
A 60 year old woman with altered mental status and thrombotic microangiopathy. Josh Veatch
 A 60 year old woman with altered mental status and thrombotic microangiopathy Josh Veatch Previously healthy 60 year old woman 2 3 months of fatigue following a URI, transient episodes being out of it
A 60 year old woman with altered mental status and thrombotic microangiopathy Josh Veatch Previously healthy 60 year old woman 2 3 months of fatigue following a URI, transient episodes being out of it
Current evidence on the discontinuation of eculizumab in patients with atypical haemolytic uraemic syndrome
 Clinical Kidney Journal, 2016, 1 10 doi: 10.1093/ckj/sfw115 Original Article ORIGINAL ARTICLE Current evidence on the discontinuation of eculizumab in patients with atypical haemolytic uraemic syndrome
Clinical Kidney Journal, 2016, 1 10 doi: 10.1093/ckj/sfw115 Original Article ORIGINAL ARTICLE Current evidence on the discontinuation of eculizumab in patients with atypical haemolytic uraemic syndrome
Case report 24 th Summer School of Internal Medicine 2015
 Case report 24 th Summer School of Internal Medicine 2015 Goldmannová D., Horák P., Skácelová M. IIIrd Internal Clinic - endocrinology, diabetology, rheumatology, nephrology University hospital Olomouc,
Case report 24 th Summer School of Internal Medicine 2015 Goldmannová D., Horák P., Skácelová M. IIIrd Internal Clinic - endocrinology, diabetology, rheumatology, nephrology University hospital Olomouc,
Non-immune acquired haemolytic anaemias. Dr.Maysem
 Non-immune acquired haemolytic anaemias Dr.Maysem Causes of Non-immune acquired haemolytic anaemias. Infections Infections can cause haemolysis in a variety of ways: -They may precipitate an acute haemolytic
Non-immune acquired haemolytic anaemias Dr.Maysem Causes of Non-immune acquired haemolytic anaemias. Infections Infections can cause haemolysis in a variety of ways: -They may precipitate an acute haemolytic
Thrombocytopenia is not mandatory to diagnose haemolytic and uremic syndrome
 Sallée et al. BMC Nephrology 2013, 14:3 RESEARCH ARTICLE Open Access Thrombocytopenia is not mandatory to diagnose haemolytic and uremic syndrome Marion Sallée 1, Khalil Ismail 1, Fadi Fakhouri 2, Henri
Sallée et al. BMC Nephrology 2013, 14:3 RESEARCH ARTICLE Open Access Thrombocytopenia is not mandatory to diagnose haemolytic and uremic syndrome Marion Sallée 1, Khalil Ismail 1, Fadi Fakhouri 2, Henri
Medical Policy An independent licensee of the Blue Cross Blue Shield Association
 Soliris (eculizumab) Page 1 of 11 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: Soliris (eculizumab) Prime Therapeutics will review Prior Authorization requests
Soliris (eculizumab) Page 1 of 11 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: Soliris (eculizumab) Prime Therapeutics will review Prior Authorization requests
Soliris. Soliris (eculizumab) Description
 Description") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.85.11 Subject: Soliris Page: 1 of 5 Last Review Date: September 20, 2018 Soliris Description Soliris
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.85.11 Subject: Soliris Page: 1 of 5 Last Review Date: September 20, 2018 Soliris Description Soliris
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Acute lung injury (ALI) transfusion-related, 363 372. See also Transfusion-related acute lung injury (TRALI) ALI. See Acute lung injury
Index Note: Page numbers of article titles are in boldface type. A Acute lung injury (ALI) transfusion-related, 363 372. See also Transfusion-related acute lung injury (TRALI) ALI. See Acute lung injury
w ahus pathology is linked to dysregulation of the alternative complement pathway.
 ahus - Pathogenesis, Etiology, and Clinical Advances Craig B. Langman MD The Isaac A Abt MD Professor of Kidney Diseases Feinberg School of Medicine, Northwestern University Head, Kidney Diseases The Ann
ahus - Pathogenesis, Etiology, and Clinical Advances Craig B. Langman MD The Isaac A Abt MD Professor of Kidney Diseases Feinberg School of Medicine, Northwestern University Head, Kidney Diseases The Ann
PREGNANCY ASSOCIATED THROMBOTIC THROMBOCYTOPENIC PURPURA AND ACUTE KIDNEY INJURY
 VII, 2013, 2 33 A, PREGNANCY ASSOCIATED THROMBOTIC THROMBOCYTOPENIC PURPURA AND ACUTE KIDNEY INJURY M. Lubomirova Clinic of Nephrology, University Hospital Aleksandrovska So a : ( ), /HELLP, (AFLP) (TTP)
VII, 2013, 2 33 A, PREGNANCY ASSOCIATED THROMBOTIC THROMBOCYTOPENIC PURPURA AND ACUTE KIDNEY INJURY M. Lubomirova Clinic of Nephrology, University Hospital Aleksandrovska So a : ( ), /HELLP, (AFLP) (TTP)
monoclonal gammopathy of undetermin Citation Rheumatology international, 33(1),
,") NAOSITE: Nagasaki University's Ac Title Author(s) Renal thrombotic microangiopathies/ in a patient with primary Sjögren's monoclonal gammopathy of undetermin Koga, Tomohiro; Yamasaki, Satoshi; Atsushi;
NAOSITE: Nagasaki University's Ac Title Author(s) Renal thrombotic microangiopathies/ in a patient with primary Sjögren's monoclonal gammopathy of undetermin Koga, Tomohiro; Yamasaki, Satoshi; Atsushi;
Plasma exchange in thrombotic microangiopathies (TMAs) other than thrombotic thrombocytopenic purpura (TTP)
 other than thrombotic thrombocytopenic purpura (TTP)") THERAPEUTIC APHERESIS AS AN IMMUNOMODULATORY TOOL Plasma exchange in thrombotic microangiopathies (TMAs) other than thrombotic thrombocytopenic purpura (TTP) Jeffrey L. Winters Therapeutic Apheresis Treatment
THERAPEUTIC APHERESIS AS AN IMMUNOMODULATORY TOOL Plasma exchange in thrombotic microangiopathies (TMAs) other than thrombotic thrombocytopenic purpura (TTP) Jeffrey L. Winters Therapeutic Apheresis Treatment
A 23 year old Caucasian male presented with shortness of breath, hypertension, bloody sputum, and a history of drug abuse (confirmed by urinalysis).
.") A 23 year old Caucasian male presented with shortness of breath, hypertension, bloody sputum, and a history of drug abuse (confirmed by urinalysis). He was found to have severe kidney injury requiring
A 23 year old Caucasian male presented with shortness of breath, hypertension, bloody sputum, and a history of drug abuse (confirmed by urinalysis). He was found to have severe kidney injury requiring
Thrombotic Thrombocytopenic
 The Treatment of TTP and the Prevention of Relapses GERALD APPEL, MD Professor of Clinical Medicine Columbia University College of Physicians and Surgeons NY-Presbyterian Hospital New York, New York Thrombotic
The Treatment of TTP and the Prevention of Relapses GERALD APPEL, MD Professor of Clinical Medicine Columbia University College of Physicians and Surgeons NY-Presbyterian Hospital New York, New York Thrombotic
4100: Cellular Therapy Essential Data Follow-Up Form
 4100: Cellular Therapy Essential Data Follow-Up Form Registry Use Only Sequence Number: Date Received: Key Fields CIBMTR Center Number: Event date: Visit: 100 day 6 months 1 year 2 years >2 years, Specify:
4100: Cellular Therapy Essential Data Follow-Up Form Registry Use Only Sequence Number: Date Received: Key Fields CIBMTR Center Number: Event date: Visit: 100 day 6 months 1 year 2 years >2 years, Specify:
Thrombotic Microangiopathy (TMA) The Clinical Facets of TMA
 The Clinical Facets of TMA") International Consensus on Management Atypical Hemolytic Uremic Syndrome in Children Loirat C. et al. Pediatr Nephrol 31: 15-39, 2016 Ruth A. McDonald, MD Professor and Vice Chair Clinical Affairs Department
International Consensus on Management Atypical Hemolytic Uremic Syndrome in Children Loirat C. et al. Pediatr Nephrol 31: 15-39, 2016 Ruth A. McDonald, MD Professor and Vice Chair Clinical Affairs Department
PLASMA EXCHANGE J MANION NEPEAN HOSPITAL
 PLASMA EXCHANGE J MANION NEPEAN HOSPITAL PLASMA The fluid portion of blood Normally approx 5% body weight or 3.5L in 70kg male Clots on standing unless anticoagulated Common plasma proteins are albumin,
PLASMA EXCHANGE J MANION NEPEAN HOSPITAL PLASMA The fluid portion of blood Normally approx 5% body weight or 3.5L in 70kg male Clots on standing unless anticoagulated Common plasma proteins are albumin,
EDUCATIONAL COMMENTARY DISSEMINATED INTRAVASCULAR COAGULATION
 EDUCATIONAL COMMENTARY DISSEMINATED INTRAVASCULAR COAGULATION Educational commentary is provided through our affiliation with the American Society for Clinical Pathology (ASCP). To obtain FREE CME/CMLE
EDUCATIONAL COMMENTARY DISSEMINATED INTRAVASCULAR COAGULATION Educational commentary is provided through our affiliation with the American Society for Clinical Pathology (ASCP). To obtain FREE CME/CMLE
Assessing thrombocytopenia in the intensive care unit: The past, present, and future
 Assessing thrombocytopenia in the intensive care unit: The past, present, and future Ryan Zarychanski MD MSc FRCPC Sections of Critical Care and of Hematology, University of Manitoba Disclosures FINANCIAL
Assessing thrombocytopenia in the intensive care unit: The past, present, and future Ryan Zarychanski MD MSc FRCPC Sections of Critical Care and of Hematology, University of Manitoba Disclosures FINANCIAL
Thrombotic microangiopathy and indications for therapeutic plasma exchange
 SPIN DOCTORS:APHERESIS FOR HEMATOLOGISTS Thrombotic microangiopathy and indications for therapeutic plasma exchange Jill Adamski 1 1 Department of Laboratory Medicine and Pathology, Mayo Clinic Arizona,
SPIN DOCTORS:APHERESIS FOR HEMATOLOGISTS Thrombotic microangiopathy and indications for therapeutic plasma exchange Jill Adamski 1 1 Department of Laboratory Medicine and Pathology, Mayo Clinic Arizona,
An international consensus approach to the management of atypical hemolytic uremic syndrome in children
 DOI 10.1007/s00467-015-3076-8 REVIEW An international consensus approach to the management of atypical hemolytic uremic syndrome in children Chantal Loirat & Fadi Fakhouri & Gema Ariceta & Nesrin Besbas
DOI 10.1007/s00467-015-3076-8 REVIEW An international consensus approach to the management of atypical hemolytic uremic syndrome in children Chantal Loirat & Fadi Fakhouri & Gema Ariceta & Nesrin Besbas
Some renal vascular disorders
 Some renal vascular disorders Introduction Nearly all diseases of the kidney involve the renal blood vessels secondarily We will discuss: -Hypertension (arterionephrosclerosis in benign HTN & hyperplastic
Some renal vascular disorders Introduction Nearly all diseases of the kidney involve the renal blood vessels secondarily We will discuss: -Hypertension (arterionephrosclerosis in benign HTN & hyperplastic
Can eculizumab be discontinued in ahus? Case report and review of the literature
 Clinical Case Report Medicine Can eculizumab be discontinued in ahus? Case report and review of the literature Tuncay Sahutoglu, MD a,, Taner Basturk, MD a, Tamer Sakaci, MD a, Yener Koc, MD a, Elbis Ahbap,
Clinical Case Report Medicine Can eculizumab be discontinued in ahus? Case report and review of the literature Tuncay Sahutoglu, MD a,, Taner Basturk, MD a, Tamer Sakaci, MD a, Yener Koc, MD a, Elbis Ahbap,
Soliris (eculizumab): Physician s guide to prescribing for patients with paroxysmal nocturnal haemoglobinuria (PNH)
: Physician s guide to prescribing for patients with paroxysmal nocturnal haemoglobinuria (PNH)") Soliris (eculizumab): Physician s guide to prescribing for patients with paroxysmal nocturnal haemoglobinuria (PNH) CONTENTS PAGE WHAT IS SOLIRIS? SOLIRIS INDICATIONS IMPORTANT SAFETY INFORMATION SOLIRIS
Soliris (eculizumab): Physician s guide to prescribing for patients with paroxysmal nocturnal haemoglobinuria (PNH) CONTENTS PAGE WHAT IS SOLIRIS? SOLIRIS INDICATIONS IMPORTANT SAFETY INFORMATION SOLIRIS
PNH ahus. Dosing and Administration. For Paroxysmal Nocturnal Hemoglobinuria (PNH) and atypical Hemolytic Uremic Syndrome (ahus) patients
 and atypical Hemolytic Uremic Syndrome (ahus) patients") For Paroxysmal Nocturnal Hemoglobinuria (PNH) and atypical Hemolytic Uremic Syndrome (ahus) patients PNH ahus Dosing and Administration Soliris is indicated for the treatment of patients with paroxysmal
For Paroxysmal Nocturnal Hemoglobinuria (PNH) and atypical Hemolytic Uremic Syndrome (ahus) patients PNH ahus Dosing and Administration Soliris is indicated for the treatment of patients with paroxysmal
PREGNANCY ASSOCIATED ATYPICAL HEMOLYTIC UREMIC SYNDROME: CLINICAL CASE AND LITERATURE REVIEW.
 18 PREGNANCY ASSOCIATED ATYPICAL HEMOLYTIC UREMIC SYNDROME: CLINICAL CASE AND LITERATURE REVIEW. Gabija Didziokaite 1, Jelena Volochovic 1, 2, Ramune Simkeviciute 2 1. Vilnius University, Faculty of Medicine
18 PREGNANCY ASSOCIATED ATYPICAL HEMOLYTIC UREMIC SYNDROME: CLINICAL CASE AND LITERATURE REVIEW. Gabija Didziokaite 1, Jelena Volochovic 1, 2, Ramune Simkeviciute 2 1. Vilnius University, Faculty of Medicine
Hemolytic uremic syndrome with simultaneous Shiga toxin producing Escherichia coli and complement abnormalities
 McCoy and Weaver BMC Pediatrics 2014, 14:278 CASE REPORT Open Access Hemolytic uremic syndrome with simultaneous Shiga toxin producing Escherichia coli and complement abnormalities Nicole McCoy 1 and Donald
McCoy and Weaver BMC Pediatrics 2014, 14:278 CASE REPORT Open Access Hemolytic uremic syndrome with simultaneous Shiga toxin producing Escherichia coli and complement abnormalities Nicole McCoy 1 and Donald
Coding... 5 Benefit Application... 5 Description of Services... 6 Clinical Evidence... 7
 TABLE OF CONTENTS Product Variations.... 1 Policy Statement.... 1 Related Policies.... 4 Policy Guidelines..... 4 Coding.... 5 Benefit Application........ 5 Description of Services..... 6 Clinical Evidence.......
TABLE OF CONTENTS Product Variations.... 1 Policy Statement.... 1 Related Policies.... 4 Policy Guidelines..... 4 Coding.... 5 Benefit Application........ 5 Description of Services..... 6 Clinical Evidence.......
Blood transfusion. Dr. J. Potgieter Dept. of Haematology NHLS - TAD
 Blood transfusion Dr. J. Potgieter Dept. of Haematology NHLS - TAD General Blood is collected from volunteer donors >90% is separated into individual components and plasma Donors should be: healthy, have
Blood transfusion Dr. J. Potgieter Dept. of Haematology NHLS - TAD General Blood is collected from volunteer donors >90% is separated into individual components and plasma Donors should be: healthy, have
Clinical Commissioning Policy Statement: Eculizumab for atypical haemolytic uraemic syndrome. September 2013 Reference: E03/PS(HSS)/a.
/a.") Clinical Commissioning Policy Statement: Eculizumab for atypical haemolytic uraemic syndrome September 2013 Reference: E03/PS(HSS)/a England 1 NHS England INFORMATION READER BOX Directorate Medical Operations
Clinical Commissioning Policy Statement: Eculizumab for atypical haemolytic uraemic syndrome September 2013 Reference: E03/PS(HSS)/a England 1 NHS England INFORMATION READER BOX Directorate Medical Operations
Acquired Drivers of Disaese ahus and autoantibodies: their role in disease and their impact on patient management
 Acquired Drivers of Disaese ahus and autoantibodies: their role in disease and their impact on patient management Veronique Fremeaux-Bacchi Cordeliers Research Center and Européen Georges Pompidou Hospital,
Acquired Drivers of Disaese ahus and autoantibodies: their role in disease and their impact on patient management Veronique Fremeaux-Bacchi Cordeliers Research Center and Européen Georges Pompidou Hospital,
Symposium. Acute Kidney Injury with Thrombocytopenia. Lalitha A V*, Suryanarayana G**, Sumithra S***
 Symposium Acute Kidney Injury with Thrombocytopenia 10.21304/2018.0502.00372 Lalitha A V*, Suryanarayana G**, Sumithra S*** *Associate Professor, Head,PICU **, Fellow in PICU, *** Assistant Professor,
Symposium Acute Kidney Injury with Thrombocytopenia 10.21304/2018.0502.00372 Lalitha A V*, Suryanarayana G**, Sumithra S*** *Associate Professor, Head,PICU **, Fellow in PICU, *** Assistant Professor,