Variable Updates January 2014
|
|
|
- Della Riley
- 5 years ago
- Views:
Transcription


1 Variable Updates January 2014
2 Surgeon National Provider Identifier (NPI) Variable Name: Surgeon NPI Intent of Variable: For sites to have the ability to track each surgeon s surgical cases. Definition: The National Provider Identifier (NPI) is a Health Insurance Portability and Accountability Act (HIPAA) Administrative Simplification Standard. The NPI is a unique identification number for covered health care providers. Covered health care providers and all health plans and health care clearinghouses must use the NPIs in the administrative and financial transactions adopted under HIPAA. The NPI is a 10-position, intelligence-free numeric identifier (10-digit number). This means that the numbers do not carry other information about healthcare providers, such as the state in which they live or their medical specialty. Criteria: Assign the Attending Surgeon s NPI. Options: Select the appropriate Surgeon (NPI). Centers for Medicare & Medicaid Services (2012). Retrieved February 19, 2013 from Simplification/NationalProvIdentStand/index.html?redirect=/nationalprovidentstand/
3 Tumor involving CNS This variable will no longer be collected for cases with January 1, 2014 operation dates. The DDC felt that this is a repeat of a child who would be captured with the variable of Childhood Malignancy.
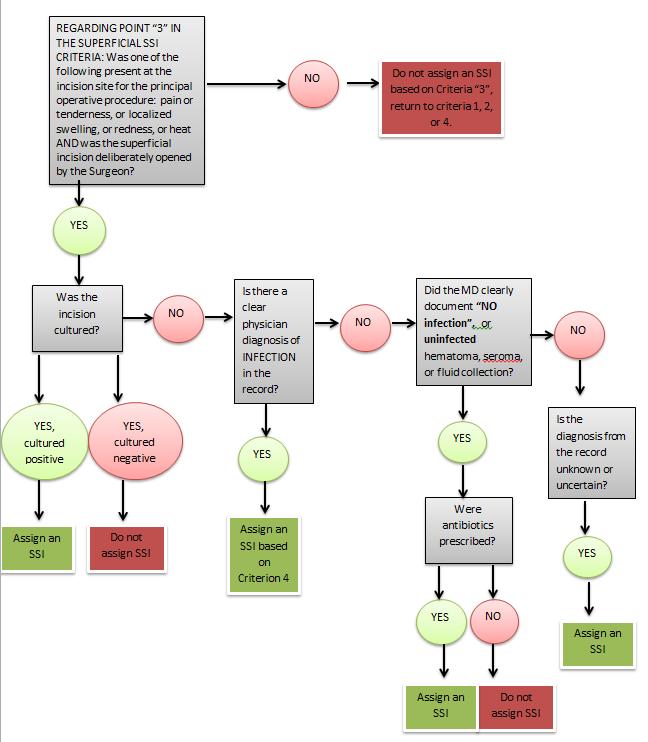
4 Superficial SSI Criteria: An infection that occurs within 30 days of the principal operative procedure AND the infection involves only skin or subcutaneous tissue of the incision AND at least ONE of the following: 1. Purulent drainage, with or without laboratory confirmation, from the superficial incision 2. Organisms isolated from an aseptically obtained culture of fluid or tissue from the superficial incision 3. Superficial incision is deliberately opened by the surgeon and has at least one of the following signs or symptoms of infection: pain or tenderness localized swelling redness or heat EXCEPTION: to this criterion (only) is if the wound is cultured and results return negative, the occurrence would not be assigned based on this criterion. 4. Diagnosis of superficial incisional SSI by the surgeon or attending physician
5
6 Superficial SSI Scenarios to Clarify (Assign Variable): Superficial SSI occurs at a drain site in which the drain was placed during the principal operative procedure. Surgical Site documentation of pus in superficial layers, redness, wound opened and cultured, cultures return negative. (Assign SSI as this scenario meets criteria with purulent drainage) Scenarios to Clarify (Do Not Assign Variable): Stitch abscess (minimal inflammation and discharge confined to the points of suture penetration) Infected burn wound Incisional SSI that extends into the fascia and muscle layers (see deep incisional SSI) Diagnosis of cellulitis alone Diagnosis of vaginitis after vaginal surgery Diagnosis of oral thrush after oral surgery Report infection that involves both superficial and deep incision sites as deep incisional SSI Notes: Only SSIs at the incision site of the principal operative procedure should be assessed. Incision sites for other or concurrent procedures, if they are in distinctly different anatomical sites should not be assessed. If there is question as to whether or not an incision site was an integral portion of the principal operative procedure, include this site in your SSI assessment. Please be aware that a single principal operative procedure can have more than one incision.
7 Organ/Space SSI Criteria: An infection that occurs within 30 days of the principal operative procedure AND involves any of the anatomy (e.g., organs or spaces), other than the incision, which was opened or manipulated during the operation AND at least ONE of the following: Purulent drainage from a drain that is placed through a stab wound into the organ/space. Organisms isolated from an aseptically obtained culture of fluid or tissue in the organ/space An abscess or other evidence of infection involving the organ/space that is found on direct examination, during reoperation, or by histopathologic or radiologic examination Diagnosis of an organ/space SSI by a surgeon or attending physician Scenarios to Clarify (Assign Variable): Anastomotic leaks involving the GI or GU system or which involve enteric contents Diagnosis of an inner ear infection following a tympanoplasty Scenarios to Clarify (Do Not Assign Variable): A diagnosis of C-Diff following a principal operative procedure will not be included as an organ/space site infection Report an organ/space SSI that drains through the incision as a deep incisional SSI Fistulas alone, unless they independently meet the other criteria listed above
8 SSI Key Notes: Diagnosis of vaginitis alone after vaginal surgery will not be assigned unless meets other criteria Diagnosis of oral thrush alone after oral surgery will not be assigned unless meets other criteria Have included an algorithm to help with infections that may meet criterion 3 in appendix J C- Diff in isolation will no longer meet criteria to assign an organ/space infection This is in conjunction with the program wide variable for surgical site infections.
9 ICD 9/ICD10 Codes Beginning January 1, 2014 sites will have the option of using ICD-9 or ICD-10 Codes for these variables with ICD code fields. Other Postoperative Occurrence (ICD Code) Postoperative Diagnosis (ICD Code) Hospital Readmission Reoperation These variables will continue to utilize the associated ICD 9 codes with the diagnoses on the collect lists to be entered Cardiac ICD 9 Congenital Malformation.
10 Sepsis Within 48 Hours Prior to Surgery (SIRS/Sepsis/Septic Shock): The criteria for Pediatric Systemic Inflammatory Response Syndrome (SIRS) described below without evidence of infection constitute SIRS. The criteria for Sepsis are the presence of SIRS accompanied by one of the criteria of Infection. The criteria for Septic Shock are the presence of Sepsis accompanied by one of the criteria for Cardiovascular Dysfunction. The criteria for SIRS/Sepsis/Septic Shock must be met within 48 hours prior to the principal operative procedure. SIRS Criteria: Two of the four following criteria must be met and must be noted within 48 hours prior to principal operative procedure, but one of the two must be either Temperature or Leukocyte count. However, temperature and leukocyte count together satisfy these criteria as two of the four following criteria. Please note the Removal of in the absence of external or painful stimuli requirement from the tachycardia and Respiratory rate options. Temperature >38 C or <36 C (oral, axillary, rectal, tympanic or central catheter probe) Leukocyte count (Table 1 below) elevated or depressed for age with leukopenia not secondary to chemotherapy Tachycardia (Table 1 below) in the absence of drugs, which persists for >30 minutes. For children < 1 yr. of age: bradycardia (Table 1 below), in the absence of deep sedation, beta blockers, or other cardioactive drugs which persists for >30 minutes. Respiratory rate (Table 1 below) which persists for >30 minutes, OR a requirement for mechanical ventilation not related to underlying neuromuscular disease. For children < 1 yr. of age: documented apnea.
11 Sepsis Within 48 Hours Prior to Surgery (SIRS/Sepsis/Septic Shock): SEPSIS Criteria: Criteria for both Pediatric Systemic Inflammatory Response Syndrome (SIRS) and Infection must be met to assign Sepsis. The criteria for SIRS must be noted within 48 hours prior to principal operative procedure. The criteria for infection may be noted within 48 hours prior to the principal operative procedure (Criterion A) or at the time of the principal operative procedure (Criterion B). Infection Criterion A: SIRS criteria must be met within 48 hours before the principal operative procedure. And One of the following: Positive blood culture Radiologic evidence of an abscess Clinical documentation of purulence at, or a positive culture from, any site which is documented by a physician as being thought to be the cause of the septic picture Infection Criterion B: Findings at principal operative procedure SIRS criteria must be met within 48 hours before the principal operative procedure. And One of the following: Ischemic/infarcted bowel requiring resection Enteric contents in the operative site Purulence in the operative site Positive intraoperative culture Perforated bowel or other viscus
12 Sepsis Within 48 Hours Prior to Surgery (SIRS/Sepsis/Septic Shock): Septic Shock Criteria: The patient must meet the criteria for Sepsis (SIRS criteria and Infection Criteria). And in addition the patient must require one of the vasoactive drugs from the list below to maintain perfusion, or an increase in dose if a patient is already receiving a vaso active drug. Dopamine Dobutamine Epinephrine Norepinephrine Vasopressin Isoproterenol Ephedrine Inamrinone Milrinone * Only the drugs from this list may be used to assign Septic Shock
13 Sepsis Within 48 Hours Prior to Surgery (SIRS/Sepsis/Septic Shock): SIRS A 10 yo girl presents with a 4 hour history of mild cramping RLQ pain which has suddenly become acute. On examination she has RLQ muscle spasm and percussion tenderness. Temp is 37 C tympanic, HR 140, RR 20, WBC 8.3. An ultrasound shows an enlarged, non cystic right ovary. At laparoscopy she has a gangrenous ovarian torsion which is reduced. The ovary is not removed. Although the patient is tachycardic and tachypneic, neither her temperature nor her WBC is abnormal for age and she does not meet the SIRS criteria. Sepsis If the patient described above had a WBC of 14.0 she would meet the SIRS criteria. If the gangrenous ovary were resected she would not meet the infection criteria because Infection Criterion B requires infarcted/perforated bowel.
14 Postoperative Systemic Sepsis Criteria for both Pediatric Systemic Inflammatory Response Syndrome (SIRS), and Infection must be met within 30 days after the principal operative procedure. To assign Postoperative Systemic Sepsis the patient must meet SIRS criteria and the criteria for Infection. Infection Criterion A may be used at any time in the 30 day postoperative period: SIRS criteria must be met within 48 hours in the postoperative period before or after one of the following findings. Positive blood culture Radiologic evidence of an abscess Clinical documentation of purulence at, or a positive culture from, any site which is documented by a physician as being thought to be the cause of the septic picture Infection Criterion B are the findings of the operation. For principal operative procedure SIRS criteria must be met within 7 days following the principal operative procedure. For reoperation SIRS criteria must be met within 48 hours before the reoperation or 7 days after the reoperation. Operative Findings: Ischemic/infarcted bowel requiring resection Enteric contents in the operative site Purulence in the operative site Positive intraoperative culture Perforated bowel or other viscus
15 Postoperative Systemic Sepsis For an event to be considered a Postoperative Occurrence of Systemic Sepsis when sepsis was present preoperatively there must be a new source of infection. If Sepsis was present preoperatively without Septic Shock, progression to Septic Shock postoperatively is assigned as a Postoperative Occurrence of Septic Shock. Only the highest level of Sepsis/ Septic Shock is assigned as an occurrence. If the patient meets criteria for sepsis and the criteria for septic shock, only the occurrence of septic shock is assigned. Do not use positive screening tests that are done to determine the presence of organisms that may only increase the risk of infection. Positive screening tests are not acceptable as proof of infection. Examples include: throat screens for beta hemolytic Streptococcus, swabs for Methicillin-resistant Staphylococcus aureus (MRSA) and Vancomycin-resistant Enterococci (VRE). There must be a positive culture from an affected site or a positive blood culture. A child may meet criteria for SIRS and may meet criteria for Cardiovascular Dysfunction, and clinically be in shock. However, unless the Sepsis criteria are met, the event may not be assigned as Septic Shock. Although this scenario occurs clinically, there is no consensus in the critical care literature for the recognition of SIRS with Shock as a separate entity.
16 Post operative Sepsis A patient has an appendectomy for perforated appendicitis with generalized peritonitis and meets the SIRS criteria preoperatively. The patient is assigned pre-operative sepsis. On POD 6 the patient meets SIRs criteria and a CT scan demonstrates a pelvic abscess, Although the patient meets post operative SIRs criteria This does not fulfill the requirement that there is a new source of infection, because the perforation which existed preoperatively is the cause of the post operative abscess. Post-operative sepsis is not assigned
17 Post operative Sepsis A patient has a gangrenous appendicitis but does not meet the SIRS criteria preoperatively. On POD 5 the patient is febrile, tachycardic and tachypneic, and meets the SIRS criteria for age. On POD 6 the patient undergoes exploratory laparotomy. The patient is found to have a small bowel obstruction due to a phlegmon. Culture from phlegmon grows aerobic and anaerobic organisms. The positive intraoperative culture meets Criterion B and postoperative sepsis is assigned.
18 Post operative Septic Shock A 12 yo patient has an appendectomy for perforated appendicitis with generalized peritonitis and meets the criteria for Preoperative Sepsis. Postoperatively, he is febrile each afternoon to 39 C, his white blood count remains elevated. On the morning of the 4 th postoperative day, his white count is 15,000. That afternoon, a CT scan is done which demonstrates a multi-loculated pelvic abscess. On return from the radiology suite, he becomes tachycardic to 150, and his blood pressure falls to 73/50. He fails to respond to a 60 ml/kg bolus of isotonic crystalloid and is begun on dopamine. Over the next hour with the continuation of isotonic crystalloid, his pulse rate falls to 120, his pressure returns to 100/48, but he continues to require dopamine to maintain perfusion. Although the patient had Sepsis preoperatively and the pelvic abscess does not constitute a new source of infection, progression to shock postoperatively which requires the use of a vasoactive drug to maintain perfusion is assigned as a Postoperative Septic Shock occurrence.
19 Post operative Sepsis/Shock A neonate is on a vasoactive drug preoperatively due to cardiac dysfunction and goes to the OR for a tracheostomy. Postoperatively, the patient develops SIRS, has a positive blood culture, and is maintained on the same dose of vasoactive drug as the preoperative dose. The patient does not require an increase in dosage of the vasoactive drug and does not require the addition of a second vasoactive drug. This patient would be assigned the occurrence of Postoperative Sepsis, but would not be assigned Post operative Septic Shock.
20 SIRS/Sepsis/Septic Shock Key Notes: The statement of in the absence of external or painful stimuli which persists for >30 minutes has been removed for the SIRs criteria requirements of tachycardia and tachypnea. Infection Criterion A may be used at any time in the 30 day postoperative period, SIRS criteria must be met in the postoperative period 48 hours before or after any one of the findings in Criterion A. Infection Criterion B: for the principal operative procedure, SIRS criteria must be met within 7 days following the principal operative procedure. Infection Criterion B: for a reoperation, SIRS criteria must be met within 48 hours before or 7 days after the reoperation
21 Congenital Malformation Tips for abstracting the Preoperative Risk Factor: Congenital Malformation 1. Always start with the diagnosis found in the medical record (not the ICD-9 problem list). 2. Review the provided Collect List and only collect the congenital malformation diagnoses that are on the Collect List. 3. Once the diagnosis has been verified, utilize the assigned ICD-9 code associated with the diagnosis provided on the collect list and enter it into the workstation. If there are multiple diagnoses on the collect list, all malformation ICD-9 codes should be entered. 4. Do not record anything in the Severity Field. This field is not required, and may be left blank.
22 Congenital Malformation 5. Congenital malformations are present at birth but may not have been diagnosed till later in infancy or childhood. The diagnoses on the list with an asterisk (*) indicates conditions to be collected only if diagnosed before the age of 4 years. 6. If a child has a syndrome, review the medical chart for any components of the syndrome that are included on the Collect List 7. Submit to Clinical Support the name, description, and ICD-9 code of any congenital malformation identified that is not included on either provided lists ( Collect or Do Not Collect ); this information will be used to modify these lists in the future.
23 Congenital Malformation Syndromes are groups of conditions or congenital malformations that tend to occur together frequently. The presentation of the associated congenital malformations and/or associated pre-operative risk factors variables may vary widely. A patient with any syndrome requires an analysis/review of the medical record for the presence of those conditions known to be associated with the syndrome. The appropriate congenital malformations associated with the syndrome that are included on the Collect List should be recorded, along with the corresponding preoperative variable, if any.
24 Congenital Malformation Variable Name: Congenital Malformations Program Legend: Pediatric Intent of Variable: Identify patients with, or with a history of, a congenital defect at the time of the principal operative procedure. Definition: A structural, functional or genetic abnormality present at birth. Criteria: Record the documented congenital malformation(s) present, or a history of the congenital malformation(s) from the Provided Collect List of malformations found in appendix J along with its associated code.
25 Congenital Malformation Scenarios to Clarify (Assign Variable): Some diagnoses can be congenital or acquired (e.g. scoliosis). For the Congenital Malformation variable, these diagnoses are only included if the diagnosis was made at the age of 3 years or before. These diagnoses are marked with an asterisk (*) in the Collect List. All other congenital malformation diagnoses (those without asterisk) on the Collect List are collected regardless of diagnostic time frame as the congenital malformation was present at birth but may not have been diagnosed till later in infancy or childhood. A patient has the diagnosis of Malrotation should be collected no matter when it is diagnosed and no matter if it associated with volvulus or not assign Congenital Anomalies of intestinal Fixation and assign the Esophageal/Gastric Disease/Intestinal variable. A patient has a diagnosis of in utero alcohol, cocaine, heroin, etc... exposure - assign Nox Affecting Newborn Alcohol Patients with any cleft palate code (749.2, , , , , , ) should be assigned Cleft Palate And Cleft Lip. Syndromes are groups of conditions or congenital malformations that tend to occur together frequently. The presentation of the associated congenital malformations and/or associated pre-operative risk factors variables may vary widely. A patient with any syndrome requires an analysis/review of the medical record for the presence of those conditions known to be associated with the syndrome. The appropriate preoperative variables that apply to the patient should be selected. VACTERL (or VATER) may include the following congenital abnormalities: Vertebral defect, anorectal defects, cardiac defects, tracheoesophageal defects, renal/kidney defects, limb defects and growth. Collect all codes that the patient has on the provided Collect List. CHARGE Association assign Conditions Due To Anomalies Of Unspecified Chromosome. Review the medical record for the presence of those known associated conditions that may be present with the syndrome. Record those that the patient has. Record those that the patient has that are on the Collect List. Remember to also select the appropriate preoperative variables which apply to the patient.
26 Congenital Malformation Thoracic Insufficiency Syndrome (Jeune s Syndrome) These patients frequently requires VEPTR surgery. Assign Congenital Musculoskeletal Deformities of Spine. Scenarios to Clarify (Do Not Assign Variable): For diagnoses that can be congenital or acquired (e.g. scoliosis), do NOT include if the diagnosis was made at the age of 4 years or older. These diagnoses are marked with an asterisk (*) in the Collect List. Notes: Collect all congenital malformation diagnoses for the patient that are listed on the provided Collect List. Do Not record congenital malformations found on the Do Not Collect list. Please note that this list is NOT all inclusive and can be found in Appendix J. Submit to clinical support the name, description and ICD-9 code of any congenital malformation identified that is not included on the provided lists; this information will be used to modify the lists in the future. This list of submitted diagnoses from the SCR s will be reviewed by the DDC-P and /or M&E Committee and the ACS for possible revision of the definition. Only specific Congenital Malformation diagnoses that are on the provided Collect List are recorded in the Congenital Malformation variable and also in the appropriate preoperative risk variable. Enter (Yes) if congenital malformation(s) is on the provided Collect List. Enter the associated code or codes from the Collect List. Assign to appropriate Neonate category. (Neonates < 1500 grams at the time of surgery / Neonates 1500 grams at the time of surgery or infants/children/teenagers with a history of a congenital defect at the time of surgery). Do NOT record anything in the Severity field.
27 Congenital Malformation/Syndrome Practice A newborn patient is transferred to your hospital for a TE fistula repair and posterior sagital anorectoplasty for an imperforate anus. Upon review of the medical chart you find the patient has VACTERL association.
28 Congenital Malformation/Syndrome Practice VACTERL (or VATER) association is a disorder that affects many body systems. VACTERL stands for Vertebral defects, Anorectal defects, Cardiac defects, Tracheoesophageal defects, Renal/kidney defects, and Limb abnormalities. People diagnosed with VACTERL association typically have at least three of these characteristic features. Affected individuals may have additional abnormalities that are not among the characteristic features of VACTERL association. Collect all codes that the patient has on the provided Collect List.
29 Congenital Malformation/Syndrome Practice Upon further chart review you find the patient has additional malformations: VSD syndactyly of the right middle and ring fingers Hemivertebra of the midthoracic spine resulting in scoliosis Right renal agenisis Single Umbilical artery Hypospadias Congenital Hypothyroidism What should you capture?
30 Congenital Malformation/Syndrome Practice Imperforate Anus - Congenital Malformation(751.2) - Esophageal/Gastric Disease/Intestinal TEF- Congenital Malformation (750.3)- Esophageal/Gastric Disease/Intestinal VSD-Cardiac Risk-Minor Cardiac Risk-(745.4) Syndactyly(of the right middle and ring fingers)- Do not collect Scoliosis*- (caused by hemivertebra of the midthoracic spine)-congenital Malformation (754.2)
31 Congenital Malformation/Syndrome Practice Right Renal Agenesis - Congenital Malformation (753.0) Single Umbilical Artery- Do not collect Hypospadias Do not collect Congenital Hypothyroidism- Congenital Malformation (243) Some diagnoses can be congenital or acquired (e.g. scoliosis). For the Congenital Malformation variable, these diagnoses are only included if the diagnosis was made at the age of 3 years or before. These diagnoses are marked with an asterisk (*) in the Collect List. All other congenital malformation diagnoses (those without asterisk) on the Collect List are collected regardless of diagnostic time frame as the congenital malformation was present at birth but may not have been diagnosed till later in infancy or childhood.
32 Congenital Malformation Key Changes Do not record anything in the Severity Field. This field is not required, and may be left blank. Diagnoses on the Collect and Do Not Collect lists have been updated The Collect list is organized by systems and alphabetical lists in the variable definition The Do not collect list is located in Appendix J Some diagnoses can be congenital or acquired (e.g. scoliosis). For the Congenital Malformation variable, these diagnoses are only included if the diagnosis was made at the age of 3 years or before. These diagnoses are marked with an asterisk (*) in the Collect List. All other congenital malformation diagnoses (those without asterisk) on the Collect List are collected regardless of diagnostic time frame as the congenital malformation was present at birth but may not have been diagnosed till later in infancy or childhood.
July 2013 Updates CONGENITAL MALFORMATION HEIGHT/WEIGHT COLLECTION SCR ADVISORY COMMITTEE- DAILY PROCESS
 July 2013 Updates CONGENITAL MALFORMATION HEIGHT/WEIGHT COLLECTION SCR ADVISORY COMMITTEE- DAILY PROCESS Congenital Malformation JULY 2013 Congenital Malformation Rationale for change: Instead of collecting
July 2013 Updates CONGENITAL MALFORMATION HEIGHT/WEIGHT COLLECTION SCR ADVISORY COMMITTEE- DAILY PROCESS Congenital Malformation JULY 2013 Congenital Malformation Rationale for change: Instead of collecting
Pediatric SC/SCR Education Session: Difficult Definitions. NSQIP Annual Meeting July 26, 2014
 Pediatric SC/SCR Education Session: Difficult Definitions NSQIP Annual Meeting July 26, 2014 Actual patient Chart Abstraction: The Challenge o Demographics o Risk factors o Events/occurrences Documentation
Pediatric SC/SCR Education Session: Difficult Definitions NSQIP Annual Meeting July 26, 2014 Actual patient Chart Abstraction: The Challenge o Demographics o Risk factors o Events/occurrences Documentation
Pediatric SCR Discussion of Complex Clinical Scenarios NSQIP Annual Meeting July 26, 2015
 Pediatric SCR Discussion of Complex Clinical Scenarios NSQIP Annual Meeting July 26, 2015 Scenario 1: Postoperative SSI A 16 year-old patient Principal Operative Procedure: Incision and Drainage for monoarticular
Pediatric SCR Discussion of Complex Clinical Scenarios NSQIP Annual Meeting July 26, 2015 Scenario 1: Postoperative SSI A 16 year-old patient Principal Operative Procedure: Incision and Drainage for monoarticular
Schematic of diagnosing surgical site infections
 Schematic of diagnosing surgical site infections Infection occurred within 30 days after an operation if no implant is in place within one year if an implant is in place eg. hip replacement Do NOT report
Schematic of diagnosing surgical site infections Infection occurred within 30 days after an operation if no implant is in place within one year if an implant is in place eg. hip replacement Do NOT report
ACS NSQIP Pediatric SCR: Complex Clinical Scenarios and Variable Review
 ACS NSQIP Pediatric SCR: Complex Clinical Scenarios and Variable Review Disclosures The following planners, speakers, moderators, and/or panelists of the CME/CEU activity have no relevant financial relationships
ACS NSQIP Pediatric SCR: Complex Clinical Scenarios and Variable Review Disclosures The following planners, speakers, moderators, and/or panelists of the CME/CEU activity have no relevant financial relationships
SURGICAL SITE INFECTIONS: SURVEILLANCE & PREVENTION
 SURGICAL SITE INFECTIONS: SURVEILLANCE & PREVENTION Facts There were an estimated 157,500 surgical site infections associated with inpatient surgeries in 2011. SSIs were the most common healthcare-associated
SURGICAL SITE INFECTIONS: SURVEILLANCE & PREVENTION Facts There were an estimated 157,500 surgical site infections associated with inpatient surgeries in 2011. SSIs were the most common healthcare-associated
January 2015 Updates. Dec.4, 2014 SCR Education Call
 January 2015 Updates Dec.4, 2014 SCR Education Call Trauma codes Trauma cases specifically: Any injury with a principal ICD-9 or ICD-10 diagnostic code will be excluded from sampling within the range of:
January 2015 Updates Dec.4, 2014 SCR Education Call Trauma codes Trauma cases specifically: Any injury with a principal ICD-9 or ICD-10 diagnostic code will be excluded from sampling within the range of:
NEW DEFINITION FORMAT AND DIFFICULT VARIABLE DEFINITIONS
 NEW DEFINITION FORMAT AND DIFFICULT VARIABLE DEFINITIONS Bruce L. Hall, MD, PhD, MBA, FACS Clinical Support Physician Lead Paula Farrell, RN, BSN ACS NSQIP Clinical Support Specialist Case Studies &
NEW DEFINITION FORMAT AND DIFFICULT VARIABLE DEFINITIONS Bruce L. Hall, MD, PhD, MBA, FACS Clinical Support Physician Lead Paula Farrell, RN, BSN ACS NSQIP Clinical Support Specialist Case Studies &
Categorizing Wound Infections: A Comparison between ACS-NSQIP and an Institutional Surgical Secondary Events Database
 : A Comparison between ACS-NSQIP and an Institutional Surgical Secondary Events Database Luke V. Selby MD, Daniel D. Sjoberg MS, Danielle Cassella MA, Mindy Sovel MPH MS, David R. Jones MD, Vivian E. Strong
: A Comparison between ACS-NSQIP and an Institutional Surgical Secondary Events Database Luke V. Selby MD, Daniel D. Sjoberg MS, Danielle Cassella MA, Mindy Sovel MPH MS, David R. Jones MD, Vivian E. Strong
RECOGNISINGSURGICAL SITE INFECTIONS(SSIs) NOVEMBER 2017
 NOVEMBER 2017") RECOGNISINGSURGICAL SITE INFECTIONS(SSIs) NOVEMBER 2017 Welcome to this training resource. It has been designed for all healthcare workers involved in coordinating SSI surveillance, SSI surveillance data
RECOGNISINGSURGICAL SITE INFECTIONS(SSIs) NOVEMBER 2017 Welcome to this training resource. It has been designed for all healthcare workers involved in coordinating SSI surveillance, SSI surveillance data
August SCR Educational Call
 ugust SCR Educational Call SCR Certification Exam CS NSQIP SCR Certification Exam Policy is posted to the CS NSQIP Main page 2014 Exam- Round 1 starts September 8 Round 1- will be open for 3 weeks Rounds
ugust SCR Educational Call SCR Certification Exam CS NSQIP SCR Certification Exam Policy is posted to the CS NSQIP Main page 2014 Exam- Round 1 starts September 8 Round 1- will be open for 3 weeks Rounds
Quality ID #357: Surgical Site Infection (SSI) National Quality Strategy Domain: Effective Clinical Care
 National Quality Strategy Domain: Effective Clinical Care") Quality ID #357: Surgical Site Infection (SSI) National Quality Strategy Domain: Effective Clinical Care 2018 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY MEASURE TYPE: Outcome DESCRIPTION: Percentage
Quality ID #357: Surgical Site Infection (SSI) National Quality Strategy Domain: Effective Clinical Care 2018 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY MEASURE TYPE: Outcome DESCRIPTION: Percentage
Discussion of Complex Clinical Scenarios and Variable Review ACS NSQIP Clinical Support Team
 Discussion of Complex Clinical Scenarios and Variable Review CS NSQIP Clinical Support Team SCR Open Q& Calls The CS NSQIP Clinical Team is trialing Open format Q& calls for NSQIP SCRs Participation in
Discussion of Complex Clinical Scenarios and Variable Review CS NSQIP Clinical Support Team SCR Open Q& Calls The CS NSQIP Clinical Team is trialing Open format Q& calls for NSQIP SCRs Participation in
Topics for discussion. Pediatric General Surgery. Physiology. Surgical Newborns. Neonatal Intestinal Obstruction
 Topics for discussion Pediatric General Surgery Professor General & Thoracic Surgery What makes Pediatric Surgery unique? Neonatal intestinal obstruction Abdominal wall defects Inguinal hernias Appendicitis
Topics for discussion Pediatric General Surgery Professor General & Thoracic Surgery What makes Pediatric Surgery unique? Neonatal intestinal obstruction Abdominal wall defects Inguinal hernias Appendicitis
Infection Control: Surgical Site Infections
 Infection Control: Surgical Site Infections Infectious Disease Epidemiology Section Office of Public Health Louisiana Dept of Health & Hospitals 800-256-2748 www.oph.dhh.louisiana.gov Your taxes at work
Infection Control: Surgical Site Infections Infectious Disease Epidemiology Section Office of Public Health Louisiana Dept of Health & Hospitals 800-256-2748 www.oph.dhh.louisiana.gov Your taxes at work
Adult Surgical Clinical Reviewer: Discussion of Complex Clinical Scenarios and Variable Review
 Adult Surgical Clinical Reviewer: Discussion of Complex Clinical Scenarios and Variable Review Disclosures The following individuals have no actual or potential conflicts of interest in relation to this
Adult Surgical Clinical Reviewer: Discussion of Complex Clinical Scenarios and Variable Review Disclosures The following individuals have no actual or potential conflicts of interest in relation to this
None of the authors has any disclosures or conflicts of interest to report
 None of the authors has any disclosures or conflicts of interest to report The Effect OF PATOS (Present At the Time Of Surgery) On The Calculation of SSI Rates for Appendectomy and Colectomy: Is PATOS
None of the authors has any disclosures or conflicts of interest to report The Effect OF PATOS (Present At the Time Of Surgery) On The Calculation of SSI Rates for Appendectomy and Colectomy: Is PATOS
MBSAQIP Complex Clinical Scenarios & Variable Review
 MBSAQIP Complex Clinical Scenarios & Variable Review Disclosure The following planners, speakers, moderators, and/or panelists of the CME/CEU activity have no relevant financial relationships with commercial
MBSAQIP Complex Clinical Scenarios & Variable Review Disclosure The following planners, speakers, moderators, and/or panelists of the CME/CEU activity have no relevant financial relationships with commercial
Demographics. MBSAQIP Case Number: *ACS NSQIP Case Number: *LMRN: *DOB: / / *Gender: Male Female
 Demographics MBSAQIP Case Number: *IDN: *ACS NSQIP Case Number: Name: *LMRN: *DOB: / / *Gender: Male Female *Race: White Black or African American American Indian or Alaska Native Native Hawaiian/Other
Demographics MBSAQIP Case Number: *IDN: *ACS NSQIP Case Number: Name: *LMRN: *DOB: / / *Gender: Male Female *Race: White Black or African American American Indian or Alaska Native Native Hawaiian/Other
Form 1: Demographics
 Form 1: Demographics Case Number: *LMRN: *DOB: / / *Gender: Male Female *Race: White Native Hawaiian/Other Pacific Islander Black or African American Asian American Indian or Alaska Native Unknown *Hispanic
Form 1: Demographics Case Number: *LMRN: *DOB: / / *Gender: Male Female *Race: White Native Hawaiian/Other Pacific Islander Black or African American Asian American Indian or Alaska Native Unknown *Hispanic
Canadian Nosocomial Infection Surveillance Program 2017 SURVEILLANCE OF SURGICAL SITES INFECTIONS FOLLOWING PEDIATRIC CARDIAC SURGERY
 Canadian Nosocomial Infection Surveillance Program 2017 SURVEILLANCE OF SURGICAL SITES INFECTIONS FOLLOWING PEDIATRIC CARDIAC SURGERY December 29, 2016 FINAL Working Group: Bonita Lee (Chair), Joanne Langley,
Canadian Nosocomial Infection Surveillance Program 2017 SURVEILLANCE OF SURGICAL SITES INFECTIONS FOLLOWING PEDIATRIC CARDIAC SURGERY December 29, 2016 FINAL Working Group: Bonita Lee (Chair), Joanne Langley,
AMERICAN COLLEGE OF SURGEONS NATIONAL SURGICAL QUALITY IMPROVEMENT PROGRAM - PEDIATRIC Data Collection Worksheet
 AMERICAN COLLEGE OF SURGEONS NATIONAL SURGICAL QUALITY IMPROVEMENT PROGRAM - PEDIATRIC Data Collection Worksheet *IDN LMRN Cycle Number Case Number DEMOGRAPHICS PATIENT First Name: MI: Last Name: Street
AMERICAN COLLEGE OF SURGEONS NATIONAL SURGICAL QUALITY IMPROVEMENT PROGRAM - PEDIATRIC Data Collection Worksheet *IDN LMRN Cycle Number Case Number DEMOGRAPHICS PATIENT First Name: MI: Last Name: Street
Validation of HAI Reporting in New Hampshire Hospitals: Data from
 Validation of HAI Reporting in New Hampshire Hospitals: Data from 2014-15 Nancy Reinhalter, RN CCRC JSI Research & Training Institute, Inc. February 22, 2017 ACKNOWLEDGEMENTS JSI Team Priscilla Davis Paddy
Validation of HAI Reporting in New Hampshire Hospitals: Data from 2014-15 Nancy Reinhalter, RN CCRC JSI Research & Training Institute, Inc. February 22, 2017 ACKNOWLEDGEMENTS JSI Team Priscilla Davis Paddy
World Journal of Colorectal Surgery
 World Journal of Colorectal Surgery Volume 3, Issue 1 2013 Article 9 ISSUE 1 Perforation Of The Caecum Owing To Benign Rectal Obstruction: A Paradigm Of Damage Control In Emergency Colorectal Surgery DIMITRIOS
World Journal of Colorectal Surgery Volume 3, Issue 1 2013 Article 9 ISSUE 1 Perforation Of The Caecum Owing To Benign Rectal Obstruction: A Paradigm Of Damage Control In Emergency Colorectal Surgery DIMITRIOS
Pediatric Surgery MUHC MCH Siste. Objectives of Training
 Preamble A rotation in Pediatric Surgery must give residents the opportunity to become familiar with the unique needs of infants and children as surgical patients. Some of the surgical diseases encountered
Preamble A rotation in Pediatric Surgery must give residents the opportunity to become familiar with the unique needs of infants and children as surgical patients. Some of the surgical diseases encountered
Annex 4. Case definitions of infections
 Protocol for validation of PPS of HAIs and antimicrobial use in European LTCF TECHNICAL DOCUMENT Annex 4. Case definitions of infections Healthcare-associated infections and antimicrobial use in European
Protocol for validation of PPS of HAIs and antimicrobial use in European LTCF TECHNICAL DOCUMENT Annex 4. Case definitions of infections Healthcare-associated infections and antimicrobial use in European
Division of Vascular and Endovascular Surgery University of South Florida School of Medicine Tampa, Florida
 Division of Vascular and Endovascular Surgery University of South Florida School of Medicine Tampa, Florida Appearance: oearly < 3 mo. olate > 3 mo.. Extent: Szilagyi Classification: Grade I: infection
Division of Vascular and Endovascular Surgery University of South Florida School of Medicine Tampa, Florida Appearance: oearly < 3 mo. olate > 3 mo.. Extent: Szilagyi Classification: Grade I: infection
The Michigan Trauma Quality Improvement Program. Ann Arbor, MI June 7, 2011
 The Michigan Trauma Quality Improvement Program Ann Arbor, MI June 7, 2011 Information Current centers 14 New centers (July 1) Botsford Covenant Spectrum St. Johns Future centers (January 1) 23 Total Information
The Michigan Trauma Quality Improvement Program Ann Arbor, MI June 7, 2011 Information Current centers 14 New centers (July 1) Botsford Covenant Spectrum St. Johns Future centers (January 1) 23 Total Information
PENETRATING COLON TRAUMA: THE CURRENT EVIDENCE
 PENETRATING COLON TRAUMA: THE CURRENT EVIDENCE Samuel Hawkins MD CASE PRESENTATION 22M BIBEMS s/p multiple GSW ABCs intact Normotensive, non-tachycardic Secondary Survey: 4 truncal bullet holes L superior
PENETRATING COLON TRAUMA: THE CURRENT EVIDENCE Samuel Hawkins MD CASE PRESENTATION 22M BIBEMS s/p multiple GSW ABCs intact Normotensive, non-tachycardic Secondary Survey: 4 truncal bullet holes L superior
American College of Surgeons National Surgical Quality Improvement Program
 American College of Surgeons National Surgical Quality Improvement Program Program Overview ACS NSQIP is a data-driven, risk-adjusted, outcomes-based program to measure and improve the quality of surgical
American College of Surgeons National Surgical Quality Improvement Program Program Overview ACS NSQIP is a data-driven, risk-adjusted, outcomes-based program to measure and improve the quality of surgical
2015 General Surgery Survival Guide
 2015 General Surgery Survival Guide Chapter 10: Hernia Repair Know What to Look for When Coding Hernia Repair Reporting hernia repair can be tricky. But if you know what to look for then half the work
2015 General Surgery Survival Guide Chapter 10: Hernia Repair Know What to Look for When Coding Hernia Repair Reporting hernia repair can be tricky. But if you know what to look for then half the work
Does Using a Laparoscopic Approach to Cholecystectomy Decrease the Risk of Surgical Site Infection?
 ANNALS OF SURGERY Vol. 237, No. 3, 358 362 2003 Lippincott Williams & Wilkins, Inc. Does Using a Laparoscopic Approach to Cholecystectomy Decrease the Risk of Surgical Site Infection? Chesley Richards,
ANNALS OF SURGERY Vol. 237, No. 3, 358 362 2003 Lippincott Williams & Wilkins, Inc. Does Using a Laparoscopic Approach to Cholecystectomy Decrease the Risk of Surgical Site Infection? Chesley Richards,
Table 0: Description of Grading System for Anatomic Severity of Disease in Emergency. Local disease confined to the organ with minimal abnormality
 Table 0: of Grading System for Anatomic Severity of Disease in Emergency Local disease confined to the organ with minimal Local disease confined to the organ with severe Local extension Table 1: Universal
Table 0: of Grading System for Anatomic Severity of Disease in Emergency Local disease confined to the organ with minimal Local disease confined to the organ with severe Local extension Table 1: Universal
Small Bowel and Colon Surgery
 Small Bowel and Colon Surgery Why Do I Need a Small Bowel Resection? A variety of conditions can damage your small bowel. In severe cases, your doctor may recommend removing part of your small bowel. Conditions
Small Bowel and Colon Surgery Why Do I Need a Small Bowel Resection? A variety of conditions can damage your small bowel. In severe cases, your doctor may recommend removing part of your small bowel. Conditions
of Trauma Assembly 28 th Page 1
 Eastern Association for the Surgery of Trauma 28 th Annual Scientific Assembly Sunrise Session 12 Disease Grading Systemss in Emergency General Surgery January 16, 2015 Disney s Contemporary Resort Lake
Eastern Association for the Surgery of Trauma 28 th Annual Scientific Assembly Sunrise Session 12 Disease Grading Systemss in Emergency General Surgery January 16, 2015 Disney s Contemporary Resort Lake
Enhanced Recovery After Colorectal Surgery at Royal Inland Hospital Kamloops, BC. Our Data Experience
 Enhanced Recovery After Colorectal Surgery at Royal Inland Hospital Kamloops, BC Our Data Experience No Disclosures 1/26/2015 2 Purpose To tell our story of how we collect and share our ERACS data 1/26/2015
Enhanced Recovery After Colorectal Surgery at Royal Inland Hospital Kamloops, BC Our Data Experience No Disclosures 1/26/2015 2 Purpose To tell our story of how we collect and share our ERACS data 1/26/2015
Final FRCA Written PAEDIATRICS Past Paper Questions November March 2014
 Final FRCA Written PAEDIATRICS Past Paper Questions November 1996- March 2014 March 2014 A 5-year-old patient presents for a myringotomy and grommet insertion as a day case. During your pre-operative assessment
Final FRCA Written PAEDIATRICS Past Paper Questions November 1996- March 2014 March 2014 A 5-year-old patient presents for a myringotomy and grommet insertion as a day case. During your pre-operative assessment
Abscess. A abscess is a localized collection of pus in the skin and may occur on any skin surface and be formed in any part of body.
 Abscess A abscess is a localized collection of pus in the skin and may occur on any skin surface and be formed in any part of body. Ethyology Bacteria causing cutaneous abscesses are typically indigenous
Abscess A abscess is a localized collection of pus in the skin and may occur on any skin surface and be formed in any part of body. Ethyology Bacteria causing cutaneous abscesses are typically indigenous
Sepsis Awareness and Education
 Sepsis Awareness and Education Meets the updated New York State Department of Health (NYSDOH) requirements for Infection Control and Barrier Precautions coursework Element VII: Sepsis Awareness and Education
Sepsis Awareness and Education Meets the updated New York State Department of Health (NYSDOH) requirements for Infection Control and Barrier Precautions coursework Element VII: Sepsis Awareness and Education
Case Scenario 3: Shock and Sepsis
 Name: Molly Boyle 1. Define the term shock (Lewis textbook): Shock is a syndrome characterized by decreased perfusion and impaired metabolism. Shock can have a number of causes that result in damage to
Name: Molly Boyle 1. Define the term shock (Lewis textbook): Shock is a syndrome characterized by decreased perfusion and impaired metabolism. Shock can have a number of causes that result in damage to
Index. Note: Page numbers of article title are in boldface type.
 Index Note: Page numbers of article title are in boldface type. A Abscess(es) in Crohn s disease, 168 169 IPAA and, 110 114 as unexpected finding in colorectal surgery, 46 Adhesion(s) trocars-related laparoscopy
Index Note: Page numbers of article title are in boldface type. A Abscess(es) in Crohn s disease, 168 169 IPAA and, 110 114 as unexpected finding in colorectal surgery, 46 Adhesion(s) trocars-related laparoscopy
Long Term Follow-up. 6 Month 1 Year Annual enter year #: What is the assessment date: / / Unknown. Is the patient alive? Yes No
 Long Term Follow-up 6 Month 1 Year Annual enter year #: What is the assessment date: / / Unknown Is the patient alive? Yes No Was an exam performed by a bariatric physician or PA/NP? Yes No Was the patient
Long Term Follow-up 6 Month 1 Year Annual enter year #: What is the assessment date: / / Unknown Is the patient alive? Yes No Was an exam performed by a bariatric physician or PA/NP? Yes No Was the patient
National Healthcare Safety Network: Central Line-associated Bloodstream Case Studies Teresa C. Horan, MPH
 National Healthcare Safety Network: Central Line-associated Bloodstream Case Studies Teresa C. Horan, MPH National Center for Emerging and Zoonotic Infectious Diseases Division of Healthcare Quality Promotion
National Healthcare Safety Network: Central Line-associated Bloodstream Case Studies Teresa C. Horan, MPH National Center for Emerging and Zoonotic Infectious Diseases Division of Healthcare Quality Promotion
LAPAROSCOPIC APPENDICECTOMY
 LAPAROSCOPIC APPENDICECTOMY WHAT IS THE APPENDIX? The appendix is a small, fingerlike pouch of the intestinal tract located where the small and large join. It has no known use. It is postulated that the
LAPAROSCOPIC APPENDICECTOMY WHAT IS THE APPENDIX? The appendix is a small, fingerlike pouch of the intestinal tract located where the small and large join. It has no known use. It is postulated that the
Scottish Surveillance of Healthcare Associated Infection Programme (SSHAIP) Health Protection Scotland (HPS) SSI Surveillance Protocol 7th Edition
 Health Protection Scotland (HPS) SSI Surveillance Protocol 7th Edition") 1 Contents Female reproductive system operations (Abdominal hysterectomy and Caesarean section)... 3 Intra-abdominal infections... 3 Endometritis... 4 Other infections of the female reproductive tract...
1 Contents Female reproductive system operations (Abdominal hysterectomy and Caesarean section)... 3 Intra-abdominal infections... 3 Endometritis... 4 Other infections of the female reproductive tract...
SCIP and NSQIP the Alphabet Soup of Surgical Quality
 SCIP and NSQIP the Alphabet Soup of Surgical Quality NSQIP National Conference Christopher C Johnson M.D. Caryn Foster RN, SCR Nicholas Hellenthal M.D., F.A.C.S. 7/26/15 Disclosure None Introduction The
SCIP and NSQIP the Alphabet Soup of Surgical Quality NSQIP National Conference Christopher C Johnson M.D. Caryn Foster RN, SCR Nicholas Hellenthal M.D., F.A.C.S. 7/26/15 Disclosure None Introduction The
Demographics IDN: DOB: / / Gender: Male Female. Race: White Black or African American American Indian or Alaska Native
 MBSAQIP Case Number: Name: Demographics IDN: LMRN: DOB: / / Gender: Male Female Race: White Black or African American American Indian or Alaska Native Native Hawaiian/Other Pacific Islander Asian Unknown
MBSAQIP Case Number: Name: Demographics IDN: LMRN: DOB: / / Gender: Male Female Race: White Black or African American American Indian or Alaska Native Native Hawaiian/Other Pacific Islander Asian Unknown
Staging Sepsis for the Emergency Department: Physician
 Staging Sepsis for the Emergency Department: Physician Sepsis Continuum 1 Sepsis Continuum SIRS = 2 or more clinical criteria, resulting in Systemic Inflammatory Response Syndrome Sepsis = SIRS + proven/suspected
Staging Sepsis for the Emergency Department: Physician Sepsis Continuum 1 Sepsis Continuum SIRS = 2 or more clinical criteria, resulting in Systemic Inflammatory Response Syndrome Sepsis = SIRS + proven/suspected
Back to Basics: What Imaging Test should I order? Jeanne G. Hill, M.D. Pediatric Radiology Medical University of South Carolina
 Back to Basics: What Imaging Test should I order? Jeanne G. Hill, M.D. Pediatric Radiology Medical University of South Carolina Disclosure Neither I nor any member of my immediate family has a relevant
Back to Basics: What Imaging Test should I order? Jeanne G. Hill, M.D. Pediatric Radiology Medical University of South Carolina Disclosure Neither I nor any member of my immediate family has a relevant
Rochester Patient Safety C. difficile Prevention Collaborative: Long Term Care Antimicrobial Stewardship (funded by NYSDOH)
") Rochester Patient Safety C. difficile Prevention Collaborative: Long Term Care Antimicrobial Stewardship (funded by NYSDOH) Clinical Practice Guideline* for the Diagnosis and Management of Acute Bacterial
Rochester Patient Safety C. difficile Prevention Collaborative: Long Term Care Antimicrobial Stewardship (funded by NYSDOH) Clinical Practice Guideline* for the Diagnosis and Management of Acute Bacterial
SURGICAL SITE INFECTIONS: SURVEILLANCE & PREVENTION
 SURGICAL SITE INFECTIONS: SURVEILLANCE & PREVENTION Disclosures: I have No conflicts of interest No commercial support No specific product will be endorsed during this presentation Facts There were an
SURGICAL SITE INFECTIONS: SURVEILLANCE & PREVENTION Disclosures: I have No conflicts of interest No commercial support No specific product will be endorsed during this presentation Facts There were an
Case Presentation and Discussion on Posterior Neck Mass. Martin Joseph S. Cabahug
 Case Presentation and Discussion on Posterior Neck Mass Martin Joseph S. Cabahug General Data: C.A, 60 y/o male Sta. Ana, Mla Chief Complaint: Posterior Neck Mass History and Physical Exam 2 wks PTA mass,
Case Presentation and Discussion on Posterior Neck Mass Martin Joseph S. Cabahug General Data: C.A, 60 y/o male Sta. Ana, Mla Chief Complaint: Posterior Neck Mass History and Physical Exam 2 wks PTA mass,
General Surgery Service
 General Surgery Service Patient Care Goals and Objectives Stomach/Duodenum and Bariatric assessed for a) Obesity surgery b) Treatment of i) Adenocarcinoma of the stomach ii) GIST iii) Carcinoid 2) Optimize
General Surgery Service Patient Care Goals and Objectives Stomach/Duodenum and Bariatric assessed for a) Obesity surgery b) Treatment of i) Adenocarcinoma of the stomach ii) GIST iii) Carcinoid 2) Optimize
Bone and Joint Infections in Diabetics: Diagnosis and Management of Diabetic Foot and Other Common Lower Extremity Infections
 Bone and Joint Infections in Diabetics: Diagnosis and Management of Diabetic Foot and Other Common Lower Extremity Infections Objectives How do you to diagnose, classify and manage DFI? How do you diagnose
Bone and Joint Infections in Diabetics: Diagnosis and Management of Diabetic Foot and Other Common Lower Extremity Infections Objectives How do you to diagnose, classify and manage DFI? How do you diagnose
Data Collection Help Sheet
 Global Outcomes in Surgery Collaboration GlobalSurg II: Determining the worldwide epidemiology of surgical site infections after gastrointestinal surgery Data Collection Help Sheet Introduction This document
Global Outcomes in Surgery Collaboration GlobalSurg II: Determining the worldwide epidemiology of surgical site infections after gastrointestinal surgery Data Collection Help Sheet Introduction This document
Medical Management of Appendicitis: Are We There Yet? Monica E. Lopez, MD, FACS, FAAP
 Medical Management of Appendicitis: Are We There Yet? Monica E. Lopez, MD, FACS, FAAP Texas Children s Hospital Objectives Discuss the surgical and non-operative approaches to the treatment of appendicitis
Medical Management of Appendicitis: Are We There Yet? Monica E. Lopez, MD, FACS, FAAP Texas Children s Hospital Objectives Discuss the surgical and non-operative approaches to the treatment of appendicitis
Difficult Abdominal Closure. Mark A. Carlson, MD
 Difficult Abdominal Closure Mark A. Carlson, MD Illustrative case 14 yo boy with delayed diagnosis of appendicitis POD9 Appendectomy 2 wk after onset of symptoms POD4: return to OR for midline laparotomy
Difficult Abdominal Closure Mark A. Carlson, MD Illustrative case 14 yo boy with delayed diagnosis of appendicitis POD9 Appendectomy 2 wk after onset of symptoms POD4: return to OR for midline laparotomy
QUESTIONS IN SURGERY General Surgery (3rd year) Surgery nr.1 (4th year)
 Surgery nr.1 (4th year)") QUESTIONS IN SURGERY General Surgery (3 rd year) 1. Bleeding: definition, classification. Physiological mechanisms of compensation and pathological mechanisms of decompensation in case of hemorrhage. Physiologic
QUESTIONS IN SURGERY General Surgery (3 rd year) 1. Bleeding: definition, classification. Physiological mechanisms of compensation and pathological mechanisms of decompensation in case of hemorrhage. Physiologic
TENNCARE Bundled Payment Initiative: Description of Bundle Risk Adjustment for Wave 8 Episodes
 TENNCARE Bundled Payment Initiative: Description of Bundle Risk Adjustment for Wave 8 Episodes Acute Seizure, Syncope, Acute Gastroenteritis, Pediatric Pneumonia, Bronchiolitis, Colposcopy, Hysterectomy,
TENNCARE Bundled Payment Initiative: Description of Bundle Risk Adjustment for Wave 8 Episodes Acute Seizure, Syncope, Acute Gastroenteritis, Pediatric Pneumonia, Bronchiolitis, Colposcopy, Hysterectomy,
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Abdominal injuries clinical presentation of, 23 24 Abdominal trauma evaluation for pediatric surgeon, 59 74 background of, 60 colon and
Index Note: Page numbers of article titles are in boldface type. A Abdominal injuries clinical presentation of, 23 24 Abdominal trauma evaluation for pediatric surgeon, 59 74 background of, 60 colon and
Appendicitis. Diagnosis and Surgery
 Appendicitis Diagnosis and Surgery What Is Appendicitis? Your side may hurt so much that you called your doctor. Or maybe you went straight to the hospital emergency room. If the symptoms came on quickly,
Appendicitis Diagnosis and Surgery What Is Appendicitis? Your side may hurt so much that you called your doctor. Or maybe you went straight to the hospital emergency room. If the symptoms came on quickly,
InterQual Level of Care 2018 Index
 InterQual Level of Care 2018 Index Long-Term Acute Care (LTAC) Criteria The Index is an alphabetical listing of conditions and/or diagnoses designed to guide the user to the criteria subset where a specific
InterQual Level of Care 2018 Index Long-Term Acute Care (LTAC) Criteria The Index is an alphabetical listing of conditions and/or diagnoses designed to guide the user to the criteria subset where a specific
FHS Appendicitis US Protocol
 FHS Appendicitis US Protocol Reviewed By: Shireen Khan, MD; Sarah Farley, MD; Anna Ellermeier, MD Last Reviewed: May 2018 Contact: (866) 761-4200 **NOTE for all examinations: 1. If documenting possible
FHS Appendicitis US Protocol Reviewed By: Shireen Khan, MD; Sarah Farley, MD; Anna Ellermeier, MD Last Reviewed: May 2018 Contact: (866) 761-4200 **NOTE for all examinations: 1. If documenting possible
SEPSIS. Sepsis Dianna Foley, RHIA, CHPS. Sepsis Stats 3/3/2015
 Sepsis Dianna Foley, RHIA, CHPS SEPSIS Sepsis Stats Sepsis 10 th leading cause of death in the U.S. Affecting 3 in every 1,000 people Accounting for 1-2 % of hospitalizations Severe Sepsis Approximately
Sepsis Dianna Foley, RHIA, CHPS SEPSIS Sepsis Stats Sepsis 10 th leading cause of death in the U.S. Affecting 3 in every 1,000 people Accounting for 1-2 % of hospitalizations Severe Sepsis Approximately
Physical Exam. Vitals stable on room air Abdomen soft, non-distented Normal external genitalia Patent anus No limb anomalies
 Case Presentation 1 day-old full-term baby girl noted to have drooling of saliva and increased secretions at birth Fetal US @32wks had shown polyhydramnios Birth weight 3515g Apgar 7@1min and 8@5min Unable
Case Presentation 1 day-old full-term baby girl noted to have drooling of saliva and increased secretions at birth Fetal US @32wks had shown polyhydramnios Birth weight 3515g Apgar 7@1min and 8@5min Unable
Clinical Payment and Coding Policy Committee Approval Date: 02/23/2018
 In the event of a conflict between a Clinical Payment and Coding Policy and any plan document under which a member is entitled to Covered Services, the plan document will govern. Plan documents include,
In the event of a conflict between a Clinical Payment and Coding Policy and any plan document under which a member is entitled to Covered Services, the plan document will govern. Plan documents include,
Building Confidence in NHSN. Peg Gilbert, RN, MS, CIC, FAPIC Quality Improvement Advisor, Regional Task Lead Great Plains Quality Innovation Network
 Building Confidence in NHSN Peg Gilbert, RN, MS, CIC, FAPIC Quality Improvement Advisor, Regional Task Lead Great Plains Quality Innovation Network Objectives Identify resources to improve reporting Examine
Building Confidence in NHSN Peg Gilbert, RN, MS, CIC, FAPIC Quality Improvement Advisor, Regional Task Lead Great Plains Quality Innovation Network Objectives Identify resources to improve reporting Examine
POSTOPERATIVE CONGENITAL ESOPHAGEAL ATRESIA COMPLICATIONS: A REVIEW
 CHILDREN S HOSPITAL II POSTOPERATIVE CONGENITAL ESOPHAGEAL ATRESIA COMPLICATIONS: A REVIEW Dr. Nguyen Thuy Hanh Ngan Neonatal Department CONTENTS 1. Background 2. Classification 3. Management 4. Complications
CHILDREN S HOSPITAL II POSTOPERATIVE CONGENITAL ESOPHAGEAL ATRESIA COMPLICATIONS: A REVIEW Dr. Nguyen Thuy Hanh Ngan Neonatal Department CONTENTS 1. Background 2. Classification 3. Management 4. Complications
Original Policy Date
 MP 7.01.90 Vertical Expandable Prosthetic Titanium Rib Medical Policy Section Surgery Issue 12/2013 Original Policy Date 12/2013 Last Review Status/Date Reviewed with literature search/12/20135:2012 Return
MP 7.01.90 Vertical Expandable Prosthetic Titanium Rib Medical Policy Section Surgery Issue 12/2013 Original Policy Date 12/2013 Last Review Status/Date Reviewed with literature search/12/20135:2012 Return
Case Report Postoperative Megarectum in an Adult Patient with Imperforate Anus and Rectourethral Fistula
 Case Reports in Gastrointestinal Medicine Volume 2015, Article ID 613926, 4 pages http://dx.doi.org/10.1155/2015/613926 Case Report Postoperative Megarectum in an Adult Patient with Imperforate Anus and
Case Reports in Gastrointestinal Medicine Volume 2015, Article ID 613926, 4 pages http://dx.doi.org/10.1155/2015/613926 Case Report Postoperative Megarectum in an Adult Patient with Imperforate Anus and
Colostomy & Ileostomy
 Colostomy & Ileostomy Indications, problems and preference By Waleed Omar Professor of Colorectal surgery, Mansoura University. Disclosure I have no disclosures. Presentation outline Stoma: Definition
Colostomy & Ileostomy Indications, problems and preference By Waleed Omar Professor of Colorectal surgery, Mansoura University. Disclosure I have no disclosures. Presentation outline Stoma: Definition
MORTALITY RISK FACTORS FOR NEONATAL INTESTINAL OBSTRUCTION
 Basrah Journal Of Surgery MORTALITY RISK FACTORS FOR NEONATAL INTESTINAL OBSTRUCTION Haithem Hussein Ali Almoamin MB, ChB, FIBMS Pediatric Surgery, Lecturer, Department of Surgery, College of Medicine,
Basrah Journal Of Surgery MORTALITY RISK FACTORS FOR NEONATAL INTESTINAL OBSTRUCTION Haithem Hussein Ali Almoamin MB, ChB, FIBMS Pediatric Surgery, Lecturer, Department of Surgery, College of Medicine,
SURGICAL SITE INFECTIONS SURVEILLANCE & PREVENTION
 SURGICAL SITE INFECTIONS SURVEILLANCE & PREVENTION Objectives List evidence based prevention strategies Define Surgical Site Infections based on NHSN definitions Describe surveillance tips Facts According
SURGICAL SITE INFECTIONS SURVEILLANCE & PREVENTION Objectives List evidence based prevention strategies Define Surgical Site Infections based on NHSN definitions Describe surveillance tips Facts According
Clinical Quality Measures for PQRS. Last Updated: June 4, 2014
 Clinical Quality Measures for PQRS Last Updated: June 4, 2014 The Michigan Bariatric Surgery Collaborative (MBSC) Quality Clinical Data Registry will submit the following measures outlined below on behalf
Clinical Quality Measures for PQRS Last Updated: June 4, 2014 The Michigan Bariatric Surgery Collaborative (MBSC) Quality Clinical Data Registry will submit the following measures outlined below on behalf
ASTS TRANSQIP Beta Phase Informational Webinar
 ASTS TRANSQIP Beta Phase Informational Webinar December 2, 2016 Ryutaro Hirose, MD Stuart Greenstein, MD TransQIP A collaborative effort between ASTS and the American College of Surgeons A National Transplant
ASTS TRANSQIP Beta Phase Informational Webinar December 2, 2016 Ryutaro Hirose, MD Stuart Greenstein, MD TransQIP A collaborative effort between ASTS and the American College of Surgeons A National Transplant
JAWDA Bariatric Quality Performance Indicators. JAWDA Quarterly Guidelines for Bariatric Surgery (BS)
") JAWDA Guidelines for Bariatric Surgery (BS) January 2019 1 Table of Contents Executive Summary... 3 About this Guidance... 4 Bariatric Surgery Indicators... 5 Appendix A: Glossary... 19 Appendix B: Approved
JAWDA Guidelines for Bariatric Surgery (BS) January 2019 1 Table of Contents Executive Summary... 3 About this Guidance... 4 Bariatric Surgery Indicators... 5 Appendix A: Glossary... 19 Appendix B: Approved
Table of Contents. Definitions document
 Definitions document Table of Contents Definitions of preoperative risk factors... 3 What is the definition of neurosurgery?... 3 What should I do if some important medical co-morbidities are not included
Definitions document Table of Contents Definitions of preoperative risk factors... 3 What is the definition of neurosurgery?... 3 What should I do if some important medical co-morbidities are not included
Severe and Tertiary Peritonitis
 Severe and Tertiary Peritonitis Addison K. May, MD FACS Professor of Surgery and Anesthesiology Division of Trauma and Surgical Critical Care Vanderbilt University Medical Center PS204: The Bad Infections:
Severe and Tertiary Peritonitis Addison K. May, MD FACS Professor of Surgery and Anesthesiology Division of Trauma and Surgical Critical Care Vanderbilt University Medical Center PS204: The Bad Infections:
Abdominal Compartment Syndrome. Jeff Johnson, MD
 Abdominal Compartment Syndrome Jeff Johnson, MD Acute Care Surgeon, Denver Health Associate Professor of Surgery, University of Colorado Denver The Abdomen A Forgotten Closed Compartment Early Animal Models
Abdominal Compartment Syndrome Jeff Johnson, MD Acute Care Surgeon, Denver Health Associate Professor of Surgery, University of Colorado Denver The Abdomen A Forgotten Closed Compartment Early Animal Models
5/1/2015 SEPSIS SURVIVING SEPSIS CAMPAIGN HOW TO APPROACH THE POSSIBLE SEPTIC CHILD 2015 INFECTION CAN BE CONFIRMED BY:
 SURVIVING SEPSIS CAMPAIGN HOW TO APPROACH THE POSSIBLE SEPTIC CHILD 2015 Omer Nasiroglu MD Baptist Children s Hospital Pediatric Emergency Department SEPSIS IS A SYSTEMIC INFLAMMATORY RESPONSE SYNDROME
SURVIVING SEPSIS CAMPAIGN HOW TO APPROACH THE POSSIBLE SEPTIC CHILD 2015 Omer Nasiroglu MD Baptist Children s Hospital Pediatric Emergency Department SEPSIS IS A SYSTEMIC INFLAMMATORY RESPONSE SYNDROME
2011 CPT Code Update. Diagnostic Radiology. Computed Tomography (CT), Abdomen and Pelvis. Deletion of Xeroradiography and Subtraction Codes
, Abdomen and Pelvis. Deletion of Xeroradiography and Subtraction Codes") 2011 CPT Code Update [The Health Insurance Portability and Accountability Act [HIPAA] transaction and code set rules require the use of the medical code set that is valid at the time a service is provided.
2011 CPT Code Update [The Health Insurance Portability and Accountability Act [HIPAA] transaction and code set rules require the use of the medical code set that is valid at the time a service is provided.
SHOCK. Emergency pediatric PICU division Pediatric Department Medical Faculty, University of Sumatera Utara H. Adam Malik Hospital
 SHOCK Emergency pediatric PICU division Pediatric Department Medical Faculty, University of Sumatera Utara H. Adam Malik Hospital 1 Definition Shock is an acute, complex state of circulatory dysfunction
SHOCK Emergency pediatric PICU division Pediatric Department Medical Faculty, University of Sumatera Utara H. Adam Malik Hospital 1 Definition Shock is an acute, complex state of circulatory dysfunction
How to Address an Inappropriately high Mortality Rate? Joe Sharma, MD Associate Professor of Surgery NSQIP Surgical Champion
 How to Address an Inappropriately high Mortality Rate? Joe Sharma, MD Associate Professor of Surgery NSQIP Surgical Champion Disclosure Slide No COI and no disclosures. Hospital Mortality rate : is it
How to Address an Inappropriately high Mortality Rate? Joe Sharma, MD Associate Professor of Surgery NSQIP Surgical Champion Disclosure Slide No COI and no disclosures. Hospital Mortality rate : is it
Division of Vascular and Endovascular Surgery University of South Florida School of Medicine Tampa, Florida
 Division of Vascular and Endovascular Surgery University of South Florida School of Medicine Tampa, Florida Appearance: oearly < 3 mo. olate > 3 mo.. Extent: Szilagyi Classification: Grade I: infection
Division of Vascular and Endovascular Surgery University of South Florida School of Medicine Tampa, Florida Appearance: oearly < 3 mo. olate > 3 mo.. Extent: Szilagyi Classification: Grade I: infection
Tracheoesophageal Fistula and Esophageal Atresia
 Patient and Family Education Tracheoesophageal Fistula and Esophageal Atresia What is tracheoesophageal fistula? The word fistula means abnormal connection. Tracheoesophageal fistula (TEF) is a condition
Patient and Family Education Tracheoesophageal Fistula and Esophageal Atresia What is tracheoesophageal fistula? The word fistula means abnormal connection. Tracheoesophageal fistula (TEF) is a condition
OTOLARYNGOLOGY ONLINE. Preauricular sinus. Management. Dr. T. Balasubramanian 6/17/2010
 1 OTOLARYNGOLOGY ONLINE Preauricular sinus Management Dr. T. Balasubramanian 6/17/2010 This e book discusses the Etiopathogenesis of preauricular sinus. Even though it is commonly encountered surgical
1 OTOLARYNGOLOGY ONLINE Preauricular sinus Management Dr. T. Balasubramanian 6/17/2010 This e book discusses the Etiopathogenesis of preauricular sinus. Even though it is commonly encountered surgical
Peritonitis SUPPURATIVE DISEASES OF SEROUS CAVITY
 Peritonitis SUPPURATIVE DISEASES OF SEROUS CAVITY peritonitis A special feature of peritonitis is the spread of infection and the intensive absorption by the peritoneum of toxic products - bacterial toxins,
Peritonitis SUPPURATIVE DISEASES OF SEROUS CAVITY peritonitis A special feature of peritonitis is the spread of infection and the intensive absorption by the peritoneum of toxic products - bacterial toxins,
Demographics (3-50): Age: years Sex (M/F): Weight: kg Height: m
: Age: years Sex (M/F): Weight: kg Height: m") EAST MULTICENTER STUDY DATA COLLECTION TOOL Multicenter Study: Colorectal resection in Emergency General Surgery To anastomose, or not to anastomose? Enrolling Center: Patient Number: The following sheets
EAST MULTICENTER STUDY DATA COLLECTION TOOL Multicenter Study: Colorectal resection in Emergency General Surgery To anastomose, or not to anastomose? Enrolling Center: Patient Number: The following sheets
Pediatric Learning Solutions A clinical education program exclusively for pediatric professionals
 Pediatric Learning Solutions A clinical education program exclusively for pediatric professionals The following Pediatric Learning Solutions courses align to focus areas of the Neonatal CCRN Exam Content
Pediatric Learning Solutions A clinical education program exclusively for pediatric professionals The following Pediatric Learning Solutions courses align to focus areas of the Neonatal CCRN Exam Content
Composite of pneumonia, re-intubation, or death within 30 days of randomisation.
 Appendix: definitions Clinical outcome measures Primary outcome measure Composite of pneumonia, re-intubation, or death within 30 days of randomisation. Pneumonia Care will be taken to distinguish between
Appendix: definitions Clinical outcome measures Primary outcome measure Composite of pneumonia, re-intubation, or death within 30 days of randomisation. Pneumonia Care will be taken to distinguish between
Anorectal Malformations
 CHAPTER Anorectal Malformations P. Stephen Almond Incidence The incidence of imperforate anus is one in every 5,000 live births, with cloaca malformations accounting for 10%. Males (58%) are more commonly
CHAPTER Anorectal Malformations P. Stephen Almond Incidence The incidence of imperforate anus is one in every 5,000 live births, with cloaca malformations accounting for 10%. Males (58%) are more commonly
APIC NHSN Webinar 9/8/2015. Topic Overview. Overall Learning Objectives
 APIC NHSN Webinar Janet Brooks, Cindy Gross, Denise Leaptrot, & Eileen Scalise Subject Matter Experts September 9, 2015 National Center for Emerging and Zoonotic Infectious Diseases Place Descriptor Here
APIC NHSN Webinar Janet Brooks, Cindy Gross, Denise Leaptrot, & Eileen Scalise Subject Matter Experts September 9, 2015 National Center for Emerging and Zoonotic Infectious Diseases Place Descriptor Here
R2R: Severe sepsis/septic shock. Surat Tongyoo Critical care medicine Siriraj Hospital
 R2R: Severe sepsis/septic shock Surat Tongyoo Critical care medicine Siriraj Hospital Diagnostic criteria ACCP/SCCM consensus conference 1991 SCCM/ESICM/ACCP/ATS/SIS International Sepsis Definitions Conference
R2R: Severe sepsis/septic shock Surat Tongyoo Critical care medicine Siriraj Hospital Diagnostic criteria ACCP/SCCM consensus conference 1991 SCCM/ESICM/ACCP/ATS/SIS International Sepsis Definitions Conference
Prevention and Management of Hysterectomy-Related Infectious Morbidity DR. S. FOULEM BSC, MD, FRSCS
 Prevention and Management of Hysterectomy-Related Infectious Morbidity DR. S. FOULEM BSC, MD, FRSCS Objectives Definition and epidemiology of surgical site infections (SSI) What are the most common infectious
Prevention and Management of Hysterectomy-Related Infectious Morbidity DR. S. FOULEM BSC, MD, FRSCS Objectives Definition and epidemiology of surgical site infections (SSI) What are the most common infectious
Catheter-Associated Urinary Tract Infection (CAUTI) Event
 Event") Catheter-Associated Urinary Tract Infection () Event Introduction: The urinary tract is the most common site of healthcare-associated infection, accounting for more than 30% of infections reported by acute
Catheter-Associated Urinary Tract Infection () Event Introduction: The urinary tract is the most common site of healthcare-associated infection, accounting for more than 30% of infections reported by acute
Annual High Claims Survey. Year Ending 31 December 2016
 Annual High Claims Survey Year Ending 31 December 2016 Released July 2017 Summary The Private Healthcare Australia Annual High Claims Survey Report analyses the nature and magnitude of high claims met
Annual High Claims Survey Year Ending 31 December 2016 Released July 2017 Summary The Private Healthcare Australia Annual High Claims Survey Report analyses the nature and magnitude of high claims met
Surgical Complication, or Not, That Is the Question
 Surgical Complication, or Not, That Is the Question Adriane Martin, DO, FACOS, CCDS Vice President Enjoin This is the Full Title of a Session Eads, TN 1 Learning Objectives At the completion of this educational
Surgical Complication, or Not, That Is the Question Adriane Martin, DO, FACOS, CCDS Vice President Enjoin This is the Full Title of a Session Eads, TN 1 Learning Objectives At the completion of this educational
General'Surgery'Service'
 General'Surgery'Service' Patient Care Goals and Objectives 1)! Stomach/Duodenum and Bariatric 2)! Interpret the results of clinical evaluations (history, physical examination) performed on patients being
General'Surgery'Service' Patient Care Goals and Objectives 1)! Stomach/Duodenum and Bariatric 2)! Interpret the results of clinical evaluations (history, physical examination) performed on patients being
Present-on-Admission (POA) Coding
 Coding") 1 Present-on-Admission (POA) Coding Michael Pine, MD, MBA Michael Pine and Associates, Inc 2 POA and Coding Guidelines (1) Unless otherwise specified, a POA modifier must be assigned to each principal
1 Present-on-Admission (POA) Coding Michael Pine, MD, MBA Michael Pine and Associates, Inc 2 POA and Coding Guidelines (1) Unless otherwise specified, a POA modifier must be assigned to each principal
Post-Cardiac Surgery Evaluation
 Post-Cardiac Surgery Evaluation 20th Annual Heart Conference October 15, 2016 Gary A Mayman PROFESSOR PEDIATRICS UNIVERSITY OF NEVADA Look Touch Listen Temperature, pulse, respiratory rate, & blood pressure
Post-Cardiac Surgery Evaluation 20th Annual Heart Conference October 15, 2016 Gary A Mayman PROFESSOR PEDIATRICS UNIVERSITY OF NEVADA Look Touch Listen Temperature, pulse, respiratory rate, & blood pressure