Management of Cancer Pain
|
|
|
- Stanley Gibson
- 5 years ago
- Views:
Transcription




1 Management of Cancer Pain Mihir M. Kamdar, MD Associate Director, Palliative Care Director, MGH Cancer Pain Clinic Depts of Anesthesia Pain/Palliative Care Massachusetts General Hospital
2 None Disclosures
3 Overview of Today s talk The Importance of the Cancer Pain Diagnosis Use Co-analgesics and Adjuvant Medications Use Opioids for Moderate to Severe pain Proper opioid selection Use of short-acting and long-acting opioids Titration, side effect management, & opioid conversion Quick Commentary: Interventional Procedures for Refractory Cancer Pain Palliative Care & Multidisciplinary Approach to Cancer Pain
4 Background and Context of Cancer Pain

5 Why is this important? Pain is a more terrible lord of mankind than even death himself - Albert Schweitzer, 1931 Cancer Pain State of the Union: 30-40% of pts with Early Disease 70-90% of pts Advanced Disease
6 How We Define Pain: An unpleasant sensory and emotional experience associated with actual or potential tissue damage Merskey, H., Bogduk, N, ed. Classification of Chronic Pain, Second Edition. IASP Task Force on Taxonomy. 1994, IASP Press: Seattle
7 How Cancer Patient s Define Pain: It s a reminder that the cancer is always there. It s a reminder that I m dying. It erodes my ability to interact with family. That s hard when I have limited time, and important things to talk about. It makes me afraid that I m going to die in agony

8 Cancer Pain Doesn t Just Impact the Individual Major Impact on Family/Caregivers Significant Healthcare Utilization: Urgent Clinic Visits ED Visits Inpatient Admissions/Readmissions for Cancer Pain Effectively Managing Cancer Pain Is Vastly Important 2
 Surgery (Post-Thoractomy/Mastectomy Pain)")
9 From Where Does Cancer Pain Arise? ~75% from Direct Tumor Effects ~25% from Cancer Therapies 1 Chemotherapy (Chemotherapy-Induced Neuropathy) Surgery (Post-Thoractomy/Mastectomy Pain) Radiation (Mucositis/Proctitis) Non-Malignant Pain 1. Bonica, J The Management of Pain. Vol. 1. Lea & Febiger. Philadelphia.
10 The Importance of Making a Cancer Pain Diagnosis

11 Diagnosing Pain **Do not just treat the symptom! Must have a diagnosis!! Diagnosis is in the History Characterize pain in full Diagnostic History Prior pain therapies Thorough Physical Exam If source unclear --> Get more data, labs/imaging etc Rule Out Onc Emergencies: Cord compression, Evolving SBO, PE etc Diagnosis --> More Effective and Targeted Therapy
12 Treating Cancer Pain
13 The WHO Cancer Pain Ladder Miguel, R. Interventional treatment of cancer pain: the fourth step in the World Health Organization analgesic ladder? Cancer Control Mar-Apr; 7 (2):
14 Non-Opioids for Cancer Pain
15 Non-Opioids Analgesics Adjuvant* Analgesics & Co-Analgesics *Drugs with other indications that may be used as analgesics - Acetaminophen - NSAIDs* - Topical Agents - Anti-Spasmodics - Corticosteroids* - Bisphosphonates/RANK-L Inhibitors* - Neuropathic Agents*
16 Opioids for Cancer Pain

17 Principles of Opioid Prescribing Derived from opium, from juice of poppy Papaver Somniferum Bind to mu, delta, and kappa opioid receptors Main effects are in dorsal horn of spinal cord Mainstay of moderate to severe cancer pain Drug selection Dosing to optimize effects Treating side effects
18 Short-Acting Immediate Release Opioids Short-Acting Opioids: Morphine (MSIR) Oxycodone Hydromorphone Fentanyl (IV or Transmucosal/Buccal/Sublingual) Oxymorphone Immediate Release Combination products (eg Opioid+Acetaminophen) Weak Mu Agonists (Tramadol & Tapentadol)
19 Long Acting Extended Release Opioids Extended Release Morphine: Morphine CR, Kadian*, Avinza* Oxycodone: Oxycodone CR Hydromorphone: Hydromorphone ER Oxymorphone: Oxymorphone ER Fentanyl: Transdermal Patch Inherently Long Acting: Methadone
20 Opioid Dosing Guidelines Use Short-acting agents for: Opioid naïve patient Dose finding total daily opioid dose Premedication prior to Incident Pain Add basal agent (long-acting opioid) in dose equal to % of 24 hour dose of PRN opioid consumed Continue PRN opioid in dose equal to 10-15% of the 24 hour dose of long-acting opioid

21 Opioid Dosing Guidelines If >3-4 doses of PRN opioid if used in 24hrs adjust long-acting opioid: Increase again by % of 24 hour dose of PRN opioid used Generally no more freq than q48-72hrs Continued evaluation & titration is critical to successful therapy Increase dose until pain relief is adequate OR intolerable and unmanageable side effects occur
22 Opioids & Special Populations Patients with Renal Insufficiency Avoid Morphine, Codeine Caution w/ Oxycodone, Hydromorphone Methadone/Fentanyl Ok Patients with bowel obstruction/unable to swallow Hydrophilic opioid elixirs (Oxycodone, Morphine, Hydromorphone) still need to get to SI Consider IV, Fentanyl, Methadone Long acting agents in patients with Gtubes Kadian/Avinza, Fentanyl Patch, Methadone

23 Case Part 1 57F w/ metastatic lung CA to chest wall - Opioid naive --> Morphine IR mg q4hrs prn - Two days later : Used total 90mg/24hrs - You decide to start a long acting agent: Morphine ER - Convert % into long-acting = 67% of 90mg is 60mg Morphone ER 30mg po q12hrs (~2/3 total daily morphine) - Continue breakthrough agent at 10-15% total daily opioid dose = Morphine IR mg q4hrs
24 Case Part 2 Same lung Ca patient Presents to clinic few weeks later Now up to Morphine ER 60mg po q12hrs Pain better, but family notes mild sedation/confusion
25 Managing Opioid Side Effects 25
26 Managing Poor Opioid Responsiveness If dose escalation adverse effects: 1. Pharmacologic strategy to lower opioid requirement Optimize non-opioid or adjuvant analgesics Intrathecal route of administration 2. Treat the side-effects 3. Opioid rotation
27 Treating Opioid Side Effects Constipation: Bowel regimen at time of starting opioid, uptitrate as needed and treat aggressively. Nausea: Tolerance may develop after few days, consider dopamine antagonist Allergy: True IgE reaction rare, more commonly non-specific histamine release Myoclonus: Dose reduction/rotation, benzo or baclofen Sedation: Tolerance may develop, consider CNS stimulant (eg Methylphenidate, Modafinil) Delirium: Dose reduction/rotation, r/o other causes, neuroleptics
28 Managing Poor Opioid Responsiveness If dose escalation adverse effects 1. Pharmacologic strategy to lower opioid requirement Optimize non-opioid or adjuvant analgesics Intrathecal route of administration 2. Treat the side-effects 3. Opioid Rotation
29 Equianalgesic Conversions Drug IV(mg) PO (mg) Morphine Oxycodone N/A 20 Hydromorphone Oxymorphone 1 10 Fentanyl 0.1 N/A Methadone* (separate conversion guidelines)
30 Incomplete Cross Tolerance Reduce equianalgesic dose by 25% 50% to account for incomplete cross-tolerance Patients will have partial but not full tolerance to a new opioid Reduce less if pain severe Reduce less if same drug by different route Reduce more if medically frail or big conversion
31 Case Part 2 Same lung Ca patient; now on Morphine ER 60mg po q12hrs but with significant sedation/confusion Decide to Rotate to Oxycodone Controlled Release Total daily Morphine ER = 120mg
32 Equianalgesic Conversions Drug IV(mg) PO (mg) Morphine Oxycodone N/A 20 Hydromorphone Oxymorphone 1 10 Fentanyl 0.1 N/A Methadone* (separate conversion guidelines)
33 Case Part 2 Total daily Morphine ER: 120mg/24hrs Morphine: Oxycodone = 3:2 120mg Morphine = 80mg Oxycodone Decrease 25-50% for incomplete x-tolerance Oxycodone 60mg/24hrs 20mg of Oxycodone CR q8hrs

34 Methadone: A Unique Opioid NMDA, NE, and 5HT effects Unique pharmacokinetics (early alpha and late beta) When used for pain: BID-TID dosing Variable and unpredictable half-life ( hrs) Steady-state in 3-5 days to up to several weeks Close monitoring needed until steady-state reached Unique equianalgesic conversion ratios QTc prolongation issues Ask for Help When Considering Methadone for Pain!
35 Common Cancer Pain Syndromes: Neuropathic & Bone Pain
")

36 Neuropathic Pain & Cancer Common Neuropathic Cancer Pain Syndromes: Most common post-treatment pain syndrome Chemotherapy Induced Peripheral Neuropathy (CIPN) Post-thoracotomy/ Tumor Involvement of Chest Wall Brachial/Lumbosacral plexopathies Post-Herpetic Neuralgia Neuropathic Agents Anti-depressants: TCAs, Duloxetine Anti-epileptics: Gabapentin, Pregabalin
 Radiation Therapy Procedures: Cryoablation, Vert Augmentation for Comp")
37 Bone Pain is a Very Common: Adjuvants Can Be Particularly Helpful Corticosteroids NSAIDs Bisphosphonates - Pamidronate, Zoledronic Acid Rank-Ligand Inhibitors Radionucleides (Radium, Samarium, Strontium) Radiation Therapy Procedures: Cryoablation, Vert Augmentation for Comp Fx 37

38 Case #3: 56M with Metastatic Prostate Cancer, admitted with back pain Paged that he is reporting 10/10 mid-back pain Nurse has given him 2mg IV morphine w/o effect 1 hr ago What do you do now? Give him another 2mg IV morphine? Give him 4mg IV morphine? Switch to IV hydromorphone?
39 Managing an Acute Cancer Pain Crisis
40 Managing Pain Crises Action Depends on Patient s Response: After ~15-30 minutes: If no pain relief and no side effect: Increase dose % If partial pain relief and no side effect: Repeat Initial Dose If good pain relief: Use this dose as Breakthrough Dose and Consider PCA If no pain relief and side effects: Rotate to Different Opioid Stay at the Bedside (or Close-By), Reassess every 30min Remember IV Ketoralac if no contraindication Call for help when out of comfort range Always look for an underlying diagnosis or source of pain Moryl et al. Managing an acute pain crisis in a patient with advanced cancer: "this is as much of a crisis as a code". JAMA 2008.
41 A Quick Word on Opioids and Addiction in Cancer Pain
42 Opioid Therapy & Chemical Dependency in Cancer Patients Risk of addiction in cancer pain thought to be Low Evidence suggests that addiction or related problematic opioid use ranges from % in cancer patients 1-4 But the risk is definitely not Zero Same risk factors for abuse as in chronic non-cancer pain 5 Prior personal hx, family hx, sig anxiety/depression, PTSD etc Consider usual opioid risk mitigation measures if mod-high risk They re dying, why not just give them what they want? 1.Macaluso, C., D. Weinberg & K.M. Foley Opioid abuse and misuse in a cancer pain population. J. Pain Symptom Manage. 3: S Passik, S.D., K.L. Kirsh, M.V. McDonald, S. Ahn, et al A pilot survey of aberrant drug-taking attitudes and behaviors in samples of cancer and AIDS patients. J. Pain Symptom Manage. 19: Passik, S.D., J. Schreiber & K.L. Kirsh A chart review of the ordering of urine toxicology screen in a cancer center: do they influence on pain management. J. Pain Symptom Manage. 19: Schug, S.A., D. Zech, S. Grond, et al A long term survey of morphine in cancer pain patients. J Pain Symptom Manage. 7: Del Fabbro Assessment and Management of Chemical Coping in Patients With Cancer. JCO 2014:32;
43 What if the Pills Don t Work? Consider Interventional Therapies for Cancer Pain
44 The Cancer Pain State of the Union Continued: 50% of pts on third tier of WHO based on prospective study >2000 pts 14-24% of pts with pain despite WHO ladder Miguel, R. Interventional treatment of cancer pain: the fourth step in the World Health Organization analgesic ladder? Cancer Control Mar-Apr; 7 (2):

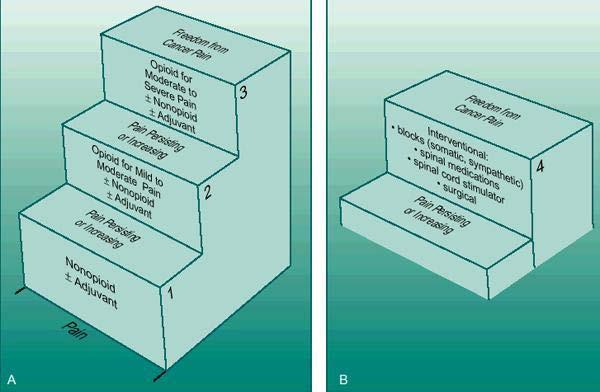
45 Interventional Tx : The 4th WHO Step?
46 What is Total Pain? The Importance of Palliative Care and the Multidisciplinary Approach

47 Understanding Total Pain Physical Pain Is Just One Element of Suffering Suffering: Physical* Emotional Social Spiritual Need to Attend to All Elements to be Effective No One Person Can Meet All These Needs = Multidisciplinary Approach is Imperative for Cancer Pain 47
48 The Take Home Points
49 Take Home Points: Cancer Pain Understand the pain syndrome: Must have make diagnosis! Optimize co-analgesics and adjuvant medications Use opioids for moderate to severe pain Proper opioid selection Use of short-acting and long-acting opioids Titration, side effect mgmt, & opioid rotation Remember: Interventional Therapies for Cancer Pain The Interdisciplinary Approach to Total Pain
50 Thank You!
PALLIATIVE TREATMENT BY DR. KHRONGKAMOL SIHABAN MEDICAL ONCOLOGIST
 PALLIATIVE TREATMENT BY DR. KHRONGKAMOL SIHABAN MEDICAL ONCOLOGIST TREATMENT IN ONCOLOGY Main treatment : surgery Neoadjuvant treatment : RT, CMT Adjuvant treatment : Tx micrometastatic disease -CMT,Targeted
PALLIATIVE TREATMENT BY DR. KHRONGKAMOL SIHABAN MEDICAL ONCOLOGIST TREATMENT IN ONCOLOGY Main treatment : surgery Neoadjuvant treatment : RT, CMT Adjuvant treatment : Tx micrometastatic disease -CMT,Targeted
Interprofessional Webinar Series
 Interprofessional Webinar Series Opioids in the Medically Ill: Principles of Administration Russell K. Portenoy, MD Chief Medical Officer MJHS Hospice and Palliative Care Director MJHS Institute for Innovation
Interprofessional Webinar Series Opioids in the Medically Ill: Principles of Administration Russell K. Portenoy, MD Chief Medical Officer MJHS Hospice and Palliative Care Director MJHS Institute for Innovation
PAIN MANAGEMENT PGY-1. Aaron D. Storms, MD Carin van Zyl, MD Adult and Pediatric Palliative Care, LAC+USC Keck School of Medicine of USC
 PAIN MANAGEMENT PGY-1 Aaron D. Storms, MD Carin van Zyl, MD Adult and Pediatric Palliative Care, LAC+USC Keck School of Medicine of USC Perception Matters A builder aged 29 came to the accident and emergency
PAIN MANAGEMENT PGY-1 Aaron D. Storms, MD Carin van Zyl, MD Adult and Pediatric Palliative Care, LAC+USC Keck School of Medicine of USC Perception Matters A builder aged 29 came to the accident and emergency
Fighting the Good Fight: How to Convert Opioids Just Right!
 Fighting the Good Fight: How to Convert Opioids Just Right! Tanya J. Uritsky, PharmD, BCPS, CPE Clinical Pharmacy Specialist - Pain Medication Stewardship Hospital of the University of Pennsylvania - Philadelphia,
Fighting the Good Fight: How to Convert Opioids Just Right! Tanya J. Uritsky, PharmD, BCPS, CPE Clinical Pharmacy Specialist - Pain Medication Stewardship Hospital of the University of Pennsylvania - Philadelphia,
Acute Pain Management in the Hospital Setting. Alexandra Phan, PharmD PGY-1 Pharmacy Practice Resident Medical Center Hospital Odessa, TX
 Acute Pain Management in the Hospital Setting Alexandra Phan, PharmD PGY-1 Pharmacy Practice Resident Medical Center Hospital Odessa, TX 2 What is Pain? An unpleasant sensory and emotional experience associated
Acute Pain Management in the Hospital Setting Alexandra Phan, PharmD PGY-1 Pharmacy Practice Resident Medical Center Hospital Odessa, TX 2 What is Pain? An unpleasant sensory and emotional experience associated
Overview of Essentials of Pain Management. Updated 11/2016
 0 Overview of Essentials of Pain Management Updated 11/2016 1 Overview of Essentials of Pain Management 1. Assess pain intensity on a 0 10 scale in which 0 = no pain at all and 10 = the worst pain imaginable.
0 Overview of Essentials of Pain Management Updated 11/2016 1 Overview of Essentials of Pain Management 1. Assess pain intensity on a 0 10 scale in which 0 = no pain at all and 10 = the worst pain imaginable.
Pain management. Coleman Palliative Care Conference: February 2016 Josh Baru MD Stacie Levine MD
 Pain management Coleman Palliative Care Conference: February 2016 Josh Baru MD Stacie Levine MD Case #1 61 yo man with history of Stage 3 colon cancer, s/p resection and adjuvant chemotherapy with FOLFOX
Pain management Coleman Palliative Care Conference: February 2016 Josh Baru MD Stacie Levine MD Case #1 61 yo man with history of Stage 3 colon cancer, s/p resection and adjuvant chemotherapy with FOLFOX
Cancer Pain: A Clinical Overview. Linda A. King, MD Section of Palliative Care and Medical Ethics
 Cancer Pain: A Clinical Overview Linda A. King, MD Section of Palliative Care and Medical Ethics Objectives Define Palliative Care Review prevalence of cancer pain Know barriers to cancer pain management
Cancer Pain: A Clinical Overview Linda A. King, MD Section of Palliative Care and Medical Ethics Objectives Define Palliative Care Review prevalence of cancer pain Know barriers to cancer pain management
4/3/2018. Management of Acute Pain Crises. Five Mistakes I ve made and why you shouldn t
 Management of Acute Pain Crises Maggie O Connor, M.D. Retired Palliative Care Physician Hope is not the conviction that something will turn out well, but the certainty that something makes sense, regardless
Management of Acute Pain Crises Maggie O Connor, M.D. Retired Palliative Care Physician Hope is not the conviction that something will turn out well, but the certainty that something makes sense, regardless
Narcotic Analgesics. Jacqueline Morgan March 22, 2017
 Narcotic Analgesics Jacqueline Morgan March 22, 2017 Pain Unpleasant sensory and emotional experience with actual or potential tissue damage Universal, complex, subjective experience Number one reason
Narcotic Analgesics Jacqueline Morgan March 22, 2017 Pain Unpleasant sensory and emotional experience with actual or potential tissue damage Universal, complex, subjective experience Number one reason
1/21/14. Cancer Related Pain: Case-Based Pharmacology. Conflicts of Interest. Learning Objective
 Cancer Related Pain: Case-Based Pharmacology Jeannine M. Brant, PhD, APRN, AOCN Oncology Clinical Nurse Specialist Nurse Scientist Billings Clinic Conflicts of Interest Jeannine Brant has served on the
Cancer Related Pain: Case-Based Pharmacology Jeannine M. Brant, PhD, APRN, AOCN Oncology Clinical Nurse Specialist Nurse Scientist Billings Clinic Conflicts of Interest Jeannine Brant has served on the
Palliative Prescribing - Pain
 Palliative Prescribing - Pain LAURA BARNFIELD 21/2/17 Aims To understand the classes of painkillers available in palliative care To gain confidence in counselling regarding opiates To gain confidence prescribing
Palliative Prescribing - Pain LAURA BARNFIELD 21/2/17 Aims To understand the classes of painkillers available in palliative care To gain confidence in counselling regarding opiates To gain confidence prescribing
GUIDELINES AND AUDIT IMPLEMENTATION NETWORK
 GUIDELINES AND AUDIT IMPLEMENTATION NETWORK General Palliative Care Guidelines The Management of Pain at the End Of Life November 2010 Aim To provide a user friendly, evidence based guide for the management
GUIDELINES AND AUDIT IMPLEMENTATION NETWORK General Palliative Care Guidelines The Management of Pain at the End Of Life November 2010 Aim To provide a user friendly, evidence based guide for the management
Opioid Case Studies. Thomas P. Pittelkow, D.O., M.P.H. Mayo Clinic College of Medicine Rochester, MN. September 29, MFMER slide-1
 Opioid Case Studies Thomas P. Pittelkow, D.O., M.P.H. Mayo Clinic College of Medicine Rochester, MN September 29, 2016 2015 MFMER slide-1 Disclosures Relevant Financial Relationship(s) None Off Label and/or
Opioid Case Studies Thomas P. Pittelkow, D.O., M.P.H. Mayo Clinic College of Medicine Rochester, MN September 29, 2016 2015 MFMER slide-1 Disclosures Relevant Financial Relationship(s) None Off Label and/or
Pain Management in the Hospital
 E P E C O Pain Management in the Hospital Denise Waugh, MD FACEP FAAHPM Medical Director of Palliative Care Services Scott and White Healthcare 724-6859 Pain is a more terrible lord of mankind than even
E P E C O Pain Management in the Hospital Denise Waugh, MD FACEP FAAHPM Medical Director of Palliative Care Services Scott and White Healthcare 724-6859 Pain is a more terrible lord of mankind than even
Tips for Managing Acute Pain
 Tips for Managing Acute Pain Daniel Johnson, MD, FAAHPM Kaiser Permanente University of Colorado Session Outline 1. Pseudoaddiction 2. Opioid Selection 3. PCA Titration 4. Co-Analgesics 5. Breakthrough
Tips for Managing Acute Pain Daniel Johnson, MD, FAAHPM Kaiser Permanente University of Colorado Session Outline 1. Pseudoaddiction 2. Opioid Selection 3. PCA Titration 4. Co-Analgesics 5. Breakthrough
Pain Management Dilemmas. Five Pain Dilemmas. Barriers: Meet Loretta. Daniel Johnson, MD, FAAHPM
 Pain Management Dilemmas Daniel Johnson, MD, FAAHPM Kaiser Permanente University of Colorado Five Pain Dilemmas 1. Barriers to Pain Management 2. Selecting and Titrating Opioids 3. Managing PCAs 4. Using
Pain Management Dilemmas Daniel Johnson, MD, FAAHPM Kaiser Permanente University of Colorado Five Pain Dilemmas 1. Barriers to Pain Management 2. Selecting and Titrating Opioids 3. Managing PCAs 4. Using
Opioid Conversions Mixture of Science and Art
 Opioid Conversions Mixture of Science and Art Matthew J. Pingree, MD Assistant Professor Division of Pain Medicine Physical Medicine and Rehabilitation and Anesthesiology Mayo Clinic, Rochester Pingree.Matthew@Mayo.edu
Opioid Conversions Mixture of Science and Art Matthew J. Pingree, MD Assistant Professor Division of Pain Medicine Physical Medicine and Rehabilitation and Anesthesiology Mayo Clinic, Rochester Pingree.Matthew@Mayo.edu
Pain. November 1, 2006 Dr. Jana Pilkey MD, FRCP(C) Internal Medicine, Palliative Medicine
 Internal Medicine, Palliative Medicine") Pain November 1, 2006 Dr. Jana Pilkey MD, FRCP(C) Internal Medicine, Palliative Medicine Objectives To be able to define pain To be able to evaluate pain To be able to classify types of pain To learn appropriate
Pain November 1, 2006 Dr. Jana Pilkey MD, FRCP(C) Internal Medicine, Palliative Medicine Objectives To be able to define pain To be able to evaluate pain To be able to classify types of pain To learn appropriate
Introduction To Pain Management In Palliative Care
 Introduction To Pain Management In Palliative Care May 9, 2005 University of Manitoba Faculty of Nursing Mike Harlos MD, CCFP, FCFP Medical Director, WRHA Palliative Care Professor, University of Manitoba
Introduction To Pain Management In Palliative Care May 9, 2005 University of Manitoba Faculty of Nursing Mike Harlos MD, CCFP, FCFP Medical Director, WRHA Palliative Care Professor, University of Manitoba
Palliative Care for Primary Care Providers QUYNH BUI, MD MPH DECEMBER 2015
 Palliative Care for Primary Care Providers QUYNH BUI, MD MPH DECEMBER 2015 Objectives Define palliative care and primary palliative care Describe the rationale for providing primary palliative care in
Palliative Care for Primary Care Providers QUYNH BUI, MD MPH DECEMBER 2015 Objectives Define palliative care and primary palliative care Describe the rationale for providing primary palliative care in
Cancer Pain Management: An Overview
 Cancer Pain Management: An Overview Dr. Mike Harlos Medical Director, WRHA Palliative Care 1 Pain An unpleasant sensory and emotional experience associated with actual or potential tissue damage, or described
Cancer Pain Management: An Overview Dr. Mike Harlos Medical Director, WRHA Palliative Care 1 Pain An unpleasant sensory and emotional experience associated with actual or potential tissue damage, or described
NEUROPATHIC CANCER PAIN STANDARDS AND GUIDELINES
 NEUROPATHIC CANCER PAIN STANDARDS AND GUIDELINES GENERAL PRINCIPLES Neuropathic pain may be relieved in the majority of patients by multimodal management A careful history and examination are essential.
NEUROPATHIC CANCER PAIN STANDARDS AND GUIDELINES GENERAL PRINCIPLES Neuropathic pain may be relieved in the majority of patients by multimodal management A careful history and examination are essential.
Opioid Pearls and Acute Pain Management
 Opioid Pearls and Acute Pain Management Jeanie Youngwerth, MD University of Colorado Denver Assistant Professor of Medicine, Hospitalist Associate Director, Colorado Palliative Medicine Fellowship Program
Opioid Pearls and Acute Pain Management Jeanie Youngwerth, MD University of Colorado Denver Assistant Professor of Medicine, Hospitalist Associate Director, Colorado Palliative Medicine Fellowship Program
What to do when you are called to see a patient with... PAIN. Susan Merel, MD Division of General Internal Medicine July 2018
 What to do when you are called to see a patient with... PAIN Susan Merel, MD Division of General Internal Medicine July 2018 Disclosures Susan Merel has no relationships with any entity producing, marketing,
What to do when you are called to see a patient with... PAIN Susan Merel, MD Division of General Internal Medicine July 2018 Disclosures Susan Merel has no relationships with any entity producing, marketing,
Universal Precautions and Opioid Risk. Assessment. Questions: How often do you screen your patients for risk of misuse when prescribing opioids?
 Learning objectives 1. Identify the contribution of psychosocial and spiritual factors to pain 2. Incorporate strategies for identifying and mitigating opioid misuse 3. Incorporate non-pharmaceutical modalities
Learning objectives 1. Identify the contribution of psychosocial and spiritual factors to pain 2. Incorporate strategies for identifying and mitigating opioid misuse 3. Incorporate non-pharmaceutical modalities
Lumbar Fusion. Reference Guide for PACU CLINICAL PATHWAY. All patient variances to the pathway are to be circled and addressed in the progress notes.
 Reference Guide for PACU Lumbar Fusion CLINICAL PATHWAY All patient variances to the pathway are to be circled and addressed in the progress notes. This Clinical Pathway is intended to assist in clinical
Reference Guide for PACU Lumbar Fusion CLINICAL PATHWAY All patient variances to the pathway are to be circled and addressed in the progress notes. This Clinical Pathway is intended to assist in clinical
Intractable pain syndrome is defined as persistent pain despite all the reasonable efforts to treat.
 Difficult Pain Syndrome/Intractable/Refractory Pain Intractable pain syndrome is defined as persistent pain despite all the reasonable efforts to treat. Reasonable efforts Differs for specialties/regions/countries
Difficult Pain Syndrome/Intractable/Refractory Pain Intractable pain syndrome is defined as persistent pain despite all the reasonable efforts to treat. Reasonable efforts Differs for specialties/regions/countries
Pain Management in Hospice and Palliative Care
 Pain Management in Hospice and Palliative Care A Case-based Approach JoAnne Nowak, M.D. Merrimack Valley Hospice Revised November 2011 Objectives Use a case study approach to stimulate discussion and illustrate
Pain Management in Hospice and Palliative Care A Case-based Approach JoAnne Nowak, M.D. Merrimack Valley Hospice Revised November 2011 Objectives Use a case study approach to stimulate discussion and illustrate
THE EAPC OPIOID GUIDELINES: PROCESS, RESULTS AND FUTURE DEVELOPMENT
 1 THE EAPC OPIOID GUIDELINES: PROCESS, RESULTS AND FUTURE DEVELOPMENT Jaegtvolden 4-5 June 2012 14. 12. 2012 2 1 3 WHO ANALGESIC LADDER (1996) NSAID +/- Adjuvant STEP II OPIODS Opids for mild to moderate
1 THE EAPC OPIOID GUIDELINES: PROCESS, RESULTS AND FUTURE DEVELOPMENT Jaegtvolden 4-5 June 2012 14. 12. 2012 2 1 3 WHO ANALGESIC LADDER (1996) NSAID +/- Adjuvant STEP II OPIODS Opids for mild to moderate
GUIDELINES ON THE MANAGEMENT OF PAIN DUE TO CANCER IN ADULTS
 GUIDELINES ON THE MANAGEMENT OF PAIN DUE TO CANCER IN ADULTS Bristol Palliative Care Collaborative Contact Numbers: Hospital Specialist Palliative Care Teams: North Bristol 0117 4146392 UH Bristol 0117
GUIDELINES ON THE MANAGEMENT OF PAIN DUE TO CANCER IN ADULTS Bristol Palliative Care Collaborative Contact Numbers: Hospital Specialist Palliative Care Teams: North Bristol 0117 4146392 UH Bristol 0117
E-Learning Module N: Pharmacological Review
 E-Learning Module N: Pharmacological Review This Module requires the learner to have read Chapter 13 of the Fundamentals Program Guide and the other required readings associated with the topic. Revised:
E-Learning Module N: Pharmacological Review This Module requires the learner to have read Chapter 13 of the Fundamentals Program Guide and the other required readings associated with the topic. Revised:
BASICS OF OPIOID PRESCRIBING 10:30-11:45AM
 PROVIDING QUALITY CARE TO PAIN PATIENTS IN IOWA BASICS OF OPIOID PRESCRIBING 10:30-11:45AM ACPE UAN: 107-000-14-013-L01-P Activity Type: Application-Based 0.125 CEU/1.25hr Learning Objectives for Pharmacists:
PROVIDING QUALITY CARE TO PAIN PATIENTS IN IOWA BASICS OF OPIOID PRESCRIBING 10:30-11:45AM ACPE UAN: 107-000-14-013-L01-P Activity Type: Application-Based 0.125 CEU/1.25hr Learning Objectives for Pharmacists:
10/08/59 PAIN IS THE MOST COMMON TREATABLE SYMPTOM OF CANCER CURRENT EVIDENCE BASED CONCEPTS: MANAGEMENT OF CANCER PAIN PAIN AN UNMET CLINICAL NEED IN
 Pain is a frequent complication of cancer, and is common in many other life-limiting illnesses MANAGEMENT OF CANCER PAIN A/Prof Ghauri Aggarwal FRACP, FAChPM, FFPMANZCA Palliative Medicine Physician Sydney
Pain is a frequent complication of cancer, and is common in many other life-limiting illnesses MANAGEMENT OF CANCER PAIN A/Prof Ghauri Aggarwal FRACP, FAChPM, FFPMANZCA Palliative Medicine Physician Sydney
Palliative and Hospice Care of the Terminally Ill Introduction
 Palliative and Hospice Care of the Terminally Ill Introduction There has been an increase in life expectancy for men and women of all races to 77.6 years Leading causes of death in older patients are chronic
Palliative and Hospice Care of the Terminally Ill Introduction There has been an increase in life expectancy for men and women of all races to 77.6 years Leading causes of death in older patients are chronic
Pain is a more terrible Lord of mankind than even death itself.
 CHRONIC OPIOID RX FOR NON-MALIGNANT PAIN Gerald M. Aronoff, M.D., DABPM Med. Dir., Carolina Pain Assoc Charlotte, North Carolina, USA Pain Pain is a more terrible Lord of mankind than even death itself.
CHRONIC OPIOID RX FOR NON-MALIGNANT PAIN Gerald M. Aronoff, M.D., DABPM Med. Dir., Carolina Pain Assoc Charlotte, North Carolina, USA Pain Pain is a more terrible Lord of mankind than even death itself.
Steven Prakken MD Chief, Medical Pain Service Duke Pain Medicine
 Steven Prakken MD Chief, Medical Pain Service Duke Pain Medicine International Association for the Study of Pain "Pain is an unpleasant sensory and emotional experience associated with actual or potential
Steven Prakken MD Chief, Medical Pain Service Duke Pain Medicine International Association for the Study of Pain "Pain is an unpleasant sensory and emotional experience associated with actual or potential
CLINICAL POLICY DEPARTMENT: Medical
 IMPTANT REMINDER This Clinical Policy has been developed by appropriately experienced and licensed health care professionals based on a thorough review and consideration of currently available generally
IMPTANT REMINDER This Clinical Policy has been developed by appropriately experienced and licensed health care professionals based on a thorough review and consideration of currently available generally
Introduction To Pain Management In Palliative Care
 Introduction To Pain Management In Palliative Care Jan. 17, 2005 University of Manitoba Faculty of Nursing Mike Harlos MD, CCFP, FCFP Medical Director, WRHA Palliative Care Associate Professor, University
Introduction To Pain Management In Palliative Care Jan. 17, 2005 University of Manitoba Faculty of Nursing Mike Harlos MD, CCFP, FCFP Medical Director, WRHA Palliative Care Associate Professor, University
CHAMP: Bedside Teaching TREATING PAIN. Stacie Levine MD. What is the approach to treating pain in the aging adult patient?
 CHAMP: Bedside Teaching TREATING PAIN Stacie Levine MD Teaching Trigger: An older adult patient is identified as having pain. Clinical Question: What is the approach to treating pain in the aging adult
CHAMP: Bedside Teaching TREATING PAIN Stacie Levine MD Teaching Trigger: An older adult patient is identified as having pain. Clinical Question: What is the approach to treating pain in the aging adult
Equianalgesic Dosing: Making Opioid Interchange Easier. Joseph Bubalo PharmD, BCPS, BCOP Oncology Clinical Pharmacist Assistant Professor Of Medicine
 Equianalgesic Dosing: Making Opioid Interchange Easier Joseph Bubalo PharmD, BCPS, BCOP Oncology Clinical Pharmacist Assistant Professor Of Medicine 1 Why Change Opioids? Side Effects Insufficient Pain
Equianalgesic Dosing: Making Opioid Interchange Easier Joseph Bubalo PharmD, BCPS, BCOP Oncology Clinical Pharmacist Assistant Professor Of Medicine 1 Why Change Opioids? Side Effects Insufficient Pain
Choose a category. You will be given the answer. You must give the correct question. Click to begin.
 Instructions for using this template. Remember this is Jeopardy, so where I have written Answer this is the prompt the students will see, and where I have Question should be the student s response. To
Instructions for using this template. Remember this is Jeopardy, so where I have written Answer this is the prompt the students will see, and where I have Question should be the student s response. To
RELIEVING VIRGINIA S PAIN AND SUFFERING 3:45-4:45PM
 PROVIDING QUALITY CARE TO PAIN PATIENTS IN IOWA RELIEVING VIRGINIA S PAIN AND SUFFERING 3:45-4:45PM ACPE UAN: 107-000-14-016-L05-P Activity Type: Application-Based 0.1 CEU/1.0 hr Learning Objectives for
PROVIDING QUALITY CARE TO PAIN PATIENTS IN IOWA RELIEVING VIRGINIA S PAIN AND SUFFERING 3:45-4:45PM ACPE UAN: 107-000-14-016-L05-P Activity Type: Application-Based 0.1 CEU/1.0 hr Learning Objectives for
Analgesics: Management of Pain In the Elderly Handout Package
 Analgesics: Management of Pain In the Elderly Handout Package Analgesics: Management of Pain in the Elderly Each patient or resident and their pain problem is unique. A complete assessment should be performed
Analgesics: Management of Pain In the Elderly Handout Package Analgesics: Management of Pain in the Elderly Each patient or resident and their pain problem is unique. A complete assessment should be performed
Review of Pain Management with Clinical and Regulatory Updates
 Review of Pain Management with Clinical and Regulatory Updates Palliative Care Collaborative: 8 th Annual Regional Conference October 10, 2014 Michael Stellini, M.D.,M.S. Medical Director, Hospice and
Review of Pain Management with Clinical and Regulatory Updates Palliative Care Collaborative: 8 th Annual Regional Conference October 10, 2014 Michael Stellini, M.D.,M.S. Medical Director, Hospice and
Complex Symptom Management at the End of Life of Pediatric Patients
 Complex Symptom Management at the End of Life of Pediatric Patients Justin N Baker, MD, FAAP, FAAHPM Chief, Division of Quality of Life and Palliative Care Director, Hematology/Oncology Fellowship Program
Complex Symptom Management at the End of Life of Pediatric Patients Justin N Baker, MD, FAAP, FAAHPM Chief, Division of Quality of Life and Palliative Care Director, Hematology/Oncology Fellowship Program
Module 2 Pain Management. Handouts. Pain Is... Please click the links button under the video. You can print and/or save the handouts.
 E L N E C End-of-Life Nursing Education Consortium SuperCore Curriculum Module 2 Pain Management Handouts Please click the links button under the video. You can print and/or save the handouts. Pain Is...
E L N E C End-of-Life Nursing Education Consortium SuperCore Curriculum Module 2 Pain Management Handouts Please click the links button under the video. You can print and/or save the handouts. Pain Is...
Pain Management Strategies Webinar/Teleconference
 Pain Management Strategies Webinar/Teleconference Barry K. Baines, MD April 16, 2009 Objectives Describe the principles of pain management. Identify considerations in the use of opioids. Describe the benefits
Pain Management Strategies Webinar/Teleconference Barry K. Baines, MD April 16, 2009 Objectives Describe the principles of pain management. Identify considerations in the use of opioids. Describe the benefits
Pain Management Management in Hepatic Hepatic and and Renal Dysfunction
 Pain Management in Hepatic and Renal Dysfunction Review the pharmacologic basis for medications used in pain management Identify pain medications which hshould ldbe avoided in patients with hepatic dysfunction
Pain Management in Hepatic and Renal Dysfunction Review the pharmacologic basis for medications used in pain management Identify pain medications which hshould ldbe avoided in patients with hepatic dysfunction
See Important Reminder at the end of this policy for important regulatory and legal information.
 Clinical Policy: Reference Number: CP.CPA.259 Effective Date: 11.16.16 Last Review Date: 11.17 Line of Business: Commercial Revision Log See Important Reminder at the end of this policy for important regulatory
Clinical Policy: Reference Number: CP.CPA.259 Effective Date: 11.16.16 Last Review Date: 11.17 Line of Business: Commercial Revision Log See Important Reminder at the end of this policy for important regulatory
Pain Management: Overview of A Practical Approach
 Pain Management: Overview of A Practical Approach Michael B. Potter, M.D. Department of Family and Community Medicine University of California, San Francisco What is Pain? An unpleasant sensory and emotional
Pain Management: Overview of A Practical Approach Michael B. Potter, M.D. Department of Family and Community Medicine University of California, San Francisco What is Pain? An unpleasant sensory and emotional
PAIN. TREATMENT TABLES Analgesics. NON-OPIOID ANALGESICS Generic Name Trade Names (Examples) Duration Initial Dose
 Duration Initial Dose") NON-OPIOID SHORT-ACTING LONG-ACTING **** O PAIN TREATMENT TABLES Analgesics NON-OPIOID ANALGESICS Generic Name Trade Names (Examples) Duration Initial Dose Tramadol 50 mg Ultram Every 4 hours 1-2 tabs,
NON-OPIOID SHORT-ACTING LONG-ACTING **** O PAIN TREATMENT TABLES Analgesics NON-OPIOID ANALGESICS Generic Name Trade Names (Examples) Duration Initial Dose Tramadol 50 mg Ultram Every 4 hours 1-2 tabs,
Long Term Care Formulary HCD - 08
 1 of 5 PREAMBLE Opioids are an important component of the pharmaceutical armamentarium for management of chronic pain. The superiority of analgesic effect of one narcotic over another is not generally
1 of 5 PREAMBLE Opioids are an important component of the pharmaceutical armamentarium for management of chronic pain. The superiority of analgesic effect of one narcotic over another is not generally
GUIDELINES ON PAIN MANAGEMENT IN UROLOGY
 GUIDELINES ON PAIN MANAGEMENT IN UROLOGY F. Francesca (chairman), P. Bader, D. Echtle, F. Giunta, J. Williams Eur Urol 2003; 44(4):383-389 Introduction Pain is defined as an unpleasant sensory and emotional
GUIDELINES ON PAIN MANAGEMENT IN UROLOGY F. Francesca (chairman), P. Bader, D. Echtle, F. Giunta, J. Williams Eur Urol 2003; 44(4):383-389 Introduction Pain is defined as an unpleasant sensory and emotional
Domain 1 Pharmacokinetic and pharmacodynamics properties of methadone
 Methadone Survey Knowledge Domains: Domain 1 Pharmacokinetic and pharmacodynamics properties of methadone Domain 2 Appropriate/inappropriate candidates for methadone Domain 3 Risk stratification with methadone
Methadone Survey Knowledge Domains: Domain 1 Pharmacokinetic and pharmacodynamics properties of methadone Domain 2 Appropriate/inappropriate candidates for methadone Domain 3 Risk stratification with methadone
Sharon A Stephen, PhD, ARNP, ACHPN. September 23, 2014
 Sharon A Stephen, PhD, ARNP, ACHPN September 23, 2014 Case-based presentation selected to discuss: Pain assessment Barriers to adequate pain relief Pharmacologic interventions Non-Pharmacologic interventions
Sharon A Stephen, PhD, ARNP, ACHPN September 23, 2014 Case-based presentation selected to discuss: Pain assessment Barriers to adequate pain relief Pharmacologic interventions Non-Pharmacologic interventions
The pain of it all. Rod MacLeod MNZM. Hibiscus Hospice, Auckland and University of Auckland
 The pain of it all Rod MacLeod MNZM Hibiscus Hospice, Auckland and University of Auckland Definition of PAIN An unpleasant sensory and emotional experience which we primarily associate with tissue damage
The pain of it all Rod MacLeod MNZM Hibiscus Hospice, Auckland and University of Auckland Definition of PAIN An unpleasant sensory and emotional experience which we primarily associate with tissue damage
HOPE. Considerations. Considerations ISING. Safe Opioid Prescribing Guidelines for ACUTE Non-Malignant Pain
 Due to the high level of prescription drug use and abuse in Lake County, these guidelines have been developed to standardize prescribing habits and limit risk of unintended harm when prescribing opioid
Due to the high level of prescription drug use and abuse in Lake County, these guidelines have been developed to standardize prescribing habits and limit risk of unintended harm when prescribing opioid
Non-opioid and adjuvant pain management
 Non-opioid and adjuvant pain management ALLISON JORDAN, MD, HMDC MEDICAL DIRECTOR OF PALLIATIVE CARE SERVICES CHRISTIAN AND ALTON MEMORIAL HOSPITALS ASSOCIATE MEDICAL DIRECTOR, BJC HOSPICE ASSISTANT PROFESSOR
Non-opioid and adjuvant pain management ALLISON JORDAN, MD, HMDC MEDICAL DIRECTOR OF PALLIATIVE CARE SERVICES CHRISTIAN AND ALTON MEMORIAL HOSPITALS ASSOCIATE MEDICAL DIRECTOR, BJC HOSPICE ASSISTANT PROFESSOR
Dose equivalent of fentanyl patch to oxycontin
 Dose equivalent of fentanyl patch to oxycontin 10-3-2018 Detailed dosage guidelines and administration information for OxyContin (oxycodone hydrochloride). Includes dose adjustments, warnings and precautions.
Dose equivalent of fentanyl patch to oxycontin 10-3-2018 Detailed dosage guidelines and administration information for OxyContin (oxycodone hydrochloride). Includes dose adjustments, warnings and precautions.
Neuropathic Pain in Palliative Care
 Neuropathic Pain in Palliative Care Neuropathic Pain in Advanced Cancer Affects 40% of patients Multiple concurrent pains are common Often complex pathophysiology with mixed components Nocioceptive Neuropathic
Neuropathic Pain in Palliative Care Neuropathic Pain in Advanced Cancer Affects 40% of patients Multiple concurrent pains are common Often complex pathophysiology with mixed components Nocioceptive Neuropathic
Prescribers of Opioids
 Pain Management in Primary Care Part Two Joshua D. Dion MSN, APRN-BC, ACNP Prescribers of Opioids Know how to start, modify, and discontinue opioids. Know how to convert from SA to LA or change from on
Pain Management in Primary Care Part Two Joshua D. Dion MSN, APRN-BC, ACNP Prescribers of Opioids Know how to start, modify, and discontinue opioids. Know how to convert from SA to LA or change from on
ANSWER # 1 PHARMACOLOGY. Methadone answers Stoltzfus 4/5/2012 METHADONE: WHY GRANDMA S TAKING A DIPHENYLHEPTANE (ANSWERS) JANUARY 26, 2017
 JANUARY 26, 2017") METHADONE: WHY GRANDMA S TAKING A DIPHENYLHEPTANE (ANSWERS) JANUARY 26, 2017 Ky Stoltzfus, MD Assistant Professor, Internal Medicine University of Kansas Medical Center ANSWER # 1 Your response might be
METHADONE: WHY GRANDMA S TAKING A DIPHENYLHEPTANE (ANSWERS) JANUARY 26, 2017 Ky Stoltzfus, MD Assistant Professor, Internal Medicine University of Kansas Medical Center ANSWER # 1 Your response might be
Pain Assessment & Management. For General Nursing Orientation
 Pain Assessment & Management For General Nursing Orientation April 2012 Overview Definition of pain Barriers to effective pain management Types of pain Objective pain assessment Approaches to management
Pain Assessment & Management For General Nursing Orientation April 2012 Overview Definition of pain Barriers to effective pain management Types of pain Objective pain assessment Approaches to management
Objectives. Patient Controlled Analgesia (PCA) Management in the Seriously Ill. Discuss principles for opioid dosing and titration for acute pain
 Management in the Seriously Ill. Discuss principles for opioid dosing and titration for acute pain") Patient Controlled Analgesia (PCA) Management in the Seriously Ill Jeanie Youngwerth, MD University of Colorado School of Medicine Associate Professor of Medicine, Hospitalist Associate Director, Colorado
Patient Controlled Analgesia (PCA) Management in the Seriously Ill Jeanie Youngwerth, MD University of Colorado School of Medicine Associate Professor of Medicine, Hospitalist Associate Director, Colorado
Opioid Use in Serious Illness
 Opioid Use in Serious Illness Jeanie Youngwerth, MD University of Colorado School of Medicine Associate Professor of Medicine, Hospitalist Director, Palliative Care Service Associate Director, Colorado
Opioid Use in Serious Illness Jeanie Youngwerth, MD University of Colorado School of Medicine Associate Professor of Medicine, Hospitalist Director, Palliative Care Service Associate Director, Colorado
POST OPERATIVE PAIN MANAGEMENT: PAIN AND COMPLICATIONS
 POST OPERATIVE PAIN MANAGEMENT: PAIN AND COMPLICATIONS November 9, 2018 Aimee LaMere, CNP Molly McNaughton, CNP Leslie Weide, MSW, LICSW, ACM Disclosures: Conflict of interest statement: We certify that,
POST OPERATIVE PAIN MANAGEMENT: PAIN AND COMPLICATIONS November 9, 2018 Aimee LaMere, CNP Molly McNaughton, CNP Leslie Weide, MSW, LICSW, ACM Disclosures: Conflict of interest statement: We certify that,
Canadian Guideline for Opioids for Chronic Non-Cancer Pain. Speaker Disclosure. Objectives. Canadian Guideline for Opioids for Chronic Non-Cancer Pain
 Canadian Guideline for Opioids for Chronic Non-Cancer Pain John Fraser Community Hospital Program New Glasgow November 1, 2017 This speaker has been asked to disclose to the audience any involvement with
Canadian Guideline for Opioids for Chronic Non-Cancer Pain John Fraser Community Hospital Program New Glasgow November 1, 2017 This speaker has been asked to disclose to the audience any involvement with
Objectives: What is your Definition of Pain? 8/16/2017
 Safe Opioid Management for the Seriously Ill Patient Sam Perna, D.O. Objectives: MDB1 1) Participants will understand the way the body s pain system works. 2) Participants will identify the elements of
Safe Opioid Management for the Seriously Ill Patient Sam Perna, D.O. Objectives: MDB1 1) Participants will understand the way the body s pain system works. 2) Participants will identify the elements of
Objectives. Controversy. Pain. Risk Stratification 1/7/2012
 Objectives Strategies in Pain Management: Scheduled, Breakthrough, and Dose Adjustments Tamara M. Green, Pharm.D PGY-1 Resident Florida A & M University Classify and distinguish between different types
Objectives Strategies in Pain Management: Scheduled, Breakthrough, and Dose Adjustments Tamara M. Green, Pharm.D PGY-1 Resident Florida A & M University Classify and distinguish between different types
Knock Out Opioid Abuse in New Jersey:
 Knock Out Opioid Abuse in New Jersey: A Resource for Safer Prescribing GUIDELINE FOR PRESCRIBING OPIOIDS FOR CHRONIC PAIN IMPROVING PRACTICE THROUGH RECOMMENDATIONS CDC s Guideline for Prescribing Opioids
Knock Out Opioid Abuse in New Jersey: A Resource for Safer Prescribing GUIDELINE FOR PRESCRIBING OPIOIDS FOR CHRONIC PAIN IMPROVING PRACTICE THROUGH RECOMMENDATIONS CDC s Guideline for Prescribing Opioids
Opioid Pain Management. John Manfredonia, DO. Disclosures. Dr. Manfredonia discloses his employment as Regional Medical Director for VistaCare
 Opioid Pain Management John Manfredonia, DO Disclosures Dr. Manfredonia discloses his employment as Regional Medical Director for VistaCare VistaCare has provided commercial support for this activity Palliative
Opioid Pain Management John Manfredonia, DO Disclosures Dr. Manfredonia discloses his employment as Regional Medical Director for VistaCare VistaCare has provided commercial support for this activity Palliative
Session II. Learning Objectives for Session II. Key Principles of Safe Prescribing. Benefits and Limitations of ER/LA Opioids
 Learning Objectives for Session II Session II Best Practices for How to Start Therapy with ER/LA Opioids, How to Stop, and What to Do in Between Upon completion of this module, the participants will be
Learning Objectives for Session II Session II Best Practices for How to Start Therapy with ER/LA Opioids, How to Stop, and What to Do in Between Upon completion of this module, the participants will be
9/30/2017. Case Study: Complete Pain Assessment and Multimodal Approach to Pain Management. Program Objectives. Impact of Poorly Managed Pain
 Case Study: Complete Pain Assessment and Multimodal Approach to Pain Management MARY BETH PARTYKA MSN ADULT NURSE PRACTITIONER ADVOCATE CHRIST MEDICAL CENTER ADULT PAIN SERVICE Program Objectives Identify
Case Study: Complete Pain Assessment and Multimodal Approach to Pain Management MARY BETH PARTYKA MSN ADULT NURSE PRACTITIONER ADVOCATE CHRIST MEDICAL CENTER ADULT PAIN SERVICE Program Objectives Identify
Opioid Rotation. Dr Bruno Gagnon, M.D., M.Sc.
 Opioid Rotation Dr Bruno Gagnon, M.D., M.Sc. Associate Professor Department of Family Medicine and Emergency Medicine, Faculty of Medicine, Université Laval Consultant in Palliative Medicine CHU de Québec-Université
Opioid Rotation Dr Bruno Gagnon, M.D., M.Sc. Associate Professor Department of Family Medicine and Emergency Medicine, Faculty of Medicine, Université Laval Consultant in Palliative Medicine CHU de Québec-Université
Mitigating Risks While Optimizing the Benefits of Pharmacologic Agents to Manage Pain in the Elderly
 Mitigating Risks While Optimizing the Benefits of Pharmacologic Agents to Manage Pain in the Elderly Mary Lynn McPherson, PharmD, MDE, MA, BCPS, CPE Professor and Executive Director, Advanced Post-Graduate
Mitigating Risks While Optimizing the Benefits of Pharmacologic Agents to Manage Pain in the Elderly Mary Lynn McPherson, PharmD, MDE, MA, BCPS, CPE Professor and Executive Director, Advanced Post-Graduate
Pain Management and Safe use of opioids in hospitals. Kyoung-Sil Kang, PharmD, BCPS Scott Tam, PharmD Lauve Casimir, RN, MSN
 Pain Management and Safe use of opioids in hospitals Kyoung-Sil Kang, PharmD, BCPS Scott Tam, PharmD Lauve Casimir, RN, MSN Bronx Care Health System Bronx Lebanon Hospital Concourse/ Fulton division, Nursing
Pain Management and Safe use of opioids in hospitals Kyoung-Sil Kang, PharmD, BCPS Scott Tam, PharmD Lauve Casimir, RN, MSN Bronx Care Health System Bronx Lebanon Hospital Concourse/ Fulton division, Nursing
Opioid Analgesics. Recommended starting dose for opioid-naïve patients
 Opioid Analgesics Goals: Restrict use of opioid analgesics to OHP-funded conditions with documented sustained improvement in pain and function and with routine monitoring for opioid misuse and abuse. Promote
Opioid Analgesics Goals: Restrict use of opioid analgesics to OHP-funded conditions with documented sustained improvement in pain and function and with routine monitoring for opioid misuse and abuse. Promote
Pharmacologic Considerations for Managing Sickle Cell Pain Claire Saadeh, PharmD, BCOP May 5, 2015
 Pharmacologic Considerations for Managing Sickle Cell Pain Claire Saadeh, PharmD, BCOP May 5, 2015 Table 1: Physiologic changes that occur during sickle cell pain crisis 1-3 Phase Description / Complications
Pharmacologic Considerations for Managing Sickle Cell Pain Claire Saadeh, PharmD, BCOP May 5, 2015 Table 1: Physiologic changes that occur during sickle cell pain crisis 1-3 Phase Description / Complications
Managing Pain after Transplant Denice Economou, RN,MN,CHPN,AOCN
 Managing Pain after Transplant Denice Economou, RN,MN,CHPN,AOCN Oncology Clinical Nurse Specialist, Senior Research Specialist City of Hope Definition of Pain Pain is an unpleasant sensory and emotional
Managing Pain after Transplant Denice Economou, RN,MN,CHPN,AOCN Oncology Clinical Nurse Specialist, Senior Research Specialist City of Hope Definition of Pain Pain is an unpleasant sensory and emotional
Overcoming challenges in pain management in older patients. David Lussier, MD, FRCP(c) March 21, 2012
 March 21, 2012") Overcoming challenges in pain management in older patients David Lussier, MD, FRCP(c) March 21, 2012 Pain An unpleasant sensory and emotional experience associated with actual or potential tissue damage,
Overcoming challenges in pain management in older patients David Lussier, MD, FRCP(c) March 21, 2012 Pain An unpleasant sensory and emotional experience associated with actual or potential tissue damage,
Agenda. Case Discussions. Managing Acute & Chronic Pain (requiring opioid analgesics) in Patients on MAT. Daniel Alford, MD Disclosures
 in Patients on MAT. Daniel Alford, MD Disclosures") Managing Acute & Chronic Pain (requiring opioid analgesics) in Patients on MAT Case Discussions August 26, 2014 PCSS MAT Webinar Sponsored by the American Psychiatric Association Daniel P. Alford, MD,
Managing Acute & Chronic Pain (requiring opioid analgesics) in Patients on MAT Case Discussions August 26, 2014 PCSS MAT Webinar Sponsored by the American Psychiatric Association Daniel P. Alford, MD,
OAT Transitions - focus on microdosing. Mark McLean MD MSc FRCPC CISAM DABAM
 OAT Transitions - focus on microdosing Mark McLean MD MSc FRCPC CISAM DABAM Disclosures No pharmaceutical industry or other financial conflicts of interest Study Physician for research funded by Canadian
OAT Transitions - focus on microdosing Mark McLean MD MSc FRCPC CISAM DABAM Disclosures No pharmaceutical industry or other financial conflicts of interest Study Physician for research funded by Canadian
Narcotic Equivalence Converter Narcotic Route Dose Duration; Select a drug: mg Convert to: mg Adapted from Tarascon Pocket Pharmacopoeia.
 Narcotic Equivalence Converter Narcotic Route Dose Duration; Select a drug: mg Convert to: mg Adapted from Tarascon Pocket Pharmacopoeia. Created: Monday, March 12. Online calculator to convert equianalgesic
Narcotic Equivalence Converter Narcotic Route Dose Duration; Select a drug: mg Convert to: mg Adapted from Tarascon Pocket Pharmacopoeia. Created: Monday, March 12. Online calculator to convert equianalgesic
Disclosures. Management of Chronic, Non- Terminal Pain. Learning Objectives. Outline. Drug Schedules. Applicable State Laws
 Disclosures Management of Chronic, Non- Terminal Pain No financial disclosures or conflicts of interest to report Michael A. Smith, PharmD, BCPS Clinical Assistant Professor, University of Michigan College
Disclosures Management of Chronic, Non- Terminal Pain No financial disclosures or conflicts of interest to report Michael A. Smith, PharmD, BCPS Clinical Assistant Professor, University of Michigan College
Amber D. Hartman, PharmD Specialty Practice Pharmacist James Cancer Center & Solove Research Institute Ohio State University Medical Center
 Pharmacologic Management of Pain Amber D. Hartman, PharmD Specialty Practice Pharmacist James Cancer Center & Solove Research Institute Ohio State University Medical Center Objectives Identify types of
Pharmacologic Management of Pain Amber D. Hartman, PharmD Specialty Practice Pharmacist James Cancer Center & Solove Research Institute Ohio State University Medical Center Objectives Identify types of
OPIOID- INDUCED NEUROTOXICITY*
 OPIOID- INDUCED NEUROTOXICITY* Sriram Yennu MD, MS, FAAHPM Palliative Care, Rehabilitation and Integrative Medicine U.T. M.D. Anderson Cancer Center *Slide Deck courtesy Dept PRIM MDACC PATIENT #1: MRS
OPIOID- INDUCED NEUROTOXICITY* Sriram Yennu MD, MS, FAAHPM Palliative Care, Rehabilitation and Integrative Medicine U.T. M.D. Anderson Cancer Center *Slide Deck courtesy Dept PRIM MDACC PATIENT #1: MRS
Morphine er to oxycontin conversion
 Morphine er to oxycontin conversion The Borg System is 100 % Morphine er to oxycontin conversion 17-4-2011 Conversion dose from Oxycontin 40mg 3x a day to morphine sulfate 15 mg?. Oxycontin vs morphine
Morphine er to oxycontin conversion The Borg System is 100 % Morphine er to oxycontin conversion 17-4-2011 Conversion dose from Oxycontin 40mg 3x a day to morphine sulfate 15 mg?. Oxycontin vs morphine
Update on Pain: Collaborative Care for the Complex Patient
 Update on Pain: Collaborative Care for the Complex Patient Nirmala R. Abraham, MD Medical Director Sycamore Pain Management Center Kettering Health Network Objectives Standardized approach to patient care
Update on Pain: Collaborative Care for the Complex Patient Nirmala R. Abraham, MD Medical Director Sycamore Pain Management Center Kettering Health Network Objectives Standardized approach to patient care
Pain and the MGH Promise
 Pain is an unpleasant sensory & emotional experience associated with actual or potential tissue damage or described in terms of such damage Our promise to patients we will always: Work as a team to evaluate,
Pain is an unpleasant sensory & emotional experience associated with actual or potential tissue damage or described in terms of such damage Our promise to patients we will always: Work as a team to evaluate,
Pain Management in the Elderly. Martha Watson, MS, APRN, GCNS Christie Bowser, RN-BC, RN
 Pain Management in the Elderly Martha Watson, MS, APRN, GCNS Christie Bowser, RN-BC, RN Objectives So How Much Do You Really Know? www.geriatricpain.org Geriatric Pain Knowledge Assessment The Geriatric
Pain Management in the Elderly Martha Watson, MS, APRN, GCNS Christie Bowser, RN-BC, RN Objectives So How Much Do You Really Know? www.geriatricpain.org Geriatric Pain Knowledge Assessment The Geriatric
PAIN MANAGEMENT IN UROLOGY
 24 PAIN MANAGEMENT IN UROLOGY F. Francesca (chairman), P. Bader, D. Echtle, F. Giunta, J. Williams Eur Urol 2003; 44(4):383-389 Introduction Pain is defined as an unpleasant sensory and emotional experience
24 PAIN MANAGEMENT IN UROLOGY F. Francesca (chairman), P. Bader, D. Echtle, F. Giunta, J. Williams Eur Urol 2003; 44(4):383-389 Introduction Pain is defined as an unpleasant sensory and emotional experience
SCOPING DOCUMENT FOR WHO Treatment Guidelines on pain related to cancer, HIV and other progressive life-threatening illnesses in adults
 SCOPING DOCUMENT FOR WHO Treatment Guidelines on pain related to cancer, HIV and other progressive life-threatening illnesses in adults BACKGROUND The justification for developing these guidelines lies
SCOPING DOCUMENT FOR WHO Treatment Guidelines on pain related to cancer, HIV and other progressive life-threatening illnesses in adults BACKGROUND The justification for developing these guidelines lies
10 mg hydrocodone equals how much oxycodone
 Cari untuk: Cari Cari 10 mg hydrocodone equals how much oxycodone Posts about dilaudid 8 vs oxycodone 30 written by buyprescriptionmedication. Can you help me with the conversion of Oxycodone IR (5mg tab)
Cari untuk: Cari Cari 10 mg hydrocodone equals how much oxycodone Posts about dilaudid 8 vs oxycodone 30 written by buyprescriptionmedication. Can you help me with the conversion of Oxycodone IR (5mg tab)
Acute pain management in opioid tolerant patients. Muhammad Laklouk
 Acute pain management in opioid tolerant patients Muhammad Laklouk General principles An adequate review and assessment Provision of effective analgesia (including attenuation of tolerance and hyperalgesia)
Acute pain management in opioid tolerant patients Muhammad Laklouk General principles An adequate review and assessment Provision of effective analgesia (including attenuation of tolerance and hyperalgesia)
Blueprint for Prescriber Continuing Education Program
 CDER Final 10/25/11 Blueprint for Prescriber Continuing Education Program I. Introduction: Why Prescriber Education is Important Health care professionals who prescribe extended-release (ER) and long-acting
CDER Final 10/25/11 Blueprint for Prescriber Continuing Education Program I. Introduction: Why Prescriber Education is Important Health care professionals who prescribe extended-release (ER) and long-acting
Disclosures. Ms. Walsh has nothing to disclose Ms. Broglio is on the speaker s bureau for Genentech and Meda Pharmaceuticals
 Anne F. Walsh, MSN, ANP BC, ACHPN, CWOCN Kathleen Broglio, MN, ANP BC, ACHPN, CPE Disclosures Ms. Walsh has nothing to disclose Ms. Broglio is on the speaker s bureau for Genentech and Meda Pharmaceuticals
Anne F. Walsh, MSN, ANP BC, ACHPN, CWOCN Kathleen Broglio, MN, ANP BC, ACHPN, CPE Disclosures Ms. Walsh has nothing to disclose Ms. Broglio is on the speaker s bureau for Genentech and Meda Pharmaceuticals
Slide 1. Slide 2. Slide 3. Opioid (Narcotic) Analgesics and Antagonists. Lesson 6.1. Lesson 6.1. Opioid (Narcotic) Analgesics and Antagonists
 Analgesics and Antagonists. Lesson 6.1. Lesson 6.1. Opioid (Narcotic) Analgesics and Antagonists") Slide 1 Opioid (Narcotic) Analgesics and Antagonists Chapter 6 1 Slide 2 Lesson 6.1 Opioid (Narcotic) Analgesics and Antagonists 1. Explain the classification, mechanism of action, and pharmacokinetics
Slide 1 Opioid (Narcotic) Analgesics and Antagonists Chapter 6 1 Slide 2 Lesson 6.1 Opioid (Narcotic) Analgesics and Antagonists 1. Explain the classification, mechanism of action, and pharmacokinetics