ACP Aaron Fieker, D.O
|
|
|
- Della Ryan
- 5 years ago
- Views:
Transcription
1 ACP 2016 Aaron Fieker, D.O
2 Colorectal cancer (CRC) Update on screening strategies and tools Irritable Bowel Syndrome (IBS) New therapeutic options C-difficile Updates on treating recurrent disease
3 CRC Facts Third most common cancer diagnosis 5% lifetime risk 95,270 new cases of colon cancer in ,220 new cases of rectal cancer in 2016 Cancer.org JAMA 2016.
4 CRC Facts Second most common cause of cancer death 49,190 deaths related in 2016 Silver Lining: Death rate has dropped over past decade Improved screening Better treatment Cancer.org NEJM 2013
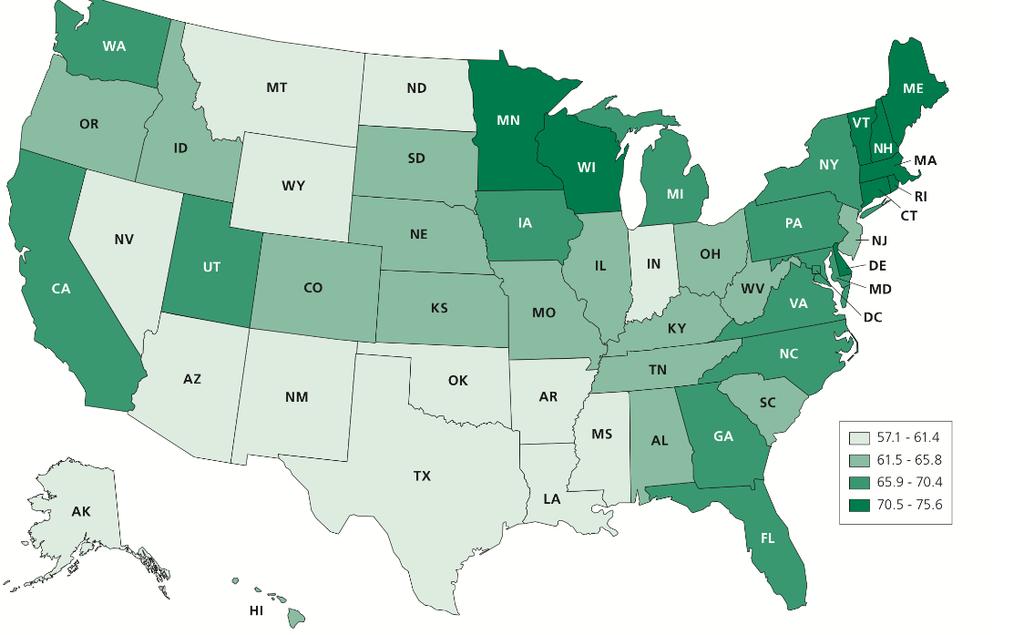
5 Screening Prevalence
6 Prospective cohort study 88,902 over 22 years Results: CRC Screening Endoscopy vs. No endoscopy Reduced incidence/mortality of distal and proximal cancers Large meta-analysis Significant reduction in incidence/mortality NEJM AJG 2016.
7 CRC Facts Risk Factors: Family history Age Gender Ethnicity IBD Diabetes Lifestyle Red meat Alcohol Processed meat Smoking Protective Physical activity Dairy consumption Fruit consumption Vegetable consumption High fiber - >10 grams/d
8 CRC Screening Screening options: Cancer prevention tests Colonoscopy and Sigmoidoscopy Cancer detection tests CT colonography Barium Enema FIT testing Cologuard Serum testing
9 CRC Screening Stool based tests: gfobt Up to 79% sensitivity reported Need 3 samples collected at home Easy and noninvasive FIT Improved sensitivity in some studies Less dietary/medication modifications Optimal number of samples not known CA Cancer J Clin 2008.
10 CRC Screening Stool DNA Cologuard Recently added to guidelines for screening Detects DNA biomarkers shed into stool KRAS mutations, aberrant NDRG4/BMP3 methylation Combines with FIT to detect blood Screening: annual (USPSTF), q3 years (manufacturer) Intended for average risk individuals
11 Stool DNA CRC Screening Compared to FIT (9989 participants) CRC - Sensitivity 92.3% (sdna) vs. 73.8% (FIT) Advanced adenoma 42.4 % vs. 23.8% High grade dysplasia and sessile serrated adenomas outperformed FIT More false positives compared to FIT Neg Predictive value 99.94% for Cancer 94.79% for advanced adenoma NEJM 2014.
12 CRC Screening Serum test SEPT9 assay Improved sensitivity in second generation assay Sensitivity/specificity for CRC 74.8%/87.4% This increases with stage Stage IV 100% Promising results for screening J Gastroenterology Hepatology 2015.
13 CRC Screening Goal: Get people screened Many options available Consider the discussion detection vs. prevention tests Screening does make a difference

14

15
16 IBS Common problem Reported to occur up to 28% of population Impact on quality of life Impact financially Days off work Use of health resources Gastro Ther Adv Gastro 2016.
17 IBS Abdominal pain with altered defecation Rome III: Abd pain/discomfort 3 days/month in last 3 months with 2 of following: Improvement with defecation Associated change in frequency of stooling Associated with change in form of stool
18 IBS New therapeutic options: Linaclotide (Linzess) Rifaximin (Xifaxan) Eluxadoline (Viberzi) FODMAP diet
19 IBS Linaclotide (Linzess) Activates guanylate cyclase C Activation of CFTR Bicarbonate and Chloride secretion Acceleration of colonic transit and fluid Inhibition of colonic nociceptors reduction in pain Minimally absorbed Main side effect was diarrhea Life Sci Gastro 2007.
20 IBS Linaclotide (Linzess) FDA approved IBS-C Chronic idiopathic constipation Dosing 290 mcg or 145 mcg daily Typically dosed 30min prior to first meal
21 IBS Linaclotide (Linzess) 3 RCT compared Linzess to Placebo All met ROME criteria All had constipation and at least 3/10 abd pain Linzess outperformed Placebo Less failure rates for pain and spontaneous BM Pain may take up to 12 weeks to respond Overall improved QL Higher rates of diarrhea Clin Gastro Hep AJG Gastro 2010.
22 IBS Rifaximin (Xifaxan) Evidence that microflora may play role in IBS Broad spectrum Minimal systemic absorption Targets the gut Low risk of bacterial resistance Well tolerated
23 IBS Rifaximin (Xifaxan) FDA approved: IBS-D Travelers diarrhea Hepatic encephalopathy Dose for IBS 550mg TID for 2 weeks Expensive
24 IBS Rifaximin (Xifaxan) TARGET 1 & 2 Trial Double blinded, placebo controlled ROME criteria for IBS without constipation Xifaxan 550mg TID for 2 weeks Followed for 10 weeks Symptom response was self reported Pimental NEJM 2011.

25 Percentage of Patients with Adequate Relief of Global IBS Symptoms in the TARGET 1 and TARGET 2 Studies Combined. Pimentel M et al. N Engl J Med 2011;364:22-32.
26 IBS Rifaximin (Xifaxan) Global relief 40% vs. 31% Bloating 35% vs. 28% Abd pain and stool consistency 44% vs. 36% Adverse events were similar *TARGET 3 Safe and effective to retreat with symptom recurrence Pimental NEJM Gastro 2015.
27 IBS Eluxadoline (Viberzi) FDA approved May 2015 Approved for IBS-D Dosing 75mg or 100mg BID 75 mg dose for cholecystectomy Abdominal pain reported
28 IBS Eluxadoline (Viberzi) Mu Opioid agonist Delta Opioid antagonist Improves diarrhea and abdominal pain
29 IBS Eluxadoline (Viberzi) Clinical response 13.8% vs. 5.7% Improved symptoms: Frequency Urgency Quality of life Adverse effects Abdominal pain Constipation Nausea Gastro Ther Adv Gastro 2016.
30 IBS Lifestyle Smoking cessation Regular physical activity Regular meals Improves symptoms Emotional improvement Improved sleep Ther Adv Gastro 2016.
31 IBS FODMAP diet Fermentable Oligosaccharides, Disaccharides, Monosaccharides And Polyols Poorly absorbed short chain carbohydrates Luminal distention b/c osmotic effects Rapid fermentation Gastro 2014.
32 IBS FODMAP diet Restricting FODMAPS Improved GI symptoms overall Improved bloating, pain, flatulence Improved stool consistence Long-term tolerability/adherence of concern Gastro Dig Dis Sci 2015.
33 Clostridium difficile Changing epidemiology NAP 1 strain Rising resistance Difficulty in treating recurrent disease
34 Rising incidence Epidemiology Incidence rates rose by 23% per year from s: cases per 100, : 84 per 100,000 Incidence nearly doubled in all age groups, predominantly effecting the elderly Increasing severity (mortality rate, longer hospital stays, complications, treatment failures) New at risk populations: Younger healthier populations Not previously exposed to Abx Not exposed to hospital or health care environment Young women in the peripartum period Janka, J. Clostridium Difficile: current perspectives. Current Opinion in Critical Care. 2009, April 15(2): Kelly, C. Clostridium difficile more difficult than ever. NEJM. 2008; 359:
35 Emerging strain NAP-1/027 Initially isolated in the 1984 This strain is being isolated more frequently Factors implicated in outbreaks: Increase production of Toxin A and B Deletion mutation of TcdC protein *A/B 16% and 23% higher Fluoroquinolone resistance **82% resistance in Quebec outbreak Production of binary toxin Thought to act synergistically with toxin A/B Janka, J. Clostridium Difficile: current perspectives. Current Opinion in Critical Care. 2009, April 15(2): *Warny, M et al. Toxin production by an emerging strain of Clostridium difficile associated with outbreaks of severe disease in North America and Europe. Lancet 2005; 366:1079. **Loo, V et al. A predominantly clonal multi-institutional outbreak of Clostridium difficile-associated diarrhea with high morbidity and mortality. NEJM 2005; 353:
36 Resistance Prior to 2000, failure rates for Vancomycin and Metronidazole were nearly identical (3.5% vs. 2.5%) Increasing resistance reported with Metronidazole Failure rates up to 26% Janka, J. Clostridium Difficile: current perspectives. Current Opinion in Critical Care. 2009, April 15(2): Kelly, C. Clostridium difficile more difficult than ever. NEJM. 2008; 359:
37 Recurrence Recurrence rates range from 15-30% Rates similar between vancomycin and metronidazole Relapse persistence of the same strain Symptoms occur about 14 days after treatment of initial infection Reinfection acquire a new strain Reportedly 33-75% of cases Symptoms usually occur around 40 days after treatment of previous infection Johnson, S. Recurrent Clostridium difficile infection: A review of risk factors, treatments, and outcomes. Journal of infection 2009 (58); Maroo, S et al. Recurrent Clostridium difficile. Gastro 2006 (103):
38 Recurrence Risk Factors: Previous episode 40% risk after 1 st recurrence to 60% after 2 or more recurrences Inadequate antitoxin antibody response Persistent disruption of colonic flora Advanced age - >65 Continued use of non-c. difficile antibiotics Long hospital stays Continued use of antacid medications *Increase severity of repeat episodes Johnson, S. Recurrent Clostridium difficile infection: A review of risk factors, treatments, and outcomes. Journal of infection 2009 (58); Kelly, C. Clostridium difficile more difficult than ever. NEJM. 2008; 359: *Pepin J, et al. Management and outcomes of a first recurrence of Clostridium difficile-associated disease in Quebec, Canada. Clin Infect Dis 2006;42:
39 Treatment First recurrence repeat treatment with same antibiotic If mild symptoms, can follow clinically without antibiotic therapy Second Recurrence A change is warranted 6 week Vancomycin pulse-tapered dosing Third or subsequent recurrence Vancomycin pulse-tapered dosing followed by additional strategies Consider FMT Leffler, D. Treatment of Clostridium difficile-associated Disease. Gastro 2009;136:
40
41 Treatment Additional Strategies EnteraGam serum-derived bovine immune globulin Considered a medical food product Requires prescription Used for diarrhea illnesses (HIV, IBS) Thought to bind c-diff toxin A/B Improves gut barrier function/permeability Petschow et al. Clin Exp Gastro. 2014
42 Treatment Investigational Agents: Human Monoclonal Antibodies (CDA1, CDB1) Prospective, randomized, double blind, placebo controlledtrial of 200 patients (Phase 2 trial) Both monoclonal antibodies infused together in individuals receiving vanomycin or metronidazole for symptomatic C-diff Primary outcome with recurrence Recurrence 7% Ab, 38% placebo *Bezlotoxumab Lowy, I et al. Treatment with Monoclonal Antibodies against Clostridium difficile toxins. NEJM. 2010; 360:
43 Treatment Investigational agents Various Vaccines currently under study ACAM-CDIFF phase I volunteer safety and immune response, phase II CDI, phase II CDI prevention Intercell IC84 phase I volunteer safety and immune response Clostridium difficile vaccine phase I volunteer safety and immune response
 produces disease Re-establish an equilibrium Brandt.")
44 Treatment Fecal Microbiota Transplantation (FMT) Installation of normal stool Methods: NGT EGD Colonoscopy Enema Rationale: imbalance of intestinal microbiota (dysbiosis) produces disease Re-establish an equilibrium Brandt. ACG.
45 Treatment FMT Early evidence in 4 th century China Oral suspension Food poisoning First reported in US 1958 Fecal enemas Severe pseudomembranous colitis Cumulative cure around 91%
46 FMT Treatment *Retrospective review of 18 pt. received stool transplant for recurrent C-diff 15/18 were disease free at 90 days ** Retrospective review of 12 patients who received stool transplant for recurrent c-diff 12/12 had durable clinical response Symptom free at 3-5 days Followed from 3 weeks to 8 years Leffler, D et al. Journal of infection 2009; 58: *Aas, J et al. Clin Infect Dis 2003;26: **Sonia, S et al. Journ Clinical Gastro. May 2010.
47 Treatment FMT Good initial and sustained response to FMT 91% at 3 months 86% at 6 months 80% at 18 months Most recurrence related to repeat abx use Effective in critically ill 17 patients with severe colitis considered for colectomy 88% response rate avoided colectomy 15/17 symptom free at 3 months ACG 2014
48 Treatment FMT RCT evaluated FMT nasoduodenal route 16 patients Stopped early 93% response with FMT 30% vancomycin alone 97% would repeat FMT 58% would choose FMT as primary trx No major AE reported Van Nood et al. NEJM Brandt et al. AJG 2012.
49 FMT Current practice Family donor Tested for various infections prior to donation Stool collected and mixed with saline Roughly 300mL slurry Instilled in TI, cecum, ascending, transverse, descending
50 Treatment FMT Pill form is likely next generation FMT Recent study in JAMA 20 patients with recurrent c-diff Cure rate was 90% No major adverse events Frozen specimens Universal donors JAMA. Oct 2014.
51 Conclusions CRC Screening is the goal IBS New therapeutics C-diff Changing landscape FMT
52 Questions?
Irritable Bowel Syndrome Now. George M. Logan, MD Friday, May 5, :35 4:05 PM
 Irritable Bowel Syndrome Now George M. Logan, MD Friday, May 5, 2017 3:35 4:05 PM Dr. Logan indicated no potential conflict of interest to this presentation. He does not intend to discuss any unapproved/investigative
Irritable Bowel Syndrome Now George M. Logan, MD Friday, May 5, 2017 3:35 4:05 PM Dr. Logan indicated no potential conflict of interest to this presentation. He does not intend to discuss any unapproved/investigative
ROME IV CRITERIA FOR IBS
 PRACTICAL CONSIDERATIONS IN THE MANAGEMENT OF IBS BRENDA HORWITZ MD PROFESSOR OF CLINICAL MEDICINE LEWIS KATZ SCHOOL OF MEDICINE AND TEMPLE UNIVERSITY HEALTH SCIENCES CENTER OR THINGS I ALWAYS WANTED TO
PRACTICAL CONSIDERATIONS IN THE MANAGEMENT OF IBS BRENDA HORWITZ MD PROFESSOR OF CLINICAL MEDICINE LEWIS KATZ SCHOOL OF MEDICINE AND TEMPLE UNIVERSITY HEALTH SCIENCES CENTER OR THINGS I ALWAYS WANTED TO
All POOPed out: fecal microbiota transplant in C. difficile
 All POOPed out: fecal microbiota transplant in C. difficile SUSAN M. KELLIE, MD, MPH PROFESSOR OF INTERNAL MEDICINE DIVISION OF INFECTIOUS DISEASES UNIVERSITY OF NEW MEXICO SCHOOL OF MEDICINE HOSPITAL
All POOPed out: fecal microbiota transplant in C. difficile SUSAN M. KELLIE, MD, MPH PROFESSOR OF INTERNAL MEDICINE DIVISION OF INFECTIOUS DISEASES UNIVERSITY OF NEW MEXICO SCHOOL OF MEDICINE HOSPITAL
Division of GIM Lecture Series Case Presentation David A. Erickson, M.D October 9th, 2013
 Division of GIM Lecture Series Case Presentation David A. Erickson, M.D October 9th, 2013 Financial Disclosures No financial disclosures Objectives Review a case of recurrent Clostridium difficile infection
Division of GIM Lecture Series Case Presentation David A. Erickson, M.D October 9th, 2013 Financial Disclosures No financial disclosures Objectives Review a case of recurrent Clostridium difficile infection
Primary Management of Irritable Bowel Syndrome
 Primary Management of Irritable Bowel Syndrome Jasmine Zia, MD Acting Instructor, Division of Gastroenterology Current Concepts in Drug Therapy CME Course April 23, 2015 Irritable Bowel Syndrome (IBS)
Primary Management of Irritable Bowel Syndrome Jasmine Zia, MD Acting Instructor, Division of Gastroenterology Current Concepts in Drug Therapy CME Course April 23, 2015 Irritable Bowel Syndrome (IBS)
Corporate Medical Policy Fecal Microbiota Transplantation
 Corporate Medical Policy Fecal Microbiota Transplantation File Name: Origination: Last CAP Review: Next CAP Review: Last Review: Fecal_microbiota_transplantation 7/2014 11/2017 11/2018 11/2017 Description
Corporate Medical Policy Fecal Microbiota Transplantation File Name: Origination: Last CAP Review: Next CAP Review: Last Review: Fecal_microbiota_transplantation 7/2014 11/2017 11/2018 11/2017 Description
Microbiome GI Disorders
 Microbiome GI Disorders Prof. Ram Dickman Neurogastroenterology Unit Rabin Medical Center Israel 1 Key Points Our gut microbiota Were to find them? Symbiosis or Why do we need them? Dysbiosis or when things
Microbiome GI Disorders Prof. Ram Dickman Neurogastroenterology Unit Rabin Medical Center Israel 1 Key Points Our gut microbiota Were to find them? Symbiosis or Why do we need them? Dysbiosis or when things
Update on Clostridium difficile infection.
 Update on Clostridium difficile infection. K. Honein Gastroenterologist, HDF Associate Professor Head of Medicine Department St Joseph University-Beirut. Introduction Gram+anaerobic bacillus responsible
Update on Clostridium difficile infection. K. Honein Gastroenterologist, HDF Associate Professor Head of Medicine Department St Joseph University-Beirut. Introduction Gram+anaerobic bacillus responsible
Treatment Update on Fecal Microbiota Transplantation. Arnab Ray, MD Ochsner Clinic Foundation Gastroenterology Department
 Treatment Update on Fecal Microbiota Transplantation Arnab Ray, MD Ochsner Clinic Foundation Gastroenterology Department Disclosure I serve as a paid medical monitor for Rebiotix Objectives The scope of
Treatment Update on Fecal Microbiota Transplantation Arnab Ray, MD Ochsner Clinic Foundation Gastroenterology Department Disclosure I serve as a paid medical monitor for Rebiotix Objectives The scope of
Xifaxan, Lotronex and Viberzi Prior Authorization and Quantity Limit Program Summary
 Xifaxan, Lotronex and Viberzi Prior Authorization and Quantity Limit Program Summary FDA APPROVED INDICATIONS DOSAGE 1,2 Lotronex (alosetron) a Indication For women with severe diarrheapredominant irritable
Xifaxan, Lotronex and Viberzi Prior Authorization and Quantity Limit Program Summary FDA APPROVED INDICATIONS DOSAGE 1,2 Lotronex (alosetron) a Indication For women with severe diarrheapredominant irritable
Fecal Microbiota Transplantation (FMT): Current Concepts in Clostridium difficile and beyond
: Current Concepts in Clostridium difficile and beyond") Fecal Microbiota Transplantation (FMT): Current Concepts in Clostridium difficile and beyond Amir Patel, MD Assistant Professor of Medicine Froedtert Hospital and the Medical College of Wisconsin I have
Fecal Microbiota Transplantation (FMT): Current Concepts in Clostridium difficile and beyond Amir Patel, MD Assistant Professor of Medicine Froedtert Hospital and the Medical College of Wisconsin I have
Fecal Microbiota Transplantation in C. diff. colitis Benefits and Limitations
 January 27th 2017, 8th Gastro Foundation Weekend for Fellows; Spier Hotel & Conference Centre, Stellenbosch Fecal Microbiota Transplantation in C. diff. colitis Benefits and Limitations Gerhard Rogler,
January 27th 2017, 8th Gastro Foundation Weekend for Fellows; Spier Hotel & Conference Centre, Stellenbosch Fecal Microbiota Transplantation in C. diff. colitis Benefits and Limitations Gerhard Rogler,
Clostridium difficile Infection (CDI) Management Guideline
 Management Guideline") Clostridium difficile Infection (CDI) Management Guideline Do not test all patients with loose or watery stools for CDI o CDI is responsible for
Clostridium difficile Infection (CDI) Management Guideline Do not test all patients with loose or watery stools for CDI o CDI is responsible for
C. difficile: When to Do Fecal Microbiota Transplant (FMT)
") C. difficile: When to Do Fecal Microbiota Transplant (FMT) Lawrence J. Brandt, MD, MACG Emeritus Chief, Gastroenterology Montefiore Medical Center Professor of Medicine and Surgery Albert Einstein College
C. difficile: When to Do Fecal Microbiota Transplant (FMT) Lawrence J. Brandt, MD, MACG Emeritus Chief, Gastroenterology Montefiore Medical Center Professor of Medicine and Surgery Albert Einstein College
Diagnosis and Management of Irritable Bowel Syndrome (IBS) For the Primary Care Provider
 For the Primary Care Provider") Diagnosis and Management of Irritable Bowel Syndrome (IBS) For the Primary Care Provider Elizabeth Coss, MD General Gastroenterologist Audie Murphy Veterans Hospital UT Health This presentation does not
Diagnosis and Management of Irritable Bowel Syndrome (IBS) For the Primary Care Provider Elizabeth Coss, MD General Gastroenterologist Audie Murphy Veterans Hospital UT Health This presentation does not
What s New for Clostridium difficile John Lynch MD MPH Harborview Medical Center University of Washington
 What s New for Clostridium difficile 2013 John Lynch MD MPH Harborview Medical Center University of Washington Pathogenic Mechanisms of Diarrhea Toxins: Preformed: S aureus, C perfringens, B cereus Formed
What s New for Clostridium difficile 2013 John Lynch MD MPH Harborview Medical Center University of Washington Pathogenic Mechanisms of Diarrhea Toxins: Preformed: S aureus, C perfringens, B cereus Formed
Spectrum of Diverticular Disease. Outline
 Spectrum of Disease ACG Postgraduate Course January 24, 2015 Lisa Strate, MD, MPH Associate Professor of Medicine University of Washington, Seattle, WA Outline Traditional theories and updated perspectives
Spectrum of Disease ACG Postgraduate Course January 24, 2015 Lisa Strate, MD, MPH Associate Professor of Medicine University of Washington, Seattle, WA Outline Traditional theories and updated perspectives
Stony Brook Adult Clostridium difficile Management Guidelines. Discontinue all unnecessary antibiotics
 Stony Brook Adult Clostridium difficile Management Guidelines Summary: Use of the C Diff Infection (CDI) PowerPlan (Adult) Required Patient with clinical findings suggestive of Clostridium difficile infection
Stony Brook Adult Clostridium difficile Management Guidelines Summary: Use of the C Diff Infection (CDI) PowerPlan (Adult) Required Patient with clinical findings suggestive of Clostridium difficile infection
Case 1. Which of the following would be next appropriate investigation/s regarding the pts diarrhoea?
 Case 1 21 yr old HIV +ve, Cd4-100 HAART naïve Profuse diarrhoea for 3/52. Stool MC&S ve Which of the following would be next appropriate investigation/s regarding the pts diarrhoea? Repeat stool MC&S Stool
Case 1 21 yr old HIV +ve, Cd4-100 HAART naïve Profuse diarrhoea for 3/52. Stool MC&S ve Which of the following would be next appropriate investigation/s regarding the pts diarrhoea? Repeat stool MC&S Stool
COLON CANCER SCREENING: AN UPDATE
 Overview COLON CANCER SCREENING: AN UPDATE Siddharth Verma, DO, JD Rutgers New Jersey Medical School Background Screening Updates in Specific Populations African Americans CRC in the younger age USPSTF
Overview COLON CANCER SCREENING: AN UPDATE Siddharth Verma, DO, JD Rutgers New Jersey Medical School Background Screening Updates in Specific Populations African Americans CRC in the younger age USPSTF
Title: Fecal microbiota transplantation in recurrent Clostridium difficile infection in a patient with concomitant inflammatory bowel disease
 Title: Fecal microbiota transplantation in recurrent Clostridium difficile infection in a patient with concomitant inflammatory bowel disease Authors: Marta Gravito-Soares, Elisa Gravito-Soares, Francisco
Title: Fecal microbiota transplantation in recurrent Clostridium difficile infection in a patient with concomitant inflammatory bowel disease Authors: Marta Gravito-Soares, Elisa Gravito-Soares, Francisco
Gut Microbiota Transplant Pro Position. Christina Surawicz, MD, MACG Professor of Medicine University of Washington Seattle WA
 Gut Microbiota Transplant Pro Position Christina Surawicz, MD, MACG Professor of Medicine University of Washington Seattle WA My Focus Recurrent Clostridium difficile infection No uniformly successful
Gut Microbiota Transplant Pro Position Christina Surawicz, MD, MACG Professor of Medicine University of Washington Seattle WA My Focus Recurrent Clostridium difficile infection No uniformly successful
When To Do Fecal Microbiota Transplant (FMT) For C. difficile
 For C. difficile") When To Do Fecal Microbiota Transplant (FMT) For C. difficile Lawrence J. Brandt, MD, MACG Emeritus Chief, Gastroenterology Montefiore Medical Center Professor of Medicine and Surgery Albert Einstein College
When To Do Fecal Microbiota Transplant (FMT) For C. difficile Lawrence J. Brandt, MD, MACG Emeritus Chief, Gastroenterology Montefiore Medical Center Professor of Medicine and Surgery Albert Einstein College
more intense treatments are needed to get rid of the infection.
 What Is Clostridium Difficile (C. Diff)? Clostridium difficile, or C. diff for short, is an infection from a bacterium that can grow in your intestines and cause bad GI symptoms. The main risk of getting
What Is Clostridium Difficile (C. Diff)? Clostridium difficile, or C. diff for short, is an infection from a bacterium that can grow in your intestines and cause bad GI symptoms. The main risk of getting
Patient presentation
 Update: Clostridium difficile Colitis David H. Kerman, MD Assistant Professor of Clinical Medicine Director, Fellowship Program Division of Gastroenterology University of Miami Miller School of Medicine
Update: Clostridium difficile Colitis David H. Kerman, MD Assistant Professor of Clinical Medicine Director, Fellowship Program Division of Gastroenterology University of Miami Miller School of Medicine
Fecal microbiota transplantation: The When,the How and the Don t. By Dr Rola Hussein
 Fecal microbiota transplantation: The When,the How and the Don t By Dr Rola Hussein Introduction Fecal microbiota transplantation (FMT) involves administration of fecal material containing distal gut microbiota
Fecal microbiota transplantation: The When,the How and the Don t By Dr Rola Hussein Introduction Fecal microbiota transplantation (FMT) involves administration of fecal material containing distal gut microbiota
ENGLISH FOR PROFESSIONAL PURPOSES UNIT 3 HOW TO DEAL WITH CLOSTRIDIUM DIFFICILE
 ENGLISH FOR PROFESSIONAL PURPOSES UNIT 3 HOW TO DEAL WITH CLOSTRIDIUM DIFFICILE The diagnosis of CDI should be based on a combination of clinical and laboratory findings. A case definition for the usual
ENGLISH FOR PROFESSIONAL PURPOSES UNIT 3 HOW TO DEAL WITH CLOSTRIDIUM DIFFICILE The diagnosis of CDI should be based on a combination of clinical and laboratory findings. A case definition for the usual
Clinical Review Criteria Fecal Microbial Transplant for Treatment of C. Difficile Infection Fecal GI Infusion Fecal Capsule (G3 OpenBiome)
") Clinical Review Criteria Fecal Microbial Transplant for Treatment of C. Difficile Infection Fecal GI Infusion Fecal Capsule (G3 OpenBiome) Criteria Codes Revision History Kaiser Foundation Health Plan
Clinical Review Criteria Fecal Microbial Transplant for Treatment of C. Difficile Infection Fecal GI Infusion Fecal Capsule (G3 OpenBiome) Criteria Codes Revision History Kaiser Foundation Health Plan
Fecal Microbiota Transplantation
 Protocol Fecal Microbiota Transplantation (20192) Medical Benefit Effective Date: 10/01/14 Next Review Date: 07/18 Preauthorization Yes Review Dates: 07/14, 07/15, 07/16, 07/17 Preauthorization is required.
Protocol Fecal Microbiota Transplantation (20192) Medical Benefit Effective Date: 10/01/14 Next Review Date: 07/18 Preauthorization Yes Review Dates: 07/14, 07/15, 07/16, 07/17 Preauthorization is required.
Star Articles in Review
 Star Articles in Review CDDW/CASL Meeting Toronto, February 10, 2014 Christina M. Surawicz, MD MACG Professor of Medicine Division of Gastroenterology Department of Medicine University of Washington Disclosure
Star Articles in Review CDDW/CASL Meeting Toronto, February 10, 2014 Christina M. Surawicz, MD MACG Professor of Medicine Division of Gastroenterology Department of Medicine University of Washington Disclosure
5 Things to Know About Irritable Bowel Syndrome
 5 Things to Know About Irritable Bowel Syndrome Mike Kolber MD, CCFP, MSc PEIP 2017 Faculty/Presenter Disclosure Presenter: Mike Kolber Relationships that may introduce potential bias and/or conflict of
5 Things to Know About Irritable Bowel Syndrome Mike Kolber MD, CCFP, MSc PEIP 2017 Faculty/Presenter Disclosure Presenter: Mike Kolber Relationships that may introduce potential bias and/or conflict of
A Trip Through the GI Tract: Common GI Diseases and Complaints. Jennifer Curtis, MD
 A Trip Through the GI Tract: Common GI Diseases and Complaints Jennifer Curtis, MD Colon Cancer How does it develop? Most cancers arise from polyps Over time these can turn into cancer Combination of genetic
A Trip Through the GI Tract: Common GI Diseases and Complaints Jennifer Curtis, MD Colon Cancer How does it develop? Most cancers arise from polyps Over time these can turn into cancer Combination of genetic
-2002: Rectal blood loss, UC? (no definite diagnosis) rectal mesalazine. -June 2008: Recurrence of rectal blood loss and urgency
 rectal mesalazine. -June 2008: Recurrence of rectal blood loss and urgency") SD, male 40 yrs. old. (680718M467.) -2002: Rectal blood loss, UC? (no definite diagnosis) rectal mesalazine -June 2008: Recurrence of rectal blood loss and urgency Total colonoscopy: ulcerative rectitis,
SD, male 40 yrs. old. (680718M467.) -2002: Rectal blood loss, UC? (no definite diagnosis) rectal mesalazine -June 2008: Recurrence of rectal blood loss and urgency Total colonoscopy: ulcerative rectitis,
Managing Clostridium Difficile: An Old Bug With
 932 The Red Section see related editorial on page x Managing Clostridium Difficile: An Old Bug With New Tricks Stephen M. Vindigni, MD, MPH 1,2 and Christina M. Surawicz, MD 1 Am J Gastroenterol (2018)
932 The Red Section see related editorial on page x Managing Clostridium Difficile: An Old Bug With New Tricks Stephen M. Vindigni, MD, MPH 1,2 and Christina M. Surawicz, MD 1 Am J Gastroenterol (2018)
Responders as percent of overall members in each category: Region: New England 50 (57% of 87 members) 46 (57% of 81 members) 21 (55% of 38 members)
 46 (57% of 81 members) 21 (55% of 38 members)") Infectious Diseases Society of America Emerging Infections Network Report for Query: Recurrent C. difficile Infections (CDI) Overall response rate: 621/1212 (51.2%) physicians responded from 09/26/12 to
Infectious Diseases Society of America Emerging Infections Network Report for Query: Recurrent C. difficile Infections (CDI) Overall response rate: 621/1212 (51.2%) physicians responded from 09/26/12 to
Faecal Microbiota Transplants: The evidence and experience
 Faecal Microbiota Transplants: The evidence and experience Dr Simon Goldenberg Consultant Microbiologist and Infection Control Doctor Guy s & St Thomas NHS Foundation Trust Gut microbiota and health Level
Faecal Microbiota Transplants: The evidence and experience Dr Simon Goldenberg Consultant Microbiologist and Infection Control Doctor Guy s & St Thomas NHS Foundation Trust Gut microbiota and health Level
Diagnosis, Management, and Prevention of Clostridium difficile infection in Long-Term Care Facilities: A Review
 Diagnosis, Management, and Prevention of Clostridium difficile infection in Long-Term Care Facilities: A Review October 18, 2010 James Kahn and Carolyn Kenney, MSIV Overview Burden of disease associated
Diagnosis, Management, and Prevention of Clostridium difficile infection in Long-Term Care Facilities: A Review October 18, 2010 James Kahn and Carolyn Kenney, MSIV Overview Burden of disease associated
Clostridium difficile: Can you smell the new updates?
 Clostridium difficile: Can you smell the new updates? Sunish Shah, Pharm.D. PGY-2 Infectious Disease Pharmacy Resident Yale-New Haven Hospital sshah1741@mail.usciences.edu Learning objectives Recognize
Clostridium difficile: Can you smell the new updates? Sunish Shah, Pharm.D. PGY-2 Infectious Disease Pharmacy Resident Yale-New Haven Hospital sshah1741@mail.usciences.edu Learning objectives Recognize
9/18/2018. Clostridium Difficile: Updates on Diagnosis and Treatment. Clostridium difficile Infection (CDI) Clostridium difficile Infection (CDI)
 Clostridium difficile Infection (CDI)") Clostridium Difficile: Updates on Diagnosis and Treatment Elizabeth Hudson, DO, MPH 9/25/18 Antibiotic-associated diarrhea and colitis were well established soon after widespread use of antibiotics In
Clostridium Difficile: Updates on Diagnosis and Treatment Elizabeth Hudson, DO, MPH 9/25/18 Antibiotic-associated diarrhea and colitis were well established soon after widespread use of antibiotics In
CLINICAL MEDICAL POLICY
 Policy Name: Policy Number: Responsible Department(s): CLINICAL MEDICAL POLICY Fecal Microbiota Transplant MP-066-MD-PA Medical Management Provider Notice Date: 10/15/2018; 01/15/2018 Issue Date: 11/15/2018;
Policy Name: Policy Number: Responsible Department(s): CLINICAL MEDICAL POLICY Fecal Microbiota Transplant MP-066-MD-PA Medical Management Provider Notice Date: 10/15/2018; 01/15/2018 Issue Date: 11/15/2018;
Clinical Policy Bulletin: Fecal Bacteriotherapy
 Clinical Policy Bulletin: Fecal Bacteriotherapy Number: 0844 Policy Aetna considers fecal bacteriotherapy medically necessary for persons with Clostridium difficile infection, with infection confirmed
Clinical Policy Bulletin: Fecal Bacteriotherapy Number: 0844 Policy Aetna considers fecal bacteriotherapy medically necessary for persons with Clostridium difficile infection, with infection confirmed
State of the Art: Management of Irritable Bowel Syndrome
 ACG/FGS Annual Spring Symposium March 16-18, 2018 Bonita Springs, FL State of the Art: Management of Irritable Bowel Syndrome William D. Chey, MD Professor of Medicine University of Michigan IBS: Rome
ACG/FGS Annual Spring Symposium March 16-18, 2018 Bonita Springs, FL State of the Art: Management of Irritable Bowel Syndrome William D. Chey, MD Professor of Medicine University of Michigan IBS: Rome
CLOSTRIDIUM DIFICILE. Negin N Blattman Infectious Diseases Phoenix VA Healthcare System
 CLOSTRIDIUM DIFICILE Negin N Blattman Infectious Diseases Phoenix VA Healthcare System ANTIBIOTIC ASSOCIATED DIARRHEA 1978: C diff first identified 1989-1992: Four large outbreaks in the US caused by J
CLOSTRIDIUM DIFICILE Negin N Blattman Infectious Diseases Phoenix VA Healthcare System ANTIBIOTIC ASSOCIATED DIARRHEA 1978: C diff first identified 1989-1992: Four large outbreaks in the US caused by J
Updates to pharmacological management in the prevention of recurrent Clostridium difficile
 Updates to pharmacological management in the prevention of recurrent Clostridium difficile Julia Shlensky, PharmD PGY2 Internal Medicine Resident September 12, 2017 2017 MFMER slide-1 Clinical Impact Increasing
Updates to pharmacological management in the prevention of recurrent Clostridium difficile Julia Shlensky, PharmD PGY2 Internal Medicine Resident September 12, 2017 2017 MFMER slide-1 Clinical Impact Increasing
ABSTRACT PURPOSE METHODS
 ABSTRACT PURPOSE The purpose of this study was to characterize the CDI population at this institution according to known risk factors and to examine the effect of appropriate evidence-based treatment selection
ABSTRACT PURPOSE The purpose of this study was to characterize the CDI population at this institution according to known risk factors and to examine the effect of appropriate evidence-based treatment selection
Xifaxan. Xifaxan (rifaximin) Description
 Description") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.01.34 Subject: Xifaxan Page: 1 of 6 Last Review Date: December 8, 2017 Xifaxan Description Xifaxan (rifaximin)
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.01.34 Subject: Xifaxan Page: 1 of 6 Last Review Date: December 8, 2017 Xifaxan Description Xifaxan (rifaximin)
Fecal Microbiota Transplantation. Description
 Section: Medicine Effective Date: April 15, 2017 Original Policy Date: September 12, 2014 Subject: Fecal Microbiota Transplantation Page: 1 of 10 Last Review Status/Date: March 2017 Fecal Microbiota Transplantation
Section: Medicine Effective Date: April 15, 2017 Original Policy Date: September 12, 2014 Subject: Fecal Microbiota Transplantation Page: 1 of 10 Last Review Status/Date: March 2017 Fecal Microbiota Transplantation
Irritable Bowel Syndrome. Mustafa Giaffer March 2017
 Irritable Bowel Syndrome Mustafa Giaffer March 2017 Introduction First described in 1771. 50% of patients present
Irritable Bowel Syndrome Mustafa Giaffer March 2017 Introduction First described in 1771. 50% of patients present
Is FMT the answer? Challenging Cases in CDI. Ted Steiner, M.D. April 1, 2016
 Is FMT the answer? Challenging Cases in CDI Ted Steiner, M.D. April 1, 2016 CONFLICT OF INTEREST DISCLOSURE SLIDE In the past 2 years I have been an employee of: In the past 2 years I have been a consultant
Is FMT the answer? Challenging Cases in CDI Ted Steiner, M.D. April 1, 2016 CONFLICT OF INTEREST DISCLOSURE SLIDE In the past 2 years I have been an employee of: In the past 2 years I have been a consultant
Fecal transplantation as a treatment option for recurrent Clostridium difficile infection
 Fecal transplantation as a treatment option for recurrent Clostridium difficile infection Josbert Keller Department of Gastroenterology Haga Teaching Hospital, The Hague Case: 81 yrs, CVA, recurrent UTI,
Fecal transplantation as a treatment option for recurrent Clostridium difficile infection Josbert Keller Department of Gastroenterology Haga Teaching Hospital, The Hague Case: 81 yrs, CVA, recurrent UTI,
Slide #43. Functional Disorders - An Update 11/8/ MA ACP Annual Scientific Meeting. Functional Disorders: An Update
 Functional Disorders: An Update Anthony Lembo, M.D. Associate Professor of Medicine Beth Israel Deaconess Medical Center Harvard Medical School Boston, MA Disclosure of Financial Relationships Anthony
Functional Disorders: An Update Anthony Lembo, M.D. Associate Professor of Medicine Beth Israel Deaconess Medical Center Harvard Medical School Boston, MA Disclosure of Financial Relationships Anthony
CLINICAL MEDICAL POLICY
 Policy Name: Policy Number: Responsible Department(s): CLINICAL MEDICAL POLICY Fecal Microbiota Transplant MP-066-MD-DE Medical Management Provider Notice Date: 10/15/2018; 04/15/2018 Issue Date: 11/15/2018;
Policy Name: Policy Number: Responsible Department(s): CLINICAL MEDICAL POLICY Fecal Microbiota Transplant MP-066-MD-DE Medical Management Provider Notice Date: 10/15/2018; 04/15/2018 Issue Date: 11/15/2018;
Colorectal Cancer Screening. Dr Kishor Muniyappa 2626 Care Drive, Suite 101 Tallahassee, FL Ph:
 Colorectal Cancer Screening Dr Kishor Muniyappa 2626 Care Drive, Suite 101 Tallahassee, FL 32308 Ph: 850-297-0351 What we ll be talking about How common is colorectal cancer? What is colorectal cancer?
Colorectal Cancer Screening Dr Kishor Muniyappa 2626 Care Drive, Suite 101 Tallahassee, FL 32308 Ph: 850-297-0351 What we ll be talking about How common is colorectal cancer? What is colorectal cancer?
Clostridium Difficile Infection: Applying New Treatment Guidelines and Strategies to Reduce Recurrence Rate
 Clostridium Difficile Infection: Applying New Treatment Guidelines and Strategies to Reduce Recurrence Rate Objectives Summarize the changing epidemiology and demographics of patients at risk for Clostridium
Clostridium Difficile Infection: Applying New Treatment Guidelines and Strategies to Reduce Recurrence Rate Objectives Summarize the changing epidemiology and demographics of patients at risk for Clostridium
Clostridium Difficile colitismore
 Clostridium Difficile colitismore virulent than ever ECHO- February 18, 2016 Charles Krasner, M.D. UNR School of Medicine Sierra NV Veterans Affairs Hospital Growing problem of pseudomembranous colitis
Clostridium Difficile colitismore virulent than ever ECHO- February 18, 2016 Charles Krasner, M.D. UNR School of Medicine Sierra NV Veterans Affairs Hospital Growing problem of pseudomembranous colitis
IBS: Updates on Diagnostics and Therapeutics for the Primary Practitioner
 Rome IV: Diagnostic Criteria* IBS: Updates on Diagnostics and Therapeutics for the Primary Practitioner Darren M. Brenner, MD, AGAF Associate Professor of Medicine and Surgery Director Northwestern Functional
Rome IV: Diagnostic Criteria* IBS: Updates on Diagnostics and Therapeutics for the Primary Practitioner Darren M. Brenner, MD, AGAF Associate Professor of Medicine and Surgery Director Northwestern Functional
What is Irritable Bowel Syndrome (IBS)?
?") What is Irritable Bowel Syndrome (IBS)? Irritable bowel syndrome (IBS) is a health issue found in your intestines (gut). IBS can cause symptoms such as: Belly pain. Cramping. Gas. Bloating (or swelling)
What is Irritable Bowel Syndrome (IBS)? Irritable bowel syndrome (IBS) is a health issue found in your intestines (gut). IBS can cause symptoms such as: Belly pain. Cramping. Gas. Bloating (or swelling)
Long-Term Care Updates
 Long-Term Care Updates April 2018 By Austin Smith, PharmD Candidate and Lindsay Slowiczek, PharmD is the most common healthcare-acquired infection (HAI) in the United States. 1,2 A 2014 prevalence survey
Long-Term Care Updates April 2018 By Austin Smith, PharmD Candidate and Lindsay Slowiczek, PharmD is the most common healthcare-acquired infection (HAI) in the United States. 1,2 A 2014 prevalence survey
Management of Clostridium Difficile: Total Colectomy versus Colon Sparing Surgery
 Management of Clostridium Difficile: Total Colectomy versus Colon Sparing Surgery Rahul Narang, MD Colon and Rectal Surgery Assistant Professor of Surgery No Disclosure Clostridium Difficile Colitis: Treatments,
Management of Clostridium Difficile: Total Colectomy versus Colon Sparing Surgery Rahul Narang, MD Colon and Rectal Surgery Assistant Professor of Surgery No Disclosure Clostridium Difficile Colitis: Treatments,
 Disorders in which symptoms cannot be explained by the presence of structural or tissue abnormalities Irritable bowel syndrome Functional heartburn Functional dyspepsia Functional constipation Functional
Disorders in which symptoms cannot be explained by the presence of structural or tissue abnormalities Irritable bowel syndrome Functional heartburn Functional dyspepsia Functional constipation Functional
! MQ is a 44 year old woman that I first saw in Sept ! In MVA in Jan 2003 requiring spinal surgery
 Case MQ is a 44 year old woman that I first saw in Sept 2006 UPDATE ON CLOSTRIDIUM DIFFICILE DISEASE Richard A. Jacobs, M.D.,PhD In MVA in Jan 2003 requiring spinal surgery Subsequently developed fecal
Case MQ is a 44 year old woman that I first saw in Sept 2006 UPDATE ON CLOSTRIDIUM DIFFICILE DISEASE Richard A. Jacobs, M.D.,PhD In MVA in Jan 2003 requiring spinal surgery Subsequently developed fecal
Colorectal Cancer: Preventable, Beatable, Treatable. American Cancer Society
 Colorectal Cancer: Preventable, Beatable, Treatable American Cancer Society Reviewed/Revised May 2018 What we ll be talking about How common is colorectal cancer? What is colorectal cancer? What causes
Colorectal Cancer: Preventable, Beatable, Treatable American Cancer Society Reviewed/Revised May 2018 What we ll be talking about How common is colorectal cancer? What is colorectal cancer? What causes
(No Image Selected) Video Submission Confirmation: No Video Upload: Abstract Author: Investigator Commercial Products or Services: No Designed Study:
 Video Submission Confirmation: No Video Upload: Abstract Author: Investigator Commercial Products or Services: No Designed Study:") Found 3 Abstracts CONTROL ID: 1745628 TITLE: Fecal Microbiota Transplantation (FMT) for Treatment of Clostridium difficile Infection (CDI) in Immunocompromised Patients CONTACT (NAME ONLY): Colleen Kelly
Found 3 Abstracts CONTROL ID: 1745628 TITLE: Fecal Microbiota Transplantation (FMT) for Treatment of Clostridium difficile Infection (CDI) in Immunocompromised Patients CONTACT (NAME ONLY): Colleen Kelly
Irritable bowel syndrome (IBS) is a chronic, potentially disabling
 is a chronic, potentially disabling") Evidence-Based Management of Irritable Bowel Syndrome With Diarrhea Mark Pimentel, MD Irritable bowel syndrome (IBS) is a chronic, potentially disabling disorder of the gastrointestinal (GI) tract with
Evidence-Based Management of Irritable Bowel Syndrome With Diarrhea Mark Pimentel, MD Irritable bowel syndrome (IBS) is a chronic, potentially disabling disorder of the gastrointestinal (GI) tract with
William Chey, MD University of Michigan Ann Arbor, MI
 Lin Chang, MD David Geffen School of Medicine at UCLA Los Angeles, CA William Chey, MD University of Michigan Ann Arbor, MI Mark Pimentel, MD Cedars-Sinai Medical Center Los Angeles, CA Accredited by Jointly
Lin Chang, MD David Geffen School of Medicine at UCLA Los Angeles, CA William Chey, MD University of Michigan Ann Arbor, MI Mark Pimentel, MD Cedars-Sinai Medical Center Los Angeles, CA Accredited by Jointly
IBS-D: What to Do When Typical Treatment Methods Fail
 Transcript Details This is a transcript of a continuing medical education (CME) activity accessible on the ReachMD network. Additional media formats for the activity and full activity details (including
Transcript Details This is a transcript of a continuing medical education (CME) activity accessible on the ReachMD network. Additional media formats for the activity and full activity details (including
New Tests and Treatments for Dyspepsia and Irritable Bowel Syndrome
 New Tests and Treatments for Dyspepsia and Irritable Bowel Syndrome Soojong Hong Chae, MD Clinical Assistant Professor Digestive Diseases and Nutrition University of South Florida ROME III Functional dyspepsia
New Tests and Treatments for Dyspepsia and Irritable Bowel Syndrome Soojong Hong Chae, MD Clinical Assistant Professor Digestive Diseases and Nutrition University of South Florida ROME III Functional dyspepsia
Updated Clostridium difficile Treatment Guidelines
 Updated Clostridium difficile Treatment Guidelines Arielle Arnold, PharmD, BCPS Clinical Pharmacist Saint Alphonsus Regional Medical Center September 29 th, 2018 Disclosures Nothing to disclose Learning
Updated Clostridium difficile Treatment Guidelines Arielle Arnold, PharmD, BCPS Clinical Pharmacist Saint Alphonsus Regional Medical Center September 29 th, 2018 Disclosures Nothing to disclose Learning
EDUCATIONAL COMMENTARY CLOSTRIDIUM DIFFICILE UPDATE
 EDUCATIONAL COMMENTARY CLOSTRIDIUM DIFFICILE UPDATE Educational commentary is provided through our affiliation with the American Society for Clinical Pathology (ASCP). To obtain FREE CME/CMLE credits click
EDUCATIONAL COMMENTARY CLOSTRIDIUM DIFFICILE UPDATE Educational commentary is provided through our affiliation with the American Society for Clinical Pathology (ASCP). To obtain FREE CME/CMLE credits click
The New Grade A: USPSTF Updated Colorectal Cancer Screening Guidelines, What does it all mean?
 The New Grade A: USPSTF Updated Colorectal Cancer Screening Guidelines, What does it all mean? Robert A. Smith, PhD Cancer Control, Department of Prevention and Early Detection American Cancer Society
The New Grade A: USPSTF Updated Colorectal Cancer Screening Guidelines, What does it all mean? Robert A. Smith, PhD Cancer Control, Department of Prevention and Early Detection American Cancer Society
Pennington Feb 19, 2015
 Trust your gut Pennington Feb 19, 2015 Crohn s Disease -an autoimmune disorder that causes inflammation of the intestinal tract along with unpredictable, often incapacitating episodes of abdominal pain
Trust your gut Pennington Feb 19, 2015 Crohn s Disease -an autoimmune disorder that causes inflammation of the intestinal tract along with unpredictable, often incapacitating episodes of abdominal pain
Virtual Lectures Planning Committee Disclosure Summary
 Mayo Medical Laboratories Virtual Lectures 2014 MFMER Virtual Lectures Planning Committee Disclosure Summary As a provider accredited by ACCME, College of Medicine, Mayo Clinic (Mayo School of CPD) must
Mayo Medical Laboratories Virtual Lectures 2014 MFMER Virtual Lectures Planning Committee Disclosure Summary As a provider accredited by ACCME, College of Medicine, Mayo Clinic (Mayo School of CPD) must
! Macrolide antibacterial. Fidaxomicin (Dificid ) package labeling. Optimer Pharmaceuticals, Inc. May 2011.
 package labeling. Optimer Pharmaceuticals, Inc. May 2011.") Disclosure! I have no conflicts of interest related to this presentation Nina Naeger Murphy, Pharm.D., BCPS Clinical Pharmacy Specialist Infectious Diseases MetroHealth Medical Center Learning Objectives!
Disclosure! I have no conflicts of interest related to this presentation Nina Naeger Murphy, Pharm.D., BCPS Clinical Pharmacy Specialist Infectious Diseases MetroHealth Medical Center Learning Objectives!
Colorectal Cancer Screening. Paul Berg MD
 Colorectal Cancer Screening Paul Berg MD What is clinical integration? AMA Definition The means to facilitate the coordination of patient care across conditions, providers, settings, and time in order
Colorectal Cancer Screening Paul Berg MD What is clinical integration? AMA Definition The means to facilitate the coordination of patient care across conditions, providers, settings, and time in order
Advancing gastroenterology, improving patient care
 American College of Gastroenterology Advancing gastroenterology, improving patient care Note to Visitors: A fully updated ACG Systematic Review on the Management of Chronic Idiopathic Constipation and
American College of Gastroenterology Advancing gastroenterology, improving patient care Note to Visitors: A fully updated ACG Systematic Review on the Management of Chronic Idiopathic Constipation and
Updates in Fecal Microbial Transplant
 Updates in Fecal Microbial Transplant Dina Kao, MD FRCPC Associate Professor, Gastroenterology University of Alberta Nikhil Pai, MD FAAP FRCPC Assistant Professor, Ped Gastroenterology McMaster University
Updates in Fecal Microbial Transplant Dina Kao, MD FRCPC Associate Professor, Gastroenterology University of Alberta Nikhil Pai, MD FAAP FRCPC Assistant Professor, Ped Gastroenterology McMaster University
Clinically proven to quickly relieve symptoms of common gastrointestinal disorders. TERRAGASTRO - Good health starts in the gut
 Clinically proven to quickly relieve symptoms of common gastrointestinal disorders GASTROINTESTINAL DISEASE Referred to as gastrointestinal diseases, they are common disorders which affect the esophagus,
Clinically proven to quickly relieve symptoms of common gastrointestinal disorders GASTROINTESTINAL DISEASE Referred to as gastrointestinal diseases, they are common disorders which affect the esophagus,
IBS - Definition. Chronic functional disorder of GI generally characterized by:
 IBS - Definition Chronic functional disorder of GI generally characterized by: 3500 3000 No. of Publications 2500 2000 1500 1000 Irritable Bowel syndrome Irritable Bowel Syndrome 500 0 1968-1977 1978-1987
IBS - Definition Chronic functional disorder of GI generally characterized by: 3500 3000 No. of Publications 2500 2000 1500 1000 Irritable Bowel syndrome Irritable Bowel Syndrome 500 0 1968-1977 1978-1987
The Epidemiology of Clostridium difficile DANIEL SAMAN, DRPH, MPH RESEARCH SCIENTIST ESSENTIA INSTITUTE OF RURAL HEALTH
 The Epidemiology of Clostridium difficile DANIEL SAMAN, DRPH, MPH RESEARCH SCIENTIST ESSENTIA INSTITUTE OF RURAL HEALTH Some history first Clostridium difficile, a spore-forming gram-positive (i.e., thick
The Epidemiology of Clostridium difficile DANIEL SAMAN, DRPH, MPH RESEARCH SCIENTIST ESSENTIA INSTITUTE OF RURAL HEALTH Some history first Clostridium difficile, a spore-forming gram-positive (i.e., thick
Long-Term Care Updates
 Long-Term Care Updates April 2017 Bezlotoxumab to Prevent Recurrent Infection By Amy Wilson, PharmD and Zara Risoldi Cochrane, PharmD, MS, FASCP Introduction The Gram-positive bacteria is a common cause
Long-Term Care Updates April 2017 Bezlotoxumab to Prevent Recurrent Infection By Amy Wilson, PharmD and Zara Risoldi Cochrane, PharmD, MS, FASCP Introduction The Gram-positive bacteria is a common cause
Common Gastrointestinal Problems in the Elderly
 Common Gastrointestinal Problems in the Elderly Brian Viviano, D.O. Objectives Understand the pathophysiology, clinical manifestations, diagnosis and management of GI diseases of the elderly. Differentiate
Common Gastrointestinal Problems in the Elderly Brian Viviano, D.O. Objectives Understand the pathophysiology, clinical manifestations, diagnosis and management of GI diseases of the elderly. Differentiate
Fecal microbiota transplantation: Breaking the chain of recurrent C. difficile infection
 Fecal microbiota transplantation: Breaking the chain of recurrent C. difficile infection Issue Date: June 2013 Vol. 8 No. 6 Author: Amy Marinski, MSN, RN, CCRN, CNL More than 3 million new cases of Clostridium
Fecal microbiota transplantation: Breaking the chain of recurrent C. difficile infection Issue Date: June 2013 Vol. 8 No. 6 Author: Amy Marinski, MSN, RN, CCRN, CNL More than 3 million new cases of Clostridium
The long-term impact of the low-fodmap diet for management of irritable bowel syndrome. Dr Miranda Lomer RD.
 The long-term impact of the low-fodmap diet for management of irritable bowel syndrome Dr Miranda Lomer RD Email: miranda.lomer@kcl.ac.uk What is IBS - ROME IV Criteria A functional bowel disorder in which
The long-term impact of the low-fodmap diet for management of irritable bowel syndrome Dr Miranda Lomer RD Email: miranda.lomer@kcl.ac.uk What is IBS - ROME IV Criteria A functional bowel disorder in which
Patient Safety Summit 2014
 Patient Safety Summit 2014 The War on C Diff Mark Mellow, MD + C Diff The Organism Gram + bacillus Anaerobic Spore forming Intestinal flora (up to 35% hospitalized patients, 3% of healthy adults) Leading
Patient Safety Summit 2014 The War on C Diff Mark Mellow, MD + C Diff The Organism Gram + bacillus Anaerobic Spore forming Intestinal flora (up to 35% hospitalized patients, 3% of healthy adults) Leading
Food Choices and Alternative Techniques in Management of IBS: Fad Versus Evidence
 Food Choices and Alternative Techniques in Management of IBS: Fad Versus Evidence Maria Vazquez Roque, MD, MSc Assistant Professor Gastroenterology and Hepatology 2010 MFMER slide-1 Objectives Gluten-free
Food Choices and Alternative Techniques in Management of IBS: Fad Versus Evidence Maria Vazquez Roque, MD, MSc Assistant Professor Gastroenterology and Hepatology 2010 MFMER slide-1 Objectives Gluten-free
Colorectal Cancer Awareness: Wiping Out This Disease. Cedrek L. McFadden, MD, FACS, FASCRS
 Colorectal Cancer Awareness: Wiping Out This Disease Cedrek L. McFadden, MD, FACS, FASCRS Colorectal Cancer: Statistics ~135,000 estimated new cases 2016 ~50,000 estimated deaths in 2016 (2 nd leading
Colorectal Cancer Awareness: Wiping Out This Disease Cedrek L. McFadden, MD, FACS, FASCRS Colorectal Cancer: Statistics ~135,000 estimated new cases 2016 ~50,000 estimated deaths in 2016 (2 nd leading
Pharmacotherapy for IBS
 Pharmacotherapy for IBS Brooks D. Cash, M.D., FACG Chief, Gastroenterology Professor of Medicine University of South Alabama Director, GI Physiology, USA Medical Center Mobile, AL Disclosures I have served
Pharmacotherapy for IBS Brooks D. Cash, M.D., FACG Chief, Gastroenterology Professor of Medicine University of South Alabama Director, GI Physiology, USA Medical Center Mobile, AL Disclosures I have served
OCTOBER 7-10 PHILADELPHIA, PENNSYLVANIA
 OMED 17 OCTOBER 7-10 PHILADELPHIA, PENNSYLVANIA 29.5 Category 1-A CME credits anticipated ACOFP / AOA s 122 nd Annual Osteopathic Medical Conference & Exposition Joint Session with ACOFP and Cleveland
OMED 17 OCTOBER 7-10 PHILADELPHIA, PENNSYLVANIA 29.5 Category 1-A CME credits anticipated ACOFP / AOA s 122 nd Annual Osteopathic Medical Conference & Exposition Joint Session with ACOFP and Cleveland
Fecal Microbiota Transplantation
 Fecal Microbiota Transplantation Policy Number: 2.01.92 Last Review: 7/2018 Origination: 5/2015 Next Review: 7/2019 Policy Blue Cross and Blue Shield of Kansas City (Blue KC) will provide coverage for
Fecal Microbiota Transplantation Policy Number: 2.01.92 Last Review: 7/2018 Origination: 5/2015 Next Review: 7/2019 Policy Blue Cross and Blue Shield of Kansas City (Blue KC) will provide coverage for
Understanding & Alleviating Constipation. Living (Well!) with Gastroparesis Program Warm-Up Class
 with Gastroparesis Program Warm-Up Class") Understanding & Alleviating Constipation Living (Well!) with Gastroparesis Program Warm-Up Class Please Remember The information presented is for educational purposes only and is in no way intended as
Understanding & Alleviating Constipation Living (Well!) with Gastroparesis Program Warm-Up Class Please Remember The information presented is for educational purposes only and is in no way intended as
Presenter. Irritable Bowel Syndrome. Objectives. Introduction. Rome Criteria. Irritable Bowel Syndrome 2/28/2018
 Presenter Irritable Bowel Syndrome Current evidence for diagnosis & management Julie Daniels DNP, CNM Assistant Professor Course Coordinator of Primary Care of Women Faculty at Frontier Nursing University
Presenter Irritable Bowel Syndrome Current evidence for diagnosis & management Julie Daniels DNP, CNM Assistant Professor Course Coordinator of Primary Care of Women Faculty at Frontier Nursing University
declara&ons Clostridium difficile infec&on. Time to wake up and smell the..., um, nevermind. OK, next slide please. Bruce Dalton, BScPhm. PharmD.
 Clostridium difficile infec&on. Time to wake up and smell the..., um, nevermind. OK, next slide please. Bruce Dalton, BScPhm. PharmD. declara&ons No financial disclosures Personal acquaintance, co- worker,
Clostridium difficile infec&on. Time to wake up and smell the..., um, nevermind. OK, next slide please. Bruce Dalton, BScPhm. PharmD. declara&ons No financial disclosures Personal acquaintance, co- worker,
What s the Latest? Rome III Criteria for IBS
 Irritable Bowel lsyndrome: What s the Latest? American College of Gastroenterology Las Vegas, January 2014 Bi Brian E. Lacy, Ph.D., PhD M.D., MD FACG Professor of Medicine Geisel School of Medicine at
Irritable Bowel lsyndrome: What s the Latest? American College of Gastroenterology Las Vegas, January 2014 Bi Brian E. Lacy, Ph.D., PhD M.D., MD FACG Professor of Medicine Geisel School of Medicine at
William D. Chey, MD Professor of Medicine University of Michigan
 Evidence-based Treatment Strategies for IBS William D. Chey, MD Professor of Medicine University of Michigan Rome III criteria for IBS Recurrent abdominal pain or discomfort at least 3 days / month in
Evidence-based Treatment Strategies for IBS William D. Chey, MD Professor of Medicine University of Michigan Rome III criteria for IBS Recurrent abdominal pain or discomfort at least 3 days / month in
Bezlotoxumab (Zinplava) as Adjunct Treatment for Clostridium difficile. Janel Liane Cala, RPh Medical Center Hospital
 as Adjunct Treatment for Clostridium difficile. Janel Liane Cala, RPh Medical Center Hospital") Bezlotoxumab (Zinplava) as Adjunct Treatment for Clostridium difficile Janel Liane Cala, RPh Medical Center Hospital Objectives Review pathophysiology, risk factors, prevention, and treatment options of
Bezlotoxumab (Zinplava) as Adjunct Treatment for Clostridium difficile Janel Liane Cala, RPh Medical Center Hospital Objectives Review pathophysiology, risk factors, prevention, and treatment options of
IBS-D: The Role of Pathophysiology in Assessment and Treatment ReachMD Page 1 of 7
 Transcript Details This is a transcript of a continuing medical education (CME) activity accessible on the ReachMD network. Additional media formats for the activity and full activity details (including
Transcript Details This is a transcript of a continuing medical education (CME) activity accessible on the ReachMD network. Additional media formats for the activity and full activity details (including
FECAL TRANSPLANTATION
 FECAL TRANSPLANTATION From Theory to Practice in Ridge Meadows Edward Auersperg 13 January 2016 The Human Genome How many different chromosomes do humans have? 46 chromosomes 23 pairs The Human Genome
FECAL TRANSPLANTATION From Theory to Practice in Ridge Meadows Edward Auersperg 13 January 2016 The Human Genome How many different chromosomes do humans have? 46 chromosomes 23 pairs The Human Genome
Rome III Criteria for IBS. Irritable Bowel Syndrome: What s the Latest? IBS: What s the Latest? Distinguishing IBS-C from CC
 Rome III Criteria for IBS Irritable Bowel Syndrome: What s the Latest? Tim Burke, DO Pacific Digestive Associates Clackamas, OR Recurrent abdominal pain or discomfort at least 3 days/month in the last
Rome III Criteria for IBS Irritable Bowel Syndrome: What s the Latest? Tim Burke, DO Pacific Digestive Associates Clackamas, OR Recurrent abdominal pain or discomfort at least 3 days/month in the last
Colorectal Cancer Screening: Cost-Effectiveness and Adverse events October, 2005
 Colorectal Cancer Screening: Cost-Effectiveness and Adverse events October, 2005 David Lieberman MD Chief, Division of Gastroenterology Oregon Health and Science University Portland VAMC Portland, Oregon
Colorectal Cancer Screening: Cost-Effectiveness and Adverse events October, 2005 David Lieberman MD Chief, Division of Gastroenterology Oregon Health and Science University Portland VAMC Portland, Oregon
Clostridium difficile Infection: Diagnosis and Management
 Clostridium difficile Infection: Diagnosis and Management Brian Viviano D.O. Case study 42 year old female with history of essential hypertension and COPD presents to ED complaining of 24 hours of intractable,
Clostridium difficile Infection: Diagnosis and Management Brian Viviano D.O. Case study 42 year old female with history of essential hypertension and COPD presents to ED complaining of 24 hours of intractable,