Guidelines for Diagnosis and Treatment of IPF
|
|
|
- Norman Eaton
- 5 years ago
- Views:
Transcription


1 Guidelines for Diagnosis and Treatment of IPF Katerina Antoniou, MD, PhD Lecturer in Thoracic Medicine ERS ILD Group Secretary Medical School, University of Crete
2 Classification of Interstitial Lung Disease Known Causes Drugs Collagen Vascular Exposures Genetic IIPs: Idiopathic Interstitial Pneumonias Granulomatous Lung Diseases Sarcoidosis Fungal Mycobacterial Unique Entities PAP EG and EP LAM Capillaritis IPF: Idiopathic Pulmonary Fibrosis Clinical history Physiology 55% 25% <2% NSIP: Nonspecific Interstitial Pneumonia AIP: Acute Interstitial Pneumonia RB-ILD: Respiratory Bronchiolitis Interstitial Lung Disease DIP: Desquamative Interstitial Pneumonia % Radiography Pathology 5% COP: Cryptogenic Organizing Pneumonia LIP: Lymphocytic Interstitial Pneumonia <1% American Thoracic Society/European Respiratory Society. Am J Respir Crit Care Med 2002;165:
3
4 Survival for UIP vs NSIP / Others NSIP Alive (%) Alive (%) Others NSIP 2 0 UIP 2 0 UIP Years Years Daniil ZD, et al. Am J Respir Crit Care Med. 1999;160: Bjoraker JA, et al. Am J Respir Crit Care Med.1998;157:
5 Idiopathic Pulmonary Fibrosis Evidence Based Guidelines for Diagnosis and Management Clinical presentation Older age (6 th 7 th decades of life) Men > women Unexplained chronic exertional dyspnea, crackles, finger clubbing Incidence and prevalence Idiopathic Pulmonary Fibrosis No large-scale studies to base formal estimates Incidence = /100,000 Prevalence = /100,00
6 Clinical findings in IPF Age: 66 yr (40-70), two- thirds > 60 yr Dyspnea on exertion > 6 mo 95% Cough 90% Fine crackles 90% Clubbing 60-70% Weight loss, malaise, fatigue 30-50% Fever rare
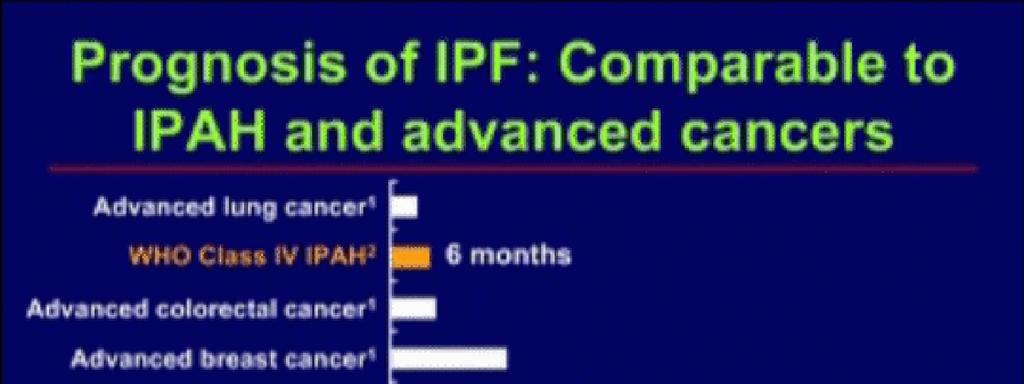
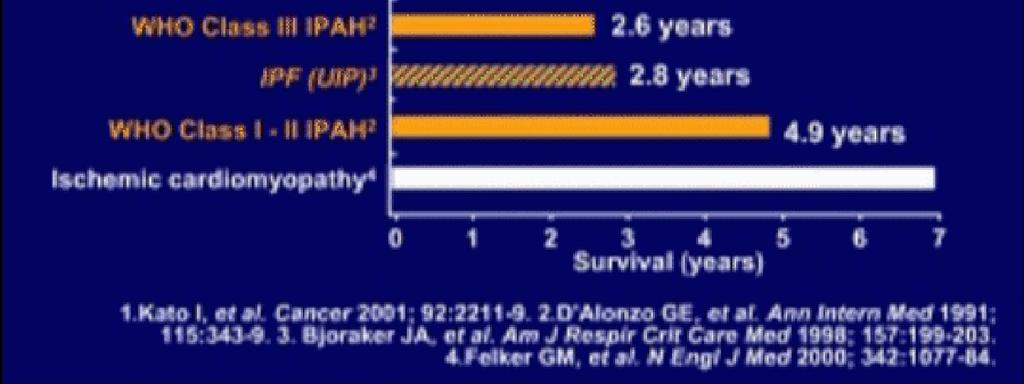
7 SINCE 1175 Am J Respir Crit Care Med 2000; 161:

8 Idiopathic pulmonary fibrosis (IPF) Specific form of chronic fibrosing interstitial pneumonia limited to the lung, associated with UIP on lung biopsy. International Consensus Statement, AJRCCM 2000
9 IPF diagnosis in the absence of SLB All four major criteria: 1. exclude all known causes 2. appropriate lung function 3. imaging 4. BAL or TBB excluding other diseases 3/4 minor criteria: 1. age >50 yr 2. slow onset 3. disease duration at least 3 months 4. crackles on auscultation peripheral/basal honeycombing little/no ground-glass International Consensus Statement, AJRCCM 2000


10 Am J Respir Crit Care Med 2011; 183:


11 BMJ 2004; 328: 1-8 Am J Respir Crit Care Med 2006; 174:



12 ORGANIZATIONS THAT HAVE ENDORSED GRADE
13 GRADING THE EVIDENCE For each question, the committee graded the quality of the evidence available (high, moderate, low, or very low), and made a recommendation for or against. Recommendations were decided based on majority vote. Recommendations were either strong or weak. Open and explicit vote of each member on each recommendation (reported in the document)
14 GRADING the evidence Quality of Evidence Study Design - Lower if: - Higher if: High Randomized controlled trial Study quality -1 Serious limitation -2 Very serious limitation Moderate Low Downgraded randomized controlled trial or upgraded observational study Well done observational study with control groups -1 Important inconsistency Directness -1 Some uncertainty -2 Major uncertainty -1 Sparse or imprecise data -1 High probability of reporting bias +1 Strong association, no plausible confounders +2 Very strong association, no major threats to validity +1 Evidence of a dose response gradient +1 All plausible confounders would have reduced the effect Very low Any other evidence (e.g. case reports, case series) ATS/ERS/JRS/ALAT IPF GUIDELINES Schünemann H et al. AJRCCM 2006 SINCE 1175
15 PROVIDING RECOMMENDATIONS Strong recommendation Patients: most people in this situation would want the recommended course of action and only a small proportion would not. Clinicians: most patients should receive the recommended course of action. Policy makers: the recommendation can be adopted as a policy in most situations. Weak recommendation Patients: the majority of people in this situation would want the recommended course of action, but many would not. Clinicians: be more prepared to help patients to make a decision that is consistent with the patient s own values. Policy makers: there is a need for substantial debate and involvement of stakeholders. Schünemann AJRCCM 2006
16 RECOMMENDATIONS The strength of the recommendations is either strong or weak based on the quality of evidence and the voting of the committee members. Thus the recommendations are either: 1) STRONG -YES, 2)STRONG -NO, 3) WEAK- YES, or 4) WEAK- NO.

17 The diagnosis of IPF requires: a)exclusion of other known causes of interstitial lung disease b)the presence of a UIP pattern on HRCT in patients not subjected to surgical lung biopsy c)specific combinations of HRCT and surgical lung biopsy pattern in patients subjected to surgical lung biopsy The major and minor criteria proposed in the 2000 ATS/ERS Consensus Statement have been eliminated Am J Respir Crit Care Med 2011; 183:
18 IPF diagnosis in the absence of SLB All four major criteria: 1. exclude all known causes 2. appropriate lung function 3. imaging 4. BAL or TBB excluding other diseases 3/4 minor criteria: 1. age >50 yr 2. slow onset 3. disease duration at least 3 months 4. crackles on auscultation International Consensus Statement, AJRCCM 2000
19 HRCT CRITERIA FOR UIP PATTERN UIP (all four features) Subpleural, basal predominance Reticular abnormality Honeycombing with or without traction bronchiectasis Absence of features listed as inconsistent with UIP pattern (see third column ) Possible UIP (all three features) Subpleural, basal predominance Reticular abnormality Absence of features listed as inconsistent with UIP pattern (see third column) Inconsistent with UIP (any of the seven features ) Upper or mid lung predominance Peribronchovascular predominance Extensive ground glass abnormality (extent > reticular abnormality) Profuse micronodules (bilateral, predominantly upper lobes) Discrete cysts (multiple, bilateral, away from areas of honeycombing) Diffuse mosaic attenuation / airtrapping (bilateral, in 3 or more lobes) Consolidation in bronchopulmonary segment(s)/lobe(s) Am J Respir Crit Care Med 2011; 183:
20 HRCT UIP PATTERN DEFINITE UIP DEFINITE UIP POSSIBLE UIP Am J Respir Crit Care Med 2011; 183:
21 Idiopathic Pulmonary Fibrosis Evidence Based Guidelines for Diagnosis and Management* HRCT Images: UIP Pattern (Extensive honeycombing) A B
22 Idiopathic Pulmonary Fibrosis Evidence Based Guidelines for Diagnosis and Management* HRCT Images: UIP Pattern (Less severe honeycombing) C D
23 Idiopathic Pulmonary Fibrosis Evidence Based Guidelines for Diagnosis and Management* HRCT Images: UIP Pattern (Extensive honeycombing) A B C D HRCT Images: UIP Pattern (Less severe honeycombing) Honeycombing (HRCT) Clustered cystic air spaces Well defined walls Typically comparable diameters (3-10 mm; occasionally as large as 2.5 cm) Sub pleural
24 Idiopathic Pulmonary Fibrosis Evidence Based Guidelines for Diagnosis and Management* HRCT Images: Possible with UIP pattern (no honeycombing) E F
25 Idiopathic Pulmonary Fibrosis Evidence Based Guidelines for Diagnosis and Management* HRCT Images: UIP Pattern (Extensive honeycombing) HRCT Images: UIP Pattern (Less severe honeycombing) HRCT Images: Possible with UIP pattern A C E B D F
26 HISTOPATHOLOGICAL CRITERIA FOR UIP PATTERN UIP (all four criteria) Probable UIP Possible UIP (all three criteria) Not UIP (any of the six criteria) Evidence of marked fibrosis/architectural distortion, +/- honeycombing in a predominantly subpleural/paraseptal distribution Presence of patchy involvement of lung parenchyma by fibrosis Presence of fibroblast foci Absence of features against a diagnosis of UIP suggesting an alternate diagnosis (see fourth column) Evidence of marked fibrosis/architectural distortion, +/- honeycombing in a subpleural/paraseptal distribution Absence of either patchy involvement or fibroblastic foci, but not both Absence of features against a diagnosis of UIP suggesting an alternate diagnosis (see fourth column) OR Honeycomb changes only Patchy or diffuse involvement of lung parenchyma by fibrosis, with or without interstitial inflammation Absence of other criteria for UIP (see UIP pattern column) Absence of features against a diagnosis of UIP suggesting an alternate diagnosis (see fourth column) Hyaline membranes Organizing pneumonia Granulomas Marked interstitial inflammatory cell infiltrate away from honeycombing Predominant airway centered changes Other features suggestive of an alternate diagnosis Am J Respir Crit Care Med 2011; 183:
27 HISTOPATHOLOGICAL CRITERIA FOR UIP PATTERN PRESERVED LUNG HONEYCOMB Am J Respir Crit Care Med 2011; 183:



28 HISTOPATHOLOGICAL CRITERIA FOR UIP PATTERN CHRONIC FIBROSIS FIBROBLAST FOCUS * Am J Respir Crit Care Med 2011; 183:


29 Idiopathic Pulmonary Fibrosis Evidence Based Guidelines for Diagnosis and Management* Surgical Lung Biopsy Specimens: Histopathology of UIP Pattern Preserved lung tissue Honeycomb spaces Chronic fibrosis * Fibroblast focus
30 Diagnosis Is bronchoalveolar lavage required for the diagnosis of IPF? Can transbronchial lung biopsy accurately identify UIP? Are autoimmune serologies required for the diagnosis of IPF? Is a multidisciplinary approach important to the accurate diagnosis of IPF? ATS/ERS/JRS/ALAT IPF GUIDELINES
31 Exclusion of other known causes Careful history (including family history), physical examination focusing on co-morbidities, medication use, environmental exposures No validated tools. The questionnaire available through the ACCP may be of use It is of particular importance to evaluate patients thoroughly for possible chronic HP ATS/ERS/JRS/ALAT IPF GUIDELINES
32 Should BAL cellular analysis be performed in the diagnostic evaluation of suspected IPF? In the evaluation of patients with suspected IPF, the most important application of BAL is in the exclusion of chronic HP; prominent lymphocytosis (>40%) should suggest the diagnosis. Recommendation: BAL cellular analysis should not be performed in the diagnostic evaluation of IPF in the majority of patients, but may be appropriate in a minority (weak recommendation; low quality evidence). Values: high value on the additional risk and cost and a low value on possible improved specificity of diagnosis. Remarks: this recommendation is only for BAL differential cell count ( cellular analysis ). It does not refer to the use of BAL in the evaluation of infection, malignancy, etc. ATS/ERS/JRS/ALAT IPF GUIDELINES
33 Should transbronchial lung biopsy be used in the evaluation of suspected IPF? Transbronchial lung biopsy is useful in the evaluation of selected conditions (e.g. sarcoidosis). A UIP pattern on HRCT makes these conditions unlikely Recommendation: Transbronchial biopsy should not be used in the evaluation of IPF in the majority of patients, but may be appropriate in a minority (weak recommendation; low quality evidence). Values: high value on the additional morbidity in patients with IPF who will subsequently undergo SLB and low value on possible diagnostic specificity. ATS/ERS/JRS/ALAT IPF GUIDELINES


34 Lung biopsy to diagnose IPF: size does matter TBBx VATS Bx 1X Magnification Slide courtesy Tom Colby

35 Potential TBBx sites UIP as seen on trichrome stained section Slide courtesy Tom Colby
36 Should serological testing for CTD be used in the evaluation of suspected IPF? CTD can present with a UIP pattern. ILD can be the sole clinical manifestation of these conditions ILD can precede the overt manifestation of a specific CTD. Recommendation: Serological testing for CTD should be performed in the evaluation of IPF in the majority of patients, but may not be appropriate in a minority (weak recommendation; very low quality evidence). Values: High value on distinguishing CTD from IPF and low value on cost. Remarks: Serological evaluation should be performed even in the absence of signs or symptoms of CTD and should include RF, anti-ccp, and ANA titer and pattern. The routine use of other serological tests such as antisynthetase antibodies (e.g. Jo-1), creatine kinase and aldolase, Sjogren s antibodies (SS-A, SS-B), and scleroderma antibodies (scl-70, PM-1) is of unclear benefit, but may be helpful in selected cases. ATS/ERS/JRS/ALAT IPF GUIDELINES
37 Should a MDD be used in the evaluation of suspected IPF? Proper communication between the various disciplines involved in the diagnosis of IPF improves inter-observer agreement among experienced clinical experts as to the ultimate diagnosis Recommendation: A MD approach should be used the evaluation of IPF (strong recommendation; low quality evidence). Values: High value on the accurate diagnosis of IPF and low value on the access to and availability of experts for MDD. Remarks: The accuracy of diagnosis improves through MDD. Timely referral to ILD experts is encouraged ATS/ERS/JRS/ALAT IPF GUIDELINES
38 Gold standard for IPF diagnosis The accuracy of the diagnosis of IPF increases with MDD between pulmonologists, radiologists, and pathologists experienced in the diagnosis of ILD MDD should include discussions of the potential for sampling error. In cases with an inconsistent UIP HRCT pattern and UIP pattern clearly present on SLB, the possibility of a diagnosis of IPF still exists and clarification by MDD among ILD experts is indicated. ATS/ERS/JRS/ALAT IPF GUIDELINES
39 HRCT/SLB pairings HRCT pattern SLB pattern (when performed) Diagnosis of IPF? UIP UIP Probable UIP Possible UIP Non-classifiable fibrosis YES Possible UIP Not UIP UIP Probable UIP Possible UIP Non-classifiable fibrosis NO YES Probable* Inconsistent with UIP Not UIP UIP Probable UIP Possible UIP Non-classifiable fibrosis Not UIP NO Possible* NO
40 Diagnostic algorithm for IPF Suspected IPF Identifiable cause for ILD? (CTD, drugs, exposures,...) NO Chest HRCT YES Not UIP UIP Possible UIP Inconsistent with UIP IPF Surgical lung biopsy MDD IPF / Not IPF UIP Possible UIP / Probable UIP Non classifiable fibrosis Not UIP Not IPF
41 NATURAL HISTORY OF IPF STABLE DISEASE PROGRESSION ACUTE WORSENING SLOW PROGRESSION RAPID PROGRESSION TIME Am J Respir Crit Care Med 2011; 183: (modified)

42 Am J Respir Crit Care Med 2000; 161:
43 RECOMMENDATIONS A strong recommendation implies that most patients would want the recommended course of action. A weak positive recommendation implies that the majority of patients would want the intervention, but many would not. Specifically, a weak negative recommendation implies that the majority of patients would not want the intervention, but many would. Therapies with a weak recommendation against their use may still be appropriate in selected patients.

44 Raghu G. Eur Respir J 2011; 37: 743-6
45 FOR AGAINST STRENGTH STRONG WEAK STRONG WEAK Evidence Prednisone alone Prednisone combined NAC+AZA+Prednisone NAC alone Interferon-gamma Anticoagulants Bosentan Pirfenidone Etanercept Cyclosporine A Colchicine L/VL M/H L/VL M/H L/VL M/H L/VL M/H Am J Respir Crit Care Med 2011; 183:
46 FOR AGAINST ABSTAIN ABSENT AGAINST FOR STRENGTH STRONG WEAK STRONG WEAK Evidence L/VL M/H L/VL M/H L/VL M/H L/VL M/H Prednisone alone NAC+AZA+Prednisone Prednisone combined NAC alone Interferon-gamma Anticoagulants Bosentan Pirfenidone Cyclosporine A Etanercept Colchicine Am J Respir Crit Care Med 2011; 183:
47 Recommendations for the treatment of IPF Treatment Data quality Recommendation Strength NAC alone Low No (5y/15n/3a) Weak P/AZA/NAC Low No (3y/17n/3a) Weak pirfenidone Low-Moderate No (4y/10n/17a) Weak* anticoagulation Very low No (1y/20n/2a/8A) Weak P/AZA Low No (21n/2a/8a) Strong Bosentan Low No (10n/13a/8A) Strong P/CYCLO Very low No (21n/2a/8a) Strong Colchicine Very low No (21n/2a/8A) Strong Corticosteroid Very low No (21n/2a/8A) Strong Cyclosporin A Very low No (18n/4a/9A) Strong Etanercept Low No (18n/4a/9A) Strong Interferon-γ-1a High No (17n/6a/8A) Strong y=yes, n=no, a= ABSTAIN-COI, A=ABSENT
48 NON-PHARMACOLOGICAL THERAPIES MODALITY DATA QUALITY RECOMENDATION STRENGTH LTOT VERY LOW YES (18y/4a/9A) STRONG REHABILITATION LOW YES (19y/3a/9A) WEAK MV AE-IPF LOW NO (2y/19n/2a/8A) WEAK LUNG TRANSPL HIGH YES (21y/1a/9A) STRONG y=yes, n=no,a= ABSTAIN, A=ABSENT
49 TREATMENT OF SELECTED COMPLICATIONS AND COMORBID CONDITIONS Should pulmonary hypertension be treated in patients with IPF? Should asymptomatic gastroesophageal reflux disease be medically treated in patients with IPF? Should patients with acute exacerbation of IPF be treated with corticosteroids?
50 TREATMENT OF SELECTED COMPLICATIONS AND COMORBID CONDITIONS MODALITY DATA QUALITY RECOMENDATION STRENGTH PH-IPF VERY LOW NO (8y/14n/1a) WEAK GE REFLUX VERY LOW YES (14y/8n/8A) WEAK CORTICOIDS AE/IPF VERY LOW YES (14y/5n/1a/11A) WEAK y=yes, n=no, a= ABSTAIN, A=ABSENT
51 FOR AGAINST STRENGTH STRONG WEAK STRONG WEAK Evidence Long term oxygen Lung transplant Mechanical ventilation Rehabilitation Treatment of PH Steroids in AE Asymptomatic GER L/VL M/H L/VL M/H L/VL M/H L/VL M/H Am J Respir Crit Care Med 2011; 183:


52 EVIDENCE-BASED TREATMENT RECOMMENDATIONS Therapies without a recommendation (newer data published subsequent to final formal face-to-face discussion): imatinib, sildenafil, BIBF 1120 Raghu G. Eur Respir J 2011; 37: 743-6

53 In a randomized, placebo-controlled trial of patients with mild to moderate IPF followed for 96 weeks, imatinib did not affect survival or lung function. Am J Respir Crit Care Med 2010; 181:
54 This study did not show a benefit for sildenafil for the primary outcome. The presence of some positive secondary outcomes creates clinical equipoise for further research. N Engl J Med 2010; 363: 620-8

55 In patients with idiopathic pulmonary fibrosis, BIBF 1120 at a dose of 150 mg twice daily, as compared with placebo, was associated with a trend toward a reduction in the decline in lung function, with fewer acute exacerbations and preserved quality of life. N Engl J Med 2011; 365:
56 FUTURE DIRECTIONS-I Additional high-quality, prospective, controlled, clinical trials of new therapies for IPF are required. Successful treatment of IPF will require a combination of therapies targeting multiple pathways involved in fibroproliferation.
57 FUTURE DIRECTIONS-II Future clinical trials should incorporate endpoints of proven clinical value, utilize sophisticated study design and statistical methodology, investigate the impact of potential preventive measures (e.g. treatment of gastroesophageal reflux), and consider combinations of promising therapies that work through distinct mechanisms.
58 FUTURE DIRECTIONS-III Genetic studies and preventive and regenerative strategies, including stem cell transplant-research and gene therapy, hold promise and should be aggressively pursued.
59 Meta-analysis of pirfenidone treatment effect Event driven analysis of either 10% decline in FVC or all cause mortality (Progression Free Survival) Based in part on unpublished data Spagnolo P, Del Giovane C, Luppi F, et al. Cochrane Database Syst Rev 2010;9:CD


60 Eur Respir J 2010; 35: PFN048.EU 60



61 N Engl J Med J 2009; 361: Lancet 2009; 374: J Clin Oncol 2009; 27: PFN048.EU 61
62 Conclusions Little quality evidence supports the efficacy of conventional immunosuppressive therapy for IPF Pirfenidone: The first EMEA drug for IPF. Several compounds are in phase 3 clinical trials (BIBF) Participation in trials should be discussed as an option for all patients Comorbidities associated with IPF, such as cough, GERD, pulmonary hypertension, and sleep apnea should be treated.
63 Conclusions Nonpharmacologic therapies are important Pulmonary rehabilitation Support groups Recognition and treatment of depression CPAP Oxygen End-of-life planning Patients should be referred early for transplant because of unpredictability of disease progression (eg, acute exacerbations).
64 CONCLUSIONS Based on the evidence published to date, there is no proven pharmacological therapy for IPF. Continued, concerted efforts should be made by physicians, patients, and sponsors to pursue well-designed clinical trials aimed at improving outcomes, including quality of life, in patients with IPF. Am J Respir Crit Care Med 2011; 183:
NONE OVERVIEW FINANCIAL DISCLOSURES UPDATE ON IDIOPATHIC PULMONARY FIBROSIS/IPF (UIP) FOR PATHOLOGISTS. IPF = Idiopathic UIP Radiologic UIP Path UIP
 FOR PATHOLOGISTS. IPF = Idiopathic UIP Radiologic UIP Path UIP") UPDATE ON IDIOPATHIC PULMONARY FIBROSIS/IPF () FOR PATHOLOGISTS Thomas V. Colby, M.D. Professor of Pathology (Emeritus) Mayo Clinic Arizona FINANCIAL DISCLOSURES NONE OVERVIEW IPF Radiologic Dx Pathologic
UPDATE ON IDIOPATHIC PULMONARY FIBROSIS/IPF () FOR PATHOLOGISTS Thomas V. Colby, M.D. Professor of Pathology (Emeritus) Mayo Clinic Arizona FINANCIAL DISCLOSURES NONE OVERVIEW IPF Radiologic Dx Pathologic
Case Presentations in ILD. Harold R. Collard, MD Department of Medicine University of California San Francisco
 Case Presentations in ILD Harold R. Collard, MD Department of Medicine University of California San Francisco Outline Overview of diagnosis in ILD Definition/Classification High-resolution CT scan Multidisciplinary
Case Presentations in ILD Harold R. Collard, MD Department of Medicine University of California San Francisco Outline Overview of diagnosis in ILD Definition/Classification High-resolution CT scan Multidisciplinary
IPF: Epidemiologia e stato dell arte
 IPF: Epidemiologia e stato dell arte Clinical Classification Diffuse parenchimal lung diseases Exposure-related: - occupational - environmental - medication Desquamative interstitial pneumonia Idiopathic
IPF: Epidemiologia e stato dell arte Clinical Classification Diffuse parenchimal lung diseases Exposure-related: - occupational - environmental - medication Desquamative interstitial pneumonia Idiopathic
Diagnostic challenges in IPF
 Medicine, Nursing and Health Sciences Diagnostic challenges in IPF Dr Ian Glaspole Central and Eastern Clinical School, Alfred Hospital and Monash University March 2015 Disclosures Consultancy fees from
Medicine, Nursing and Health Sciences Diagnostic challenges in IPF Dr Ian Glaspole Central and Eastern Clinical School, Alfred Hospital and Monash University March 2015 Disclosures Consultancy fees from
Usual Interstitial pneumonia and Nonspecific Interstitial Pneumonia. Nitra and the Gangs.
 Usual Interstitial pneumonia and Nonspecific Interstitial Pneumonia Nitra and the Gangs. บทน ำและบทท ๓, ๑๐, ๑๒, ๑๓, ๑๔, ๑๕, ๑๗ Usual Interstitial Pneumonia (UIP) Most common & basic pathologic pattern
Usual Interstitial pneumonia and Nonspecific Interstitial Pneumonia Nitra and the Gangs. บทน ำและบทท ๓, ๑๐, ๑๒, ๑๓, ๑๔, ๑๕, ๑๗ Usual Interstitial Pneumonia (UIP) Most common & basic pathologic pattern
A Review of Interstitial Lung Diseases. Paul J. Wolters, MD Associate Professor Department of Medicine University of California San Francisco
 A Review of Interstitial Lung Diseases Paul J. Wolters, MD Associate Professor Department of Medicine University of California San Francisco Outline Overview of diagnosis in ILD Why it is important Definition/Classification
A Review of Interstitial Lung Diseases Paul J. Wolters, MD Associate Professor Department of Medicine University of California San Francisco Outline Overview of diagnosis in ILD Why it is important Definition/Classification
Differential diagnosis
 Differential diagnosis Idiopathic pulmonary fibrosis (IPF) is part of a large family of idiopathic interstitial pneumonias (IIP), one of four subgroups of interstitial lung disease (ILD). Differential
Differential diagnosis Idiopathic pulmonary fibrosis (IPF) is part of a large family of idiopathic interstitial pneumonias (IIP), one of four subgroups of interstitial lung disease (ILD). Differential
Non-neoplastic Lung Disease II
 Pathobasic Non-neoplastic Lung Disease II Spasenija Savic Prince Pathology Program Systematic approach to surgical lung biopsies with ILD Examples (chronic ILD): Idiopathic interstitial pneumonias: UIP,
Pathobasic Non-neoplastic Lung Disease II Spasenija Savic Prince Pathology Program Systematic approach to surgical lung biopsies with ILD Examples (chronic ILD): Idiopathic interstitial pneumonias: UIP,
Medical Policy An independent licensee of the Blue Cross Blue Shield Association
 Idiopathic Pulmonary Fibrosis Page 1 of 10 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: Idiopathic Pulmonary Fibrosis (Esbriet /pirfenidone, Ofev /nintedanib)
Idiopathic Pulmonary Fibrosis Page 1 of 10 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: Idiopathic Pulmonary Fibrosis (Esbriet /pirfenidone, Ofev /nintedanib)
A Review of Interstitial Lung Diseases
 Outline A Review of Interstitial Lung Diseases Paul J. Wolters, MD Associate Professor Department of Medicine University of California San Francisco Overview of diagnosis in ILD Why it is important Definition/Classification
Outline A Review of Interstitial Lung Diseases Paul J. Wolters, MD Associate Professor Department of Medicine University of California San Francisco Overview of diagnosis in ILD Why it is important Definition/Classification
IPF - Inquadramento clinico
 IPF - Inquadramento clinico Sergio Harari Unità Operativa di Pneumologia UTIR Servizio di Fisiopat. Resp. e Emodinamica Polmonare Ospedale S. Giuseppe, Milano Clinical Classification Diffuse parenchimal
IPF - Inquadramento clinico Sergio Harari Unità Operativa di Pneumologia UTIR Servizio di Fisiopat. Resp. e Emodinamica Polmonare Ospedale S. Giuseppe, Milano Clinical Classification Diffuse parenchimal
An earlier and more confident diagnosis of idiopathic pulmonary fibrosis
 Eur Respir Rev 2012; 21: 124, 141 146 DOI: 10.1183/09059180.00000812 CopyrightßERS 2012 REVIEW: IPF An earlier and more confident diagnosis of idiopathic pulmonary fibrosis Roland M. du Bois ABSTRACT:
Eur Respir Rev 2012; 21: 124, 141 146 DOI: 10.1183/09059180.00000812 CopyrightßERS 2012 REVIEW: IPF An earlier and more confident diagnosis of idiopathic pulmonary fibrosis Roland M. du Bois ABSTRACT:
Summary: Key Learning Points, Clinical Strategies, and Future Directions
 Summary: Key Learning Points, Clinical Strategies, and Future Directions Introduction Idiopathic pulmonary fibrosis (IPF), a peripheral lobular fibrosis of unknown cause, is a chronic, progressive lung
Summary: Key Learning Points, Clinical Strategies, and Future Directions Introduction Idiopathic pulmonary fibrosis (IPF), a peripheral lobular fibrosis of unknown cause, is a chronic, progressive lung
Progress in Idiopathic Pulmonary Fibrosis
 Progress in Idiopathic Pulmonary Fibrosis David A. Lynch, MB Disclosures Progress in Idiopathic Pulmonary Fibrosis David A Lynch, MB Consultant: t Research support: Perceptive Imaging Boehringer Ingelheim
Progress in Idiopathic Pulmonary Fibrosis David A. Lynch, MB Disclosures Progress in Idiopathic Pulmonary Fibrosis David A Lynch, MB Consultant: t Research support: Perceptive Imaging Boehringer Ingelheim
IDIOPATHIC PULMONARY FIBROSIS Guidelines for Diagnosis and Management
 IDIOPATHIC PULMONARY FIBROSIS Guidelines for Diagnosis and Management An ATS Pocket Publication This publication was produced in collaboration with Boehringer Ingelheim Pharmaceuticals, Inc. GUIDELINES
IDIOPATHIC PULMONARY FIBROSIS Guidelines for Diagnosis and Management An ATS Pocket Publication This publication was produced in collaboration with Boehringer Ingelheim Pharmaceuticals, Inc. GUIDELINES
INTERSTITIAL LUNG DISEASE. Radhika Reddy MD Pulmonary/Critical Care Long Beach VA Medical Center January 5, 2018
 INTERSTITIAL LUNG DISEASE Radhika Reddy MD Pulmonary/Critical Care Long Beach VA Medical Center January 5, 2018 Interstitial Lung Disease Interstitial Lung Disease Prevalence by Diagnosis: Idiopathic Interstitial
INTERSTITIAL LUNG DISEASE Radhika Reddy MD Pulmonary/Critical Care Long Beach VA Medical Center January 5, 2018 Interstitial Lung Disease Interstitial Lung Disease Prevalence by Diagnosis: Idiopathic Interstitial
Diffuse Interstitial Lung Diseases: Is There Really Anything New?
 : Is There Really Anything New? Sujal R. Desai, MBBS, MD ESTI SPEAKER SUNDAY Society of Thoracic Radiology San Antonio, Texas March 2014 Diffuse Interstitial Lung Disease The State of Play DILDs Is There
: Is There Really Anything New? Sujal R. Desai, MBBS, MD ESTI SPEAKER SUNDAY Society of Thoracic Radiology San Antonio, Texas March 2014 Diffuse Interstitial Lung Disease The State of Play DILDs Is There
5/9/2015. Multi-disciplinary Approach to Diffuse Lung Disease: The Imager s Perspective. No, I am not a pulmonologist! Radiology
 Multi-disciplinary Approach to Diffuse Lung Disease: The Imager s Perspective No, I am not a pulmonologist! Radiology Pathology Clinical 1 Everyone needs a CT Confidence in diagnosis Definitive HRCT +
Multi-disciplinary Approach to Diffuse Lung Disease: The Imager s Perspective No, I am not a pulmonologist! Radiology Pathology Clinical 1 Everyone needs a CT Confidence in diagnosis Definitive HRCT +
CTD-related Lung Disease
 13 th Cambridge Chest Meeting King s College, Cambridge April 2015 Imaging of CTD-related Lung Disease Dr Sujal R Desai King s College Hospital, London Disclosure Statement No Disclosures / Conflicts of
13 th Cambridge Chest Meeting King s College, Cambridge April 2015 Imaging of CTD-related Lung Disease Dr Sujal R Desai King s College Hospital, London Disclosure Statement No Disclosures / Conflicts of
Outline Definition of Terms: Lexicon. Traction Bronchiectasis
 HRCT OF IDIOPATHIC INTERSTITIAL PNEUMONIAS Disclosures Genentech, Inc. Speakers Bureau Tadashi Allen, MD University of Minnesota Assistant Professor Diagnostic Radiology 10/29/2016 Outline Definition of
HRCT OF IDIOPATHIC INTERSTITIAL PNEUMONIAS Disclosures Genentech, Inc. Speakers Bureau Tadashi Allen, MD University of Minnesota Assistant Professor Diagnostic Radiology 10/29/2016 Outline Definition of
4/17/2010 C ini n ca c l a Ev E a v l a ua u t a ion o n of o ILD U dat a e t e i n I LDs
 Update in ILDs Diagnosis 101: Clinical Evaluation April 17, 2010 Jay H. Ryu, MD Mayo Clinic, Rochester MN Clinical Evaluation of ILD Outline General aspects of ILDs Classification of ILDs Clinical evaluation
Update in ILDs Diagnosis 101: Clinical Evaluation April 17, 2010 Jay H. Ryu, MD Mayo Clinic, Rochester MN Clinical Evaluation of ILD Outline General aspects of ILDs Classification of ILDs Clinical evaluation
Disclosures. Fibrotic lung diseases: Basic Principles, Common Problems, and Reporting. Relevant financial relationships: None. Off-label usage: None
 Fibrotic lung diseases: Basic Principles, Common Problems, and Reporting Brandon T. Larsen, MD, PhD Senior Associate Consultant Department of Laboratory Medicine and Pathology Mayo Clinic Arizona Arizona
Fibrotic lung diseases: Basic Principles, Common Problems, and Reporting Brandon T. Larsen, MD, PhD Senior Associate Consultant Department of Laboratory Medicine and Pathology Mayo Clinic Arizona Arizona
Connective Tissue Disorder- Associated Interstitial Lung Disease (CTD-ILD) and Updates
 and Updates") Connective Tissue Disorder- Associated Interstitial Lung Disease (CTD-ILD) and Updates Maria Elena Vega, M.D Assistant Professor of Medicine Lewis Katz School of Medicine at Temple University Nothing to
Connective Tissue Disorder- Associated Interstitial Lung Disease (CTD-ILD) and Updates Maria Elena Vega, M.D Assistant Professor of Medicine Lewis Katz School of Medicine at Temple University Nothing to
Diagnosing Idiopathic Pulmonary Fibrosis on Evidence-Based Guidelines
 Diagnosing Idiopathic Pulmonary Fibrosis on Evidence-Based Guidelines Rebecca Keith, MD Assistant Professor, Division of Pulmonary and Critical Care Medicine National Jewish Health, Denver, CO Objectives
Diagnosing Idiopathic Pulmonary Fibrosis on Evidence-Based Guidelines Rebecca Keith, MD Assistant Professor, Division of Pulmonary and Critical Care Medicine National Jewish Health, Denver, CO Objectives
11/10/2014. Multi-disciplinary Approach to Diffuse Lung Disease: The Imager s Perspective. Radiology
 Multi-disciplinary Approach to Diffuse Lung Disease: The Imager s Perspective Radiology Pathology Clinical 1 Role of HRCT Diagnosis Fibrosis vs. inflammation Next step in management Response to treatment
Multi-disciplinary Approach to Diffuse Lung Disease: The Imager s Perspective Radiology Pathology Clinical 1 Role of HRCT Diagnosis Fibrosis vs. inflammation Next step in management Response to treatment
Overview of Idiopathic Pulmonary Fibrosis: Diagnosis and Therapy
 Overview of Idiopathic Pulmonary Fibrosis: Diagnosis and Therapy Jeff Swigris, DO, MS Director, ILD Program National Jewish Health Disclosures Speaker - Boehringer Ingelheim and Genentech Objectives Describe
Overview of Idiopathic Pulmonary Fibrosis: Diagnosis and Therapy Jeff Swigris, DO, MS Director, ILD Program National Jewish Health Disclosures Speaker - Boehringer Ingelheim and Genentech Objectives Describe
Disclosures. Traditional Paradigm. Overview 4/17/2010. I have relationships with the following organizations and companies:
 Disclosures Pharmacological Therapy for ILD What to Use and How to Use It Harold R Collard MD Interstitial Lung Disease Program University of California San Francisco (UCSF) I have relationships with the
Disclosures Pharmacological Therapy for ILD What to Use and How to Use It Harold R Collard MD Interstitial Lung Disease Program University of California San Francisco (UCSF) I have relationships with the
INTERSTITIAL LUNG DISEASES: FOCUS ON IDIOPATHIC PULMONARY FIBROSIS (IPF)
") INTERSTITIAL LUNG DISEASES: FOCUS ON IDIOPATHIC PULMONARY FIBROSIS (IPF) Marilyn K. Glassberg Csete, M.D. Professor of Medicine, Surgery, and Pediatrics Director, Interstitial and Rare Lung Disease Program
INTERSTITIAL LUNG DISEASES: FOCUS ON IDIOPATHIC PULMONARY FIBROSIS (IPF) Marilyn K. Glassberg Csete, M.D. Professor of Medicine, Surgery, and Pediatrics Director, Interstitial and Rare Lung Disease Program
International consensus statement on idiopathic pulmonary fibrosis
 Eur Respir J 2001; 17: 163 167 Printed in UK all rights reserved Copyright #ERS Journals Ltd 2001 European Respiratory Journal ISSN 0903-1936 PERSPECTIVE International consensus statement on idiopathic
Eur Respir J 2001; 17: 163 167 Printed in UK all rights reserved Copyright #ERS Journals Ltd 2001 European Respiratory Journal ISSN 0903-1936 PERSPECTIVE International consensus statement on idiopathic
Update on Therapies for Idiopathic Pulmonary Fibrosis. Outline
 Update on Therapies for Idiopathic Pulmonary Fibrosis Paul Wolters Associate Professor University of California, San Francisco Outline Classification of Interstitial lung disease Clinical classification
Update on Therapies for Idiopathic Pulmonary Fibrosis Paul Wolters Associate Professor University of California, San Francisco Outline Classification of Interstitial lung disease Clinical classification
Interstitial Lung Disease (ILD)
") Interstitial Lung Disease (ILD) ILD comprises more than 130 distinct disorders Characterized by cellular proliferation, cellular infiltration, and/or fibrosis of the lung parenchyma not due to infection
Interstitial Lung Disease (ILD) ILD comprises more than 130 distinct disorders Characterized by cellular proliferation, cellular infiltration, and/or fibrosis of the lung parenchyma not due to infection
Unpaid scientific collaborator & advisor with Veracyte, Inc.
 Diagnosis and Classification of Idiopathic Interstitial Pneumonias: Role of Histopathology in the Golden Age of Consensus Jeffrey L. Myers, M.D. A. James French Professor of Diagnostic Pathology Vice Chair
Diagnosis and Classification of Idiopathic Interstitial Pneumonias: Role of Histopathology in the Golden Age of Consensus Jeffrey L. Myers, M.D. A. James French Professor of Diagnostic Pathology Vice Chair
Idiopathic Pulmonary of Care
 Chapter 6.1 Living Medical etextbook A Digital Tool at the Point of Care From Projects In Knowledge Pulmonology Idiopathic Pulmonary Fibrosis @Point of Care IPF Case Study: Typical Presentation, Role of
Chapter 6.1 Living Medical etextbook A Digital Tool at the Point of Care From Projects In Knowledge Pulmonology Idiopathic Pulmonary Fibrosis @Point of Care IPF Case Study: Typical Presentation, Role of
DIAGNOSTIC NOTE TEMPLATE
 DIAGNOSTIC NOTE TEMPLATE SOAP NOTE TEMPLATE WHEN CONSIDERING A DIAGNOSIS OF IDIOPATHIC PULMONARY FIBROSIS (IPF) CHIEF COMPLAINT HISTORY OF PRESENT ILLNESS Consider IPF as possible diagnosis if any of the
DIAGNOSTIC NOTE TEMPLATE SOAP NOTE TEMPLATE WHEN CONSIDERING A DIAGNOSIS OF IDIOPATHIC PULMONARY FIBROSIS (IPF) CHIEF COMPLAINT HISTORY OF PRESENT ILLNESS Consider IPF as possible diagnosis if any of the
Liebow and Carrington's original classification of IIP
 Liebow and Carrington's original classification of IIP-- 1969 Eric J. Stern MD University of Washington UIP Usual interstitial pneumonia DIP Desquamative interstitial pneumonia BIP Bronchiolitis obliterans
Liebow and Carrington's original classification of IIP-- 1969 Eric J. Stern MD University of Washington UIP Usual interstitial pneumonia DIP Desquamative interstitial pneumonia BIP Bronchiolitis obliterans
Imaging: how to recognise idiopathic pulmonary fibrosis
 REVIEW IDIOPATHIC PULMONARY FIBROSIS Imaging: how to recognise idiopathic pulmonary fibrosis Anand Devaraj Affiliations: Dept of Radiology, St George s Hospital, London, UK. Correspondence: Anand Devaraj,
REVIEW IDIOPATHIC PULMONARY FIBROSIS Imaging: how to recognise idiopathic pulmonary fibrosis Anand Devaraj Affiliations: Dept of Radiology, St George s Hospital, London, UK. Correspondence: Anand Devaraj,
UIP Possibile e Probabile
 UIP Possibile e Probabile Sergio Harari U.O. di Pneumologia e UTIR Servizio di Emodinamica e Fisiopatologia Respiratoria Ospedale San Giuseppe - Milano Current definition of IPF IPF is a distinct type
UIP Possibile e Probabile Sergio Harari U.O. di Pneumologia e UTIR Servizio di Emodinamica e Fisiopatologia Respiratoria Ospedale San Giuseppe - Milano Current definition of IPF IPF is a distinct type
Manish Powari Regional Training Day 10/12/2014
 Manish Powari Regional Training Day 10/12/2014 Large number of different types of Interstitial Lung Disease (ILD). Most are very rare Most patients present with one of a smaller number of commoner diseases
Manish Powari Regional Training Day 10/12/2014 Large number of different types of Interstitial Lung Disease (ILD). Most are very rare Most patients present with one of a smaller number of commoner diseases
IPF AND OTHER FIBROSING LUNG DISEASE: WHAT DRUGS MIGHT WORK AND ON WHOM DO THEY W ORK?
 IPF AND OTHER FIBROSING LUNG DISEASE: WHAT DRUGS MIGHT WORK AND ON WHOM DO THEY W ORK? KEVIN K. BROWN, MD PROFESSOR AND VICE CHAIRMAN, DEPARTMENT OF MEDICINE NATIONAL JEWISH HEALTH DENVER, CO Kevin K.
IPF AND OTHER FIBROSING LUNG DISEASE: WHAT DRUGS MIGHT WORK AND ON WHOM DO THEY W ORK? KEVIN K. BROWN, MD PROFESSOR AND VICE CHAIRMAN, DEPARTMENT OF MEDICINE NATIONAL JEWISH HEALTH DENVER, CO Kevin K.
Strategies for Updated Treatment Options for IPF
 Strategies for Updated Treatment Options for IPF Paul W. Noble, MD Vera and Paul Guerin Family Distinguished Chair in Pulmonary Medicine Professor and Chair Department of Medicine Director, Women's Guild
Strategies for Updated Treatment Options for IPF Paul W. Noble, MD Vera and Paul Guerin Family Distinguished Chair in Pulmonary Medicine Professor and Chair Department of Medicine Director, Women's Guild
Pulmonary manifestations of CTDs Diagnosis, differential diagnosis and treatment
 Prague, June 2014 Pulmonary manifestations of CTDs Diagnosis, differential diagnosis and treatment Katerina M. Antoniou, MD, PhD As. Professor in Thoracic Medicine ERS ILD Group Secretary Medical School,
Prague, June 2014 Pulmonary manifestations of CTDs Diagnosis, differential diagnosis and treatment Katerina M. Antoniou, MD, PhD As. Professor in Thoracic Medicine ERS ILD Group Secretary Medical School,
The radiological differential diagnosis of the UIP pattern
 5th International Conference on Idiopathic Pulmonary Fibrosis, Modena, 2015, June 12th The radiological differential diagnosis of the UIP pattern Simon Walsh King s College Hospital Foundation Trust London,
5th International Conference on Idiopathic Pulmonary Fibrosis, Modena, 2015, June 12th The radiological differential diagnosis of the UIP pattern Simon Walsh King s College Hospital Foundation Trust London,
Financial disclosure COMMON DIAGNOSES IN HRCT. High Res Chest HRCT. HRCT Pre test. I have no financial relationships to disclose. Anatomy Nomenclature
 Financial disclosure I have no financial relationships to disclose. Douglas Johnson D.O. Cardiothoracic Imaging Gaston Radiology COMMON DIAGNOSES IN HRCT High Res Chest Anatomy Nomenclature HRCT Sampling
Financial disclosure I have no financial relationships to disclose. Douglas Johnson D.O. Cardiothoracic Imaging Gaston Radiology COMMON DIAGNOSES IN HRCT High Res Chest Anatomy Nomenclature HRCT Sampling
Wim Wuyts. Treatment of idiopathic interstitial pneumonias. March 12 th Interstitial lung diseases state of the art.
 nterstitial ungdiseases euven Department of pneumology Unit for interstitial lung diseases University Hospitals Leuven March 12 th 2015 Interstitial lung diseases state of the art Treatment of idiopathic
nterstitial ungdiseases euven Department of pneumology Unit for interstitial lung diseases University Hospitals Leuven March 12 th 2015 Interstitial lung diseases state of the art Treatment of idiopathic
Case 4 History. 58 yo man presented with prox IP joint swelling 2 months later pain and swelling in multiple joints Chest radiograph: bi-basilar
 Case 4 History 58 yo man presented with prox IP joint swelling 2 months later pain and swelling in multiple joints Chest radiograph: bi-basilar basilar infiltrates suggestive of pulmonary fibrosis Open
Case 4 History 58 yo man presented with prox IP joint swelling 2 months later pain and swelling in multiple joints Chest radiograph: bi-basilar basilar infiltrates suggestive of pulmonary fibrosis Open
Katerina M. Antoniou, MD, PhD As. Professor in Thoracic Medicine ERS ILD Group Secretary Medical School, University of Crete Prague, June 2014
 Hypersensitivity pneumonitis: Causes, clinical course, diagnosis and differential diagnosis, treatment Katerina M. Antoniou, MD, PhD As. Professor in Thoracic Medicine ERS ILD Group Secretary Medical School,
Hypersensitivity pneumonitis: Causes, clinical course, diagnosis and differential diagnosis, treatment Katerina M. Antoniou, MD, PhD As. Professor in Thoracic Medicine ERS ILD Group Secretary Medical School,
Idiopathic Pulmonary Fibrosis Treatable and Not Idiopathic
 Idiopathic Pulmonary Fibrosis Treatable and Not Idiopathic Brett Ley, MD University of California San Francisco CTS 1/26/18 Disclosures Speaker s bureau honorarium from Genentech (makers of pirfenidone)
Idiopathic Pulmonary Fibrosis Treatable and Not Idiopathic Brett Ley, MD University of California San Francisco CTS 1/26/18 Disclosures Speaker s bureau honorarium from Genentech (makers of pirfenidone)
Challenges in Pulmonary and Critical Care: 2018
 Challenges in Pulmonary and Critical Care: 2018 Interstitial Lung Disease: Evolving Our Understanding of a Deadly Disease 1 Faculty Kevin Flaherty, MD, MS Professor in Pulmonary and Critical Care Medicine
Challenges in Pulmonary and Critical Care: 2018 Interstitial Lung Disease: Evolving Our Understanding of a Deadly Disease 1 Faculty Kevin Flaherty, MD, MS Professor in Pulmonary and Critical Care Medicine
Pathologic Assessment of Interstitial Lung Disease
 Pathologic Assessment of Interstitial Lung Disease Dry and itchy? It could be eczema or fungal infection. We don t need to worry, the drugs aren t that dangerous. Kirk D. Jones, MD UCSF Dept. of Pathology
Pathologic Assessment of Interstitial Lung Disease Dry and itchy? It could be eczema or fungal infection. We don t need to worry, the drugs aren t that dangerous. Kirk D. Jones, MD UCSF Dept. of Pathology
Bronchoalveolar Lavage and Histopathologic Diagnosis Based on Biopsy
 Idiopathic Pulmonary Fibrosis Bronchoalveolar Lavage and Histopathologic Diagnosis Based on Biopsy JMAJ 46(11): 469 474, 2003 Yukihiko SUGIYAMA Professor, Division of Pulmonary Medicine, Department of
Idiopathic Pulmonary Fibrosis Bronchoalveolar Lavage and Histopathologic Diagnosis Based on Biopsy JMAJ 46(11): 469 474, 2003 Yukihiko SUGIYAMA Professor, Division of Pulmonary Medicine, Department of
COI: no conflicts of interest to declare
 Idiopathic versus secondary Usual Interstitial Pneumonia (UIP) pattern in a series of 96 consecutive surgical lung biopsies: The value of histologic ancillary findings in a multidisciplinary discussion
Idiopathic versus secondary Usual Interstitial Pneumonia (UIP) pattern in a series of 96 consecutive surgical lung biopsies: The value of histologic ancillary findings in a multidisciplinary discussion
Challenges in the Diagnosis of Interstitial Lung Disease
 Challenges in the Diagnosis of Interstitial Lung Disease Kirk D. Jones, MD UCSF Dept. of Pathology kirk.jones@ucsf.edu Overview New Classification of IIP Prior classification Modifications for new classification
Challenges in the Diagnosis of Interstitial Lung Disease Kirk D. Jones, MD UCSF Dept. of Pathology kirk.jones@ucsf.edu Overview New Classification of IIP Prior classification Modifications for new classification
Daria Manos RSNA 2016 RC 401. https://medicine.dal.ca/departments/depar tment-sites/radiology/contact/faculty/dariamanos.html
 Daria Manos RSNA 2016 RC 401 https://medicine.dal.ca/departments/depar tment-sites/radiology/contact/faculty/dariamanos.html STEP1: Is this fibrotic lung disease? STEP 2: Is this a UIP pattern? If yes:
Daria Manos RSNA 2016 RC 401 https://medicine.dal.ca/departments/depar tment-sites/radiology/contact/faculty/dariamanos.html STEP1: Is this fibrotic lung disease? STEP 2: Is this a UIP pattern? If yes:
PFF HEALTH CARE PROFESSIONAL WEBINAR SERIES. Welcome!
 PFF HEALTH CARE PROFESSIONAL WEBINAR SERIES Welcome! AGENDA TOPICS Welcome & Introduction Dr. Gregory Cosgrove, MD Chief Medical Officer Pulmonary Fibrosis Foundation PFF Resources Dolly Kervitsky, RCP,
PFF HEALTH CARE PROFESSIONAL WEBINAR SERIES Welcome! AGENDA TOPICS Welcome & Introduction Dr. Gregory Cosgrove, MD Chief Medical Officer Pulmonary Fibrosis Foundation PFF Resources Dolly Kervitsky, RCP,
Difficulties Diagnosing Idiopathic Pulmonary Fibrosis
 1. er Encuentro Entre Neumólogos y Radiólogos, Madrid, Spain, 2016, October 14th Difficulties Diagnosing Idiopathic Pulmonary Fibrosis Simon Walsh King s College Hospital Foundation Trust London, United
1. er Encuentro Entre Neumólogos y Radiólogos, Madrid, Spain, 2016, October 14th Difficulties Diagnosing Idiopathic Pulmonary Fibrosis Simon Walsh King s College Hospital Foundation Trust London, United
Hypersensitivity Pneumonitis Common Diagnostic and Treatment Dilemmas
 Hypersensitivity Pneumonitis Common Diagnostic and Treatment Dilemmas Rishi Raj MD Director, Interstitial Lung Diseases Program Clinical Professor of Pulmonary and Critical Care Medicine Stanford University
Hypersensitivity Pneumonitis Common Diagnostic and Treatment Dilemmas Rishi Raj MD Director, Interstitial Lung Diseases Program Clinical Professor of Pulmonary and Critical Care Medicine Stanford University
TBLB is not recommended as the initial biopsy option in cases of suspected IPF and is unreliable in the diagnosis of rare lung disease (other than
 TBLB is not recommended as the initial biopsy option in cases of suspected IPF and is unreliable in the diagnosis of rare lung disease (other than PAP) BAL is not required as a diagnostic tool in patients
TBLB is not recommended as the initial biopsy option in cases of suspected IPF and is unreliable in the diagnosis of rare lung disease (other than PAP) BAL is not required as a diagnostic tool in patients
New Horizons The Future of IPF and ILD
 New Horizons The Future of IPF and ILD Talmadge E. King, Jr., M.D. Julius R. Krevans Distinguished Professorship in Internal Medicine Chair, Department of Medicine University of California San Francisco
New Horizons The Future of IPF and ILD Talmadge E. King, Jr., M.D. Julius R. Krevans Distinguished Professorship in Internal Medicine Chair, Department of Medicine University of California San Francisco
Challenges in the Diagnosis of Interstitial Lung Disease
 Challenges in the Diagnosis of Interstitial Lung Disease Kirk D. Jones, MD UCSF Dept. of Pathology kirk.jones@ucsf.edu Overview New Classification of IIP Prior classification Modifications for new classification
Challenges in the Diagnosis of Interstitial Lung Disease Kirk D. Jones, MD UCSF Dept. of Pathology kirk.jones@ucsf.edu Overview New Classification of IIP Prior classification Modifications for new classification
June 2013 Pulmonary Case of the Month: Diagnosis Makes a Difference. Lewis J. Wesselius, MD 1 Henry D. Tazelaar, MD 2
 June 2013 Pulmonary Case of the Month: Diagnosis Makes a Difference Lewis J. Wesselius, MD 1 Henry D. Tazelaar, MD 2 Departments of Pulmonary Medicine 1 and Laboratory Medicine and Pathology 2 Mayo Clinic
June 2013 Pulmonary Case of the Month: Diagnosis Makes a Difference Lewis J. Wesselius, MD 1 Henry D. Tazelaar, MD 2 Departments of Pulmonary Medicine 1 and Laboratory Medicine and Pathology 2 Mayo Clinic
Controversies in Clinical Trials. Pirfenidone for Idiopathic Pulmonary Fibrosis (IPF)
") Controversies in Clinical Trials Pirfenidone for Idiopathic Pulmonary Fibrosis (IPF) Controversies to be highlighted by IPF Post-hoc analyses Story Primary end point selection Changing prespecified endpoints
Controversies in Clinical Trials Pirfenidone for Idiopathic Pulmonary Fibrosis (IPF) Controversies to be highlighted by IPF Post-hoc analyses Story Primary end point selection Changing prespecified endpoints
National Jewish Health. Idiopathic Pulmonary Fibrosis: A Guide for Providers
 National Jewish Health Idiopathic Pulmonary Fibrosis: A Guide for Providers Table of Contents National Jewish Health Materials were developed through a partnership between National Jewish Health and PVI,
National Jewish Health Idiopathic Pulmonary Fibrosis: A Guide for Providers Table of Contents National Jewish Health Materials were developed through a partnership between National Jewish Health and PVI,
A case of a patient with IPF treated with nintedanib. Prof. Kreuter and Prof. Heussel
 A case of a patient with IPF treated with nintedanib Prof. Kreuter and Prof. Heussel Case Overview This case describes the history of a patient with IPF who, at the time of diagnosis, had symptoms typical
A case of a patient with IPF treated with nintedanib Prof. Kreuter and Prof. Heussel Case Overview This case describes the history of a patient with IPF who, at the time of diagnosis, had symptoms typical
Therapies for Idiopathic Pulmonary Fibrosis Pharmacologic, Non-Pharmacologic
 Therapies for Idiopathic Pulmonary Fibrosis Pharmacologic, Non-Pharmacologic Amy Olson, MD, MSPH Associate Professor, Division of Pulmonary and Critical Care Medicine National Jewish Health, Denver, CO
Therapies for Idiopathic Pulmonary Fibrosis Pharmacologic, Non-Pharmacologic Amy Olson, MD, MSPH Associate Professor, Division of Pulmonary and Critical Care Medicine National Jewish Health, Denver, CO
Lines and crackles. Making sense of ILD
 Lines and crackles Making sense of ILD Case JM 65 year old male Gradual shortness of breath, going on over a year Some dry cough Ex-smoker, quit 10 years ago Crackles in the bases CXR presented Sent to
Lines and crackles Making sense of ILD Case JM 65 year old male Gradual shortness of breath, going on over a year Some dry cough Ex-smoker, quit 10 years ago Crackles in the bases CXR presented Sent to
Conflicts of Interest. Advisory Board: Boehringer-Ingleheim, Genentech/Roche DSMB: Bristol-Myers Squibb, Fibrogen Clinical Endpoint Committee; Merck
 Conflicts of Interest Advisory Board: Boehringer-Ingleheim, Genentech/Roche DSMB: Bristol-Myers Squibb, Fibrogen Clinical Endpoint Committee; Merck The Idiopathic Interstitial Pneumonias Idiopathic pulmonary
Conflicts of Interest Advisory Board: Boehringer-Ingleheim, Genentech/Roche DSMB: Bristol-Myers Squibb, Fibrogen Clinical Endpoint Committee; Merck The Idiopathic Interstitial Pneumonias Idiopathic pulmonary
ERS 2016 Congress Highlights Interstitial Lung Disease (ILD)
") ERS 216 Congress Highlights Interstitial Lung Disease (ILD) London, UK September 3 rd 7 th 216 The 26 th European Respiratory Society International Congress, (ERS) the largest respiratory meeting in the
ERS 216 Congress Highlights Interstitial Lung Disease (ILD) London, UK September 3 rd 7 th 216 The 26 th European Respiratory Society International Congress, (ERS) the largest respiratory meeting in the
ESBRIET (pirfenidone) oral capsule and oral tablet OFEV (nintedanib) oral capsule
 oral capsule and oral tablet OFEV (nintedanib) oral capsule") OFEV (nintedanib) oral capsule Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific benefit plan. This Pharmacy Coverage
OFEV (nintedanib) oral capsule Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific benefit plan. This Pharmacy Coverage
New Therapies and Trials in IPF
 Conflict of interest disclosure I have the following real or perceived conflicts of interest that relate to this presentation: New Therapies and Trials in IPF Talmadge E. King, Jr., M.D. Julius R. Krevans
Conflict of interest disclosure I have the following real or perceived conflicts of interest that relate to this presentation: New Therapies and Trials in IPF Talmadge E. King, Jr., M.D. Julius R. Krevans
Nintedanib and Pirfenidone: New Medications in the Management of Idiopathic Pulmonary Fibrosis
 Nintedanib and Pirfenidone: New Medications in the Management of Idiopathic Pulmonary Fibrosis Brad Zimmermann, PharmD, MBA Pharmacy Grand Rounds May 02, 2017 Rochester, Minnesota 2017 MFMER slide-1 Objectives
Nintedanib and Pirfenidone: New Medications in the Management of Idiopathic Pulmonary Fibrosis Brad Zimmermann, PharmD, MBA Pharmacy Grand Rounds May 02, 2017 Rochester, Minnesota 2017 MFMER slide-1 Objectives
Patient with FVC>90% predicted. Demosthenes Bouros, Vasilios Tzilas University of Athens
 Patient with FVC>90% predicted Demosthenes Bouros, Vasilios Tzilas University of Athens CASE OVERVIEW A 63-year-old, male patient with progressive exertional dyspnoea lasting for 2 years and dry cough
Patient with FVC>90% predicted Demosthenes Bouros, Vasilios Tzilas University of Athens CASE OVERVIEW A 63-year-old, male patient with progressive exertional dyspnoea lasting for 2 years and dry cough
Disclosures. Clinical Approach: Evaluating CTD-ILD for the pulmonologist. ILD in CTD. connective tissue disease or collagen vascular disease
 Disclosures Clinical Approach: Evaluating CTD-ILD for the pulmonologist Industry relationships: Actelion, atyr Pharma, Boehringer-Ingelheim, Genentech- Roche, Gilead Aryeh Fischer, MD Associate Professor
Disclosures Clinical Approach: Evaluating CTD-ILD for the pulmonologist Industry relationships: Actelion, atyr Pharma, Boehringer-Ingelheim, Genentech- Roche, Gilead Aryeh Fischer, MD Associate Professor
Diagnosing ILD. What is important in 2016? Chris Grainge
 Diagnosing ILD What is important in 2016? Chris Grainge Senior Staff Specialist Respiratory Medicine John Hunter Hospital Conjoint A/Prof University of Newcastle Conflict of interest I have acted as a
Diagnosing ILD What is important in 2016? Chris Grainge Senior Staff Specialist Respiratory Medicine John Hunter Hospital Conjoint A/Prof University of Newcastle Conflict of interest I have acted as a
Annual Rheumatology & Therapeutics Review for Organizations & Societies
 Annual Rheumatology & Therapeutics Review for Organizations & Societies A Rheumatologist s Approach to Interstitial Lung Disease Outline ILD classification and patterns in CTD The clinical landscape and
Annual Rheumatology & Therapeutics Review for Organizations & Societies A Rheumatologist s Approach to Interstitial Lung Disease Outline ILD classification and patterns in CTD The clinical landscape and
Criteria for confident HRCT diagnosis of usual interstitial pneumonia (UIP)
") Criteria for confident HRCT diagnosis of usual interstitial pneumonia (UIP) Assem El Essawy (1) & Amr A. Nassef (٢) Abstract Identification of interstitial pneumonia (IP) was mainly based on histological
Criteria for confident HRCT diagnosis of usual interstitial pneumonia (UIP) Assem El Essawy (1) & Amr A. Nassef (٢) Abstract Identification of interstitial pneumonia (IP) was mainly based on histological
Nonspecific interstitial pneumonia and usual interstitial pneumonia: comparison of the clinicopathologic features and prognosis
 Original Article Nonspecific interstitial pneumonia and usual interstitial pneumonia: comparison of the clinicopathologic features and prognosis Xia Li 1, Chang Chen 2, Jinfu Xu 1, Jinming Liu 1, Xianghua
Original Article Nonspecific interstitial pneumonia and usual interstitial pneumonia: comparison of the clinicopathologic features and prognosis Xia Li 1, Chang Chen 2, Jinfu Xu 1, Jinming Liu 1, Xianghua
Significance of granulomatous inflammation in usual interstitial pneumonia
 Case report SARCOIDOSIS VASCULITIS AND DIFFUSE LUNG DISEASES 2015; 32; 160-166 Mattioli 1885 Significance of granulomatous inflammation in usual interstitial pneumonia R. Tomic 1, H.J. Kim 1, M. Bors 1,
Case report SARCOIDOSIS VASCULITIS AND DIFFUSE LUNG DISEASES 2015; 32; 160-166 Mattioli 1885 Significance of granulomatous inflammation in usual interstitial pneumonia R. Tomic 1, H.J. Kim 1, M. Bors 1,
Case 1 : Question. 1.1 What is the intralobular distribution? 1. Centrilobular 2. Perilymphatic 3. Random
 Interesting case Case 1 Case 1 : Question 1.1 What is the intralobular distribution? 1. Centrilobular 2. Perilymphatic 3. Random Case 1: Answer 1.1 What is the intralobular distribution? 1. Centrilobular
Interesting case Case 1 Case 1 : Question 1.1 What is the intralobular distribution? 1. Centrilobular 2. Perilymphatic 3. Random Case 1: Answer 1.1 What is the intralobular distribution? 1. Centrilobular
Current diagnostic recommendations for ILD: The multidisciplinary meeting TSANZSRS ASM
 Medicine, Nursing and Health Sciences Current diagnostic recommendations for ILD: The multidisciplinary meeting Dr Ian Glaspole Central and Eastern Clinical School, Alfred Hospital and Monash University
Medicine, Nursing and Health Sciences Current diagnostic recommendations for ILD: The multidisciplinary meeting Dr Ian Glaspole Central and Eastern Clinical School, Alfred Hospital and Monash University
Thoracic lung involvement in rheumatoid arthritis: Findings on HRCT
 Thoracic lung involvement in rheumatoid arthritis: Findings on HRCT Poster No.: C-2488 Congress: ECR 2015 Type: Educational Exhibit Authors: R. E. Correa Soto, M. J. Martín Sánchez, J. M. Fernandez 1 1
Thoracic lung involvement in rheumatoid arthritis: Findings on HRCT Poster No.: C-2488 Congress: ECR 2015 Type: Educational Exhibit Authors: R. E. Correa Soto, M. J. Martín Sánchez, J. M. Fernandez 1 1
IPF : Dalla Diagnosi alla Terapia
 IV Forum di Pneumologia Interventistica Bologna 5-6 Giugno 2015 IPF : Dalla Diagnosi alla Terapia Sergio Harari U.O. di Pneumologia e UTIR Servizio di Emodinamica e Fisiopatologia Respiratoria Ospedale
IV Forum di Pneumologia Interventistica Bologna 5-6 Giugno 2015 IPF : Dalla Diagnosi alla Terapia Sergio Harari U.O. di Pneumologia e UTIR Servizio di Emodinamica e Fisiopatologia Respiratoria Ospedale
Idiopathic interstitial pneumonias (IIPs) are a group of
 are a group of") SYMPOSIA C. Isabela S. Silva, MD, PhD and Nestor L. Müller, MD, PhD Abstract: The idiopathic interstitial pneumonias (IIPs) are a group of diffuse parenchymal lung diseases of unknown etiology characterized
SYMPOSIA C. Isabela S. Silva, MD, PhD and Nestor L. Müller, MD, PhD Abstract: The idiopathic interstitial pneumonias (IIPs) are a group of diffuse parenchymal lung diseases of unknown etiology characterized
Cryptogenic Organizing Pneumonia Diagnosis Approach Based on a Clinical-Radiologic-Pathologic Consensus
 Cryptogenic Organizing Pneumonia Diagnosis Approach Based on a Clinical-Radiologic-Pathologic Consensus Poster No.: C-1622 Congress: ECR 2012 Type: Scientific Exhibit Authors: C. Cordero Lares, E. Zorita
Cryptogenic Organizing Pneumonia Diagnosis Approach Based on a Clinical-Radiologic-Pathologic Consensus Poster No.: C-1622 Congress: ECR 2012 Type: Scientific Exhibit Authors: C. Cordero Lares, E. Zorita
UIP OR NOT UIP PATTERN: THAT IS NOT THE ONLY QUESTION!
 UIP OR NOT UIP PATTERN: THAT IS NOT THE ONLY QUESTION! STÉPHANE JOUNEAU 11 JULY 2014 Respiratory Medicine Department, Pontchaillou Hospital, Rennes, France CASE OVERVIEW This case highlights how a usual
UIP OR NOT UIP PATTERN: THAT IS NOT THE ONLY QUESTION! STÉPHANE JOUNEAU 11 JULY 2014 Respiratory Medicine Department, Pontchaillou Hospital, Rennes, France CASE OVERVIEW This case highlights how a usual
Idiopathic Pulmonary Fibrosis: The Importance of Qualitative and Quantitative Phenotyping
 Idiopathic Pulmonary Fibrosis: The Importance of Qualitative and Quantitative Phenotyping K. R. Flaherty Division of Pulmonary and Critical Care Medicine, University of Michigan Health System, Ann Arbor,
Idiopathic Pulmonary Fibrosis: The Importance of Qualitative and Quantitative Phenotyping K. R. Flaherty Division of Pulmonary and Critical Care Medicine, University of Michigan Health System, Ann Arbor,
Radiologic Approach to Smoking Related Interstitial Lung Disease
 Radiologic Approach to Smoking Related Interstitial Lung Disease Poster No.: C-1854 Congress: ECR 2013 Type: Educational Exhibit Authors: K.-N. Lee, J.-Y. Han, E.-J. Kang, J. Kang; Busan/KR Keywords: Toxicity,
Radiologic Approach to Smoking Related Interstitial Lung Disease Poster No.: C-1854 Congress: ECR 2013 Type: Educational Exhibit Authors: K.-N. Lee, J.-Y. Han, E.-J. Kang, J. Kang; Busan/KR Keywords: Toxicity,
The Egyptian Journal of Hospital Medicine (July 2017) Vol.68 (2), Page
 Vol.68 (2), Page") The Egyptian Journal of Hospital Medicine (July 2017) Vol.68 (2), Page 1135-1140 Role of High Resolution Computed Tomography in Diagnosis of Interstitial Lung Diseases in Patients with Collagen Diseases
The Egyptian Journal of Hospital Medicine (July 2017) Vol.68 (2), Page 1135-1140 Role of High Resolution Computed Tomography in Diagnosis of Interstitial Lung Diseases in Patients with Collagen Diseases
T he diagnostic evaluation of a patient with
 546 REVIEW SERIES Challenges in pulmonary fibrosis? 1: Use of high resolution CT scanning of the lung for the evaluation of patients with idiopathic interstitial pneumonias Michael B Gotway, Michelle M
546 REVIEW SERIES Challenges in pulmonary fibrosis? 1: Use of high resolution CT scanning of the lung for the evaluation of patients with idiopathic interstitial pneumonias Michael B Gotway, Michelle M
UPDATE ON INTERSTITIAL LUNG DISEASE. Thomas V. Colby, M.D.
 UPDATE ON INTERSTITIAL LUNG DISEASE Thomas V. Colby, M.D. FINANCIAL DISCLOSURES NONE Topics Discussed 1. Idiopathic pulmonary fibrosis (IPF) 2. Idiopathic interstitial pneumonias (IIPs) 3. Interstitial
UPDATE ON INTERSTITIAL LUNG DISEASE Thomas V. Colby, M.D. FINANCIAL DISCLOSURES NONE Topics Discussed 1. Idiopathic pulmonary fibrosis (IPF) 2. Idiopathic interstitial pneumonias (IIPs) 3. Interstitial
Role of Pirfenidone in Idiopathic Pulmonary Fibrosis - A Longitudinal Cohort Study
 36 Journal of The Association of Physicians of India Vol. 64 May 2016 Original Article Role of Pirfenidone in Idiopathic Pulmonary Fibrosis - A Longitudinal Cohort Study KP Suraj 1, Neethu K Kumar 2, E
36 Journal of The Association of Physicians of India Vol. 64 May 2016 Original Article Role of Pirfenidone in Idiopathic Pulmonary Fibrosis - A Longitudinal Cohort Study KP Suraj 1, Neethu K Kumar 2, E
Official ATS/ERS/JRS/ALAT Clinical Practice Guidelines: Treatment of Idiopathic Pulmonary Fibrosis
 Official ATS/ERS/JRS/ALAT Clinical Practice Guidelines: Treatment of Idiopathic Pulmonary Fibrosis An Update of the 2011 Clinical Practice Guideline Online Supplement Ganesh Raghu, Bram Rochwerg, Yuan
Official ATS/ERS/JRS/ALAT Clinical Practice Guidelines: Treatment of Idiopathic Pulmonary Fibrosis An Update of the 2011 Clinical Practice Guideline Online Supplement Ganesh Raghu, Bram Rochwerg, Yuan
Cigna Drug and Biologic Coverage Policy
 Cigna Drug and Biologic Coverage Policy Subject Idiopathic Pulmonary Fibrosis Therapy Table of Contents Coverage Policy... 1 General Background... 4 Coding/Billing Information... 7 References... 7 Effective
Cigna Drug and Biologic Coverage Policy Subject Idiopathic Pulmonary Fibrosis Therapy Table of Contents Coverage Policy... 1 General Background... 4 Coding/Billing Information... 7 References... 7 Effective
Current Management of IPF and. Dr R Lakshmi Narasimhan Dept of Pulmonary Medicine
 Current Management of IPF and fibrosing ILDs Dr R Lakshmi Narasimhan Dept of Pulmonary Medicine Introduction Idiopathic pulmonary fibrosis clinical course is variable and long term survival is poor Therapy
Current Management of IPF and fibrosing ILDs Dr R Lakshmi Narasimhan Dept of Pulmonary Medicine Introduction Idiopathic pulmonary fibrosis clinical course is variable and long term survival is poor Therapy
Systemic lupus erythematosus (SLE): Pleuropulmonary Manifestations
: Pleuropulmonary Manifestations") 08/30/10 09/26/10 Systemic lupus erythematosus (SLE): Pleuropulmonary Manifestations Camila Downey S. Universidad de Chile, School of Medicine, Year VII Harvard University, School of Medicine Sept 17,
08/30/10 09/26/10 Systemic lupus erythematosus (SLE): Pleuropulmonary Manifestations Camila Downey S. Universidad de Chile, School of Medicine, Year VII Harvard University, School of Medicine Sept 17,
Interstitial Lung Disease ILD: Definition
 Interstitial Lung Disease 2007 Paul F. Simonelli,, MD, PhD, FCCP Clinical Director Center for Interstitial Lung Disease Columbia University Medical Center 1. ILD is not one disorder ILD: Definition 2.
Interstitial Lung Disease 2007 Paul F. Simonelli,, MD, PhD, FCCP Clinical Director Center for Interstitial Lung Disease Columbia University Medical Center 1. ILD is not one disorder ILD: Definition 2.
Management of Co morbidities in Idiopathic Pulmonary Fibrosis. Disclosures
 Management of Co morbidities in Idiopathic Pulmonary Fibrosis Joyce S. Lee, MD MAS Director, Interstitial Lung Disease Clinic University of California, San Francisco Disclosures Intermune, advisory board
Management of Co morbidities in Idiopathic Pulmonary Fibrosis Joyce S. Lee, MD MAS Director, Interstitial Lung Disease Clinic University of California, San Francisco Disclosures Intermune, advisory board
HYPERSENSITIVITY PNEUMONITIS
 HYPERSENSITIVITY PNEUMONITIS A preventable fibrosis MOSAVIR ANSARIE MB., FCCP INTERSTITIAL LUNG DISEASES A heterogeneous group of non infectious, non malignant diffuse parenchymal disorders of the lower
HYPERSENSITIVITY PNEUMONITIS A preventable fibrosis MOSAVIR ANSARIE MB., FCCP INTERSTITIAL LUNG DISEASES A heterogeneous group of non infectious, non malignant diffuse parenchymal disorders of the lower
Presente e futuro della terapia della fibrosi polmonare idiopatica
 Presente e futuro della terapia della fibrosi polmonare idiopatica Antonella Caminati U.O. di Pneumologia e Terapia Semi Intensiva Servizio di Fisiopatologia Respiratoria ed Emodinamica Polmonare Osp.
Presente e futuro della terapia della fibrosi polmonare idiopatica Antonella Caminati U.O. di Pneumologia e Terapia Semi Intensiva Servizio di Fisiopatologia Respiratoria ed Emodinamica Polmonare Osp.