Ketamine and Methadone Supra- Regional Audit Presentation
|
|
|
- Shanon Patterson
- 5 years ago
- Views:
Transcription
1 Ketamine and Methadone Supra- Regional Audit Presentation Audit Group: Alison Coackley, Anthony Thompson, Graham Whyte, Helen Bonwick, Ruth Clark, Agnes Noble, Aileen Scott, Andrew Dickman, Sarah Fradsham External Experts: Dr Anne Garry, Dr Kosta Levshankov
2 Background to audit Methadone re-audit New ketamine audit Supra- regional Two parts:- Health care professionals questionnaire, Prospective data collection in individual units
3 Plan for Presentation Methadone: Current Standards, Literature review, Audit results. Ketamine: Literature review, Audit results. Standards and Guidelines for methadone and ketamine. Comments from external experts Discussion
4 Ketamine literature review September 2012 Dr Anthony Thompson
5 Ketamine Revision Class general anaesthetic Indications anaesthesia, pain unresponsive to standard treatments Contraindications any situation where raised Blood Pressure/Intracranial pressure is hazardous. Acute Porphyria
6 Pharmacology 1 NMDA receptor channel complex Involved in developing central sensitisation of dorsal horn neurones which transmit pain signals At rest the channel is blocked by Magnesium ions
7 Pharmacology 2 But if prolonged stimulus and excitation the channel unblocks and Calcium moves into the cell This causes neuronal hyper excitability and reduction on opioid responsiveness, hyperalgesia and allodynia
8 Pharmacology 3 KETAMINE is the most potent NMDA receptor channel blocker available clinically Binds to the channel sites when open and activated Antagonises the hyper excitation state
9 Pharmacology 4 Multiple receptor activities Interacts with other calcium, sodium channels Dopamine receptors, cholinergic transmission, noradrenergic and serotonergic re-uptake and opioid-like and antiinflammatory effects
10 Pharmacology 5 Commercially available Ketamine is equal enantiomers of S(+) and R(-) forms of the drug Bioavailability - parenterally 93%, orally 17% Oral Ketamine Norketamine (equipotent)
11 Pharmacokinetics Bioavailability 93% intramuscular (im), 45% nasal, 30% sublingual, 30% PR, 20% oral (PO) Onset 5min im, min s/c, 30 min PO t ½ h im, 3h PO, Duration 30min-2h im, 4-6h PO
12 Cautions Psychiatric disorder, epilepsy, glaucoma, hypertension, cardiac failure, history of strokes Plasma concentration raised by diazepam, CYP3A4 inhibitors e.g. clarithromycin, ketoconazole
13 Undesirable effects Dose related Psychomimetic euphoria, dysphasia, blunted affect, vivid dreams and nightmares, inattention, memory, illusions, hallucinations, altered body image Delirium, dizziness, diplopia, blurred vision, nystagmus, hearing, HYPERTENSION, tachycardia, hyper salivation, nausea and vomiting, injection site erythema, URINARY TRACT TOXICITY
14 Urinary tract toxicity 1 Unclear of cause, direct irritation or metabolites Frequency, urgency, urge incontinence, dysuria, haematuria Interstitial cystitis, detrusor over activity, reduced bladder capacity, vesico-ureteric reflux, hydronephrosis, papillary necrosis, renal impairment
15 Urinary tract toxicity 2 If symptoms of urinary tract infection and NO evidence of bacterial infection, consider discontinuing and seeking Urology review Symptoms settle in a few weeks, gradual reduction in dose ideally to prevent pain escalation
16 The Literature Review
17 Cochrane Collaboration 2009 Bell, Eccleston and Kalso 2009 To determine the effectiveness of ketamine as an adjuvant to opioids in the treatment of cancer pain Medline, embase, cancerlit, Cochrane library Selection criteria adult, cancer, on opioid, received ketamine or placebo/active control
18 Cochrane Collaboration 2009 Data 4 RCTs (2 excluded, poor design) and 32 case studies Results 2 trials included, small numbers of patients Conclusion More RCTS needed, current evidence insufficient
19 Results 2 studies Mercandante 2000, Italy, Placebo, 3 hour trial Yang 1996, Taiwan, Morphine active control Both cross over trials
20 Mercandante patients 7 men 3 women years Pain unrelieved by morphine Diagnosed with neuropathic pain
21 Mercandante doses ketamine IV bolus 0.25mg/kg and 0.5mg/kg as adjuvant vs. normal saline 2 day washout between treatments No rescue doses described
22 Outcomes Mercandante 2000 Pain score at 30, 60, 90, 120, 180 minutes and adverse effects Pain score 0-10
23 Effectiveness 0.25mg/kg dose Mercandante 2000 Pain score reduced after 30 mins vs. normal saline After 60 mins effect lessened but some benefit even after 180 mins noted
24 0.5mg/kg dose Mercandante 2000 Significant reduction at 30 mins and maintained throughout the 180 mins
25 Yang hospital patients 10 men 10 women Cancer pain effectively treated with morphine
26 Yang 1996 Assessed intrathecal 1mg/kg ketamine as adjuvant vs. morphine alone Morphine dose titrated until stable 48 hours then randomly crossed over to morphine PLUS Ketamine or continued on morphine (control) alone, administered twice daily intrathecally No washout period Rescue doses available Morphine 5mg im
27 Yang 1996 Outcomes Patient pain score 0-10 Pain frequency Morphine dose Total morphine dose Total rescue doses Frequency of intrathecal titration
28 Yang 1996 Co-administration of ketamine reduced the dose of morphine needed Was as effective as intrathecal morphine alone
29 Adverse effects No withdrawals in either study Hallucinations commonest treated with diazepam Mild effects including light flashes, buzzing in head, insobriety, drowsy, nausea and vomiting, dry mouth, confusion
30 Conclusions No evidence based conclusion due to small numbers
31 32 case studies Opioid AND ketamine 246 patients Other Reports Various routes used po,im,s/c,iv,s/c infusion, epidural, intrathecal Various doses 1mg/kg/day s/c infusion to 600mg/day iv, 67.2mg/day intrathecal Various time scales 4 hours to 12 months
32 Case Studies Most used morphine, some fentanyl, hydromorphone, diamorphine or alone 16 reports described dramatic relief of refractory cancer pain Commonest adverse effects sedation and hallucinations One had sedation settling with opioid reduction Only 2 studies out of 32 had patient withdrawal
33 Case studies Inflamed infusion sites, nystagmus, hyperalgesia post cessation Post mortem myelopathy post intrathecal infusion with vasculitis Lloyd Williams s/c infusion sites, 0.1% hydrocortisone cream to maintain sites
34 Therapeutic Review Rachel Quibell, Eric Prommer, Mary Mihalyo, Andrew Wilcock and Robert Twycross Journal of Pain and Symptom Management Volume 41, March 2011 PCF 4 Chapter 13 Anaesthesia Page
35 Dose and Use Therapeutic Review Advise long term ketamine only if Burst has failed Due to renal tract concerns
36 50mg/5ml Co-administration Oral Ketamine 10-25mg TDS/QDS and PRN Titrate up in steps to 100mg QDS Consider dose reduction if drowsy/psychomimetic issues Can be opioid sparing effect
37 Oral Ketamine Some centres attempt withdrawal over several weeks Benefit can persist with out ketamine for weeks/months
38 Maximal dilution 0.9% saline 100mg/24 hrs. Burst Ketamine If not effective increase to 300mg/24 hrs. If not effective again, increase to 500 mg/24 hrs. Stop 3 days after last dose increment Prophylactic use
39 Other Routes Sublingual (s/l) Subcutaneous stats (s/c) Intravenous (IV) Continuous IV Infusion (CIVI)
40 Opioid reduction Some centres reduce regular opioid dose 25-50% when starting parenteral ketamine
41 Other Papers of Interest The use of Ketamine in severe cases of refractory pain syndromes in the palliative care setting : A case series Kerr et al, Buffalo, New York Journal Of Palliative Medicine, Volume 14, Number 9, complex cases, non-cancer
42 Sub-anaesthetic doses unresponsive to escalating opioid doses Sickle cell, paraplegia, multiple issues including Chronic Obstructive Pulmonary Disease, Ischaemic heart disease, Raynaud`s, quadriplegia 2 used CIVI, 2 used CSCI Ketamine Conclusion ketamine has a role in reducing opioid tolerance and hyperalgesia, few side effects
43 Kate Jackson et al, Victoria, Australia 2001 Burst Ketamine for refractory cancer pain: an open label audit of 39 patients (J. Of Pain and Symptom Management Vol. 22 No 4 p834) 2010 The effectiveness and adverse effects profile of Burst Ketamine in refractory cancer pain (J. of Palliative acre Autumn 2010;26,3)
44 2001 Study Multi centre unblinded open label audit39 patients 18 month study, 4 Pall Care Centres Short duration Ketamine (3-5 days) 100mg-300mg-500mg per 24 hours CSCI 43 pains 29 responded Response rate 67% 24/29 maintained good pain control (8 week max.)
45 2001 Study 12 had adverse Psychomimetic effects Dose related Cancer patients Taking opioid, NSAIDS and neuropathic agents Suggested need for further investigation into the place of Ketamine in cancer pain management
46 2010 Study The VCOG PM1-100 Study Multi centre study Response rate 22/44 i.e. 50% 100mg-300mg-500mg per 24 hrs. CSCI Would the early promising results continue Open label study of effectiveness and incidence of adverse effects (AE) 53 patients registered, 44 eligible aged 35-82, 21 men 23 women
47 2010 Study 77% needed 300mg or more, 41% needed 500mg Response rate dropped to 50% but 9% had complete response (pain free) Ketamine role not purely for neuropathic pain, but bone metastases with nerve damage Dose related AE Cardiovascular stability noted
48 Need RCTs Blinded 2010 Study Conclusions Limited opportunities in Palliative Care Difficult to blind with AE being noticeable The lack of level I and II evidence should NOT preclude the use of Ketamine Burst Treatment
49 Other Nuggets Burst Ketamine to reverse opioid tolerance in cancer pain Letter to editor, Mercandante, J. Pall. Med. Vol. 25 No. 4 p Case reports Hyper excited opioid excess state Ketamine as co-analgesic OR reversal of opioid tolerance
50 Ketamine Mouthwash 1 Cooney et al EAPC 2011 Palliative Care Department, Dooraradoyle, Limerick Retrospective study 12 months Patients who received the mouthwash Dose, number of doses, duration, concurrent analgesics, adverse effects
51 Ketamine Mouthwash 2 Received Ketamine 20mg in 10ml Bioxtra mouthwash, 6 hourly, swish and spit All were head and neck, post radiotherapy (DXT) Useful and safe Mild stinging when first used only
52 Ketamine Mouthwash 3 Slatkin et al, Pain Medicine, Volume 4, number 3, 2003 Duarte, California Topical ketamine in the treatment of mucositis pain Case study, 32 year old lady, DXT Unclear if local or systemic effect Anti-inflammatory? Sodium channel?
53 Mercandante Letter 2003 Possible hyperalgesic effect of opioids NMDA receptor involved Development of this reversed/shifted by NMDA antagonists Wind up increased neuronal response to repeated stimuli Ketamine inhibits this wind up Reversal of central changes resets the nerve system
54 A Randomised Controlled Trial D.Currow, J Hardy et al Brisbane, Sydney, Adelaide Randomised double blind controlled multi centre study of subcutaneous ketamine in the management of cancer pain
55 Currow and Hardy et al Stable opioid dose Severe pain Adequate co-analgesics Randomised to Placebo or Ketamine mg per 24 hrs. CSCI Response greater than 2 point drop in BPI scale Pain score day 6 end point
56 Currow and Hardy et al Results 185 patients March February 2011 High placebo response 26/92 (28%) with no difference between placebo and active arms Trial does NOT support the role of s/c Ketamine in the treatment of cancer pain in advanced cancer
57 Urinary tract damage Storr et al, Cumbria, Palliative Medicine, 2009 ; 23: Describes 3 cases developing significant urological symptoms Case 1- oral 50mg QDS Case 2 oral 170mg QDS Case 3 oral 200mg QDS Temporal link
58 Refractory Depression Intravenous Ketamine Burst for refractory depression in a patient with advanced cancer Stefanczky-Saphieha et al, J. Palliative Medicine, Vol. 11, No.9, 2008, Toronto Studies in non cancer suggest NMDA antagonist role in rapid improvement from severe depression, even single Iv doses Burst Ketamine used with success for major depressive disorder in advanced cancer Suggest RCTs
59 Role of Ketamine in Analgesia Literature review, Legge et al, West Virginia, USA American society of consultant pharmacists vol.21, issue 1, 2006 Medline, Cochrane Conclusion Useful with Opioids
60 Palliative Sedation Letter J. of Pain and Symptom management Vol.36 no.4 October 2008 Carter et al, Bristol Case study 100mg IV, 300mg agitated, settled with 500mg rapidly IV Monotherapy role (?)
61 Conversion from s/c to oral J. of Pain and Symptom management. Vol.41, No.6, June 2011 Benitez-Rosario et al, Tenerife A strategy for conversion from s/c to oral Ketamine in Cancer Patients: Effect of a 1:1 Ratio 29 patients enrolled Stable on s/c ketamine
62 Conversion from s/c to oral Converted to oral ketamine for maintenance Mean s/c dose 300mg/24 hours Used 1:1 ratio Given TDS Close monitoring No adverse effects reported
63 And finally from me
64 Systematic review Hocking and Cousins Ketamine in chronic pain management: an evidence based review Anaesthetic Analgesia. 2003;97: Good therapeutic response to parenteral ketamine suggests oral response
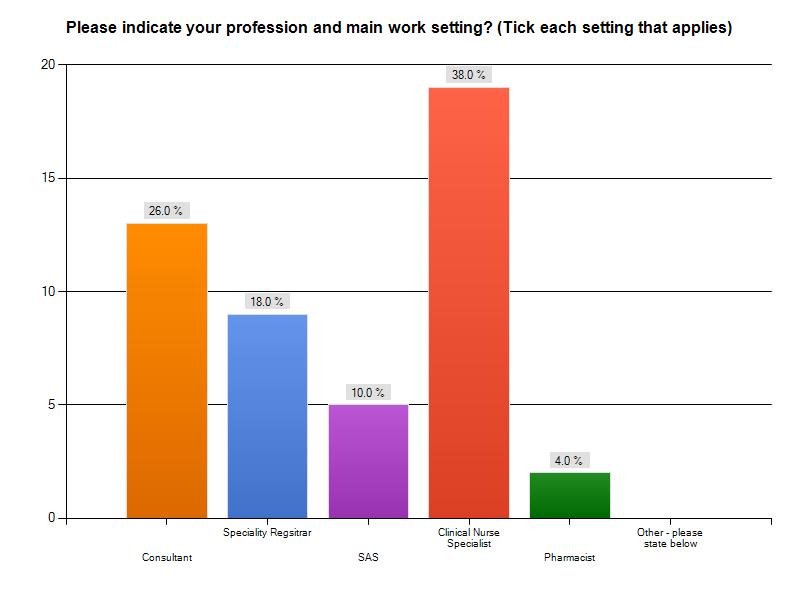
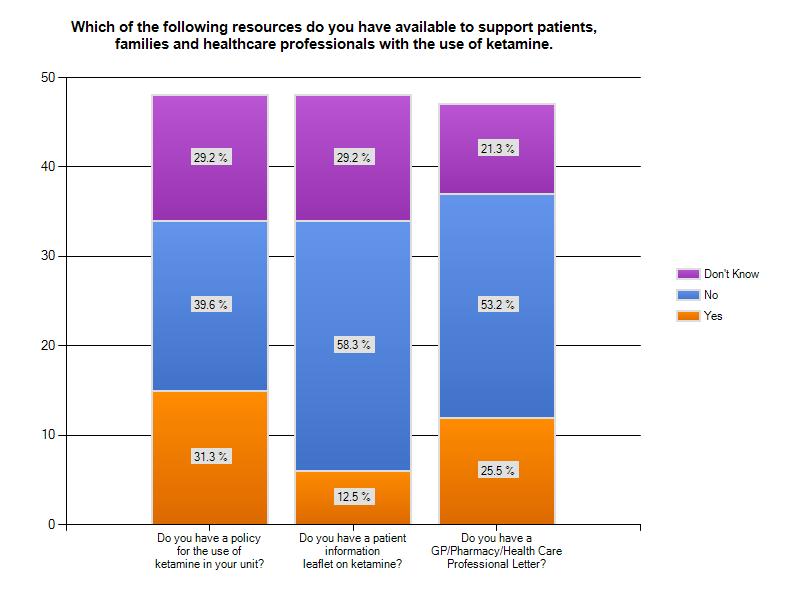
65 Ketamine and Methadone Practice and Experience Survey Supra Regional Survey Monkey Questionnaire Ketamine 50 responses Methadone 46 responses Dr Graham Whyte
66 Ketamine Results (n=50) 66

67 67
68 68

69 Yes 58% No 40% 69
70 70
71 Professions involved in starting Ketamine in last 12months Confidence by profession Consultants 85% StR 78% SSAS 80% CNS 21% Consultants 8.4/10 StR s 5.6/10 SSAS 5.4/10 CNS 1.6/10 71
72 Methadone Comparative Professional Group % Converted to Methadone past 12 months Consultant 54% 6.8/10 StR 38% 4.8/10 SSAS 60% 5.6/10 CNS 0% 1.6/10 Average Confidence Level in Initiating Methadone 72

73 73
74 Examples of doses used: Haloperidol-burst ketamine 3mg in driver with ketamine oral ketamine - 1.5mg nocte and PRN available Haloperidol oral and sc- 1.5mg stat or up to 5mg over 24 hours Diazepam oral 2.5 mg up to tds Midazolam sc 2.5-5mg stat and 5-10mg via CSCI If giving Ketamine orally I would prescribe oral haloperidol mg od. If giving Ketamine s/c I may prescribe S/C haloperidol 3-5mg but may also give it orally 74
75 What route of administration do you use? Equal preference for Burst and Oral Ketamine Burst 100mg/24 hours upto 500mg/24 hrs 5-7 days Oral 10 mg tds most common dosage. 75
76 Burst ketamine; easier to administer and control in the inpatient setting severe - burst, less severe- oral/if low mood like oral too Oral ketamine as regime I am most familiar with My experience is primarily with burst ketamine so I would have preference for this Depends on the patient and no preferred regime 76
77 77
78 78

79 79
80 Prospective data collection of current practice : Ketamine results Dr Aileen Scott
81 ICN
82 Sex
83 Age
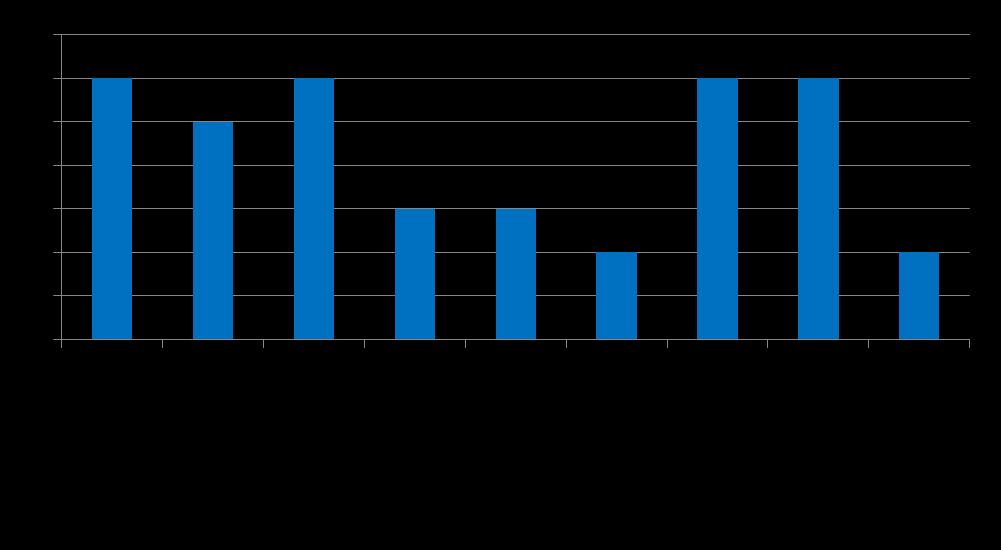
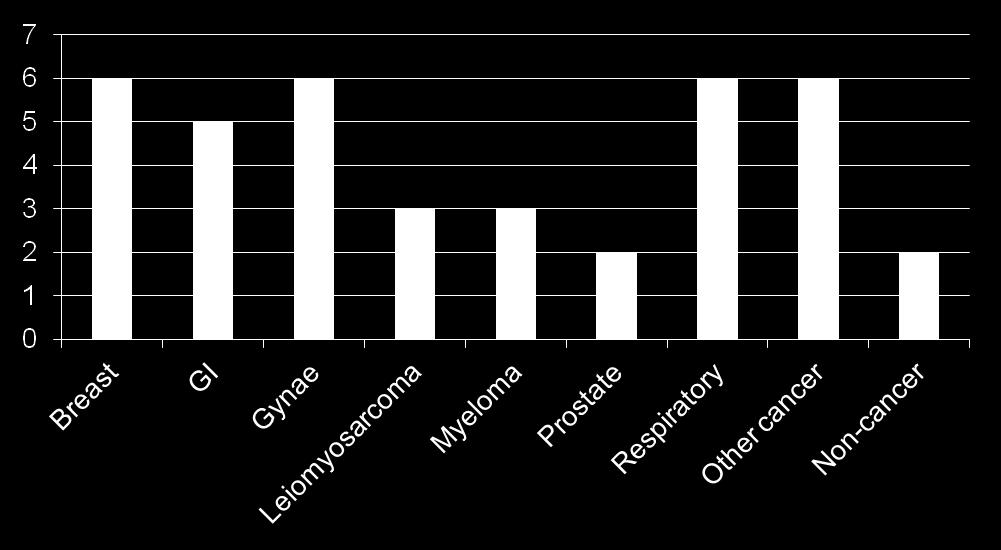
84 Diagnosis
85 Setting

86 Is this the patient s first use of ketamine?
87 Indication for ketamine

88 Pre-use checks

89 Route used
90 Ketamine mouthwash Used in one patient for oral mucosal pain No concurrent medication prescribed Commenced at 10mg BD and continued and discharged on this dose


91 Reasons for using oral ketamine
92 Oral ketamine Starting dose range 5-20mg TDS Maximum dose range mg TDS


93 Reasons for using subcutaneous ketamine
94 Burst ketamine regimens Starting dose range: mg over 24 hours Maximum dose range: mg over 24 hours
95 Burst ketamine Additional medications prescribed
96 Subcutaneous infusion regimens Starting dose range: mg over 24 hours Maximum dose range: mg over 24 hours Various regimens used Titrated in increments of 50mg and 100mg over varying numbers of days In 2 cases doses did not change
97 Subcutaneous ketamine Additional medication prescribed
98 Diluent used

99 Checks after ketamine commenced

100 Were any side effects observed?


101 What adjuvants were used prior to starting ketamine?

102 How much opioid was the patient on prior to starting ketamine?

103 Did the patient s opioid dose change following commencement of ketamine?
104 Patients converted from SC to oral ketamine Patient 1 100mg/24 hours to 20mg TDS Patient 2 500mg/24 hours to 10mg TDS Patient 3 400mg/24 hours to 10mg TDS
105 Was the patient discharged on ketamine?

106 On discharge, who was provided with information about ketamine?

107 What follow-up was arranged for the patient?


108 Was the patient pain-free at 4 weeks?
109 Ketamine Standards and Guidelines Dr Sarah Fradsham
110 General principles in the Use of Ketamine
111 Introduction Ketamine is a drug used for the induction and maintenance of general anaesthesia Ketamine has a role in treatment of pain unresponsive to standard treatments (e.g. neuropathic, inflammatory, ischaemic, procedural pains) 1,2,3 Ketamine is a dissociative anaesthetic with analgesic properties at sub-anaesthetic doses 3,5
112 The NMDA receptor channel is involved with sensitisation of the dorsal horn neurones which transmit pain signals. Prolonged stimulation (pain) causes hyper excitability and reduced opioid responsiveness, hyperalgesia and allodynia 4.
113 Ketamine is a potent NMDA receptor channel blocker, as well as other actions on the following channels calcium, sodium, dopamine, cholinergic, noradrenergic, serotonergic reuptake and opioid-like effects and anti-inflammatory effects 6,7
114 Ketamine has been used as an analgesic in many clinical settings including post-operative, chronic non-cancer pain, cancer pain, and procedural pain (e.g. burns dressings) and painful mucositis 8,9. in cancer pain, ketamine has been used mainly ORALLY (PO) or SUBCUTANEOUSLY (CSCI)
115 Subcutaneous use can be Burst (see below) or more prolonged subcutaneous use. Side effects are dose related. 40% occurrence with CSCI, less so with PO. Ketamine abuse is common on the street and associated with adverse media attention as a result.
116 Ketamine can cause urinary tract problems, tachycardia, hypertension and intracranial hypertension and Psychomimetic side effects e.g. vivid dreams, hallucinations, altered body image and mood. These psychomimetic side effects can be managed with Midazolam and/or haloperidol. Co-administration is recommended 11,12 (see manufacturers PI)
117 Ketamine undergoes extensive first pass metabolism Mainly to Norketamine As an analgesic it is equipotent to parenteral ketamine 10
118 Less than 10% is excreted unchanged, half in the faeces and half renally. Norketamine is renally excreted and long term use leads to hepatic enzyme induction and enhanced ketamine metabolism.
119 Formulations and Supply Oral solution Made to order Sugar free Made to order Martindale e.g 50mg/5ml (other strengths are avaliable) Different flavours Unlicensed
120 Preparation of oral Ketamine:Pharmacy Guidelines Use 100mg/ml 10ml vials (cheapest) To prepare 100ml 50mg/5ml oral solution 10ml vial of ketamine 100mg/ml 90ml purified water Refrigerate Use within a week of manufacture Not recommended to do in ward environment
121 Injectable preparations Pfizer 10mg/ml 20ml ampoule 50mg/ml 10ml ampoule 100mg/ml 10ml ampoule Off label
122 Guidelines
123 Guidelines Ketamine for pain control should be initiated by a Palliative care physician experienced in the use of ketamine. This is usually done in a specialist palliative care inpatient unit. [Level 4] The majority of the evidence for the use of ketamine for pain control supports the use of burst ketamine. This is therefore recommended as first line treatment. Long term ketamine is only recommended if burst ketamine has failed due to concerns regarding urinary tract toxicity. [Level 4] Suggested doses and regimes are described in Table 1.
124 Table 1- Doses and Regimens [Level 4]
125 Guidelines cont Compatibility in syringe drivers [Level2] For subcutaneous regimens it is recommended that ketamine is diluted with sodium chloride 0.9%. When giving subcutaneous ketamine via a syringe driver it is compatible with morphine plus additional drugs when mixed with sodium chloride 0.9% 13. Box A describes compatibility data for drug mixtures containing ketamine.
126 Box A. Compatibility data
127 Guidelines- Monitoring Ketamine can cause tachycardia and intracranial hypertension. Due to this the blood pressure and pulse rate should be checked prior to the commencement of ketamine and twice daily during the dose titration phase or throughout the duration of burst ketamine. [Level 4] If the pulse rate rises above 20bpm from baseline or above 100bpm or the the blood pressure rises by 20mmHg on consecutive readings, a dose reduction should be considered. If the pulse rate or blood pressure does not return to baseline readings with a dose reduction then ketamine should be discontinued. [Level 4]
128 Guidelines- Monitoring As ketamine has an opiate sparing effect, patients should be monitored for signs of opiate toxicity. During the dose titration phase this should include twice daily monitoring of respiratory rate along with blood pressure and pulse rate as described above. The patients conscious level should also be monitored and if there is any concern regarding opiate toxicity the patient should be reviewed by a clinician and consideration of a dose reduction of the regular opiates should be made. [Level 4] ( see opiate reduction below)
129 Guidelines- Monitoring To assess the effectiveness of ketamine patients should have pain scores recorded prior to the commencement of ketamine and twice daily during the dose titration phase. This will help to establish whether further incremental increases in the doses are needed. Pain scores should also be recorded at follow up reviews for patients on long term ketamine or those that have received burst ketamine to establish ongoing effectiveness of pain control. [Level 4] For those patients maintained on long term ketamine reassessment should be carried out by a palliative care specialist monthly or sooner depending on symptoms or clinical need. [Level 4]
130 Guidelines- Opioid reduction As ketamine has an opiate sparing effect a dose reduction of 25% should be considered in those patients commencing parenteral or oral ketamine or if patients develop signs of opiate toxicity. [Level 4] All units commencing ketamine should ensure naloxone is available for use in the case of respiratory depression associated with opiate overdose/ toxicity. [Level 4] Use of ketamine is not recommended in patients on transdermal opioids due to the risk of opiate toxicity. In these patients an opiate conversion should be considered prior to commencing ketamine. [Level 4]
131 Guidelines- Conversions [Level 4] Evidence regarding conversions is limited however, when converting from PO ketamine to Subcutaneous ketamine for use in a CSCI, a conversion of 1:1 is suggested PO ketamine undergoes extensive first pass hepatic metabolism to norketamine which provides the main analgesic effect. The maximum blood concentration of norketamine is greater after PO administration than after parenteral administration therefore when converting from SC:PO a conversion of 3:1 is suggested. In both cases, there should be the provision for close monitoring and ability to alter the dose as necessary.
132 Guidelines- Adjuvant medications Ketamine can cause undesirable psychomimetic effects such as hallucinations, euphoria, vivid dreams which can be distressing to patients. It is therefore suggested that ketamine is given concurrently with midazolam or haloperidol to control any undesirable effects. [Level 4] Suggested doses include Haloperidol 2mg-5mg po nocte or 2mg-5mg via CSCI over 24hrs or Midazolam 5mg-10mg via CSCI. [Level 4]
133 Guidelines- Urinary Toxicity Ketamine has been linked to urinary tract toxicity including interstitial cystitis, papillary necrosis and renal impairment. If a patient develops symptoms of a urinary tract infection and there is NO evidence of bacterial infection consider discontinuing the ketamine. The patient may require a urology review. [Level 4]
134 Guidelines- Discharge Patients discharged on ketamine should be followed up by a specialist palliative care clinician within 4 weeks to review pain control. [Level 4] Dose alterations of ketamine should be undertaken in a specialist inpatient unit or after specialist palliative care outpatient review. [Level 4] When a patient is discharged on ketamine standardised information should be give to the patients, GP and community pharmacist. [Level 4]
135 Guidelines Discharge Units should liaise with the patients GP and community pharmacy prior to discharge to confirm future supplies of ketamine. [Level 4] Patients on oral ketamine should be aware that they need to request a repeat prescription at least 7 days in advance of their own supply running out. [Level 4] Units should consider the use of a ketamine card to be given to patients on discharge to inform other health professionals that the patient is on ketamine. [Level 4]
136 Standards
137 Standards The decision to commence ketamine, the indication and regimen to be used should be clearly documented in the patient s case notes. [Grade D] Prior to commencing ketamine, the patient s heart rate, blood pressure, respiratory rate and pain score should be recorded. These should be rechecked twice daily until ketamine is discontinued or the titration is complete. [Grade D] If administering ketamine via a subcutaneous infusion, then sodium chloride 0.9% should be used for dilution. [Grade D] Ketamine should always be prescribed in milligrams (mg). [Grade D]
138 Standards If a patient is discharged on ketamine, the discharge letter should include a named contact and telephone number for further advice. [Grade D] For patients who are discharged on ketamine, units should have standardised information to give to the patient, their GP and community pharmacist. [Grade D] Patients discharged on ketamine (oral or subcutaneous) should have at least monthly follow-up with a Palliative Medicine clinician experienced in the use of ketamine. [Grade D] Specialist Palliative Care units should have a policy for the use of ketamine as an analgesic. [Grade D]
139 Ketamine References 1. Persson J et al The analgesic effect of racemic ketamine in patients with chronic ischaemic pain due to lower extremity arteriosclerosis obliterans. Acta Anaesthesilogica Scandinavica 42: Graven-Nielsen T et al (2000) Ketamine reduces muscle pain, temporal summation and referred pain in fibromyalgic patients. Pain 85: Visser E and Schug SA (2006) The role of Ketamine in pain management Biomed pharmocother. 60 :
140 4. Elliott K et al (1994) The NMDA receptor antagonists, LY and MK-801, and the nitric oxide synthase inhibitor, NG-nitro-L-arginine, attenuate analgesic tolerance to the mu-opioid morphine but not kappa opioids. Pain. 56 : Fallon MT and Welsh J (1996) The role of ketamine in pain control. European Journal of Palliative Care. 3: Meller S et al (1996) Ketamine : relief from chronic pain through actions at the NMDA receptor? Pain. 68:
141 7. Kawasaki C et al (2001) Ketamine isomers suppress superantigen-induced proinflammatory cytokine production in human whole blood. Can J Anaesthes. 48 : Richardson P and Mustard L (2009) The management of pain in the burns unit. Burns. 35 : Slatkin NE and Rhiner M (2003) Topical ketamine in the treatment of mucositis pain. Pain Medicine. 4:
142 10. Hizaji Y et al (2002) Contribution of CYP3A4, CYP2B6 and CYP2C9 isoforms to N-demethylation of ketamine in human liver microsomes. Drug Metabolism & Disposition. 30 : Chu PS et al (2008) The destruction of the lower urinary tract by ketamine abuse : anew syndrome? BJU Int. 102 : Palliative Care Formulary Quibell R et al. Therapeutic review: Journal of Pain and Symptom Management Volume 41, March Dickman A. Drugs in palliative care. OUP.
143 Time to hear from the experts...

144 Any Questions?
Ketamine. Ruth Clark and Kath Mitchell
 Ketamine Ruth Clark and Kath Mitchell Aims and Objectives To give an overview of mechanism of action of ketamine To give a brief Literature Review To review dosing, routes of administration, side effects,
Ketamine Ruth Clark and Kath Mitchell Aims and Objectives To give an overview of mechanism of action of ketamine To give a brief Literature Review To review dosing, routes of administration, side effects,
Ketamine and Methadone Supra- Regional Audit Presentation
 Ketamine and Methadone Supra- Regional Audit Presentation Audit Group: Alison Coackley, Anthony Thompson, Graham Whyte, Helen Bonwick, Ruth Clark, Agnes Noble, Aileen Scott, Andrew Dickman, Sarah Fradsham
Ketamine and Methadone Supra- Regional Audit Presentation Audit Group: Alison Coackley, Anthony Thompson, Graham Whyte, Helen Bonwick, Ruth Clark, Agnes Noble, Aileen Scott, Andrew Dickman, Sarah Fradsham
SHARED CARE GUIDELINE FOR THE USE OF KETAMINE (oral and subcutaneous injection) FOR ANALGESIA IN ADULT PALLIATIVE CARE PATIENTS
 FOR ANALGESIA IN ADULT PALLIATIVE CARE PATIENTS") BEDFORDSHIRE AND LUTON JOINT PRESCRIBING COMMITTEE SHARED CARE GUIDELINE FOR THE USE OF KETAMINE (oral and subcutaneous injection) FOR ANALGESIA IN ADULT PALLIATIVE CARE PATIENTS PATIENT S NAME: PATIENT
BEDFORDSHIRE AND LUTON JOINT PRESCRIBING COMMITTEE SHARED CARE GUIDELINE FOR THE USE OF KETAMINE (oral and subcutaneous injection) FOR ANALGESIA IN ADULT PALLIATIVE CARE PATIENTS PATIENT S NAME: PATIENT
Ketamine and Methadone Supra- Regional Audit Presentation
 Ketamine and Methadone Supra- Regional Audit Presentation Audit Group: Alison Coackley, Anthony Thompson, Graham Whyte, Helen Bonwick, Ruth Clark, Agnes Noble, Aileen Scott, Andrew Dickman, Sarah Fradsham
Ketamine and Methadone Supra- Regional Audit Presentation Audit Group: Alison Coackley, Anthony Thompson, Graham Whyte, Helen Bonwick, Ruth Clark, Agnes Noble, Aileen Scott, Andrew Dickman, Sarah Fradsham
NEUROPATHIC CANCER PAIN STANDARDS AND GUIDELINES
 NEUROPATHIC CANCER PAIN STANDARDS AND GUIDELINES GENERAL PRINCIPLES Neuropathic pain may be relieved in the majority of patients by multimodal management A careful history and examination are essential.
NEUROPATHIC CANCER PAIN STANDARDS AND GUIDELINES GENERAL PRINCIPLES Neuropathic pain may be relieved in the majority of patients by multimodal management A careful history and examination are essential.
GUIDELINES FOR CONVERSION FROM A STRONG OPIOID TO METHADONE
 GUIDELINES FOR CONVERSION FROM A STRONG OPIOID TO METHADONE GENERAL PRINCIPLES Methadone may be used as a strong opioid alternative when severe cancer-related pain responds poorly to other opioids, or
GUIDELINES FOR CONVERSION FROM A STRONG OPIOID TO METHADONE GENERAL PRINCIPLES Methadone may be used as a strong opioid alternative when severe cancer-related pain responds poorly to other opioids, or
SHARED CARE GUIDELINE For
 SHARED CARE GUIDELINE For Ketamine in Palliative Care Implementation Date: 26.1.2011 Review Date: 26.1.2013 This guidance has been prepared and approved for use within Gateshead in consultation with Primary
SHARED CARE GUIDELINE For Ketamine in Palliative Care Implementation Date: 26.1.2011 Review Date: 26.1.2013 This guidance has been prepared and approved for use within Gateshead in consultation with Primary
GUIDELINES ON THE MANAGEMENT OF PAIN DUE TO CANCER IN ADULTS
 GUIDELINES ON THE MANAGEMENT OF PAIN DUE TO CANCER IN ADULTS Bristol Palliative Care Collaborative Contact Numbers: Hospital Specialist Palliative Care Teams: North Bristol 0117 4146392 UH Bristol 0117
GUIDELINES ON THE MANAGEMENT OF PAIN DUE TO CANCER IN ADULTS Bristol Palliative Care Collaborative Contact Numbers: Hospital Specialist Palliative Care Teams: North Bristol 0117 4146392 UH Bristol 0117
Palliative Care and the Critical Role of the Pharmacist. Arti Thakerar Education/ Palliative Care Peter MacCallum Cancer Centre
 Palliative Care and the Critical Role of the Pharmacist Arti Thakerar Education/ Palliative Care Peter MacCallum Cancer Centre Overview What is palliative care Role of a pharmacist in palliative care Issues
Palliative Care and the Critical Role of the Pharmacist Arti Thakerar Education/ Palliative Care Peter MacCallum Cancer Centre Overview What is palliative care Role of a pharmacist in palliative care Issues
PAIN AND SYMPTOM MANAGEMENT GUIDANCE IN THE LAST DAYS OF LIFE
 PAIN AND SYMPTOM MANAGEMENT GUIDANCE IN THE LAST DAYS OF LIFE Reference: DCM029 Version: 1.1 This version issued: 07/06/18 Result of last review: Minor changes Date approved by owner (if applicable): N/A
PAIN AND SYMPTOM MANAGEMENT GUIDANCE IN THE LAST DAYS OF LIFE Reference: DCM029 Version: 1.1 This version issued: 07/06/18 Result of last review: Minor changes Date approved by owner (if applicable): N/A
PRESCRIBING GUIDELINES FOR SYMPTOM MANAGEMENT IN THE DYING PATIENT
 PRESCRIBING GUIDELINES FOR SYMPTOM MANAGEMENT IN THE DYING PATIENT A collaboration between: St. Rocco s Hospice, Bridgewater Community Healthcare NHS Trust, NHS Warrington Clinical Commissioning Group,
PRESCRIBING GUIDELINES FOR SYMPTOM MANAGEMENT IN THE DYING PATIENT A collaboration between: St. Rocco s Hospice, Bridgewater Community Healthcare NHS Trust, NHS Warrington Clinical Commissioning Group,
Supporting Last Days of Life Symptom Control Medication Guidance: Algorithm. Agitation & Anxiety
 Agitation & Anxiety (Exclude or treat REVERSIBLE causes*) Patient is anxious / frightened, but lucid Patient is confused, agitated and / or hallucinating MIDAZOLAM 2.5-5mg s/c (Max total 24 hour dose of
Agitation & Anxiety (Exclude or treat REVERSIBLE causes*) Patient is anxious / frightened, but lucid Patient is confused, agitated and / or hallucinating MIDAZOLAM 2.5-5mg s/c (Max total 24 hour dose of
LINCOLNSHIRE Clinical Commissioning Groups in association with UNITED LINCOLNSHIRE HOSPITALS TRUST
 LINCOLNSHIRE Clinical Commissioning Groups in association with UNITED LINCOLNSHIRE HOSPITALS TRUST SHARED CARE GUIDELINE: Ketamine for use in palliative care for the management of pain unresponsive to
LINCOLNSHIRE Clinical Commissioning Groups in association with UNITED LINCOLNSHIRE HOSPITALS TRUST SHARED CARE GUIDELINE: Ketamine for use in palliative care for the management of pain unresponsive to
Specialist Palliative Care Audit and Guidelines Group (SPAGG)
") Specialist Palliative Care Audit and Guidelines Group (SPAGG) Clinical Guideline for the Prescribing and Administration of Furosemide via continuous subcutaneous infusion (CSCI) for Heart Failure Patients
Specialist Palliative Care Audit and Guidelines Group (SPAGG) Clinical Guideline for the Prescribing and Administration of Furosemide via continuous subcutaneous infusion (CSCI) for Heart Failure Patients
The Role of Ketamine in the Management of Complex Acute Pain
 The Role of Ketamine in the Management of Complex Acute Pain Dr James Bennett Consultant Anaesthetist Consultant Lead for Inpatient Pain Service East Sussex Healthcare NHS Trust STAPG Committee Member
The Role of Ketamine in the Management of Complex Acute Pain Dr James Bennett Consultant Anaesthetist Consultant Lead for Inpatient Pain Service East Sussex Healthcare NHS Trust STAPG Committee Member
Supportive Care. End of Life Phase
 Supportive Care End of Life Phase Guidelines for Health Care Professionals In the care of patients with established renal failure who are in the last days of life References: Chambers E J (2004) End of
Supportive Care End of Life Phase Guidelines for Health Care Professionals In the care of patients with established renal failure who are in the last days of life References: Chambers E J (2004) End of
ANTICIPATORY PRESCRIBING FOR PATIENTS AT END OF LIFE WITH RENAL IMPAIRMENT
 ANTICIPATORY PRESCRIBING FOR PATIENTS AT END OF LIFE WITH RENAL Doses of opiates must be proptional to current analgesic medication Please refer ALL patients on Methadone Ketamine to SPCT f advice. Patients
ANTICIPATORY PRESCRIBING FOR PATIENTS AT END OF LIFE WITH RENAL Doses of opiates must be proptional to current analgesic medication Please refer ALL patients on Methadone Ketamine to SPCT f advice. Patients
Palliative Care Impact Survey
 September 2018 Contents Introduction...3 Headlines...3 Approach...4 Findings...4 Which guideline are used...4 How and where the guidelines are used...6 Alternative sources of information...7 Use of the
September 2018 Contents Introduction...3 Headlines...3 Approach...4 Findings...4 Which guideline are used...4 How and where the guidelines are used...6 Alternative sources of information...7 Use of the
Analgesia. This is widely used in palliative care. It has antipyretic and analgesic effects but no anti-
 Page 1 of 8 Analgesia The World Health Organisation (WHO, 1990) has devised a model to assist health care professionals in the management of cancer pain. The recommendations include managing pain, by the
Page 1 of 8 Analgesia The World Health Organisation (WHO, 1990) has devised a model to assist health care professionals in the management of cancer pain. The recommendations include managing pain, by the
1. GUIDELINES FOR THE MANAGEMENT OF AGITATION IN ADVANCED CANCER
 1. GUIDELINES FOR THE MANAGEMENT OF AGITATION IN ADVANCED CANCER 1.1 GENERAL PRINCIPLES There are many causes of agitation in palliative care patients, which makes recommendations for treatment difficult.
1. GUIDELINES FOR THE MANAGEMENT OF AGITATION IN ADVANCED CANCER 1.1 GENERAL PRINCIPLES There are many causes of agitation in palliative care patients, which makes recommendations for treatment difficult.
Syringe driver in Palliative Care
 Syringe driver in Palliative Care Introduction: Syringe drivers are portable, battery operated devices widely used in palliative care to deliver medication as a continuous subcutaneous infusion over 24
Syringe driver in Palliative Care Introduction: Syringe drivers are portable, battery operated devices widely used in palliative care to deliver medication as a continuous subcutaneous infusion over 24
Palliative Prescribing - Pain
 Palliative Prescribing - Pain LAURA BARNFIELD 21/2/17 Aims To understand the classes of painkillers available in palliative care To gain confidence in counselling regarding opiates To gain confidence prescribing
Palliative Prescribing - Pain LAURA BARNFIELD 21/2/17 Aims To understand the classes of painkillers available in palliative care To gain confidence in counselling regarding opiates To gain confidence prescribing
End of life prescribing guidance
 End of life prescribing guidance Introduction This guidance has been prepared to ASSIST IN DECISION MAKING for the prescribing and monitoring of medicines useful in the management of symptoms commonly
End of life prescribing guidance Introduction This guidance has been prepared to ASSIST IN DECISION MAKING for the prescribing and monitoring of medicines useful in the management of symptoms commonly
EAST LANCASHIRE GUIDELINES FOR THE MANAGEMENT OF SYMPTOMS IN THE LAST DAYS OF LIFE
 EAST LANCASHIRE SPECIALIST PALLIATIVE CARE TEAM EAST LANCASHIRE GUIDELINES FOR THE MANAGEMENT OF SYMPTOMS IN THE LAST DAYS OF LIFE Reviewed and updated August 2009 Next review date August 2011 Approved
EAST LANCASHIRE SPECIALIST PALLIATIVE CARE TEAM EAST LANCASHIRE GUIDELINES FOR THE MANAGEMENT OF SYMPTOMS IN THE LAST DAYS OF LIFE Reviewed and updated August 2009 Next review date August 2011 Approved
PAIN MANAGEMENT Patient established on oral morphine or opioid naive.
 PAIN MANAGEMENT Patient established on oral morphine or opioid naive. Important; It is the responsibility of the prescriber to ensure that guidelines are followed when prescribing opioids. Every member
PAIN MANAGEMENT Patient established on oral morphine or opioid naive. Important; It is the responsibility of the prescriber to ensure that guidelines are followed when prescribing opioids. Every member
Symptom Management Guidelines for End of Life Care
 Symptom Management Guidelines for End of Life Care The following pages are guidelines for the management of common symptoms in the last few days of life. General principles: 1. Consider how symptoms can
Symptom Management Guidelines for End of Life Care The following pages are guidelines for the management of common symptoms in the last few days of life. General principles: 1. Consider how symptoms can
PAIN MANAGEMENT Person established taking oral morphine or opioid naive.
 PAIN MANAGEMENT Person established taking oral morphine or opioid naive. Important; it is the responsibility of the prescriber to ensure that guidelines are followed when prescribing opioids. Every member
PAIN MANAGEMENT Person established taking oral morphine or opioid naive. Important; it is the responsibility of the prescriber to ensure that guidelines are followed when prescribing opioids. Every member
Care of the Dying. For dosing in severe renal impairment see separate guidance for care of the dying in severe renal failure.
 Care of the Dying Early diagnosis of the dying process allows for adequate preparation of the patient, the family and the carers. This clinical guidance covers the prescribing and management of patients
Care of the Dying Early diagnosis of the dying process allows for adequate preparation of the patient, the family and the carers. This clinical guidance covers the prescribing and management of patients
Controlled Document Number: Version Number: 1. Controlled Document Sponsor: Controlled Document Lead (Author): On: July Review Date: July 2020
: On: July Review Date: July 2020") Guidelines for the Use of Naloxone in Palliative Care in Adult Patients CONTROLLED DOCUMENT CATEGORY: CLASSIFICATION: Controlled Document Number: Version Number: 1 Controlled Document Sponsor: Controlled
Guidelines for the Use of Naloxone in Palliative Care in Adult Patients CONTROLLED DOCUMENT CATEGORY: CLASSIFICATION: Controlled Document Number: Version Number: 1 Controlled Document Sponsor: Controlled
GUIDELINES AND AUDIT IMPLEMENTATION NETWORK
 GUIDELINES AND AUDIT IMPLEMENTATION NETWORK General Palliative Care Guidelines The Management of Pain at the End Of Life November 2010 Aim To provide a user friendly, evidence based guide for the management
GUIDELINES AND AUDIT IMPLEMENTATION NETWORK General Palliative Care Guidelines The Management of Pain at the End Of Life November 2010 Aim To provide a user friendly, evidence based guide for the management
For patients and their carers this means smoother symptom control, better support in a crisis, and avoidance of admission if that is their choice.
 Bedfordshire Palliative Care Palliative Care Medicines Guidance This folder has been produced to support professionals providing palliative care in any setting. Its aim is to make best practice in palliative
Bedfordshire Palliative Care Palliative Care Medicines Guidance This folder has been produced to support professionals providing palliative care in any setting. Its aim is to make best practice in palliative
Algorithms for Symptom Management. In End of Life Care
 Algorithms for Symptom Management In End of Life Care The Use of Drugs Beyond Licence (off label) -The Medicines and Healthcare Products Regulatory Agency (MHRA) in the UK regulates the activity of the
Algorithms for Symptom Management In End of Life Care The Use of Drugs Beyond Licence (off label) -The Medicines and Healthcare Products Regulatory Agency (MHRA) in the UK regulates the activity of the
Renal Palliative Care Last Days of Life
 Renal Palliative Care Last Days of Life Introduction This guideline is an aid to clinical decision-making and good practice for patients with stage 4-5 chronic kidney disease (egfr
Renal Palliative Care Last Days of Life Introduction This guideline is an aid to clinical decision-making and good practice for patients with stage 4-5 chronic kidney disease (egfr
In our patients the cause of seizures can be broadly divided into structural and systemic causes.
 Guidelines for the management of Seizures Amalgamation and update of previous policies 7 (Seizure guidelines, ND, 2015) and 9 (Status epilepticus, KJ, 2011) Seizures can occur in up to 15% of the Palliative
Guidelines for the management of Seizures Amalgamation and update of previous policies 7 (Seizure guidelines, ND, 2015) and 9 (Status epilepticus, KJ, 2011) Seizures can occur in up to 15% of the Palliative
SYMPTOM MANAGEMENT GUIDANCE FOR PATIENTS RECEIVING PALLIATIVE CARE AT ROYAL DERBY HOSPITAL
 SYMPTOM MANAGEMENT GUIDANCE FOR PATIENTS RECEIVING PALLIATIVE CARE AT ROYAL DERBY HOSPITAL If a patient is believed to be approaching the end of their life, medication should be prescribed in anticipation
SYMPTOM MANAGEMENT GUIDANCE FOR PATIENTS RECEIVING PALLIATIVE CARE AT ROYAL DERBY HOSPITAL If a patient is believed to be approaching the end of their life, medication should be prescribed in anticipation
Analgesia for Patients with Substance Abuse Disorders. Lisa Jennings CN November 2015
 Analgesia for Patients with Substance Abuse Disorders Lisa Jennings CN November 2015 Definitions n Addiction: A pattern of drug use characterised by aberrant drug-taking behaviours & the compulsive use
Analgesia for Patients with Substance Abuse Disorders Lisa Jennings CN November 2015 Definitions n Addiction: A pattern of drug use characterised by aberrant drug-taking behaviours & the compulsive use
BACKGROUND Measuring renal function :
 A GUIDE TO USE OF COMMON PALLIATIVE CARE DRUGS IN RENAL IMPAIRMENT These guidelines bring together information and recommendations from the Palliative Care formulary (PCF5 ) BACKGROUND Measuring renal
A GUIDE TO USE OF COMMON PALLIATIVE CARE DRUGS IN RENAL IMPAIRMENT These guidelines bring together information and recommendations from the Palliative Care formulary (PCF5 ) BACKGROUND Measuring renal
Enhanced Community Palliative Support Services. Lynne Ghasemi St Luke s Hospice
 Enhanced Community Palliative Support Services Lynne Ghasemi St Luke s Hospice Learning Outcomes Define the different types of pain Describe the process of pain assessment Discuss pharmacological management
Enhanced Community Palliative Support Services Lynne Ghasemi St Luke s Hospice Learning Outcomes Define the different types of pain Describe the process of pain assessment Discuss pharmacological management
Acute pain management in opioid tolerant patients. Muhammad Laklouk
 Acute pain management in opioid tolerant patients Muhammad Laklouk General principles An adequate review and assessment Provision of effective analgesia (including attenuation of tolerance and hyperalgesia)
Acute pain management in opioid tolerant patients Muhammad Laklouk General principles An adequate review and assessment Provision of effective analgesia (including attenuation of tolerance and hyperalgesia)
BJF Acute Pain Team Formulary Group
 Title Analgesia Guidelines for Acute Pain Management (Adults) in BGH Document Type Issue no Clinical guideline Clinical Governance Support Team Use Issue date April 2013 Review date April 2015 Distribution
Title Analgesia Guidelines for Acute Pain Management (Adults) in BGH Document Type Issue no Clinical guideline Clinical Governance Support Team Use Issue date April 2013 Review date April 2015 Distribution
PENNINE LANCASHIRE GUIDELINES FOR THE MANAGEMENT OF SYMPTOMS IN THE LAST DAYS OF LIFE
 PENNINE LANCASHIRE GUIDELINES FOR THE MANAGEMENT OF SYMPTOMS IN THE LAST DAYS OF LIFE Originally produced: July 2006 First Review: August 2009 Second Review: November 2011 For review November 2013 Approved
PENNINE LANCASHIRE GUIDELINES FOR THE MANAGEMENT OF SYMPTOMS IN THE LAST DAYS OF LIFE Originally produced: July 2006 First Review: August 2009 Second Review: November 2011 For review November 2013 Approved
Diamorphine 4 hour. alfentanil (500microgram/mL) Calculated by dividing 24 hour oral morphine dose by 30
 Calculated by dividing 24 hour oral morphine dose by 30") If more information is required please seek help from specialist palliative care pioid dose conversion chart, syringe driver doses, rescue/prn doses and opioid patches Use the conversion chart to work
If more information is required please seek help from specialist palliative care pioid dose conversion chart, syringe driver doses, rescue/prn doses and opioid patches Use the conversion chart to work
Guidelines on the Safe Practice of Acute Pain Management
 Page 1 of 7 Guidelines on the Safe Practice of Acute Pain Version Effective Date 1 1 MAY 1994 (Reviewed Feb 2002) 2 1 DEC 2014 Document No. HKCA P11 v2 Prepared by College Guidelines Committee Endorsed
Page 1 of 7 Guidelines on the Safe Practice of Acute Pain Version Effective Date 1 1 MAY 1994 (Reviewed Feb 2002) 2 1 DEC 2014 Document No. HKCA P11 v2 Prepared by College Guidelines Committee Endorsed
PALLIATIVE CARE PRESCRIBING FOR PATIENTS WHO ARE SUBSTANCE MISUSERS
 PALLIATIVE CARE PRESCRIBING FOR PATIENTS WHO ARE SUBSTANCE MISUSERS Background information Substance misusers who develop palliative care needs are likely to have psychological, social and existential
PALLIATIVE CARE PRESCRIBING FOR PATIENTS WHO ARE SUBSTANCE MISUSERS Background information Substance misusers who develop palliative care needs are likely to have psychological, social and existential
MMG035 Symptom Management Guidelines for a Person thought to be in the Last Few Days and Hours of Life
 MMG035 Symptom Management Guidelines for a Person thought to be in the Last Few Days and Hours of Life The following pages are guidelines for the management of common symptoms for a person thought to be
MMG035 Symptom Management Guidelines for a Person thought to be in the Last Few Days and Hours of Life The following pages are guidelines for the management of common symptoms for a person thought to be
1
 Disclosures I do not have a vested interest in or affiliation with any corporate organization offering financial support or grant monies for this continuing education activity, or any affiliation with
Disclosures I do not have a vested interest in or affiliation with any corporate organization offering financial support or grant monies for this continuing education activity, or any affiliation with
Mid Essex Locality Guideline for Management of Adult Acute and Chronic Non-Cancer Pain in Primary care
 Guideline for Management of Adult Acute and Chronic Non-Cancer Pain in Primary care If possible patients should be assessed using a simple visual analogue scale VAS to determine the most appropriate stage
Guideline for Management of Adult Acute and Chronic Non-Cancer Pain in Primary care If possible patients should be assessed using a simple visual analogue scale VAS to determine the most appropriate stage
Collaboration. Opioids. Ketamine. epidural Best Practice. Waterloo Wellington HPC Protocol
 HPC hpcconnection.ca Neuro - axial Nursing cross sector Collaboration Analgesia Pharmacists Intractable patient centered Opioids Ketamine Interventional Consensus Anesthesia Physicians evidence based epidural
HPC hpcconnection.ca Neuro - axial Nursing cross sector Collaboration Analgesia Pharmacists Intractable patient centered Opioids Ketamine Interventional Consensus Anesthesia Physicians evidence based epidural
patient group direction
 CYCLIZINE v01 1/7 CYCLIZINE PGD Details Version 1.0 Legal category Staff grades Approved by POM Paramedic (Non-ECP) Nurse (Non-ECP) Emergency Care Practitioner (Paramedic) Emergency Care Practitioner (Nurse)
CYCLIZINE v01 1/7 CYCLIZINE PGD Details Version 1.0 Legal category Staff grades Approved by POM Paramedic (Non-ECP) Nurse (Non-ECP) Emergency Care Practitioner (Paramedic) Emergency Care Practitioner (Nurse)
DBL NALOXONE HYDROCHLORIDE INJECTION USP
 Name of medicine Naloxone hydrochloride Data Sheet New Zealand DBL NALXNE HYDRCHLRIDE INJECTIN USP Presentation DBL Naloxone Hydrochloride Injection USP is a sterile, clear, colourless solution, free from
Name of medicine Naloxone hydrochloride Data Sheet New Zealand DBL NALXNE HYDRCHLRIDE INJECTIN USP Presentation DBL Naloxone Hydrochloride Injection USP is a sterile, clear, colourless solution, free from
Care in the Last Days of Life
 Care in the Last Days of Life Introduction This guideline is an aid to clinical decision making and good practice in person-centred care for patients who are deteriorating and at risk of dying. The patient
Care in the Last Days of Life Introduction This guideline is an aid to clinical decision making and good practice in person-centred care for patients who are deteriorating and at risk of dying. The patient
Trust Guideline for the Management of Patient Controlled Analgesia (PCA) in Adults
 in Adults") Patient Controlled Analgesia (PCA) in Adults A clinical guideline recommended for use For Use in: In all Clinical Areas By: Anaesthetists, Ward Nurses, Recovery Staff Acute Pain Service Staff For: Adult
Patient Controlled Analgesia (PCA) in Adults A clinical guideline recommended for use For Use in: In all Clinical Areas By: Anaesthetists, Ward Nurses, Recovery Staff Acute Pain Service Staff For: Adult
Care of the Dying Management in Severe Renal Failure
 Care of the Dying Management in Severe Renal Failure Clinical Guideline Early diagnosis of the dying process allows for adequate preparation of the patient, the family and the carers. This clinical guidance
Care of the Dying Management in Severe Renal Failure Clinical Guideline Early diagnosis of the dying process allows for adequate preparation of the patient, the family and the carers. This clinical guidance
What do we want for pain medications?
 New Trends in Pain Pharmacotherapy Dr. Chi Wai Cheung MBBS(HK), FHKCA, FHKAM(Anaesthesiology), Dip Pain Mgt(HKCA) Clinical Assistant Professor Department of Anaesthesiology The University of Hong Kong
New Trends in Pain Pharmacotherapy Dr. Chi Wai Cheung MBBS(HK), FHKCA, FHKAM(Anaesthesiology), Dip Pain Mgt(HKCA) Clinical Assistant Professor Department of Anaesthesiology The University of Hong Kong
Substitution Therapy for Opioid Use Disorder The Role of Suboxone
 Substitution Therapy for Opioid Use Disorder The Role of Suboxone Methadone/Buprenorphine 101 Workshop, December 10, 2016 Leslie Lappalainen, MD, CCFP, dip ABAM Prepared by Mandy Manak, MD, ABAM, CCSAM
Substitution Therapy for Opioid Use Disorder The Role of Suboxone Methadone/Buprenorphine 101 Workshop, December 10, 2016 Leslie Lappalainen, MD, CCFP, dip ABAM Prepared by Mandy Manak, MD, ABAM, CCSAM
Methadone Maintenance
 Methadone Maintenance A Practical Guide to Pharmacotherapy Methadone/Buprenorphine 101 Workshop, April 1, 2017 Ron Joe, MD, DABAM Objectives I. Pharmacology Of Methadone II. Practical Application of Pharmacology
Methadone Maintenance A Practical Guide to Pharmacotherapy Methadone/Buprenorphine 101 Workshop, April 1, 2017 Ron Joe, MD, DABAM Objectives I. Pharmacology Of Methadone II. Practical Application of Pharmacology
[Type text] Anticipatory Medication STAT dose and Syringe Driver Guidance [Type text]
![[Type text] Anticipatory Medication STAT dose and Syringe Driver Guidance [Type text]](/thumbs/92/110296570.jpg "[Type text] Anticipatory Medication STAT dose and Syringe Driver Guidance [Type text]") [Type text] Anticipatory Medication STAT dose and Syringe Driver Guidance [Type text] Patients with egfr greater than 30mL/min Patients with egfr less than 30mL/min Symptom Drug Dose Symptom Drug Dose
[Type text] Anticipatory Medication STAT dose and Syringe Driver Guidance [Type text] Patients with egfr greater than 30mL/min Patients with egfr less than 30mL/min Symptom Drug Dose Symptom Drug Dose
SPAGG. Coversheet for Specialist Palliative Audit and Guideline Group Agreed Documentation
 SPAGG Coversheet for Specialist Palliative Audit and Guideline Group Agreed Documentation This sheet is to accompany all documentation agreed by SPAGG. This will assist maintenance of the guidelines as
SPAGG Coversheet for Specialist Palliative Audit and Guideline Group Agreed Documentation This sheet is to accompany all documentation agreed by SPAGG. This will assist maintenance of the guidelines as
SEEING KETAMINE IN A NEW LIGHT
 SEEING KETAMINE IN A NEW LIGHT BobbieJean Sweitzer, M.D., FACP Professor of Anesthesiology Director of Perioperative Medicine Northwestern University Bobbie.Sweitzer@northwestern.edu LEARNING OBJECTIVES
SEEING KETAMINE IN A NEW LIGHT BobbieJean Sweitzer, M.D., FACP Professor of Anesthesiology Director of Perioperative Medicine Northwestern University Bobbie.Sweitzer@northwestern.edu LEARNING OBJECTIVES
Cardiac Catheter Labs Intravenous Drug Therapy Guide
 Title of Guideline (must include the word Guideline (not protocol, policy, procedure etc) Contact Name and Job Title (author) Cardiac Catheter Lab IV Medicines Guideline Helen Buxton ( Senior Cath Lab
Title of Guideline (must include the word Guideline (not protocol, policy, procedure etc) Contact Name and Job Title (author) Cardiac Catheter Lab IV Medicines Guideline Helen Buxton ( Senior Cath Lab
Pain management in palliative care. Dr. Stepanie Lippett and Sister Karen Davies-Linihan
 Pain management in palliative care Dr. Stepanie Lippett and Sister Karen Davies-Linihan contents Concept of total pain Steps in pain management Recognising neuropathic pain WHO analgesic ladder Common
Pain management in palliative care Dr. Stepanie Lippett and Sister Karen Davies-Linihan contents Concept of total pain Steps in pain management Recognising neuropathic pain WHO analgesic ladder Common
Core Safety Profile. Pharmaceutical form(s)/strength: 5mg/ml and 25 mg/ml, Solution for injection, IM/IV FI/H/PSUR/0010/002 Date of FAR:
/strength: 5mg/ml and 25 mg/ml, Solution for injection, IM/IV FI/H/PSUR/0010/002 Date of FAR:") Core Safety Profile Active substance: Esketamine Pharmaceutical form(s)/strength: 5mg/ml and 25 mg/ml, Solution for injection, IM/IV P-RMS: FI/H/PSUR/0010/002 Date of FAR: 29.05.2012 4.3 Contraindications
Core Safety Profile Active substance: Esketamine Pharmaceutical form(s)/strength: 5mg/ml and 25 mg/ml, Solution for injection, IM/IV P-RMS: FI/H/PSUR/0010/002 Date of FAR: 29.05.2012 4.3 Contraindications
Acute painful crisis in patients with sickle cell disease: Clinical Guidelines (HN-506a)
") Acute painful crisis in patients with sickle cell disease: Clinical Guidelines (HN-506a) Introduction The majority of acute painful crises in patients with sickle cell disease will be managed independently
Acute painful crisis in patients with sickle cell disease: Clinical Guidelines (HN-506a) Introduction The majority of acute painful crises in patients with sickle cell disease will be managed independently
Care of the Dying Management in Severe Renal Failure
 Care of the Dying Management in Severe Renal Failure Clinical Guideline Early recognition of the dying process allows for adequate preparation of the patient, the family and the carers. This clinical guidance
Care of the Dying Management in Severe Renal Failure Clinical Guideline Early recognition of the dying process allows for adequate preparation of the patient, the family and the carers. This clinical guidance
Anticipatory Medications for End of Life Patients. Doses must be proportional to the current analgesic medication YES NO YES NO
 Anticipatory Medications for End of Life Patients oses must be proportional to the current analgesic medication Please refer ALL patients on Methadone or Ketamine to palliative care team for advice. Patients
Anticipatory Medications for End of Life Patients oses must be proportional to the current analgesic medication Please refer ALL patients on Methadone or Ketamine to palliative care team for advice. Patients
Pain. Christine Illingworth. Community Nurse St Luke s Hospice 17/5/17
 Pain Christine Illingworth Community Nurse St Luke s Hospice 17/5/17 What is pain? Pain is an unpleasant sensory and emotional experience associated with actual or potential tissue damage Pain is whatever
Pain Christine Illingworth Community Nurse St Luke s Hospice 17/5/17 What is pain? Pain is an unpleasant sensory and emotional experience associated with actual or potential tissue damage Pain is whatever
SCOPING DOCUMENT FOR WHO Treatment Guidelines on pain related to cancer, HIV and other progressive life-threatening illnesses in adults
 SCOPING DOCUMENT FOR WHO Treatment Guidelines on pain related to cancer, HIV and other progressive life-threatening illnesses in adults BACKGROUND The justification for developing these guidelines lies
SCOPING DOCUMENT FOR WHO Treatment Guidelines on pain related to cancer, HIV and other progressive life-threatening illnesses in adults BACKGROUND The justification for developing these guidelines lies
The Use of Transdermal Opioids in Palliative Care. G. Whyte, P.Powell, C. Littlewood, A. Coackley, G. Leng External Reviewer/Expert : S.
 The Use of Transdermal Opioids in Palliative Care G. Whyte, P.Powell, C. Littlewood, A. Coackley, G. Leng External Reviewer/Expert : S. Simpson 1 Introduction Dr Graham Whyte Literature Review Dr Paula
The Use of Transdermal Opioids in Palliative Care G. Whyte, P.Powell, C. Littlewood, A. Coackley, G. Leng External Reviewer/Expert : S. Simpson 1 Introduction Dr Graham Whyte Literature Review Dr Paula
OST. Pharmacology & Therapeutics. Leo O. Lanoie, MD, MPH, FCFP, CCSAM, ABAM, MRO
 OST Pharmacology & Therapeutics Leo O. Lanoie, MD, MPH, FCFP, CCSAM, ABAM, MRO Disclaimer In the past two years I have received no payment for services from any agency other than government or academic.
OST Pharmacology & Therapeutics Leo O. Lanoie, MD, MPH, FCFP, CCSAM, ABAM, MRO Disclaimer In the past two years I have received no payment for services from any agency other than government or academic.
Agonists: morphine, fentanyl Agonists-Antagonists: nalbuphine Antagonists: naloxone
 Opioid Definition All drugs, natural or synthetic, that bind to opiate receptors Agonists: morphine, fentanyl Agonists-Antagonists: nalbuphine Antagonists: naloxone Opioid agonists increase pain threshold
Opioid Definition All drugs, natural or synthetic, that bind to opiate receptors Agonists: morphine, fentanyl Agonists-Antagonists: nalbuphine Antagonists: naloxone Opioid agonists increase pain threshold
Analgesic Drugs PHL-358-PHARMACOLOGY AND THERAPEUTICS-I. Mr.D.Raju,M.pharm, Lecturer
 Analgesic Drugs PHL-358-PHARMACOLOGY AND THERAPEUTICS-I Mr.D.Raju,M.pharm, Lecturer Mechanisms of Pain and Nociception Nociception is the mechanism whereby noxious peripheral stimuli are transmitted to
Analgesic Drugs PHL-358-PHARMACOLOGY AND THERAPEUTICS-I Mr.D.Raju,M.pharm, Lecturer Mechanisms of Pain and Nociception Nociception is the mechanism whereby noxious peripheral stimuli are transmitted to
Clinical Guideline. Guidelines for the use of opioid analgesics in the management of acute pain in adults
 Clinical Guideline Guidelines for the use of opioid analgesics in the management of acute pain in adults Document detail Document location West Kent and MTW Formulary Version 1.0 Effective from July 2017
Clinical Guideline Guidelines for the use of opioid analgesics in the management of acute pain in adults Document detail Document location West Kent and MTW Formulary Version 1.0 Effective from July 2017
Continence PGD transdermal oxybutynin Kentera patch 36mg
 Continence PGD transdermal oxybutynin Kentera patch 36mg Patient group direction for the supply of transdermal oxybutynin Kentera patch 36mg to patients suffering from urinary frequency, urgency or incontinence
Continence PGD transdermal oxybutynin Kentera patch 36mg Patient group direction for the supply of transdermal oxybutynin Kentera patch 36mg to patients suffering from urinary frequency, urgency or incontinence
survey Parenteral anti-epileptics What is your experience? May July 2015
 Parenteral anti-epileptics What is your experience? May July 2015 Number of responses = 99 1a) In patients with pre-existing epilepsy controlled by PO medication that are imminently dying (prognosis
Parenteral anti-epileptics What is your experience? May July 2015 Number of responses = 99 1a) In patients with pre-existing epilepsy controlled by PO medication that are imminently dying (prognosis
Long Term Care Formulary HCD - 08
 1 of 5 PREAMBLE Opioids are an important component of the pharmaceutical armamentarium for management of chronic pain. The superiority of analgesic effect of one narcotic over another is not generally
1 of 5 PREAMBLE Opioids are an important component of the pharmaceutical armamentarium for management of chronic pain. The superiority of analgesic effect of one narcotic over another is not generally
HOPE. Considerations. Considerations ISING. Safe Opioid Prescribing Guidelines for ACUTE Non-Malignant Pain
 Due to the high level of prescription drug use and abuse in Lake County, these guidelines have been developed to standardize prescribing habits and limit risk of unintended harm when prescribing opioid
Due to the high level of prescription drug use and abuse in Lake County, these guidelines have been developed to standardize prescribing habits and limit risk of unintended harm when prescribing opioid
GUIDELINES FOR THE MANAGEMENT OF PALLIATIVE CARE PATIENTS WITH A HISTORY OF SUBSTANCE MISUSE
 GUIDELINES FOR THE MANAGEMENT OF PALLIATIVE CARE PATIENTS WITH A HISTORY OF SUBSTANCE MISUSE 41.1 GENERAL PRINCIPLES The ICD 10 diagnostic criteria for dependency syndrome are listed in Table 41.1 below.
GUIDELINES FOR THE MANAGEMENT OF PALLIATIVE CARE PATIENTS WITH A HISTORY OF SUBSTANCE MISUSE 41.1 GENERAL PRINCIPLES The ICD 10 diagnostic criteria for dependency syndrome are listed in Table 41.1 below.
Opioid Conversion Guidelines
 Opioid Conversion Guidelines March 2015 Gippsland Region Palliative Care Consortium Clinical Practice Group Title Keywords Ratified Opioid, Conversion, Drug, Therapy, Palliative, Guideline, Palliative,
Opioid Conversion Guidelines March 2015 Gippsland Region Palliative Care Consortium Clinical Practice Group Title Keywords Ratified Opioid, Conversion, Drug, Therapy, Palliative, Guideline, Palliative,
MEDICAL POLICY SUBJECT: KETAMINE INFUSION THERAPY FOR THE TREATMENT OF CHRONIC PAIN SYNDROMES POLICY NUMBER: CATEGORY: Technology Assessment
 Clinical criteria used to make utilization review decisions are based on credible scientific evidence published in peer reviewed medical literature generally recognized by the medical community. Guidelines
Clinical criteria used to make utilization review decisions are based on credible scientific evidence published in peer reviewed medical literature generally recognized by the medical community. Guidelines
Goals for sedation during mechanical ventilation
 New Uses of Old Medications Gina Riggi, PharmD, BCCCP, BCPS Clinical Pharmacist Trauma ICU Jackson Memorial Hospital Disclosure I do not have anything to disclose Objectives Describe the use of ketamine
New Uses of Old Medications Gina Riggi, PharmD, BCCCP, BCPS Clinical Pharmacist Trauma ICU Jackson Memorial Hospital Disclosure I do not have anything to disclose Objectives Describe the use of ketamine
Resuscitation Fluids
 Resuscitation Fluids Acceptable Fluids (also known as): Sodium Chloride Hartmann s Solution (Ringer-Lactate Solution, Compound Sodium Lactate) 4.5% Albumin Solution (PPS) Gelofusine 20ml/kg Bolus Can be
Resuscitation Fluids Acceptable Fluids (also known as): Sodium Chloride Hartmann s Solution (Ringer-Lactate Solution, Compound Sodium Lactate) 4.5% Albumin Solution (PPS) Gelofusine 20ml/kg Bolus Can be
Policy/Standard Operating Procedure/ Clinical Guideline. ELHT/CP22 Version 5.1. ELHT/CP22 Version 4.1
 TRUST WIDE/DIVISIONAL DOCUMENT Delete as appropriate Policy/Standard Operating Procedure/ Clinical Guideline DOCUMENT TITLE: Policy and Procedure for the T34 Ambulatory Syringe Pump in adults (Palliative
TRUST WIDE/DIVISIONAL DOCUMENT Delete as appropriate Policy/Standard Operating Procedure/ Clinical Guideline DOCUMENT TITLE: Policy and Procedure for the T34 Ambulatory Syringe Pump in adults (Palliative
MORPHINE ADMINISTRATION
 Introduction Individualised Administration Drug of Choice Route of Administration & Doses Monitoring of Neonates & high risk patients Team Management Responsibility Morphine Protocol Flow Chart Introduction
Introduction Individualised Administration Drug of Choice Route of Administration & Doses Monitoring of Neonates & high risk patients Team Management Responsibility Morphine Protocol Flow Chart Introduction
Neuropathic Pain in Palliative Care
 Neuropathic Pain in Palliative Care Neuropathic Pain in Advanced Cancer Affects 40% of patients Multiple concurrent pains are common Often complex pathophysiology with mixed components Nocioceptive Neuropathic
Neuropathic Pain in Palliative Care Neuropathic Pain in Advanced Cancer Affects 40% of patients Multiple concurrent pains are common Often complex pathophysiology with mixed components Nocioceptive Neuropathic
PERIOPERATIVE PAIN MANAGEMENT: WHAT S UP WITH METHADONE?
 PERIOPERATIVE PAIN MANAGEMENT: WHAT S UP WITH METHADONE? Sandra Z Perkowski, VMD, PhD, DACVAA University of Pennsylvania, School of Veterinary Medicine, Philadelphia, PA Pre-emptive and multimodal use
PERIOPERATIVE PAIN MANAGEMENT: WHAT S UP WITH METHADONE? Sandra Z Perkowski, VMD, PhD, DACVAA University of Pennsylvania, School of Veterinary Medicine, Philadelphia, PA Pre-emptive and multimodal use
Doncaster & Bassetlaw Cancer Locality. Palliative Care Core Formulary
 Doncaster & Bassetlaw Cancer Locality Palliative Core Formulary Approved by Doncaster & Bassetlaw Hospitals NHS Foundation Trust Drugs and Therapeutics Committee. DJ14/2155 Oct 2014 Review date: Oct 2017
Doncaster & Bassetlaw Cancer Locality Palliative Core Formulary Approved by Doncaster & Bassetlaw Hospitals NHS Foundation Trust Drugs and Therapeutics Committee. DJ14/2155 Oct 2014 Review date: Oct 2017
SUBCUTANEOUS AS REQUIRED & SYRINGE PUMP PRESCRIPTION & ADMINISTRATION RECORD (SPAR) Name: Address: Postcode: Date of Birth: NHS Number:
 Name: Address: Postcode: Date of Birth: NHS Number:") FILE IN PATIENT S COMMUNITY HEALTH RECORD FOLDER : SUBCUTANEOUS AS REQUIRED & SYRINGE PUMP PRERIPTION & ADMINISTRATION RECORD (SPAR) Abbreviations used in this document to be listed here with the full
FILE IN PATIENT S COMMUNITY HEALTH RECORD FOLDER : SUBCUTANEOUS AS REQUIRED & SYRINGE PUMP PRERIPTION & ADMINISTRATION RECORD (SPAR) Abbreviations used in this document to be listed here with the full
Corporate Medical Policy
 Corporate Medical Policy Intravenous Anesthetics for the Treatment of Chronic Pain File Name: Origination: Last CAP Review: Next CAP Review: Last Review: intravenous_anesthetics_for_the_treatment_of_chronic_pain
Corporate Medical Policy Intravenous Anesthetics for the Treatment of Chronic Pain File Name: Origination: Last CAP Review: Next CAP Review: Last Review: intravenous_anesthetics_for_the_treatment_of_chronic_pain
01/07/2018 ISCHAEMIC PAIN IN NON-RECONSTRUCTABLE CRITICAL LIMB ISCHAEMIA PRESENTATION OUTLINE
 ISCHAEMIC PAIN IN NON-RECONSTRUCTABLE CRITICAL LIMB ISCHAEMIA Dr. Áine Ní Laoire The Oxford Advanced Pain & Symptom Management Course Nottingham 27 th June 2018 PRESENTATION OUTLINE A Typical Case Background
ISCHAEMIC PAIN IN NON-RECONSTRUCTABLE CRITICAL LIMB ISCHAEMIA Dr. Áine Ní Laoire The Oxford Advanced Pain & Symptom Management Course Nottingham 27 th June 2018 PRESENTATION OUTLINE A Typical Case Background
Opioid overdose versus opioid toxicity. Dr Colette Reid
 Opioid overdose versus opioid toxicity Dr Colette Reid Overview Asked to discuss and clarify the differences between the two entities Literature searches: opioids and overdose; opioids and toxicity; opioids
Opioid overdose versus opioid toxicity Dr Colette Reid Overview Asked to discuss and clarify the differences between the two entities Literature searches: opioids and overdose; opioids and toxicity; opioids
Opioid Conversion Ratios - Guide to Practice 2010
 Opioid Conversion Ratios - Guide to Practice 2010 Released December 2010. 2010. The EMR PCC grants permission to reproduce parts of this publication for clinical and educational use only, provided that
Opioid Conversion Ratios - Guide to Practice 2010 Released December 2010. 2010. The EMR PCC grants permission to reproduce parts of this publication for clinical and educational use only, provided that
LONG TERM PHARMACOTHERAPY OF OPIOID DEPENDENCE
 LONG TERM PHARMACOTHERAPY OF OPIOID DEPENDENCE DR. SHILPA ADARKAR ASSOCIATE PROFESSOR DEPARTMENT OF PSYCHIATRY & DRUG DEADDICTION CENTRE OF EXCELLENCE SETH GSMC & KEMH LONG TERM OPTIONS FULL AGONIST PARTIAL
LONG TERM PHARMACOTHERAPY OF OPIOID DEPENDENCE DR. SHILPA ADARKAR ASSOCIATE PROFESSOR DEPARTMENT OF PSYCHIATRY & DRUG DEADDICTION CENTRE OF EXCELLENCE SETH GSMC & KEMH LONG TERM OPTIONS FULL AGONIST PARTIAL
Immodium / loprarmide
 Immodium / loprarmide IMODIUM (loperamide hydrochloride) is indicated for the control and symptomatic relief of acute nonspecific diarrhea and of chronic diarrhea associated with inflammatory bowel disease.
Immodium / loprarmide IMODIUM (loperamide hydrochloride) is indicated for the control and symptomatic relief of acute nonspecific diarrhea and of chronic diarrhea associated with inflammatory bowel disease.
Hydration at the End of Life:
 Hydration at the End of Life: A systematic literature review and audit of current practice November 12 th 2015 Dr Alison Coackley- Consultant in Palliative Medicine, Clatterbridge Cancer Centre Dr Catherine
Hydration at the End of Life: A systematic literature review and audit of current practice November 12 th 2015 Dr Alison Coackley- Consultant in Palliative Medicine, Clatterbridge Cancer Centre Dr Catherine
NEW ZEALAND DATA SHEET ACUPAN TM. 3. PHARMACEUTICAL FORM White, round, biconvex, film-coated tablets (7 mm diameter) engraved APN on one face.
 engraved APN on one face.") 1. PRODUCT NAME ACUPAN 30 mg tablets 2. QUALITATIVE AND QUANTITATIVE COMPOSITION Each tablet contains nefopam hydrochloride 30 mg. For a full list of excipients, see section 6.1. 3. PHARMACEUTICAL FORM
1. PRODUCT NAME ACUPAN 30 mg tablets 2. QUALITATIVE AND QUANTITATIVE COMPOSITION Each tablet contains nefopam hydrochloride 30 mg. For a full list of excipients, see section 6.1. 3. PHARMACEUTICAL FORM
Pain Management Strategies Webinar/Teleconference
 Pain Management Strategies Webinar/Teleconference Barry K. Baines, MD April 16, 2009 Objectives Describe the principles of pain management. Identify considerations in the use of opioids. Describe the benefits
Pain Management Strategies Webinar/Teleconference Barry K. Baines, MD April 16, 2009 Objectives Describe the principles of pain management. Identify considerations in the use of opioids. Describe the benefits
Associate Professor Supranee Niruthisard Department of Anesthesiology Faculty of Medicine Chulalongkorn University January 21, 2008
 Associate Professor Supranee Niruthisard Department of Anesthesiology Faculty of Medicine Chulalongkorn University January 21, 2008 PAIN MECHANISMS Somatic Nociceptive Visceral Inflammatory response sensitizes
Associate Professor Supranee Niruthisard Department of Anesthesiology Faculty of Medicine Chulalongkorn University January 21, 2008 PAIN MECHANISMS Somatic Nociceptive Visceral Inflammatory response sensitizes
BREATHLESSNESS MANAGEMENT
 Guideline Name: Breathlessness BACKGROUND Breathlessness is a common symptom in patients with cancer, end-stage heart failure and end-stage chronic obstructive pulmonary disease (COPD). There are many
Guideline Name: Breathlessness BACKGROUND Breathlessness is a common symptom in patients with cancer, end-stage heart failure and end-stage chronic obstructive pulmonary disease (COPD). There are many
What s New 2003? What new treatments? What have you discontinued? More information please!
 What s New 2003? What new treatments? What have you discontinued? More information please! 1 What s New 2003? Submissions = 137 UK = 52 (38%) Doctors = 60% Nurses = 25% Pharmacists = 15% 2 What s New?
What s New 2003? What new treatments? What have you discontinued? More information please! 1 What s New 2003? Submissions = 137 UK = 52 (38%) Doctors = 60% Nurses = 25% Pharmacists = 15% 2 What s New?
General Anesthesia. Mohamed A. Yaseen
 General Anesthesia Mohamed A. Yaseen M.S,c Surgery Before Anesthesia General Anesthesia ( GA ) Drug induced absence of perception of all sensation allowing surgery or other painful procedure to be carried
General Anesthesia Mohamed A. Yaseen M.S,c Surgery Before Anesthesia General Anesthesia ( GA ) Drug induced absence of perception of all sensation allowing surgery or other painful procedure to be carried