Pneumonia Update Overview. Community-Acquired Pneumonia. Management of the Hospitalized Patient. Care of the Hospitalized Patient
|
|
|
- Deborah Stafford
- 6 years ago
- Views:
Transcription
 Pneumonia developing outside the hospital But not HCAP Healthcare Associated")
1 Pneumonia Update 2010 Management of the Hospitalized Patient Scott A. Flanders, M.D. Professor of Medicine Director, Hospitalist Program University of Michigan Overview Community Acquired Pneumonia (CAP) Pneumonia developing outside the hospital But not HCAP Healthcare Associated Pneumonia (HCAP) Pneumonia developing outside the hospital But the patient has been touched by the healthcare system Community-Acquired Pneumonia Care of the Hospitalized Patient Admission Decision Etiologies and Etiologic Testing Antibiotic Therapy Discharge Decision Prevention
2 Community-Acquired Pneumonia Care of the Hospitalized Patient Admission Decision (Predicting ICU Care) Etiologies and Etiologic Testing Antibiotic Therapy Predicting the Need for ICU Care Decades of Research Finds an Answer! After years of research and millions of NIH dollars we are able to confidently say that single most important variable predictive of severe CAP requiring intensive care is THE NEED FOR MECHANICAL VENTILATION Rocket Science and the IDSA / ATS Guidelines for Severe Pneumonia. CID. 2009
3 Admission Decision Predicting the Need for ICU Level Care SMART COP: Sens=92%, Spec=62% Sensitivity AUC SMART COP 0.87 PSI IV&V 0.69 CURB Specificity CID 2008 Community-Acquired Pneumonia Care of the Hospitalized Patient Admission Decision Etiologies and Etiologic Testing Antibiotic Therapy

4 Etiologies in CAP (Mild-Moderate Dz) Typical bacteria S. Pneumo 45% H. Flu 20% S. Aureus 10% K. Pneumo 3% Other 15-20% CID, % 20-25% 40-50% No Pathogen Atypicals Typicals Atypical bacteria Mycoplasma 65% Chlamydiophila 30% Legionella 5% Viral Pneumonia 193 patients with extensive testing for viral agents Rank order of viruses (15%) Viral vs. Bacterial Influenza (n=7) hmpv (n=7) RSV (n=5) Rhinovirus Parainfluenza Coronavirus Adenovirus Nothing reliable, but Older More frail More cardiac disease Less leukocytosis (74% nl) Seasonal No difference in outcomes CHEST 2008


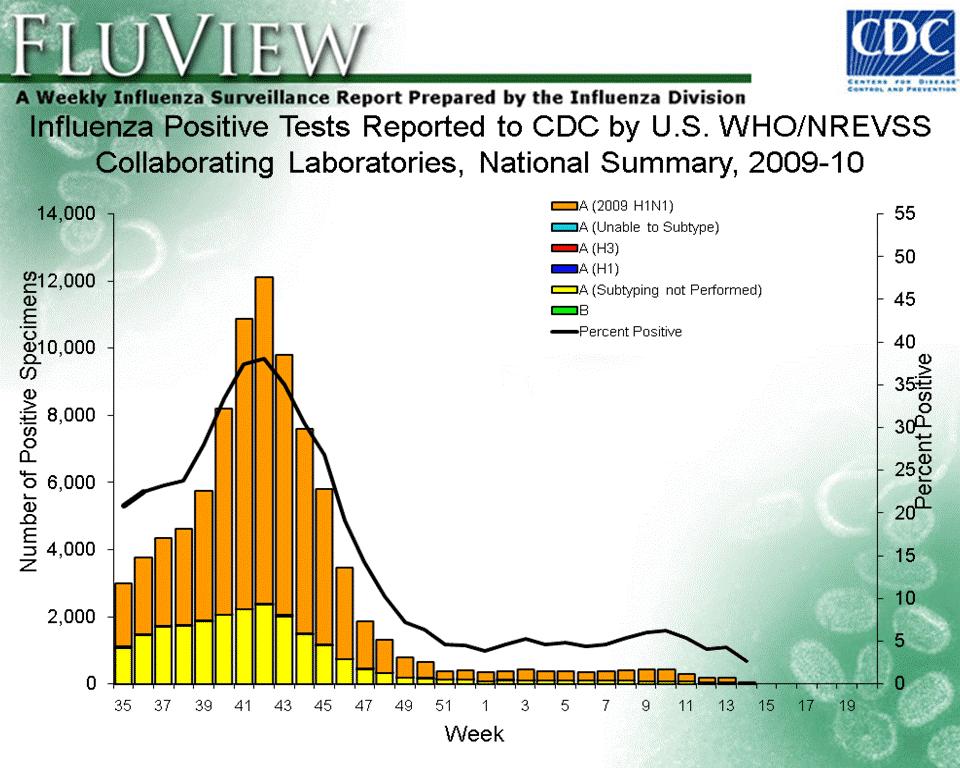
5 Centers for Disease Control and Prevention
 Virus (S-OIV) 87% of deaths and 71% of severe cases in patients aged 5-59 Swine Origin Influenza A (H1N1) Virus (S-OIV): Severe Disease;")
6 Chowell G et al. N Engl J Med 2009;361: Swine Origin Influenza A (H1N1) Virus (S-OIV) 87% of deaths and 71% of severe cases in patients aged 5-59 Swine Origin Influenza A (H1N1) Virus (S-OIV): Severe Disease; 18 cases Clinical Presentation Temp >38 100% Cough 100% Dyspnea 100% LDH abnl 100% Bilateral patchy basilar inflitrates 100% CPK abnl 63% Lymphopenia 61% Hypotension 50% Comorbidities 44% Clinical Course ARDS / vent 67% ARDS in 24 hrs 55% Renal Failure 33% Bacterial Infxn <5% Death Associations Pressors after fluids Intubation in 24 hrs Renal Failure APACHE / SOFA / P/F ratio NOT steroids NEJM 2009
 60% CPK elevation (median 1000 IU/L) DFA negative, PCR positive Rapid tests only 40-60% sensitive Arch")
7 Swine Origin Influenza A (H1N1) Virus (S-OIV): Severe Disease; U of M 10 patients at U of M with severe H1N1 (S-OIV) All with ARDS (100% oscillatory vent / ECMO) 9 obese: BMI >30 7 extreme obesity BMI >40 50% with PE, 60% renal failure on CRRT 90% shock with pressors (0% bacterial infection) 60% CPK elevation (median 1000 IU/L) DFA negative, PCR positive Rapid tests only 40-60% sensitive Arch Intern Med, 2009 MMWR 2009 Lung: cut surface Swine Origin Influenza A (H1N1) Virus (S-OIV) Treatment Oseltamivir (Tamiflu) 150 mg p.o. bid x 10 days : critically ill / ICU 75 mg p.o. bid x 5 days : non-icu Zanamivir (Relenza) 10 mg (2 oral inhalations) bid x 5 days Rimantadine (If seasonal flu circulating) 100 mg p.o. bid x 7 days
 Lancet 2009 CA-MRSA")

8 CA-MRSA Narrative review of published 12 studies / series Clinical Features % of Patients Flu Prodrome Leucopenia Shock Multi-lobar Necrotizing PVL Mortality (avg 40) Lancet 2009 CA-MRSA Systematic review of 74 articles describing 114pts Estimated incidence of per 100,000 Clinical Features Associated with Death Multiorgan Failure Mechanical Ventilation Shock ARDS ICU Flu-like symptoms Leucopenia DIC Rash Eur Resp J 2009
9 CA-MRSA IDSA Emerging Infections Network Survey physicians across U.S. 30% treated 560 cases of S. Aureus CAP % of pts MRSA 72% + Sputum Cx 77% + Blood Cx 43% Vanco Rx 73% (Many CA-MRSA isolates are resistant to macrolides and fluoroquinolones) CID; 2007 Risk factors CA-MRSA Past skin infection (abscess) IVDU Influenza (concurrent with flu; resp sx 2-6 d prior to ED) In sick patients with above risk factors consider empiric rx Ann Emerg Med 2007 Treatment: Vancomycin or Linezolid (NOT Daptomycin) Vanco troughs mcg / ml Controversial (NOT RECOMMENDED FOR ALL)?Clindamycin for anti-toxin effect? (rule out resistance first) Avoid Beta-lactams (increase exotoxin production) IVIG Lancet ID 2009 Blood Cultures for CAP: QI Worthy? Systematic review of 15 studies on the utility of blood cultures 13 studies included; 3800 immunocompetent pts All studies observational, only 3 required cultures True Positive Rate 0-14% Antibiotic narrowing 0-3% Antibiotic broadening 0-1% Afshar, J Hosp Med, 2009
10 Predicting Bacteremia in CAP Risk Factors No prior antibiotics Liver disease Pleuritic pain Tachycardia (125) Tachypnea (>30) Hypotension (<90) Derived from 3116 patients Prospectively validated OR Points CID, 2009 Predicting Bacteremia in CAP 50 Risk for Bacteremia % 20-25% 15% 5-10% <5% >4 # of Risk Variables CID, 2009 Etiologies / Diagnosis Who has gram negative rods or pseudomonas? (560 non-immunosuppressed pts with CAP) Gram negative predictors OR (95% CI) Aspiration 2.3 ( ) Prior admit* 3.5 ( ) Prior antibiotics** 1.9 ( ) Pulmonary comorbidity 2.8 ( ) 1 of the above factors 4.2 ( ) 2 of the above factors 9.1 ( ) 3 of the above factors 39.3 ( ) Pseudomonas predictors Pulmonary comorbidity 5.8 ( ) Prior admit 3.8 ( ) (*48 hrs in last month, **any in past month) Archives Int Med. 2003
11 Community-Acquired Pneumonia Care of the Hospitalized Patient Admission Decision Etiologies and Etiologic Testing Antibiotic Therapy Antibiotic Regimens and Outcomes Study Patients Design [RX] vs. BL Mono Gleason 00ʼ 13,000 Retrospec BL+macro: HR=.74 fluoro: HR=.64 Dudas 00ʼ 3000 Retrospec BL+macro: lower 30d mortality and LOS Houck 01ʼ 10,000 Retrospec BL+macro: lower 30d mortality Brown 03ʼ 45,000 Retrospec BL+macro: lower 30 d mortality Flanders 03ʼ 340 Retrospec BL+doxy: lower 30 d Morten 04ʼ/06ʼ;420 / 700 Retrospec Guideline concordant rx: lower 48h mortality Bratzler 09ʼ 27,730 Retrospec BL + macro: HR=0.7 fluoro: HR=0.7 Antibiotic Therapy Is it the Atypical Coverage that is Important? Shefet D, et al. Cochrane 2005 (Updated 2008) Meta-analysis of 24 RCTs ; atypical coverage vs. not Hospitalized patients; 11/24 Severe Pneumonia 18/24 identified trial were pharma sponsored Atypical drugs: 19 fluoro; 4 macrolide; 1 both Atypical Coverage vs. Non-Atypical Outcome RR (95% CI) Mortality 1.1 ( ) Clinical failure.92 ( ) Clinical Failure Subset Atypical orgs 0.5 ( ) Legionella 0.2 ( ) (only 43 cases)
12 Following the Guidelines McCabe, et al. Arch Intern Med, 2009 Retrospective study, 113 hospitals, 54,000 pts > 18 yo Compared GL rx (ATS / IDSA 2007) vs. discordant rx Adjusted for severity, comorbidities, vaccination, etc. Arnold, et al. Arch Intern Med, 2009 Retrospective internatl. study, 43 hospitals, 1650 pts > 65 Compared GL rx vs undertreatment and overtreatment Adjusted for severity, process measures Mortality for GL Concordant vs. Discordant Rx OR=0.70 ( ) Also Less sepsis, renal failure Earlier oral therapy McCabe, C. et al. Arch Intern Med 2009;169: Copyright restrictions may apply. Worse Drug Classes Associated with Mortality Cefepime, Aminoglycosides Carbapenems, Vanco Better Cephalosporins Macrolides Fluoro McCabe, C. et al. Arch Intern Med 2009;169: Copyright restrictions may apply.
13 Copyright restrictions may apply. Mortality for Guideline Concordant Treatment vs. Undertreatment HR=0.62 ( ) vs. Overtreatment HR= 0.51 ( ) Arnold, F. W. et al. Arch Intern Med 2009;169: Arnold, et al Confounding By Indication Given these studies, if there is an unrecognized or unmeasured confounder with an impact as large as a 20-40% reduction in mortality; it is difficult to imagine what such a confounder must be. Sharpe, Arch Intern Med, What variable might lead a doctor to give patients (who are not going to do as well) guideline discordant treatment? OR 2. Is there something different about doctors and hospitals that follow guideline that might lead to improved outcomes? Confounding By Indication Given these studies, if there is an unrecognized or unmeasured confounder with an impact as large as a 20-40% reduction in mortality; it is difficult to imagine what such a confounder must be. Sharpe, Arch Intern Med, What variable might lead a doctor to give patients (who are not going to do as well) guideline discordant treatment? OR How about physician judgment? 2. Is there something different about doctors and hospitals that follow guidelines that might lead to improved outcomes? I expect they do all sorts of things better
 or CA-MRSA Rx (Vanco or Linezolid) if risk factors: independent of ICU status Antibiotic Treatment A Role for Procalcitonin?")
14 Antibiotic Therapy The Guidelines:Inpatient IDSA / ATS 2007 β-lactam + macrolide (or doxycycline) Respiratory fluoroquinolone ICU: ß-lactam+macrolide, or ß-lactam+fluoroquinolone Anti-pseudomonal (many options) or CA-MRSA Rx (Vanco or Linezolid) if risk factors: independent of ICU status Antibiotic Treatment A Role for Procalcitonin? Multicenter, randomized controlled trial 6 Swiss emergency departments 1360 patients presenting with LRTIʼs 70% CAP, 15% COPD, 10% Acute Bronchitis 93% hospitalized 50% PSI risk classes IV and V Randomized to usual care vs PCT based rx Override allowed: ICU / severe instability, legionella JAMA 2009 PCT Algorithm for Antibiotic Treatment JAMA 2009
15 Antibiotic Exposure All Abx Exposure: 7d vs. 11d CAP Adverse effects: 23% vs. 33% No effect on death, ICU admit, readmission, or complications COPD Bronchitis Copyright restrictions Schuetz, may apply. P. et al. JAMA 2009;302: Antibiotic Therapy Short Course Therapy Am J Med, 2007; Meta-Analysis: 15 RCTs < 7 days vs. > 7 days Clinical Failure OR= 0.89 ( ) Antibiotic Therapy Short Course Therapy Am J Med, 2007; Meta-Analysis: 15 RCTs < 7 days vs. > 7 days Adverse Events OR= 0.86 ( ) Mortality OR= 0.81 ( )
16 Antibiotic Therapy Stopping Antibiotics Pts should be afebrile for hours Have no more than 1 CAP-associated instability* Usually this is after 5 days of therapy *HR<100 SBP>90 RR<24 Temp <37.8 O2 Sat >90 Mental status at baseline Taking orals Overview Community Acquired Pneumonia (CAP) Pneumonia developing outside the hospital But not HCAP Healthcare Associated Pneumonia (HCAP) Pneumonia developing outside the hospital But the patient has been touched by the healthcare system Healthcare Associated Infections Home Therapy IV Wound Care Nursing care through health agency Hospital or Dialysis Clinic in past 30 days for Dialysis / Any IV therapy Hospitalized 2 days in past 90? days Nursing Home or Long-Term Care Facility
17 MDR Pathogens Pseudomonas aeruginosa Drug resistant gram negatives ESBL producing Klebsiella Enterobacter Serratia Acinetobacter spp. MRSA MDR= Multidrug-resistant Risk Factors for MDR Infections Antimicrobial rx in past 90 days Current hospitalization > 5 days High rates of resistance in community or ward Risk factors for HCAP Home Therapy Hospital or Dialysis Clinic in past 30 days Hospitalized 2 days in past 90? days Nursing Home or Long-Term Care Facility Family member with multidrug resistant pathogen Immunosuppressive disease or therapy MDR= Multidrug-resistant Etiologies (HEALTH CARE ASSOCIATED PNEUMONIA) (Culture + CAP at an Academic Medical Center) CAP HCAP Patients 208 (33%) 431 (67%) S. Pneumo 41% 10% MRSA 12% 30% Psuedomonas 4% 25% Other GNR 2% 10% Inapprop. RX 13% 30% Mortality 9% 25% (HCAP: 70% hospitalized in past 90 days, 20% in past 180d) *As of 2005 CMS excludes HCAP from CAP GL Recs* AAC, 2007
18 HCAP Outcomes Prospective cohort study 55 Italian hospitals 2 active 1 week surveillance periods HCAP: Dialysis or hospital clinic in past 30days Chemo in past 30 days 2 days of hospitalization in past 6 months Nursing home or long term care Annals Intern Med 2009 HCAP Outcomes CAP HCAP Patients 223 (62%) 90 (25%) Recent Hosp 0% 80% (6 months) Antacids 23% 53% Bilat Infiltrate 20% 34% GL Adherent 59% 27% Hosp Mortality 6.7% 17.8% (Death assoc with low consciousness, leucopenia, no GL rx) Annals Intern Med 2009 Antimicrobial Therapy Treatment for Patients at Risk for MDR Organisms Anti-pseudomonal beta-lactam + Aminoglycoside or Fluoroquinolone + Vancomycin or Linezolid IDSA/ATS 2005 Kollef CID 2008
19 Treating HCAP by the Guidelines Survey of 1300 faculty Hospitalists, Pulm/Crit Care, ED Why Did They (we) Fail? Single Agent for 70 GNRs 60 9 clinical case questions 50 Also asked: 2. No MRSA coverage 40 Are you familiar with the 30 HCAP guidelines? 20 Do you agree with the 10 HCAP guidelines? 0 GL Agreement CAP GL Concordance HCAP GL Concordance Seymann, et al. CID, In Press Predicting MDR Infections Retrospective review 640 culture + pneumonia pts MDR Variables OR Recent Hosp 4.2 NH or LTC 2.8 Dialysis 2.1 ICU 1.6 MRSA Risk Recent Hosp 2.4 NH 1.9 ICU 1.7 % with resistant infections Arch Intern Med, >6 Points: 4pts-recent hosp 3pts-NH 2pts-HD 1pt-ICU 10pts max (Of all patients with HCAP criteria only 50% had MDR organisms) Nursing Home Acquired Pneumonia Non-Severe Pneumonia Loeb, et al JAMA 2006 RCT 20 Nursing Homes; Pneumonia pathway vs. Usual care 350 patients in each arm, mean age 85 Pathway: if po, HR <100, RR<30, SBP>90, sat > 90% then po Levo Pathway Usual Care Admission 10% 20% (p=0.001) Hosp days / pt (p=0.004) Mortality 3% 6% (p=0.23) Costs / resident $1200 $2200 (p < 0.05)
* Both positive: 90% MDRs Both negative: 0% MDRs ADL Score: 6 components, score each 1 point=independent, 2=partial, 3=independent El Solh CID 2004 Niederman Clin Chest Med 2007 Nursing Home")
20 Nursing Home Acquired Pneumonia (NHAP) Predictors of Drug Resistant Bacteria 135 nursing home patients admitted to ICU Antibiotic use > 48 hrs in past 6 months Poor functional status (ADL score > 12.5)* Both positive: 90% MDRs Both negative: 0% MDRs ADL Score: 6 components, score each 1 point=independent, 2=partial, 3=independent El Solh CID 2004 Niederman Clin Chest Med 2007 Nursing Home Acquired Pneumonia (NHAP) Effect of Guidelines on NHAP outcomes 334 non-icu patients admitted with CAP from NH 77% treated per 2003 GL (no HCAP coverage) 23% treated per 2005 GL (HCAP rx) Propensity score and process measure adjusted No difference in in-hospital or 30 d mortality Longer time to orals and LOS with 2005 GL rx El Solh, 2009
21 HCAP Treatment Algorithm Cur Opinion Infect Dis 2009 HCAP Treatment Algorithm ADD Indwelling Devices (PICC, urinary Catheter, feeding tube) Advanced Respiratory Disease (Severe COPD, Bronchiectasis) Cur Opinion Infect Dis 2009 Prevention PPIs and Hospital Acquired Pneumonia (HAP) All adult admits for > 3d; AMC in Boston: Excluded ICU pts 52% received acid suppressive rx (83% were PPIs) Propensity matched risk assessment of PPI use Condition Odds Ratio HAP 1.3 Aspiration pneumonia 1.4 Non-aspiration pneumonia 1.5 (180,000 excess HAP cases and 33,000 deaths /yr) JAMA 2009
22 Preventing HCAP / HAP Hand hygiene Elevate HOB > 45 degrees Minimize feeding tubes Avoid contributing drugs (PPI, Sedatives) Oral hygiene Brushing q 8 hrs Chlorhexidine mouth wash Oropharyngeal decontamination (Tobra, Colistin, Ampho B; 30 d mortality OR 0.86 ( ) NEJM 2009 CAP / HCAP Key Points START CAP: Risk stratifying for CA-MRSA, Pseudomonas and consider rx CAP: Considering SO-H1N1 as a possible etiology HCAP: Risk stratifying for MDR pathogens HCAP: Treating those at low risk with narrow spectrum abx HCAP: Treating those at high risk with broad spectrum abx STOP CAP: Routinely treating beyond 7 days CAP: Doing blood cultures in everyone HCAP: Treating all NHAP with broad spectrum abx HCAP: Routinely treating beyond 8 days CAP / HCAP Key Points CONSIDER CAP: SMART-COP to risk stratify for ICU admissions CAP: Atypical coverage may not be adding much CAP: Procalcitonin may be coming soon CAP/HCAP: Avoiding / Stopping unnecessary PPIs, antipsychotics HCAP / HAP: oral hygiene
Pneumonia Update Overview. Community-Acquired Pneumonia. Management of the Hospitalized Patient. Care of the Hospitalized Patient
 Pneumonia Update 2009 Management of the Hospitalized Patient Scott A. Flanders, M.D. Professor of Medicine Director, Hospitalist Program University of Michigan Overview Community Acquired Pneumonia (CAP)
Pneumonia Update 2009 Management of the Hospitalized Patient Scott A. Flanders, M.D. Professor of Medicine Director, Hospitalist Program University of Michigan Overview Community Acquired Pneumonia (CAP)
Pneumonia Update Overview" Community-Acquired Pneumonia" Management of the Hospitalized Patient. Care of the Hospitalized Patient"
 Pneumonia Update 2010 Management of the Hospitalized Patient Scott A. Flanders, M.D." Professor of Medicine" Director, Hospitalist Program" University of Michigan" Overview" Community Acquired Pneumonia
Pneumonia Update 2010 Management of the Hospitalized Patient Scott A. Flanders, M.D." Professor of Medicine" Director, Hospitalist Program" University of Michigan" Overview" Community Acquired Pneumonia
Brice Taylor Assistant Professor Division of Pulmonary and Critical Care Medicine
 Brice Taylor Assistant Professor Division of Pulmonary and Critical Care Medicine Discuss advances in predicting prognosis Understand dwhat we know (and don t know) about the Microbiology Recognize important
Brice Taylor Assistant Professor Division of Pulmonary and Critical Care Medicine Discuss advances in predicting prognosis Understand dwhat we know (and don t know) about the Microbiology Recognize important
Community Acquired & Nosocomial Pneumonias
 Community Acquired & Nosocomial Pneumonias IDSA/ATS 2007 & 2016 Guidelines José Luis González, MD Clinical Assistant Professor of Medicine Outline Intro - Definitions & Diagnosing CAP treatment VAP & HAP
Community Acquired & Nosocomial Pneumonias IDSA/ATS 2007 & 2016 Guidelines José Luis González, MD Clinical Assistant Professor of Medicine Outline Intro - Definitions & Diagnosing CAP treatment VAP & HAP
Pneumonia Community-Acquired Healthcare-Associated
 Pneumonia Community-Acquired Healthcare-Associated Edwin Yu Clin Infect Dis 2007;44(S2):27-72 Am J Respir Crit Care Med 2005; 171:388-416 IDSA / ATS Guidelines Microbiology Principles and Practice of Infectious
Pneumonia Community-Acquired Healthcare-Associated Edwin Yu Clin Infect Dis 2007;44(S2):27-72 Am J Respir Crit Care Med 2005; 171:388-416 IDSA / ATS Guidelines Microbiology Principles and Practice of Infectious
CAP, HCAP, HAP, VAP. 1. In 1898, William Osler described community-acquired pneumonia as:
 1. In 1898, William Osler described community-acquired pneumonia as: Brad Sharpe, M.D. Professor of Clinical Medicine Department of Medicine UCSF sharpeb@medicine.ucsf.edu I have no relevant financial
1. In 1898, William Osler described community-acquired pneumonia as: Brad Sharpe, M.D. Professor of Clinical Medicine Department of Medicine UCSF sharpeb@medicine.ucsf.edu I have no relevant financial
Bradley A. Sharpe, M.D. Associate Professor Medicine Department of Medicine UCSF -- William Osler, M.D.
 Bradley A. Sharpe, M.D. Associate Professor Medicine Department of Medicine UCSF sharpeb@medicine.ucsf.edu a. An ailment that often leads to suffocation and death. b. A friend of the aged. c. A common
Bradley A. Sharpe, M.D. Associate Professor Medicine Department of Medicine UCSF sharpeb@medicine.ucsf.edu a. An ailment that often leads to suffocation and death. b. A friend of the aged. c. A common
MDR AGENTS: RISK FACTORS AND THERAPEUTIC STRATEGIES
 MDR AGENTS: RISK FACTORS AND THERAPEUTIC STRATEGIES 1 Marin H. Kollef, MD Professor of Medicine Virginia E. and Sam J. Golman Chair in Respiratory Intensive Care Medicine Washington University School of
MDR AGENTS: RISK FACTORS AND THERAPEUTIC STRATEGIES 1 Marin H. Kollef, MD Professor of Medicine Virginia E. and Sam J. Golman Chair in Respiratory Intensive Care Medicine Washington University School of
Bradley A. Sharpe, M.D. Associate Professor Medicine Department of Medicine UCSF
 Maximizing Care for Community- Acquired Pneumonia Bradley A. Sharpe, M.D. Associate Professor Medicine Department of Medicine UCSF sharpeb@medicine.ucsf.edu 1. In 1898, William Osler described community-acquired
Maximizing Care for Community- Acquired Pneumonia Bradley A. Sharpe, M.D. Associate Professor Medicine Department of Medicine UCSF sharpeb@medicine.ucsf.edu 1. In 1898, William Osler described community-acquired
Pneumonia in Older Adults: An Update
 Pneumonia in Older Adults: An Update - 2010 Suzanne F. Bradley, M.D. Professor of Internal Medicine Geriatrics & Infectious Diseases University of Michigan Medical School GRECC - VA Ann Arbor HCS ID Hospitalizations
Pneumonia in Older Adults: An Update - 2010 Suzanne F. Bradley, M.D. Professor of Internal Medicine Geriatrics & Infectious Diseases University of Michigan Medical School GRECC - VA Ann Arbor HCS ID Hospitalizations
Community Acquired Pneumonia. Background & Rationale to North American Guidelines. Lionel Mandell MD FRCPC Brussels Belgium
 Community Acquired Pneumonia Background & Rationale to North American Guidelines Lionel Mandell MD FRCPC Brussels Belgium Consider Impact of the disease Issues to reflect upon Impact of the Disease 3-4
Community Acquired Pneumonia Background & Rationale to North American Guidelines Lionel Mandell MD FRCPC Brussels Belgium Consider Impact of the disease Issues to reflect upon Impact of the Disease 3-4
Pneumonia in the Hospitalized
 Pneumonia in the Hospitalized Patient: Use of Steroids Nicolette Myers, MD Pulmonary/Sleep/Critical Care November 9, 2018 Park Nicollet Clinic Facts About Pneumonia CAP is the 8 th most common cause of
Pneumonia in the Hospitalized Patient: Use of Steroids Nicolette Myers, MD Pulmonary/Sleep/Critical Care November 9, 2018 Park Nicollet Clinic Facts About Pneumonia CAP is the 8 th most common cause of
UPDATE IN HOSPITAL MEDICINE
 UPDATE IN HOSPITAL MEDICINE FLORIDA CHAPTER ACP MEETING 2016 Himangi Kaushal, M.D., F.A.C.P. Program Director Memorial Healthcare System Internal Medicine Residency DISCLOSURES None OBJECTIVES Review some
UPDATE IN HOSPITAL MEDICINE FLORIDA CHAPTER ACP MEETING 2016 Himangi Kaushal, M.D., F.A.C.P. Program Director Memorial Healthcare System Internal Medicine Residency DISCLOSURES None OBJECTIVES Review some
Antimicrobial Stewardship in Community Acquired Pneumonia
 Antimicrobial Stewardship in Community Acquired Pneumonia Medicine Review Course 2018 Dr Lee Tau Hong Consultant Department of Infectious Diseases National Centre for Infectious Diseases Scope 1. Diagnosis
Antimicrobial Stewardship in Community Acquired Pneumonia Medicine Review Course 2018 Dr Lee Tau Hong Consultant Department of Infectious Diseases National Centre for Infectious Diseases Scope 1. Diagnosis
How do we define pneumonia?
 Robert L. Keith MD FCCP Associate Professor of Medicine Division of Pulmonary Sciences & Critical Care Medicine Denver VA Medical Center University of Colorado Denver How do we define pneumonia? Fever
Robert L. Keith MD FCCP Associate Professor of Medicine Division of Pulmonary Sciences & Critical Care Medicine Denver VA Medical Center University of Colorado Denver How do we define pneumonia? Fever
Care Guideline DRAFT for review cycle 08/02/17 CARE OF THE ADULT PNEUMONIA PATIENT
 Care Guideline DRAFT for review cycle 08/02/17 CARE OF THE ADULT PNEUMONIA PATIENT Target Audience: All MHS employed providers within Primary Care, Urgent Care, and In-Hospital Care. The secondary audience
Care Guideline DRAFT for review cycle 08/02/17 CARE OF THE ADULT PNEUMONIA PATIENT Target Audience: All MHS employed providers within Primary Care, Urgent Care, and In-Hospital Care. The secondary audience
Pneumonia Severity Scores:
 Pneumonia Severity Scores: Are they Accurate Predictors of Mortality? JILL McEWEN, MD FRCPC Clinical Professor Department of Emergency Medicine University of British Columbia Vancouver, BC Canada President,
Pneumonia Severity Scores: Are they Accurate Predictors of Mortality? JILL McEWEN, MD FRCPC Clinical Professor Department of Emergency Medicine University of British Columbia Vancouver, BC Canada President,
Upper...and Lower Respiratory Tract Infections
 Upper...and Lower Respiratory Tract Infections Robin Jump, MD, PhD Cleveland Geriatric Research Education and Clinical Center (GRECC) Louis Stokes Cleveland VA Medical Center Case Western Reserve University
Upper...and Lower Respiratory Tract Infections Robin Jump, MD, PhD Cleveland Geriatric Research Education and Clinical Center (GRECC) Louis Stokes Cleveland VA Medical Center Case Western Reserve University
Disclosures. Case 1. Acute Bronchitis. Acute Bronchitis. Community-Acquired Pneumonia and other Respiratory Tract Infections. What do you recommend?
 Community-Acquired Pneumonia and other Respiratory Tract Infections none Disclosures Joel T. Katz, M.D. Associate Professor of Medicine Division of Infectious Diseases Brigham and Women s Hospital Case
Community-Acquired Pneumonia and other Respiratory Tract Infections none Disclosures Joel T. Katz, M.D. Associate Professor of Medicine Division of Infectious Diseases Brigham and Women s Hospital Case
Guidelines/Guidance/CAP/ Hospitalized Child. PHM Boot Camp 2014 Jay Tureen, MD June 19, 2014
 Guidelines/Guidance/CAP/ Hospitalized Child PHM Boot Camp 2014 Jay Tureen, MD June 19, 2014 CAP in Children: Epi Greatest cause of death in children worldwide Estimated > 2 M deaths in children In developed
Guidelines/Guidance/CAP/ Hospitalized Child PHM Boot Camp 2014 Jay Tureen, MD June 19, 2014 CAP in Children: Epi Greatest cause of death in children worldwide Estimated > 2 M deaths in children In developed
CARE OF THE ADULT PNEUMONIA PATIENT
 Care Guideline CARE OF THE ADULT PNEUMONIA PATIENT Target Audience: The target audience for this Care Guideline is all MultiCare providers and staff, including those associated with our clinically integrated
Care Guideline CARE OF THE ADULT PNEUMONIA PATIENT Target Audience: The target audience for this Care Guideline is all MultiCare providers and staff, including those associated with our clinically integrated
Michael S. Niederman, M.D. Clinical Director Pulmonary and Critical Care Medicine New York Presbyterian Hospital Weill Cornell Medical Center
 CA-MRSA Pneumonia Michael S. Niederman, M.D. Clinical Director Pulmonary and Critical Care Medicine New York Presbyterian Hospital Weill Cornell Medical Center Professor of Clinical Medicine Weill Cornell
CA-MRSA Pneumonia Michael S. Niederman, M.D. Clinical Director Pulmonary and Critical Care Medicine New York Presbyterian Hospital Weill Cornell Medical Center Professor of Clinical Medicine Weill Cornell
Potential Conflicts of Interests
 Potential Conflicts of Interests Research Grants Agency for Healthcare Research and Quality Akers Bioscience, Inc. Pfizer, Inc. Scientific Advisory Boards Pfizer, Inc. Cadence Pharmaceuticals Kimberly
Potential Conflicts of Interests Research Grants Agency for Healthcare Research and Quality Akers Bioscience, Inc. Pfizer, Inc. Scientific Advisory Boards Pfizer, Inc. Cadence Pharmaceuticals Kimberly
COPD exacerbation. Dr. med. Frank Rassouli
 Definition according to GOLD report: - «An acute event - characterized by a worsening of the patients respiratory symptoms - that is beyond normal day-to-day variations - and leads to a change in medication»
Definition according to GOLD report: - «An acute event - characterized by a worsening of the patients respiratory symptoms - that is beyond normal day-to-day variations - and leads to a change in medication»
Update in Hospital Medicine. Update in Hospital Medicine 2009
 2009 Bradley A. Sharpe, MD UCSF Division of Hospital Medicine PE in Acute COPD Exacerbations Question: What is the prevalence of PE in patients with COPD who need hospitalization? Design: Systematic review,
2009 Bradley A. Sharpe, MD UCSF Division of Hospital Medicine PE in Acute COPD Exacerbations Question: What is the prevalence of PE in patients with COPD who need hospitalization? Design: Systematic review,
Hospital-acquired Pneumonia
 Hospital-acquired Pneumonia Hospital-acquired pneumonia (HAP) Pneumonia that occurs at least 2 days after hospital admission. The second most common and the leading cause of death due to hospital-acquired
Hospital-acquired Pneumonia Hospital-acquired pneumonia (HAP) Pneumonia that occurs at least 2 days after hospital admission. The second most common and the leading cause of death due to hospital-acquired
Severe β-lactam allergy. Alternative (use for mild-moderate β-lactam allergy) therapy
 therapy") Recommended Empirical Antibiotic Regimens for MICU Patients Notes: The antibiotic regimens shown are general guidelines and should not replace clinical judgment. Always assess for antibiotic allergies.
Recommended Empirical Antibiotic Regimens for MICU Patients Notes: The antibiotic regimens shown are general guidelines and should not replace clinical judgment. Always assess for antibiotic allergies.
Pneumonia: The Forgotten Killer
 Pneumonia: The Forgotten Killer David Glenn Weismiller, MD, ScM, FAAFP Department of Family and Community Medicine University of Nevada, Las Vegas School of Medicine Disclosure Statement It is the policy
Pneumonia: The Forgotten Killer David Glenn Weismiller, MD, ScM, FAAFP Department of Family and Community Medicine University of Nevada, Las Vegas School of Medicine Disclosure Statement It is the policy
Community-Acquired Pneumonia. Lisa G. Winston, MD University of California, San Francisco San Francisco General Hospital. Nothing to disclose.
 Community-Acquired Pneumonia Lisa G. Winston, MD University of California, San Francisco San Francisco General Hospital Nothing to disclose. Community-Acquired Pneumonia Talk will focus on adults Guideline
Community-Acquired Pneumonia Lisa G. Winston, MD University of California, San Francisco San Francisco General Hospital Nothing to disclose. Community-Acquired Pneumonia Talk will focus on adults Guideline
Guidelines for Pneumonia
 Guidelines for Pneumonia Michael S. Niederman, MD Professor of Medicine Vice-Chairman, Department of Medicine State University of New York at Stony Brook Chairman, Department of Medicine Winthrop-University
Guidelines for Pneumonia Michael S. Niederman, MD Professor of Medicine Vice-Chairman, Department of Medicine State University of New York at Stony Brook Chairman, Department of Medicine Winthrop-University
Viral Threat on Respiratory Failure
 Viral Threat on Respiratory Failure Younsuck Koh, MD, PhD, FCCM Department of Pulmonary and Critical Care Medicine Asan Medical Center University of Ulsan College of Medicine Seoul, Korea No Conflict of
Viral Threat on Respiratory Failure Younsuck Koh, MD, PhD, FCCM Department of Pulmonary and Critical Care Medicine Asan Medical Center University of Ulsan College of Medicine Seoul, Korea No Conflict of
Charles Krasner, M.D. University of NV, Reno School of Medicine Sierra NV Veterans Affairs Medical Center
 Charles Krasner, M.D. University of NV, Reno School of Medicine Sierra NV Veterans Affairs Medical Center Kathy Peters is a 63 y.o. patient that presents to your urgent care office today with a history
Charles Krasner, M.D. University of NV, Reno School of Medicine Sierra NV Veterans Affairs Medical Center Kathy Peters is a 63 y.o. patient that presents to your urgent care office today with a history
Sepsis new definitions of sepsis and septic shock and Novelities in sepsis treatment
 Sepsis new definitions of sepsis and septic shock and Novelities in sepsis treatment What is sepsis? Life-threatening organ dysfunction caused by a dysregulated host response to infection A 1991 consensus
Sepsis new definitions of sepsis and septic shock and Novelities in sepsis treatment What is sepsis? Life-threatening organ dysfunction caused by a dysregulated host response to infection A 1991 consensus
Aspiration pneumonia in older people
 Aspiration pneumonia in older people Ayman Morish, M.D. Internal medicine, Critical care Medicine and Geriatrics Fellow. Contents Epidemiology Causes of aspiration pneumonia Issues of older age Management
Aspiration pneumonia in older people Ayman Morish, M.D. Internal medicine, Critical care Medicine and Geriatrics Fellow. Contents Epidemiology Causes of aspiration pneumonia Issues of older age Management
Clinical Practice Guidelines for Nursing- and Healthcareassociated Pneumonia (NHCAP) [Complete translation] $
![Clinical Practice Guidelines for Nursing- and Healthcareassociated Pneumonia (NHCAP) [Complete translation] $](/thumbs/80/82455300.jpg "Clinical Practice Guidelines for Nursing- and Healthcareassociated Pneumonia (NHCAP) [Complete translation] $") respiratory investigation 51 (2013) 103 126 Contents lists available at SciVerse ScienceDirect Respiratory Investigation journal homepage: www.elsevier.com/locate/resinv Guideline Clinical Practice Guidelines
respiratory investigation 51 (2013) 103 126 Contents lists available at SciVerse ScienceDirect Respiratory Investigation journal homepage: www.elsevier.com/locate/resinv Guideline Clinical Practice Guidelines
Community Acquired Pneumonia: Measures to Improve Management and Healthcare Quality
 Community Acquired Pneumonia: Measures to Improve Management and Healthcare Quality Gonzalo Bearman MD, MPH Assistant Professor of Internal Medicine Divisions of Quality Health Care & Infectious Diseases
Community Acquired Pneumonia: Measures to Improve Management and Healthcare Quality Gonzalo Bearman MD, MPH Assistant Professor of Internal Medicine Divisions of Quality Health Care & Infectious Diseases
Dilemmas in Septic Shock
 Dilemmas in Septic Shock William Janssen, M.D. Assistant Professor of Medicine National Jewish Health University of Colorado Denver Health Sciences Center A 62 year-old female presents to the ED with fever,
Dilemmas in Septic Shock William Janssen, M.D. Assistant Professor of Medicine National Jewish Health University of Colorado Denver Health Sciences Center A 62 year-old female presents to the ED with fever,
Pneumococcal pneumonia
 Pneumococcal pneumonia Wei Shen Lim Consultant Respiratory Physician & Honorary Professor of Medicine Nottingham University Hospitals NHS Trust University of Nottingham Declarations of interest Unrestricted
Pneumococcal pneumonia Wei Shen Lim Consultant Respiratory Physician & Honorary Professor of Medicine Nottingham University Hospitals NHS Trust University of Nottingham Declarations of interest Unrestricted
PNEUMONIA. Patient Case: Chief Complaint: I have been short of breath and have been coughing up rust-colored phlegm for the past 3 days.
 PNEUMONIA Relevant Guidelines: 2008 IDSA CAP guidelines: http://www.idsociety.org/guidelines/patient_care/idsa_practice_guidelines/infections_by_org an_system/lower/upper_respiratory/community-acquired_pneumonia_(cap)/
PNEUMONIA Relevant Guidelines: 2008 IDSA CAP guidelines: http://www.idsociety.org/guidelines/patient_care/idsa_practice_guidelines/infections_by_org an_system/lower/upper_respiratory/community-acquired_pneumonia_(cap)/
Pneumonia 2017 OMAR PIRZADA
 Pneumonia 2017 OMAR PIRZADA Pneumonia Pneumonia is common 0.5-1% of adults per year, 5-12% presenting to GP with LRTi 22-42% will be admitted to hospital Symptoms and signs Case 1 26 year old man Sudden
Pneumonia 2017 OMAR PIRZADA Pneumonia Pneumonia is common 0.5-1% of adults per year, 5-12% presenting to GP with LRTi 22-42% will be admitted to hospital Symptoms and signs Case 1 26 year old man Sudden
HEALTHCARE-ASSOCIATED PNEUMONIA: EPIDEMIOLOGY, MICROBIOLOGY & PATHOPHYSIOLOGY
 HEALTHCARE-ASSOCIATED PNEUMONIA: EPIDEMIOLOGY, MICROBIOLOGY & PATHOPHYSIOLOGY David Jay Weber, M.D., M.P.H. Professor of Medicine, Pediatrics, & Epidemiology Associate Chief Medical Officer, UNC Health
HEALTHCARE-ASSOCIATED PNEUMONIA: EPIDEMIOLOGY, MICROBIOLOGY & PATHOPHYSIOLOGY David Jay Weber, M.D., M.P.H. Professor of Medicine, Pediatrics, & Epidemiology Associate Chief Medical Officer, UNC Health
Epidemiology of Infectious Complications of H1N1 Influenza Virus Infection
 Epidemiology of Infectious Complications of H1N1 Influenza Virus Infection Lyn Finelli, DrPH, MS Lead, Influenza Surveillance and Outbreak Response Epidemiology and Prevention Branch Influenza Division
Epidemiology of Infectious Complications of H1N1 Influenza Virus Infection Lyn Finelli, DrPH, MS Lead, Influenza Surveillance and Outbreak Response Epidemiology and Prevention Branch Influenza Division
Nosocomial Pneumonia. <5 Days: Non-Multidrug-Resistant Bacteria
 Nosocomial Pneumonia Meredith Deutscher, MD Troy Schaffernocker, MD Ohio State University Burden of Hospital-Acquired Pneumonia Second most common nosocomial infection in the U.S. 5-10 episodes per 1000
Nosocomial Pneumonia Meredith Deutscher, MD Troy Schaffernocker, MD Ohio State University Burden of Hospital-Acquired Pneumonia Second most common nosocomial infection in the U.S. 5-10 episodes per 1000
Avian Influenza A (H7N9): Clinical Management. KW Choi Associate Consultant IDCTC, HA/ ICB, CHP
: Clinical Management. KW Choi Associate Consultant IDCTC, HA/ ICB, CHP") Avian Influenza A (H7N9): Clinical Management KW Choi Associate Consultant IDCTC, HA/ ICB, CHP Initial symptoms: nonspecific, similar to most other causes of ILI, CAP High index of suspicion and alertness
Avian Influenza A (H7N9): Clinical Management KW Choi Associate Consultant IDCTC, HA/ ICB, CHP Initial symptoms: nonspecific, similar to most other causes of ILI, CAP High index of suspicion and alertness
Guidelines. 14 Nov Marc Bonten
 Guidelines 14 Nov 2014 Marc Bonten Treatment of Community-Acquired Pneumonia SWAB/ NVALT guideline 2011, replaced SWAB guideline 2005 Empirical treatment must cover the most likely causative pathogen.
Guidelines 14 Nov 2014 Marc Bonten Treatment of Community-Acquired Pneumonia SWAB/ NVALT guideline 2011, replaced SWAB guideline 2005 Empirical treatment must cover the most likely causative pathogen.
Epidemiology and Etiology of Community-Acquired Pneumonia 761 Lionel A. Mandell
 LOWER RESPIRATORY TRACT INFECTIONS Preface Thomas M. File, Jr xiii Community-Acquired Pneumonia: Pathophysiology and Host Factors with Focus on Possible New Approaches to Management of Lower Respiratory
LOWER RESPIRATORY TRACT INFECTIONS Preface Thomas M. File, Jr xiii Community-Acquired Pneumonia: Pathophysiology and Host Factors with Focus on Possible New Approaches to Management of Lower Respiratory
Guidelines 2017 for the management of hospitalacquired pneumonia (HAP) and. ventilator-associated. pneumonia (VAP)
 and. ventilator-associated. pneumonia (VAP)") Guidelines 2017 for the management of hospitalacquired pneumonia (HAP) and ventilator-associated Modifiez le style des sous-titres du masque pneumonia (VAP) Filip Moerman Présentation pour les soins int
Guidelines 2017 for the management of hospitalacquired pneumonia (HAP) and ventilator-associated Modifiez le style des sous-titres du masque pneumonia (VAP) Filip Moerman Présentation pour les soins int
Objectives. Pneumonia. Pneumonia. Epidemiology. Prevalence 1/7/2012. Community-Acquired Pneumonia in infants and children
 Objectives Community-Acquired in infants and children Review of Clinical Practice Guidelines by the Pediatric Infectious Diseases Society and the Infectious Diseases Society of America - 2011 Sabah Charania,
Objectives Community-Acquired in infants and children Review of Clinical Practice Guidelines by the Pediatric Infectious Diseases Society and the Infectious Diseases Society of America - 2011 Sabah Charania,
KAISER PERMANENTE OHIO COMMUNITY ACQUIRED PNEUMONIA
 KAISER PERMANENTE OHIO COMMUNITY ACQUIRED PNEUMONIA Methodology: Expert opinion Issue Date: 8-97 Champion: Pulmonary Medicine Most Recent Update: 6-08, 7-10, 7-12 Key Stakeholders: Pulmonary Medicine,
KAISER PERMANENTE OHIO COMMUNITY ACQUIRED PNEUMONIA Methodology: Expert opinion Issue Date: 8-97 Champion: Pulmonary Medicine Most Recent Update: 6-08, 7-10, 7-12 Key Stakeholders: Pulmonary Medicine,
ANWICU knowledge
 ANWICU knowledge www.anwicu.org.uk This presenta=on is provided by ANWICU We are a collabora=ve associa=on of ICUs in the North West of England. Permission to provide this presenta=on has been granted
ANWICU knowledge www.anwicu.org.uk This presenta=on is provided by ANWICU We are a collabora=ve associa=on of ICUs in the North West of England. Permission to provide this presenta=on has been granted
Influenza A (H1N1)pdm09 in Minnesota Epidemiology
pdm09 in Minnesota Epidemiology") Influenza A (H1N1)pdm09 in Minnesota Epidemiology Infectious Disease Epidemiology, Prevention and Control Division PO Box 64975 St. Paul, MN 55164-0975 Number of Influenza Hospitalizations by Influenza
Influenza A (H1N1)pdm09 in Minnesota Epidemiology Infectious Disease Epidemiology, Prevention and Control Division PO Box 64975 St. Paul, MN 55164-0975 Number of Influenza Hospitalizations by Influenza
Sepsi: nuove definizioni, approccio diagnostico e terapia
 GIORNATA MONDIALE DELLA SEPSI DIAGNOSI E GESTIONE CLINICA DELLA SEPSI Giovedì, 13 settembre 2018 Sepsi: nuove definizioni, approccio diagnostico e terapia Nicola Petrosillo Società Italiana Terapia Antiinfettiva
GIORNATA MONDIALE DELLA SEPSI DIAGNOSI E GESTIONE CLINICA DELLA SEPSI Giovedì, 13 settembre 2018 Sepsi: nuove definizioni, approccio diagnostico e terapia Nicola Petrosillo Società Italiana Terapia Antiinfettiva
The Challenge of Managing Staphylococcus aureus Bacteremia
 The Challenge of Managing Staphylococcus aureus Bacteremia M A R G A R E T G R A Y B S P F C S H P C L I N I C A L P R A C T I C E M A N A G E R N O R T H / I D P H A R M A C I S T A L B E R T A H E A
The Challenge of Managing Staphylococcus aureus Bacteremia M A R G A R E T G R A Y B S P F C S H P C L I N I C A L P R A C T I C E M A N A G E R N O R T H / I D P H A R M A C I S T A L B E R T A H E A
PULMONARY EMERGENCIES
 EMERGENCIES I. Pneumonia A. Bacterial Pneumonia (most common cause of a focal infiltrate) 1. Epidemiology a. Accounts for up to 10% of hospital admissions in the U.S. b. Most pneumonias are the result
EMERGENCIES I. Pneumonia A. Bacterial Pneumonia (most common cause of a focal infiltrate) 1. Epidemiology a. Accounts for up to 10% of hospital admissions in the U.S. b. Most pneumonias are the result
Continuous Infusion of Antibiotics In The ICU: What Is Proven? Professor of Medicine Vice-Chairman, Department of Medicine SUNY at Stony Brook
 Continuous Infusion of Antibiotics In The ICU: What Is Proven? Michael S. Niederman, M.D. Chairman, Department of Medicine Winthrop-University Hospital Mineola, NY Professor of Medicine Vice-Chairman,
Continuous Infusion of Antibiotics In The ICU: What Is Proven? Michael S. Niederman, M.D. Chairman, Department of Medicine Winthrop-University Hospital Mineola, NY Professor of Medicine Vice-Chairman,
Respiratory Syncytial Virus (RSV) in Older Adults: A Hidden Annual Epidemic. Webinar Agenda
 in Older Adults: A Hidden Annual Epidemic. Webinar Agenda") Respiratory Syncytial Virus (RSV) in Older Adults: A Hidden Annual Epidemic Wednesday, November 2, 2016 12:00 PM ET Webinar Agenda Agenda Welcome and Introductions William Schaffner, MD, NFID Medical Director
Respiratory Syncytial Virus (RSV) in Older Adults: A Hidden Annual Epidemic Wednesday, November 2, 2016 12:00 PM ET Webinar Agenda Agenda Welcome and Introductions William Schaffner, MD, NFID Medical Director
Treatment of febrile neutropenia in patients with neoplasia
 Treatment of febrile neutropenia in patients with neoplasia George Samonis MD, PhD Medical Oncologist Infectious Diseases Specialist Professor of Medicine The University of Crete, Heraklion,, Crete, Greece
Treatment of febrile neutropenia in patients with neoplasia George Samonis MD, PhD Medical Oncologist Infectious Diseases Specialist Professor of Medicine The University of Crete, Heraklion,, Crete, Greece
Community-Acquired Pneumonia OBSOLETE 2
 Community-Acquired Pneumonia OBSOLETE 2 Clinical practice guidelines serve as an educational reference, and do not supersede the clinical judgment of the treating physician with respect to appropriate
Community-Acquired Pneumonia OBSOLETE 2 Clinical practice guidelines serve as an educational reference, and do not supersede the clinical judgment of the treating physician with respect to appropriate
Swine Influenza Update #3. Triage, Assessment, and Care of Patients Presenting with Respiratory Symptoms
 Updated 12:00 p.m. April 30, 2009 Swine Influenza Update #3 Introduction: This document revises our last update which was sent April 28 th, 2009. The most important revisions include the following: 1.
Updated 12:00 p.m. April 30, 2009 Swine Influenza Update #3 Introduction: This document revises our last update which was sent April 28 th, 2009. The most important revisions include the following: 1.
Lanny Hsieh, M.D. Infectious Diseases Hospitalist Program
 Lanny Hsieh, M.D. Infectious Diseases Hospitalist Program Definition of Fever Arbitrary 38.0-38.4 (low grade may be significant in immunocompromised patients) > 38.5 (nurse will call you) Be aware of
Lanny Hsieh, M.D. Infectious Diseases Hospitalist Program Definition of Fever Arbitrary 38.0-38.4 (low grade may be significant in immunocompromised patients) > 38.5 (nurse will call you) Be aware of
CLAIRE NOWLAN & SAM SEARLE. Pneumonia in the nursing home
 CLAIRE NOWLAN & SAM SEARLE Pneumonia in the nursing home No disclosures or conflicts of interest PMHX: A. FIB. GERD MIXED DEMENTIA MMSE 16/30 HTN Mr. Hack 86 years old RAMIPRIL 4 MG OD PARIET 20MG OD DONEPEZIL
CLAIRE NOWLAN & SAM SEARLE Pneumonia in the nursing home No disclosures or conflicts of interest PMHX: A. FIB. GERD MIXED DEMENTIA MMSE 16/30 HTN Mr. Hack 86 years old RAMIPRIL 4 MG OD PARIET 20MG OD DONEPEZIL
Getting Smart About: Upper Respiratory Infections
 Getting Smart About: Upper Respiratory Infections Daniel Z. Uslan, MD Assistant Clinical Professor Director, Antimicrobial Stewardship Program UCLA Health System Disclosures None relevant to the topic
Getting Smart About: Upper Respiratory Infections Daniel Z. Uslan, MD Assistant Clinical Professor Director, Antimicrobial Stewardship Program UCLA Health System Disclosures None relevant to the topic
Journal Club The ELITE Trial. Sandra Katalinic, Pharmacy Resident University Hospital of Northern British Columbia April 28, 2010
 Journal Club The ELITE Trial Sandra Katalinic, Pharmacy Resident University Hospital of Northern British Columbia April 28, 2010 Overview Journal article Title, journal, authors, funding Abstract Introduction
Journal Club The ELITE Trial Sandra Katalinic, Pharmacy Resident University Hospital of Northern British Columbia April 28, 2010 Overview Journal article Title, journal, authors, funding Abstract Introduction
Community Acquired Pneumonia. Abdullah Alharbi, MD, FCCP
 Community Acquired Pneumonia Abdullah Alharbi, MD, FCCP A 68 y/ male presented to the ED with SOB and productive coughing for 2 days. Reports poor oral intake since onset due to nausea and intermittent
Community Acquired Pneumonia Abdullah Alharbi, MD, FCCP A 68 y/ male presented to the ED with SOB and productive coughing for 2 days. Reports poor oral intake since onset due to nausea and intermittent
SPECTRUM OF DISEASE. Rogelio Perez-Padilla MD National Institute of Respiratory Diseases, Mexico
 SPECTRUM OF DISEASE INFLUENZA A H1N1 Rogelio Perez-Padilla MD National Institute of Respiratory Diseases, Mexico DEATHS ARDS PNEUMONIA ILI (fever) Use of health services Respiratory infections (mild) Self-care
SPECTRUM OF DISEASE INFLUENZA A H1N1 Rogelio Perez-Padilla MD National Institute of Respiratory Diseases, Mexico DEATHS ARDS PNEUMONIA ILI (fever) Use of health services Respiratory infections (mild) Self-care
27/11/2012. Parainfuenza 1, 2 3 Rhinovirus Coronavirus Adenovirus Respiratory syncytial virus (RSV) Chlamydophila pneumoniae Mycoplasma pneumonite
 Chlamydophila pneumoniae Mycoplasma pneumonite") 8 «Evidence-based Medicine-» 27/11/2012,,,, : :,,,,,,,, (30%-50%) () (5%-10%) (40%-50%) 20% Infuenza A B Parainfuenza 1, 2 3 Rhinovirus Coronavirus Adenovirus Respiratory syncytial virus (RSV) Chlamydophila
8 «Evidence-based Medicine-» 27/11/2012,,,, : :,,,,,,,, (30%-50%) () (5%-10%) (40%-50%) 20% Infuenza A B Parainfuenza 1, 2 3 Rhinovirus Coronavirus Adenovirus Respiratory syncytial virus (RSV) Chlamydophila
10/2/2017. Pneumonia: Are We Missing the Mark? Objectives. Pneumonia
 Pneumonia: Are We Missing the Mark? LaDawna Goering, DNP, APN, ANP-BC Nick Van Hise, Pharm. D, BCPS Objectives Diagnose Pneumonia Evaluate severity of illness tools and site of care decisions Review diagnostic
Pneumonia: Are We Missing the Mark? LaDawna Goering, DNP, APN, ANP-BC Nick Van Hise, Pharm. D, BCPS Objectives Diagnose Pneumonia Evaluate severity of illness tools and site of care decisions Review diagnostic
Methicillin-Resistant Staphylococcus aureus (MRSA) S urveillance Report 2008 Background Methods
 S urveillance Report 2008 Background Methods") Methicillin-Resistant Staphylococcus aureus (MRSA) Surveillance Report 2008 Oregon Active Bacterial Core Surveillance (ABCs) Office of Disease Prevention & Epidemiology Oregon Department of Human Services
Methicillin-Resistant Staphylococcus aureus (MRSA) Surveillance Report 2008 Oregon Active Bacterial Core Surveillance (ABCs) Office of Disease Prevention & Epidemiology Oregon Department of Human Services
Pediatric influenza-associated deaths in Arizona,
 Pediatric influenza-associated deaths in Arizona, 2004-2012 (Poster is shared here as an 8.5 x11 document for easier viewing. All content is identical, though graphs and tables are formatted differently.)
Pediatric influenza-associated deaths in Arizona, 2004-2012 (Poster is shared here as an 8.5 x11 document for easier viewing. All content is identical, though graphs and tables are formatted differently.)
GUIDE TO INFECTION CONTROL IN THE HOSPITAL. Carbapenem-resistant Enterobacteriaceae
 GUIDE TO INFECTION CONTROL IN THE HOSPITAL CHAPTER 47: Carbapenem-resistant Enterobacteriaceae Authors E-B Kruse, MD H. Wisplinghoff, MD Chapter Editor Michelle Doll, MD, MPH) Topic Outline Key Issue Known
GUIDE TO INFECTION CONTROL IN THE HOSPITAL CHAPTER 47: Carbapenem-resistant Enterobacteriaceae Authors E-B Kruse, MD H. Wisplinghoff, MD Chapter Editor Michelle Doll, MD, MPH) Topic Outline Key Issue Known
Deep discoveries: the ED. Brian H. Rowe, MD, MSc, CCFP(EM) Canada Research Chair in Emergency Airway Diseases Department of Emergency Medicine
 Canada Research Chair in Emergency Airway Diseases Department of Emergency Medicine") Deep discoveries: Treating respiratory infections in the ED. Brian H. Rowe, MD, MSc, CCFP(EM) Canada Research Chair in Emergency Airway Diseases Department of Emergency Medicine University of Alberta Respiratory
Deep discoveries: Treating respiratory infections in the ED. Brian H. Rowe, MD, MSc, CCFP(EM) Canada Research Chair in Emergency Airway Diseases Department of Emergency Medicine University of Alberta Respiratory
Hospital Acquired Pneumonias
 Hospital Acquired Pneumonias Hospital Acquired Pneumonia ( HAP ) Hospital acquired pneumonia ( HAP ) is defined as an infection of the lung parenchyma developing during hospitalization and not present
Hospital Acquired Pneumonias Hospital Acquired Pneumonia ( HAP ) Hospital acquired pneumonia ( HAP ) is defined as an infection of the lung parenchyma developing during hospitalization and not present
Supplementary Online Content
 Supplementary Online Content Lee JS, Nsa W, Hausmann LRM, et al. Quality of care for elderly patients hospitalized for pneumonia in the United States, 2006 to 2010. JAMA Intern Med. Published online September
Supplementary Online Content Lee JS, Nsa W, Hausmann LRM, et al. Quality of care for elderly patients hospitalized for pneumonia in the United States, 2006 to 2010. JAMA Intern Med. Published online September
MCH-Immunization Conference. September 2012
 MCH-Immunization Conference September 2012 Rosalyn Singleton MD Arctic Investigations Program-CDC Alaska Native Tribal Health Consortium, Anchorage, AK DISCLAIMER: The results and conclusions presented
MCH-Immunization Conference September 2012 Rosalyn Singleton MD Arctic Investigations Program-CDC Alaska Native Tribal Health Consortium, Anchorage, AK DISCLAIMER: The results and conclusions presented
Bronchitis/Pneumonia Core Content Keith Conover, M.D., FACEP /15/02 Clinical Spectrum Chest pain, shoulder pain, neck pain, abdominal pain,
 Bronchitis/Pneumonia Core Content Keith Conover, M.D., FACEP 1.0 10/15/02 Clinical Spectrum Chest pain, shoulder pain, neck pain, abdominal pain, headache Links with smoking, pollen count, FH of asthma
Bronchitis/Pneumonia Core Content Keith Conover, M.D., FACEP 1.0 10/15/02 Clinical Spectrum Chest pain, shoulder pain, neck pain, abdominal pain, headache Links with smoking, pollen count, FH of asthma
Consequences for the clinicians
 30th Symposium : What will change in your daily practice with the new Elewijt, 26-05-2008 EUCAST breakpoints for antibiotic susceptibility testing Consequences for the clinicians Y.Van Laethem,MD CHU St
30th Symposium : What will change in your daily practice with the new Elewijt, 26-05-2008 EUCAST breakpoints for antibiotic susceptibility testing Consequences for the clinicians Y.Van Laethem,MD CHU St
Influenza-Associated Pediatric Deaths Case Report Form
 STATE USE ONLY DO NOT SEND INFORMATION IN THIS SECTION TO CDC Form approved OMB No. 0920-0007 Last Name: First Name: County: Address: City: State, Zip: Patient Demographics 1. State: 2. County: 3. State
STATE USE ONLY DO NOT SEND INFORMATION IN THIS SECTION TO CDC Form approved OMB No. 0920-0007 Last Name: First Name: County: Address: City: State, Zip: Patient Demographics 1. State: 2. County: 3. State
HEALTHCARE-ASSOCIATED PNEUMONIA: DIAGNOSIS, TREATMENT & PREVENTION
 HEALTHCARE-ASSOCIATED PNEUMONIA: DIAGNOSIS, TREATMENT & PREVENTION David Jay Weber, M.D., M.P.H. Professor of Medicine, Pediatrics, & Epidemiology Associate Chief Medical Officer, UNC Health Care Medical
HEALTHCARE-ASSOCIATED PNEUMONIA: DIAGNOSIS, TREATMENT & PREVENTION David Jay Weber, M.D., M.P.H. Professor of Medicine, Pediatrics, & Epidemiology Associate Chief Medical Officer, UNC Health Care Medical
POLICY FOR TREATMENT OF LOWER RESPIRATORY TRACT INFECTIONS
 POLICY F TREATMENT OF LOWER RESPIRATY TRACT INFECTIONS Written by: Dr M Milupi, Consultant Microbiologist Date: June 2018 Approved by: The Drugs & Therapeutics Committee Date: July 2018 Implementation
POLICY F TREATMENT OF LOWER RESPIRATY TRACT INFECTIONS Written by: Dr M Milupi, Consultant Microbiologist Date: June 2018 Approved by: The Drugs & Therapeutics Committee Date: July 2018 Implementation
The Old Man s Friend (And the Ire of Many an ED QI Director) Objectives. Terminology 10/22/2009
 Objectives. Terminology 10/22/2009") Pneumonia Management & Chris Fee, MD Assistant Clinical Professor UCSF Department of Emergency Medicine The Old Man s Friend (And the Ire of Many an ED QI Director) 7th leading cause of death in US 915,000
Pneumonia Management & Chris Fee, MD Assistant Clinical Professor UCSF Department of Emergency Medicine The Old Man s Friend (And the Ire of Many an ED QI Director) 7th leading cause of death in US 915,000
PNEUMONIA IN CHILDREN. IAP UG Teaching slides
 PNEUMONIA IN CHILDREN 1 INTRODUCTION 156 million new episodes / yr. worldwide 151 million episodes developing world 95% in developing countries 19% of all deaths in children
PNEUMONIA IN CHILDREN 1 INTRODUCTION 156 million new episodes / yr. worldwide 151 million episodes developing world 95% in developing countries 19% of all deaths in children
New Surveillance Definitions for VAP
 New Surveillance Definitions for VAP 2012 Critical Care Canada Forum Toronto Dr. John Muscedere Associate Professor of Medicine, Queen s University Kingston, Ontario Presenter Disclosure Dr. J. G. Muscedere
New Surveillance Definitions for VAP 2012 Critical Care Canada Forum Toronto Dr. John Muscedere Associate Professor of Medicine, Queen s University Kingston, Ontario Presenter Disclosure Dr. J. G. Muscedere
Avian Influenza Clinical Picture, Risk profile & Treatment
 Avian Influenza Clinical Picture, Risk profile & Treatment Jantjie Taljaard Adult ID Unit Tygerberg Academic Hospital University of Stellenbosch jjt@sun.ac.za 083 419 1452 CLINICAL PICTURE The clinical
Avian Influenza Clinical Picture, Risk profile & Treatment Jantjie Taljaard Adult ID Unit Tygerberg Academic Hospital University of Stellenbosch jjt@sun.ac.za 083 419 1452 CLINICAL PICTURE The clinical
Dr Conroy Wong. Professor Richard Beasley. Dr Sarah Mooney. Professor Innes Asher
 Professor Richard Beasley University of Otago Director Medical Research Institute of New Zealand Wellington Dr Sarah Mooney Physiotherapy Advanced Clinician Counties Manukau Health NZ Respiratory and Sleep
Professor Richard Beasley University of Otago Director Medical Research Institute of New Zealand Wellington Dr Sarah Mooney Physiotherapy Advanced Clinician Counties Manukau Health NZ Respiratory and Sleep
Severe community-acquired pneumonia
 BJA Education, 16 (5): 167 172 (2016) doi: 10.1093/bjaed/mkv052 Advance Access Publication Date: 13 November 2015 Matrix reference 2C01, 2C02, 2C03, 3C00 Severe community-acquired pneumonia AJ Morgan MBChB
BJA Education, 16 (5): 167 172 (2016) doi: 10.1093/bjaed/mkv052 Advance Access Publication Date: 13 November 2015 Matrix reference 2C01, 2C02, 2C03, 3C00 Severe community-acquired pneumonia AJ Morgan MBChB
Marcos I. Restrepo, MD, MSc, FCCP
 Thank you for viewing this presentation. We would like to remind you that this material is the property of the author. It is provided to you by the ERS for your personal use only, as submitted by the author.
Thank you for viewing this presentation. We would like to remind you that this material is the property of the author. It is provided to you by the ERS for your personal use only, as submitted by the author.
Things your mother never told you about antibiotics, UTI s, and Pneumonia. Rob Kaplan, MD July 12 and 14, 2017
 Things your mother never told you about antibiotics, UTI s, and Pneumonia Rob Kaplan, MD July 12 and 14, 2017 Objectives After this talk participants will: Be able to articulate some of the principles
Things your mother never told you about antibiotics, UTI s, and Pneumonia Rob Kaplan, MD July 12 and 14, 2017 Objectives After this talk participants will: Be able to articulate some of the principles
Critical Care Nursing Theory. Pneumonia. - Pneumonia is an acute infection of the pulmonary parenchyma
 - is an acute infection of the pulmonary parenchyma - is a common infection encountered by critical care nurses when it complicates the course of a serious illness or leads to acute respiratory distress.
- is an acute infection of the pulmonary parenchyma - is a common infection encountered by critical care nurses when it complicates the course of a serious illness or leads to acute respiratory distress.
Isolation Precautions in Clinics
 Purpose Audience General principles Possible Exposures To define isolation precautions in a clinic setting. Clinics Isolation status should be determined primarily by the suspected disease and/or pathogen.
Purpose Audience General principles Possible Exposures To define isolation precautions in a clinic setting. Clinics Isolation status should be determined primarily by the suspected disease and/or pathogen.
ESCMID Online Lecture Library. by author
 INFLUENZA IN CHILDREN Cristian Launes Infectious Diseases Unit. Department of Paediatrics. Hospital Sant Joan de Déu (Universitat de Barcelona) Innovation in Severe Acute Respiratory Infections (SARI),
INFLUENZA IN CHILDREN Cristian Launes Infectious Diseases Unit. Department of Paediatrics. Hospital Sant Joan de Déu (Universitat de Barcelona) Innovation in Severe Acute Respiratory Infections (SARI),
Neutropenic Fever. CID 2011; 52 (4):e56-e93
:e56-e93") Neutropenic Fever www.idsociety.org CID 2011; 52 (4):e56-e93 Definitions Fever: Single oral temperature of 101 F (38.3 C) Temperature 100.4 F (38.0 C) over 1 hour Neutropenia: ANC < 500 cells/mm 3 Expected
Neutropenic Fever www.idsociety.org CID 2011; 52 (4):e56-e93 Definitions Fever: Single oral temperature of 101 F (38.3 C) Temperature 100.4 F (38.0 C) over 1 hour Neutropenia: ANC < 500 cells/mm 3 Expected
2009 (Pandemic) H1N1 Influenza Virus
 H1N1 Influenza Virus") 2009 (Pandemic) H1N1 Influenza Virus September 15, 2009 Olympia, Washington Anthony A Marfin Washington State Department of Health Goals Understand current situation & pattern of transmission of 2009 H1N1
2009 (Pandemic) H1N1 Influenza Virus September 15, 2009 Olympia, Washington Anthony A Marfin Washington State Department of Health Goals Understand current situation & pattern of transmission of 2009 H1N1
The IDSA/ATS consensus guidelines on the management of CAP in adults
 The IDSA/ATS consensus guidelines on the management of CAP in adults F. Piffer F. Tardini R. Cosentini U.O. Medicina d'urgenza, Gruppo NIV, Fondazione Ospedale Maggiore Policlinico, Mangiagalli e Regina
The IDSA/ATS consensus guidelines on the management of CAP in adults F. Piffer F. Tardini R. Cosentini U.O. Medicina d'urgenza, Gruppo NIV, Fondazione Ospedale Maggiore Policlinico, Mangiagalli e Regina
Original Article Mahidol Univ J Pharm Sci 2015; 42 (4), MT. Nguyen 1, TD. Dang Nguyen 1* 1
, MT. Nguyen 1, TD. Dang Nguyen 1* 1") Original Article Mahidol Univ J Pharm Sci 2015; 42 (4), 195-202 Investigation on hospital-acquired pneumonia and the association between hospital-acquired pneumonia and chronic comorbidity at the Department
Original Article Mahidol Univ J Pharm Sci 2015; 42 (4), 195-202 Investigation on hospital-acquired pneumonia and the association between hospital-acquired pneumonia and chronic comorbidity at the Department
Pneumonia. Dr. Rami M Adil Al-Hayali Assistant professor in medicine
 Pneumonia Dr. Rami M Adil Al-Hayali Assistant professor in medicine Definition Pneumonia is an acute respiratory illness caused by an infection of the lung parenchyma, associated with recently developed
Pneumonia Dr. Rami M Adil Al-Hayali Assistant professor in medicine Definition Pneumonia is an acute respiratory illness caused by an infection of the lung parenchyma, associated with recently developed
Usefulness of Procalcitonin in the management of Infections in ICU. P Damas CHU Sart Tilman Liège
 Usefulness of Procalcitonin in the management of Infections in ICU P Damas CHU Sart Tilman Liège Procalcitonin Peptide 116 AA Produced by parenchymal cells during «sepsis»: IL1, TNF, IL6 : stimulators
Usefulness of Procalcitonin in the management of Infections in ICU P Damas CHU Sart Tilman Liège Procalcitonin Peptide 116 AA Produced by parenchymal cells during «sepsis»: IL1, TNF, IL6 : stimulators
PNEUMONIA. I. Background 6 th most common cause of death in U.S. Most common cause of infection related mortality
 Page 1 of 8 September 4, 2001 Donald P. Levine, M.D. University Health Center Suite 5C Office: 577-0348 dlevine@intmed.wayne.edu Assigned reading: pages 153-160; 553-563 PNEUMONIA the most widespread and
Page 1 of 8 September 4, 2001 Donald P. Levine, M.D. University Health Center Suite 5C Office: 577-0348 dlevine@intmed.wayne.edu Assigned reading: pages 153-160; 553-563 PNEUMONIA the most widespread and
RESPIRATORY VIRAL INFECTIONS
 RESPIRATORY VIRAL INFECTIONS Disclosures NONE Infectious Diseases in Clinical Practice February 2014 Jennifer Babik, MD, PhD Division of Infectious Diseases University of California, San Francisco Learning
RESPIRATORY VIRAL INFECTIONS Disclosures NONE Infectious Diseases in Clinical Practice February 2014 Jennifer Babik, MD, PhD Division of Infectious Diseases University of California, San Francisco Learning