Protocol for the finishing stage
|
|
|
- Diana Gilmore
- 5 years ago
- Views:
Transcription
1 DOI: /odfen/ J Dentofacial Anom Orthod 2015;19:105 The author Protocol for the finishing stage J. Faure Former university lecturer; former head of DFO Dept, University of Toulouse, France. In private practice in Auch (France) ABSTRACT Finishing is the most effective weapon in the battle against relapse. The choice of method depends on analyzing the type of relapse that is feared and the impact of aging, and on the help to be expected with retention. The present article deals with the practical requirements of finishing: duration, pre-finishing assessment, final arch wire bending, possible occlusal buffing, and elastic vertical interarcade traction. The theoretic protocol is illustrated by 3 cases followed up through finishing until appliance removal. The stability of occlusal results of course depends on the accuracy and fineness of finishing, but also on overall treatment management: anterior dentition control, anchorage control during retraction period, and choice of devices and extractions. Finishing can thus be said to be an important step - but one that begins on the first day of treatment. KEY WORDS Finishing, relapse, retention INTRODUCTION The choice of finishing strategy is indissociable from the analysis of relapse (and aging). The literature on relapse, however, provides little convincing information that might guide our approach to finishing 2,3,5-8,10,11. It is difficult, in adapting treatment, to distinguish the effects of retention or aging from real relapse ; there is also often confusion between relapse and what we would call treatment failure. Relapse is often assessed simply by measuring crowding. There are few studies with high levels of evidence. Many studies implicated occasional effects 3, for example, of a certain treatment attitude, clinical choice, atypical growth, physiological or anatomic problem, etc. Such reports are often incomplete or low on level of evidence, but it is certainly helpful to take them on board in our therapeutic behavior. Finishing differs from the main work in its timing (last touches), limited extent and, in our opinion, prime importance. Finishing is not a subsidiary but a major step. Address for correspondence: Jacques Faure 10, Place Lannes Auch, France faure_ja@club-internet.fr Article received: Accepted for publication: This is an Open Access article distributed under the terms of the Creative Commons Attribution License ( which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. 1 Article available at or
2 J. FAURE A perfectly finished program requires precautions taken during the main work itself, as mistakes cannot always be rectified by finishing. Perfect finishing in orthodontics thus depends on: initial treatment choices (control of anchorage, choice of extractions), and finishing itself. In what follows, we shall briefly present our choices, the material procedures of finishing and their timing, richly illustrated from case reports. We shall not enter into the intricacies of defining ideal occlusion, leaving the reader to refer to the criteria of the American Board of Orthodontics Grading System 1, which seem to command consensus in static terms. Functional and dynamic imperatives and esthetic criteria, on the other hand, are not well-defined. Our approach to perfect finishing consists in balancing the patient s maxillofacial architecture, especially anterior dentition, as well as possible, respecting the recognized rules of occlusal dynamics, and adopting a cautious attitude toward known threats to stability of treatment: third molar progression, anterior interdental dysharmony, late growth, etc. 3 We shall then focus on our efforts to refine static occlusion. To this aim, we present our finishing protocol. GENERAL LINES Duration: 6 months Consecrating 6 months of treatment, with 4 or 5 appointments, is surely not excessive to deal in detail with static and dynamic occlusion: Poling 9 advises 4 to 7 months. But this must not prolong the total treatment duration: to have 6 months for finishing, the other steps need to be performed as quickly as possible. Time-saving should begin from the outset of multibracket treatment, so as to achieve molar and canine class I relations with 2 mm incisor overbite, perfect alignment and leveling and closed spaces within a year and a half at most. The patient will then accept 6 months finishing without objection. Thus rapidly achieving good prefinishing occlusion is the first step toward perfectly finished occlusion. Dissociation between dental finishing/correction and preparation The transition to the finishing stage involves a break in the practitioner s concerns: where we had been concerned with the main aspects of objective occlusion, we now turn to what is more esthetically and functionally important: intercuspation, incisor alignment adjustment, artistic deformation, refining canine class I, adjusting the canine guide, etc. We need to look at what has been achieved, plan the finishing work 2 Faure J. Protocol for the finishing stage

3 PROTOCOL FOR THE FINISHING STAGE and take account of how long treatment has already lasted and how much cooperation can be expected of the patient, in order to estimate how much time we can reasonably allow for finishing. One major function of finishing is to test the quality of malocclusion correction. Otherwise, there is a risk of removing devices as soon as they seem to have triumphed over class II and signs of class I occlusion are observed. Unfortunately, however, this is often just a case of Sunday bite induced by the maxillomandibular elastic bands and, no sooner have the devices been removed than the patient slips right back into class II with severe overjet. Unfortunately, in some cases the finishing stage cannot be strictly defined: finishing work on the arch is required during the anterior retraction stage (case n 1) to help correct malocclusion. Analysis of occlusion status and finishing strategy In our opinion, occlusion analysis does not require a complicated clinical form, but does include: static aspect, with articulating paper to trace the numerous contacts and intercuspal balance; dynamic aspect, with systematic examination of lateralities and especially propulsion. For us, analysis of occlusion defects is in strict parallel to correction, systematizing intervention and avoiding a lot of points getting overlooked. A radiological check-up is essential. A panoramic view serves to check tooth parallelism and excessive interroot space if implant sites are to be prepared. It also avoids corono-radicular angles being detected too late when they might lead to threatening proximities: treatment in this case (figs 1-6) of severe class III, ended with perfect occlusion, with a slight linear and angular mandibular compensation that had to be accepted, and maxillary decompensation that doubtless ensured anterior stability; systematic end-of-treatment panoramic unfortunately showed severe mandibular canine angulation; it was too late to correct the tooth axes to achieve compromise after the devices had been removed. Figure 1 a, b, c: Lateral, three-quarter smile and frontal views. Fanny D., born Jan End of treatment, 14 yrs 10 mo. J Dentofacial Anom Orthod 2015;19:105 3



4 J. FAURE Figure 2 a, b, c: Right, frontal and left intraoral vestibular views. Fanny D., born Jan End of treatment, Nov. 2002, 14 yrs 10 mo. Figure 3 a, b: Intraoral views, canine region close-up, checking alignment, leveling and coronary axes. Fanny D., born Jan End of treatment, Nov. 2002, 14 yrs 10 mo. Figure 4 Lateral teleradiograph. Fanny D., born Jan End of treatment, Nov. 2002, 14 yrs 10 mo. 4 Faure J. Protocol for the finishing stage

5 PROTOCOL FOR THE FINISHING STAGE Figure 5 Diagram and Steiner and Tweed analyses. Fanny D., born Jan End of treatment, Nov. 2002, 14 yrs 10 mo Fanny D., born Jan. 26, End of treatment, Nov. 2002, 14 yrs 10 mo Plan d Occ: Occ plane / Ht Faciale Post: Post facial height / Ht Faciale Ant: Ant facial height Figure 6 Panoramic view. Fanny D., born Jan End of treatment, Nov. 2002, 14 yrs 10 mo. J Dentofacial Anom Orthod 2015;19:105 5
6 J. FAURE Main treatment procedures The main therapeutic procedures comprise: elastic vertical traction, worn permanently. Traction should be exerted on the arch (welded brass spurs or pinched stops) rather than on this or that tooth: unitary dental displacement is governed by the arch (especially 2 nd order shaping), whereas maxillomandibular traction controls extensive gaps (dental group or arcade sector or half-arcade). Arch anchorages may seem to hinder implementing shaping at the same site, but this is not actually true: angulations can be introduced on either side of the weld without putting its at risk, to perform a step, for example (fig. 7). Occlusal sharpening regularizes anatomic abnormalities hindering occlusion. Occlusal adjustment should not replace finishing, often by inducing dental intrusion or extrusion in case of gauge error; buffing is indicated in coronary dysmorphism causing a gap or occlusal trauma. Shaping on.019 x.026 arch, by 139- type forceps, is certainly the most precise method, enabling any practitioner to perform a release on the arch with 0.2 mm precision; it is the method we prefer. Poling 9 underlined the risk of weakening the arch at the torsion points, but we think the risk of fracture is virtually non-existent. Some authors recommend an alternative solution, ungluing and regluing the bracket when badly positioned. This is attractive, being in line with the philosophy of a straight arch, but is open to theoretical and practical objections: If 13 shows 0.5 mm extrusion and 5 tip-forward, the bracket should be released and reglued with a 0.5-mm shorter gauge and in-built 5 tip-back. The problem is that, once the original bracket has been released, we have no reference for positioning the new one! Figure 7 Introducing a step in an interdental space already bearing a welded spur: angles mesial and distal to the weld. 6 Faure J. Protocol for the finishing stage
7 PROTOCOL FOR THE FINISHING STAGE Experience shows that practitioners usually glue the second bracket back precisely in the position of the first, exactly matching the anatomic data at first fitting 9. The smaller the desired change in position, the less the precision of correction by regluing 9. We consider the ungluing-regluing method indicated only for big mistakes in positioning (>1.5 mm), which almost never happen. Another argument supports the choice of pliers shaping rather than ungluing-gluing as recommended by some: this is the spread of selfligating brackets (which we have used for many years now); time saving compared to ablating and replacing an arch now leaves more time for touching up and a strategy of rational finishing (notably respecting the rule of the 3 orders) conducted methodically and rigorously. No-one would hesitate now to remove a terminal arch with a single application of pliers. CHECKS At each stage, of course, we check the result of the previous stage, statically and dynamically; the protocol can be revised at any time. Hierarchy of interventions on the arch Intervention should follow a rigorous protocol. Three chronological rules are to be observed intervention according to arcade: first intervention on mandibular arcade, then on maxillary arcade; intervention according to order: first, 1 st order; second, 2 nd order; third, 3 rd order; intervention according to extension or location: first intervention for a general problem; second intervention for a localized problem. For example, in case of bilateral tip-to-tip, with clear crossed occlusion only in 14/44-45 and 25/35-36, we begin by overall maxillary expansion (and possibly mandibular contraction); then secondly we correct remaining crossed occlusions by individual inset/offset procedures. FINISHING ARCHES Some schools recommend loosening the bridle during finishing, using more elastic material and under-sized arches in titanium or nickel-titanium of.018 x.025 or.016 x.022 section or round.016 or.014 arches, in the hope that nature will finish occlusion. In contrast, we think that, near the end of treatment, position control needs to be maintained or increased to correct the last remaining little imperfections. Finishing thus uses.019 x.026 nickelchromium arches in 95% of cases. J Dentofacial Anom Orthod 2015;19:105 7
8 J. FAURE Full-groove steel arches, section.022 x.028 We only use full-groove arches for severe general problems of arcade shape. Transversally, bilateral crossed occlusion problems can be easily resolved by maxillary expansion or mandibular contraction or both, with either a.022 x.028 active arch or 2 arches. Vertically, in case of strong mandibular Spee curve, a full-groove arch solves the problem quickly. Steel arch, section.019 x.026 A.019 x.026 arch has the advantage of enabling most finishing corrections to be performed in a single procedure, without risk of bracket detachment. It is possible to introduce 1 st or 2 nd order shaping in the arch up to 1 to 1.5 mm (step-up/step-down or inset/offset ). Shaping on this scale with a fullgroove arch would inevitably lead to detachment. But it can also be introduced in 2 stages (fig. 8: 0.75 mm step, increased to 1.5 mm at next appointment). The.019 x.026 arch is the optimal compromise between malleability and elasticity for occasional finishing. Moreover, loss of position control is minimal with a.019 x.026 arch in a.022 x.028 groove: negligible for axial rotation or mesio-distal tilt, and only 7 for torque. If the power of a full-groove arch is needed (e.g., strong Spee curve), it should be introduced first, and then, for occasional finishing, either revert to a.019 x.026 arch or finish with a full-groove arch in 2 stages (cf. below and fig. 8). FREQUENCY OF INTERVENTION The frequency of finishing operations depends on the large number of occlusal contacts. Ranking according to order is as follows: 2 nd order: approx. 70% These are general interventions, notably correction of strong Spee curves; they are often occasional, especially to intrude/extrude single teeth in the lateral sectors (step-up or stepdown); axial corrections (tip back/tip forward, with 2 identical consecutive steps) are more frequent in the anterior sector, for esthetic reasons, optimizing the esthetic shaping already included in the brackets. 1 st order: approx. 30% General interventions (arch expansion/contraction) are frequent. Occasional interventions are rarer: slight vestibular or palatal displacement (offset + inset» or inset + offset), to correct, for example, an overly vestibular lateral, incisor (residual class II division 2 occlusion), or axial rotation due to general gluing error (inset + inset or offset + offset ). 3 rd order: exceptional Third-order intervention is very rare in our practice. Torque control with a.019 x.026 arch in a.022 x.028 groove is excellent, with just 7 play or loss of control. 8 Faure J. Protocol for the finishing stage
9 PROTOCOL FOR THE FINISHING STAGE Two-stage step introduction 30 step: 1/2 90 step: 1 Figure 8 Introducing a large step in 2 stages: 30 then 90 (h = 0.75 mm then 1.5 mm). With Roth prescription, a severely retracted superior central incisor at risk of under-version ends up at 14 minus 7 = +7 (+14 : incorporated Roth torque; 7 loss of undersizing control); residual version greatly exceeds the natural version of 1 to 2 4. These rare interventions usually concern incisor groups, to achieve angular under-compensation or overdecompensation. What is sought is a final position in angular over-decompensation: in severe skeletal class II, for example, final slight incisor angular superior protrusion (+3 to +5 ) and slight inferior retrusion ( 3 to 5 ), or class III compensation, is recom- mended by some authors (Planché, Andrews) to guard against any slight tendency to relapse. Such angular overdecompensation comes obviously at the price of linear over-compensation; likewise, over-decompensation of bilabioversion requires reduced superior and inferior incisor torque. Occasional intervention may exceptionally be needed to correct ectopic included canines that have undergone difficult traction (e.g., vestibular maxillary canines) to avoid fenestration. In such cases, it is wise to provide torque breakers to soften, the impact of torque correction. J Dentofacial Anom Orthod 2015;19:105 9

10 J. FAURE CONCLUSION A long finishing stage using pliers provides perfect static occlusion, rigorous intercuspation and canine and molar class I relations, while ensuring functional and esthetic excellence. This stage is not enough in itself to ensure stability, which depends also on the architectural balance of the face and anterior dentition: i.e., the critical therapeutic choices regarding extraction and mechanics, anchorage, final incisor positioning and functional balance, etc. Thus, finishing begins on the day when the brackets are fitted; the first steps are critical as initial mistakes preclude perfect occlusion, and any delay leaves less time for finishing. Even with perfect treatment strategy and rigorous finishing, definitive stability is not guaranteed, and final occlusion may wobble, either for functional reasons (recurrent dysfunction) or simply with aging. Even so, a rigorous protocol, close attention and time spent on finishing help conjure the specter of relapse, or at least reduce its frequency and severity. CASE 1 Diagnosis Manon G. consulted in May 2011 at the age of 13 years 8 months. Her face presented as class II hyperdivergent; intraoral examination, however, found molar class I with only moderate overjet (figs 9-12). Cephalometry confirmed the severity of skeletal class II, borderline surgical, and the degree of linear and especially angular compensation trying to hide it. Bilabioversion related to DMD was superimposed on class II (T1 and T2) linear compensation. Figure 9 a, b, c: Lateral, smile and frontal views. Nov. 5 (13 yrs 8mo); 1 st documents. 10 Faure J. Protocol for the finishing stage



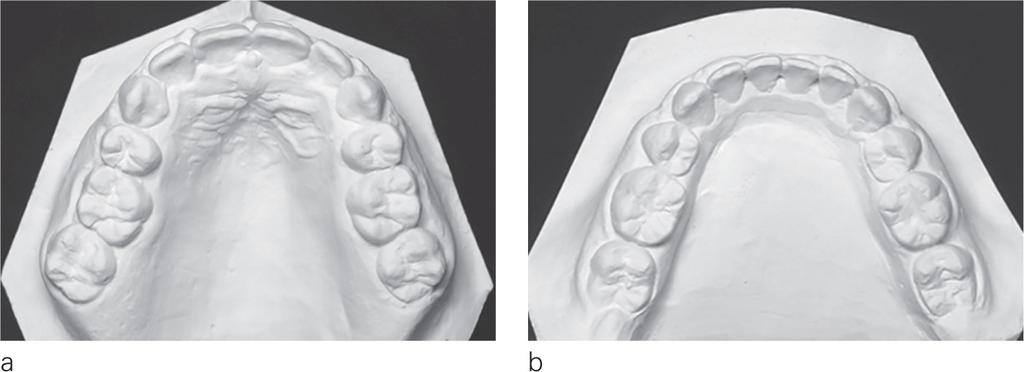
11 PROTOCOL FOR THE FINISHING STAGE Figure 10 a, b, c: Right, frontal and left intraoral views. Nov. 5 (13 yrs 8mo); 1 st documents. Figure 11 a, b, c: Molds, right, frontal and left views. Nov. 5 (13 yrs 8mo); 1 st documents. Figure 12 a, b, c: Occlusal maxillary and mandibular views and Spee curve. 5 (13 yrs 8mo); 1 st documents. J Dentofacial Anom Orthod 2015;19:105 11
 in a")
12 J. FAURE Figure 13 a, b: Teleradiograph with Steiner lines and panoramic view. 5 (13 yrs 8mo); 1 st documents. Treatment plan The incisor positioning objective involved a very slight compromise to balance a difficult frame, at the cost of heavy devices (miniscrews to avoid any loss of anchorage) in a difficult case (figs 14 and 15). Achieving perfectly finished stable occlusion required extreme mechanical precautions to maintain anchorage, enabling rigorous control of skeletal and dental class II correction and correction of linear bilabioversion. We used straight arch attachments, with.022 x.028 groove, Roth prescription and inbuilt 10 and 15 tip--back on the mandibular molars (passive self-ligating brackets). 12 Faure J. Protocol for the finishing stage
13 PROTOCOL FOR THE FINISHING STAGE 5 1 F6 Problem Rounded Solution Individualized Result Figure 14 Steiner chevrons. Discrepancy -4 Spee curve -1 Relocation i -11->-10 Extraction -5 ->0 +15 IMT II Relocation 6 Total -21-> Available space 0 Diameter of 8s -22 Present deficit -22 Residual growth* +9.5 Anchorage loss +4 Expected deficit -8.5 According to:space gain = xage Figure 15 Steiner box and posterior space box. J Dentofacial Anom Orthod 2015;19:105 13
 The degree of anterior retraction to be achieved, especially on the maxilla, required early finishing operations, during the actual retraction stage, although we would")
, due to slight excess of maxillary incisors gauge and arcade flexion induced by the")
; direct mechanical incisor retraction blocked by closed bite.")
14 J. FAURE Treatment and finishing: Aug (13yrs 11mo) Aug (16yrs 11mo) The degree of anterior retraction to be achieved, especially on the maxilla, required early finishing operations, during the actual retraction stage, although we would usually try to avoid this. Finishing will optimally adjust occlusion when malocclusion correction has been completed. Early finishing operations were needed as incisor retraction was blocked by closed bite (figs 16 and 17), due to slight excess of maxillary incisors gauge and arcade flexion induced by the retraction imposed (.019 x.026 arch); reshaping comprised 2nd order action (maxillary incisor intrusion, especially of 11-21) and radiculo-palatal torque (figs 18-21). Figure 16 a, b, c Right, frontal and left vestibular intra-oral views, Aug (14yrs 11mo); direct mechanical incisor retraction blocked by closed bite. Figure 17 a, b, c Right, frontal and left vestibular intra-oral views, Aug (14yrs 11mo); incisor retraction: introduction of step-up 3-2. Figure 18 a, b, c Maxillary, mandibular arches and coordination. 14 Faure J. Protocol for the finishing stage

 show over-decompensation: of bilabioversion (especially angular); and of initial class II compensation: mandibular incisor reduced from 31-9 mm to 23-4.5 mm (fig. 27).")
15 PROTOCOL FOR THE FINISHING STAGE Figure 19 a, b, c: Maxillary arch seen from right, front and left. Figure 20 a, b, c: Maxillary arch, close-up of flat part, seen from right, front and left. Intrusion step: intrusion of the 4 incisors Arch angulation:stronger intrusionof Radiculo-palatal torque on the 4 incisors Torque: +10 Angulation +10 Figure 21 Diagram of mechanical analysis. Retraction was completed without difficulty, and individual finishings were added. Final documents (figs 22-26) show over-decompensation: of bilabioversion (especially angular); and of initial class II compensation: mandibular incisor reduced from 31-9 mm to mm (fig. 27). Final (figs and Tables 1-2) and post-treatment documents show occlusion stability. J Dentofacial Anom Orthod 2015;19:105 15
; ablation.")


16 J. FAURE Figure 22 a, b, c: Lateral, smile and frontal views; Aug (16yrs 11mo); ablation. Figure 23 a, b, c: Right, frontal and left vestibular intra-oral views; Aug (16yrs 11mo); ablation. Figure 24 a, b, c: Molds: Right, frontal and left vestibular views; Aug (16yrs 11mo); ablation. Figure 25 a, b: Molds: occlusal, maxillary and mandibular views; Aug (16yrs 11mo); ablation. 16 Faure J. Protocol for the finishing stage

17 PROTOCOL FOR THE FINISHING STAGE Figure 26 a, b: Teleradiograph with Steiner lines and panoramic view at end of treatment; Aug (16yrs 11mo); ablation. Problem Objective Result 6.5 AoBo AoBo Figure 27 Check of anterior dentition. J Dentofacial Anom Orthod 2015;19:105 17
18 J. FAURE Table 1: Steiner analysis. Manon G. born Sept Steiner Cephalometry Cephalometry Norm May y 8mo Aug 14 16y 11m SNA SNB ANB SND /NAmm /NA /NBmm /NB Pog/NB / / Occl/ SN GoGn/SN SE SL Table 2: Tweed analysis. Manon G. born Sept Tweed Cephalometry Cephalometry Norm May 11 13y 8m Aug 14 16y 11m FMIA 27 +/ FMA 25 +/ IMPA 88 +/ SNA SNB ANB 2 +/ AoBo 2 mm Occlusion plane Angle Z 75 +/ Upper lip / Total chin / Post facial height 45 mm Ant facial height 65 mm Post/Ant Index 0, Progression ratio 2/1 18 Faure J. Protocol for the finishing stage


 confirmed slight hyperdivergent Figure 28 a, b, c: Lateral, smile and frontal views.")
19 PROTOCOL FOR THE FINISHING STAGE CASE 2 Diagnosis Carol T., born January 1995, consulted in February 2007, aged 12 years 1 month. Facial examination found class III with notable cheek-bone aplasia (fig. 28). Intra-oral examination confirmed this impression, with slight molar class III, despite overjet in 11-21, due to crowding (fig. 29). Cephalometry (figs 31 and 32) confirmed slight hyperdivergent Figure 28 a, b, c: Lateral, smile and frontal views. 1 st documents. Dec (12y 11m). Figure 29 a, b, c: Right, frontal and left vestibular views. 1 st documents. Dec (12y 11m). Figure 30 Panoramic view. 1 st documents. Dec (12y 11m). J Dentofacial Anom Orthod 2015;19:105 19


20 J. FAURE class III and strong bilabioversion, reducing, as is often the case, the sensation of slight skeletal dysmorphism and saving the class III. Bilabioversion was stronger in the maxilla than mandible, due to class III compensations superimposed on the bilabioversion. Figure 31 a and b: Teleradiography and Tweed cephalometry. 1 st documents. Dec (12y 11m). Tweed analysis Inter-incisor Chin Figure 32 a and b: Teleradiography with Steiner lines, and Steiner cephalometry. 1 st documents. Dec (12y 11m). Steiner analysis. 20 Faure J. Protocol for the finishing stage
21 PROTOCOL FOR THE FINISHING STAGE Treatment plan Space calculations were very negative in the anterior (fig. 33) and posterior sectors (fig. 34), and extraction of the 4 first premolars and 4 third molars was inevitable (figs 30-34). Sacrificing the premolars enabled an anterior strategy free of compromise, with rigorous anchorage (fig. 32). 1 Problem Solution Individ. Result Post-tt Crowding -5 Repositioning 1-6 Spee curve -1 Extractions Total >-15 Figure 33 Steiner chevrons and anterior box. Posterior space Free space (TMD) Distal 37-47: Expected anchorage loss Posterior growth, girl* Expected free space at 18 yrs -15 No hope of "salvaging"4x8s *posterior growth calculated as: Y = xage Tweed calculation gave post. growth = 3mm Figure 34 Posterior space box. J Dentofacial Anom Orthod 2015;19:105 21
 Straight arch attachments with Roth prescription and 10 and 15 built-in tip-back on mandibular molars improved anchorage (passive")
 comprised mainly 2 nd order shaping (steps, accentuated maxillary and inversed mandibular Spee curve, tip-back on 11, etc.")

22 J. FAURE Multibracket treatment and finishing (March 2008 (13y 2m) Oct (15y 9m) Straight arch attachments with Roth prescription and 10 and 15 built-in tip-back on mandibular molars improved anchorage (passive selfligating brackets). Intercuspation finishing was of course rigorous. The terminal arch (fig ) comprised mainly 2 nd order shaping (steps, accentuated maxillary and inversed mandibular Spee curve, tip-back on 11, etc.), but also 1 st order (fig. 36b) and even 3 rd order (fig. 37a and c, and fig. 45). Figure 35 a, b, c: Right, frontal and left vestibular views. Finishing: Aug. 2010, 15y 7m. Figure 36 a, b, c: Right frontal and left view, maxillary arch: Finishing: Aug. 2010, 15y 7m. Figure 37 a, b, c:: Right frontal and left view, maxillary arch. Finishing: detail of 2 nd order control: Aug. 2010, 15y 7m. 22 Faure J. Protocol for the finishing stage

, as planned since the outset in September 2011 (fig. 34). Post-treatment stability was excellent (figs 47 and 48).")

23 PROTOCOL FOR THE FINISHING STAGE Ablation documents (figs 39-45) confirmed precise static occlusion adjustment. Finishing comprised class III overdecompensation, especially maxillary, where linear and particularly angular protrusion was very strong (torque over-correction), to counter possible slight late type-c relapse (figs 44-46). Third molars were extracted (fig. 48), as planned since the outset in September 2011 (fig. 34). Post-treatment stability was excellent (figs 47 and 48). Figure 38 a, b, c: Mandibular arch, right, frontal and left views: Finishing: Aug. 2010, 15y 7m Inverted Spee curve on / Inverted Spee curve on Figure 39 a, b, c: Lateral, smile and frontal views; ablation, Oct. 2010, 15y 9m. Figure 40 a, b, c: Right, frontal and left vestibular views; ablation, Oct. 2010, 15y 9m. J Dentofacial Anom Orthod 2015;19:105 23

 views; ablation, Oct.")

24 J. FAURE Figure 41 a, b, c: Molds: Right, frontal and left vestibular views: ablation, Oct. 2010, 15y 9m. Figure 42 a, b, c: Molds: occlusal, maxillary and mandibular (with Spee curve) views; ablation, Oct. 2010, 15y 9m. Figure 43 Panoramic end of treatment view; ablation, Oct. 2010, 15y 9m. 24 Faure J. Protocol for the finishing stage
25 PROTOCOL FOR THE FINISHING STAGE Figure 44 a, b: Teleradiograph with Steiner lines and end-of-treatment cephalometry; ablation, Oct. 2010, 15y 9m. Figure 45 a, b: Teleradiograph with Tweed lines and end-of-treatment cephalometry; ablation, Oct. 2010, 15y 9m. Tweed analysis Interincisor Chin J Dentofacial Anom Orthod 2015;19:105 25



26 J. FAURE Figure 46 Control of anterior dentition. Figure 47 a, b, c: Lateral, smile and frontal views: 3 years post-treatment: Oct. 2013, 18y 9m. Figure 48 a, b, c: Right, frontal and left vestibular intra-oral views: 3 years post-treatment: Oct. 2013, 18y 9m. 26 Figure 49 Panoramic view after extraction of years post-treatment: Oct. 2013, 18y 9m. Faure J. Protocol for the finishing stage
.")

.")
27 PROTOCOL FOR THE FINISHING STAGE CASE 3 Diagnosis Audrey, born January 1998, consulted in May 2011, aged 13 years 4 months. Above all, her smile was impaired by crowding in both arcades (figs 50 and 51). Facial examination found vertical excess and difficult labial contact. Teleradiography confirmed insufficient occlusal contact, with slight anterior gap; cephalometry found hyperdivergent class I (figs 53 and 54). Figure 50 a, b, c: Lateral, smile and frontal views. 1 st documents, May 2011 (13y 4m). Figure 51 a, b, c: Right, frontal and left intra-oral views. 1 st documents, May 2011 (13y 4m). Figure 52 Panoramic view. 1 st documents, May 2011 (13y 4m). J Dentofacial Anom Orthod 2015;19:105 27

28 J. FAURE Intra-oral examination found superior protrusion with overjet, confirmed on cephalometry (figs 53 and 54). Posterior DMD was moderate (figs 52 and 56). Treatment plan An anterior alignment-advancement plan was abandoned, mainly due to the vertical problem: anterior balance would have been precarious. Figure 53 a and b: Lateral teleradiograph with Steiner lines and Steiner cephalometry. 1st documents, May 2011 (13y 4m). Figure 54 a and b: Lateral teleradiograph with Tweed lines and Tweed cephalometry. 1st documents, May 2011 (13y 4m). Tweed analysis 28 Faure J. Protocol for the finishing stage
29 PROTOCOL FOR THE FINISHING STAGE A second-premolar extraction strategy avoided strong incisor retraction, while balancing the anterior box; the permitted anchorage loss should be of good prognosis for 3 rd molar salvage (fig. 55 and 56). Figure 55 Steiner chevrons. 1 st documents, May 2011 (13y 4m). Figure 56 Steiner box and posterior space box. J Dentofacial Anom Orthod 2015;19:105 29
.")
. Figure 57 a, b, c: Right, frontal and left vestibular intra-oral views.")

30 J. FAURE Treatment and finishing: April 2012 (14 years 3 months) - November 2014 (16 years 10 months) The patient was fitted with straight arch brackets with Roth prescription and built-in 10 and 15 mandibular molar tip-back for better anchorage control (passive self-ligating brackets). Multibracket treatment was begun in April 2012 (14 years 3 months) and finishing in March 2014 (16 years 2 months) (figs 57 and 60), with mainly 2 nd order interventions. Multibracket treatment was completed in November 2014 (16 years 10 months). Figure 57 a, b, c: Right, frontal and left vestibular intra-oral views. Start of finishing, March 2014 (16y 2m): superior incisor intrusion steps to avoid contact with inferior brackets and facilitate superior incisor retraction (transient closed bite). Figure 58 a, b, c: Right, frontal and left vestibular intra-oral views. Finishing, August 2014 (16y 7m): suppression of incisor intrusion steps (retraction terminated), correction of 21, intrusion of 15, extrusion of 46. Figure 59 a, b, c: Right, frontal and left vestibular intra-oral views. Finishing, August 2014 (16y 7m): vertical interarcade traction and renewed intermaxillary traction II (insufficient class II correction). 30 Faure J. Protocol for the finishing stage

.")
.")
31 PROTOCOL FOR THE FINISHING STAGE The photographs of the terminal arches show the finishing results (figs 61-65): mainly 2 nd order interventions (step, Spee curve, accentuated in maxilla and inverted in mandible, tipforward on 21, intrusion step-down molar groups with a slight gauge excess etc.) but also 3rd order (reduction of superior incisor torque). Figure 60 a, b, c: Right, frontal and left vestibular intra-oral views. End of finishing, Nov (16y 10m). Figure 61 a, b, c: Occlusal views of terminal arches: maxillary, mandibular (upside-down) and coordination. November 2014 (16 years10 months). Distal vestibular rotation of 21 Figure 62 a, b, c: Maxillary terminal arch: right, frontal and left views. November 2014 (16 years10 months). J Dentofacial Anom Orthod 2015;19:105 31
.")


32 J. FAURE Figure 63 a, b, c: Mandibular terminal arch (upside-down): right (left side), frontal and left (right side) views. November 2014 (16 years10 months). Figure 64 a, b: Mandibular terminal arch (upside-down) on glass plate: right (left side), frontal and left (right side) views: evidence of 2 nd order. November 2014 (16 years10 months). (a) Spee curve on and / Step-down and step-up on and (b) Spee curve on and / Step-up and step-down on and Figure 65 a, b, c: Maxillary terminal arch on glass plate: right, frontal and left views: evidence of 2 nd order. November 2014 (16 years10 months). Spee curve and / Angulation and / Negative torque on superior incisors / Step up and Faure J. Protocol for the finishing stage
33 PROTOCOL FOR THE FINISHING STAGE End of multibracket treatment documents show over-compensation of linear and angular superior protrusion, guaranteeing stability (from 7.5 mm/34 to 2.5 mm/18.5 ) (figs 66 and 67). Rigorous intercuspation, and beaming smile (figs 68, 69 and 70). Figure 66 a, b: Teleradiograph with Steiner lines and Steiner cephalometry. November 2014 (16 years10 months)). Figure 67 a, b: Teleradiograph with Tweed lines and Tweed cephalometry. November 2014 (16 years10 months). Tweed analysis Interincisor Chin J Dentofacial Anom Orthod 2015;19:105 33



34 J. FAURE Figure 68 a, b, c: Lateral, smile and frontal views. Ablation. November 2014 (16 years 10 months). Figure 69 End-of-treatment smile. Figure 70 a, b, c: Right, frontal and left vestibular intra-oral views. Ablation. November 2014 (16 years 10 months). 34 Faure J. Protocol for the finishing stage

.")
. Figure 73 a, b: Intra-oral occlusion views, with retention.")
35 PROTOCOL FOR THE FINISHING STAGE Third-molar progression will be followed up (fig. 71). Retention comprises a transparent maxillary splint and a metal wire glued to the mandibular arcade from 33 to 43 (figs 72 and 73). Conflict of interest: The author declares no conflict of interest. Figure 71 Panoramic end-of-treatment view. November 2014 (16 years 10 months). Figure 72 a, b, c: Right, frontal and left vestibular intra-oral views with retention. November 2014 (16 years 10 months). Figure 73 a, b: Intra-oral occlusion views, with retention. November 2014 (16 years 10 months). J Dentofacial Anom Orthod 2015;19:105 35
36 J. FAURE REFERENCES 1. American Board of Orthodontics Grading System for Dental Casts and Panoramic Radiographs. Revised Jjune 2012; Artun J, Garol J, Little RM. Long-term stability of mandibular incisors following successful treatment of Class II, Division 1 malocclusions. Angle Orthod 1996;66: Blake M, Bibby K. Retention and stability: A review of litterature. Am J Orthod Dentofacial Orthop 1998;114: Demange Ch. L inclinaison vestibulo-linguale naturelle des dents. Rev Orthop Dento Faciale 1997;31: De la Cruz AR, Sampson P, Little RM, Artun J, Shapiro PA. Long-term changes in arch form after orthodontic treatment and retention. Am J Orthod Dentofacial Orthop 1995;107(5): DeGuzman L, Bahirael D, Vig PS, Weyant RJ, O Brien K. The validation of the PAR index for malocclusion severity and treatment difficulty. Am J Orthod Dentofacial Orthop 1995;107: Miyazaki H, Moteji E, Yatabe K, Isshiki Y. Occlusal stability after extraction orthodontic therapy in adult and adolescent patient. Am J Orthod Dentofacial Orthop 1997;112: Ormiston JP, Huang GJ, Little RM, Decker JD, Seuk GD. Retrospective analysis of long-term stable and unstable orthodontic treatment outcomes. Am J Orthod Dentofacial Orthop 2005;128: Poling R. A method of finishing the occlusion. Am J Orthod Dentofacial Orthop 1999;115: Richmond S et al. The development of the PAR index (Peer Aassessment Rating): reliability and variability. European J Orthod 1992;14: Rothe LE, et al. Trabecular and cortical bone as risk factors for orthodontic relapse. Am J Orthod Dentofacial Orthop 2006;130(4): Sadowsky C, Schneider BJ, BeGole EA, Tahir E. Long term stability after orthodontic treatment. Non extraction with prolonged retention. Am J Orthod Dentofacial Orthop 1994;106: Faure J. Protocol for the finishing stage
Regarding morphological differences of the maxillary anterior teeth of monozygotic twin sisters
 DOI: 10.1051/odfen/2012406 J Dentofacial Anom Orthod 2013;16:106 Ó RODF / EDP Sciences C L I N I C A L C A S E S Regarding morphological differences of the maxillary anterior teeth of monozygotic twin
DOI: 10.1051/odfen/2012406 J Dentofacial Anom Orthod 2013;16:106 Ó RODF / EDP Sciences C L I N I C A L C A S E S Regarding morphological differences of the maxillary anterior teeth of monozygotic twin
Management of three impacted teeth detected early
 DOI: 10.1051/odfen/ 2018124 J Dentofacial Anom Orthod 2017;20:310 The authors C L I N I C A L C A S E Management of three impacted teeth detected early P. Guézénec Qualified Specialist in Dento facial
DOI: 10.1051/odfen/ 2018124 J Dentofacial Anom Orthod 2017;20:310 The authors C L I N I C A L C A S E Management of three impacted teeth detected early P. Guézénec Qualified Specialist in Dento facial
EUROPEAN SOCIETY OF LINGUAL ORTHODONTISTS
 EUROPEAN SOCIETY OF LINGUAL ORTHODONTISTS CANDIDATE NUMBER:44 CASE NUMBER: 2 Year: 2010 ESLO 01 RÉSUMÉ OF CASE 5 CASE CATEGORY: CLASS II DIVISION 1 MALOCCLUSION A MALOCCLUSION WITH SIGNIFICANT MANDIBULAR
EUROPEAN SOCIETY OF LINGUAL ORTHODONTISTS CANDIDATE NUMBER:44 CASE NUMBER: 2 Year: 2010 ESLO 01 RÉSUMÉ OF CASE 5 CASE CATEGORY: CLASS II DIVISION 1 MALOCCLUSION A MALOCCLUSION WITH SIGNIFICANT MANDIBULAR
OF LINGUAL ORTHODONTICS
 EUROPEAN SOCIETY OF LINGUAL ORTHODONTICS CANDIDATE NUMBER: KDr. KP. kanarelis CASE NUMBER: 2 Year: 2010 WBLO 01 RESUME OF CASE 2 CASE CATEGORY: ADULT MALOCCLUSION NAME : MARIA A. BORN: 18.04.1983 SEX:
EUROPEAN SOCIETY OF LINGUAL ORTHODONTICS CANDIDATE NUMBER: KDr. KP. kanarelis CASE NUMBER: 2 Year: 2010 WBLO 01 RESUME OF CASE 2 CASE CATEGORY: ADULT MALOCCLUSION NAME : MARIA A. BORN: 18.04.1983 SEX:
EUROPEAN SOCIETY OF LINGUAL ORTHODONTISTS
 EUROPEAN SOCIETY OF LINGUAL ORTHODONTISTS CANDIDATE NUMBER: 44 CASE NUMBER: 1 Year: ESLO 01 RÉSUMÉ OF CASE 1 CASE CATEGORY: ADULT MALOCCLUSION NAME: K.N BORN: 03/03/1980 SEX: Male PRE-TREATMENT RECORDS:
EUROPEAN SOCIETY OF LINGUAL ORTHODONTISTS CANDIDATE NUMBER: 44 CASE NUMBER: 1 Year: ESLO 01 RÉSUMÉ OF CASE 1 CASE CATEGORY: ADULT MALOCCLUSION NAME: K.N BORN: 03/03/1980 SEX: Male PRE-TREATMENT RECORDS:
Combined use of digital imaging technologies: ortho-surgical treatment
 DOI: 10.1051/odfen/2018059 J Dentofacial Anom Orthod 2018;21:210 The authors Combined use of digital imaging technologies: ortho-surgical treatment L. Petitpas Private practice, 54700 Pont-à-Mousson Are
DOI: 10.1051/odfen/2018059 J Dentofacial Anom Orthod 2018;21:210 The authors Combined use of digital imaging technologies: ortho-surgical treatment L. Petitpas Private practice, 54700 Pont-à-Mousson Are
OF LINGUAL ORTHODONTICS
 EUROPEAN SOCIETY OF LINGUAL ORTHODONTICS CANDIDATE NUMBER: KDr. KP. kanarelis CASE NUMBER: 1 Year: 2010 WBLO 01 RESUME OF CASE 1 CASE CATEGORY: ADULT MALOCCLUSION NAME : IOANNIS.G BORN: 03.01.1989 SEX:
EUROPEAN SOCIETY OF LINGUAL ORTHODONTICS CANDIDATE NUMBER: KDr. KP. kanarelis CASE NUMBER: 1 Year: 2010 WBLO 01 RESUME OF CASE 1 CASE CATEGORY: ADULT MALOCCLUSION NAME : IOANNIS.G BORN: 03.01.1989 SEX:
UNILATERAL UPPER MOLAR DISTALIZATION IN A SEVERE CASE OF CLASS II MALOCCLUSION. CASE PRESENTATION. 1*
 UNILATERAL UPPER MOLAR DISTALIZATION IN A SEVERE CASE OF CLASS II MALOCCLUSION. CASE PRESENTATION. 1* Department of Orthodontics and Pedodontics 1 Faculty of Dental Medicine, University of Medicine and
UNILATERAL UPPER MOLAR DISTALIZATION IN A SEVERE CASE OF CLASS II MALOCCLUSION. CASE PRESENTATION. 1* Department of Orthodontics and Pedodontics 1 Faculty of Dental Medicine, University of Medicine and
Crowded Class II Division 2 Malocclusion
 Class II Division 2 Malocclusion Crowded Class II Division 2 Malocclusion Clinicians: Drs. Chris Chang, Hsin-Yin Yeh, Sophia Pei-Wen Shu, W. Eugene Roberts Patient: Miss Jhan Pre-treatment Diagnosis An
Class II Division 2 Malocclusion Crowded Class II Division 2 Malocclusion Clinicians: Drs. Chris Chang, Hsin-Yin Yeh, Sophia Pei-Wen Shu, W. Eugene Roberts Patient: Miss Jhan Pre-treatment Diagnosis An
MBT System as the 3rd Generation Programmed and Preadjusted Appliance System (PPAS) by Masatada Koga, D.D.S., Ph.D
 by Masatada Koga, D.D.S., Ph.D") MBT System as the 3rd Generation Programmed and Preadjusted Appliance System (PPAS) by Masatada Koga, D.D.S., Ph.D Dr. Masatada Koga, D.D.S., Ph.D, is an assistant professor in the Department of Orthodontics
MBT System as the 3rd Generation Programmed and Preadjusted Appliance System (PPAS) by Masatada Koga, D.D.S., Ph.D Dr. Masatada Koga, D.D.S., Ph.D, is an assistant professor in the Department of Orthodontics
Angle Class II, division 2 malocclusion with deep overbite
 BBO Case Report Angle Class II, division 2 malocclusion with deep overbite Arno Locks 1 Angle Class II, division 2, malocclusion is characterized by a Class II molar relation associated with retroclined
BBO Case Report Angle Class II, division 2 malocclusion with deep overbite Arno Locks 1 Angle Class II, division 2, malocclusion is characterized by a Class II molar relation associated with retroclined
EUROPEAN SOCIETY OF LINGUAL ORTHODONTISTS
 EUROPEAN SOCIETY OF LINGUAL ORTHODONTISTS Dr. Masatoshi Sana Year: ESLO 01 RÉSUMÉ OF CASE 8 CASE CATEGORY: TRANS / VERTICAL DISCREPANCY NAME: Akiko T. BORN : 15/03/1973 SEX: F PRE-TREATMENT RECORDS: AGE:
EUROPEAN SOCIETY OF LINGUAL ORTHODONTISTS Dr. Masatoshi Sana Year: ESLO 01 RÉSUMÉ OF CASE 8 CASE CATEGORY: TRANS / VERTICAL DISCREPANCY NAME: Akiko T. BORN : 15/03/1973 SEX: F PRE-TREATMENT RECORDS: AGE:
Case Report: Long-Term Outcome of Class II Division 1 Malocclusion Treated with Rapid Palatal Expansion and Cervical Traction
 Case Report Case Report: Long-Term Outcome of Class II Division 1 Malocclusion Treated with Rapid Palatal Expansion and Cervical Traction Roberto M. A. Lima, DDS a ; Anna Leticia Lima, DDS b Abstract:
Case Report Case Report: Long-Term Outcome of Class II Division 1 Malocclusion Treated with Rapid Palatal Expansion and Cervical Traction Roberto M. A. Lima, DDS a ; Anna Leticia Lima, DDS b Abstract:
EUROPEAN SOCIETY OF LINGUAL ORTHODONTISTS
 EUROPEAN SOCIETY OF LINGUAL ORTHODONTISTS CANDIDATE NUMBER : 13 Dr. Masatoshi Sana CASE NUMBER : Year : ESLO 01 RÉSUMÉ OF CASE 2 CASE CATEGORY: CLASS I MALOCCLUSION NAME: BORN: SEX: Yukari K. 08/03/1979
EUROPEAN SOCIETY OF LINGUAL ORTHODONTISTS CANDIDATE NUMBER : 13 Dr. Masatoshi Sana CASE NUMBER : Year : ESLO 01 RÉSUMÉ OF CASE 2 CASE CATEGORY: CLASS I MALOCCLUSION NAME: BORN: SEX: Yukari K. 08/03/1979
Gentle-Jumper- Non-compliance Class II corrector
 15 CASE REPORT Gentle-Jumper- Non-compliance Class II corrector Amit Prakash 1,O.P.Mehta 2, Kshitij Gupta 3 Swapnil Pandey 4 Deep Kumar Suryawanshi 4 1 Senior lecturer Bhopal - INDIA 2 Professor Bhopal
15 CASE REPORT Gentle-Jumper- Non-compliance Class II corrector Amit Prakash 1,O.P.Mehta 2, Kshitij Gupta 3 Swapnil Pandey 4 Deep Kumar Suryawanshi 4 1 Senior lecturer Bhopal - INDIA 2 Professor Bhopal
Correction of Crowding using Conservative Treatment Approach
 Case Report Correction of Crowding using Conservative Treatment Approach Dr Tapan Shah, 1 Dr Tarulatha Shyagali, 2 Dr Kalyani Trivedi 3 1 Senior Lecturer, 2 Professor, Department of Orthodontics, Darshan
Case Report Correction of Crowding using Conservative Treatment Approach Dr Tapan Shah, 1 Dr Tarulatha Shyagali, 2 Dr Kalyani Trivedi 3 1 Senior Lecturer, 2 Professor, Department of Orthodontics, Darshan
Dr Robert Drummond. BChD, DipOdont Ortho, MChD(Ortho), FDC(SA) Ortho. Canad Inn Polo Park Winnipeg 2015
, FDC(SA) Ortho. Canad Inn Polo Park Winnipeg 2015") Dr Robert Drummond BChD, DipOdont Ortho, MChD(Ortho), FDC(SA) Ortho Canad Inn Polo Park Winnipeg 2015 Severely compromised FPM with poor prognosis Children often present with a developing dentition affected
Dr Robert Drummond BChD, DipOdont Ortho, MChD(Ortho), FDC(SA) Ortho Canad Inn Polo Park Winnipeg 2015 Severely compromised FPM with poor prognosis Children often present with a developing dentition affected
Treatment of Class II non-extraction using the Bioprogressive method
 DOI: 10.1051/odfen/2014013 J Dentofacial Anom Orthod 2014;17:407 Ó RODF / EDP Sciences Treatment of Class II non-extraction using the Bioprogressive method P. Guezenec CD SQODF, membre titulaire de la
DOI: 10.1051/odfen/2014013 J Dentofacial Anom Orthod 2014;17:407 Ó RODF / EDP Sciences Treatment of Class II non-extraction using the Bioprogressive method P. Guezenec CD SQODF, membre titulaire de la
The conservative treatment of Class I malocclusion with maxillary transverse deficiency and anterior teeth crowding
 B B O C a s e R e p o r t The conservative treatment of Class I malocclusion with maxillary transverse deficiency and anterior teeth crowding Lincoln I. Nojima* Abstract This report describes the treatment
B B O C a s e R e p o r t The conservative treatment of Class I malocclusion with maxillary transverse deficiency and anterior teeth crowding Lincoln I. Nojima* Abstract This report describes the treatment
EUROPEAN SOCIETY OF LINGUAL ORTHODONTICS
 EUROPEAN SOCIETY OF LINGUAL ORTHODONTICS CANDIDATE NUMBER: Dr. Stefan Blasius Year: 2010 WBLO 01 EUROPEAN SOCIETY OF LINGUAL ORTHODONTICS CANDIDATE NUMBER: Dr. Stefan Blasius Year: 2010 WBLO 01 RÉSUMÉ
EUROPEAN SOCIETY OF LINGUAL ORTHODONTICS CANDIDATE NUMBER: Dr. Stefan Blasius Year: 2010 WBLO 01 EUROPEAN SOCIETY OF LINGUAL ORTHODONTICS CANDIDATE NUMBER: Dr. Stefan Blasius Year: 2010 WBLO 01 RÉSUMÉ
Research & Reviews: Journal of Dental Sciences
 Research & Reviews: Journal of Dental Sciences Orthodontic Camouflage of Skeletal Class I, Class II and Class III Malocclusion in Borderline Cases Report of Three Cases Dr. Seema Kapil Lahoti 1 *, Dr.
Research & Reviews: Journal of Dental Sciences Orthodontic Camouflage of Skeletal Class I, Class II and Class III Malocclusion in Borderline Cases Report of Three Cases Dr. Seema Kapil Lahoti 1 *, Dr.
Angle Class I malocclusion with anterior open bite treated with extraction of permanent teeth
 Angle Class I malocclusion with anterior open bite treated with extraction of permanent teeth Matheus Melo Pithon 1 This clinical case reports the orthodontic treatment of a Class I malocclusion with anterior
Angle Class I malocclusion with anterior open bite treated with extraction of permanent teeth Matheus Melo Pithon 1 This clinical case reports the orthodontic treatment of a Class I malocclusion with anterior
Mesial Step Class I or Class III Dependent upon extent of step seen clinically and patient s growth pattern Refer for early evaluation (by 8 years)
") Orthodontics and Dentofacial Development Overview Development of Dentition Treatment Retention and Relapse Growth of Naso-Maxillary Complex Develops postnatally entirely by intramenbranous ossification
Orthodontics and Dentofacial Development Overview Development of Dentition Treatment Retention and Relapse Growth of Naso-Maxillary Complex Develops postnatally entirely by intramenbranous ossification
Sample Case #1. Disclaimer
 ABO Sample Cases Disclaimer Sample Case #1 The following sample questions and answers were composed and vetted by a panel of experts in orthodontics and are intended to provide an example of the types
ABO Sample Cases Disclaimer Sample Case #1 The following sample questions and answers were composed and vetted by a panel of experts in orthodontics and are intended to provide an example of the types
Early Mixed Dentition Period
 REVIEW ARTIC CLE AODMR The Effects of a Prefabricated Functional Appliance in Early Mixed Dentition Period Toshio Iwata 1, Takashi Usui 2, Nobukazu Shirakawa 2, Toshitsugu Kawata 3 1 Doctor of Philosophy
REVIEW ARTIC CLE AODMR The Effects of a Prefabricated Functional Appliance in Early Mixed Dentition Period Toshio Iwata 1, Takashi Usui 2, Nobukazu Shirakawa 2, Toshitsugu Kawata 3 1 Doctor of Philosophy
Case Report. profile relaxed relaxed smiling. How would you treat this malocclusion?
 Pre-Treatment profile relaxed relaxed smiling How would you treat this malocclusion? Case R. C. 16 years, 9 months introduction This female adolescent with bilabial protrusion and flared upper anterior
Pre-Treatment profile relaxed relaxed smiling How would you treat this malocclusion? Case R. C. 16 years, 9 months introduction This female adolescent with bilabial protrusion and flared upper anterior
Nonsurgical Treatment of Adult Open Bite Using Edgewise Appliance Combined with High-Pull Headgear and Class III Elastics
 Case Report Nonsurgical Treatment of Adult Open Bite Using Edgewise Appliance Combined with High-Pull Headgear and Class III Elastics Isao Saito, DDS, PhD a ; Masaki Yamaki, DDS, PhD b ; Kooji Hanada,
Case Report Nonsurgical Treatment of Adult Open Bite Using Edgewise Appliance Combined with High-Pull Headgear and Class III Elastics Isao Saito, DDS, PhD a ; Masaki Yamaki, DDS, PhD b ; Kooji Hanada,
Angle Class II, division 2 malocclusion with severe overbite and pronounced discrepancy*
 O C a s e R e p o r t ngle Class II, division 2 malocclusion with severe overbite and pronounced discrepancy* Daniela Kimaid Schroeder** bstract This article reports the treatment of a young patient at
O C a s e R e p o r t ngle Class II, division 2 malocclusion with severe overbite and pronounced discrepancy* Daniela Kimaid Schroeder** bstract This article reports the treatment of a young patient at
A Modified Three-piece Base Arch for en masse Retraction and Intrusion in a Class II Division 1 Subdivision Case
 Dhaval Ranjitbhai Lekhadia, Gautham Hegde RESEARCH ARTICLE 10.5005/jp-journals-10029-1149 A Modified Three-piece Base Arch for en masse Retraction and Intrusion in a Class II Division 1 Subdivision Case
Dhaval Ranjitbhai Lekhadia, Gautham Hegde RESEARCH ARTICLE 10.5005/jp-journals-10029-1149 A Modified Three-piece Base Arch for en masse Retraction and Intrusion in a Class II Division 1 Subdivision Case
Keeping all these knowledge in mind I will show you 3 cases treated with the Forsus appliance.
 Due to technical difficulties there were some audio problems with the webinar recording. Starting at 27:54, please use this guide to follow along with Dr. Kercelli s presentation. Keeping all these knowledge
Due to technical difficulties there were some audio problems with the webinar recording. Starting at 27:54, please use this guide to follow along with Dr. Kercelli s presentation. Keeping all these knowledge
Angle Class I malocclusion with bimaxillary dental protrusion and missing mandibular first molars*
 B B O C a s e R e p o r t Angle Class I malocclusion with bimaxillary dental protrusion and missing mandibular first molars* Aldino Puppin Filho** Abstract This case report describes the orthodontic treatment
B B O C a s e R e p o r t Angle Class I malocclusion with bimaxillary dental protrusion and missing mandibular first molars* Aldino Puppin Filho** Abstract This case report describes the orthodontic treatment
Class II Correction using Combined Twin Block and Fixed Orthodontic Appliances: A Case Report
 Case Report Print ISSN: 2321-6379 Online ISSN: 2321-595X DOI: 10.17354/ijss/2017/506 Class II Correction using Combined Twin Block and Fixed Orthodontic Appliances: A Case Report Ahmed Alassiry Assistant
Case Report Print ISSN: 2321-6379 Online ISSN: 2321-595X DOI: 10.17354/ijss/2017/506 Class II Correction using Combined Twin Block and Fixed Orthodontic Appliances: A Case Report Ahmed Alassiry Assistant
Case Report n 2. Patient. Age: ANB 8 OJ 4.5 OB 5.5
 Case Report n 2 Patient Age: 12.11 Diagnosis Angle cl.ii div.2 ANB 8 OJ 4.5 OB 5.5 Author: Dr. Case History The patient is a thirteen year old girl who exhibits delayed development, both physically and
Case Report n 2 Patient Age: 12.11 Diagnosis Angle cl.ii div.2 ANB 8 OJ 4.5 OB 5.5 Author: Dr. Case History The patient is a thirteen year old girl who exhibits delayed development, both physically and
The Tip-Edge appliance and
 Figure 1: Internal surfaces of the edgewise archwire slot are modified to create the Tip-Edge archwire slot. Tipping surfaces (T) limit crown tipping during retraction. Uprighting surfaces (U) control
Figure 1: Internal surfaces of the edgewise archwire slot are modified to create the Tip-Edge archwire slot. Tipping surfaces (T) limit crown tipping during retraction. Uprighting surfaces (U) control
Treatment of Class II, Division 2 Malocclusion with Miniscrew Supported En-Masse Retraction: Is Deepbite Really an Obstacle for Extraction Treatment?
 TURKISH JOURNAL of DOI: 10.5152/TurkJOrthod.2017.17034 CASE REPORT Treatment of Class II, Division 2 Malocclusion with Miniscrew Supported En-Masse Retraction: Is Deepbite Really an Obstacle for Extraction
TURKISH JOURNAL of DOI: 10.5152/TurkJOrthod.2017.17034 CASE REPORT Treatment of Class II, Division 2 Malocclusion with Miniscrew Supported En-Masse Retraction: Is Deepbite Really an Obstacle for Extraction
KJLO. A Sequential Approach for an Asymmetric Extraction Case in. Lingual Orthodontics. Case Report INTRODUCTION DIAGNOSIS
 KJLO Korean Journal of Lingual Orthodontics Case Report A Sequential Approach for an Asymmetric Extraction Case in Lingual Orthodontics Ji-Sung Jang 1, Kee-Joon Lee 2 1 Dream Orthodontic Clinic, Gimhae,
KJLO Korean Journal of Lingual Orthodontics Case Report A Sequential Approach for an Asymmetric Extraction Case in Lingual Orthodontics Ji-Sung Jang 1, Kee-Joon Lee 2 1 Dream Orthodontic Clinic, Gimhae,
Experience with Contemporary Tip-Edge plus Technique A Case Report.
 IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-issn: 2279-0853, p-issn: 2279-0861. Volume 13, Issue 3 Ver. I. (Mar. 2014), PP 12-17 Experience with Contemporary Tip-Edge plus Technique A Case
IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-issn: 2279-0853, p-issn: 2279-0861. Volume 13, Issue 3 Ver. I. (Mar. 2014), PP 12-17 Experience with Contemporary Tip-Edge plus Technique A Case
Attachment G. Orthodontic Criteria Index Form Comprehensive D8080. ABBREVIATIONS CRITERIA for Permanent Dentition YES NO
 First Review IL HFS Dental Program Models Second Review Ortho cad Attachment G Orthodontic Criteria Index Form Comprehensive D8080 Ceph Film X-Rays Photos Narrative Patient Name: DOB: ABBREVIATIONS CRITERIA
First Review IL HFS Dental Program Models Second Review Ortho cad Attachment G Orthodontic Criteria Index Form Comprehensive D8080 Ceph Film X-Rays Photos Narrative Patient Name: DOB: ABBREVIATIONS CRITERIA
2008 JCO, Inc. May not be distributed without permission. Correction of Asymmetry with a Mandibular Propulsion Appliance
 2008 JCO, Inc. May not be distributed without permission. www.jco-online.com CASE REPORT Correction of Asymmetry with a Mandibular Propulsion Appliance JOSÉ AUGUSTO MENDES MIGUEL, DDS, MSC, PHD GUSTAVO
2008 JCO, Inc. May not be distributed without permission. www.jco-online.com CASE REPORT Correction of Asymmetry with a Mandibular Propulsion Appliance JOSÉ AUGUSTO MENDES MIGUEL, DDS, MSC, PHD GUSTAVO
An Effectiv Rapid Molar Derotation: Keles K
 An Effectiv ective e and Precise Method forf Rapid Molar Derotation: Keles K TPA Ahmet Keles, DDS, DMSc 1 /Sedef Impar, DDS 2 Most of the time, Class II molar relationships occur due to the mesiopalatal
An Effectiv ective e and Precise Method forf Rapid Molar Derotation: Keles K TPA Ahmet Keles, DDS, DMSc 1 /Sedef Impar, DDS 2 Most of the time, Class II molar relationships occur due to the mesiopalatal
Class II Correction with Invisalign Molar rotation.
 Tips from your peers to help you treat with confidence. Class II Correction with Invisalign Molar rotation. Dr. Mazyar Moshiri. Class II Correction with Invisalign Molar Rotation. Dr. Mazyar Moshiri. Orthodontic
Tips from your peers to help you treat with confidence. Class II Correction with Invisalign Molar rotation. Dr. Mazyar Moshiri. Class II Correction with Invisalign Molar Rotation. Dr. Mazyar Moshiri. Orthodontic
System Orthodontic Treatment Program By Dr. Richard McLaughlin, Dr. John Bennett and Dr. Hugo Trevisi
 A Clinical Review of the MBT Versatile+ Appliance System Orthodontic Treatment Program By Dr. Richard McLaughlin, Dr. John Bennett and Dr. Hugo Trevisi Treatment Philosophy of the MBT Appliance System
A Clinical Review of the MBT Versatile+ Appliance System Orthodontic Treatment Program By Dr. Richard McLaughlin, Dr. John Bennett and Dr. Hugo Trevisi Treatment Philosophy of the MBT Appliance System
SURGICAL - ORTHODONTIC TREATMENT OF CLASS II DIVISION 1 MALOCCLUSION IN AN ADULT PATIENT: A CASE REPORT
 Case Report International Journal of Dental and Health Sciences Volume 02, Issue 02 SURGICAL - ORTHODONTIC TREATMENT OF CLASS II DIVISION 1 MALOCCLUSION IN AN ADULT PATIENT: A CASE REPORT Amit Dahiya 1,Minakshi
Case Report International Journal of Dental and Health Sciences Volume 02, Issue 02 SURGICAL - ORTHODONTIC TREATMENT OF CLASS II DIVISION 1 MALOCCLUSION IN AN ADULT PATIENT: A CASE REPORT Amit Dahiya 1,Minakshi
The Tip-Edge Concept: Eliminating Unnecessary Anchorage Strain
 Welcome Ron Not Ron? Click here. My Account The Tip-Edge Concept: Eliminating Unnecessary Anchorage Strain VOLUME 26 : NUMBER 03 : PAGES (165-178) 1992 CHRISTOPHER K. KESLING, DDS, MS Tooth movement in
Welcome Ron Not Ron? Click here. My Account The Tip-Edge Concept: Eliminating Unnecessary Anchorage Strain VOLUME 26 : NUMBER 03 : PAGES (165-178) 1992 CHRISTOPHER K. KESLING, DDS, MS Tooth movement in
With judicious treatment planning, the clinical
 CLINICIAN S CORNER Selecting custom torque prescriptions for the straight-wire appliance Earl Johnson San Francisco, Calif Selecting custom torque prescriptions based on the treatment needs of each patient
CLINICIAN S CORNER Selecting custom torque prescriptions for the straight-wire appliance Earl Johnson San Francisco, Calif Selecting custom torque prescriptions based on the treatment needs of each patient
Maxillary Expansion and Protraction in Correction of Midface Retrusion in a Complete Unilateral Cleft Lip and Palate Patient
 Case Report Maxillary Expansion and Protraction in Correction of Midface Retrusion in a Complete Unilateral Cleft Lip and Palate Patient Masayoshi Kawakami, DDS, PhD a ; Takakazu Yagi, DDS, PhD b ; Kenji
Case Report Maxillary Expansion and Protraction in Correction of Midface Retrusion in a Complete Unilateral Cleft Lip and Palate Patient Masayoshi Kawakami, DDS, PhD a ; Takakazu Yagi, DDS, PhD b ; Kenji
INDICATIONS. Fixed Appliances are indicated when precise tooth movements are required
 DEFINITION Fixed Appliances are devices or equipments that are attached to the teeth, cannot be removed by the patient and are capable of causing tooth movement. INDICATIONS Fixed Appliances are indicated
DEFINITION Fixed Appliances are devices or equipments that are attached to the teeth, cannot be removed by the patient and are capable of causing tooth movement. INDICATIONS Fixed Appliances are indicated
Non Extraction philosophy: Distalization using Jone s Jig appliance- a case report
 IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-issn: 2279-0853, p-issn: 2279-0861.Volume 13, Issue 9 Ver. IV (Sep. 2014), PP 36-41 Non Extraction philosophy: Distalization using Jone s Jig appliance-
IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-issn: 2279-0853, p-issn: 2279-0861.Volume 13, Issue 9 Ver. IV (Sep. 2014), PP 36-41 Non Extraction philosophy: Distalization using Jone s Jig appliance-
Invisalign technique in the treatment of adults with pre-restorative concerns
 Mampieri and Giancotti Progress in Orthodontics 2013, 14:40 REVIEW Open Access Invisalign technique in the treatment of adults with pre-restorative concerns Gianluca Mampieri * and Aldo Giancotti Abstract
Mampieri and Giancotti Progress in Orthodontics 2013, 14:40 REVIEW Open Access Invisalign technique in the treatment of adults with pre-restorative concerns Gianluca Mampieri * and Aldo Giancotti Abstract
EUROPEAN SOCIETY OF LINGUAL ORTHODONTICS
 EUROPEAN SOCIETY OF LINGUAL ORTHODONTICS EUROPEAN SOCIETY OF LINGUAL ORTHODONTICS KANARELIS PANAGIOTIS (TAKIS) CASE NUMBER: 1 Year: 2012 WBLO 1 RÉSUMÉ OF CASE 1 CASE CATEGORY: ADULT MALOCCLUSION NAME:
EUROPEAN SOCIETY OF LINGUAL ORTHODONTICS EUROPEAN SOCIETY OF LINGUAL ORTHODONTICS KANARELIS PANAGIOTIS (TAKIS) CASE NUMBER: 1 Year: 2012 WBLO 1 RÉSUMÉ OF CASE 1 CASE CATEGORY: ADULT MALOCCLUSION NAME:
6. Timing for orthodontic force
 6. Timing for orthodontic force Orthodontic force is generally less than 300gm, so early mechanical stability is enough for immediate orthodontic force. There is no actually difference in success rate
6. Timing for orthodontic force Orthodontic force is generally less than 300gm, so early mechanical stability is enough for immediate orthodontic force. There is no actually difference in success rate
Treatment of a Patient with Class I Malocclusion and Severe Tooth Crowding Using Invisalign and Fixed Appliances
 36 Dental Medicine Research 34 1 36 40, 2014 Case Report Treatment of a Patient with Class I Malocclusion and Severe Tooth Crowding Using Invisalign and Fixed Appliances Yumiko OGURA, Wakana YANAGISAWA,
36 Dental Medicine Research 34 1 36 40, 2014 Case Report Treatment of a Patient with Class I Malocclusion and Severe Tooth Crowding Using Invisalign and Fixed Appliances Yumiko OGURA, Wakana YANAGISAWA,
Orthodontic Treatment Using The Dental VTO And MBT System
 Orthodontic Treatment Using The Dental VTO And MBT System by Dr. Hideyuki Iyano Dr. Hideyuki Iyano, Department of Orthodontics, Ohu University School of Dentistry, Japan. He is also a member of the Japan
Orthodontic Treatment Using The Dental VTO And MBT System by Dr. Hideyuki Iyano Dr. Hideyuki Iyano, Department of Orthodontics, Ohu University School of Dentistry, Japan. He is also a member of the Japan
Mx1 to NA = 34 & 10 mm. Md1 to NB = 21 & 3 mm.
 Chapter 16 Clinical cases: mixed dentition and adolescent, CLII non-extraction 219 Full CLII div I OJ = 15 OB = 8 SNA = 82 SNB = 75 Mx1 to NA = 34 & 10 mm. Md1 to NB = 21 & 3 mm. Md1 to A-pog = -2 GO-GN
Chapter 16 Clinical cases: mixed dentition and adolescent, CLII non-extraction 219 Full CLII div I OJ = 15 OB = 8 SNA = 82 SNB = 75 Mx1 to NA = 34 & 10 mm. Md1 to NB = 21 & 3 mm. Md1 to A-pog = -2 GO-GN
Correction of Class II Division 2 Malocclusion by Fixed Functional Class II Corrector Appliance: Case Report
 Case Report To cite: Kumar M, Sharma H, Bohara P. Correction of class II division 2 malocclusion by fixed functional class II corrector appliance: case report. Journal of contemporary orthodontics, February
Case Report To cite: Kumar M, Sharma H, Bohara P. Correction of class II division 2 malocclusion by fixed functional class II corrector appliance: case report. Journal of contemporary orthodontics, February
Arrangement of the artificial teeth:
 Lecture Prosthodontic Dr. Osama Arrangement of the artificial teeth: It s the placement of the teeth on a denture with definite objective in mind or it s the setting of teeth on temporary bases. Rules
Lecture Prosthodontic Dr. Osama Arrangement of the artificial teeth: It s the placement of the teeth on a denture with definite objective in mind or it s the setting of teeth on temporary bases. Rules
The Modified Twin Block Appliance in the Treatment of Class II Division 2 Malocclusions
 Journal of Orthodontics/Vol. 28/2001/271 280 The Modified Twin Block Appliance in the Treatment of Class II Division 2 Malocclusions F. M. V. DYER H. F. MCKEOWN P. J. SANDLER Department of Orthodontics,
Journal of Orthodontics/Vol. 28/2001/271 280 The Modified Twin Block Appliance in the Treatment of Class II Division 2 Malocclusions F. M. V. DYER H. F. MCKEOWN P. J. SANDLER Department of Orthodontics,
ORTHODONTICS Treatment of malocclusion Assist.Lec.Kasem A.Abeas University of Babylon Faculty of Dentistry 5 th stage
 Lec: Treatment of class I malocclusion Class I occlusion can be defined by Angles, classification as the mesiobuccal cusp of the upper 1 st permanent molar occlude with the developmental groove of the
Lec: Treatment of class I malocclusion Class I occlusion can be defined by Angles, classification as the mesiobuccal cusp of the upper 1 st permanent molar occlude with the developmental groove of the
ISW for the treatment of adult anterior crossbite with severe crowding combined facial asymmetry case
 International Research Journal of Medicine and Biomedical Sciences Vol.3 (2),pp. 15-29, November 2018 Available online at http://www.journalissues.org/irjmbs/ https://doi.org/10.15739/irjmbs.18.004 Copyright
International Research Journal of Medicine and Biomedical Sciences Vol.3 (2),pp. 15-29, November 2018 Available online at http://www.journalissues.org/irjmbs/ https://doi.org/10.15739/irjmbs.18.004 Copyright
#45 Ortho-Tain, Inc PREVENTIVE ERUPTION GUIDANCE -- PREVENTIVE OCCLUSAL DEVELOPMENT
 #45 Ortho-Tain, Inc. 1-800-541-6612 PREVENTIVE ERUPTION GUIDANCE -- PREVENTIVE OCCLUSAL DEVELOPMENT Analysis and Diagnosis of Occlusion: The ideal child of 5 y ears of age that probably has the best chance
#45 Ortho-Tain, Inc. 1-800-541-6612 PREVENTIVE ERUPTION GUIDANCE -- PREVENTIVE OCCLUSAL DEVELOPMENT Analysis and Diagnosis of Occlusion: The ideal child of 5 y ears of age that probably has the best chance
Maxillary Growth Control with High Pull Headgear- A Case Report
 IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-issn: 2279-0853, p-issn: 2279-0861.Volume 17, Issue 01 Ver. X January. (2018), PP 09-13 www.iosrjournals.org Maxillary Growth Control with High
IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-issn: 2279-0853, p-issn: 2279-0861.Volume 17, Issue 01 Ver. X January. (2018), PP 09-13 www.iosrjournals.org Maxillary Growth Control with High
ADOLESCENT TREATMENT. Thomas J. Cangialosi. Stella S. Efstratiadis. CHAPTER 18 Pages CLASS II DIVISION 1 WHY NOW?
 ADOLESCENT By Thomas J. Cangialosi and Stella S. Efstratiadis From Riolo, M. and Avery, J. Eds., Essentials for Orthodontic Practice, EFOP Press of EFOP, LLC. Ann Arbor and Grand Haven, Michigan, U.S.A.,
ADOLESCENT By Thomas J. Cangialosi and Stella S. Efstratiadis From Riolo, M. and Avery, J. Eds., Essentials for Orthodontic Practice, EFOP Press of EFOP, LLC. Ann Arbor and Grand Haven, Michigan, U.S.A.,
Forsus Class II Correctors as an Effective and Efficient Form of Anchorage in Extraction Cases
 Forsus Class II Correctors as an Effective and Efficient Form of Anchorage in Extraction Cases by Lisa Alvetro, DDS, MSD After receiving her DDS summa cum laude from Ohio State University, Dr. Alvetro
Forsus Class II Correctors as an Effective and Efficient Form of Anchorage in Extraction Cases by Lisa Alvetro, DDS, MSD After receiving her DDS summa cum laude from Ohio State University, Dr. Alvetro
We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists. International authors and editors
 We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists 3,900 116,000 120M Open access books available International authors and editors Downloads Our
We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists 3,900 116,000 120M Open access books available International authors and editors Downloads Our
ortho case report Sagittal First international magazine of orthodontics By Dr. Luis Carrière Special Reprint
 Cover image courtesy of K Line Europe GmbH (www.kline-europe.de) ortho Special Reprint international magazine of orthodontics 1 2017 case report Sagittal First By Dr. Luis Carrière Sagittal First Author:
Cover image courtesy of K Line Europe GmbH (www.kline-europe.de) ortho Special Reprint international magazine of orthodontics 1 2017 case report Sagittal First By Dr. Luis Carrière Sagittal First Author:
Enhanced Control in the Transverse Dimension using the Unitek MIA Quad Helix System by Dr. Sven G. Wiezorek
 Enhanced Control in the Transverse Dimension using the Unitek MIA Quad Helix System by Dr. Sven G. Wiezorek Dr. Wiezorek studied dental medicine at Kiel University, Germany from 1987 to 1993. He then finished
Enhanced Control in the Transverse Dimension using the Unitek MIA Quad Helix System by Dr. Sven G. Wiezorek Dr. Wiezorek studied dental medicine at Kiel University, Germany from 1987 to 1993. He then finished
Unilateral Horizontally Impacted Maxillary Canine and First Premolar Treated with a Double Archwire Technique
 Case Report Unilateral Horizontally Impacted Maxillary Canine and First Premolar Treated with a Double Archwire Technique Chien-Lun Peng a ; Yu-Yu Su b ; Sheng-Yang Lee c Abstract: A patient with a unilateral
Case Report Unilateral Horizontally Impacted Maxillary Canine and First Premolar Treated with a Double Archwire Technique Chien-Lun Peng a ; Yu-Yu Su b ; Sheng-Yang Lee c Abstract: A patient with a unilateral
The ASE Example Case Report 2010
 The ASE Example Case Report 2010 The Requirements for Case Presentation in The Angle Society of Europe are specified in the Appendix I to the Bylaws. This example case report exemplifies how these requirements
The ASE Example Case Report 2010 The Requirements for Case Presentation in The Angle Society of Europe are specified in the Appendix I to the Bylaws. This example case report exemplifies how these requirements
MANAGEMENT OF CLASS II DIVISION 2 MALOCCLUSION AN INSIGHT
 MANAGEMENT OF CLASS II DIVISION 2 MALOCCLUSION AN INSIGHT Dr. C.S. Ramachandra Author: Prof. Dr. C.S. Ramachandra Diplomat Indian Board of Orthodontics Professor & Head Dept. of Orthodontics, Principal,
MANAGEMENT OF CLASS II DIVISION 2 MALOCCLUSION AN INSIGHT Dr. C.S. Ramachandra Author: Prof. Dr. C.S. Ramachandra Diplomat Indian Board of Orthodontics Professor & Head Dept. of Orthodontics, Principal,
MOLAR DISTALIZATION WITH MODIFIED GRAZ IMPLANT SUPPORTED PENDULUM SPRINGS. A CASE REPORT.
 MOLAR DISTALIZATION WITH MODIFIED GRAZ IMPLANT SUPPORTED PENDULUM SPRINGS. A CASE REPORT. Author : Dr. Arundhati P. Tandur MDS, MDORCPS [Glasgow], IMORTHRCS [England], Diplomate of Indian Board Vice-Principal
MOLAR DISTALIZATION WITH MODIFIED GRAZ IMPLANT SUPPORTED PENDULUM SPRINGS. A CASE REPORT. Author : Dr. Arundhati P. Tandur MDS, MDORCPS [Glasgow], IMORTHRCS [England], Diplomate of Indian Board Vice-Principal
Concepts of occlusion Balanced occlusion. Monoplane occlusion. Lingualized occlusion. Figure (10-1)
") Any contact between teeth of opposing dental arches; usually, referring to contact between the occlusal surface. The static relationship between the incising or masticatory surfaces of the maxillary or
Any contact between teeth of opposing dental arches; usually, referring to contact between the occlusal surface. The static relationship between the incising or masticatory surfaces of the maxillary or
AUSTRALASIAN ORTHODONTIC BOARD
 AUSTRALASIAN ORTHODONTIC BOARD CASE IDENTIFICATION 18 - ST AUSTRALASIAN ORTHODONTIC BOARD CASE DETAILS (Form 2) After you have received your AOB Number, you must submit to your State Convenor 1 : Form
AUSTRALASIAN ORTHODONTIC BOARD CASE IDENTIFICATION 18 - ST AUSTRALASIAN ORTHODONTIC BOARD CASE DETAILS (Form 2) After you have received your AOB Number, you must submit to your State Convenor 1 : Form
Correction of a maxillary canine-first premolar transposition using mini-implant anchorage
 CASE REPORT Correction of a maxillary canine-first premolar transposition using mini-implant anchorage Mehmet Oguz Oztoprak, DDS, MSc, a Cigdem Demircan, DDS, b Tulin Arun, PhD, DDS, MSc c Transposition
CASE REPORT Correction of a maxillary canine-first premolar transposition using mini-implant anchorage Mehmet Oguz Oztoprak, DDS, MSc, a Cigdem Demircan, DDS, b Tulin Arun, PhD, DDS, MSc c Transposition
TWO PHASE FOR A BETTER FACE!! TWIN BLOCK AND HEADGEAR FOLLOWED BY FIXED THERAPY FOR CLASS II CORRECTION
 Case Report NUJHS Vol. 5, No.2, June 2015, ISSN 2249-7110 TWO PHASE FOR A BETTER FACE!! TWIN BLOCK AND HEADGEAR FOLLOWED BY FIXED THERAPY FOR CLASS II CORRECTION 1 2 3 4 U S Krishna Nayak, Ashutosh Shetty,
Case Report NUJHS Vol. 5, No.2, June 2015, ISSN 2249-7110 TWO PHASE FOR A BETTER FACE!! TWIN BLOCK AND HEADGEAR FOLLOWED BY FIXED THERAPY FOR CLASS II CORRECTION 1 2 3 4 U S Krishna Nayak, Ashutosh Shetty,
THE MBT VERSATILE+ APPLIANCE SYSTEM
 THE MBT VERSATILE+ APPLIANCE SYSTEM McLaughlin, Bennett, Trevisi The MBT Versatile+ Appliance System THE DEVELOPMENT OF A TREATMENT MECHANICS AND APPLIANCE PHILOSOPHY The first fully programmed preadjusted
THE MBT VERSATILE+ APPLIANCE SYSTEM McLaughlin, Bennett, Trevisi The MBT Versatile+ Appliance System THE DEVELOPMENT OF A TREATMENT MECHANICS AND APPLIANCE PHILOSOPHY The first fully programmed preadjusted
Nonextraction Treatment of Upper Canine Premolar Transposition in an Adult Patient
 Case Report Nonextraction Treatment of Upper Canine Premolar Transposition in an Adult Patient Shingo Kuroda a ; Yasuko Kuroda b Abstract: This article reports the successful treatment of a unilateral
Case Report Nonextraction Treatment of Upper Canine Premolar Transposition in an Adult Patient Shingo Kuroda a ; Yasuko Kuroda b Abstract: This article reports the successful treatment of a unilateral
Use of a Tip-Edge Stage-1 Wire to Enhance Vertical Control During Straight Wire Treatment: Two Case Reports
 Case Report Use of a Tip-Edge Stage-1 Wire to Enhance Vertical Control During Straight Wire Treatment: Two Case Reports Helen Taylor, BDS, MScD, DOrth, MOrth, FDSRCS(Eng) a Abstract: Vertical control is
Case Report Use of a Tip-Edge Stage-1 Wire to Enhance Vertical Control During Straight Wire Treatment: Two Case Reports Helen Taylor, BDS, MScD, DOrth, MOrth, FDSRCS(Eng) a Abstract: Vertical control is
Volume 22 No. 14 September Dentists, Federally Qualified Health Centers and Health Maintenance Organizations For Action
 State of New Jersey Department of Human Services Division of Medical Assistance & Health Services Volume 22 No. 14 September 2012 TO: Dentists, Federally Qualified Health Centers and Health Maintenance
State of New Jersey Department of Human Services Division of Medical Assistance & Health Services Volume 22 No. 14 September 2012 TO: Dentists, Federally Qualified Health Centers and Health Maintenance
Checklist with summary points
 Checklist with summary points Question 1: Are your doctor Invisalign preferences on your home page up to date? Go to your doctor home page and open up your doctor preferences pages. Be sure to update item
Checklist with summary points Question 1: Are your doctor Invisalign preferences on your home page up to date? Go to your doctor home page and open up your doctor preferences pages. Be sure to update item
Class III malocclusion occurs in less than 5%
 CDABO CASE REPORT Orthodontic correction of a Class III malocclusion in an adolescent patient with a bonded RPE and protraction face mask Steven W. Smith, DDS, a and Jeryl D. English, DDS, MS b Dallas,
CDABO CASE REPORT Orthodontic correction of a Class III malocclusion in an adolescent patient with a bonded RPE and protraction face mask Steven W. Smith, DDS, a and Jeryl D. English, DDS, MS b Dallas,
The 20/20 Molar Tube. Ronald M. Roncone, D.D.S., M.S.
 The 20/20 Molar Tube by Ronald M. Roncone, D.D.S., M.S. A) Finish torque STAGE 3: Interactive to Active GOALS 4-6 months B) Finish root uprighting C) Maintain arch form D) Set occlusion with active settling
The 20/20 Molar Tube by Ronald M. Roncone, D.D.S., M.S. A) Finish torque STAGE 3: Interactive to Active GOALS 4-6 months B) Finish root uprighting C) Maintain arch form D) Set occlusion with active settling
Treatment of an open bite case with 3M Clarity ADVANCED Ceramic Brackets and miniscrews.
 SM 3M Health Care Academy Treatment of an open bite case with 3M Clarity ADVANCED Ceramic Brackets and miniscrews. Dr. J.C. Pérez-Varela MD, DDS, MS, Ph.D. Specialist in Orthodontics. Doctor of Medicine
SM 3M Health Care Academy Treatment of an open bite case with 3M Clarity ADVANCED Ceramic Brackets and miniscrews. Dr. J.C. Pérez-Varela MD, DDS, MS, Ph.D. Specialist in Orthodontics. Doctor of Medicine
Introduction. Facial findings. Intraoral findings. Frontal and lateral cephalometric photographs
 Journal of Dental and Oral Health Scient Open Access Exploring the World of Science ISSN: 2369-4475 Case Report A Case of Orthodontic Treatment for a Patient with Occlusal Abnormality This article was
Journal of Dental and Oral Health Scient Open Access Exploring the World of Science ISSN: 2369-4475 Case Report A Case of Orthodontic Treatment for a Patient with Occlusal Abnormality This article was
The following standards and procedures apply to the provision of orthodontic services for children in the Medicaid/NJ FamilyCare (NJFC) programs.
 programs.") B.4.2.11 Orthodontic Services The following standards and procedures apply to the provision of orthodontic services for children in the Medicaid/NJ FamilyCare (NJFC) programs. Orthodontic Consultation
B.4.2.11 Orthodontic Services The following standards and procedures apply to the provision of orthodontic services for children in the Medicaid/NJ FamilyCare (NJFC) programs. Orthodontic Consultation
Treatment of Angle Class III. Department of Paedodontics and Orthodontics Dr. habil. Melinda Madléna associate professor
 Department of Paedodontics and Orthodontics Dr. habil. Melinda Madléna associate professor Disorders in Angle Class III The position of the lower jaw is foreward regarding to the upper jaw Mesialocclusion
Department of Paedodontics and Orthodontics Dr. habil. Melinda Madléna associate professor Disorders in Angle Class III The position of the lower jaw is foreward regarding to the upper jaw Mesialocclusion
Transverse malocclusion, posterior crossbite and severe discrepancy*
 O C a s e R e p o r t Transverse malocclusion, posterior crossbite and severe discrepancy* Roberto Carlos odart randão** bstract This article reports the orthodontic treatment of a 14 years and 2 months
O C a s e R e p o r t Transverse malocclusion, posterior crossbite and severe discrepancy* Roberto Carlos odart randão** bstract This article reports the orthodontic treatment of a 14 years and 2 months
Fixed Twin Blocks. Guidelines for case selection are similar to those for removable Twin Block appliances.
 Fixed Twin Blocks Development of Fixed Twin Blocks Dr Clark has enjoyed the cooperation of Dynaflex in developing the Fixed Twin Block. Six years of clinical testing has confirmed that this technique produces
Fixed Twin Blocks Development of Fixed Twin Blocks Dr Clark has enjoyed the cooperation of Dynaflex in developing the Fixed Twin Block. Six years of clinical testing has confirmed that this technique produces
Class II correction with Invisalign - Combo treatments. Carriere Distalizer.
 Tips from your peers to help you treat with confidence. Class II correction with Invisalign - Combo treatments. Carriere Distalizer. Dr. Clark D. Colville. Carriere Distalizer and Invisalign Combo. A distalization
Tips from your peers to help you treat with confidence. Class II correction with Invisalign - Combo treatments. Carriere Distalizer. Dr. Clark D. Colville. Carriere Distalizer and Invisalign Combo. A distalization
ISW for the treatment of moderate crowding dentition with unilateral second molar impaction
 International Research Journal of Public and Environmental Health Vol.5 (6),pp. 90-103, September 2018 Available online at https://www.journalissues.org/irjpeh/ https://doi.org/10.15739/irjpeh.18.013 Copyright
International Research Journal of Public and Environmental Health Vol.5 (6),pp. 90-103, September 2018 Available online at https://www.journalissues.org/irjpeh/ https://doi.org/10.15739/irjpeh.18.013 Copyright
#39 Ortho-Tain, Inc
 1 #39 Ortho-Tain, Inc. 1-800-541-6612 OPTIMUM ORTHODONTICS FOR THE 5 TO 12 YEAR-OLD BY COMBINING REMOVABLE AND FIXED APPLIANCES WITH THE USE OF THE NITE-GUIDE AND OCCLUS-O-GUIDE APPLIANCES INTRODUCTION:
1 #39 Ortho-Tain, Inc. 1-800-541-6612 OPTIMUM ORTHODONTICS FOR THE 5 TO 12 YEAR-OLD BY COMBINING REMOVABLE AND FIXED APPLIANCES WITH THE USE OF THE NITE-GUIDE AND OCCLUS-O-GUIDE APPLIANCES INTRODUCTION:
Skeletal class III maloeclusion treated using a non-surgieal approach supplemented with mini-implants: a case report
 Journal oforthodontîcz^ol 40, 2013, 256-263! CLINICAL SECTION Skeletal class III maloeclusion treated using a non-surgieal approach supplemented with mini-implants: a case report Marcel Marchiori Farret^
Journal oforthodontîcz^ol 40, 2013, 256-263! CLINICAL SECTION Skeletal class III maloeclusion treated using a non-surgieal approach supplemented with mini-implants: a case report Marcel Marchiori Farret^
CASE: EXTRACTION Dr. TRAINING M (CA) Caucasian AGE: 8.6 VISUAL NORMS RMO X: 02/06/ R: 02/21/2003 MISSING PERMANENT TEETH RMO 2003
 Caucasian AGE: 8.6 VISUAL NORMS RMO X: 02/06/ R: 02/21/2003 MISSING PERMANENT TEETH RMO 2003") O C RMO CASE: EXTRACTION Dr. TRAINING M (CA) Caucasian AGE:. X: // - R: // MISSING PERMANENT TEETH VISUAL NORMS RMO R L RMO Diagnostic Services RMO, Inc. ()- Post Office Box ()- Canoga Park, CA - EXTRACTION
O C RMO CASE: EXTRACTION Dr. TRAINING M (CA) Caucasian AGE:. X: // - R: // MISSING PERMANENT TEETH VISUAL NORMS RMO R L RMO Diagnostic Services RMO, Inc. ()- Post Office Box ()- Canoga Park, CA - EXTRACTION
Crowded Class II Division 2 Malocclusion with Class I Molars Due to Blocked In Lower Second Premolars
 IJOI 35 iaoi CASE REPORT Crowded Class II Division 2 Malocclusion with Class I Molars Due to Blocked In Lower Second Premolars Abstract An 8y2mo female presented a Class II Division 2 malocclusion associated
IJOI 35 iaoi CASE REPORT Crowded Class II Division 2 Malocclusion with Class I Molars Due to Blocked In Lower Second Premolars Abstract An 8y2mo female presented a Class II Division 2 malocclusion associated
Corporate Medical Policy
 Corporate Medical Policy File Name: Origination: Last CAP Review: Next CAP Review: Last Review: orthodontics_for_pediatric_patients 2/2014 10/2017 10/2018 10/2017 Description of Procedure or Service Children
Corporate Medical Policy File Name: Origination: Last CAP Review: Next CAP Review: Last Review: orthodontics_for_pediatric_patients 2/2014 10/2017 10/2018 10/2017 Description of Procedure or Service Children
Extractions of first permanent molars in orthodontics: Treatment planning, technical considerations and two clinical case reports
 Case Report 41 Extractions of first permanent molars in orthodontics: Treatment planning, technical considerations and two clinical case reports Ashok Surana a, Siddhartha Dhar b, SurajitChakrabarty c,
Case Report 41 Extractions of first permanent molars in orthodontics: Treatment planning, technical considerations and two clinical case reports Ashok Surana a, Siddhartha Dhar b, SurajitChakrabarty c,
Quantitative management of morphological problems of the incisor-canine group
 DOI: 10.1051/odfen/2013405 J Dentofacial Anom Orthod 2013;16:105 Ó RODF / EDP Sciences Quantitative management of morphological problems of the incisor-canine group Jacques FAURE ABSTRACT The maxillary
DOI: 10.1051/odfen/2013405 J Dentofacial Anom Orthod 2013;16:105 Ó RODF / EDP Sciences Quantitative management of morphological problems of the incisor-canine group Jacques FAURE ABSTRACT The maxillary
Crowding and protrusion treated by unusual extractions
 SM 3M Health Care Academy Crowding and protrusion treated by unusual extractions Gianluigi Fiorillo, DDS Dr. Gianluigi Fiorillo received his degree in Dentistry from La Sapienza University of Rome in 1992
SM 3M Health Care Academy Crowding and protrusion treated by unusual extractions Gianluigi Fiorillo, DDS Dr. Gianluigi Fiorillo received his degree in Dentistry from La Sapienza University of Rome in 1992
Ectopic upper canine associated to ectopic lower second bicuspid. Case report
 Original Article Published on 15-06-2001 In Italiano, per favore En Español, por favor Ectopic upper canine associated to ectopic lower second bicuspid. Case report A.R. Mazzocchi* * MD DDS. Corresponding
Original Article Published on 15-06-2001 In Italiano, per favore En Español, por favor Ectopic upper canine associated to ectopic lower second bicuspid. Case report A.R. Mazzocchi* * MD DDS. Corresponding
Benefit Changes for Texas Health Steps Orthodontic Dental Services Effective January 1, 2012
 Benefit Changes for Texas Health Steps Orthodontic Dental Services Effective January 1, 2012 Information posted November 14, 2011 Effective for dates of service on or after January 1, 2012, the following
Benefit Changes for Texas Health Steps Orthodontic Dental Services Effective January 1, 2012 Information posted November 14, 2011 Effective for dates of service on or after January 1, 2012, the following
The practice of orthodontics is faced with new
 CLINICIAN S CORNER A new approach to correction of crowding William Randol Womack, DDS, a Jae H. Ahn, DDS, MSD, b Zahra Ammari, DDS, MDSc, c and Anamaría Castillo, DDS, MS c Phoenix, Ariz, and Santa Clara,
CLINICIAN S CORNER A new approach to correction of crowding William Randol Womack, DDS, a Jae H. Ahn, DDS, MSD, b Zahra Ammari, DDS, MDSc, c and Anamaría Castillo, DDS, MS c Phoenix, Ariz, and Santa Clara,