A Cusp-fossa Equilibration Technique Using a Numbered Leaf Gauge*
|
|
|
- Emory Piers Watson
- 6 years ago
- Views:
Transcription
1 A Cusp-fossa Equilibration Technique Using a Numbered Leaf Gauge* Richard W. Huffman, D.D.S. * * Oceanside, California, U.S.A. INTRODUCTION Occlusal equilibration is one form of occlusal therapy. A less technique-sensitive equilibration procedure is presented in which a numbered leaf gauge is used to replace operator-guided manipulative procedures to register premature contacts in centric relation jaw closure. The leaf gauge is used as part of the cusp-fossa analysis technique which fulfills gnathological criteria. The signs and symptoms of occlusal disease are generally classified as tooth symptoms, TMJ or muscle symptoms, or periodontal problems. 1 Persons suffering from the signs and symptoms of "occlusal disease" or "pathological occlusion" require some form of occlusal therapy in order to solve their problems. The various forms of occlusal therapy usually considered are: equilibration; restorative procedures, prosthetic or orthodontic; orthognathic surgery; or various combinations of these modalities. The fastest, and usually the least expensive form of occlusal therapy is occlusal equilibration. It is the purpose of this paper to discuss occlusal equilibration as a treatment modality to alleviate the signs and symptoms of occlusal disease. One must have a philosophy of occlusion prior to attempting any form of occlusal treatment. I believe the gnathological concept as advocated by McCollum and Stuart provides the kindest, most comfortable, and most stable occlusion. 2 According to the gnathological concept, the prerequisites for occlusal equilibration (or any form of occlusal therapy) are: * Presented to the Twelfth Congress of the International Academy of Gnathology. August 1985, Coronado, California. ** Professor, Emeritus Director of Occlusion and T.M.J. Clinics, The Ohio State University College of Dentistry. The Journal of Gnathology Vol. 6, No. 1,
2 Huffman 1. The posterior teeth must stop the jaw closure and neither guide nor deflect the closure. A cusp to fossa relationship provides the most ideal closure stops. 2. The anterior teeth must be coupled together to provide immediate disclusion of the posterior teeth in any eccentric jaw movement. 3. This disclusion must be in harmony with the dictates of the temporomandibu lar joints; one cannot arbitrarily alter the form of the canines or anteriors, disregarding joint function. In my experience of treating patients with the signs and symptoms of occlusal disease it is only possible to equilibrate approximately 60% of them. The other 40% require other treatment modalities such as orthodontics, restorative, prosthetic, etc. The only way to determine which patients are among the 60% who are equilibratable is to mount casts accurately and perform a diagnostic equilibration prior to attempting intraoral procedures. This is especially true if you are teaching undergraduate dental students or graduate dentists who are just entering into the area of occlusal therapy. For the same reason, in the 60% who are equilibratable it is important to develop a reliable technique which is equally effective and teachable to the inexperienced as well as the experienced operator. Probably the most difficult part of any equilibration technique is obtaining and marking the true centric relation prematurities in a step by step fashion as the equilibration proceeds. I believe the leaf gauge accomplishes this prerequisite better than any of the jaw manipulative techniques or other mechanical devices. A leaf gauge (Fig. 1) is a very simple device similar to a feeler gauge, except that al I leaves are of the same thickness. Leaves may be made of mylar, polyester, polycarbonate, acetate, or other types of plastic material. Ideally they should bend freely but not crease and should rebound to their original shape for reuse. Long introduced the leaf gauge in 1973 at which time he discussed its construction and use in locating and recording centric relation and in adjusting occlusion. 3 Williamson has done electromyographic research utilizing the leaf gauge relative to its clinical application in determining and recording centric relation and has confirmed its efficacy. 4 Golsen and Shaw have confirmed the use of the leaf gauge and its effectiveness in tripodizing the mandible for interocclusal record techniques and in occlusal adjustments. 5 24
3
4
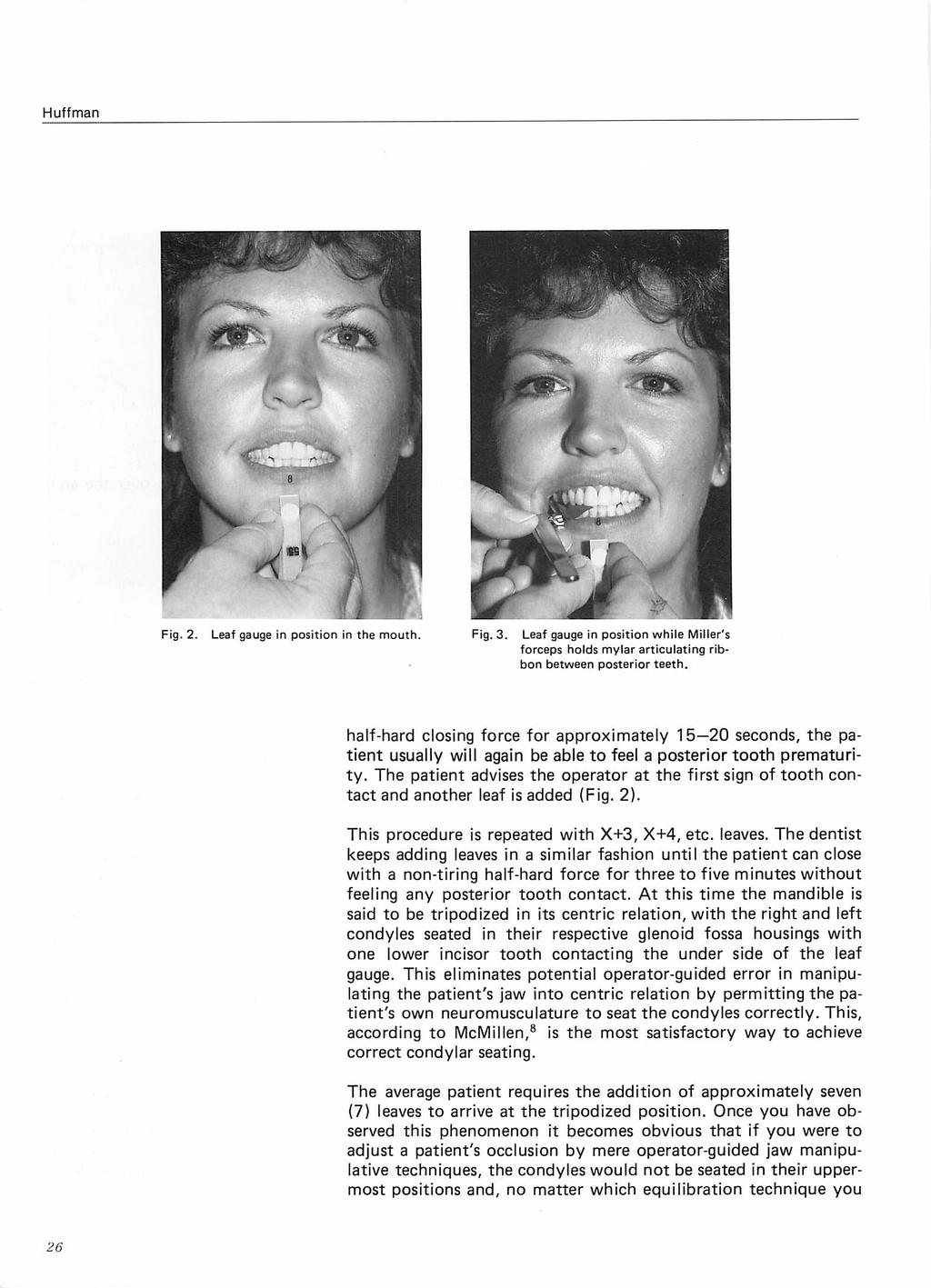
5 A Cusp-fossa Equilibration Technique Using a Numbered Leaf Gauge use, you will end up with deflective malocclusion. The next time you perform an occlusal equilibration by whatever manipulative technique you normally employ, we suggest testing it with a leaf gauge when you have finished. You can very easily determine whether you have deflection remaining or not. HOW TO USE THE LEAF GAUGE FOR EQUILIBRA TION When using the leaf gauge for occlusal equilibration, the finalized number of leaves is determined by that number wherein the patient cannot feel posterior tooth contact after biting on the leaves for three minutes. At that point remove one leaf, wipe off the first premature area with a dry 2 x 2 gauze sponge and position a strip of mylar articulating film held in a Miller forceps over the arch of teeth ( Fig. 3). Position the leaf gauge and instruct the patient to close on the back teeth and, as soon as a posterior tooth contact is felt, to tap up and down - thereby marking the first premature contact. The operator then analyzes the marks, using the cusp-to-fossa criteria, and adjusts the prematurity. In addition to the marks on the teeth, the operator uses spray-painted diagnostic casts for reference along with a selective grinding list based on information derived during the diagnostic equilibration. After the prematurity is adjusted, the patient closes again with the same number of leaves in place as before the adjustment to make sure enough tooth structure has been removed. This is done by testing for tooth contact with.0005" plastic "shim stock" (Shim Stock, Artus Corp., Englewood, N.J.). If it holds the shim stock the tooth is re-marked with the mylar marking film (either Accufilm II [Parkell Products, Inc., Farmingdale, N.Y.] or MOS II Truespot [MOS Products, Inc., Anaheim, Cal.]) and readjusted. If the shim stock pulls free and no other tooth contacts, another leaf is removed and the next prematurity is marked, adjusted, and retested in a similar fashion. This procedure is repeated until all of the posterior teeth hold shim stock uniformly, there is no longer any deflection upon closure, and all of the marks have migrated to the cusp tips and fossa bases with no marks on inclined planes. When these criteria have been satisfied, the equilibration is complete. As an additional test, 30 gauge Kerr's green casting wax can be used for further verification of the accuracy of the equilibration. To do this, two strips of wax are cut and are placed over the upper right and left posterior teeth. The patient closes on these strips which, after removal, are examined for tooth perforations. The Journal of Gnathology Vol. 6, No. 1,
6 Huffman A satisfactory equilibration is indicated when either multiple perforations made by all the cusps (or no perforations) are seen in both strips. In the absence of these two circumstances, the existence of only one perforation in either strip indicates that the equilibration is not yet complete. During the equilibration process, the patient's neuromuscular response is constantly being modified until, when the equilibration is complete, the dentist will have elicited a neuromuscular response which enables the patient to permit the dentist to forcefully and repeatedly close the mandible into centric relation closure without resistance. Once centric relation closure has been established and perfected, the dentist is ready to check for eccentric disclusion. Our technique organizes the ridge and groove directions for eccentric as we do the centric adjustments; therefore, additional adjustments are rarely required in the eccentric excursions. However, both working and balancing movements are checked using an operatorguided lateral movement similar to that used when making a pantographic recording. Adjustments are made as necessary (following the recommended technique). Occasionally, when canine disclusion cannot be established ideally as determined by the diagnostic equilibration, we may elect to build up the canines with acid etch composite to achieve disclusion. If this is the case we only equilibrate centric relation occlusion, add the acid etch composite to the canine (and/or anteriors), then check and adjust the eccentric relations as necessary. Clark and Adler discussed the various current philosophies of occlusal equilibration. 9 It shall not be the purpose of this paper to reiterate these concepts nor to argue their pros and cons. There are many published definitions of occlusal equilibration. 10 Each dental specialty offers its own unique definition. There seem to be as many definitions as there are authors. The periodontists make reference to the health and well being of the periodontium as part of their definitions. The members of the American Equilibration Society, whose interest lies in TMJ dysfunction, make reference to the health and stability of the temporomandibular joints and the normalization of function of the muscles of mastication by selective grinding of the teeth. The restorative dentists stress restoration of normal jaw function and stability of the occlusion as they define "occlusal equilibration." For purposes of this paper we shall use a more generalized definition: "Occlusal equilibration is the process of correcting stomatognathic dysfunction by recontouring tooth surfaces through selective grinding procedures." 10 28
7 A Cusp-fossa Equilibration Technique Using a Numbered Leaf Gauge Fig. 4. Enameling of cast diagram. QUADIWIT I QUADIWIT II QUADIWIT Ill QUAD&AllT IV The actual technique is described in detail in our manual 10 and wil I only be discussed briefly in this article. We use a modification of Guichet's "enameling of cast" exercise incorporated into our teaching of occlusal equilibration (Fig. 4).11 The marks represent three things: 1. Areas where articulating film marks would be located on opposing cusps if a particular type of prematurity were present. 2. Areas where facets of wear would be evident with such a prematurity. 3. Indications of the area to be analyzed for adjustment by selective grinding. Quadrant 1 (Cast I) represents the marks which would be made by articulating film on opposing teeth if a working type of centric prematurity was present. It also depicts areas of potential working side eccentric interferences. Quadrant 2 (Cast 11) represents the marks which would be made by articulating film on opposing teeth if a balancing type of centric prematurity was present. It also depicts areas of potential balancing eccentric interferences. Quadrant 3 (Cast 11) represents opposing premature articulating film marks if a centric prematurity exists resulting in a straight P.A. deflective slide, with no lateral slide. Quadrant 4 (Cast 11) represents opposing marks in protrusive excursions. We recommend diagnostic equilibration on accurately mounted casts before any intraoral procedures are performed. The patient should be free of pain and be neuromuscularly relaxed on bite- The Journal of Gnathology Vol. 6, No. 1,
8 Huffman plane therapy prior to mounting diagnostic casts. Opposing arch marks will be analyzed on the basis of the marks on the various quadrants of the enameling of cast. If a patient has a lateral component to the centric hit and slide, the marks will correspond to those found on either Quadrant 1 or 2. Any type of centric slide as well as any working or balancing eccentric interference involves marks on the distal inclines of the mandibular teeth and the mesial inclines of the maxillary teeth. Any type of working prematurity (Quadrant 1) either in centric or eccentric involves opposing marks on a centric cusp opposing a non-centric cusp, e.g. lower buccal cusp with upper buccal cusp or upper lingual cusp with lower lingual cusp. All working types of prematurities involve marks on the outer inclines of the centric cusps and the inner inclines of the noncentric or shearing cusps. Since we always adjust the centric cusp, only one of the teeth would be adjusted in this instance. Balancing types contact (Quadrant 2) in either centric or eccentric always involve contacts of a centric cusp against a centric cusp, e.g. mandibular buccal cusp vs. maxillary lingual cusp. Furthermore, these marks are always on the inner inclines of both cusps. Since we advocate adjusting centric cusps, both the mandibular and maxillary cusps must be adjusted in this situation. Dawson, in his text, recommends only adjusting one of the cusps in this situation and offers the operator the choice of either the mandibular or maxillary. 12 We will elaborate later why this option is inadequate. ANALYZING THE ARTICU- LATING FILM MARKS When adjusting an occlusion on diagnostic casts or in the patient's mouth, we use a mylar articulating film which marks on both sides so that we can see the mark on the mandibular and maxillary teeth which are in premature contact. These marks are analyzed on a cusp-to-fossa basis. The mark that appears on an inclined plane of the centric cusp (mandibular buccal or maxillary lingual) is analyzed to see what direction it would have to move to migrate to the tip of the anatomical cusp. When the opposing arch mark is analyzed, we find if its mark migrates in the same direction and magnitude it will place its mark over a fossa. We then adjust that pair of prematurities as described in the next section on how to adjust. HOW TO ADJUST We follow the basic ideas presented by Glickman in his text; namely, that of grooving, spheroiding, and pointing ( Fig. 5 a-f)
9
10 Huffman Fig. 5e. Spheroiding starts with a back and forth mesiodistal movement of the bur in two curved planes. The first curved plane of contour lies between the central ridge of the buccal surface of the cusp and the distobuccal developmental groove (the central ridge lies along the greatest vertical convexity of the outer surface of a cusp and extends cervically from the cusp tip). The second curved plane of contour lies between the central ridge and the mesiobuccal developmental groove. As the bur moves across these planes, it eliminates the flat planes of wear and recreates the spherical contours of the original tooth form. Fig. 5f. Pointing of the cusp is the end result of the combined grooving and spheroiding procedures. The cusp has been repositioned while surrounding surfaces have been reshaped, smoothed, and rounded. We adjust centric relation first and adjust only the centric holding cusps. The reason for adjusting centric first is that we teach undergraduate dental students and dentists in our postgraduate occlusion courses to perform a diagnostic equilibration on mounted casts prior to intraoral selective grinding. This mounting is made on a semiadjustable articulator, preferably a Whip-Mix model It is financially impractical to pantograph a patient, mount casts on a fully adjustable articulator, and program the instrument merely for purposes of a diagnostic equilibration. Since only centric relation is accurate on a semiadjustable articulator we would be in error to adjust eccentrics first. By using the leaf gauge, the patient's own neuromusculature seats the condyles in their tripodized centric relation position, making the equilibration more accurate if centric is done first. The potential of operator-induced mandibular guidance error is eliminated. Also, by using this technique, eccentric interferences, the most difficult to record, are essentially eliminated. The centric cusps are adjusted rather than the noncentric cusps because we desire to narrow the occlusal table during the occlusal equilibration. Examination of tooth morphology indicates that occlusal tables are narrowed by the inward curvature of the outer surfaces of the centric cusps, whose tips are "warped" towards 32

11

12
13 A Cusp-fossa Equilibration Technique Using a Numbered Leaf Gauge THE IDEAL OCCLUSION COMPROMISE We realize that the ideal gnathological occlusion involves tripodized jaw closure stops in which the cusp tips never touch anything, anytime, anywhere, and we insist on this criteria when restoring a mouth with waxing and casting procedures. However, it is impractical to arrive at tripodized occlusal stops during occlusal equilibration, which is only a subtractive procedure. Therefore, our occlusal stops are located on the cusp tips, which oppose fossa whenever possible or occasionally on flat areas of marginal ridges. There are three ways to unlock an occlusion or provide freedom of mandibular movement. One way, which is undesirable, is to provide perfectly flat cusp posterior teeth. Another way is the G nathological approach of tripodized jaw closure stops coupled with immediate canine disclusion. The Pankey-Mann-Schuyler concept, which uses the cusp tips as jaw closure stops, incorporates some slight 11 long" and "wide centric" as the mechanism to unlock the occlusion. We can eliminate or minimize any long or wide centric even though we have the cusp tips as the jaw closure stops by pointing the centric cusps, perfectly organizing the ridge and groove direction, and by coupling the anterior teeth, especially the canines for immediate disclusion. CONCLUSIONS Successful occlusal equilibration is based upon the patient being neuromuscularly relaxed and symptom-free by means of biteplane therapy. Since not everyone can be equilibrated, it is important to diagnostically equilibrate accurately mounted casts and to keep a sequential grinding list prior to attempting intraoral selective grinding. Permitting the patient's own neuromusculature to seat the condyles in their respective tripodized superior position using a leaf gauge, permits the inexperienced as well as the experienced operator to adjust to true centric relation occlusion. Using the cusp-fossa analysis of opposing premature marks permits the operator to satisfy the gnathological criteria of occlusion. By adjusting the centric holding cusps rather than the shearing cusps and applying the principles of grooving, spheroiding, and pointing, an enhanced tooth morphology is easily accomplished. As centric is adjusted in this manner, the ridge and groove direction is organized for the eccentric excursive jaw movements at the same time that centric relation is corrected. This eliminates or minimizes the necessity of adjusting working and balancing eccentric interferences, making the procedure more efficient. Using a small round-end fissure finishing bur permits easy enhancement of occlusal morphology and leaves a smooth surface, eliminating the necessity of additional polishing which could destroy the centric stops. The Journal of Gnathology Vol. 6, No. 1,
14 Huffman SUMMARY A logical, efficient occlusal equilibration technique has been presented which satisfies the gnathological principles of occlusion. The technique is feasible, practical, and can be mastered by the inexperienced as well as experienced operator. It is one method of occlusal therapy which effectively helps the signs and symptoms of a pathological occlusion. It constitutes the most economical form of occlusal therapy. It is the most foolproof form of occlusal therapy because it can all be done on diagnostic casts prior to attempting any intraoral irreversible procedures. The immediate and continued relief of symptoms experienced by patients makes them appreciate the dental profession. REFERENCES 1. Ramfjord, S.P., Ash, M.M.: Occlusion, ed. 3, Phil., W.B. Saunders Co., McCollum, 8.8., Stuart, C.: A research report, So. Pasadena, CA, Scientific Press, Long, J.H.: Locating centric relation with a leaf gauge, J. Prosthet. Dent, 29: , June Williamson, E.H., Steinke, R.M., Murse, P.K. and Swift, T.R.: Centric relation: A comparison of muscle-determined position and operator guidance. Am. J. Orthod. Vol. 77, , Feb Golsen, L.F., Shaw, A.F. : Use of leaf gauge in occlusal diagnosis and therapy. Quintessence Int., #6, June Shankland, W.E., Ralston, S.J.: The fabrication and use of a leaf gauge to locate centric relation. Ohio Dent. J., Vol. 57: 43-45, Rosenblum, R.H., Huffman, R.W.: A leaf gauge with consecutively numbered leaves. J. Prosthet. Dent. 54: , Nov McMillan, L.B.: Border movements of the human mandible. J. Prosthet. Dent., Vol. 27: , Clark, G.T., Adler, R.C.: A critical evaluation of occlusal therapy: occlusal adjustment procedures. J.A.D.A., Vol. 110: , May Huffman, R.W., Regenos, J.W.: Principles of Occlusion: A laboratory and clinical teaching manual, H&R Press, Columbus, OH., 1980 rev. ed. 11. Guichet, N.F.: Continuing education course, The Ohio State University, Dawson, P.E.: Evaluation, diagnosis, and treatment of occlusal problems, C.V. Mosby Co., St. Louis Glickman, I.: Clinical Periodontology, 4th ed., W.B. Saunders Co., Phila., PA, Dr. Richard W. Huffman 266 Luiseno Ave. Oceanside C.A U.S.A. 36
Occlusal rehabilitation of posterior fixed prostheses: A clinical report
 J Korean Acad Prosthodont : Volume 39, Number 3, 2001 Occlusal rehabilitation of posterior fixed prostheses: A clinical report In-Sung Yeo, DDS a, and Jae-Ho Yang, DDS, MSD, PhD b College of Dentistry,
J Korean Acad Prosthodont : Volume 39, Number 3, 2001 Occlusal rehabilitation of posterior fixed prostheses: A clinical report In-Sung Yeo, DDS a, and Jae-Ho Yang, DDS, MSD, PhD b College of Dentistry,
Concepts of occlusion Balanced occlusion. Monoplane occlusion. Lingualized occlusion. Figure (10-1)
") Any contact between teeth of opposing dental arches; usually, referring to contact between the occlusal surface. The static relationship between the incising or masticatory surfaces of the maxillary or
Any contact between teeth of opposing dental arches; usually, referring to contact between the occlusal surface. The static relationship between the incising or masticatory surfaces of the maxillary or
Restoring Severe Anterior Wear Cases; A Step by step Process
 0 Restoring Severe Anterior Wear Cases; Solving the Most Difficult Cases: A Step by Step Process" A Step by step Process Friday, February 6, 2015 Glenn E. DuPont, D.D.S. 1 The presence of worn dentition,
0 Restoring Severe Anterior Wear Cases; Solving the Most Difficult Cases: A Step by Step Process" A Step by step Process Friday, February 6, 2015 Glenn E. DuPont, D.D.S. 1 The presence of worn dentition,
A Systematic Approach for Rehabilitation of Occlusion in Fixed Partial Denture
 Rita Zarina et al Mini Review 10.5005/jp-journals-10052-0097 A Systematic Approach for Rehabilitation of Occlusion in Fixed Partial Denture 1 Rita Zarina, 2 JL Jaini, 3 Rajan S Raj ABSTRACT Long-term success
Rita Zarina et al Mini Review 10.5005/jp-journals-10052-0097 A Systematic Approach for Rehabilitation of Occlusion in Fixed Partial Denture 1 Rita Zarina, 2 JL Jaini, 3 Rajan S Raj ABSTRACT Long-term success
Dr Mohammed Alfarsi Page 1 9 December Principles of Occlusion
 Dr Mohammed Alfarsi Page 1 9 December 2013 Principles of Occlusion Overview: The occlusion is a very large, yet easy to manage once properly understood, topic. Thus, no one handout is enough to fully understand
Dr Mohammed Alfarsi Page 1 9 December 2013 Principles of Occlusion Overview: The occlusion is a very large, yet easy to manage once properly understood, topic. Thus, no one handout is enough to fully understand
Full-mouth rehabilitation of a patient with severe attrition using the Hobo twin-stage procedure
 Full-mouth rehabilitation of a patient with severe attrition using the Hobo twin-stage procedure Saurav Banerjee, Nabarun Chakraborty, Rajwinder Singh, Tapas Gupta Abstract Excessive occlusal wear can
Full-mouth rehabilitation of a patient with severe attrition using the Hobo twin-stage procedure Saurav Banerjee, Nabarun Chakraborty, Rajwinder Singh, Tapas Gupta Abstract Excessive occlusal wear can
OCCLUSION IN NEWLY FABRICATED BRIDGE*
 15 OCCLUSION IN NEWLY FABRICATED BRIDGE* (OKLUSI PADA GIGI TIRUAN JEMBATAN YANG BARU DIBUAT) Natasya Ahmad Tarib, Marlynda Ahmad Department of Prosthodontics, Faculty of Dentistry, University Kebangsaan
15 OCCLUSION IN NEWLY FABRICATED BRIDGE* (OKLUSI PADA GIGI TIRUAN JEMBATAN YANG BARU DIBUAT) Natasya Ahmad Tarib, Marlynda Ahmad Department of Prosthodontics, Faculty of Dentistry, University Kebangsaan
Arrangement of the artificial teeth:
 Lecture Prosthodontic Dr. Osama Arrangement of the artificial teeth: It s the placement of the teeth on a denture with definite objective in mind or it s the setting of teeth on temporary bases. Rules
Lecture Prosthodontic Dr. Osama Arrangement of the artificial teeth: It s the placement of the teeth on a denture with definite objective in mind or it s the setting of teeth on temporary bases. Rules
Implant and Tooth Supported Full-Mouth Rehabilitation with Hobo Twin-Stage Technique
 10.5005/JP-Journals-10012-1099 Koshika Tandon et al CASE REPORT Implant and Tooth Supported Full-Mouth Rehabilitation with Hobo Twin-Stage Technique Koshika Tandon, Ajay Singh, Himanshu Gupta, Rajdeep
10.5005/JP-Journals-10012-1099 Koshika Tandon et al CASE REPORT Implant and Tooth Supported Full-Mouth Rehabilitation with Hobo Twin-Stage Technique Koshika Tandon, Ajay Singh, Himanshu Gupta, Rajdeep
OCCLUSION. Principles & Treatment. José dos Santos, Jr, DDS, PhD. São Paulo, Brazil
 OCCLUSION Principles & Treatment José dos Santos, Jr, DDS, PhD São Paulo, Brazil Former Professor Division of Occlusion Department of Restorative Dentistry University of Texas Health Science Center at
OCCLUSION Principles & Treatment José dos Santos, Jr, DDS, PhD São Paulo, Brazil Former Professor Division of Occlusion Department of Restorative Dentistry University of Texas Health Science Center at
Jaw relation registration in RPD
 Jaw relation registration in RPD Why to Record the Jaw Relations? To establish and maintain a harmonious relationship with all oral structures and to provide a masticatory apparatus that is efficient and
Jaw relation registration in RPD Why to Record the Jaw Relations? To establish and maintain a harmonious relationship with all oral structures and to provide a masticatory apparatus that is efficient and
The Effect of the Central Bearing Plate Form on the Fischer Angle
 The Effect of the Central Bearing Plate Form on the Fischer Angle Yasuhiro Kamimura, D.D.S. Kobe City, Japan INTRODUCTION The Fischer angle, which has been defined as "the angle between the inclinations
The Effect of the Central Bearing Plate Form on the Fischer Angle Yasuhiro Kamimura, D.D.S. Kobe City, Japan INTRODUCTION The Fischer angle, which has been defined as "the angle between the inclinations
AN EVALUATION OF MANDIBULAR BORDER MOVEMENTS THEIR CHARACTER AND SIGNIFICANCE
 AN EVALUATION OF MANDIBULAR BORDER MOVEMENTS THEIR CHARACTER AND SIGNIFICANCE HARRY C. LUNDEEN, D.D.S. EDWIN F. SHRYOCK, D.D.S.,M.S. and CHARLES H. GIBBS, PhD. The University of Florida, College of Dentistry,
AN EVALUATION OF MANDIBULAR BORDER MOVEMENTS THEIR CHARACTER AND SIGNIFICANCE HARRY C. LUNDEEN, D.D.S. EDWIN F. SHRYOCK, D.D.S.,M.S. and CHARLES H. GIBBS, PhD. The University of Florida, College of Dentistry,
Full mouth occlusal rehabilitation; by Pankey Mann Schuyler philosophy
 Case Report DOI: 10.18231/2455-8486.2017.0006 Jinsa P. Devassy 1, Ankitha Sivadas 2, Shabas Muhammed 3 1 Consultant Prosthodontist, Ernakulam, Kerala, 2 Assistant Professor, 3 PG Student, Dept. of Prosthodontics,
Case Report DOI: 10.18231/2455-8486.2017.0006 Jinsa P. Devassy 1, Ankitha Sivadas 2, Shabas Muhammed 3 1 Consultant Prosthodontist, Ernakulam, Kerala, 2 Assistant Professor, 3 PG Student, Dept. of Prosthodontics,
Tooth preparation for posterior fi xed partial denture (FPD) Tooth preparation for anterior fi xed partial denture (FPD)
 Tooth preparation for anterior fi xed partial denture (FPD)") CHAPTER 17 Tooth preparation for posterior fi xed partial denture (FPD) 1 Defi nition and feature of FPD 2 Actual sequence of tooth preparation for posterior FPD Verify abutment teeth Occlusal guide groove
CHAPTER 17 Tooth preparation for posterior fi xed partial denture (FPD) 1 Defi nition and feature of FPD 2 Actual sequence of tooth preparation for posterior FPD Verify abutment teeth Occlusal guide groove
Occlusion & Prosthodontics
 Occlusion & Prosthodontics Occlusion and Prosthodontic Treatments Babak Shokati DDS, MSc. MSc. Candidate (Prosthodontics) Occlusion: A Controversial Issue Occlusion related issues and contradictory debates:
Occlusion & Prosthodontics Occlusion and Prosthodontic Treatments Babak Shokati DDS, MSc. MSc. Candidate (Prosthodontics) Occlusion: A Controversial Issue Occlusion related issues and contradictory debates:
Re-evaluation of the Condylar Path as the Reference for Occlusion
 Original Article Hobo et al - Re-evaluation of the Condylar Path 1 Re-evaluation of the Condylar Path as the Reference for Occlusion Sumiya Hobo, Hisao Takayama The condylar path is "the path traveled
Original Article Hobo et al - Re-evaluation of the Condylar Path 1 Re-evaluation of the Condylar Path as the Reference for Occlusion Sumiya Hobo, Hisao Takayama The condylar path is "the path traveled
AD2 MEASURES CONDYLE DISPLACEMENT (MCD) MANUAL
 MANUAL") AD2 MEASURES CONDYLE DISPLACEMENT (MCD) MANUAL Dr. Jorge Ayala Puente, DDS* Dr. Gonzalo Gutiérrez Álvarez, DDS* Dr. José Miguel Obach M., DDS Translation: Dr. Barbara Fernández Lübbert, DDS Edited: Dr.
AD2 MEASURES CONDYLE DISPLACEMENT (MCD) MANUAL Dr. Jorge Ayala Puente, DDS* Dr. Gonzalo Gutiérrez Álvarez, DDS* Dr. José Miguel Obach M., DDS Translation: Dr. Barbara Fernández Lübbert, DDS Edited: Dr.
Occlusion in complete denture
 Occlusion in complete denture Occlusion is a concept that is pertinent to all dental patients wheather they have their own teeth or not.it is a term used to describe the contact relationship between the
Occlusion in complete denture Occlusion is a concept that is pertinent to all dental patients wheather they have their own teeth or not.it is a term used to describe the contact relationship between the
ALTERNATE OCCLUSAL SCHEMES
 ALTERNATE OCCLUSAL SCHEMES The same basic concepts need to be applied to all occlusal schemes. Some challenges include missing teeth, transposed teeth, crossbites, and anterior open bites. POSTERIOR CROSSBITES
ALTERNATE OCCLUSAL SCHEMES The same basic concepts need to be applied to all occlusal schemes. Some challenges include missing teeth, transposed teeth, crossbites, and anterior open bites. POSTERIOR CROSSBITES
Arrangement of posterior artificial teeth Standardized parameters Curve of Wilson Curve of Spee
 . Arrangement of posterior artificial teeth Posterior teeth are set up in tight centric occlusion. The mandibular teeth are set in the wax occlusion rim over the residual ridge in their ideal buccolingual
. Arrangement of posterior artificial teeth Posterior teeth are set up in tight centric occlusion. The mandibular teeth are set in the wax occlusion rim over the residual ridge in their ideal buccolingual
Splint Appliance. Selection Guide. Great Lakes. See inside...
 Great Lakes Splint Appliance Selection Guide This guide includes helpful tips on how to choose the right splint for your patient and information on standard function and specifications for Great Lakes
Great Lakes Splint Appliance Selection Guide This guide includes helpful tips on how to choose the right splint for your patient and information on standard function and specifications for Great Lakes
Principle of Occlusion
 Principle of Occlusion Mohammed Alfarsi BDS, MDSc(Pros), PhD www.drmohdalfarsi.com com.+*()ا&%$ر"!. www Overview Principle of Occlusion Overview Principle of Occlusion Point centric Long centric Freedom
Principle of Occlusion Mohammed Alfarsi BDS, MDSc(Pros), PhD www.drmohdalfarsi.com com.+*()ا&%$ر"!. www Overview Principle of Occlusion Overview Principle of Occlusion Point centric Long centric Freedom
The De Vreugd Occlusal Compass
 The De Vreugd Occlusal Compass A Guide to Creating Functional Morphology in Wax Each color on the DeVreugd Occlusal Compass represents directions in which the mandibular buccal cusps travel during chewing
The De Vreugd Occlusal Compass A Guide to Creating Functional Morphology in Wax Each color on the DeVreugd Occlusal Compass represents directions in which the mandibular buccal cusps travel during chewing
Symposium on Occlusal Articulation. Mandibular Movement Recordings and Articulator Adjustments Simplified. Harry C. Lundeen, D.D.S.
 Symposium on Occlusal Articulation Mandibular Movement Recordings and Articulator Adjustments Simplified Harry C. Lundeen, D.D.S. Judging from the volume of writing that has appeared in the dental literature
Symposium on Occlusal Articulation Mandibular Movement Recordings and Articulator Adjustments Simplified Harry C. Lundeen, D.D.S. Judging from the volume of writing that has appeared in the dental literature
أ.م. هدى عباس عبد اهلل CROWN AND BRIDGE جامعة تكريت كلية. Lec. (2) طب االسنان
 طب االسنان") Lec. (2) CROWN AND BRIDGE أ.م. هدى عباس عبد اهلل Patient selection and examination A thorough diagnosis must first be made of the patient's dental condition, considering both hard and soft tissues. this
Lec. (2) CROWN AND BRIDGE أ.م. هدى عباس عبد اهلل Patient selection and examination A thorough diagnosis must first be made of the patient's dental condition, considering both hard and soft tissues. this
Surveying. 3rd year / College of Dentistry/University of Baghdad ( ) Page 1
 Page 1") د. فائزة Lec.3 Prosthodontics Surveying The ideal requirements for successful removable partial denture are: 1. Be easily inserted and removed by the patient. 2. Resist dislodging forces. 3. It should
د. فائزة Lec.3 Prosthodontics Surveying The ideal requirements for successful removable partial denture are: 1. Be easily inserted and removed by the patient. 2. Resist dislodging forces. 3. It should
Shadeguides Finding the Centric Relation The Kois Deprogrammer
 Maciej Zarow Shadeguides Finding the Centric Relation The Kois Deprogrammer 21 Jun 2018 Finding the centric relation might sometimes seem hard, but with appropriate devices, such as the Kois Deprogrammer
Maciej Zarow Shadeguides Finding the Centric Relation The Kois Deprogrammer 21 Jun 2018 Finding the centric relation might sometimes seem hard, but with appropriate devices, such as the Kois Deprogrammer
ANTERIOR OPEN BITE AS A COMPLICATION OF THE TREATMENT OF BRUXISM WITH ANTERIOR BITE PLANE: A CASE REPORT
 CLINICAL DENTISTRY AND RESEARCH 2011; 35(3): 53-58 ANTERIOR OPEN BITE AS A COMPLICATION OF THE TREATMENT OF BRUXISM WITH ANTERIOR BITE PLANE: A CASE REPORT Gülay Uzun, DDS, PhD Professor, School of Dental
CLINICAL DENTISTRY AND RESEARCH 2011; 35(3): 53-58 ANTERIOR OPEN BITE AS A COMPLICATION OF THE TREATMENT OF BRUXISM WITH ANTERIOR BITE PLANE: A CASE REPORT Gülay Uzun, DDS, PhD Professor, School of Dental
Horizontal jaw relations: The relationship of mandible to maxilla in a
 Horizontal relations Horizontal jaw relations: The relationship of mandible to maxilla in a horizontal plane (in anteroposterior and side to side direction). a- Protruded or forward relation. b-lateral
Horizontal relations Horizontal jaw relations: The relationship of mandible to maxilla in a horizontal plane (in anteroposterior and side to side direction). a- Protruded or forward relation. b-lateral
Using the Lucia Jig to take an accurate & reliable centric relation bite registration
 Trimming Instructions Trimming the silicone bite records is an important step to ensure an accurate fit on the model. Trimming eliminates all the interferences so there is no movement once the models are
Trimming Instructions Trimming the silicone bite records is an important step to ensure an accurate fit on the model. Trimming eliminates all the interferences so there is no movement once the models are
Basic Concept in Full Mouth Rehabilitation An Overview
 Basic Concept in Full Mouth Rehabilitation An Overview Dr Ankush Jain*,Dr Umesh Palekar**, Dr Rajeev Srivastava***, Dr Vivek Choukse*** ABSTRACT: Full mouth rehabilitation continues to be the biggest challenge
Basic Concept in Full Mouth Rehabilitation An Overview Dr Ankush Jain*,Dr Umesh Palekar**, Dr Rajeev Srivastava***, Dr Vivek Choukse*** ABSTRACT: Full mouth rehabilitation continues to be the biggest challenge
Dzakovich Conclusions
 Definitions Attrition Tooth wear resulting from contact between opposing teeth. Erosion A gradual tooth-surface loss process caused by an electrolytic or chemical mechanism without bacteria being involved.
Definitions Attrition Tooth wear resulting from contact between opposing teeth. Erosion A gradual tooth-surface loss process caused by an electrolytic or chemical mechanism without bacteria being involved.
TOOTH SELECTION & ARRANGEMENT IN REMOVABLRE PARTIAL DENTURE
 TOOTH SELECTION & ARRANGEMENT IN REMOVABLRE PARTIAL DENTURE DR ZURYATI AB GHANI BDS (WALES), Grad Dip Clin Dent (Adelaide), Doctor in Clinical Dentistry (prosthodontics( prosthodontics), Adelaide, FRACDS
TOOTH SELECTION & ARRANGEMENT IN REMOVABLRE PARTIAL DENTURE DR ZURYATI AB GHANI BDS (WALES), Grad Dip Clin Dent (Adelaide), Doctor in Clinical Dentistry (prosthodontics( prosthodontics), Adelaide, FRACDS
Chicago Midwinter Meeting February 21, Staging Complex Restorative Cases Putting things into the proper order
 Chicago Midwinter Meeting February 21, 2019 Staging Complex Restorative Cases Putting things into the proper order Thomas R. McDonald, D.M.D. tmcdent@aol.com 1 COMPREHENSIVE PATIENT EVALUATION PATIENT
Chicago Midwinter Meeting February 21, 2019 Staging Complex Restorative Cases Putting things into the proper order Thomas R. McDonald, D.M.D. tmcdent@aol.com 1 COMPREHENSIVE PATIENT EVALUATION PATIENT
Full mouth rehabilitation of a patient with enamel hypoplasia using hobo s twin-tables technique for occlusal rehabilitation-a case Report
 J. Adv Oral Research Case Report All Rights Res Full mouth rehabilitation of a patient with enamel hypoplasia using hobo s twin-tables technique for occlusal rehabilitation-a case Report Hemal S. Agrawal
J. Adv Oral Research Case Report All Rights Res Full mouth rehabilitation of a patient with enamel hypoplasia using hobo s twin-tables technique for occlusal rehabilitation-a case Report Hemal S. Agrawal
OCCLUSION: PHYSIOLOGIC vs. NON-PHYSIOLOGIC
 Oral Anatomy and Occlusion Prosthodontic Component OCCLUSION: PHYSIOLOGIC vs. NON-PHYSIOLOGIC By: Dr. Babak Shokati, DDS, MSc. MSc. Prosthodontics Definition of Masticatory System by The Academy of Prosthodontics
Oral Anatomy and Occlusion Prosthodontic Component OCCLUSION: PHYSIOLOGIC vs. NON-PHYSIOLOGIC By: Dr. Babak Shokati, DDS, MSc. MSc. Prosthodontics Definition of Masticatory System by The Academy of Prosthodontics
Case report: Lingualized occlusion -A better way for enhancing function & esthetic
 Case report: Lingualized occlusion -A better way for enhancing function & esthetic 1Dr. Vishrut Shah, 2 Dr. Sunil Dhaded, 3 Dr. Chandrashekar Sajjan 1Post graduate student, Department of Prosthodontics,
Case report: Lingualized occlusion -A better way for enhancing function & esthetic 1Dr. Vishrut Shah, 2 Dr. Sunil Dhaded, 3 Dr. Chandrashekar Sajjan 1Post graduate student, Department of Prosthodontics,
INSIGHT & INNOVATION. Envelope of Parafunction: 7 Steps of Treatment Planning Many methods and theories have been
 Envelope of Parafunction: 7 Steps of Treatment Planning Many methods and theories have been employed in regard to treatment planning and correct restorative sequence. Assuming that the patient has healthy
Envelope of Parafunction: 7 Steps of Treatment Planning Many methods and theories have been employed in regard to treatment planning and correct restorative sequence. Assuming that the patient has healthy
Horizontal Jaw Relation
 Horizontal Jaw Relation Horizontal Jaw Relation It is the relationship of the mandible to the maxilla in a horizontal plane. It can also be described as the relationship of the mandible to the maxilla
Horizontal Jaw Relation Horizontal Jaw Relation It is the relationship of the mandible to the maxilla in a horizontal plane. It can also be described as the relationship of the mandible to the maxilla
See the end from the beginning
 Staub Cranial See the end from the beginning with Staub Cranial Recently a new technology was introduced to the United States that will revolutionize the way our industry restores teeth. The Staub Cranial
Staub Cranial See the end from the beginning with Staub Cranial Recently a new technology was introduced to the United States that will revolutionize the way our industry restores teeth. The Staub Cranial
Morphology of an Anatomic Crown. By: Assistant Professor Dr. Baydaa Ali Al - Rawi
 Morphology of an Anatomic Crown By: Assistant Professor Dr. Baydaa Ali Al - Rawi October 4, 2009 Elevated landmarks Depressed landmarks A) Elevated landmarks : 1. Dental lobe : is one of the primary centers
Morphology of an Anatomic Crown By: Assistant Professor Dr. Baydaa Ali Al - Rawi October 4, 2009 Elevated landmarks Depressed landmarks A) Elevated landmarks : 1. Dental lobe : is one of the primary centers
Prosthetic Options in Implant Dentistry. Hakimeh Siadat, DDS, MSc Associate Professor
 Prosthetic Options in Dentistry Hakimeh Siadat, DDS, MSc Associate Professor Dental Research Center, Department of Prosthodontics & Dental s Faculty of Dentistry, Tehran University of Medical Sciences
Prosthetic Options in Dentistry Hakimeh Siadat, DDS, MSc Associate Professor Dental Research Center, Department of Prosthodontics & Dental s Faculty of Dentistry, Tehran University of Medical Sciences
Muscles of mastication [part 1]
![Muscles of mastication [part 1]](/thumbs/76/73586850.jpg "Muscles of mastication [part 1]") Muscles of mastication [part 1] In this lecture well have the muscles of mastication, neuromuscular function, and its relationship to the occlusion morphology. The fourth determinant of occlusion is the
Muscles of mastication [part 1] In this lecture well have the muscles of mastication, neuromuscular function, and its relationship to the occlusion morphology. The fourth determinant of occlusion is the
Fundamental & Preventive Curvatures of Teeth and Tooth Development. Lecture Three Chapter 15 Continued; Chapter 6 (parts) Dr. Margaret L.
 Dr. Margaret L.") Fundamental & Preventive Curvatures of Teeth and Tooth Development Lecture Three Chapter 15 Continued; Chapter 6 (parts) Dr. Margaret L. Dennis Proximal contact areas Contact areas are on the mesial and
Fundamental & Preventive Curvatures of Teeth and Tooth Development Lecture Three Chapter 15 Continued; Chapter 6 (parts) Dr. Margaret L. Dennis Proximal contact areas Contact areas are on the mesial and
Complex Occlusal Rehabilitation: A Case Report
 Complex Occlusal Rehabilitation: A Case Report DR. ALI TUNKIWALA INTRODUCTION The most difficult problems in clinical practice are those where there is interaction of various pathogenic factors with consequent
Complex Occlusal Rehabilitation: A Case Report DR. ALI TUNKIWALA INTRODUCTION The most difficult problems in clinical practice are those where there is interaction of various pathogenic factors with consequent
You. Fix. Could. This? Treatment solutions for typical and atypical adult relapse. 78 SEPTEMBER 2017 // orthotown.com
 by Dan Grob, DDS, MS, editorial director, Orthotown magazine You Could Fix This? Treatment solutions for typical and atypical adult relapse 78 SEPTEMBER 2017 // orthotown.com OT0917_Mechanics_AG.indd 78
by Dan Grob, DDS, MS, editorial director, Orthotown magazine You Could Fix This? Treatment solutions for typical and atypical adult relapse 78 SEPTEMBER 2017 // orthotown.com OT0917_Mechanics_AG.indd 78
Linear Occlusion. By Dr. John P. Frush
 Linear Occlusion By Dr. John P. Frush Doctor Frush graduated from the University of Southern California in 1935 and has a private practice in San Marino, California. He is a member of the American Prosthodontic
Linear Occlusion By Dr. John P. Frush Doctor Frush graduated from the University of Southern California in 1935 and has a private practice in San Marino, California. He is a member of the American Prosthodontic
Aesthetic and functional restoration of the severely worn dentition
 A SYSTEMATIC APPROACH TO FULL-MOUTH RECONSTRUCTION OF THE SEVERELY WORN DENTITION JAY LERNER Aesthetic and functional restoration of the severely worn dentition represents a significant clinical challenge.
A SYSTEMATIC APPROACH TO FULL-MOUTH RECONSTRUCTION OF THE SEVERELY WORN DENTITION JAY LERNER Aesthetic and functional restoration of the severely worn dentition represents a significant clinical challenge.
For many years, patients with
 Dr. Robert Lowe is one of the great teachers in dentistry. Recently, he received the Gordon J. Christensen Award from the Chicago Dental Society in recognition of his excellence in teaching. Some of my
Dr. Robert Lowe is one of the great teachers in dentistry. Recently, he received the Gordon J. Christensen Award from the Chicago Dental Society in recognition of his excellence in teaching. Some of my
DR. PETER DAWSON S PHILOSOPHY OF FUNCTIONAL OCCLUSION
 DR. PETER DAWSON S PHILOSOPHY OF FUNCTIONAL OCCLUSION WHO IS PETER DAWSON? WHO IS PETER DAWSON? Peter Dawson is a dentist that specializes in the treatment of the exposed exterior surfaces of the teeth.
DR. PETER DAWSON S PHILOSOPHY OF FUNCTIONAL OCCLUSION WHO IS PETER DAWSON? WHO IS PETER DAWSON? Peter Dawson is a dentist that specializes in the treatment of the exposed exterior surfaces of the teeth.
529-A Treatment and Management of the Edentulous Patient. Upon completion of this course the student should be able to:
 Course & Title: Session & Topic: 529-A Treatment and Management of the Edentulous Patient Jaw Relations General Goal: To understand the principles of orientational, horizontal and vertical jaw relations
Course & Title: Session & Topic: 529-A Treatment and Management of the Edentulous Patient Jaw Relations General Goal: To understand the principles of orientational, horizontal and vertical jaw relations
A CLASSIFICATION SYSTEM FOR THE MANAGEMENT OF BIOMECHANICAL FACTORS IN DENTISTRY
 A CLASSIFICATION SYSTEM FOR THE MANAGEMENT OF BIOMECHANICAL FACTORS IN DENTISTRY I. INTRODUCTION Virtually all Masticatory System structural breakdowns are a result of either microbial or biomechanical
A CLASSIFICATION SYSTEM FOR THE MANAGEMENT OF BIOMECHANICAL FACTORS IN DENTISTRY I. INTRODUCTION Virtually all Masticatory System structural breakdowns are a result of either microbial or biomechanical
Clinical Management of Tooth Size Discrepanciesjerd_
 Clinical Management of Tooth Size Discrepanciesjerd_520 155..159 Guest Experts DN GRUER, DDS, PhD* GVIN C. HEYMNN, DDS, MS ssociate Editor EDWRD J. SWIFT, JR., DMD, MS Esthetic anterior dental appearance
Clinical Management of Tooth Size Discrepanciesjerd_520 155..159 Guest Experts DN GRUER, DDS, PhD* GVIN C. HEYMNN, DDS, MS ssociate Editor EDWRD J. SWIFT, JR., DMD, MS Esthetic anterior dental appearance
A Comparative Evaluation of Static and Functional Methods for Recording Centric Relation and Condylar Guidance: A Clinical Study
 J Indian Prosthodont Soc (July-Sept 2012) 12(3):175 181 DOI 10.1007/s13191-012-0154-5 ORIGINAL ARTICLE A Comparative Evaluation of Static and Functional Methods for Recording Centric Relation and Condylar
J Indian Prosthodont Soc (July-Sept 2012) 12(3):175 181 DOI 10.1007/s13191-012-0154-5 ORIGINAL ARTICLE A Comparative Evaluation of Static and Functional Methods for Recording Centric Relation and Condylar
MBT System as the 3rd Generation Programmed and Preadjusted Appliance System (PPAS) by Masatada Koga, D.D.S., Ph.D
 by Masatada Koga, D.D.S., Ph.D") MBT System as the 3rd Generation Programmed and Preadjusted Appliance System (PPAS) by Masatada Koga, D.D.S., Ph.D Dr. Masatada Koga, D.D.S., Ph.D, is an assistant professor in the Department of Orthodontics
MBT System as the 3rd Generation Programmed and Preadjusted Appliance System (PPAS) by Masatada Koga, D.D.S., Ph.D Dr. Masatada Koga, D.D.S., Ph.D, is an assistant professor in the Department of Orthodontics
An Investigation into Condylar Position with Leaf Gauge and Bimanual Manipulation
 An Investigation into Condylar Position with Leaf Gauge and Bimanual Manipulation Donald H. Downs, D.D.S. Colorado Springs, CO. U.S.A. INTRODUCTION The information derived from th is study is worth serious
An Investigation into Condylar Position with Leaf Gauge and Bimanual Manipulation Donald H. Downs, D.D.S. Colorado Springs, CO. U.S.A. INTRODUCTION The information derived from th is study is worth serious
THE MBT VERSATILE+ APPLIANCE SYSTEM
 THE MBT VERSATILE+ APPLIANCE SYSTEM McLaughlin, Bennett, Trevisi The MBT Versatile+ Appliance System THE DEVELOPMENT OF A TREATMENT MECHANICS AND APPLIANCE PHILOSOPHY The first fully programmed preadjusted
THE MBT VERSATILE+ APPLIANCE SYSTEM McLaughlin, Bennett, Trevisi The MBT Versatile+ Appliance System THE DEVELOPMENT OF A TREATMENT MECHANICS AND APPLIANCE PHILOSOPHY The first fully programmed preadjusted
BOCL-01: Bonding Materials Checklist
 Task 19: Gather materials to bond partner using toothpaste as etchant Take a photo of gathered materials and submit with this completed checklist BOCL-01: Bonding Materials Checklist Date: Patient: Operator:
Task 19: Gather materials to bond partner using toothpaste as etchant Take a photo of gathered materials and submit with this completed checklist BOCL-01: Bonding Materials Checklist Date: Patient: Operator:
Significant improvement with limited orthodontics anterior crossbite in an adult patient
 VARIA Significant improvement with limited orthodontics anterior crossbite in an adult patient Arzu Ari-Demirkaya Istanbul, Turkey Summary Objectives. Orthodontic treatment is known to last as long as
VARIA Significant improvement with limited orthodontics anterior crossbite in an adult patient Arzu Ari-Demirkaya Istanbul, Turkey Summary Objectives. Orthodontic treatment is known to last as long as
Combi ArtiCulAtor SyStem instruction manual
 Denar Combi Articulator System instruction manual table of contents I. Rationale for Development... 2 II. Benefits and Features... 3 III. Set Path Condylar Insert... 5 IV. Adjustable Path Condylar Insert...
Denar Combi Articulator System instruction manual table of contents I. Rationale for Development... 2 II. Benefits and Features... 3 III. Set Path Condylar Insert... 5 IV. Adjustable Path Condylar Insert...
Occlusion and removable prosthodontics
 12 Occlusion and removable prosthodontics R. Jagger Synopsis Occlusal considerations for removable prostheses are essentially the same as for fixed restorations. The approach to establishing occlusion
12 Occlusion and removable prosthodontics R. Jagger Synopsis Occlusal considerations for removable prostheses are essentially the same as for fixed restorations. The approach to establishing occlusion
The width of the MCXL step bur is 1.4 mm wide and has a blunt end. As the bur approaches the inside of
 As I teach first year dental students how to prep a tooth for a full gold crown, get an impression, pour and mount models, wax-up, cast and polish, they are almost always amazed at all the required steps
As I teach first year dental students how to prep a tooth for a full gold crown, get an impression, pour and mount models, wax-up, cast and polish, they are almost always amazed at all the required steps
Case Report Use of Zirconia to Restore Severely Worn Dentition: A Case Report
 Volume 2012, Article ID 324597, 4 pages doi:10.1155/2012/324597 Case Report Use of Zirconia to Restore Severely Worn Dentition: A Case Report Manish Agrawal, 1 Banashree Sankeshwari, 1 and Channaveer V.
Volume 2012, Article ID 324597, 4 pages doi:10.1155/2012/324597 Case Report Use of Zirconia to Restore Severely Worn Dentition: A Case Report Manish Agrawal, 1 Banashree Sankeshwari, 1 and Channaveer V.
Introduction to Occlusion and Mechanics of Mandibular Movement
 Introduction to Occlusion and Mechanics of Mandibular Movement Dr. Pauline Hayes Garrett Department of Endodontics, Prosthodontics, and Operative Dentistry University of Maryland, Baltimore Assigned reading
Introduction to Occlusion and Mechanics of Mandibular Movement Dr. Pauline Hayes Garrett Department of Endodontics, Prosthodontics, and Operative Dentistry University of Maryland, Baltimore Assigned reading
CPR for Complex Dental Treatment; From Concept, to Prototype, to Restoration
 Reality or Resin; Free Hand Artistry with Anterior Bonding Dennis B. Hartlieb, DDS CPR for Complex Dental Treatment; From Concept, to Prototype, to Restoration Wish List: 1. Reversible (no prep/ minimal
Reality or Resin; Free Hand Artistry with Anterior Bonding Dennis B. Hartlieb, DDS CPR for Complex Dental Treatment; From Concept, to Prototype, to Restoration Wish List: 1. Reversible (no prep/ minimal
How to provide intraoral scans to SomnoMed for the production of SomnoDent device.
 How to provide intraoral scans to SomnoMed for the production of SomnoDent device. KEY QUESTIONS: 1. Where do I send my Case? Send intra-oral scan files (maxilla and mandible in protrusive bite) and an
How to provide intraoral scans to SomnoMed for the production of SomnoDent device. KEY QUESTIONS: 1. Where do I send my Case? Send intra-oral scan files (maxilla and mandible in protrusive bite) and an
Checklist with summary points
 Checklist with summary points Question 1: Are your doctor Invisalign preferences on your home page up to date? Go to your doctor home page and open up your doctor preferences pages. Be sure to update item
Checklist with summary points Question 1: Are your doctor Invisalign preferences on your home page up to date? Go to your doctor home page and open up your doctor preferences pages. Be sure to update item
CLEAR, THIN, & STRONG
 CLEAR, THIN, & STRONG making bite splints successful through effective design Elizabeth D. Caughey, DDS Pankey Institute Visiting Faculty from Atlanta, GA Summer 2015 START WITH THE GOAL visualize a smooth,
CLEAR, THIN, & STRONG making bite splints successful through effective design Elizabeth D. Caughey, DDS Pankey Institute Visiting Faculty from Atlanta, GA Summer 2015 START WITH THE GOAL visualize a smooth,
6610 NE 181st Street, Suite #1, Kenmore, WA
 660 NE 8st Street, Suite #, Kenmore, WA 9808 www.northshoredentalacademy.com.08.900 READ CHAPTER The Professional Dental Assistant (p.-9) No Key Terms Recall Questions:,,,, and 6 CLASS SYLLABUS DAY READ
660 NE 8st Street, Suite #, Kenmore, WA 9808 www.northshoredentalacademy.com.08.900 READ CHAPTER The Professional Dental Assistant (p.-9) No Key Terms Recall Questions:,,,, and 6 CLASS SYLLABUS DAY READ
Case Report: Long-Term Outcome of Class II Division 1 Malocclusion Treated with Rapid Palatal Expansion and Cervical Traction
 Case Report Case Report: Long-Term Outcome of Class II Division 1 Malocclusion Treated with Rapid Palatal Expansion and Cervical Traction Roberto M. A. Lima, DDS a ; Anna Leticia Lima, DDS b Abstract:
Case Report Case Report: Long-Term Outcome of Class II Division 1 Malocclusion Treated with Rapid Palatal Expansion and Cervical Traction Roberto M. A. Lima, DDS a ; Anna Leticia Lima, DDS b Abstract:
Nature of Contacts in Centric Occlusion in 32 Adults
 Nature of Contacts in Centric Occlusion in 32 Adults J. RUSSELL ANDERSON, JR. and GEORGE E. MYERS Crown and Bridge Department, University of Michigan School of Dentistry, Ann Arbor, Michigan 4814, USA
Nature of Contacts in Centric Occlusion in 32 Adults J. RUSSELL ANDERSON, JR. and GEORGE E. MYERS Crown and Bridge Department, University of Michigan School of Dentistry, Ann Arbor, Michigan 4814, USA
Lec. 3-4 Dr. Saif Alarab Clinical Technique for Class I Amalgam Restorations The outline form
 Lec. 3-4 Dr. Saif Alarab Clinical Technique for Class I Amalgam Restorations Class I refers to -Restorations on the occlusal surfaces of posterior teeth, - The occlusal two thirds of facial and lingual
Lec. 3-4 Dr. Saif Alarab Clinical Technique for Class I Amalgam Restorations Class I refers to -Restorations on the occlusal surfaces of posterior teeth, - The occlusal two thirds of facial and lingual
Fixed Partial Denture
 University of Minnesota School of Dentistry Fixed Partial Denture Self-guided Instructional Material for Dental Students Authors Ranier M. Adarve, DMD, MS, MHPE Lisa Fedor James, DDS, Cert. Pros. Fixed
University of Minnesota School of Dentistry Fixed Partial Denture Self-guided Instructional Material for Dental Students Authors Ranier M. Adarve, DMD, MS, MHPE Lisa Fedor James, DDS, Cert. Pros. Fixed
Nine Steps To Occlusal Harmony
 Nine Steps To Occlusal Harmony Dr. Ali Tunkiwala has graduated from Nair Hospital Dental College in 1996 & completed his Masters Degree in Prosthetic Dentistry from Mumbai University (GDC, Mumbai) in 1998.
Nine Steps To Occlusal Harmony Dr. Ali Tunkiwala has graduated from Nair Hospital Dental College in 1996 & completed his Masters Degree in Prosthetic Dentistry from Mumbai University (GDC, Mumbai) in 1998.
PREDICTABILITY IN COMPREHENSIVE RECONSTRUCTION Bite registration and recovery process for comprehensive reconstructive cases.
 PREDICTABILITY IN COMPREHENSIVE RECONSTRUCTION Bite registration and recovery process for comprehensive reconstructive cases. By Matt Roberts The most predictable comprehensive restorative techniques revolve
PREDICTABILITY IN COMPREHENSIVE RECONSTRUCTION Bite registration and recovery process for comprehensive reconstructive cases. By Matt Roberts The most predictable comprehensive restorative techniques revolve
Annals and Essences of Dentistry
 doi:10.5368/aedj.2013.5.4.3.1 DEVELOPMENT OF HARMONIOUS OCCLUSION FOR COMPLETE DENTURE PATIENT USING FUNCTIONALLY GENERATED PATH TECHNIQUE- A CASE REPORT 1 Ravi Rakesh Dev J 2 swetha Hima Bindu O 3 Aparna
doi:10.5368/aedj.2013.5.4.3.1 DEVELOPMENT OF HARMONIOUS OCCLUSION FOR COMPLETE DENTURE PATIENT USING FUNCTIONALLY GENERATED PATH TECHNIQUE- A CASE REPORT 1 Ravi Rakesh Dev J 2 swetha Hima Bindu O 3 Aparna
Central Incisor DR.Ahmed Al-Jobory B.D.S.,M.Sc. Conservative Department
 Dental Anatomy Lecture 3 Central Incisor DR.Ahmed Al-Jobory B.D.S.,M.Sc. Conservative Department The permanent maxillary Incisors Maxillary incisor are four in number. The maxillary central incisor is
Dental Anatomy Lecture 3 Central Incisor DR.Ahmed Al-Jobory B.D.S.,M.Sc. Conservative Department The permanent maxillary Incisors Maxillary incisor are four in number. The maxillary central incisor is
Bone Reduction Surgical Guide for the Novum Implant Procedure: Technical Note
 Bone Reduction Surgical Guide for the Novum Implant Procedure: Technical Note Stephen M. Parel, DDS 1 /Steven L. Ruff, CDT 2 /R. Gilbert Triplett, DDS, PhD 3 /Sterling R. Schow, DMD 4 The Novum System
Bone Reduction Surgical Guide for the Novum Implant Procedure: Technical Note Stephen M. Parel, DDS 1 /Steven L. Ruff, CDT 2 /R. Gilbert Triplett, DDS, PhD 3 /Sterling R. Schow, DMD 4 The Novum System
Gnathology and Pankey-Mann-Schuyler : fulfilling the requirements of occlusion in oral rehabilitation
 The University of Toledo The University of Toledo Digital Repository Master s and Doctoral Projects Gnathology and Pankey-Mann-Schuyler : fulfilling the requirements of occlusion in oral rehabilitation
The University of Toledo The University of Toledo Digital Repository Master s and Doctoral Projects Gnathology and Pankey-Mann-Schuyler : fulfilling the requirements of occlusion in oral rehabilitation
Deprogrammers made. Deprogrammers can be used for... How do deprogrammers work?
 Deprogrammers made asy Easy Deprogrammers made Deprogrammers can be used for... Headache sufferers Bruxers and/or clenchers Muscle relaxation Determining proper joint position Protection against wear Diagnosis
Deprogrammers made asy Easy Deprogrammers made Deprogrammers can be used for... Headache sufferers Bruxers and/or clenchers Muscle relaxation Determining proper joint position Protection against wear Diagnosis
SECTION I PART A INTRODUCTION TO THE STUDY OF OCCLUSION
 I - A - 1 SECTION I PART A INTRODUCTION TO THE STUDY OF OCCLUSION INTRODUCTION Occlusion is the key to oral function and subsequently the key to restorative oral diagnosis. In spite of this, occlusion
I - A - 1 SECTION I PART A INTRODUCTION TO THE STUDY OF OCCLUSION INTRODUCTION Occlusion is the key to oral function and subsequently the key to restorative oral diagnosis. In spite of this, occlusion
SURVEYING OF REMOVABLE PARITAL DENTURES FEB, 11, 2015
 SURVEYING OF REMOVABLE PARITAL DENTURES FEB, 11, 2015 Dental Surveyor: It is a mechanical device used to determine the relative parallelism of the teeth surfaces and the undercuts areas in relation to
SURVEYING OF REMOVABLE PARITAL DENTURES FEB, 11, 2015 Dental Surveyor: It is a mechanical device used to determine the relative parallelism of the teeth surfaces and the undercuts areas in relation to
Attachment G. Orthodontic Criteria Index Form Comprehensive D8080. ABBREVIATIONS CRITERIA for Permanent Dentition YES NO
 First Review IL HFS Dental Program Models Second Review Ortho cad Attachment G Orthodontic Criteria Index Form Comprehensive D8080 Ceph Film X-Rays Photos Narrative Patient Name: DOB: ABBREVIATIONS CRITERIA
First Review IL HFS Dental Program Models Second Review Ortho cad Attachment G Orthodontic Criteria Index Form Comprehensive D8080 Ceph Film X-Rays Photos Narrative Patient Name: DOB: ABBREVIATIONS CRITERIA
Parafunction poses a risk for any. Predictable Esthetics through Functional Design: The Role of Harmonious Disclusion
 Predictable Esthetics through Functional Design: The Role of Harmonious Disclusion BRIAN S. VENCE, DDS* ABSTRACT The goal of this clinical report is to describe and illustrate the principles for achieving
Predictable Esthetics through Functional Design: The Role of Harmonious Disclusion BRIAN S. VENCE, DDS* ABSTRACT The goal of this clinical report is to describe and illustrate the principles for achieving
Application of ARCUS digma I, II systems for full mouth reconstruction: a case report
 https://doi.org/10.14368/jdras.2016.32.4.345 ISSN 2384-4353 eissn 2384-4272 Case Report Application of ARCUS digma I, II systems for full mouth reconstruction: a case report Chan Park* Department of Prosthodontics,
https://doi.org/10.14368/jdras.2016.32.4.345 ISSN 2384-4353 eissn 2384-4272 Case Report Application of ARCUS digma I, II systems for full mouth reconstruction: a case report Chan Park* Department of Prosthodontics,
Connect your Scanner to SomnoMed Canada. SOMGauge Protrusive Bite Recording - Manual. Scanning Impressions - Lower and Upper
 IOS Instructions How to create and submit the best scans to SomnoMed Canada for the creation of a custom SomnoDent Sleep Apnea Appliance Its a simple process: STEP 1 Connect your Scanner to SomnoMed Canada
IOS Instructions How to create and submit the best scans to SomnoMed Canada for the creation of a custom SomnoDent Sleep Apnea Appliance Its a simple process: STEP 1 Connect your Scanner to SomnoMed Canada
Case Report Replacement of Missing Anterior Teeth in a Patient with Temporomandibular Disorder
 Case Reports in Dentistry, Article ID 393627, 4 pages http://dx.doi.org/10.1155/2014/393627 Case Report Replacement of Missing Anterior Teeth in a Patient with Temporomandibular Disorder Satheesh B. Haralur
Case Reports in Dentistry, Article ID 393627, 4 pages http://dx.doi.org/10.1155/2014/393627 Case Report Replacement of Missing Anterior Teeth in a Patient with Temporomandibular Disorder Satheesh B. Haralur
Removable Prosthodontics. Summative Evaluations
 Department of General Dentistry Division of Removable Prosthodontics Summative Evaluations For Competency #9 Rev. February 2010 Ronni A. Schnell, D.M.D., M.A.G.D. General Guidelines for the Removable Prosthodontics
Department of General Dentistry Division of Removable Prosthodontics Summative Evaluations For Competency #9 Rev. February 2010 Ronni A. Schnell, D.M.D., M.A.G.D. General Guidelines for the Removable Prosthodontics
Dentistry continues to evolve. Esthetic Templates for Complex Restorative Cases: Rationale and Management
 Esthetic Templates for Complex Restorative Cases: Rationale and Management DEAN E. KOIS, DMD* KYLE K. SCHMIDT, DDS* ARIEL J. RAIGRODSKI, DMD, MS ABSTRACT Complex restorative cases require difficult clinical
Esthetic Templates for Complex Restorative Cases: Rationale and Management DEAN E. KOIS, DMD* KYLE K. SCHMIDT, DDS* ARIEL J. RAIGRODSKI, DMD, MS ABSTRACT Complex restorative cases require difficult clinical
Oral splints come in a plethora
 DigiSplint - the CAD/CAM splint By Terry Whitty Intraoral scans are now becoming more common... and whereas these digital impressions are popular in restorative dentistry, they are equally suited to splint
DigiSplint - the CAD/CAM splint By Terry Whitty Intraoral scans are now becoming more common... and whereas these digital impressions are popular in restorative dentistry, they are equally suited to splint
SPLINT THERAPY: WHAT WORKS, WHAT DOESN T AND WHY?
 Clinical Research Foundation (A non-profit Foundation for Research and Charitable Endeavors) SPLINT THERAPY: WHAT WORKS, WHAT DOESN T AND WHY? Terry T. Tanaka, DDS Clinical Professor, Advanced Education
Clinical Research Foundation (A non-profit Foundation for Research and Charitable Endeavors) SPLINT THERAPY: WHAT WORKS, WHAT DOESN T AND WHY? Terry T. Tanaka, DDS Clinical Professor, Advanced Education
A Systematic Technique for Carving Amalgam and Composite Restorations
 Ó Operative Dentistry, 2011, 36-3, 335-339 Clinical Technique/Case Report A Systematic Technique for Carving Amalgam and Composite Restorations A Kilistoff Clinical Relevance The purpose of this technique
Ó Operative Dentistry, 2011, 36-3, 335-339 Clinical Technique/Case Report A Systematic Technique for Carving Amalgam and Composite Restorations A Kilistoff Clinical Relevance The purpose of this technique
TMJ UNDERSTANDING SYNDROME SPECIAL REPORT By Paul R. White, D.D.S. Special Report: Understanding TMJ Syndrome
 SPECIAL REPORT Special Report: Understanding TMJ Syndrome UNDERSTANDING TMJ SYNDROME By Paul R. White, D.D.S. 804.715.1647 www.smilerichmond.com 804.715.1647 www.smilerichmond.com 1 UNDERSTANDING TMJ SYNDROME
SPECIAL REPORT Special Report: Understanding TMJ Syndrome UNDERSTANDING TMJ SYNDROME By Paul R. White, D.D.S. 804.715.1647 www.smilerichmond.com 804.715.1647 www.smilerichmond.com 1 UNDERSTANDING TMJ SYNDROME
Maximizing Insurance Benefits
 Maximizing Insurance Benefits For Splint Patients This guide contains dental insurance information and dental codes to assist you in processing insurance claims for splint treatment. Reference: American
Maximizing Insurance Benefits For Splint Patients This guide contains dental insurance information and dental codes to assist you in processing insurance claims for splint treatment. Reference: American
CATCH IT RIGHT -A CASE REPORT ON OCCLUSAL SPLINT
 www.djas.co.in ISSN No-2321-1482 DJAS 4(III), 195-200, 2016 All rights are reserved CASE REPORT Dental JOURNAL of Advance Studies CATCH IT RIGHT -A CASE REPORT ON OCCLUSAL SPLINT 1 2 3 Monika Makkar, Poonam
www.djas.co.in ISSN No-2321-1482 DJAS 4(III), 195-200, 2016 All rights are reserved CASE REPORT Dental JOURNAL of Advance Studies CATCH IT RIGHT -A CASE REPORT ON OCCLUSAL SPLINT 1 2 3 Monika Makkar, Poonam
3000 Series Articulator System
 3000 Series Articulator System Models 3040 and 3140 Instruction Manual Whip Mix Corporation 361 Farmington Ave. P.O. Box 17183 Louisville, KY 40217-0183 USA 502-637-1451 800-626-5651 Fax 502-634-4512 www.whipmix.com
3000 Series Articulator System Models 3040 and 3140 Instruction Manual Whip Mix Corporation 361 Farmington Ave. P.O. Box 17183 Louisville, KY 40217-0183 USA 502-637-1451 800-626-5651 Fax 502-634-4512 www.whipmix.com
TURN CLASS II INTO SIMPLE CLASS I PATIENTS.
 TURN CLASS II INTO SIMPLE CLASS I PATIENTS. THE CARRIERE MOTION TM APPLIANCE fast gentle natural The Carriere Philosophy. Fast. Shortens overall treatment time by up to four months as it treats Class II
TURN CLASS II INTO SIMPLE CLASS I PATIENTS. THE CARRIERE MOTION TM APPLIANCE fast gentle natural The Carriere Philosophy. Fast. Shortens overall treatment time by up to four months as it treats Class II
Occlusion and Attachments
 THE VOICE OF TECHNO-CLINICAL DENTISTRY Occlusion and Attachments The Underlying Scheme for Successful Overdentures Dennis Urban, CDT Vol. 9 No. 4 - April 2010 - Reprint 2 Spectrum dialogue Vol. 9 No. 4
THE VOICE OF TECHNO-CLINICAL DENTISTRY Occlusion and Attachments The Underlying Scheme for Successful Overdentures Dennis Urban, CDT Vol. 9 No. 4 - April 2010 - Reprint 2 Spectrum dialogue Vol. 9 No. 4
THE NORTH, SOUTH, EAST AND WEST OF OCCLUSION. Dr Tom Bereznicki BDS (Edin)
") THE NORTH, SOUTH, EAST AND WEST OF OCCLUSION Dr Tom Bereznicki BDS (Edin) At one end of the spectrum are dentists who believe that they can go through their working lives with scant regard for their patient
THE NORTH, SOUTH, EAST AND WEST OF OCCLUSION Dr Tom Bereznicki BDS (Edin) At one end of the spectrum are dentists who believe that they can go through their working lives with scant regard for their patient