The Detroit Dental Health Project. On behalf of community organizations, investigators, and staff
|
|
|
- Giles Damian Clark
- 5 years ago
- Views:
Transcription

1 The Detroit Dental Health Project On behalf of community organizations, investigators, and staff 1

2 Question Why do some African-American children (<6 years old) and their main caregivers have better oral health than others who live in the same community and share similar social, economic, and cultural characteristics? 2
3 Families Included in the DDHP African-American children under 6 years of age. Caregiver of child primary decision maker about: Feeding, taking care of mouth and teeth, visiting the doctor or dentist. Majority are maternal caregivers. Household income below 250% of the 2000 poverty level. 39 Census tracts within Detroit were identified - 35,000 households of which approximately 17% were expected to have eligible children. 3


 level Access and use of dental")
4 Interactions with the DDHP families 5-year follow-up of a representative sample of 1,021 low-income African-American families in Detroit Social and behavioral determinants of health Wave I Multi-dimensional intervention Wave II Main outcome: Dental caries (ICDAS) Wave III Diet, nutrition & Blood lead (trace elements) level Access and use of dental care services 4


5 Detroit and Suburbs: 2005 Projected Household Income by Census Tract Push pins represent dentists in private practice. 5
6 Sampling Two-stage selection of African-American families in the poorest 39 Census Tracts in Detroit Stage 1 Stage 2 - Selected 118 blocks out of 1,526 blocks in 39 Census Tracts - Adjacent blocks were linked to the 118 blocks to create segments of a minimum size (100 housing units) - A total of 565 blocks formed the 118 segments - Listed 17,269 buildings of which 14,406 were housing units -> 12,655 housing units randomly selected - Screening visit by trained staff 10,695 were occupied (84.5% occupancy rate) 9,781 were successfully contacted and screened (91.5% contact rate) - Of the 9,781 contacted housing units, 1,386 (14.2%) had an eligible African- American child under 6 years of age - 1,021 families completed the first (Wave 1) interview/examination 6
7 Wave I ( ) Questionnaire/interview Psychosocial and Behavioral Determinants of Health Lead Exposure: blood & saliva (adults only) Nutrition: adults & children (Block FFQ ) Dental and Oral Health Assessment Caries: adults & children Periodontal health: adults 7
8 Social and Behavioral Factors Parenting stress Caregiver oral health beliefs and attitudes Self-efficacy Quality of life Depressive symptoms Everyday discrimination Religiosity Social support (family, neighborhood) Access to dental care and dental visits Rating of availability of dental services Dental insurance Trust in medical and dental providers Oral health behaviors and practices for child and caregiver 8

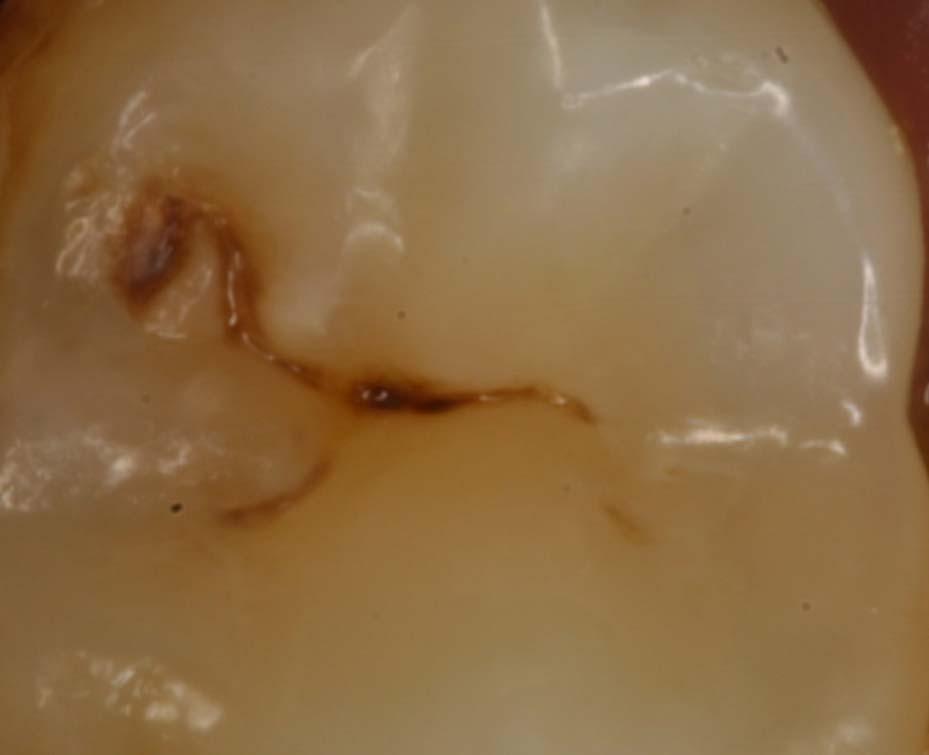
9 Early Carious Lesions Early lesions 9


10 Early Carious Lesions: Occluding Tooth Surfaces 10


11 Early Carious Lesions 11

12 Cavitated Lesions 12

13 Cavitated Lesions Early tooth decay Early tooth decay Cavitated tooth decay 13
14 Diet, Nutrition & Lead Exposure Questionnaire: caregiver and index child Nutrition: Block FFQ for adults and children 3-5 years New questionnaire was designed and tested for 0-2 year old children Food sufficiency Height and weight measurements Blood and saliva samples (adult only) For lead and other metal assay 14
15 Dental and Oral Health Assessment Main Outcome (caries) Caregiver and child Periodontal disease Pocket depth & gingival bleeding Oral Hygiene status 15
16 Tracking Families (1,021) Mobility is high Disconnected telephone numbers Families may temporarily live with neighbors, friends, or relatives 654 (64%) completed Wave III (2007). 16


17 Families moved an average of 2 times in the past 5 years 17
18 Wave II ( ) 791 families (77%) returned for interviews and examinations Questionnaire/interview Psychosocial and behavioral factors Lead Exposure child only Nutrition child only Dental and Oral Health Assessment Tailored Educational Intervention Motivational Interviewing with DVD 18
19 Wave III (March September 2007) 654 families (64%) returned for interviews and examinations Questionnaire/interview Psychosocial and behavioral factors Nutrition child only Dental and Oral Health Assessment Evaluation of Educational Intervention Motivational Interviewing with DVD 19
20 What have we learned from the DDHP? So far 20
21 Families 21
22 Characteristics Caregivers: Age: years (avg = 29.3) Females (95.5%) Relationship: 86% mothers 4% fathers 6% grandmothers 4% other caregivers 53% unemployed at baseline ( ) EDUCATION REPORTED ANNUAL INCOME some high school high school diploma some college college degree Children: Age: 0-5 years (avg = 2.6) Females (52.2%) <$10,000 $10,000-$29,999 >$30,000 22
23 Dental Caries 23
24 Early Childhood Caries (ECC) and Severe ECC Status by Child's Age (Baseline , weighted %) 100% 90% 80% % % 13 50% 40% S-ECC ECC-Only No cavities 30% 20% % % total Child's age 24
25 Percentage of Children with New Non-cavitated and Cavitated Lesions in Primary Teeth Percentage of Children W1-W2 W1-W Non-cavitated (ICDAS 1) Non-cavitated (ICDAS 2) Cavitated (ICDAS 3-6) 25
26 Mean Number of New Non-cavitated and Cavitated Lesions in Children s Primary Teeth W1-W2 W1-W Non-cavitated (ICDAS 1) Non-cavitated (ICDAS 2) Cavitated (ICDAS 3-6) 26
27 Percentage of Children with New Non-cavitated and Cavitated Lesions in Permanent Teeth Percentage of Children W1-W2 W1-W Non-cavitated (ICDAS 1) Non-cavitated (ICDAS 2) Cavitated (ICDAS 3-6) 27
28 Mean Number of New Non-cavitated and Cavitated Lesions in Children s Permanent Teeth Number of Lesions W1-W2 W1-W Non-cavitated (ICDAS 1) Non-cavitated (ICDAS 2) Cavitated (ICDAS 3-6) 28
29 Periodontal Disease 29

30 Gingivitis: Bleeding and Inflammation 30

31 Early Periodontitis (Gum Disease) 31
32 Gum Diseases in Adults at Baseline ( ) Percentage of Adults None Bleeding Bleeding + Mild Gum Disease 16.3 Bleeding + Severe Gum Dise ase 5.1 Moderate Gum Disease 1.0 Severe Gum Dis eas e 32
33 Conclusion: Dental Diseases While the children and caregivers have advanced dental caries; early or mild forms of dental caries and periodontal disease are more common. Hence, preventive or minimal interventions are indicated. 33
34 Food Intake and Tooth Decay 34
35 Diet and Dental Caries: Caregivers More severe dental caries is related to more frequent consumption of soft drinks (p=.02) Mean DMFS scores were significantly related to the proportion of energy from sugars D t MFS Lowest tertile ( 9.6% of energy from sugar) 44.4 Middle ( % of energy from sugar) 49.7 Highest (17.8% of energy from sugar) 52.4 p=.001 Burt BA, Kolker JL, Sandretto AM, Yuan Y, Sohn W, Ismail AI. Dietary Patters Related to Caries in a Low-Income Adult Population. Caries Research 2004; 40:
36 Diet and Dental Caries: Children Higher levels of decay were associated with higher consumption of soda and powdered/sugared sports drinks (e.g. Gatorade) 54% of all sugar consumed came from sugared beverages (soda, sports drinks) Kolker JL, Burt B, Sandretto A, Yuan Y, Sohn W, Lang S, Ismail AI. Dental caries and dietary patterns in low-income African-American children. Pediatr Dent 2007; 29: Children who consumed more soft drinks as they aged, were more likely to have after 2 years: greater number of new lesions (IRR=1.75) new filled surfaces (IRR=2.67) Children who were consistently high consumers of soft drinks were also more likely to have a greater number of new filled surfaces (IRR=2.68) after 2 years Lim S, Sohn, Burt BA, Sandretto AM, Kolker JL, Marshall TA, Ismail AI. Cariogenicity of soft drinks, milk, and fruit juice in low income African-American children: A longitudinal study. J Am Dent Assoc 2008; 139:
37 Dental Caries and Consumption of Soft Drinks, Milk and 100% Fruit Juice Number of Lesions New decayed, missing, filled Consistently High Milk and Juice Decreased Soft Drinks Increased Soft Drinks Consitently High Soft Drinks 37
38 Obesity in Detroit 38
39 Diet and Obesity: Caregivers Most frequently consumed foods: Tap water Sugared soda Potato chips 7.4% eat 2 or more servings of vegetables per day 7.8% eat 2 or more servings of fruits per day Average daily intake = 2,090 kcals 15% of energy came from sugars Burt B, Kolker J, Sandretto A, Yuan Y, Sohn W, Ismail AI. Dietary patterns related to caries in a low-income adult population. Caries Res 2006; 40:
40 Diet and Obesity: Children Most frequently consumed foods: Cold cereal Potato chips Sliced cheese Bread Bologna Ketchup No vegetables were in the top 18 most frequently consumed foods (although several fruits appeared) 54% of sugar intake came from sweetened beverages Kolker JL, Burt B, Sandretto A, Yuan Y, Sohn W, Lang S, Ismail AI. Dental caries and dietary patterns in low-income African-American children. Pediatr Dent 2007; 29:
41 Diet and Obesity: Children The assumption is that most children grow out of their obesity That is what you see with a national sample of African-American children in the U.S. Unfortunately that is not what we see with the DDHP cohort 41
42 Change in Weight-for-Age from Baseline ( ) to Wave 3 (2007) Percentage of Children Underw eight Healthy At Risk Overw eight Underweight Healthy At Risk Overweight 42
43 Transition Probablities of Weight Class among African-American children in NLSY (3-5 year olds) Normal Overweight Obese Normal Overweight Obese
44 Transition Probablities of Weight Class among DDHP children Normal Overweight Obese Normal weight Overweight Obese
45 Diet and Obesity: Children This suggests that we need to act very early in life to prevent obesity in our children as they grow older 45
46 Determinants of Caries Development and Progression Social & Behavioral Factors 46
47 Psychosocial factors: Depression Depressive symptoms are highly prevalent among caregivers 35% scored 16 or above on CES-D 16% scored 26 or above Protective Factors: financial support (OR=0.59) childcare support (OR=0.40) emotional support (OR=0.32) Risk Factors: experience of everyday discrimination (OR=2.7) Seifert K, Finlayson TL, Williams DR, Delva J, Ismail AI. Modifiable risk and protective factors for depressive symptoms in low-income African-American mothers. Am J of Orthopsychiatry 2007; 77(1):
48 Depressive Symptoms in Caregivers at Baseline ( ) and Wave 3 (2007) Percentage of Adults No Symptoms Both Waves Symptoms Both Waves Increase in Symptoms Decrease in Symptoms Baseline to Wave
49 Social Support and Depressive Symptoms CES-D Score Yes No Errands*** Financial *** Transportation *** Childcare *** Emotional*** *** p<
50 Discrimination and Depressive Symptoms CES-D score W1 W Never Fewer than 5 areas 5 or more areas Areas include: being treated with less courtesy, less respect, receiving poorer service, people acting as if I am not smart, as if they are afraid of me, as if I am dishonest, as if they are better than me, called names, threatened or harassed, unfairly stopped by police, unfairly discouraged by a teacher. ***Differences within wave are statistically significant (p<.001) 50
51 Stressors and Depressive Symptoms CES-D Score No Yes 5 0 Crime occurs often Drugs a serious problem** Had to cut or skip meals b/c of money*** ** p<.01 *** p<
52 Psychosocial factors: Fatalism 79% of caregivers endorsed a fatalistic health belief Children of Fatalistic Caregivers: Brushed less frequently (8.5 v times per week, p<0.01) Finlayson TL, Siefert K, Ismail AI, Sohn W. Maternal self-efficacy and 1-5 year old children s brushing habits. Community Dent Oral Epidemiol 2007; 35: Experienced more severe disease at baseline 2.7 times that of children of non-fatalistic caregivers Finlayson TL, Seifert, Ismail AI, Sohn W. Psychosocial factors and oral health among low-income African-American children in Detroit. Community Dent Oral Epidemiol 2007; 35: Experienced more new disease over a 2-year period (OR=1.3 for new d t mfs; OR=1.4 for new d 2 mfs) 52
53 Caregiver Fatalism and New Tooth Decay in Children Between Baseline ( ) and Wave 3 (2007) Number of Lesions Cavitated Non-cavitated 1 0 Fatal-Fatal Not Fatal-Not Fatal Becam e Not Fatal Becam e Fatal 53
54 Psychosocial factors: Self-efficacy If mothers were confident in their ability to make sure their child s teeth were brushed, children brushed more frequently (r=0.18, p<0.0001) Finlayson TL, Siefert K, Ismail AI, Sohn W. Maternal self-efficacy and 1-5 year old children s brushing habits. Community Dent Oral Epidemiol 2007; 35: Being tired, busy or depressed were most common situations in which mothers were not confident that they could take care of their children s oral health needs 54
55 Psychosocial factors: Parenting Stress Parenting stress scores are fairly normally distributed; most report sometimes feeling stressed Parenting stress is inversely related to early childhood caries. 1-3 year olds: odds of having ECC is reduced by about one-third for every unit increase in parenting stress (OR=0.62, p<0.05) 4-5 year olds: odds of having ECC is reduced by about one-fourth (OR=0.72, p<0.10) Finlayson TL, Seifert, Ismail AI, Sohn W. Psychosocial factors and oral health among low-income African-American children in Detroit. Community Dent Oral Epidemiol 2007; 35:
56 Religiosity and Tooth Decay Children of caregivers who reported being Very/fairly religious were less likely to develop tooth decay than children of less religious caregivers 56
57 Use of Health Services and Caries 57
58 Type of Dental Insurance and Caries in Children at Baseline ( ) Number of Lesions Cavitated Non-cavitated Private Medicaid None 58
59 Type of Dental Insurance and New Non-cavitated and Cavitated Lesions in Children between Baseline ( ) and Wave 3 (2007) 7 Number of Lesions New Cavitated New Non-cavitated 1 0 Private Medicaid None 59
60 Dental Health of Children Receiving Dental Care Under Medicaid 60
61 DDHP-Medicaid data analysis Medicaid claims data Wave 1 Baseline Exam (n = 698) Visited dentists (n = 350) Did not visit dentists (n = 348) Prevention-only visit (n = 216) Treatment visit (n = 134) Wave 2 Exam (n = 698) Caries Transition Matrix between W1 and W2 61
62 Type of Dental Visit and Caries Status N (%) Children with untreated cavities at baseline % of cavities at baseline that were left untreated at Wave 2 No dental visit 348 (50.9%) 20.4% 74.9% Preventive-only visit 216 (30.4%) 25.8% 75.2% Treatment visit 134 (18.7%) 55.8% 28.6% Total % 55.5% 62
63 Summary: Children s Caries Status Child s age Caregiver s age Caregiver s tooth decay Child s soda consumption Caregiver having a fatalistic belief ( most children eventually develop dental cavities ) Parental stress Religiosity Social support (SES,WIC participation, child insurance weak) 63
64 Lead Levels in Children and Adults 64
65 Lead Levels Adults: 5 with high blood lead levels (0.5%) at baseline Re-tested at Wave 3 none with high lead Children: 35 with high blood lead levels (5.0%) in Re-tested in with high lead, but lower than baseline 65
66 Policy Implications 66
67 Policy Implications Dental Caries We need comprehensive, integrated, and sustainable models to combat the problem of tooth decay in children and adults Medicaid policy should change: all care should be provided, not only preventive care Collaboration among the different programs in Detroit should be the basis for forming solutions Engagement of families and organizations in developing solutions is essential 67
68 Summary Prevalence and severity of tooth decay is high among low-income children in Detroit Development of caries is fast: By the age of 2: 20% have at least one cavity 30% have severe early tooth decay (including non-cavitated lesions) Access to dental care is a major problem Providing ONLY preventive care is ineffective Caregivers tooth decay experience is a significant predictor of infant tooth decay development and progression Children s soda drinking pattern over time increases the development and progression of tooth decay Psychosocial factors (fatalistic belief, parenting stress, social support, preventive orientation) play important roles in tooth decay development 68
69 Next Steps Community-based interventions to eliminate disparities Dental anxiety Social support Motivational education Diet and nutritional literacy Management and coordination of dental care Best clinical care focusing on prevention Community/home follow-up Starts in
70 Thank you! 70
71 Transition of Disease: Children w1->w2 w1->w3 w2->w3 Increment N Mean SD N Mean SD N Mean SD Primary Teeth d d f fd fd c m(97) D12mfs D2mfs Permanent Teeth d d f fd fd c m(97) d12mfs d2mfs
72 Transition of Disease: Adults w1->w2 w1->w3 w2->w3 Increment N Mean SD N Mean SD N Mean SD d d f fd fd c cd cd m(97) d12mfs d2mfs
73 Disease Transitions Between Baseline ( ) and Wave 3 (2007) New d 2 mfs New d t mfs New Non- Cavitated New Cavitated New Filled 0 New Filled 1 New Filled 2 New Missing due to caries Baseline Age Incidence Severity Incidence Severity Incidence Severity Children Incidence Adults Severity Incidence Severity Incidence Severity Incidence Severity Incidence Severity Red indicates significant difference between age groups (p<0.05) 73
74 Motivational Intervention (Wave 2) Motivational Interviewing (MI) Individual-centered, directive Aid caregiver in making informed decisions and adopt behaviors that will prevent child from developing disease Randomly assigned children into two groups DVD-only Caregiver shown18 minute video focusing on how to keep a child free from tooth decay Received brochure with child s picture and standard recipe of goals for preventing tooth decay DVD + MI Showed video Developed personal goals for preventing tooth decay Discussed barriers to reaching goals Received brochure with child s picture and personalized goals for preventing tooth decay 74
75 Motivational Intervention: Evaluation Wave 2 Evaluation Questionnaire Oral health behaviors (e.g. brushing frequency) Oral health practices (e.g. providing health snacks, taking child to the dentist) Oral Health Self-efficacy Oral Health Knowledge Oral Health Related Fatalism Wave 2 Follow-up (6 months post-intervention) Oral health behaviors (e.g. brushing frequency) Oral health practices (e.g. providing health snacks, taking child to the dentist) Wave 3 Evaluation Questionnaire Oral health behaviors (e.g. brushing frequency) Oral health practices (e.g. providing health snacks, taking child to the dentist) Oral Health Self-efficacy Oral Health Knowledge Oral Health Related Fatalism Treatment Self-Regulation Questionnaire 75
76 Motivational Intervention: 6-month Results Wave 2 Follow-up - differences Same caregiver in both waves (n=582) Behaviors DVD+MI DVD-Only p Times child brushes per day ** Days child brushes at bedtime * Caregiver reports checking for pre-cavities ** Caregiver reports making sure child brushes at bedtime * Caregiver reports making sure child brushes 2x per day * * p<.05; ** p<.01; *** p<
77 Motivational Intervention: 2-Year Results Wave 3 Evaluation Same caregiver in both waves (n=582) Behaviors (Differences only) DVD+MI DVD-Only p Caregivers reporting making sure child brushes at bedtime 74.3% 68.0% * Caregivers reporting making sure child brushes 2x per day 77.4% 71.8% * I don t think about my child s teeth or overall oral health (1=Not at all true 10=Very true) * * p<.05; ** p<.01; *** p<.001 Significant differences in times child brushes per day, days per week child brushes at bedtime, and proportion of caregivers reporting checking for precavities disappear; however, results are in expected direction. 77
78 Motivational Intervention: 2-Year Results Wave 3 Evaluation Same caregiver in both waves (n=582) Child Dental Outcomes (W2-W3) DVD+MI DVD-Only p Primary teeth New non-cavitated New cavitated New dtmfs New d2mfs Permanent teeth New non-cavitated New cavitated New dtmfs New d2mfs
79 Motivational Intervention: Results 6-month follow-up: brief MI intervention appears to have impact on: Behavioral outcomes: More MI Caregivers report: Greater brushing frequency for the children Checking for pre-cavities 2-year follow-up: Behavioral outcomes: More MI caregivers report: Ensuring child brushes at bedtime Ensuring child brushes 2x per day Clinical outcomes: no differences (preliminary) Continuing to examine clinical outcomes with zero-inflated negative binomial models accounting for sampling and weighting 79
Social cognitive, behavioral, and psychosocial predictors of young African American children s oral health in Detroit
 Social cognitive, behavioral, and psychosocial predictors of young African American children s oral health in Detroit Tracy L. Finlayson, PhD 1 Kristine A. Siefert, PhD, MPH 2 and Amid I. Ismail, BDS,
Social cognitive, behavioral, and psychosocial predictors of young African American children s oral health in Detroit Tracy L. Finlayson, PhD 1 Kristine A. Siefert, PhD, MPH 2 and Amid I. Ismail, BDS,
The following resources related to this article are available online at jada.ada.org ( this information is current as of May 19, 2009 ):
:") Cariogenicity of Soft Drinks, Milk and Fruit Juice in Low-Income African-American Children: A Longitudinal Study Sungwoo Lim, Woosung Sohn, Brian A. Burt, Anita M. Sandretto, Justine L. Kolker, Teresa
Cariogenicity of Soft Drinks, Milk and Fruit Juice in Low-Income African-American Children: A Longitudinal Study Sungwoo Lim, Woosung Sohn, Brian A. Burt, Anita M. Sandretto, Justine L. Kolker, Teresa
Child oral health: Habits in Australian homes
 RCH NATIONAL Child Health POLL Child oral health: Habits in Australian homes Poll report Dr Anthea Rhodes, Director Poll 10, March 2018 Embargoed 00.01 AM March 7, 2018 Report highlights One in three (32%)
RCH NATIONAL Child Health POLL Child oral health: Habits in Australian homes Poll report Dr Anthea Rhodes, Director Poll 10, March 2018 Embargoed 00.01 AM March 7, 2018 Report highlights One in three (32%)
Detroit Dental Health Project. Parenting, Social Determinants, Health Services, Quality of Life, and Outcomes Questionnaire
 Detroit Dental Health Project Parenting, Social Determinants, Health Services, Quality of Life, and Outcomes Questionnaire CAREGIVER NAME: CAREGIVER ID: INDEX CHILD NAME: INDEX CHILD ID: VISIT DATE: /
Detroit Dental Health Project Parenting, Social Determinants, Health Services, Quality of Life, and Outcomes Questionnaire CAREGIVER NAME: CAREGIVER ID: INDEX CHILD NAME: INDEX CHILD ID: VISIT DATE: /
2012 Ph.D. APPLIED EXAM Department of Biostatistics University of Washington
 2012 Ph.D. APPLIED EXAM Department of Biostatistics University of Washington Background Dental caries is an infectious, transmissible bacterial disease that is a common childhood condition in the United
2012 Ph.D. APPLIED EXAM Department of Biostatistics University of Washington Background Dental caries is an infectious, transmissible bacterial disease that is a common childhood condition in the United
PERINATAL CARE AND ORAL HEALTH
 PERINATAL CARE AND ORAL HEALTH Lakshmi Mallavarapu, DDS Terry Reilly Health Services Boise, Idaho CE objectives Recognize the necessity of Oral Care during Perinatal Period Examine and assess teeth and
PERINATAL CARE AND ORAL HEALTH Lakshmi Mallavarapu, DDS Terry Reilly Health Services Boise, Idaho CE objectives Recognize the necessity of Oral Care during Perinatal Period Examine and assess teeth and
ORAL HEALTH MECHANISM OF ACTION INFLUENTIAL FACTORS 5/8/2017
 ORAL HEALTH Oral health is a state of being free from chronic mouth & facial pain, oral & throat cancer, oral sores, birth defects such as cleft lip & palate, periodontal (gum) disease, tooth decay & tooth
ORAL HEALTH Oral health is a state of being free from chronic mouth & facial pain, oral & throat cancer, oral sores, birth defects such as cleft lip & palate, periodontal (gum) disease, tooth decay & tooth
Objectives. Describe how to utilize caries risk assessment for management of early childhood caries
 Objectives Define Early Childhood Caries Describe how to utilize caries risk assessment for management of early childhood caries Explain how to implement early childhood caries management within a dental
Objectives Define Early Childhood Caries Describe how to utilize caries risk assessment for management of early childhood caries Explain how to implement early childhood caries management within a dental
Dental caries prevention. Preventive programs for children 5DM
 Dental caries prevention Preventive programs for children 5DM Definition of Terms Preventive dentistry: usage of all the means to achieve and maintain the optimal oral health prevention of dental caries,
Dental caries prevention Preventive programs for children 5DM Definition of Terms Preventive dentistry: usage of all the means to achieve and maintain the optimal oral health prevention of dental caries,
ARE YOU MOUTHWISE? AN ORAL HEALTH OVERVIEW FOR PRIMARY CARE
 ARE YOU MOUTHWISE? AN ORAL HEALTH OVERVIEW FOR PRIMARY CARE Funding providing by: Developed by: Terry L. Buckenheimer, DMD Karen Pesce Buckenheimer, R.N., BSN Executive Director, MORE HEALTH, Inc. Why
ARE YOU MOUTHWISE? AN ORAL HEALTH OVERVIEW FOR PRIMARY CARE Funding providing by: Developed by: Terry L. Buckenheimer, DMD Karen Pesce Buckenheimer, R.N., BSN Executive Director, MORE HEALTH, Inc. Why
Promoting Oral Health
 Promoting Oral Health Hope Saltmarsh, RDH, M.Ed. Doug Johnson, DMD October 2009 11/3/2009 12:14:04 PM 5864_ER_RED 1 Learning Objectives Identify Bright Futures recommendations for oral health. Describe
Promoting Oral Health Hope Saltmarsh, RDH, M.Ed. Doug Johnson, DMD October 2009 11/3/2009 12:14:04 PM 5864_ER_RED 1 Learning Objectives Identify Bright Futures recommendations for oral health. Describe
The Essential Guide to Children s Dental Health
 Ages 0-11 The Essential Guide to Children s Dental Health What every parent should know.. Introduction Most parents don t realize that tooth decay is the number one chronic disease among Tulsa-area children.
Ages 0-11 The Essential Guide to Children s Dental Health What every parent should know.. Introduction Most parents don t realize that tooth decay is the number one chronic disease among Tulsa-area children.
A GUIDE TO CARING FOR YOUR CHILD S TEETH AND MOUTH
 A GUIDE TO CARING FOR YOUR CHILD S TEETH AND MOUTH A COLLABORATION BETWEEN Use this guide to learn about oral health and taking care of your child s teeth from birth to kindergarten and into their teen
A GUIDE TO CARING FOR YOUR CHILD S TEETH AND MOUTH A COLLABORATION BETWEEN Use this guide to learn about oral health and taking care of your child s teeth from birth to kindergarten and into their teen
Food, Nutrition & Dental Health Summary
 By Liz Pearson, RD www.lizpearson.com Food, Nutrition & Dental Health Summary Canadian Health Measures Survey (2007 to 2009) 57% of 6 11 year olds have or have had a cavity 59% of 12 19 year olds have
By Liz Pearson, RD www.lizpearson.com Food, Nutrition & Dental Health Summary Canadian Health Measures Survey (2007 to 2009) 57% of 6 11 year olds have or have had a cavity 59% of 12 19 year olds have
Healthy Smile Happy Child. Daniella DeMaré Healthy Smile Happy Child Project Coordinator (204)
") Healthy Smile Happy Child Daniella DeMaré Healthy Smile Happy Child Project Coordinator ddemare@chrim.ca (204) 789-3500 What s on the Agenda? Early Childhood Caries (ECC) and Risk Factors: what every health
Healthy Smile Happy Child Daniella DeMaré Healthy Smile Happy Child Project Coordinator ddemare@chrim.ca (204) 789-3500 What s on the Agenda? Early Childhood Caries (ECC) and Risk Factors: what every health
Oral Health Education
 e C ity Fre v a K I DS Oral Health Education for Pregnant Women, Children Birth through Age Five, and Their Families TM A Quick Reference for Home Visitors TM Cavity Free K I DS Cavity Free Kids Oral Health
e C ity Fre v a K I DS Oral Health Education for Pregnant Women, Children Birth through Age Five, and Their Families TM A Quick Reference for Home Visitors TM Cavity Free K I DS Cavity Free Kids Oral Health
Oral Health Matters The forgotten part of overall health
 Oral Health Matters The forgotten part of overall health In 2000, the Surgeon General issued a report Oral Health in America. In the Report, the Surgeon General focused on why oral health is important.
Oral Health Matters The forgotten part of overall health In 2000, the Surgeon General issued a report Oral Health in America. In the Report, the Surgeon General focused on why oral health is important.
Oral Health in Colorado
 Oral Health in Colorado Progress and Opportunities Sara Schmitt Director of Community Health Policy Prepared for the Delta Dental of Colorado Foundation September 2017 About Us: Inform State and National
Oral Health in Colorado Progress and Opportunities Sara Schmitt Director of Community Health Policy Prepared for the Delta Dental of Colorado Foundation September 2017 About Us: Inform State and National
Effectiveness of Primary Care Interventions to Address Childhood Obesity. Disclosure and Presentation Support 11/22/16
 Effectiveness of Primary Care Interventions to Address Childhood Obesity A Review and Directions for the Future Session III: Supporting and Promoting Involvement Diane Dooley, M.D., M.H.S. Co- authors:
Effectiveness of Primary Care Interventions to Address Childhood Obesity A Review and Directions for the Future Session III: Supporting and Promoting Involvement Diane Dooley, M.D., M.H.S. Co- authors:
Oral Health Care: The window to overall health. Head 2 Toe Conference May 9, 2013 Christy Cogil, RN, CFNP and Dr. Melissa Ravago, DMD
 Oral Health Care: The window to overall health Head 2 Toe Conference May 9, 2013 Christy Cogil, RN, CFNP and Dr. Melissa Ravago, DMD Oral Health in America Oral health is essential to the general health
Oral Health Care: The window to overall health Head 2 Toe Conference May 9, 2013 Christy Cogil, RN, CFNP and Dr. Melissa Ravago, DMD Oral Health in America Oral health is essential to the general health
A transition scoring system of caries increment with adjustment of reversals in longitudinal study: evaluation using primary tooth surface data
 Community Dent Oral Epidemiol 2011; 39: 61 68 All rights reserved Ó 2010 John Wiley & Sons A/S A transition scoring system of caries increment with adjustment of reversals in longitudinal study: evaluation
Community Dent Oral Epidemiol 2011; 39: 61 68 All rights reserved Ó 2010 John Wiley & Sons A/S A transition scoring system of caries increment with adjustment of reversals in longitudinal study: evaluation
Cavities are Preventable
 Cavities are Preventable Childhood cavities can be prevented. They are caused by germs in the mouth interacting with sugars in food and drinks. You can t avoid germs or sugars, but you can limit exposure
Cavities are Preventable Childhood cavities can be prevented. They are caused by germs in the mouth interacting with sugars in food and drinks. You can t avoid germs or sugars, but you can limit exposure
Delta Dental of Illinois Children s Oral Health Report
 2017 Delta Dental of Illinois Children s Oral Health Report A Report on the Oral Health of Illinois Children Shining a Spotlight on the Oral Health of Illinois Children As the leading dental benefits provider
2017 Delta Dental of Illinois Children s Oral Health Report A Report on the Oral Health of Illinois Children Shining a Spotlight on the Oral Health of Illinois Children As the leading dental benefits provider
Preventing early childhood caries through medical and dental provider education and collaboration
 Preventing early childhood caries through medical and dental provider education and collaboration Objectives Describe an Oregon model for training medical providers to provide Early Childhood Caries Prevention
Preventing early childhood caries through medical and dental provider education and collaboration Objectives Describe an Oregon model for training medical providers to provide Early Childhood Caries Prevention
Healthy Drinks for Healthy Alaskans Alaska Public Health Summit Session 302 Thursday January 18, am
 Healthy Drinks for Healthy Alaskans Alaska Public Health Summit Session 302 Thursday January 18, 2018 10 11 am Karol Fink MS RDN Director Obesity Prevention Program Ann Potempa MPH Director Play Every
Healthy Drinks for Healthy Alaskans Alaska Public Health Summit Session 302 Thursday January 18, 2018 10 11 am Karol Fink MS RDN Director Obesity Prevention Program Ann Potempa MPH Director Play Every
Dietary Patterns and Oral Health among School Children Aged 6-12 years Old in Kirkuk City
 Tikrit Journal for Dental Sciences 4 (2016) 112-123 Dietary Patterns and Oral Health among School Children Aged 6-12 years Old in Kirkuk City Hiba Hazem Salih. (1) Key words Oral health, children, school,
Tikrit Journal for Dental Sciences 4 (2016) 112-123 Dietary Patterns and Oral Health among School Children Aged 6-12 years Old in Kirkuk City Hiba Hazem Salih. (1) Key words Oral health, children, school,
Healthy Smile Happy Child s New Lift the Lip Video
 Healthy Smile Happy Child s New Lift the Lip Video Daniella DeMaré Project Coordinator Healthy Smile Happy Child Initiative Sandy Kostyniuk Program Consultant, Manitoba and Saskatchewan Region The Public
Healthy Smile Happy Child s New Lift the Lip Video Daniella DeMaré Project Coordinator Healthy Smile Happy Child Initiative Sandy Kostyniuk Program Consultant, Manitoba and Saskatchewan Region The Public
Oral Health Improvement. Prevention in Practice Vicky Brand
 Oral Health Improvement Prevention in Practice Vicky Brand Quiz Question A B C The % of 5 yr olds in 05/06 in Greater Manchester who experienced tooth decay was just over Which of the following is more
Oral Health Improvement Prevention in Practice Vicky Brand Quiz Question A B C The % of 5 yr olds in 05/06 in Greater Manchester who experienced tooth decay was just over Which of the following is more
Oral health education for caries prevention
 Oral health education for caries prevention Objective Understand the fundamentals that inform oral health education programmes. Understand how to segment oral health information for preventive purposes
Oral health education for caries prevention Objective Understand the fundamentals that inform oral health education programmes. Understand how to segment oral health information for preventive purposes
Knowledge, Attitude and Practice about Oral Health among General Population of Peshawar
 SHORT COMMUNICATION Knowledge, Attitude and Practice about Oral Health among General Population of Peshawar Farzeen Khan, Aisha Ayub 3 and Zeeshan Kibria 1 ABSTRACT To determine the level of knowledge
SHORT COMMUNICATION Knowledge, Attitude and Practice about Oral Health among General Population of Peshawar Farzeen Khan, Aisha Ayub 3 and Zeeshan Kibria 1 ABSTRACT To determine the level of knowledge
SMILE, CALIFORNIA! WIC s Role in the Oral Health Plan
 SMILE, CALIFORNIA! WIC s Role in the Oral Health Plan Jennifer Byrne, CCPH Project Manager Perinatal and Infant Oral Health Quality Improvement Project California Department of Public Health If you don
SMILE, CALIFORNIA! WIC s Role in the Oral Health Plan Jennifer Byrne, CCPH Project Manager Perinatal and Infant Oral Health Quality Improvement Project California Department of Public Health If you don
Presented by. Oral Health In Group Child Care. A Medical / Dental Collaborative. Contributors. Objectives 12/3/2012
 Oral Health In Group Child Care Presented by C Eve J Kimball, MD PAAAP Chapter Oral Health Advisor Healthy Teeth, Healthy Children A Pennsylvania Medical/Dental Partnership Support for this program is
Oral Health In Group Child Care Presented by C Eve J Kimball, MD PAAAP Chapter Oral Health Advisor Healthy Teeth, Healthy Children A Pennsylvania Medical/Dental Partnership Support for this program is
Pediatric Dental Surgery Rates for Early Childhood Caries. (Tooth Decay) in Manitoba (2007/08 to 2012/13):
 in Manitoba (2007/08 to 2012/13):") Pediatric Dental Surgery Rates for Early Childhood Caries (Tooth Decay) in Manitoba (27/8 to 212/13): Sharing Evidence with Manitoba Communities, Decision-Makers and Stakeholders January 216 (revised)
Pediatric Dental Surgery Rates for Early Childhood Caries (Tooth Decay) in Manitoba (27/8 to 212/13): Sharing Evidence with Manitoba Communities, Decision-Makers and Stakeholders January 216 (revised)
HELPING YOUR CLIENTS MAKE HEALTHY CHOICES: SUGAR
 HELPING YOUR CLIENTS MAKE HEALTHY CHOICES: SUGAR Thursday, April 13, 2017 Presented by: Pam McFarlane (MDA) and Amanda Nash, RD (HSF) Outline About the Heart and Stroke and MDA Oral Health and Dental Care
HELPING YOUR CLIENTS MAKE HEALTHY CHOICES: SUGAR Thursday, April 13, 2017 Presented by: Pam McFarlane (MDA) and Amanda Nash, RD (HSF) Outline About the Heart and Stroke and MDA Oral Health and Dental Care
Early Childhood Oral Health for MCH Professionals. Julia Richman, DDS, MSD, MPH
 Early Childhood Oral Health for MCH Professionals Julia Richman, DDS, MSD, MPH Who are we? A. Medical care providers (ie MD, RN) B. Dental care providers C. Social services providers D. Other public health
Early Childhood Oral Health for MCH Professionals Julia Richman, DDS, MSD, MPH Who are we? A. Medical care providers (ie MD, RN) B. Dental care providers C. Social services providers D. Other public health
Oral Care during Pregnancy
 Published on: 22 Mar 2012 Oral Care during Pregnancy Introduction Pregnancy influences nearly every aspect of a woman's life, including the oral health. Diet and hormonal changes during pregnancy may increase
Published on: 22 Mar 2012 Oral Care during Pregnancy Introduction Pregnancy influences nearly every aspect of a woman's life, including the oral health. Diet and hormonal changes during pregnancy may increase
Building a Community Dental Health Network 75% Cavity Free 5 Year Olds by 2020 UCSF DPH 175-February 28,2017
 Building a Community Dental Health Network 75% Cavity Free 5 Year Olds by 2020 UCSF DPH 175-February 28,2017 Kim Caldewey, PA, MPH Dental Health Program Manger Dental Health: A Public Health Approach California
Building a Community Dental Health Network 75% Cavity Free 5 Year Olds by 2020 UCSF DPH 175-February 28,2017 Kim Caldewey, PA, MPH Dental Health Program Manger Dental Health: A Public Health Approach California
Oral Health Care for Pregnant Women
 Oral Health Care for Pregnant Women Renee Samelson MD, MPH, FACOG Associate Clinical Professor Maternal Fetal Medicine Albany Medical College Committee on Oral Health Access to Care Institute of Medicine
Oral Health Care for Pregnant Women Renee Samelson MD, MPH, FACOG Associate Clinical Professor Maternal Fetal Medicine Albany Medical College Committee on Oral Health Access to Care Institute of Medicine
Swiss Food Panel. -A longitudinal study about eating behaviour in Switzerland- ENGLISH. Short versions of selected publications. Zuerich,
 Vertrag 10.008123 ENGLISH Swiss Food Panel -A longitudinal study about eating behaviour in Switzerland- Short versions of selected publications Zuerich, 16.10. 2013 Address for Correspondence ETH Zurich
Vertrag 10.008123 ENGLISH Swiss Food Panel -A longitudinal study about eating behaviour in Switzerland- Short versions of selected publications Zuerich, 16.10. 2013 Address for Correspondence ETH Zurich
Oral Health: An Essential Component of Primary Care. Executive Summary
 Oral Health: An Essential Component of Primary Care Executive Summary June 2015 Executive Summary The Problem Oral health is essential for healthy development and healthy aging, yet nationwide there is
Oral Health: An Essential Component of Primary Care Executive Summary June 2015 Executive Summary The Problem Oral health is essential for healthy development and healthy aging, yet nationwide there is
Dental Care Remains the No. 1 Unmet Health Care Need for Children and Low-Income Adults
 Oral Health and Access to Dental Care for Ohioans, 2007 Dental Care Remains the No. 1 Unmet Health Care Need for Children and Low-Income Adults Oral Health and Access to Dental Care for Ohioans, 2007
Oral Health and Access to Dental Care for Ohioans, 2007 Dental Care Remains the No. 1 Unmet Health Care Need for Children and Low-Income Adults Oral Health and Access to Dental Care for Ohioans, 2007
Dental health status of Hong Kong preschool children. Citation Hong Kong Dental Journal, 2009, v. 6 n. 1, p. 6-12
 Title Dental health status of Hong Kong preschool children Author(s) Lo, ECM; Loo, EKY; Lee, CK Citation Hong Kong Dental Journal, 2009, v. 6 n. 1, p. 6-12 Issued Date 2009 URL http://hdl.handle.net/10722/58042
Title Dental health status of Hong Kong preschool children Author(s) Lo, ECM; Loo, EKY; Lee, CK Citation Hong Kong Dental Journal, 2009, v. 6 n. 1, p. 6-12 Issued Date 2009 URL http://hdl.handle.net/10722/58042
Healthy Eating Policy
 Healthy Eating Policy Policy Code: TPN21 Policy Start Date: October 2014 Policy Review Date: October 2015 Healthy Eating Policy Page 1 of 5 1. Policy Statement 1.1 Children are provided with regular drinks
Healthy Eating Policy Policy Code: TPN21 Policy Start Date: October 2014 Policy Review Date: October 2015 Healthy Eating Policy Page 1 of 5 1. Policy Statement 1.1 Children are provided with regular drinks
Health Impact Assessment
 EMBARGOED UNTIL TUESDAY, JUNE 26 AT 12:01 AM EST. Health Impact Assessment National Nutrition Standards for Snack and a la Carte Foods and Beverages Sold in Schools Executive Summary Introduction The foods
EMBARGOED UNTIL TUESDAY, JUNE 26 AT 12:01 AM EST. Health Impact Assessment National Nutrition Standards for Snack and a la Carte Foods and Beverages Sold in Schools Executive Summary Introduction The foods
Message to Dental Professionals
 BROUGHT TO YOU BY Message to Dental Professionals You educate patients about oral health and hygiene on a daily basis. When discussing the oral health of children ages 0 (birth) to 5, make sure parents
BROUGHT TO YOU BY Message to Dental Professionals You educate patients about oral health and hygiene on a daily basis. When discussing the oral health of children ages 0 (birth) to 5, make sure parents
Linking Research to Clinical Practice
 Linking Research to Clinical Practice Non Fluoride Caries Preventive Agents Denise M. Bowen, RDH, MS The purpose of Linking Research to Clinical Practice is to present evidence based information to clinical
Linking Research to Clinical Practice Non Fluoride Caries Preventive Agents Denise M. Bowen, RDH, MS The purpose of Linking Research to Clinical Practice is to present evidence based information to clinical
Key Dietary Messages
 Key Dietary Messages Developed by Dr. Teresa Marshall, Ph.D Department of Preventive and Community Dentistry College of Dentistry, University of Iowa Dietary Behavior Number of meals/s Meal patterns Between-meal/
Key Dietary Messages Developed by Dr. Teresa Marshall, Ph.D Department of Preventive and Community Dentistry College of Dentistry, University of Iowa Dietary Behavior Number of meals/s Meal patterns Between-meal/
Family Matters in Oral Health
 Family Matters in Oral Health CONNECTING CHILDREN S AND CAREGIVERS DENTAL HEALTH HABITS FEBRUARY 2018 When parents or other caregivers receive dental care, it s good for more than just their own health.
Family Matters in Oral Health CONNECTING CHILDREN S AND CAREGIVERS DENTAL HEALTH HABITS FEBRUARY 2018 When parents or other caregivers receive dental care, it s good for more than just their own health.
PENNSYLVANIA ORAL HEALTH COLLECTIVE IMPACT INITIATIVE
 PENNSYLVANIA ORAL HEALTH COLLECTIVE IMPACT INITIATIVE PA Chapter American Academy of Pediatrics An Initiative supported by the Pennsylvania Head Start Association Your Hosts Lisa Schildhorn, MS Executive
PENNSYLVANIA ORAL HEALTH COLLECTIVE IMPACT INITIATIVE PA Chapter American Academy of Pediatrics An Initiative supported by the Pennsylvania Head Start Association Your Hosts Lisa Schildhorn, MS Executive
The Role of Home Visitors in Improving Oral Health. Oral Health
 The Role of Home Visitors in Improving Oral Health Jenny Kattlove, MS Senior Director of Programs The Children s Partnership Jennifer Byrne, BA Project Manger California Department of Public Health Dr.
The Role of Home Visitors in Improving Oral Health Jenny Kattlove, MS Senior Director of Programs The Children s Partnership Jennifer Byrne, BA Project Manger California Department of Public Health Dr.
Message to Dental Professionals
 BROUGHT TO YOU BY Message to Dental Professionals You educate patients about oral health and hygiene on a daily basis. When discussing the oral health of children ages 0 (birth) to 5, make sure parents
BROUGHT TO YOU BY Message to Dental Professionals You educate patients about oral health and hygiene on a daily basis. When discussing the oral health of children ages 0 (birth) to 5, make sure parents
A guide to dental health for your baby and the family
 Patient information A guide to dental health for your baby and the family Contents Good dental care from the beginning 2 Registration with a dentist 3 Fluoride toothpaste 4 Brushing your child s teeth
Patient information A guide to dental health for your baby and the family Contents Good dental care from the beginning 2 Registration with a dentist 3 Fluoride toothpaste 4 Brushing your child s teeth
HEALTHY SMILE, HAPPY LIFE
 Flyers HEALTHY SMILE, HAPPY LIFE Oral health is part of being well, and the foundation for a healthy and active lifestyle. When our mouths, gums or teeth aren t healthy, our bodies may be more susceptible
Flyers HEALTHY SMILE, HAPPY LIFE Oral health is part of being well, and the foundation for a healthy and active lifestyle. When our mouths, gums or teeth aren t healthy, our bodies may be more susceptible
Thinking About Another Sweet Gulp? Think Again
 Thinking About Another Sweet Gulp? Think Again John Tran University of Illinois at Chicago College of Dentistry ttran50@uic.edu According to a recent Center for Disease Control (CDC) report, more than
Thinking About Another Sweet Gulp? Think Again John Tran University of Illinois at Chicago College of Dentistry ttran50@uic.edu According to a recent Center for Disease Control (CDC) report, more than
Cultural Perspectives of Early Childhood Caries
 Cultural Perspectives of Early Childhood Caries Robert J Schroth, L Harms, J Edwards, ME Moffatt & members of the Manitoba Collaborative Project for the Prevention of Early Childhood Tooth Decay umschrot@cc.umanitoba.ca
Cultural Perspectives of Early Childhood Caries Robert J Schroth, L Harms, J Edwards, ME Moffatt & members of the Manitoba Collaborative Project for the Prevention of Early Childhood Tooth Decay umschrot@cc.umanitoba.ca
Learning Objectives. Nutrition and Oral Health for Children
 Learning Objectives Nutrition and Oral Health for Children Beth Ogata, MS, RD Nutrition 527 April 4, 2006 Describe oral health problems for children List nutrition-related risk factors for oral health
Learning Objectives Nutrition and Oral Health for Children Beth Ogata, MS, RD Nutrition 527 April 4, 2006 Describe oral health problems for children List nutrition-related risk factors for oral health
Alabama Medicaid Agency. 1st Look Program
 Alabama Medicaid Agency 1st Look Program Overview 1 st Look Program goals Qualified Physicians Who qualifies for the program? Billing/Eligible Services Documentation Requirements Referrals Program Contacts
Alabama Medicaid Agency 1st Look Program Overview 1 st Look Program goals Qualified Physicians Who qualifies for the program? Billing/Eligible Services Documentation Requirements Referrals Program Contacts
Pediatric Overweight and Obesity
 Pediatric Overweight and Obesity Cambria Garell, MD Assistant Clinical Professor UCLA Fit for Healthy Weight Program Associate Program Director Pediatric Residency Program Mattel Children s Hospital UCLA
Pediatric Overweight and Obesity Cambria Garell, MD Assistant Clinical Professor UCLA Fit for Healthy Weight Program Associate Program Director Pediatric Residency Program Mattel Children s Hospital UCLA
Dental Care and Health An Update. Dr. Ranjini Pillai, DDS, MPH, FAGD, FICOI
 Dental Care and Health An Update Dr. Ranjini Pillai, DDS, MPH, FAGD, FICOI WHO s Definition of Health? Health is a state of complete physical, mental, and social wellbeing and not merely the absence of
Dental Care and Health An Update Dr. Ranjini Pillai, DDS, MPH, FAGD, FICOI WHO s Definition of Health? Health is a state of complete physical, mental, and social wellbeing and not merely the absence of
Early Childhood Caries in American Indian Children: DISPARITIES & PREVENTION
 Early Childhood Caries in American Indian Children: DISPARITIES & PREVENTION UCSF Dental Public Health Seminar Series, May 10, 2016 Tamanna Tiwari, MPH, MDS, BDS Clinical Instructor School of Dental Medicine
Early Childhood Caries in American Indian Children: DISPARITIES & PREVENTION UCSF Dental Public Health Seminar Series, May 10, 2016 Tamanna Tiwari, MPH, MDS, BDS Clinical Instructor School of Dental Medicine
Community Health Priority: Alcohol & Other Drug Misuse and Abuse
 Alcohol & Other Drug Misuse and Abuse Melissa Dotter, MS Drug Free Communities Coordinator 715.261.1962 melissa.dotter@co.marathon.wi.us Creating a culture in communities where alcohol is used responsibly
Alcohol & Other Drug Misuse and Abuse Melissa Dotter, MS Drug Free Communities Coordinator 715.261.1962 melissa.dotter@co.marathon.wi.us Creating a culture in communities where alcohol is used responsibly
PATIENT INFORMATION DIABETES AND ORAL HEALTH
 PATIENT INFORMATION DIABETES AND ORAL HEALTH www.dentalcareireland.ie DIABETES AND ORAL HEALTH People with poor diabetes control can be more prone to oral health problems such as gum disease, dry mouth,
PATIENT INFORMATION DIABETES AND ORAL HEALTH www.dentalcareireland.ie DIABETES AND ORAL HEALTH People with poor diabetes control can be more prone to oral health problems such as gum disease, dry mouth,
MODULE 15: ORAL HEALTH ACROSS THE LIFESPAN
 MODULE 15: ORAL HEALTH ACROSS THE LIFESPAN Oral Health Across the Lifespan MODULE 15: ORAL HEALTH ACROSS THE LIFESPAN Part 3: Oral Health in Childhood Erin Hartnett DNP, APRN-BC, CPNP Learning Objectives
MODULE 15: ORAL HEALTH ACROSS THE LIFESPAN Oral Health Across the Lifespan MODULE 15: ORAL HEALTH ACROSS THE LIFESPAN Part 3: Oral Health in Childhood Erin Hartnett DNP, APRN-BC, CPNP Learning Objectives
Message to Medical Professionals
 BROUGHT TO YOU BY Message to Medical Professionals You educate patients on health, wellness, and prevention on a daily basis. A vital part of patient education is raising awareness among parents and caregivers
BROUGHT TO YOU BY Message to Medical Professionals You educate patients on health, wellness, and prevention on a daily basis. A vital part of patient education is raising awareness among parents and caregivers
Oral Health Advice. Recovery Focussed Pharmaceutical Care for Patients Prescribed Substitute Opiate Therapy. Fluoride toothpaste approx 1450ppmF
 Recovery Focussed Pharmaceutical Care for Patients Prescribed Substitute Opiate Therapy Oral Health Advice Fluoride toothpaste approx 1450ppmF Choosing the right toothbrush Brief Intervention Oral Health
Recovery Focussed Pharmaceutical Care for Patients Prescribed Substitute Opiate Therapy Oral Health Advice Fluoride toothpaste approx 1450ppmF Choosing the right toothbrush Brief Intervention Oral Health
Dental Health E-presentation.
 Dental Health E-presentation www.healthycornwall.org.uk Learning Outcomes This short E-presentation has been developed to give you a basic understanding of the importance of good dental health and dental
Dental Health E-presentation www.healthycornwall.org.uk Learning Outcomes This short E-presentation has been developed to give you a basic understanding of the importance of good dental health and dental
Healthy Smiles for Young Children
 Healthy Smiles for Young Children Basic Oral Health Care During Pregnancy During Pregnancy: Have a dental checkup. Brush at least twice a day with fluoride toothpaste. Floss daily. Limit sweets and avoid
Healthy Smiles for Young Children Basic Oral Health Care During Pregnancy During Pregnancy: Have a dental checkup. Brush at least twice a day with fluoride toothpaste. Floss daily. Limit sweets and avoid
Secrets Supermoms Know About Their Child s Oral Health
 Secrets Supermoms Know About Their Child s Oral Health Learn how to keep your kids happy, healthy and showing off that bright smile with this handy guide! Contents Chapter 1: Introduction Chapter 2: Supermom
Secrets Supermoms Know About Their Child s Oral Health Learn how to keep your kids happy, healthy and showing off that bright smile with this handy guide! Contents Chapter 1: Introduction Chapter 2: Supermom
KEY INDICATORS OF NUTRITION RISK
 NUTRITION TOOLS KEY INDICATORS OF Consumes fewer than 2 servings of fruit or fruit juice per day. Consumes fewer than 3 servings of vegetables per day. Food Choices Fruits and vegetables provide dietary
NUTRITION TOOLS KEY INDICATORS OF Consumes fewer than 2 servings of fruit or fruit juice per day. Consumes fewer than 3 servings of vegetables per day. Food Choices Fruits and vegetables provide dietary
Course #:
 Welcome to Lesson 7: Indicators of Problems of the Dental Health for Individuals with Disabilities webcast series. Please adjust your computer volume so that it is at a comfortable listening level for
Welcome to Lesson 7: Indicators of Problems of the Dental Health for Individuals with Disabilities webcast series. Please adjust your computer volume so that it is at a comfortable listening level for
U.S. Army Center for Health Promotion & Preventive Medicine
 A Healthy Mouth for Your Baby U.S. Army Center for Health Promotion & Preventive Medicine Directorate of Health Promotion and Wellness Oral Fitness Program Aberdeen Proving Ground Maryland, 21010-5403
A Healthy Mouth for Your Baby U.S. Army Center for Health Promotion & Preventive Medicine Directorate of Health Promotion and Wellness Oral Fitness Program Aberdeen Proving Ground Maryland, 21010-5403
NUTRITION SUPERVISION
 NUTRITION SUPERVISION MIDDLE CHILDHOOD 5 10 YEARS MIDDLE CHILDHOOD Overview Middle childhood (ages 5 to 10) is characterized by slow, steady physical growth. However, cognitive, emotional, and social development
NUTRITION SUPERVISION MIDDLE CHILDHOOD 5 10 YEARS MIDDLE CHILDHOOD Overview Middle childhood (ages 5 to 10) is characterized by slow, steady physical growth. However, cognitive, emotional, and social development
ORAL HEALTH IN PREGNANCY
 ORAL HEALTH IN PREGNANCY Caring for your mouth, teeth and gums is important during pregnancy Healthy Teeth, Happy Smiles! Brush your teeth twice a day and change your toothbrush regularly. Floss every
ORAL HEALTH IN PREGNANCY Caring for your mouth, teeth and gums is important during pregnancy Healthy Teeth, Happy Smiles! Brush your teeth twice a day and change your toothbrush regularly. Floss every
Enhanced CPD Programme Module 2b
 Enhanced CPD Programme Module 2b Introduction Aim To present the key oral health improvement messages and the evidence-base that underpins these for use in practice. Learning Outcomes By the end of this
Enhanced CPD Programme Module 2b Introduction Aim To present the key oral health improvement messages and the evidence-base that underpins these for use in practice. Learning Outcomes By the end of this
Exploring the Association Between Caregivers Oral Health Literacy & Children s Caries Status
 Exploring the Association Between Caregivers Oral Health Literacy & Children s Caries Status David Avenetti, DDS Pediatric Dental Resident MSD and MPH Candidate Penelope Leggott, BDS, MS, Committee Chair
Exploring the Association Between Caregivers Oral Health Literacy & Children s Caries Status David Avenetti, DDS Pediatric Dental Resident MSD and MPH Candidate Penelope Leggott, BDS, MS, Committee Chair
Developed by: The Inter Tribal Council of Arizona, Inc. Dental Clinical and Prevention Support Center
 Inter Tribal Council of Arizona, Inc. Dental Clinical and Prevention Support Center 2214 North Central Avenue, Suite 100 Phoenix, Arizona 85004 602-258-4822 602-258-4825 fax www.itcaonline.com Developed
Inter Tribal Council of Arizona, Inc. Dental Clinical and Prevention Support Center 2214 North Central Avenue, Suite 100 Phoenix, Arizona 85004 602-258-4822 602-258-4825 fax www.itcaonline.com Developed
THESIS. Presented in Partial Fulfillment of the Requirements for the Degree Master of Science in the Graduate School of The Ohio State University
 Identifying Risk Factors Associated with Early Childhood Caries in Children Under Three Years of Age THESIS Presented in Partial Fulfillment of the Requirements for the Degree Master of Science in the
Identifying Risk Factors Associated with Early Childhood Caries in Children Under Three Years of Age THESIS Presented in Partial Fulfillment of the Requirements for the Degree Master of Science in the
Parental Attitudes and Tooth Brushing Habits in Preschool Children in Mangalore, Karnataka: A Cross-sectional Study
 10.5005/jp-journals-10005-1210 Fawaz Pullishery et al RESEARCH ARTICLE Parental Attitudes and Tooth Brushing Habits in Preschool Children in Mangalore, Karnataka: A Cross-sectional Study Fawaz Pullishery,
10.5005/jp-journals-10005-1210 Fawaz Pullishery et al RESEARCH ARTICLE Parental Attitudes and Tooth Brushing Habits in Preschool Children in Mangalore, Karnataka: A Cross-sectional Study Fawaz Pullishery,
Complimentary Feeding
 Modifiable Protective & Risk Factors Associated with Overweight and Obesity Birth through age 5 Complimentary Feeding Jose M. Saavedra, MD, Chief Medical Officer Nestlé Nutrition & Associate Professor
Modifiable Protective & Risk Factors Associated with Overweight and Obesity Birth through age 5 Complimentary Feeding Jose M. Saavedra, MD, Chief Medical Officer Nestlé Nutrition & Associate Professor
WASHINGTON STATE COMPARISONS TO: KITSAP COUNTY CORE PUBLIC HEALTH INDICATORS May 2015
 WASHINGTON STATE COMPARISONS TO: KITSAP COUNTY CORE PUBLIC HEALTH INDICATORS This is a companion document to the Core Public Health Indicators that provides a comparison of to Washington State for the
WASHINGTON STATE COMPARISONS TO: KITSAP COUNTY CORE PUBLIC HEALTH INDICATORS This is a companion document to the Core Public Health Indicators that provides a comparison of to Washington State for the
Workshop on Understanding the Relationship Between Food Insecurity and Obesity Sentinel Populations November 16, 2010
 Workshop on Understanding the Relationship Between Food Insecurity and Obesity Sentinel Populations November 16, 2010 Rural Populations Christine M. Olson, Cornell University Definitions of Rural Rural
Workshop on Understanding the Relationship Between Food Insecurity and Obesity Sentinel Populations November 16, 2010 Rural Populations Christine M. Olson, Cornell University Definitions of Rural Rural
INSTRUCTOR S GUIDE. Oral Health. First Edition, 2006
 INSTRUCTOR S GUIDE Oral Health First Edition, 2006 California Childcare Health Program Administered by the University of California, San Francisco School of Nursing, Department of Family Health Care Nursing
INSTRUCTOR S GUIDE Oral Health First Edition, 2006 California Childcare Health Program Administered by the University of California, San Francisco School of Nursing, Department of Family Health Care Nursing
PHACS County Profile Report for Searcy County. Presented by: Arkansas Center for Health Disparities and Arkansas Prevention Research Center
 PHACS County Profile Report for Searcy County Presented by: Arkansas Center for Health Disparities and Arkansas Prevention Research Center Contents Introduction... Page 2 Demographics...Page 3 Social Environment
PHACS County Profile Report for Searcy County Presented by: Arkansas Center for Health Disparities and Arkansas Prevention Research Center Contents Introduction... Page 2 Demographics...Page 3 Social Environment
Childhood Obesity Epidemic- African American Community
 Childhood Obesity Epidemic- African American Community Link D Juanna Satcher MD MPH Assistant Professor of Pediatrics Baylor College of Medicine Gulf Coast Apollo Chapter Objectives Summarize obesity rates
Childhood Obesity Epidemic- African American Community Link D Juanna Satcher MD MPH Assistant Professor of Pediatrics Baylor College of Medicine Gulf Coast Apollo Chapter Objectives Summarize obesity rates
RISK FACTORS BY AGE (Wandera et al. 2000)
") RISK ASSESSMENT Stacey Lubetsky DMD ST. BARNABAS HOSPITAL RISK ASSESSMENT The primary thrust of early risk assessment is to screen for parent-infant groups who are at risk of ECC and would benefit from
RISK ASSESSMENT Stacey Lubetsky DMD ST. BARNABAS HOSPITAL RISK ASSESSMENT The primary thrust of early risk assessment is to screen for parent-infant groups who are at risk of ECC and would benefit from
HEALTH SURVEILLANCE INDICATORS: YOUTH ORAL HEALTH. Public Health Relevance. Highlights
 HEALTH SURVEILLANCE INDICATORS: YOUTH ORAL HEALTH Public Health Relevance Good dental and oral health contribute to physical, mental and social well-being. Tooth decay, especially untreated dental caries,
HEALTH SURVEILLANCE INDICATORS: YOUTH ORAL HEALTH Public Health Relevance Good dental and oral health contribute to physical, mental and social well-being. Tooth decay, especially untreated dental caries,
Message to Educators HOW TO USE THESE MATERIALS
 BROUGHT TO YOU BY Message to Educators As someone who works with children, you know how a child s smile can brighten your day. Yet parents may not always make the connection between oral health, overall
BROUGHT TO YOU BY Message to Educators As someone who works with children, you know how a child s smile can brighten your day. Yet parents may not always make the connection between oral health, overall
A Few SoundBites on Diet, Nutrition and Oral Health
 A Few SoundBites on Diet, Nutrition and Oral Health Carole A. Palmer EdD, RD Tufts University: School of fdental lmedicine i Friedman School of Nutrition Science and Policy Conflict of Interest Disclosure
A Few SoundBites on Diet, Nutrition and Oral Health Carole A. Palmer EdD, RD Tufts University: School of fdental lmedicine i Friedman School of Nutrition Science and Policy Conflict of Interest Disclosure
Prevalence, Trends and Disparities in Beverage Consumption Among Young Children aged 0-24 months from NHANES
 Prevalence, Trends and Disparities in Beverage Consumption Among Young Children aged 0-24 months from NHANES Anna Maria Siega-Riz, PhD Professor of Public Health Sciences and Obstetrics and Gynecology
Prevalence, Trends and Disparities in Beverage Consumption Among Young Children aged 0-24 months from NHANES Anna Maria Siega-Riz, PhD Professor of Public Health Sciences and Obstetrics and Gynecology
Healthy Smiles for Young Children
 Healthy Smiles for Young Children During Pregnancy: Have a dental checkup. Brush at least twice a day with fluoride toothpaste. Floss daily. Limit sweets and avoid sticky foods. Visit your doctor for pre-natal
Healthy Smiles for Young Children During Pregnancy: Have a dental checkup. Brush at least twice a day with fluoride toothpaste. Floss daily. Limit sweets and avoid sticky foods. Visit your doctor for pre-natal
Visit DeltaDentalMN.org/SmilesAtSchool for additional program materials, including educational videos, activities and lesson plans.
 Smiles@School is a statewide initiative of Delta Dental of Minnesota Foundation to support children s oral health through education, prevention and dental sealant programs in schools. Education is the
Smiles@School is a statewide initiative of Delta Dental of Minnesota Foundation to support children s oral health through education, prevention and dental sealant programs in schools. Education is the
Meeting the Oral Health Needs of Children
 Meeting the Oral Health Needs of Children Shelly Gehshan Director Advancing Children s Dental Health Initiative The Pew Center on the States 1 Why Does Oral Health Matter? Poor oral health can affect a
Meeting the Oral Health Needs of Children Shelly Gehshan Director Advancing Children s Dental Health Initiative The Pew Center on the States 1 Why Does Oral Health Matter? Poor oral health can affect a
Beverage Guidelines: 1 up to 3 Years
 Beverage Guidelines: nutritionally-equivalent nondairy beverages like soy, rice, or lactose-free milks with medical permission). nutritionally-equivalent nondairy beverages like soy, rice, or lactose-free
Beverage Guidelines: nutritionally-equivalent nondairy beverages like soy, rice, or lactose-free milks with medical permission). nutritionally-equivalent nondairy beverages like soy, rice, or lactose-free
Diet and tooth decay Prevention
 Diet and tooth decay Prevention Santa Clara County Dental Society Indian Health Center San Jose Gardner Family Health Network WHAT IS TOOTH DECAY? WHAT IS A CAVITY? Tooth decay or a cavity of dental caries
Diet and tooth decay Prevention Santa Clara County Dental Society Indian Health Center San Jose Gardner Family Health Network WHAT IS TOOTH DECAY? WHAT IS A CAVITY? Tooth decay or a cavity of dental caries
Risk indicators for dental caries using the International Caries Detection and Assessment System (ICDAS)
") Community Dent Oral Epidemiol 2008; 36: 55 68 All rights reserved Ó 2007 The Authors. Journal compilation Ó 2007 Blackwell Munksgaard Risk indicators for dental caries using the International Caries Detection
Community Dent Oral Epidemiol 2008; 36: 55 68 All rights reserved Ó 2007 The Authors. Journal compilation Ó 2007 Blackwell Munksgaard Risk indicators for dental caries using the International Caries Detection
Feature Article. An Oral Health Education Program for Latino Immigrant Parents
 Feature Article An Oral Health Education Program for Latino Immigrant Parents Ruth M. Brown, RN, MSN; Daryl Canham, RN, EdD, C; and Virginia Young Cureton, RN, DrPH ABSTRACT: A high prevalence of dental
Feature Article An Oral Health Education Program for Latino Immigrant Parents Ruth M. Brown, RN, MSN; Daryl Canham, RN, EdD, C; and Virginia Young Cureton, RN, DrPH ABSTRACT: A high prevalence of dental
11 surprising things that promote tooth decay
 11 surprising things that promote tooth decay Originally published: June 18, 2014 9:49 PM Updated: June 23, 2014 1:33 PM Copyright 2014 Newsday. All rights reserved. Mothers near and far have long told
11 surprising things that promote tooth decay Originally published: June 18, 2014 9:49 PM Updated: June 23, 2014 1:33 PM Copyright 2014 Newsday. All rights reserved. Mothers near and far have long told
Oral Health Care During Pregnancy
 Oral Health Care During Pregnancy Prepared by National Maternal and Child Oral Health Resource Center Georgetown University Research to Policy and Practice Forum: Periodontal Health and Birth Outcomes
Oral Health Care During Pregnancy Prepared by National Maternal and Child Oral Health Resource Center Georgetown University Research to Policy and Practice Forum: Periodontal Health and Birth Outcomes
Epidemiologic Study of Dental Caries Experience and
 Epidemiologic Study of Dental Caries Experience and Between-Meal Eating Patterns R. A. BAGRAMIAN and A. L. RUSSELL School of Dentistry, University of Michigan, Ann Arbor, Michigan 48104, USA The relationship
Epidemiologic Study of Dental Caries Experience and Between-Meal Eating Patterns R. A. BAGRAMIAN and A. L. RUSSELL School of Dentistry, University of Michigan, Ann Arbor, Michigan 48104, USA The relationship
A Healthy Mouth for Your Baby
 A Healthy Mouth for Your Baby U.S. DEPARTMENT OF HEALTH AND HUMAN SERVICES National Institutes of Health Healthy teeth are important even baby teeth. Children need healthy teeth to help them chew and to
A Healthy Mouth for Your Baby U.S. DEPARTMENT OF HEALTH AND HUMAN SERVICES National Institutes of Health Healthy teeth are important even baby teeth. Children need healthy teeth to help them chew and to