APOSTILA(DE(ARTIGOS( ( WEBINAR( INSTALAÇÃO*DE*IMPLANTES*NA*REGIÃO*POSTERIOR*DE* MAXILA*COM*POUCA*DISPONIBILIDADE*ÓSSEA* * * * * * * * * * * * * * * *
|
|
|
- Laureen Horton
- 5 years ago
- Views:
Transcription



1 APOSTILA(DE(ARTIGOS( ( WEBINAR( INSTALAÇÃO*DE*IMPLANTES*NA*REGIÃO*POSTERIOR*DE* MAXILA*COM*POUCA*DISPONIBILIDADE*ÓSSEA* * * * * * * * * * * * * * * * * * DR.(EDUARDO(DIAS( 2015(


2 CONTINUING EDUCATION 34 SELECTION AND IDEAL TRIDIMENSIONAL IMPLANT POSITION FOR SOFT TISSUE AESTHETICS André P. Saadoun, DDS, MS* Marcel LeGall, DDS* Bernard Touati, DDS, DSO SAADOUN While single-tooth replacement can be accomplished with predictability using implant therapy, this procedure is challenging in the anterior region where numerous criteria must be evaluated by the restorative team. The available height of bone, soft tissue volume, and threedimensional position of the anticipated implant restoration are among the numerous concerns that must be addressed prior to the initiation of treatment. This article provides a comprehensive review for the selection and placement of implants in the aesthetic region and illustrates these principles with a case presentation. Key Words: implant, aesthetic, provisional, soft tissue, emergence profile The single-unit implant-supported restoration has proven to be an efficacious means of replacing a missing tooth. 1 Although this procedure appears simple to perform, the restoration of an anterior tooth particularly a maxillary central incisor is quite challenging. In order to be considered successful, an implant-supported restoration must achieve a harmonious balance between functional, aesthetic, and biological imperatives. This concept has resulted in the development of restoration-driven implant placement, 2 in which implants are positioned in relation to the anticipated requisites of the restorative phase rather than the availability of bone. Restoration-driven implant therapy often requires the development of an adequate volume of osseous structure to support the implant and the soft tissue to sculpt the prosthetic site. This restoration-generated site development presumes that the three-dimensional configuration of the prosthesis will affect the anatomical form and tone of the free gingival margin. If implant selection and placement are dictated by the definitive crown, then the healing and maturation of the soft tissues are guided by the placement of the provisional restoration at stage II to promote ideal scalloping and papillae reformation according to the double-guidance concept. 3 As the ceramic crown emerges from the implant, it should support the most coronal 4 mm of the soft tissue including the free gingival margin of the restorationgingival interface. The components of the aesthetic profile comprise the osseous, gingival, and restorative triad and their relationship to the adjacent dentition. The critical interdependence of these three components and the necessity of systematic reconstruction of the deficiencies within the triad cannot be underestimated if aesthetic results are to be achieved with consistency mm 2.5 mm 11 9 NOVEMBER/DECEMBER *Private practice, Paris, France. Editor-in-Chief, Practical Periodontics & Aesthetic Dentistry; private practice, Paris, France. André P. Saadoun, DDS, MS 12 Avenue Paul Doumer Paris, France Tel: (011) Fax: (011) andre.p.saadoun@wanadoo.fr 4.3 mm 3.6 mm 8.6 mm 5 mm Figure 1. Diagram of ideal tooth/bone relationship with optimal interdental alveolar bone. Pract Periodont Aesthet Dent 1999;11(9):

.")
. Surgical procedures involved in ridge augmentation. Failure to consider these factors will compromise the aesthetic result.")
3 Practical Periodontics & AESTHETIC DENTISTRY The hard tissue, however, remains the principal determinant of the aesthetic outcome. Therefore, successful and predictable results can be accomplished if the optimal osseous dimension is initially reconstructed to achieve implant stability and to support the optimal gingival contours that, consequently, can sustain the development of an aesthetic restorative profile. 5 Prior to implant placement, the following factors should be analyzed by the implant team: Type of smile (ie, high, medium, or low). Biotype of adjacent periodontium (quality and quantity of keratinized gingiva). Osseous topography of the edentulous ridge (Seibert s Class I, II, or III). Anticipated form, position, and type of restoration (screwed or cemented). Surgical procedures involved in ridge augmentation. Failure to consider these factors will compromise the aesthetic result. 6 Figure 2. Diagram indicates that the minimum interproximal bone between two adjacent implants should not be less than 3 mm and 2 mm from the adjacent teeth. Buccal convexity 1.8 mm 4.3 mm 2.5 mm 3.6 mm 2 mm 8.6 mm 2 mm + implant radius Implant Selection, Position, and Angulation As the objective of implant treatment is the accurate replication of the natural dentition, 7 it is critical to possess an understanding of crown and root anatomy (Figure 1). Since the placement of the implant within the edentulous space significantly impacts the functional, periodontal, and aesthetic result, the implant must be perfectly aligned with the anticipated restoration, adapted to the site, and positioned in the tridimensional space. Implant Selection Since the implant replaces the root of the missing tooth, the transition between the properly sized implant and the anatomic crown must be harmonious in order to establish an aesthetic emergence profile. To determine the shape and width of the crown to be replaced, the dimensions of the contralateral tooth should be analyzed and the root size and anatomy at the level of implant placement should be evaluated. Implant diameter is dictated by the corresponding root anatomy at the crest of bone. Under normal conditions, the crest of bone appears to be 1.5 mm to 2 mm apical to the crest of the cementoenamel junction (CE J) of the extracted tooth or adjacent teeth. Following the determination of crown/root size, interdental crest width, and periodontal prerequisites, an implant of corresponding dimensions can be selected to provide a natural emergence profile for an aesthetic restoration (Table). G.M. Level Bone level Crown enamel Figure 3. Diagram demonstrates ideal positioning of an implant buccopalatally. Too buccally Optimal Too palatally Figure 4. Illustration of optimal implant position on the buccopalatal axis Vol. 11, No. 9
4 Saadoun Table Implant Recommendation Based on Crown/Root Diameter of Maxillary Teeth Mesiodistal at Mesiodistal at Buccolingual at Mesiodistal Cementoenamel Cementoenamel Cementoenamel Recommended Tooth (mm) Crown Junction Junction 2 mm Junction Implant (mm) Central incisor , 4.3, 5.0 Lateral incisor , 3.5 Canine , 4.3 First premolar , 4.3 Second premolar , 4.3 First molar , 4.3, 5.0, 6.0 Second molar , 4.3, 5.0, 6.0 Angulation Angulation refers to the proper orientation of an implant in three-dimensional space (ie, mesiodistal, buccolingual, apicocoronal). 8 In addition, the exact rotation of the hexagon can be regarded as the fourth dimension the flat surface of the hexagonal implant should be parallel to the buccocortical plate to allow optimal positioning whenever an asymmetrical prosthetic abutment is utilized. In order to ensure proper implant angulation, a surgical template should be utilized to transfer prosthetic parameters (eg, tooth position, emergence profile, gingival margin, arch form, vertical dimension) to the surgical site. Mesiodistal Placement According to Adell et al, 9 an implant with a diameter of 4.1 mm requires a minimum mesiodistal space of 7 mm between two adjacent teeth (ie, 4.1 mm for the implant and 1.5 mm of clearance on each side). The mesiodistal position of the implant, however, also depends on the coronal and cervical width of the replaced tooth, the proximity of the adjacent roots, and the presence or absence of diastemata. The mesiodistal implant axis should pass by the center of the future crown and the bisecting line angle of the adjacent roots. Moreover, a direct relationship exists between the height of the interproximal bone and the height and shape of the papillae. 10 In order to develop and/or maintain the integrity of the interdental papillae, a distance of 2 mm at the cervical implant level is suggested as appropriate between an implant and the adjacent teeth; this distance should be a minimum of 3 mm between two implants. 11 If the interproximal distance between tooth/implant and two implants is less, horizontal bone loss will occur and increase the vertical distance between the remaining crestal bone and the apical proximal contact of the adjacent crowns. Consequently, this phenomenon jeopardizes the existence or may prevent the formation of the interdental papilla, which compromises the definitive aesthetic result. All this information should allow the selection of the proper implant diameter by subtraction (Figure 2). Faciolingual Placement This orientation varies with the type of restoration connection (ie, screwed or cemented). This placement determines the proximal dimensions of the crown and its anticipated aesthetic appearance. Occlusally, the collar of the implant should remain inside the virtual line that connects the incisal borders of the adjacent teeth. Cervically, the longitudinal axis of the implant should be 4 mm inside the cervical envelope of the adjacent teeth and the external implant collar surface should be 2 mm from the buccal contour of the adjacent teeth (Figure 3). 1,8 If the implant axis is aligned with the axis of the restoration, the crown height is the same as that of the tooth it replaces (Figure 4). If the implant axis has a palatal inclination, the crown exhibits a facial ridge lap that impairs proper hygiene. In order to achieve an acceptable aesthetic result, a palatally positioned implant should generally be placed to a greater apical extent. For every 1 mm of palatal positioning, the implant should be placed an additional 1 mm apically. 12 If the implant axis exhibits a facial inclination, the implant emergence is located coronally to the cervical contour of the adjacent teeth. This results in an excessively long crown, and the collar is misaligned with that of the adjacent contralateral tooth. 13 In order to prevent a buccal angulation and an improper implant/crown ratio and occlusal relationship, it is recommended to orient the implant 5 palatally and to place the implant closer to the palatal cortical aspect. This also prevents and/or limits the premature resorption of the buccocortical plate, which may occur in instances where it is too thin. 9 PPAD 1065


5 Practical Periodontics & AESTHETIC DENTISTRY Day 1 implant placement 1 year postoperatively C.T.A. 1.2 mm J.E. 1 mm Sulcus: 1 mm C.T.A. 1.5 mm J.E. 1.5 mm Sulcus: 1 mm Biological width 2 mm Biological width 3 mm Figure 5. Diagram of apicocoronal position at implant placement following tooth extraction and 1 year postoperatively. Apicocoronal Placement The exact apicocoronal location of the implant shoulder is dependent upon the cervical bone resorption morphology, the diameter of the implant, the size discrepancy between the root and the diameter of the implant, the thickness of the marginal gingiva, and the proximal tissue. The implant collar should be 2 mm apical to the line of CEJ of the neighboring tooth if no gingival recession is evident and 3 mm from the gingival margin when gingival recession is present. Consequently, the optimal reference line in all instances is not the CEJ, but the buccogingival contour. 14 The implant should be at a maximum of 3 mm from the gingival margin displayed in the surgical guide or on the adjacent teeth (Figure 5) to allow space for the crown to emerge from a round implant to a triangular emergence profile and for the development of the biological volume. 15 If the discrepancy between the tooth and the implant diameter increases, the implant shoulder must be placed more apically to achieve an aesthetically acceptable emergence profile. The height of soft tissues determines the length available for the emergence profile. Long-term peri-implant considerations, however, dictate that the sulcus should remain shallow. While soft tissue heights of less than 2 mm are challenging for aesthetic restoration, a height of more than 4 mm establishes satisfactory aesthetics but has been noted to result in a deep sulcus with long-term soft tissue complications mm Day 1 insertion Gingival recession 0.7 mm to 1 mm Bone resorption 0.9 mm to 1.6 mm 1 year postoperatively C.A. 1.5 mm J.E. 1.5 mm S.D. 1 mm Figure 6. Relationship of biological volume and gingival margin on submerged implant at insertion and 6 months following the subsequent abutment connection. If the position is too apical, it will subsequently result in the formation of an infrabony defect, a peri-implant pocket, complications in the second phase, difficulty at abutment connection, and excess cement at seating of the restoration. If the position is too occlusal, it can induce by vertical overcontour pressure a recession of the soft tissue, a limitation in the emergence profile, and an unaesthetic result. A more ideal emergence profile can be obtained when the diameter of the implant is similar to the diameter of the tooth to be replaced. 17 Therefore, the elimination of the variations in apicocoronal implant placement, due to emergence profile considerations and periodontal defects, can be obtained with a properly selected implant diameter Vol. 11, No. 9
. Figure 7. Orthodontic treatment can be utilized to develop or improve implant sites (as depicted for appropriate mesiodistal placement). Figure 8.")

6 Saadoun necessary to augment the hard and soft tissue and place the implant platform at 3 mm to maintain the 4 mm of soft tissue required to allow the development of an adequate emergence profile and obtain an optimal aesthetic result (Figure 6). Figure 7. Orthodontic treatment can be utilized to develop or improve implant sites (as depicted for appropriate mesiodistal placement). Figure 8. Buccal view of implant-supported restoration. Soft tissue integration has been prepared by the provisional restoration placed at implant exposure. Since the biological height in submerged implants is approximately 3 mm and the sulcus depth 1 mm, 18 it is critical to position the platform of the implant in relation to these biological dimensions. It is also important to consider that the majority of the submerged implants lose approximately 0.9 mm to 1.6 mm of crestal bone during the first year of function. 19 Care should also be taken to maintain or reestablish a minimum of 2 mm of buccal bone thickness. 9 The apicocoronal position of the implant and its long-term gingival marginal stability is dictated by the balance between the crestal level of bone, the biological height of the junctional epithelium and connective attachment (at implant placement and 1 year postoperatively), and the sulcus depth. It is therefore Occlusal Considerations Obtaining and maintaining a nontraumatic occlusal relationship with the opposing dentition is a decisive factor in preserving osseointegration and, consequently, the aesthetics of the implant prosthesis. In the authors experience, if the occlusal forces developed between the prosthetic occlusal surfaces are excessive axially or laterally, they may induce cervical bone loss around the implant collar, increase the gingival recession, or compromise the gingival level and the definitive aesthetic result. 20 In order to accommodate axial forces during function, an aesthetic implant position and orientation must consider the future occlusal relation with the opposing dentition. This can be achieved by aligning the implant axis as close as possible to the one of the opposing teeth. The palatal orientation of a maxillary anterior implant is more favorable than a buccal position, which considerably increases the lateral forces to be dissipated on a thin buccal bone. In addition, an appropriate accommodation for axial forces can be made by avoiding an unfavorable vertical ratio between the prosthetic crown and the osseointegrated portion of the implant by limiting the prosthetic overbite and overjet and by establishing a nontraumatic occlusal relation during maximum intercuspidation, incision, and mastication. This correct axis could be achieved by reestablishing the normal bone morphology prior to or in conjunction with implant placement. Soft Tissue Management In order to achieve natural soft tissue aesthetics, the contour, height, and width of the gingiva at the implant site must correspond to the soft tissues that surround the adjacent natural teeth. Adequate bone must exist for placement of the implant, along with proper soft tissue framing that consists of interproximal papillae and an adequate zone of attached gingiva with the potential for tissue augmentation. The status of the gingiva must be evaluated for the diagnosis and treatment planning in order to determine its quantity, quality, color, texture, and biotype (ie, scalloped or flat). It is also a prerequisite to measure the thickness of the gingiva that encompasses the maxilla (ie, buccal 1 mm to 2 mm; palatal 3 mm to 4 mm) and the mandible (ie, buccal and lingual 1 mm). This PPAD 1067



7 Practical Periodontics & AESTHETIC DENTISTRY examination allows the restorative team to decide if keratinized peri-implant gingiva is adequate for a single-unit implant restoration in the aesthetic zone. Although the presence of alveolar mucosa free of inflammation around the submerged implant does not appear to be required for long-term osseointegration, 9 the presence of a band of keratinized gingiva appears to be conducive to the establishment and maintenance of aesthetics. Recession can be prevented by keratinized gingiva, which may be less sensitive to tooth brushing than the alveolar mucosa. While keratinized tissue is no less sensitive to inflammation, it is less likely to recede due to its thickness, which can also conceal the metallic appearance of the corresponding abutment. The presence of keratinized gingiva is not sufficient in itself to ensure an aesthetic result postoperatively, but it is a prerequisite to achieve this objective. Sufficient hard tissue must be present, however, to support the 4 mm of soft tissue that is required to develop and maintain the biologic width around implants. In order to develop a natural emergence profile for the definitive restoration, it is essential if soft tissue is at an adequate level or deficient to increase the keratinized tissue. It is necessary to overcontour the soft tissues by a minimum of 2 mm to 3 mm, as they tend to recede by 1 mm during surgical and restorative procedures. 21 The guideline for this level is an imaginary line drawn from the papillary height to the papillary height of the proximal teeth. 22 Due to 1 mm of soft tissue recession that occurs in the 6 months following implant exposure, tissue volume must be increased by an additional 20% to achieve an aesthetic gingival marginal contour around a restoration to prevent marginal level discrepancies between adjacent teeth. 11 Consequently, the primary objectives in the restoration of gingival aesthetics are to establish an excess of hard and soft tissues, to compensate for future resorption, and to fabricate a restoration that will dictate the shape and form of the gingiva. This overcontouring of the tissues can be performed prior to stage I surgery or through hard and soft tissue augmentation at implant insertion. Soft tissue augmentation procedures can also be utilized 3 to 4 months following implant placement and after implant exposition with a connective tissue graft or a roll technique. At every surgical phase, the possibility of using connective tissue grafting should be evaluated and potentially performed to prepare for the aesthetic emergence profile with limited incision or gingivoplasty and provisional restoration guidance. When the definitive restoration has been completed, however, the surgical potential of aesthetic tissue management is severely limited. 23 Figure 9. Occlusal view of definitive metal-ceramic implant-supported crown restoration (Laboratory: Jean-Marc Etienne, MDT). Figure 10. Facial view of two unaesthetic restorations on the central incisors following initial periodontal preparation. Figure 11. Surgical stent with the pilot drill in place in the socket following atraumatic extraction Vol. 11, No. 9
 and healing abutments.")

 or by immediate implant")
8 Saadoun Figure 12. Occlusal view demonstrates immediate placement of 5 mm abutments (Bioesthetic, Nobel Biocare, Yorba Linda, CA). Figure 13. Postoperative retroalveolar radiograph demonstrates the optimal connection between implants (Replace, Nobel Biocare, Yorba Linda, CA) and healing abutments. In certain instances, orthodontics may be utilized to provide an alternative solution (Figures 7 through 9). This can be achieved when the root socket is moved coronally to allow bone regeneration in the defect. The resultant modification in soft tissue topography is concomitant with the change in the osseous configuration. The proximal papilla can be preserved at implant placement by excluding them from the flap design using two proximal divergent incisions (although healing scars could remain) or by immediate implant placement after extraction without flap elevation through sulcular incision. Implant exposure is more complex to realize in the aesthetic area. Uncovering the implant can be accomplished by using the palatal flap design or by using a soft tissue punch to minimize tissue reflection. The soft tissue punch is primarily indicated when adequate keratinized attached gingiva and intact papillae are present to achieve optimal soft tissue architecture. 24 Gradual tissue expansion can be performed with a small abutment and then the provisional restoration at the subsequent treatment stage to transfer the gingival margin to the master model. The expansion ensures that restorative dimensions are increased progressively below the gingival tissues to provide for a proper emergence profile and to establish contours that are aesthetic and conductive to hygiene procedures. 5 Immediate placement of the implant in a singlestage surgery should be considered when the tooth to be replaced is still in the socket because the potential of successful peri-implant tissue management is optimal. The implant and a contoured healing abutment can also be placed in a single-stage approach to facilitate margin closure, maintain ideal soft tissue morphology, and prevent soft tissue collapse. 25 As this one-stage surgical approach also minimizes surgical trauma and decreases the duration of treatment, this procedure has a significant role in the soft tissue development and restoration of the site. The use of a one-stage nonsubmerged implant with an anatomical healing abutment (eg, Bioesthetic, Nobel Biocare, Yorba Linda, CA) can also achieve a proper three-dimensional fit that may aid in the support and shaping of the gingival tissues (Figures 10 through 13). Figure 14. Facial view of marginal gingival contour after removal of both abutments. Note the scalloping of the tissue and maintenance of the central interdental papilla. Provisionalization and Prosthetic Stage The patient s goal for treatment is not the implant placement itself, but the functional and aesthetic restoration. Since aesthetics is critical, the placement of a customized provisional restoration allows the tissue to heal in the exact cervical contour and emergence profile of the definitive PPAD 1069



9 Practical Periodontics & AESTHETIC DENTISTRY prosthesis. When the soft tissues are not adapted to the provisional restoration, the incision should facilitate delicate exposure to provide for any necessary augmentation or adjustment of soft tissue defects (Figures 14 through 16). All biological, functional, and aesthetic objectives must be achieved in the provisional phase prior to the placement of the definitive restoration. The objective of the prosthetic phase is to use a provisional restoration that has the optimal form of the desired restoration to develop the restorative gingival interface and the prospective prosthetic recipient site. Once the soft tissues have been molded by the refined provisional crown and have become stable following 6 months of healing, the subgingival peri-prosthetic envelope is transferred to the final laboratory model using a customized impression coping, flowable composite resin, and lowviscosity polyvinylsiloxane according to the prototype duplication concept. 5 A well-adapted cervical contoured metal-ceramic abutment is subsequently screwed to the implant, and the definitive ceramic restoration is cemented (Figures 17 and 18). Discussion An understanding of the biological variables and periodontal implications enables the precise selection and placement of the implant and the determination of the timed sequences of peri-implant tissue management. A correlation between marginal bone loss at adjacent teeth and the horizontal distance between the implant and the tooth has been established by radiological evaluation. As this distance is decreased, bone loss is increased particularly in the lateral maxillary incisor region. 26 With a horizontal distance of 0 mm to 1 mm, the average vertical bone loss was 2.22 mm postoperatively and 0.14 mm 1 year following the placement of the crown restoration (Figure 19). A positive correlation between the interproximal distance and the presence of infrabony pockets has also been noted. The frequency of infrabony pocketing is higher with increasing interdental distance. 27 Two infrabony pockets in the same region were present only if the interdental distance was greater than 3.1 mm. When the distance exceeded 4.6 mm, no further increase of infrabony pocket frequency was observed (Figure 20). Therefore, crestal bone loss increases by 1 mm when the interdental distance between two implants is equal to or less than 3 mm, 11 and less than 2 mm between the implant and the adjacent tooth. 26 Consequently, it would be necessary to maintain a minimum of 2 mm of bone between the implant collar Figure 15. The prosthetic abutments (Bioesthetic, Nobel Biocare, Yorba Linda, CA) are subsequently screwed in correct orientation. Figure 16. Facial view of nonfunctional provisional composite restorations at insertion 6 weeks following surgery (Laboratory: Marc Leriche, CDT). Figure 17. Customized metal-ceramic abutments were screwed onto the implants Vol. 11, No. 9



10 Saadoun Figure 18. Postoperative facial view of the definitive implantsupported restorations. Note the buccogingival contour, the height, and the position of the central proximal papilla. 2.4 mm 1.2 mm 1 mm Figure 19. Illustration of interproximal bone resorption 1 year following implant placement. Day 1 insertion Interproximal implant distance > 3.1 mm 2 mm 1 year postoperatively Vertical bone loss Infrabony defect Figure 20. Diagram of implant in site with 3.1 mm of proximal bone at placement and 1 year postoperatively. Note the two shallow infrabony defects present. and the proximal cervical surface of the adjacent teeth and provide a minimum of 3 mm of bone between the lateral surfaces of two adjacent implants. 11 Implant diameter selection would then be determined by the interproximal distance, which can be observed on well-aligned natural teeth with healthy periodontia. The vertical aspect of implant placement should be established 3 mm apical of the anticipated buccogingival margin. It has been demonstrated that the crestal peri-implant bone changes around submerged and nonsubmerged implants were not significantly different following a period of osseointegration and abutment connection. 28 With nonsubmerged implants, the greatest bone loss occurred immediately after implant placement; bone levels remained consistent following the osseointegration period. Using submerged implants, minimal bone loss was evident following insertion and osseointegration. Following reentry surgery and attachment of the transmucosal abutment, additional bone resorption had occurred. The rate of peri-implant bone loss was similar to the trends documented during the postsurgical healing period. When the coronal extent of the soft tissue and the bone level around the submerged and nonsubmerged implants were compared, no statistically significant differences were detected. The apical extension of the epithelium and the quantity of connective tissue, however, did differ between implant types. In submerged implants, the apical extension of the epithelium was always located below the implant-abutment gap, which resulted in a greater connective tissue contact at the implant surface. It was speculated that this apical position of the junctional epithelium was the result of microbiological contamination by microleakage and/or micromovements. In contrast, the connective tissue surrounding the nonsubmerged implants resembled the dimensions of the natural dentition. The combined epithelium and connective tissue contact was 2.95 mm on the submerged implant and slightly greater than the 2.62 mm observed on nonsubmerged implants. 18 The interproximal height of bone and the presence or absence of a full papilla are related to each other and contribute to the definitive aesthetic outcome. The distance between the bone crest and apical contact point between the teeth or crown restorations should not exceed 5 mm. 10 These values can be applied as a guide for the bone regeneration process and the restorative phase in implant patients with anatomical deficiencies. Consequently, the level of the bone itself due to the expected resorption must be increased by 2 mm in order to support the gingival margin and the interproximal papilla PPAD 1071
11 Practical Periodontics & AESTHETIC DENTISTRY that are necessary for aesthetic development. The flat regenerated marginal bone could be reshaped in subsequent stages to establish a normal scalloping prior to implant placement. In addition, the soft tissue generally recedes at each stage of implant surgery. The buccal recession of the gingival margin three months following abutment connection in first- or second-stage surgery reaches 0.75 mm at six months and 0.90 mm at one year. 11 Therefore, the soft tissue should be overcontoured during the provisional phase (approximately 6 months following abutment connection surgery) which, along with keratinized soft tissue attachment around the implant site, have been proven to be necessary to establish a stable long-term gingival margin. Conclusion The development and maintenance of the aesthetic hard and soft tissue complex are important particularly when implant treatment is performed in the aesthetic zone. The site selected for the implant must be guided in the mesiodistal, apicocoronal, and buccolingual dimensions by the anticipated restoration. The essence of any aesthetic implant restoration remains the initial site development. 29 The volume of the osseous support must allow the implant to be placed in the ideal situation, while the soft tissue morphology must mimic that of the adjacent teeth following the anticipated recession. Implant selection and the interdental papilla volume (height and width) are determined by the implant s mesiodistal position. The length of the crown restoration is indicated by its buccopalatal orientation. The emergence profile and peri-implant pocket depth are influenced by the apicocoronal location. The histological variation of the biological volume at bone level and the clinical change of the gingival margin between the phase of the implant placement and 6 months after implant exposition should be considered in the selection of the implant diameter and for adequate treatment planning to achieve an optimal aesthetic aspect for the implant-supported restoration. The cervical contour of the provisional restoration determines the shape of the buccal gingiva and height of the interdental papillae. Finally, the ceramic restoration must possess a form that complements the surrounding tissues, facilitates proper plaque control and occlusal function, and presents a harmonious natural appearance. Acknowledgment The authors mention their gratitude to Dr. Mario Groisman, Brazil, for his contribution in the discussion. References 1. Saadoun AP, Sullivan DY, Krichek M, LeGall M. Single-tooth implant: Management for success. Pract Periodont Aesthet Dent 1994;6(3): Garber DA, Belser UC. Restoration-driven implant placement with restoration-generated site development. Compend Cont Educ Dent 1995;16(8): Touati B. Double guidance approach for the improvement of the single-tooth replacement. Dent Implantol Update 1997;8(12): Salama H, Salama MA, Li TF, et al. Treatment planning 2000: An esthetically oriented revision of the original implant protocol. J Esthet Dent 1997;9(2): Touati B, Guez G, Saadoun AP. Aesthetic soft tissue integration and optimized emergence profile: Provisionalization and customized impression coping. Pract Periodont Aesthet Dent 1999; 11(3); Bahat O, Daftary F. Surgical reconstruction A prerequisite for long-term implant success: A philosophic approach. Pract Periodont Aesthet Dent 1995;7(9): Hebel KS, Gajjar R. Achieving superior aesthetic results: Parameters for implant and abutment selection. Int J Dent Symp 1997;4: Saadoun AP, Le Gall M. Implant positioning for periodontal, functional, and aesthetic results. Pract Periodont Aesthet Dent 1992;4(7): Adell R, Eriksson B, Lekholm U, et al. Long-term follow-up study of osseointegrated implants in the treatment of totally edentulous jaws. Int J Oral Maxillofac Impl 1990;5(4): Tarnow DP, Magne AW, Fletcher P. The effect from the distance from the contact point to the crest of bone on the presence or absence of interproximal dental papilla. J Periodontol 1992; 63(12): Tarnow DP, Cho S, Wallace S. Effect of interdental distance on crestal bone loss around implants. J Periodontol In press. 12. Weisgold AS, Arnoux JP, Lu J. Single-tooth anterior implant: A world of caution. Part I. J Esthet Dent 1997;9(5): Grunder U, Spielmann HP, Gaberthuel T. Implant-supported single tooth replacement in the aesthetic region: A complex challenge. Pract Periodont Aesthet Dent 1996;8(9): Saadoun AP. The key to peri-implant esthetics: Hard-and-soft tissue management. Dent Implantol Update 1997;8(6): Berglundh T, Lindhe J. Dimension of the peri-implant mucosa: Biological width revisited. J Clin Periodontol 1996;23(10): Bichacho N, Landsberg CJ. Single implant restorations: Prosthetically induced soft tissue topography. Pract Periodont Aesthet Dent 1997;9(7); Wöhrle PS. The synergy of taper and diameter: Enhancing the art and science of implant dentistry with the Replace implant system. Int J Dent Symp 1997;4: Buser D, Weber HP, Lang NP. Tissue integration on non-submerged implants. 1-year results of a prospective study with 100 ITI hollow-cylinder and hollow-screw implants. Clin Oral Impl Res 1990;1(1): Alberktsson T, Zarb G, Worthington P, Eriksson AR. The long-term efficacy of currently used dental implants: A review. Int J Oral Maxillofac Impl 1986;1(1): Le Gall MG. The impact of occlusion on implants and implant componentry. Part 1. Dent Implantol Update 1996;7(8): Bengazi F, Wennström JL, Lekholm U. Recession of the soft tissue margin at oral implants. A 2-year longitudinal prospective study. Clin Oral Impl Res 1996;7(4): Jovanovic SA, Paul SJ, Nishimura RD. Anterior implant-supported reconstructions: A surgical challenge. Pract Periodont Aesthet Dent 1999;11(5): Hürzeler MB, Weng D. Periimplant tissue management: Optimal timing for an aesthetic result. Pract Periodont Aesthet Dent 1996; 8(9): Salinas TJ, Sadan A. Establishing soft tissue integration with natural tooth-shaped abutments. Pract Periodont Aesthet Dent 1998; 10(1): Saadoun AP, Le Gall M. Periodontal implications in implant treatment planning for aesthetic results. Pract Periodont Aesthet Dent 1998;11(5): Esposito M, Ekestubbe A, Gröndahl K. Radiological evaluation of marginal bone loss at tooth surfaces facing single Brånemark implants. Clin Oral Impl Res 1993;4(3): Tal H. Relationship between the interproximal distance of roots and the prevalence of intrabony pockets. J Periodontol 1983; 55: Fiorellini JP, Buser D, Paquette DW, et al. A radiographic evaluation of bone healing around submerged and non-submerged dental implants in beagle dogs. J Periodontol 1999;70(3): Salama H. Salama MA, Li T-F, et al. Treatment planning 2000: An esthetically oriented revision of the original implant protocol. J Esthet Dent 1997;9(2): Vol. 11, No. 9
12 CONTINUING EDUCATION (CE) EXERCISE NO CONTINUING CE EDUCATION NEW YORK UNIVERSITY College of Dentistry Center for Continuing Dental Education New York City, NY To submit your CE Exercise answers, please use the answer sheet found within the CE Editorial Section of this issue and complete as follows: 1) Identify the article; 2) Place an X in the appropriate box for each question of each exercise; 3) Clip answer sheet from the page and mail it to the CE Department at Montage Media Corporation. For further instructions, please refer to the CE Editorial Section. The 10 multiple-choice questions for this Continuing Education (CE) Exercise are based on the article Selection and ideal tridimensional implant position for soft tissue aesthetics by André P. Saadoun, DDS, MS, Marcel LeGall, DDS, and Bernard Touati, DDS, DSO. This article is on Pages Learning Objectives: This article reviews and describes the importance of utilizing restoration-driven therapy for accurate implant placement. Upon reading and completion of this exercise, the reader will possess: A heightened awareness of the role of the soft tissues in aesthetic implant restorations. An understanding of the functional and aesthetic factors that influence implant placement. 1. As the ceramic crown emerges from the implant, it should support: a. The most coronal 4 mm of the soft tissue. b. The most incisal 7 mm of the soft tissue. c. The most coronal 7 mm of the soft tissue. d. The most incisal 4 mm of the soft tissue. 2. All the following factors must be considered prior to implant placement EXCEPT: a. Type of smile. b. Potential height of the replacement crown. c. Osseous topography of the edentulous ridge. d. Surgical procedures necessary for adequate site preparation. 3. The dimensions of the contralateral dentition must be analyzed in order to: a. Determine the length of the crown to be replaced. b. Analyze the root position. c. Analyze the edentulous ridge. d. Determine the shape and width of the crown to be replaced. 4. Cervical bone resorption morphology is a factor in determining the: a. Mesiodistal placement of the implant collar. b. Faciolingual placement of the implant shoulder. c. Gingival placement of the implant collar. d. Apicocoronal placement of the implant shoulder. 5. Optimal implant placement within an edentulous site affects all the following EXCEPT: a. Facial aesthetics. b. Periodontal health. c. Implant longevity. d. Occlusal function. 6. Faciolingual placement and orientation determines: a. Length of the implant collar surface. b. Definitive aesthetic result. c. The proximal dimensions of the crown. d. Implant emergence. 7. In order to maintain the integrity of the interdental papillae: a. 1 mm must be maintained at the cervical implant level. b. A distance between 3 mm and 4 mm must be maintained between two implants. c. 5 mm must be maintained at the cervical implant level from the adjacent teeth. d. A distance between 5 mm and 7 mm must be maintained between two implants. 8. If the soft tissue is at an adequate or deficient level, keratinized tissue must be increased to: a. Develop a natural emergence profile. b. Support the 6 mm of soft tissue required to maintain biologic width. c. Prevent bone loss. d. Ensure an aesthetic result. 9. Proper angulation involves orientation of the implant with regard to all the following EXCEPT: a. Ridge morphology. b. Hexagonal rotation. c. Mesiodistal placement. d. Apicocoronal orientation. 10. What is the objective of the prosthetic phase? a. To achieve the definitive restoration. b. To develop the restorative-gingival interface. c. To support contoured healing. d. To achieve cementation of the crown molding Vol. 11, No. 9

13 RESEAR.CH AND SECTION EDITOR LOUIS J. BOUC:HER EDUCATION Clinical results of osseointegrated implants supporting fixed prostheses in edentulous jaws R. Adell, D.D.S., Ph.D.* University of Gijieborg, Giiteborg, Sweden T he osseointegration method for achieving fixed, electively removable dental prostheses in edentulous patients has been thoroughly reviewed in a series of articles. Both the rationale for and the proposed mechanism of osseointegration have been discussed in detail. Treatment indications, patient selection considerations: methods, complications, and clinical results over a 15-year period have also been reported.2-4 The following is an update of material and results from the Giiteborg clinical data on osseointegration. MATERIAL The material comprised a total of about 4,100 implants installed in 650 jaws of 600 patients, most of whom were treated in GGteborg, Sweden (Table I). About 900 of these fixtures were inserted in 150 jaws at several other centers in Scandinavia and abroad where the osseointegration method is now used regularly. Patient characteristics did not differ from those described earlier.2 The mean age was 53 years at the time of implant installation, with a range of 20 to 77 years of age and a slight predominance of women by about 60%. Removable dentures were present in opposing jaw in 60% of the patients. Most jaws were severely resorbed (Fig. l), often with inverted spatial relations in the sagittal plane. The patients were selected mainly according to their degree of suffering from their edentulous state as judged by the team of examining medical and dental specialists. Selection was not made to fulfill any desired optimal jawbone anatomy. The material was divided into the following observation groups: 1. The development group, observed for 10 to 17 years 2. Routine group I, observed for 6 to 10 years 3. Routine group IIa, observed for 5 to 6 years 4. Routine group IIb, observed for 1 to 4 years Presented at the Toronto Conference on Osseointegration in Clinical Dentistry, Toronto, Ont., Canada. Associate Professor, Departmrnt of Oral Surgery. Fig. 1. Preoperative lateral cephalogram of a typical patient treated by this method. Table I. Total material GGteborg Other centers (14) Total Fixtures 3, ,l no Jaws Pdtients In the following presentation of results, three parts of the clinical material were excluded: (1) fixtures that had been prosthesis loaded for less than 1 year, (2) fixtures placed in bone grafts, and (3) fixtures belonging to the development group. The routine groups, which were statistically analyzed, consisted of almost 2,000 implants that had been inserted in 300 jaws (Tables II and III). About 50% of these fixtures and jaws were observed for more than 5 years (Tables II and III). METHODS The outlines reviewed by Brinemark et a1.3 and Adell et al., which concerned examination and selection of patients, surgery, prosthodontics, oral hygiene, THE JOURNAL OF PROSTHETIC DENTISTRY 251
 Upper jaw Lower jaw Routine group I 81 91 1 (1 year: 84) (1 year: 91) Routine group IIa 82 91 (1 year: 86) (1 year: 92) Routine group IIb 9.")
14 ADELL Table IV. Distribution of persisting fixtures (in percents) Upper jaw Lower jaw Routine group I (1 year: 84) (1 year: 91) Routine group IIa (1 year: 86) (1 year: 92) Routine group IIb (1 year: 97) (1 year: 99) Bracketed figures from observations of more than 5 years. Table V. Distribution of jaws with continuously stable prostheses (in percents) Upper Lower jaw jaw Routine group I 88 Routine group IIa Routine group IIb Fig. 2. A, Schematic representation of standard prosthesis design in mandible. B, Clinical appearance of a lower prosthesis on osseointegrated fixtures 5 years after treatment. Patient wears a conventional removable denture in upper jaw. Table II. Number of fixtures for statistical analysis Routine group Upper jaw Lower jaw Total Routine group 1,017 IIa I Routine group IIb Total 840 1,121 1,961 *Observed for more than 5 years. Table III. Number analysis Routine group Upper jaw of jaws for statistical Lower jaw Total Routine group 147 IIa I Routine group IIb Total *Observed for more than 5 years. Bracketed figures from observations of more than 5 years. and follow-up registrations, were closely followed. After a two-step surgical procedure, the patients were provided with removable dental prostheses. The prostheses resembled conventional fixed partial dentures but were screwed onto abutments on the fixtures (Fig. 2). The abutment-fixture units were immobile. All patients were followed up continuously with annual standardized clinical and radiologic examinations that were recorded in a computerized system. Two samples were selected. One sample, A, of 152 patients (97 women and 55 men) was used for retrieving questionnaires on the opinions of the patients 3 years or more after treatment. The other sample, B, comprised 95 fixtures (42 from upper and 53 from lower jaws in 10 women and six men) followed up for 3 years. Clinical mucosal reactions around the abutments were examined in this latter sample. RESULTS Thk anchorage function or the fixture survival rate was defined as the number of stable prosthesissupporting and osseointegrated fixtures in relation to the total number of fixtures installed. The long-term anchorage function of fixtures exceeded 80% in the maxillae and 90% in the mandibles (Table IV). For routine group IIb even better results were obtained. Anchorage function was also calculated for prostheses as the number of jaws in which the patients enjoyed continuously stable prostheses in relation to the total 252 AUGUST 1983 VOLUME 50 NUMBER 2
15 OSSEOINTEGRATED IMPLANTS number of jaws treated, although some exchange of supporting fixturles may have taken place. The anchorage function for prostheses was between 90% and 100% for upper and 100% for lower jaws (Table V). Only nine patients had their prostheses changed to complete dentures. All nine situations involved the maxillae and were reviewed earlier.2 The longest continuous functiloning time for a prosthesis on osseointegrated fixtures is 17 years. In sample A, 90% of the women patients and 95% of the men patients stated that, if necessary, they would be treated again with a fixture-anchored prosthesis. About 85% of the women and 95% of the men patients felt that their prostheses were integral parts of their bodies. In sample B there was a mean pocket depth of 3 mm, and the percent:5 o f plaque- and gingivitis-affected quadrants around the abutments were 15% and 8%, respectively. DISCUSSION The preliminary results gained from sample A corroborate the findings from other psychosocial studies on the (effects of treatment with jawboneanchored prostheses.5,6 Such treatment not only meant a rehabilitation of the masticatory system4 but also implied a considerable increase in the self-confidence of the patients, which in turn elicited widespread positive psychosocial consequences. The anchorage function for fixtures and prostheses was even better than that reported earlier. The number of fixture losses was small, and lost fixtures occurred, with few exceptions, only during the first year after completion of surgical treatment. The anchorage function of prostheses was the most relevant parameter from the patient s point of view in determining the success or failure of the method. During the last 2 years not one patient required a return to a removable denture. Clinical soft ti,ssue reactions to the abutments were mild and would not have been associated with periodontitis if teeth had been present in the same sites. Moreover, biops:les and microbiologic samples from osseointegrated fi.kture-abutment marginal sites in other samples of the total material were indicative of only occasional mild inflammatory reactions. Marginal bone height variations were discussed at length by Adell et al.* They stated that a mean 1.5 mm of marginal bone was lost during the first year after prosthesis loading. This was interpreted as a response to the surgical trauma and to the initial marginal torque stress apiplied peroperatively. After the first year only 0.1 mm of marginal bone per year was lost for all groups, although a number of fractured fixtures, which caused a considerable marginal bone loss, were still included in the material. Parts of the total patient sample of material were excluded for the following reasons: 1. No reliable conclusions on the long-term prognosis can be drawn from patients observed for only 1 year. 2. The quality and behavior of bone tissue in a graft may differ from that of original jaw bone, and the results of fixtures in grafts have already been reviewed in a separate article.* 3. The clinical procedures in the development group were not as standardized as those in the routine groups, although the same basic principles were applied. The development group has also been reviewed separately.2 The 5-year limit was regarded as an important time of reference. It is common in medical literature for comparison of various treatments; it should, therefore, be regarded as a standard for prostheses on teeth. It has been specifically recommended by the 1978 Harvard Conference on dental implants.9 PROGNOSIS The anchorage function for fixtures and, as a consequence, the anchorage function for prostheses depended on a maintained osseointegration and a maintained marginal bone height. The number of fixtures lost was small. Only a minute portion of marginal bone height resorbed. Because these losses occurred mainly during the first year after installation of abutments, a predictable prognosis could be made for each patient after the first year of prosthesis wear. CONCLUSIONS The osseointegration method with jawboneanchored prostheses gave a 5- to IO-year implant survival rate of 81% in the maxillae and 91% in the mandibles. Very few fixtures were lost during the first year after abutment connection. Continuously stable prostheses were worn in more than 90% of the upper and in 100% of the lower jaws observed for 5 to 10 years. The osseointegration method fulfills and exceeds the demands by the 1978 Harvard Conference on dental implantation methods and implies a considerable psychosocial improvement for the individual. The handling of numerical data of the computerized registration system by instruction nurse Barbro Svensson is gratefully acknowledged. THE JOURNAL OF PROSTHETIC DENTISTRY 253
16 ADELL REFERENCES 1. Albrektsson, T., Branemark, P-I., Hansson, H. A., and Lind- Strom, J.: Osseointegrated titanium implants. Acta Orthop Stand 52:155, Adell, R., Lekholm, U., Rockier, B., and Branemark, P-I.: A 15-year study of osseointegrated implants in the treatment of the edentulous jaw. Int J Oral Surg 6~387, Brinemark, P-I., Hansson, B. O., Adell, R., Breine, U., Lindstriim, J., Hall&, O., and ohman, A.: Osseointegrated implants in the treatment of the edentulous jaw. Experience from a IO-year period. Stand J Plast Reconstr Surg 11: Suppl 16, Haraldson, T.: Functional Evaluation of Bridges on Osseointegrated Implants in the Edentulous Jaw. Thesis, University of Giiteborg, Blomberg, S.: Rehabilitering med kzkbensforankrad betterslttning. I. Klinisk-psykiatriska aspekter. Tandhikartidningen 64~669, Blomberg, S., Brinemark, P-I., and Carlsson, G. E.: Psykoso- ciala effekter av behandling med kikbensforankrade broar pi osseointegrerade implantat. Likartidningen (In press.) 7. Lindhe, J.: The Soft Tissue Response. Symposium on Osseointegration in Glinical Dentistry, Toronto, Breine, U., and Branemark, P-I.: Reconstruction of alveolar jaw bone. An experimental and clinical study of immediate and preformed autologous bone grafts in combination with osseointegrated implants. Stand J Plast Reconstr Surg 14~23, Srhnitman, P. A., and Shulman, L. B.: Recommendations of the consensus development conference on dental implants. J Am Dent Assoc 98:373, Repin1 reqwrts to: DR. GEORGE A. ZARB UNMRSITY OF TORONTO FACLILTY OF DENTISTRY 124 EDWARD ST. TORONTO, ONT. MSG lg6 CANADA 254 AUGUST 1983 VOLUME 50 NUMBER 2
17 Luigi Canullo Giampiero Rossi Fedele Giuliano Iannello Søren Jepsen Platform switching and marginal bone-level alterations: the results of a randomized-controlled trial Authors affiliations: Luigi Canullo, Private Practice, Rome, Italy Luigi Canullo, Sren Jepsen, UniversityofBonn, Bonn, Germany Giampiero Rossi Fedele, Private Practice, London, UK Giuliano Iannello, Data Analyst, Rome, Italy Correspondence to: Dr Luigi Canullo Via Nizza Rome Italy Tel.: þ Fax: þ luigicanullo@yahoo.com Key words: bone level, bone loss, dental implants, implant design, platform switching Abstract Objectives: This randomized-controlled trial aimed to evaluate marginal bone level alterations at implants restored according to the platform-switching concept, using different implant/abutment mismatching. Material and methods: Eighty implants were divided according to the platform diameter in four groups: 3.8 mm (control), 4.3 mm (test group 1 ), 4.8 mm (test group 2 ) and 5.5 mm (test group 3 ), and randomly placed in the posterior maxilla of 31 patients. After 3 months, implants were connected to a 3.8-mm-diameter abutment and final restorations were performed. Radiographic bone height was measured by two independent examiners at the time of implant placement (baseline), and after 9, 15, 21 and 33 months. Results: After 21 months, all 80 implants were clinically osseointegrated in the 31 patients treated. A total of 69 implants were available for analysis, as 11 implants had to be excluded from the study due to early unintentional cover screw exposure. Radiographic evaluation showed a mean bone loss of 0.99 mm (SD ¼ 0.42 mm) for test group 1, 0.82 mm (SD ¼ 0.36 mm) for test group 2 and 0.56 mm (SD ¼ 0.31 mm) for test group 3. These values were statistically significantly lower (Po0.005) compared with control (1.49 mm, SD ¼ 0.54 mm). After 33 months, five patients were lost to follow-up. Evaluation of the remaining 60 implants showed no difference compared with 21 months data except for test group 2 (0.87 mm) and test group 3 (0.64 mm). There was an inverse correlation between the extent of mismatching and the amount of bone loss. Conclusions: This study suggested that marginal bone level alterations could be related to the extent of implant/abutment mismatching. Marginal bone levels were better maintained at implants restored according to the platform-switching concept. Date: Accepted 26 September 2009 To cite this article: Canullo L, Fedele GR, Iannello G, Jepsen S. Platform switching and marginal bone-level alterations: the results of a randomized-controlled trial. Clin. Oral Impl. Res. 21, 2010; doi: /j x It has been demonstrated that following implant surgery, remodeling takes occurs and is characterized by a reduction in bone dimension, both horizontally and vertically (Cardaropoli et al. 2006). The radiographic marginal bone level showed a mean loss of 0.9 mm at the time of abutment connection and crown placement and a further mean loss of 0.7 mm at 1 year. Similar results were reported in a retrospective study, which showed a range of resorption of 2 3 mm after 1 year depending on arch, jaw region, smoking status, case type, bone quality, surface type and implant design (Manz 2000). It has been suggested that this biologic process resulting in loss of crestal bone height may be altered when the outer edge of the implant abutment interface is horizontally repositioned inwardly and away from the outer edge of the implant platform. This prosthetic concept has been c 2009 John Wiley & Sons A/S 115
18 Canullo et al Platform switching introduced as platform switching and radiographic follow-up has demonstrated a smaller than expected vertical change in the crestal bone height around implants (Lazzara & Porter 2006). Outcomes following platform switching have also been studied histologically both in animals and humans. Whereas, Becker et al. (2007) did not find histological differences in bone resorption between traditionally restored and platform-switched implants after 28 days of healing in dogs, Jung et al. (2008) and Cochran et al. (2009) reported only minimal bone loss around loaded implants with non-matching implant abutment diameters following a 6-month loading period. Luongo et al. (2008) examined histologically a human implant removed 2 months after placement and speculated that the inward shift of the inflammatory connective tissue zone at the implant abutment junction could be the reason for bone preservation around platform-switched implants. Similar conclusions were drawn by Degidi et al. (2008) who reported no resorption of the coronal bone at a human implant that had been retrieved after a 1-month loading period. Using three-dimensional finite-element models, Maeda et al. (2007) examined the possible biomechanical advantage of platform switching in an in vitro study and suggested that by this configuration, the stress concentration would be shifted away from the cervical bone implant interface. In a controlled study with 30 patients, Vela-Nebot et al. (2006) found a significant reduction of mean bone loss of 0.7 mm at 30 platform-switched implants compared with 2.5 mm at the 30 control implants, 6 months after abutment attachment. In a limited number of patients, where implants were placed in extraction sockets, Canullo & Rasperini (2007) observed that immediate loading with platform switching could provide peri-implant hard-tissue stability with soft-tissue and papilla preservation. Hürzeler et al. (2008) observed in a preliminary study, including 15 patients who had received 14 wide-diameter implants with platform-switched abutments and eight implants with regular diameter, less mean crestal bone resorption (0.12 vs mm) 1 year after final restoration. In another recent prospective study with 45 patients, Cappiello et al. (2008) showed that 12 months after loading, the vertical bone loss in 75 implants restored according to the platform-switching protocol varied between 0.6 and 1.2 mm (mean: mm), while in 56 control implants with matching abutments, bone loss was between 1.3 and 2.1 mm (mean: mm). Very recently in a prospective multicenter trial, Prosper et al. (2009) reported no bone loss (mean: mm) at 60 platform-switched implants compared with 60 implants with regular abutments (mean: mm) 24 months following placement. At present, information from studies with a longer observation period is lacking. Furthermore, it is not known whether marginal bone level alterations may be affected by the extent of implant abutment mismatching. The aim of this randomized controlled study was to assess radiographically marginal bone level alterations in implants restored according to the platform-switching concept using different mismatching implant abutment diameters compared with traditionally restored implants. Material and methods Study design and patient selection Eighty consecutive implants in 31 patients were inserted for implant-supported restorations in the posterior maxilla. All patients were in general good health. They were followed for a period of 30 months after prosthetic rehabilitation. The exclusion criteria were: Sites with acute infection. Patients with a full mouth plaque score and a full mouth bleeding score 425%. Sites with o7 mm width of bone crest. Sites with interproximal or buccal bone defects. Smokers with 410 cigarettes/day. Patients with diabetes. Pregnant or lactating women. Patients with a history of bisphosphonate therapy. Implants of all subjects included in the study were randomly assigned to one of the four treatment regimens (implant diameter 3.8, 4.3, 4.8 and 5.5 mm). Random assignment was performed according to predefined randomization tables. A balanced random permuted block approach, ensuring that, at any point in a trial, roughly equal numbers of participants were allocated to all the comparison groups, was used to prepare the randomization tables in order to avoid unequal balance between the four treatments. In order to reduce the chance of unfavorable splits between test and control groups in terms of key prognostic factors, the randomization process took into account the following variables: patient s gender, age, presence of adjacent teeth, distal extension sites and site location in the dental arch. Assignment was performed using a sealed envelope. Patients were informed about the procedure but were blinded whether they received test or control implants. A signed informed consent form was required. The present study was performed following the principles outlined in the Declaration of Helsinki on experimentation involving human subjects. Surgical protocol Before the surgical procedure, a full-mouth professional prophylaxis appointment was scheduled. Patients received 1 g amoxicillin/clavulanate 1 h before surgery and continued with 2 g/day for 6 days (Laskin et al. 2000). The characteristics of the site were: Presence of a wide ridge of bone allowing the insertion of a wide platform implant according to the Branemark protocol. Absence of infection. Absence of bone horizontal regenerative procedure requirement. Crestal incision was performed after anesthesia. One to four 13 mm implants (Global, Sweden & Martina, Padua, Italy), platform diameter of mm, were inserted in a standardized way in the posterior maxilla. A minimal distance of 2.5 mm between implants and between implants and teeth was always observed. When required, sinus lift augmentation was performed but the coronal part of all implants was always placed in at least 4 mm of native bone. Once the implant site was prepared to receive a 3.8-mmdiameter implant, surgeons assistants were asked to open the sealed envelope containing the randomization. If required, the implant site was then enlarged according 116 Clin. Oral Impl. Res. 21, 2010/ c 2009 John Wiley & Sons A/S

19 Canullo et al Platform switching to the randomization, to insert a wider than 3.8-mm-diameter implant. The rootshaped implant used in this study presented micro-threads in the coronal portion and a sand-blasted and acid-etched surface in the entire length of the body. All implants were inserted with the platform at the bone level. A 3.8-mm-diameter cover screw was used for each implant. Tension-free suture was performed using a 5 monofilament. Patients were instructed to have a soft diet and to avoid chewing in the treated area until the suture removal. Oral hygiene at the surgical site was limited to soft brushing for the first 2 weeks. Regular brushing in the rest of the mouth and rinse with 0.12% chlorexidine were prescribed for 2 weeks. Thereafter, conventional brushing and flossing were permitted. After 2 weeks, sutures were removed. Implants were allowed for a submerged healing. Two to 3 months later, the uncovering procedure was carried out. Only uneventfully healed implants were accepted in this study. Three months after the first surgery, by performing a crestal incision just over the area corresponding to the implant, the cover screws were exposed and removed. Attached keratinized mucosa was present both on the palatal and buccal aspect around all implants. Subsequently, a 3.8-healing abutment was inserted. After 1 week, a 3.8 mm coping transfer was used and an impression was taken. For restoration, in test and control groups, always a 3.8 abutment was used. In the test groups, this restoration resulted in a mismatching of mm of implant abutment diameters (Fig. 1). All restorations were a splinted single-unit crowns in order to protect implants from inhomogeneous loading. Two weeks after the re-opening procedure, crowns were cemented using a provisional cement (Temp Bond, Kerr, WA, USA). Radiographical and clinical assessments For each patient, an individual customized digital film holder was fabricated to ensure areproducibleradiographicanalysis. At the time of the final abutment and crown connection, periodontal parameters [bleeding on probing (BOP), probing pocket depth (PPD), modified plaque index on adjacent teeth and implants] were assessed. Furthermore, digital periapical standardized radiographs were taken to control the perfect adaptation of the abutment on the implant. Every 6 months for 30 months after the final restoration, clinical assessments were performed in order to evaluate periodontal parameters at implants and neighboring (mesial and distal) teeth. Every 6 months for 30 months after the final restoration, periapical standardized digital radiographs were taken in order to evaluate marginal bone level alterations after loading (Figs 2 and 3). A computerized measuring technique was applied to digital periapical radiographs. Evaluation of the marginal bone level around implants was performed using an image analysis software (Autocad 2006, version Z 54.10, Autodesk, San Rafael, CA, USA), which was able to compensate radiographic distortion (Canullo et al. 2009a, 2009b). The software calculated bone remodeling at the mesial and distal aspects of the implants. Because each implant was inserted at the bone-level crest, Fig. 1. SEM image of implants of the control and test groups. According to implant platform diameter, implants were divided into four groups: 3.8 (Control Group) with no mismatching, 4.3 (test group 1 )witha mismatching of 0.25 mm, 4.8 (test group 2 ) with a mismatching of 0.05 mm and 5.5 mm (test group 3 )witha mismatching of 0.85 mm. The abutment diameter was 3.8 mm in all groups. the distance was measured from the mesial and distal margin of the implant neck to the most coronal point where the bone appeared to be in contact with the implant. For each implant, mean values of mesial and distal records were used. All measurements were made and collected by the same two calibrated examiners, different from the implant surgeon. For each pair of measurements, mean values were used. Statistical analysis Firstly, the data were checked for normal distribution (Kolmogorov Smirnov and Shapiro Wilk normality tests) and then subjected to ANOVA. In order to evaluate the different impact of different diameters on bone resorption, univariate GLM test was conducted. Bone resorption was set as adependentvariableandthediameterof implants and patients were selected as independent factors. We observed that the diameter effect was significant whereas the patient effect was not significant. Results From December 2005 to September 2006, 31 consecutive patients (17 men and 14 women) were included in this study. At the time of implant insertion, the patients ranged in age from 36 to 78 years (mean age: 52.1 years). Missing teeth had been extracted due to advanced periodontitis or endodontic failure at least 6 months before surgery. In association with implant insertion, 21 sinus lift augmentations with a lateral window approach were carried out using nano-structured hydroxyapatite (Nanobone, Artoss, Rostock, Germany) as the only bone filler. All implants were clinically osseointegrated, stable and showed no sign of infection. All implants were loaded 14 weeks after insertion. All 31 patients could be followed up for 21 months. Eleven implants in 10 patients were excluded from the analysis because of early unintentional cover screw exposure. Thus, a total of 69 implants in 31 patients were included for the analysis after 21 months: 17 for test group 1, 15 for test group 2, 18 for test group 3 and 19 for the control group. Thereafter, five patients were lost to follow-up and 26 patients were available for the 33-months c 2009 John Wiley & Sons A/S 117 Clin. Oral Impl. Res. 21, 2010/
 at the time of implant insertion, (b) abutment connection and (c) 33 months after surgery.")


20 Canullo et al Platform switching Discussion Fig. 2. Periapical radiographs of a patient treated with 3.8 and 5.5 mm implants (a) at the time of implant insertion, (b) abutment connection and (c) 33 months after surgery. Regardless of implant diameter, the diameters of the cover screw, the healing abutment and the prosthetic abutment were always 3.8 mm. Fig. 3. Periapical radiographs of a patient treated with 4.8, 4.3 and 5.5 mm implants (a) at the time of implant insertion, (b) abutment connection and (c) 33 months after surgery. Regardless of implant diameter, the diameters of the cover screw, the healing abutment and the prosthetic abutment were always 3.8 mm. Fig. 4. Mean marginal bone-level alterations over the observation period for test and control groups. evaluation of a total of 61 implants: 17 for test group 1, 13 for test group 2, 14 for test group 3 and 17 for control group. Periodontal parameters For the duration of the study, BOP was not detected at any implant, and PPD did not exceed 3 mm. Radiographic results Figure 4 displays the mean marginal bonelevel alterations for the different groups of implants over the study period. At the last follow-up, radiographic analysis showed a bone resorption of 0.99 mm for test group 1 (Time 1: 0.74 mm, SD: 0.39 mm; Time 2: 0.95 mm, SD: 0.35 mm; Time 3: 0.99 mm, SD: mm; Time 4: 0.99 mm, SD: 0.42 mm), 0.83 mm for test group 2 (Time 1: 0.64 mm, SD: 0.40 mm; Time 2: 0.78 mm, SD: 0.35 mm; Time 3: 0.82 mm, SD: mm; Time 4: 0.87 mm, SD:0.43 mm) and 0.64 mm for test group 3 (Time 1: 0.41 mm, SD: 0.28 mm; Time 2: 0.51 mm, SD: 0.29 mm; Time 3: 0.56 mm, SD: 0.31 mm; Time 4: 0.64 mm, SD: 0.32 mm). Control group mean value was 1.48 mm (Time 1: 1.23 mm, SD: 0.67; Time 2: 1.46 mm, SD: 0.53 mm; Time 3: 1.49 mm, SD: mm; Time 4: 1.48 mm, SD: 0.42 mm) (Fig. 5). For each time point, all test group mean values were statistically significantly lower (Po0.005) compared with control group values. Furthermore, there was a significant inverse correlation ( 0.63, Po0.001, Pearson) between the amount of abutment implant diameter mismatching and the extent of marginal bone loss. In this study, over a period of almost 3 years, it could be demonstrated that implants restored according to the platform-switching concept experienced significantly less marginal bone loss than implants with matching implant abutment diameters. In addition, it was observed that marginal bone levels were even better maintained with increasing implant/abutment mismatching. First limitation of this study was that standardized radiographic evaluation only provided information about mesial and distal bone level. Buccal and oral bone levels were not evaluative. One limitation of the present study design was that, not all patients could receive all four configurations of implants/abutments under study, due to limited space in the edentulous areas. However, a possible influence of the factor patient on the outcomes could be ruled out. In only four patients (out of the 31 at 21-month followup and 26 at the 33-month follow-up), the order of implant types with regard to bone loss deviated from that shown by the mean values. More specifically, in three patients, a 4.3 mm implant experienced slightly less bone loss than a 4.8 mm implant with wider platform, and in one patient, a 4.3 mm implant showed slightly more bone loss than a 3.8 mm control implant. In other words, in the vast majority of patients, the marginal bone level alterations observed followed the same pattern confirming the ranking sequence documented by the mean values. Another limitation for the evaluation of marginal bone level alterations is the fact that standardized conventional radiographs only provide information about mesial and distal bone levels. However, it has to be realized that this limitation applies to all studies of this kind (Abrahamsson & Berglundh 2009; Lang & Jepsen 2009). It can be speculated that the findings of a reduced bone loss at platform-switched implants in the present study may be related to their increased implant diameter rather than to the platform. However, comparative studies of implants with different diameters in relation to marginal bone loss did not show different outcomes (Friberg et al. 2002). Further studies could be helpful to clarify the relevance of 118 Clin. Oral Impl. Res. 21, 2010/ c 2009 John Wiley & Sons A/S
.")
21 Canullo et al Platform switching Fig. 5. Marginal bone loss (means SD) in the test and control groups 9, 15, 21 and 33 months after surgery. For each time point, all test group mean values were statistically significantly lower compared with the control group values (P 0.005, ANOVA, followed by Scheffe). wide-diameter implants rather than platform switching in preserving marginal bone. In the present study, implants with micro-threads in the marginal portion were used. The possible influence on such a design on the marginal bone loss was addressed in an experimental study in dogs (Abrahamsson & Berglundh 2006). The authors reported that the marginal bone level was located at a more coronal position at implants when compared with implants without micro-threads in the marginal portion, and suggested that the possible positive effects may be related to the osseous healing events after implant placement rather than bone preservation during function. The unintentional perforation of submerged two-stage implants during healing can result in significant bone destruction. Van Assche et al. (2008) showed, in a retrospective study aimed to determine the consequence of early cover screw exposure, 2 mm of mean bone re-modeling. Therefore, in the present study, implants with early exposition were excluded from further analysis. The most extensive marginal bone level alterations were seen at the first follow-up after 9 months, whereas, in the 2-year observation period, thereafter, only minor further bone loss could be observed. Previous experimental and clinical studies, in fact, showed that the most pronounced marginal bone level changes were identified after surgical trauma resulting from implant installation and abutment connection, while after functional loading, only minor signs of bone loss occurred (Brägger et al. 1998; Åstrand et al. 2004; Berglundh et al. 2005; Broggini et al. 2006). During the first year of loading, particularly two-piece implants were frequently associated with crestal bone loss of about mm (Albrektsson et al. 1986; Smith & Zarb 1989; Jung et al. 1996). The result of the present study, where control implants exhibited mean marginal bone-level alterations of 1.49 mm are well in line with these previous findings. Several explanations for these observed changes in crestal bone height have been suggested; some authors discussed a potential role of the microgap at the implant abutment interface for the bacterial colonization of the implant sulcus (Mombelli et al. 1987; Ericsson et al. 1995; Hermann et al. 2001a, 2001b; King et al. 2002), while others described the establishment of an adequately dimensioned biological width to be associated with marginal bone resorption at sites with a thin mucosa (Berglundh & Lindhe 1996; Hermann et al. 2000) and in conjunction with abutment re-connection (Abrahamsson et al. 1997). Butt joint connections associated with implant abutment configurations with matching diameters have been linked to inflammation, an inflammatory cell infiltrate and bone loss of mm (Broggini et al. 2003, 2006). The reasons for the reduced bone loss observed in platform-switched implants in the present study can only be speculated upon. The horizontal inward re-positioning of the implant abutment interface has been suggested to overcome some of the problems associated with two-piece implants. Platform switching may increase the distance between the abutment-associated inflammatory cell infiltrate and the marginal bone level, and thereby decrease its bone-resorptive effect. Also, there might be a reduction in the amount of marginal bone loss necessary to expose a minimum amount of implant surface to which the soft tissue can attach (Lazzara & Porter 2006). These assumptions are supported by recent animal studies (Jung et al. 2008; Weng et al. 2008; Cochran et al. 2009) and human histological observations (Degidi et al. 2008; Luongo et al. 2008). Clinical case series of immediate implants (Canullo & Rasperini 2007; Calvo-Guirado et al. 2009) and prospective-controlled studies have evaluated bone responses (Vela- Nebot et al. 2006; Cappiello et al. 2008; Hürzeler et al. 2008; Canullo et al. 2009a; Prosper et al. 2009) as well as soft-tissue responses (Canullo et al. 2009b) to platformswitched implants. The magnitude of the marginal bone level alterations observed varied among the studies. This may be due to different observation periods (6 24 months), implant types, study populations and radiographic analysis methods. However, compared with control implants with matching abutment implant dimensions, these studies could collectively demonstrate statistically significantly less marginal bone loss as assessed on radiographs at implants restored according to the platform-switching concept. The present study, with a longer follow-up of almost 3 years, not only confirmed these data but could also for the first time establish a relationship between the extent of platform switching and the amount of marginal bone loss. These findings could possibly be attributed to a wider space for horizontal repositioning of the biological width and/or a better distribution of loading stress at the bone/implant interface. Future experimental and clinical studies will help to unravel the biological processes involved as well as the significance of these findings for long-term implant success. c 2009 John Wiley & Sons A/S 119 Clin. Oral Impl. Res. 21, 2010/
22 Canullo et al Platform switching Acknowledgements: We highly appreciated the skills and commitment of Dr Audrenn Gautier for language suggestions and Dr Roberto Cocchetto for the effective help in protocol finalization. Furthermore, the authors are particularly grateful to Dr Valeria Caponi, Claudia Muollo, Dr Andrea Diociaiuti, Dr Paola Cicchese and Dr Giuseppe Goglia for the friendly support in radiographic measurements and patient recruitment. The authors declare that there are no conflicts of interest. This study was self-supported. References Abrahamsson, I. & Berglundh, T. (2006) Tissue characteristics at microthreaded implants. An experimental study in dogs. Clinical Implant Dentistry & Related Research 8: Abrahamsson, I. & Berglundh, T. (2009) Effects of different implant surfaces and designs onmarginal bone-level alterations: a review. Clinical Implant Dentistry & Related Research 20: Abrahamsson, I., Berglundh, T. & Lindhe, J. (1997) The mucosal barrier following abutment dis/reconnection. An experimental study in dogs. Journal of Clinical Periodontology 24: Albrektsson, T., Zarb, G., Worthington, P. & Eriksson, A.R. (1986) The long-term efficacy of currently used dental implants: a review and proposed criteria of success. The International Journal of Oral & Maxillofacial Implants 1: Åstrand, P., Engquist, B., Anzen, B., Bergendal, T., Hallmann, M., Karlsson, U., Kvint, S., Lysell, L. & Rundcranz, T. (2004) A three-year follow-up report of a comparative study of ITI dental implants and Brånemark system implants in the treatment of the partially edentulous maxilla. Clinical Implant Dentistry & Related Research 6: Becker, J., Ferrari, D., Herten, M., Kirsch, A., Schaer, A. & Schwarz, F. (2007) Influence of platform switching on crestal bone changes at non-submerged titanium implants: a histomorphometrical study in dogs. Journal of Clinical Periodontology 34: Berglundh, T., Abrahamsson, I. & Lindhe, J. (2005) Bone reactions to longstanding functional load at implants: an experimental study in dogs. Journal of Clinical Periodontology 32: Berglundh, T. & Lindhe, J. (1996) Dimension of the periimplant mucosa. Biological width revisited. Journal of Clinical Periodontology 22: Brägger, U., Häfeli, U., Huber, B., Hämmerle, C.H. &Lang,N.P.(1998)Evaluationofpostsurgical crestal bone levels adjacent to non-submerged dental implants. Clinical Oral Implants Research 9: Broggini, N., McManus, L.M., Hermann, J.S., Medina, R., Schenk, R.K., Buser, D. & Cochran, D.L. (2006) Peri-implant inflammation defined by the implant-abutment interface. Journal of Dental Research 85: Broggini, N., McManus, L.M., Hermann, J.S., Medina, R.U., Oates, T.W., Schenk, R.K., Buser, D., Mellonig, J.T. & Cochran, D.L. (2003) Persistent acute inflammation at the implant-abutment interface. Journal of Dental Research 82: Calvo-Guirado, J.L., Ortiz-Ruiz, A.J., López-Marí, L., Delgado-Ruiz, R., Maté-Sánchez, J. & Bravo Gonzalez, L.A. (2009) Immediate maxillary restoration of single-tooth implants using platform switching for crestal bone preservation: a 12- month study. The International Journal of Oral & Maxillofacial Implants 24: Canullo, L., Goglia, G., Iurlaro, G. & Iannello, G. (2009a) Short-term bone level observations associated with Platform Switching in immediately placed and restored single maxillary implants: a preliminary report. International Journal of Prosthodontics 22: Canullo, L., Iurlaro, G. & Iannello, G. (2009b) Double-blind randomized controlled trial study on post-extraction immediately restored implants using the switching platform concept: soft tissue response. Preliminary report. Clinical Oral Implants Research 20: Canullo, L. & Rasperini, G. (2007) Preservation of peri-implant soft and hard tissues using platform switching of implants placed in immediate extraction sockets: a proof-of-concept study with 12- to 36-month follow-up. The International Journal of Oral & Maxillofacial Implants 22: Cappiello, M., Luongo, R., Di Iorio, D., Bugea, C., Cocchetto, R. & Celletti, R. (2008) Evaluation of peri-implant bone loss around platform-switched implants. International Journal of Periodontics and Restorative Dentistry 28: Cardaropoli, G., Lekholm, U. & Wennström, J.L. (2006) Tissue alterations at implant-supported single-tooth replacements: a 1-year prospective clinical study. Clinical Oral Implants Research 17: Cochran, D.L, Bosshardt, D.D., Grize, L., Higginbottom, F.L., Jones, A.A., Jung, R.E., Wieland, M. &Dard,M.(2009)Boneresponsetoloadedimplants with non-matching implant-abutment diameters in the canine mandible. Journal of Periodontology 80: Degidi, M., Iezzi, G., Scarano, A. & Piattelli, A. (2008) Immediately loaded titanium implant with a tissue-stabilizing/maintaining design ( beyond platform switch ) retrieved from man after 4 weeks: a histological and histomorphometrical evaluation. A case report. Clinical Oral Implants Research 19: Ericsson, I., Persson, L.G., Berglundh, T., Marinello, C.P., Lindhe, J. & Klinge, B. (1995) Different types of inflammatory reactions in peri-implant soft tissues. Journal of Clinical Periodontology 22: Friberg, B., Ekkestubbe, A. & Sennerby, L. (2002) Clinical outcome of Brånemark System implants of various diameters: a retrospective study. The International Journal of Oral & Maxillofacial Implants 17: Hermann, J.S., Buser, D., Schenk, R.K., Higginbottom, F.L. & Cochran, D.L. (2000) Biologic width around titanium implants. A physiologically formed and stable dimension over time. Clinical Oral Implants Research 11: Hermann, J.S., Buser, D., Schenk, R.K., Schoolfield, J.D. & Cochran, DL. (2001a) Biologic Width around one- and two-piece titanium implants. Clinical Oral Implants Research 12: Hermann, J.S., Schoolfield, J.D., Schenk, R.K., Buser, D. & Cochran, D.L. (2001b) Influence of the size of the microgap on crestal bone changes around titanium implants. A histometric evaluation of unloaded non-submerged implants in the canine mandible. Journal of Periodontololgy 72: Hürzeler, M., Fickl, S., Zuhr, O. & Wachtel, H.C. (2008) Peri-implant bone level around implants with platform switched abutments: preliminary data from a prospective study. The International Journal of Oral and Maxillofacial Surgery 66: Jung, R.E., Jones, A.A., Higginbottom, F.L., Wilson, T.G., Schoolfield, J., Buser, D., Hämmerle, C.H. & Cochran, D.L. (2008) The influence of nonmatching implant and abutment diameters on radiographic crestal bone levels in dogs. Journal of Periodontology 79: Jung, Y.C., Han, C.H. & Lee, K.W. (1996) A 1-year radiographic evaluation of marginal bone around dental implants. The International Journal of Oral & Maxillofacial Implants 11: King, G.N., Hermann, J.S., Schoolfield, J.D., Buser, D. & Cochran, D.L. (2002) Influence of the size of the microgap on crestal bone levels in nonsubmerged dental implants: a radiographic study in the canine mandible. Journal of Periodontology 73: Lang, N.P. & Jepsen, S. (2009) Implant surfaces and design (Working Group 4). Clinical Oral Implants Research 20: Laskin, D.M., Dent, C.D., Morris, H.F., Ochi, S. & Olson, J.W. (2000) The influence of preoperative antibiotics on success of endosseous implants at 36 months. Annals of Periodontology 5: Lazzara, R.J. & Porter, S.S. (2006) Platform switching: a new concept in implant dentistry for controlling postrestorative crestal bone levels. International Journal of Periodontics and Restorative Dentistry 26: Luongo, R., Traini, T., Guidone, P.C., Bianco, G., Cocchetto, R. & Celletti, R. (2008) Hard and soft tissue responses to the platform-switching technique. International Journal of Periodontics and Restorative Dentistry 28: Clin. Oral Impl. Res. 21, 2010/ c 2009 John Wiley & Sons A/S
23 Canullo et al Platform switching Maeda, Y., Miura, J., Taki, I. & Sogo, M. (2007) Biomechanical analysis on platform switching: is there any biomechanical rationale? Clinical Oral Implants Research 18: Manz, M.C. (2000) Factors associated with radiographic vertical bone loss around implants placed in a clinical study. Annals of Periodontology 5: Mombelli, A., van Oosten, M.A., Schurch, E. Jr & Lang, N.P. (1987) The microbiota associated with successful or failing osseointegrated titanium implants. Oral Microbiology & Immunology 2: Prosper, L., Redaelli, S., Pasi, M., Zarone, F., Radaelli, G. & Gherlone, E.F. (2009) A randomized prospective multicenter trial evaluating the platform-switching technique for the prevention of postrestorative crestal bone loss. The International Journal of Oral & Maxillofacial Implants 24: Smith, D.E. & Zarb, G.A. (1989) Criteria for success of osseointegrated endosseous implants. Journal of Prosthetic Dentistry 62: Van Assche, N., Collaert, B., Coucke, W. & Quirynen, M. (2008) Correlation between early perforation of cover screws and marginal bone loss: a retrospective study. Journal of Clinical Periodontology 35: Vela-Nebot, X., Rodríguez-Ciurana, X., Rodado- Alonso, C. & Segalà-Torres, M. (2006) Benefits of an implant platform modification technique to reduce crestal bone resorption. Implant Dentistry 15: Weng, D., Nagata, M.J., Bell, M., Bosco, A.F., de Melo, L.G. & Richter, E.J. (2008) Influence of microgap location and configuration on the periimplant bone morphology in submerged implants. An experimental study in dogs. Clinical Oral Implants Research 11: c 2009 John Wiley & Sons A/S 121 Clin. Oral Impl. Res. 21, 2010/
24 23 Short Porous Implants in the Posterior Maxilla: A 3-year Report of a Prospective Study Giuseppe Corrente, MO, 005* Roberto Abundo, MO, 005* Alessandro Bermond des Ambrois, Luca Savio, 005** Michele Perelli, 005** MO** The aim of this ongoing prospective study was to determine the 36-month survival rate of short porous implants in the posterior maxilla with 2 to 7 mm of initial bane height in 48 patients. Farty-eight implants were placed; 35 were in sites with abone height af 5 mm or less and 13 patients required sinus elevatian with osteotomes in addition to a xenograft. Ali implants were loaded with single crowns. At the end of the follow-up period the survival rate was 97.92%. The use af short porous implants showed good predictability in the treatment of the posterior maxilla in this interim 3-year reporto (lnt J Periodontics Restorative Dent 2009; 29:23-29.) *Adjunct Professor, Department of Periodontics, University of Pennsylvania, Philadelphia, Pennsylvania; Private Practice, Torino, Italy. **Private Practice, Torino, Italy. Correspondence to: Dr Giuseppe Corrente, Corso Sicila 51, Torino, Italy; fax: ; info@sicor-corsi.com. When treating the posterior maxilla, anatomic problems are frequently encountered, especially when periodontally involved teeth have been previously extracted or the patient has been edentulous in the areafor a long time. Inthis area, bone isoften of poor quality, with rare trabeculae and wide marrow spaces. Reduced crestal height is often associated with an increasein the volume of the maxillary sinus(pneumatization).varioussurgical techniques as well as new implant surfaces have been developed in attempts to solve these problerns.l> Data from the literature indicate that when "traditiona!" implants (machined surfaces) are used for the prosthetic rehabilitation ofthese areas,they have to be at least 11 to 13 mm in length and 3.75 to 4.00 mm in diameter=? This leads to a need for more invasive surgical procedures to increase the amount of bone required in the sinus for implant placement. Implant placement may take place simultaneously with grafting when the residual basal height is 5 mm or more, or it may be performed in a second surgical procedure when the amount is lessthan 5 mm This procedure, performed Volume 29, Number 1, 2009
25 24 by means of opening a lateral window on the sinuswall,1,bhasshown positive results clinically11-13but is associated with increased morbidity related to complications, higher costs, and an increased riskof infection risk. 14,15The osteotome crestal approach5,16-1bis lessinvasive;here, localsinuselevation is achieved with a crestal approach by means of osteotomes and, if required, graft material to indirectly elevate the sinus membrane to provide sufficient support for implants and encourage new bone formation. Furthermore, the development of new implant surfacesoffers the possibility to increase the bone-implant contact area,providing successfullongterm clinical results,even with implants of reduced length and diarneter.'? In particular, the porous sintered implant (Endopore, lnnova), treated with spherical titanium particles, encourages mechanical interlocking between the implant itself and the bone. This allows for three-dimensional bone interdigitation, resulting in an interface zone structure that is resistant not only to compressive and shearforces but also to interface tensile forces. 2o As shown in variousclinicalstudies,these implants have shown positive resultsin both the short term and the long term.",22 The objective of this preliminary clinical study was to evaluate the use of short, porous-surface implants in the prosthetic rehabilitation of edentulous sites in the posterior maxilla, associated, if required, with local sinus elevation by means of osteotomes according to the technique described by Deporter et al.1b Method and materiais Forty-eight patients took part in the study (22 men, 26 women). They did not present with any systemicdisease. Nonsmokers and moderate smokers (fewerthan 10 cigarettes per day) were involved, and 48 press-fit implants were placed by 3 different surgeons. Ali implants were placed in the premolar/molar region and, when required, patients were treated with a localized sinus lift with the use of osteotomes and deproteinized bovine bone (Bio-Oss, Geistlich). The initial measurements of the available bone (residualcrestalheight) were recorded with digital radiography obtained using the parallelinq technique by means of Rinn film holders. The implants used were of two lengths (5 and 7 mm) and two different diameters (4.1 and 5 mm) and were chosen according to the available crestal height and width. In most cases, the implants were placed following a twostage approach (according to the surgeon's choice at the end of the surgery) with the smooth collar submerged at the crestallevel. The healing period was 4 months for a routine surgery and at least 6 months in patients where sinus lifts were performed. The implants were then loaded with single crowns (cemented or screwed on). Clinical and radiographic examinations were scheduled at 1, 6, and 12 months after crown insertion, then yearly. The data were subjected to Kaplan-Meier analysisto provide a cumulative survival rate (SR).23 Results Ali but one implant integrated suecessfully. This implant (4.1 X 7 mm) was positioned in a first molar area with a residual crestal height of 3 mm and was removed at the second surgical stage 6 months following the initial insertion healing period. with an uneventful Ali implants showed minimal crestal bone resorption that never exceeded the smooth collar of the implant (1 mm for 5-mm implants, 2 mm for 7-mm implants) as determined by the scheduled radiographic examinations. Figures 1 to 3 show the types of implants involved in the study (diameters and lengths), the sites of implant placement (sequentially numbered), and the preoperative basal bone height present at each site. The mean loading period for the implants reported in the study was 20 months. Half ofthe implants were observed for a longer period (Table 1). The International Journal of Periodontics & Restorative Dentistry
26 ~ ~ 12 c c (\J (\J Ci 20 Ci 10 E E '+o 15 Õ 8 o z 10 5 O 4.1 x 7 5 x 5 5 x 7 Implant dimensions (mm) o z O,-- R2nd premolar r-- R1st molar n,-- r-- R 2nd L 2nd L 1st molar premolar molar Implant sites n L 2nd molar Fig 1 Number and size (diameter X length) of implants used. Fig 2 Locations of implants placed. V> 2 12 Follow-up time (mo) of implants in 10 study 8 Time No.of %of in situ (mo) implants implants Vi Õ o z O Bone height (mm) Fig 3 Preoperative crestal bone height Total Volume 29, Number 1,2009
27 ~ 97.2:! 96 ~ 95.~ '"> 94 :::> Vl ~ 90 O Time (mo) Fig 4 Cumulative survival af implants. In29 patients, 4.1 x 7-mm implants were placed; in 10 patients 5 x5-mm implants were placed; and in the remaining 9 patients 5 x 7-mm implants were placed (Figs5 and 6).Ten implants were placed in second premolar sites, 34 implants were used to replace a first molar, and 4 replaced a second molar. The presurgical residual crestal height was 5 mm or less in 35 patients, and consequently a localized sinus lift was required prior to implant placement. In 13 patients, deproteinized bovine bone was inserted to achieve the desired height, while in the 35 remaining patients the compacting and apical movement of the autogenous bone was sufficient to provide the necessary bone volume. The overali mean height was 4.4 mm and ali implants were inserted with the smooth collar at the crestal levei. An SR of 97.92% (95% confidence intervai, 93.8% to 99.1 %) was shown after 36 months (Fig 4). Discussion Various studies have shown the importance of the implant surface in achieving osseointegration and stability over time. Among various options, the sintered porous surface allows for a three-dimensional interlocking with bone,24,2senabling resistance to the tensile and axial forces that are distributed along the implant. The bony ingrowth between the pores provides more mechanical binding between implant and bone than with conventional implant surfaces.26-29this can occur even in poor-quality bone, such as that in the posterior maxilla. A comparison of 7-mm or shorter implants shows that sintered porous implants have been more successful than those with machined or different rough surfaces. 3o In addition, the surgical technique of the localized sinus lift with a crestal approach allows for lessinvasive surgery and reduced healing period and postsurgical discomfort for the patient.17,31-32 In ali the present patients, no vertigo was observed or reported. 33 The technique was suecessful in clinical situations with reduced basal bone height (average of 4.4 mm); in extreme cases, a deproteinized bovine bone substitute was used as graft material for the sinus lift. The results of this 3-year report from a prospective study were consistent with those of a recent meta-analysis of osteotome sinus floor elevation." A longe r observation period and a greater number of patients are required to confirm the encouraging results in terms of predictability of these porous-surface, short implants placed in association with an osteotome sinus lift. The International Journal of Periadontics & Restorative Dentistry
 At 2 months after extraction, following spontaneous bone healing, crestal bone height is reduced. Fig Se (left) A porous-surface implant of 7 mm in length and 4.")
28 27 Fig Sa (left) Case 1. The right first premolar presents with periodontal problems and furcation involvement. An extraction is required. Fig Sb (right) At 2 months after extraction, following spontaneous bone healing, crestal bone height is reduced. Fig Se (left) A porous-surface implant of 7 mm in length and 4. 1 mm in diameter has been placed with a localized sinus lift with crestal approach by means of osteotomes with autogenous bone. A one-stage surgical approach was chosen. Following a 6-month healing period, the integrated implant was loaded. A well-mantained crestal profile can be noticed. Fig Sd (right) Fig 6a (left) Case 2. Preoperative radiograph. Following severe periodontal disease, an extensive bone defect is present after extraction of the right first premolar. A vertical guided bone regeneration procedure with deproteinized bovine bone and fibrin sealant has been performed. Fig 6b (right) Eight months after guided bone regeneration, an implant of 7 mm in length and 4. 1 mm in diameter was placed in the augmented site. A localized sinus lift was performed and the implant was left submerged to heal. Fig 6e (Ieft) One-year radiograph. Complete recorticalization of the sinus floor can be observed. Fig 6d (right) Volume 29, Number 1,2009
29 28 Acknowledgment The authors wish to thank Prof Giuseppe Migliaretti, Department of Public Health and Microbiology, University oftorino, Italy, for the statistical analysis. References 1. Boyne PJ, James RA. Grafting of the maxillary sinus floor with autogenous marrow and bone. J Oral Surg 1980;38: Tatum H Jr. Maxillary and sinus implant reconstructions. Dent Clin North Am 1986; 30: Bahat O, Fontanessi RV Efficacy of implant placement after bone grafting for threedimensional reconstruction ofthe posterior jaw. Int J Periodontics Restorative Dent 2001 ;21 : Summers RB. A new concept in maxillary implant surgery: The osteotome technique. Compendium 1994;15:152, , 158 passim; quiz Summers RB. The osteotome technique: Part 3-Less invasive methods of elevating the sinus floor. Compendium 1994; 15:698,700, Buser D, Mericske-Stern R, Bernard JP, et ai. Long-term evaluation of non-submerged ITI implants. Part 1: 8-year life table analysis of a prospective multi-center study with 2359 implants. Clin Oral Implants Res 1997;8: Jemt T, Lekholm U. Implant treatment in edentulous maxillae: A 5-year follow-up report on patients with different degrees of jaw resorption. Int J Oral Maxillofac Implants 1995;10: Smiler DG, Jonhson PW, Lozada JL, et ai. Sinus lift grafts and endosseous implants. Treatment of the atrophic posterior maxil- Ia. Dent Clin North Am 1992;36: Garg AK. Augmentation grafting of the maxillary sinus for placement of dental implants: Anatomy, physiology, and procedures. Implant Dent 1999;8: Rosen PS, Summers RB, Mellado JR, et ai. The bone-added osteotome sinus floor elevation technique: Multicenter retrospective report of consecutively treated patients. Int J Oral Maxillofac Implants 1999;14: Raghoebar GM, Timmenga NM, Reintsema H, Stegenga B, Vissink A. Maxillary bone grafting for insertion of endosseous implants: Results after months. Clin Oral Implants Res 2001; 12: Hürzeler MB, Kirsch A, Ackermann KL, Ouifiones CR. Reconstruction of severely resorbed maxilla with dental implants in the augmented maxillary sinus: A 5-year clinical investigation. Int J Oral Maxillofac Implants 1996;11 : Bahat O. Bránernark system implants in the posterior maxilla: Clinical study of 660 implants followed for 5 to 12 years. Int J Oral Maxillofac Implants 2000;15: Regev E, Smith RA, Perrot DH, Pogrel MA. Maxillary sinus complications related to endosseous implants.lntj Oral Maxillofac Implants 1995;10: Schwartz-Arad D, Herzberg R, Dolev E. The prevalence of surgical complications of the sinus graft procedure and their impact on implant survival. J Periodontol 2004;75: Coatoam GW, Krieger JT. A four-year study examining the results of indirect sinus augmentation procedures. J Oral Implantol 1997;23: Zitzmann NU, Schárer P. Sinus elevation procedures in the resorbed posterior maxilla. Comparison of the crestal and lateral approaches. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 1998;85: Deporter D, Todescan R, Caudry S. Simplifying management of the posterior maxilla using short, porous-surfaced dental implants and simultaneous indirect sinus elevation. Int J Periodontics Restorative Dent 2000;20: Renouard F, Nisand D. Impact of implant length and dia meter on survival rates. Clin Orallmplants Res 2006;17: The International Journal of Periodontics & Restorative Dentistry
30 Deporter DA, Watson PA, Pilliar RM, Chipman ML, Valiquette N. A histological comparison in the dog of porous-coated vs. threaded dental implants. J Dent Res 1990;69: Deporter DA, Todescan R, Watson PA, Pharoah M, Pilliar RM, Tomlinson GA prospective human clinical trial of Endopore dental implants in restoring the partially edentulous A maxilla using fixed prostheses, Int J Oral Maxillofac Implants 2001;16: Deporter D, Watson P, Pharoah M, Todescan R,Tomlinson G. Ten-year results of prospective study using porous-surfaced dental implants and a mandibular overdenture. Clin Implant Dent Relat Res 2002;4: Kaplan E, Meier P.Nonparametric estimation from incomplete observations, J Am StatAssoc 1958;53: Hagi D, Deporter DA, Pilliar RM, Arenovich T A targeted with short «review of study outcomes or = 7 mm) endosseous dental implants placed in partially edentulous patients. J Periodontol 2004;75: Emmerich D, AttW, Stappert C Sinusfloor elevation using osteotomes: A systematic review and rneta-analysis. J Periodontol 2005;76: Davarpanah M, Martinez H, Tecucianu JF, Hage G, Lazzara R. The modified osteotome technique. Int J Periodontics Restorative Dent 2001 ;21: Pefiarrocha M, PérezH, Garciá A, Guarinos J. Benign paroxysmal positional vertigo as a complication of osteotome expansion of the maxillary alveolar ridqe. J Oral Maxillofac Surg 2001 ;59: PilliarRM. Overview of surface variability of metallic endosseous dental implants: Textured and porous surface-structured desiqns. Implant Dent 1998;7: Cochran DL A comparison of endosseous dental implant surfaces, J Periodontol 1999;70: Pilliar RM, Simmons CA Mechanical factors and osseointegration: Influence of implant desiqn. In: Zarb GA (ed). Osteoporosis and Dental lrnplants. Chicago: Quintessence, 2001 : Oyonarte R, Pilliar RM, Deporter DA, Woodside DG. Peri-implant bone response to orthodontic loading: Part 2. Implant surface geometry and its effect on regional bone rernodelinq. Am J Orthod Dentofacial Orthop 2005;128: Pilhar RM, Sagals G, Meguid SA, Oyonarte R,Deporter DA Threaded versus poroussurfaced implants as anchorage units for orthodontic treatment: Three-dimensionai finite element analysis of peri-implant bone tissue stresses, Int J Oral Maxillofac Implants 2006;21 : Vaillancourt H, Pilliar RM, McCammond D. Factors affecting crestal bone loss with dental implants partially covered with a porous coating: A finite element analysis. Int J Oral Maxillofac Implants 1996; 11: Volume 29, Number 1,2009
31 Immediate Implants Placed into Infected Sites: A Histomorphometric Study in Dogs Arthur B. Novaes, Jr, DSc*/Guaracilei M. Vidigal, Jr, MSc**/Arthur B. Novaes, DSc***/ Marcio F. M. Grisi, DSc****/Sergio Polloni, MSc****/Adalberto Rosa, MSc***** To study the effect of chronically infected sites on the immediate placement of implants, periapical lesions were induced in the third and fourth premolars of four dogs and the contralateral teeth were used as controls. Nine months after the induction of periapical lesions, experimental and control teeth were extracted, and 28 IMZ implants were immediately placed. After a healing period of 12 weeks, the animals were sacrificed, the hemimandibles were removed, and specimens were prepared to be hard-sectioned and stained with toluidine blue. All areas healed without inflammation or exudation and all implants were clinically immobile and were radiographically determined to be surrounded by normal-appearing bone. Histologically, there were no signs of infection, and the histomorphometric analyses revealed that 28.6% and 38.7% had osseointegrated for the experimental and control implants, respectively. The difference was not statistically significant. It was concluded that chronically infected sites, such as those showing signs of periapical pathosis, may not be a contraindication for immediate implants, if certain clinical measures and preoperative and postoperative care are taken. (INT J ORAL MAXILLOFAC IMPLANTS 1998;13: ) Key words: immediate implants, implants, IMZ, infected site, osseointegration Since the work of Lazzara 1 and others, 2 7 immediate placement of implants has been considered a routine clinical procedure. However, some prerequisites have been established for the indication of immediate implants, such as the extent of bone resorption, the morphology of the defect and whether it will allow placement of the implant at an ideal *****Professor and Chairman, Graduate Periodontology, School of Dentistry, Federal University of Rio de Janeiro, Rio de Janeiro, Brazil. *****Professor, Department of Periodontology, School of Dentistry, Grande Rio University, Rio de Janeiro, Brazil. *****Chairman, Department of Periodontology, School of Dentistry, Ribeirao Preto, University of São Paulo, São Paulo, Brazil. *****Professor, Department of Periodontology, School of Dentistry, Ribeirao Preto, University of São Paulo, São Paulo, Brazil. *****Professor, Department of Oral Surgery, School of Dentistry, Ribeirao Preto, University of São Paulo, São Paulo, Brazil. Reprint requests: Dr Arthur B. Novaes, Jr, Faculdade de Odontologia de Ribeirao Preto, University of São Paulo, Av. do Cafe s/n, Ribeirao Preto, São Paulo, Brazil. novaesjr@forp.usp.br. angle for an esthetic restoration, 8 and the presence or absence of infection. Some authors 3,9 12 consider the presence of infection, such as periapical pathosis, to be a contraindication for the procedure. In a recent clinical report, Novaes Jr and Novaes 13 described three patients in whom immediate implants were successfully placed into infected sites. They reported that chronically infected sites may not necessarily be a contraindication for the placement of immediate implants if appropriate clinical procedures are carefully followed. The objective of this study was to determine histomorphometrically whether chronically infected sites, induced in dogs, would affect the osseointegration of immediate implants. Materials and Methods Four young healthy dogs, weighing 12 to 14 kg, were used in the study in accordance with the Institutional Animal Care and Use Committee. Phase I. The dogs were not fed the night before the procedure. They were anesthetized with an intravenous injection of sodium pentobarbital (30 mg/kg, 500 mg of pentobarbital diluted in 20 ml sodium 422 Volume 13, Number 3, 1998 COPYRIGHT 2000 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY. NO PARTOF THIS ARTICLE MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITH- OUT WRITTEN PERMISSION FROM THE PUBLISHER.
 Apex of extracted root from the experimental side showing areas of root resorption and presence of chronic inflammatory process indicative of periapical pathosis.")
.")


32 Novaes et al Fig 1 (Above) Radiograph of experimental side 9 months after root canal instrumentation. Arrows indicate periapical lesions. Fig 2 (Right) Apex of extracted root from the experimental side showing areas of root resorption and presence of chronic inflammatory process indicative of periapical pathosis. Fig 3 Experimental side 12 weeks after implant placement. Good quality bone around implants and no evidence of radiolucent areas indicating residual infection. Fig 4 Control side 12 weeks after implant placement. Note normal-appearing bone around implants. chloride, resulting in a 25% solution). Bilateral third and fourth mandibular premolars were used, the right side as experimental and the left side as control. On the experimental side, the crowns of the teeth were cut with burs at the cementoenamel junction and removed, exposing the roots and root canals. The pulpal tissue was removed, and the roots were gently instrumented with endodontic files without care to avoid contamination of the canals, since the objective of this procedure was to induce periapical lesions. Radiographs were taken every 3 months to evaluate the size of the developing periapical lesions, and only after 9 months were the lesions large enough to proceed to Phase II (Fig 1). The control side underwent no treatment in this phase. The lesions were considered to be infected because of the experiment design that allowed contamination of the canals for 9 months; the development of periapical lesions, which were visible on the radiographs (Fig 1); the presence of the inflammatory process around the apex of the extracted roots (Fig 2); and the fact that, prior to the surgical procedure, compression of the soft tissues induced purulent exudate to drain through the gingival sulcus and/or the open root canals. Phase II. Nine months after the periapical lesions had been induced in the experimental teeth, the animals were anesthetized in the same manner as described for Phase I. The night before surgery, the animals received an intramuscular injection of 20,000 IU of penicillin and erythromycin (Pentabiótico Veterinário Pequeno Porte, Laboratório Fontoura- White, São Paulo, Brazil) at a dose of 1.0 g/10 kg COPYRIGHT 2000 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY. NO PARTOF THIS ARTICLE MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITH- OUT WRITTEN PERMISSION FROM THE PUBLISHER. The International Journal of Oral & Maxillofacial Implants 423
33 Novaes et al body weight. This is a broad-spectrum antibiotic commonly used to treat infections in small animals. Since each dose allows antibiotic coverage for 4 days, another dose was injected 4 days later, providing 8 days in total of antibiotic coverage. Full-thickness flaps in the area of the third and fourth mandibular premolars were created on the experimental and control sides. The teeth were sectioned in a buccolingual direction at the bifurcation so that the roots could be individually extracted without damaging the bony walls. At the time of extraction, two roots fractured on the control side and were not removed. Following extraction, the alveoli were meticulously debrided and rinsed with a 50 mg/ml solution of tetracycline hydrochloride. IMZ implants (Interpore International, Irvine, CA), mm and slightly larger than the extracted roots, were placed immediately after debridement and rinsing. Fifteen implants were placed on the right side (experimental), and only 13 were placed on the left side (control) since the two roots that fractured were not extracted. (Currently, placement of implants slightly larger than the extracted roots is also possible in humans because of the availability of wide-diameter and wide-tapered implants.) The implants were placed according to the manufacturer s instructions, and flaps were sutured over them to achieve complete coverage. The animals were kept in separate cages and on a soft diet until the sutures were removed 10 days later. They were sacrificed after 12 weeks with an overdose of pentobarbital. Hemimandibles were dissected, radiographed, (Figs 3 and 4), and fixed in a 4% solution of phosphate-buffered formalin (ph 7.0) for 48 hours and then transferred to a solution of 70% ethanol until processing. The specimens were dehydrated in ascending concentrations of alcohol up to 100%, infiltrated and embedded in resin (Technovit 7200 VLC; Kulzer, Werheim, Germany), hard-sectioned using the technique described by Donath and Breuner, 14 and stained with toluidine blue. The roots removed from the experimental side were fixed in 10% formalin, processed for histology, and stained with hematoxylin and eosin to ascertain the presence of the periapical inflammatory process. Histomorphometric Analysis. One longitudinal histologic section from each implant was evaluated using an optic microscope (Carl Zeiss, Oberkuchen/ Wurett, Germany) with a magnification 250. The image selected in the microscope was captured by a video camera and transferred to a Targa Plus plaque connected to a computer with morphometry software (Vidas 21 v2.1, Kontron E lectronic, Munich, Germany) through which the sections were analyzed. With this system, the percentage of implantbone contact, which was determined from the middle one third of the implants, was considered as percentage of osseointegration. The analysis was performed by a single investigator (GMV Jr), who had no knowledge of which were experimental or control sections. Statistical Analysis. The results were analyzed through the confidence interval at the 95% level and using Student s t test. Results Clinical and Radiographic Findings. Healing progressed uneventfully during the 12-week postoperative period, without evidence of significant inflammation or exudation on either the experimental or the control sides. At the time of sacrifice, clinical inspection revealed that all implants were clinically immobile and had no signs of infection. Radiographs taken just before sacrifice showed normal-appearing bone, both around the 15 experimental implants, which showed no evidence of the preexisting periapical lesions (Fig 3), as well as around the 13 control implants (Fig 4). Histologic and Histomorphometric Findings. Histologic processing of the roots extracted from the experimental side confirmed the presence of a chronic inflammatory process around the apex of the roots, along with areas of root resorption (Fig 2). One of the initial 15 experimental implants was also excluded because an oblique section of the block was obtained, and it was therefore not possible to perform the histomorphometry. All remaining implants were included in the study. H istologic analysis showed implants placed in predominantly medullary bone with tissues well healed around them (Figs 5 and 6) and no evidence of the chronic infection on the experimental sides. Histomorphometric measurement around titanium plasma-sprayed implants was found to be somewhat more difficult than around smooth surface implants performed by the authors in other studies, because the plasma spray was separated from the body of the implants in some areas (Fig 7). In areas where this phenomenon did not occur, measurement was easier (Fig 8). The mean percentage of direct bone-implant contact around the midportion of the 14 experimental implants was 28.6 ± 24.8%, with a range of 2.5 to 100%; the mean percentage of bone-implant contact around the 12 control implants was 38.7 ± 25.5%, with a range of 3.9 to 91.2%. The difference was not statistically significant (t = 1.01; P >.05) (Table 1). 424 Volume 13, Number 3, 1998 COPYRIGHT 2000 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY. NO PARTOF THIS ARTICLE MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITH- OUT WRITTEN PERMISSION FROM THE PUBLISHER.
 Low-power photomicrograph ( 4) of implant in the control side 12 weeks after placement.")
 showing area of osseointegration; compact bone-implant interface highlights the Haversian system in the compact bone.")


34 Novaes et al Fig 5 (Left) Low-power photomicrograph (magnification 4) of implant 12 weeks after placement. Note highly medullary bone but normal tissues around implant. Fig 6 (Right) Low-power photomicrograph ( 4) of implant in the control side 12 weeks after placement. Fig 7 High-power photomicrograph ( 80) showing direct bone-implant contact and presence of portions of the plasma spray separated from the body of the implant. Fig 8 High-power photomicrograph ( 80) showing area of osseointegration; compact bone-implant interface highlights the Haversian system in the compact bone. Discussion Although the issue of immediate implant placement in infected sites has not itself been studied, some authors 3,9 12,15 consider it a contraindication for the procedure. This investigation had the objective of studying this issue in dogs, following the induction of periapical lesions in the mandibular third and fourth premolars, using the contralateral teeth as controls. After a 12-week healing period following implant placement, the results showed that healing occurred uneventfully; all implants, control and experimental, were clinically immobile at the time of sacrifice, and there was no significant inflammation or exudation. Radiographically, all implants were surrounded by normal-appearing bone, and they showed no signs of the preexisting radiolucent lesions on the experimental sides. For the histomorphometric analysis, the middle one third of the implant was used, as suggested by Evans et al, 16 for several reasons: to avoid misinterpreting loss of crestal bone and epithelial downgrowth adjacent to the polished collar of implants, commonly seen in dogs as reported by Block et al, 17 Gammage et al, 18 and Weber et al 19 ; to avoid the apical one third because of the vent present in the apical region of the implant; and because the implants approximated or slightly penetrated the superior wall of the inferior alveolar canal. However, the main interest in the middle one third was because it corresponded to the area where the periapical lesions had COPYRIGHT 2000 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY. NO PARTOF THIS ARTICLE MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITH- OUT WRITTEN PERMISSION FROM THE PUBLISHER. The International Journal of Oral & Maxillofacial Implants 425
35 Novaes et al Table 1 Percentage of Bone-Implant Contact at Experimental and Control Sites Bone-implant contact (%) Implants Experimental Control Mean SD Difference between control and experimental = 10.1% (38.7 to 28.7). 95% confidence interval for difference: 10.4 to 30.5; t = with 24 degrees of freedom; P =.320. been. As can be seen in the preoperative radiographs (Fig 1), the lesions were several millimeters above the superior wall of the inferior alveolar canal. The percentages of osseointegration in this study were 38.7% for the control implants and 28.6% for the experimental implants, a difference that was not statistically significant. Our findings are lower than the 47.9% reported by Ettinger et al, 20 which can be explained in part by the fact that the implants in this study were placed in highly medullary bone, a finding only observed during the histologic evaluation of the sections. F urthermore, three experimental and two control implants (Table 1) had very low percentages of osseointegration (less than 6.0%), far below the average seen for the remaining implants. If one were to exclude these implants from the analysis, the results would be comparable. The small percentages of osseointegration for these five implants could perhaps be explained, as pointed out by Ettinger et al, 20 by the quality of bone at those sites, by the remodeling process going on at that time, and by the use of a single longitudinal section for analysis. The commonly used single longitudinal section has limitations, since different specimens from the same implant may reveal higher percentages of osseointegration because the implant-bone interface is a dynamic three-dimensional entity. 20 According to the objectives of this study, the presence of chronically infected sites did not compromise healing and osseointegration of the immediately placed implants. Residual infection was not detected (1) clinically both sides healed well without significant inflammation and without exudation; (2) radiographically all implants had good quality bone around them without radiolucent areas that could indicate the presence of residual lesions; or (3) histologically, which was most important. Summary The results of this study support the clinical findings in humans reported previously 13 and permit the conclusion that chronically infected sites, such as those showing the presence of periapical pathosis, may not be a contraindication for immediate implants if appropriate antibiotics are administered preoperatively and postoperatively, and if meticulous cleansing and debridement of the alveoli are performed before implant placement, as described previously. 13 Acknowledgments The authors thank Dr Liane C. A. Aragones and the Napio Center of the School of Dentistry of Bauru, University of São Paulo, Brazil, for processing the histologic specimens, and Interpore International for providing the implants and drills. References 01. Lazzara RJ. Immediate implant placement into extraction sites. Surgical and restorative advantages. Int J Periodont Rest Dent 1989;9: Nyman S, Lang NP, Buser D, Bragge U. Bone regeneration adjacent to titanium dental implants using guided tissue regeneration: A report of two cases. Int J Oral Maxillofac Implants 1990;5: Becker W, Becker BE. Guided tissue regeneration for implants placed into extraction sockets and for implant dehiscences. Surgical techniques and case reports. Int J Periodont Rest Dent 1990;10: Balshi TJ, Hernandez RE, Cutler RH, Hertzog CF. Treatment of osseous defects using Vycril mesh (Polyglactin 910) and the Brånemark implant. Int J Oral Maxillofac Implants 1991;6: Novaes AB Jr, Novaes AB. IMZ implants placed into extraction sockets in association with membrane therapy (Gengiflex) and porous hydroxyapatite. A case report. Int J Oral Maxillofac Implants 1992;7: Novaes AB Jr, Novaes AB. Bone formation over an IMZ implant placed into an extraction socket in association with membrane therapy (Gengiflex). Clin Oral Implants Res 1993;4: Gelb DA. Immediate implant surgery: Three year retrospective evaluation of 50 consecutive cases. Int J Oral Maxillofac Implants 1993;8: Nevins M, Mellonig JT. The advantages of localized ridge augmentation prior to implant placement. A staged event. Int J Periodont Rest Dent 1994;14: Lundgren D, Nyman S. Bone regeneration in 2 stages for retention of implants. Clin Oral Implants Res 1991;2: Werbitt MJ, Goldberg PV. The immediate implant: Bone preservation and bone regeneration. Int J Periodont Rest Dent 1992;12: Volume 13, Number 3, 1998 COPYRIGHT 2000 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY. NO PARTOF THIS ARTICLE MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITH- OUT WRITTEN PERMISSION FROM THE PUBLISHER.
36 Novaes et al 11. Wilson TG Jr. Guided tissue regeneration around dental implants in immediate and recent extraction sockets: Initial observations. Int J Periodont Rest Dent 1992;12: Barzilay I. Immediate implants: Their current status. Int J Prosthodont 1993;6: Novaes AB Jr, Novaes AB. Immediate implants placed into infected sites: A clinical report. Int J Oral Maxillofac Implants 1995;10: Donath K, Breuner G. A method for the study of undecalcified bones and teeth with attached soft tissue. J Oral Pathol 1992;11: Tolman DE, Keller EE. Endosseous implant placement immediately following dental extraction and alveoloplasty: Preliminary report with a 6-year follow-up. Int J Oral Maxillofac Implants 1991;6: Evans GH, Mendez AJ, Caudill RF. Loaded and nonloaded titanium versus hydroxylapatite-coated threaded implants in the canine mandible. Int J Oral Maxillofac Implants 1996;11: Block MS, Kent JN, Kay JF. Evaluation of hydroxylapatitecoated titanium dental implants in dogs. J Oral Maxillofac Surg 1987;45: Gammage DD, Bowman AE, Meffert RM, Cassingham RJ, Davenport WA. A histologic and scanning electron microcraphic comparison of the osseous interface in loaded IMZ and Integral implants. Int J Periodont Rest Dent 1990;10: Weber HP, Buser D, Donath K, Fiorellioni JP, Doppalapudi V, Paquette DW, et al. Comparison of healed tissues adjacent to submerged and non-submerged unloaded titanium dental implants. Clin Oral Implants Res 1996;7: Ettinger RL, Spivey JD, Han D-H, Moorbusch GF. Measurement of the interface between boen and immediate endosseous implants: A pilot study in dogs. Int J Oral Maxillofac Implants 1993;8: COPYRIGHT 2000 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY. NO PARTOF THIS ARTICLE MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITH- OUT WRITTEN PERMISSION FROM THE PUBLISHER. The International Journal of Oral & Maxillofacial Implants 427



37 2 The Excessive Loss of Branemark Fixtures in Type IV Bone: A 5-Year Analysis* Robert A. Jaffin and Charles L. Berman The predictability of branemark implants has been well documented. High success rates in the maxilla and mandible in fully and partially edentulous patients can be expected. A host of factors may be attributed to the etiology of fixture loss. However, the quality of bone stands out as the single greatest determinant in fixture loss. Types I, II, and III bone offer good strength. Type IV bone has a thin cortex and poor medullary strength with low trabecular density. Ninety percent of 1,054 implants placed were in Types I, II, and III bone. Only 3% of these fixtures were lost; of the 10% of the fixtures placed in Type IV bone, 35% failed. Presurgical determination of Type IV bone may be one method to decrease implant failure. J Periodontol 1991; 62:2^1. Key Words: Implants, osseointegrated. The predictability of Branemark implants has been well documented.1'2 Long-term success rates of 96% to 99% in the edentulous mandible and 90% over 5 years, and 80% over 10 years have been reported in the edentulous maxilla.3 Reports on partially edentulous cases show high success rates.4,5 Centers world wide have substantiated the findings of the Institute for Applied Biotechnology.6 When proper protocol is followed, most Branemark cylindrical screw implants composed of commercially pure titanium will become integrated into bone and soft tissue and remain disease free for many years. The etiology of fixture loss may be attributed to a host of factors: occlusal overload, infection in the mouth, operator error, and bone of insufficient quantity and/or quality.7 In order to evaluate occlusal overload, it must be determined whether the maximum number of fixtures of optimal length were utilized. If not, then the failure was in treatment planning and/or skill and not the fault of the implant or occlusion. Overload is most often encountered in patients with few and short (7 mm) fixtures. Other instances of overload may be due to poor bone quality and hyperfunction. Infection may contaminate a site; therefore, periodontal disease and carious infections must be eradicated before fixture installation. Surgical error can lead to drilling in an elliptical manner, thereby widening the site. Improper irrigation can cause bone death. Previous reports of implant success/failure have not placed sufficient emphasis on the quality of bone. Engquist tried to correlate fixture loss in overdenture patients to bone qual- *Private practice, Hackensack, nj. Jaw Bone Anatomy Homogeneous cortical bone Thick cortical bone with marrow cavity Jaw Bone Anatomy Thin cortical bone Very thin cortical with dense trabecular bone. with low bone of good density trabecular strength bone of poor strength IV Figure 1. Jaw bone anatomy, describing 4 bone types. ity.8 Branemark described four types of bone which encompass most situations (Fig. 1). Types I, II, and III bone have
* 1.7 10 433 7+ (6)* 1.")

38 Volume 62 Number 1 JAFFIN, BERMAN 3 Table 1: Fixture Loss by Location and Bone Type Position Posterior Mandible Anterior to Mental Foramina Maxilla Types I, II, and III Type IV Total Number Number Number Number Non- Number Non- Number Non- Placed Integrated % Lost Placed Integrated % Lost Placed Integrated % Lost (3)* (6)* Total (9) 6.1 Removed for psychiatric and positional reasons. enough cortex to stabilize the implant at installation and have sufficient strength to hold integrated implants in function. Type IV bone offers little cortex and minimal internal strength. The purpose of this article is to present an analysis of fixture loss over 5 years of a private periodontal practice, in the placement of 1,054 consecutively installed and uncovered Branemark implants and to correlate successful/ failure rates to bone Type IV. MATERIALS AND METHODS All patients underwent an extensive presurgical work-up, including medical and psychological histories. Patients were not accepted for implants if they could not tolerate the surgical procedure, could not accept the possible failure of fixtures, or had received radiation to the head or neck within the past 18 months. A team approach was utilized in diagnosis. Every patient was evaluated by the prosthodontist/restorative dentist before fixture installation. Guide Stents were fabricated in most cases. Radiographic evaluation included periapicals, panorex, lateral cephalometry, and CT scans where indicated. Reformatted scans Houncefield radiological and density measurements were included in some patients. Dental infection, periodontal disease, and hopeless teeth were treated before fixture installation. All patients washed with Hibiclens before surgery. On the day of the surgery, patients were given 1 gram of penicillin, 1 hour before surgery. In addition, patients scrubbed their mouths with.12% Chlorhexidine thoroughly. Patients were dressed in scrub suits and draped, in the operating room, utilizing sterile technique. Fixtures were installed according to the Branemark technique. Bone type was determined during osteotomy, in site preparation, with either the round bur or 2 mm twist drill. In a few patients, bone type differed from site to site. If Type IV bone or soft Type III bone was noted, the bone was not tapped before fixtures were installed. More recently, self-tapping fixtures were utilized. The maximum number of fixtures of optimal length were placed. This was determined by the size of the area and the number of teeth Table 2: Percent of Type TV Fixtures Position % Uncovered Maxilla 52/ % Posterior Mandible 30/ % Anterior to Mental Foramina 20/ % Total 102/1, % missing. Following surgery, patients were advised to apply pressure to the area with wet cold gauze. Appropriate antibiotics were prescribed for 1 week. Sutures were removed at 7 to 14 days and removable prosthesis were altered and relined by the restorative dentist at that time. The quantity and quality of bone was noted for each fixture site. Second stage surgery occurred 3 to 6 months after fixture installation, utilizing the technique previously described.9 RESULTS From October 1984 through September 1989, 1,054 Branemark fixtures were installed and uncovered in 246 jaws; 444 were placed in the maxilla; 433 were placed anterior to the mental foramina, and 177 in the posterior mandible. A total of 952 fixtures were placed in bone Types I, II, and III and 102 in Type IV. A total of 65 fixtures (37 in the maxilla; 21 in the posterior mandible, and 7 in the anterior mandible) did not integrate and were removed after placement, at second stage, or after rehabilitation; another 9 were removed for psychiatric and positional reasons (Table 1). The Type IV bone fixture loss rate greatly exceeded that in other types of bone: 44% (23/52) in the maxilla; 37% (11/30) in the posterior mandible; and 10% (2/20) in the anterior mandible. This is a total failure rate of 35% (36/ 102). Fixture failure rates in Types I, II, and III bone were considerably lower: 3.6% (14/392) in the maxilla; 1.2% (5/ 413) in the anterior mandible; and 6.8% (10/147) in the posterior mandible. Overall, the failure rate was 3% (29/ 952). Table 2 shows the percentage of Type IV fixtures to


39 4 PREDICTABILITY OF IMPLANTS IN BONE OF DIFFERING QUALITY J Periodontol January 1991 Table 3: Percent of Type IV Lost to Total Losses Position % Lost Maxilla 23/37 62% Posterior Mandible 11/21 52% Anterior to Mental Foramina 2/7 29% Total 36/65 55% the total number of fixtures and Table 3 shows the percentage of Type IV fixture loss to total losses. DISCUSSION Previous reports on implant success rates have not attempted to isolate fixture failure rate by bone type. While compiling statistics, it became evident that Type IV bone was the single greatest determinant in predicting fixture failure. In Types I, II, and III, total fixture failure rate was 3% (29/952), however, in Type IV bone, 36 of 102 implants did not integrate (35%). The non-integrated fixtures were removed usually at the time of second stage surgery. Some lost integration after the final prosthesis was placed. Of the 24 patients with Type IV bone, 8 were not restored according to the original prescription. In some cases, an over-denture was constructed instead of a fixed prosthesis. In others, the original prosthesis was lost and an over-denture fabricated or additional fixtures were placed at a later time. Although periapical radiographs offer some diagnostic help in identitfying Type IV bone, they may be deceiving since a thick buccal or lingual plate may obscure the soft medullary nature of the internal bone. The diagnosis of Type IV bone is usually made at osteotomy. By this time, the tentative restorative treatment plan has usually been decided. Presurgical evaluation of Type IV bone could enhance the predictability of the treatment. An alternative treatment (fixed vs. removable) may be discussed with the patient. Additional fixtures (if room permits) may also be prescribed. A shorter cantilever may also enhance the prognosis. Press fit implants may also prove to be a viable alternative but need further investigation. The utilization of reformatted CT scans has aided in treatment planning cases. They offer parasagittal views of bone not available through standard dental radiography. CT scans can also provide radiological densitometric readings of bone (Houncefield Units). This evaluation provides the surgeon with a relative idea of the internal morphology of the bone. Advanced knowledge of Type IV bone can lead to an alternative treatment plan or one that does not include implants. REFERENCES 1. Adell R, Lekholm U, Rockler B, Branemark PI. A 15 year study of osseointegrated implants in the treatment of the edentulous jaw. Int J Oral Surg 1981;10: Laney WR, Tolman D, Keller E, et al. Dental implants: Tissue integrated prosthesis utilizing the osseointegration concept. Mayo Clinic Proc 1986; 61: Branemark PI, Hansson BO, Adell R, et al. Osseointegrated implants in the treatment of the edentulous jaw: Experience from a 10 year period. Scand J Plast Reconst Surg (Suppl); 1977: Jemt T, Lekholm U, Adell R. Osseointegration in the treatment of partially edentulous patients: A preliminary study of 876 consecutively installed fixtures. Int J Oral Maxillofac Imp 1989; 4: Ericsson I, Lekholm U, Branemark PI, Lindhe J, Glantz PO, Nyman S. A clinical evaluation of fixed bridge work supported by a combination of teeth and osseointegrated titanium fixtures. J Clin Periodontol 1986; 13: Albrektsson T, Bergman B, Folmertt, et al. A multicenter study of osseointegrated oral implants. J Prosthet Dent 198; 60: Jaffin R, Berman C. Coping with the dilemmas of osseointegration treatment. Presented at the Annual Meeting of The American Academy of Periodontology; October 26, 1988; San Diego, CA. 8. Engquist B, Bergendal T, Kallis T. A retrospective multicentered evaluation of osseointegrated implants supporting overdentures. Int J of Oral and Maxfac Impl 1988; 3: Jaffin R. Biologic and clinical rationale for second stage surgery and maintenance. Dent Clin North Am 1989; 33: Send reprint requests to: Dr. Robert A. Jaffin, 274 State Street, Hackensack, NJ Accepted for publication June 4, 1990.
40 Interventional Medicine & Applied Science, Vol. 5 (4), pp (2013) REVIEW Role of primary stability for successful osseointegration of dental implants: Factors of influence and evaluation FAWAD JAVED 1, *, HAMEEDA BASHIR AHMED 2, ROBERTO CRESPI 3, GEORGIOS E. ROMANOS 4 1 Eng. A.B. Research Chair for Growth Factors and Bone Regeneration, 3D Imaging and Biomechanical Laboratory, College of Applied Medical Sciences, King Saud University, Riyadh, Saudi Arabia 2 Department of Dentistry, Al-Farabi Dental College, Riyadh, Saudi Arabia 3 Department of Dentistry, Vita Salute University, San Raffaele Hospital, Milan, Italy 4 Department of Dental Medicine, Stony Brook University, Stony Brook, NY, USA *Corresponding author: Dr. Fawad Javed; Eng. A.B. Research Chair for Growth Factors and Bone Regeneration, 3D Imaging and Biomechanical Laboratory, College of Applied Medical Sciences, King Saud University, Riyadh, Saudi Arabia; fawjav@gmail.com (Received: September 24, 2013; Revised manuscript received: September 29, 2013; Accepted: September 30, 2013) Abstract: A secure implant primary (mechanical) stability is positively associated with a successful implant integration and long-term successful clinical outcome. Therefore, it is essential to assess the initial stability at different time-points to ensure a successful osseointegration. The present study critically reviews the factors that may play a role in achieving a successful initial stability in dental implants. Databases were searched from 1983 up to and including October 2013 using different combinations of various keywords. Bone quality and quantity, implant geometry, and surgical technique adopted may significantly influence primary stability and overall success rate of dental implants. Keywords: dental implants, bone density, implant surface topography, osseointegration, primary stability, surgical technique Introduction Traditionally, endosseous implants are loaded once bone healing has occurred, which takes approximately 3 months in the mandible and 6 months in the maxilla [1, 2]. Today, modifications of this treatment protocol using immediate loading of implants are an eminent and acknowledged treatment strategy for the rehabilitation of missing teeth [3 5]. Histologic and histomorphometric evaluation of immediately loaded implants recovered from humans has also shown a high degree of bone-to-implant contact percentages [6, 7]. However, for any implant procedure, successful implant integration is a prerequisite criterion, which depends on a series of procedure-related and patient-dependent measures [8]. Successful osseointegration from the clinical standpoint is a measure of implant stability, which occurs after implant integration [9]. Two terms, such as the primary and the secondary implant stability, are related to implant therapy. Primary stability is associated with the mechanical engagement of an implant with the surrounding bone, whereas bone regeneration and remodelling phenomena determine the secondary (biological) stability to the implant [9, 10]. A secure primary stability is positively associated with a secondary stability [11]. Extent of implant stability may also depend on the situation of surrounding tissues [3, 12]. Bone quantity and quality, implant geometry, and surgical technique adopted are also among the predominant clinical factors that affect primary stability [13]. Therefore, it is essential to assess the implant stability at different time-points in order to ensure a successful osseointegration. In this context, the objective of the present review was to assess the factors that may play a role in achieving a successful primary stability in dental implants. Materials and Methods The National Library of Medicine, Washington DC (MEDLINE PubMed) was searched for appropriate articles addressing the focused question. Databases were searched from 1983 up to and including October 2013 using the following terms in different combinations: bone, dental, design, implant, immediate DOI: /IMAS ISSN Akadémiai Kiadó, Budapest
41 Primary stability and osseointegration loading, implant length, implant diameter, maxilla, mandible, narrow implant, osseointegration, primary stability, surgical technique, and wide implant. The eligibility criteria were based on human and experimental studies, use of control group, articles published only in English language, and reference list of potentially related original and review studies. The second step was to hand-search the reference lists of original and review studies that were found to be relevant in the first step. After final selection of the papers, those that fulfilled the selection criteria were processed for data extraction. The structure of the present literature review was customized to mainly summarize the relevant information. Pre-requisites for a successful primary stability Primary stability is accomplished when the implant is placed in the bone in such a position that it is wellseated. This allows the implant to mechanically adapt to the host bone until secondary stability is achieved [13]. Impaired primary implant stability has been shown to jeopardize the osseointegration process [14]. The success of this adaptation, however, depends on several factors, including the density and dimension of the bone surrounding the implant, the implant design, and surgical technique used (Fig. 1). Fig. 1. Factors affecting implant stability Bone density and quality The significance of bone density and its association with implant dentistry has existed for more than two decades. Several classifications regarding bone density have been recommended as shown in Fig. 2. Bone quality is often referred to as the amount (and their topographic relationship) of cortical and cancellous bone in which the recipient site is drilled. A poor bone quantity and quality have been indicated as the main risk factors for implant failure as it may be associated with excessive bone resorption and impairment in the healing process compared with higher density bone [15 17]. Clinical studies have reported dental implants in the mandible to have higher survival rates compared to those in the maxilla, especially for the posterior maxilla [18, 19]. Bone quality has been considered as the basic cause of this difference. In the posterior maxilla, there is commonly thinner cortical bone combined with thicker trabecular bone compared to the mandible [20, 21]. Clinically, a poor degree of bone mineralization or limited bone resistance is observed in bones with poor densities, which are often referred to as soft bones [20, 22]. It has been shown that achieving optimum primary stability in soft bones is difficult and is also related to a higher implant failure rate for the implants placed in such bones [15, 23]. Turkyilmaz et al. [24] reported the bone quality around the implant to be superior in the mandible compared to the maxilla. A clinical study [25] with 158 implant sites from 85 patients indicated a strong correlation between bone density and dental implant stability. Results by Miyamoto et al. [26] demonstrated that dental implant stability is positively associated with the thickness of cortical bone thickness. In contrast to the previous studies, additional studies in the posterior mandible showed high failure rates due to the poor bone quality as well as other additional factors [27, 28]. Computerized tomography (CT) has been regarded as the best radiographic method for analyzing the morphological and qualitative analysis of the residual bone [29 31]. It is also a valuable means for evaluating the relative distribution of cortical and cancellous bone [32]. However, the density of the surrounding bone seems to play an essential role in high occlusal forces, and therefore, the high bone-to-implant (BIC) percentages of a thin, carpet -like bone in contact with the implant surface seems to be not clinically significant compared to lower rate of BIC in a thick bone. Intraoperative surgical techniques, such as bone condensing, undersizing the osteotomy, improve the bone density and increase the primary (mechanical) stability. In contrast to that, loading effects on the periimplant bone under delayed or immediate loading conditions influence the secondary (biological) stability increasing the percentage of the bone-to-implant (BIC) contacts [27, 33]. Interventional Medicine & Applied Science 163 ISSN Akadémiai Kiadó, Budapest

42 Javed et al. Fig. 2. Bone dentistry classifications Implant design Implant design refers to the three-dimensional structure of an implant with all the components and features that characterize it. It has been reported that the implant design is a vital parameter for attaining primary stability [34]. The texture of an implant s surface can influence the bone implant interface. Studies [6, 33, 35] have demonstrated a relationship between implant design and osseointegration. Implants of varying designs, placed in different bone qualities, reach various degrees of stability, which may determine their future clinical performance [36, 37]. Originally, implants were fabricated in a parallel design; however, they were not appropriate for most applications. Tapered implants were later introduced to enhance aesthetics and assist implant placement between adjacent natural teeth [38]. The hypothesis behind using tapered implants was to provide a degree of compression of the cortical bone in an implant site with inadequate bone [39]. Cylindrical wide body implants increase the risk of labial bone perforation especially in thin alveolar ridges due to presence of buccal concavities, whereas the decrease in diameter of the tapered implants toward the apical region accommodates for the labial concavity [40]. However, according to Chong et al. [34], if bone quality and quantity are optimal, then they may compensate for implant design inadequacy. Implant surface characteristics and diameter have also been shown to influence primary stability. Rough implant surfaces present a larger surface area and allow a firmer mechanical link to the surrounding tissues [11]. In vitro studies [41, 42] have shown that sandblasted implant surfaces promote peri-implant osteogenesis by enhancing the growth and metabolic activity of osteoblasts [41, 42]. Studies [6, 43, 44] have shown that surface topography and roughness positively influence the healing process by promoting favorable cellular responses and cell surface interactions. In poor bone quality sites, implants with an acid-etched surfaces can achieve a significantly higher bone-to-implant contact compared to implants with a machined surface [45]. Clinical studies have shown that implants with smaller diameters (less than 3.0 millimeters) provide sufficient primary stability in cases with a limited bone volume [46, 47]. It is accepted that all implants display some extent of bone loss after osseointegration and through time of function. It has been claimed that the introduction of microthreads or retention grooves at the neck of the implant may assist in reducing distributing stress and reducing the extent of bone loss following the implant installation [48]. In the reality, crestal bone preservation can be associated with the surgical technique and the presence of platform switching [49]. In addition, the progressive thread design seems to decrease the compression of the crestal bone preserving in that way the crestal bone loss [49]. ISSN Akadémiai Kiadó, Budapest 164 Interventional Medicine & Applied Science
43 Primary stability and osseointegration Surgical technique Besides the quantity and quality of bone and morphology of the implant, the surgical technique adopted also influences primary stability. Therefore, the undersized drilling technique was introduced to locally optimize bone density and subsequently improve primary stability. Numerous modifications in surgical technique have been described which might assist in enhancing primary stability of dental implants. Some studies [50, 51] recommend the use of a final drill diameter which is smaller than the diameter of the implant; however, Summers [52] recommended the technique of bone condensing, where, after using the pilot drill, the cancellous bone is pushed aside with condensers (osteotomes), thus, increasing the density of the surrounding bone, increasing in that way the initial implant stability. It has been reported high survival rates with the immediate loading of dental implants, which are attributed to high primary stability [43, 53]. Some studies have also preferred insertion torque as a determinant of implant stability, and torque values of 32, 35, or 40 Ncm and higher have been chosen as thresholds for immediate loading [54, 55]. This threshold seems to be important due to the selection of implant abutment connections, which have the need of this torque to engage the abutment to the implant body via the fixation screw based on the manufacturer guidelines. Also implants placed in a weak bone (poor bone quality) may be loaded immediately and demonstrate high survival rates when the final torque in the implant abutment connection is lower, i.e., nearly Ncm [13]. Methods of evaluation of the primary stability Two methods are usually employed to measure the clinical stability of an implant, namely, the Periotest (PT) and resonance frequency analysis (RFA) measurement using Osstell device. The PT gauges temporal contact of the tip of the instrument during repetitive percussions on the implant. PT values include a narrow range over the scale of the instrument and, thus, provide comparatively less sensitive information concerning implant stability [56]. It has been suggested that the measurement of the moment of force or torque (required for seating an implant in bone) can also be used to measure the primary stability of an implant [57]. The RFA device measures the resonance frequency of a transductor attached to the implant body, which is stimulated by different frequencies. According to a study by Sul et al. [58], RFA is a reliable indicator for identifying implant stability with assurance. This instrument has a graphic display panel showing the implant stability quotient (ISQ) values, which indicate the firmness at the implant tissue interface [59]. ISQ values greater than 65 have been regarded as most favorable for implant stability, whereas ISQ values below 45 indicate a poor primary stability [60]. However, there is no justification for a routine clinical use of the PT and RFA techniques [61], as a disadvantage of the ISQ evaluation technique is that the value is dependent on the insertion of the magnet (transducer) to the implant. When the transducer is not well screwed on the implant body (without to use the final insertion torque), a low ISQ value has been evaluated. In addition, the ISQ value is possible to be performed only before the final abutment is connected and cannot be performed with the prosthetic restoration. Further modifications of this technique are needed in order to be able to evaluate the implant stability in a precise and clinical reliable way. Effect of micromotions on primary stability When the ends of a fractured long bone are reduced, then there should be absolutely no movement between the fragments to endorse fracture healing [62]. This happens because movements, even at the micrometer range, can induce a stress or strain that may hinder the formation of new cells in the gap. The same phenomenon is applied at the bone-to-implant interface [63]. The induction of micromotion during functional loading may primarily be responsible for failure of osseointegration and ultimately implant loss [64]. Micromotions above micrometers may negatively influence osseointegration and bone remodelling by forming fibrous tissues and inducing bone resorption at the bone-to-implant interface [65 67]. Therefore, a high initial (mechanical) stability is essential for a successful osseointegration of dental implants. Studies [27, 33, 68] have reported that a well-controlled micromotion positively influenced bone formation; therefore, more advanced clinical conditions, like immediate functional loading of implants placed in healed ridges or also fresh extraction sockets, seem to improve the peri-implant bone density and improve the implant integration. Conclusions This literature review highlights the importance of achieving a successful primary stability for successful implant integration. Bone quality and quantity, implant geometry, and surgical technique adopted may significantly influence implant initial stability and overall success rate of dental implants. Interventional Medicine & Applied Science 165 ISSN Akadémiai Kiadó, Budapest
44 Javed et al. * * * Funding sources: The authors thank the College of Dentistry Research Centre and Deanship of Scientific Research at King Saud University, Saudi Arabia for funding this research project (Project # FR 0075). Authors contributions: FJ wrote the manuscript and revised it prior to submission, HBA performed the literature search and revised the manuscript for English vocabulary. RC wrote the manuscript and revised it prior to submission. GER designed and mentored the study, wrote the manuscript and revised it prior to submission. Conflict of interest: None. References 1. Branemark PI: Osseointegration and its experimental background. J Prosthet Dent 50, (1983) 2. de Freitas RM, Susin C, Spin-Neto R, Marcantonio C, Wikesjö UME, Pereira LAVD, Marcantonio E Jr: Horizontal ridge augmentation of the atrophic anterior maxilla using rhbmp-2/acs or autogenous bone grafts: A proof-of-concept randomized clinical trial. J Clin Periodontol 40, (2013) 3. Javed F, Romanos GE: Impact of diabetes mellitus and glycemic control on the osseointegration of dental implants: a systematic literature review. J Periodontol 80, (2009) 4. Romanos GE: Treatment of advanced periodontal destruction with immediately loaded implants and simultaneous bone augmentation: a case report. J Periodontol 74, (2003) 5. Penarroch a M, Boronat A, Garcia B: Immediate loading of immediate mandibular implants with a full-arch fixed prosthesis: a preliminary study. J Oral Maxillofac Surg 67, (2009) 6. Romanos GE, Johansson CB: Immediate loading with complete implant-supported restorations in an edentulous heavy smoker: Histologic and histomorphometric analyses. Int J Oral Maxillofac Implants 20, (2005) 7. Romanos GE, Testori T, Degidi M, Piattelli A: Histologic and histomorphometric findings from retrieved, immediately occlusally loaded implants in humans. J Periodontol 76, (2005) 8. Beer A, Gahleitner A, Holm A, Tschabitscher M, Homolka P: Correlation of insertion torques with bone mineral density from dental quantitative CT in the mandible. Clin Oral Implants Res 14, (2003) 9. Natali AN, Carniel EL, Pavan PG: Investigation of viscoelastoplastic response of bone tissue in oral implants press fit process. J Biomed Mater Res B Appl Biomater 91, (2009) 10. Greenstein G, Cavallaro J, Romanos G, Tarnow D: Clinical recommendations for avoiding and managing surgical complications associated with implant dentistry: A review. J Periodontol 79, (2008) 11. Davies JE: Mechanisms of endosseous integration. Int J Prosthodont 11, (1998) 12. Javed F, Almas K: Osseointegration of dental implants in patients undergoing bisphosphonate treatment: A literature review. J Periodontol 81, (2010) 13. Romanos GE: Bone quality and the immediate loading of implants Critical aspects based on literature, research, and clinical experience. Implant Dent 18, (2009) 14. Roos J, Sennerby L, Albrektsson T: An update on the clinical documentation on currently used bone anchored endosseous oral implants. Dent Update 24, (1997) 15. Jaffin RA, Berman CL: The excessive loss of Branemark fixtures in type IV bone: A 5-year analysis. J Periodontol 62, 2 4 (1991) 16. Ulm C, Kneissel M, Schedle A, Solar P, Matejka M, Schneider B, Donath K: Characteristic features of trabecular bone in edentulous maxillae. Clin Oral Implants Res 10, (1999) 17. Herrmann I, Lekholm U, Holm S, Kultje C: Evaluation of patient and implant characteristics as potential prognostic factors for oral implant failures. Int J Oral Maxillofac Implants 20, (2005) 18. Jemt T, Stenport V: Implant treatment with fixed prostheses in the edentulous maxilla. Part 2: Prosthetic technique and clinical maintenance in two patient cohorts restored between 1986 and 1987 and 15 years later. Int J Prosthodont 24, (2011) 19. Jemt T, Stenport V, Friberg B: Implant treatment with fixed prostheses in the edentulous maxilla. Part 1: Implants and biologic response in two patient cohorts restored between 1986 and 1987 and 15 years later. Int J Prosthodont 24, (2011) 20. Jacobs R: Preoperative radiologic planning of implant surgery in compromised patients. Periodontol , (2003) 21. Shibli JA, Mangano C, Mangano F, Rodrigues JA, Cassoni A, Bechara K, Ferreia JD, Dottore AM, Iezzi G, Piattelli A: Boneto-implant contact around immediately loaded direct laser metalforming transitional implants in human posterior maxilla. J Periodontol 84, (2013) 22. Lazzara R, Siddiqui AA, Binon P, Feldman SA, Weiner R, Phillips R, Gonshor A: Retrospective multicenter analysis of 3i endosseous dental implants placed over a five-year period. Clin Oral Implants Res 7, (1996) 23. Johns RB, Jemt T, Heath MR, Hutton JE, McKenna S, McNamara DC, van Steenberghe D, Taylor R, Watson RM, Herrmann I: A multicenter study of overdentures supported by Branemark implants. Int J Oral Maxillofac Implants 7, (1992) 24. Turkyilmaz I, Tozum TF, Tumer C: Bone density assessments of oral implant sites using computerized tomography. J Oral Rehabil 34, (2007) 25. Turkyilmaz I, McGlumphy EA: Influence of bone density on implant stability parameters and implant success: A retrospective clinical study. BMC Oral Health 8, 32 (2008) 26. Miyamoto I, Tsuboi Y, Wada E, Suwa H, Iizuka T: Influence of cortical bone thickness and implant length on implant stability at the time of surgery Clinical, prospective, biomechanical, and imaging study. Bone 37, (2005) 27. Schwartz-Arad D, Samet N: Single tooth replacement of missing molars: A retrospective study of 78 implants. J Periodontol 70, (1999) 28. Becktor JP, Eckert SE, Isaksson S, Keller EE: The influence of mandibular dentition on implant failures in bone-grafted edentulous maxillae. Int J Oral Maxillofac Implants 17, (2002) 29. Turkyilmaz I, Tozum TF, Tumer C, Ozbek EN: Assessment of correlation between computerized tomography values of the bone, and maximum torque and resonance frequency values at dental implant placement. J Oral Rehabil 33, (2006) 30. Lee S, Gantes B, Riggs M, Crigger M: Bone density assessments of dental implant sites: 3. Bone quality evaluation during osteotomy and implant placement. Int J Oral Maxillofac Implants 22, (2007) 31. Al-Askar M, O Neill R, Stark PC, Griffin T, Javed F, Al-Hezaimi K: Effect of single and contiguous teeth extractions on alveolar bone remodeling: A study in dogs. Clin Implant Dent Relat Res 15, (2013) 32. Shahlaie M, Gantes B, Schulz E, Riggs M, Crigger M: Bone density assessments of dental implant sites: 1. Quantitative computed tomography. Int J Oral Maxillofac Implants 18, (2003) 33. Romanos GE, Toh CG, Siar CH, Wicht H, Yacoob H, Nentwig GH: Bone-implant interface around titanium implants under different loading conditions: a histomorphometrical analysis in the Macaca fascicularis monkey. J Periodontol 74, (2003) ISSN Akadémiai Kiadó, Budapest 166 Interventional Medicine & Applied Science
45 Primary stability and osseointegration 34. Chong L, Khocht A, Suzuki JB, Gaughan J: Effect of implant design on initial stability of tapered implants. J Oral Implantol 35, (2009) 35. Delaunay CP, Kapandji AI: Acetabular screw rings and surface treatment. Clin Orthop Relat Res (1997) 36. Teerlinck J, Quirynen M, Darius P, van Steenberghe D: Periotest: an objective clinical diagnosis of bone apposition toward implants. Int J Oral Maxillofac Implants 6, (1991) 37. Dhert WJ, Verheyen CC, Braak LH, de Wijn JR, Klein CP, de Groot K, Rozing PM: A finite element analysis of the push-out test: Influence of test conditions. J Biomed Mater Res 26, (1992) 38. Shapoff CA: Clinical advantages of tapered root form dental implants. Compend Contin Educ Dent 23, 42 44, 46, 48 passim (2002) 39. O Sullivan D, Sennerby L, Meredith N: Influence of implant taper on the primary and secondary stability of osseointegrated titanium implants. Clin Oral Implants Res 15, (2004) 40. Garber DA, Salama H, Salama MA: Two-stage versus onestage is there really a controversy? J Periodontol 72, (2001) 41. Guizzardi S, Galli C, Martini D, Belletti S, Tinti A, Raspanti M, Taddei P, Ruggeri A, Scandroglio R: Different titanium surface treatment influences human mandibular osteoblast response. J Periodontol 75, (2004) 42. Franchi M, Bacchelli B, Giavaresi G, De Pasquale V, Martini D, Fini M, Giardino R, Ruggeri A: Influence of different implant surfaces on peri-implant osteogenesis: Histomorphometric analysis in sheep. J Periodontol 78, (2007) 43. Crespi R, Capparé P, Gherlone E, Romanos GE: Immediate versus delayed loading of dental implants placed in fresh extraction sockets in the maxillary esthetic zone: A clinical comparative study. Int J Oral Maxillofac Implants 23, (2008) 44. Borsari V, Giavaresi G, Fini M, Torricelli P, Salito A, Chiesa R, Chiusoli L, Volpert A, Rimondini L, Giardino R: Physical characterization of different-roughness titanium surfaces, with and without hydroxyapatite coating, and their effect on human osteoblastlike cells. J Biomed Mater Res B Appl Biomater 75, (2005) 45. Veis AA, Papadimitriou S, Trisi P, Tsirlis AT, Parissis NA, Kenealy JN: Osseointegration of Osseotite and machined-surfaced titanium implants in membrane-covered critical-sized defects: A histologic and histometric study in dogs. Clin Oral Implants Res 18, (2007) 46. Hallman M: A prospective study of treatment of severely resorbed maxillae with narrow nonsubmerged implants: Results after 1 year of loading. Int J Oral Maxillofac Implants 16, (2001) 47. Degidi M, Nardi D, Piattelli A: Immediate restoration of smalldiameter implants in cases of partial posterior edentulism: A 4-year case series. J Periodontol 80, (2009) 48. Hansson S, Werke M: The implant thread as a retention element in cortical bone: The effect of thread size and thread profile: a finite element study. J Biomech 36, (2003) 49. Romanos GE, Nentwig GH: Immediate functional loading in the maxilla using implants with platform switching: Five-year results. Int J Oral Maxillofac Implants 24, (2009) 50. Friberg B, Ekestubbe A, Mellström D, Sennerby L: Brånemark implants and osteoporosis: A clinical exploratory study. Clin Implant Dent Relat Res 3, (2001) 51. Friberg B, Ekestubbe A, Sennerby L: Clinical outcome of Brånemark system implants of various diameters: A retrospective study. Int J Oral Maxillofac Implants 17, (2002) 52. Summers RB: A new concept in maxillary implant surgery: The osteotome technique. Compendium 15, 152, , 158 passim; quiz 162 (1994) 53. Crespi R, Capparè P, Gherlone E, Romanos GE: Immediate occlusal loading of implants placed in fresh sockets after tooth extraction. Int J Oral Maxillofac Implants 22, (2007) 54. Hui E, Chow J, Li D, Liu J, Wat P, Law H: Immediate provisional for single-tooth implant replacement with Brånemark system: Preliminary report. Clin Implant Dent Relat Res 3, (2001) 55. Lorenzoni M, Pertl C, Zhang K, Wimmer G, Wegscheider WA: Immediate loading of single-tooth implants in the anterior maxilla. Preliminary results after one year. Clin Oral Implants Res 14, (2003) 56. Olive J, Aparicio C: Periotest method as a measure of osseointegrated oral implant stability. Int J Oral Maxillofac Implants 5, (1990) 57. Trisi P, Perfetti G, Baldoni E, Berardi D, Colagiovanni M, Scogna G: Implant micromotion is related to peak insertion torque and bone density. Clin Oral Implants Res 20, (2009) 58. Sul YT, Johansson CB, Jeong Y, Wennerberg A, Albrektsson T: Resonance frequency and removal torque analysis of implants with turned and anodized surface oxides. Clin Oral Implants Res 13, (2002) 59. Ertugrul AS, Tekin Y, Alpaslan NZ, Bozoglan A, Sahin H, Dikilitas A: Comparison of peri-implant crevicular fluid levels of adrenomedullin and human beta defensins 1 and 2 from mandibular implants with different implant stability quotient levels in nonsmoker patients. J Periodontal Res (2013) 60. Ram akrishna R, Nayar S: Clinical assessment of primary stability of endosseous implants placed in the incisor region, using resonance frequency analysis methodology: An in vivo study. Indian J Dent Res 18, (2007) 61. Ham merle CH, van Steenberghe D: The first EAO Consensus Conference February 2006, Pfaffikon, Switzerland. Clin Oral Implants Res 17, Suppl 2, 1 (2006) 62. Per ren SM: Evolution of the internal fixation of long bone fractures. The scientific basis of biological internal fixation: Choosing a new balance between stability and biology. J Bone Joint Surg Br 84, (2002) 63. Chang PK, Chen YC, Huang CC, Lu WH, Chen YC, Tsai HH: Distribution of micromotion in implants and alveolar bone with different thread profiles in immediate loading: A finite element study. Int J Oral Maxillofac Implants 27, e (2012) 64. Sakka S, Coulthard P: Implant failure: Etiology and complications. Med Oral Patol Oral Cir Bucal 16, e42 44 (2011) 65. Pilliar RM, Lee JM, Maniatopoulos C: Observations on the effect of movement on bone ingrowth into porous-surfaced implants. Clin Orthop Relat Res (208), (1986) 66. Brunski JB: Avoid pitfalls of overloading and micromotion of intraosseous implants. Dent Implantol Update 4, (1993) 67. Søballe K, Hansen ES, Brockstedt-Rasmussen H, Bünger C: Hydroxyapatite coating converts fibrous tissue to bone around loaded implants. J Bone Joint Surg Br 75, (1993) 68. Javed F, Romanos GE: The role of primary stability for successful immediate loading of dental implants. A literature review. J Dent 38, (2010) Interventional Medicine & Applied Science 167 ISSN Akadémiai Kiadó, Budapest
46 IMPLANT DENTISTRY / VOLUME 19, NUMBER A 10-Year Longitudinal Study of 160 Implants Simultaneously Installed in Severely Atrophic Posterior Maxillas Grafted With Autogenous Bone and a Synthetic Bioactive Resorbable Graft Marcelo C. Manso, DDS, MScD, PhD,* and Thomas Wassal, DDS, MSc, PhD T he posterior edentulous maxilla has always presented the great challenge when implant placement are considered. Low-quality bone and expanded maxillary sinus are often special concerns. Sinus lift procedures by the maxilla lateral wall approach, introduced by Tatum 1 and first published by Boyne and James, 2 proved to be safe and was well consecrated during the 90s with the Consensus Conference on the Sinus Graft. 3 The simultaneous approach (sinus lift with immediate implant placement) has been advocated by several studies. 3 7 A polemic and controversial aspect relates to the necessity or lack of existing residual bone, of at least 5 mm to promote the primary stability. Block and Kent 4 reported their first technique using medullarcortical blocks to achieve the primary stability where 3 mm of residual native bone was present. Again, in 1997, the author showed further results and Purpose: This study intended to evaluate by clinical and imaging parameters the long-term predictability of osseointegrated implants inserted with specific simultaneous sinus lift approach in very atrophic posterior maxillas using a synthetic bioactive resorbable graft and autogenous bone graft. Patients and Methods: Atotalof 160 implants were inserted in 57 maxillary sinus of 45 consecutive patients (16 men, 29 women) presenting 4 mm or less of residual subsinus bone in a simultaneous approach with the sinus lift procedure. All patients were surgically treated by the same surgeon and received the same modified technical and biomaterial protocol with a composite graft made of autogenous bone and a synthetic bioactive resorbable graft (OsteoGen, Impladent, Holliswood, NY) in a 1:1 rate. Among the inclusions criteria was a minimum loading time of 6 months to assure bone response activity. All patients were followed up for a mean period of 61.7 months (range, months) with clinical, digital pictures, and radiographic aspects. Specific cases were followed up with computerized tomography scans (27.2%) with the consent form signed. Results: Survival and success rates were 98.05% and 94.85%, respectively. Conclusion: Advanced posterior maxillary resorption with extensive expanded sinus (SA-4 condition) can be safely treated by a simultaneous sinus lift approach and implant insertion using the technical protocol and biomaterials studied. (Implant Dent 2010;19: ) Key Words: atrophic maxilla, sinus lift, synthetic bioactive graft, bone graft *Maxillofacial Surgeon, Head of Graduate and Advanced Implant Dentistry Programs, Brazilian Institute of Implant Dentistry, Rio de Janeiro, Brazil. Maxillofacial Surgeon, Head of Master and Post-Doctoral Programs, São Leopoldo Mandic Dental School and Dental Research Center, São Paulo, Brazil. Reprint requests and correspondence to: Marcelo Corrêa Manso, DDS, MScD, PhD, Largo do Machado 54, conj 907, Laranjeiras, Rio de Janeiro, Brazil, Telephone: / , marcelo@manso.odo.br ISSN /10/ Implant Dentistry Volume 19 Number 4 Copyright 2010 by Lippincott Williams & Wilkins DOI: /ID.0b013e3181e59d03 so begun a lot of researches. 5 Another author with the same methodology reported a 100% success rate of an important 3.5 years follow-up study of 100 implants simultaneously placed during sinus lifts with 5 mm of residual subsinus bone. 6 As a matter of fact, the use of intramembranous corticocancellous bone grafts harvested from iliac crest as a way to achieve primary stabilization of threaded implants in simultaneous sinus-lift approach is still being advocated. 7 Although the simultaneous concept always looked for better results, the staged approach demonstrated predictable success rates. However, the majority of those studies used extraoral donor sites for the largest reconstructions such as iliac crest, tibia, or calvaria. 5,6,8,9 Since 1998, after a pioneer study, 10 several authors have been showing good
47 352 STUDY OF 160 IMPLANTS IN SEVERELY ATROPHIC POSTERIOR MAXILLAS MANSO AND WASSAL Table 1. Inclusion/Exclusion Criteria for the Population Studied (Stages I and II) Inclusion Consecutive patients by the same surgeon 4 mm or less of subsinus bone with simultaneous approach At least 6 mo of prosthetic load Table 2. Stage I From Implant Surgery to Prosthetic Impression Authorization; Stage II After Prosthetic Functional Loading (6 mo at Least) Aspect Stage I Stage II Patients Sinus Implants results for the simultaneous approach without extra-oral involvement However, problems with the primary stabilization of the implants in such scarce amount of bone is frequently reported and solutions based on particulate graft condensation around the implants and placement of nonthreaded implants have been considered. Several biomaterials have been advocated with trustable results for sinus lift procedures when mixed with autogenous bone graft (ABG) and controversies turns around the ideal rate. 15,16 The synthetic bioactive resorbable graft (SBRG) has been studied for decades, but a consistence study involving specific data collection about extreme expanded sinus conditions with immediate implant placement is lacking As so, this study intended to evaluate by clinical and imaging parameters the long-term predictability of a specific simultaneous approach protocol described for very atrophic posterior maxillas using SBRG/ABG composite grafts and also threaded implants. 14 PATIENTS AND METHODS Patients Atotalof160implantswereinserted in 57 maxillary sinus of 45 consecutive patients (16 men, 29 women) presenting 5 mmofresidualsubsinus bone in a simultaneous approach with the sinus lift procedure. All patients were surgically treated by the same surgeon and received a same technical and biomaterial protocol. The inclusion/ Exclusion Debilitating systemic diseases Use of restrictive medicines Less than 6 mo of prosthetic load exclusion criteria are listed in Table 1 and was relevant to a minimum loading time (prosthetic loaded) of 6 months to assure bone response activity. The study was approved by the ethical committee of Sao Leopoldo Mandic s Dental Research Center (Campinas/São Paulo, Brazil) and recognized by the Brazilian Educational and Culture Ministry, PhD committee. The population and implant distribution is presented in Table 2. Pre- and Postoperative Medication Antibiotics consisted of 300 mg of clindamycin (Dalacin-C; Pharmacia/ Pfizer, Sao Paulo, Brazil) 1 hour before surgery and 3 times a day after, then continued for 14 days after surgery. Patients with intolerance history received clavulanate-potentiated amoxicilin (Clavulin; Glaxo Smith Kline, Rio de Janeiro, Brazil) with the same dosage. A combination of nonsteroidal drugs (acetaminophen/ ibuprofen) and a long-acting glucocorticoid (dexamethasone) was also used for pain and anti-inflammatory control for 72 hours after surgery (decreasing dose on second and third day). Implant Selection One hundred sixty-one implants (9 cylinders and 152 threaded) were from SteriOss System (NobelBiocare Company, Yorba Linda, CA); 11 implants were from Branemark System-MKIII TiUnite (NobelBiocare Company, Gotemborg, Sweden) and 9 implants were from 3i-Osseotite (Implant Innovation, Palm Beach, FL). This number of implants represented exclusively those placed in areas with residual subantral bone measuring 4 mm or less, other implants even in the same sinus were not quantified. Biomaterials The biomaterials strategy were the same in all cases and consisted of a composite graft. Autogenous bone were collected from the mandible retromolar area, particulated with a bone mill (Neodent, Parana, Brazil) and represented 50% to 60% of the graft. The remaining volume were filled with a SBRG (OsteoGen HA Resorb, Impladent, Holliswood, NY) when limited to 40%. Surgical Technique All patients underwent surgical procedures under local anesthesia with mepivacaine (3%) with epinephrine (1:100,000) (Scandicaine; Septodont, São Paulo, Brazil) and perioral sedation with midazolam (Dormonid; Roche, São Paulo, Brazil). The surgical procedure for maxillary sinus augmentation has been described elsewhere. 14 In brief, lateral maxillary sinus osteotomy by Tatum was performed with the lower aspect of approximately 7 mm over the sinus floor limit, combined with stripping off the sinus membrane to create a subsinus cavity into which the implants and the graft material could be placed (Fig. 1, A C). The implants socket were drilled according to the manufacturer s specifications except for the last drill that was substituted for a reduced screw-tap to perform bone threads smaller than the implant diameter (Fig. 1, B). Finally, the usual screwtap was used only for a quarter turn to make easier the contra angle-driven insertion of the implants. The grafts were applied using an incremental approach: the autogenous bone was first placed in direct contact with the implant bodies, and SBRG layers were interposed with new autogenous layers. The external layers were carefully receiving more and more percentage of SBRG and finally the most external layer constituted only SBRG (Fig. 1, D). At this time, a collagen membrane (Colla-Cote, Zimmer Dental, USA) was used for dressing the graft. Second stage surgeries were performed after 11 months elevating a fullthickness flap for direct visualization of bone healing at the lateral aspect of the maxilla. Healing caps were placed, and interrupted mattress sutures were applied (Fig. 1, E).
.")
48 IMPLANT DENTISTRY / VOLUME 19, NUMBER loss around the implant neck was measured by using an implant computer mapping scale. All implants studied were digitally fractioned and measured by specific software in mm scale (Ulead Photoimpact 4.2 Canon,Tokyo, Japan). The values were applied to the radiographic images and a mathematic parameter could inform precise results. A diagnostic scale was created to classify the bone crest situation around each implant neck (Table 3). Finally, the majority of the extensive cases underwent computerized tomography (CT) scan evaluation (Fig. 1, G) with the consent form signed. CT scans were studied for the concerning two aspects: bone maintenance and maxillary sinus health (medical radiologic diagnoses). The final analysis was executed concerning clinical surviving and success parameters based in both Misch et al 22 and Albrektsson et al 23 parameters. Gender distribution, smoke, postoperative infection, maxilla lateral wall bone regeneration, membrane perforation, and early implant exposure were also registered and correlated to failures and/or marginal bone loss. RESULTS A total of 45 patients (16 men, 29 women) ranging in age from 26 to 80 years (mean, 54 years) met the criteria for inclusion in this study. All patients could be evaluated on stage I. One patient was moved away during the beginning of the stage II study due to home care and return time inobservances. This patient represented 2 sinus and 6 implants. Fig. 1. Left sinus aspect of a bilateral atrophic maxilla reconstruction. Panoramic view: base line subsinus bone (A); 3.25 screw tap (B); threaded implants well positioned (C); external SBRG layer (D); lateral wall aspect after 11 months (E); panoramic view with temporary rehabilitation (F); sinus CT view after almost 7 years (G); and intraoral x-ray (H). Table 3. Peri-implant MBL Classification and Implant Body Correlation Level 0 Level 1 Levels Level 2 (2.1;2.2;2.3 ) Treatment and Follow-Up Protocol Immediate and 15 days postoperative x-rays were done to assure final biomaterial retention. After that, patients were examined monthly until the recovery surgery with healing caps placement could be performed. This stage was considered as the stage I and represented success of early implant osseointegration and graft healing. Normally, clinicians took 1 or 2 months performing metal-ceramic rehabilitation, and the patients should be at least 6 months in function to be approved for the retrospective functional study (stage II). During the recall, new x-rays (panoramic and intra-oral) were requested and a clinical evaluation was performed. The clinical parameters investigated were pain, bleeding, mobility, exudations, or chewing discomfort. Crest bone Bone Crest Level (Intraoral x-ray) Necklace level, mm Between the necklace base and the first thread (not exposed), 1 mm Threads exposed (out of bone), 0.6 mm each Stage I Evaluation All 57 sinus were considered satisfactory treated with 160 implants primary stabilized, well maintained and showed good osseointegration during the second stage surgery. One patient developed a moderate infection during the second week postoperative and was treated satisfactory with flap debridement and additional antibiotics. Thirtyseven implants (25%) of 18 patients (41%) had cover screws early exposed and all of them became osseointegrated at the second stage analysis (20 N counter clock torque). All maxillary sinuses, except one, presented full bone healing of the lateral wall when direct inspections were performed. One patient (80 years old) presented a partial bone defect at the upper aspect of the original bone window but also developed a satisfactory osseointegration of the 3 implants placed at that sinus and a good radiographic and clinical control after 42 months (6 implants, 2 bilateral sinus). Five sinuses (8.77%) were victims of perioperative Schneiderian membrane perforations. All perforations could be treated by a modified approach that used acollagenmembrane(colla-cote,zimmer Dental) with one extremity covering the hole (direct contact with the membrane) and the other exteriorizing the bone window and resting over the lateral wall. As the grafts were being applied, they could carefully enhance
49 354 STUDY OF 160 IMPLANTS IN SEVERELY ATROPHIC POSTERIOR MAXILLAS MANSO AND WASSAL Table 4. Stage I Evaluation Results Aspect Sample Analyzed Found Percentage Patient with premature cover screw exposure Implants with premature cover screw exposure Fail at the 2nd stage Infection Graft fail Lateral wall defect Membrane perforation Table 5. Stage II MBL Evaluation MBL Level Sample Percentage 0 and Total the collagen membrane stabilization. There was no statistic correlation between membrane perforations and failures or infections when Fisher s exact test was applied (P 0.39/P 0.05). There were no correlation between perforations and smokers. Ten patients were smokers and only 1 had a membrane perforation. In the other hand, from 35 nonsmokers, 4 had membrane perforations. The Fisher s exact test also identified no significance (P 0.69/P 0.05). (Statistical Program BioEstat version 4.0; Mamirauá Maintainable Development Institute, PR, Brazil). Stage I results are summarized in Table 4. Stage II Evaluation Fifty-five sinuses with 154 implants of 44 patients satisfied the inclusion criteria for this stage and could be studied. One patient had 1 implant failed during the final prosthetic procedure (final torque adjustment). This patient (male, smoker, and no membrane perforation episode) had 2 more implants in the same conditions (2 mm of subsinus bone). After explantation, the new bone repaired presented stable to receive a new implant in the same area, but the patient declined. The remaining 2 implants received a metal-ceramic prosthesis and presented satisfactory after 2.5 years. All other implants studied could receive functional loading with fixed prostheses and could be evaluated by the research criteria. Marginal bone loss (MBL) results are summarized in Table 5. Five implants (3.2%) lost 3 points in the indexed scale presented. Two of those were in 1 patient that also lost 2 implants after 5 years due the development of a perimplantite infection. Twelve patients (27.2%) representing 17 maxillary sinus (30.3%) and 51 implants (33.1%) accepted to undergo CT scans examinations. All sinus CT scans showed satisfactory bone maintenance and were medical-radiologically diagnosed as healthy. Stage I and II Results The cumulative analyses included 154 implants, 55 sinus, and 44 patients. The total period included was 10 years with a mean of 61.7 months when considered the recall date for research evaluation. All sinuses were attested healthy and a 100% success could be concluded for Stage I (primary stabilization and bone reconstruction technique). A total of 3 implants failed where one was before loading and the others were at a same patient 5 years later. Five implants were considered with unsatisfied marginal bone maintenance. As so, a survival rate of 98.05% and a success rate of 94.8% was established. DISCUSSION This study demonstrated a high survival rate for simultaneous implant placement with grafting of the maxillary sinus with SBRG and ABG. Other studies have been advocating the simultaneous approach with other biomaterials. 6,10,12 The ABG has been emphasized as an important factor to be present in association with other biomaterials such as hydroxyapatite (HA) bovine matrix and demineralized freeze-dried bone allograft. 5,12,24,25 In one study, the authors, for the first time, stated that the absence of ABG could be a probable cause for failures when large sinus expansion are considered. 25 They reported that their final success tax was in disagreement to the similar studies with ABG associated. 26,27 Hallman et al 16 studied patients treated with an 80:20 percent relationship of HA bovine matrix (BioOss, Geistlich Pharmaceutical, Wolhusen, Switzerland) and ABG in sinus lift treated with staged approaches, also considered that the little resorption found for the BioOss should be a special concern in cases with extensive expanded sinus because the great amount of remaining particles reduce the space for new vital bone regeneration. Another recent study emphasized this concept and strongly recommended the presence of ABG in a composite graft to achieve greater amount of new vital bone. 28 The authors also found this correlation by using histology and histomorphometry observations and considered the distance between the outlying host bone and the center of the graft a crucial factor. Peleg et al 10 reported a pioneer study with 100% success of 55 implants HA coated in a simultaneous sinus lift approach in 20 sinus where only 1 or 2 mm of residual bone was present. They used only cylinders implants (no threads) and extolled a good graft condensation around the implant bodies as to achieve better primary stability and advised about problems with the final position due to the direction changes that the cylinders could suffer during insertion. Other studies also reported nonthreaded cylinders as an important factor to achieve adequate primary stability In our study, the drilling modification earlier described used a modified technique for installing threaded implants simultaneously to sinus-lift procedure in so atrophic conditions with predictable primary stability. 14 As so, all 160 implants could receive preplanned positions and satisfactory primary stabilizations (Fig. 2, A F).
 after 11 months complete bone heal; F,")
50 IMPLANT DENTISTRY / VOLUME 19, NUMBER Fig. 2. Bilateral sinus in atrophic maxilla. A, CT scan view pre-op base line subsinus bone; B, implants installed right side; C, implants installed left side; D and E, lateral wall aspect (right and left) after 11 months complete bone heal; F, CTs view after 5 years. Recently, Peleg et al 12 evaluated atrophic posterior maxillas where only the simultaneous approach was instituted. The research represented a 9 years longitudinal study with a total of 2132 osseointegrated implants installed in a multicentric group of patients and surgeons. The authors reported a cumulative survival rate higher than 97% (44 implants failed) using several biomaterials strategies and considered the amount of remaining subsinus bone as an important factor to failures. An important aspect was the moment and etiology of the failures. Of 44 implants failed, 33 (75%) were diagnosed as infection and lack of osseointegration denoting early and preloading failures. In this study, these aspects were included on Stage I where no failures occurred (100% success) what could be directly correlated to surgical technique, biomaterial acting and/or implant surface behavior. The waiting time between the first and the second stage surgeries was 11 months to allow enough SBRG resorption with new bone deposition and mineralization. A direct inspection of the lateral wall was performed in all cases, and only 1 patient showed partial unsatisfactory bone heal with no implant failure. The direct bone wall inspection is a concept first presented by Avera et al 28 and is based on the centrifugal mediolateral ossification of the grafts as so a centripetal anterior-posterior healing of the lateral wall of the maxilla, resulting in the center of this bone wall as the last area to be healed. The MBL around the implants is another consideration. Herzberg et al 29 confronted simultaneous and staged sinus lift approaches, among others factors, measuring periodically the threads exteriorized from the bone in normal radiographs by Haas methodology. 30 The authors found a better MBL behavior for implants in simultaneous approach than for staged and also could present and confront the survival rate (95.5%) with the success rate (83.8%) based on Albrektsson et al 23 patterns. In our study, we developed the Haas concept and digitally mapped each implant used. Using real measurements of several segments of the implants, we could identify the exact MBL. Eighty-three percent of the totality of implants were classified with level 1 and were considered with a superb behavior. A progressive fall of the percentages were registered for each sublevel denoting a favorable proportion (Table 5). Another relevant aspect in this segment analysis is that some implants presented an apical bone level since the beginning due to technical aspects, healing reasons or even a surgical option. Therefore, the MBL diagnose should consider this important delta relationship. This concept was well discussed and introduced by Roos et al as an implement to Albrektsson et al patterns Misch et al 22 presented further aspects to be considered for success or failure diagnose and proposed an implant quality scale with 4 levels. In our study, a total of 5 implants were considered with unsatisfactory MBL behavior and out of level 1 and 2 (where no intervention is needed) of the authors scale and also in agreement with Albrektsson et al patterns. 23 As CT analyses were a patient option, only part of the population was studied (30.3% of the sinuses and 33% of the implants). This aspect agrees with other studies and was considered satisfactory. The premature exposure of the implants cover screws was a frequent occurrence (25%). However, no difference was registered when both groups were compared after a minimum prosthetic loading time. The premature exposure is considered to act as premature stimulus to biologic perimplant space organization. 33 Also, no correlation between the premature exposure and loss of osseointegration due to micromovements was found. Finally, membrane perforation was also studied and 8.77% of the sinuses (N 5) were victims of this kind of incident. However, no correlation could be found with implant failures or infection (Fisher s exact statistical test). Other studies showed higher prevalence and also exceptional results. 16,34,35 One of them related 58% of perforations with no correlation to failures when only single implants with simultaneous approach were considered. Herzberg et al 29 reported 46% of occurrence and no correlation with implant failures, but considered a strong correlation to postoperatory complications. CONCLUSIONS With data collected in this study, we could conclude the following: Patientspresentingextensiveposterior edentulism, associated with advanced posterior maxillary re-
51 356 STUDY OF 160 IMPLANTS IN SEVERELY ATROPHIC POSTERIOR MAXILLAS MANSO AND WASSAL sorption and severe sinus expansion, can be treated by a simultaneous sinus lift approach and implant placement in accordance with the technical protocol described. A1:1ratioofacompositegraft, with ABG and a SBRG (Osteo- Gen), can satisfactorily treat many serious maxillary atrophies by performing simultaneous implant placements and sinus lift approach, without using extraoral donor sites. Thetechnicalprotocolandbiomaterials studied showed a satisfactory success rate that complied with acceptable international criteria. DISCLOSURE The authors claim to have no financial interest, directly or indirectly, in any entity that is commercially related to the products mentioned in this article. REFERENCES 1. Tatum H. Maxillary and sinus implant reconstructions. Dent Clin North Am. 1986;30: Boyne PJ, James RA. Grafting of the maxillary sinus floor with autogenous marrow and bone. JOralSurg.1980;38: Shulman LB, Jensen OT, Block NS, et al. A consensus conference on the sinus graft. In: Jensen OT, ed. The Sinus Bone Graft. Vol. 19. Hannover Park, IL: Quintessence; 1999: Block M, Kent JM. Maxillary sinus grafting for totally and partially edentulous patients. J Am Dent Assoc. 1993;124: Block MS, Kent JN. Sinus augmentation for dental implants: The use of autogenous bone. JOralMaxillofacSurg. 1997;55: Daelemans P, Hermans M, Godet F, et al. Autologous bone graft to augmentation the maxillary sinus in conjunction with immediate endosseus implants: A retrospective study up to 5 years. Int J Periodontics Restorative Dent.1997;17: Acocella A, Sacco R, Nardi P, et al. Simultaneous implant placement in sinus floor augmentation using iliac boné block grafts in severe maxillary atrophies: Case report. Implant Dent. 2008;17: Watzek G, Ulm CW, Haas R. Anatomic and physiologic fundamentals of sinus floor augmentation. In: Jensen OT, ed. The Sinus Bone Graft. Vol. 4. Hannover Park, IL: Quintessence; 1999: Suba Z, Takács D, Matusovits D, et al. Maxillary sinus floor grafting with betatricalcium phosphate in humans: Density and microarchitecture of the newly formed bone. Clin Oral Implants Res. 2006;17: Peleg M, Mazor Z, Chaushu G, et al. Sinus floor augmentation with simultaneous implant placement in the severely atrophic maxilla. JPeriodontol.1998;69: Buchmann R, Khoury F, Faust C, et al. Peri-implant conditions in periodontally compromised patients following maxillary sinus augmentation. A long-term posttherapy trial. Clin Oral Implants Res. 1999; 10: Peleg M, Garg A, Mazor Z. Predictability of simultaneous implant placement in the severely atrophic posterior maxilla: A 9-year longitudinal experience study of 2132 implants placed into 731 human sinus grafts. Int J Oral Maxillofac Implants. 2006;21: Mardinger O, Nissan J, Chaushu G. Sinus floor augmentation with simultaneous implant placement in the severely atrophic maxilla: Technical problems and complications. JPeriodontol.2007;78: Manso MC, Velloso GR. Instalação imediata de implantes rosqueados em seios maxilares extremamente pneumatizados (condiçõessa-4):apresentaçãodatécnica. Rev Bras de Implant.2001;7: Fugazzotto PA. Immediate implant placement following a modified trephine/ osteotome approach: Success rates of 116 implants to 4 years in function. Int J Oral Maxillofac Implants.2002;17: Hallman M, Headin M, Sennerby L, et al. A prospective 1 year clinical and radiographic study of implants placed after maxillary sinus floor augmentation with bovine hydroxiapatite and autogenous bone. J Oral Maxillofac Surg. 2002;60: Ricci JL, Blumenthal NC, Spivak JM, et al. Evaluation of a low-temperature calcium phosphate particulate implant material: Physical-chemical properties and in vivo bone response. J Oral Maxillofac Surg. 1992;50: Wagner JR, Perel M. A resorbable bone fill and its uses in implant procedures. Dental Implantol Update. 1992;3: Hurzeler MB, Quinones CR, Morrison EC, et al. Treatment of peri-implantitis using guided bone regeneration and bone grafts alone or in combination, in beagle dogs. Part II: Histologic findings. Int J Oral Maxillofac Implants. 1997;12: Manso MC. Reconstrução óssea em implantodontia: Apresentação de um protocolo de condutas. Rev Bras de Implant. 2002;8: Ganz SD, Valen M. Predictable synthetic bone grafting procedures for implant reconstruction: Part two. J Oral Implantol. 2002;28: Misch CE, Wang HL, Palti A, et al. The International Congress of Oral Implantologists Consensus Congress on Implant Success, Padua, Italy, Contemporary Implant Dentistry. Vol. 42. St. Louis, MO: Mosby Elsevier; 2008: Albrektsson T, Zarb G, Worthington P, et al. The long-term efficacy of currently used dental implants: A review and proposed criteria of success. Int J Oral Maxillofac Implants. 1986;1: Tong DC, Rioux K, Drangsholt N, et al. A review of survive rates for implants placed in grafted maxillary sinuses using meta-analysis. Int J Oral Maxillofac Implants. 1998;13: Valentini P, Abensur D, Wenz B, et al. Sinus grafting with porous bone mineral (Bio-oss) for implant placement: A 5 year study on 15 patients. Int J Periodontics Restorative Dent. 2000;20: Tulasne JF, Riachi P. Greffe osseuse du sinus maxillayre et implants de branemark. Implants. 1993; Raghoebar GM, Brouwer TJ, Reintsema H, et al. Augmentation of the maxillary sinus floor with autogenous bone for the placement of endosseous implants: A preliminary report. J Oral Maxillofac Surg. 1993;51: Avera SP, Stampley WA, McAllister BS. Histologic and clinical observations of resorbable and nonresorbable barrier membranes used in maxillary sinus graft containment. Int J Oral Maxillofac Implant. 1997;12: Herzberg R, Dolev E, Schwartz- Arad D. Implant marginal bone loss in maxillary sinus grafts. Int J Oral Maxillofac Implants. 2006;21: Haas R, Mensdorff-Pouilly N, Mailath G, et al. Single tooth implants. A preliminary report of 76 implants. J Prosthet Dent. 1995;73: Roos J, Sennerby L, Lekholm U, et al. A qualitative and quantitative method for evaluating implant success: A 5-year retrospective analysis of the Brånemark implant. Int J Oral Maxillofac Implants. 1997; 12: Block MS, Kent JN, Kallukaran FU, et al. Bone maintenance 5 to 10 years after sinus grafting. J Oral Maxillofac Surg. 1998;56: Abrahamsson I, Berlundh T, Moon IS, et al. Peri-implant tissues at submerged and no submerged titanium implants. J Clin Periodontol. 1999;9: Fugazzotto PA, Vlassis J. A simplified classification and repair system for sinus membrane perforation. J Periodontol. 2003;74: Krennmair G, Krainhofner M, Schmid-Schamp M, et al. Maxillary sinus lift for single implant supported restorations: A clinical study. Int J Oral Maxillofac Implants. 2007;22:

52 IMPLANT DENTISTRY / VOLUME 19, NUMBER Abstract Translations GERMAN / DEUTSCH AUTOR(EN): Marcelo C. Manso, DDS, MScD, PhD, Thomas Wassal, DDS, MSc, PhD Eine 10-Jahresstudie im Längsverlauf an 160 gleichzeitig in schwer atrophische hintere Oberkiefer eingesetzten Implantaten mit vorheriger Transplantierung mit autogenem Knochengewebe und einem synthetischen bioaktiven resorbierbaren Transplantat ABSTRACT: Zielsetzung: Die vorliegende Studie zielte darauf ab, die langfristige Zuverlässigkeit Knochengewebsintegrierender Implantate mittels klinischer und Bildgebender Parameter zu beurteilen. Die Implantate wurden mit einer speziellen gleichzeitigen Sinusanhebungsmethode in sehr atrophischen hinteren Oberkiefern unter Verwendung eines synthetischen bioaktiven resorbierbaren Transplantats (SBRG) sowie einem autogenen Knochentransplantat eingepflanzt. Materialien und Methoden: Insgesamt 160 Implantate wurden in den Oberkiefersinus von 45 aufeinander folgenden Patienten (16 männlich, 29 weiblich) eingepflanzt. Dabei herrschten Höhen von 4 mm oder weniger an verbleibenden Untersinusknochen vor und die Behandlung wurde gleichzeitig mit der Sinusanhebung durchgeführt. Alle Patienten wurden vom gleichen Chirurgen operiert und alle wurden unter Beibehaltung des gleichen veränderten Technik- und Biomaterialprotokoll mit einem zusammengesetzten Transplantat aus autogenem Knochengewebe (ABG) und einem synthetischen bioaktiven resorbierbaren Transplantat- SBRG (OsteoGen, Impladent, Holyswood, NY/USA) in einem Verhältnis von 1:1 behandelt. Zu den Einschlusskriterien gehörte eine minimale Belastungszeit von 6 Monaten, um die Knochengewebsreaktionsaktivität zu gewährleisten. Alle Patienten mussten sich durchschnittlich in einem Zeitraum von 61,7 Monaten (zwischen 20 bis 132 Monaten) Nachuntersuchungen unterziehen. Dabei wurden klinische, digitale Aufnahmen sowie Röntgenbilder gemacht. In besonderen Fällen wurde zusätzlich ein CT-Scan (27,2%) gemacht. Hierzu unterzeichnete der Patient vorher die entsprechende Einverständniserklärung. Ergebnisse: Die Überlebens- und Erfolgsraten wurden entsprechend auf 98,05% und 94,85% berechnet. Schlussfolgerung: Eine fortgeschrittene Resorption im hinteren Oberkiefer mit einem massiv erweiterten Sinus (SA-4-Zustand) kann auf sichere Art und Weise durch eine gleichzeitige Sinusanhebung und Implantateinpflanzung unter Anwendung des in der Studie aufgeführten technischen Protokolls und der Biomaterialien behandelt werden. SCHLÜSSELWÖRTER: atrophischer Oberkiefer; Sinusanhebung, synthetisches bioaktives Transplantat; Knochentransplantat SPANISH / ESPAÑOL AUTOR(ES): Marcelo C. Manso, DDS, MScD, PhD, Thomas Wassal, DDS, MSc, PhD Un estudio longitudinal de diez años de 160 implantes colocados simultáneamente en maxilares posteriores severamente atrofiados injertados con hueso autógeno y un injerto reabsorvible bioactivo sintético ABSTRACTO: Propósito: Este estudio tuvo la intención de evaluar, usando parámetros clínicos y de imágenes, la previsibilidad de largo plazo de implantes oseointegrados colocados con un método específico de elevación simultánea del seno en maxilares posteriores muy atrofiados usando un injerto reabsorvible bioactivo sintético (SBRG por sus siglas en inglés) y un injerto de hueso autógeno. Materiales y métodos: Se colocaron un total de 160 implantes en 57 senos maxilares de 45 pacientes consecutivos (16 hombres, 29 mujeres) que presentaban un hueso en el subseno residual de 4 mm o menos en un método simultáneo con el procedimiento de elevación del seno. Todos los pacientes fueron tratados quirúrgicamente por el mismo cirujano y recibieron el mismo protocolo técnico y de biomaterial con un injerto de aleación hecha por hueso autógeno (ABG por sus siglas en inglés) y un injerto reabsorvible bioactivo sintético, SBRG (OsteoGen, Implandent, Holyswood, NY/ EE.UU.) en una relación uno a uno. Entre los criterios de inclusión se incluyó unperíodomínimodecargade6meses para asegurar una actividad de respuesta del hueso. Todos los pacientes fueron seguidos durante un período medio de 61,7 meses (rango de 20 a 132 meses) con imágenes clínicas y digitales y aspectos radiográficos. Los casos específicos fueron seguidos con tomografías computadas (27,2%) con formulario de consentimiento firmado. Resultados: Se calcularon las tasas de supervivencia y de éxito en 98,05% y 94,85% respectivamente. Conclusión: La reabsorción avanzada del maxilar posterior con extensa expansión del seno (condición SA-4) puede tratarse sin problemas usando un método de elevación simultánea del seno y colocación del implante usando el protocolo técnico y los biomateriales estudiados. PALABRAS CLAVES: Maxilar atrofiado; elevación del seno; injerto bioactivo sintético; injerto de hueso PORTUGUESE / PORTUGUÊS AUTOR(ES): Marcelo C. Manso, Cirurgião-Dentista, Mestre em Odontologia, PhD, Thomas Wassal, Cirurgião-Dentista, Mestre em Ciência, PhD Estudo longitudinal de dez anos de 160 implantes instalados simultaneamente em maxilas posteriores gravemente atróficas enxertadas com osso autógeno e enxerto reabsorvível bioativo sintético
53 358 STUDY OF 160 IMPLANTS IN SEVERELY ATROPHIC POSTERIOR MAXILLAS MANSO AND WASSAL RESUMO: Objetivo: Este estudo pretendia avaliar por parâmetros clínicos e de imageamento a previsibilidade de longo prazo de implantes osseointegrados inseridos com abordagem específica simultânea de elevação da cavidade em maxilas posteriores atróficas usando enxerto reabsorvível bioativo sintético (SBRG) e enxerto de osso autógeno. Métodos: Um total de 160 implantes foi inserido em 57 cavidades maxilares de 45 pacientes consecutivos (16 masculinos, 29 femininos) apresentando 4 mm ou menos de osso da subcavidade residual numa abordagem simultânea ao procedimento de elevação da cavidade. Todos os pacientes foram tratados cirurgicamente pelo mesmo cirurgião e receberam o mesmo protocolo de biomaterial técnico modificado com um enxerto composto feito de osso autógeno (ABG) eumenxertoreabsorvívelbioativosintético SBRG (Osteo- Gen, Impladent, Holyswood, Nova York/Estados Unidos) numa taxa de 1:1. Entre os critérios de inclusão estava um tempo de carregamento mínimo de 06 meses para garantir a atividade de resposta do osso. Todos os pacientes foram acompanhados por um período médio de 61,7 meses (intervalo de 20 a 132 meses) com fotografias clínicas e digitais e aspectos radiográficos. Casos específicos foram acompanhados de mapeamentos por tomografia computadorizada (27,2%) com formulário de consentimento assinado. Resultados: As taxas de sobrevivência e sucesso foram calculadas em 98,05% e 94,85%, respectivamente. Conclusão: Areabsorção maxilar posterior avançada com extensa cavidade expandida (condição SA-4) pode ser tratada com segurança por uma abordagem simultânea de elevação da cavidade e inserção de implante usando o protocolo técnico e os biomateriais estudados. PALAVRAS-CHAVE: maxila atrófica; elevação da cavidade, enxerto bioativo sintético; enxerto de osso RUSSIAN / : Marcelo C Manso,,,, Thomas Wassal,,, 160 -, :. -,, - (SBRG) (16, 29 ), 4.., -, (ABG) SBRG (OsteoGen, Impladent, Holyswood, NY/USA) ш 1:1., 6, -. 61,7 ( ), ш,. (27,2%).. ш 98,05% 94,85%.. ш ( SA-4) -,. :,,, TURKISH / TÜRKÇE YAZARLAR: Marcelo C. Manso, DDS, MScD, PhD, Thomas Wassal, DDS, MSc, PhD Otojen kemik ve sentetik bir biyo-aktif rezorbabl greft ile greftlenen ciddi şekilde atrofiye uğramış posterior maksillada eşzamanlı olarak yerleştirilen 160 implantın on yıllık çalışması ÖZET: Amaç: Bu çalışmanın amacı, büyük ölçüde atrofiye uğramış posteriormaksillada,sinüs kaldırma yaklaşımı ile eşzamanlı olarak yerleştirilen osseo-entegre implantların uzun vadedeki başarısınıklinikvegörüntülemeparametrelerikullanarak
54 IMPLANT DENTISTRY / VOLUME 19, NUMBER değerlendirmekti. Gereç ve Yöntem: Bir sinüs kaldırma prosedürü ileeşzamanlıolarakrezidüel subsinüs kemiği 4 mm veya daha az olan ard ardına 45 hastanın (16 erkek, 29 kadın) 57 maksiller sinüsünde toplam 160 adet implant yerleştirildi. Hastaların tümü aynıcerrahtarafındantedaviedildiveolgulara,otojen kemik ve sentetik bir biyo-aktif rezorbabl greftten (OsteoGen, Impladent, Holyswood, NY/USA) oluşan kompozit bir greft 1:1 oranında aynı modifiye teknik ve biyo-materyal protokolü ile uygulandı. Çalışmaya dahil edilme kriterlerinden biri de, kemik yanıt aktivitesini sağlamak için minimum 6 aylık yükleme süresiydi. Hastaların tümü ortalama 61.7 ay (20 ila 132 ay) boyunca hem klinik açıdan, hemdedijitalresimlerveradyografi ile takip edildi. Bazı olgulara, olur formu imzalandıktan sonra BT (%27.2) uygulandı. Bulgular: Sağkalım ve başarı oranları sırasıyla %98.05 ve %94.85 idi. Sonuç: Posterior maksillada ileri derecede rezorpsiyon ile genişlemiş sinüs (SA-4) durumu, eşzamanlı sinüs kaldırma ve implant yerleştirme yaklaşımı ile burada çalışılanteknikprotokolvebiyo-materyallerkullanılarak güvenli bir şekilde tedavi edilebilir. ANAHTAR KELİMELER: Atrofik maksilla, sinüs kaldırma, sentetik biyo-aktif greft, kemik grefti JAPANESE /
55 360 STUDY OF CHINESE / KOREAN / 160 IMPLANTS IN SEVERELY ATROPHIC POSTERIOR MAXILLAS MANSO AND WASSAL

56

57

58

59

60

61

62

63

64

65

66

67

68

69

70
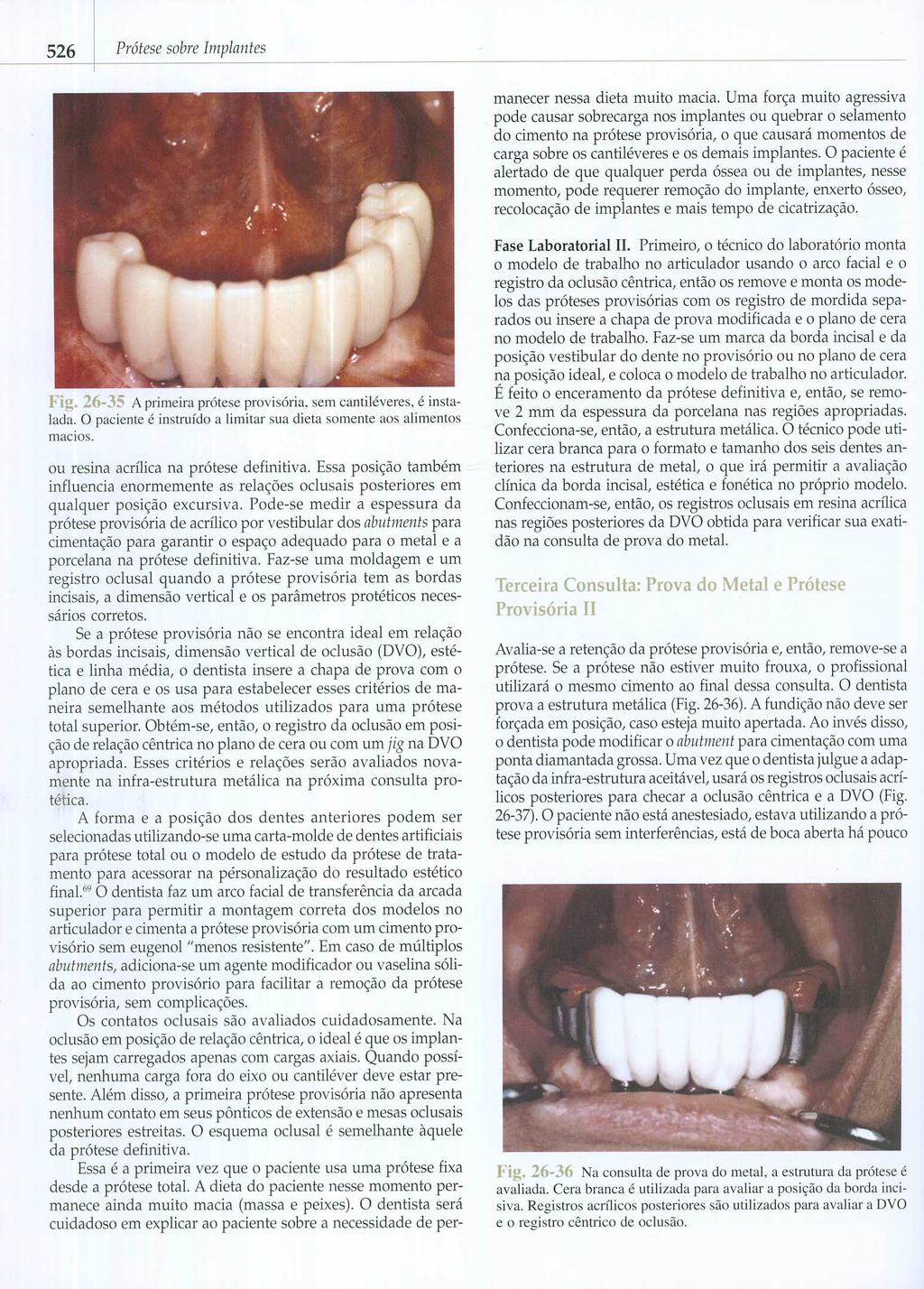
71

72

73
74 Immediate Placement of Implants into Periodontally Infected Sites in Dogs: A Histomorphometric Study of Bone-Implant Contact Arthur B. Novaes, Jr, DSc 1 /Andréa M. Marcaccini, MScD 2 /Sérgio L. S. Souza, DSc 3 / Mário Taba, Jr, DSc 3 /Márcio F. M. Grisi, DSc 3 Purpose: The placement of implants allows for re-establishment of function and esthetics following tooth loss. Immediate implant placement is a relatively recent procedure and has advantages, such as reduced number of surgical procedures, preservation of alveolar bone, reduction of cost and period of edentulism, and increased patient acceptance. However, there are some specific contraindications for the technique, such as the presence of an infection caused by periodontal disease and periapical lesions. The objective of this study was to evaluate the percentage of bone-implant contact of immediate implants placed in periodontally infected sites. Materials and Methods: In the first phase, periodontitis was induced with ligatures in the mandibular premolars of 5 mongrel dogs, using the contralateral teeth as controls (received prophylaxis only). After 3 months, in the second phase of the study, 40 implants were placed in the alveoli of both experimental and control teeth. After a healing period of 12 weeks, the animals were euthanized, and the hemimandibles were removed, dissected, fixed, and prepared for histomorphometric analysis of percentage of bone-implant contact. The Mann- Whitney test was used for statistical analysis. Results: The results of the histomorphometric analysis indicated mean bone-implant contact of 62.4% in the control group and 66.0% in the experimental group, a difference that was not statistically significant. Discussion: Histomorphometric results revealed similar bone-implant contact in both groups, with no signs of infection. Conclusions: It was concluded that periodontally infected sites may not be a contraindication for immediate implantation in this animal model system, if adequate pre- and postoperative care is taken. (INT J ORAL MAXILLOFAC IMPLANTS 2003;18: ) Key words: dental implants, immediate dental implantation, induced periodontitis, infection, osseointegration Conventional endosseous implant protocol recommends a waiting period of up to 6 months after tooth extraction before implant placement. This 1 Chairman of Periodontology and Department of Buccomaxillofacial Surgery and Traumatology and Periodontology, School of Dentistry of Ribeirão Preto, University of São Paulo, Ribeirão Preto, SP, Brazil. 2 Graduate Student in Periodontology, Department of Buccomaxillofacial Surgery and Traumatology and Periodontology, School of Dentistry of Ribeirão Preto, University of São Paulo, Ribeirão Preto, SP, Brazil. 3 Professor of Periodontology, Department of Buccomaxillofacial Surgery and Traumatology and Periodontology, School of Dentistry of Ribeirão Preto, University of São Paulo, Ribeirão Preto, SP, Brazil. Reprint requests: Arthur B. Novaes Jr, Departamento de Cirurgia e Traumatologia Buco-Maxilo-Facial e Periodontia, Faculdade de Odontologia de Ribeirão Preto, USP, Av. do Café, s/n, , Ribeirão Preto, SP, Brazil. novaesjr@.forp.usp.br delay is associated with inevitable postextraction bone loss, which can contribute to insufficient bone for implant placement and a long treatment period. Immediate placement of root-form implants was first described by Schulte 1 after 8 years of follow-up in humans. This technique was developed so that problems related to conventional implant placement would be minimized or eliminated. 2 7 Immediate implant placement is as safe and efficient as conventional placement, 8 10 with apparent osseointegration even in different anatomic areas. 11,12 Preservation of bone height allows the placement of longer implants in the posterior maxilla, avoiding an additional surgical procedure to reconstruct the bone volume lost during healing. 13 Immediate implant healing, with or without guided bone regeneration (GBR), can present a similar Plaque Index, degree of gingival recession, and clinical attachment level as conventionally placed implants, 14 confirming the The International Journal of Oral & Maxillofacial Implants 391

75 NOVAES ET AL This investigation evaluated histomorphometrically the percent of bone-implant contact of immediate implants placed into periodontally infected alveoli in dogs. MATERIALS AND METHODS Fig 1 A silk suture is placed into an infrabony pocket created around premolar teeth. success rate reported by Watzek and coworkers 15 when they placed implants to replace residual roots. The advantages of immediate implant placement are: elimination of the waiting period for regeneration of the extraction sockets; maintenance of alveolar dimension; fewer surgeries; decreased toothless period, which reduces cost and increases patient acceptance 12,14,16 ; and potentially better axial placement, esthetics, and subsequent biomechanical prosthetic restoration. Schwartz-Arad and Chaushu 10 consider immediate implants contraindicated when there is purulent exudate present; bone loss to the apex; intimate contact with certain anatomic structures, such as the mandibular canal, maxillary sinuses, or nasal cavity; or clinical conditions that prevent primary flap closure. Although some consider infected sites a contraindication, Novaes Jr and Novaes 17 reported that success can be achieved if certain clinical pre- and postoperative measures are followed, such as antibiotic administration, meticulous cleaning, and alveolar debridement before surgery. Primary flap closure is also desirable when placing immediate implants, and surgical techniques to extend the flap and reduce or avoid exposure of the implant must be considered. 18 Immediate implant placement can be contraindicated in the presence of periapical and periodontal lesions. 16,19 22 However, Novaes Jr and associates, 23 in a histomorphometric evaluation of immediate implant placement in dogs with induced periapical lesions, reported that osseointegration occurred in both experimental and control sites. According to these authors, immediate implant placement in the presence of periapical endodontic lesions is not contraindicated if appropriate therapy is carried out. However, immediate placement in periodontally infected extraction sites needs to be studied more comprehensively. Five young adult male mongrel dogs, weighing approximately 10 kg each, were used in this study. The animals had intact maxillae, atraumatic occlusion, and no oral viral or fungal lesions, and they were in good general health, with no systemic involvement. The procedures were in accordance with guidelines approved by the Council of the American Psychological Society (1980) for the use of animal experiments and were divided into 2 phases. Phase I The dogs were not fed the night before the surgical procedure. They received 2% Rompun (Bayer, Porto Alegre, RS, Brazil; 20 mg/kg at the dosage of 0.5 ml/10 kg intramuscularly); and were then anesthetized with 1 ml/kg thiopental (Cristália Laboratory, Itapira, SP, Brazil; 20 mg/kg Thiopental, diluted in 50 ml saline intravenously). Surgery was carried out by quadrants in each animal. In the first, second, third, and fourth mandibular premolars on the control side, the teeth received prophylaxis only. The contralateral side was used as the experimental group, where periodontitis was induced according to the technique of Schliephake and Kracht. 24 In summary, a nonresorbable silk suture was placed into infrabony pockets of approximately 1 mm in depth, which were created around each premolar after dissection of the marginal periodontium (Fig 1). After repositioning of the periodontal flaps, the wound was closed with resorbable sutures. The silk sutures were left in place for 3 months, during which time the animals were examined clinically every 4 weeks. At the end of 3 months, radiographs were taken to confirm the loss of alveolar bone height. Since the purpose of this phase was to induce periodontal infection, no prophylactic measures were taken. Phase II After 3 months of periodontal disease induction, the ligatures were removed. Attachment loss was observed clinically, which resulted in an increase of probing pocket depth and exposure of the bifurcations. The root surfaces were not cleaned, and granulation tissue was not removed. Periodontal infection was confirmed by the presence of deep periodontal pockets, bleeding on 392 Volume 18, Number 3, 2003
76 NOVAES ET AL probing, exudation after soft tissue compression, and radiographic evidence of bone loss and furcation involvement. After confirmation of periodontal disease at the experimental sites, the animals were anesthetized in the same manner as described in phase I of the experiment. The night before the second surgery, the animals received 20,000 IU penicillin and 1.0 g streptomycin/10 kg body weight intramuscularly (Pentabiótico Veterinário de Pequeno Porte, Wyeth Laboratory, São Bernardo do Campo, SP, Brazil). Because each dose provided antibiotic coverage for 4 days, another dose was injected 4 days later, for a total of 8 days of antibiotic coverage. This is a broad-spectrum antibiotic commonly used to treat infections in small animals 23 and has a systemic and local effect on the control of the periodontal infection. Full-thickness flaps were created on the experimental and control sides in the area of the first to fourth mandibular premolars. The teeth were sectioned in a buccolingual direction at the bifurcation, so that the roots could be individually extracted without damaging the bony walls. After extraction, the sites were meticulously debrided following a protocol previously described, 17 which involved curettage of the alveoli to remove all soft tissue tags and to stimulate resorption of the cortical lining, so as to expose the marrow cavities. The sites were then irrigated with a 50 mg/ml solution of tetracycline hydrochloride, and Frialit-2 implants (Friadent, Mannhein, Germany) with a grit-blasted/acid-etched surface, 4.5 mm in diameter and 8 mm in length, were placed immediately (4 implants each side; n = 40 implants total). The implants were placed according to the manufacturer s instructions, and flaps were sutured with resorbable sutures. The implants used are well suited for immediate implantation since they are rootlike in shape, ie, they are wider cervically to adapt clinically to the alveolar walls and taper apically so that smaller amounts of bone need to be removed during site preparation. The animals were maintained on a soft diet for 14 days. Healing was evaluated periodically, and the teeth were cleaned monthly with ultrasonic points. The animals were sacrificed with an overdose of thiopental 12 weeks after implant placement. Hemimandibles were removed, dissected, and fixed in 4% phosphate-buffered formalin (ph 7) for 48 hours and transferred to a solution of 70% ethanol until processing. The specimens were dehydrated in increasing concentrations of alcohol up to 100%; infiltrated and embedded in resin (LR White, London Resin Company, Berkshire, England); hard-sectioned using the technique described by Donath and Breuner 25 ; and stained with Stevenel s blue and Alizarin red S. Histomorphometric Analysis One longitudinal histologic mesiodistal section from each implant was evaluated, in accordance with several authors, using an optic microscope (Axiophot, Zeiss, Oberkochen, Germany) at 50 magnification. The microscopic images were captured by a videocamera (Sony CCD-IRIS, Sony Electronics, San Jose, CA) and digitized by a video grabber (Snappy, Play, Rancho Cordova, CA). Morphometry software (MetaMorf, Universal Imaging, West Chester, PA) was used to analyze the sections. With this system, the percent of implant-bone contact was determined from the middle third of the implants in accordance with Novaes Jr and associates 23 and Evans and colleagues. 30 The middle third of the implants was analyzed purposely to avoid the cervical third, because of possible resorption of the bone crest, and the apical third, because implants could closely approximate or slightly penetrate the superior wall of the inferior alveolar canal. The measurements started 2 mm below the bone margin, an area still possibly affected by the induced infection, because the anaerobic bacteria and their products induce a complex immune and inflammatory process within the periodontal tissues that will not only affect the whole quadrant in question, but may even be disseminated to other parts of the body. 31 A single blinded investigator, who had no knowledge of whether the sections were experimental or control, performed the analysis. Statistical Analysis The Mann-Whitney test was used for statistical analysis, with the level of significance set at 5%, using the implants as well as the dogs as experimental units. RESULTS Clinical Findings In phase I (first 3 months), periodontal infection was successfully induced on the experimental side (Fig 2a), with the presence of deep periodontal pockets as well as bleeding on probing and exudation after soft tissue compression. Bone loss and furcation involvement were observed radiographically (Fig 2b) on the experimental side. The control side had normal periodontal structures (Fig 2c). Based on these findings, phase II began with extraction of the teeth. Figure 3a depicts the control teeth and Fig 3b the experimental teeth. After The International Journal of Oral & Maxillofacial Implants 393





77 NOVAES ET AL Fig 2a Plaque accumulation during the 3 months of phase I on the experimental side. Fig 2b Radiographic aspect of experimental teeth after 3 months of phase I. Note bone loss in bifurcation and interproximal areas, indicating presence of periodontal disease. Fig 2c Radiographic aspect of control teeth after phase I. Good quality bone is apparent, and there is no evidence of radiolucencies. Fig 3a Clinical aspect of control side at the time of extraction. Normal levels of alveolar bone can be seen. Fig 3b Clinical aspect of teeth at extraction on experimental side after cleaning and removal of granulation tissue to demonstrate the bifurcation and bone loss. 394 Volume 18, Number 3, 2003
 showing bone (orange) in direct contact with implant (black) of the experimental group.")
.")

78 NOVAES ET AL Fig 4 Immediate implantation of root-analog implants after extraction of premolar teeth in dogs. Fig 5a Photomicrograph ( 50) showing bone (orange) in direct contact with implant (black) of the experimental group. Fig 5b Photomicrograph ( 125) showing bone (orange) in direct contact with implant (black) of the control group. Fig 5c Photomicrograph ( 125) of the same area, using polarized light microscopy. extraction, implants were placed on both sides (Fig 4). Healing progressed uneventfully during the 12- week postoperative period, without significant inflammation or exudate on either the experimental or the control side. At the time of sacrifice, radiographic evaluation showed a loss of 3 implants in the experimental group and 5 implants in the control group. All other implants were clinically stable at the end of the experiment. Histologic Observations The bone-implant interface had mineralized bone matrix in intimate contact with the implant surface. The bone tissue was characterized by concentric or parallel lamellar formations. Trabecular spaces of different diameters were covered by endosteum, and at some points were in close contact with the implant surface. Histomorphometric Findings Histomorphometric analysis revealed small differences in the percentage of bone-implant contact (Figs 5a and 5b). Figure 5c shows the same structures as in Fig 5b with polarized light microscopy. The mean percentage of direct bone-implant contact around the middle third of the experimental implants was 66.0 ± 19.6% (range 15.71% to 85.61%) and around the control implants was 62.4 ± 19.6% (range 21.18% to 88.52%). The difference was not statistically significant (Table 1; P.5). When each dog was used as an experimental unit, the differences were also not statistically significant. This analysis indicated mean bone-implant contact in the control group of ± 8.4% (range 53.09% to 76.35%) and in the experimental group ± 9.61% (range 45.73% to 80.57%). The International Journal of Oral & Maxillofacial Implants 395
79 NOVAES ET AL Table 1 DISCUSSION Percentage of Bone-Implant Contact Implant Control Experimental no. group group Mean Median SD Mann-Whitney test (P =.597). Different animals have been used to establish experimental periodontal disease with histologic, pathologic, and microbiologic characteristics similar to those of humans, including rats, 32,33 squirrel monkeys, 34 rhesus monkeys, 35 arctoides monkeys, 36 cynomolgus monkeys, and ferrets. 40 It has thus been shown that the placement of silk ligatures at the gingival margin leads to plaque accumulation and marginal periodontitis, with loss of connective tissue attachment and loss of alveolar bone in all of these animals. The more commonly used animal is the dog, as cited in the following studies. Dogs are susceptible to naturally occurring periodontal disease and experimental periodontitis, leading to alveolar bone loss. In dogs, periodontitisassociated plaque is easily induced, 41,42 and among the observed effects are enhanced subgingival plaque accumulation; a pronounced increase in gingival exudation; rapid formation of periodontal pockets; loss of alveolar bone, attachment, and tooth substance (resorption); and an apical displacement of the gingival margin. 43,44 The techniques used most often to induce this are the placement of an elastic band or a silk suture in the cementoenamel junction 45,46 or surgical creation of bone defects. 47,48 In the present study, both silk sutures and surgically created bone defects, in accordance with Schliephake and Kracht, 24 were used and resulted in a Class III furcation lesion, observed both clinically and radiographically. Healing occurred without problems. However, at sacrifice, there was a loss of 3 implants in the experimental group and 5 implants in the control group. This may occur if the diameter of the distal alveolus of the fourth premolar is slightly larger than that of the implant used. In spite of the fact that there was initial vertical bone-implant contact in the present study, soft tissue may have migrated into the vacant spaces as a result of the smaller diameter of the implant. In addition, implant loss is considered a normal finding in animals, especially in dogs For the histometric analysis, the middle third of the implants was analyzed 23,30 to intentionally avoid the cervical third (because of possible resorption of the bone crest ) and the apical third (because implants can closely approximate or slightly penetrate the superior wall of the inferior alveolar canal); both are common findings in studies with dogs. The percent of bone-implant contact in this study was 62.4% for control implants and 66.0% for experimental implants, which was not statistically significantly different. This percent of boneimplant contact is greater than the mean of 47.9% reported by Ettinger and associates, 55 who suggested that there can be a wide variation in boneimplant contact, depending on the quality of bone at any site and the remodeling process that is going on at the time. Implant surface characteristics may have positively influenced these results as suggested by Wong and coworkers. 56 They concluded in their paper that rough surfaces, such as the one used in this study, allow stronger early biomechanical retention with better bone-implant contact versus smooth surfaces. Immediate implant placement has the advantage of preserving the height and width of the alveolar bone. 11,21,57 59 Thus, it is one more treatment option that can be used when the loss of teeth is inevitable because of periodontal disease, if bone loss caused by the disease is not so dramatic as to prevent implant support. According to Lazzara, 3 one of the main diagnostic parameters that must be considered when evaluating a patient for dental implants is the amount of bone at the receptor site. Both the vertical height and the buccolingual bone dimensions must be considered in determining whether an endosseous implant can be placed. With these parameters, immediate implantation in cases of periodontal disease can be possible, safe, and easy, with results similar to those in disease-free sites. 396 Volume 18, Number 3, 2003
80 NOVAES ET AL SUMMARY The objective of this study was to evaluate the extent of bone-implant contact of implants placed in alveoli immediately after extraction of teeth with periodontal disease. In this animal population, the results of this study support the conclusion that periodontally infected sites may not be a contraindication for immediate implants, if appropriate antibiotics are administered preoperatively and postoperatively, and if meticulous cleansing and debridement of the alveoli are performed before implant placement, as described by Novaes Jr and Novaes 17 and Novaes and coworkers. 23 ACKNOWLEDGMENTS This study was supported by Friadent, Mannheim, Germany, and State of São Paulo Foundation for the Support of Research (FAPESP) (Process no. 98/ ). We would also like to thank Márcia S. Z. Graeff and Professor Enilza M. Espreafico, Department of Morphology, School of Medicine of Ribeirão Preto, University of São Paulo, Brazil, for their excellent technical assistance with the histomorphometric analysis. The authors wish to express their gratitude to Adriana L. G. Almeida for her assistance in the histologic processing of the implants. REFERENCES 1. Schulte W. The intra-osseous Al 2 O 3 (Frialit) Tuebingen implant. Developmental status after eight years (II). Quintessence Int 1984;15: Anneroth G, Hedström KG, Kjellman O, Köndell P-Å, Nordenram Å. Endosseous titanium implants in extraction sockets. An experimental study in monkeys. Int J Oral Surg 1985;14: Lazzara RJ. Immediate implant placement into extraction sites: Surgical and restorative advantages. Int J Periodontics Restorative Dent 1989;9: Schulte W, d Hoedt B, Axmann D, Gomez G. 15 Jahre Tübinger Implantat und seine Weiterentwicklung zum Frialit-2 System. Z Zahnärztl Implantol 1992;VIII, Novaes AB Jr, Novaes AB. IMZ implants placed into extraction sockets in association with membrane therapy (Gengiflex) and porous hydroxyapatite: A case report. Int J Oral Maxillofac Implants 1992;7: Novaes AB Jr, Novaes AB. Bone formation over a TiAl6V4 (IMZ) implant placed into an extraction socket in association with membrane therapy (Gengiflex). Clin Oral Implants Res 1993;4: Gomez-Roman G, Schulte W, d Hoedt B, Axman-Krcmar D. The Frialit-2 implant system: Five-year clinical experience in single-tooth and immediately postextraction applications. Int J Oral Maxillofac Implants 1997;12: Krump JL, Barnett BG. The immediate implant: A treatment alternative. Int J Oral Maxillofac Implants 1991;6: Barzilay I, Graser GN, Iranpour B, Natiella JR. Immediate implantation of a pure titanium implant into an extraction socket: Report of a pilot procedure. Int J Oral Maxillofac Implants 1991;6: Schwartz-Arad D, Chaushu G. The ways and wherefores of immediate placement of implants into fresh extraction sites: A literature review. J Periodontol 1997;68: Parr GR, Steflik DE, Sisk AL. Histomorphometric and histologic observations of bone healing around immediate implants in dogs. Int J Oral Maxillofac Implants 1993;8: Barzilay I, Graser GN, Iranpour B, Natiella JR, Proskin HM. Immediate implantation of pure titanium implants into extraction sockets of Macaca fascicularis. Part II: Histologic observations. Int J Oral Maxillofac Implants 1996;11: Wong K. Immediate implantation of endosseous dental implants in the posterior maxilla and anatomic advantages for this region: A case report. Int J Oral Maxillofac Implants 1996;11: Brägger U, Hämmerle CHF, Lang NP. Immediate transmucosal implants using the principle of guided tissue regeneration (II). A cross-sectional study comparing the clinical outcome 1 year after immediate to standard implant placement. Clin Oral Implants Res 1996;7: Watzek G, Haider R, Mensdorff-Pouilly N, Haas R. Immediate and delayed implantation for complete restoration of the jaw following extraction of all residual teeth: A retrospective study comparing different types of serial immediate implantation. Int J Oral Maxillofac Implants 1995;10: Barzilay I. Immediate implants: Their current status. Int J Prosthodont 1993;6: Novaes AB Jr, Novaes AB. Immediate implants placed into infected sites: A clinical report. Int J Oral Maxillofac Implants 1995;10: Novaes AB Jr, Novaes AB. Soft tissue management for primary closure in guided bone regeneration: Surgical technique and case report. Int J Oral Maxillofac Implants 1997; 12: Becker W, Becker BE. Guided tissue regeneration for implants placed into extraction sockets and for implant dehiscences: Surgical techniques and case reports. Int J Periodontics Restorative Dent 1990;10: Tolman DE, Keller EE. Endosseous implant placement immediately following dental extraction and alveoloplasty: Preliminary report with 6-year follow-up. Int J Oral Maxillofac Implants 1991;6: Werbitt MJ, Goldberg PV. The immediate implant: Bone preservation and bone regeneration. Int J Periodontics Restorative Dent 1992;12: Wilson TG Jr. Guided tissue regeneration around dental implants in immediate and recent extraction sites: Initial observations. Int J Periodontics Restorative Dent 1992;12: Novaes AB Jr, Vidigal GM Jr, Novaes AB, Grisi MFM, Polloni S, Rosa A. Immediate implants placed into infected sites: A histomorphometric study in dogs. Int J Oral Maxillofac Implants 1998;13: Schliephake H, Kracht D. Vertical ridge augmentation using polylactic membranes in conjunction with immediate implants in periodontally compromised extraction sites: An experimental study in dogs. Int J Oral Maxillofac Implants 1997;12: Donath K, Breuner G. A method for the study of undecalcified bones and teeth with attached soft tissues. J Oral Pathol 1982;11: The International Journal of Oral & Maxillofacial Implants 397
81 NOVAES ET AL 26. Caudill RF, Meffert RM. Histologic analysis of the osseointegration of endosseous implants in simulated extraction sockets with and without e-ptfe barriers. Part I. Preliminary findings. Int J Periodontics Restorative Dent 1991;11: Lekholm U, Becker W, Dahlin C, Becker B, Donath K, Morrison E. The role of early versus late removal of GTAM membranes on bone formation al oral implants placed into immediate extraction sockets. An experimental study in dogs. Clin Oral Implants Res 1993;4: Parr JA, Young T, Dunn-Jena P, Garetto LP. Histomorphometrical analysis of the bone-implant interface: Comparison of microradiography and bright-field microscopy. Biomaterials 1996;17: Terheyden H, Jepsen S, Möller B, Tucker MM, Rueger DC. Sinus floor augmentation with simultaneous placement of dental implants using a combination of deproteinized bone xenografts and recombinant human osteogeneic protein-1. A histometric study in miniature pigs. Clin Oral Implants Res 1999;10: Evans GH, Mendez AJ, Caudill RF. Loaded and nonloaded titanium versus hydroxylapatite-coated threaded implants in the canine mandible. Int J Oral Maxillofac Implants 1996; 11: Page RC. The pathobiology of periodontal diseases may affect systemic diseases: Inversion of a paradigm. Ann Periodontol 1998;3: Klausen B. Microbiological and immunological aspects of experimental periodontal disease in rats: A review article. J Periodontol 1991;62: Györfi A, Fazekas A, Suba Z, Ender F, Rosivall L. Neurogenic component in ligature-induced periodontitis in the rat. J Clin Periodontol 1994;21: Kennedy JE, Polson AM. Experimental marginal periodontitis in squirrel monkeys. J Periodontol 1973;44: Caton JG, Zander HA. Primate model for testing periodontal treatment procedures: I. Histologic investigation of localized periodontal pockets produced by orthodontic elastics. J Periodontol 1975;46: Slots J, Hausmann E. Longitudinal study of experimentally induced periodontal disease in Macaca arctoides: Relationship between microflora and alveolar bone loss. Infect Immun 1979;23: Kornman KS, Holt SC, Robertson PB. The microbiology of ligature-induced periodontitis in the cynomolgus monkey. J Periodontal Res 1981;16: Brecx MC, Nalbandian J, Ooya K, Kornman KS, Robertson PB. Morphological studies on periodontal disease in the cynomolgus monkey. II. Light microscopic observations on ligature-induced periodontitis. J Periodontal Res 1985;20: Nemeth E, Kulkarni GW, McCulloch CAG. Disturbances of gingival fibroblast population homeostasis due to experimentally induced inflammation in the cynomolgus monkey (Macaca fascicularis): Potential mechanism of disease progression. J Periodontal Res 1993;28: Fischer RG, Klinge B. Clinical and histological evaluation of ligature-induced periodontitis in the domestic ferret. J Clin Periodontol 1994;21: Lindhe J, Hamp S-E, Löe H. Experimental periodontitis in the beagle dog. J Periodontal Res 1973;8: Ericsson I, Lindhe J, Rylander H, Okamoto H. Experimental periodontal breakdown in the dog. Scand J Dent Res 1975;83: Schroeder HE, Lindhe J. Conversion of stable established gingivitis in the dog into destructive periodontitis. Arch Oral Biol 1975;20: Giargia M, Ericsson I, Lindhe J, Berglundh T, Neiderud A- M. Tooth mobility and resolution of experimental periodontitis. An experimental study in the dog. J Clin Periodontol 1994;21: Lindhe J, Ericsson I. Effect of ligature placement and dental plaque on periodontal tissue breakdown in the dog. J Periodontol 1978;49: Schroeder HE, Lindhe J. Conditions and pathological features of rapidly destructive, experimental periodontitis in dogs. J Periodontol 1980;51: Nishimura K, Noguchi Y, Yamada M, Shigeyama Y, Yamasaki A, Yamaoka A. Experimental periodontitis. J Osaka Dent Univ 1987;21: Al-Ali W, Bissada NF, Greenwell H. The effect of local doxycycline with and without tricalcium phosphate on the regenerative healing potential of periodontal osseous defects in dogs. J Periodontol 1989;60: Zarb GA, Symington JM. Osseointegrated dental implants: Preliminary report on a replication study. J Prosthet Dent 1983;50: Barzilay I, Graser GN, Iranpour B, Proskin HM. Immediate implantation of pure titanium implants into extraction sockets of Macaca fascicularis. Part I: clinical and radiographic assessment. Int J Oral Maxillofac Implants 1996;11: Rosenquist B, Grenthe B. Immediate placement of implants into extraction sockets: Implant survival. Int J Oral Maxillofac Implants 1996;11: Block MS, Kent JN, Kay JF. Evaluation of hydroxylapatitecoated titanium dental implants in dogs. J Oral Maxillofac Surg 1987;45: Gammage DD, Bowman AE, Meffert RM, Cassingham RJ, Davenport WA. Histologic and scanning electron micrographic comparison of the osseous interface in loaded IMZ and Integral implants. Int J Periodontics Restorative Dent 1990;10: Weber HP, Buser D, Donath K, et al. Comparison of healed tissues adjacent to submerged and non-submerged unloaded titanium dental implants. A histometric study in beagle dogs. Clin Oral Implants Res 1996 Mar;7: Ettinger RL, Spivey JD, Han D-H, Koorbusch GF. Measurement of the interface between bone and immediate endosseous implants: A pilot study in dogs. Int J Oral Maxillofac Implants 1993;8: Wong M, Eulenberger J, Schenk R. Effect of surface topology on the osseointegration of implant materials in trabecular bone. J Biomed Mater Res 1995;29: Ashman A. An immediate tooth root replacement: An implant cylinder and synthetic bone combination. J Oral Implantol 1990;16: Gelb DA. Immediate implant surgery: Three-year retrospective evaluation of 50 consecutive cases. Int J Oral Maxillofac Implants 1993;8: Knox R, Lee K, Meffert R. Placement of hydroxyapatitecoated endosseous implants in fresh extraction sites: A case report. Int J Periodontics Restorative Dent 1993;13: Volume 18, Number 3, 2003
82 Evaluation of Implant-Abutment Microgap and Bacterial Leakage in Five External-Hex Implant Systems: An In Vitro Study Eduardo Cláudio Lopes de Chaves e Mello Dias, DDS, MSc 1 /Edecir Décio Cargnin Bisognin, DDS, MSc 2 / Nassim David Harari, DDS, MSc, PhD 3 /Sílvio Jorge Machado, BBM 4 /Cristiano Pereira da Silva, DDS, MSc 5 / Glória Dulce de Almeida Soares, Eng, MSc, PhD 6 /Guaracilei Maciel Vidigal Jr, DDS, MSc, PhD 7 Purpose: The aim of the present study was to verify the presence of a microgap between implants and prosthetic abutments on their external surfaces in five different external-hex implant systems and to determine whether bacterial leakage occurs through the implant-abutment (I-A) interface. Materials and Methods: Ten samples of each implant system were used. Eight samples of each implant system were inoculated with 0.3 µl of a suspension of Escherichia coli for bacterial leakage evaluation. Two other samples were used as controls. Sample analysis was accomplished at 24 and 48 hours and on the 5 th, 7 th, and 14 th day after inoculation. After microbiologic analysis, all samples were prepared for I-A interface evaluation by scanning electron microscopy. The mean of the microgap misfit was obtained from six points at 1,000 and 3,000 magnifications. Results: The Neodent implant system (0.51 ± 0.39 µm) showed the closest adaptation, followed by Dentoflex (1.44 ± 0.73 µm), Titanium Fix (1.88 ± 1.28 µm), SIN (2.46 ± 3.38 µm), and Conexão (2.68 ± 3.02 µm). Twenty-five percent of the Dentoflex samples showed bacterial leakage through the I-A interface; no other implant system presented bacterial leakage. Conclusion: The width of the microgap at the I-A interface was less than 3 µm in all systems. A direct correlation between bacterial leakage and I-A interface misfit was not observed. INT J ORAL MAXILLOFAC IMPLANTS 2012;27: Key words: dental implant, microbial leakage, misfit 1 Master in Oral Implantology, Grande Rio University UNIGRANRIO Vitória, ES, Brazil. 2 Master in Oral Implantology, Grande Rio University UNIGRANRIO Centro, Macapá, AP, Brazil. 3 Associate Professor, Department of Oral Implantology, Grande Rio University UNIGRANRIO Duque de Caxias, RJ, Brazil. 4 Coordinator, Multidisciplinary Laboratory Department of Microbiology, Grande Rio University UNIGRANRIO Duque de Caxias, RJ, Brazil. 5 Master in Microbiology, Grande Rio University UNIGRANRIO Duque de Caxias, RJ, Brazil. 6 DSc in Metallurgical and Materials Engineering, Universidade Federal do Rio de Janeiro, COPPE/UFRJ, Cidade Universitária, Rio de Janeiro, RJ, Brazil. 7 Professor and Chair, Department of Oral Implantology, Grande Rio University UNIGRANRIO Copacabana, RJ, Brazil. Correspondence to: Dr Eduardo Cláudio Lopes de Chaves e Mello Dias, Av Rio Branco, 1305 / 103, Praia do Canto Vitória-ES Brazil, CEP: Fax: eduardodias@uol.com.br Since the introduction of osseointegration, classical longitudinal studies have demonstrated the longterm success of osseointegrated implants. 1,2 Several factors can negatively influence the longevity of an implant, including the presence of subclinical inflammation at the implant-abutment (I-A) interface. 3 6 Surveys of dental implant systems show that external-hexagon connections are used in more than 90% of systems on the market, accounting for the majority (ie, 66.9%) of the titanium dental implant market in Therefore, adequate knowledge of this connection and its biologic and biomechanical effects is necessary. It has been demonstrated that the design of the I-A interface can influence the dimensions and health of the peri-implant soft tissues and bone crest. 8,9 Some authors have suggested that the remodeling of the crestal bone that occurs after stage-two surgery is a result of an inflammatory process in the peri-implant tissues caused by the accumulation of bacterial biofilm at the I-A interface. 4,6,10,11 Because bacterial biofilm is considered an important etiologic factor in peri-implantitis, bacterial leakage at the I-A interface can negatively affect the outcome of treatment and interfere in long-term results. 12 Colonization of the internal parts of osseointegrated implants following bacterial leakage has been demonstrated in several implant systems Bacterial biofilm at the I-A interface impairs the subcrestal biologic width, leading 346 Volume 27, Number 2, BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY. NO PART OF MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION FROM THE PUBLISHER.
83 Dias et al Table 1 Characteristics of the Tested Samples System Implant model Abutment (code) Tightening torque (Ncm) Neodent Titamax TI Conexão (Conexão Sistema de Prótese Ltda) Porous SIN (SIN Sistema de Implantes Ltda) SCO4010 MA Dentoflex (Dentoflex Ind. e Com. de Produtos Odontológicos Ltda) IMHE MARFHE Titanium Fix (A S Technology) SP311 AES All implants featured a 4.1-mm platform and a 0.7-mm external-hex I-A connection. it to a more apical position and causing marginal bone loss. 22 Finally, the most common consequence is soft tissue marginal recession of approximately 1 mm after stage-two surgery, which can negatively influence the esthetic result. 23 Therefore, the I-A interfaces of all implant systems should be evaluated to determine their ability to prevent bacterial leakage. The aim of the present study was to evaluate the I-A interfaces of five different implant systems using scanning electron microscopy (SEM) and to determine their capacity for bacterial leakage through this interface. MATERIALS AND METHODS Fifty samples of five different implant systems were used (10 samples per implant system). Each sample was composed of one implant and its abutment. The implant systems and characteristics of their components are described in Table 1. Microbiologic Testing Protocol For the evaluation of bacterial leakage at the I-A interface, 10 samples of each implant system were used: eight samples for the test group, one sample for a positive control, and one for a negative control. The samples were inoculated with 0.3 µl Escherichia coli suspension containing 10 8 colony-forming units per milliliter (reference no , American Type Culture Collection); this was applied inside the hollow of the internal portion of the implant using a micropipette (Pipetman, Gilson SAA). E coli is a gram-negative bacteria measuring 1 to 1.5 µm in diameter and 2 to 6 µm in length. It is widely for in vitro studies, especially for evaluating contamination, disinfection, and sterilization. In addition, it is easy to handle in the laboratory, has a generation time of 20 minutes, and can be found in the oral cavity of healthy individuals. 24 Immediately after the inoculation, the abutment was connected to the implant and torque was applied to the abutment screw as recommended by the manufacturer (Table 1). Then a sterile swab was rubbed across the I-A interface to reveal the presence of any external contamination caused by spilling of the suspension. The access channels of the abutment screws were closed with gutta-percha (Dentsply), and sealed with a cyanomethyl methacrylate adhesive glue (Henkel) applied over the gutta-percha, as proposed by Do Nascimento et al. 25 The samples and swabs were then placed in separate tubes containing the culture medium (MacConkey broth). For each implant system, one assay was performed as a positive control and another was performed as a negative control. In the positive control, 0.3 µl of the E coli suspension was inoculated directly into the hollow portion of the implant, then immediately placed into the tube with the culture medium, without an abutment being attached. In the negative control, the I-A assembly was placed directly into the tube with the culture medium without inoculating with the E coli suspension. The tubes containing the inoculated samples and the culture medium, as well as the positive and negative controls and swabs, were incubated at 37 C in a microbiologic incubator (Quimis Aparelhos Científicos, Model Q-316M). The presence of bacteria in the culture medium, indicating bacterial leakage during the experimental periods of 24 hours, 48 hours, and the 5 th, 7 th, and 14 th day after inoculation, was identified by clouding of the culture medium. From each sample with positive signs of bacterial leakage, a small portion (1 µl) of the contaminated culture medium was placed onto MacConkey agar plates to confirm the presence of viable colonies consistent with the presence of E coli. Samples from colonies on agar plates were gram-stained and observed with an optical microscope (Coleman) to confirm the presence of gram-negative bacteria. Microgap Evaluation at the I-A Interface To evaluate the I-A microgap, all test samples were sterilized in an autoclave (Cristofoli Lister 12L) for 22 minutes The International Journal of Oral & Maxillofacial Implants BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY. NO PART OF MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION FROM THE PUBLISHER.
.")

84 Dias et al Abutment 200 µm 100 µm 0 µm Implant Fig 1 Diagram of misfit analysis at the I-A interface showing points 1, 2, and 3, which are equivalent to the outermost point and the 100-µm diameter and 200-µm diameter points, respectively. Fig 2 Longitudinal section of a Dentoflex sample I-A interface (magnification 3,000). Table 2 Average Values of I-A Microgap and Percentage of Samples with Bacterial Leakage Implant system Mean microgap (μm) (± SD) Leakage (%) Neodent 0.51 ± Dentoflex 1.44 ± Titanium Fix 1.88 ± SIN 2.46 ± Conexão 2.68 ± SD = standard deviation. Table 3 Distribution of Misfit in All Groups According to the Classification of Misfit Proposed by Kano et al 26 Classification Percentage of samples Type I 7.5 Type II Type III 5 Type IV 40 No classification 6.25 Misfit classifications: type I = no horizontal or vertical measurable misfit; type II = horizontal misfit only; type III = vertical misfit only; type IV = horizontal and vertical misfit; no classification = could not be evaluated. at a temperature of 121 C and a pressure of 1.0 KgF/cm 2. The abutments were tightened on the implants with the torque recommended by the manufacturer, as described in Table 1, using a manual torque wrench. The samples were embedded in epoxy resin (Epofix, Struers S/A). They were cut longitudinally and sanded in the longitudinal direction using a sequence of silicon carbide sandpapers with grain sizes of 100, 220, 320, 400, 600, and 1,200 (3M Brasil). Then the samples were polished with diamond paste with granule sizes of 6 µm, 3 µm, and 1 µm. Finally, aluminum oxide was used to remove any traces of fat and impurities. All samples were washed with alcohol and dried. The I-A interfaces were measured using SEM (JEOL JSM-6460LV) with magnifications of 1,000 and 3,000 at three points on each side. The outermost point was designated point 1, point 2 was located 100 µm from the edge, and point 3 was 200 µm from the edge; this method produced six measurements of each sample (Fig 1). Statistical Analysis The nonparametric Kruskal-Wallis test and the multiple-comparisons Fisher protected least significant difference test were used to evaluate the results of I-A misfit. A significance level of 5% was used. RESULTS Microbiologic Results Only two samples of the Dentoflex implant system exhibited bacterial leakage (Table 2), for which the swab tests had been negative. One sample of the Conexão implant system presented clouding of the culture medium, but for this sample, the swab test had been positive. The complete microbiologic test was repeated for this sample, and both clouding of the sample medium and the swab test were negative. All samples exhibiting bacterial leakage resulting in clouding of the medium 348 Volume 27, Number 2, BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY. NO PART OF MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION FROM THE PUBLISHER.
. Fig 6 Longitudinal section of type IV I-A interface misfit (both horizontal and vertical misfit) (magnification 500).")


 (Table 3) (Figs 3 to 6). The Kruskal-Wallis test showed significant differences among groups (P <.05).")
85 Dias et al Fig 3 Longitudinal section of type I I-A interface misfit (magnification 500). Fig 4 Longitudinal section of type II I-A interface misfit (horizontal misfit only) (magnification 500). Fig 5 Longitudinal section of type III I-A interface misfit (magnification 500). Fig 6 Longitudinal section of type IV I-A interface misfit (both horizontal and vertical misfit) (magnification 500). within 24 hours of inoculation. The samples of Neodent, SIN, and Titanium Fix implant systems did not present evidence of bacterial leakage at any time. Microgap Evaluation Misfit values ranged from 0 to 18.4 µm; average values of the I-A microgap are presented in Table 2. However, misfits were not observed continuously along the I-A interface of all samples but in discrete areas (Fig 2). Vertical and horizontal discrepancies at the outer edge of the I-A interface were also observed in all systems. According to the classification system to measure the I-A microgap proposed by Kano et al, 26 most of the I-A interfaces observed were classified as type II (horizontal misfit only) and type IV (both horizontal and vertical misfit) (Table 3) (Figs 3 to 6). The Kruskal-Wallis test showed significant differences among groups (P <.05). The Fisher least significant difference test showed a significant difference only between the Neodent and Conexão implant systems. No other statistically significant differences were found between groups. DISCUSSION Studies that have evaluated external abutment misfit may have overestimated the influence of microgaps at the I-A interface. 13,14,27 In the current study, despite the presence of misfits at the most external portion of the interface, as evaluated using SEM, only a few samples showed bacterial leakage. This might be explained by the fact that a vertical misfit observed at the outer edge of the I-A interface is not continuous from the periphery to the inner portion of the implant, but instead is intermittent, as observed in the longitudinally sectioned samples. Possibly, the path of the microgap is localized to restricted areas and thus it does not always maintain The International Journal of Oral & Maxillofacial Implants BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY. NO PART OF MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION FROM THE PUBLISHER.
86 Dias et al a uniform width from the external to the internal portion of the implant. It may be that the microgap has a sinuous or incomplete path through the I-A interface; more studies to evaluate this interface in a threedimensional way are necessary. The degree of bacterial leakage in a specific implant system presumably is a multifactorial condition dependent on the precision of fit between the implant and the abutment, the degree of micromovement between the components, and the amount of torque used to connect the components. 28 In this study, the implants were connected to the abutments with the manufacturers recommended torque and first subjected to bacterial analysis and later to SEM analysis. Thus, the question of deformation arises. In an in vitro study, 15 implant-supported frameworks were cyclically loaded for 200,000 cycles with a load of 200 N. The data failed to show that gaps at the I-A interface were significantly different from those of as-manufactured abutments. 29 This suggests that the torque forces used to connect implants to abutments do not cause significant deformation at the I-A interface. The results of the bacterial leakage, which occurred within the first day, corroborate the findings of Jansen et al. 13 The use of a sterile swab rubbed across the I-A interface just after connecting the abutment to the implant to evaluate the possibility of external contamination caused by spilling the suspension, turned out to be an important step in the present study. In one implant system, the sample and swab tubes became cloudy, suggesting contamination caused by a spill not visible to the naked eye. Although the use of viable bacteria was effective in detecting bacterial leakage, it presents some limitations such as bacteria size, since bacteria smaller than E coli exist. Culture-independent methods, like checkerboard DNA-DNA hybridization, may help to provide additional information on the presence of bacterial leakage at the I-A interface. The presence of micromovement at the I-A interface is an important factor that should be considered. Micromovements can act as a pump, creating a flux between the external and internal parts of the implants. Hermann et al 3 observed less crestal bone loss around implants that received a laser weld at the I-A interface and therefore functioned as a one-piece implant without micromovements at the I-A interface than around two-piece implants. It was concluded that this difference was mainly related to the presence of the micromovement rather than to the microgap size, although it should be considered that the size of the microgap could be related to the level of micromovement and the quantity of local toxins and bacteria. Furthermore, rigidity at the I-A interface does not necessarily indicate a lack of microgaps, which can play an important role as a reservoir for commensal and/or pathogenic bacteria, especially anaerobic and microaerophilic species representing a potential source of tissue inflammation. 24,25,30 Recently, Baixe et al 31 observed larger microgaps for flat-to-flat I-A interfaces than for conical interface systems. However, some studies have demonstrated that the conical I-A interface fails to prevent bacterial leakage. 21,24 Probably the higher prevalence of I-A interface types I and IV could be related to the manufacturers efforts to prevent crestal bone interference during abutment placement at stage-two surgery. With this goal in mind, some abutments are deliberately manufactured undersize by some micrometers in diameter in relation to the implant diameter. Because I-A misfit influences crestal bone levels, it is possible that its size exerts an important influence on peri-implant health Some implant systems evaluated in this study had high standard deviations for misfit, although this could be a result of manufacturing inaccuracies. Some samples had no misfit, while others showed microgaps of more than 13 µm in diameter. Hermann et al 3 showed that the size of the microgap at the outer edge of the I-A interface did not significantly influence crestal bone levels. Moreover, an in vitro study showed no direct relationship between the size of the microgap and bacterial leakage. 13 Similarly, the present study was not able to establish this relationship. This could be related to the fact that prior studies evaluated only peripheral misfit at the I-A interface and suggests that increased misfit at the I-A external surface may not be the only determining factor in the occurrence of bacterial leakage through this interface. Since this misfit is not very deep, it may not reach the inner portion of the implant. CONCLUSIONS The size of the microgap at the implant-abutment (I-A) interface was less than 3 µm in all five systems tested. A misfit on the most external portion of the I-A interface may not be continuous internally. The misfit at the I-A external surface may not be the only determining factor in the occurrence of bacterial leakage through this interface. Only two samples of one implant system allowed bacterial leakage. A direct correlation between bacterial leakage and misfit at the I-A interface was not observed. 350 Volume 27, Number 2, BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY. NO PART OF MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION FROM THE PUBLISHER.
87 Dias et al ACKNOWLEDGMENTS The authors wish to thank Neodent, Curitiba, Brazil; Conexão Sistema de Prótese Ltda, São Paulo, Brazil; SIN Sistema de Implantes Ltda, São Paulo, Brazil; Dentoflex Industria e Comércio de Produtos Odontológicos Ltda, São Paulo, Brazil; and AS Technology, São José dos Campos, Brazil, for providing the tested implant components. The authors would also like to thank Dr Edson Jorge Lima Moreira for his help with statistical analysis in the study. REFERENCES 1. Adell R, Lekholm U, Rockler B, Brånemark PI. A 15-year study of osseointegrated implants in the treatment of the edentulous jaw. Int J Oral Surg 1981;10: van Steenberghe D, Lekholm U, Bolender C, et al. Applicability of osseointegrated oral implants in the rehabilitation of partial edentulism: A prospective multicenter study on 558 fixtures. Int J Oral Maxillofac Implants 1990;5: Hermann JS, Schoolfield JD, Schenk RK, Buser D, Cochran DL. Influence of the size of the microgap on the crestal bone changes round titanium implants. A histometric evaluation of unloaded non-submerged implants in the canine mandible. J Periodontol 2001;72: Broggini N, McManus LM, Hermann JS, et al. Persistent acute inflammation at the implant-abutment interface. J Dent Res 2003;82: Weng D, Nagata MJH, Bell M, Bosco AF, de Melo LGN, Richter EJ. Influence of microgap location and configuration on the periimplant bone morphology in submerged implants. An experimental study in dogs. Clin Oral Implants Res 2008;19: Broggini N, McManus LM, Hermann JS, Medina RU, Buser D, Cochran DL. Peri-implant inflammation defined by the implant-abutment interface. J Dent Res. 2006;85: Tsuge T, Hagiwara Y. Influence of lateral-oblique cyclic loading on abutment screw loosening of internal and external hexagon implants. Dent Mater J 2009;28: O Mahony A, MacNeill SR, Cobb CM. Design features that may influence bacterial plaque retention: A retrospective analysis of failed implants. Quintessence Int 2000;31: Puchades-Roman L, Palmer RM, Palmer PJ. A clinical, radiographic and microbiologic comparison of Astra Tech and Brånemark single tooth implants. Clin Implant Dent Relat Res 2000;2: Ericsson I, Person LG, Berglundh T, Marinello CP, Lindhe J, Klinge B. Different types of inflammatory reaction in peri-implant soft tissues. J Clin Periodontol 1995;22: Brägger U, Hafeli U, Huber B, Hämmerle CH, Lang NP. Evaluation of postsurgical crestal bone levels adjacent to non-submerged dental implants. Clin Oral Implants Res 1998;9: Zitzmann NU, Abrahamssom I, Berglundh T, Lindhe J. Soft tissue reaction to plaque formation at implant abutments with different surfaces topography. An experimental study in dogs. J Clin Periodontol 2002;29: Jansen VK, Conrads G, Richter E. Microbial leakage and marginal fit of the implant-abutment interface. Int J Oral Maxillofac Implants 1997;12: Coelho PG, Sudack P, Suzuki M, Kurtz KS, Romanos GE, Silva NRFA. In vitro evaluation of the implant abutment connections sealing capability of different implant systems. J Oral Rehabil 2008;35: Quirynen M, van Steenberghe D. Bacterial colonization of the internal part of two-stage implants. An in vivo study. Clin Oral Implants Res 1993;4: Quirynen M, Bollen CML, Eyssen H, van Steenberghe D. Microbial penetration along the implant components of the Brånemark system. An in vitro study. Clin Oral Implants Res 1994;5: Persson LG, Lekholm U, Leonhardt Å, Dahlen G, Lindhe J. Bacterial colonization on internal surfaces of Brånemark system implant components. Clin Oral Implants Res 1996;7: Guindy JS, Besimo CE, Besimo R, Schiel H, Meyer J. Bacterial leakage into and from prefabricated screw-retained implant-borne crowns in vitro. J Oral Rehabil 1998;25: Gross M, Abramovich I, Weiss EI. Microleakage at the abutmentimplant interface of osseointegrated implants: A comparative study. Int J Oral Maxillofac Implants 1999;14: Piattelli A, Scarano A, Paolantonio M, et al. Fluids and microbial penetration in the internal part of cemented-retained versus screwretained implant-abutment connections. J Periodontol 2001;72: Aloise JP, Curcio R, Laporta MZ, Rossi L, da Silva AMA, Rapoport A. Microbial leakage through the implant-abutment interface of Morse taper implants in vitro. Clin Oral Implants Res 2010;21: Grunder U, Gracis S, Capelli M. Influence of the 3-D bone-to-implant relationship on esthetics. Int J Periodontics Restorative Dent 2005; 25: Small PN, Tarnow DP. Gingival recession around implants: A 1-year longitudinal prospective study. Int J Maxillofac Implants 2000;15: Deconto MA, Salvoni AD, Wassal T. In vitro microbiological bacterial seal analysis of the implant/abutment connection in Morse taper implants: A comparative study between 2 abutments. Implant Dent 2010;19: Do Nascimento C, Barbosa RES, Issa JPM, Watanabe E, Ito IY, Albuquerque RF Jr. Use of checkerboard DNA-DNA hybridization to evaluate the internal contamination of dental implants and comparison of bacterial leakage with cast or pre-machined abutments. Clin Oral Implants Res 2009;20: Kano SC, Binon PP, Curtis DA. A classification system to measure the implant-abutment microgap. Int J Oral Maxillofac Implants 2007;22: King GN, Hermann JS, Schoolfield JD, Buser D, Cochran DL. Influence of the size of the microgap on crestal bone levels in non-submerged dental implants: A radiographic study in canine mandibles. J Periodontol 2002;73: Steinebrunner L, Wolfart S, Bössmann K, Matthias K. In vitro evaluation of bacterial leakage along the implant-abutment interface of different implant systems. Int J Oral Maxillofac Implants 2005;20: Hecker DM, Eckert SE, Choi Y-G. Cyclic loading of implant-supported prostheses: Comparison of gaps at the prosthetic-abutment interface when cycled abutments are replaced with as-manufactured abutments. J Prosthet Dent 2006;95: Besimo CE, Guindy JS, Lewetag D, Meyer J. Prevention of bacterial leakage into and from prefabricated screw-retained crowns on implants in vitro. Int J Oral Maxillofac Implants 1999;14: Baixe S, Fauxpoint G, Arntz Y, Etienne O. Microgap between zirconia abutments and titanium implants. Int J Oral Maxillofac Implants 2010;25: Hermann JS, Buser D, Schenk RK, Cochran DL. Crestal bone changes around titanium implants. A histometric evaluation of unloaded non-submerged and submerged implants in the canine mandible. J Periodontol 2000;71: Oh T-J, Yoon J, Misch CE. The causes of early implant bone loss: Myth or science? J Periodontol 2002;73: Todescan FF, Pustiglioni FE, Imbronito AV, Albrektsson T, Gioso M. Influence of the microgap in the peri-implant hard and soft tissues: A histomorphometric study in dogs. Int J Oral Maxillofac Implants 2002;17: The International Journal of Oral & Maxillofacial Implants BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY. NO PART OF MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION FROM THE PUBLISHER.

88 A New Concept in Maxillary lmplant Surgery: The Osteotome Technique Robert B. Summers,DMD Practice Limited to Periodontics and lmplantology Ardmore, Pmnsylaania Attending Staff Bryn MnwrHospital Bryn Mnwr,Pmnsylaanin Implantology Staff Albcrt Einstein Medical Cmt er Guest Lecturer Unionsity of P.ennsylaania School of DmtalMedicine Phikdelphia, P ennsy la ania Editor's Note: The Compendium rs pleased to introduce a nans surgical methodology t'or maxillary implant placement.this article is tlre first ot' a fuur-part sqies dnoted to the osteotome technique. Oaerall concepts are provided in this issue. Part 2 Apnl199q wii detail ridge enlargement procedures. Part 3 (fune L994) will describe a less inaasit:e sinus elwation surgery. A final article will deal with the tuberosity. We are pleased to bring thb technique to your attmtion. he standard method of pre' paring a bone site to receive an endosseous implant (the Abstract This article reviews the limitations of drilling into soft bone to place endosseous implants. Differences among bone types and the anatomy of the maxilla are described. The osteotome technique, which is a new method of placing implants into maxillary bone without drilling, and the rationale for two other procedures, the osteotome sinus floor elevation and the ridge expansion osteotomy, are detailed. How osteotomes conserve osseous tissue and may improve bone density around the implant is also discussed. A pilot study that shows excellent results with several types of press-fit implants using the osteotome technique is provided. The author concludes that the osteotome technique is superior to drilting for many applications in soft maxillary bone. Furtherutore, the osteotome technique allows more implants to be inserted in a greater variety of sites during a routine office procedure. Learning Objectives After reading ihis article the reader should be able to:. explain the advantages and rationale of the osteotome technique compared to drilling in the maxilla.. describe the osteotome technique.. recognize the potential applications of the osteotome technique. o describe two new procedures, the osteotome sinus floor elevation and the ridge expansion osteotomy, performed with the osteotome instruments. osteotomy) involves the removal of bone with a graded series of drills of increasing sizes. The largest driil in the series approximates the length and diameter of the implani to be inserted.l In areas where there is adequate bone of good quality, a careful surgical technique with drills can produce consistent results.2j In the mandible, Briinemark classificaiion type I and II bone predominates. Lr this area, drilling is the practical and convenient means of placing implants.3-s A dense crestal cortex is generally available for initial fixation of the implant. Often the implant can be placed to take advantage of one or both of the buccal and lingual cortical plates.{5 Placing implants in the maxilla 152 Compend Contin Educ Dent, Vol. XV. No. 2

89 W, Figure 1A-Different bone types. Type I is homogeneous compact bone. \--r' Figure lb-type ll bone has a thick cortical layer and a dense core. Figure 1C-Type lll bone has a thin cortical layer and a trabecular core of good strength. Figure 1D-Type lv bone has a thin cortical layer and a cancellous core of poor strength. presents a different set of surgical problems compared to the mandible. in the maxilla, the bone is generally type III or [V.]5 The hard cortex is thin or entirely absent. Re. sorption and prominent sinuses often limit the number of good sites available for a routine procedure. Spiny ridge areas, too narrow in buccopalatal dimension for drilling, are common2i,6 (Figure 1). The qualitv of maxillary bone can be extremely variable in a single location. It is likely that a maxilla will contain voids, fatty marrow, and fibrous inclusioni. The resorbed maxilla is generally an undercut shape, so that the surgeon is forced to place implants with a flared inclination toward the buccal. The arch form results in more difficult emergence angulations and complex abutment needs.t'8'10 As osteotomy preparation progresses toward the posterior, the surgeon usually notices softer bone texture. The ability to drill ac- 154 Compend Contin Educ Dent, Vol. XV, No. 2 Figure 2A-The osteotomes developed by the author. curately in the posterior maxilla diminishes with the loss of tactile sensitivity in soft bone when using rotating insfruments. Also, inadvertent sinus penetration and overpreparation of soft bone is corunon with drills. Other factors, such as torquing of the handpiece and reproduciog a consistent angle of penetration, become more demanding as bone density decreases in the posterior maxilla.e'll With the drilling technique, visibitity is reduced in the posterior maxilla because the handpiece and contra-angie obscure the surgeon's vision. To compensate for loss of tactile sensitivity and provide control in soft bone, the surgeon must place both hands as close as possible to the rotating drill, blocking the line of sight. Adjacent and opposing teeth limit access, and the irrigation stream required for drilling further impairs visualization. The frustration of placing implants with drills in soft maxillary bone has been experienced by all Figure 2B-Note the Goncave tips and continuous taper. implant surgeons. Long-term, multicenter studies verify that results with drilling in type IV bone have not approached the success rates of drilling into other bone types.t2 The literature is replete with cautionary statements about the diminished potential of the maxilla compared with the mandible for routine drilling procedures. A more conservative approach is generall/ advissd.z,a,e Less cantilevering is used in the maxilla, and shorter-length implants are avoided unless bone quality of the implant site is good. Fixed cases in a resorbed maxilla often end around the second premolar because of the sinus.2 More traumatic surgery, such as sinus or ridge-crest grafting, has been the alternative used to compensate for anatomic and bone-quality limitations.r3ra The Osteotome Technique Because of the problems of drilling in the maxilla, this article presents a means of osteotomy preparation in which the bone is not

90 'removed. This method is called the osteotome technique. The obfective of this technique is to maintain, if possible, all of the existing maxillary bone by pushing the bone aside with minimal trauma while developing an accurately shaped osteotomy. The osteotome technique attempts to retain all of the bone that is present, and to take advantage of the softer bone quality by relocating the bone to suit the needs of the surgery. In addition, pushing or tapping the osteotomes into place hopefully will compact the osseous layer around the osteotomy, which will form a denser bone interface with the implant (Figures 2A and 2B). Drilling always takes bone away from a site. Often there is a marginal quantity of bone to start with. During the driliing process, there is no practical means to immediately improve adjacent bone quality. In addition, drilling creates heat, which is the main obstade to osseointegration. With the osteotome technique, the bone layer next to the osteotomy can be improved because of the instrumentation used to prepare the site. This potentiai compaction of bone may heip to maintain fixation of the newly placed implanr. Also, the osteotome technique is essentiaily heatless (Figure 3). Expansion of the Ridge ln contrast to drilling, the osteotome technique improves maxillary anatomy by widening the ridge as the instruments are inserted. The osteotomes, developed by the author (Summers Osteotome Kit"), are shaped so that the next larger osteotome tip fits into the opening created by the previous instrument. Bone buccal and palatal to the osteotomy is pushed laterally with successive penetrations of the larger osteotomes. In a narrow ridge, expansion of the a Implant Innovations, Inc, West Palm Beach, FL Figure 3-The bone layer adjacentto the osteotomy is compacted with the ostestome technique. I I lnros" ll O I :-1..'... wn r\4m FigureLRidgeexpansionosteotomycanbeittempt.aat@ 3 mm. Buccal and lingual bone movei laterally as the osteoto-", ur" inserted. Figure5_Theo5teotomesjnusf oore evation(os@ntofthe penetrating osteotomes, allowing the sinus floor to be displaied upwards. buccopalatal dimension of the site is an inherent beneficial characteristic of the osteotome technique. This is called a ridge expansion osteotomy (REO), in contrast to a drilled site, in which the buccopaiatai bone width is not changed. The REO (Figure 4) allows more narrow ridge sites to be used for implants within the scope of a routine office procedure. The osteotomes have concave tips with a sharpened edge. This design allows the instruments to shave a layer of bone from the side wall of the osteotomy during insertion. The concave tips tend to coilect and hold bone, assisting in pushing this material in front of the advancing osteotome. Additional bone can be added from the adjacent ridge or another source Compend Contin Educ Dent. Vol. XV, No.2 l55

91 Figure 6A-The small diameter osteotome (No. 1 size) is shown starting the osteotomy into the tuberosity. Figure 6B-Osteotomy near completion with a No. 3 osteotome inserted to 10 mm. Figure 6C-ln a partially edentulous patient, three consecutive osteotomy sites prepared with the osteotome technique. Three 13-mm hexcylinder implants were placed. Figure 7A-Osteotome technique distal to a remaining molar. and conveniently carriedinto the osteotomy with the instnrments. The piling up of bone in front of the osteotomes facilitates elevation of the sinus floor. The osteotome sinus floor elevation (OSFE) procedure is simpler, more predictable, probably safer, and less traumatic than previously described techniques Figure 5). Although access is an issue with any technique in the posterior maxilla, osteotomes have an advantage to drilling in most cases. The surgeon's hands are placed well away from the penetrating tips, providing improved visibility. The straight-line shape and long handles of osteotomes facilitate precise control and alignment with landmarks and paralleling pins. Also, there is no irrigation stream to obscure the surgeon's vision. 156 Compend Contin Educ Dent. Vol. XV, No.2 Figure 7B-Access is adequate for a second implant. Osteotome Access Into the Edentulous Tuberosity The entire posterior maxilla, inciuding the tuberosity, is usually accessible for straight-in osteotome use (Figures 6.4. through 6C). Even if a maxillary molar remains, osteotomes frequently can be used with precision distal to the remaining tooth. When the moiar area is edentulous, probing and positioning with osteotomes in thai entire segment is possible in an average patient (Figures 7 A and 7B). One advantage of osteotomes over drilling anywhere in the maxilla is in terms of tactile sensitivity. The instruments are extremely sensitive to changes in bone texture and density, so they are useful for probing. This feature allows the surgeon to locate the best quality bone in a site by penetrating and redirecting the smaller diameter osteotomes along differing axes. Often there is a tactile difference in the bone next to the sinus that can be discerned with the osteotomes. The instruments are relatively nondestructive compared to drills when used as penetrating probes, so a site usuady is not degraded or destroyed by the probing process. Other potential benefits of the oste' otome technique indude: 1. Alteration of the anterior or posterior sinus boundary during a routine osteotomy. 2. More upright (less flared) positioning of implants. The osteotome technique provides greater flexibilify for the surgeon to match opposing landmarks because of the REO feature. 3. Development of future implant sites. 4. Addition of bone into the osteotomy as the site is developed. Upcoming articles will appear inthe Compendium that will detail the use of the ostestome technique for REO, OSFE, and the tuberosity. Methods and Materials This report will encompass L43 consecutively placed press-fit implants of severai shapes and diameters inserted into type IV bone by the osteotome technique. Both hydroxyapatite-coated and
- coated implants were used in the study.")
92 Table l-lmplants By Type and Design Type Micro-VenPn Micro-VenP Integraleb Hexcylinder Hexcylinder Hexrylinder Hexcylinder Total Diameter 3.25 mm 4.25 mm 4.0 mm 3.3 mm 4.0 mm 3.3 mm 4.0 mm Surface HA HA HA HA HA TPS TPS adentsply/lmplant Division, Encino, CA bcalcitek, Inc, Carlsbad, CA titanium-plasma-spray (TPS)- coated implants were used in the study. It should be noted that many of the implants used in this study have a neck design that is wider than the shaft. In spite of careful bone preparation with osteotomes, in spongy bone, it was often the larger-diameter neck that ailowed initial fixation of the implant. Preoperative evaluation and stent fabrication were performed in the customary manner. Some of the patients had preoperative computed tomography scans. Final de. termination of bone type was based on clinical assessment during surgery. Table 1 lists the type of implants used in the osteotome study group/ and Table 2 shows the loading time and location of theimplants. Results All impiants in the study have been judged by standards as recommended by Albrektsson et al,rs SHd,r6 and van Steenberge.tT Periodic films were taken to assess bone height and quality. Loss of bone height around the implanis must be less than 2 mm for implant success. Each implant had to be immobile continuously when evaluated bimanually. Sixteen percent of the final prostheses were 158 Compend Contin Educ Dent, Vol. XV. No.2 Hex Internal Internal None External External External External No. Placed 't2 143 cemented and could not be removed for inspection of mobility of individual implants. Two of the implants in the study are listed as failures because of mobility. A treated ailing implant is also listed as failed (Table 3). All other implants in this study met the criteria for successful,loaded implants to the date this article was submitted for publication. Discussion The author has used the osteotome technique in the maxilla for the lasi 5 years with consistently excellent results. Both screw-shape and press-fit implants have been used. The instruments presented were not designed for any specific type of implant. However, the author's clinical experience indicates that press-fit implants are best suited to the osteotome technique. An attempt was made to include sites in this study that would be considered difficuit or high risk because of: 1. very soft and spongy bone; 2. spiny ridge segments of less than 4-mm buccopalatal width; 3. sites with less than 10 mm of preoperative bone height adjacent to or beneath the sinus. In all of these situations, the use of osteotomes appear superior to drilling. The author estimates that Table 2-Period of Studv Stage I surgery February 1990 to March 1992 Stage ll surgery September 1990 to September 1992 Months of Loading lmplant Length Number. 8mm 10 mm '13 mm 15/16 mm Location Anterior Premolar Molar Tuberosity Number of lmplants Number 32* u Average months of loading: I8 months Average age of patients: 59 years Number of patients in study: 55 '22j6 of implants in study 20Vo of the sites in this study could not have been adequately developed with routine drilling techniques. The reader should note that 99 of 743 implants in this study were 13 mm or longer. Aside from the tuberosity, where longer implants would be expected, to some degree, the implant length related to the surgeon's ability to alter the floor and boundarv of the sinus with osteotomes, which provided a deeper site. Drilling does not improve local anatomy or bone quality. Osteotomes allow a simple means to expand the ridge, deepen sites, create I t }? -j {
 Failed/infection 1 (removed) Failed/mobility (still in service) Z (treated/implants are firm)")
93 a Table 3-Success Rate AfterAverage Loading of 18 Months Failures No. Results lmplants lost between insertion and uncovering 0 Faile during abutment connection 1 (removed) Failed/infection 1 (removed) Failed/mobility (still in service) Z (treated/implants are firm) Failed/ailing (still in service) 1 (treated/good) Totalfailed 5* 'Total failures (5 of 143 implans) indicates a 9696 success rate for the osteotome technique in type lv bone with loaded implans at 18 months. more usable sites, and possibly improve bone quality. The osteotome technique is heatless and offers excelient tactile sensitivity, control, and visibility. Torque is nonexistent and access is as good, or better, than drills in the posterior maxilla. Conclusion The osteotome technique is a useful and predictable procedure for implant placement in soft maxillary bone. This technique improves the chances of placing implants throughout the maxilla, Visit us at the Chicago Midwinter Meeting for a demonstration, Booth # Compend Contin Educ Dent, Vol. XV, No.2 Clrde '13 on Reader Seruice Now in four new widths: 2 mm,3 mm, especially around the sinus and in the tuberosity, during a routine office procedure. The osteotome technique is gentle, does not generate heat, and takes advantage of available bone by relocating it in a variety of surgical applications. For many patients, the osteotome technique can help simplify implant surgery by reducing the need for more traumatic, timeconsuming, and costly procedures. Acknowledgment The author wishes to acknowledge the counsel of Drs. Leonard Abrams, Charles Berman, Richard Lazzara, and D. Walter Cohen in the development of this project. A special thank you is extended to professional artist Robin Pierce of Implant Innovations,Inc., who executed the illustrations contained in this artide. References 1. Brinemark P-L Zarb GA, Albrekcson T: Tissue-Integrated Prosthesis: OsseoinEgration in Clinical Dmtrsfry. Chicago, Quintessence, pp 17-77, , Adell R, Lekholm U, Rockler B, et at A 1S-year study of osseointegrated implants in the Fea&rmt of the edentulous jaw. Int I OraI Surg 10:387416,1987. laffin RA, Berrran CL: The e<cessive loss of Brdnemark fixtures in type [V bone: a Fyear analysis. I Pniodontol 6L24,1991. Babbish CA: Dental lmplants: Pinciples and Practice. Philadelphia, WB Saunders Co,1991. Misch C: Density of bone: effect on keatment plan, surgical approach, healing, and progressive bone loadhg.int I Oral Implantol 6:23-31, Bahat O: Treatnrent planning and place ment of implants h the posterior uraxillae: report of 732 consecutive Nobelpharma implants. Int I Oral Maxillofac Implants 2: , 193. Bahat O: Surgical planning for optimal aesthetic and functional resulb of osseointegrated implants in the partially edentulous mouth. I Calif Dent Assoc 20(65):31.46,1,992. Friberg B,JemtT, Lekholm U: Early failures of4&11 consecutively placed Brinemark dental implants: a study from stage I surgery to the connection of completed prosthesis. Int I Oral Maxillofac Implants 6: , q Kopp CD: Brdnemark osseointegration. Dmt Clin North Am 33(4lz ,, Balshi Tf: Preventing and resolving complications with osseointegrated im-
The International Journal of Periodontics & Restorative Dentistry
 The International Journal of Periodontics & Restorative Dentistry 3 Influence of the 3-D Bone-to-Implant Relationship on Esthetics Ueli Grunder, DMD* Stefano Gracis, DMD** Matteo Capelli, DMD** There are
The International Journal of Periodontics & Restorative Dentistry 3 Influence of the 3-D Bone-to-Implant Relationship on Esthetics Ueli Grunder, DMD* Stefano Gracis, DMD** Matteo Capelli, DMD** There are
Prosthetic Options in Implant Dentistry. Hakimeh Siadat, DDS, MSc Associate Professor
 Prosthetic Options in Dentistry Hakimeh Siadat, DDS, MSc Associate Professor Dental Research Center, Department of Prosthodontics & Dental s Faculty of Dentistry, Tehran University of Medical Sciences
Prosthetic Options in Dentistry Hakimeh Siadat, DDS, MSc Associate Professor Dental Research Center, Department of Prosthodontics & Dental s Faculty of Dentistry, Tehran University of Medical Sciences
Rehabilitating a Compromised Site for Restoring Form, Function and Esthetics- A Case Report
 Research & Reviews: Journal of Dental Sciences Rehabilitating a Compromised Site for Restoring Form, Function and Esthetics- A Case Report Priyanka Prakash* Division of Periodontology, Department of Dental
Research & Reviews: Journal of Dental Sciences Rehabilitating a Compromised Site for Restoring Form, Function and Esthetics- A Case Report Priyanka Prakash* Division of Periodontology, Department of Dental
Patients esthetic demands and
 Predictable Periimplant Gingival Esthetics: Use of the Natural Tooth as a Provisional following Implant Placement ROBERT C. MARGEAS, DDS* ABSTRACT Maintaining the interdental papilla and bone height following
Predictable Periimplant Gingival Esthetics: Use of the Natural Tooth as a Provisional following Implant Placement ROBERT C. MARGEAS, DDS* ABSTRACT Maintaining the interdental papilla and bone height following
The 2B-3D rule for implant planning, placement and restoration
 IJOI 27 INTERDISCIPLINARY TREATMENT The 2B-3D rule for implant planning, placement and restoration 1. What is biologic width? Is there a golden rule for implant planning, placement and restoration as the
IJOI 27 INTERDISCIPLINARY TREATMENT The 2B-3D rule for implant planning, placement and restoration 1. What is biologic width? Is there a golden rule for implant planning, placement and restoration as the
Controlling Tissue Contours with a Prosthetically Driven Approach to Implant Dentistry
 Controlling Tissue Contours with a Prosthetically Driven Approach to Implant Dentistry Go online for in-depth content by Timothy F. Kosinski, DDS, MAGD With continual improvements in the design and production
Controlling Tissue Contours with a Prosthetically Driven Approach to Implant Dentistry Go online for in-depth content by Timothy F. Kosinski, DDS, MAGD With continual improvements in the design and production
The majority of the early research concerning
 Gingival Recession Around Implants: A 1-Year Longitudinal Prospective Study Paula N. Small, DDS, MPH 1 /Dennis P. Tarnow, DDS 2 A longitudinal study was performed, which measured the soft tissue around
Gingival Recession Around Implants: A 1-Year Longitudinal Prospective Study Paula N. Small, DDS, MPH 1 /Dennis P. Tarnow, DDS 2 A longitudinal study was performed, which measured the soft tissue around
Dental Implant Placement in the Maxillary Anterior Region: Guidelines for Aesthetic Success Michael Tischler, DDS
 Page 1 of 10 Issue Date: March 2005, Posted On: 5/2/2005 Dental Implant Placement in the Maxillary Anterior Region: Guidelines for Aesthetic Success Michael Tischler, DDS Figure 1. A 43-year-old female
Page 1 of 10 Issue Date: March 2005, Posted On: 5/2/2005 Dental Implant Placement in the Maxillary Anterior Region: Guidelines for Aesthetic Success Michael Tischler, DDS Figure 1. A 43-year-old female
Immediate Implant Placement:
 Immediate Implant Placement: Parameters Influencing Tissue Remodeling Bernard Touati, DDS and Mario Groisman, DDS In esthetic implant therapy, the patient s objective is to obtain an imperceptible, natural-looking
Immediate Implant Placement: Parameters Influencing Tissue Remodeling Bernard Touati, DDS and Mario Groisman, DDS In esthetic implant therapy, the patient s objective is to obtain an imperceptible, natural-looking
Osseointegrated dental implant treatment generally
 Placement of Dental Implants Without Flap Surgery: A Clinical Report Bader H. Al-Ansari, BDS, MScD*/Robert R. Morris, DMD** Traditionally, the procedure of implant placement requires a surgical periosteal
Placement of Dental Implants Without Flap Surgery: A Clinical Report Bader H. Al-Ansari, BDS, MScD*/Robert R. Morris, DMD** Traditionally, the procedure of implant placement requires a surgical periosteal
Immediate implant placement in the Title central incisor region: a case repo. Journal Journal of prosthodontic research,
 Immediate implant placement in the Title central incisor region: a case repo Author(s) Sekine, H; Taguchi, T; Yamagami, M; Alternative Takanashi, T; Furuya, K Journal Journal of prosthodontic research,
Immediate implant placement in the Title central incisor region: a case repo Author(s) Sekine, H; Taguchi, T; Yamagami, M; Alternative Takanashi, T; Furuya, K Journal Journal of prosthodontic research,
MANAGEMENT OF ATROPHIC ANTERIOR MAXILLA USING RIDGE SPLIT TECHNIQUE, IMMEDIATE IMPLANTATION AND TEMPORIZATION
 Case Report International Journal of Dental and Health Sciences Volume 02, Issue 06 MANAGEMENT OF ATROPHIC ANTERIOR MAXILLA USING RIDGE SPLIT TECHNIQUE, IMMEDIATE IMPLANTATION AND TEMPORIZATION Rakshith
Case Report International Journal of Dental and Health Sciences Volume 02, Issue 06 MANAGEMENT OF ATROPHIC ANTERIOR MAXILLA USING RIDGE SPLIT TECHNIQUE, IMMEDIATE IMPLANTATION AND TEMPORIZATION Rakshith
Dental Implants and Esthetics
 Continuing Education Brought to you by Dental Implants and Esthetics Course Author(s): Charles J. Goodacre, DDS, MSD; Chad J. Anderson, MS, DMD CE Credits: 1 hour Intended Audience: Dentists, Dental Hygienists,
Continuing Education Brought to you by Dental Implants and Esthetics Course Author(s): Charles J. Goodacre, DDS, MSD; Chad J. Anderson, MS, DMD CE Credits: 1 hour Intended Audience: Dentists, Dental Hygienists,
Dental Implant Treatment Planning and Restorative Considerations
 Dental Implant Treatment Planning and Restorative Considerations Aldo Leopardi, BDS, DDS, MS Practice Limited to Implant, Fixed and Removable Prosthodontics Greenwood Village, Colorado www.knowledgefactoryco.com
Dental Implant Treatment Planning and Restorative Considerations Aldo Leopardi, BDS, DDS, MS Practice Limited to Implant, Fixed and Removable Prosthodontics Greenwood Village, Colorado www.knowledgefactoryco.com
Creating emergence profiles in immediate implant dentistry
 Creating emergence profiles in immediate implant dentistry AUTHORS Dr. Daniel Capitán Maraver Dr. Manuel Fuentes Ortiz Visiting lecturers in the Master s Degree in Clinical Practice in Implantology and
Creating emergence profiles in immediate implant dentistry AUTHORS Dr. Daniel Capitán Maraver Dr. Manuel Fuentes Ortiz Visiting lecturers in the Master s Degree in Clinical Practice in Implantology and
Evaluation of peri-implant tissue response according to the presence of keratinized mucosa Abstract Purpose: Materials and methods Results:
 Evaluation of peri-implant tissue response according to the presence of keratinized mucosa Bum-Soo Kim 1, Young-Kyun Kim 1, Pil-Young Yun 1, Yang-Jin Lee 2, Hyo-Jeong Lee 3, Su-Gwan Kim 4 1Department of
Evaluation of peri-implant tissue response according to the presence of keratinized mucosa Bum-Soo Kim 1, Young-Kyun Kim 1, Pil-Young Yun 1, Yang-Jin Lee 2, Hyo-Jeong Lee 3, Su-Gwan Kim 4 1Department of
Inclusive Tooth Replacement System
 Optimizing Anterior Esthetics with the Inclusive Tooth Replacement System by Timothy F. Kosinski, DDS, MAGD Implant treatment has changed so much over the years. In the past it was acceptable to place
Optimizing Anterior Esthetics with the Inclusive Tooth Replacement System by Timothy F. Kosinski, DDS, MAGD Implant treatment has changed so much over the years. In the past it was acceptable to place
Case Report. RapidSorb Rapid Resorbable Fixation System. Ridge augmentation in a one-step surgical protocol.
 Case Report RapidSorb Rapid Resorbable Fixation System. Ridge augmentation in a one-step surgical protocol. RapidSorb Rapid Resorbable Fixation System. Ridge augmentation in a one-step surgical protocol.
Case Report RapidSorb Rapid Resorbable Fixation System. Ridge augmentation in a one-step surgical protocol. RapidSorb Rapid Resorbable Fixation System. Ridge augmentation in a one-step surgical protocol.
The patient gave a history of hypertension and gastritis for which was taking Lacidipine 4mg, Omeprazole 20mg and Simvastatin 40mg.
 A.S. was referred by her general dental practitioner for assessment for possible implant placement to restore the space where her bridge replacing her maxillary central incisors had recently failed. Fig
A.S. was referred by her general dental practitioner for assessment for possible implant placement to restore the space where her bridge replacing her maxillary central incisors had recently failed. Fig
Patient s Presenting Complaint V.C. presented with discomfort and mobility from the crowned maxillary left central incisor tooth. Fig 1.
 Patient s Presenting Complaint V.C. presented with discomfort and mobility from the crowned maxillary left central incisor tooth. Fig 1. A longitudinal root fracture was suspected and confirmed when the
Patient s Presenting Complaint V.C. presented with discomfort and mobility from the crowned maxillary left central incisor tooth. Fig 1. A longitudinal root fracture was suspected and confirmed when the
Surgical reconstruction of lost papilla around implant with a modified technique: A case report
 Journal of Periodontology & Implant Dentistry Case Report Surgical reconstruction of lost papilla around implant with a modified technique: A case report Mahdi Faraji* Andre Van Zyl University of Pretoria,
Journal of Periodontology & Implant Dentistry Case Report Surgical reconstruction of lost papilla around implant with a modified technique: A case report Mahdi Faraji* Andre Van Zyl University of Pretoria,
The following resources related to this article are available online at jada.ada.org ( this information is current as of July 11, 2011):
:") Implants or Pontics: Decision Making for Anterior Tooth Replacement Frank Spear J Am Dent Assoc 2009;140;1160-1166 The following resources related to this article are available online at jada.ada.org (
Implants or Pontics: Decision Making for Anterior Tooth Replacement Frank Spear J Am Dent Assoc 2009;140;1160-1166 The following resources related to this article are available online at jada.ada.org (
Smile Line Rehabilitation with Dental Implants. Agenda. Agenda. Smile line revitalization with implants Priest Prosthodontics, LLC 1
 Smile Line Rehabilitation with Dental Implants Board Certified Prosthodontist Hilton Head Island, SC Agenda Implant placement and esthetic potential Single immediate implant placement Soft tissue preservation
Smile Line Rehabilitation with Dental Implants Board Certified Prosthodontist Hilton Head Island, SC Agenda Implant placement and esthetic potential Single immediate implant placement Soft tissue preservation
Implant Site Development Part I
 REVIEW ARTICLE Implant Site Development Part I 1 Umang Nayar, 2 Shankar Iyer IJCID Implant Site Development Part I 1 Consultant, Dental Surgeon and Periodontist at Max Health Care, New Delhi, Professor
REVIEW ARTICLE Implant Site Development Part I 1 Umang Nayar, 2 Shankar Iyer IJCID Implant Site Development Part I 1 Consultant, Dental Surgeon and Periodontist at Max Health Care, New Delhi, Professor
MODIFIED SINGLE ROLL FLAP APPROACH FOR SIMULTANEOUS IMPLANT PLACEMENT AND GINGIVAL AUGMENTATION
 Journal of IMAB ISSN: 1312-773X https://www.journal-imab-bg.org https://doi.org/10.5272/jimab.2017233.1667 Journal of IMAB - Annual Proceeding (Scientific Papers). 2017 Jul-Sep;23(3): Case report MODIFIED
Journal of IMAB ISSN: 1312-773X https://www.journal-imab-bg.org https://doi.org/10.5272/jimab.2017233.1667 Journal of IMAB - Annual Proceeding (Scientific Papers). 2017 Jul-Sep;23(3): Case report MODIFIED
Planning for esthetics Part II: adjacent implant restorations
 C L I N I C A L Planning for esthetics Part II: adjacent implant restorations William C Martin, 1 Emma Lewis, 2 Dean Morton 3 1 DMD, MS, Associate Professor & Clinical Director, Center for Implant Dentistry,
C L I N I C A L Planning for esthetics Part II: adjacent implant restorations William C Martin, 1 Emma Lewis, 2 Dean Morton 3 1 DMD, MS, Associate Professor & Clinical Director, Center for Implant Dentistry,
Esthetic management of multiple missing anterior teeth A Case report
 IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-issn: 2279-0853, p-issn: 2279-0861. Volume 13, Issue 1 Ver. II (Jan. 2014), PP 97-101 Esthetic management of multiple missing anterior teeth A
IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-issn: 2279-0853, p-issn: 2279-0861. Volume 13, Issue 1 Ver. II (Jan. 2014), PP 97-101 Esthetic management of multiple missing anterior teeth A
Pouch Roll Technique for Implant Soft Tissue Augmentation: A Variation of the Modified Roll Technique
 e116 Pouch Roll Technique for Implant Soft Tissue Augmentation: A Variation of the Modified Roll Technique Sang-Hoon Park, DDS, MS* Hom-Lay Wang, DDS, MSD, PhD** This paper presents three cases of peri-implant
e116 Pouch Roll Technique for Implant Soft Tissue Augmentation: A Variation of the Modified Roll Technique Sang-Hoon Park, DDS, MS* Hom-Lay Wang, DDS, MSD, PhD** This paper presents three cases of peri-implant
Replacement of a congenitally missing lateral incisor in the maxillary anterior aesthetic zone using a narrow diameter implant: A case report
 C A S E R E P O R T Replacement of a congenitally missing lateral incisor in the maxillary anterior aesthetic zone using a narrow diameter implant: A case report Rhoodie Garrana 1 and Govindrau Mohangi
C A S E R E P O R T Replacement of a congenitally missing lateral incisor in the maxillary anterior aesthetic zone using a narrow diameter implant: A case report Rhoodie Garrana 1 and Govindrau Mohangi
Contemporary Implant Dentistry
 Contemporary Implant Dentistry C H A P T ER 1 4 O F C O N T E M P OR A R Y O R A L A N D M A X I L L OFA C IA L S U R G E RY B Y : D R A R A S H K H O J A S T EH Dental implant is suitable for: completely
Contemporary Implant Dentistry C H A P T ER 1 4 O F C O N T E M P OR A R Y O R A L A N D M A X I L L OFA C IA L S U R G E RY B Y : D R A R A S H K H O J A S T EH Dental implant is suitable for: completely
Extraction with Immediate Implant Placement and Ridge Preservation in the Posterior
 Extraction with Immediate Implant Placement and Ridge Preservation in the Posterior by Timothy F. Kosinski, DDS, MAGD The following case presentation illustrates the diagnosis, planning and treatment for
Extraction with Immediate Implant Placement and Ridge Preservation in the Posterior by Timothy F. Kosinski, DDS, MAGD The following case presentation illustrates the diagnosis, planning and treatment for
Significance of crown shape in the replacement of a central incisor with a single implantsupported
 PROSTHODONTICS Significance of crown shape in the replacement of a central incisor with a single implantsupported crown Luca Gobbato, DDS 1 /Gianluca Paniz, DDS 2 /Fabio Mazzocco, DDS 3 / Andrea Chierico,
PROSTHODONTICS Significance of crown shape in the replacement of a central incisor with a single implantsupported crown Luca Gobbato, DDS 1 /Gianluca Paniz, DDS 2 /Fabio Mazzocco, DDS 3 / Andrea Chierico,
Interproximal Papilla Levels Following Early Versus Delayed Placement of Single-Tooth Implants: A Controlled Clinical Trial
 Interproximal Papilla Levels Following Early Versus Delayed Placement of Single-Tooth Implants: A Controlled Clinical Trial Lars Schropp, DDS, PhD /Flemming Isidor, DDS, PhD, Dr Odont /Lambros Kostopoulos,
Interproximal Papilla Levels Following Early Versus Delayed Placement of Single-Tooth Implants: A Controlled Clinical Trial Lars Schropp, DDS, PhD /Flemming Isidor, DDS, PhD, Dr Odont /Lambros Kostopoulos,
Bone Reduction Surgical Guide for the Novum Implant Procedure: Technical Note
 Bone Reduction Surgical Guide for the Novum Implant Procedure: Technical Note Stephen M. Parel, DDS 1 /Steven L. Ruff, CDT 2 /R. Gilbert Triplett, DDS, PhD 3 /Sterling R. Schow, DMD 4 The Novum System
Bone Reduction Surgical Guide for the Novum Implant Procedure: Technical Note Stephen M. Parel, DDS 1 /Steven L. Ruff, CDT 2 /R. Gilbert Triplett, DDS, PhD 3 /Sterling R. Schow, DMD 4 The Novum System
by Paul S. Petrungaro, DDS, MS,
 Cr e a t i o n a n d Preservation o f Na t u ra l So f t Tissue Em e r g e n c e Profiles Ar o u n d Dental Implants in the Esthetic Zone by Paul S. Petrungaro, DDS, MS, FICD, FACD, DICOI Chicago, IL Lake
Cr e a t i o n a n d Preservation o f Na t u ra l So f t Tissue Em e r g e n c e Profiles Ar o u n d Dental Implants in the Esthetic Zone by Paul S. Petrungaro, DDS, MS, FICD, FACD, DICOI Chicago, IL Lake
Working together as a team, the periodontist
 The Team Approach to Esthetic Immediate Implant Placement Bobby L. Butler, DDS; and Greggory Kinzer, DDS Working together as a team, the periodontist and restorative dentist can provide an increased level
The Team Approach to Esthetic Immediate Implant Placement Bobby L. Butler, DDS; and Greggory Kinzer, DDS Working together as a team, the periodontist and restorative dentist can provide an increased level
Masking Buccal Plate Remodeling in the Esthetic Zone with Connective Tissue Grafts: Concepts and Techniques with Immediate Implants
 Peer-Reviewed and Indexed Annual Implant Issue Masking Buccal Plate Remodeling in the Esthetic Zone with Connective Tissue Grafts: Concepts and Techniques with Immediate Implants of Continuing Education
Peer-Reviewed and Indexed Annual Implant Issue Masking Buccal Plate Remodeling in the Esthetic Zone with Connective Tissue Grafts: Concepts and Techniques with Immediate Implants of Continuing Education
Then and Now. Implant Therapy:
 Implant Therapy: Then and Now by Timothy F. Kosinski, DDS, MAGD Implant dentistry has come a long way since blade and subperiostal implants were widely used. Improvements in implant design and site preparation
Implant Therapy: Then and Now by Timothy F. Kosinski, DDS, MAGD Implant dentistry has come a long way since blade and subperiostal implants were widely used. Improvements in implant design and site preparation
Several extraction socket classifications have been
 Case Report Type 3 ReceSSion DefeCTS Clinical Management of Type 3 Recession Defects With Immediate Implant and Provisional Restoration Therapy: A Case Report Dennis P. Tarnow, DDS; and Stephen J. Chu,
Case Report Type 3 ReceSSion DefeCTS Clinical Management of Type 3 Recession Defects With Immediate Implant and Provisional Restoration Therapy: A Case Report Dennis P. Tarnow, DDS; and Stephen J. Chu,
The refinement of adhesive technology and contemporary
 CONTINUING EDUCATION 3 4 THE INTERPROXIMAL HEIGHT OF BONE: A GUIDEPOST TO PREDICTABLE AESTHETIC STRATEGIES AND SOFT TISSUE CONTOURS IN ANTERIOR TOOTH REPLACEMENT Henry Salama, DMD* Maurice A. Salama, DMD
CONTINUING EDUCATION 3 4 THE INTERPROXIMAL HEIGHT OF BONE: A GUIDEPOST TO PREDICTABLE AESTHETIC STRATEGIES AND SOFT TISSUE CONTOURS IN ANTERIOR TOOTH REPLACEMENT Henry Salama, DMD* Maurice A. Salama, DMD
Periimplant Regeneration Fenestration
 Indication Sheet PIR Periimplant Regeneration Fenestration Treatment concept of Dr. Jean-Pierre Gardella (surgeon) and Dr. Christian Richelme (prosthodontist), Marseille, France > Filling of a peri-implant
Indication Sheet PIR Periimplant Regeneration Fenestration Treatment concept of Dr. Jean-Pierre Gardella (surgeon) and Dr. Christian Richelme (prosthodontist), Marseille, France > Filling of a peri-implant
The effect of peri-implant bone exposure on soft tissue healing and bone loss in two adjacent implants
 Research Article J Periodontal Implant Sci 2012;42:20-24 http://dx.doi.org/10.5051/jpis.2012.42.1.20 on soft tissue healing and bone loss in two adjacent implants Seung-Yun Shin 1, Seung-Boem Kye 1, Jongrak
Research Article J Periodontal Implant Sci 2012;42:20-24 http://dx.doi.org/10.5051/jpis.2012.42.1.20 on soft tissue healing and bone loss in two adjacent implants Seung-Yun Shin 1, Seung-Boem Kye 1, Jongrak
Restoration of Congenitally Missing Lateral Incisors with Single Stage Implants: An Interdisciplinary Approach
 10.5005/jp-journals-10012-1045 CASE REPORT Restoration of Congenitally Missing Lateral Incisors with Single Stage Implants: An Interdisciplinary Approach 1 Mitha M Shetty, 2 Akshai KR Shetty, 3 N Kalavathy,
10.5005/jp-journals-10012-1045 CASE REPORT Restoration of Congenitally Missing Lateral Incisors with Single Stage Implants: An Interdisciplinary Approach 1 Mitha M Shetty, 2 Akshai KR Shetty, 3 N Kalavathy,
Use of the natural tooth as a provisional after immediate implant placement
 Use of the natural tooth as a provisional after immediate implant placement By Robert Margeas, DDS Research on the preservation of the tissue architecture, reduction of surgical sequences and greater aesthetic
Use of the natural tooth as a provisional after immediate implant placement By Robert Margeas, DDS Research on the preservation of the tissue architecture, reduction of surgical sequences and greater aesthetic
REGENERATIONTIME. A Case Report by. Ridge Augmentation and Delayed Implant Placement on an Upper Lateral Incisor
 A Case Report by Dr. Daniele Cardaropoli Ridge Augmentation and Delayed Implant Placement on an Upper Lateral Incisor The Situation An adult female patient presented with an endodontic/prosthetic failure
A Case Report by Dr. Daniele Cardaropoli Ridge Augmentation and Delayed Implant Placement on an Upper Lateral Incisor The Situation An adult female patient presented with an endodontic/prosthetic failure
All Dentistry is Cosmetic Betsy Bakeman, DDS Arkansas State Dental Association
 All Dentistry is Cosmetic Betsy Bakeman, DDS Arkansas State Dental Association Patients have traditionally sought treatment when concerned with the way their teeth look, function or feel. Over the past
All Dentistry is Cosmetic Betsy Bakeman, DDS Arkansas State Dental Association Patients have traditionally sought treatment when concerned with the way their teeth look, function or feel. Over the past
Socket preservation in the daily practice: A clinical case report
 Clinical Socket preservation in the daily practice: A clinical case report Rabih Abi Nader 1 and Carine Tabarani 2 Abstract Soft tissue contour depends on the underlying bone anatomy. Following tooth extraction,
Clinical Socket preservation in the daily practice: A clinical case report Rabih Abi Nader 1 and Carine Tabarani 2 Abstract Soft tissue contour depends on the underlying bone anatomy. Following tooth extraction,
Practical Advanced Periodontal Surgery
 Practical Advanced Periodontal Surgery Serge Dibart Blackwell Munksgaard Chapter 8 Papillary Construction After Dental Implant Therapy Peyman Shahidi, DOS, MScD, Serge Dibart, DMD, and Yun Po Zhang, PhD,
Practical Advanced Periodontal Surgery Serge Dibart Blackwell Munksgaard Chapter 8 Papillary Construction After Dental Implant Therapy Peyman Shahidi, DOS, MScD, Serge Dibart, DMD, and Yun Po Zhang, PhD,
CASE REPORT. CBCT-Assisted Treatment of the Failing Long Span Bridge with Staged and Immediate Load Implant Restoration
 Computer Aided Implantology Academy Newsletter - Newsletter 20 - July 2009 CASE REPORT CBCT-Assisted Treatment of the Failing Long Span Bridge with Staged and Immediate Load Implant Restoration Case Report
Computer Aided Implantology Academy Newsletter - Newsletter 20 - July 2009 CASE REPORT CBCT-Assisted Treatment of the Failing Long Span Bridge with Staged and Immediate Load Implant Restoration Case Report
Bone Grafting and Immediate Implant Placement in the Anterior
 Bone Grafting and Immediate Implant Placement in the Anterior by Timothy F. Kosinski, DDS, MAGD Whether a consequence of periodontal disease, caries or trauma to the root, losing an anterior tooth is psychologically
Bone Grafting and Immediate Implant Placement in the Anterior by Timothy F. Kosinski, DDS, MAGD Whether a consequence of periodontal disease, caries or trauma to the root, losing an anterior tooth is psychologically
A retrospective study on separate single-tooth implant restorations to replace two or more consecutive. maxillary posterior teeth up to 6 years.
 Original Article A retrospective study on separate single-tooth implant restorations to replace two or more consecutive maxillary posterior teeth up to 6 years follow up Myat Nyan Department of Prosthodontics,
Original Article A retrospective study on separate single-tooth implant restorations to replace two or more consecutive maxillary posterior teeth up to 6 years follow up Myat Nyan Department of Prosthodontics,
Oral Rehabilitation with CAMLOG implants after loss of dentition due to an accident
 Case Report 13 2011 Oral Rehabilitation with CAMLOG implants after loss of dentition due to an accident Dr Hitoshi Minagawa Tokyo, Japan Prosthetics Dr Hitoshi Minagawa successfully completed his studies
Case Report 13 2011 Oral Rehabilitation with CAMLOG implants after loss of dentition due to an accident Dr Hitoshi Minagawa Tokyo, Japan Prosthetics Dr Hitoshi Minagawa successfully completed his studies
For many years, patients with
 Dr. Robert Lowe is one of the great teachers in dentistry. Recently, he received the Gordon J. Christensen Award from the Chicago Dental Society in recognition of his excellence in teaching. Some of my
Dr. Robert Lowe is one of the great teachers in dentistry. Recently, he received the Gordon J. Christensen Award from the Chicago Dental Society in recognition of his excellence in teaching. Some of my
Optimizing Lateral Incisor Function and Esthetics with the Hahn Tapered Implant System
 Optimizing Lateral Incisor Function and Esthetics with the Hahn Tapered Implant System by Timothy Kosinski, DDS, MAGD Maxillary lateral incisor agenesis (MLIA) is a condition in which at least one of the
Optimizing Lateral Incisor Function and Esthetics with the Hahn Tapered Implant System by Timothy Kosinski, DDS, MAGD Maxillary lateral incisor agenesis (MLIA) is a condition in which at least one of the
An Introduction to Dental Implants
 An Introduction to Dental Implants Aims: This article provides an introduction to dental implants, outlining the categories of dental implants, the phases involved in implant dentistry and assessing a
An Introduction to Dental Implants Aims: This article provides an introduction to dental implants, outlining the categories of dental implants, the phases involved in implant dentistry and assessing a
Periimplant Regeneration Fenestration
 Indication Sheet PIR-1 Periimplant Regeneration Fenestration Treatment concept of Dr. Jean-Pierre Gardella (surgeon) and Dr. Christian Richelme (prosthodontist), Marseille, France > Filling of a peri-implant
Indication Sheet PIR-1 Periimplant Regeneration Fenestration Treatment concept of Dr. Jean-Pierre Gardella (surgeon) and Dr. Christian Richelme (prosthodontist), Marseille, France > Filling of a peri-implant
Dr. Jyoti Bansal, Dr. Abhishek Bansal, Dr. Suresh D.K., Dr. Anish Manocha
 Case Report 1 2 3 4 Dr. Jyoti Bansal, Dr. Abhishek Bansal, Dr. Suresh D.K., Dr. Anish Manocha Bansal J, Bansal A, DK Suresh, Manocha A. Immediate loading of single stage implants with minimally invasive
Case Report 1 2 3 4 Dr. Jyoti Bansal, Dr. Abhishek Bansal, Dr. Suresh D.K., Dr. Anish Manocha Bansal J, Bansal A, DK Suresh, Manocha A. Immediate loading of single stage implants with minimally invasive
Case Study. Case # 1 Author: Dr. Suheil Boutros (USA) 2013 Zimmer Dental, Inc. All rights reserved. 6557, Rev. 03/13.
 2013 Zimmer Dental, Inc. All rights reserved. 6557, Rev. 03/13.") Placement of a Zimmer Trabecular Metal Dental Implant with Simultaneous Ridge Augmentation and Immediate Non-Functional Loading Following Tooth Extraction and Orthodontic Treatment for Implant Site Development
Placement of a Zimmer Trabecular Metal Dental Implant with Simultaneous Ridge Augmentation and Immediate Non-Functional Loading Following Tooth Extraction and Orthodontic Treatment for Implant Site Development
The International Journal of Periodontics & Restorative Dentistry
 The International Journal of Periodontics & Restorative Dentistry 313 Timing, Positioning, and Sequential Staging in Esthetic Implant Therapy: A Four-Dimensional Perspective Akiyoshi Funato, DDS* Maurice
The International Journal of Periodontics & Restorative Dentistry 313 Timing, Positioning, and Sequential Staging in Esthetic Implant Therapy: A Four-Dimensional Perspective Akiyoshi Funato, DDS* Maurice
Developing Keratinized Mucosa Around Nonsubmerged Dental Implants. Part I: The Use of Vascularized Flaps
 CLINICAL AND RESEARCH REPORTS Developing Keratinized Mucosa Around Nonsubmerged Dental Implants. Part I: The Use of Vascularized Flaps Jay R. Beagle Despite the continued debate regarding the need for
CLINICAL AND RESEARCH REPORTS Developing Keratinized Mucosa Around Nonsubmerged Dental Implants. Part I: The Use of Vascularized Flaps Jay R. Beagle Despite the continued debate regarding the need for
Immediate Loading with Flapless Implant Surgery for Rehabilitation of Single Bound Edentulous Space
 Case Report Immediate Loading with Flapless Implant Surgery for Rehabilitation of Single Bound Edentulous Space Nidhi Bhatia 1, Shweta Bali 2, Meenu Taneja Bhasin 3, Priyanka Aggarwal 4, Vaibhav Joshi
Case Report Immediate Loading with Flapless Implant Surgery for Rehabilitation of Single Bound Edentulous Space Nidhi Bhatia 1, Shweta Bali 2, Meenu Taneja Bhasin 3, Priyanka Aggarwal 4, Vaibhav Joshi
Since the introduction of osseointegrated dental implants
 CLINICAL Papilla Formation in Response to Computer-Assisted Implant Surgery and Immediate Restoration Paul A. Schnitman, DDS, MSD 1 * Chie Hayashi, DDS, PhD, MMSc 2 This retrospective analysis was undertaken
CLINICAL Papilla Formation in Response to Computer-Assisted Implant Surgery and Immediate Restoration Paul A. Schnitman, DDS, MSD 1 * Chie Hayashi, DDS, PhD, MMSc 2 This retrospective analysis was undertaken
Initially, implant dentistry was focused on
 CASE LETTER Correction of Esthetic Complications of a Malpositioned Implant: A Case Letter Sergio Alexandre Gehrke, PhD INTRODUCTION Initially, implant dentistry was focused on successful osseointegration
CASE LETTER Correction of Esthetic Complications of a Malpositioned Implant: A Case Letter Sergio Alexandre Gehrke, PhD INTRODUCTION Initially, implant dentistry was focused on successful osseointegration
Esthetic Crown Lengthening for Upper Anterior Teeth: Indications and Surgical Techniques
 I J Pre Clin Dent Res 2014;1(2):49-53 April-June All rights reserved International Journal of Preventive & Clinical Dental Research Esthetic Crown Lengthening for Upper Anterior Teeth: Indications and
I J Pre Clin Dent Res 2014;1(2):49-53 April-June All rights reserved International Journal of Preventive & Clinical Dental Research Esthetic Crown Lengthening for Upper Anterior Teeth: Indications and
Consensus Report Tissue augmentation and esthetics (Working Group 3)
") B. Klinge Thomas F. Flemmig Consensus Report Tissue augmentation and esthetics (Working Group 3) Members of working group: Matteo Chiapasco Jan-Eirik Ellingsen Ronald Jung Friedrich Neukam Isabella Rocchietta
B. Klinge Thomas F. Flemmig Consensus Report Tissue augmentation and esthetics (Working Group 3) Members of working group: Matteo Chiapasco Jan-Eirik Ellingsen Ronald Jung Friedrich Neukam Isabella Rocchietta
Restorative Dentistry and Papilla Reconstruction in Reduced Periodontium
 CLINICAL AND RESEARCH REPORT Restorative Dentistry and Papilla Reconstruction in Reduced Periodontium Robert Azzi, Daniel Etienne, Bernard Schweitz Restoring the loss of periodontal soft and hard tissues
CLINICAL AND RESEARCH REPORT Restorative Dentistry and Papilla Reconstruction in Reduced Periodontium Robert Azzi, Daniel Etienne, Bernard Schweitz Restoring the loss of periodontal soft and hard tissues
Labial and lingual/palatal bone thickness of maxillary and mandibular anteriors in human cadavers in Koreans
 Research Article J Periodontal Implant Sci 2011;41:60-66 doi: 10.5051/jpis.2011.41.2.60 Labial and lingual/palatal bone thickness of maxillary and mandibular anteriors in human cadavers in Koreans Ji Young
Research Article J Periodontal Implant Sci 2011;41:60-66 doi: 10.5051/jpis.2011.41.2.60 Labial and lingual/palatal bone thickness of maxillary and mandibular anteriors in human cadavers in Koreans Ji Young
Implant Esthetic Failure
 Kevin G. Murphy, DDS, MS Associate Professor of Periodontics Baltimore College of Dentistry University of Maryland Faculty, Pankey Foundation Key Biscayne, FL Private Practice, Baltimore, MD PROVISIONAL
Kevin G. Murphy, DDS, MS Associate Professor of Periodontics Baltimore College of Dentistry University of Maryland Faculty, Pankey Foundation Key Biscayne, FL Private Practice, Baltimore, MD PROVISIONAL
In the esthetic zone, osseointegration
 CASE REPORT A Method for Obtaining Peri-Implant Soft-Tissue Contours by Using Screw- Retained Provisional Restorations as Impression Copings: A Clinical Report Bi-Yuan Tsai, DDS, MS* In the esthetic zone,
CASE REPORT A Method for Obtaining Peri-Implant Soft-Tissue Contours by Using Screw- Retained Provisional Restorations as Impression Copings: A Clinical Report Bi-Yuan Tsai, DDS, MS* In the esthetic zone,
The surgical placement of dental implants has
 Flapless Implant Surgery: A 10-year Clinical Retrospective Analysis Luis Dominguez Campelo, DDS 1 /Jose R. Dominguez Camara, MD, DDS 2 Purpose: This article is a retrospective clinical analysis of implants
Flapless Implant Surgery: A 10-year Clinical Retrospective Analysis Luis Dominguez Campelo, DDS 1 /Jose R. Dominguez Camara, MD, DDS 2 Purpose: This article is a retrospective clinical analysis of implants
ABSTRACT INTRODUCTION /jp-journals
 Prathapan Parayaruthottam, Vincy Antony Case Report 10.5005/jp-journals-10012-1137 Replacement of Missing Maxillary Central Incisor with an Osseointegrated Implant-supported Prosthesis from an Orthodontic
Prathapan Parayaruthottam, Vincy Antony Case Report 10.5005/jp-journals-10012-1137 Replacement of Missing Maxillary Central Incisor with an Osseointegrated Implant-supported Prosthesis from an Orthodontic
Principles of Periodontal flap surgery. Dr.maryam khosravi
 Principles of Periodontal flap surgery Dr.maryam khosravi Goals of periodontal SURGICAL phase 1 - Controlling or eliminating periodontal disease. 2 Correcting anatomic conditions that may a. favor periodontal
Principles of Periodontal flap surgery Dr.maryam khosravi Goals of periodontal SURGICAL phase 1 - Controlling or eliminating periodontal disease. 2 Correcting anatomic conditions that may a. favor periodontal
Periodontal Disease. Radiology of Periodontal Disease. Periodontal Disease. The Role of Radiology in Assessment of Periodontal Disease
 Radiology of Periodontal Disease Steven R. Singer, DDS srs2@columbia.edu 212.305.5674 Periodontal Disease! Includes several disorders of the periodontium! Gingivitis! Marginal Periodontitis! Localized
Radiology of Periodontal Disease Steven R. Singer, DDS srs2@columbia.edu 212.305.5674 Periodontal Disease! Includes several disorders of the periodontium! Gingivitis! Marginal Periodontitis! Localized
Restorative Driven Implant Solutions Utilizing the Latest Technology
 Restorative Driven Implant Solutions Utilizing the Latest Technology Go online for in-depth content by Timothy F. Kosinski, DDS, MAGD As a general dentist who has placed nearly 7,000 dental implants, I
Restorative Driven Implant Solutions Utilizing the Latest Technology Go online for in-depth content by Timothy F. Kosinski, DDS, MAGD As a general dentist who has placed nearly 7,000 dental implants, I
Management of a complex case
 2 Soft- and hard-tissue reconstruction of a severely deficient site prior to implant placement: a case report Management of a complex case Younes Khosroshahy, DDS, MFDS RCS (Eng), Dip Imp Dent RCSEd, Blue
2 Soft- and hard-tissue reconstruction of a severely deficient site prior to implant placement: a case report Management of a complex case Younes Khosroshahy, DDS, MFDS RCS (Eng), Dip Imp Dent RCSEd, Blue
Rehabilitation of atrophic partially edentulous mandible using ridge split technique and implant supported removable prosthesis
 CASE REPORT Rehabilitation of atrophic partially edentulous mandible using ridge split technique and implant supported removable prosthesis Dr Ashish Yadav 1, Dr Aratee Gupta 2, Dr Archana Singh 3, 1,3-
CASE REPORT Rehabilitation of atrophic partially edentulous mandible using ridge split technique and implant supported removable prosthesis Dr Ashish Yadav 1, Dr Aratee Gupta 2, Dr Archana Singh 3, 1,3-
Benefits of CBCT in Implant Planning
 10.5005/jp-journals-10012-1032 CLINICAL SCIENCE 1 Gregori M Kurtzman, 2 Douglas F Dompkowski 1 Private General Practice in Silver Spring, Maryland, USA 2 Private Periodontal Practice in Bethesda, Maryland,
10.5005/jp-journals-10012-1032 CLINICAL SCIENCE 1 Gregori M Kurtzman, 2 Douglas F Dompkowski 1 Private General Practice in Silver Spring, Maryland, USA 2 Private Periodontal Practice in Bethesda, Maryland,
Osseointegrated implant-supported
 CLINICAL SCREWLESS FIXED DETACHABLE PARTIAL OVERDENTURE TREATMENT FOR ATROPHIC PARTIAL EDENTULISM OF THE ANTERIOR MAXILLA Dennis Flanagan, DDS This is a case report of the restoration of a partially edentulous
CLINICAL SCREWLESS FIXED DETACHABLE PARTIAL OVERDENTURE TREATMENT FOR ATROPHIC PARTIAL EDENTULISM OF THE ANTERIOR MAXILLA Dennis Flanagan, DDS This is a case report of the restoration of a partially edentulous
Advanced Probing Techniques
 Module 21 Advanced Probing Techniques MODULE OVERVIEW The clinical periodontal assessment is one of the most important functions performed by dental hygienists. This module begins with a review of the
Module 21 Advanced Probing Techniques MODULE OVERVIEW The clinical periodontal assessment is one of the most important functions performed by dental hygienists. This module begins with a review of the
Case Report Alveolar Ridge Augmentation using Subepithelial Connective Tissue Grafts: A Case report
 Alveolar Ridge Augmentation using Subepithelial Connective Tissue Grafts: A Case report Po-Yu Lai, DDS, MS School of Dentistry, National Yang-Ming University Shing-Wai Yip, DDS, MS, DScD Prosthodontics
Alveolar Ridge Augmentation using Subepithelial Connective Tissue Grafts: A Case report Po-Yu Lai, DDS, MS School of Dentistry, National Yang-Ming University Shing-Wai Yip, DDS, MS, DScD Prosthodontics
From planning to surgery: a totally digital working flow for Leone implants placement
 Dr. Giancarlo Romagnuolo Roma, Italy From planning to surgery: a totally digital working flow for Leone implants placement Keywords guided surgery, 3D implant planning, single missing tooth, delayed immediate
Dr. Giancarlo Romagnuolo Roma, Italy From planning to surgery: a totally digital working flow for Leone implants placement Keywords guided surgery, 3D implant planning, single missing tooth, delayed immediate
أ.م. هدى عباس عبد اهلل CROWN AND BRIDGE جامعة تكريت كلية. Lec. (2) طب االسنان
 طب االسنان") Lec. (2) CROWN AND BRIDGE أ.م. هدى عباس عبد اهلل Patient selection and examination A thorough diagnosis must first be made of the patient's dental condition, considering both hard and soft tissues. this
Lec. (2) CROWN AND BRIDGE أ.م. هدى عباس عبد اهلل Patient selection and examination A thorough diagnosis must first be made of the patient's dental condition, considering both hard and soft tissues. this
ijcrr Vol 04 issue 12 Category: Case Report Received on:22/04/12 Revised on:07/05/12 Accepted on:22/05/12
 SURGICAL RECONSTRUCTION OF INTERDENTAL PAPILLA USING AN INTERPOSED SUBEPITHELIAL CONNECTIVE TISSUE GRAFT: A CASE REPORT ijcrr Vol 04 issue 12 Category: Case Report Received on:22/04/12 Revised on:07/05/12
SURGICAL RECONSTRUCTION OF INTERDENTAL PAPILLA USING AN INTERPOSED SUBEPITHELIAL CONNECTIVE TISSUE GRAFT: A CASE REPORT ijcrr Vol 04 issue 12 Category: Case Report Received on:22/04/12 Revised on:07/05/12
(Images are at the end of article)
") Long term provisionalization during periodontal surgery and extraction site tissue grafting: A Case Review Michael Tischler, DDS Diplomate American Board Of Oral Implantology/Implant Dentistry (Images
Long term provisionalization during periodontal surgery and extraction site tissue grafting: A Case Review Michael Tischler, DDS Diplomate American Board Of Oral Implantology/Implant Dentistry (Images
The Use of Alpha-Bio Tec's Narrow NeO Implants with Cone Connection for Restoration of Limited Width Ridges
 Case Study 48 The Use of Alpha-Bio Tec's Narrow NeO Implants with Cone Connection for Restoration of Limited Width Ridges Dr. Amir Gazmawe DMD, Specialist in Prosthodontics, Israel Dr. Amir Gazmawe graduated
Case Study 48 The Use of Alpha-Bio Tec's Narrow NeO Implants with Cone Connection for Restoration of Limited Width Ridges Dr. Amir Gazmawe DMD, Specialist in Prosthodontics, Israel Dr. Amir Gazmawe graduated
INTRODUCTION. long-term results in the restoration of both totally and partially
 CLINICAL RESTORATION OF THE SOFT-TISSUE MARGIN IN SINGLE-TOOTH IMPLANT IN THE ANTERIOR MAXILLA Jamil Awad Shibli, DDS, MS, PhD Susana d Avila, DDS, MS KEY WORDS Dental implants Subepithelial connective
CLINICAL RESTORATION OF THE SOFT-TISSUE MARGIN IN SINGLE-TOOTH IMPLANT IN THE ANTERIOR MAXILLA Jamil Awad Shibli, DDS, MS, PhD Susana d Avila, DDS, MS KEY WORDS Dental implants Subepithelial connective
MINI System CASE REPORT. Name: Dr. Achraf Souayah Na<on: Tunisia
 MINI System SE REPORT Name: Dr. chraf Souayah Na
MINI System SE REPORT Name: Dr. chraf Souayah Na
Integrating Natural Hard and Soft Tissue
 ACCREDITATION ESSENTIALS Integrating Natural Hard and Soft Tissue An Implant-Supported Restoration in the Esthetic Zone Somkiat Aimplee, DDS, MSc The successful replacement of anterior teeth with implants
ACCREDITATION ESSENTIALS Integrating Natural Hard and Soft Tissue An Implant-Supported Restoration in the Esthetic Zone Somkiat Aimplee, DDS, MSc The successful replacement of anterior teeth with implants
EFFECTIVE DATE: 04/24/14 REVISED DATE: 04/23/15, 04/28/16, 06/22/17, 06/28/18 POLICY NUMBER: CATEGORY: Dental
 MEDICAL POLICY SUBJECT: DENTAL IMPLANTS PAGE: 1 OF: 5 If a product excludes coverage for a service, it is not covered, and medical policy criteria do not apply. If a commercial product (including an Essential
MEDICAL POLICY SUBJECT: DENTAL IMPLANTS PAGE: 1 OF: 5 If a product excludes coverage for a service, it is not covered, and medical policy criteria do not apply. If a commercial product (including an Essential
Implant Placement in Maxillary Anterior Region Along with Soft and Hard Tissue Grafting- A Case Report.
 IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-issn: 2279-0853, p-issn: 2279-0861.Volume 15, Issue 10 Ver. XII (October. 2016), PP 68-73 www.iosrjournals.org Implant Placement in Maxillary Anterior
IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-issn: 2279-0853, p-issn: 2279-0861.Volume 15, Issue 10 Ver. XII (October. 2016), PP 68-73 www.iosrjournals.org Implant Placement in Maxillary Anterior
Core build-up using post systems
 Core build-up using post systems Dr. Gergely Pataky Department of Conservative Dentistry What to speak about today General considerations Classification of post systems Dowel-core or fibre post? Biologic
Core build-up using post systems Dr. Gergely Pataky Department of Conservative Dentistry What to speak about today General considerations Classification of post systems Dowel-core or fibre post? Biologic
Thick vs. Thin Gingival Biotypes: A Key Determinant in Treatment Planning for Dental Implants
 r s Thick vs. Thin Gingival Biotypes: A Key Determinant in Treatment Planning for Dental Implants richard t. kao, dds, phd; mark c. fagan, ms, dds; and gregory j. conte, ms, dmd abstract During the treatment
r s Thick vs. Thin Gingival Biotypes: A Key Determinant in Treatment Planning for Dental Implants richard t. kao, dds, phd; mark c. fagan, ms, dds; and gregory j. conte, ms, dmd abstract During the treatment
The Brånemark osseointegration method, using titanium dental implants (fixtures)
") Early Failures in 4,641 Consecutively Placed Brånemark Dental Implants: A Study From Stage 1 Surgery to the Connection of Completed Prostheses Bertil Friberg, DDS/Torsten Jemt, DDS, PhD/Ulf Lekholm, DDS,
Early Failures in 4,641 Consecutively Placed Brånemark Dental Implants: A Study From Stage 1 Surgery to the Connection of Completed Prostheses Bertil Friberg, DDS/Torsten Jemt, DDS, PhD/Ulf Lekholm, DDS,
Alveolar ridge preservation techniques
 Alveolar ridge preservation techniques Semmelweis University, Department of Periodontology, Budapest Dr. Windisch Péter Head of Department of Periodontology Changes of the alveolar ridge dimensions after
Alveolar ridge preservation techniques Semmelweis University, Department of Periodontology, Budapest Dr. Windisch Péter Head of Department of Periodontology Changes of the alveolar ridge dimensions after
Areview of recent studies concerning molar. Single Molar Replacement with a Progressive Thread Design Implant System: A Retrospective Clinical Report
 Single Molar Replacement with a Progressive Thread Design Implant System: A Retrospective Clinical Report George E. Romanos, Dr med dent 1 /Georg H. Nentwig, Prof Dr med dent 2 Many clinical studies have
Single Molar Replacement with a Progressive Thread Design Implant System: A Retrospective Clinical Report George E. Romanos, Dr med dent 1 /Georg H. Nentwig, Prof Dr med dent 2 Many clinical studies have
Successful osseointegration of implants has been
 Therapeutic Management for Immediate Implant Placement in Sites with Periapical Deficiencies Where Coronal Bone Is Present: Technique and Case Report Cyril I. Evian, DMD 1 /Ahmed Al-Momani, BDS 2 /Edwin
Therapeutic Management for Immediate Implant Placement in Sites with Periapical Deficiencies Where Coronal Bone Is Present: Technique and Case Report Cyril I. Evian, DMD 1 /Ahmed Al-Momani, BDS 2 /Edwin
Course Objectives. HDA 2018 Dental Implant Complications. What are some common failures / problems we all encounter?
 HDA 2018 Dental Implant Complications 1 Course Objectives - Understand protocols for diagnosing and treatment planning to minimize complications - Recognize and manage intraoperative complications during
HDA 2018 Dental Implant Complications 1 Course Objectives - Understand protocols for diagnosing and treatment planning to minimize complications - Recognize and manage intraoperative complications during
Flapless, Immediate Implantation & Immediate Loading with Socket Preservation in the Esthetic Area Using the Alpha-Bio Tec's NeO Implants
 Flapless Surgery Case Study 48 Flapless, Immediate Implantation & Immediate Loading with Socket Preservation in the Esthetic Area Using the Alpha-Bio Tec's NeO Implants Dr. Gadi Schneider DMD, Specialist
Flapless Surgery Case Study 48 Flapless, Immediate Implantation & Immediate Loading with Socket Preservation in the Esthetic Area Using the Alpha-Bio Tec's NeO Implants Dr. Gadi Schneider DMD, Specialist
The International Journal of Periodontics & Restorative Dentistry
 The International Journal of Periodontics & Restorative Dentistry 335 Considerations of Implant Abutment and Crown Contour: Critical Contour and Subcritical Contour Huan Su, DDS* Oscar González-Martín,
The International Journal of Periodontics & Restorative Dentistry 335 Considerations of Implant Abutment and Crown Contour: Critical Contour and Subcritical Contour Huan Su, DDS* Oscar González-Martín,
COURSE CURRICULUM FOR AESTHETIC DENTISTRY
 COURSE CURRICULUM FOR AESTHETIC DENTISTRY Esthetic Dentistry is actually the fourth dimension in clinical dentistry. In addition to biologic, Physiologic, and mechanical factors, all of which must be understood
COURSE CURRICULUM FOR AESTHETIC DENTISTRY Esthetic Dentistry is actually the fourth dimension in clinical dentistry. In addition to biologic, Physiologic, and mechanical factors, all of which must be understood