Cutaneous Drug Reactions
|
|
|
- Dale Richardson
- 5 years ago
- Views:
Transcription

1 Cutaneous Drug Reactions Andrei Metelitsa, MD, FRCPC, FAAD Co-Director, Institute for Skin Advancement Clinical Associate Professor, Dermatology University of Calgary, Canada
2 Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any means graphic, electronic, or mechanical, including photocopying, recording, or information storage and retrieval systems without prior written permission of Sea Courses Inc. except where permitted by law. Sea Courses is not responsible for any speaker or participant s statements, materials, acts or omissions.
3 Faculty/Presenter Disclosure Faculty: Andrei Metelitsa Relationships with commercial interests: Speakers Bureau/Honoraria: none Consulting Fees: none 3
4 Disclosure of Commercial Support This program has received financial support from Galderma Canada Inc. in the form of an unrestricted educational grant Potential for conflict(s) of interest: Dr. Andrei Metelitsa has not received speaking honoraria from the companies 4
5 Learning Objectives Recognize common pattern of drug eruptions Exanthematous Urticarial Bullous Vasculitis SJS/TEN
6 Drug Reactions Occur in about 2-3% of hospitalized patients Of all adverse drug reactions, cutaneous and allergic reactions make up 14% Vary in severity (trivial to life threatening) Some are expected others are sporadic
7 Epidemiology Women > men Old age Immunosupression Number of Drugs Genetic Predisposition Primary drugs in hospitalized patients penicillins, sulfonamides, NSAIDS
8 Basics of Drug reactions Consider drugs (medications, OTC, herbals, etc ) as a potential cause of a skin reaction Most drug reactions are inflammatory, generalized, and symmetric (some exceptions like fixed drug eruption) Diagnosis: Apperance Timing Biopsy (Allergy testing is of very limited value not generally recommended) Always document drug reactions in the patient s chart with the medication and description of the reaction
9 Timing Immediate reactions < one hour of the last administered dose Example: urticaria, angioedema, anaphylaxis Delayed reactions > one hour, but usually > six hours and occasionally weeks to months after the start of administration Example: morbilliform eruptions, fixed drug eruption, SJS, TEN, vasculitis
10 Drug History Remember the seven I s : Instilled (eye drops, ear drops) Inhaled (steroids, beta adrenergic) Ingested (capsules, tablets, syrup) Inserted (suppositories) Injected (IM, IV) Incognito (herbs, non- traditional medicine, homeopathic, vitamins, over-the-counter) Intermittent (patients may not reveal medications they take on an intermittent basis unless specifically asked)
11 Drug timeline Start with the onset as day 0, and work backwards and forwards Coumadin > Day Morphine Pantoprazole Clindamycin Cephalexin Acetaminophen
12 Mechanism of Drug Reactions Type 1 IgE dependent drug reactions urticaria, angioedema, anaphylaxis Type 2 Cytotoxic drug-induced reactions pemphigus and petechiae Type 3 Immune complex Vasculitis, urticarial vasculitis Type 4 Delayed Hypersensivity most common exanthem, fixed and lichenoid drug Non-immune overdose, drug interactions Idiosyncratic DRESS, drug induced lupus


13 Exanthematous Drug Eruptions
14 Exanthematous Drug Eruptions Most common, type 4 hypersensivity reaction Morbilliform Usually develops 7-14 days after start of new medication Penicillins, sulfonamides, cephalosporins, anticonvulsants Begins on trunk and upper extremities -> confluent maculopapular rash Mucous membranes spared Pruritus and low grade fever
15 Exanthematous Drug Eruptions DDx Viral exanthem very similar, lack of eosinophilia (peds population more common) DRESS facial edema TEN/SJS mucous membranes, annular lesions Treatment is supportive Stop culprit drug Topical steroids for symptom relief Disappears within 2 weeks without any complications or sequelae

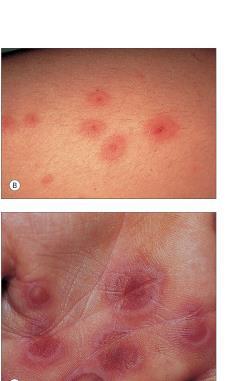
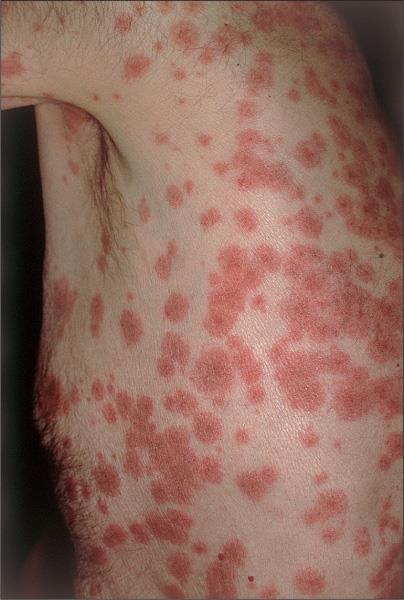
16 Drug-induced Urticaria Urticaria to penicillin (Bologna et. al Dermatology)
17 Drug-induced Urticaria Type 1 hypersensivity reaction by IgE antibodies Erythematous and edematous papules and plaques with pruritus Appear within minutes to days of drug administration Antibiotics (penicillins, cephalosporins) Duration of lesions less than 24 hrs Urticarial vasculitis more than 24 hrs Acute urticaria <6 weeks Angioedema subcutaneous swelling of the face (eyelids, lips, nose)
18 Drug-induced Urticaria Stop the culprit drug Consider antihistamines Newer agent bilastine 20 mg daily (Blexten in Canada)

19 Vasculitis
20 Drug-induced vasculitis Small vessel vasculitiis (type 3 reaction) Idiopathic, infections (hep C, staph), drugs Purpuric papules (non-blancheable), often legs Systemic symptoms: fever, myalgia, headache Presents within 7 to 21 days of drug administration Common drugs: NSAIDS (oral and topical), sulfonamides, cephalosporins,
21 Drug-induced vasculitis Stop culprit drug Topical steroids Systemic corticosteroids needed if significant systemic involvement Rule out Kidney and GI involvement


22 AGEP
23 AGEP Acute Generalized Exanthematous Pustulosis Acute, febrile eruptions with skin lesions numerous small sterile pustules, large erythema 90% are drug induced Antibiotics (penicillins, cephalosporins, calcium channel blockers, antimalarials) Lesions typically last for 1-2 weeks followed by superficial desquamation Withdraw culprit drug Topical steroids

24 DRESS Bologna et. al Dermatology
25 DRESS Drug reaction, eosinophilia, systemic symptoms Anticonvulsants (phenytoin, carbamazepine, phenobarbital) and sulfonamides Develops 2 to 6 weeks after the drug was started Edema of the face hallmark of DRESS Fever, exanthem, +/- arthralgia Prominent eosinophilia Most common organ involved liver (hepatitis) 10% mortality myocarditis, pneumonitis, nephritis, thyroiditis
26 DRESS Treatment Stop culprit drug Mild cases topical steroids More severe cases - systemic corticosteroids Slow taper over several weeks or even months

27 Fixed drug eruption
28 Fixed drug eruption (FDE) Peculiar and uncommon type of reaction where single or few skin lesions occur in same (fixed) sites with each administration of drug. They can be oval erythematous or dusky red plaques They can be widespread (generalized fixed drug eruption). There is strong predilection towards genital areas. NSAIDs, sulfa, acetaminophen, etc, are often involved. This is likely a localized type IV hypersensitivity

29 Fixed Drug Eruption

30 Bullous Pemphigoid
31 Bullous Pemphigoid Most common autoimmune subepidermal blistering disease Age over 60 years Intensely pruritic eruption Widespread blister formation Diuretics (furosemide), NSAIDS, antibioitcs, ACE in Intensely pruritic eruption with widespread blister formation Tense blisters, contain a clear fluid, and may persist for several days, leaving eroded and crusted areas

32 Bullous Pemphigoid
33 BP Treatment Ultrapotent Topical Steroids Systemic steroids very slow taper over 6 months! \ 0.5-1mg/kg Steroid sparing agents Methotrexate, azathioprine, cellcept

34
35

36
37 Erythema Multiforme A self-limited but potentially recurrent disease Abrupt onset of papular target lesions, with the vast majority of lesions appearing within 24 hours A preceding HSV infection is the most common precipitating factor; occasionally, there are other preceding infections (Mycoplasma) and drug exposure Erythema multiforme does not carry the risk of progressing to toxic epidermal necrolysis Habif TP. Clinical Dermatology Dorland s Online Dictionary; Lazar AJF, et al. In: Robbins and Cotran Pathologic Basis of Disease, Professional Edition
38 Erythema Multiforme subtypes Erythema multiforme minor: typical and/or atypical papular target lesions with LITTLE OR NO mucosal involvement and no systemic symptoms Erythema multiforme major: typical and/or occasionally atypical papular target lesions with SEVERE mucosal involvement and systemic features DermAtlas; Habif TP. Clinical Dermatology Dorland s Online Dictionary; Lazar AJF, et al. In: Robbins and Cotran Pathologic Basis of Disease, Professional Edition
39
40 Natural History Almost all of the lesions appearing within 24 hours and full development by 72 hours Pruritic or burning sensations within the lesions may be described Individual lesions remain fixed at the same site for 7 days or more DermAtlas; For most individuals with EM, the episode lasts 2 weeks and heals without sequelae Habif TP. Clinical Dermatology Dorland s Online Dictionary; Lazar AJF, et al. In: Robbins and Cotran Pathologic Basis of Disease, Professional Edition
41 DDx DermAtlas; Habif TP. Clinical Dermatology Dorland s Online Dictionary; Lazar AJF, et al. In: Robbins and Cotran Pathologic Basis of Disease, Professional Edition
42 Treatment Treat triggers if identified (e.g. HSV or M. pneumoniae) Oral antihistamines for 3 or 4 days may reduce the stinging and burning of the skin Topical corticosteroids In severe forms of EM with functional impairment, early therapy with systemic corticosteroids Recurrent EM - prophylaxis for at least 6 months with oral valacyclovir Habif TP. Clinical Dermatology Dorland s Online Dictionary; Lazar AJF, et al. In: Robbins and Cotran Pathologic Basis of Disease, Professional Edition
43 SJS/TEN Rare, potentially fatal drug reactions mucocutaneous tenderness and erythema as well as extensive exfoliation SJS is characterized by <10% body surface area of epidermal detachment and TEN by >30% The medications most frequently incriminated are nonsteroidal anti-inflammatory drugs, antibiotics and antiepileptics DermAtlas; TEN and SJS usually occur 7-21 days after initiation of the responsible drug Treatment: consider IVIG Habif TP. Clinical Dermatology Dorland s Online Dictionary; Lazar AJF, et al. In: Robbins and Cotran Pathologic Basis of Disease, Professional Edition

44

45 TEN DermAtlas; Habif TP. Clinical Dermatology Dorland s Online Dictionary; Lazar AJF, et al. In: Robbins and Cotran Pathologic Basis of Disease, Professional Edition

46 Phototoxic Reactions

47 Photosensitivity Phototoxic reactions Exaggerated sunburn, sun-exposed sites Photoallergic reactions Chronic Both sun-exposed and non-sun exposed
48 PEARLs Exanthematous reaction and urticaria are most common DRESS edema of the face, systemic features AGEP hundreds of sterile pustules FDE recurrent oval plaque, same site BP pruritic, tense blisters in elderly
Emergency Dermatology Dr Melissa Barkham
 Emergency Dermatology Dr Melissa Barkham Spotlight Seminar 30 th September 2010 Why is this important? Urgent recognition and treatment of dermatologic emergencies can be life saving and prevent long term
Emergency Dermatology Dr Melissa Barkham Spotlight Seminar 30 th September 2010 Why is this important? Urgent recognition and treatment of dermatologic emergencies can be life saving and prevent long term
Herbal and homeopathic products, often considered natural and non-toxic, can also cause adverse drug reactions.
 Idiosyncratic and potentially serious cutaneous adverse drug reactions (CADRs), although relatively rare, account for significant morbidity and mortality. RANNAKOE J LEHLOENYA, BSc, MB ChB, FCDerm (SA)
Idiosyncratic and potentially serious cutaneous adverse drug reactions (CADRs), although relatively rare, account for significant morbidity and mortality. RANNAKOE J LEHLOENYA, BSc, MB ChB, FCDerm (SA)
Drug Allergy A Guide to Diagnosis and Management
 Drug Allergy A Guide to Diagnosis and Management (Version 1 April 2015 updated April 2018) Author: Jed Hewitt Chief Pharmacist, Governance & Professional Practice Date of Preparation: April 2015 Updated:
Drug Allergy A Guide to Diagnosis and Management (Version 1 April 2015 updated April 2018) Author: Jed Hewitt Chief Pharmacist, Governance & Professional Practice Date of Preparation: April 2015 Updated:
Pediatric Dermatology
 Pediatric Dermatology --------- Emergencies & Urgencies Nicholas V. Nguyen, M.D. Director, Pediatric Dermatology Disclosures In the past 12 months, I have had the following financial relationships with
Pediatric Dermatology --------- Emergencies & Urgencies Nicholas V. Nguyen, M.D. Director, Pediatric Dermatology Disclosures In the past 12 months, I have had the following financial relationships with
Future of Pediatrics: Blisters, Hives and Other Tales from the Emergency Room June 14 th, 2016
 A. Yasmine Kirkorian MD Assistant Professor of Dermatology & Pediatrics Children s National Health System George Washington University School of Medicine & Health Sciences Future of Pediatrics: Blisters,
A. Yasmine Kirkorian MD Assistant Professor of Dermatology & Pediatrics Children s National Health System George Washington University School of Medicine & Health Sciences Future of Pediatrics: Blisters,
Allergic Emergencies and Anaphylaxis. George Porfiris MD, CCFP(EM),FCFP TEGH
,FCFP TEGH") Allergic Emergencies and Anaphylaxis George Porfiris MD, CCFP(EM),FCFP TEGH Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted
Allergic Emergencies and Anaphylaxis George Porfiris MD, CCFP(EM),FCFP TEGH Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted
DERMATOLOGIC EMERGENCIES. Mary Evers D.O., F.A.O.C.D. Georgetown, Texas
 DERMATOLOGIC EMERGENCIES Mary Evers D.O., F.A.O.C.D. Georgetown, Texas SKIN EMERGENCIES??? Subclassifications: Autoimmune (Anaphylaxis, Vasculitis, Pemphigus) Erythroderma (AGEP, DRESS, SJS, TEN) Infectious
DERMATOLOGIC EMERGENCIES Mary Evers D.O., F.A.O.C.D. Georgetown, Texas SKIN EMERGENCIES??? Subclassifications: Autoimmune (Anaphylaxis, Vasculitis, Pemphigus) Erythroderma (AGEP, DRESS, SJS, TEN) Infectious
They are updated regularly as new NICE guidance is published. To view the latest version of this NICE Pathway see:
 bring together everything NICE says on a topic in an interactive flowchart. are interactive and designed to be used online. They are updated regularly as new NICE guidance is published. To view the latest
bring together everything NICE says on a topic in an interactive flowchart. are interactive and designed to be used online. They are updated regularly as new NICE guidance is published. To view the latest
GOOD MORNING! AUGUST 5, 2014
 GOOD MORNING! AUGUST 5, 2014 PREP QUESTION During the health supervision visit of a term newborn boy, his mother relates that a cousins child died at age 4 months from sudden infant death syndrome. She
GOOD MORNING! AUGUST 5, 2014 PREP QUESTION During the health supervision visit of a term newborn boy, his mother relates that a cousins child died at age 4 months from sudden infant death syndrome. She
Cutaneous Adverse Drug Reactions in Domestic Animals. Katherine Doerr, DVM, Dip. ACVD. Veterinary Dermatology Center
 Cutaneous Adverse Drug Reactions in Domestic Animals Katherine Doerr, DVM, Dip. ACVD Veterinary Dermatology Center Maitland, Rockledge, Waterford Lakes, FL Not highly studied in veterinary medicine Unknown
Cutaneous Adverse Drug Reactions in Domestic Animals Katherine Doerr, DVM, Dip. ACVD Veterinary Dermatology Center Maitland, Rockledge, Waterford Lakes, FL Not highly studied in veterinary medicine Unknown
PedsCases Podcast Scripts
 PedsCases Podcast Scripts This is a text version of a podcast from Pedscases.com on Drug Allergy. These podcasts are designed to give medical students an overview of key topics in pediatrics. The audio
PedsCases Podcast Scripts This is a text version of a podcast from Pedscases.com on Drug Allergy. These podcasts are designed to give medical students an overview of key topics in pediatrics. The audio
Skin Manifestations of Drug Reactions
 Skin Manifestations of Drug Reactions Dr Carol Hlela, Division of Dermatology Department of Medicine, University of Cape Town and Red Cross Children s Hospital What are the Skin Manifestations of Drug
Skin Manifestations of Drug Reactions Dr Carol Hlela, Division of Dermatology Department of Medicine, University of Cape Town and Red Cross Children s Hospital What are the Skin Manifestations of Drug
Five things not to miss in Dermatology. Dr Judy Wismer Associate Clinical Professor Michael G DeGroote School of Medicine
 Five things not to miss in Dermatology Dr Judy Wismer Associate Clinical Professor Michael G DeGroote School of Medicine Key Descriptives Fever, skin pain Purpura, necrosis Bullae, Mucosal, Skin sloughing
Five things not to miss in Dermatology Dr Judy Wismer Associate Clinical Professor Michael G DeGroote School of Medicine Key Descriptives Fever, skin pain Purpura, necrosis Bullae, Mucosal, Skin sloughing
REGISTRY OF SEVERE CUTANEOUS ADVERSE REACTIONS TO DRUGS AND COLLECTION OF BIOLOGICAL SAMPLES. R e g i S C A R PATIENT'S DATA. Age country of birth
 REGISTRY OF SEVERE CUTANEOUS ADVERSE REACTIONS TO DRUGS AND COLLECTION OF BIOLOGICAL SAMPLES R e g i S C A R PATIENT'S DATA Initials of the patient date of birth Age country of birth Gender male female
REGISTRY OF SEVERE CUTANEOUS ADVERSE REACTIONS TO DRUGS AND COLLECTION OF BIOLOGICAL SAMPLES R e g i S C A R PATIENT'S DATA Initials of the patient date of birth Age country of birth Gender male female
Syndrome de Lyell Approche diagnostique. seminaires iris. Veronique del Marmol Alexandre Chamoun Service de Dermatologie Hôpital Erasme.
 Syndrome de Lyell Approche diagnostique Veronique del Marmol Alexandre Chamoun Service de Dermatologie Hôpital Erasme Serge Jennes Hôpital Militaire Rash benign Pustulose exanthematique Aigue et généralisée
Syndrome de Lyell Approche diagnostique Veronique del Marmol Alexandre Chamoun Service de Dermatologie Hôpital Erasme Serge Jennes Hôpital Militaire Rash benign Pustulose exanthematique Aigue et généralisée
Concentrate on Descriptors. An Approach to Skin Diseases in the ER
 Concentrate on Descriptors An Approach to Skin Diseases in the ER Toby Maurer, MD University of California, San Francisco Vasculitis-leaky blood vessels Targetoid lesions-round lesions with blue or red
Concentrate on Descriptors An Approach to Skin Diseases in the ER Toby Maurer, MD University of California, San Francisco Vasculitis-leaky blood vessels Targetoid lesions-round lesions with blue or red
Big rashes in little patients:
 ! Big rashes in little patients: Severe drug eruptions and cutaneous infections!! Marcia Hogeling, MD, FAAD Assistant Clinical Professor Director, Pediatric Dermatology Division of Dermatology David Geffen
! Big rashes in little patients: Severe drug eruptions and cutaneous infections!! Marcia Hogeling, MD, FAAD Assistant Clinical Professor Director, Pediatric Dermatology Division of Dermatology David Geffen
Emergency Dermatology. Emergency Dermatology
 Emergency Dermatology These are rapidly progressive skin conditions and some are potentially lifethreatening. Early recognition is important to implement prompt supportive care and therapy. Some are drug
Emergency Dermatology These are rapidly progressive skin conditions and some are potentially lifethreatening. Early recognition is important to implement prompt supportive care and therapy. Some are drug
An unpredictable, dose-independent adverse drug reaction which is immunologically or IgEmediated.
 R H E U M A T I S M D I S O R D E R S A N D A L L E R G I E S APPROACH TO DRUG ALLERGY Dr Bernard Thong DEFINITION OF DRUG ALLERGY An unpredictable, dose-independent adverse drug reaction which is immunologically
R H E U M A T I S M D I S O R D E R S A N D A L L E R G I E S APPROACH TO DRUG ALLERGY Dr Bernard Thong DEFINITION OF DRUG ALLERGY An unpredictable, dose-independent adverse drug reaction which is immunologically
AOU Ospedali Riuniti - Ancona
 AOU Ospedali Riuniti - Ancona Ospedale Materno-Infantile di Alta Specializzazione G. Salesi UOC Pediatria Allergia a farmaci e infezioni: tra coesistenza e casualità fabrizio franceschini Drug Hypersensitivity
AOU Ospedali Riuniti - Ancona Ospedale Materno-Infantile di Alta Specializzazione G. Salesi UOC Pediatria Allergia a farmaci e infezioni: tra coesistenza e casualità fabrizio franceschini Drug Hypersensitivity
Skin Manifestations of Systemic Disease. Approach to Dermatalogic Diagnosis 9/6/2016. Go Ahead---Judge a Book by its Cover!
 Go Ahead---Judge a Book by its Cover! Skin Manifestations of Systemic Disease Amelie Hollier, DNP, FNP-BC, FAANP Lafayette, LA President, APEA Objectives Compare diseases of the skin with reactions of
Go Ahead---Judge a Book by its Cover! Skin Manifestations of Systemic Disease Amelie Hollier, DNP, FNP-BC, FAANP Lafayette, LA President, APEA Objectives Compare diseases of the skin with reactions of
New product information wording Extracts from PRAC recommendations on signals
 20 July 2017 EMA/PRAC/406976/2017 Pharmacovigilance Risk Assessment Committee (PRAC) New product information wording Extracts from PRAC recommendations on signals Adopted at the 3-6 July 2017 PRAC The
20 July 2017 EMA/PRAC/406976/2017 Pharmacovigilance Risk Assessment Committee (PRAC) New product information wording Extracts from PRAC recommendations on signals Adopted at the 3-6 July 2017 PRAC The
DERMATOLOGICAL EMERGENCIES. DR. Ian Hoyle MBBS DIP IMC RCS (Ed), DA (UK),FRACGP,FACRRM,DIP DERM(Wales) TASMANIAN SKIN AND BODY CENTRE
, DA (UK),FRACGP,FACRRM,DIP DERM(Wales) TASMANIAN SKIN AND BODY CENTRE") DERMATOLOGICAL EMERGENCIES DR. Ian Hoyle MBBS DIP IMC RCS (Ed), DA (UK),FRACGP,FACRRM,DIP DERM(Wales) TASMANIAN SKIN AND BODY CENTRE Dermatological Emergencies INFECTIONS ERYTHRODERMA DRUG ERUPTIONS STEVENS-JOHNSON
DERMATOLOGICAL EMERGENCIES DR. Ian Hoyle MBBS DIP IMC RCS (Ed), DA (UK),FRACGP,FACRRM,DIP DERM(Wales) TASMANIAN SKIN AND BODY CENTRE Dermatological Emergencies INFECTIONS ERYTHRODERMA DRUG ERUPTIONS STEVENS-JOHNSON
Bugs and Drugs: What s New in Hypersensitivity Reactions?
 Bugs and Drugs: What s New in Hypersensitivity Reactions? Erin Mathes, MD Associate Professor of Dermatology and Pediatrics University of California, San Francisco DISCLOSURE OF RELATIONSHIPS WITH INDUSTRY
Bugs and Drugs: What s New in Hypersensitivity Reactions? Erin Mathes, MD Associate Professor of Dermatology and Pediatrics University of California, San Francisco DISCLOSURE OF RELATIONSHIPS WITH INDUSTRY
Andrei Metelitsa, MD, FRCPC, FAAD Co-Director, Institute for Skin Advancement Clinical Associate Professor, Dermatology University of Calgary, Canada
 Andrei Metelitsa, MD, FRCPC, FAAD Co-Director, Institute for Skin Advancement Clinical Associate Professor, Dermatology University of Calgary, Canada Copyright 2017 by Sea Courses Inc. All rights reserved.
Andrei Metelitsa, MD, FRCPC, FAAD Co-Director, Institute for Skin Advancement Clinical Associate Professor, Dermatology University of Calgary, Canada Copyright 2017 by Sea Courses Inc. All rights reserved.
Managing Penicillin Allergy
 Managing Penicillin Allergy Brian T. Kelly, MD MA April 12, 2019 Objectives Review penicillin allergy prevalence, morbidity, and management Describe the penicillin testing and oral challenge process Provide
Managing Penicillin Allergy Brian T. Kelly, MD MA April 12, 2019 Objectives Review penicillin allergy prevalence, morbidity, and management Describe the penicillin testing and oral challenge process Provide
A. Erythema multiforme and related diseases
 Go Back to the Top To Order, Visit the Purchasing Page for Details Chapter Erythema, Erythroderma (Exfoliative Dermatitis) Erythema is caused by telangiectasia or hyperemia in the papillary and reticular
Go Back to the Top To Order, Visit the Purchasing Page for Details Chapter Erythema, Erythroderma (Exfoliative Dermatitis) Erythema is caused by telangiectasia or hyperemia in the papillary and reticular
Personalized Medical Care:Recognition, Management, and Maybe Prevention of Cutaneous Hypersensitivity Reactions
 Personalized Medical Care:Recognition, Management, and Maybe Prevention of Cutaneous Hypersensitivity Reactions Bernard A. Cohen, M.D. Johns Hopkins Children s Center Baltimore, Maryland (NO disclosures)
Personalized Medical Care:Recognition, Management, and Maybe Prevention of Cutaneous Hypersensitivity Reactions Bernard A. Cohen, M.D. Johns Hopkins Children s Center Baltimore, Maryland (NO disclosures)
Dermergency! An Approach to Identification and Management of Life-Threatening Rashes
 Dermergency! An Approach to Identification and Management of Life-Threatening Rashes Gabby Anderson, PharmD PGY2 Emergency Medicine Pharmacy Resident anderson.gabrielle@mayo.edu Pharmacy Grand Rounds January
Dermergency! An Approach to Identification and Management of Life-Threatening Rashes Gabby Anderson, PharmD PGY2 Emergency Medicine Pharmacy Resident anderson.gabrielle@mayo.edu Pharmacy Grand Rounds January
Cutaneous drug reactions
 Maintenance of Certification clinical management series Series editor: James T. Li, MD, PhD Cutaneous drug reactions David A. Khan, MD Dallas, Tex INSTRUCTIONS Credit can now be obtained, free for a limited
Maintenance of Certification clinical management series Series editor: James T. Li, MD, PhD Cutaneous drug reactions David A. Khan, MD Dallas, Tex INSTRUCTIONS Credit can now be obtained, free for a limited
Dermatology Pearls for Inpatient Medicine. Dr Peter J Green MD FRCPC Professor, Division of Dermatology Dalhousie University
 Dermatology Pearls for Inpatient Medicine Dr Peter J Green MD FRCPC Professor, Division of Dermatology Dalhousie University Objectives 1. Review spectrum of cutaneous manifestations seen with inpatient
Dermatology Pearls for Inpatient Medicine Dr Peter J Green MD FRCPC Professor, Division of Dermatology Dalhousie University Objectives 1. Review spectrum of cutaneous manifestations seen with inpatient
Prevalence and pattern of adverse cutaneous drug reactions presenting to a tertiary care hospital
 International Journal of Research in Dermatology Janardhan B et al. Int J Res Dermatol. 2017 Mar;3(1):74-78 http://www.ijord.com Original Research Article DOI: http://dx.doi.org/10.18203/issn.2455-4529.intjresdermatol20164248
International Journal of Research in Dermatology Janardhan B et al. Int J Res Dermatol. 2017 Mar;3(1):74-78 http://www.ijord.com Original Research Article DOI: http://dx.doi.org/10.18203/issn.2455-4529.intjresdermatol20164248
Drug Allergy HSJ 19/09/2011
 Drug Allergy HSJ 19/09/2011 BSACI Guidelines Definitions Mechanisms Clinical Features Risk factors Diagnosis Investigations Criteria for referral/investigation Mirakian et al. Clin Exp All 2008 ; 39: 43-61
Drug Allergy HSJ 19/09/2011 BSACI Guidelines Definitions Mechanisms Clinical Features Risk factors Diagnosis Investigations Criteria for referral/investigation Mirakian et al. Clin Exp All 2008 ; 39: 43-61
9/9/17. Disclosures" Dermatology in Primary Care: Recognition and treatment of common disorders of the skin" A preview" Classic skin infections"
 Disclosures Dermatology in Primary Care: Recognition and treatment of common disorders of the skin I have no conflicts of interest to disclose. I may discuss off-label use of treatments for cutaneous disease.
Disclosures Dermatology in Primary Care: Recognition and treatment of common disorders of the skin I have no conflicts of interest to disclose. I may discuss off-label use of treatments for cutaneous disease.
Drug Allergy: A Rash ionale for Treatment
 Drug Allergy: A Rash ionale for Treatment Heather A. Powell, PharmD, BCPS Assistant Professor of Clinical Sciences Roosevelt University College of Pharmacy Jordan O. Powell, PharmD Clinical Pharmacist
Drug Allergy: A Rash ionale for Treatment Heather A. Powell, PharmD, BCPS Assistant Professor of Clinical Sciences Roosevelt University College of Pharmacy Jordan O. Powell, PharmD Clinical Pharmacist
CUTANEOUS DRUG REACTIONS OR I WOULDN T HAVE SEEN IT, IF I HADN T BELIEVED IT Edmund J. Rosser Jr., DVM, DACVD
 CUTANEOUS DRUG REACTIONS OR I WOULDN T HAVE SEEN IT, IF I HADN T BELIEVED IT Edmund J. Rosser Jr., DVM, DACVD DERMATOLOGY Pathogenesis Immunologic: can involve Type I, II, III, IV hypersensitivity reactions.
CUTANEOUS DRUG REACTIONS OR I WOULDN T HAVE SEEN IT, IF I HADN T BELIEVED IT Edmund J. Rosser Jr., DVM, DACVD DERMATOLOGY Pathogenesis Immunologic: can involve Type I, II, III, IV hypersensitivity reactions.
Dermatologic drug reactions
 Immunol Allergy Clin N Am 24 (2004) 399 423 Dermatologic drug reactions Jeffrey K. McKenna, MD, Kristin M. Leiferman, MD* Department of Dermatology, University of Utah, 30 North 1900 East, 4B454 School
Immunol Allergy Clin N Am 24 (2004) 399 423 Dermatologic drug reactions Jeffrey K. McKenna, MD, Kristin M. Leiferman, MD* Department of Dermatology, University of Utah, 30 North 1900 East, 4B454 School
Cutanous Manifestation of Lupus Erythematosus. Presented By: Dr. Naif S. Al Shahrani Salman Bin Abdaziz university
 Cutanous Manifestation of Lupus Erythematosus Presented By: Dr. Naif S. Al Shahrani Salman Bin Abdaziz university A 50-year old lady, who is otherwise healthy, presented to the dermatology clinic with
Cutanous Manifestation of Lupus Erythematosus Presented By: Dr. Naif S. Al Shahrani Salman Bin Abdaziz university A 50-year old lady, who is otherwise healthy, presented to the dermatology clinic with
An Evidenced-Based Approach to the Adult with a Morbilliform Eruption
 Relatively An Evidenced-Based Approach to the Adult with a Morbilliform Eruption Ben Kaffenberger, MD Assistant Professor, Dermatology Director, Inpatient Dermatology Consult Service Ohio State University
Relatively An Evidenced-Based Approach to the Adult with a Morbilliform Eruption Ben Kaffenberger, MD Assistant Professor, Dermatology Director, Inpatient Dermatology Consult Service Ohio State University
Goals of this talk. Morbilliform. Common Morphologies in the Hospital 11/7/2017. Hospital Based Dermatology: Common and Tough Consult Cases
 Hospital Based Dermatology: Common and Tough Consult Cases Lindy P. Fox MD Associate Professor of Clinical Dermatology Director, Hospital Consultation Service University of California, San Francisco lindy.fox@ucsf.edu
Hospital Based Dermatology: Common and Tough Consult Cases Lindy P. Fox MD Associate Professor of Clinical Dermatology Director, Hospital Consultation Service University of California, San Francisco lindy.fox@ucsf.edu
What's New in Oncodermatopathology: Immunotherapy Reactions
 What's New in Oncodermatopathology: Immunotherapy Reactions Emily Y. Chu, M.D., Ph.D. Assistant Professor of Dermatology & Pathology and Laboratory Medicine Hospital of the University of Pennsylvania March
What's New in Oncodermatopathology: Immunotherapy Reactions Emily Y. Chu, M.D., Ph.D. Assistant Professor of Dermatology & Pathology and Laboratory Medicine Hospital of the University of Pennsylvania March
Adverse Cutaneous Drug Reactions to Cardiovascular Drugs
 Adverse Cutaneous Drug Reactions to Cardiovascular Drugs Esen Özkaya Kurtuluş Didem Yazganoğlu 123 Adverse Cutaneous Drug Reactions to Cardiovascular Drugs Esen Özkaya Kurtuluş Didem Yazganoğlu Adverse
Adverse Cutaneous Drug Reactions to Cardiovascular Drugs Esen Özkaya Kurtuluş Didem Yazganoğlu 123 Adverse Cutaneous Drug Reactions to Cardiovascular Drugs Esen Özkaya Kurtuluş Didem Yazganoğlu Adverse
To update the use of IVIG and CORTICOIDS IN management of SJS/ TEN To remind Doctors being careful when giving
 Present : Dr Pham Thi Minh Rang Internal Department No2-Hospital for children No2 AIMS To update the use of IVIG and CORTICOIDS IN management of SJS/ TEN To remind Doctors being careful when giving To
Present : Dr Pham Thi Minh Rang Internal Department No2-Hospital for children No2 AIMS To update the use of IVIG and CORTICOIDS IN management of SJS/ TEN To remind Doctors being careful when giving To
New product information wording Extracts from PRAC recommendations on signals
 12 October 2017 EMA/PRAC/610988/2017 Pharmacovigilance Risk Assessment Committee (PRAC) New product information wording Extracts from PRAC recommendations on signals Adopted at the 25-29 September 2017
12 October 2017 EMA/PRAC/610988/2017 Pharmacovigilance Risk Assessment Committee (PRAC) New product information wording Extracts from PRAC recommendations on signals Adopted at the 25-29 September 2017
Discoid Lupus Erythematosus. DLE Treatment. Tacrolimus (Protopic ) DLE Treatment. Uses for Tacrolimus (Protopic ) 9/7/2016
 DLE Treatment. Uses for Tacrolimus (Protopic ) 9/7/2016") Common Immune mediated Dermatoses William H. Miller, Jr VMD Professor of Dermatology College of Veterinary Medicine Cornell University Ithaca, NY 14853 Discoid Lupus Erythematosus Most common autoimmune
Common Immune mediated Dermatoses William H. Miller, Jr VMD Professor of Dermatology College of Veterinary Medicine Cornell University Ithaca, NY 14853 Discoid Lupus Erythematosus Most common autoimmune
SKIN REACTIONS WITH PSYCHOTROPICS: A SYSTEMATIC REVIEW
 SKIN REACTIONS WITH PSYCHOTROPICS: A SYSTEMATIC REVIEW *Anderson Isaac, PharmD Candidate, 2019 Pooja Patel, PharmD Candidate, 2019 Katelyn Thomasson, PharmD Candidate, 2019 Erika Tillery, PharmD, BCPP,
SKIN REACTIONS WITH PSYCHOTROPICS: A SYSTEMATIC REVIEW *Anderson Isaac, PharmD Candidate, 2019 Pooja Patel, PharmD Candidate, 2019 Katelyn Thomasson, PharmD Candidate, 2019 Erika Tillery, PharmD, BCPP,
=ﻰﻤاﻤﺤﻠا ﺔﻴﻘﻠﺤﻠا ﺔذﺒاﻨﻠا
 1 / 15 Erythema Annulare Centrifugum and Other Figurate Erythemas The figurate erythemas include a variety of eruptions characterized by annular and polycyclic lesions. Classification of this group has
1 / 15 Erythema Annulare Centrifugum and Other Figurate Erythemas The figurate erythemas include a variety of eruptions characterized by annular and polycyclic lesions. Classification of this group has
Department of Dermatology, Christian Medical College and Hospital, Ludhiana, Punjab, India.
 Bullous pemphigoid mimicking granulomatous inflammation Abhilasha Williams, Emy Abi Thomas. Department of Dermatology, Christian Medical College and Hospital, Ludhiana, Punjab, India. Egyptian Dermatology
Bullous pemphigoid mimicking granulomatous inflammation Abhilasha Williams, Emy Abi Thomas. Department of Dermatology, Christian Medical College and Hospital, Ludhiana, Punjab, India. Egyptian Dermatology
Learning Objectives. History 8/1/2016. An Approach to Pediatric Rashes
 An Approach to Pediatric Rashes Neethi Patel, D.O. Learning Objectives 1.To identify common features of rashes seen in the pediatric population as well as pathognomonic features of certain pathologies
An Approach to Pediatric Rashes Neethi Patel, D.O. Learning Objectives 1.To identify common features of rashes seen in the pediatric population as well as pathognomonic features of certain pathologies
Cutaneous Reactions to Drugs in Children
 REVIEW ARTICLE Cutaneous Reactions to Drugs in Children Alissa R. Segal, PharmD, PhC a, Kevin M. Doherty, PharmD b, John Leggott, MD c, Barrett Zlotoff, MD d a Department of Pharmacy Practice, Massachusetts
REVIEW ARTICLE Cutaneous Reactions to Drugs in Children Alissa R. Segal, PharmD, PhC a, Kevin M. Doherty, PharmD b, John Leggott, MD c, Barrett Zlotoff, MD d a Department of Pharmacy Practice, Massachusetts
Endocarditis. By : Mehrnoush. dianatkhah
 Endocarditis By : Mehrnoush. dianatkhah Case 5.31, 31 years old woman CC : Fever, dyspnea, 3 days postpartum PMH : Mitral prolapse Fever 38.5 WBC : 8900 ESR : 84 CRP : 10.4 Cr : 0.6 NT Pro BNP: 5469 Physical
Endocarditis By : Mehrnoush. dianatkhah Case 5.31, 31 years old woman CC : Fever, dyspnea, 3 days postpartum PMH : Mitral prolapse Fever 38.5 WBC : 8900 ESR : 84 CRP : 10.4 Cr : 0.6 NT Pro BNP: 5469 Physical
The mechanisms of common drug hypersensitivities and implications for testing
 The mechanisms of common drug hypersensitivities and implications for testing R J Heddle 17 May 2016 Adverse Drug Reactions (ADR) Type A 85-90% of ADR Any individual, given sufficient dose & exposure Predictable
The mechanisms of common drug hypersensitivities and implications for testing R J Heddle 17 May 2016 Adverse Drug Reactions (ADR) Type A 85-90% of ADR Any individual, given sufficient dose & exposure Predictable
PACKAGE LEAFLET: INFORMATION FOR THE USER
 PACKAGE LEAFLET: INFORMATION FOR THE USER Fucidin 250 mg Tablets sodium fusidate Read all of this leaflet carefully before you start taking this medicine because it contains important information for you.
PACKAGE LEAFLET: INFORMATION FOR THE USER Fucidin 250 mg Tablets sodium fusidate Read all of this leaflet carefully before you start taking this medicine because it contains important information for you.
Disclaimer. This is a broad survey and cannot cover all differential diagnoses or each condition in thorough detail
 Objectives Pediatric Infections: Differentiating Benign from Serious Eileen Klein, MD, MPH Rashes Infectious vs non-infectious Viral vs bacterial Respiratory and GI illnesses When do you treat When do
Objectives Pediatric Infections: Differentiating Benign from Serious Eileen Klein, MD, MPH Rashes Infectious vs non-infectious Viral vs bacterial Respiratory and GI illnesses When do you treat When do
Cases of Non-Infectious Vulvovaginitis
 Cases of Non-Infectious Vulvovaginitis 2 nd PANHELLANIC CONGRESS on Lower Genital Tract Disorders December 14-16 Grand Hyatt Athens Lynette J. Margesson MD FRCPC Assistant Professor of Obstetrics & Gynecology
Cases of Non-Infectious Vulvovaginitis 2 nd PANHELLANIC CONGRESS on Lower Genital Tract Disorders December 14-16 Grand Hyatt Athens Lynette J. Margesson MD FRCPC Assistant Professor of Obstetrics & Gynecology
A Case Report on Amoxicillin Induced Stevens- Johnson Syndrome
 Open Journal of Clinical & Medical Case Reports Volume 2 (2016) Issue 11 A Case Report on Amoxicillin Induced Stevens- Johnson Syndrome Rajendra Singh Airee*; Aastha Rawal; Binu Mathew; H. Doddayya Abstract
Open Journal of Clinical & Medical Case Reports Volume 2 (2016) Issue 11 A Case Report on Amoxicillin Induced Stevens- Johnson Syndrome Rajendra Singh Airee*; Aastha Rawal; Binu Mathew; H. Doddayya Abstract
VI.2 Elements for a public summary. VI.2.1 Overview of disease epidemiology
 VI.2 Elements for a public summary VI.2.1 Overview of disease epidemiology Sinus infection (Acute bacterial sinusitis) Sinus infection (upper respiratory infection) is short-lived infection of the sinuses,
VI.2 Elements for a public summary VI.2.1 Overview of disease epidemiology Sinus infection (Acute bacterial sinusitis) Sinus infection (upper respiratory infection) is short-lived infection of the sinuses,
NEOFEN 60 mg suppository
 PACKAGE LEAFLET: INFORMATION FOR THE USER NEOFEN 60 mg suppository IBUPROFEN This leaflet is a copy of the Summary of Product Characteristics and Patient Information Leaflet for a medicine, which outlines
PACKAGE LEAFLET: INFORMATION FOR THE USER NEOFEN 60 mg suppository IBUPROFEN This leaflet is a copy of the Summary of Product Characteristics and Patient Information Leaflet for a medicine, which outlines
Bacterial Infections in Pediatric Dermatology. Patrick McMahon, MD Children s Hospital of Philadelphia
 Bacterial Infections in Pediatric Dermatology Patrick McMahon, MD Children s Hospital of Philadelphia Fill In The Blank When you see on the skin, you think of a bacterial skin infection SEND SWABS VIRAL
Bacterial Infections in Pediatric Dermatology Patrick McMahon, MD Children s Hospital of Philadelphia Fill In The Blank When you see on the skin, you think of a bacterial skin infection SEND SWABS VIRAL
If a drug trigger is suspected, stop the offending drug as this may reduce the risk of relapse.
 There is so much we don't know in medicine that could make a difference, and often we focus on the big things, and the little things get forgotten. To highlight some smaller but important issues, we've
There is so much we don't know in medicine that could make a difference, and often we focus on the big things, and the little things get forgotten. To highlight some smaller but important issues, we've
Rashes Not To Be Missed In Children
 May 2016 Rashes Not To Be Missed In Children Dr Chan Yuin Chew Dermatologist Dermatology Associates Gleneagles Medical Centre Scope of presentation Focus on rashes May lead to significant morbidity if
May 2016 Rashes Not To Be Missed In Children Dr Chan Yuin Chew Dermatologist Dermatology Associates Gleneagles Medical Centre Scope of presentation Focus on rashes May lead to significant morbidity if
An Approach to Common and not so Common Rashes in the Office FMF 2014 Christie Freeman MD, CCFP, DipPDerm, MSc
 An Approach to Common and not so Common Rashes in the Office FMF 2014 Christie Freeman MD, CCFP, DipPDerm, MSc 1 Common Rashes Tinea Corporis: Annular- this is not the only criteria Advancing erythematous
An Approach to Common and not so Common Rashes in the Office FMF 2014 Christie Freeman MD, CCFP, DipPDerm, MSc 1 Common Rashes Tinea Corporis: Annular- this is not the only criteria Advancing erythematous
Adverse Drug Reactions (ADRs) Outline
 Outline") Adverse Drug Reactions (ADRs) Outline 1. What are Adverse Drug Reactions (ADRs)? WHAT WHY HOW 2. How important are ADRs and are they preventable? 3. What are the classifications and mechanisms of ADRs?
Adverse Drug Reactions (ADRs) Outline 1. What are Adverse Drug Reactions (ADRs)? WHAT WHY HOW 2. How important are ADRs and are they preventable? 3. What are the classifications and mechanisms of ADRs?
Mark A. Bechtel, MD Clinical Associate Professor Division Director, Dermatology Ohio State University Medical Center
 Dermatologic Emergencies Mark A. Bechtel, MD Clinical Associate Professor Division Director, Dermatology Ohio State University Medical Center Clinical Features of SJS/TEN Initial symptoms Fever, stinging
Dermatologic Emergencies Mark A. Bechtel, MD Clinical Associate Professor Division Director, Dermatology Ohio State University Medical Center Clinical Features of SJS/TEN Initial symptoms Fever, stinging
Objectives 8/30/2012. How Do I Deal with a Person s Multiple (and Single) Drug Allergies? Adverse Drug Reactions
 Drug Allergies? Adverse Drug Reactions") How Do I Deal with a Person s Multiple (and Single) Drug Allergies? Faoud Ishmael, MD, PhD Assistant Professor of Medicine Section of Allergy and Immunology Penn State College of Medicine I have no conflicts
How Do I Deal with a Person s Multiple (and Single) Drug Allergies? Faoud Ishmael, MD, PhD Assistant Professor of Medicine Section of Allergy and Immunology Penn State College of Medicine I have no conflicts
8/8/2016. Overview. Back to Basics: Immunology. Adverse Reactions to Drugs: Dispelling Myths
 Adverse Reactions to Drugs: Dispelling Myths Allison Ramsey, MD NPA Annual Conference September 30, 2016 Overview Review of types of hypersensitivity reactions Penicillin allergy IV contrast allergy Local
Adverse Reactions to Drugs: Dispelling Myths Allison Ramsey, MD NPA Annual Conference September 30, 2016 Overview Review of types of hypersensitivity reactions Penicillin allergy IV contrast allergy Local
Egyptian Dermatology Online Journal Vol. 6 No 1: 14, June 2010
 Wells Syndrome H. Gammaz, H. Amer, A. Adly and S. Mahmoud Egyptian Dermatology Online Journal 6 (1): 14 Al-Haud Al-Marsoud Hospital, Cairo, Egypt e-mail: hananderma@hotmail.com Submitted: April 15, 2010
Wells Syndrome H. Gammaz, H. Amer, A. Adly and S. Mahmoud Egyptian Dermatology Online Journal 6 (1): 14 Al-Haud Al-Marsoud Hospital, Cairo, Egypt e-mail: hananderma@hotmail.com Submitted: April 15, 2010
Urticaria and Angioedema. Allergy and Immunology Awareness Program
 Urticaria and Angioedema Allergy and Immunology Awareness Program 1 Urticaria and Angioedema Allergy and Immunology Awareness Program Urticaria Commonly known as hives, urticarial is an itchy rash with
Urticaria and Angioedema Allergy and Immunology Awareness Program 1 Urticaria and Angioedema Allergy and Immunology Awareness Program Urticaria Commonly known as hives, urticarial is an itchy rash with
Package leaflet: Information for the user
 Package leaflet: Information for the user Dalacin C 150mg Capsules clindamycin hydrochloride PFIZER Read all of this leaflet carefully before you start taking this medicine because it contains important
Package leaflet: Information for the user Dalacin C 150mg Capsules clindamycin hydrochloride PFIZER Read all of this leaflet carefully before you start taking this medicine because it contains important
Goals of this lecture. Case 2/24/2012. Drug eruptions. The red leg. Pyoderma gangrenosum
 Goals of this lecture Lindy P. Fox, MD Associate Professor Director, Hospital Consultation Service Department of Dermatology University of California, San Francisco Drug eruptions Tell the difference between
Goals of this lecture Lindy P. Fox, MD Associate Professor Director, Hospital Consultation Service Department of Dermatology University of California, San Francisco Drug eruptions Tell the difference between
Dilantin (phenytoin) ROBERT A. SCHWARTZ
 ROBERT A. SCHWARTZ") Dilantin (phenytoin) ROBERT A. SCHWARTZ Bailey & Galyen Attorney in Charge, Mass Tort Litigation Managing Attorney, Houston 18333 Egret Bay Blvd., Suite 120 Houston, Texas 77058 Toll Free: (866) 715-1529
Dilantin (phenytoin) ROBERT A. SCHWARTZ Bailey & Galyen Attorney in Charge, Mass Tort Litigation Managing Attorney, Houston 18333 Egret Bay Blvd., Suite 120 Houston, Texas 77058 Toll Free: (866) 715-1529
Drug hypersensitivity cutaneous diseases in the elderly
 2018;66:158-162 Clinical Observations in Geriatrics Drug hypersensitivity cutaneous diseases in the elderly R. Buquicchio¹, E. Boni², S. Procoli³, G. Serviddio 4, M.T. Ventura³ ¹ Dermatological Clinic,
2018;66:158-162 Clinical Observations in Geriatrics Drug hypersensitivity cutaneous diseases in the elderly R. Buquicchio¹, E. Boni², S. Procoli³, G. Serviddio 4, M.T. Ventura³ ¹ Dermatological Clinic,
REFERRAL GUIDELINES - SUMMARY
 Clinical Immunology & Allergy Unit LEEDS TEACHING HOSPITALS NHS TRUST REFERRAL GUIDELINES - SUMMARY THESE GUIDELINES ARE DESIGNED TO ENSURE THAT PATIENTS REQUIRING SECONDARY CARE ARE SEEN EFFICIENTLY AND
Clinical Immunology & Allergy Unit LEEDS TEACHING HOSPITALS NHS TRUST REFERRAL GUIDELINES - SUMMARY THESE GUIDELINES ARE DESIGNED TO ENSURE THAT PATIENTS REQUIRING SECONDARY CARE ARE SEEN EFFICIENTLY AND
Angioedema. Disclosures. Question #1. Objectives. Question #3. Question #2 12/28/2015. Differentiate the various angioedema subtypes
 None Disclosures Jason Knuffman, M.D. Allergy and Clinical Immunology Quincy Medical Group Unity Point Health System Quincy, IL Objectives Question #1 Differentiate the various angioedema subtypes Identify
None Disclosures Jason Knuffman, M.D. Allergy and Clinical Immunology Quincy Medical Group Unity Point Health System Quincy, IL Objectives Question #1 Differentiate the various angioedema subtypes Identify
From. The Department of Pediatrics Dr. Mehtas Hospital
 From The Department of Pediatrics Dr. Mehtas Hospital Case history A 12 yr old girl : Fever 5 days Redness of eyes & erythematous rashes over the body for 2 days Past: Febrile fits at 9 mo. Of age Afebrile
From The Department of Pediatrics Dr. Mehtas Hospital Case history A 12 yr old girl : Fever 5 days Redness of eyes & erythematous rashes over the body for 2 days Past: Febrile fits at 9 mo. Of age Afebrile
ANTIBIOTICS ACUTE RHINOSINUSITIS IN CHILDREN
 MARCH 2016 DRUG ANTIBIOTICS This optimal usage guide is mainly intended f primary care health professionnals. It is provided f infmation purposes only and should not replace the clinician s judgement.
MARCH 2016 DRUG ANTIBIOTICS This optimal usage guide is mainly intended f primary care health professionnals. It is provided f infmation purposes only and should not replace the clinician s judgement.
Danger Signs in Drug Hypersensitivity
 Danger Signs in Drug Hypersensitivity Kathrin Scherer, MD*, Andreas J. Bircher, MD KEYWORDS Drug hypersensitivity Adverse drug reaction Clinical danger signs Immediate-type hypersensitivity Delayed-type
Danger Signs in Drug Hypersensitivity Kathrin Scherer, MD*, Andreas J. Bircher, MD KEYWORDS Drug hypersensitivity Adverse drug reaction Clinical danger signs Immediate-type hypersensitivity Delayed-type
A case of bullous pemphigoid following pemphigus foliaceus
 #2228 A case of bullous pemphigoid following pemphigus foliaceus Priyanka Vedak MD 1, Danielle Levine MD 1,3, Lyn Duncan MD 2,3, Hensin Tsao 1,3, Daniela Kroshinsky MD MPH 1,3 1. Department of Dermatology,
#2228 A case of bullous pemphigoid following pemphigus foliaceus Priyanka Vedak MD 1, Danielle Levine MD 1,3, Lyn Duncan MD 2,3, Hensin Tsao 1,3, Daniela Kroshinsky MD MPH 1,3 1. Department of Dermatology,
Hien Nguyen Reeves, MD, ABAI, ABIM Clinical instructor UBC, Kelowna, BC
 Hien Nguyen Reeves, MD, ABAI, ABIM Clinical instructor UBC, Kelowna, BC Disclosures Grants/Research Support: None Speakers Bureau/Honoraria: Pfizer Canada, CME Speaker Schering-Plough Merck Pictures Dermatology
Hien Nguyen Reeves, MD, ABAI, ABIM Clinical instructor UBC, Kelowna, BC Disclosures Grants/Research Support: None Speakers Bureau/Honoraria: Pfizer Canada, CME Speaker Schering-Plough Merck Pictures Dermatology
Diagnosis and Management of Drug-induced Stevens-Johnson Syndrome: Report of Two Cases
 10.5005/jp-journals-10011-1189 CASE REPORT JIAOMR Diagnosis and Management of Drug-induced Stevens-Johnson Syndrome: Report of Two Cases 1 M Venkateshwarlu, 2 B Radhika 1 Professor and Head, Department
10.5005/jp-journals-10011-1189 CASE REPORT JIAOMR Diagnosis and Management of Drug-induced Stevens-Johnson Syndrome: Report of Two Cases 1 M Venkateshwarlu, 2 B Radhika 1 Professor and Head, Department
Pathophysiology of autoimmune and allergic diseases. Hypersensitivity reactions type II type IV
 Pathophysiology of autoimmune and allergic diseases Hypersensitivity reactions type II type IV Audrey NOSBAUM, Florence HACARD, Marc VOCANSON, Frédéric BERARD, Jean François NICOLAS Allergologie et Immunologie
Pathophysiology of autoimmune and allergic diseases Hypersensitivity reactions type II type IV Audrey NOSBAUM, Florence HACARD, Marc VOCANSON, Frédéric BERARD, Jean François NICOLAS Allergologie et Immunologie
They re Scratching and You re Scratching Your Head: An Approach to the Diagnosis and Management of Acute and Chronic Urticaria
 They re Scratching and You re Scratching Your Head: An Approach to the Diagnosis and Management of Acute and Chronic Urticaria Adelle R. Atkinson, MD, FRCPC Sea Courses May/June 2017 Copyright 2017 by
They re Scratching and You re Scratching Your Head: An Approach to the Diagnosis and Management of Acute and Chronic Urticaria Adelle R. Atkinson, MD, FRCPC Sea Courses May/June 2017 Copyright 2017 by
Objectives. Terminology. Recognize common pediatric dermatologic conditions. Review treatment plans Identify skin manifestations of systemic disease
 Pediatric Visual Dermatological Diagnosis Fernando Vega, M.D. Objectives Recognize common pediatric dermatologic conditions Expand differential diagnosis Review treatment plans Identify skin manifestations
Pediatric Visual Dermatological Diagnosis Fernando Vega, M.D. Objectives Recognize common pediatric dermatologic conditions Expand differential diagnosis Review treatment plans Identify skin manifestations
Correspondence should be addressed to Wanjarus Roongpisuthipong; rr
 Dermatology Research and Practice, Article ID 237821, 5 pages http://dx.doi.org/10.1155/2014/237821 Research Article Retrospective Analysis of Corticosteroid Treatment in Stevens-Johnson Syndrome and/or
Dermatology Research and Practice, Article ID 237821, 5 pages http://dx.doi.org/10.1155/2014/237821 Research Article Retrospective Analysis of Corticosteroid Treatment in Stevens-Johnson Syndrome and/or
Vasculitis local: systemic
 Vasculitis Inflammation of the vessel wall. Signs and symptoms: 1- local: according to the involved tissue 2- systemic:(fever, myalgia, arthralgias, and malaise) Pathogenesis 1- immune-mediated 2- infectious
Vasculitis Inflammation of the vessel wall. Signs and symptoms: 1- local: according to the involved tissue 2- systemic:(fever, myalgia, arthralgias, and malaise) Pathogenesis 1- immune-mediated 2- infectious
Title: Cutaneous Adverse Drug Reactions in Indian population: A systematic review
 Title: Cutaneous Adverse Drug Reactions in Indian population: A systematic review Review question(s) To carry out a systematic review of the published evidence of the cutaneous adverse drug reactions in
Title: Cutaneous Adverse Drug Reactions in Indian population: A systematic review Review question(s) To carry out a systematic review of the published evidence of the cutaneous adverse drug reactions in
Journal of Global Trends in Pharmaceutical Sciences
 An Elsevier Indexed Journal ISSN-2230-7346 Journal of Global Trends in Pharmaceutical Sciences A CASE STUDY ON HERBAL THERAPY INDUCED ERYTHEMA MULTIFORME S. Showkath Ali * 1, S. Priyanka 2, Bandla Aswani
An Elsevier Indexed Journal ISSN-2230-7346 Journal of Global Trends in Pharmaceutical Sciences A CASE STUDY ON HERBAL THERAPY INDUCED ERYTHEMA MULTIFORME S. Showkath Ali * 1, S. Priyanka 2, Bandla Aswani
Presumed anaphylaxis to Hydrochlorothiazide in a 67 year old female with known sulphonamide allergy. By: Cody Clovechok
 Presumed anaphylaxis to Hydrochlorothiazide in a 67 year old female with known sulphonamide allergy. By: Cody Clovechok Home for the Summer Program - June and July, 2017 Lac du Bonnet, Manitoba Supervisor:
Presumed anaphylaxis to Hydrochlorothiazide in a 67 year old female with known sulphonamide allergy. By: Cody Clovechok Home for the Summer Program - June and July, 2017 Lac du Bonnet, Manitoba Supervisor:
S003 CPC Self-Assessment
 S003 CPC Self-Assessment Alina G. Bridges, D.O. Associate Professor Program Director, Dermatopathology Fellowship Department of Dermatology, Division of Dermatopathology and Cutaneous Immunopathology Mayo
S003 CPC Self-Assessment Alina G. Bridges, D.O. Associate Professor Program Director, Dermatopathology Fellowship Department of Dermatology, Division of Dermatopathology and Cutaneous Immunopathology Mayo
PACKAGE LEAFLET: INFORMATION FOR THE USER
 PACKAGE LEAFLET: INFORMATION FOR THE USER Fucidin 250 mg/5 ml Oral Suspension fusidic acid Read all of this leaflet carefully before you start taking this medicine because it contains important information
PACKAGE LEAFLET: INFORMATION FOR THE USER Fucidin 250 mg/5 ml Oral Suspension fusidic acid Read all of this leaflet carefully before you start taking this medicine because it contains important information
Clozapine Induced Skin Rash a report of two cases
 Jambulkar et al. : Clozapine induced skin rash 405 Case Report Clozapine Induced Skin Rash a report of two cases Reena Jambulkar 1, Sagar Karia 2, Akshay Chordia 3, Avinash De Sousa 4, Nilesh Shah 5 1,3
Jambulkar et al. : Clozapine induced skin rash 405 Case Report Clozapine Induced Skin Rash a report of two cases Reena Jambulkar 1, Sagar Karia 2, Akshay Chordia 3, Avinash De Sousa 4, Nilesh Shah 5 1,3
CPC. Chutika Srisuttiyakorn, M.D. Kobkul Aunhachoke, M.D. Phramongkutklao Hospital Bangkok, Thailand
 CPC Chutika Srisuttiyakorn, M.D. Kobkul Aunhachoke, M.D. Phramongkutklao Hospital Bangkok, Thailand A 53 year-old woman with fever, facial swelling and rashes on face, trunk and upper extremities for 3
CPC Chutika Srisuttiyakorn, M.D. Kobkul Aunhachoke, M.D. Phramongkutklao Hospital Bangkok, Thailand A 53 year-old woman with fever, facial swelling and rashes on face, trunk and upper extremities for 3
Chapter 65 Allergy and Immunology for the Internist. ingestion provoke an IgE antibody response and clinical symptoms in sensitive individuals.
 Chapter 65 Allergy and Immunology for the Internist 1 I. Basic Information A. Definition of Allergens: Proteins of appropriate size that after inhalation, injection (e.g. drug, venom) or ingestion provoke
Chapter 65 Allergy and Immunology for the Internist 1 I. Basic Information A. Definition of Allergens: Proteins of appropriate size that after inhalation, injection (e.g. drug, venom) or ingestion provoke
Cutaneous drug eruptions are seen commonly
 REVIEW ARTICLE Cutaneous drug reactions in children Sandipan Dhar, Raghubir Banerjee, Rajib Malakar Department of Pediatric Dermatology, Institute of Child Health, Kolkata, West Bengal, India ABSTRACT
REVIEW ARTICLE Cutaneous drug reactions in children Sandipan Dhar, Raghubir Banerjee, Rajib Malakar Department of Pediatric Dermatology, Institute of Child Health, Kolkata, West Bengal, India ABSTRACT
VARICELLA. Infectious and Tropical Pediatric Division, Department of Child Health, Medical Faculty, University of Sumatera Utara
 VARICELLA (Chicken pox) Infectious and Tropical Pediatric Division, Department of Child Health, Medical Faculty, University of Sumatera Utara Definition : Varicella is a common contagious disease caused
VARICELLA (Chicken pox) Infectious and Tropical Pediatric Division, Department of Child Health, Medical Faculty, University of Sumatera Utara Definition : Varicella is a common contagious disease caused
Questions. Answers. Share your photos and diagnoses with us!
 Illustrated quizzes on problems seen in everyday practice Case 1 A 56-year-old woman presented with a two-week history of pruritic urticarial plaques and tense bullae on both erythematous and normal skin.
Illustrated quizzes on problems seen in everyday practice Case 1 A 56-year-old woman presented with a two-week history of pruritic urticarial plaques and tense bullae on both erythematous and normal skin.
in Pediatric Medicine
 in Pediatric Medicine Martin Belson, MD Pediatric Emergency Medicine Associates, LLC Pediatric Sedation Services, LLC Children s Healthcare of Atlanta, Scottish Rite and Egleston Wellstar Hospital Systems
in Pediatric Medicine Martin Belson, MD Pediatric Emergency Medicine Associates, LLC Pediatric Sedation Services, LLC Children s Healthcare of Atlanta, Scottish Rite and Egleston Wellstar Hospital Systems
RABEPRAZOL 10mg and 20mg Gastro-resistant Tablets
 PACKAGE LEAFLET: INFORMATION FOR THE USER RABEPRAZOL 10mg and 20mg Gastro-resistant Tablets RABEPRAZOLE This leaflet is a copy of the Summary of Product Characteristics and Patient Information Leaflet
PACKAGE LEAFLET: INFORMATION FOR THE USER RABEPRAZOL 10mg and 20mg Gastro-resistant Tablets RABEPRAZOLE This leaflet is a copy of the Summary of Product Characteristics and Patient Information Leaflet
A Retrospective Study of Spectrum of Nevirapine Induced Cutaneous Drug Reactions in HIV Positive Patients
 Journal of US-China Medical Science 12 (2015) 85-89 doi: 10.17265/1548-6648/2015.02.008 D DAVID PUBLISHING A Retrospective Study of Spectrum of Nevirapine Induced Cutaneous Drug Reactions in HIV Positive
Journal of US-China Medical Science 12 (2015) 85-89 doi: 10.17265/1548-6648/2015.02.008 D DAVID PUBLISHING A Retrospective Study of Spectrum of Nevirapine Induced Cutaneous Drug Reactions in HIV Positive
Annual Scientific Meeting 2018
 Annual Scientific Meeting 2018 Reported by HYY Kwong, HL Lo, SH Ng, PY Ngan, W Ngan, HW Wong, WF Wu Date: 23-24 June 2018 Venue: Sheraton Hong Kong Hotel & Towers, Tsim Sha Tsui, Hong Kong Organiser: Hong
Annual Scientific Meeting 2018 Reported by HYY Kwong, HL Lo, SH Ng, PY Ngan, W Ngan, HW Wong, WF Wu Date: 23-24 June 2018 Venue: Sheraton Hong Kong Hotel & Towers, Tsim Sha Tsui, Hong Kong Organiser: Hong