Only the Mohs Knows: Management of Periocular Skin Cancers
|
|
|
- Ira Nelson
- 5 years ago
- Views:
Transcription

1 Only the Mohs Knows: Management of Periocular Skin Cancers Andrew R. Harrison, M.D. Director, Oculoplastic and Orbital Surgery University of Minnesota
2 Overview Common Eyelid Skin Cancers Management Options for Removal of Eyelid Skin Cancers Reconstruction Of Eyelid Defects
3 POLLING QUESTION What is your level of training? 1. Medical student 2. Ophthalmology Resident 3. Ophthalmologist 4. Oculoplastic Surgeon
4 Eyelid Neoplasms 2/3 Benign 1/3 Malignant
5 Rule of 9s 90 % Basal Cell 9 % Squamous Cell 0.9 % Sebaceous Cell

6 Features of Malignancy Destruction of lid architecture Lash loss Telangiectasias Rapid Growth Nodular appearance Central Ulceration Recur after excision
 Usually 6 th 7 th decade 5 15% age 25 40 Fair")
7 Basal Cell Carcinoma 700,000 new cases each year 90 % are in the head and neck (10% eyelid) Usually 6 th 7 th decade 5 15% age Fair Complexion

8 Basal Cell Carcinoma 53% lower eyelid 27% medial canthus 12% upper eyelid 8% lateral canthus

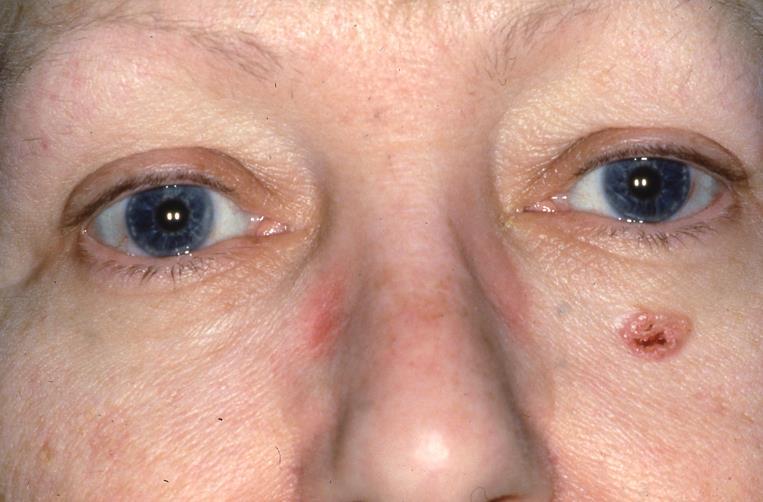
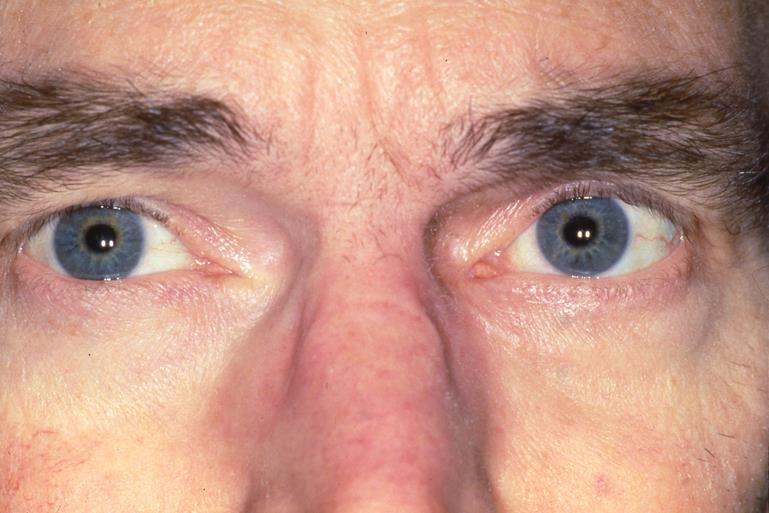
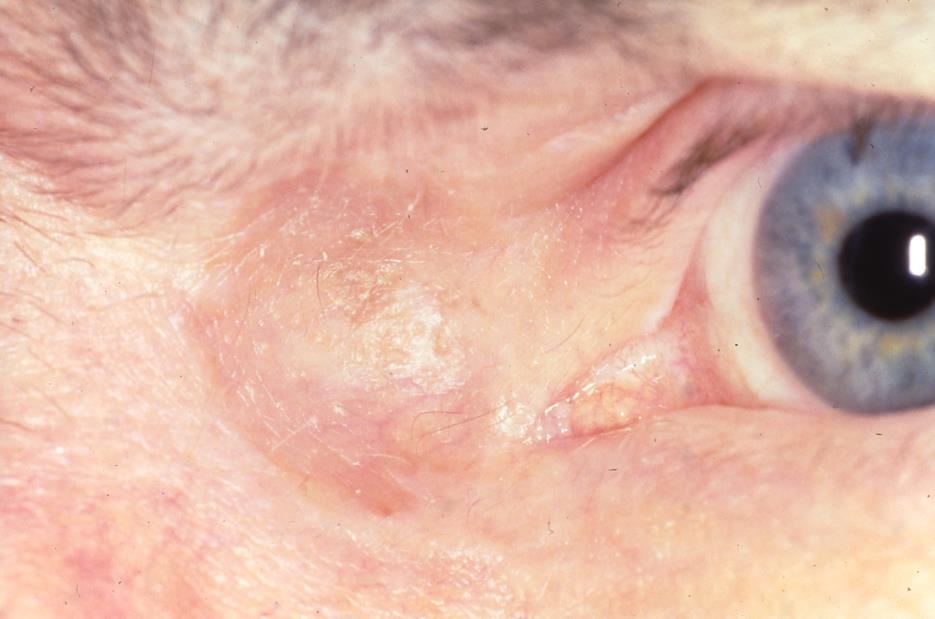
9 Basal Cell Carcinoma

10 Basal Cell Carcinoma
11
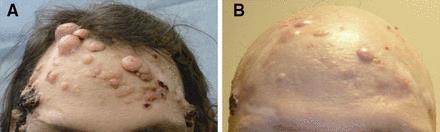
12 Gorlin Syndrome aka Basal Cell Nevus Syndrome Autosomal Dominant 1 in 31,000 people Most develop BCCs in adolescence or early adulthood
 Palmar")

13 Associated Findings in Gorlin Syndrome Keratocystic odontogenic tumors Medulloblastomas and fibromas (ovarian and cardiac) Palmar and plantar pits Cleft lip or palate Frontal and temporopariental bossing Hypertelorism Mandibular prognathism Scoliosis or kyphosis Bifid ribs



14 Gorlin Syndrome Defect in Patched 1 gene (PCTH1) tumor suppressor gene that inhibits the hedgehog signaling pathway





15 Roles of Sonic Hedgehog signaling: - Limb development - Neural differentiation - Facial morphogenesis

16 Vismodegib Approved by FDA in Jan 2012 for tx of locally advanced or metastatic basal cell carcinomas Blocks hedgehog pathway Works by inhibiting SMO $250/pill

17 Jean Tang et al, 2012 Randomized, double-blind, placebo-controlled 41 patients with Basal Cell Nevus Syndrome followed for mean of 8 months
18 Lower rate of new BCCs with vismodegib (2 vs 29 cases/group/year) Larger decrease in size (-65% vs -11%)
19 Vismodegib
20 54% of patients discontinued treatment due to side effects Loss of taste Muscle cramps Hair loss Weight loss Dysgeusia and muscle cramps resolved in 1 month Hair growth resumed within 3 months
21 After stopping vismodegib: BCCs and pits recurred at same sites Sum of the longest BCC diameters returned to baseline Lower rate of new surgically eligible BCCs after treatment with vismodegib (0.69 per month vs 2.4 per month)
22


23 3 months on vismodegib

24 Squamous Cell Carcinoma Risk Factors Sun exposure Fair Complexion Radiation Exposure Metastatic Potential 0 40% Regional Nodes and Distant Sites Potential for perineural invasion



25 Squamous Cell Carcinoma


26 Sebaceous Gland Carcinoma masquerade Propensity to recur Metastatic potential More common in upper eyelid 65-70% Female, 7-8 th decade 1% in Europe and 30% in Asia 22% mortality



27 Sebaceous Gland Carcinoma

28 Melanoma Rare in the periocular region though lentigo maligna (in situ) lesions are common in the malar region Malignant transformation of normal skin melanocytes Blonde hair, blue eye Areas with high UV exposure

29 Melanoma History Unprotected extensive sun exposure Pre-existing pigmented lesion May occur de novo Historical change in pigment density, distribution or surface New nodule formation in a flat lesion


30 Melanoma Exam A, B, C, D, E Asymmetry Border Color Diameter > 6 mm Evolving
31 Melanoma Breslow depth Tumor depth vs 5 yr survival Stage I < 0.75mm Stage II mm Stage III mm Stage IV mm Stage V > 3.0mm <1mm % 1-2mm 80-96% 2-4mm 60-75% >4mm 50%




32 Sentinel Lymph node biopsy
33 Sentinel Lymph Node Biopsy Identifies 20-25% of patients who have occult nodal disease Identifies patients who may need lymphadenectomy and/or adjuvant therapy Improves survival 30% improvement in 10 year survival
34 Melanoma -treatment Wide margin excision permanent sections slow Mohs Typically 1 cm margin in other areas Eyelid margins of thin melanomas(<2mm) 5mm considered adequate in one study
35 Management Step 1 = BIOPSY Kersten, Ophthalmology % of clinically benign lesions turned out to be malignant All excised lesions should be sent for pathologic evaluation If clinical suspicion of malignancy is high and path result does not agree, consider rebiopsy

36 Where to Biopsy?

37 Biopsy! Shave, Incise, Excise Just Do It!
38 POLLING QUESTION What is your preferred method for removing basal cell carcinoma from the eyelid? 1. Resect in OR with wide margins 2. Resect in OR with frozen section margin control 3. Mohs surgery 4. Electrodessication with curretage
39 Management Options Resection with frozen sections Mohs micrographic surgery Radiation Chemotherapy Cryotherapy Electrodessication and Curettage Immunotherapy (Aldara)
40 Management Options Resection with frozen sections Mohs micrographic surgery
41 Surgical Resection Requires coordination with pathologist minutes OR time per frozen section (if you are lucky!) Single procedure Recurrence Rate for Primary BCC= 5.5% Recurrence Rate for Recurrent BCC= 18%

42 Mohs Micrographic Surgery Described by Fred Mohs in the 1930s General Surgeon at U W Madison First described as micrographic chemosurgery Color coded mapping of tumor margins Microscopic control of margins
43 Mohs Micrographic Surgery Dr. Mohs was filming removal of an eyelid carcinoma and had a delay and used frozen sections instead of fixed sections Mohs publishes paper with 66 BCC and SCC of the eyelid with 5 year cure rates of 100%
44 Mohs Micrographic Surgery Dermatologic Surgeon/Pathologist performs excision and reviews frozen sections Allows separation of resecting and reconstructing surgeon Preserves the most normal tissue Recurrence Rate with primary BCC = 1% Recurrence Rate with recurrent BCC = 8%

45 Mohs Micrographic Surgery
46 Resection with Frozen Sections Small Central Nodular Tumor Amenable to pentagonal wedge resection Older patients who desire a single setting procedure



47
48 Resection with Frozen Sections Melanocytic Lesions slow Mohs Permanent rather than frozen sections Sebaceous Gland Carcinoma Resection of eyelid mass with wide margins Topical MMC chemotherapy of conjunctival and corneal involvement


49 Now the tumor is gone. What next?
 Don t burn")
50 Eyelid Reconstruction - Principles Follow the reconstructive ladder (maybe) Don t burn bridges

51 Eyelid Reconstruction - Principles Avoid vertical traction on the eyelid margin Don t hesitate to support the lateral canthus!
52 Eyelid Reconstruction - Principles Close deep tissue first with appropriate suture to avoid undue tension on skin edges Undermine widely Often allows simple closure Anterior and Posterior Lamellae need to be reconstructed separately Only one may be a free graft

53 Eyelid Reconstruction - Anatomy Anterior Lamella Skin Orbicularis Posterior Lamella Tarsus Conjunctiva


54 Eyelid Reconstruction - Anatomy
55 Anterior lamella defects
56 What would you do?

57 POLLING QUESTION HOW WOULD YOU CLOSE THE DEFECT? 1. Skin graft 2. Advancement flap 3. Granulate
58

59 Ans

60 Patient after Mohs surgery large defect in right lower eyelid, sparing the lid margin

61 Surgical Planning O-Z Double Advancement Flaps


62 Creating skin flaps


63 Closure and excision of dog ear deformity
64 O-to-Z closure, before and after


65 O-to-Z closure, before and after
66
")
67 O to Z Closure (the IOL flap)

68 O to Z Closure

69 O to Z Closure

70 Double advancement flaps

71

72
73 Full Thickness Skin Graft Donor Sites Upper eyelid Pre/Post Auricular Supraclavicular Volar surface of the upper arm

74 Full Thickness Skin Graft
75 Full Thickness Skin Graft

76
77
78
79 Up to 25 % Direct closure Lower Eyelid Defects Lateral canthotomy and inferior cantholysis % Tenzel semicircular flap Greater than 50 % Hughes flap + skin graft Hewes flap +Trippier flap Mustarde flap
80 POLLING QUESTION How do you close the eyelid margin? 1. 3 non-absorbable sutures across the margin 2. Vertical mattress suture 3. Buried vertical mattress suture

81

82
83

84 Buried vertical mattress margin suture
85

86 s/p Mohs

87 Tenzel Flap
88 Tenzel Flap

89 Tenzel Flap

90 Tenzel Flap

91 Tenzel Flap

92 Hughes Flap

93 Hughes Flap
94 Hughes Flap

95 Hughes Flap
96 Hughes flap

97 Hughes Flap

98 Hughes Flap
99 Hughes Flap

100 Hughes Flap

101 Hughes Flap

102 Hughes Flap

103 Hughes Flap

104 Hughes Flap

105 Hughes Flap

106 Hughes Flap

107 Hewes Flap

108 Pre-op after Mohs surgery

109 Hewes flap posterior lamella Tarsus and conjunctiva, upper lid Superior tarsal border

110 Hewes flap posterior lamella Tarso-conjunctival flap

111 Hewes flap posterior lamella Tarso-conjunctival flap filling defect in lower eyelid.

112 Upper eyelid skin and orbicularis flap Hewes anterior lamella

113 Anterior lamellar flap from upper eyelid replacing lower eyelid defect. Hewes anterior lamella


114 Hewes flap closure of upper lid harvest site

115 Hewes flap outcome

116

117

118

119


120

121 Mustarde Flap

122 Mustarde cheek rotation flap

123 Mustarde Flap

124 Mustarde Flap

125 Mustarde Flap

126
127

128

129
130
131 Cheek rotation flap
132 Medial Canthal Defects Granulate (secondary intention) Skin Graft Upper eylid flap Glabellar Flap Paramedian forehead flap

133 s/p Mohs

134 Full Thickness Skin Graft

135 s/p Mohs

136 s/p FTSG

137 Upper eyelid transposition flap

138 Upper eyelid transposition flap

139 Upper eyelid transposition flap

140 Upper eyelid transposition flap


141 Rhomboid Flap

142 Rhomboid Flap

143 Glabellar Rotation Flap
144 s/p Mohs


145 Glabellar Rotation Flap

146 Glabellar Rotation Flap
147 Upper Eyelid Defects Up to 25 % Direct closure +/- canthotomy/cantholysis % Tenzel flap Tarsal transfer flap Greater than 50% Cutler Beard Flap +/- graft

148
149 Reverse Tenzel

150 s/p melanoma resection

151 Cutler Beard Flap

152 Cutler Beard Flap

153 Cutler Beard Flap

154 Cutler Beard Flap

155 Cutler Beard Flap

156 Cutler Beard Flap

157 Cutler Beard Flap


158 Cutler Beard Flap

159 COMPLEX MOH S DEFECT PLANNING SEBACEOUS CELL CARCINOMA


160


161


162 PREOPERATIVE POSTOPERATIVE

163 The lacrimal system The punctum and proximal canaliculus are often excised with medial canthus and lower lid tumors Reconstruct with silicone stent when there is residual canaliculus

164 If no canalicular system late reconstruction with Jones tube Jones Tube
165 Summary Suspect malignancy Especially BCC Biopsy all suspicious lesions Know your local Mohs surgeons Use basic reconstructive procedures

166 Don t Forget Your Sunscreen

167 Don t forget your sunglasses!

168 I can t wait to see what this tan will look like in 30 years
169 THANK YOU!
Technicians & Nurses Program
 ASCRS ASOA Symposium & Congress Technicians & Nurses Program May 6-10, 2016 New Orleans Evaluation and Treatment of Eyelid Malignancies Richard C. Allen MD PhD FACS Professor Section of Ophthalmology Dept.
ASCRS ASOA Symposium & Congress Technicians & Nurses Program May 6-10, 2016 New Orleans Evaluation and Treatment of Eyelid Malignancies Richard C. Allen MD PhD FACS Professor Section of Ophthalmology Dept.
Periocular Malignancies
 Periocular Malignancies Andrew Gurwood, O.D., F.A.A.O., Dipl. Marc Myers, O.D., F.A.A.O. Drs. Myers and Gurwood have no financial interests to disclose. Course Description Discussion of the most common
Periocular Malignancies Andrew Gurwood, O.D., F.A.A.O., Dipl. Marc Myers, O.D., F.A.A.O. Drs. Myers and Gurwood have no financial interests to disclose. Course Description Discussion of the most common
Exenteration. Introduction. The skin. Epidermal malignancies 8/3/2017. Neglected basal cell carcinoma
 Jeremiah Tao, MD, FACS Director, Oculoplastic and Orbital Surgery Associate Professor, UC Irvine Neglected basal cell carcinoma Exenteration Introduction Chief question with any eyelid lesion: Suspicious
Jeremiah Tao, MD, FACS Director, Oculoplastic and Orbital Surgery Associate Professor, UC Irvine Neglected basal cell carcinoma Exenteration Introduction Chief question with any eyelid lesion: Suspicious
MOHS MICROGRAPHIC SURGERY: AN OVERVIEW
 MOHS MICROGRAPHIC SURGERY: AN OVERVIEW SKIN CANCER: Skin cancer is far and away the most common malignant tumor found in humans. The most frequent types of skin cancer are basal cell carcinoma, squamous
MOHS MICROGRAPHIC SURGERY: AN OVERVIEW SKIN CANCER: Skin cancer is far and away the most common malignant tumor found in humans. The most frequent types of skin cancer are basal cell carcinoma, squamous
Management of Lid Lacerations
 Ocular Ocular Trauma Management of Lid Lacerations Nitin Vichare MS, DNB, FAICO Nitin Vichare MS, DNB,FAICO Dept. of Ophthalmology, Command Hospital, (Southern Command), Pune, Maharashtra Eyelids are not
Ocular Ocular Trauma Management of Lid Lacerations Nitin Vichare MS, DNB, FAICO Nitin Vichare MS, DNB,FAICO Dept. of Ophthalmology, Command Hospital, (Southern Command), Pune, Maharashtra Eyelids are not
Skin Malignancies Non - Melanoma & Melanoma Marilyn Ng, MD Dept. of Surgery M&M Conference Downstate Medical Center July 19, 2012
 Skin Malignancies Non - Melanoma & Melanoma Marilyn Ng, MD Dept. of Surgery M&M Conference Downstate Medical Center July 19, 2012 Case Presentation 57 yo man with 3 month hx of a nonhealing < 1 cm right
Skin Malignancies Non - Melanoma & Melanoma Marilyn Ng, MD Dept. of Surgery M&M Conference Downstate Medical Center July 19, 2012 Case Presentation 57 yo man with 3 month hx of a nonhealing < 1 cm right
Clinical characteristics
 Skin Cancer Fernando Vega, MD Seattle Healing Arts Clinical characteristics Precancerous lesions Common skin cancers ACTINIC KERATOSIS Precancerous skin lesions Actinic keratoses Dysplastic melanocytic
Skin Cancer Fernando Vega, MD Seattle Healing Arts Clinical characteristics Precancerous lesions Common skin cancers ACTINIC KERATOSIS Precancerous skin lesions Actinic keratoses Dysplastic melanocytic
Skin Cancer 101: Diagnosis and Management of the Most Common Cancer
 Skin Cancer 101: Diagnosis and Management of the Most Common Cancer Sarah Patton, PA-C, MSHS Skin Surgery Center www.skinsurgerycenter.com Seattle/Bellevue, WA Skin cancer Skin cancer is by far the most
Skin Cancer 101: Diagnosis and Management of the Most Common Cancer Sarah Patton, PA-C, MSHS Skin Surgery Center www.skinsurgerycenter.com Seattle/Bellevue, WA Skin cancer Skin cancer is by far the most
Living Beyond Cancer Skin Cancer Detection and Prevention
 Living Beyond Cancer Skin Cancer Detection and Prevention Cutaneous Skin Cancers Identification Diagnosis Treatment options Prevention What is the most common cancer in people? What is the most common
Living Beyond Cancer Skin Cancer Detection and Prevention Cutaneous Skin Cancers Identification Diagnosis Treatment options Prevention What is the most common cancer in people? What is the most common
Eyelid basal cell carcinoma Patient information
 Eyelid basal cell carcinoma Patient information Your procedure relates to the face, eyelids, orbit or tear drainage system that together are treated by specialist surgeons in the field of oculoplastic
Eyelid basal cell carcinoma Patient information Your procedure relates to the face, eyelids, orbit or tear drainage system that together are treated by specialist surgeons in the field of oculoplastic
Skin Cancer. 5 Warning Signs. American Osteopathic College of Occupational and Preventive Medicine OMED 2012, San Diego, Monday, October 8, 2012 C-1
 Skin Cancer AMERICAN OSTEOPATHIC COLLEGE OF OCCUPATIONAL & PREVENTIVE MEDICINE OMED 2012 October 8, 2012 E. Robert Wanat II, D.O., M.P.H. Learning Objectives: Identify the 3 Basic Types of Skin Cancer
Skin Cancer AMERICAN OSTEOPATHIC COLLEGE OF OCCUPATIONAL & PREVENTIVE MEDICINE OMED 2012 October 8, 2012 E. Robert Wanat II, D.O., M.P.H. Learning Objectives: Identify the 3 Basic Types of Skin Cancer
Identifying Skin Cancer. Mary S. Stone MD Professor of Dermatology and Pathology University of Iowa Carver College of Medicine March, 2018
 Identifying Skin Cancer Mary S. Stone MD Professor of Dermatology and Pathology University of Iowa Carver College of Medicine March, 2018 American Cancer Society web site Skin Cancer Melanoma Non-Melanoma
Identifying Skin Cancer Mary S. Stone MD Professor of Dermatology and Pathology University of Iowa Carver College of Medicine March, 2018 American Cancer Society web site Skin Cancer Melanoma Non-Melanoma
Glenn D. Goldman, MD. University of Vermont Medical Center. University of Vermont College of Medicine
 Glenn D. Goldman, MD University of Vermont Medical Center University of Vermont College of Medicine Recognize and identify the main types of skin cancer and their precursors Identify and understand new
Glenn D. Goldman, MD University of Vermont Medical Center University of Vermont College of Medicine Recognize and identify the main types of skin cancer and their precursors Identify and understand new
5/20/2015. Mohs Surgery BCCA High risk anatomic locations. Mohs Surgery High risk anatomic locations. Mohs Surgery Histologically Aggressive BCCA
 Mohs Surgery BCCA High risk anatomic locations High risk areas H zone nasal ala, nasal septum, nasal ala groove, periorbital region, periauricual region, region around and in ear canal, ear pinna and scalp
Mohs Surgery BCCA High risk anatomic locations High risk areas H zone nasal ala, nasal septum, nasal ala groove, periorbital region, periauricual region, region around and in ear canal, ear pinna and scalp
Benign versus Cancerous Lesions How to tell the difference FMF 2014 Christie Freeman MD, CCFP, DipPDerm, MSc
 1 Benign versus Cancerous Lesions How to tell the difference FMF 2014 Christie Freeman MD, CCFP, DipPDerm, MSc Benign lesions Seborrheic Keratoses: Warty, stuck-on Genetics and birthdays Can start in late
1 Benign versus Cancerous Lesions How to tell the difference FMF 2014 Christie Freeman MD, CCFP, DipPDerm, MSc Benign lesions Seborrheic Keratoses: Warty, stuck-on Genetics and birthdays Can start in late
Cutaneous Malignancies: A Primer COPYRIGHT. Marissa Heller, M.D.
 Cutaneous Malignancies: A Primer Marissa Heller, M.D. Associate Director of Dermatologic Surgery Department of Dermatology Beth Israel Deaconess Medical Center December 10, 2016 Skin Cancer Non-melanoma
Cutaneous Malignancies: A Primer Marissa Heller, M.D. Associate Director of Dermatologic Surgery Department of Dermatology Beth Israel Deaconess Medical Center December 10, 2016 Skin Cancer Non-melanoma
Periocular skin cancer
 Periocular skin cancer Information for patients Skin cancer involving the skin of the eyelid or around the eye is called a periocular skin cancer. Eyelid skin cancers occur most often on the lower eyelid,
Periocular skin cancer Information for patients Skin cancer involving the skin of the eyelid or around the eye is called a periocular skin cancer. Eyelid skin cancers occur most often on the lower eyelid,
SKIN CANCER. Most common cancer diagnosis 40% of all cancers
 SKIN CANCER Most common cancer diagnosis 40% of all cancers OBJECTIVES Review common and uncommon cancers of the skin. Special emphasis on melanoma and dysplastic nevus Review pathology/tnm/staging, which
SKIN CANCER Most common cancer diagnosis 40% of all cancers OBJECTIVES Review common and uncommon cancers of the skin. Special emphasis on melanoma and dysplastic nevus Review pathology/tnm/staging, which
Intraoperative Dermoscopy for Identification of Early Basal Cell Carcinomas in Basal Cell Nevus Syndrome
 Intraoperative Dermoscopy for Identification of Early Basal Cell Carcinomas in Basal Cell Nevus Syndrome Disclosures I have no industry related, financial, or other disclosures Goals Discuss the clinical
Intraoperative Dermoscopy for Identification of Early Basal Cell Carcinomas in Basal Cell Nevus Syndrome Disclosures I have no industry related, financial, or other disclosures Goals Discuss the clinical
Glenn D. Goldman, MD. Fletcher Allen Health Care. University of Vermont College of Medicine
 Glenn D. Goldman, MD Fletcher Allen Health Care University of Vermont College of Medicine Recognize and identify the main types of skin cancer Understand how and why Mohs surgery is utilized for the treatment
Glenn D. Goldman, MD Fletcher Allen Health Care University of Vermont College of Medicine Recognize and identify the main types of skin cancer Understand how and why Mohs surgery is utilized for the treatment
Dermatopathology: The tumor is composed of keratinocytes which show atypia, increase mitoses and abnormal mitoses.
 Squamous cell carcinoma (SCC): A common malignant tumor of keratinocytes arising in the epidermis, usually from a precancerous condition: 1- UV induced actinic keratosis, usually of low grade malignancy.
Squamous cell carcinoma (SCC): A common malignant tumor of keratinocytes arising in the epidermis, usually from a precancerous condition: 1- UV induced actinic keratosis, usually of low grade malignancy.
Reconstruction of seventeen full-thickness defects of the eyelids with twenty-two Hübner tarsomarginal grafts *
 British Journal of Plastic Surgery (2005) 58, 361 365 Reconstruction of seventeen full-thickness defects of the eyelids with twenty-two Hübner tarsomarginal grafts * G. Dagregorio a, *, V. Huguier b, V.
British Journal of Plastic Surgery (2005) 58, 361 365 Reconstruction of seventeen full-thickness defects of the eyelids with twenty-two Hübner tarsomarginal grafts * G. Dagregorio a, *, V. Huguier b, V.
with laser resurfacing, 36, 37 Cryotherapy, lower eyelid cicatricial ectropion after, 151 Cutler-Beard flap. See Fullthickness
 INDEX A Abrasion, from silicone tubing, 230 Acquired immunodeficiency syndrome, eyelid tumor with, 193 AIDS. See Acquired immunodeficiency syndrome Anatomy, eyelid, 155 156 Aneurysm, cerebral, Muller s
INDEX A Abrasion, from silicone tubing, 230 Acquired immunodeficiency syndrome, eyelid tumor with, 193 AIDS. See Acquired immunodeficiency syndrome Anatomy, eyelid, 155 156 Aneurysm, cerebral, Muller s
Large majority caused by sun exposure Often sun exposure before age 20 Persons who burn easily and tan poorly are at greatest risk.
 Basics of Skin Cancer Detection and Treatment of Non- Melanoma Skin Cancers Large majority caused by sun exposure Often sun exposure before age 20 Persons who burn easily and tan poorly are at greatest
Basics of Skin Cancer Detection and Treatment of Non- Melanoma Skin Cancers Large majority caused by sun exposure Often sun exposure before age 20 Persons who burn easily and tan poorly are at greatest
Learning Objectives. Tanning. The Skin. Classic Features. Sun Reactive Skin Type Classification. Skin Cancers: Preventing, Screening and Treating
 Learning Objectives Skin Cancers: Preventing, Screening and Treating Robert A. Baldor, MD, FAAFP Professor, Family Medicine & Community Health University of Massachusetts Medical School Distinguish the
Learning Objectives Skin Cancers: Preventing, Screening and Treating Robert A. Baldor, MD, FAAFP Professor, Family Medicine & Community Health University of Massachusetts Medical School Distinguish the
MOHS MICROGRAPHIC SURGERY
 MOHS MICROGRAPHIC SKIN CANCER Skin cancer is by far the most common malignant tumor in humans. The most common types of skin cancer are basal cell carcinoma, squamous cell carcinoma, and melanoma. Both
MOHS MICROGRAPHIC SKIN CANCER Skin cancer is by far the most common malignant tumor in humans. The most common types of skin cancer are basal cell carcinoma, squamous cell carcinoma, and melanoma. Both
Eyelid Reconstruction An Oculoplastic Surgical Coding Minicourse. Riva Lee Asbell Philadelphia, PA. Part II
 INTRODUCTION Eyelid Reconstruction An Oculoplastic Surgical Coding Minicourse Riva Lee Asbell Philadelphia, PA Part II In this second part of the Minicourse on Surgical Coding for Eyelid Reconstruction
INTRODUCTION Eyelid Reconstruction An Oculoplastic Surgical Coding Minicourse Riva Lee Asbell Philadelphia, PA Part II In this second part of the Minicourse on Surgical Coding for Eyelid Reconstruction
Lower Eyelid Reconstruction after Basal Cell Carcinoma Removal
 Lower Eyelid Reconstruction after Basal Cell Carcinoma Removal A Decision Management Tool Pooja Sethi 1, Soroosh Behshad 1, Alejandra A. Valenzuela 1 Corresponding author address: From Department of Ophthalmology,
Lower Eyelid Reconstruction after Basal Cell Carcinoma Removal A Decision Management Tool Pooja Sethi 1, Soroosh Behshad 1, Alejandra A. Valenzuela 1 Corresponding author address: From Department of Ophthalmology,
Kevin T. Kavanagh, MD
 Kevin T. Kavanagh, MD Axial Based upon a named artery. Survival length depends upon the artery not the width of the flap. Random Has random unnamed vessels supplying it. Survival length is directly proportional
Kevin T. Kavanagh, MD Axial Based upon a named artery. Survival length depends upon the artery not the width of the flap. Random Has random unnamed vessels supplying it. Survival length is directly proportional
Cutaneous Melanoma: Epidemiology (USA) The Sentinel Node in Head and Neck Melanoma. Cutaneous Melanoma: Epidemiology (USA)
 The Sentinel Node in Head and Neck Melanoma. Cutaneous Melanoma: Epidemiology (USA)") The Sentinel Node in Head and Neck Melanoma Cutaneous Melanoma: Epidemiology (USA) 6 th leading cause of cancer among men and women 68,720 new cases of invasive melanoma in 2009 8,650 deaths from melanoma
The Sentinel Node in Head and Neck Melanoma Cutaneous Melanoma: Epidemiology (USA) 6 th leading cause of cancer among men and women 68,720 new cases of invasive melanoma in 2009 8,650 deaths from melanoma
UWMC Roosevelt Clinic Rotation Goals 2011 Procedural Dermatology Fellowship Program 1
 Procedural Dermatology Fellowship Objectives University of Washington Medical Center-Roosevelt Rotation The primary goal of the University of Washington rotation of the Procedural Dermatology fellowship
Procedural Dermatology Fellowship Objectives University of Washington Medical Center-Roosevelt Rotation The primary goal of the University of Washington rotation of the Procedural Dermatology fellowship
1. Written information to patient /GP: fax ASAP to GP & offer copy of consultation letter.
 Skin Cancer follow up guidelines If NEW serious diagnosis given: 1. Written information to patient /GP: fax ASAP to GP & offer copy of consultation letter. 2. Free prescription information details. 3.
Skin Cancer follow up guidelines If NEW serious diagnosis given: 1. Written information to patient /GP: fax ASAP to GP & offer copy of consultation letter. 2. Free prescription information details. 3.
Periocular Skin Malignancies May 2008
 TITLE: Periocular Skin Malignancies SOURCE: Grand Rounds Presentation, The University of Texas Medical Branch, Department of Otolaryngology DATE: May 8, 2008 RESIDENT PHYSICIAN: Jeffrey Buyten, MD FACULTY
TITLE: Periocular Skin Malignancies SOURCE: Grand Rounds Presentation, The University of Texas Medical Branch, Department of Otolaryngology DATE: May 8, 2008 RESIDENT PHYSICIAN: Jeffrey Buyten, MD FACULTY
PanMidlands Ocular Cancer Pathway March 2008 Approved by The Midland Oculoplastic Surgery Society
 PanMidlands Ocular Cancer Pathway March 2008 Approved by The Midland Oculoplastic Surgery Society Periocular Skin Pathway Referrals to Oculoplastics Strong Indication: Lesion within orbital rim Medial
PanMidlands Ocular Cancer Pathway March 2008 Approved by The Midland Oculoplastic Surgery Society Periocular Skin Pathway Referrals to Oculoplastics Strong Indication: Lesion within orbital rim Medial
Case Scenario 1 Worksheet. Primary Site C44.4 Morphology 8743/3 Laterality 0 Stage/ Prognostic Factors
 CASE SCENARIO 1 9/10/13 HISTORY: Patient is a 67-year-old white male and presents with lesion located 4-5cm above his right ear. The lesion has been present for years. No lymphadenopathy. 9/10/13 anterior
CASE SCENARIO 1 9/10/13 HISTORY: Patient is a 67-year-old white male and presents with lesion located 4-5cm above his right ear. The lesion has been present for years. No lymphadenopathy. 9/10/13 anterior
A superficial radiotherapy B single pass curettage C excision with 2 mm margins D excision with 5 mm margins E Mohs micrographic surgery.
 1- A 63-year-old woman presents with a non-healing lesion on her right temple that has been present for over two years. On examination there is a 6 mm well defined lesion with central ulceration, telangiectasia
1- A 63-year-old woman presents with a non-healing lesion on her right temple that has been present for over two years. On examination there is a 6 mm well defined lesion with central ulceration, telangiectasia
Know who is at risk: LOOK! for ABCDs, rapidly changing lesions, do a biopsy when indicated
 Lindy P. Fox, MD Associate Professor Director, Hospital Consultation Service Department of Dermatology University of California, San Francisco Applies to adults without history of malignancy or premalignant
Lindy P. Fox, MD Associate Professor Director, Hospital Consultation Service Department of Dermatology University of California, San Francisco Applies to adults without history of malignancy or premalignant
Mohs. Micrographic Surgery. For Treating Skin Cancer
 Mohs Micrographic Surgery For Treating Skin Cancer Skin Cancer Basics Skin cancer is common. Over the past three decades, more people have had skin cancer than all other cancers combined. Each year in
Mohs Micrographic Surgery For Treating Skin Cancer Skin Cancer Basics Skin cancer is common. Over the past three decades, more people have had skin cancer than all other cancers combined. Each year in
29/06/1439 بسم ا هلل ا لرحمن ا لر حيم
 بسم ا هلل ا لرحمن ا لر حيم 1 LID RECONSTRUCTION by Ali M ISMAIL professor of ophthalmology @SOHAG U H Occuloplastic fellow @NNUH Occuloplastic fellow @Cambridge UH Honor fellow @ Mooorfield eye Hospital
بسم ا هلل ا لرحمن ا لر حيم 1 LID RECONSTRUCTION by Ali M ISMAIL professor of ophthalmology @SOHAG U H Occuloplastic fellow @NNUH Occuloplastic fellow @Cambridge UH Honor fellow @ Mooorfield eye Hospital
General information about skin cancer
 Skin Cancer General information about skin cancer Key points Skin cancer is a disease in which malignant (cancer) cells form in the tissues of the skin. There are different types of cancer that start in
Skin Cancer General information about skin cancer Key points Skin cancer is a disease in which malignant (cancer) cells form in the tissues of the skin. There are different types of cancer that start in
Skin Cancer - Non-Melanoma
 Skin Cancer - Non-Melanoma Introduction Each year, millions of people find out that they have skin cancer. Skin cancer is almost 100% curable if found early and treated right away. It is possible to prevent
Skin Cancer - Non-Melanoma Introduction Each year, millions of people find out that they have skin cancer. Skin cancer is almost 100% curable if found early and treated right away. It is possible to prevent
Usefulness of the orbicularis oculi myocutaneous flap in periorbital reconstruction
 Archives of Craniofacial Surgery Arch Craniofac Surg Vol.19 No.4, 254-259 Usefulness of the orbicularis oculi myocutaneous flap in periorbital reconstruction Original Article Geon Woo Kim 1, Yong Chan
Archives of Craniofacial Surgery Arch Craniofac Surg Vol.19 No.4, 254-259 Usefulness of the orbicularis oculi myocutaneous flap in periorbital reconstruction Original Article Geon Woo Kim 1, Yong Chan
Mc Gregor Flap for Lower Eyelid Defect
 IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-issn: 2279-0853, p-issn: 2279-0861.Volume 16, Issue 4 Ver. V (April. 2017), PP 69-74 www.iosrjournals.org Mc Gregor Flap for Lower Eyelid Defect
IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-issn: 2279-0853, p-issn: 2279-0861.Volume 16, Issue 4 Ver. V (April. 2017), PP 69-74 www.iosrjournals.org Mc Gregor Flap for Lower Eyelid Defect
Frequently Asked Questions
 Ida Orengo, M.D. Mohsin Mir, M.D. Department of Dermatology 1977 Butler Boulevard, Suite E6.200 Houston, TX 77030 (713) 798-6925 / (713) 798-6624 telephone (713) 798-5535 fax Frequently Asked Questions
Ida Orengo, M.D. Mohsin Mir, M.D. Department of Dermatology 1977 Butler Boulevard, Suite E6.200 Houston, TX 77030 (713) 798-6925 / (713) 798-6624 telephone (713) 798-5535 fax Frequently Asked Questions
Know who is at risk: LOOK! for ABCDs, rapidly changing lesions, do a biopsy when indicated
 Lindy P. Fox, MD Assistant Professor Director, Hospital Consultation Service Department of Dermatology University of California, San Francisco Applies to adults without history of malignancy or premalignant
Lindy P. Fox, MD Assistant Professor Director, Hospital Consultation Service Department of Dermatology University of California, San Francisco Applies to adults without history of malignancy or premalignant
Entropion. Geoffrey J. Gladstone. Examination. Congenital Entropion-Epiblepharon. Etiology
 Entropion 2 Geoffrey J. Gladstone Entropion, or inward rotation of the eyelid margin, is an eyelid malposition commonly seen by general ophthalmologists and oculoplastic surgeons. The severe corneal irritation
Entropion 2 Geoffrey J. Gladstone Entropion, or inward rotation of the eyelid margin, is an eyelid malposition commonly seen by general ophthalmologists and oculoplastic surgeons. The severe corneal irritation
Merkel Cell Carcinoma Case # 2
 DISCHARGE SUMMARY Admitted: 10/11/2010 Discharged: 10/13/2010 Merkel Cell Carcinoma Case # 2 Chief Compliant: A 79 year old lady status post tumor on the scalp excision and left neck likely dissection
DISCHARGE SUMMARY Admitted: 10/11/2010 Discharged: 10/13/2010 Merkel Cell Carcinoma Case # 2 Chief Compliant: A 79 year old lady status post tumor on the scalp excision and left neck likely dissection
Regeneron and Sanofi are financial supporters of The Skin Cancer Foundation and collaborated in the development of this article. US-ONC /2018
 A D E E P E R L O O K When detected early, most cases of local cutaneous squamous cell carcinoma are easily treated and usually cured. But when they become more advanced, this second most common form of
A D E E P E R L O O K When detected early, most cases of local cutaneous squamous cell carcinoma are easily treated and usually cured. But when they become more advanced, this second most common form of
Interesting Case Series. Aggressive Tumor of the Midface
 Interesting Case Series Aggressive Tumor of the Midface Adrian Frunza, MD, Dragos Slavescu, MD, and Ioan Lascar, MD, PhD Bucharest Emergency Clinical Hospital, Bucharest University School of Medicine,
Interesting Case Series Aggressive Tumor of the Midface Adrian Frunza, MD, Dragos Slavescu, MD, and Ioan Lascar, MD, PhD Bucharest Emergency Clinical Hospital, Bucharest University School of Medicine,
Oncology and surgery. Dra. Irene Palacios. Clínica Universidad de Navarra
 Oncology and surgery Dra. Irene Palacios. Clínica Universidad de Navarra HOW TO MANAGE HIGH RISK SCC Yaouhi Gloria Xu Anokhi Jambusaria-Pahlajani HOW TO STAGE SCC Problem with tumor depth Often not posible
Oncology and surgery Dra. Irene Palacios. Clínica Universidad de Navarra HOW TO MANAGE HIGH RISK SCC Yaouhi Gloria Xu Anokhi Jambusaria-Pahlajani HOW TO STAGE SCC Problem with tumor depth Often not posible
LUMPS AND BUMPS: AN ORGANIZED APPROACH TO DIAGNOSIS AND MANAGEMENT
 LUMPS AND BUMPS: AN ORGANIZED APPROACH TO DIAGNOSIS AND MANAGEMENT Tammy P. Than, M.S., O.D., F.A.A.O. The University of Alabama at Birmingham / School of Optometry 1716 University Blvd. Birmingham, AL
LUMPS AND BUMPS: AN ORGANIZED APPROACH TO DIAGNOSIS AND MANAGEMENT Tammy P. Than, M.S., O.D., F.A.A.O. The University of Alabama at Birmingham / School of Optometry 1716 University Blvd. Birmingham, AL
Lisa M. DiFrancesco, M.D., Mark A. Codner, M.D., and Clinton D. McCord, M.D.
 CME Upper Eyelid Reconstruction Lisa M. DiFrancesco, M.D., Mark A. Codner, M.D., and Clinton D. McCord, M.D. Atlanta, Ga. Learning Objectives: After studying this article, the participant should be able
CME Upper Eyelid Reconstruction Lisa M. DiFrancesco, M.D., Mark A. Codner, M.D., and Clinton D. McCord, M.D. Atlanta, Ga. Learning Objectives: After studying this article, the participant should be able
Identifying Benign and Malignant Skin Lesions. No Disclosures. Common Benign Lesions. Benign Lesions 2/25/2018. Stucco Keratoses.
 Dermatology in Primary Care Identifying Benign and Malignant Skin Lesions Christy Quire Baker, APRN, FNP-BC, DCNP Dermatology Certified Nurse Practitioner No Disclosures Common Benign Lesions Seborrheic
Dermatology in Primary Care Identifying Benign and Malignant Skin Lesions Christy Quire Baker, APRN, FNP-BC, DCNP Dermatology Certified Nurse Practitioner No Disclosures Common Benign Lesions Seborrheic
Malignant Melanoma Early Stage. A guide for patients
 This melanoma patient brochure is designed to help educate melanoma patients and their caregivers. It was developed under the guidance of Dr. Michael Smylie, Professor, Department of Oncology, University
This melanoma patient brochure is designed to help educate melanoma patients and their caregivers. It was developed under the guidance of Dr. Michael Smylie, Professor, Department of Oncology, University
Melanoma and Dermoscopy. Disclosure Statement: ABCDE's of melanoma. Co-President, Usatine Media
 Melanoma and Dermoscopy Richard P. Usatine, MD, FAAFP Professor, Family and Community Medicine Professor, Dermatology and Cutaneous Surgery Medical Director, University Skin Clinic University of Texas
Melanoma and Dermoscopy Richard P. Usatine, MD, FAAFP Professor, Family and Community Medicine Professor, Dermatology and Cutaneous Surgery Medical Director, University Skin Clinic University of Texas
Periocular Skin Malignancies
 Periocular Skin Malignancies Jeffrey Buyten, MD Faculty Advisor: Vicente Resto, MD, PhD The University of Texas Medical Branch Department of Otolaryngology Grand Rounds Presentation May 8, 2008 Outline
Periocular Skin Malignancies Jeffrey Buyten, MD Faculty Advisor: Vicente Resto, MD, PhD The University of Texas Medical Branch Department of Otolaryngology Grand Rounds Presentation May 8, 2008 Outline
Modalities of Radiation
 Modalities of Radiation Superficial radiotherapy Orthovoltage Megavoltage Photons Electrons Brachytherapy Interstitial Moulds When to refer? The vast majority of skin cancers will be managed without any
Modalities of Radiation Superficial radiotherapy Orthovoltage Megavoltage Photons Electrons Brachytherapy Interstitial Moulds When to refer? The vast majority of skin cancers will be managed without any
Frozen section control of excision of eyelid basal cell carcinomas: 81/2 years' experience
 British Journal of Ophthalmology, 1989, 73, 328-332 Frozen section control of excision of eyelid basal cell carcinomas: 81/2 years' experience HELENA J FRANK From the Royal Victoria Hospital, Bournemouth
British Journal of Ophthalmology, 1989, 73, 328-332 Frozen section control of excision of eyelid basal cell carcinomas: 81/2 years' experience HELENA J FRANK From the Royal Victoria Hospital, Bournemouth
Pearls for Keeping it Simple in Cutaneous Reconstruction
 Pearls for Keeping it Simple in Cutaneous Reconstruction Jerry D. Brewer, MD, MS, FAAD brewer.jerry@mayo.edu Professor of Dermatology Division of Dermatologic Surgery Department of Dermatology Mayo Clinic
Pearls for Keeping it Simple in Cutaneous Reconstruction Jerry D. Brewer, MD, MS, FAAD brewer.jerry@mayo.edu Professor of Dermatology Division of Dermatologic Surgery Department of Dermatology Mayo Clinic
IT S FUNDAMENTAL MY DEAR WATSON! A SHERLOCKIAN APPROACH TO DERMATOLOGY
 IT S FUNDAMENTAL MY DEAR WATSON! A SHERLOCKIAN APPROACH TO DERMATOLOGY Skin, Bones, and other Private Parts Symposium Dermatology Lectures by Debra Shelby, PhD, DNP, FNP-BC, FADNP, FAANP Debra Shelby,
IT S FUNDAMENTAL MY DEAR WATSON! A SHERLOCKIAN APPROACH TO DERMATOLOGY Skin, Bones, and other Private Parts Symposium Dermatology Lectures by Debra Shelby, PhD, DNP, FNP-BC, FADNP, FAANP Debra Shelby,
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES
 PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES OCULAR ONCOLOGY PERIOCULAR CUTANEOUS MALIGNANCY Site Group: Ocular Periocular Cutaneous Malignancies Prepared by: Harmeet S. Gill MD, FRCSC
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES OCULAR ONCOLOGY PERIOCULAR CUTANEOUS MALIGNANCY Site Group: Ocular Periocular Cutaneous Malignancies Prepared by: Harmeet S. Gill MD, FRCSC
Anatomic Divisions. Ocular Surface. Intraocular. Orbital. Lacrimal. Eyelid
 Anatomic Divisions Ocular Surface Intraocular Orbital Lacrimal Eyelid Ocular Surface Melanocytic Squamous Neoplasia Lymphoid Melanocytic Nevi PAM (Primary Acquired Melanosis) Ocular Melanocytosis Melanoma
Anatomic Divisions Ocular Surface Intraocular Orbital Lacrimal Eyelid Ocular Surface Melanocytic Squamous Neoplasia Lymphoid Melanocytic Nevi PAM (Primary Acquired Melanosis) Ocular Melanocytosis Melanoma
Epithelial Cancer- NMSC & Melanoma
 Epithelial Cancer- NMSC & Melanoma David Chin MB, BCh, BAO, LRCP, LRCS (Ireland) MCh(MD), PhD (UQ), FRCS, FRACS (Plast) Plastic & Reconstructive Surgeon Visiting Scientist Melanoma Genomic Group & Drug
Epithelial Cancer- NMSC & Melanoma David Chin MB, BCh, BAO, LRCP, LRCS (Ireland) MCh(MD), PhD (UQ), FRCS, FRACS (Plast) Plastic & Reconstructive Surgeon Visiting Scientist Melanoma Genomic Group & Drug
Advances in Surgical Management of Primary Melanoma: Identifying Patients Who Need More than Conventional Wide Local Excision
 Advances in Surgical Management of Primary Melanoma: Identifying Patients Who Need More than Conventional Wide Local Excision Christopher J. Miller, MD Director of Penn Dermatology Oncology Center Associate
Advances in Surgical Management of Primary Melanoma: Identifying Patients Who Need More than Conventional Wide Local Excision Christopher J. Miller, MD Director of Penn Dermatology Oncology Center Associate
Using the Mohs Technique for Thin Melanomas
 Dermatology Associates Mohs Micrographic Surgery 2300 W Stone Drive Kingsport TN 37660 Telephone 423-246-4961 1-800-445-7274 (VA Toll Free) Fax 423-245-1200 Using the Mohs Technique for Thin Melanomas
Dermatology Associates Mohs Micrographic Surgery 2300 W Stone Drive Kingsport TN 37660 Telephone 423-246-4961 1-800-445-7274 (VA Toll Free) Fax 423-245-1200 Using the Mohs Technique for Thin Melanomas
Dermatology for the PCP Deanna G. Brown, MD, FAAD Susong Dermatology Consulting Staff at CHI Memorial
 Dermatology for the PCP Deanna G. Brown, MD, FAAD Susong Dermatology Consulting Staff at CHI Memorial Cutaneous Oncology for the PCP Deanna G. Brown, MD, FAAD Susong Dermatology Consulting Staff at CHI
Dermatology for the PCP Deanna G. Brown, MD, FAAD Susong Dermatology Consulting Staff at CHI Memorial Cutaneous Oncology for the PCP Deanna G. Brown, MD, FAAD Susong Dermatology Consulting Staff at CHI
Nonmelanoma skin cancers
 Skin cancer Philip Clarke Nonmelanoma skin cancers Treatment options Background Australia has one of the highest skin cancer rates in the world. Early detection and treatment of skin cancer is vital to
Skin cancer Philip Clarke Nonmelanoma skin cancers Treatment options Background Australia has one of the highest skin cancer rates in the world. Early detection and treatment of skin cancer is vital to
Section 1. Lids and lacrimal COPYRIGHTED MATERIAL
 Section Lids and lacrimal COPYRIGHTED MATERIAL Basal cell carcinoma Basal cell carcinoma (BCC) is a proliferation of the basal cells of the dermis in human skin. There are four recognised types of BCC:
Section Lids and lacrimal COPYRIGHTED MATERIAL Basal cell carcinoma Basal cell carcinoma (BCC) is a proliferation of the basal cells of the dermis in human skin. There are four recognised types of BCC:
MOHS MICROGRAPHIC SURGERY
 MOHS MICROGRAPHIC SURGERY What are the aims of this leaflet? This leaflet has been written to help you understand more about Mohs micrographic surgery. It tells you what it is, what is involved and what
MOHS MICROGRAPHIC SURGERY What are the aims of this leaflet? This leaflet has been written to help you understand more about Mohs micrographic surgery. It tells you what it is, what is involved and what
Eyelid Reconstruction December 2002
 TITLE: Eyelid Reconstruction SOURCE: Grand Rounds Presentation, UTMB, Dept. of Otolaryngology DATE: December 18, 2002 RESIDENT PHYSICIAN: Michael Underbrink, M.D. FACULTY ADVISOR: Karen Calhoun, M.D. SERIES
TITLE: Eyelid Reconstruction SOURCE: Grand Rounds Presentation, UTMB, Dept. of Otolaryngology DATE: December 18, 2002 RESIDENT PHYSICIAN: Michael Underbrink, M.D. FACULTY ADVISOR: Karen Calhoun, M.D. SERIES
Epidemiology. Objectives 8/28/2017
 Case based Discussion of Head and Neck Melanoma: Review of Epidemiology, Risk Factors, Identification, Treatments and Prevention Jacqueline M. Doucette MS FNP-C Objectives Define and identify melanoma
Case based Discussion of Head and Neck Melanoma: Review of Epidemiology, Risk Factors, Identification, Treatments and Prevention Jacqueline M. Doucette MS FNP-C Objectives Define and identify melanoma
Repair of Eyelid Trauma
 Repair of Eyelid Trauma Yunia Irawati, MD Plastic Reconstruction Division, Department of Ophthalmology FKUI / RSCM Introduction Eyelid trauma defined as a trauma to external surface of the lids with or
Repair of Eyelid Trauma Yunia Irawati, MD Plastic Reconstruction Division, Department of Ophthalmology FKUI / RSCM Introduction Eyelid trauma defined as a trauma to external surface of the lids with or
Melanoma. Kaushik Mukherjee MD A. Scott Pearson MD
 Melanoma Kaushik Mukherjee MD A. Scott Pearson MD Disclosures You still have to study Not all inclusive No Western blots Extensive use of Google Image Search and Sabiston Melanoma Basics 8 th most common
Melanoma Kaushik Mukherjee MD A. Scott Pearson MD Disclosures You still have to study Not all inclusive No Western blots Extensive use of Google Image Search and Sabiston Melanoma Basics 8 th most common
Basic Standards for Fellowship Training in Mohs Micrographic Surgery
 Basic Standards for Fellowship Training in Mohs Micrographic Surgery American Osteopathic Association and American Osteopathic College of Dermatologists September, 1992 BOT/93 BOT 7/2011, Eff. 7/2012 Basic
Basic Standards for Fellowship Training in Mohs Micrographic Surgery American Osteopathic Association and American Osteopathic College of Dermatologists September, 1992 BOT/93 BOT 7/2011, Eff. 7/2012 Basic
Principles of Facial Reconstruction After Mohs Surgery
 Objectives Principles of Facial Reconstruction After Mohs Surgery Identify important functional anatomy and aesthetic units of the face. Describe techniques used in facial reconstruction. Discuss postoperative
Objectives Principles of Facial Reconstruction After Mohs Surgery Identify important functional anatomy and aesthetic units of the face. Describe techniques used in facial reconstruction. Discuss postoperative
Coding Wars: The Coding and Documentation Weapons to Win the Battle
 Coding Wars: The Coding and Documentation Weapons to Win the Battle Howard W. Rogers M.D., Ph.D. Advanced Dermatology Norwich, CT rogershoward@sbcglobal.net Conflict of Interest Statement I have no relevant
Coding Wars: The Coding and Documentation Weapons to Win the Battle Howard W. Rogers M.D., Ph.D. Advanced Dermatology Norwich, CT rogershoward@sbcglobal.net Conflict of Interest Statement I have no relevant
Melanoma: The Basics. What is a melanocyte?
 Melanoma: The Basics What is a melanocyte? A melanocyte is a normal cell, found in the skin, which produces melanin. Melanin is a black or dark brown pigment that is seen in the skin, hair, and parts of
Melanoma: The Basics What is a melanocyte? A melanocyte is a normal cell, found in the skin, which produces melanin. Melanin is a black or dark brown pigment that is seen in the skin, hair, and parts of
Melanoma Case Scenario 1
 Melanoma Case Scenario 1 History and physical 11/5/16 Patient is a single, 48-year-old male in good health who presented to his primary physician for a yearly physical exam during which a 3.4 x 2.8 x 1.5
Melanoma Case Scenario 1 History and physical 11/5/16 Patient is a single, 48-year-old male in good health who presented to his primary physician for a yearly physical exam during which a 3.4 x 2.8 x 1.5
BACK TO TABLE OF CONTENTS FOCUS ON MELANOMA Oncology Annual Report BAPTIST HEALTH LEXINGTON ONCOLOGY ANNUAL REPORT
 FOCUS ON MELANOMA 2014 Oncology Annual Report BAPTIST HEALTH LEXINGTON 1 2014 ONCOLOGY ANNUAL REPORT TABLE OF CONTENTS What is melanoma?...3 Who is at risk for melanoma?...3 What causes melanoma?...4 What
FOCUS ON MELANOMA 2014 Oncology Annual Report BAPTIST HEALTH LEXINGTON 1 2014 ONCOLOGY ANNUAL REPORT TABLE OF CONTENTS What is melanoma?...3 Who is at risk for melanoma?...3 What causes melanoma?...4 What
Dermatological Manifestations in the Elderly. Sanjay Siddha Staff Dermatologist UHN & MSH
 Dermatological Manifestations in the Elderly Sanjay Siddha Staff Dermatologist UHN & MSH Disclosure No actual or potential conflicts of interest or commercial relationships to declare Objectives Recognize
Dermatological Manifestations in the Elderly Sanjay Siddha Staff Dermatologist UHN & MSH Disclosure No actual or potential conflicts of interest or commercial relationships to declare Objectives Recognize
A PRACTICAL APPROACH TO ATYPICAL MELANOCYTIC LESIONS BIJAN HAGHIGHI M.D, DIRECTOR OF DERMATOPATHOLOGY, ST. JOSEPH HOSPITAL
 A PRACTICAL APPROACH TO ATYPICAL MELANOCYTIC LESIONS BIJAN HAGHIGHI M.D, DIRECTOR OF DERMATOPATHOLOGY, ST. JOSEPH HOSPITAL OBJECTIVES Discuss current trends and changing concepts in our understanding of
A PRACTICAL APPROACH TO ATYPICAL MELANOCYTIC LESIONS BIJAN HAGHIGHI M.D, DIRECTOR OF DERMATOPATHOLOGY, ST. JOSEPH HOSPITAL OBJECTIVES Discuss current trends and changing concepts in our understanding of
David B. Troxel, MD. Common Medicolegal Situations: Misdiagnosis of Melanoma
 Common Medicolegal Situations: Misdiagnosis of Melanoma David B. Troxel, MD Medical Director, The Doctors Company, Napa, California Clinical Professor Emeritus, University of California at Berkeley Past
Common Medicolegal Situations: Misdiagnosis of Melanoma David B. Troxel, MD Medical Director, The Doctors Company, Napa, California Clinical Professor Emeritus, University of California at Berkeley Past
Collaborative Stage for TNM 7 - Revised 12/02/2009 [ Schema ]
![Collaborative Stage for TNM 7 - Revised 12/02/2009 [ Schema ]](/thumbs/82/86783199.jpg "Collaborative Stage for TNM 7 - Revised 12/02/2009 [ Schema ]") CS Tumor Size Collaborative Stage for TNM 7 - Revised 12/02/2009 [ Schema ] Note: the specific tumor size as documented in the medical record. If the ONLY information regarding tumor size is the physician's
CS Tumor Size Collaborative Stage for TNM 7 - Revised 12/02/2009 [ Schema ] Note: the specific tumor size as documented in the medical record. If the ONLY information regarding tumor size is the physician's
Index. Note: Page numbers of article titles are in boldface type. A Age as factor in melanoma, Anorectal melanoma RT for, 1035
 Index Note: Page numbers of article titles are in boldface type. A Age as factor in melanoma, 947 948 Anorectal melanoma RT for, 1035 B Bacille Calmette-Guerin (BCG) in melanoma, 1008 BCG. See Bacille
Index Note: Page numbers of article titles are in boldface type. A Age as factor in melanoma, 947 948 Anorectal melanoma RT for, 1035 B Bacille Calmette-Guerin (BCG) in melanoma, 1008 BCG. See Bacille
Skin Cancer Awareness
 Skin Cancer Awareness Presented by BHS Call: 800-327-2251 Visit: www.bhsonline.com 2016 BHS. All rights reserved. 1 Training Summary More than 3.5 million new cases of skin cancer will be diagnosed in
Skin Cancer Awareness Presented by BHS Call: 800-327-2251 Visit: www.bhsonline.com 2016 BHS. All rights reserved. 1 Training Summary More than 3.5 million new cases of skin cancer will be diagnosed in
Case Scenario 1. 7/13/12 Anterior floor of mouth biopsy: Infiltrating squamous cell carcinoma, not completely excised.
 Case Scenario 1 7/5/12 History A 51 year old white female presents with a sore area on the floor of her mouth. She claims the area has been sore for several months. She is a current smoker and user of
Case Scenario 1 7/5/12 History A 51 year old white female presents with a sore area on the floor of her mouth. She claims the area has been sore for several months. She is a current smoker and user of
Melanoma Case Scenario 1
 Melanoma Case Scenario 1 History and physical 11/5/16 Patient is a single, 48-year-old male in good health who presented to his primary physician for a yearly physical exam during which a 3.4 x 2.8 x 1.5
Melanoma Case Scenario 1 History and physical 11/5/16 Patient is a single, 48-year-old male in good health who presented to his primary physician for a yearly physical exam during which a 3.4 x 2.8 x 1.5
Primary Cutaneous Melanoma Pathology Reporting Proforma DD MM YYYY. *Tumour site. *Specimen laterality. *Specimen type
 Primary Cutaneous Melanoma Pathology Reporting Proforma Includes the International Collaboration on Cancer reporting dataset denoted by * Family name Given name(s) Date of birth DD MM YYYY Sex Male Female
Primary Cutaneous Melanoma Pathology Reporting Proforma Includes the International Collaboration on Cancer reporting dataset denoted by * Family name Given name(s) Date of birth DD MM YYYY Sex Male Female
I have a skin lump doc! What s next? 12 th August 2017 Dr. Sue-Ann Ho Ju Ee
 I have a skin lump doc! What s next? 12 th August 2017 Dr. Sue-Ann Ho Ju Ee Some thoughts Is this skin cancer? How common is this? How likely is this in this patient? What happens next if it s something
I have a skin lump doc! What s next? 12 th August 2017 Dr. Sue-Ann Ho Ju Ee Some thoughts Is this skin cancer? How common is this? How likely is this in this patient? What happens next if it s something
Contrast with Australian Guidelines A/Pr Pascale Guitera,
 Contrast with Australian Guidelines A/Pr Pascale Guitera, Dermatologist, Sydney University NO CONFLICT OF INTEREST Sydney Melanoma Diagnostic Centre, RPAH 2011 2008 225 pages 16 pages http://www.cancer.org.au/file/healthprofessionals/clinica
Contrast with Australian Guidelines A/Pr Pascale Guitera, Dermatologist, Sydney University NO CONFLICT OF INTEREST Sydney Melanoma Diagnostic Centre, RPAH 2011 2008 225 pages 16 pages http://www.cancer.org.au/file/healthprofessionals/clinica
Policy #: 127 Latest Review Date: June 2011
 Name of Policy: Mohs Micrographic Surgery Policy #: 127 Latest Review Date: June 2011 Category: Surgery Policy Grade: Active Policy but no longer scheduled for regular literature reviews and updates. Background/Definitions:
Name of Policy: Mohs Micrographic Surgery Policy #: 127 Latest Review Date: June 2011 Category: Surgery Policy Grade: Active Policy but no longer scheduled for regular literature reviews and updates. Background/Definitions:
Melanoma Quality Reporting
 Melanoma Quality Reporting September 1, 2013 December 31, 2016 Laurence McCahill, MD Surgical Oncologist Metro Health Surgical Oncology Metro Health Professional Building 2122 Health Drive SW Wyoming,
Melanoma Quality Reporting September 1, 2013 December 31, 2016 Laurence McCahill, MD Surgical Oncologist Metro Health Surgical Oncology Metro Health Professional Building 2122 Health Drive SW Wyoming,
Alcohol should be avoided for 3 days prior to surgery and 2 days after the procedure.
 Mohs Surgery Information Packet Be sure to bring the following to your appointment: Insurance Card Insurance Referral ( If required by your insurance) Name and address of your primary care provider as
Mohs Surgery Information Packet Be sure to bring the following to your appointment: Insurance Card Insurance Referral ( If required by your insurance) Name and address of your primary care provider as
S quamous cell carcinoma (SCC) is an invasive epithelial
 is an invasive epithelial") 1161 CLINICAL SCIENCE Squamous cell carcinoma of the eyelids M J Donaldson, T J Sullivan, K J Whitehead, R M Williamson... See end of article for authors affiliations... Correspondence to: Timothy J Sullivan,
1161 CLINICAL SCIENCE Squamous cell carcinoma of the eyelids M J Donaldson, T J Sullivan, K J Whitehead, R M Williamson... See end of article for authors affiliations... Correspondence to: Timothy J Sullivan,
Benign vs. Cancer. Oculofacial Biopsy. Evolution of skin cancer. Richard E. Castillo, OD, DO
 Oculofacial Biopsy Richard E. Castillo, OD, DO Benign vs. Cancer Evolution of skin cancer Metaplasia Dysplasia Carcinoma-in-situ Invasive carcinoma Intravasation Overview Preoperative Planning Choosing
Oculofacial Biopsy Richard E. Castillo, OD, DO Benign vs. Cancer Evolution of skin cancer Metaplasia Dysplasia Carcinoma-in-situ Invasive carcinoma Intravasation Overview Preoperative Planning Choosing
cally, a distinct superior crease of the forehead marks this spot. The hairline and
 4 Forehead The anatomical boundaries of the forehead unit are the natural hairline (in patients without alopecia), the zygomatic arch, the lower border of the eyebrows, and the nasal root (Fig. 4.1). The
4 Forehead The anatomical boundaries of the forehead unit are the natural hairline (in patients without alopecia), the zygomatic arch, the lower border of the eyebrows, and the nasal root (Fig. 4.1). The
Catholic University of Louvain, St - Luc University Hospital Head and Neck Oncology Programme. Anatomopathology. Pathology 1 Sept.
 Anatomopathology Pathology 1 Anatomopathology Biopsies Frozen section Surgical specimen Peculiarities for various tumor site References Pathology 2 Biopsies Minimum data, which should be given by the pathologist
Anatomopathology Pathology 1 Anatomopathology Biopsies Frozen section Surgical specimen Peculiarities for various tumor site References Pathology 2 Biopsies Minimum data, which should be given by the pathologist
WHAT DOES THE PATHOLOGY REPORT MEAN?
 Melanoma WHAT IS MELANOMA? Melanoma is a type of cancer that affects cells called melanocytes. These cells are found mainly in skin but also in the lining of other areas such as nose and rectum, and also
Melanoma WHAT IS MELANOMA? Melanoma is a type of cancer that affects cells called melanocytes. These cells are found mainly in skin but also in the lining of other areas such as nose and rectum, and also
Cancer of the Oral Cavity
 The International Federation of Head and Neck Oncologic Societies Current Concepts in Head and Neck Surgery and Oncology Cancer of the Oral Cavity Ashok Shaha Principals of Management of Oral Cancer A)
The International Federation of Head and Neck Oncologic Societies Current Concepts in Head and Neck Surgery and Oncology Cancer of the Oral Cavity Ashok Shaha Principals of Management of Oral Cancer A)