Glucose Lowering Medications and CV Risk Reduction: A New Era Jane EB Reusch MD ADA President for Medicine and Science
|
|
|
- Margery Hawkins
- 5 years ago
- Views:
Transcription





1 Glucose Lowering Medications and CV Risk Reduction: A New Era Jane EB Reusch MD ADA President for Medicine and Science Professor of Medicine, Division of Endocrinology, Metabolism and Diabetes and Associate Director Center for Women s Health Research University of Colorado Anschutz Medical Campus VA Staff Physician and Merit Investigator




2 CONSIDERATIONS: Patient Centered Phenotype Centered Glucose management is complex and imperfect New recommendations for the ~20% DM + CVD EASD-ADA updates
3 Disclosures Investigator Initiated Trial Support: Merck: Sitagliptin impact on exercise capacity (T2D) Funding: NIH, VA Consultant: Oramed Board of Directors ADA
4 Diabetes Shortens Life Span Age of onset Age of onset CVD CHF Tailored Therapy CVD CHF Tailored Therapy JAMA. 2015;314(1): doi: /jama Copyright 2017 American Medical Association. All rights reserved.
5 Premature mortality persists in people with DM Framingham Intensive multifactorial treatment (STENO-2) Preis, et al. Circulation (2011);119(13): Gaede P, et al. Diabetologia 2016; 59:
6 CVOT History: Why now? Worth it? In light of premature CV mortality we need to get this right Year Drug Safety concerns and response 1992 Human proinsulin Trials and development suspended CV issues and risk of acute myocardial infarction [a] 2005 Muraglitazar Risk of death, major CV adverse events, CHF [b] 2007 Rosiglitazone CV risk; withdrawn from market in many countries [c] 2008 FDA issued guidance document for the evaluation of CV risk [d] Studies are required to demonstrate that new anti-diabetic therapies do not increase CV risk in comparison with existing therapies a. Galloway JA, et al. Diab Care. 1992;15: ; b. Nissen SE, et al. JAMA. 2005;294: ; c. Nissen SE, et al. N Engl J Med. 2007;356: ; d. FDA Guidance For Industry, December
7 FDA Guidance: Cardiovascular Outcome Trials (CVOT) CVOT are designed and powered to assess non-inferiority versus placebo in addition to standard of care in a high risk CVD patient population (prior CVD ± high risk patients without proven CVD). Major endpoint composite of Major Adverse Cardiovascular Events: -Usual is 3 point MACE new nonfatal MI, new stroke, CV death based on careful adjudication to confirm accuracy of the events* Key understandings: -Powered for safety. -Studied populations provide data on SECONDARY PROTECTION. -Original studies not powered for subgroup analysis -Different design does not consistently enable direct comparison of results of one study to another.

8 Completed and Ongoing CVOTs 2018 by American Diabetes Association William T. Cefalu et al. Dia Care 2018;41:14-31
9 Antihyperglycemic Therapy: Safety and CVD/CHF considerations Insulin: - ORIGIN trial (Glargine U-100). - DEVOTE trial (Degludec vs. Glargine U-100). Thiazoledinediones: - PROACTIVE trial (Pioglitazone). - RECORD trial (Rosiglitazone). DPP-4 inhibitor: - SAVOR TIMI (Saxagliptin). - EXAMINE (Alogliptin). - TECOS (Sitagliptin) CVD Safety CVD Safety Heart Failure CVD Safety Heart Failure
10 DPP-4 Inhibitor CVD Outcome Trials Agent Population Composite Outcome Key Finding Heart Failure Saxagliptin SAVOR TIMI CVD or risk factors 3 point MACE Safety HR 1.00 Increased HR 1.27 Alogliptin EXAMINE CVD 3 point MACE Safety HR 0.96 Unchanged Sitiglipitin TECOS CVD 4 point MACE Safety HR 0.98 Unchanged Scirica BM et al. N Engl J Med. 2103;369: White WB et al. N Engl J Med. 2013;369: White WB et al. N Engl J Med. 2015;373: Pfeffer MA et al. N Engl J Med. 2015;373(23):
11 Beyond Safety SGLT2 inhibitors GLP1 Receptor Agonists
12 EMPA-REG: CV Death, MI, and Stroke Patients With Event/Analyzed Empagliflozin Placebo HR (95% CI) P Value 3-point MACE 490/ / ( )*.0382 CV death 172/ / ( ) <.0001 Non-fatal MI 213/ / ( ).2189 Non-fatal stroke 150/ / ( ).1638 Heart Failure Patients With Event, % 3% 7% *95.02% CI. Favors empagliflozin Favors placebo Zinman B, et al. N Engl J Med. 2015;373:

13 Patients With Event, % EMPA-REG: CV Death HR: 0.62 (95% CI: ); P <.0001 Placebo Empagliflozin Time, mo Zinman B, et al. N Engl J Med. 2015;373:
14 Patients With Event, % EMPA-REG: Hospitalization for Heart Failure Placebo HR: 0.65 (95% CI: ); P =.002 Empagliflozin Time, mo Cumulative incidence function Zinman B, et al. N Engl J Med. 2015;373:
15 CANVAS and CANVAS-R Trial Neal B et al. N Engl J Med. 2017;377:
16 CVD-REAL Study Real world study of 6 countries (US, Norway, Denmark, Sweden, Germany, UK) for relative rates death and hospitalization for heart failure in pts. newly started on SGLT2i or matched controls (n=154,528 in both). Baseline 3% HF, 13% CVD, 27% microvascular disease. Canagliflozin 53%, Dapagliflozin 42%, Empagliflozin 5%. Lowered relative rates in SGLT2i patients: Heart failure 0.61 (95% CI , p<0.001). All cause death 0.49 (95% CI , p<0.001). No significant heterogeneity by country. Kosiborod M et al. Circulation :
17 Who are the people in CVOT studies?
18 EMPA-REG: Baseline Characteristics T2D Placebo (n = 2333) Empagliflozin 10 mg (n = 2345) Empagliflozin 25 mg (n = 2342) HbA1c, % 8.08 (0.84) 8.07 (0.86) 8.06 (0.84) Time since diagnosis of type 2 diabetes, y (18.1) 406 (17.3) 434 (18.6) > 5 to (24.5) 585 (24.9) 590 (25.2) > 10 YEARS!! 1339 (57.4) 1354 (57.7) 1318 (56.3) Glucose-lowering medication* Metformin 1734 (74.3) 1729 (73.7) 1730 (73.9) Sulfonylurea 992 (42.5) 985 (42.0) 1029 (43.9) Thiazolidinedione 101 (4.3) 96 (4.1) 102 (4.4) Insulin 1135 (48.6) 1132 (48.3) 1120 (47.8) Mean daily dose, U 65 (50.6) 65 (47.9) 66 (48.9) *Medication taken alone or in combination Placebo, n = 1135; empagliflozin 10 mg, n = 1132; empagliflozin 25 mg, n = 1120 Data are n (%) or mean (SD) in patients treated with 1 dose of study drug. Zinman B, et al. N Engl J Med. 2015;373:
19 EMPA-REG: Baseline Characteristics CVD Characteristic Data are n (%) in patients treated with 1 dose of study drug. Placebo (n = 2333) Empagliflozin 10 mg (n = 2345) Empagliflozin 25 mg (n = 2342) Any CV risk factor, no. (%) 2307 (98.9) 2333 (99.5) 2324 (99.2) Coronary artery disease, no. (%) 1763 (75.6) 1782 (76.0) 1763 (75.3) Multi-vessel coronary artery disease, no. (%) 1100 (47.1) 1078 (46.0) 1101 (47.0) History of MI, no. (%) 1083 (46.4) 1107 (47.2) 1083 (46.2) Coronary artery bypass graft, no. (%) 563 (24.1) 594 (25.3) 581 (24.8) History of stroke, no. (%) 553 (23.7) 535 (22.8) 549 (23.4) Peripheral artery disease, no. (%) 479 (20.5) 465 (19.8) 517 (22.1) Single vessel coronary artery disease, no. (%) 238 (10.2) 258 (11.0) 240 (10.2) Cardiac failure*, no. (%) 244 (10.5) 240 (10.2) 222 (9.5) *Based on narrow standardized MedDRA query "cardiac failure." Zinman B, et al. N Engl J Med. 2015;373:
20 Patients With Event (%) LEADER: Primary Outcome a CV Death, Nonfatal MI, or Nonfatal Stroke HR: 0.87 (95% CI, ) p<.001 for noninferiority p=.01 for superiority Placebo Liraglutide CI upper limit <1.3 Liraglutide met the noninferiority criterion (did not increase the risk of CV events vs. placebo) (primary objective) Time From Randomization (Months) No. at risk Liraglutide Placebo CI upper limit <1.0 Liraglutide demonstrated superiority (reduced risk for CV events) vs. placebo a The primary composite outcome in the time-to-event analysis was the first occurrence of CV death, nonfatal MI, or nonfatal stroke The cumulative incidences were estimated with the use of the Kaplan-Meier method, and the hazard ratios with the use of the Cox proportional-hazard regression model The data analyses were truncated at 54 months, because <10% of the patients had an observation time beyond 54 months Marso SP, et al. Am Heart J. 2013;166:
21 Patients, % LEADER: Patient Population Majority of LEADER patients Are High Cardiovascular Risk 81.3 N = n = 7592 n = 1748 Previous CVD No Previous CVD Marso SP, et al. Am Heart J. 2013;166:
22 SUSTAIN-6 CV Outcomes: Semaglutide vs Placebo N= 3,297 Median f/u: 2.1 yr Hospitalization for HF: 3.6 vs 3.3 % HR 1.11 (95 % CI, ) Marso SP, et al. NEJM, 2016; Sept 16
23 Comparison of Major Outcome Relative Rates in LEADER, SUSTAIN 6 and EXSCEL Trials LEADER SUSTAIN 6 EXSCEL 3-point MACE Nonfatal MI Nonfatal Stroke Cardiac death Death any cause Hospital Heart Failure Nephropathy Retinopathy Red Color is statistically significant versus study control group.




24 Pharmacologic Approaches to Glycemic Treatment: Standards of Medical Care in Diabetes Diabetes Care 2018; 41 (Suppl. 1): S73-S85
25 Coronary Heart Disease: Recommendations creening In asymptomatic patients, routine screening for CAD is not recommended as it does not improve outcomes as long as ASCVD risk factors are treated. A Consider investigations for CAD in the presence of: Atypical cardiac symptoms (e.g. unexplained dyspnea, chest discomfort) Signs or symptoms of associated vascular disease including carotid bruits, transient ischemic attack, stroke, claudication or PAD EKG abnormalities (e.g. Q waves). E Cardiovascular Disease and Risk Management: Standards of Medical Care in Diabetes Diabetes Care 2018; 41 (Suppl. 1): S86-S104
26 Questions from Portland How do you respond to questions around these drugs that they are expensive blood pressure medicines? The FDA advisory committee was a very close vote for CV approval: Do you have any insight into that? Real-world A1c efficacy of these products fall short; should the real world CV outcomes also not also be questioned? For empagliflozin, the hazard ratios for CV deaths was only statistically significant in Latin America and Asian study sites, but not in Europe and N America. Do you have insight into that? How do these best-case drug interventions compare to best-case diet and exercise interventions?
27 2018 ADA Standards of Care Note/Disclosure: ADA/EASD just incorporated New trial results coming out every few months New FDA guidance yesterday

28 Previous Patient Centered Patient/Disease Features more stringent A1C 7% less stringent Risk of hypoglycemia/drug adverse effects low high Disease Duration newly diagnosed long-standing Life expectancy Important comorbidities long short absent Few/mild severe Established vascular complications absent Few/mild severe Patient attitude & expected treatment efforts highly motivated, adherent, excellent self-care capabilities less motivated, nonadherent, poor self-care capabilities Resources & support system readily available Glycemic Targets: Standards of Medical Care in Diabetes Diabetes Care 2018; 41 (Suppl. 1): S55-S64 limited



29 Publications Diabetologia Diabetes Care 2018;41:1-33 https//:doi.org/ /dci Copyright ADA & EASD 2018
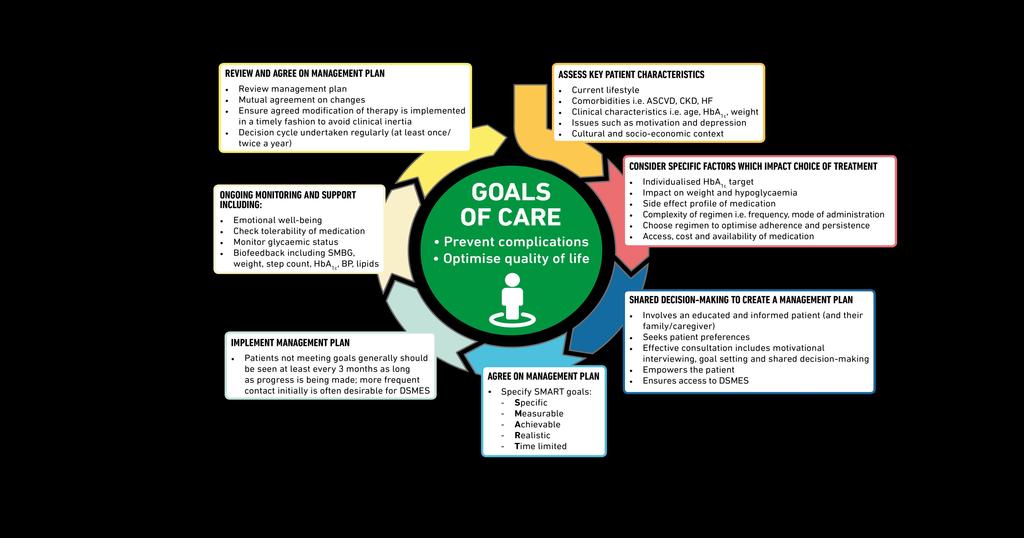
30 Putting the Patient at the Center of Care Copyright ADA & EASD 2018

31 Balancing Risks and Benefits for Personalized Goals More Stringent Control No hypoglycaemia Less complexity/polyphar macy Lifestyle or metformin only Short disease duration Long life expectancy No CVD Less Stringent Control History of severe hypoglycaemia High burden of therapy Longer disease duration Limited life expectancy Extensive co-morbidity CVD Copyright ADA & EASD 2018

32 Copyright ADA & EASD 2018
33 Improving Glycemic Management Focus on treatments for glycemic control Behavioral approaches Medications Metabolic surgery Addresses increasing complexity of patient centered therapeutic decisions in the context of expanding therapeutic options and new information on benefits and risks Copyright ADA & EASD 2018
34 Key Considerations Patient and Provider Barriers


35 Lifestyle as Medicine


36 Pharmacologic Approaches to Glycemic Treatment: Standards of Medical Care in Diabetes Diabetes Care 2018; 41 (Suppl. 1): S73-S85

37 JACC
38 LOOK Intensive Lifestyle AHEAD: Look Diabetes Support/Education Year 1yr Weight 8.6% 0.7% Year 1yr Fitness 20.4% 5% HR recovery P< A1c <7% 46-73% 45-50% Glucose/BP/Cholesterol % % CAD outcome 153 SNP-prediction unchanged 153 SNP-prediction unchanged CKD 0 63 per 100 person-years 0 91 cases per 100 per/yr Physical Function Decline Cognitive Function Fitness Preserve physical HRQoL Clinically significant depression Slowed progression* Favor ILI Favor ILI Favor ILI Favor ILI LOOK AHEAD: Look Again Diabetologia Aug;58(8): ; Curr Nutr Rep Dec;3(4): ; J Gerontol A Biol Sci Med Sci Mar;70(3):345-53*; Obesity. 2011;19:83 93; Eur J Prev Cardiol May;21(5):608-17;

39 Diabetes is usually for life
40 How to support lifestyle change? Providers need to reinforce the use lifestyle as medicine Messaging needs to be non-judgmental and realistic People with diabetes need a toolkit Use of Diabetes Self Management Education (DSME) and Certified Diabetes Educators (CDE) enhances success
41 Background on Behavioral Theory Human Behavior is influenced by motivation and ability Models vary, but generally identify factors related to motivation and ability: Motivation: Cognitive factors Environmental/Social factors Ability: Behavioral factors Bandura, Social Cognitive Theory, 1986


42 Human behavior is influenced by motivation and ability Provide a reminder Provide Training Courtesy of A Huebschmann Fogg Behavior Model,
43 Diabetes Self-Management Education and Support (DSMES) Is available to patients at critical times (repeated as needed) Individualized to the needs of the person, including language and culture Structured theory-driven written curriculum with supporting materials Delivered in group or individual settings by trained educators Promote healthy eating, physical activity, good medication-taking behavior, and increase self-efficacy Supports person and their family in developing attitudes, beliefs, knowledge and skills to self-manage diabetes Includes core content and monitoring of patient progress, including health status, quality of life. Evidence-based Copyright ADA & EASD 2018
44 Empathic patient-centered care Patients with diabetes often live with multiple chronic conditions Providers & health care systems should prioritise the delivery of empathic, individualised patient-centred care To determine what is the best management option for each patient, consider each individual s personal, social and biomedical context, his/her values, reasons he/she values the available options, and relative contribution of each option in terms of benefits, harms, costs and inconveniences. Copyright ADA & EASD 2018
45 5A s Adapted to be DM Specific Ask Ask for permission to discuss dietary habits and activity Explore readiness for change. Assess Assess lifestyle habits and history. Success and failures of prior attempts to alter behavior and perceived barriers for making changes. Advise Advise the patient about the health risks of poor lifestyle habits, the benefits of changes, the need for long-term strategy, and treatment options. Agree Agree on realistic expectations, targets, behavioral changes, and specific details of the treatment plan. Arrange/Assist Assist in identifying and addressing barriers; provide resources; assist in finding and consulting with appropriate providers; arrange regular follow up. Adapted From Obesity Algorithm Obesity Medicine Association courtesy of T Halliday.


46 If patients hear from a physician or other healthcare professional that they are overweight, they are ~6x more likely to perceive themselves as overweight ~2.5x more likely to attempt weight loss In this study 45.2% of individuals with BMI 25 had been told they were overweight 66.4% of individuals with BMI 30 had been told they were overweight Post RE, et al. Arch Intern Med Courtesy T Halliday



47 Tools: Use trustworthy sources People eat food (not carbohydrate, protein and fat):
48 Lifestyle take home points: Diet and Exercise are the cornerstones of successful diabetes management (on or off medication) People with diabetes and the providers need skills to implement sustainable lifestyle intervention Provider silence on lifestyle in unacceptable Patient support in the form of diabetes self management education is crucial (early and often) If at first you don t succeed-try something else


49 Lifestyle can add or subtract medications Still..Diabetes is progressive

50 UKPDS: Progressive Hyperglycemia Secondary to Beta-Cell Failure NOT your fault!
51 Clinical Inertia Clinical inertia: failure of healthcare providers to initiate or intensify therapy when indicated, due to: overestimation of care provided use of soft reasons to avoid intensification of therapy lack of education, training, and practice organization aimed at achieving therapeutic goals Reusch addition: health care system barriers adding burden to providers to intensify therapy Copyright ADA & EASD 2018
52 How are we doing?
53 Cardiovascular (CV) Risk Factor Targets and CV Disease Event Risk in Diabetes: We are not getting the job done Percent at target levels for any one, two, or all three factors among the 2016 persons with diabetes: Any 1 of 3 Any 2 of 3 3 of % 26.5% 7.2% Percent CVD risk reduction for being at target level among the 2016 persons with diabetes for each of the measures: Blood pressure LDL-C HBA1c 17% 33% 37% Percent lower adjusted risk of CVD events with one, two, or three risk factors at target level: Any 1 of 3 Any 2 of 3 3 of 3 36% 52% 62% Wong, et al. Diabetes Care 2016 May; 39(5)

54

55 Diabetes is VERY Demanding
56 Persistence and medication adherence Mean medication adherence rate 75%, average proportion of patients adherent to medication < 70%. Adherence slightly varies between orals vs injectable therapy and individual classes Discontinuation rates range from 10% to 60% (both in observational studies and in clinical trials) Copyright ADA & EASD 2018
57 Summary and Points for Discussion Traditional CVD risk factor modification remains the top priority for CVD prevention Healthy diet, increased physical activity and decreased sedentary activity are all effective THERAPY The primary goal for antihyperglycemic agents is to improve glucose control; combination therapy is often needed Polypharmacy, cost, durability, adherence and cost effectiveness must be considered* Studies demonstrating dual efficacy of antihyperglycemic agents on glucose and CVD/CHF change the landscape ONLY in people with high CHD risk or established CHD No data address the person with T2D and CHD on metformin with glucose at goal
58 Where are the gaps? Underlying biology: The mechanisms for the interaction between GLP-1RA and SGLT2I and decreased CVD and CHF risk need clarification Diabetes is a progressive disease: The timing and physiological context in which these drugs are administered needs to be tested (TZDs/Estrogen) No data demonstrating a role for these agent in primary prevention despite theoretical benefit whereas lifestyle change confers consistent benefits for primary prevention Health care delivery: Chronic disease with social stigma Glucose management is difficult in short patient visit PCPs and people with DM need support when starting GLP1 RA and SGLT2 inhibitors Reallocation of the $327 Billion / 1 in 4 US Health Care dollars


59 Consensus and Harmonization ADA-EASD ADA, AACE, Endocrine Society, AAFP scheduling discussion about Glycemic Targets ACC Expert Consensus Decision Pathways on Novel Pathways for Cardiovascular Risk Reduction in Patients with Type 2 Diabetes
60 Thank you! Questions?
61
62 Key points to emphasize Update informed by evidence generated in the past 2 years Greater focus on lifestyle interventions, with increased emphasis on weight loss and obesity management, including metabolic surgery Greater focus on patient related issues and self-management which have a major impact on success of any pharmacological interventions Preferred choices of glucose-lowering agents driven by new evidence from CVOTs and consideration of areas of major clinical need (for example weight and risk of hypoglycaemia) GLP-1 RAs are preferred to insulin as first injectable Copyright ADA & EASD 2018
DISCLOSURES. Learning objectives NAVIGATING THE TREATMENT OF TYPE 2 DIABETES: WHAT S NEW? Investigator Initiated Trial Support:
 NAVIGATING THE TREATMENT OF TYPE 2 DIABETES: WHAT S NEW? Jane E-B Reusch MD Professor of Medicine, Biochemistry and Bioengineering Associate Director Center for Women s Health Research University of Colorado
NAVIGATING THE TREATMENT OF TYPE 2 DIABETES: WHAT S NEW? Jane E-B Reusch MD Professor of Medicine, Biochemistry and Bioengineering Associate Director Center for Women s Health Research University of Colorado
Disclosures of Interest. Publications Diabetologia Key points to emphasize
 Disclosures of Interest No conflicts or disclosures How to Use the American Diabetes Association s Type 2 Diabetes Treatment Algorithm Rashida Downing, MD, FAAFP Primary Care Physician JenCare Medical
Disclosures of Interest No conflicts or disclosures How to Use the American Diabetes Association s Type 2 Diabetes Treatment Algorithm Rashida Downing, MD, FAAFP Primary Care Physician JenCare Medical
Can We Reduce Heart Failure by Treating Diabetes? CVOT Data on SGLT2 Inhibitors and GLP-1Receptor Agonists
 Can We Reduce Heart Failure by Treating Diabetes? CVOT Data on SGLT2 Inhibitors and GLP-1Receptor Agonists Robert R. Henry, MD Professor of Medicine University of California, San Diego Relevant Conflict
Can We Reduce Heart Failure by Treating Diabetes? CVOT Data on SGLT2 Inhibitors and GLP-1Receptor Agonists Robert R. Henry, MD Professor of Medicine University of California, San Diego Relevant Conflict
Management of Type 2 Diabetes Cardiovascular Outcomes Trials Tom Blevins MD Texas Diabetes and Endocrinology Austin, Texas
 Management of Type 2 Diabetes Cardiovascular Outcomes Trials 2018 Tom Blevins MD Texas Diabetes and Endocrinology Austin, Texas Speaker Disclosure Dr. Blevins has disclosed that he has received grant support
Management of Type 2 Diabetes Cardiovascular Outcomes Trials 2018 Tom Blevins MD Texas Diabetes and Endocrinology Austin, Texas Speaker Disclosure Dr. Blevins has disclosed that he has received grant support
Update on Diabetes Cardiovascular Outcome Trials
 Update on Diabetes Cardiovascular Outcome Trials Jay S. Skyler, MD, MACP Division of Endocrinology, Diabetes, and Metabolism and Diabetes Research Institute University of Miami Miller School of Medicine
Update on Diabetes Cardiovascular Outcome Trials Jay S. Skyler, MD, MACP Division of Endocrinology, Diabetes, and Metabolism and Diabetes Research Institute University of Miami Miller School of Medicine
LATE BREAKING STUDIES IN DM AND CAD. Will this change the guidelines?
 LATE BREAKING STUDIES IN DM AND CAD Will this change the guidelines? Objectives 1. Discuss current guidelines for prevention of CHD in diabetes. 2. Discuss the FDA Guidance for Industry regarding evaluating
LATE BREAKING STUDIES IN DM AND CAD Will this change the guidelines? Objectives 1. Discuss current guidelines for prevention of CHD in diabetes. 2. Discuss the FDA Guidance for Industry regarding evaluating
Cardiologists and HbA1c: Novel Diabetes Drugs and Cardiovascular Disease Outcomes
 Biomarkers 2018 Cardiologists and HbA1c: Novel Diabetes Drugs and Cardiovascular Disease Outcomes Gregg C. Fonarow, MD, FACC, FAHA, FHFSA Elliot Corday Professor of Cardiovascular Medicine UCLA Division
Biomarkers 2018 Cardiologists and HbA1c: Novel Diabetes Drugs and Cardiovascular Disease Outcomes Gregg C. Fonarow, MD, FACC, FAHA, FHFSA Elliot Corday Professor of Cardiovascular Medicine UCLA Division
Update on Cardiovascular Outcome Trials in Diabetes Jay S. Skyler, MD, MACP
 Update on Cardiovascular Outcome Trials in Diabetes Jay S. Skyler, MD, MACP Division of Endocrinology, Diabetes, and Metabolism and Diabetes Research InsAtute University of Miami Miller School of Medicine
Update on Cardiovascular Outcome Trials in Diabetes Jay S. Skyler, MD, MACP Division of Endocrinology, Diabetes, and Metabolism and Diabetes Research InsAtute University of Miami Miller School of Medicine
Case Studies in Type 2 Diabetes Mellitus: Focus on Cardiovascular Outcomes Trials
 Case Studies in Type 2 Diabetes Mellitus: Focus on Cardiovascular Outcomes Trials Louis Kuritzky MD Clinical Assistant Professor Emeritus Department of Community Health and Family Medicine College of Medicine
Case Studies in Type 2 Diabetes Mellitus: Focus on Cardiovascular Outcomes Trials Louis Kuritzky MD Clinical Assistant Professor Emeritus Department of Community Health and Family Medicine College of Medicine
Updates in Diabetes and Cardiovascular Disease Management: Are You Making the Link?
 Updates in Diabetes and Cardiovascular Disease Management: Are You Making the Link? Denise Kolanczyk, PharmD, BCPS AQ Cardiology 1 Erika Hellenbart, PharmD, BCPS 2 Jennifer D Souza, PharmD, CDE, BC ADM
Updates in Diabetes and Cardiovascular Disease Management: Are You Making the Link? Denise Kolanczyk, PharmD, BCPS AQ Cardiology 1 Erika Hellenbart, PharmD, BCPS 2 Jennifer D Souza, PharmD, CDE, BC ADM
Diabete: terapia nei pazienti a rischio cardiovascolare
 Diabete: terapia nei pazienti a rischio cardiovascolare Giorgio Sesti Università Magna Graecia di Catanzaro Cardiovascular mortality in relation to diabetes mellitus and a prior MI: A Danish Population
Diabete: terapia nei pazienti a rischio cardiovascolare Giorgio Sesti Università Magna Graecia di Catanzaro Cardiovascular mortality in relation to diabetes mellitus and a prior MI: A Danish Population
Diabetes and Heart Failure: The Role of SGLT2 Inhibitors
 22 nd Annual Heart Failure 2018 Symposium Diabetes and Heart Failure: The Role of SGLT2 Inhibitors Gregg C. Fonarow, MD, FACC, FAHA, FHFSA Elliot Corday Professor of Cardiovascular Medicine UCLA Division
22 nd Annual Heart Failure 2018 Symposium Diabetes and Heart Failure: The Role of SGLT2 Inhibitors Gregg C. Fonarow, MD, FACC, FAHA, FHFSA Elliot Corday Professor of Cardiovascular Medicine UCLA Division
CANVAS Program Independent commentary
 CANVAS Program Independent commentary Cliff Bailey Aston University, Birmingham, UK 2017 Disclosures and disclaimers Clifford J Bailey CJB has attended advisory boards, undertaken ad hoc consultancy, received
CANVAS Program Independent commentary Cliff Bailey Aston University, Birmingham, UK 2017 Disclosures and disclaimers Clifford J Bailey CJB has attended advisory boards, undertaken ad hoc consultancy, received
Cardiovascular Outcomes With Newer Diabetes Drugs: Results From The EMPA-REG and LEADER Trials
 Cardiovascular Outcomes With Newer Diabetes Drugs: Results From The EMPA-REG and LEADER Trials Rajiv Roy, MD Endocrinology Sharp Rees-Stealy Medical Group Background Between 1990 and 2010: Incidence of
Cardiovascular Outcomes With Newer Diabetes Drugs: Results From The EMPA-REG and LEADER Trials Rajiv Roy, MD Endocrinology Sharp Rees-Stealy Medical Group Background Between 1990 and 2010: Incidence of
Overview T2DM medications. Winnie Ho
 Overview T2DM medications Winnie Ho Diabetes in Australia 1.7 million Australians with diabetes, of these 85% have T2DM 2-fold excess risk CV death in patients with diabetes Risk factor for progression
Overview T2DM medications Winnie Ho Diabetes in Australia 1.7 million Australians with diabetes, of these 85% have T2DM 2-fold excess risk CV death in patients with diabetes Risk factor for progression
Current principles of diabetes management
 Current principles of diabetes management Prof. Martin Haluzík, MD, DSc. 3 Department of Medicine, General University Hospital and 1st Faculty of Medicine, Charles University in Prague, Czech Republic
Current principles of diabetes management Prof. Martin Haluzík, MD, DSc. 3 Department of Medicine, General University Hospital and 1st Faculty of Medicine, Charles University in Prague, Czech Republic
Diabetes new challenges, new agents, new order
 Diabetes new challenges, new agents, new order Ken Earle St Georges University Hospitals NHS Foundation Trust Overview Cardiovascular disease unmet needs Treating evident and residual risk Integrating
Diabetes new challenges, new agents, new order Ken Earle St Georges University Hospitals NHS Foundation Trust Overview Cardiovascular disease unmet needs Treating evident and residual risk Integrating
Endocrinologist Sweetgrass Endocrinology
 Endocrinologist Sweetgrass Endocrinology Sanders, Cummings Ask Justice Department to Investigate Insulin Prices The Department of Justice and the FTC are asked to investigate whether Lilly, Novo Nordisk,
Endocrinologist Sweetgrass Endocrinology Sanders, Cummings Ask Justice Department to Investigate Insulin Prices The Department of Justice and the FTC are asked to investigate whether Lilly, Novo Nordisk,
OLD AND NEW DRUGS FOR CONTROLING DIABETES THERAPEUTIC CLASSES AND MECHANISM OF ACTION
 OLD AND NEW DRUGS FOR CONTROLING DIABETES THERAPEUTIC CLASSES AND MECHANISM OF ACTION Biljana Parapid, MD, PhD, FESC Belgrade University School of Medicine, Belgrade (Serbia) @biljana_parapid COI International
OLD AND NEW DRUGS FOR CONTROLING DIABETES THERAPEUTIC CLASSES AND MECHANISM OF ACTION Biljana Parapid, MD, PhD, FESC Belgrade University School of Medicine, Belgrade (Serbia) @biljana_parapid COI International
Diabetes and Cardiovascular Risk Management Denise M. Kolanczyk, PharmD, BCPS-AQ Cardiology
 Diabetes and Cardiovascular Risk Management Denise M. Kolanczyk, PharmD, BCPS-AQ Cardiology Disclosures In compliance with the accrediting board policies, the American Diabetes Association requires the
Diabetes and Cardiovascular Risk Management Denise M. Kolanczyk, PharmD, BCPS-AQ Cardiology Disclosures In compliance with the accrediting board policies, the American Diabetes Association requires the
Top HF Trials to Impact Your Practice
 Top HF Trials to Impact Your Practice Biykem Bozkurt, MD, FACC The Mary and Gordon Cain Chair & Professor of Medicine Medical Care Line Executive, DeBakey VA Medical Center, Director, Winters Center for
Top HF Trials to Impact Your Practice Biykem Bozkurt, MD, FACC The Mary and Gordon Cain Chair & Professor of Medicine Medical Care Line Executive, DeBakey VA Medical Center, Director, Winters Center for
No Increased Cardiovascular Risk for Lixisenatide in ELIXA
 ON ISSUES IN THE MANAGEMENT OF TYPE 2 DIABETES JUNE 2015 Coverage of data from ADA 2015, June 5 9 in Boston, Massachusetts No Increased Cardiovascular Risk for Lixisenatide in ELIXA First Cardiovascular
ON ISSUES IN THE MANAGEMENT OF TYPE 2 DIABETES JUNE 2015 Coverage of data from ADA 2015, June 5 9 in Boston, Massachusetts No Increased Cardiovascular Risk for Lixisenatide in ELIXA First Cardiovascular
La lezione dei trials di safety cardiovascolare. Edoardo Mannucci
 La lezione dei trials di safety cardiovascolare Edoardo Mannucci Conflitti di interessi Negli ultimi due anni, E. Mannucci ha ricevuto compensi per relazioni e/o consulenze da: Abbott, AstraZeneca, Boehringer
La lezione dei trials di safety cardiovascolare Edoardo Mannucci Conflitti di interessi Negli ultimi due anni, E. Mannucci ha ricevuto compensi per relazioni e/o consulenze da: Abbott, AstraZeneca, Boehringer
Medical therapy advances London/Manchester RCP February/June 2016
 Medical therapy advances London/Manchester RCP February/June 2016 Advances in medical therapies for diabetes mellitus Duality of interest: The speaker or institutions with which he is associated has received
Medical therapy advances London/Manchester RCP February/June 2016 Advances in medical therapies for diabetes mellitus Duality of interest: The speaker or institutions with which he is associated has received
Sodium-Glucose Co-Transporter 2 (SGLT-2) Inhibitors Drug Class Prior Authorization Protocol
 Inhibitors Drug Class Prior Authorization Protocol") Sodium-Glucose Co-Transporter 2 (SGLT-2) Inhibitors Drug Class Prior Authorization Protocol Line of Business: Medicaid P&T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has
Sodium-Glucose Co-Transporter 2 (SGLT-2) Inhibitors Drug Class Prior Authorization Protocol Line of Business: Medicaid P&T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has
What s New in Type 2 Diabetes? 2018 Diabetes Updates
 What s New in Type 2 Diabetes? 2018 Diabetes Updates Gretchen Ray, PharmD, PhC, BCACP, CDE Associate Professor, UNM College of Pharmacy January 28, 2018 gray@salud.unm.edu OBJECTIVES Describe the most
What s New in Type 2 Diabetes? 2018 Diabetes Updates Gretchen Ray, PharmD, PhC, BCACP, CDE Associate Professor, UNM College of Pharmacy January 28, 2018 gray@salud.unm.edu OBJECTIVES Describe the most
ESC GUIDELINES ON DIABETES AND CARDIOVASCULAR DISEASES
 ESC GUIDELINES ON DIABETES AND CARDIOVASCULAR DISEASES Pr. Michel KOMAJDA Institute of Cardiology - IHU ICAN Pitie Salpetriere Hospital - University Pierre and Marie Curie, Paris (France) DEFINITION A
ESC GUIDELINES ON DIABETES AND CARDIOVASCULAR DISEASES Pr. Michel KOMAJDA Institute of Cardiology - IHU ICAN Pitie Salpetriere Hospital - University Pierre and Marie Curie, Paris (France) DEFINITION A
LEADER Liraglutide and cardiovascular outcomes in type 2 diabetes
 LEADER Liraglutide and cardiovascular outcomes in type 2 diabetes Presented at DSBS seminar on mediation analysis August 18 th Søren Rasmussen, Novo Nordisk. LEADER CV outcome study To determine the effect
LEADER Liraglutide and cardiovascular outcomes in type 2 diabetes Presented at DSBS seminar on mediation analysis August 18 th Søren Rasmussen, Novo Nordisk. LEADER CV outcome study To determine the effect
Cardiovascular Impact of Medications for Treating Type 2 Diabetes
 Friday CME Breakfast Lecture Cardiovascular Impact of Medications for Treating Type 2 Diabetes Thomas Blevins, MD Endocrinologist, Private Practice Texas Diabetes and Endocrinology Austin, Texas Educational
Friday CME Breakfast Lecture Cardiovascular Impact of Medications for Treating Type 2 Diabetes Thomas Blevins, MD Endocrinologist, Private Practice Texas Diabetes and Endocrinology Austin, Texas Educational
The EMPA-REG OUTCOME trial: Design and results. David Fitchett, MD University of Toronto, Canada
 The EMPA-REG OUTCOME trial: Design and results David Fitchett, MD University of Toronto, Canada Asian Cardio Diabetes Forum April 23 24, 2016 Kuala Lumpur, Malaysia Life Expectancy Is Reduced by ~12 Years
The EMPA-REG OUTCOME trial: Design and results David Fitchett, MD University of Toronto, Canada Asian Cardio Diabetes Forum April 23 24, 2016 Kuala Lumpur, Malaysia Life Expectancy Is Reduced by ~12 Years
2019 Update on Recent Guideline Releases for Diabetes, Hypertension, and Dyslipidemia: Can We, Please, All Just Get on the Same Page?!
 2019 Update on Recent Guideline Releases for Diabetes, Hypertension, and Dyslipidemia: Can We, Please, All Just Get on the Same Page?! Jeremy L. Johnson, PharmD, BCACP, CDE, BC-ADM Assistant Professor,
2019 Update on Recent Guideline Releases for Diabetes, Hypertension, and Dyslipidemia: Can We, Please, All Just Get on the Same Page?! Jeremy L. Johnson, PharmD, BCACP, CDE, BC-ADM Assistant Professor,
Can Treating Diabetes with SGLT2 inhibitors Prevent Heart Failure?
 UCSD Hawaii 2017 Symposium Can Treating Diabetes with SGLT2 inhibitors Prevent Heart Failure? Gregg C. Fonarow, MD, FACC, FAHA Elliot Corday Professor of Cardiovascular Medicine UCLA Division of Cardiology
UCSD Hawaii 2017 Symposium Can Treating Diabetes with SGLT2 inhibitors Prevent Heart Failure? Gregg C. Fonarow, MD, FACC, FAHA Elliot Corday Professor of Cardiovascular Medicine UCLA Division of Cardiology
Preventing Serious Health Consequences of Type 2 Diabetes
 Preventing Serious Health Consequences of Type 2 Diabetes The Evidence Hertzel C. Gerstein MD MSc FRCPC Professor and Population Health Institute Chair in Diabetes Research McMaster University and Hamilton
Preventing Serious Health Consequences of Type 2 Diabetes The Evidence Hertzel C. Gerstein MD MSc FRCPC Professor and Population Health Institute Chair in Diabetes Research McMaster University and Hamilton
Update on Cardiovascular Outcome Trials in Diabetes. Rury R. Holman, FMedSci NIHR Senior Investigator 11 th February 2013
 Update on Cardiovascular Outcome Trials in Diabetes Rury R. Holman, FMedSci NIHR Senior Investigator 11 th February 2013 Residual Vascular Risk in People with Diabetes 2 Analyses based on 530,083 participants
Update on Cardiovascular Outcome Trials in Diabetes Rury R. Holman, FMedSci NIHR Senior Investigator 11 th February 2013 Residual Vascular Risk in People with Diabetes 2 Analyses based on 530,083 participants
New Strategies for Cardiovascular Risk reduction in Diabetes
 New Strategies for Cardiovascular Risk reduction in Diabetes Dr. Godwin LEUNG Tat Chi MB ChB(HK), MRCP (UK), FHKCP, FHKAM (Medicine) FRCP (Glasg), FACC Specialist in Cardiology % event as first CV event
New Strategies for Cardiovascular Risk reduction in Diabetes Dr. Godwin LEUNG Tat Chi MB ChB(HK), MRCP (UK), FHKCP, FHKAM (Medicine) FRCP (Glasg), FACC Specialist in Cardiology % event as first CV event
Cardiovascular Benefits of Two Classes of Antihyperglycemic Medications
 Cardiovascular Benefits of Two Classes of Antihyperglycemic Medications Nathan Woolever, Pharm.D., Resident Pharmacist Pharmacy Grand Rounds November 6 th, 2018 Franciscan Healthcare La Crosse, WI 2017
Cardiovascular Benefits of Two Classes of Antihyperglycemic Medications Nathan Woolever, Pharm.D., Resident Pharmacist Pharmacy Grand Rounds November 6 th, 2018 Franciscan Healthcare La Crosse, WI 2017
Stephen Clement M.D. CDE Medical Director, Endocrine Services Inova Fairfax Hospital
 Stephen Clement M.D. CDE Medical Director, Endocrine Services Inova Fairfax Hospital Financial Disclosures Consulting Panel for GSK on Hepatitis Vaccines Case Study BH is a 67 y/o female with T2 DM for
Stephen Clement M.D. CDE Medical Director, Endocrine Services Inova Fairfax Hospital Financial Disclosures Consulting Panel for GSK on Hepatitis Vaccines Case Study BH is a 67 y/o female with T2 DM for
What s New in Type 2 Diabetes? 2018 Diabetes Updates
 What s New in Type 2 Diabetes? 2018 Diabetes Updates Jessica Conklin, PharmD, PhC, BCACP, CDE, AAHIP Associate Professor, UNM College of Phar macy jeconklin@salud.unm.edu Luis Gonzales, PharmD, PhC UNM
What s New in Type 2 Diabetes? 2018 Diabetes Updates Jessica Conklin, PharmD, PhC, BCACP, CDE, AAHIP Associate Professor, UNM College of Phar macy jeconklin@salud.unm.edu Luis Gonzales, PharmD, PhC UNM
01/09/2017. Outline. SGLT 2 inhibitor? Diabetes Patients: Complex and Heterogeneous. Association between diabetes and cardiovascular events
 MICROVASCULAR COMPLICATIONS Incidence of outcome g 1 Cardioprotective Effects of SGLT2s Relevant for Which T2 Diabetes Patient? SGLT 2 inhibitor? 58 year old, waist circumference 5 cm, PMH: IHD On statin,
MICROVASCULAR COMPLICATIONS Incidence of outcome g 1 Cardioprotective Effects of SGLT2s Relevant for Which T2 Diabetes Patient? SGLT 2 inhibitor? 58 year old, waist circumference 5 cm, PMH: IHD On statin,
In compliance with the accrediting board policies, the American Diabetes Association requires the following disclosure to the participants:
 In compliance with the accrediting board policies, the American Diabetes Association requires the following disclosure to the participants: Entity Activity Financial Consideration Comments Novo Nordisk
In compliance with the accrediting board policies, the American Diabetes Association requires the following disclosure to the participants: Entity Activity Financial Consideration Comments Novo Nordisk
Disclosures. Diabetes and Cardiovascular Risk Management. Learning Objectives. Atherosclerotic Cardiovascular Disease
 Disclosures Diabetes and Cardiovascular Risk Management Tony Hampton, MD, MBA Medical Director Advocate Aurora Operating System Advocate Aurora Healthcare Downers Grove, IL No conflicts or disclosures
Disclosures Diabetes and Cardiovascular Risk Management Tony Hampton, MD, MBA Medical Director Advocate Aurora Operating System Advocate Aurora Healthcare Downers Grove, IL No conflicts or disclosures
CV outcomes Studies and Implications for diabetes management. Seraj Abualnaja, MD, FRCPC Consultant Interventional cardiologist DSFH
 CV outcomes Studies and Implications for diabetes management Seraj Abualnaja, MD, FRCPC Consultant Interventional cardiologist DSFH Case 49 y female with the following medical problems DM typ2 Hypertension
CV outcomes Studies and Implications for diabetes management Seraj Abualnaja, MD, FRCPC Consultant Interventional cardiologist DSFH Case 49 y female with the following medical problems DM typ2 Hypertension
Oral Hypoglycemics and Risk of Adverse Cardiac Events: A Summary of the Controversy
 Oral Hypoglycemics and Risk of Adverse Cardiac Events: A Summary of the Controversy Jeffrey Boord, MD, MPH Advances in Cardiovascular Medicine Kingston, Jamaica December 7, 2012 VanderbiltHeart.com Outline
Oral Hypoglycemics and Risk of Adverse Cardiac Events: A Summary of the Controversy Jeffrey Boord, MD, MPH Advances in Cardiovascular Medicine Kingston, Jamaica December 7, 2012 VanderbiltHeart.com Outline
Cardiologists and HbA1c: Novel Diabetes Drugs and the Cardiologist as Diabetician
 Biomarkers 2019 Cardiologists and HbA1c: Novel Diabetes Drugs and the Cardiologist as Diabetician Gregg C. Fonarow, MD, FACC, FAHA, FHFSA Elliot Corday Professor of Cardiovascular Medicine UCLA Division
Biomarkers 2019 Cardiologists and HbA1c: Novel Diabetes Drugs and the Cardiologist as Diabetician Gregg C. Fonarow, MD, FACC, FAHA, FHFSA Elliot Corday Professor of Cardiovascular Medicine UCLA Division
Hanyang University Guri Hospital Chang Beom Lee
 Hanyang University Guri Hospital Chang Beom Lee Meal prayer, Van Brekelenkam 17 th C Introduction 2012 ADA/EASD Position Statement Proper Patients for Pioglitazone β-cell Preservation by Pioglitazone Benefit
Hanyang University Guri Hospital Chang Beom Lee Meal prayer, Van Brekelenkam 17 th C Introduction 2012 ADA/EASD Position Statement Proper Patients for Pioglitazone β-cell Preservation by Pioglitazone Benefit
Diabetes Guidelines in View of Recent Clinical Trials Are They Still Applicable?
 Diabetes Guidelines in View of Recent Clinical Trials Are They Still Applicable? Jay S. Skyler, MD, MACP Division of Endocrinology, Diabetes, and Metabolism and Diabetes Research Institute University of
Diabetes Guidelines in View of Recent Clinical Trials Are They Still Applicable? Jay S. Skyler, MD, MACP Division of Endocrinology, Diabetes, and Metabolism and Diabetes Research Institute University of
The Diabetes Link to Heart Disease
 The Diabetes Link to Heart Disease Anthony Abe DeSantis, MD September 18, 2015 University of WA Division of Metabolism, Endocrinology and Nutrition Oswald Toosweet Case #1 68 yo M with T2DM Diagnosed DM
The Diabetes Link to Heart Disease Anthony Abe DeSantis, MD September 18, 2015 University of WA Division of Metabolism, Endocrinology and Nutrition Oswald Toosweet Case #1 68 yo M with T2DM Diagnosed DM
Disclosures. Objectives. Bryan Cardiology Conference DM2 & Cardiovascular Outcome Trials 8/28/2017
 Bryan Cardiology Conference DM2 & Cardiovascular Outcome Trials Shannon Wakeley MD Complete Endocrinology 9/2/2017 Disclosures Speakers Bureau: Astra Zeneca, Sanofi, Abbvie, Boehringer-Ingelheim, Medtronic,
Bryan Cardiology Conference DM2 & Cardiovascular Outcome Trials Shannon Wakeley MD Complete Endocrinology 9/2/2017 Disclosures Speakers Bureau: Astra Zeneca, Sanofi, Abbvie, Boehringer-Ingelheim, Medtronic,
Navigating the New Options for the Management of Type 2 Diabetes
 Navigating the New Options for the Management of Type 2 Diabetes Clinical Associate Professor Mark Kennedy Department of General Practice, University of Melbourne Chair, Primary Care Diabetes Society of
Navigating the New Options for the Management of Type 2 Diabetes Clinical Associate Professor Mark Kennedy Department of General Practice, University of Melbourne Chair, Primary Care Diabetes Society of
IMPROVED DIAGNOSIS OF TYPE 2 DIABETES AND TAILORING MEDICATIONS
 IMPROVED DIAGNOSIS OF TYPE 2 DIABETES AND TAILORING MEDICATIONS Dr Bidhu Mohapatra, MBBS, MD, FRACP Consultant Physician Endocrinology and General Medicine Introduction 382 million people affected by diabetes
IMPROVED DIAGNOSIS OF TYPE 2 DIABETES AND TAILORING MEDICATIONS Dr Bidhu Mohapatra, MBBS, MD, FRACP Consultant Physician Endocrinology and General Medicine Introduction 382 million people affected by diabetes
Eugene Barrett M.D., Ph.D. University of Virginia 6/18/2007. Diagnosis and what is it Glucose Tolerance Categories FPG
 Diabetes Mellitus: Update 7 What is the unifying basis of this vascular disease? Eugene J. Barrett, MD, PhD Professor of Internal Medicine and Pediatrics Director, Diabetes Center and GCRC Health System
Diabetes Mellitus: Update 7 What is the unifying basis of this vascular disease? Eugene J. Barrett, MD, PhD Professor of Internal Medicine and Pediatrics Director, Diabetes Center and GCRC Health System
Newer Diabetes Treatments Drug Class Update with New Drug Evaluation: Semaglutide and Ertugliflozin
 Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35 Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35 Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
The Death of Sulfonylureas? A Review of New Diabetes Medications
 The Death of Sulfonylureas? A Review of New Diabetes Medications Kelly Hoenig, Pharm.D., BCPS Cedar Rapids Family Medicine Residency 2/4/17 Objectives Review GLP-1 Agonists, DPP-IV Inhibitors and SGLT-2
The Death of Sulfonylureas? A Review of New Diabetes Medications Kelly Hoenig, Pharm.D., BCPS Cedar Rapids Family Medicine Residency 2/4/17 Objectives Review GLP-1 Agonists, DPP-IV Inhibitors and SGLT-2
Empagliflozin (Jardiance ) for the treatment of type 2 diabetes mellitus, the EMPA REG OUTCOME study
 for the treatment of type 2 diabetes mellitus, the EMPA REG OUTCOME study") Empagliflozin (Jardiance ) for the treatment of type 2 diabetes mellitus, the EMPA REG OUTCOME study POSITION STATEMENT: Clinicians should continue to follow MHRA advice and NICE technology appraisal guidance
Empagliflozin (Jardiance ) for the treatment of type 2 diabetes mellitus, the EMPA REG OUTCOME study POSITION STATEMENT: Clinicians should continue to follow MHRA advice and NICE technology appraisal guidance
Diabetes Drugs and Cardiac Disease. Disclosures
 Diabetes Drugs and Cardiac Disease Robert J. Rushakoff, MD Professor of Medicine University of California, San Francisco robert.rushakoff@ucsf.edu Disclosures None 1 Written Comments As I have said every
Diabetes Drugs and Cardiac Disease Robert J. Rushakoff, MD Professor of Medicine University of California, San Francisco robert.rushakoff@ucsf.edu Disclosures None 1 Written Comments As I have said every
GLP 1 agonists Winning the Losing Battle. Dr Bernard SAMIA. KCS Congress: Impact through collaboration
 GLP 1 agonists Winning the Losing Battle Dr Bernard SAMIA KCS Congress: Impact through collaboration CONTACT: Tel. +254 735 833 803 Email: kcardiacs@gmail.com Web: www.kenyacardiacs.org Disclosures I have
GLP 1 agonists Winning the Losing Battle Dr Bernard SAMIA KCS Congress: Impact through collaboration CONTACT: Tel. +254 735 833 803 Email: kcardiacs@gmail.com Web: www.kenyacardiacs.org Disclosures I have
Current Updates & Challenges In Managing Diabetes in CVD
 Current Updates & Challenges In Managing Diabetes in CVD Preventive Cardiovascular Conference 2016 Instituit Jantung Negara 12 th November 2016 Nor Azmi Kamaruddin Diabetes Clinic Department of Medicine
Current Updates & Challenges In Managing Diabetes in CVD Preventive Cardiovascular Conference 2016 Instituit Jantung Negara 12 th November 2016 Nor Azmi Kamaruddin Diabetes Clinic Department of Medicine
Drug Class Update with New Drug Evaluation: Non-insulin Diabetes Treatments (SGLT-2 Inhibitors and GLP-1 Receptor Agonists)
") Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35 Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35 Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Review of FDA Guidance on Cardiovascular Outcomes for Diabetes Medication Trials and Application to Clinical Management
 Katherine S. O Neal Pharm.D., MBA, BCACP, CDE, BC-ADM, AE-C Associate Professor The University of Oklahoma Health Sciences Center College of Pharmacy Department of Internal Medicine Oklahoma City, OK Member,
Katherine S. O Neal Pharm.D., MBA, BCACP, CDE, BC-ADM, AE-C Associate Professor The University of Oklahoma Health Sciences Center College of Pharmacy Department of Internal Medicine Oklahoma City, OK Member,
Managing Perioperative Diabetes What s new? Kathryn A. Myers MD FRCPC Chair Chief Division of GIM Professor of Medicine Western University
 Managing Perioperative Diabetes What s new? Kathryn A. Myers MD FRCPC Chair Chief Division of GIM Professor of Medicine Western University Objectives: By the end of this session, you will be able to: Identify
Managing Perioperative Diabetes What s new? Kathryn A. Myers MD FRCPC Chair Chief Division of GIM Professor of Medicine Western University Objectives: By the end of this session, you will be able to: Identify
The Flozins Quest for Clarity?
 The Flozins Quest for Clarity? Choosing Wisely with Academic Detailing 2018 ARE THEY THE REAL DEAL Disclosure statements The Academic Detailing Service is operated by Dalhousie Continuing Professional
The Flozins Quest for Clarity? Choosing Wisely with Academic Detailing 2018 ARE THEY THE REAL DEAL Disclosure statements The Academic Detailing Service is operated by Dalhousie Continuing Professional
Educational Objectives
 Educational Objectives Recognize the rationale for cardiovascular outcome trials (CVOTs) in T2DM and review data from recent CVOTs of anti hyperglycemic agents Examine alignment of managed care T2DM treatment
Educational Objectives Recognize the rationale for cardiovascular outcome trials (CVOTs) in T2DM and review data from recent CVOTs of anti hyperglycemic agents Examine alignment of managed care T2DM treatment
Management of Type 2 Diabetes Mellitus. Heather Corn, MD, MS Endocrinology, Diabetes, and Metabolism
 Management of Type 2 Diabetes Mellitus Heather Corn, MD, MS Endocrinology, Diabetes, and Metabolism Disclosures Working for Intermountain Healthcare Some of the views represented are the opinion of ABIM-certified
Management of Type 2 Diabetes Mellitus Heather Corn, MD, MS Endocrinology, Diabetes, and Metabolism Disclosures Working for Intermountain Healthcare Some of the views represented are the opinion of ABIM-certified
Update Diabetes Therapie. Marc Y Donath
 Update Diabetes Therapie Marc Y Donath Recent CV outcome studies in Diabetes N Engl J Med. 2015 373:2117-28 (Empa-Reg outcome study) N Engl J Med. 2016 June 13 (LEADER trial) N Engl J Med. 2017 June 12
Update Diabetes Therapie Marc Y Donath Recent CV outcome studies in Diabetes N Engl J Med. 2015 373:2117-28 (Empa-Reg outcome study) N Engl J Med. 2016 June 13 (LEADER trial) N Engl J Med. 2017 June 12
Diabetes and the Heart
 Diabetes and the Heart Jeffrey Boord, MD, MPH Advances in Cardiovascular Medicine Kingston, Jamaica December 6, 2012 Outline Screening for diabetes in patients with CAD Screening for CAD in patients with
Diabetes and the Heart Jeffrey Boord, MD, MPH Advances in Cardiovascular Medicine Kingston, Jamaica December 6, 2012 Outline Screening for diabetes in patients with CAD Screening for CAD in patients with
Newer Therapies for Type 2 Diabetes
 Newer Therapies for Type 2 Diabetes Sandra Indacochea Sobel, MD Clinical Assistant Professor of Medicine Clinical Chief of Endocrinology, UPMC Mercy Division of Endocrinology, Diabetes, and Metabolism
Newer Therapies for Type 2 Diabetes Sandra Indacochea Sobel, MD Clinical Assistant Professor of Medicine Clinical Chief of Endocrinology, UPMC Mercy Division of Endocrinology, Diabetes, and Metabolism
Terapia con agonisti GLP1 e outcome cardiovascolare. Edoardo Mannucci
 Terapia con agonisti GLP e outcome cardiovascolare Edoardo Mannucci Conflitti di interessi Negli ultimi due anni, E. Mannucci ha ricevuto compensi per relazioni e/o consulenze da: Abbott, AstraZeneca,
Terapia con agonisti GLP e outcome cardiovascolare Edoardo Mannucci Conflitti di interessi Negli ultimi due anni, E. Mannucci ha ricevuto compensi per relazioni e/o consulenze da: Abbott, AstraZeneca,
Cardiovascular Consequences of Diabetes Mellitus
 Cardiovascular Consequences of Diabetes Mellitus William J. Elliott, M.D., Ph.D. 05 MAY 18 Disclosure Statement The speaker s research and educational activities have been supported in the past (but NOT
Cardiovascular Consequences of Diabetes Mellitus William J. Elliott, M.D., Ph.D. 05 MAY 18 Disclosure Statement The speaker s research and educational activities have been supported in the past (but NOT
Why is Earlier and More Aggressive Treatment of T2 Diabetes Better?
 Blood glucose (mmol/l) Why is Earlier and More Aggressive Treatment of T2 Diabetes Better? Disclosures Dr Kennedy has provided CME, been on advisory boards or received travel or conference support from:
Blood glucose (mmol/l) Why is Earlier and More Aggressive Treatment of T2 Diabetes Better? Disclosures Dr Kennedy has provided CME, been on advisory boards or received travel or conference support from:
When Statins Aren t Enough: Appropriate Therapies for High-Risk Patients with Diabetes
 When Statins Aren t Enough: Appropriate Therapies for High-Risk Patients with Diabetes Kim K. Birtcher, MS, PharmD, AACC, FNLA, CLS, BCPS (AQ-Cardiology), CDE Clinical Professor University of Houston College
When Statins Aren t Enough: Appropriate Therapies for High-Risk Patients with Diabetes Kim K. Birtcher, MS, PharmD, AACC, FNLA, CLS, BCPS (AQ-Cardiology), CDE Clinical Professor University of Houston College
T2 Diabetes in Sep-16. Stephen Leow Disclosures. Why do we treat diabetes? Agenda. Targets
 Stephen Leow Disclosures I have received honoraria, sat on the advisory boards or received grants from Novo Nordisk, Sanofi Aventis, Eli Lilly, Boehringer Ingleheim, Jansenn Cilag, Mundipharma, BioCSL,
Stephen Leow Disclosures I have received honoraria, sat on the advisory boards or received grants from Novo Nordisk, Sanofi Aventis, Eli Lilly, Boehringer Ingleheim, Jansenn Cilag, Mundipharma, BioCSL,
Heart Failure Management in T2 DM A Practical Approach. David Fitchett MD St Michael s Hospital Toronto
 Heart Failure Management in T2 DM A Practical Approach David Fitchett MD St Michael s Hospital Toronto Faculty: Faculty Disclosure David Fitchett MD,, FRCP(C) Associate Professor of Medicine, University
Heart Failure Management in T2 DM A Practical Approach David Fitchett MD St Michael s Hospital Toronto Faculty: Faculty Disclosure David Fitchett MD,, FRCP(C) Associate Professor of Medicine, University
Type 2 Diabetes: Where Do We Start with Treatment? DIABETES EDUCATION. Diabetes Mellitus: Complications and Co-Morbid Conditions
 Diabetes Mellitus: Complications and Co-Morbid Conditions ADA Guidelines for Glycemic Control: 2016 Retinopathy Between 2005-2008, 28.5% of patients with diabetes 40 years and older diagnosed with diabetic
Diabetes Mellitus: Complications and Co-Morbid Conditions ADA Guidelines for Glycemic Control: 2016 Retinopathy Between 2005-2008, 28.5% of patients with diabetes 40 years and older diagnosed with diabetic
A Guidance Statement from the American College of Physicians
 Hemoglobin A1c Targets for Glycemic Control with Pharmacologic Therapy in Non-Pregnant Adults with Type 2 Diabetes Mellitus: A Guidance Statement from the American College of Physicians Timothy J. Wilt,
Hemoglobin A1c Targets for Glycemic Control with Pharmacologic Therapy in Non-Pregnant Adults with Type 2 Diabetes Mellitus: A Guidance Statement from the American College of Physicians Timothy J. Wilt,
The Clinical Unmet need in the patient with Diabetes and ACS
 The Clinical Unmet need in the patient with Diabetes and ACS Professor Kausik Ray (UK) BSc(hons), MBChB, MD, MPhil, FRCP (lon), FRCP (ed), FACC, FESC, FAHA Diabetes is a global public health challenge
The Clinical Unmet need in the patient with Diabetes and ACS Professor Kausik Ray (UK) BSc(hons), MBChB, MD, MPhil, FRCP (lon), FRCP (ed), FACC, FESC, FAHA Diabetes is a global public health challenge
MANAGING THE HYPERGLYCEMIA OF DIABETES: SHOULD CVOTs IMPACT MEDICATIONS?
 MANAGING THE HYPERGLYCEMIA OF DIABETES: SHOULD CVOTs IMPACT MEDICATIONS? Ralph A. DeFronzo, M.D. Professor of Medicine Chief, Diabetes Division University of Texas Health Science Center San Antonio, Texas
MANAGING THE HYPERGLYCEMIA OF DIABETES: SHOULD CVOTs IMPACT MEDICATIONS? Ralph A. DeFronzo, M.D. Professor of Medicine Chief, Diabetes Division University of Texas Health Science Center San Antonio, Texas
Diabetes Management in CAD Patients. Stuart R. Chipkin, MD Research Professor School of Public Health and Health Sciences University of Massachusetts
 Diabetes Management in CAD Patients Stuart R. Chipkin, MD Research Professor School of Public Health and Health Sciences University of Massachusetts Disclosure Stuart R. Chipkin, MD, FACE Nothing to disclose
Diabetes Management in CAD Patients Stuart R. Chipkin, MD Research Professor School of Public Health and Health Sciences University of Massachusetts Disclosure Stuart R. Chipkin, MD, FACE Nothing to disclose
NEW DIABETES CARE MEDICATIONS
 NEW DIABETES CARE MEDICATIONS James Bonucchi DO, ECNU, FACE Adult Medicine and Endocrinology Specialists Disclosures Speakers bureau Sanofi AZ BI Diabetes Diabetes cost ADA 2017 data Ever increasing disorder.
NEW DIABETES CARE MEDICATIONS James Bonucchi DO, ECNU, FACE Adult Medicine and Endocrinology Specialists Disclosures Speakers bureau Sanofi AZ BI Diabetes Diabetes cost ADA 2017 data Ever increasing disorder.
Multi-factor approach to reduce cardiovascular risk in diabetes
 Multi-factor approach to reduce cardiovascular risk in diabetes Prof. Nicola Napoli, MD PhD Division of Endocrinology and Diabetes Università Campus Bio-Medico di Roma Washington University in St Louis
Multi-factor approach to reduce cardiovascular risk in diabetes Prof. Nicola Napoli, MD PhD Division of Endocrinology and Diabetes Università Campus Bio-Medico di Roma Washington University in St Louis
Clinical Relevance of Blood Pressure Lowering Effect of Modern Antidiabetic Drugs
 Clinical Relevance of Blood Pressure Lowering Effect of Modern Antidiabetic Drugs Professor Guntram Schernthaner Medical University of Vienna, Austria guntram.schernthaner@meduniwien.ac.at Agenda Glucose
Clinical Relevance of Blood Pressure Lowering Effect of Modern Antidiabetic Drugs Professor Guntram Schernthaner Medical University of Vienna, Austria guntram.schernthaner@meduniwien.ac.at Agenda Glucose
Diabetes Mellitus: Implications of New Clinical Trials and New Medications
 Diabetes Mellitus: Implications of New Clinical Trials and New Medications Estimates of Diagnosed Diabetes in Adults, 2005 Alka M. Kanaya, MD Asst. Professor of Medicine UCSF, Primary Care CME October
Diabetes Mellitus: Implications of New Clinical Trials and New Medications Estimates of Diagnosed Diabetes in Adults, 2005 Alka M. Kanaya, MD Asst. Professor of Medicine UCSF, Primary Care CME October
Glycemic control a matter of life and death
 Glycemic control a matter of life and death Linda Garcia Mellbin MD PhD Specialist in Cardiology & Internal medicine Dep of Cardiology Karolinska University Hospital /Karolinska Institutet Mortality (%)
Glycemic control a matter of life and death Linda Garcia Mellbin MD PhD Specialist in Cardiology & Internal medicine Dep of Cardiology Karolinska University Hospital /Karolinska Institutet Mortality (%)
Help the Heart. An Update on GLP-1 Agonists and SGLT2 Inhibitors. Tara Hawley, PharmD PGY1 Pharmacy Resident Mayo Clinic Health System Eau Claire
 Help the Heart An Update on GLP-1 Agonists and SGLT2 Inhibitors Tara Hawley, PharmD PGY1 Pharmacy Resident Mayo Clinic Health System Eau Claire Mayo Clinic Grand Rounds May 16, 2017 2017 MFMER slide-1
Help the Heart An Update on GLP-1 Agonists and SGLT2 Inhibitors Tara Hawley, PharmD PGY1 Pharmacy Resident Mayo Clinic Health System Eau Claire Mayo Clinic Grand Rounds May 16, 2017 2017 MFMER slide-1
Gli endpoint micro-vascolari nei trial di outcome cardiovascolare
 Gli endpoint micro-vascolari nei trial di outcome cardiovascolare Giorgio Sesti University Magna Graecia of Catanzaro ITALY Potenziali conflitti di interesse Il Prof Giorgio Sesti dichiara di aver ricevuto
Gli endpoint micro-vascolari nei trial di outcome cardiovascolare Giorgio Sesti University Magna Graecia of Catanzaro ITALY Potenziali conflitti di interesse Il Prof Giorgio Sesti dichiara di aver ricevuto
Regulatory Hurdles for Drug Approvals
 Regulatory Hurdles for Drug Approvals William R. Hiatt, MD Professor of Medicine/Cardiology University of Colorado School of Medicine President, CPC Clinical Research 25 min Conflicts CPC Clinical Research
Regulatory Hurdles for Drug Approvals William R. Hiatt, MD Professor of Medicine/Cardiology University of Colorado School of Medicine President, CPC Clinical Research 25 min Conflicts CPC Clinical Research
Cardiovascular disease and diabetes Vascular harmony
 Cardiovascular disease and diabetes 2018 Vascular harmony Robert Chilton Professor of Medicine University of Texas Health Science Center Director of Cardiac Catheterization labs Director of clinical proteomics
Cardiovascular disease and diabetes 2018 Vascular harmony Robert Chilton Professor of Medicine University of Texas Health Science Center Director of Cardiac Catheterization labs Director of clinical proteomics
Halting the Rise, Newest Non- Insulin Options for Lowering A1c
 Halting the Rise, Newest Non- Insulin Options for Lowering A1c Alecia Rottinghaus, PharmD PGY-1 Pharmacy Resident Iowa City Veterans Affairs Health Care System January 29 th, 2019 Disclosures Alecia Rottinghaus
Halting the Rise, Newest Non- Insulin Options for Lowering A1c Alecia Rottinghaus, PharmD PGY-1 Pharmacy Resident Iowa City Veterans Affairs Health Care System January 29 th, 2019 Disclosures Alecia Rottinghaus
The Alphabet Soup of Diabetes. Egils Bogdanovics M.D. Hungerford Diabetes Center
 The Alphabet Soup of Diabetes Egils Bogdanovics M.D. Hungerford Diabetes Center Insulin: January 11, 1922 12 year old Leonard Thompson, on a starvation diet for 2 years received his first insulin injection
The Alphabet Soup of Diabetes Egils Bogdanovics M.D. Hungerford Diabetes Center Insulin: January 11, 1922 12 year old Leonard Thompson, on a starvation diet for 2 years received his first insulin injection
The Burden of the Diabetic Heart
 The Burden of the Diabetic Heart Dr. Ghaida Kaddaha (MBBS, MRCP-UK, FRCP-london) Diabetes Unit Rashid Hospital Dubai U.A.E Risk of CVD in Diabetes Morbidity and mortality from CVD is 2-4 fold higher than
The Burden of the Diabetic Heart Dr. Ghaida Kaddaha (MBBS, MRCP-UK, FRCP-london) Diabetes Unit Rashid Hospital Dubai U.A.E Risk of CVD in Diabetes Morbidity and mortality from CVD is 2-4 fold higher than
The Many Faces of T2DM in Long-term Care Facilities
 The Many Faces of T2DM in Long-term Care Facilities Question #1 Which of the following is a risk factor for increased hypoglycemia in older patients that may suggest the need to relax hyperglycemia treatment
The Many Faces of T2DM in Long-term Care Facilities Question #1 Which of the following is a risk factor for increased hypoglycemia in older patients that may suggest the need to relax hyperglycemia treatment
Diabetes and Heart Failure: Challenges and Opportunities
 AHA Get With The Guidelines-Heart Failure Webinar Diabetes and Heart Failure: Challenges and Opportunities Gregg C. Fonarow, MD, FACC, FAHA, FHFSA Elliot Corday Professor of Cardiovascular Medicine UCLA
AHA Get With The Guidelines-Heart Failure Webinar Diabetes and Heart Failure: Challenges and Opportunities Gregg C. Fonarow, MD, FACC, FAHA, FHFSA Elliot Corday Professor of Cardiovascular Medicine UCLA
Evaluating the Cardiovascular Benefits of Antidiabetic Medications
 Evaluating the Cardiovascular Benefits of Antidiabetic Medications Target Audience: Pharmacists ACPE#: 0202-0000-18-054-L01-P Activity Type: Application-based Disclosures Stuart T. Haines has no relevant
Evaluating the Cardiovascular Benefits of Antidiabetic Medications Target Audience: Pharmacists ACPE#: 0202-0000-18-054-L01-P Activity Type: Application-based Disclosures Stuart T. Haines has no relevant
Halting the Rise, Newest Non- Insulin Options for Lowering A1c
 Halting the Rise, Newest Non- Insulin Options for Lowering A1c Alecia Rottinghaus, PharmD PGY-1 Pharmacy Resident Iowa City Veterans Affairs Health Care System January 29 th, 2019 Disclosures Alecia Rottinghaus
Halting the Rise, Newest Non- Insulin Options for Lowering A1c Alecia Rottinghaus, PharmD PGY-1 Pharmacy Resident Iowa City Veterans Affairs Health Care System January 29 th, 2019 Disclosures Alecia Rottinghaus
Individualizing Management of T2DM in the Hospital Setting to Reduce Macro and Microvascular Complications
 Individualizing Management of T2DM in the Hospital Setting to Reduce Macro and Microvascular Complications This CME activity is provided by Integrity Continuing Education. This CEU/CNE activity is co-provided
Individualizing Management of T2DM in the Hospital Setting to Reduce Macro and Microvascular Complications This CME activity is provided by Integrity Continuing Education. This CEU/CNE activity is co-provided
3. Cardiovascular Disease?
 Swiss recommendations 2016 Swiss Society of Endocrinology and Diabetology 1. Deficiency? Basal Premixed- Basal + GLP-1 RA (Xultophy ) or Basal Bolus 2. egfr < 30 ml/min? 3. Cardiovascular Disease? 4. Heart
Swiss recommendations 2016 Swiss Society of Endocrinology and Diabetology 1. Deficiency? Basal Premixed- Basal + GLP-1 RA (Xultophy ) or Basal Bolus 2. egfr < 30 ml/min? 3. Cardiovascular Disease? 4. Heart
TYP 2 DIABETES. Marc Donath
 TYP 2 DIABETES Marc Donath Treatment of Typ 2 Diabetes GLP-1 Anti-IL-1β Insulin sulfonylureas Metformin UCP-1 IL-1β Sport SGLT2i Bariatric surgery Cardiomyocytes Control Glucose Dyntar et al. Diabetes
TYP 2 DIABETES Marc Donath Treatment of Typ 2 Diabetes GLP-1 Anti-IL-1β Insulin sulfonylureas Metformin UCP-1 IL-1β Sport SGLT2i Bariatric surgery Cardiomyocytes Control Glucose Dyntar et al. Diabetes
CARDIOVASCULAR RISK FACTOR CONTROL IN TYPE 2 DIABETES MELLITUS AND NEW TRIAL EVIDENCE
 CARDIOVASCULAR RISK FACTOR CONTROL IN TYPE 2 DIABETES MELLITUS AND NEW TRIAL EVIDENCE *Peter M. Nilsson Department of Clinical Sciences, Lund University, Skåne University Hospital, Malmö, Sweden *Correspondence
CARDIOVASCULAR RISK FACTOR CONTROL IN TYPE 2 DIABETES MELLITUS AND NEW TRIAL EVIDENCE *Peter M. Nilsson Department of Clinical Sciences, Lund University, Skåne University Hospital, Malmö, Sweden *Correspondence
10/27/2011. Challenges in Anti-diabetic Global Drug Development A Shift from Surrogate to Outcome Trials. Disclaimer
 Challenges in Anti-diabetic Global Drug Development A Shift from Surrogate to Outcome Trials Eckhard Leifke, MD PhD Senior Medical Director Takeda Global Research Development Center, Inc. Presentation
Challenges in Anti-diabetic Global Drug Development A Shift from Surrogate to Outcome Trials Eckhard Leifke, MD PhD Senior Medical Director Takeda Global Research Development Center, Inc. Presentation
Content Development Committee
 1 Content Development Committee Cardiologists: Family Physicians: Shaun Goodman, MD, MSc, FRCPC, FACC, FESC, FAHA, FCCS (Chair) Associate Head, Division of Cardiology, St. Michael s Hospital Professor,
1 Content Development Committee Cardiologists: Family Physicians: Shaun Goodman, MD, MSc, FRCPC, FACC, FESC, FAHA, FCCS (Chair) Associate Head, Division of Cardiology, St. Michael s Hospital Professor,
DIABETES DEBATE - IS NEW BETTER?
 DIABETES DEBATE - IS NEW BETTER? WHAT MEDICATION CLASS AFTER METFORMIN TO CONTROL BLOOD SUGAR Dr. Lydia Hatcher, MD, CCFP, FCFP, CHE, D-CAPM Associate Clinical Professor of Family Medicine, McMaster Chief
DIABETES DEBATE - IS NEW BETTER? WHAT MEDICATION CLASS AFTER METFORMIN TO CONTROL BLOOD SUGAR Dr. Lydia Hatcher, MD, CCFP, FCFP, CHE, D-CAPM Associate Clinical Professor of Family Medicine, McMaster Chief