IMPROVED DIAGNOSIS OF TYPE 2 DIABETES AND TAILORING MEDICATIONS
|
|
|
- Mitchell Pope
- 5 years ago
- Views:
Transcription
1 IMPROVED DIAGNOSIS OF TYPE 2 DIABETES AND TAILORING MEDICATIONS Dr Bidhu Mohapatra, MBBS, MD, FRACP Consultant Physician Endocrinology and General Medicine
2 Introduction 382 million people affected by diabetes worldwide 592 millions by 2035 Recent Australian survey: 5.4% adults over the age of 18 Type 2 diabetes is the fasted growing non-communicable disease Fourth largest disease burden Obesity is the strongest risk factor for type 2 diabetes Annual cost $14 billion
3 Jenny 46 year old female Abnormal FBG 6.4 mmol/l No past medical history Several vitamins but no prescription medications Father type 2 diabetes BMI 27.9 BP 121/80 mmhg
4 Jenny 75 gm OGTT FBG 6.5 2Hr Glu 8.5 HBA1C 6.4% Lipid profile: TC 7.2,HDL 5.6, HDL 1.0, TG 1.1 What next?
5 Diagnostic criteria of type 2 DM (ADS and RACGP) FBG > 7.0 mmol/l ( on two separate occasions ) 2 hr post prandial > 11.0 mmol/l ( on two separate occasions ) HBA1C > 6.5% (48 mmol/mol) ( on two separate occasions )
6 Screening and diagnosis of type 2 diagnosis RACGP guidelines 2014 FBG or RBG < 5.5 Diabetes unlikely Retest every 3 years
7 FBG > 7 or RBG > 11.1 Confirm with FBG or HBA1C FBG > 7 FBG HBA1C < 6.5 HBA1C > 6.5 Diabetes OGTT Life style and diet
8 HBA1C > 6.5 % Repeat FBG or HBA1C HBA1C > 6.5% FBG HBA1C < 6.5 FBG > 7.0 Diabetes OGTT life style changes
9 FBG mmol/l or RBG mmol/l OGTT
10 OGTT FBG < 6.1 FBG FBG < 7 FBG > 7.0 2h < 7.8 2h < 7.8 2h h > 11.1 No diabetes IFG IGT Diabetes excess macro vascular risk excess macro- and micro
11 Case -Jenny FBG 6.4 OGTT FBG 6.5, BG2h 8.5, HBA1C 6.4% Intensive life style modification weight loss increase physical activity Good compliance with recommendations Lost 6kg FBG Annual OGTT isolated IFG HBA1C Dyslipidemia improved
12 Prediabetes: stage between normal glucose level and clinical type 2 diabetes Diabetes is defined by the threshold level above which there is significant increase incident of retinopathy But cardiovascular events increases linearly at level way below the diabetes diagnosis level It suggest the disease before the official diagnosis of diabetes
13 Prediabetes Annual risk of progression to diabetes Normoglycemia: 0.7% per year Prediabetes: 5-10% per year Increase risk for macrovascular disease and retinopathy Finnish study and DPP : Lifestyle intervention - 58% reduction in the progression Metformin 31% reduction in the progression Metformin + Life style =no additional benefit
14 OGTT- what to tell the patient? More validated but less reproducible Affected bycarbohydrate intake 150gm carb per day for 3 days duration of fasting preceding the test- fasting after 2200 hour except water, no caffeine or smoking time of the day the test performed hour Activity during the test seated for 2 hours
15 What if OGTT is unreliable? Repeating the test at least in two circumstances: Marginally abnormal results and potential for incorrect preparation and administration of the test Marginally abnormal results and major implications in life (eg. Loss of job; difficulty obtaining insurance
16 Case - Jenny By age 54 Less diligence with life style changes Gained weight OGTT : FBG 6.8, BG2h 14, HBA1C 6.9% Repeat: FBG 8.2, BG2h 12.4 Lipids: TC 7.4, LDL 5.3, HDL 1.1, TG 2.1
17 Case- Jenny By age 54 Less diligence with life style changes Gained weight OGTT : FBG 6.8, BG2h 14, HBA1C 6.9% Repeat: BFG 8.2, BG2h 12.4 Lipids: TC 7.4, LDL 5.3, HDL 1.1, TG 2.1 Metformin, Statin and Aspirin BP in target, no microalbuminuria and retinopathy
18 Australian diabetes society treatment algorithm
19 Metformin- first line of treatment Well tolerated and effective HBA1C reduction 1.5% UKPDS Myocardial infarction risk reduction 39% Mortality reduction 36% Mechanism: reduction of hepatic glucose output Start low dose and then increase
20 Case - jenny 56 year of age Metformin 2gm daily Life style changes HBA1C 7.9 % FBG 8-9
21
22 sulfonylureas Stimulates insulin secretion from pancreatic beta cells Risk of hypoglycemia, severe hypoglycemia rare Weight gain around 2-3 kg First generation sulfonylurea- tolbutamide increases mortality JAMA 1971
23 sulfonylureas Metaanalysis in type 2 diabetes on sulfonylurea use: - Increase risk of cardiovascular events but no major events Diabetes Obes Metab 2013 ADVANCE trial : - no increase CVD risk with the use of gliclazide-modified release NEJM 2008
24 Thiazolidinediones: PPAAR gamma agonist Insulin sensitizers Preserve beta cell function Durability of action Concerns: - Fractures - Weight gain - Fluid retention/heart failure - Bladder cancer
25 Rosiglitazone Metaanalysis of 42 studies Increase cardiovascular death : OR 1.64 ( ) NEJM 2007
26 PROactive trial: pioglitazone Secondary prevention of CVD 16% reduction of death, stroke and MI Lancet 2005

27 GLP-1 analogue- Mechanism of action
28 GLP 1 analogue Subcutaneous injections ( exenatide and liraglutide) Benefit: HBA1C reduction Post prandial hyperglycemia control Weight loss No hypoglycemia Neuroprotective effect and beneficial effect on BP, LVEF, HR Lancet 2014
29 GLP 1 analogue Concern: GI side effects pancreatitis
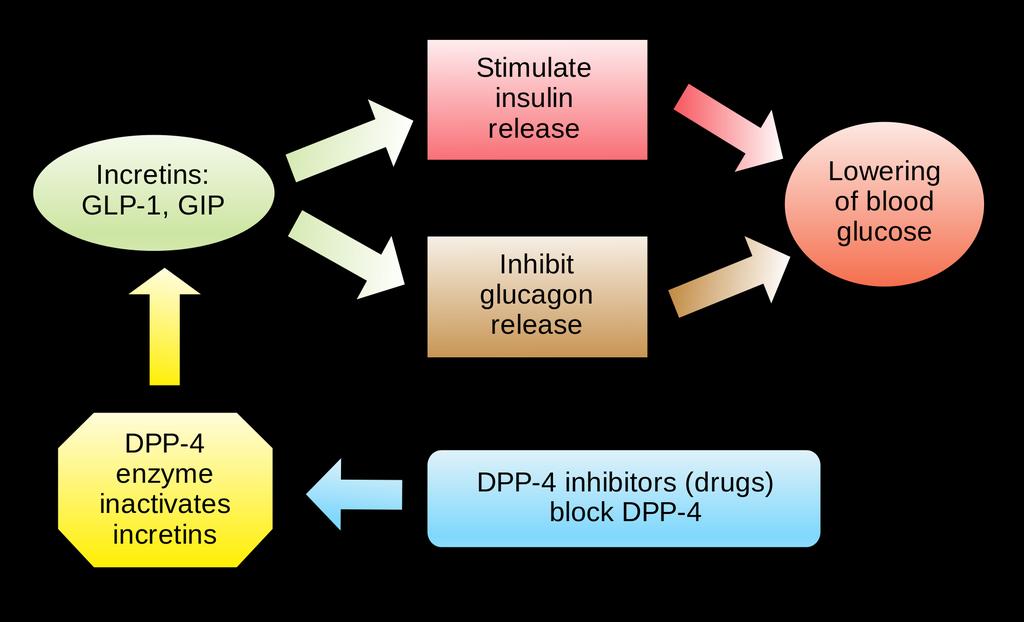
30 DPP-4 inhibitors
31 DPP-4 inhibitors: Gliptines Benefit: No hypoglycemia Weight neutral CRF safe with dose adjustment HBA1C reduction 1% Recent metaanalysis of RCTs: Trend towards increase risk of heart failure but no increase mortality
32 Pancreatic safety GLP1 agonist/dpp-4 inhibitors Trend towards increase acute pancreatitis But statistically non-significant Pancreatic cancer
33 SGLT-2 inhibitors: Dapagliflozin, canagliflozin, empagliflozine Increase renal glucose loss Type 2 diabetes SGLT-2 upregulated Benefit: Significant reduction of HBA1C Weight loss Improve lipid profile Systolic BP reduction by 10mmHg
34 SGLT-2 inhibitors May 2015 FDA warning Association between SGLT-2 inhibitors and DKA Euglycemic DKA Mechanism: fall of both plasma glucose and insulin increase endogenous glucose production Diabetes Care 2015
35 Empa-Reg outcome study Empagliflozin ( 10-25mg) Significant reduction in cardiovascular events/deaths and heart failure admissions NEJM 2015
36 Case Jenny HBA1C 7.9 Gliclazide slow release 120mg daily Metformin 2gm daily After 1 year HBA1C 7.8% She was advised for additional medication But she was reluctant and opted to try with diet Lost follow up
37 Case - jenny Represented 2 years later HBA1C 9.2 FBG 12.1 Lipid: TG1.2, TC 4.4, HDL 1.0,LDL 2.8 No urine microalbumin
38 Insulin therapy KISS principle It is the only therapy like to reduce HBA1C < 7 in patients with HBA1C > 8.5 Diabetes Care 2012 Safe and effective Single dose 0.2 units/kg, usually 10-20units to start with, then self titration Risk of hypoglycemia is lower compared to type 1 DM Weight gain 2-4 kg, likely if symptoms and glycosuria Oral agents insulin secretogogues can be discontinued
39 conclusion Progressive beta cell dysfunction has inevitable resulted in the need to add insulin to standard therapy in type 2 diabetes SGLT-2 inhibitors are effective adjunct to metformin/insulin with associated weight reduction Individualized approach using dietary weight loss strategy and the sequential addition of AHA remains the best practice for glycemic control of type 2 diabetes.
40 Thank you
Diabetes Guidelines in View of Recent Clinical Trials Are They Still Applicable?
 Diabetes Guidelines in View of Recent Clinical Trials Are They Still Applicable? Jay S. Skyler, MD, MACP Division of Endocrinology, Diabetes, and Metabolism and Diabetes Research Institute University of
Diabetes Guidelines in View of Recent Clinical Trials Are They Still Applicable? Jay S. Skyler, MD, MACP Division of Endocrinology, Diabetes, and Metabolism and Diabetes Research Institute University of
LATE BREAKING STUDIES IN DM AND CAD. Will this change the guidelines?
 LATE BREAKING STUDIES IN DM AND CAD Will this change the guidelines? Objectives 1. Discuss current guidelines for prevention of CHD in diabetes. 2. Discuss the FDA Guidance for Industry regarding evaluating
LATE BREAKING STUDIES IN DM AND CAD Will this change the guidelines? Objectives 1. Discuss current guidelines for prevention of CHD in diabetes. 2. Discuss the FDA Guidance for Industry regarding evaluating
Non-insulin treatment in Type 1 DM Sang Yong Kim
 Non-insulin treatment in Type 1 DM Sang Yong Kim Chosun University Hospital Conflict of interest disclosure None Committee of Scientific Affairs Committee of Scientific Affairs Insulin therapy is the mainstay
Non-insulin treatment in Type 1 DM Sang Yong Kim Chosun University Hospital Conflict of interest disclosure None Committee of Scientific Affairs Committee of Scientific Affairs Insulin therapy is the mainstay
Wayne Gravois, MD August 6, 2017
 Wayne Gravois, MD August 6, 2017 Americans with Diabetes (Millions) 40 30 Source: National Diabetes Statistics Report, 2011, 2017 Millions 20 10 0 1980 2009 2015 2007 - $174 Billion 2015 - $245 Billion
Wayne Gravois, MD August 6, 2017 Americans with Diabetes (Millions) 40 30 Source: National Diabetes Statistics Report, 2011, 2017 Millions 20 10 0 1980 2009 2015 2007 - $174 Billion 2015 - $245 Billion
NEW DIABETES CARE MEDICATIONS
 NEW DIABETES CARE MEDICATIONS James Bonucchi DO, ECNU, FACE Adult Medicine and Endocrinology Specialists Disclosures Speakers bureau Sanofi AZ BI Diabetes Diabetes cost ADA 2017 data Ever increasing disorder.
NEW DIABETES CARE MEDICATIONS James Bonucchi DO, ECNU, FACE Adult Medicine and Endocrinology Specialists Disclosures Speakers bureau Sanofi AZ BI Diabetes Diabetes cost ADA 2017 data Ever increasing disorder.
Diabetes and New Meds for Cardiovascular Risk Reduction. F. Dwight Chrisman, MD, FACC. Disclosures: BI Boehringer Ingelheim speaker
 Diabetes and New Meds for Cardiovascular Risk Reduction F. Dwight Chrisman, MD, FACC Disclosures: BI Boehringer Ingelheim speaker 1 Prevalence of DM DM state specific prevalence 2006 4%-6% 6-8% 8-10% 10-12%
Diabetes and New Meds for Cardiovascular Risk Reduction F. Dwight Chrisman, MD, FACC Disclosures: BI Boehringer Ingelheim speaker 1 Prevalence of DM DM state specific prevalence 2006 4%-6% 6-8% 8-10% 10-12%
Diabetes Mellitus: Implications of New Clinical Trials and New Medications
 Diabetes Mellitus: Implications of New Clinical Trials and New Medications Estimates of Diagnosed Diabetes in Adults, 2005 Alka M. Kanaya, MD Asst. Professor of Medicine UCSF, Primary Care CME October
Diabetes Mellitus: Implications of New Clinical Trials and New Medications Estimates of Diagnosed Diabetes in Adults, 2005 Alka M. Kanaya, MD Asst. Professor of Medicine UCSF, Primary Care CME October
Overview T2DM medications. Winnie Ho
 Overview T2DM medications Winnie Ho Diabetes in Australia 1.7 million Australians with diabetes, of these 85% have T2DM 2-fold excess risk CV death in patients with diabetes Risk factor for progression
Overview T2DM medications Winnie Ho Diabetes in Australia 1.7 million Australians with diabetes, of these 85% have T2DM 2-fold excess risk CV death in patients with diabetes Risk factor for progression
Cardiovascular Benefits of Two Classes of Antihyperglycemic Medications
 Cardiovascular Benefits of Two Classes of Antihyperglycemic Medications Nathan Woolever, Pharm.D., Resident Pharmacist Pharmacy Grand Rounds November 6 th, 2018 Franciscan Healthcare La Crosse, WI 2017
Cardiovascular Benefits of Two Classes of Antihyperglycemic Medications Nathan Woolever, Pharm.D., Resident Pharmacist Pharmacy Grand Rounds November 6 th, 2018 Franciscan Healthcare La Crosse, WI 2017
Comprehensive Diabetes Treatment
 Comprehensive Diabetes Treatment Joshua L. Cohen, M.D., F.A.C.P. Professor of Medicine Interim Director, Division of Endocrinology & Metabolism The George Washington University School of Medicine Diabetes
Comprehensive Diabetes Treatment Joshua L. Cohen, M.D., F.A.C.P. Professor of Medicine Interim Director, Division of Endocrinology & Metabolism The George Washington University School of Medicine Diabetes
OBESITY IN TYPE 2 DIABETES
 OBESITY IN TYPE 2 DIABETES Ashley Crowl, PharmD, BCACP Assistant Professor University of Kansas Objectives Review how to manage obesity in patients with type-2 diabetes mellitus Compare antiobesity agents
OBESITY IN TYPE 2 DIABETES Ashley Crowl, PharmD, BCACP Assistant Professor University of Kansas Objectives Review how to manage obesity in patients with type-2 diabetes mellitus Compare antiobesity agents
Disclosures. Diabetes and Cardiovascular Risk Management. Learning Objectives. Atherosclerotic Cardiovascular Disease
 Disclosures Diabetes and Cardiovascular Risk Management Tony Hampton, MD, MBA Medical Director Advocate Aurora Operating System Advocate Aurora Healthcare Downers Grove, IL No conflicts or disclosures
Disclosures Diabetes and Cardiovascular Risk Management Tony Hampton, MD, MBA Medical Director Advocate Aurora Operating System Advocate Aurora Healthcare Downers Grove, IL No conflicts or disclosures
The Many Faces of T2DM in Long-term Care Facilities
 The Many Faces of T2DM in Long-term Care Facilities Question #1 Which of the following is a risk factor for increased hypoglycemia in older patients that may suggest the need to relax hyperglycemia treatment
The Many Faces of T2DM in Long-term Care Facilities Question #1 Which of the following is a risk factor for increased hypoglycemia in older patients that may suggest the need to relax hyperglycemia treatment
The Death of Sulfonylureas? A Review of New Diabetes Medications
 The Death of Sulfonylureas? A Review of New Diabetes Medications Kelly Hoenig, Pharm.D., BCPS Cedar Rapids Family Medicine Residency 2/4/17 Objectives Review GLP-1 Agonists, DPP-IV Inhibitors and SGLT-2
The Death of Sulfonylureas? A Review of New Diabetes Medications Kelly Hoenig, Pharm.D., BCPS Cedar Rapids Family Medicine Residency 2/4/17 Objectives Review GLP-1 Agonists, DPP-IV Inhibitors and SGLT-2
Oral Hypoglycemics and Risk of Adverse Cardiac Events: A Summary of the Controversy
 Oral Hypoglycemics and Risk of Adverse Cardiac Events: A Summary of the Controversy Jeffrey Boord, MD, MPH Advances in Cardiovascular Medicine Kingston, Jamaica December 7, 2012 VanderbiltHeart.com Outline
Oral Hypoglycemics and Risk of Adverse Cardiac Events: A Summary of the Controversy Jeffrey Boord, MD, MPH Advances in Cardiovascular Medicine Kingston, Jamaica December 7, 2012 VanderbiltHeart.com Outline
Old oral antidiabetic agents in the armamentarium of diabetes mellitus treatment: Safety and efficacy
 Old oral antidiabetic agents in the armamentarium of diabetes mellitus treatment: Safety and efficacy Melpomeni Peppa Assistant Professor of Endocrinology 2 nd Dept of Internal Medicine-Propaedeutic, Athens
Old oral antidiabetic agents in the armamentarium of diabetes mellitus treatment: Safety and efficacy Melpomeni Peppa Assistant Professor of Endocrinology 2 nd Dept of Internal Medicine-Propaedeutic, Athens
Disclosures of Interest. Publications Diabetologia Key points to emphasize
 Disclosures of Interest No conflicts or disclosures How to Use the American Diabetes Association s Type 2 Diabetes Treatment Algorithm Rashida Downing, MD, FAAFP Primary Care Physician JenCare Medical
Disclosures of Interest No conflicts or disclosures How to Use the American Diabetes Association s Type 2 Diabetes Treatment Algorithm Rashida Downing, MD, FAAFP Primary Care Physician JenCare Medical
Dr Tahseen A. Chowdhury Royal London Hospital. New Guidelines in Diabetes: NICE or Nasty?
 Dr Tahseen A. Chowdhury Royal London Hospital New Guidelines in Diabetes: NICE or Nasty? I have no conflicts of interest I do not undertake talks / advisory bodies / research for any pharma company Consultant
Dr Tahseen A. Chowdhury Royal London Hospital New Guidelines in Diabetes: NICE or Nasty? I have no conflicts of interest I do not undertake talks / advisory bodies / research for any pharma company Consultant
New Treatments for Type 2 diabetes. Nandini Seevaratnam April 2016 Rushcliffe Patient Forum
 New Treatments for Type 2 diabetes Nandini Seevaratnam April 2016 Rushcliffe Patient Forum Overview Growing population of Type 2 diabetes Basic science on what goes wrong Current treatments Why there is
New Treatments for Type 2 diabetes Nandini Seevaratnam April 2016 Rushcliffe Patient Forum Overview Growing population of Type 2 diabetes Basic science on what goes wrong Current treatments Why there is
Diabesity. Metabolic dysfunction that ranges from mild blood glucose imbalance to full fledged Type 2 DM Signs
 Diabesity Metabolic dysfunction that ranges from mild blood glucose imbalance to full fledged Type 2 DM Signs Abdominal obesity Low HDL, high LDL, and high triglycerides HTN High blood glucose (F>100l,
Diabesity Metabolic dysfunction that ranges from mild blood glucose imbalance to full fledged Type 2 DM Signs Abdominal obesity Low HDL, high LDL, and high triglycerides HTN High blood glucose (F>100l,
Type 2 Diabetes. Stopping Smoking. Consider referral to smoking cessation. Consider referring for weight management advice.
 Type 2 Diabetes Stopping Smoking Consider referral to smoking cessation BMI > 25 kg m² Set a weight loss target of a 5-10% reduction Consider referring for weight management advice Control BP to
Type 2 Diabetes Stopping Smoking Consider referral to smoking cessation BMI > 25 kg m² Set a weight loss target of a 5-10% reduction Consider referring for weight management advice Control BP to
Type 2 Diabetes: Where Do We Start with Treatment? DIABETES EDUCATION. Diabetes Mellitus: Complications and Co-Morbid Conditions
 Diabetes Mellitus: Complications and Co-Morbid Conditions ADA Guidelines for Glycemic Control: 2016 Retinopathy Between 2005-2008, 28.5% of patients with diabetes 40 years and older diagnosed with diabetic
Diabetes Mellitus: Complications and Co-Morbid Conditions ADA Guidelines for Glycemic Control: 2016 Retinopathy Between 2005-2008, 28.5% of patients with diabetes 40 years and older diagnosed with diabetic
Guidelines to assist General Practitioners in the Management of Type 2 Diabetes. April 2010
 Guidelines to assist General Practitioners in the Management of Type 2 Diabetes April 2010 Foreword The guidelines were devised by the Diabetes Day Centre in Beaumont Hospital in consultation with a number
Guidelines to assist General Practitioners in the Management of Type 2 Diabetes April 2010 Foreword The guidelines were devised by the Diabetes Day Centre in Beaumont Hospital in consultation with a number
Learning and Earning with Gateway Professional Education CME/CEU Webinar Series. Diabetes Update July 6, :00pm 1:00pm
 Learning and Earning with Gateway Professional Education CME/CEU Webinar Series Diabetes Update July 6, 2017 12:00pm 1:00pm Jennifer Pennock Holst, MD Endocrinology, Diabetes & Metabolism AHN Center for
Learning and Earning with Gateway Professional Education CME/CEU Webinar Series Diabetes Update July 6, 2017 12:00pm 1:00pm Jennifer Pennock Holst, MD Endocrinology, Diabetes & Metabolism AHN Center for
ESC GUIDELINES ON DIABETES AND CARDIOVASCULAR DISEASES
 ESC GUIDELINES ON DIABETES AND CARDIOVASCULAR DISEASES Pr. Michel KOMAJDA Institute of Cardiology - IHU ICAN Pitie Salpetriere Hospital - University Pierre and Marie Curie, Paris (France) DEFINITION A
ESC GUIDELINES ON DIABETES AND CARDIOVASCULAR DISEASES Pr. Michel KOMAJDA Institute of Cardiology - IHU ICAN Pitie Salpetriere Hospital - University Pierre and Marie Curie, Paris (France) DEFINITION A
A factorial randomized trial of blood pressure lowering and intensive glucose control in 11,140 patients with type 2 diabetes
 A factorial randomized trial of blood pressure lowering and intensive glucose control in 11,140 patients with type 2 diabetes Hypotheses: Among individuals with type 2 diabetes, the risks of major microvascular
A factorial randomized trial of blood pressure lowering and intensive glucose control in 11,140 patients with type 2 diabetes Hypotheses: Among individuals with type 2 diabetes, the risks of major microvascular
Management of Type 2 Diabetes Cardiovascular Outcomes Trials Tom Blevins MD Texas Diabetes and Endocrinology Austin, Texas
 Management of Type 2 Diabetes Cardiovascular Outcomes Trials 2018 Tom Blevins MD Texas Diabetes and Endocrinology Austin, Texas Speaker Disclosure Dr. Blevins has disclosed that he has received grant support
Management of Type 2 Diabetes Cardiovascular Outcomes Trials 2018 Tom Blevins MD Texas Diabetes and Endocrinology Austin, Texas Speaker Disclosure Dr. Blevins has disclosed that he has received grant support
Vipul Lakhani, MD Oregon Medical Group Endocrinology
 Vipul Lakhani, MD Oregon Medical Group Endocrinology Disclosures None Objectives Be able to diagnose diabetes and assess control Be able to identify appropriate classes of medications for diabetes treatment
Vipul Lakhani, MD Oregon Medical Group Endocrinology Disclosures None Objectives Be able to diagnose diabetes and assess control Be able to identify appropriate classes of medications for diabetes treatment
Navigating the New Options for the Management of Type 2 Diabetes
 Navigating the New Options for the Management of Type 2 Diabetes Clinical Associate Professor Mark Kennedy Department of General Practice, University of Melbourne Chair, Primary Care Diabetes Society of
Navigating the New Options for the Management of Type 2 Diabetes Clinical Associate Professor Mark Kennedy Department of General Practice, University of Melbourne Chair, Primary Care Diabetes Society of
Quick Reference Guide
 2018 Clinical Practice Guidelines Quick Reference Guide 416569-18 guidelines.diabetes.ca diabetes.ca 1-800-BANTING (226-8464) Screening and Diagnosis Assess risk ANNUALLY if: Family history (First-degree
2018 Clinical Practice Guidelines Quick Reference Guide 416569-18 guidelines.diabetes.ca diabetes.ca 1-800-BANTING (226-8464) Screening and Diagnosis Assess risk ANNUALLY if: Family history (First-degree
Dr A Pokrajac MD MSc MRCP Consultant
 Dr A Pokrajac MD MSc MRCP Consultant Onset at 5-15 years of T1DM Can be present at diagnosis of T2DM Detect in regular MA/Cr screening (2X first urine sample, no UTI, no other causes) Contributing Factors
Dr A Pokrajac MD MSc MRCP Consultant Onset at 5-15 years of T1DM Can be present at diagnosis of T2DM Detect in regular MA/Cr screening (2X first urine sample, no UTI, no other causes) Contributing Factors
DM-2 Therapy Update: GLP-1, SGLT-2 Inhibitors, and Inhaled Insulin, Oh My!
 DM-2 Therapy Update: GLP-1, SGLT-2 Inhibitors, and Inhaled Insulin, Oh My! Kevin M. Pantalone, DO, ECNU, CCD Associate Staff Director of Clinical Research Department of Endocrinology Endocrinology and
DM-2 Therapy Update: GLP-1, SGLT-2 Inhibitors, and Inhaled Insulin, Oh My! Kevin M. Pantalone, DO, ECNU, CCD Associate Staff Director of Clinical Research Department of Endocrinology Endocrinology and
Should Psychiatrists be diagnosing (and treating) metabolic syndrome
 metabolic syndrome") Should Psychiatrists be diagnosing (and treating) metabolic syndrome David Hopkins Clinical Director, Diabetes King s College Hospital, London Diabetes prevalence (thousands) Diabetes in the UK: 1995-2010
Should Psychiatrists be diagnosing (and treating) metabolic syndrome David Hopkins Clinical Director, Diabetes King s College Hospital, London Diabetes prevalence (thousands) Diabetes in the UK: 1995-2010
The ABCs (A1C, BP and Cholesterol) of Diabetes
 of Diabetes") The ABCs (A1C, BP and Cholesterol) of Diabetes Gregg Simonson, PhD Director, Professional Training and Consulting International Diabetes Center; Adjunct Assistant Professor, University of Minnesota Department
The ABCs (A1C, BP and Cholesterol) of Diabetes Gregg Simonson, PhD Director, Professional Training and Consulting International Diabetes Center; Adjunct Assistant Professor, University of Minnesota Department
Diabetes 2013: Achieving Goals Through Comprehensive Treatment. Session 2: Individualizing Therapy
 Diabetes 2013: Achieving Goals Through Comprehensive Treatment Session 2: Individualizing Therapy Joshua L. Cohen, M.D., F.A.C.P. Professor of Medicine Interim Director, Division of Endocrinology & Metabolism
Diabetes 2013: Achieving Goals Through Comprehensive Treatment Session 2: Individualizing Therapy Joshua L. Cohen, M.D., F.A.C.P. Professor of Medicine Interim Director, Division of Endocrinology & Metabolism
Intensification of Diabetic Therapy. Case studies
 Intensification of Diabetic Therapy Case studies Patient #1 1 st visit: 64 year old male, H/O prediabetes, lost weight 280 lbs. to 240 lbs. ER for dental abscess, glucose >300 A1C 11.4%, no diabetic medication,
Intensification of Diabetic Therapy Case studies Patient #1 1 st visit: 64 year old male, H/O prediabetes, lost weight 280 lbs. to 240 lbs. ER for dental abscess, glucose >300 A1C 11.4%, no diabetic medication,
CURRENT CONTROVERSIES IN DIABETES CARE
 CURRENT CONTROVERSIES IN DIABETES CARE Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest Diabetes Mellitus: U.S. Impact
CURRENT CONTROVERSIES IN DIABETES CARE Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest Diabetes Mellitus: U.S. Impact
Diabetes and the Heart
 Diabetes and the Heart Jeffrey Boord, MD, MPH Advances in Cardiovascular Medicine Kingston, Jamaica December 6, 2012 Outline Screening for diabetes in patients with CAD Screening for CAD in patients with
Diabetes and the Heart Jeffrey Boord, MD, MPH Advances in Cardiovascular Medicine Kingston, Jamaica December 6, 2012 Outline Screening for diabetes in patients with CAD Screening for CAD in patients with
Diabetes Mellitus II CPG
 1 Diabetes Mellitus II CPG Candidates for Screening Integrated Complex Care Patients: Check Yearly Prediabetes: Check Yearly No Diabetes Mellitus (DM) Risk Factors: Check at Age 45, Repeat Every 3 Years
1 Diabetes Mellitus II CPG Candidates for Screening Integrated Complex Care Patients: Check Yearly Prediabetes: Check Yearly No Diabetes Mellitus (DM) Risk Factors: Check at Age 45, Repeat Every 3 Years
Adult Diabetes Clinician Guide NOVEMBER 2017
 Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Adult Diabetes Clinician Guide Introduction NOVEMBER 2017 This evidence-based guideline summary is based on the 2017 KP National Diabetes Guideline.
Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Adult Diabetes Clinician Guide Introduction NOVEMBER 2017 This evidence-based guideline summary is based on the 2017 KP National Diabetes Guideline.
TREATMENTS FOR TYPE 2 DIABETES. Susan Henry Diabetes Specialist Nurse
 TREATMENTS FOR TYPE 2 DIABETES Susan Henry Diabetes Specialist Nurse How can we improve outcomes in Type 2 diabetes? Earlier diagnosis Better patient education Stress central role of lifestyle management
TREATMENTS FOR TYPE 2 DIABETES Susan Henry Diabetes Specialist Nurse How can we improve outcomes in Type 2 diabetes? Earlier diagnosis Better patient education Stress central role of lifestyle management
Quick Reference Guide
 2013 Clinical Practice Guidelines Quick Reference Guide (Updated November 2016) 416569-16 guidelines.diabetes.ca diabetes.ca 1-800-BANTING (226-8464) Copyright 2016 Canadian Diabetes Association SCREENING
2013 Clinical Practice Guidelines Quick Reference Guide (Updated November 2016) 416569-16 guidelines.diabetes.ca diabetes.ca 1-800-BANTING (226-8464) Copyright 2016 Canadian Diabetes Association SCREENING
Drug Class Monograph
 Drug Class Monograph Class: Sodium-Glucose Co-Transporter 2 (SGLT-2) Inhibitors Drugs: Farxiga (dapagliflozin), Invokamet (canagliflozin/metformin), Invokana (canagliflozin), Jardiance (empagliflozin),
Drug Class Monograph Class: Sodium-Glucose Co-Transporter 2 (SGLT-2) Inhibitors Drugs: Farxiga (dapagliflozin), Invokamet (canagliflozin/metformin), Invokana (canagliflozin), Jardiance (empagliflozin),
How can we improve outcomes in Type 2 diabetes?
 How can we improve outcomes in Type 2 diabetes? Earlier diagnosis Better patient education Stress central role of lifestyle management Identify and treat all risk factors Use rational pharmacological therapy
How can we improve outcomes in Type 2 diabetes? Earlier diagnosis Better patient education Stress central role of lifestyle management Identify and treat all risk factors Use rational pharmacological therapy
CURRENT ISSUES IN DIABETES MANAGEMENT. Screening for Diabetes Advantages of HbA1c as a Diagnostic Test. Diagnosis of Diabetes 2013
 CURRENT ISSUES IN DIABETES MANAGEMENT Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest Screening for Diabetes 2013 BMI
CURRENT ISSUES IN DIABETES MANAGEMENT Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest Screening for Diabetes 2013 BMI
Medical therapy advances London/Manchester RCP February/June 2016
 Medical therapy advances London/Manchester RCP February/June 2016 Advances in medical therapies for diabetes mellitus Duality of interest: The speaker or institutions with which he is associated has received
Medical therapy advances London/Manchester RCP February/June 2016 Advances in medical therapies for diabetes mellitus Duality of interest: The speaker or institutions with which he is associated has received
Diabetes Risk Assessment and Treatment
 Diabetes Risk Assessment and Treatment Todd T. Brown, MD, PhD Professor of Medicine and Epidemiology Division of Endocrinology, Diabetes, & Metabolism Johns Hopkins University Baltimore, Maryland, USA
Diabetes Risk Assessment and Treatment Todd T. Brown, MD, PhD Professor of Medicine and Epidemiology Division of Endocrinology, Diabetes, & Metabolism Johns Hopkins University Baltimore, Maryland, USA
Sodium-Glucose Co-Transporter 2 (SGLT-2) Inhibitors Drug Class Prior Authorization Protocol
 Inhibitors Drug Class Prior Authorization Protocol") Sodium-Glucose Co-Transporter 2 (SGLT-2) Inhibitors Drug Class Prior Authorization Protocol Line of Business: Medicaid P&T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has
Sodium-Glucose Co-Transporter 2 (SGLT-2) Inhibitors Drug Class Prior Authorization Protocol Line of Business: Medicaid P&T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has
The Flozins Quest for Clarity?
 The Flozins Quest for Clarity? Choosing Wisely with Academic Detailing 2018 ARE THEY THE REAL DEAL Disclosure statements The Academic Detailing Service is operated by Dalhousie Continuing Professional
The Flozins Quest for Clarity? Choosing Wisely with Academic Detailing 2018 ARE THEY THE REAL DEAL Disclosure statements The Academic Detailing Service is operated by Dalhousie Continuing Professional
Management of Type 2 Diabetes
 Management of Type 2 Diabetes Pathophysiology Insulin resistance and relative insulin deficiency/ defective secretion Not immune mediated No evidence of β cell destruction Increased risk with age, obesity
Management of Type 2 Diabetes Pathophysiology Insulin resistance and relative insulin deficiency/ defective secretion Not immune mediated No evidence of β cell destruction Increased risk with age, obesity
MANAGING DIABETES IN 2016 WHAT TO ADD, WHEN AND WHY?
 MANAGING DIABETES IN 2016 WHAT TO ADD, WHEN AND WHY? Faculty: Maria Wolfs MD, MHSc, FRCPC Assistant Professor, University of Toronto Staff Endocrinologist, St. Michael's Hospital Relationships with commercial
MANAGING DIABETES IN 2016 WHAT TO ADD, WHEN AND WHY? Faculty: Maria Wolfs MD, MHSc, FRCPC Assistant Professor, University of Toronto Staff Endocrinologist, St. Michael's Hospital Relationships with commercial
The Clinical Unmet need in the patient with Diabetes and ACS
 The Clinical Unmet need in the patient with Diabetes and ACS Professor Kausik Ray (UK) BSc(hons), MBChB, MD, MPhil, FRCP (lon), FRCP (ed), FACC, FESC, FAHA Diabetes is a global public health challenge
The Clinical Unmet need in the patient with Diabetes and ACS Professor Kausik Ray (UK) BSc(hons), MBChB, MD, MPhil, FRCP (lon), FRCP (ed), FACC, FESC, FAHA Diabetes is a global public health challenge
DIABETES DEBATE - IS NEW BETTER?
 DIABETES DEBATE - IS NEW BETTER? WHAT MEDICATION CLASS AFTER METFORMIN TO CONTROL BLOOD SUGAR Dr. Lydia Hatcher, MD, CCFP, FCFP, CHE, D-CAPM Associate Clinical Professor of Family Medicine, McMaster Chief
DIABETES DEBATE - IS NEW BETTER? WHAT MEDICATION CLASS AFTER METFORMIN TO CONTROL BLOOD SUGAR Dr. Lydia Hatcher, MD, CCFP, FCFP, CHE, D-CAPM Associate Clinical Professor of Family Medicine, McMaster Chief
Professor Rudy Bilous James Cook University Hospital
 Professor Rudy Bilous James Cook University Hospital Rate per 100 patient years Rate per 100 patient years 16 Risk of retinopathy progression 16 Risk of developing microalbuminuria 12 12 8 8 4 0 0 5 6
Professor Rudy Bilous James Cook University Hospital Rate per 100 patient years Rate per 100 patient years 16 Risk of retinopathy progression 16 Risk of developing microalbuminuria 12 12 8 8 4 0 0 5 6
Diabetes Treatment Update
 Diabetes Treatment Update Timothy C. Evans, MD PhD FACP University of Washington Department of Medicine Disclosure: Dr. Evans has no significant financial interest in any of the products or manufacturers
Diabetes Treatment Update Timothy C. Evans, MD PhD FACP University of Washington Department of Medicine Disclosure: Dr. Evans has no significant financial interest in any of the products or manufacturers
Diabetes Mellitus: A Cardiovascular Disease
 Diabetes Mellitus: A Cardiovascular Disease Nestoras Mathioudakis, M.D. Assistant Professor of Medicine Division of Endocrinology, Diabetes, & Metabolism September 30, 2013 1 The ABCs of cardiovascular
Diabetes Mellitus: A Cardiovascular Disease Nestoras Mathioudakis, M.D. Assistant Professor of Medicine Division of Endocrinology, Diabetes, & Metabolism September 30, 2013 1 The ABCs of cardiovascular
IDF Regions and global projections of the number of people with diabetes (20-79 years), 2013 and Diabetes Atlas -sixth Edition: IDF 2013
, 2013 and Diabetes Atlas -sixth Edition: IDF 2013") IDF Regions and global projections of the number of people with diabetes (20-79 years), 2013 and 2035 Diabetes Atlas -sixth Edition: IDF 2013 Diabetes Atlas -sixth Edition: IDF 2013 Chronic complications
IDF Regions and global projections of the number of people with diabetes (20-79 years), 2013 and 2035 Diabetes Atlas -sixth Edition: IDF 2013 Diabetes Atlas -sixth Edition: IDF 2013 Chronic complications
Managing Perioperative Diabetes What s new? Kathryn A. Myers MD FRCPC Chair Chief Division of GIM Professor of Medicine Western University
 Managing Perioperative Diabetes What s new? Kathryn A. Myers MD FRCPC Chair Chief Division of GIM Professor of Medicine Western University Objectives: By the end of this session, you will be able to: Identify
Managing Perioperative Diabetes What s new? Kathryn A. Myers MD FRCPC Chair Chief Division of GIM Professor of Medicine Western University Objectives: By the end of this session, you will be able to: Identify
Diabetes Update: Intensifying Insulin Therapy Nuts, Bolts and Other Items
 Diabetes Update: Intensifying Insulin Therapy Nuts, Bolts and Other Items Hayley A. Miller, MD Physician, Internal Medicine, Diabetes and Metabolism, Sandy Clinic, Intermountain Healthcare Objectives:
Diabetes Update: Intensifying Insulin Therapy Nuts, Bolts and Other Items Hayley A. Miller, MD Physician, Internal Medicine, Diabetes and Metabolism, Sandy Clinic, Intermountain Healthcare Objectives:
What s New in Diabetes Medications. Jena Torpin, PharmD
 What s New in Diabetes Medications Jena Torpin, PharmD 1 Objectives Discuss new medications in the management of diabetes Understand the mechanism of the medications discussed Understand the side effects
What s New in Diabetes Medications Jena Torpin, PharmD 1 Objectives Discuss new medications in the management of diabetes Understand the mechanism of the medications discussed Understand the side effects
Abbreviations DPP-IV dipeptidyl peptidase IV DREAM Diabetes REduction Assessment with ramipril and rosiglitazone
 Index Abbreviations DPP-IV dipeptidyl peptidase IV DREAM Diabetes REduction Assessment with ramipril and rosiglitazone Medication GAD glutamic acid decarboxylase GLP-1 glucagon-like peptide 1 NPH neutral
Index Abbreviations DPP-IV dipeptidyl peptidase IV DREAM Diabetes REduction Assessment with ramipril and rosiglitazone Medication GAD glutamic acid decarboxylase GLP-1 glucagon-like peptide 1 NPH neutral
Diabetes in the UK: Update on Diabetes Treatment and Care. Why is diabetes increasing? Obesity Increased waist circumference.
 Update on Diabetes Treatment and Care Tahseen A Chowdhury Consultant Diabetologist Royal London and Mile End Hospitals Diabetes prevalence (thousands) Diabetes in the UK: 1995-21 3 25 2 15 1 5 Type 1 Type
Update on Diabetes Treatment and Care Tahseen A Chowdhury Consultant Diabetologist Royal London and Mile End Hospitals Diabetes prevalence (thousands) Diabetes in the UK: 1995-21 3 25 2 15 1 5 Type 1 Type
Diabetes Mellitus case studies. Jana Vinklerová
 Diabetes Mellitus case studies Jana Vinklerová Definition of diabetes (metabolic disorder) Chronically raised blood glucose (hyperglycaemia) Insulin/Glucagon Insulin is responsible for lowering glucose
Diabetes Mellitus case studies Jana Vinklerová Definition of diabetes (metabolic disorder) Chronically raised blood glucose (hyperglycaemia) Insulin/Glucagon Insulin is responsible for lowering glucose
Diabete: terapia nei pazienti a rischio cardiovascolare
 Diabete: terapia nei pazienti a rischio cardiovascolare Giorgio Sesti Università Magna Graecia di Catanzaro Cardiovascular mortality in relation to diabetes mellitus and a prior MI: A Danish Population
Diabete: terapia nei pazienti a rischio cardiovascolare Giorgio Sesti Università Magna Graecia di Catanzaro Cardiovascular mortality in relation to diabetes mellitus and a prior MI: A Danish Population
What s New in Diabetes Treatment. Disclosures
 What s New in Diabetes Treatment Shiri Levy M.D. Henry Ford Hospital Senior Staff Physician Service Chief, West Bloomfield Hospital Endocrinology, Metabolism, Bone and Mineral Disorders Disclosures None
What s New in Diabetes Treatment Shiri Levy M.D. Henry Ford Hospital Senior Staff Physician Service Chief, West Bloomfield Hospital Endocrinology, Metabolism, Bone and Mineral Disorders Disclosures None
Chief of Endocrinology East Orange General Hospital
 Targeting the Incretins System: Can it Improve Our Ability to Treat Type 2 Diabetes? Darshi Sunderam, MD Darshi Sunderam, MD Chief of Endocrinology East Orange General Hospital Age-adjusted Percentage
Targeting the Incretins System: Can it Improve Our Ability to Treat Type 2 Diabetes? Darshi Sunderam, MD Darshi Sunderam, MD Chief of Endocrinology East Orange General Hospital Age-adjusted Percentage
Evidence-Based Glucose Management in Type 2 Diabetes
 Evidence-Based Glucose Management in Type 2 Diabetes James R. Gavin III, MD, PhD CEO and Chief Medical Officer Healing Our Village, Inc. Clinical Professor of Medicine Emory University School of Medicine
Evidence-Based Glucose Management in Type 2 Diabetes James R. Gavin III, MD, PhD CEO and Chief Medical Officer Healing Our Village, Inc. Clinical Professor of Medicine Emory University School of Medicine
Multiple Small Feedings of the Mind: Diabetes. Sonja K Fredrickson, MD, BC-ADM March 7, 2014
 Multiple Small Feedings of the Mind: Diabetes Sonja K Fredrickson, MD, BC-ADM March 7, 2014 Question 1: Setting A1c Goals Describe the evidence based approach to determining the target HgbA1c in different
Multiple Small Feedings of the Mind: Diabetes Sonja K Fredrickson, MD, BC-ADM March 7, 2014 Question 1: Setting A1c Goals Describe the evidence based approach to determining the target HgbA1c in different
Management of Diabetes Mellitus: A Primary Care Perspective. Screening for Diabetes Advantages of HbA1c as a Diagnostic Test
 Management of Diabetes Mellitus: A Primary Care Perspective Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest Screening
Management of Diabetes Mellitus: A Primary Care Perspective Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest Screening
Oral Pharmacologic Treatment of Type 2 Diabetes Mellitus
 Oral Pharmacologic Treatment of Type 2 Diabetes Mellitus You should be offering psychosocial care to all patients with diabetes, says the ADA. Here are the specific recommendations. Summary Recommendation
Oral Pharmacologic Treatment of Type 2 Diabetes Mellitus You should be offering psychosocial care to all patients with diabetes, says the ADA. Here are the specific recommendations. Summary Recommendation
CASE A2 Managing Between-meal Hypoglycemia
 Managing Between-meal Hypoglycemia 1 I would like to discuss this case of a patient who, overall, was doing well on her therapy until she made an important lifestyle change to lose weight. This is a common
Managing Between-meal Hypoglycemia 1 I would like to discuss this case of a patient who, overall, was doing well on her therapy until she made an important lifestyle change to lose weight. This is a common
Dept of Diabetes Main Desk
 Dept of Diabetes Main Desk 01202 448060 Glucose management in Type 2 Diabetes in Adults The natural history of type 2 diabetes is for HbA1c to deteriorate with time. A stepwise approach to treatment is
Dept of Diabetes Main Desk 01202 448060 Glucose management in Type 2 Diabetes in Adults The natural history of type 2 diabetes is for HbA1c to deteriorate with time. A stepwise approach to treatment is
Hanyang University Guri Hospital Chang Beom Lee
 Hanyang University Guri Hospital Chang Beom Lee Meal prayer, Van Brekelenkam 17 th C Introduction 2012 ADA/EASD Position Statement Proper Patients for Pioglitazone β-cell Preservation by Pioglitazone Benefit
Hanyang University Guri Hospital Chang Beom Lee Meal prayer, Van Brekelenkam 17 th C Introduction 2012 ADA/EASD Position Statement Proper Patients for Pioglitazone β-cell Preservation by Pioglitazone Benefit
Age-adjusted Percentage of U.S. Adults Who Were Obese or Who Had Diagnosed Diabetes
 Age-adjusted Percentage of U.S. Adults Who Were Obese or Who Had Diagnosed Diabetes Obesity (BMI 30 kg/m 2 ) 1994 2000 2009 No Data 26.0% Diabetes 1994 2000 2009
Age-adjusted Percentage of U.S. Adults Who Were Obese or Who Had Diagnosed Diabetes Obesity (BMI 30 kg/m 2 ) 1994 2000 2009 No Data 26.0% Diabetes 1994 2000 2009
The Diabetes Link to Heart Disease
 The Diabetes Link to Heart Disease Anthony Abe DeSantis, MD September 18, 2015 University of WA Division of Metabolism, Endocrinology and Nutrition Oswald Toosweet Case #1 68 yo M with T2DM Diagnosed DM
The Diabetes Link to Heart Disease Anthony Abe DeSantis, MD September 18, 2015 University of WA Division of Metabolism, Endocrinology and Nutrition Oswald Toosweet Case #1 68 yo M with T2DM Diagnosed DM
MANAGING DIABETES IN 2017 WHAT TO ADD, WHEN AND WHY? December 8, 2017 Maria Wolfs MD MHSc FRCPC
 MANAGING DIABETES IN 2017 WHAT TO ADD, WHEN AND WHY? December 8, 2017 Maria Wolfs MD MHSc FRCPC Faculty Disclosure Faculty: Maria Wolfs MD, MHSc, FRCPC Assistant Professor, University of Toronto Endocrinologist,
MANAGING DIABETES IN 2017 WHAT TO ADD, WHEN AND WHY? December 8, 2017 Maria Wolfs MD MHSc FRCPC Faculty Disclosure Faculty: Maria Wolfs MD, MHSc, FRCPC Assistant Professor, University of Toronto Endocrinologist,
Glycemic control a matter of life and death
 Glycemic control a matter of life and death Linda Garcia Mellbin MD PhD Specialist in Cardiology & Internal medicine Dep of Cardiology Karolinska University Hospital /Karolinska Institutet Mortality (%)
Glycemic control a matter of life and death Linda Garcia Mellbin MD PhD Specialist in Cardiology & Internal medicine Dep of Cardiology Karolinska University Hospital /Karolinska Institutet Mortality (%)
Newer Drugs in the Management of Type 2 Diabetes Mellitus
 Newer Drugs in the Management of Type 2 Diabetes Mellitus Dr. C. Dinesh M. Naidu Professor of Pharmacology, Kamineni Institute of Medical Sciences, Narketpally. 1 Presentation Outline Introduction Pathogenesis
Newer Drugs in the Management of Type 2 Diabetes Mellitus Dr. C. Dinesh M. Naidu Professor of Pharmacology, Kamineni Institute of Medical Sciences, Narketpally. 1 Presentation Outline Introduction Pathogenesis
Updates in Diabetes and Cardiovascular Disease Management: Are You Making the Link?
 Updates in Diabetes and Cardiovascular Disease Management: Are You Making the Link? Denise Kolanczyk, PharmD, BCPS AQ Cardiology 1 Erika Hellenbart, PharmD, BCPS 2 Jennifer D Souza, PharmD, CDE, BC ADM
Updates in Diabetes and Cardiovascular Disease Management: Are You Making the Link? Denise Kolanczyk, PharmD, BCPS AQ Cardiology 1 Erika Hellenbart, PharmD, BCPS 2 Jennifer D Souza, PharmD, CDE, BC ADM
Diabetes Mellitus. Medical Management and Latest Developments Dr Ahmad Abou-Saleh
 Diabetes Mellitus Medical Management and Latest Developments Dr Ahmad Abou-Saleh What is Diabetes Mellitus? A disease characterised by a state of chronic elevation of blood glucose levels due to: - The
Diabetes Mellitus Medical Management and Latest Developments Dr Ahmad Abou-Saleh What is Diabetes Mellitus? A disease characterised by a state of chronic elevation of blood glucose levels due to: - The
Quick Reference Guide
 2018 Clinical Practice Guidelines Quick Reference Guide 416569-18 guidelines.diabetes.ca diabetes.ca 1-800-BANTING (226-8464) Screening and diagnosis of type 2 diabetes in adults Assess risk factors for
2018 Clinical Practice Guidelines Quick Reference Guide 416569-18 guidelines.diabetes.ca diabetes.ca 1-800-BANTING (226-8464) Screening and diagnosis of type 2 diabetes in adults Assess risk factors for
Practical Diabetes. Nic Crook. (and don t use so many charts) Kuirau Specialists 1239 Ranolf Street Rotorua. Rotorua Hospital Private Bag 3023 Rotorua
 Kuirau Specialists 1239 Ranolf Street Rotorua. Rotorua Hospital Private Bag 3023 Rotorua") Practical Diabetes (and don t use so many charts) Nic Crook Rotorua Hospital Private Bag 3023 Rotorua Kuirau Specialists 1239 Ranolf Street Rotorua Worldwide rates of diabetes mellitus: predictions 80
Practical Diabetes (and don t use so many charts) Nic Crook Rotorua Hospital Private Bag 3023 Rotorua Kuirau Specialists 1239 Ranolf Street Rotorua Worldwide rates of diabetes mellitus: predictions 80
Update on Diabetes Canadian Society of Internal Medicine Oct 11, 2018
 https://www.australiawidefirstaid.com.au/what-is-diabetes/ Update on Diabetes Canadian Society of Internal Medicine Oct 11, 2018 Praveena Sivapalan MD, FRCPC Division of General Internal Medicine, University
https://www.australiawidefirstaid.com.au/what-is-diabetes/ Update on Diabetes Canadian Society of Internal Medicine Oct 11, 2018 Praveena Sivapalan MD, FRCPC Division of General Internal Medicine, University
Management of Diabetes Mellitus: A Primary Care Perspective
 Management of Diabetes Mellitus: A Primary Care Perspective Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest Screening
Management of Diabetes Mellitus: A Primary Care Perspective Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest Screening
Pharmacology Updates. Quang T Nguyen, FACP, FACE, FTOS 11/18/17
 Pharmacology Updates Quang T Nguyen, FACP, FACE, FTOS 11/18/17 14 Classes of Drugs Available for the Treatment of Type 2 DM in the USA ### Class A1c Reduction Hypoglycemia Weight Change Dosing (times/day)
Pharmacology Updates Quang T Nguyen, FACP, FACE, FTOS 11/18/17 14 Classes of Drugs Available for the Treatment of Type 2 DM in the USA ### Class A1c Reduction Hypoglycemia Weight Change Dosing (times/day)
Oral Agents. Ian Gallen Consultant Community Diabetologist Royal Berkshire Hospital Reading UK
 Oral Agents Ian Gallen Consultant Community Diabetologist Royal Berkshire Hospital Reading UK What would your ideal diabetes drug do? Effective in lowering HbA1c No hypoglycaemia No effect on weight/ weight
Oral Agents Ian Gallen Consultant Community Diabetologist Royal Berkshire Hospital Reading UK What would your ideal diabetes drug do? Effective in lowering HbA1c No hypoglycaemia No effect on weight/ weight
Older Adults & Optimal Outcome. Individualizing Diabetes Management. Mary Moyer Janci BC-FNP BC-ADM CDE Teaching Associate Diabetes Care Center UWMC
 Older Adults & Optimal Outcome Individualizing Diabetes Management Mary Moyer Janci BC-FNP BC-ADM CDE Teaching Associate Diabetes Care Center UWMC What is Diabetes? METABOLIC DISEASE Food breakdown (carbohydrates,
Older Adults & Optimal Outcome Individualizing Diabetes Management Mary Moyer Janci BC-FNP BC-ADM CDE Teaching Associate Diabetes Care Center UWMC What is Diabetes? METABOLIC DISEASE Food breakdown (carbohydrates,
Current Diabetes Care for Internists:2011
 Current Diabetes Care for Internists:2011 Petch Rawdaree, DM, MSc, DLSHTM Faculty of Medicine Vajira Hospital University of Bangkok Metropolis 19 th January 2011 ก ก 1. ก ก ก ก 2. ก ก ก ก ก 3. ก ก ก ก
Current Diabetes Care for Internists:2011 Petch Rawdaree, DM, MSc, DLSHTM Faculty of Medicine Vajira Hospital University of Bangkok Metropolis 19 th January 2011 ก ก 1. ก ก ก ก 2. ก ก ก ก ก 3. ก ก ก ก
Management of Type 2 Diabetes. Why Do We Bother to Achieve Good Control in DM2. Insulin Secretion. The Importance of BP and Glucose Control
 Insulin Secretion Management of Type 2 Diabetes DG van Zyl Why Do We Bother to Achieve Good Control in DM2 % reduction 0-5 -10-15 -20-25 -30-35 -40 The Importance of BP and Glucose Control Effects of tight
Insulin Secretion Management of Type 2 Diabetes DG van Zyl Why Do We Bother to Achieve Good Control in DM2 % reduction 0-5 -10-15 -20-25 -30-35 -40 The Importance of BP and Glucose Control Effects of tight
MANAGEMENT OF TYPE 2 DIABETES
 MANAGEMENT OF TYPE 2 DIABETES 3 Month trial of lifestyle changes. Refer to DESMOND structured education programme. Set glycaemic target HbA1c < 7.0% (53mmol/mol) or individualised If HbA1c > 53mmol/mol
MANAGEMENT OF TYPE 2 DIABETES 3 Month trial of lifestyle changes. Refer to DESMOND structured education programme. Set glycaemic target HbA1c < 7.0% (53mmol/mol) or individualised If HbA1c > 53mmol/mol
Case study for CME Diabetes up-to-date management
 Case study for CME Diabetes up-to-date management Dr Ole Schmiedel, MRCP MD FRACP Physician and Endocrinologist Service Clinical Director Auckland Diabetes Centre GP referral to Auckland Diabetes Centre
Case study for CME Diabetes up-to-date management Dr Ole Schmiedel, MRCP MD FRACP Physician and Endocrinologist Service Clinical Director Auckland Diabetes Centre GP referral to Auckland Diabetes Centre
6/1/2018. Lou Haenel, IV, DO, FACE, FACOI Endocrinology Roper St Francis Charleston, SC THE OMINOUS OCTET: HOW PATHOPHYSIOLOGY AND THERAPY MERGE
 Lou Haenel, IV, DO, FACE, FACOI Endocrinology Roper St Francis Charleston, SC THE OMINOUS OCTET: HOW PATHOPHYSIOLOGY AND THERAPY MERGE 1 2 3 Sulfonylureas Glipizide Glyburide Glimeperide 4 Metformin Gold
Lou Haenel, IV, DO, FACE, FACOI Endocrinology Roper St Francis Charleston, SC THE OMINOUS OCTET: HOW PATHOPHYSIOLOGY AND THERAPY MERGE 1 2 3 Sulfonylureas Glipizide Glyburide Glimeperide 4 Metformin Gold
Vascular complications
 Vascular complications December 8, 2018 Faculty Disclosure Faculty: Kim Connelly, MBBS, PhD, FRACP Associate Professor of Medicine, University of Toronto Cardiologist, St. Michael s Hospital Relationships
Vascular complications December 8, 2018 Faculty Disclosure Faculty: Kim Connelly, MBBS, PhD, FRACP Associate Professor of Medicine, University of Toronto Cardiologist, St. Michael s Hospital Relationships
Type 2 Diabetes in Adolescents
 Type 2 Diabetes in Adolescents Disclosures Paid consultant, Eli Lilly, Inc, Pediatric Type 2 Diabetes Clinical Trials Outline The burden of diabetes Treatment and Prevention Youth Diabetes Prevention Clinic
Type 2 Diabetes in Adolescents Disclosures Paid consultant, Eli Lilly, Inc, Pediatric Type 2 Diabetes Clinical Trials Outline The burden of diabetes Treatment and Prevention Youth Diabetes Prevention Clinic
CV Risk Management in Diabetes Mellitus
 CV Risk Management in Diabetes Mellitus J R Minkoff MD, FACP Endocrinology Clinical Professor of Family and Community Medicine University of California, San Francisco Mr. B 40 y/o Latino male c/o fatigue,
CV Risk Management in Diabetes Mellitus J R Minkoff MD, FACP Endocrinology Clinical Professor of Family and Community Medicine University of California, San Francisco Mr. B 40 y/o Latino male c/o fatigue,
Alia Gilani Health Inequalities Pharmacist
 Alia Gilani Health Inequalities Pharmacist THE SOUTH ASIAN HEALTH FOUNDATION (U.K.) (Registered Charity No. 1073178) 1. Case Study 2. Factors influencing prescribing 3. Special Considerations 4. Prescribing
Alia Gilani Health Inequalities Pharmacist THE SOUTH ASIAN HEALTH FOUNDATION (U.K.) (Registered Charity No. 1073178) 1. Case Study 2. Factors influencing prescribing 3. Special Considerations 4. Prescribing
Preventing Serious Health Consequences of Type 2 Diabetes
 Preventing Serious Health Consequences of Type 2 Diabetes The Evidence Hertzel C. Gerstein MD MSc FRCPC Professor and Population Health Institute Chair in Diabetes Research McMaster University and Hamilton
Preventing Serious Health Consequences of Type 2 Diabetes The Evidence Hertzel C. Gerstein MD MSc FRCPC Professor and Population Health Institute Chair in Diabetes Research McMaster University and Hamilton
DIABETIC RECOGNITION AND MANAGEMENT FOR THE RURAL PHYSICIAN
 DIABETIC RECOGNITION AND MANAGEMENT FOR THE RURAL PHYSICIAN DOUGLAS NOLAN, D.O. I have no conflicts of interest to disclose 1 OBJECTIVES Identify the criteria for diagnosing Pre-diabetes Identify the criteria
DIABETIC RECOGNITION AND MANAGEMENT FOR THE RURAL PHYSICIAN DOUGLAS NOLAN, D.O. I have no conflicts of interest to disclose 1 OBJECTIVES Identify the criteria for diagnosing Pre-diabetes Identify the criteria
ADVANCE Endpoints. Primary outcome. Secondary outcomes
 ADVANCE Trial-NEJM 11,140 type 2 patients with h/o microvascular or macrovascular disease or 1 vascular disease risk factor Control A1c to 6.5% vs standard tx Intensive arm received gliclazide XL 30 to
ADVANCE Trial-NEJM 11,140 type 2 patients with h/o microvascular or macrovascular disease or 1 vascular disease risk factor Control A1c to 6.5% vs standard tx Intensive arm received gliclazide XL 30 to
American Diabetes Association 2018 Guidelines Important Notable Points
 American Diabetes Association 2018 Guidelines Important Notable Points The Standards of Medical Care in Diabetes-2018 by ADA include the most current evidencebased recommendations for diagnosing and treating
American Diabetes Association 2018 Guidelines Important Notable Points The Standards of Medical Care in Diabetes-2018 by ADA include the most current evidencebased recommendations for diagnosing and treating