Susan L. Pinkard, RN Manager, Therapeutic Apheresis Hoxworth Blood Center University Of Cincinnati Academic Health Center Cincinnati, Ohio
|
|
|
- Erin McDonald
- 5 years ago
- Views:
Transcription


1 Susan L. Pinkard, RN Manager, Therapeutic Apheresis Hoxworth Blood Center University Of Cincinnati Academic Health Center Cincinnati, Ohio

2 The Good: What indications we using to initiate photopheresis Our treatment schedule Blood Priming -indications in small children and in patients with lack of ability to tolerate fluid shifts. Outcomes. -indications in small children and in patients with lack of ability to tolerate fluid shifts. The Bad: Managing patients with low body weight Managing patients that do not tolerate fluid shift Managing the instrument when there is abnormal plasma: high bilirubin/liver enzymes high triglycerides Receiving TPN/lipids The Ugly: Managing fluid balance in small children Maintaining HCT of 28% System pressure and red cell pump alarms..don t give up!


3 BMT Indications: As prophylaxis for transplant GFR 65 Pre Week -2; week -1 then following with WBC recovery Acute gut, liver and skin GVHD steroid refractory Chronic GVHD (steroid refractory) including: Skin BOOP Gut/Liver Other uses: CTCL Scleroderma Post lung/cardiac transplant

4 BMT Treatment Schedule: Initiating therapy - both pediatric and adult patients 5 days/week x 4 weeks Tapering Monthly reduction by 1 day/week Never taper immunosuppression drugs the week prior to or the week after tapering photopheresis
5 BMT: First line treatment - methylprednisolone at 1-2mg/kg. Therapy effective - if there is stable disease (no progression) after 2 days of treatment and a response (improvement) after 5 days. Patients with significant progression of disease after 2 days or no evidence of a response after 5 days will be considered to have steroid refractory GVHD. Note: Recent studies have shown no benefit to higher doses of steroids in patients that have not responded to 2mg/kg. Second line treatment of steroid-refractory GVHD is MMF at 15mg/kg three times daily. Patients with significant progression of disease after 3 days or no evidence of a response after 7 days will be considered to have refractory GVHD. Third line treatment of steroid-refractory GVHD is Photopheresis Patients with significant progression of disease after 3 days or no evidence of a response after 7 days will be considered to have refractory acute GVHD.
6 Initiating Therapy - both pediatric and adult patients 2 consecutive days x 6-8 weeks Looking for a response may extend longer Tapering - 2 consecutive days every other week x 4-6 cycles Followed every 3 weeks then to monthly At 1 year consider discontinuing
7 BMT: Quick turn around in patient s condition = shortened hospital stay better outcome Other Conditions: Overall improvement in disease Patient satisfaction compliance to treatment plan Example: CTCL patient receives treatments 2 consecutive days monthly No improvement seen for 4-6 months Patient becomes discouraged, seeks other means of treatment Aggressive upfront therapy improves outcome reduces the need to become aggressive with other medical regimens (chemo, interferon = side effects)


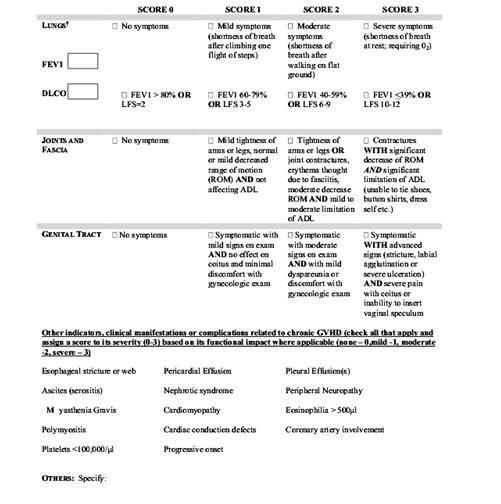
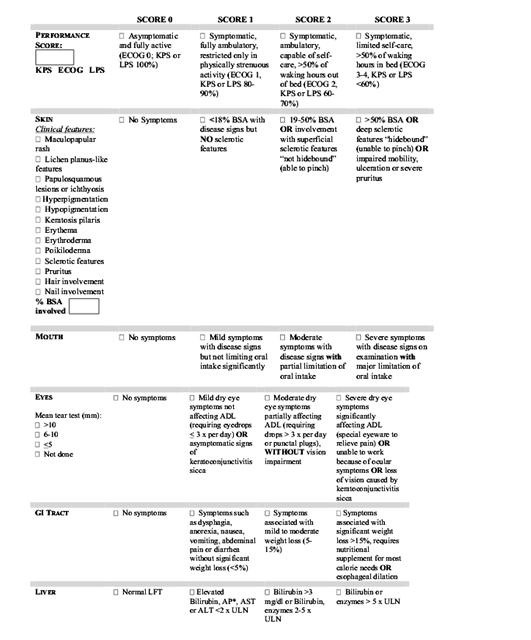
8 Full acute/chronic GVHD exam with staging Performed at just prior to the initiation of treatment (baseline), at two weeks after start of therapy, monthly for 3 months, then every 3 months thereafter



9 CT SCAN - Mosaic attenuation in the lungs with rarefaction of the peripheral pulmonary architecture, diminished prominence of the pulmonary vasculature and bronchial tree with markedly decreased attenuation of the lung parenchyma consist with BO. Poikilodema
10 ASSESSMENT TOOL
11 Laboratory Studies (including) Performed at just prior to the initiation of treatment (baseline), at two weeks after start of therapy, monthly for 3 months, then every 3 months thereafter Plasma cytokines Lymphocyte subsets Activation markers B cell panel sil2r CD45 RA/RO BAFF Foxp3
12 Why? Low body weight calculate patient s total blood volume determine safe ECV range 10-15% of TBV If exceed 15% TBV or patient does not tolerate fluid shifts Prime Instrument Patients that do not tolerate fluid shift including pulmonary, cardiac or renal insufficiency patients What do we use? Compatible Packed Red Blood Cell unit 300mL volume We do not dilute PRBC unit to patient HCT but do add 100mL NS to the unit + return of prime solution
13 Non - blood prime procedures 1500 ml per treatment Blood prime procedures 1500 ml plus the amount processed to prime the instrument roughly 1800 ml Why? Our validation showed that WBC counts on collected cells were significantly improved the more processed With prime approximately 3-4 times patient starting WBC Without prime approximately 6-8 times the patient starting WBC
14 Non - Prime Procedures Maximum collect rate 35 ml/min Blood Prime Procedures During priming do not exceed 20mL/min After prime increase based on child s size and line function ml/min

15 ACD-A Used for all procedures regardless of pediatric or adult procedure WB : AC Ratio Platelet counts under :1 Platelet counts greater than :1 Why ACD-A vs Heparin Acute GVHD gut bleeding Children risk of falling No prolonged anticoagulation
16 Calcium Gluconate 5grams added to 50mL Normal Saline = 100mL volume. Approximately 50mg/mL. Infusion Rate initially started at 10mL/hr (500mg/hr). Must use an infusion pump. Monitor ionized calcium levels: Initially 15 minutes 30 minutes Then every 30 minutes unless needed more frequently performed at bedside using i STAT. Adjust infusion rate as warranted by testing results.

17 What impacts outcome? The sooner treatment is initiated the better the chance of a positive outcome Tapering of other therapies and photopheresis treatments must be done at a different intervals otherwise impact is unknown Compliance with all treatment therapies Following through with medications Compliance with photo schedule
18 Managing patients with low body weight Managing patients that do not tolerate fluid shift Managing the instrument when there is abnormal plasma: o high bilirubin/liver enzymes o high triglycerides o Receiving TPN/lipids
19 Blood Prime instrument Determine if Buffy Coat to be harvested from PRBC unit or patient 6-12 kg kids mainly harvest from PRBC unit kg dependent on how stable child is End Buffy Coat early HCT no more than 16% Reduces reinfusion volume Monitor ionized calcium levels closely until appropriate infusion rate is determined Understand the instrument has an increased anticoagulant infusion at initiation and reinfusion so may need to adjust calcium gluconate infusion rate initially to be higher and then reduce during procedure unit 20 minutes prior to completion
20 Blood Prime regardless if required by calculation of Safe ECV Determine maximum intake usually set at 15% of TBV Watch Buffy coat harvest closely and stop once -% is reached Instrument automatically stops the buffy coat harvest at 24% Ending Buffy early reduces volume as well as reduces photo time

21 Lipemic Plasma? Why as patient not on high fat diet Drugs such as MMF and Cyclosporine cause hyperlipidemia What can we do? Attempt to decrease Bowl Optic Sensor - red cell pump alarm We have had to plasma exchange prior to performing photopheresis
22 Neon plasma linked to liver enzyme elevation especially elevated bilirubin Bright yellow usually ok Dark neon usually instrument looks at it as Red Cells Watch hematocrit on screen if rapidly rises to 3 remove HCT sensor until line becomes pink and then replace sensor allowing you to collect a good buffy coat
23 TPN that contains lipids vs TPN with piggybacked in lipids Prefer piggyback lipids so we can control infusion time following photopheresis Discontinue TPN approximately 2 hours prior to treatment Food during the treatment process We do not limit Diets pre treatment Attempt to limit McDonald s and high fat content foods not always possible

24 Managing fluid balance in small children Maintaining HCT of 28% System pressure and red cell pump alarms..don t give up!
25 Determine if Buffy Coat to be harvested from PRBC unit or patient 6-12 kg kids mainly harvest from PRBC unit kg dependent on how stable child is Harvest from patient reduces volume intake End Buffy Coat early HCT no more than 16% Reduces the treatment volume and reinfusion volume Reducing the Reinfusion Volume May be necessary
26 Blood Prime Procedures Can use some of the Red cells from the PRBC unit if patient can tolerate increased volume to maintain HCT 28% or greater. We give approximately 10/kg if HCT borderline after obtaining physician order Patient already exposed to unit thus limits need for d for additional transfusion Non-Blood Prime Procedures Transfuse as needed

27 Frequently only option is turn machine off Wait for bowl to stop Verify the tubing in the key holes is not kinked adjust if needed Restart watching for the purging of air in the return bag If air not removed stop again tap bowl and restart
28 So Much Fun!!! Adjustments to Bowl Optic Sensor Schedule advanced user training with Therakos


29
Photopheresis Technical Challenges. Lindsay Palomino, BSN RN HP May 6, 2016
 Photopheresis Technical Challenges Lindsay Palomino, BSN RN HP May 6, 2016 No relevant disclosures SCCA Apheresis Unit! Therakos CellEx Photopheresis System For technical challenges and troubleshooting:
Photopheresis Technical Challenges Lindsay Palomino, BSN RN HP May 6, 2016 No relevant disclosures SCCA Apheresis Unit! Therakos CellEx Photopheresis System For technical challenges and troubleshooting:
The impact of processing less blood with the Therakos Cellex Photopheresis System for pediatric patients
 The impact of processing less blood with the Therakos Cellex Photopheresis System for pediatric patients Joanna Wigfield, DO Pediatric Hematology/Oncology Fellow Phoenix Children s Hospital Phoenix Children
The impact of processing less blood with the Therakos Cellex Photopheresis System for pediatric patients Joanna Wigfield, DO Pediatric Hematology/Oncology Fellow Phoenix Children s Hospital Phoenix Children
White Cell Depletion for Leukocytosis
 White Cell Depletion for Leukocytosis Objectives Discuss the indication for leukoreduction Identify IV access needs for patients receiving leukapheresis Outline ways to maintain fluid and electrolyte balance
White Cell Depletion for Leukocytosis Objectives Discuss the indication for leukoreduction Identify IV access needs for patients receiving leukapheresis Outline ways to maintain fluid and electrolyte balance
Review of New Platforms for Blood Prime
 Review of New Platforms for Blood Prime Edwin A. Burgstaler, MT, HP(ASCP) ASFA 2015 Annual Meeting May, 2015 2015 MFMER slide-1 Objectives The participant will recognize the basic steps in performing a
Review of New Platforms for Blood Prime Edwin A. Burgstaler, MT, HP(ASCP) ASFA 2015 Annual Meeting May, 2015 2015 MFMER slide-1 Objectives The participant will recognize the basic steps in performing a
Active UMMC Protocols
 UMMC CRRT 2018 Active UMMC Protocols 1. Standard CRRT Protocol PrismaFlex & NxStage CVVH with Fixed Ratio Regional Citrate Anticoagulation 2. No Anticoagulation Protocol PrismaFlex & NxStage CVVH with
UMMC CRRT 2018 Active UMMC Protocols 1. Standard CRRT Protocol PrismaFlex & NxStage CVVH with Fixed Ratio Regional Citrate Anticoagulation 2. No Anticoagulation Protocol PrismaFlex & NxStage CVVH with
Edwin A. Burgstaler MT, HP (ASCP) Jeffrey L. Winters MD. ASFA 2017 Annual Meeting May 5, MFMER slide-1
 Jeffrey L. Winters MD. ASFA 2017 Annual Meeting May 5, MFMER slide-1") Comparison of Hematopoietic Progenitor Cell (HPC) Collection Using the Spectra Optia Continuous Mononuculear Cell (CMNC) Collections with a 26:1 Anticoagulant Ratio Versus an Anticoagulant ing Technique
Comparison of Hematopoietic Progenitor Cell (HPC) Collection Using the Spectra Optia Continuous Mononuculear Cell (CMNC) Collections with a 26:1 Anticoagulant Ratio Versus an Anticoagulant ing Technique
Operation-Fluids-Electrolytes-Acid Base COMPLICATIONS OF DIALYSIS 2
 Operation-Fluids-Electrolytes-Acid Base COMPLICATIONS OF DIALYSIS 2 Maureen Craig, RN, MSN, CNN University of California Davis Medical Center Sacramento, California macraig@ucdavis.edu Hospital Details
Operation-Fluids-Electrolytes-Acid Base COMPLICATIONS OF DIALYSIS 2 Maureen Craig, RN, MSN, CNN University of California Davis Medical Center Sacramento, California macraig@ucdavis.edu Hospital Details
EXTRACORPOREAL PHOTOPHERESIS MAGGIE FOSTER MANAGER ROTHERHAM PHOTOPHERESIS UNIT
 EXTRACORPOREAL PHOTOPHERESIS MAGGIE FOSTER MANAGER ROTHERHAM PHOTOPHERESIS UNIT AIM OF PRESENTATION Explain about Photopheresis. Rotherham service. Conditions treated Advantages /disadvantages of XTS &
EXTRACORPOREAL PHOTOPHERESIS MAGGIE FOSTER MANAGER ROTHERHAM PHOTOPHERESIS UNIT AIM OF PRESENTATION Explain about Photopheresis. Rotherham service. Conditions treated Advantages /disadvantages of XTS &
Heparin Drip. Ordering
 Heparin Drip Ordering Nurse entering of Heparin drip orders for physicians should only occur in situations when it is not feasible for the physician to enter orders directly Select the Heparin IV Drip
Heparin Drip Ordering Nurse entering of Heparin drip orders for physicians should only occur in situations when it is not feasible for the physician to enter orders directly Select the Heparin IV Drip
BC Cancer Protocol Summary for Treatment of Chronic Lymphocytic Leukemia or Prolymphocytic Leukemia with Fludarabine and rituximab
 BC Cancer Protocol Summary for Treatment of Chronic Lymphocytic Leukemia or Prolymphocytic Leukemia with Fludarabine and rituximab Protocol Code Tumour Group Contact Physicians LYCLLFLUDR Lymphoma Dr.
BC Cancer Protocol Summary for Treatment of Chronic Lymphocytic Leukemia or Prolymphocytic Leukemia with Fludarabine and rituximab Protocol Code Tumour Group Contact Physicians LYCLLFLUDR Lymphoma Dr.
Blood/Blood Component Utilization and Administration Annual Compliance Education
 Blood/Blood Component Utilization and Administration Annual Compliance Education This course contains annual compliance education necessary to meet compliance and regulatory requirements. Instructions:
Blood/Blood Component Utilization and Administration Annual Compliance Education This course contains annual compliance education necessary to meet compliance and regulatory requirements. Instructions:
Therapeutic apheresis (introduction) Orieji Illoh, MD November 21, 2006
 Orieji Illoh, MD November 21, 2006") Therapeutic apheresis (introduction) Orieji Illoh, MD November 21, 2006 Apheresis Removal of blood Separation into component parts One component is retained and remainder is returned History First tried
Therapeutic apheresis (introduction) Orieji Illoh, MD November 21, 2006 Apheresis Removal of blood Separation into component parts One component is retained and remainder is returned History First tried
Paired Comparison of Therapeutic Plasma Exchange using Fenwal Amicus vs. TerumoBCT Spectra Optia
 Paired Comparison of Therapeutic Plasma Exchange using Fenwal Amicus vs. TerumoBCT Spectra Optia Edwin A. Burgstaler MT, HP (ASCP) Sandra C. Bryant M.S. Jeffrey L. Winters M.D. ASFA Annual Meeting May
Paired Comparison of Therapeutic Plasma Exchange using Fenwal Amicus vs. TerumoBCT Spectra Optia Edwin A. Burgstaler MT, HP (ASCP) Sandra C. Bryant M.S. Jeffrey L. Winters M.D. ASFA Annual Meeting May
MASSIVE TRANSFUSION DR.K.HITESH KUMAR FINAL YEAR PG DEPT. OF TRANSFUSION MEDICINE
 MASSIVE TRANSFUSION DR.K.HITESH KUMAR FINAL YEAR PG DEPT. OF TRANSFUSION MEDICINE CONTENTS Definition Indications Transfusion trigger Massive transfusion protocol Complications DEFINITION Massive transfusion:
MASSIVE TRANSFUSION DR.K.HITESH KUMAR FINAL YEAR PG DEPT. OF TRANSFUSION MEDICINE CONTENTS Definition Indications Transfusion trigger Massive transfusion protocol Complications DEFINITION Massive transfusion:
Extracorporeal Photopheresis and Crohn s Disease. Jill Adamski MD, PhD Transfusion Medicine Department of Pathology
 Extracorporeal Photopheresis and Crohn s Disease Jill Adamski MD, PhD Transfusion Medicine Department of Pathology Outline 1. Crohn s Disease (CD) 2. Extracoporeal Photopheresis (ECP) 3. Pilot studies
Extracorporeal Photopheresis and Crohn s Disease Jill Adamski MD, PhD Transfusion Medicine Department of Pathology Outline 1. Crohn s Disease (CD) 2. Extracoporeal Photopheresis (ECP) 3. Pilot studies
NICU Nutrition Pathway
 NICU Nutrition Pathway Safely Infusing NICU TPN Starter and Custom TPN April17 th 2018 Pharmacists: Paul Kasprzak RPH BCPS Kelly Kopec PharmD Major Practice Changes in the Preparation and Administration
NICU Nutrition Pathway Safely Infusing NICU TPN Starter and Custom TPN April17 th 2018 Pharmacists: Paul Kasprzak RPH BCPS Kelly Kopec PharmD Major Practice Changes in the Preparation and Administration
ADULT TRANSFUSION GUIDELINES ORDERED COMPONENT
 ADULT TRANSFUSIN GUIDELINES RDERED Packed red cells (RBCs) RBCs, WBCs, platelets & plasma (minimal) Increase red cell mass and oxygen carrying capacity; generally indicated when Hgb is 7 gm or Hct 21 unless
ADULT TRANSFUSIN GUIDELINES RDERED Packed red cells (RBCs) RBCs, WBCs, platelets & plasma (minimal) Increase red cell mass and oxygen carrying capacity; generally indicated when Hgb is 7 gm or Hct 21 unless
Blood Group Incompatible Renal Transplantation and Apheresis. Liz Wright Clinical Nurse Specialist Great Ormond Street Hospital NHS FT
 Blood Group Incompatible Renal Transplantation and Apheresis Liz Wright Clinical Nurse Specialist Great Ormond Street Hospital NHS FT Background There is growing interest in transplantation across the
Blood Group Incompatible Renal Transplantation and Apheresis Liz Wright Clinical Nurse Specialist Great Ormond Street Hospital NHS FT Background There is growing interest in transplantation across the
BRAVTPCARB. Protocol Code: Breast. Tumour Group: Dr. Karen Gelmon. Contact Physician:
 BCCA Protocol Summary for Palliative Therapy for Metastatic Breast Cancer using Trastuzumab (HERCEPTIN), PACLitaxel and CARBOplatin as First-Line Treatment for Advanced Breast Cancer Protocol Code: Tumour
BCCA Protocol Summary for Palliative Therapy for Metastatic Breast Cancer using Trastuzumab (HERCEPTIN), PACLitaxel and CARBOplatin as First-Line Treatment for Advanced Breast Cancer Protocol Code: Tumour
What is an Apheresis Donation?
 What are Platelets? Platelets are colorless, irregularly shaped bodies found in blood. The primary role of platelets is to prevent bleeding in injured blood vessel walls by forming an aggregate at the
What are Platelets? Platelets are colorless, irregularly shaped bodies found in blood. The primary role of platelets is to prevent bleeding in injured blood vessel walls by forming an aggregate at the
Apheresis: Clinical Indications
 PART 2 Apheresis: Clinical Indications Clinical Vignettes: Hematology Cardiology/Vascular Neurology Solid Organ Transplantation Anatomy of an ASFA Fact Sheet Hematology 40 yo M presenting to the Emergency
PART 2 Apheresis: Clinical Indications Clinical Vignettes: Hematology Cardiology/Vascular Neurology Solid Organ Transplantation Anatomy of an ASFA Fact Sheet Hematology 40 yo M presenting to the Emergency
Physician Orders ADULT Order Set: Respiratory Failure Orders
 [R] = will be ordered Height: cm Weight: kg Allergies: [ ] No known allergies [ ]Medication allergy(s): [ ] Latex allergy [ ]Other: Admission/Transfer/Discharge [ ] Patient Status Initial Inpatient Attending
[R] = will be ordered Height: cm Weight: kg Allergies: [ ] No known allergies [ ]Medication allergy(s): [ ] Latex allergy [ ]Other: Admission/Transfer/Discharge [ ] Patient Status Initial Inpatient Attending
I. Subject: Continuous Aerosolization of Bronchodilators
 I. Subject: Continuous Aerosolization of Bronchodilators II. Indications: A. Acute airflow obstruction in which treatment with an aerosolized bronchodilator is desired for an extended period of time, i.e.
I. Subject: Continuous Aerosolization of Bronchodilators II. Indications: A. Acute airflow obstruction in which treatment with an aerosolized bronchodilator is desired for an extended period of time, i.e.
RELEASED. first steps. Icon Icon name What it means
 Icon Icon name What it means Connection The connection icon appears green when the Sensor feature is on and your transmitter is successfully communicating with your pump. The connection icon appears gray
Icon Icon name What it means Connection The connection icon appears green when the Sensor feature is on and your transmitter is successfully communicating with your pump. The connection icon appears gray
Session 1: Circuit, Anticoagulation and Monitoring. Ashita Tolwani, MD, MSc Noel Oabel, BSN, RN, CNN 2019
 Session 1: Circuit, Anticoagulation and Monitoring Ashita Tolwani, MD, MSc Noel Oabel, BSN, RN, CNN 2019 Goals n Learn how to set up citrate anticoagulation for CVVH, CVVHD, CVVHDF using Prismaflex n Determine
Session 1: Circuit, Anticoagulation and Monitoring Ashita Tolwani, MD, MSc Noel Oabel, BSN, RN, CNN 2019 Goals n Learn how to set up citrate anticoagulation for CVVH, CVVHD, CVVHDF using Prismaflex n Determine
Cycle 1 PERTuzumab (day 1) and trastuzumab (day 2) loading doses: Drug Dose BC Cancer Administration Guideline
 and trastuzumab (day 2) loading doses: Drug Dose BC Cancer Administration Guideline") BC Cancer Protocol Summary for Palliative Therapy for Metastatic Breast Cancer Using PERTuzumab, Trastuzumab (HERCEPTIN), and PACLItaxel as First-Line Treatment for Advanced Breast Cancer Protocol Code:
BC Cancer Protocol Summary for Palliative Therapy for Metastatic Breast Cancer Using PERTuzumab, Trastuzumab (HERCEPTIN), and PACLItaxel as First-Line Treatment for Advanced Breast Cancer Protocol Code:
BC Cancer Protocol Summary for Adjuvant Therapy for Breast Cancer Using Weekly PACLitaxel and Trastuzumab (HERCEPTIN)
") BC Cancer Protocol Summary for Adjuvant Therapy for Breast Cancer Using Weekly PACLitaxel and Trastuzumab (HERCEPTIN) Protocol Code: Tumour Group: Contact Physician: UBRAJTTW Breast Dr. Angela Chan ELIGIBILITY:
BC Cancer Protocol Summary for Adjuvant Therapy for Breast Cancer Using Weekly PACLitaxel and Trastuzumab (HERCEPTIN) Protocol Code: Tumour Group: Contact Physician: UBRAJTTW Breast Dr. Angela Chan ELIGIBILITY:
FLUID MANAGEMENT AND BLOOD COMPONENT THERAPY
 Manual: Section: Protocol #: Approval Date: Effective Date: Revision Due Date: 10/2019 LifeLine Patient Care Protocols Adult/Pediatrics AP1-011 10/2018 10/2018 FLUID MANAGEMENT AND BLOOD COMPONENT THERAPY
Manual: Section: Protocol #: Approval Date: Effective Date: Revision Due Date: 10/2019 LifeLine Patient Care Protocols Adult/Pediatrics AP1-011 10/2018 10/2018 FLUID MANAGEMENT AND BLOOD COMPONENT THERAPY
Corporate Medical Policy
 Corporate Medical Policy Extracorporeal Photopheresis File Name: Origination: Last CAP Review: Next CAP Review: Last Review: extracorporeal_photopheresis 9/2010 8/2017 8/2018 8/2017 Description of Procedure
Corporate Medical Policy Extracorporeal Photopheresis File Name: Origination: Last CAP Review: Next CAP Review: Last Review: extracorporeal_photopheresis 9/2010 8/2017 8/2018 8/2017 Description of Procedure
2/2/2011. Blood Components and Transfusions. Why Blood Transfusion?
 Blood Components and Transfusions Describe blood components Identify nursing responsibilities r/t blood transfusion Discuss factors r/t blood transfusion including blood typing, Rh factor, and cross matching
Blood Components and Transfusions Describe blood components Identify nursing responsibilities r/t blood transfusion Discuss factors r/t blood transfusion including blood typing, Rh factor, and cross matching
An Overview of Blood and Marrow Transplantation
 An Overview of Blood and Marrow Transplantation October 24, 2009 Stephen Couban Department of Medicine Dalhousie University Objectives What are the types of blood and marrow transplantation? Who may benefit
An Overview of Blood and Marrow Transplantation October 24, 2009 Stephen Couban Department of Medicine Dalhousie University Objectives What are the types of blood and marrow transplantation? Who may benefit
Chapter 8 ADMINISTRATION OF BLOOD COMPONENTS
 Chapter 8 ADMINISTRATION OF BLOOD COMPONENTS PRACTICE POINTS Give the right blood product to the right patient at the right time. Failure to correctly check the patient or the pack can be fatal. At the
Chapter 8 ADMINISTRATION OF BLOOD COMPONENTS PRACTICE POINTS Give the right blood product to the right patient at the right time. Failure to correctly check the patient or the pack can be fatal. At the
5/9/2018. Bone marrow failure diseases (aplastic anemia) can be cured by providing a source of new marrow
 can be cured by providing a source of new marrow") 5/9/2018 or Stem Cell Harvest Where we are now, and What s Coming AA MDS International Foundation Indianapolis IN Luke Akard MD May 19, 2018 Infusion Transplant Conditioning Treatment 2-7 days STEM CELL
5/9/2018 or Stem Cell Harvest Where we are now, and What s Coming AA MDS International Foundation Indianapolis IN Luke Akard MD May 19, 2018 Infusion Transplant Conditioning Treatment 2-7 days STEM CELL
Blood Transfusion. What is blood transfusion? What are blood banks? When is a blood transfusion needed? Who can donate blood?
 What is blood transfusion? A blood transfusion is a safe, common procedure in which blood is given through an intravenous (IV) line in one of the blood vessels. A blood transfusion usually takes two to
What is blood transfusion? A blood transfusion is a safe, common procedure in which blood is given through an intravenous (IV) line in one of the blood vessels. A blood transfusion usually takes two to
BMTCN REVIEW COURSE PRE-TRANSPLANT CARE
 BMTCN REVIEW COURSE PRE-TRANSPLANT CARE Jennifer Shamai MS, RN, AOCNS, BMTCN Professional Practice Leader Department of Clinical Practice And Professional Education Click How to edit the Master Experts
BMTCN REVIEW COURSE PRE-TRANSPLANT CARE Jennifer Shamai MS, RN, AOCNS, BMTCN Professional Practice Leader Department of Clinical Practice And Professional Education Click How to edit the Master Experts
R-GDP: Rituximab, Gemcitabine, Dexamethasone &Cisplatin
 : Rituximab, Gemcitabine, Dexamethasone &Cisplatin INDICATION Relapsed or refractory Hodgkin and non-hodgkin lymphoma. Omit Rituximab for patients with Hodgkin Lymphoma or high grade T cell non-hodgkin
: Rituximab, Gemcitabine, Dexamethasone &Cisplatin INDICATION Relapsed or refractory Hodgkin and non-hodgkin lymphoma. Omit Rituximab for patients with Hodgkin Lymphoma or high grade T cell non-hodgkin
Transfusion Therapy & Safety. Mary Grabowski, RN, BSN, BSIA Transfusion Safety Officer PSONEC Fundamentals September, 2015
 Transfusion Therapy & Safety Mary Grabowski, RN, BSN, BSIA Transfusion Safety Officer PSONEC Fundamentals September, 2015 Topics Blood Components Special Processing/Attributes Irradiation Leukoreduction
Transfusion Therapy & Safety Mary Grabowski, RN, BSN, BSIA Transfusion Safety Officer PSONEC Fundamentals September, 2015 Topics Blood Components Special Processing/Attributes Irradiation Leukoreduction
Acute Stroke with Alteplase Administration Order Set
 Review Due Date: 2017 October PATIENT CARE DERS Weight: Adverse Reactions or Intolerances Drug No Yes (list) Food No Yes (list) _ Latex No Yes Admission Admit to Neurology service: Dr. Critical Care Diagnosis:
Review Due Date: 2017 October PATIENT CARE DERS Weight: Adverse Reactions or Intolerances Drug No Yes (list) Food No Yes (list) _ Latex No Yes Admission Admit to Neurology service: Dr. Critical Care Diagnosis:
CRRT Procedures. and Guidelines. CRRT: Guidelines
 CRRT Procedures 2013 and Guidelines Guidelines for the utilization of CRRT (Continuous Renal Replacement Therapies) at Monroe Carell Jr. Children s Hospital at Vanderbilt CRRT: Guidelines CRRT Contacts:
CRRT Procedures 2013 and Guidelines Guidelines for the utilization of CRRT (Continuous Renal Replacement Therapies) at Monroe Carell Jr. Children s Hospital at Vanderbilt CRRT: Guidelines CRRT Contacts:
Nivolumab and Ipilimumab
 Nivolumab and Ipilimumab Indication Advanced (unresectable or metastatic) melanoma. (NICE TA400) ICD-10 codes Codes prefixed with C43 Regimen details Cycles 1-4 Nivolumab and Ipilimumab every 3 weeks Day
Nivolumab and Ipilimumab Indication Advanced (unresectable or metastatic) melanoma. (NICE TA400) ICD-10 codes Codes prefixed with C43 Regimen details Cycles 1-4 Nivolumab and Ipilimumab every 3 weeks Day
Parenteral Nutrition Recommendations for Pediatric Patients
 Fluid Dextrose Amino acid Lipid Parenteral Nutrition Recommendations for Pediatric Patients (Calculated for normal organ function and normal caloric requirements) PN orders are due by 11 AM daily Newborn
Fluid Dextrose Amino acid Lipid Parenteral Nutrition Recommendations for Pediatric Patients (Calculated for normal organ function and normal caloric requirements) PN orders are due by 11 AM daily Newborn
Implementing therapy-delivery, dose adjustments and fluid balance. Eileen Lischer MA, BSN, RN, CNN University of California San Diego March 6, 2018
 Implementing therapy-delivery, dose adjustments and fluid balance. Eileen Lischer MA, BSN, RN, CNN University of California San Diego March 6, 2018 Objectives By the end of this session the learner will
Implementing therapy-delivery, dose adjustments and fluid balance. Eileen Lischer MA, BSN, RN, CNN University of California San Diego March 6, 2018 Objectives By the end of this session the learner will
ULYRICE. Protocol Code. Lymphoma. Tumour Group. Dr. Laurie Sehn. Contact Physician
 BCCA Protocol Summary for the Treatment of Relapsed or Refractory Advanced Stage Aggressive B-Cell Non-Hodgkin s Lymphoma with Ifosfamide, CARBOplatin, Etoposide and rituximab Protocol Code Tumour Group
BCCA Protocol Summary for the Treatment of Relapsed or Refractory Advanced Stage Aggressive B-Cell Non-Hodgkin s Lymphoma with Ifosfamide, CARBOplatin, Etoposide and rituximab Protocol Code Tumour Group
Acknowledgements. Department of Hematological Malignancy and Cellular Therapy, University of Kansas Medical Center
 The Addition of Extracorporeal Photopheresis (ECP) to Tacrolimus and Methotrexate to Prevent Acute and Chronic Graft- Versus Host Disease in Myeloablative Hematopoietic Cell Transplant (HCT) Anthony Accurso,
The Addition of Extracorporeal Photopheresis (ECP) to Tacrolimus and Methotrexate to Prevent Acute and Chronic Graft- Versus Host Disease in Myeloablative Hematopoietic Cell Transplant (HCT) Anthony Accurso,
Principles And Practice For PHOTOPHERESIS
 Principles And Practice For PHOTOPHERESIS Presented by Regina Mack, RN., HP(ASCP) Baylor Scott&White Health System Dallas, Texas Apheresis Department Warnings and Disclosures Off-label and investigative
Principles And Practice For PHOTOPHERESIS Presented by Regina Mack, RN., HP(ASCP) Baylor Scott&White Health System Dallas, Texas Apheresis Department Warnings and Disclosures Off-label and investigative
BC Cancer Protocol for Treatment of Platinum Resistant Epithelial Ovarian Cancer with Bevacizumab and PACLitaxel
 BC Cancer Protocol for Treatment of Platinum Resistant Epithelial Ovarian Cancer with Bevacizumab and PACLitaxel Protocol Code Tumour Group Contact Physician UGOOVBEVP Gynecologic Oncology Dr. Anna Tinker
BC Cancer Protocol for Treatment of Platinum Resistant Epithelial Ovarian Cancer with Bevacizumab and PACLitaxel Protocol Code Tumour Group Contact Physician UGOOVBEVP Gynecologic Oncology Dr. Anna Tinker
Case Study 1: Red Cell Exchange
 Case Study 1: Red Cell Exchange Education Session VI: Pediatric Apheresis Leon Su, MD Section Chief, Transfusion Medicine and Apheresis None Disclosures 8 year old female SCD History of CVA in 2012 Hgb
Case Study 1: Red Cell Exchange Education Session VI: Pediatric Apheresis Leon Su, MD Section Chief, Transfusion Medicine and Apheresis None Disclosures 8 year old female SCD History of CVA in 2012 Hgb
CRRT Fundamentals Pre-Test. AKI & CRRT 2017 Practice Based Learning in CRRT
 CRRT Fundamentals Pre-Test AKI & CRRT 2017 Practice Based Learning in CRRT Question 1 A 72-year-old man with HTN presents to the ED with slurred speech, headache and weakness after falling at home. He
CRRT Fundamentals Pre-Test AKI & CRRT 2017 Practice Based Learning in CRRT Question 1 A 72-year-old man with HTN presents to the ED with slurred speech, headache and weakness after falling at home. He
Pharmacy Prior Authorization
 Pharmacy Prior Authorization AETA BETTER HEALTH PESLVAIA & AETA BETTER HEALTH KIDS Promacta (Medicaid) This fax machine is located in a secure location as required by HIPAA regulations. Complete/review
Pharmacy Prior Authorization AETA BETTER HEALTH PESLVAIA & AETA BETTER HEALTH KIDS Promacta (Medicaid) This fax machine is located in a secure location as required by HIPAA regulations. Complete/review
Ipilimumab in Melanoma
 Ipilimumab in Melanoma Indication: Advanced (unresectable or metastatic) melanoma in adults who have received prior therapy LCNDG criteria to be met: Histologically confirmed unresectable stage III or
Ipilimumab in Melanoma Indication: Advanced (unresectable or metastatic) melanoma in adults who have received prior therapy LCNDG criteria to be met: Histologically confirmed unresectable stage III or
GUIDELINES FOR THE TRANSFUSION OF BLOOD COMPONENTS
 CHILDREN S HOSPITALS AND CLINICS OF MINNESOTA Introduction: GUIDELINES FOR THE TRANSFUSION OF BLOOD COMPONENTS These guidelines have been developed in conjunction with the hospital Transfusion Committee.
CHILDREN S HOSPITALS AND CLINICS OF MINNESOTA Introduction: GUIDELINES FOR THE TRANSFUSION OF BLOOD COMPONENTS These guidelines have been developed in conjunction with the hospital Transfusion Committee.
ELIGIBILITY: small cell or neuroendocrine cancer (pure or mixed) administration of this protocol is restricted to BCCA Cancer Centres
 administration of this protocol is restricted to BCCA Cancer Centres") BCCA Protocol Summary for Treatment of Small Cell or Neuroendocrine Carcinoma of Gynecologic System Origin using PACLitaxel, CISplatin, Etoposide and CARBOplatin with Radiation (GO 95 02) Protocol Code:
BCCA Protocol Summary for Treatment of Small Cell or Neuroendocrine Carcinoma of Gynecologic System Origin using PACLitaxel, CISplatin, Etoposide and CARBOplatin with Radiation (GO 95 02) Protocol Code:
CRRT Fundamentals Pre- and Post- Test. AKI & CRRT Conference 2018
 CRRT Fundamentals Pre- and Post- Test AKI & CRRT Conference 2018 Question 1 Which ONE of the following statements regarding solute clearance in CRRT is MOST correct? A. Convective and diffusive solute
CRRT Fundamentals Pre- and Post- Test AKI & CRRT Conference 2018 Question 1 Which ONE of the following statements regarding solute clearance in CRRT is MOST correct? A. Convective and diffusive solute
PEDIATRIC SPINE SURGERY POST-OP PLAN - Phase:.
 - Phase:. PHYSICIAN S Diagnosis Weight Allergies DETAILS Patient Care Patient Activity Bedrest Maintain Surgical Drain Maintain JP Drain, Measure Output q12h, and PRN Convert IV to INT when tolerating
- Phase:. PHYSICIAN S Diagnosis Weight Allergies DETAILS Patient Care Patient Activity Bedrest Maintain Surgical Drain Maintain JP Drain, Measure Output q12h, and PRN Convert IV to INT when tolerating
Extracorporeal Photopheresis after Solid-Organ Transplant and for Graftversus-Host Disease, Autoimmune Disease and Cutaneous T-Cell Lymphoma
 MP 8.01.16 Extracorporeal Photopheresis after Solid-Organ Transplant and for Graftversus-Host Disease, Autoimmune Disease and Cutaneous T-Cell Lymphoma Medical Policy Section Therapy Issue 12/2013 Original
MP 8.01.16 Extracorporeal Photopheresis after Solid-Organ Transplant and for Graftversus-Host Disease, Autoimmune Disease and Cutaneous T-Cell Lymphoma Medical Policy Section Therapy Issue 12/2013 Original
SARASOTA MEMORIAL HOSPITAL NURSING PROCEDURE
 SARASOTA MEMORIAL HOSPITAL NURSING PROCEDURE TITLE: ISSUED FOR: INTERMITTENT FLUID AND MEDICATION THERAPY Nursing DATE: REVIEWED: PAGES: RESPONSIBILITY: RN, LPN I, LPN II Per Job Description 03/81 8/09
SARASOTA MEMORIAL HOSPITAL NURSING PROCEDURE TITLE: ISSUED FOR: INTERMITTENT FLUID AND MEDICATION THERAPY Nursing DATE: REVIEWED: PAGES: RESPONSIBILITY: RN, LPN I, LPN II Per Job Description 03/81 8/09
Risk Evaluation and Mitigation Strategy (REMS): Cytokine release syndrome and neurological toxicities
: Cytokine release syndrome and neurological toxicities") Risk Evaluation and Mitigation Strategy (REMS): Cytokine release syndrome and neurological toxicities A REMS is a program required by the FDA to manage known or potential serious risks associated with
Risk Evaluation and Mitigation Strategy (REMS): Cytokine release syndrome and neurological toxicities A REMS is a program required by the FDA to manage known or potential serious risks associated with
Wales Critical Care & Trauma Network (North) CITRATE GUIDELINES (Approved May 2015)
 CITRATE GUIDELINES (Approved May 2015)") Wales Critical Care & Trauma Network (North) CITRATE GUIDELINES (Approved May 2015) BCU Citrate Guideline v6 Nov 2015 (Approved by CCSC May 15) 1 BCU Critical Care Guideline for Renal Replacement Therapy
Wales Critical Care & Trauma Network (North) CITRATE GUIDELINES (Approved May 2015) BCU Citrate Guideline v6 Nov 2015 (Approved by CCSC May 15) 1 BCU Critical Care Guideline for Renal Replacement Therapy
PACKAGE LEAFLET: INFORMATION FOR THE USER. octaplaslg mg/ml solution for infusion Human plasma proteins
 PACKAGE LEAFLET: INFORMATION FOR THE USER octaplaslg 45-70 mg/ml solution for infusion Human plasma proteins Read all of this leaflet carefully before you start using this medicine. - Keep this leaflet.
PACKAGE LEAFLET: INFORMATION FOR THE USER octaplaslg 45-70 mg/ml solution for infusion Human plasma proteins Read all of this leaflet carefully before you start using this medicine. - Keep this leaflet.
IR Central Venous Access [ ] Pre Procedure
![IR Central Venous Access [ ] Pre Procedure](/thumbs/90/104119758.jpg "IR Central Venous Access [ ] Pre Procedure") IR Central Venous Access [1050200001] Pre Procedure Case Request/Scheduling Procedure Enter IR Case Request if not already completed (All hospitals except Grant Medical Center) [ ] Case Request IR Lab
IR Central Venous Access [1050200001] Pre Procedure Case Request/Scheduling Procedure Enter IR Case Request if not already completed (All hospitals except Grant Medical Center) [ ] Case Request IR Lab
Extracorporeal Photopheresis
 Extracorporeal Photopheresis Policy Number: 8.01.36 Last Review: 9/2014 Origination: 2/2002 Next Review: 9/2015 Policy Blue Cross and Blue Shield of Kansas City (Blue KC) will provide coverage for extracorporeal
Extracorporeal Photopheresis Policy Number: 8.01.36 Last Review: 9/2014 Origination: 2/2002 Next Review: 9/2015 Policy Blue Cross and Blue Shield of Kansas City (Blue KC) will provide coverage for extracorporeal
*Note - If associate is unsuccessful in their attempt to complete the dosage calculation test
 Competency Statement: Demonstrates ability to use basic mathematic concepts related to the correct administration of medications. Instructional Strategies: Review of basic math concepts, completion of
Competency Statement: Demonstrates ability to use basic mathematic concepts related to the correct administration of medications. Instructional Strategies: Review of basic math concepts, completion of
BPG 03: Continuous Renal Replacement Therapy (CRRT)
") BPG 03: Continuous Renal Replacement Therapy (CRRT) Statement of Best Practice Patient s requiring Continuous Renal Replacement Therapy (CRRT) will receive appropriate therapy to meet their individual
BPG 03: Continuous Renal Replacement Therapy (CRRT) Statement of Best Practice Patient s requiring Continuous Renal Replacement Therapy (CRRT) will receive appropriate therapy to meet their individual
Name of Policy: Extracorporeal Photopheresis
 Name of Policy: Extracorporeal Photopheresis Policy #: 028 Latest Review Date: June 2014 Category: Therapy Policy Grade: A Background/Definitions: As a general rule, benefits are payable under Blue Cross
Name of Policy: Extracorporeal Photopheresis Policy #: 028 Latest Review Date: June 2014 Category: Therapy Policy Grade: A Background/Definitions: As a general rule, benefits are payable under Blue Cross
Photopheresis in Acute Graft-versus- Host Disease Hildegard T. Greinix Medical University of Vienna Austria
 Photopheresis in Acute Graft-versus- Host Disease Hildegard T. Greinix Medical University of Vienna Austria Univ. Klinik für Innere Medizin I Acute GvHD is Serious Complication of Allo HCT Challenge: GvL
Photopheresis in Acute Graft-versus- Host Disease Hildegard T. Greinix Medical University of Vienna Austria Univ. Klinik für Innere Medizin I Acute GvHD is Serious Complication of Allo HCT Challenge: GvL
Lab Values Explained. working at full strength. Other possible causes of an elevated BUN include dehydration and heart failure.
 Patient Education Lab Values Explained Common Tests to Help Diagnose Kidney Disease Lab work, urine samples and other tests may be given as you undergo diagnosis and treatment for renal failure. The test
Patient Education Lab Values Explained Common Tests to Help Diagnose Kidney Disease Lab work, urine samples and other tests may be given as you undergo diagnosis and treatment for renal failure. The test
PHYSIOLOGY AND MANAGEMENT OF THE SEPTIC PATIENT
 PHYSIOLOGY AND MANAGEMENT OF THE SEPTIC PATIENT Melanie Sanchez, RN, MSNE, OCN, CCRN Clinical Nurse III City of Hope National Medical Center HOW THE EXPERTS TREAT HEMATOLOGIC MALIGNANCIES LAS VEGAS, NV
PHYSIOLOGY AND MANAGEMENT OF THE SEPTIC PATIENT Melanie Sanchez, RN, MSNE, OCN, CCRN Clinical Nurse III City of Hope National Medical Center HOW THE EXPERTS TREAT HEMATOLOGIC MALIGNANCIES LAS VEGAS, NV
Presentation Created by; Shana Chiborak RN CNCC (C) Nurse Coordinator Blood Management Service May 2016
 Nurse Coordinator Blood Management Service May 2016") Presentation Created by; Shana Chiborak RN CNCC (C) Nurse Coordinator Blood Management Service May 2016 What is Cryoprecipitate? Cryoprecipitate contains factor VIII (8), fibrinogen, and von Willebrand
Presentation Created by; Shana Chiborak RN CNCC (C) Nurse Coordinator Blood Management Service May 2016 What is Cryoprecipitate? Cryoprecipitate contains factor VIII (8), fibrinogen, and von Willebrand
MASSIVE TRANSFUSION PROTOCOL
 MASSIVE TRANSFUSION PROTOCOL IF YOU ANTICIPATE EMERGENT NEED FOR LARGE AMOUNTS OF BLOOD IN A SHORT PERIOD OF TIME Call Blood Bank: 6622121 Tell them you have a patient who needs a Massive Transfusion and
MASSIVE TRANSFUSION PROTOCOL IF YOU ANTICIPATE EMERGENT NEED FOR LARGE AMOUNTS OF BLOOD IN A SHORT PERIOD OF TIME Call Blood Bank: 6622121 Tell them you have a patient who needs a Massive Transfusion and
CHAPTER 3 SECTION 1.6B HEART-LUNG AND LUNG TRANSPLANTATION TRICARE POLICY MANUAL M, MARCH 15, 2002 SURGERY AND RELATED SERVICES
 TRICARE POLICY MANUAL 6010.47-M, MARCH 15, 2002 SURGERY AND RELATED SERVICES CHAPTER 3 SECTION 1.6B ISSUE DATE: October 27, 1995 AUTHORITY: 32 CFR 199.4(e)(5) I. CODES A. CPT 1 Procedure Codes 33930, 33935,
TRICARE POLICY MANUAL 6010.47-M, MARCH 15, 2002 SURGERY AND RELATED SERVICES CHAPTER 3 SECTION 1.6B ISSUE DATE: October 27, 1995 AUTHORITY: 32 CFR 199.4(e)(5) I. CODES A. CPT 1 Procedure Codes 33930, 33935,
LYMPHAPHERESIS IN ORGAN TRANSPLANTATIOH:
 Cytapheresis and Plasma Exchange: Clinical Indications, pages 219-226 1982 Alan R. Llss, Inc., 150 Fifth Avenue, New York, NY 10011 LYMPHAPHERESIS IN ORGAN TRANSPLANTATIOH: PRELIMINARY REPORT S. Iwatsuki,
Cytapheresis and Plasma Exchange: Clinical Indications, pages 219-226 1982 Alan R. Llss, Inc., 150 Fifth Avenue, New York, NY 10011 LYMPHAPHERESIS IN ORGAN TRANSPLANTATIOH: PRELIMINARY REPORT S. Iwatsuki,
ADULT POST NEUROLOGIC INTERVENTION ORDERS 2 of 4
 9 Actual 9 Estimated DOWNTIME INTERVENTION 1 of 4 Weight kg 9 Actual 9 Estimated Height cm ALLERGIES: REFER TO ALLERGY PROFILE/ POWERCHART Admit to Dr.: Bed Type: Dx: ( ) Check, circle and/or fill in all
9 Actual 9 Estimated DOWNTIME INTERVENTION 1 of 4 Weight kg 9 Actual 9 Estimated Height cm ALLERGIES: REFER TO ALLERGY PROFILE/ POWERCHART Admit to Dr.: Bed Type: Dx: ( ) Check, circle and/or fill in all
Cisplatin + Etoposide IV / Oral therapy followed by Chemo-radiotherapy in Small Cell Carcinoma of the Cervix
 Cisplatin + Etoposide IV / Oral therapy followed by Chemo-radiotherapy in Small Cell Carcinoma of the Cervix Indication: Neoadjuvant chemotherapy followed by Chemo-radiotherapy in Small Cell Carcinoma
Cisplatin + Etoposide IV / Oral therapy followed by Chemo-radiotherapy in Small Cell Carcinoma of the Cervix Indication: Neoadjuvant chemotherapy followed by Chemo-radiotherapy in Small Cell Carcinoma
Consent Laboratory Transfuse RBC
 Peds Blood Product Infusion Order Set (386) [386] Blood product review will be performed unless exclusion criteria met. MD: Please note if transfusion giv en outside of parameter, please justify use in
Peds Blood Product Infusion Order Set (386) [386] Blood product review will be performed unless exclusion criteria met. MD: Please note if transfusion giv en outside of parameter, please justify use in
PEDIATRIC SPINE SURGERY POST-OP PLAN - Phase: Pediatric Spine Surgery General Orders
 - Phase: Pediatric Spine Surgery General Orders PHYSICIAN S Diagnosis Weight Allergies Patient Care Patient Activity Bedrest Maintain Surgical Drain Maintain JP Drain, Measure Output q12h, and PRN Convert
- Phase: Pediatric Spine Surgery General Orders PHYSICIAN S Diagnosis Weight Allergies Patient Care Patient Activity Bedrest Maintain Surgical Drain Maintain JP Drain, Measure Output q12h, and PRN Convert
DERBY-BURTON CANCER NETWORK CONTROLLED DOC NO:
 OBINUTUZUMAB+CHLORAMBUCIL Regimen RDH; Day 1 and 2 Dose to be given on Ward Available for Routine Use in Burton in-patient Derby in-patient Burton day-case Derby day-case Burton community Derby community
OBINUTUZUMAB+CHLORAMBUCIL Regimen RDH; Day 1 and 2 Dose to be given on Ward Available for Routine Use in Burton in-patient Derby in-patient Burton day-case Derby day-case Burton community Derby community
CELLULAR THERAPY QUIZ. Correct answers and rationale
 CELLULAR THERAPY QUIZ Correct answers and rationale In January 2018, registered cellular therapy (CT) facilities were asked to participate in the quiz to determine the educational needs of the users regarding
CELLULAR THERAPY QUIZ Correct answers and rationale In January 2018, registered cellular therapy (CT) facilities were asked to participate in the quiz to determine the educational needs of the users regarding
Infusion of intravenous gamma globulin (immunoglobulins)
") Infusion of intravenous gamma globulin (immunoglobulins) OBJECTIVES Intravenous gamma globulin therapy is indicated for replacement therapy in patients with primary and secondary antibody deficiency syndromes.
Infusion of intravenous gamma globulin (immunoglobulins) OBJECTIVES Intravenous gamma globulin therapy is indicated for replacement therapy in patients with primary and secondary antibody deficiency syndromes.
BC Cancer Protocol Summary for Treatment of Platinum Resistant Epithelial Ovarian Cancer with Bevacizumab and Vinorelbine
 BC Cancer Protocol Summary for Treatment of Platinum Resistant Epithelial Ovarian Cancer with Bevacizumab and Vinorelbine Protocol Code Tumour Group Contact Physician UGOOVBEVV Gynecologic Oncology Dr.
BC Cancer Protocol Summary for Treatment of Platinum Resistant Epithelial Ovarian Cancer with Bevacizumab and Vinorelbine Protocol Code Tumour Group Contact Physician UGOOVBEVV Gynecologic Oncology Dr.
R-GDP: Rituximab, Gemcitabine, Dexamethasone &Cisplatin
 : Rituximab, &Cisplatin INDICATION Relapsed or refractory Hodgkin and non-hodgkin lymphoma. Omit Rituximab for patients with Hodgkin Lymphoma. TREATMENT INTENT Palliative or curative depending on context.
: Rituximab, &Cisplatin INDICATION Relapsed or refractory Hodgkin and non-hodgkin lymphoma. Omit Rituximab for patients with Hodgkin Lymphoma. TREATMENT INTENT Palliative or curative depending on context.
ACTEMRA Risk Mitigation Strategy Presenter Name, Degree
 ACTEMRA Risk Mitigation Strategy Presenter Name, Degree Medical Science Liaison Genentech, Inc. 1 Indications and Dosage Rheumatoid Arthritis (RA) (1 of 2) Indication in RA ACTEMRA (tocilizumab) is indicated
ACTEMRA Risk Mitigation Strategy Presenter Name, Degree Medical Science Liaison Genentech, Inc. 1 Indications and Dosage Rheumatoid Arthritis (RA) (1 of 2) Indication in RA ACTEMRA (tocilizumab) is indicated
Extracorporeal Photopheresis Description
 Subject: Extracorporeal Photopheresis Page: 1 of 36 Last Review Status/Date: September 2015 Extracorporeal Photopheresis Description Extracorporeal photopheresis (ECP) is a leukapheresis-based immunomodulatory
Subject: Extracorporeal Photopheresis Page: 1 of 36 Last Review Status/Date: September 2015 Extracorporeal Photopheresis Description Extracorporeal photopheresis (ECP) is a leukapheresis-based immunomodulatory
ISOVALERIC ACIDAEMIA -ACUTE DECOMPENSATION (standard version)
") Contact Details Name: Hospital Telephone: This protocol has 5 pages ISOVALERIC ACIDAEMIA -ACUTE DECOMPENSATION (standard version) Please read carefully. Meticulous treatment is very important as there
Contact Details Name: Hospital Telephone: This protocol has 5 pages ISOVALERIC ACIDAEMIA -ACUTE DECOMPENSATION (standard version) Please read carefully. Meticulous treatment is very important as there
FloTrac Sensor and Edwards PreSep Central Venous Oximetry Catheter Case Presentations
 Edwards FloTrac Sensor & Edwards Vigileo Monitor FloTrac Sensor and Edwards PreSep Central Venous Oximetry Catheter Case Presentations 1 Topics System Configuration FloTrac Sensor and PreSep Catheter Thoracotomy
Edwards FloTrac Sensor & Edwards Vigileo Monitor FloTrac Sensor and Edwards PreSep Central Venous Oximetry Catheter Case Presentations 1 Topics System Configuration FloTrac Sensor and PreSep Catheter Thoracotomy
Basic Fluid and Electrolytes
 Basic Fluid and Electrolytes Chapter 22 Basic Fluid and Electrolytes Introduction Infants and young children have a greater need for water and are more vulnerable to alterations in fluid and electrolyte
Basic Fluid and Electrolytes Chapter 22 Basic Fluid and Electrolytes Introduction Infants and young children have a greater need for water and are more vulnerable to alterations in fluid and electrolyte
ADULT Updated: September 4, 2018
 Updated: September 4, 2018 Regimen Reference Order ARIA: LYMP [R-CHOP alt. R-DHAP] Planned Course: Indication for Use: Every 21 days for 6 cycles (R-CHOP given on cycles 1, 3 and 5; R-DHAP given on cycles
Updated: September 4, 2018 Regimen Reference Order ARIA: LYMP [R-CHOP alt. R-DHAP] Planned Course: Indication for Use: Every 21 days for 6 cycles (R-CHOP given on cycles 1, 3 and 5; R-DHAP given on cycles
St George Hospital Renal Department Guideline: INTERNAL ONLY ANTICOAGULATION - COMMENCEMENT OF HAEMODIALYSIS
 ANTICOAGULATION - COMMENCEMENT OF HAEMODIALYSIS Summary Aim: To prevent clotting of the extracorporeal circuit during haemodialysis If there are no contraindications, heparin can be used. In the first
ANTICOAGULATION - COMMENCEMENT OF HAEMODIALYSIS Summary Aim: To prevent clotting of the extracorporeal circuit during haemodialysis If there are no contraindications, heparin can be used. In the first
Components of Blood. N26 Blood Administration 4/24/2012. Cabrillo College ADN/C. Madsen RN, MSN 1. Formed elements Cells. Plasma. What can we give?
 Components of Blood Formed elements Cells Erythrocytes (RBCs) Leukocytes (WBCs) Thrombocytes (platelets) Plasma 90% water 10% solutes Proteins, clotting factors 1 What can we give? Whole blood Packed RBC
Components of Blood Formed elements Cells Erythrocytes (RBCs) Leukocytes (WBCs) Thrombocytes (platelets) Plasma 90% water 10% solutes Proteins, clotting factors 1 What can we give? Whole blood Packed RBC
Iron Overload in Sickle Cell Disease Review of Cause and Treatment
 Iron Overload in Sickle Cell Disease Review of Cause and Treatment Susan M. Carson RN, MSN, CPNP Nurse Practitioner III Hematology Program Children s Hospital Los Angeles Objectives Describe the effect
Iron Overload in Sickle Cell Disease Review of Cause and Treatment Susan M. Carson RN, MSN, CPNP Nurse Practitioner III Hematology Program Children s Hospital Los Angeles Objectives Describe the effect
GOOVIPPC. Protocol Code: Gynecology. Tumour Group: Paul Hoskins. Contact Physician: James Conklin. Contact Pharmacist:
 BCCA Protocol Summary for Primary Treatment of Stage III less than or equal to 1 cm Visible Residual Invasive Epithelial Ovarian Cancer or Stage I Grade 3 or Stage II Grade 3 Papillary Serous Ovarian Cancer
BCCA Protocol Summary for Primary Treatment of Stage III less than or equal to 1 cm Visible Residual Invasive Epithelial Ovarian Cancer or Stage I Grade 3 or Stage II Grade 3 Papillary Serous Ovarian Cancer
IV Fluids. Nursing B23. Objectives. Serum Osmolality
 IV Fluids Nursing B23 Objectives Discuss the purpose of IV Discuss nursing interventions in IV therapy Identify complications of IV therapy Differentiate between peripheral line, central line, and PICC
IV Fluids Nursing B23 Objectives Discuss the purpose of IV Discuss nursing interventions in IV therapy Identify complications of IV therapy Differentiate between peripheral line, central line, and PICC
Chapter 4 Section 24.1
 Surgery Chapter 4 Section 24.1 Issue Date: October 27, 1995 Authority: 32 CFR 199.4(e)(5) 1.0 CPT 1 PROCEDURE CODES 32850-32854, 33930-33935 2.0 DIAGNOSTIC RELATED GROUPS (DRGs) 495 for lung transplant.
Surgery Chapter 4 Section 24.1 Issue Date: October 27, 1995 Authority: 32 CFR 199.4(e)(5) 1.0 CPT 1 PROCEDURE CODES 32850-32854, 33930-33935 2.0 DIAGNOSTIC RELATED GROUPS (DRGs) 495 for lung transplant.
Pharmacy Prior Authorization
 Pharmacy Prior Authorization MERC CARE (MEDICAID) Promacta (Medicaid) This fax machine is located in a secure location as required by HIPAA regulations. Complete/review information, sign and date. Fax
Pharmacy Prior Authorization MERC CARE (MEDICAID) Promacta (Medicaid) This fax machine is located in a secure location as required by HIPAA regulations. Complete/review information, sign and date. Fax
Lung Pathway Group Cisplatin & IV Vinorelbine in Non- Small Cell Lung Cancer (NSCLC)
") Lung Pathway Group Cisplatin & IV Vinorelbine in Non- Small Cell Lung Cancer (NSCLC) Indication: First line in radical/induction treatment in locally advanced NSCLC First line palliative treatment in advanced/metastatic
Lung Pathway Group Cisplatin & IV Vinorelbine in Non- Small Cell Lung Cancer (NSCLC) Indication: First line in radical/induction treatment in locally advanced NSCLC First line palliative treatment in advanced/metastatic
CLINICAL GUIDELINES. Summary of Literature and Recommendations Concerning Immunization and Steroid Injections Thomas J. Gilbert M.D., M.P.P.
 CLINICAL GUIDELINES Summary of Literature and Recommendations Concerning Immunization and Steroid Injections Thomas J. Gilbert M.D., M.P.P. 11/2/15 Several practices routinely delay steroid injections
CLINICAL GUIDELINES Summary of Literature and Recommendations Concerning Immunization and Steroid Injections Thomas J. Gilbert M.D., M.P.P. 11/2/15 Several practices routinely delay steroid injections
Standard care plan for Carboplatin and Etoposide Chemotherapy References
 CHEMOTHERAPY CARE PLAN Document Title: Document Type: Subject: Approved by: Currency: Carboplatin/Etoposide Chemotherapy Clinical Guideline Standard Care Plan 2 Years Review date: Author(s): Standard care
CHEMOTHERAPY CARE PLAN Document Title: Document Type: Subject: Approved by: Currency: Carboplatin/Etoposide Chemotherapy Clinical Guideline Standard Care Plan 2 Years Review date: Author(s): Standard care
Lung Injury after HCT
 Lung Injury after HCT J. Douglas Rizzo, MD, MS Financial Disclosure None SCS06_1.ppt Background HCT an important therapeutic modality for malignant and non-malignant diseases Pulmonary Toxicity common
Lung Injury after HCT J. Douglas Rizzo, MD, MS Financial Disclosure None SCS06_1.ppt Background HCT an important therapeutic modality for malignant and non-malignant diseases Pulmonary Toxicity common
Math for Meds. College of Southern Nevada. Practice Problems. Nursing 211
 Math for Meds College of Southern Nevada Nursing 211 Name: Date: Directions: 1. Solve the dosage calculation problems utilizing the method of your choice. 2. Show your work! 3.Divide math out to the thousandth
Math for Meds College of Southern Nevada Nursing 211 Name: Date: Directions: 1. Solve the dosage calculation problems utilizing the method of your choice. 2. Show your work! 3.Divide math out to the thousandth
BRAJACTT. Protocol Code. Breast. Tumour Group. Dr. Karen Gelmon. Contact Physician
 BC Cancer Protocol Summary for Adjuvant Therapy for Breast Cancer using DOXOrubicin and Cyclophosphamide followed by PACLitaxel and Trastuzumab (HERCEPTIN) Protocol Code Tumour Group Contact Physician
BC Cancer Protocol Summary for Adjuvant Therapy for Breast Cancer using DOXOrubicin and Cyclophosphamide followed by PACLitaxel and Trastuzumab (HERCEPTIN) Protocol Code Tumour Group Contact Physician
SARASOTA MEMORIAL HOSPITAL DEPARTMENT POLICY
 PS1006 SARASOTA MEMORIAL HOSPITAL DEPARTMENT POLICY TITLE: PHARMACEUTICALS FOR CRITICAL CARE AREAS, HEMODIALYSIS, PACU, EMERGENCY CARE CENTER, CARDIAC CARE AREAS, NEURO PROGRESSIVE CARE, AND THE MECKLER
PS1006 SARASOTA MEMORIAL HOSPITAL DEPARTMENT POLICY TITLE: PHARMACEUTICALS FOR CRITICAL CARE AREAS, HEMODIALYSIS, PACU, EMERGENCY CARE CENTER, CARDIAC CARE AREAS, NEURO PROGRESSIVE CARE, AND THE MECKLER