Classification of Glomerular Diseases and Defining Individual Glomerular Lesions: Developing International Consensus
|
|
|
- Lindsey Chambers
- 6 years ago
- Views:
Transcription
1 Classification of Glomerular Diseases and Defining Individual Glomerular Lesions: Developing International Consensus Mark Haas MD, PhD Department of Pathology & Laboratory Medicine Cedars-Sinai Medical Center Los Angeles, California USA
2 Statement of Disclosure Mark Haas serves as a paid consultant on pathology adjudication committees for two industry-sponsored clinical trials: Shire ViroPharma Treatment of Acute ABMR AstraZeneca Treatment of Proliferative Lupus Nephritis Neither represents a conflict of interest relevant to any of the material presented in this talk.
3 Brief summary of currently used glomerular disease classifications Similarities/differences in derivation, approach The Oxford/MEST classification of IgA nephropathy: the evidence-based standard Update to include crescents Expert opinion-based classifications: the ISN/RPS lupus nephritis classification Improving this and other opinion-based classifications Mayo Clinic/RPS proposals for standardization of reporting of GN and grading of chronic changes Ongoing international efforts to standardize definitions of individual glomerular lesions across different classifications
4 Currently Utilized Morphologic Classification Schemes for Glomerular Diseases IgA Nephropathy Oxford (MEST) Classification Cattran et al, Kidney Int 76: , 2009 Roberts et al, Kidney Int 76: ISN/RPS Classification of Lupus Nephritis Weening et al, Kidney Int 65: , 2004 Columbia Classifiation of FSGS D Agati et al, Am J Kidney Diseases 43: , 2004 Classification of ANCA-GN (Leiden) Berden et al, J Am Soc Nephrol 21: , 2010 Classification of Diabetic Nephropathy (Leiden) Cohen Tervaert et al, J Am Soc Nephrol 21: , 2010
5 These Classifications Differ in How They Were Derived Oxford Classification of IgA Nephropathy Evidence-based derivation based on reproducibility between pathologists and correlation with clinical outcomes (slope of egfr decline, composite endpoint of ESRD/>50% decline in egfr) - Took 5 years to develop ISN/RPS Classification of Lupus Nephritis Consensus of expert opinion, based on existing literature and experience with previous iterations of the WHO classification Columbia Classification of FSGS Consensus of expert opinion, based on existing literature Classifications of ANCA-GN and Diabetic Nephropathy Consensus of expert opinion, based on existing literature and single-center clinico-pathologic studies
6 The Classifications Also Differ in Their Approach The Oxford Classification is not a grading system per se, but rather assesses five morphologic parameters shown to correlate with clinical outcomes and/or response to therapy, using evidence-based cutoffs for these parameters (M, E, S, T, C). However, with regard to clinical correlation Oxford has generally proved superior to previous classifications of IgA nephropathy based on specific classes or grades (e.g., Lee and Haas). By contrast, each of the other classifications divide lesions into specific histologic subtypes (Columbia FSGS, ANCA- GN), or numbered classes and subclasses (ISN/RPS, Diabetic Nephropathy).

7 M1 M1E1 M1S1 M1S1T2
8 Multivariate Determinants of Survival from ESRD or >50% Decline in egfr (2394 patients) All patients No Immunosuppression Any Immunosuppression HR 95% CI p HR 95% CI p HR 95% CI p egfr at biopsy < < TA MAP (mmhg) <0.001 TA Proteinuria (g/day) < < <0.001 M (1 versus 0) E (1 versus 0) S (1 versus 0) T (1-2 versus 0) < < <0.001 Crescents (any versus none)
9 Multivariate Determinants of Survival from ESRD or >50% Decline in egfr (2394 patients) All patients No Immunosuppression Any Immunosuppression HR 95% CI p HR 95% CI p HR 95% CI p egfr at biopsy < < TA MAP (mmhg) <0.001 TA Proteinuria (g/day) < < <0.001 M (1 versus 0) E (1 versus 0) S (1 versus 0) T (1-2 versus 0) < < <0.001 Crescents (any versus none) Haas, Verhave,., Troyanov, Katafuchi, JASN 28: , 2017
10 Haas, Verhave,., Troyanov, Katafuchi, JASN 28: , 2017

11 A crescent (C) score was thus added to the Oxford MEST score (MEST-C): C0 no crescents (cellular or fibrocellular) C1 crescents in <25% of glomeruli identifies patients at risk of poor outcome if not given immunosuppressive therapy C2 crescents in >25% of glomeruli identifies patients at risk of poor outcome even if given immunosuppressive therapy
12 ISN/RPS Classification of Lupus Nephritis (2004) Class I Minimal mesangial lupus nephritis Normal glomeruli by LM, mesangial immune deposits by IF Class II Mesangial proliferative lupus nephritis Purely mesangial hypercellularity or matrix expansion by LM with mesangial immune deposits (may be few subendothelial and/or subepithelial deposits by IF or EM, but not by LM) Class III Focal lupus nephritis (segmental and/or global, active and/or sclerosing, endocapillary and/or extracapillary GN involving <50% of glomeruli, with or without mesangial alterations) (A) Purely active lesions; focal proliferative (A/C) Active and chronic lesions; focal proliferative and sclerosing (C) Chronic inactive; focal sclerosing
13 ISN/RPS Classification (2004), continued Class IV Diffuse lupus nephritis (segmental and/or global, active and/or sclerosing, endocapillary and/or extracapillary GN involving >50% glomeruli, with or without mesangial alterations) Class IV is further divided into diffuse segmental (IV-S) when >50% of involved glomeruli have segmental lesions (involving less than half of the glomerular tuft) and diffuse global (IV-G) when >50% of involved glomeruli have global lesions (involving at least half of the tuft) (A) Purely active lesions; diffuse segmental [IV-S (A)] or diffuse global [IV-G (A)] proliferative (A/C) Active and chronic lesions; diffuse segmental [IV-S (A/C)] or diffuse global [IV-G (A/C)] proliferative and sclerosing (C) Chronic inactive; diffuse segmental [IV-S (C)] or diffuse global [IV-G (C)] sclerosing of Class V Membranous lupus nephritis (with or without mesangial alterations) Class VI Advanced sclerosing lupus nephritis (>90% globally sclerotic without residual activity)
14 Furness and Taub, Am J Surg Pathol 30: , 2006 Kappa values ISN/RPS Class 0.53 WHO 1995 Class 0.44 ISN/RPS IV-G vs IV-S 0.35 ISN/RPS (A) vs (A/C) vs (C) 0.33

15 G S
16 Yokoyama et al, Kidney Int 66: , 2004
17 Plan for Resolution of the IV-G/IV-S Issue (I. Bajema et al, Leiden) Level 1: Recommend abandoning the segmental/global subdivision within Class IV as specified in ISN/RPS classification. Level 2: Evaluate the clinical significance of glomerular necrotizing lesions, defined as fibrin associated with GBM disruption and/or lysis of the mesangial matrix, with or without karyorrhexis. Incorporate such lesions into a revised classification if so indicated by the data.
18 The Designations of A, A/C, and C within Classes III and IV are not very helpful (or reproducible) The great majority of Class III and IV lesions are A/C A biopsy with multiple necrotizing and crescentic lesions and 15% IFTA will be graded A/C, as will a biopsy with 60% IFTA and a single glomerulus with endocapillary hypercellularity and/or a cellular crescent Level 1 recommendation: Replace A, A/C, and C with a modified version of the more granular NIH activity and chronicity indices Level 2: Establish evidence-based cutoffs and weighting for the different components of AI and CI
19 Activity & Chronicity Indices in Lupus Nephritis Activity Index (each 0 3; max 24) Austin et al., Am J Med 75: , 1983 Glomerular cell proliferation Cellular crescents x2 Fibrinoid necrosis/karyorrhexis x2 Wire loops, hyaline thrombi Glomerular leukocyte infiltration Interstitial mononuclear cell infiltration Chronicity Index (each 0 3; max 12) Glomerular sclerosis Fibrous crescents Interstitial fibrosis Tubular atrophy Modified AI (each 0-3; max 24) Modified CI (each 0-3; max 12) Endocapillary hypercellularity Cellular/fibrocellular crescents x2 Fibrinoid necrosis x2 Hyaline deposits ( WL, hyal. thrombi) Glomerular neutrophils, karyorrhexis Interstitial Inflammation Glomerular sclerosis (glob + segm) Fibrous crescents Interstitial fibrosis Tubular atrophy For modified indices: 0 - none; 1 - <25%; %; 3 - >50%
20 The ISN/RPS Classes are based entirely on glomerular lesions, and do not consider tubulo-interstital or vascular lesions However, in a number of different glomerular diseases (e.g., IgA nephropathy), it is well documented that one of if not the strongest predictor of poor clinical outcomes (e.g., ESRD, 50% reduction in egfr, doubling of SCr, rate of egfr decline) is the extent of interstitial fibrosis and tubular atrophy (IFTA)
21 Interstitial inflammation Tubular atrophy Interstitial fibrosis Yu et al, Kidney Int 77: , 2010
22 Activity and chronicity indices DO include interstitial fibrosis (CI), tubular atrophy (CI), and interstitial inflammation (AI); level 2 studies will evaluate cutoffs, whether IF and TA should be considered separately or together, and whether inflammation in areas of IF/TA should be considered in the AI. The prognostic impact of vascular lesions including TMA, lupus vasculopathy (vascular IC deposits without associated inflammation), and vasculitis will be evaluated in level 2.
23 Classification and Reporting of GN: The 2015 Mayo Clinic/RPS Consensus Meeting 2 Basic Goals Develop a basic classification of GN based primarily on etiology/pathophysiology, rather than morphologic pattern Develop a way to incorporate this into the pathology report: Logical Sequential Reproducible And most importantly addresses the key clinical questions
24 An Example 61-year old man with monoclonal gammopathy (IgG-kappa with M spikes ranging from 0.5 to 0.9 g/dl over time), low serum C3 with normal C4, microscopic and intermittent gross hematuria, few RBC casts. Serum creatinine 1.3 mg/dl Bone marrow 8% plasma cells: MGUS

25

26 C3 Negative IgG, IgM, IgA, C1q, kappa and lambda


27 Mesangial deposits Subendothelial and subepithelial deposits
28 Diagnosis Primary disease: C3 glomerulonephritis Pattern of injury: Mesangial and focal/segmental endocapillary proliferative GN Additional features: Mild (10%) tubular atrophy and interstitial fibrosis
29 Summary The main aim and purpose of consensus meeting was to classify glomerulonephritis based on the underlying pathophysiology and etiology. Based on current knowledge there are five basic classes of GN: immune complex GN pauci-immune GN anti-gbm GN monoclonal Ig GN C3 glomerulopathy Specific entities exist within each group The consensus document provides guidelines for the kidney biopsy report on glomerulonephritis


30
31 A proposal for standardized grading of chronic changes in native kidney biopsy specimens S. Sethi et al, Kidney Int 91: , 2017 Score= 0 Score= 1 Score= 2 Score= 3 Glomerulosclerosis (GS score) <10% 10-25% 26-50% >50% Interstitial fibrosis (IF score) <10% 10-25% 26-50% >50% Tubular atrophy (TA score) <10% 10-25% 26-50% >50% Arteriosclerosis (CV score) < thickness of media Minimal chronic changes 0-1 Mild chronic changes 2-4 Moderate chronic changes 5-7 Severe chronic changes >7 thickness of media

32 Interstitial inflammation Tubular atrophy Interstitial fibrosis Yu et al, Kidney Int 77: , 2010

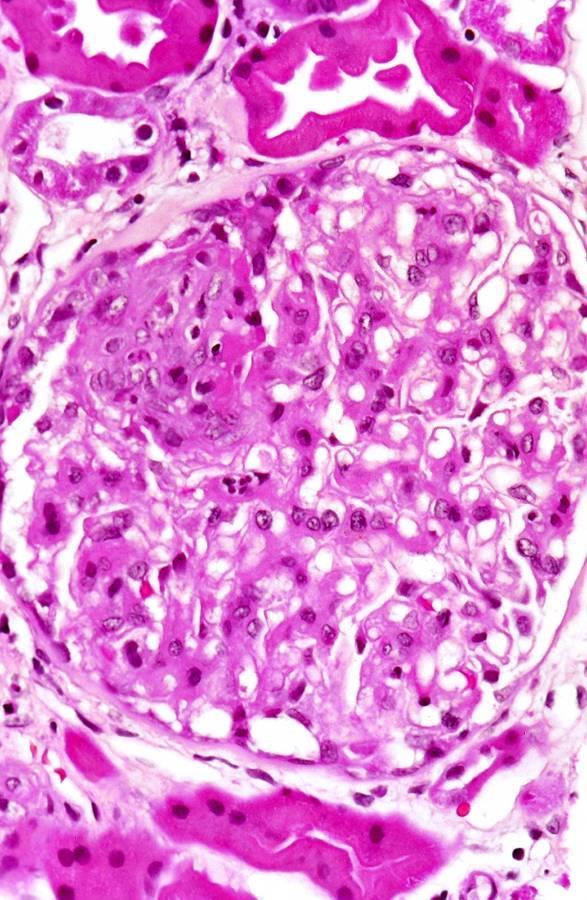
33 Is this a crescent?
34 Definition of a Cellular Crescent Oxford IgAN ISN/RPS Neptune/INTEGRATE Cure GN extracapillary hypercellu- extracapillary cell extracapillary cell >10% of Bowman s larity of >2 cell layers and proliferation of >2 proliferation of >2 cell space with >2 layers involving >10% of the cell layers, with cell layers with >50% cells or fibrosis; capsular circumference, >50% of the lesion of the lesion occupied composed of >50% composed of >50% cells occupied by cells by cells and <50% by cells and <50% and fibrin, and <50% and involving matrix matrix fibrous matrix >25% of the circumference of Bowman s capsule
35 In response to this need for uniform definitions of individual lesions seen on renal biopsies, in 2016 the Renal Pathology Society (RPS) agreed to form a committee consisting of 12 RPS members from North America, Europe, and Asia to develop a consensus set of definitions for individual glomerular lesions seen on histologic examination of renal biopsies that can be applied across the varying disease classification schemes that currently exist, and can be applied to future disease classifications as well.
36 At a meeting of the committee held in San Antonio, Texas in concert with the USCAP meeting in March 2017, a list of individual glomerular lesions to be defined was compiled. This list includes 53 lesions subdivided into seven categories: mesangial (3), capillary (14), extracapillary (15), sclerosing and collapse (8), necrosis (2), glomerular size (3), and injury patterns (8).
37 How can we improve on current classifications that are based on expert opinion? A 2-step approach: 1. Modify definitions of and cutoffs/thresholds for specific lesions where there are inconsistencies, vagueness, and omissions; use examples to clarify details and illustrate difficult issues 2. Evidence-based, multicenter study involving scoring of parameters and relation to clinical outcome(s), using results to guide modification of the existing classification

38 Thank you for your attention. Any questions?
Classification of Glomerular Diseases and Defining Individual Glomerular Lesions: Developing International Consensus
 Classification of Glomerular Diseases and Defining Individual Glomerular Lesions: Developing International Consensus Mark Haas MD, PhD Department of Pathology & Laboratory Medicine Cedars-Sinai Medical
Classification of Glomerular Diseases and Defining Individual Glomerular Lesions: Developing International Consensus Mark Haas MD, PhD Department of Pathology & Laboratory Medicine Cedars-Sinai Medical
IgA Nephropathy: Morphologic Findings Associated with Disease Progression and Therapeutic Response A Working Group Approach
 I IgA Nephropathy: Morphologic Findings Associated with Disease Progression and Therapeutic Response A Working Group Approach Mark Haas Department of Pathology & Lab Medicine Cedars-Sinai Medical Center
I IgA Nephropathy: Morphologic Findings Associated with Disease Progression and Therapeutic Response A Working Group Approach Mark Haas Department of Pathology & Lab Medicine Cedars-Sinai Medical Center
Mayo Clinic/ RPS Consensus Report on Classification, Diagnosis, and Reporting of Glomerulonephritis
 Mayo Clinic/ RPS Consensus Report on Classification, Diagnosis, and Reporting of Glomerulonephritis Sanjeev Sethi, MD, PhD Department of Laboratory Medicine and Pathology Disclosure Relevant Financial
Mayo Clinic/ RPS Consensus Report on Classification, Diagnosis, and Reporting of Glomerulonephritis Sanjeev Sethi, MD, PhD Department of Laboratory Medicine and Pathology Disclosure Relevant Financial
Dr Ian Roberts Oxford. Oxford Pathology Course 2010 for FRCPath Illustration-Cellular Pathology. Oxford Radcliffe NHS Trust
 Dr Ian Roberts Oxford Oxford Pathology Course 2010 for FRCPath Plan of attack: Diagnostic approach to the renal biopsy Differential diagnosis of the clinical syndromes of renal disease Microscopy Step
Dr Ian Roberts Oxford Oxford Pathology Course 2010 for FRCPath Plan of attack: Diagnostic approach to the renal biopsy Differential diagnosis of the clinical syndromes of renal disease Microscopy Step
Glomerular pathology in systemic disease
 Glomerular pathology in systemic disease Lecture outline Lupus nephritis Diabetic nephropathy Glomerulonephritis Associated with Bacterial Endocarditis and Other Systemic Infections Henoch-Schonlein Purpura
Glomerular pathology in systemic disease Lecture outline Lupus nephritis Diabetic nephropathy Glomerulonephritis Associated with Bacterial Endocarditis and Other Systemic Infections Henoch-Schonlein Purpura
Dr Ian Roberts Oxford. Oxford Pathology Course 2010 for FRCPath Illustration-Cellular Pathology. Oxford Radcliffe NHS Trust
 Dr Ian Roberts Oxford Oxford Pathology Course 2010 for FRCPath Present the basic diagnostic features of the commonest conditions causing proteinuria & haematuria Highlight diagnostic pitfalls Nephrotic
Dr Ian Roberts Oxford Oxford Pathology Course 2010 for FRCPath Present the basic diagnostic features of the commonest conditions causing proteinuria & haematuria Highlight diagnostic pitfalls Nephrotic
Enterprise Interest None
 Enterprise Interest None Lupus Nephritis Ingeborg Bajema Lupus nephritis: the basics Up to 60% of patients with SLE develop lupus nephritis during the course of their disease Lupus nephritis is associated
Enterprise Interest None Lupus Nephritis Ingeborg Bajema Lupus nephritis: the basics Up to 60% of patients with SLE develop lupus nephritis during the course of their disease Lupus nephritis is associated
Surgical Pathology Report
 Louisiana State University Health Sciences Center Department of Pathology Shreveport, Louisiana Accession #: Collected: Received: Reported: 6/1/2012 09:18 6/2/2012 09:02 6/2/2012 Patient Name: Med. Rec.
Louisiana State University Health Sciences Center Department of Pathology Shreveport, Louisiana Accession #: Collected: Received: Reported: 6/1/2012 09:18 6/2/2012 09:02 6/2/2012 Patient Name: Med. Rec.
Lupus Nephritis. Ingeborg Bajema
 Lupus Nephritis Ingeborg Bajema Lupus nephritis: the basics Up to 60% of patients with SLE develop lupus nephritis during the course of their disease Lupus nephritis is associated with considerable morbidity
Lupus Nephritis Ingeborg Bajema Lupus nephritis: the basics Up to 60% of patients with SLE develop lupus nephritis during the course of their disease Lupus nephritis is associated with considerable morbidity
Case 3. ACCME/Disclosure. Laboratory results. Clinical history 4/13/2016
 Case 3 Lynn D. Cornell, M.D. Mayo Clinic, Rochester, MN Cornell.Lynn@mayo.edu USCAP Renal Case Conference March 13, 2016 ACCME/Disclosure Dr. Cornell has nothing to disclose Clinical history 57-year-old
Case 3 Lynn D. Cornell, M.D. Mayo Clinic, Rochester, MN Cornell.Lynn@mayo.edu USCAP Renal Case Conference March 13, 2016 ACCME/Disclosure Dr. Cornell has nothing to disclose Clinical history 57-year-old
A clinical syndrome, composed mainly of:
 Nephritic syndrome We will discuss: 1)Nephritic syndrome: -Acute postinfectious (poststreptococcal) GN -IgA nephropathy -Hereditary nephritis 2)Rapidly progressive GN (RPGN) A clinical syndrome, composed
Nephritic syndrome We will discuss: 1)Nephritic syndrome: -Acute postinfectious (poststreptococcal) GN -IgA nephropathy -Hereditary nephritis 2)Rapidly progressive GN (RPGN) A clinical syndrome, composed
Renal Pathology 1: Glomerulus. With many thanks to Elizabeth Angus PhD for EM photographs
 Renal Pathology 1: Glomerulus With many thanks to Elizabeth Angus PhD for EM photographs Anatomy of the Kidney http://www.yalemedicalgroup.org/stw/page.asp?pageid=stw028980 The Nephron http://www.beltina.org/health-dictionary/nephron-function-kidney-definition.html
Renal Pathology 1: Glomerulus With many thanks to Elizabeth Angus PhD for EM photographs Anatomy of the Kidney http://www.yalemedicalgroup.org/stw/page.asp?pageid=stw028980 The Nephron http://www.beltina.org/health-dictionary/nephron-function-kidney-definition.html
Histopathology: Glomerulonephritis and other renal pathology
 Histopathology: Glomerulonephritis and other renal pathology These presentations are to help you identify basic histopathological features. They do not contain the additional factual information that you
Histopathology: Glomerulonephritis and other renal pathology These presentations are to help you identify basic histopathological features. They do not contain the additional factual information that you
Glomerular diseases mostly presenting with Nephritic syndrome
 Glomerular diseases mostly presenting with Nephritic syndrome 1 The Nephritic Syndrome Pathogenesis: proliferation of the cells in glomeruli & leukocytic infiltrate Injured capillary walls escape of RBCs
Glomerular diseases mostly presenting with Nephritic syndrome 1 The Nephritic Syndrome Pathogenesis: proliferation of the cells in glomeruli & leukocytic infiltrate Injured capillary walls escape of RBCs
Case # 2 3/27/2017. Disclosure of Relevant Financial Relationships. Clinical history. Clinical history. Laboratory findings
 Case # 2 Christopher Larsen, MD Arkana Laboratories Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position to influence or control the content
Case # 2 Christopher Larsen, MD Arkana Laboratories Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position to influence or control the content
Statement of Disclosure
 Statement of Disclosure Mark Haas serves as a paid consultant on pathology adjudication committees for two industry-sponsored clinical trials: Shire ViroPharma Treatment of Acute ABMR AstraZeneca Treatment
Statement of Disclosure Mark Haas serves as a paid consultant on pathology adjudication committees for two industry-sponsored clinical trials: Shire ViroPharma Treatment of Acute ABMR AstraZeneca Treatment
Monoclonal Gammopathies and the Kidney. Tibor Nádasdy, MD The Ohio State University, Columbus, OH
 Monoclonal Gammopathies and the Kidney Tibor Nádasdy, MD The Ohio State University, Columbus, OH Monoclonal gammopathy of renal significance (MGRS) Biopsies at OSU (n=475) between 2007 and 2016 AL or AH
Monoclonal Gammopathies and the Kidney Tibor Nádasdy, MD The Ohio State University, Columbus, OH Monoclonal gammopathy of renal significance (MGRS) Biopsies at OSU (n=475) between 2007 and 2016 AL or AH
Ordering Physician. Collected REVISED REPORT. Performed. IgG IF, Renal MCR. Lambda IF, Renal MCR. C1q IF, Renal. MCR Albumin IF, Renal MCR
 RenalPath Level IV Wet Ts IgA I Renal IgM I Renal Kappa I Renal Renal Bx Electron Microscopy IgG I Renal Lambda I Renal C1q I Renal C3 I Renal Albumin I Renal ibrinogen I Renal Mayo Clinic Dept. of Lab
RenalPath Level IV Wet Ts IgA I Renal IgM I Renal Kappa I Renal Renal Bx Electron Microscopy IgG I Renal Lambda I Renal C1q I Renal C3 I Renal Albumin I Renal ibrinogen I Renal Mayo Clinic Dept. of Lab
The Banff Classification for Diagnosis of Renal Allograft Rejection: Updates from the 2017 Banff Conference
 The Banff Classification for Diagnosis of Renal Allograft Rejection: Updates from the 2017 Banff Conference Mark Haas Cedars-Sinai Medical Center Los Angeles, California, USA Statement of Disclosure Mark
The Banff Classification for Diagnosis of Renal Allograft Rejection: Updates from the 2017 Banff Conference Mark Haas Cedars-Sinai Medical Center Los Angeles, California, USA Statement of Disclosure Mark
Interesting case seminar: Native kidneys Case Report:
 Interesting case seminar: Native kidneys Case Report: Proximal tubulopathy and light chain deposition disease presented as severe pulmonary hypertension with right-sided cardiac dysfunction and nephrotic
Interesting case seminar: Native kidneys Case Report: Proximal tubulopathy and light chain deposition disease presented as severe pulmonary hypertension with right-sided cardiac dysfunction and nephrotic
Dr Ian Roberts Oxford
 Dr Ian Roberts Oxford Oxford Pathology Course 2010 for FRCPath Present the basic diagnostic features of the commonest conditions causing renal failure Highlight diagnostic pitfalls. Crescentic GN: renal
Dr Ian Roberts Oxford Oxford Pathology Course 2010 for FRCPath Present the basic diagnostic features of the commonest conditions causing renal failure Highlight diagnostic pitfalls. Crescentic GN: renal
Dr. Ghadeer Mokhtar Consultant pathologists and nephropathologist, KAU
 Dr. Ghadeer Mokhtar Consultant pathologists and nephropathologist, KAU CLINICAL HISTORY A 4 year old Saudi girl presented to the ER with generalized body swelling, decrease urine output with passing dark
Dr. Ghadeer Mokhtar Consultant pathologists and nephropathologist, KAU CLINICAL HISTORY A 4 year old Saudi girl presented to the ER with generalized body swelling, decrease urine output with passing dark
Prof. Franco Ferrario Nephropathology Unit Department of Pathology San Gerardo Hospital Università Milan Bicocca Monza, Italy.
 The role of repeated biopsies in the management of Lupus Nephritis Franco Ferrario, Milan, Italy Chairs: David Jayne, Cambridge, UK Vladimir Tesar, Prague, Czech Republic Prof. Franco Ferrario Nephropathology
The role of repeated biopsies in the management of Lupus Nephritis Franco Ferrario, Milan, Italy Chairs: David Jayne, Cambridge, UK Vladimir Tesar, Prague, Czech Republic Prof. Franco Ferrario Nephropathology
Approach to Glomerular Diseases: Clinical Presentation Nephrotic Syndrome Nephritis
 GLOMERULONEPHRITIDES Vivette D Agati Jai Radhakrishnan Approach to Glomerular Diseases: Clinical Presentation Nephrotic Syndrome Nephritis Heavy Proteinuria Renal failure Low serum Albumin Hypertension
GLOMERULONEPHRITIDES Vivette D Agati Jai Radhakrishnan Approach to Glomerular Diseases: Clinical Presentation Nephrotic Syndrome Nephritis Heavy Proteinuria Renal failure Low serum Albumin Hypertension
Case Presentation Turki Al-Hussain, MD
 Case Presentation Turki Al-Hussain, MD Director, Renal Pathology Chapter Saudi Society of Nephrology & Transplantation Consultant Nephropathologist & Urological Pathologist Department of Pathology & Laboratory
Case Presentation Turki Al-Hussain, MD Director, Renal Pathology Chapter Saudi Society of Nephrology & Transplantation Consultant Nephropathologist & Urological Pathologist Department of Pathology & Laboratory
Year 2004 Paper one: Questions supplied by Megan
 QUESTION 53 Endothelial cell pathology on renal biopsy is most characteristic of which one of the following diagnoses? A. Pre-eclampsia B. Haemolytic uraemic syndrome C. Lupus nephritis D. Immunoglobulin
QUESTION 53 Endothelial cell pathology on renal biopsy is most characteristic of which one of the following diagnoses? A. Pre-eclampsia B. Haemolytic uraemic syndrome C. Lupus nephritis D. Immunoglobulin
ORIGINAL ARTICLE. Statistical tools used: Statistical tools used were Kappa coefficient, fisher test and odds ratio.
 SIGNIFICANCE OF ACTIVITY AND CHRONICITY INDICES OF LUPUS NEPHRITIS ON RENAL OUTCOME WITH EMPHASIS ON REPEATABILITY - EXPERIENCE FROM SOUTHINDIA Seema H.S 1, Isha Garg 2, Priya Alexander 3 HOW TO CITE THIS
SIGNIFICANCE OF ACTIVITY AND CHRONICITY INDICES OF LUPUS NEPHRITIS ON RENAL OUTCOME WITH EMPHASIS ON REPEATABILITY - EXPERIENCE FROM SOUTHINDIA Seema H.S 1, Isha Garg 2, Priya Alexander 3 HOW TO CITE THIS
Journal of Nephropathology
 www.nephropathol.com DOI: 10.15171/jnp.2018.24 J Nephropathol. 2018;7(3):101-105 Journal of Nephropathology Relationship of CD147 kidney expression with various pathologic lesions, biochemical and demographic
www.nephropathol.com DOI: 10.15171/jnp.2018.24 J Nephropathol. 2018;7(3):101-105 Journal of Nephropathology Relationship of CD147 kidney expression with various pathologic lesions, biochemical and demographic
Glomerular pathology-2 Nephritic syndrome. Dr. Nisreen Abu Shahin
 Glomerular pathology-2 Nephritic syndrome Dr. Nisreen Abu Shahin 1 The Nephritic Syndrome Pathogenesis: inflammation proliferation of the cells in glomeruli & leukocytic infiltrate Injured capillary walls
Glomerular pathology-2 Nephritic syndrome Dr. Nisreen Abu Shahin 1 The Nephritic Syndrome Pathogenesis: inflammation proliferation of the cells in glomeruli & leukocytic infiltrate Injured capillary walls
CHAPTER 2. Primary Glomerulonephritis
 2nd Report of the PRIMARY GLOMERULONEPHRITIS CHAPTER 2 Primary Glomerulonephritis Sunita Bavanandan Lee Han Wei Lim Soo Kun 21 PRIMARY GLOMERULONEPHRITIS 2nd Report of the 2.1 Introduction This chapter
2nd Report of the PRIMARY GLOMERULONEPHRITIS CHAPTER 2 Primary Glomerulonephritis Sunita Bavanandan Lee Han Wei Lim Soo Kun 21 PRIMARY GLOMERULONEPHRITIS 2nd Report of the 2.1 Introduction This chapter
Lab 3, case 1. Is this an example of nephrotic or nephritic syndrome? Why? Which portion of the nephron would you expect to be abnormal?
 Lab 3, case 1 12-year-old Costa Rican boy is brought into clinic by his parents because of dark brownish-red urine over the last 24 hours. The family has been visiting friends in Indianapolis for two weeks.
Lab 3, case 1 12-year-old Costa Rican boy is brought into clinic by his parents because of dark brownish-red urine over the last 24 hours. The family has been visiting friends in Indianapolis for two weeks.
Biopsy Features of Kidney Allograft Rejection Banff B. Ivanyi, MD Department of Pathology, University of Szeged, Szeged, Hungary
 Biopsy Features of Kidney Allograft Rejection Banff 2017 B. Ivanyi, MD Department of Pathology, University of Szeged, Szeged, Hungary Treatment of allograft dysfunction should rely on the biopsy findings
Biopsy Features of Kidney Allograft Rejection Banff 2017 B. Ivanyi, MD Department of Pathology, University of Szeged, Szeged, Hungary Treatment of allograft dysfunction should rely on the biopsy findings
C1q nephropathy the Diverse Disease
 C1q nephropathy the Diverse Disease Danica Galešić Ljubanović School of Medicine, University of Zagreb Dubrava University Hospital Zagreb, Croatia Definition Dominant or codominant ( 2+), mesangial staining
C1q nephropathy the Diverse Disease Danica Galešić Ljubanović School of Medicine, University of Zagreb Dubrava University Hospital Zagreb, Croatia Definition Dominant or codominant ( 2+), mesangial staining
Cover Page. The handle holds various files of this Leiden University dissertation
 Cover Page The handle http://hdl.handle.net/1887/47854 holds various files of this Leiden University dissertation Author: Wilhelmus, S. Title: Systemic lupus erythematosus: pathogenesis, diagnosis, and
Cover Page The handle http://hdl.handle.net/1887/47854 holds various files of this Leiden University dissertation Author: Wilhelmus, S. Title: Systemic lupus erythematosus: pathogenesis, diagnosis, and
Glomerular diseases with organized deposits
 Glomerular diseases with organized deposits Banu Sis, MD, FRCPC University of Alberta, Edmonton, AB, Canada Ulusal Patoloji Kongresi, Manavgat, Antalya 8/11/2012 What is an organized deposit? A number
Glomerular diseases with organized deposits Banu Sis, MD, FRCPC University of Alberta, Edmonton, AB, Canada Ulusal Patoloji Kongresi, Manavgat, Antalya 8/11/2012 What is an organized deposit? A number
Nephrology Grand Rounds. Mansi Mehta November 24, 2015
 Nephrology Grand Rounds Mansi Mehta November 24, 2015 Case 51yo F with PMH significant for Hypertension referred to renal clinic for evaluation of elevated Cr. no known history of CKD; baseline creatinine
Nephrology Grand Rounds Mansi Mehta November 24, 2015 Case 51yo F with PMH significant for Hypertension referred to renal clinic for evaluation of elevated Cr. no known history of CKD; baseline creatinine
CHAPTER 2 PRIMARY GLOMERULONEPHRITIS
 CHAPTER 2 Sunita Bavanandan Lim Soo Kun 19 5th Report of the 2.1: Introduction This chapter covers the main primary glomerulonephritis that were reported to the MRRB from the years 2005-2012. Minimal change
CHAPTER 2 Sunita Bavanandan Lim Soo Kun 19 5th Report of the 2.1: Introduction This chapter covers the main primary glomerulonephritis that were reported to the MRRB from the years 2005-2012. Minimal change
Atypical IgA Nephropathy
 Atypical IgA Nephropathy Richard J. Glassock, MD, MACP Geffen School of Medicine at UCLA XXXIII Chilean Congress of Nephrology, Hypertension and Transplantation Puerto Varas, Chile October 6, 2016 IgA
Atypical IgA Nephropathy Richard J. Glassock, MD, MACP Geffen School of Medicine at UCLA XXXIII Chilean Congress of Nephrology, Hypertension and Transplantation Puerto Varas, Chile October 6, 2016 IgA
Advances in the European Validation Study of the Oxford Classification of IgA Nephropathy (VALIGA)
") Advances in the European Validation Study of the Oxford Classification of IgA Nephropathy (VALIGA) One of the major aims of the IWG is to facilitate European Nephrologists interested in the area of immune-mediated
Advances in the European Validation Study of the Oxford Classification of IgA Nephropathy (VALIGA) One of the major aims of the IWG is to facilitate European Nephrologists interested in the area of immune-mediated
substance staining with IgG, C3 and IgA (trace) Linear deposition of IgG(+), IgA.M(trace) and C3(+++) at the DEJ
 Linear deposition of IgG(+), IgA.M(trace) and C3(+++) at the DEJ") Direct Immunofluorescence: Skin Diagnosis Findings Picture Pemphigus Vulgaris and it s Intracellular cement variants substance staining with IgG, C3 and IgA (trace) Bullous Pemphigoid and it s variants
Direct Immunofluorescence: Skin Diagnosis Findings Picture Pemphigus Vulgaris and it s Intracellular cement variants substance staining with IgG, C3 and IgA (trace) Bullous Pemphigoid and it s variants
MICROSCOPIC HEMATURIA AND DIFFUSE NECROTIZING GLOMERULONEPHRITIS
 MICROSCOPIC HEMATURIA AND DIFFUSE NECROTIZING GLOMERULONEPHRITIS Hatim Q. AlMaghrabi, MD, FRCPC Consultant at King Abdulaziz Medical City (NGHA) Jeddah Case Presentation 70 years old female Known hypertensive
MICROSCOPIC HEMATURIA AND DIFFUSE NECROTIZING GLOMERULONEPHRITIS Hatim Q. AlMaghrabi, MD, FRCPC Consultant at King Abdulaziz Medical City (NGHA) Jeddah Case Presentation 70 years old female Known hypertensive
Journal of Nephropathology
 www.nephropathol.com DOI: 10.12860/jnp.2014.22 J Nephropathol. 2014; 3(3): 115-120 Journal of Nephropathology Clinicopathological correlations in lupus nephritis; a single center experience Hamid Nasri
www.nephropathol.com DOI: 10.12860/jnp.2014.22 J Nephropathol. 2014; 3(3): 115-120 Journal of Nephropathology Clinicopathological correlations in lupus nephritis; a single center experience Hamid Nasri
Kidney Summary. Mark Haas Cedars-Sinai Medical Center Los Angeles, California, USA
 Kidney Summary Mark Haas Cedars-Sinai Medical Center Los Angeles, California, USA Key Issues to Address re: the Classification 1. Incorporation of i-ifta + tubulitis into the TCMR classification - Defining
Kidney Summary Mark Haas Cedars-Sinai Medical Center Los Angeles, California, USA Key Issues to Address re: the Classification 1. Incorporation of i-ifta + tubulitis into the TCMR classification - Defining
Immune complex deposits in ANCA-associated crescentic glomerulonephritis: A study of 126 cases
 Kidney International, Vol. 65 (2004), pp. 2145 2152 Immune complex deposits in ANCA-associated crescentic glomerulonephritis: A study of 126 cases MARK HAAS and JOSEPH A. EUSTACE Department of Pathology
Kidney International, Vol. 65 (2004), pp. 2145 2152 Immune complex deposits in ANCA-associated crescentic glomerulonephritis: A study of 126 cases MARK HAAS and JOSEPH A. EUSTACE Department of Pathology
RENAL EVENING SPECIALTY CONFERENCE
 RENAL EVENING SPECIALTY CONFERENCE Harsharan K. Singh, MD The University of North Carolina at Chapel Hill Disclosure of Relevant Financial Relationships No conflicts of interest to disclose. CLINICAL HISTORY
RENAL EVENING SPECIALTY CONFERENCE Harsharan K. Singh, MD The University of North Carolina at Chapel Hill Disclosure of Relevant Financial Relationships No conflicts of interest to disclose. CLINICAL HISTORY
29th Annual Meeting of the Glomerular Disease Collaborative Network
 29th Annual Meeting of the Glomerular Disease Collaborative Network Updates on the Pathogenesis IgA Nephropathy and IgA Vasculitis (HSP) J. Charles Jennette, M.D. Brinkhous Distinguished Professor and
29th Annual Meeting of the Glomerular Disease Collaborative Network Updates on the Pathogenesis IgA Nephropathy and IgA Vasculitis (HSP) J. Charles Jennette, M.D. Brinkhous Distinguished Professor and
FIBRILLARY GLOMERULONEPHRITIS DIAGNOSTIC CRITERIA, PITFALLS, AND DIFFERENTIAL DIAGNOSIS
 FIBRILLARY GLOMERULONEPHRITIS DIAGNOSTIC CRITERIA, PITFALLS, AND DIFFERENTIAL DIAGNOSIS Guillermo A. Herrera MD Louisiana State University, Shreveport Fibrils in bundles 10-20 nm d Diabetic fibrillosis
FIBRILLARY GLOMERULONEPHRITIS DIAGNOSTIC CRITERIA, PITFALLS, AND DIFFERENTIAL DIAGNOSIS Guillermo A. Herrera MD Louisiana State University, Shreveport Fibrils in bundles 10-20 nm d Diabetic fibrillosis
Pathogenetic features of severe segmental lupus nephritis
 Nephrol Dial Transplant (2010) 25: 153 159 doi: 10.1093/ndt/gfp424 Advance Access publication 23 August 2009 Pathogenetic features of severe segmental lupus nephritis Venkata Y. Behara 1, William L. Whittier
Nephrol Dial Transplant (2010) 25: 153 159 doi: 10.1093/ndt/gfp424 Advance Access publication 23 August 2009 Pathogenetic features of severe segmental lupus nephritis Venkata Y. Behara 1, William L. Whittier
Index. electron microscopy, 81 immunofluorescence microscopy, 80 light microscopy, 80 Amyloidosis clinical setting, 185 etiology/pathogenesis,
 A Acute antibody-mediated rejection (Acute AMR) clinical features, 203 clinicopathologic correlations, 206 pathogenesis, 205 206 204 205 light microscopy, 203 204 Acute cellular rejection (ACR) clinical
A Acute antibody-mediated rejection (Acute AMR) clinical features, 203 clinicopathologic correlations, 206 pathogenesis, 205 206 204 205 light microscopy, 203 204 Acute cellular rejection (ACR) clinical
NEPHRITIC SYNDROME. By Dr Mai inbiek
 NEPHRITIC SYNDROME By Dr Mai inbiek Nephritic Syndrome The nephritic Syndrome is a clinical complex, usually of acute onset. Is caused by inflammatory lesions of glomeruli. Characterized by; 1) Hematuria
NEPHRITIC SYNDROME By Dr Mai inbiek Nephritic Syndrome The nephritic Syndrome is a clinical complex, usually of acute onset. Is caused by inflammatory lesions of glomeruli. Characterized by; 1) Hematuria
N. Hiramatsu, T. Kuroiwa, H. Ikeuchi, A. Maeshima, Y. Kaneko, K. Hiromura, K. Ueki and Y. Nojima
 Rheumatology 28;47:72 77 Advance Access publication 4 April 28 doi:1.193/rheumatology/ken19 Revised classification of lupus nephritis is valuable in predicting renal outcome with an indication of the proportion
Rheumatology 28;47:72 77 Advance Access publication 4 April 28 doi:1.193/rheumatology/ken19 Revised classification of lupus nephritis is valuable in predicting renal outcome with an indication of the proportion
Cover Page. The handle holds various files of this Leiden University dissertation
 Cover Page The handle http://hdl.handle.net/1887/47854 holds various files of this Leiden University dissertation Author: Wilhelmus, S. Title: Systemic lupus erythematosus: pathogenesis, diagnosis, and
Cover Page The handle http://hdl.handle.net/1887/47854 holds various files of this Leiden University dissertation Author: Wilhelmus, S. Title: Systemic lupus erythematosus: pathogenesis, diagnosis, and
Crescentic Glomerulonephritis (RPGN)
") Crescentic Glomerulonephritis (RPGN) Background Rapidly progressive glomerulonephritis (RPGN) is defined as any glomerular disease characterized by extensive crescents (usually >50%) as the principal histologic
Crescentic Glomerulonephritis (RPGN) Background Rapidly progressive glomerulonephritis (RPGN) is defined as any glomerular disease characterized by extensive crescents (usually >50%) as the principal histologic
Case Report A Case of Proliferative Glomerulonephritis with Monoclonal IgG Deposits That Showed Predominantly Membranous Features
 Hindawi Case Reports in Nephrology Volume 2017, Article ID 1027376, 5 pages https://doi.org/10.1155/2017/1027376 Case Report A Case of Proliferative Glomerulonephritis with Monoclonal IgG Deposits That
Hindawi Case Reports in Nephrology Volume 2017, Article ID 1027376, 5 pages https://doi.org/10.1155/2017/1027376 Case Report A Case of Proliferative Glomerulonephritis with Monoclonal IgG Deposits That
Glomerular Pathology- 1 Nephrotic Syndrome. Dr. Nisreen Abu Shahin
 Glomerular Pathology- 1 Nephrotic Syndrome Dr. Nisreen Abu Shahin The Nephrotic Syndrome a clinical complex resulting from glomerular disease & includes the following: (1) massive proteinuria (3.5 gm /day
Glomerular Pathology- 1 Nephrotic Syndrome Dr. Nisreen Abu Shahin The Nephrotic Syndrome a clinical complex resulting from glomerular disease & includes the following: (1) massive proteinuria (3.5 gm /day
Membranoproliferative Glomerulonephritis
 Membranoproliferative Glomerulonephritis MPGN is characterizedby alterations in the GBM and mesangium and by proliferation of glomerular cells. 5% to 10% of cases of 1ry nephrotic syndrome in children
Membranoproliferative Glomerulonephritis MPGN is characterizedby alterations in the GBM and mesangium and by proliferation of glomerular cells. 5% to 10% of cases of 1ry nephrotic syndrome in children
Tuesday Conference 7/23/2013. Hasan Fattah
 Tuesday Conference 7/23/2013 Hasan Fattah 48 AA male, PMH: HTN, proteinuria since 2009, sent from primary clinic for high Cr evaluation (7.1), last known of 1.1 in 2010 associated with sub-nephrotic range
Tuesday Conference 7/23/2013 Hasan Fattah 48 AA male, PMH: HTN, proteinuria since 2009, sent from primary clinic for high Cr evaluation (7.1), last known of 1.1 in 2010 associated with sub-nephrotic range
Case Report Nephrotic Syndrome Secondary to Proliferative Glomerulonephritis with Monoclonal Immunoglobulin Deposits of Lambda Light Chain
 Hindawi Publishing Corporation Case Reports in Nephrology Volume 214, Article ID 164694, 6 pages http://dx.doi.org/1.1155/214/164694 Case Report Nephrotic Syndrome Secondary to Proliferative Glomerulonephritis
Hindawi Publishing Corporation Case Reports in Nephrology Volume 214, Article ID 164694, 6 pages http://dx.doi.org/1.1155/214/164694 Case Report Nephrotic Syndrome Secondary to Proliferative Glomerulonephritis
Renal manifestations of IgG4-related systemic disease
 Renal manifestations of IgG4-related systemic disease Lynn D. Cornell, M.D. Mayo Clinic Rochester, MN While autoimmune pancreatitis (AIP) has been recognized since the first description by Sarles et al
Renal manifestations of IgG4-related systemic disease Lynn D. Cornell, M.D. Mayo Clinic Rochester, MN While autoimmune pancreatitis (AIP) has been recognized since the first description by Sarles et al
C3 GLOMERULOPATHIES. Budapest Nephrology School Zoltan Laszik
 C3 GLOMERULOPATHIES Budapest Nephrology School 8.30.2018. Zoltan Laszik 1 Learning Objectives Familiarize with the pathogenetic mechanisms of glomerular diseases Learn the pathologic landscape and clinical
C3 GLOMERULOPATHIES Budapest Nephrology School 8.30.2018. Zoltan Laszik 1 Learning Objectives Familiarize with the pathogenetic mechanisms of glomerular diseases Learn the pathologic landscape and clinical
RENAL HISTOPATHOLOGY
 RENAL HISTOPATHOLOGY Peter McCue, M.D. Department of Pathology, Anatomy & Cell Biology Sidney Kimmel Medical College There are no conflicts of interest. 1 Goals and Objectives! Goals Provide introduction
RENAL HISTOPATHOLOGY Peter McCue, M.D. Department of Pathology, Anatomy & Cell Biology Sidney Kimmel Medical College There are no conflicts of interest. 1 Goals and Objectives! Goals Provide introduction
Overview of glomerular diseases
 Overview of glomerular diseases *Endothelial cells are fenestrated each fenestra: 70-100nm in diameter Contractile, capable of proliferation, makes ECM & releases mediators *Glomerular basement membrane
Overview of glomerular diseases *Endothelial cells are fenestrated each fenestra: 70-100nm in diameter Contractile, capable of proliferation, makes ECM & releases mediators *Glomerular basement membrane
Glomerular tip adhesions predict the progression of IgA nephropathy
 Maeda et al. BMC Nephrology 2013, 14:272 RESEARCH ARTICLE Open Access Glomerular tip adhesions predict the progression of IgA nephropathy Kunihiro Maeda 1, Shogo Kikuchi 2, Naoto Miura 1, Keisuke Suzuki
Maeda et al. BMC Nephrology 2013, 14:272 RESEARCH ARTICLE Open Access Glomerular tip adhesions predict the progression of IgA nephropathy Kunihiro Maeda 1, Shogo Kikuchi 2, Naoto Miura 1, Keisuke Suzuki
Case Presentation Turki Al-Hussain, MD
 Case Presentation Turki Al-Hussain, MD Director, Renal Pathology Chapter Saudi Society of Nephrology & Transplantation Consultant Nephropathologist & Urological Pathologist Department of Pathology & Laboratory
Case Presentation Turki Al-Hussain, MD Director, Renal Pathology Chapter Saudi Society of Nephrology & Transplantation Consultant Nephropathologist & Urological Pathologist Department of Pathology & Laboratory
Management of Rejection
 Management of Rejection I have no disclosures Disclosures (relevant or otherwise) Deborah B Adey, MD Professor of Medicine University of California, San Francisco Kidney and Pancreas Transplant Center
Management of Rejection I have no disclosures Disclosures (relevant or otherwise) Deborah B Adey, MD Professor of Medicine University of California, San Francisco Kidney and Pancreas Transplant Center
J Nephropharmacol. 2014; 3(2): Journal of Nephropharmacology
: Journal of Nephropharmacology") J Nephropharmacol. 2014; 3(2): 33 37. NPJ Journal of Nephropharmacology Pathological patterns of mesangioproliferative glomerulonephritis seen at a tertiary care center Ghadeer A. Mokhtar 1*, Sawsan Jalalah
J Nephropharmacol. 2014; 3(2): 33 37. NPJ Journal of Nephropharmacology Pathological patterns of mesangioproliferative glomerulonephritis seen at a tertiary care center Ghadeer A. Mokhtar 1*, Sawsan Jalalah
Transplantation and 6-Month Follow-up of Renal Transplantation from a Donor with Systemic Lupus Erythematosus and Lupus Nephritis
 American Journal of Transplantation 2005; 5: 1772 1776 Blackwell Munksgaard Case Report Copyright C Blackwell Munksgaard 2005 doi: 10.1111/j.1600-6143.2005.00922.x Transplantation and 6-Month Follow-up
American Journal of Transplantation 2005; 5: 1772 1776 Blackwell Munksgaard Case Report Copyright C Blackwell Munksgaard 2005 doi: 10.1111/j.1600-6143.2005.00922.x Transplantation and 6-Month Follow-up
A Case of IgG2 Heavy Chain Deposition Disease in a Patient with Kappa Positive Plasma Cell Dyscrasia
 Published online: August 14, 2014 2296 9705/14/0051 0006$39.50/0 This is an Open Access article licensed under the terms of the Creative Commons Attribution-NonCommercial 3.0 Unported license (CC BY-NC)
Published online: August 14, 2014 2296 9705/14/0051 0006$39.50/0 This is an Open Access article licensed under the terms of the Creative Commons Attribution-NonCommercial 3.0 Unported license (CC BY-NC)
Redefining lupus nephritis: clinical implications of pathophysiologic subtypes
 Redefining lupus nephritis: clinical implications of pathophysiologic subtypes 1 Renal Division, Department of Medicine, Peking University First Hospital, Institute of Nephrology, Peking University, Key
Redefining lupus nephritis: clinical implications of pathophysiologic subtypes 1 Renal Division, Department of Medicine, Peking University First Hospital, Institute of Nephrology, Peking University, Key
Clinical Study Glomerulonephritis with Crescents in Children: Etiology and Predictors of Renal Outcome
 International Scholarly Research Network ISRN Pediatrics Volume 2011, Article ID 507298, 5 pages doi:10.5402/2011/507298 Clinical Study Glomerulonephritis with Crescents in Children: Etiology and Predictors
International Scholarly Research Network ISRN Pediatrics Volume 2011, Article ID 507298, 5 pages doi:10.5402/2011/507298 Clinical Study Glomerulonephritis with Crescents in Children: Etiology and Predictors
Glomerular Diseases. Anna Vinnikova, MD Nephrology
 Glomerular Diseases Anna Vinnikova, MD Nephrology Classification of Glomerular Diseases http://what-when-how.com/acp-medicine/glomerular-diseases-part-1/ Classification of pathologic and clinical manifestations
Glomerular Diseases Anna Vinnikova, MD Nephrology Classification of Glomerular Diseases http://what-when-how.com/acp-medicine/glomerular-diseases-part-1/ Classification of pathologic and clinical manifestations
RENAL BIOPSIES in patients with the clinical
 RENAL BIOPSY TEACHING CASE Crescentic Glomerulonephritis With a Paucity of Glomerular Immunoglobulin Localization Alexis A. Harris, MD, Ronald J. Falk, MD, and J. Charles Jennette, MD RENAL BIOPSIES in
RENAL BIOPSY TEACHING CASE Crescentic Glomerulonephritis With a Paucity of Glomerular Immunoglobulin Localization Alexis A. Harris, MD, Ronald J. Falk, MD, and J. Charles Jennette, MD RENAL BIOPSIES in
Prof. Rosanna Coppo Director of the Nephrology, Dialysis and Transplantation Department Regina Margherita Hospital Turin, Italy. Slide 1.
 ROLE OF PATHOLOGY AND CLINICAL FEATURES IN PREDICTING PROGRESSION OF IGA NEPHROPATHY: RESULTS FROM THE ERA-EDTA RESEARCH VALIGA Rosanna Coppo, Turin, Italy Chairs: François Berthoux, Saint-Etienne, France
ROLE OF PATHOLOGY AND CLINICAL FEATURES IN PREDICTING PROGRESSION OF IGA NEPHROPATHY: RESULTS FROM THE ERA-EDTA RESEARCH VALIGA Rosanna Coppo, Turin, Italy Chairs: François Berthoux, Saint-Etienne, France
Pathology of Kidney Allograft Dysfunction. B. Ivanyi, MD Department of Pathology, University of Szeged, Szeged, Hungary
 Pathology of Kidney Allograft Dysfunction B. Ivanyi, MD Department of Pathology, University of Szeged, Szeged, Hungary The gold standard for exploration of the cause of an allograft dysfunction is to perform
Pathology of Kidney Allograft Dysfunction B. Ivanyi, MD Department of Pathology, University of Szeged, Szeged, Hungary The gold standard for exploration of the cause of an allograft dysfunction is to perform
Histological appraisal of lupus nephritis factors have always been suspected, but remain unproven (3). The wide range of autoantibodies produced in SL
. The wide range of autoantibodies produced in SL") Hong Kong Journal Nephrol of 2000;2(1):13-18. Nephrology 2000;2(1):13-18. FMM LAI, et al R E V I E W A R T I C L E Histological appraisal of lupus nephritis Fernand MM LAI 1, Philip KT LI 2, Paul CL CHOI
Hong Kong Journal Nephrol of 2000;2(1):13-18. Nephrology 2000;2(1):13-18. FMM LAI, et al R E V I E W A R T I C L E Histological appraisal of lupus nephritis Fernand MM LAI 1, Philip KT LI 2, Paul CL CHOI
Immune profile of IgA-dominant diffuse proliferative glomerulonephritis
 Clin Kidney J (2014) 7: 479 483 doi: 10.1093/ckj/sfu090 Exceptional Case Immune profile of IgA-dominant diffuse proliferative glomerulonephritis Eric Wallace 1, Nicolas Maillard 2, Hiroyuki Ueda 2, Stacy
Clin Kidney J (2014) 7: 479 483 doi: 10.1093/ckj/sfu090 Exceptional Case Immune profile of IgA-dominant diffuse proliferative glomerulonephritis Eric Wallace 1, Nicolas Maillard 2, Hiroyuki Ueda 2, Stacy
Glomerulonephritis. Dr Rodney Itaki Anatomical Pathology Discipline.
 Glomerulonephritis Dr Rodney Itaki Anatomical Pathology Discipline. University of Papua New Guinea School of Medicine & Health Sciences Division of Pathology Gross anatomy Ref: Goggle Images Microanatomy
Glomerulonephritis Dr Rodney Itaki Anatomical Pathology Discipline. University of Papua New Guinea School of Medicine & Health Sciences Division of Pathology Gross anatomy Ref: Goggle Images Microanatomy
CASE OF THE WEEK 1
 www.nephro-pathology.com CASE OF THE WEEK 1 Clinical Presentation: A 17 year old Indian boy presented with anasarca, decreased urine output and episodes of nausea and vomiting over the last three weeks.
www.nephro-pathology.com CASE OF THE WEEK 1 Clinical Presentation: A 17 year old Indian boy presented with anasarca, decreased urine output and episodes of nausea and vomiting over the last three weeks.
Lupus Related Kidney Diseases. Jason Cobb MD Assistant Professor Renal Division Emory University School of Medicine October 14, 2017
 Lupus Related Kidney Diseases Jason Cobb MD Assistant Professor Renal Division Emory University School of Medicine October 14, 2017 Financial Disclosures MedImmune Lupus Nephritis Kidney Biopsy Biomarkers
Lupus Related Kidney Diseases Jason Cobb MD Assistant Professor Renal Division Emory University School of Medicine October 14, 2017 Financial Disclosures MedImmune Lupus Nephritis Kidney Biopsy Biomarkers
The value of repeat biopsy in the management of lupus nephritis: an international multicentre study in a large cohort of patients
 Nephrol Dial Transplant (2013) 28: 3014 3023 doi: 10.1093/ndt/gft272 Advance Access publication 24 August 2013 Original Articles The value of repeat biopsy in the management of lupus nephritis: an international
Nephrol Dial Transplant (2013) 28: 3014 3023 doi: 10.1093/ndt/gft272 Advance Access publication 24 August 2013 Original Articles The value of repeat biopsy in the management of lupus nephritis: an international
CASE 4 A RARE CASE OF INTRALUMINAL GLOMERULAR CAPILLARY DEPOSITS
 CASE 4 A RARE CASE OF INTRALUMINAL GLOMERULAR CAPILLARY DEPOSITS DR ANNIE JOJO, Dr Seethalekshmy N V, Dr Nanda Kachare DEPARTMENT OF PATHOLOGY, AMRITA INSTITUTE OF MEDICAL SCIENCES, KOCHI. 54 yrs female,
CASE 4 A RARE CASE OF INTRALUMINAL GLOMERULAR CAPILLARY DEPOSITS DR ANNIE JOJO, Dr Seethalekshmy N V, Dr Nanda Kachare DEPARTMENT OF PATHOLOGY, AMRITA INSTITUTE OF MEDICAL SCIENCES, KOCHI. 54 yrs female,
Long-term follow-up of juvenile acute nonproliferative glomerulitis (JANG)
") Pediatr Nephrol (2007) 22:1957 1961 DOI 10.1007/s00467-007-0555-6 BRIEF REPORT Long-term follow-up of juvenile acute nonproliferative glomerulitis (JANG) Teruo Fujita & Kandai Nozu & Kazumoto Iijima &
Pediatr Nephrol (2007) 22:1957 1961 DOI 10.1007/s00467-007-0555-6 BRIEF REPORT Long-term follow-up of juvenile acute nonproliferative glomerulitis (JANG) Teruo Fujita & Kandai Nozu & Kazumoto Iijima &
Clinicopathological analysis of proliferative glomerulonephritis with monoclonal IgG deposits in 5 renal allografts
 Wen et al. BMC Nephrology (2018) 19:173 https://doi.org/10.1186/s12882-018-0969-3 RESEARCH ARTICLE Open Access Clinicopathological analysis of proliferative glomerulonephritis with monoclonal IgG deposits
Wen et al. BMC Nephrology (2018) 19:173 https://doi.org/10.1186/s12882-018-0969-3 RESEARCH ARTICLE Open Access Clinicopathological analysis of proliferative glomerulonephritis with monoclonal IgG deposits
Validation of the Oxford Classification of IgA Nephropathy: A Single-Center Study in Korean Adults
 original article korean j intern med 202;27:293-300 pissn 226-3303 eissn 2005-6648 Validation of the Oxford Classification of IgA Nephropathy: A Single-Center Study in Korean Adults Hoyoung Lee, Sul Hee
original article korean j intern med 202;27:293-300 pissn 226-3303 eissn 2005-6648 Validation of the Oxford Classification of IgA Nephropathy: A Single-Center Study in Korean Adults Hoyoung Lee, Sul Hee
Pathology of Complement Mediated Renal Disease
 Pathology of Complement Mediated Renal Disease Mariam Priya Alexander, MD Associate Professor of Pathology GN Symposium Hong Kong Society of Nephrology July 8 th, 2017 2017 MFMER slide-1 The complement
Pathology of Complement Mediated Renal Disease Mariam Priya Alexander, MD Associate Professor of Pathology GN Symposium Hong Kong Society of Nephrology July 8 th, 2017 2017 MFMER slide-1 The complement
Complement in vasculitis and glomerulonephritis. Andy Rees Clinical Institute of Pathology Medical University of Vienna
 Complement in vasculitis and glomerulonephritis Andy Rees Clinical Institute of Pathology Medical University of Vienna 41 st Heidelberg Nephrology Seminar March 2017 The complement system An evolutionary
Complement in vasculitis and glomerulonephritis Andy Rees Clinical Institute of Pathology Medical University of Vienna 41 st Heidelberg Nephrology Seminar March 2017 The complement system An evolutionary
What s hiding behind IgA nephropathy?
 What s hiding behind IgA nephropathy? Bauerova L. Department of Pathology, the First Faculty of Medicine and General Hospital, Charles University Prague (nephropathology training: Department of Clinical
What s hiding behind IgA nephropathy? Bauerova L. Department of Pathology, the First Faculty of Medicine and General Hospital, Charles University Prague (nephropathology training: Department of Clinical
Clinical and pathologic characteristics of focal segmental glomerulosclerosis pathologic variants
 original article http://www.kidney-international.org & 2006 International Society of Nephrology Clinical and pathologic characteristics of focal segmental glomerulosclerosis pathologic variants DB Thomas
original article http://www.kidney-international.org & 2006 International Society of Nephrology Clinical and pathologic characteristics of focal segmental glomerulosclerosis pathologic variants DB Thomas
Secondary IgA Nephropathy & HSP
 Secondary IgA Nephropathy & HSP Anjali Gupta, MD 1/11/11 AKI sec to Hematuria? 65 cases of ARF after an episode of macroscopic hematuria have been reported in the literature in patients with GN. The main
Secondary IgA Nephropathy & HSP Anjali Gupta, MD 1/11/11 AKI sec to Hematuria? 65 cases of ARF after an episode of macroscopic hematuria have been reported in the literature in patients with GN. The main
IgA Nephropathy - «Maladie de Berger»
 IgA Nephropathy - «Maladie de Berger» B. Vogt, Division de Néphrologie/Consultation d Hypertension CHUV, Lausanne 2011 Montreux CME SGN-SSN IgA Nephropathy 1. Introduction 2. Etiology and Pathogenesis
IgA Nephropathy - «Maladie de Berger» B. Vogt, Division de Néphrologie/Consultation d Hypertension CHUV, Lausanne 2011 Montreux CME SGN-SSN IgA Nephropathy 1. Introduction 2. Etiology and Pathogenesis
ACCME/Disclosure. Case #1. Case History. Dr. Bracamonte has nothing to disclose
 Case #1 ACCME/Disclosure Dr. Erika Bracamonte Associate Professor of Pathology University of Arizona, College of Medicine Banner University Medical Center, Tucson Dr. Bracamonte has nothing to disclose
Case #1 ACCME/Disclosure Dr. Erika Bracamonte Associate Professor of Pathology University of Arizona, College of Medicine Banner University Medical Center, Tucson Dr. Bracamonte has nothing to disclose
C3G An Update What is C3 Glomerulopathy Anyway? Patrick D. Walker, M.D. Nephropath Little Rock, Arkansas USA
 C3G An Update What is C3 Glomerulopathy Anyway? Patrick D. Walker, M.D. Nephropath Little Rock, Arkansas USA C3 Glomerulopathy Overview Discuss C3 Glomerulopathy (C3G) How did we get to the current classification
C3G An Update What is C3 Glomerulopathy Anyway? Patrick D. Walker, M.D. Nephropath Little Rock, Arkansas USA C3 Glomerulopathy Overview Discuss C3 Glomerulopathy (C3G) How did we get to the current classification
RECURRENT AND DE NOVO RENAL DISEASES IN THE ALLOGRAFT. J. H. Helderman,MD,FACP,FAST
 RECURRENT AND DE NOVO RENAL DISEASES IN THE ALLOGRAFT J. H. Helderman,MD,FACP,FAST Vanderbilt University Medical Center Professor of Medicine, Pathology and Immunology Medical Director, Vanderbilt Transplant
RECURRENT AND DE NOVO RENAL DISEASES IN THE ALLOGRAFT J. H. Helderman,MD,FACP,FAST Vanderbilt University Medical Center Professor of Medicine, Pathology and Immunology Medical Director, Vanderbilt Transplant
Clinical and pathological characteristics of patients with glomerular diseases at a university teaching hospital: 5-year prospective review
 Clinical and pathological characteristics of patients with glomerular diseases at a university teaching hospital: 5-year prospective review KW Chan, TM Chan, IKP Cheng Objective. To examine the prevalence
Clinical and pathological characteristics of patients with glomerular diseases at a university teaching hospital: 5-year prospective review KW Chan, TM Chan, IKP Cheng Objective. To examine the prevalence
Segmental glomerulonephritis
 M. S. DUNNILL AND P. R. MILLARD From the Gibson Laboratories, Radcliffe Infirmary, Oxford J. clin. Path., 1975, 28, 167-175 SYNOPSIS The renal biopsy findings in 40 patients with segmental glomerulonephritis
M. S. DUNNILL AND P. R. MILLARD From the Gibson Laboratories, Radcliffe Infirmary, Oxford J. clin. Path., 1975, 28, 167-175 SYNOPSIS The renal biopsy findings in 40 patients with segmental glomerulonephritis
Association of glomerular C4d deposition with morphologic variables of Oxford classification in IgA nephropathy patients; a preliminary study
 Immunopathol Persa. 2016;2(2):e18 Original Immunopathologia Persa http www.immunopathol.comm Association of glomerular C4d deposition with morphologic variables of Oxford classification in IgA nephropathy
Immunopathol Persa. 2016;2(2):e18 Original Immunopathologia Persa http www.immunopathol.comm Association of glomerular C4d deposition with morphologic variables of Oxford classification in IgA nephropathy
An unusual association between focal segmental sclerosis and lupus nephritis: a distinct concept from lupus podocytopathy?
 CEN Case Rep (2015) 4:70 75 DOI 10.1007/s13730-014-0142-1 CASE REPORT An unusual association between focal segmental sclerosis and lupus nephritis: a distinct concept from lupus podocytopathy? Hironari
CEN Case Rep (2015) 4:70 75 DOI 10.1007/s13730-014-0142-1 CASE REPORT An unusual association between focal segmental sclerosis and lupus nephritis: a distinct concept from lupus podocytopathy? Hironari
Histopathology: Hypertension and diabetes in the kidney These presentations are to help you identify basic histopathological features.
 Histopathology: Hypertension and diabetes in the kidney These presentations are to help you identify basic histopathological features. They do not contain the additional factual information that you need
Histopathology: Hypertension and diabetes in the kidney These presentations are to help you identify basic histopathological features. They do not contain the additional factual information that you need
RECURRENT AND DE NOVO RENAL DISEASES IN THE ALLOGRAFT
 RECURRENT AND DE NOVO RENAL DISEASES IN THE ALLOGRAFT HISTOPATHOLOGIC DISORDERS AFFECTING THE ALLOGRAFT OTHER THAN REJECTION RECURRENT DISEASE DE NOVO DISEASE TRANSPLANT GLOMERULOPATHY Glomerular Non-glomerular
RECURRENT AND DE NOVO RENAL DISEASES IN THE ALLOGRAFT HISTOPATHOLOGIC DISORDERS AFFECTING THE ALLOGRAFT OTHER THAN REJECTION RECURRENT DISEASE DE NOVO DISEASE TRANSPLANT GLOMERULOPATHY Glomerular Non-glomerular
IgA nephropathy: unusual forms
 IgA nephropathy: unusual forms Khalil EL KAROUI Service de néphrologie et transplantation rénale, INSERM U1151 Hôpital Henri Mondor, Créteil Actualités Néphrologiques J. Hamburger 23 Avril 2018 Introduction:
IgA nephropathy: unusual forms Khalil EL KAROUI Service de néphrologie et transplantation rénale, INSERM U1151 Hôpital Henri Mondor, Créteil Actualités Néphrologiques J. Hamburger 23 Avril 2018 Introduction: