MANAGING DIABETES IN 2016 WHAT TO ADD, WHEN AND WHY?
|
|
|
- Leona Jordan
- 6 years ago
- Views:
Transcription
1 MANAGING DIABETES IN 2016 WHAT TO ADD, WHEN AND WHY?
2 Faculty: Maria Wolfs MD, MHSc, FRCPC Assistant Professor, University of Toronto Staff Endocrinologist, St. Michael's Hospital Relationships with commercial interests: Not Applicable Potential for conflict(s) of interest: Not Applicable
3 Mitigating Potential Bias All the recommendations involving clinical medicine are based on evidence that is accepted within the profession All scientific research referred to, reported, or used is in the support or justification of patient care Recommendations conform to the generally accepted standards.
4 Learning Objectives At the end of the session, participants will be able to: Identify patient factors that impact the addition of non-insulin pharmacotherapy in Type 2 Diabetes Discuss the glycemic and cardiovascular end-point evidence among non-insulin pharmacotherapies in Type 2 Diabetes Apply evidence based diabetes management to individual patient care
5 Diabetes increases CV risk 2-3 fold Lancet 2010; 375:
6 Diabetes and heart failure Gilbert R Lancet 2015;385;
7 Absolute Risk of MI by Diabetes Status # of events per 1000 person years Booth, Kapral, Fung, Tu, Lancet. 2006;367:29-36
8 Absolute Risk of MI by Diabetes Status # of events per 1000 person years Booth, Kapral, Fung, Tu, Lancet. 2006;367:29-36
9 Yes No Does lowering glucose decrease the risk of microvascular complications? Maybe
10 10
11 Yes Does lowering glucose decrease the risk of microvascular complications?
12 Glycemic lowering trials ACCORD 2008 ADVANCE y FU VADT y FU DCCT y FU UKPDS-SU y FU UKPDS-MET y FU Kumamato Mean age (y) 62 ± 7 66 ± 6 60 ± ± 9 53 ± 8 48 ± 12 Duration DM (y) New dx New dx 6.5 Baseline HbA1c (%) Prior CV event (%) None Excluded Excluded Excluded Study duration (y) Int vs std HbA1c 6.4 vs vs vs vs vs vs vs 9.4 (%) Micro benefit Nephro Nephro Yes Yes No Yes Macro benefit Major harms Nonfatal MI (ARR 1%) Mortality (ARI 1%) No No (5y FU) No Yes (10y FU) No Yes (in EDIC) No Yes (10y FU) Yes Hypo Hypo Hypo Hypo Hypo Hypo Med Clin N Am 99 (2015) 47 67
13 Microvascular complications ACCORD 2008 ADVANCE y FU VADT y FU DCCT y FU UKPDS-SU y FU UKPDS-MET y FU Kumamato Mean age (y) 62 ± 7 66 ± 6 60 ± ± 9 53 ± 8 48 ± 12 Duration DM (y) New dx New dx 6.5 Baseline HbA1c (%) Prior CV event (%) None Excluded Excluded Excluded Study duration (y) Int vs std HbA1c 6.4 vs vs vs vs vs vs vs 9.4 (%) Micro benefit Nephro Nephro Yes Yes No Yes Macro benefit Major harms Nonfatal MI (ARR 1%) Mortality (ARI 1%) No No (5y FU) No Yes (10y FU) No Yes (in EDIC) No Yes (10y FU) Yes Hypo Hypo Hypo Hypo Hypo Hypo Med Clin N Am 99 (2015) 47 67
14 Microvascular complications ACCORD 2008 ADVANCE y FU VADT y FU DCCT y FU UKPDS-SU y FU UKPDS-MET y FU Kumamato Mean age (y) 62 ± 7 66 ± 6 60 ± ± 9 53 ± 8 48 ± 12 Duration DM (y) New dx New dx 6.5 Baseline HbA1c (%) Prior CV event (%) None Excluded Excluded Excluded Study duration (y) % in A1c = 40% microvascular complications Int vs std HbA1c 6.4 vs vs vs vs vs vs vs 9.4 (%) Micro benefit Nephro Nephro Yes Yes No Yes Macro benefit Major harms Nonfatal MI (ARR 1%) Mortality (ARI 1%) No No (5y FU) No Yes (10y FU) No Yes (in EDIC) No Yes (10y FU) Yes Hypo Hypo Hypo Hypo Hypo Hypo Med Clin N Am 99 (2015) 47 67
15 Yes No Does lowering glucose decrease the risk of macrovascular complications? Maybe
16 16
17 Maybe Does lowering glucose decrease the risk of macrovascular complications?
18 Macrovascular complications ACCORD 2008 ADVANCE y FU VADT y FU DCCT y FU UKPDS-SU y FU UKPDS-MET y FU Kumamato Mean age (y) 62 ± 7 66 ± 6 60 ± ± 9 53 ± 8 48 ± 12 Duration DM (y) New dx New dx 6.5 Baseline HbA1c (%) Prior CV event (%) None Excluded Excluded Excluded Study duration (y) Int vs std HbA1c 6.4 vs vs vs vs vs vs vs 9.4 (%) Micro benefit Nephro Nephro Yes Yes No Yes Macro benefit Major harms Nonfatal MI (ARR 1%) Mortality (ARI 1%) No No (5y FU) Med Clin N Am 99 (2015) No Yes (10y FU) No Yes (in EDIC) No Yes (10y FU) Yes Hypo Hypo Hypo Hypo Hypo Hypo
19 Glycemic control and CV events Major Cardiovascular event 0.91 ( ) Turnbull FM, et al. Diabetologia 2009; 52:
20 Glycemic control and CV events Myocardial infarction 0.85 ( ) Turnbull FM, et al. Diabetologia 2009; 52:
21 Intensive Glycemic Control DM2 Benefit If No Hx of Vascular Disease History of macrovascular disease Absent History of microvascular disease Absent 0.84 ( ) 0.89 ( ) Turnbull FM, et al. Diabetologia 2009; 52:
22 Intensive Glycemic Control DM2 Benefit If No Hx of Vascular Disease History of macrovascular disease Absent History of microvascular disease Absent 0.84 ( ) 0.89 ( ) Turnbull FM, et al. Diabetologia 2009; 52:
23 Intensive Glycemic Control DM2 Benefit If No Hx of Vascular Disease History of macrovascular disease Absent History of microvascular disease Absent 0.84 ( ) 0.89 ( ) Turnbull FM, et al. Diabetologia 2009; 52:

24 Rosiglitazone increases risk of MI Nissen SE, Wolski K. N Engl J Med 2007;356:
25 2008 U.S. FDA CV Safety Guidance for New Antihyperglycemic Agents Upper bound of the 95% CI for the estimated risk ratio of <1.3* Upper bound of the 95% CI for the estimated risk ratio of * Upper bound of the 95% CI for the estimated risk ratio of >1.8 Approvable: May be no need for postmarketing study Approvable: need for postmarketing study { Not approvable * With a reassuring point estimate for overall CV risk { Superiority Non-inferiority Non-inferiority { Inferior Underpowered Non-inferiority Boundary HR Hazard ratio Participants with higher CV risk 2 years of CV safety data Prospective, independent and blinded adjudication of CV events (include MACE)** Design and conduct should allow for future meta-analysis Hirshberg B, Raz I. Diabetes Care. 2011;34:S101-6.
26 Case Mr. Singh 59 year old man Self-employed contractor A1c 6.3% 75g OGTT Fasting glucose 6.2 mmol/l (<6.1) 2hr glucose 8.9 mmol/l (<7.8)
27 Goldenberg R, Punthakee Z, Canadian Diabetes Association 2013 Clinical Practice Guidelines for the Prevention and Management of Diabetes in Canada:Definition, Classification and Diagnosis of Diabetes, Prediabetes and Metabolic Syndrome. Can J Diabetes 2013;37(suppl 1):S61-S68. Diagnosis of Prediabetes Test Result Prediabetes Category Fasting Plasma Glucose (mmol/l) 2-hr Plasma Glucose in a 75-g Oral Glucose Tolerance Test (mmol/l) Glycated Hemoglobin (A1C) (%) Impaired fasting glucose (IFG) Impaired glucose tolerance (IGT) Prediabetes
28 What is his risk of progressing to diabetes in the next five years? 25% 50% 75% 100%

29 Progression to diabetes FPG of 6.1 to 6.9 mmol/l + A1C of 6.0% to 6.4% predictive of 100% progression to type 2 diabetes over 5-year period Heianza Y Diabetic Med 20012;29;e279 e285 Zhang X et al. Diabetes Care. 2010;33:
30 What would you do next? Reassess with labs in 6 months Refer to local diabetes education centre (DEC) Refer to endocrinologist Start metformin Start acarbose
31 Diabetes Prevention Program Trial Metformin 31% Lifestyle 58% Diabetes Prevention Program (DPP) Research Group. N Engl J Med 2002;346:


32 Acarbose progression to DM2 by 25% 25% Chiasson JL, et al. Lancet 2002;359:
33 Metformin Medication Coverage on ODB Formulary Cost for 30 Day Supply Metformin 500mg tablets Glumetza (extended release metformin) Yes 1 g BID - $7 No 1g (2x500mg tabs) daily - $35 2 g (2x1000mg tabs) daily - $73 Henry Halapy, RPh, Diabetes Pharmacist, St. Michael s Hospital 2015
34 Metformin and risk of MI 0.90 ( ) Boussageon R et al. PLoS Med (4): e doi: /journal.pmed
35 Metformin
36 Mr. Singh 4 years later 63 year old contractor Attended local DEC x 2 visit Widowed gained 5 kg Metformin 1 g bid Labs A1c 7.6% egfr > 60 ml/min ACR 1.2 mg/mmol
37 What would you do next? Refer to local diabetes education centre (DEC) Refer to endocrinologist Acarbose Secretagogue (e.g. Gliclazide MR) DPP4 inhibitor (e.g. Sitagliptin) SGLT2 inhibitor (e.g. Canagliflozin, Empagliflozin) Incretin (e.g. Liraglutide)
38
39
40
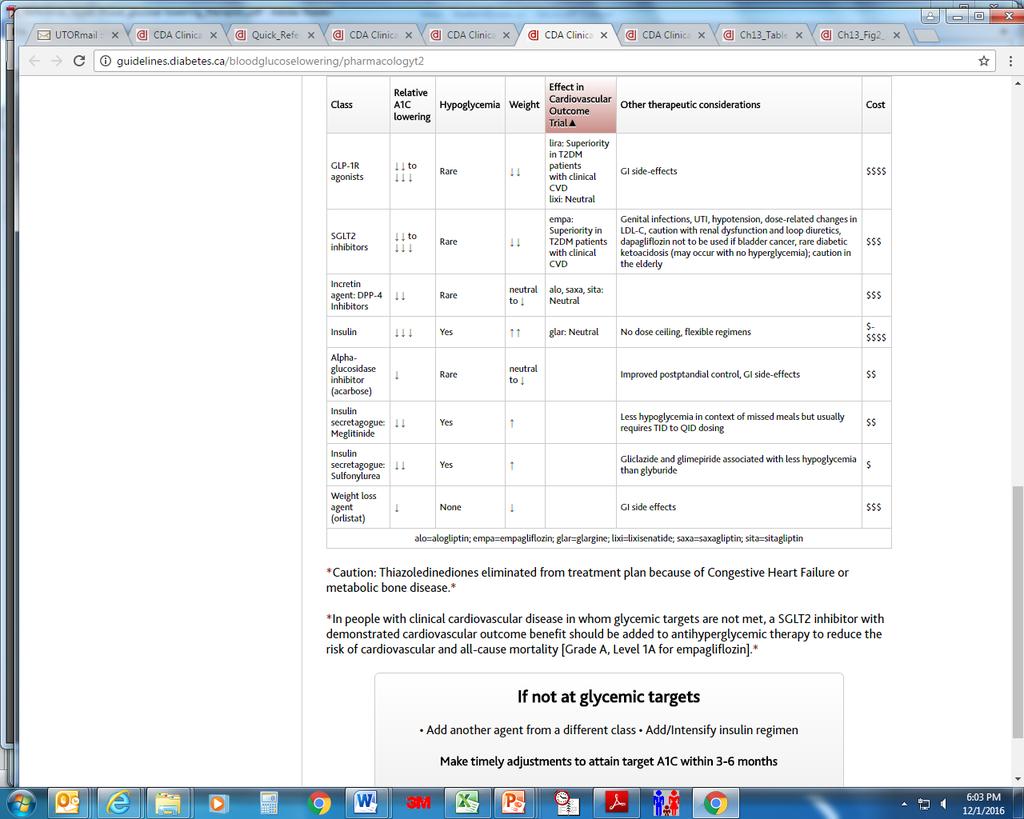
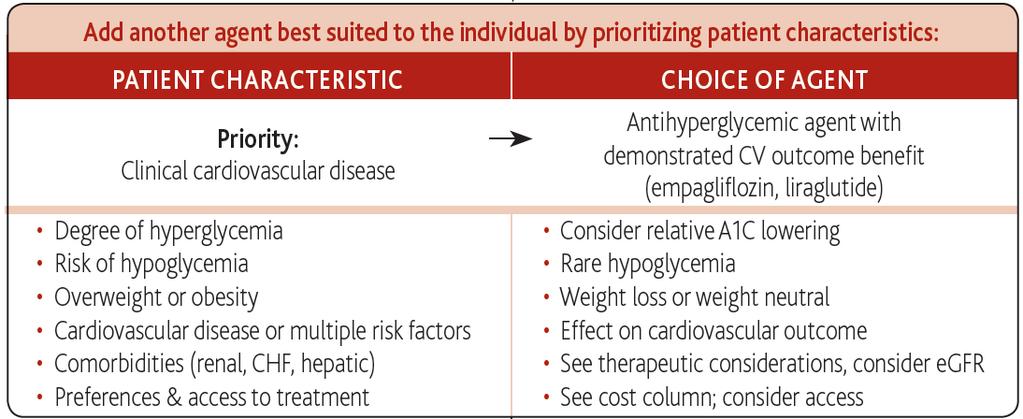
41 Add another class of agent best suited to the individual (agents listed in alphabetical order): Class Relative A1C Lowering Hypoglycemi a Weight Effect in Cardiovascular Outcome Trial Other therapeutic considerations Cost α-glucosidase inhibitor (acarbose) Rare Neutral to Improved postprandial control, GI side-effects $$ DPP-4 Inhibitors Rare Neutral to alo, saxa, sita: Neutral Caution with saxagliptin in heart failure $$$ GLP-1R agonists to Rare lira: Superiority in T2DM patients with clinical CVD lixi: Neutral GI side-effects $$$$ Insulin Yes Neutral (glar) No dose ceiling, flexible regimens $-$$$$ Insulin secretagogue: Meglitinide Sulfonylurea Yes Yes Less hypoglycemia in context of missed meals but usually requires TID to QID dosing Gliclazide and glimepiride associated with less hypoglycemia than glyburide $$ $ SGLT2 inhibitors to Rare empa: Superiority in T2DM patients with clinical CVD Genital infections, UTI, hypotension, doserelated changes in LDL-C, caution with renal dysfunction and loop diuretics, dapagliflozin not to be used if bladder cancer, rare diabetic ketoacidosis (may occur with no hyperglycemia) $$$
42
43 Add another class of agent best suited to the individual (agents listed in alphabetical order): Class Relative A1C Lowering Hypoglycemi a Weight Effect in Cardiovascular Outcome Trial Other therapeutic considerations Cost α-glucosidase inhibitor (acarbose) Rare Neutral to Improved postprandial control, GI side-effects $$ DPP-4 Inhibitors Rare Neutral to alo, saxa, sita: Neutral Caution with saxagliptin in heart failure $$$ GLP-1R agonists to Rare lira: Superiority in T2DM patients with clinical CVD lixi: Neutral GI side-effects $$$$ Insulin Yes Neutral (glar) No dose ceiling, flexible regimens $-$$$$ Insulin secretagogue: Meglitinide Sulfonylurea Yes Yes Less hypoglycemia in context of missed meals but usually requires TID to QID dosing Gliclazide and glimepiride associated with less hypoglycemia than glyburide $$ $ SGLT2 inhibitors to Rare empa: Superiority in T2DM patients with clinical CVD Genital infections, UTI, hypotension, doserelated changes in LDL-C, caution with renal dysfunction and loop diuretics, dapagliflozin not to be used if bladder cancer, rare diabetic ketoacidosis (may occur with no hyperglycemia) $$$
44 Add another class of agent best suited to the individual (agents listed in alphabetical order): Class Relative A1C Lowering Hypoglycemi a Weight Effect in Cardiovascular Outcome Trial Other therapeutic considerations Cost α-glucosidase inhibitor (acarbose) Rare Neutral to Improved postprandial control, GI side-effects $$ DPP-4 Inhibitors Rare Neutral to alo, saxa, sita: Caution with saxagliptin in heart failure $$$ α-glucosidase Neutral inhibitor GLP-1R agonists to Rare lira: Superiority GI side-effects $$$$ in T2DM patients with clinical CVD lixi: Neutral Insulin Yes Neutral (glar) No dose ceiling, flexible regimens $-$$$$ Insulin secretagogue: Meglitinide Sulfonylurea Yes Yes Less hypoglycemia in context of missed meals but usually requires TID to QID dosing Gliclazide and glimepiride associated with less hypoglycemia than glyburide $$ $ SGLT2 inhibitors to Rare empa: Superiority in T2DM patients with clinical CVD Genital infections, UTI, hypotension, doserelated changes in LDL-C, caution with renal dysfunction and loop diuretics, dapagliflozin not to be used if bladder cancer, rare diabetic ketoacidosis (may occur with no hyperglycemia) $$$
45 Alpha-glucosidase inhibitors Medication Coverage on ODB Formulary Cost for 30 Day Supply Alpha-glucosidase inhibitors Acarbose (Glucobay ) LU code 175 failed treatment with other drugs 176 in combination with other drugs 50mg tabs TID $ mg tabs TID - $34 Henry Halapy, RPh, Diabetes Pharmacist, St. Michael s Hospital 2015
46 Acarbose and CV events Myocardial infarction Hanefeld M et al. Eur Heart J 2004;25(1):10-16
47 Acarbose GI side effect slow titration! Week Breakfast Lunch Dinner
48 Acarbose
49 Acarbose
50 Add another class of agent best suited to the individual (agents listed in alphabetical order): Class Relative A1C Lowering Hypoglycemi a Weight Effect in Cardiovascular Outcome Trial Other therapeutic considerations Cost α-glucosidase inhibitor (acarbose) Rare Neutral to Improved postprandial control, GI side-effects $$ Insulin secretagogues DPP-4 Inhibitors Rare Neutral to alo, saxa, sita: Caution with saxagliptin in heart failure Neutral $$$ GLP-1R agonists to Rare lira: Superiority in T2DM patients with clinical CVD lixi: Neutral GI side-effects $$$$ Insulin Yes Neutral (glar) No dose ceiling, flexible regimens $-$$$$ Insulin secretagogue: Meglitinide Sulfonylurea Yes Yes Less hypoglycemia in context of missed meals but usually requires TID to QID dosing Gliclazide and glimepiride associated with less hypoglycemia than glyburide $$ $ SGLT2 inhibitors to Rare empa: Superiority in T2DM patients with clinical CVD Genital infections, UTI, hypotension, doserelated changes in LDL-C, caution with renal dysfunction and loop diuretics, dapagliflozin not to be used if bladder cancer, rare diabetic ketoacidosis (may occur with no hyperglycemia) $$$
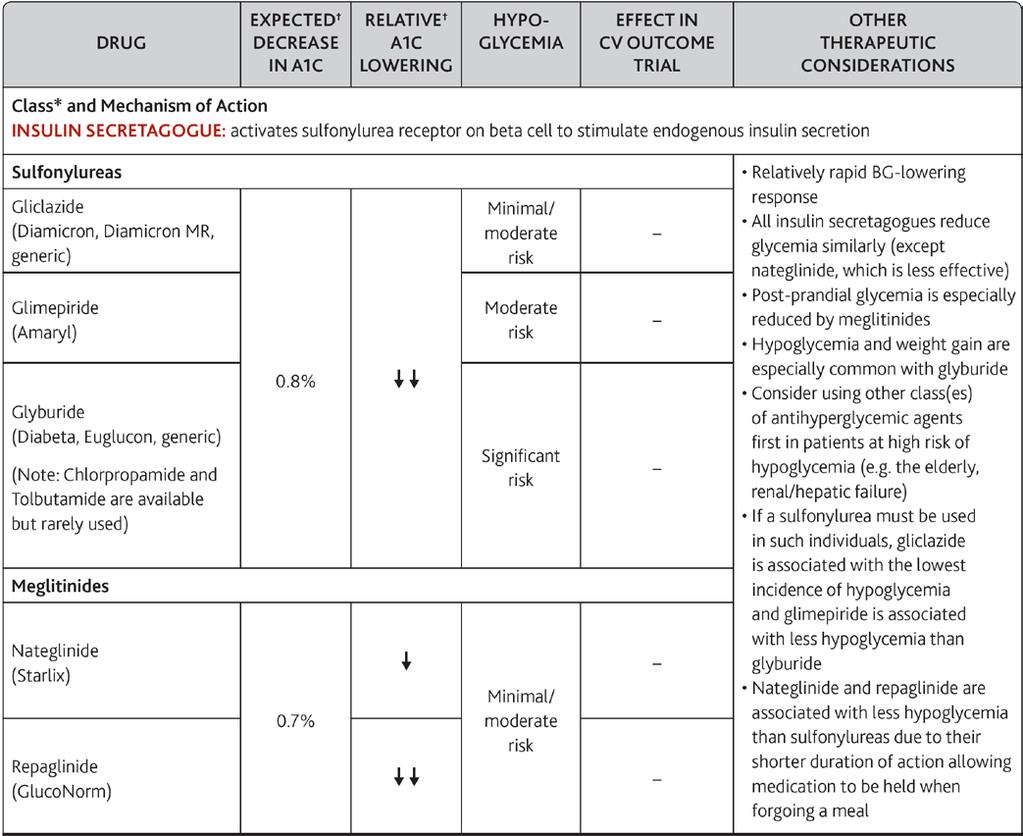
51 Insulin secretagogues Medication Coverage on ODB Formulary Cost for 30 Day Supply Insulin secretagogues Glyburide Yes 10 mg BID - $4 Gliclazide (Diamicron ) Yes 160 mg BID - $7 Gliclazide MR (Diamicron MR ) Yes 4 x 30mg MR tabs - $11 2 x 60mg MR - $15 Glimepiride (Amaryl ) No 8 mg daily - $59 Repaglinide (Gluconorm ) EAP i.e. Section 8 4 mg QID -$58 Nateglinide (Starlix ) No 180 mg TID - $106 Henry Halapy, RPh, Diabetes Pharmacist, St. Michael s Hospital 2015
52 Sulphonylureas and CV events Outcome # trials OR 95% CI p Mortality MACE Stroke MI CV death Monami M et al. Diabetes, Obesity & Metabolism; 2013; 15:
53
54 Mr. Singh 4 years later 63 year old contractor Attended local DEC x 2 visit Widowed gained 5 kg Metformin 1 g bid Labs A1c 7.6% egfr > 60 ml/min ACR 1.2 mg/mmol
55 Mr. Singh 6 years later 69 year old retired man Metformin 1g bid Gliclazide MR 60mg bid Recent diagnosis of CAD and CHF Labs A1c 7.9% egfr 68 mmol/min ACR 2.4 mg/mmol
56 What would you do next? Refer to local diabetes education centre (DEC) Refer to endocrinologist DPP4 inhibitor (e.g. Sitagliptin) SGLT2 inhibitor (e.g. Empagliflozin) Incretin (e.g. Liraglutide)
57
58
59
60 Add another class of agent best suited to the individual (agents listed in alphabetical order): Class Relative A1C Lowering Hypoglycemi a Weight Effect in Cardiovascular Outcome Trial Other therapeutic considerations Cost α-glucosidase inhibitor (acarbose) Rare Neutral to Improved postprandial control, GI side-effects $$ DPP-4 Inhibitors Rare Neutral to alo, saxa, sita: Neutral Caution with saxagliptin in heart failure $$$ GLP-1R agonists to Rare lira: Superiority in T2DM patients with clinical CVD lixi: Neutral GI side-effects $$$$ Insulin SGLT2 inhibitors Yes Neutral (glar) No dose ceiling, flexible regimens $-$$$$ Insulin secretagogue: Meglitinide Yes $$ Sulfonylurea Yes Less hypoglycemia in context of missed meals but usually requires TID to QID dosing Gliclazide and glimepiride associated with less hypoglycemia than glyburide $ SGLT2 inhibitors to Rare empa: Superiority in T2DM patients with clinical CVD Genital infections, UTI, hypotension, doserelated changes in LDL-C, caution with renal dysfunction and loop diuretics, dapagliflozin not to be used if bladder cancer, rare diabetic ketoacidosis (may occur with no hyperglycemia) $$$
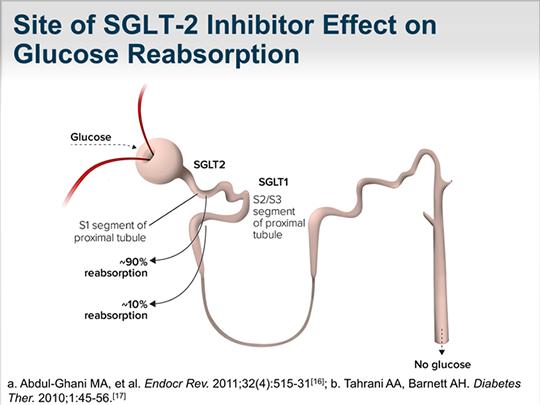
61 SGLT2 Inhibitors
62 SGLT2 Inhibitors Medication Coverage on ODB Formulary Cost for 30 Day Supply SGLT-2 Inhibitors Canagliflozin (Invokana ) Dapaglifozin (Forxiga ) Empagliflozin (Jardiance ) Yes 100 mg daily - $ mg daily - $78 Yes 5 mg daily - $91 10 mg daily - $91 Yes 10 mg daily - $92 25 mg daily - $92 Henry Halapy, RPh, Diabetes Pharmacist, St. Michael s Hospital
63 CV outcomes SGLT2 Inhibitor Courtesy of A. Y. Y. Cheng 2016
64 Empagliflozin and CV Outcomes Primary outcome CV death 14% 38% Death from any cause 32% CHF hospitalization 35% Zinman B et al. N Engl J Med DOI: /NEJMoa
 Zinman B et al. N Engl J Med 2015. DOI: 10.")
65 Genital infections Genital infections 5% male balanitis (if not circumcised) 10% female ml more urine per day (1 extra void) Zinman B et al. N Engl J Med DOI: /NEJMoa
66 SGLT2 Inhibitor CV end point studies CANVAS CANagliflozin cardiovascular Assessment Study Estimated Study Completion Date June 2017 DECLARE-TIMI 58 Dapagliflozin Effect on CardiovascuLAR Events Estimated Primary Completion Date April 2019
67 SGLT2 Inhibitor safety data Euglycemic DKA Decreased insulin dose Decreased renal clearance of ketone bodies SGLT2 inhibitors increase glucagon secretion Increased risk of fractures and bone loss Canagliflozin studies
68 Incretin therapies

69 Incretin therapies GLP-1 t ½ 90 seconds DPP4 degrades GLP-1
70 Add another class of agent best suited to the individual (agents listed in alphabetical order): Class Relative A1C Lowering Hypoglycemi a Weight Effect in Cardiovascular Outcome Trial Other therapeutic considerations Cost α-glucosidase inhibitor (acarbose) DPP-4 Inhibitors Rare Neutral to Improved postprandial control, GI side-effects $$ GLP-1R agonist Rare Neutral to alo, saxa, sita: Caution with saxagliptin in heart failure $$$ Neutral GLP-1R agonists to Rare lira: Superiority in T2DM patients with clinical CVD lixi: Neutral GI side-effects $$$$ Insulin Yes Neutral (glar) No dose ceiling, flexible regimens $-$$$$ Insulin secretagogue: Meglitinide Sulfonylurea Yes Yes Less hypoglycemia in context of missed meals but usually requires TID to QID dosing Gliclazide and glimepiride associated with less hypoglycemia than glyburide $$ $ SGLT2 inhibitors to Rare empa: Superiority in T2DM patients with clinical CVD Genital infections, UTI, hypotension, doserelated changes in LDL-C, caution with renal dysfunction and loop diuretics, dapagliflozin not to be used if bladder cancer, rare diabetic ketoacidosis (may occur with no hyperglycemia) $$$
71 Incretin therapies Medication Coverage on ODB Formulary Cost for 30 Day Supply GLP-1 agonists Liraglutide (Victoza ) Dulaglutide (Trulicity ) Exenatide (Byetta ) No 1.2mg sc daily - $ mg sc daily - $253 No 0.75mg sc weekly - $ mg sc weekly - $277 No 5-10mcg sc BID - $144
72 LEADER Liraglutide 0.87 ( ) ARR 1.9% NNT 52 N Engl J Med 2016;375:
73 SUSTAIN-6 Semaglutide 0.74 ( ) ARR 2.3% NNT 43 N Engl J Med 2016;375:
74 CV outcomes GLP-1 RA Courtesy of A. Y. Y. Cheng 2016
75 GLP-1 Agonists
76 Add another class of agent best suited to the individual (agents listed in alphabetical order): Class Relative A1C Lowering Hypoglycemi a Weight Effect in Cardiovascular Outcome Trial Other therapeutic considerations Cost α-glucosidase inhibitor (acarbose) Rare Neutral to Improved postprandial control, GI side-effects $$ DPP-4 Inhibitors Rare Neutral to alo, saxa, sita: Neutral Caution with saxagliptin in heart failure $$$ GLP-1R agonists to Rare lira: Superiority in T2DM patients GI side-effects $$$$ DPP-4 with inhibitors clinical CVD lixi: Neutral Insulin Yes Neutral (glar) No dose ceiling, flexible regimens $-$$$$ Insulin secretagogue: Meglitinide Sulfonylurea Yes Yes Less hypoglycemia in context of missed meals but usually requires TID to QID dosing Gliclazide and glimepiride associated with less hypoglycemia than glyburide $$ $ SGLT2 inhibitors to Rare empa: Superiority in T2DM patients with clinical CVD Genital infections, UTI, hypotension, doserelated changes in LDL-C, caution with renal dysfunction and loop diuretics, dapagliflozin not to be used if bladder cancer, rare diabetic ketoacidosis (may occur with no hyperglycemia) $$$
77 Incretin therapies Medication Coverage on ODB Formulary Cost for 30 Day Supply DPP-IV inhibitors Sitagliptin (Januvia ) Saxagliptin (Onglyza ) Linagliptin (Trajenta ) Yes 25mg daily - $89 50mg daily - $ mg daily -$89 Yes 2.5mg daily - $71 5mg daily - $85 Yes 5mg daily - $77
78 DPP4 Inhibitors + metformin Medication Coverage on ODB Formulary Cost for 30 Day Supply Combination pills Janumet (sitagliptin + metformin) Janumet XR (sitagliptin + sustained release metformin) Komboglyze (saxagliptin + metformin) Jentodueto (linagliptin + metformin) Yes 50/500mg BID - $96 50/850mg BID - $96 50mg/1000mg BID - $96 Yes 50/1000mg 2 tabs together once daily - $96 Yes 2.5mg/500mg BID - $76 2.5mg/850mg BID - $76 2.5mg/1000mg BID - $76 Yes 2.5mg/500mg BID - $80 2.5mg/850mg BID - $80 2.5mg/1000mg BID - $80

79 CV outcomes DPP4 inhibitor Courtesy of A. Y. Y. Cheng 2016

80 Scirica BM et al. N Engl J Med 2013;369: SAVOR-TIMI 53 Saxagliptin and CV events Hospitalization for Heart Failure 3.5% 2.8% 1.27 ( ) 0.007
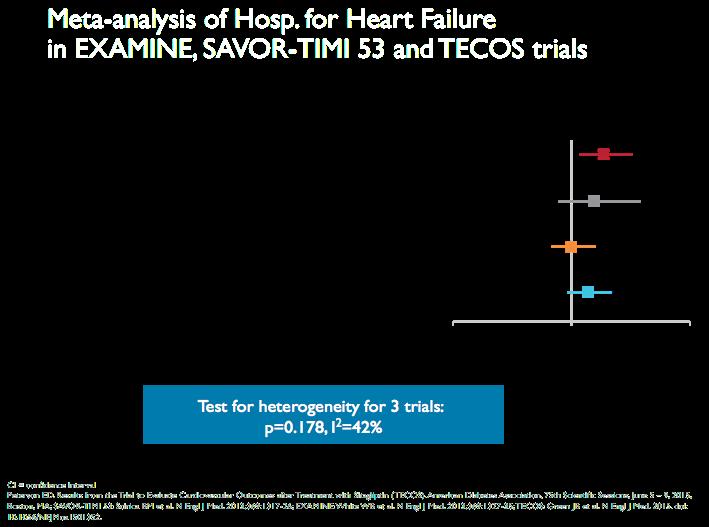
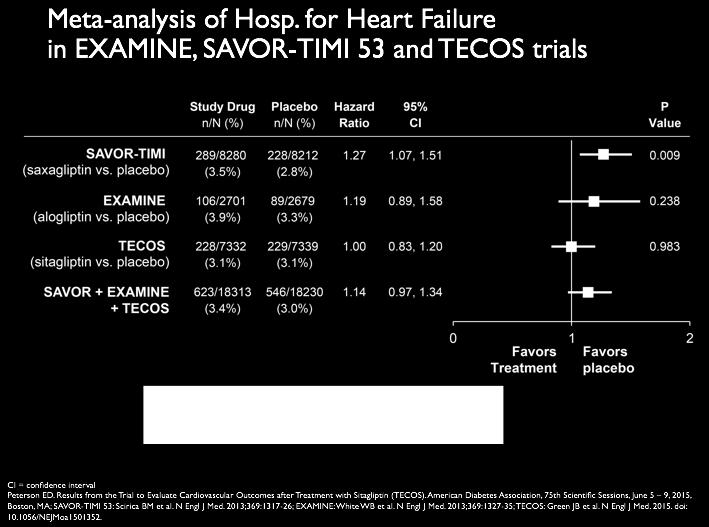
81 Heart Failure Hospitalization with DPP4i 1.14 ( )
82 DPP4 Inhibitors and CV endpoints Linagliptin CARdiovascular Outcome Trial of LINAgliptin Versus Glimepiride in Type 2 Diabetes (CAROLINA ) Estimated Study Completion Date: September 2018
83 DPP4 Inhibitor pancreas safety data Study arms SAVOR-TIMI 53 1,2 EXAMINE 3 TECOS 4 Placebo n=8,212 Saxaglptinn =8,220 Placebo n=2,679 Alogliptin n=2,701 Placebo n=7,339 Sitagliptin n=7,332 Acute pancreatitis (n) Chronic pancreatitis (n) Malignancy (%) Pancreatic cancer (n) Scirica BM et al. N Engl J Med. 2013;369:1317-2; 3 White WB et al. N Engl J Med. 2013;369: Raz I et al. Diabetes Care. 2014;37: Green JB et al. N Engl J Med doi: /NEJMoa
84 DPP4 Inhibitor safety data Pancreatitis Insufficient data should be discontinued if pancreatitis confirmed should not be started if history of pancreatitis Pancreatic cancer monitoring for and reporting of pancreatic adverse effects by FDA and European Societies Joint pain
85 DPP4 - Inhibitors
86 Mr. Singh 69 year old retired man Metformin 1g bid Gliclazide MR 60mg bid Recent diagnosis of CAD and CHF Labs A1c 7.9% egfr 68 mmol/min ACR 2.4 mg/mmol
87 What would you do next? Refer to local diabetes education centre (DEC) Refer to endocrinologist DPP4 inhibitor (e.g. Sitagliptin) SGLT2 inhibitor (e.g. Empagliflozin) Incretin (e.g. Liraglutide)
88 Mr. Singh 4 years later 73 year old man Metformin 1 g bid Gliclazide MR 60 mg bid Empagliflozin 10 mg Labs A1c 7.2% egfr 44 ml/min ACR 4.2 mg/mmol
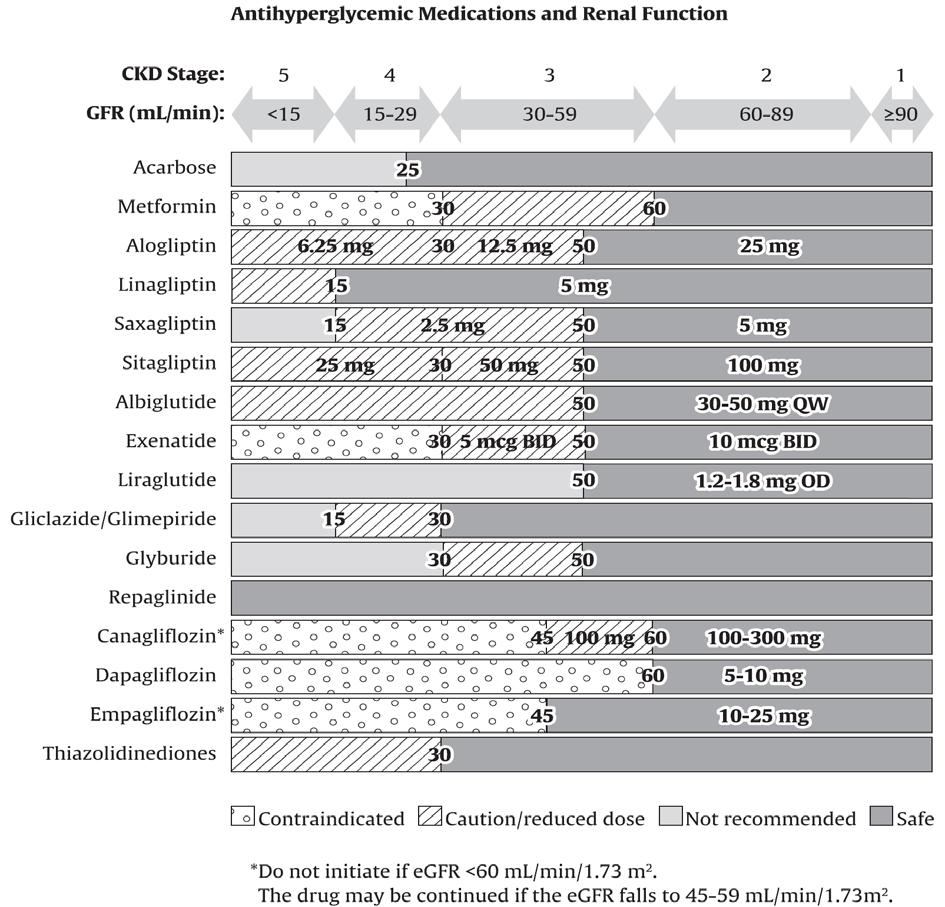
89 Which medications need adjustment for his renal impairment? Metformin Gliclazide MR Canagliflozin
90 Which medications need adjustment for renal impairment? Metformin Gliclazide MR Canagliflozin
91
92

93 Mr. Singh 3 months later 73 year old man Metformin 500 mg bid Gliclazide MR 60 mg bid Labs A1c 8.2 % egfr 42 ml/min
94 Refer to local DEC What would you do next? Refer to endocrinologist Start basal insulin (e.g. 10 units hs) Start mixed insulin Start linagliptin
95 Which oral medication should be discontinued with basal insulin? Metformin Secretagogues Acarbose DPP4 inhibitors SGLT2 inhibitors Incretins (e.g. liraglutide) Thiazoladinediones
96 Which oral medication should be discontinued with basal insulin? Metformin off label in Canada Secretagogues off label in Canada Acarbose DPP4 inhibitors linagliptin not approved SGLT2 inhibitors Incretins (e.g. liraglutide) Thiazoladinediones
97 Which oral medication should be discontinued with mixed insulin? Metformin Secretagogues Acarbose DPP4 inhibitors SGLT2 inhibitors Incretins (e.g. liraglutide) Thiazoladinediones
98 Which oral medication should be discontinued with mixed insulin? Metformin off label use in Canada Secretagogues Acarbose DPP4 inhibitors linagliptin not approved SGLT2 inhibitors Incretins (e.g. liraglutide) off label use Thiazoladinediones
99 Learning Objectives At the end of the session, participants will be able to: Identify patient factors that impact the addition of non-insulin pharmacotherapy in Type 2 Diabetes Discuss the glycemic and cardiovascular end-point evidence among non-insulin pharmacotherapies in Type 2 Diabetes Apply evidence based diabetes management to individual patient care
100
101 Add another class of agent best suited to the individual (agents listed in alphabetical order): Class Relative A1C Lowering Hypoglycemi a Weight Effect in Cardiovascular Outcome Trial Other therapeutic considerations Cost α-glucosidase inhibitor (acarbose) Rare Neutral to Improved postprandial control, GI side-effects $$ DPP-4 Inhibitors Rare Neutral to alo, saxa, sita: Neutral Caution with saxagliptin in heart failure $$$ GLP-1R agonists to Rare lira: Superiority in T2DM patients with clinical CVD lixi: Neutral GI side-effects $$$$ Insulin Yes Neutral (glar) No dose ceiling, flexible regimens $-$$$$ Insulin secretagogue: Meglitinide Sulfonylurea Yes Yes Less hypoglycemia in context of missed meals but usually requires TID to QID dosing Gliclazide and glimepiride associated with less hypoglycemia than glyburide $$ $ SGLT2 inhibitors to Rare empa: Superiority in T2DM patients with clinical CVD Genital infections, UTI, hypotension, doserelated changes in LDL-C, caution with renal dysfunction and loop diuretics, dapagliflozin not to be used if bladder cancer, rare diabetic ketoacidosis (may occur with no hyperglycemia) $$$
102
103
104 Learning Objectives At the end of the session, participants will be able to: Identify patient factors that impact the addition of non-insulin pharmacotherapy in Type 2 Diabetes Discuss the glycemic and cardiovascular end-point evidence among non-insulin pharmacotherapies in Type 2 Diabetes Apply evidence based diabetes management to individual patient care
MANAGING DIABETES IN 2017 WHAT TO ADD, WHEN AND WHY? December 8, 2017 Maria Wolfs MD MHSc FRCPC
 MANAGING DIABETES IN 2017 WHAT TO ADD, WHEN AND WHY? December 8, 2017 Maria Wolfs MD MHSc FRCPC Faculty Disclosure Faculty: Maria Wolfs MD, MHSc, FRCPC Assistant Professor, University of Toronto Endocrinologist,
MANAGING DIABETES IN 2017 WHAT TO ADD, WHEN AND WHY? December 8, 2017 Maria Wolfs MD MHSc FRCPC Faculty Disclosure Faculty: Maria Wolfs MD, MHSc, FRCPC Assistant Professor, University of Toronto Endocrinologist,
Managing Perioperative Diabetes What s new? Kathryn A. Myers MD FRCPC Chair Chief Division of GIM Professor of Medicine Western University
 Managing Perioperative Diabetes What s new? Kathryn A. Myers MD FRCPC Chair Chief Division of GIM Professor of Medicine Western University Objectives: By the end of this session, you will be able to: Identify
Managing Perioperative Diabetes What s new? Kathryn A. Myers MD FRCPC Chair Chief Division of GIM Professor of Medicine Western University Objectives: By the end of this session, you will be able to: Identify
DIABETES DEBATE - IS NEW BETTER?
 DIABETES DEBATE - IS NEW BETTER? WHAT MEDICATION CLASS AFTER METFORMIN TO CONTROL BLOOD SUGAR Dr. Lydia Hatcher, MD, CCFP, FCFP, CHE, D-CAPM Associate Clinical Professor of Family Medicine, McMaster Chief
DIABETES DEBATE - IS NEW BETTER? WHAT MEDICATION CLASS AFTER METFORMIN TO CONTROL BLOOD SUGAR Dr. Lydia Hatcher, MD, CCFP, FCFP, CHE, D-CAPM Associate Clinical Professor of Family Medicine, McMaster Chief
Disclaimers 22/03/2018. Role of DPP-4 Inhibitors, GLP-1 Agonists, and SGLT-2 Inhibitors in the treatment of Diabetes Mellitus Type 2
 Disclaimers Role of DPP-4 Inhibitors, GLP-1 Agonists, and SGLT-2 Inhibitors in the treatment of Diabetes Mellitus Type 2 I have not received money or gifts from medical device companies or from the pharmaceutical
Disclaimers Role of DPP-4 Inhibitors, GLP-1 Agonists, and SGLT-2 Inhibitors in the treatment of Diabetes Mellitus Type 2 I have not received money or gifts from medical device companies or from the pharmaceutical
Oral and Injectable Non-insulin Antihyperglycemic Agents
 Appendix 5: Diabetes Education and Medical Management in Adults with Diabetes Oral and Injectable Non-insulin s This directive will be implemented by RPhs, RNs or RDs who have been deemed authorized implementers.
Appendix 5: Diabetes Education and Medical Management in Adults with Diabetes Oral and Injectable Non-insulin s This directive will be implemented by RPhs, RNs or RDs who have been deemed authorized implementers.
The Flozins Quest for Clarity?
 The Flozins Quest for Clarity? Choosing Wisely with Academic Detailing 2018 ARE THEY THE REAL DEAL Disclosure statements The Academic Detailing Service is operated by Dalhousie Continuing Professional
The Flozins Quest for Clarity? Choosing Wisely with Academic Detailing 2018 ARE THEY THE REAL DEAL Disclosure statements The Academic Detailing Service is operated by Dalhousie Continuing Professional
The Death of Sulfonylureas? A Review of New Diabetes Medications
 The Death of Sulfonylureas? A Review of New Diabetes Medications Kelly Hoenig, Pharm.D., BCPS Cedar Rapids Family Medicine Residency 2/4/17 Objectives Review GLP-1 Agonists, DPP-IV Inhibitors and SGLT-2
The Death of Sulfonylureas? A Review of New Diabetes Medications Kelly Hoenig, Pharm.D., BCPS Cedar Rapids Family Medicine Residency 2/4/17 Objectives Review GLP-1 Agonists, DPP-IV Inhibitors and SGLT-2
Canadian Society of Internal Medicine Annual Meeting 2016 Montreal, QC
 Canadian Society of Internal Medicine Annual Meeting 2016 Montreal, QC Choosing the Right Agent for your Patient with diabetes: Individualizing type 2 diabetes management in light of the expanding therapies
Canadian Society of Internal Medicine Annual Meeting 2016 Montreal, QC Choosing the Right Agent for your Patient with diabetes: Individualizing type 2 diabetes management in light of the expanding therapies
Very Practical Tips for Managing Type 2 Diabetes
 Very Practical Tips for Managing Type 2 Diabetes Jean-François Yale, MD, FRCPC McGill University Health Centre, Montreal, Canada Jean-francois.yale@mcgill.ca www.dryale.ca OBJECTIVES DISCLOSURES The participant
Very Practical Tips for Managing Type 2 Diabetes Jean-François Yale, MD, FRCPC McGill University Health Centre, Montreal, Canada Jean-francois.yale@mcgill.ca www.dryale.ca OBJECTIVES DISCLOSURES The participant
Table 1. Antihyperglycemic agents for use in type 2 diabetes
 Table 1. Antihyperglycemic agents for use in type 2 diabetes DRUG IN ALPHA-GLUCOSIDASE INHIBITOR: inhibits pancreatic alpha-amyle and intestinal alpha-glucoside Acarbose (Glucobay) 0.6% Negligible Not
Table 1. Antihyperglycemic agents for use in type 2 diabetes DRUG IN ALPHA-GLUCOSIDASE INHIBITOR: inhibits pancreatic alpha-amyle and intestinal alpha-glucoside Acarbose (Glucobay) 0.6% Negligible Not
Quick Reference Guide
 2013 Clinical Practice Guidelines Quick Reference Guide (Updated November 2016) 416569-16 guidelines.diabetes.ca diabetes.ca 1-800-BANTING (226-8464) Copyright 2016 Canadian Diabetes Association SCREENING
2013 Clinical Practice Guidelines Quick Reference Guide (Updated November 2016) 416569-16 guidelines.diabetes.ca diabetes.ca 1-800-BANTING (226-8464) Copyright 2016 Canadian Diabetes Association SCREENING
Type 2 Diabetes: Where Do We Start with Treatment? DIABETES EDUCATION. Diabetes Mellitus: Complications and Co-Morbid Conditions
 Diabetes Mellitus: Complications and Co-Morbid Conditions ADA Guidelines for Glycemic Control: 2016 Retinopathy Between 2005-2008, 28.5% of patients with diabetes 40 years and older diagnosed with diabetic
Diabetes Mellitus: Complications and Co-Morbid Conditions ADA Guidelines for Glycemic Control: 2016 Retinopathy Between 2005-2008, 28.5% of patients with diabetes 40 years and older diagnosed with diabetic
LATE BREAKING STUDIES IN DM AND CAD. Will this change the guidelines?
 LATE BREAKING STUDIES IN DM AND CAD Will this change the guidelines? Objectives 1. Discuss current guidelines for prevention of CHD in diabetes. 2. Discuss the FDA Guidance for Industry regarding evaluating
LATE BREAKING STUDIES IN DM AND CAD Will this change the guidelines? Objectives 1. Discuss current guidelines for prevention of CHD in diabetes. 2. Discuss the FDA Guidance for Industry regarding evaluating
Quick Reference Guide
 2018 Clinical Practice Guidelines Quick Reference Guide 416569-18 guidelines.diabetes.ca diabetes.ca 1-800-BANTING (226-8464) Screening and Diagnosis Assess risk ANNUALLY if: Family history (First-degree
2018 Clinical Practice Guidelines Quick Reference Guide 416569-18 guidelines.diabetes.ca diabetes.ca 1-800-BANTING (226-8464) Screening and Diagnosis Assess risk ANNUALLY if: Family history (First-degree
Multiple Small Feedings of the Mind: Diabetes. Sonja K Fredrickson, MD, BC-ADM March 7, 2014
 Multiple Small Feedings of the Mind: Diabetes Sonja K Fredrickson, MD, BC-ADM March 7, 2014 Question 1: Setting A1c Goals Describe the evidence based approach to determining the target HgbA1c in different
Multiple Small Feedings of the Mind: Diabetes Sonja K Fredrickson, MD, BC-ADM March 7, 2014 Question 1: Setting A1c Goals Describe the evidence based approach to determining the target HgbA1c in different
Faculty/Presenter Disclosure
 DIABETES UPATE 2016 Faculty/Presenter Disclosure Faculty/Presenter: tina kader Relationships with commercial interests: Grants/research support: BI; Sanofi Speaker s bureau/honoraria: eli lilly sanofi;
DIABETES UPATE 2016 Faculty/Presenter Disclosure Faculty/Presenter: tina kader Relationships with commercial interests: Grants/research support: BI; Sanofi Speaker s bureau/honoraria: eli lilly sanofi;
Sodium-Glucose Co-Transporter 2 (SGLT-2) Inhibitors Drug Class Prior Authorization Protocol
 Inhibitors Drug Class Prior Authorization Protocol") Sodium-Glucose Co-Transporter 2 (SGLT-2) Inhibitors Drug Class Prior Authorization Protocol Line of Business: Medicaid P&T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has
Sodium-Glucose Co-Transporter 2 (SGLT-2) Inhibitors Drug Class Prior Authorization Protocol Line of Business: Medicaid P&T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has
Oral Hypoglycemics and Risk of Adverse Cardiac Events: A Summary of the Controversy
 Oral Hypoglycemics and Risk of Adverse Cardiac Events: A Summary of the Controversy Jeffrey Boord, MD, MPH Advances in Cardiovascular Medicine Kingston, Jamaica December 7, 2012 VanderbiltHeart.com Outline
Oral Hypoglycemics and Risk of Adverse Cardiac Events: A Summary of the Controversy Jeffrey Boord, MD, MPH Advances in Cardiovascular Medicine Kingston, Jamaica December 7, 2012 VanderbiltHeart.com Outline
What s New in Diabetes Treatment. Disclosures
 What s New in Diabetes Treatment Shiri Levy M.D. Henry Ford Hospital Senior Staff Physician Service Chief, West Bloomfield Hospital Endocrinology, Metabolism, Bone and Mineral Disorders Disclosures None
What s New in Diabetes Treatment Shiri Levy M.D. Henry Ford Hospital Senior Staff Physician Service Chief, West Bloomfield Hospital Endocrinology, Metabolism, Bone and Mineral Disorders Disclosures None
What the Pill Looks Like. How it Works. Slows carbohydrate absorption. Reduces amount of sugar made by the liver. Increases release of insulin
 Diabetes s Oral s - Pills These are some of the pills that are currently available in Canada to treat diabetes. Each medication has benefits and side effects you should be aware of. Your diabetes team
Diabetes s Oral s - Pills These are some of the pills that are currently available in Canada to treat diabetes. Each medication has benefits and side effects you should be aware of. Your diabetes team
Overview T2DM medications. Winnie Ho
 Overview T2DM medications Winnie Ho Diabetes in Australia 1.7 million Australians with diabetes, of these 85% have T2DM 2-fold excess risk CV death in patients with diabetes Risk factor for progression
Overview T2DM medications Winnie Ho Diabetes in Australia 1.7 million Australians with diabetes, of these 85% have T2DM 2-fold excess risk CV death in patients with diabetes Risk factor for progression
CASES DR TINA KADER MCGILL JGH; LMC CVPH CDE
 CASES DR TINA KADER MCGILL JGH; LMC CVPH CDE Faculty/Presenter Disclosure Faculty/Presenter: tina kader Relationships with commercial interests: Grants/research support: BI; Sanofi Speaker s bureau/honoraria:
CASES DR TINA KADER MCGILL JGH; LMC CVPH CDE Faculty/Presenter Disclosure Faculty/Presenter: tina kader Relationships with commercial interests: Grants/research support: BI; Sanofi Speaker s bureau/honoraria:
TYP 2 DIABETES. Marc Donath
 TYP 2 DIABETES Marc Donath Treatment of Typ 2 Diabetes GLP-1 Anti-IL-1β Insulin sulfonylureas Metformin UCP-1 IL-1β Sport SGLT2i Bariatric surgery Cardiomyocytes Control Glucose Dyntar et al. Diabetes
TYP 2 DIABETES Marc Donath Treatment of Typ 2 Diabetes GLP-1 Anti-IL-1β Insulin sulfonylureas Metformin UCP-1 IL-1β Sport SGLT2i Bariatric surgery Cardiomyocytes Control Glucose Dyntar et al. Diabetes
Update Diabetes Therapie. Marc Y Donath
 Update Diabetes Therapie Marc Y Donath Recent CV outcome studies in Diabetes N Engl J Med. 2015 373:2117-28 (Empa-Reg outcome study) N Engl J Med. 2016 June 13 (LEADER trial) N Engl J Med. 2017 June 12
Update Diabetes Therapie Marc Y Donath Recent CV outcome studies in Diabetes N Engl J Med. 2015 373:2117-28 (Empa-Reg outcome study) N Engl J Med. 2016 June 13 (LEADER trial) N Engl J Med. 2017 June 12
What s New in Type 2 Diabetes? 2018 Diabetes Updates
 What s New in Type 2 Diabetes? 2018 Diabetes Updates Gretchen Ray, PharmD, PhC, BCACP, CDE Associate Professor, UNM College of Pharmacy January 28, 2018 gray@salud.unm.edu OBJECTIVES Describe the most
What s New in Type 2 Diabetes? 2018 Diabetes Updates Gretchen Ray, PharmD, PhC, BCACP, CDE Associate Professor, UNM College of Pharmacy January 28, 2018 gray@salud.unm.edu OBJECTIVES Describe the most
Diabete: terapia nei pazienti a rischio cardiovascolare
 Diabete: terapia nei pazienti a rischio cardiovascolare Giorgio Sesti Università Magna Graecia di Catanzaro Cardiovascular mortality in relation to diabetes mellitus and a prior MI: A Danish Population
Diabete: terapia nei pazienti a rischio cardiovascolare Giorgio Sesti Università Magna Graecia di Catanzaro Cardiovascular mortality in relation to diabetes mellitus and a prior MI: A Danish Population
Quick Reference Guide
 2018 Clinical Practice Guidelines Quick Reference Guide 416569-18 guidelines.diabetes.ca diabetes.ca 1-800-BANTING (226-8464) Screening and diagnosis of type 2 diabetes in adults Assess risk factors for
2018 Clinical Practice Guidelines Quick Reference Guide 416569-18 guidelines.diabetes.ca diabetes.ca 1-800-BANTING (226-8464) Screening and diagnosis of type 2 diabetes in adults Assess risk factors for
In-Hospital Management of Diabetes. Dr Benjamin Schiff Assistant Professor McGill University
 In-Hospital Management of Diabetes Dr Benjamin Schiff Assistant Professor McGill University No conflict of interest to declare CLINICAL SCENARIO 62 y/o male with hx of DM 2, COPD, and HT is admitted with
In-Hospital Management of Diabetes Dr Benjamin Schiff Assistant Professor McGill University No conflict of interest to declare CLINICAL SCENARIO 62 y/o male with hx of DM 2, COPD, and HT is admitted with
Cardiovascular Benefits of Two Classes of Antihyperglycemic Medications
 Cardiovascular Benefits of Two Classes of Antihyperglycemic Medications Nathan Woolever, Pharm.D., Resident Pharmacist Pharmacy Grand Rounds November 6 th, 2018 Franciscan Healthcare La Crosse, WI 2017
Cardiovascular Benefits of Two Classes of Antihyperglycemic Medications Nathan Woolever, Pharm.D., Resident Pharmacist Pharmacy Grand Rounds November 6 th, 2018 Franciscan Healthcare La Crosse, WI 2017
Update on Cardiovascular Outcome Trials in Diabetes. Rury R. Holman, FMedSci NIHR Senior Investigator 11 th February 2013
 Update on Cardiovascular Outcome Trials in Diabetes Rury R. Holman, FMedSci NIHR Senior Investigator 11 th February 2013 Residual Vascular Risk in People with Diabetes 2 Analyses based on 530,083 participants
Update on Cardiovascular Outcome Trials in Diabetes Rury R. Holman, FMedSci NIHR Senior Investigator 11 th February 2013 Residual Vascular Risk in People with Diabetes 2 Analyses based on 530,083 participants
Pharmacology Updates. Quang T Nguyen, FACP, FACE, FTOS 11/18/17
 Pharmacology Updates Quang T Nguyen, FACP, FACE, FTOS 11/18/17 14 Classes of Drugs Available for the Treatment of Type 2 DM in the USA ### Class A1c Reduction Hypoglycemia Weight Change Dosing (times/day)
Pharmacology Updates Quang T Nguyen, FACP, FACE, FTOS 11/18/17 14 Classes of Drugs Available for the Treatment of Type 2 DM in the USA ### Class A1c Reduction Hypoglycemia Weight Change Dosing (times/day)
TREATMENTS FOR TYPE 2 DIABETES. Susan Henry Diabetes Specialist Nurse
 TREATMENTS FOR TYPE 2 DIABETES Susan Henry Diabetes Specialist Nurse How can we improve outcomes in Type 2 diabetes? Earlier diagnosis Better patient education Stress central role of lifestyle management
TREATMENTS FOR TYPE 2 DIABETES Susan Henry Diabetes Specialist Nurse How can we improve outcomes in Type 2 diabetes? Earlier diagnosis Better patient education Stress central role of lifestyle management
How can we improve outcomes in Type 2 diabetes?
 How can we improve outcomes in Type 2 diabetes? Earlier diagnosis Better patient education Stress central role of lifestyle management Identify and treat all risk factors Use rational pharmacological therapy
How can we improve outcomes in Type 2 diabetes? Earlier diagnosis Better patient education Stress central role of lifestyle management Identify and treat all risk factors Use rational pharmacological therapy
Update on Therapies for Type 2 Diabetes: Angela D. Mazza, DO July 31, 2015
 Update on Therapies for Type 2 Diabetes: 2015 Angela D. Mazza, DO July 31, 2015 Objectives To present the newer available therapies for the management of T2D To discuss the advantages and disadvantages
Update on Therapies for Type 2 Diabetes: 2015 Angela D. Mazza, DO July 31, 2015 Objectives To present the newer available therapies for the management of T2D To discuss the advantages and disadvantages
Management of Diabetes
 Management of Diabetes Mellitus: Which Drugs for Which Patients? Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine baron@medicine.ucsf.edu Disclosure No relevant financial relationships
Management of Diabetes Mellitus: Which Drugs for Which Patients? Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine baron@medicine.ucsf.edu Disclosure No relevant financial relationships
What s New in Type 2 Diabetes? 2018 Diabetes Updates
 What s New in Type 2 Diabetes? 2018 Diabetes Updates Jessica Conklin, PharmD, PhC, BCACP, CDE, AAHIP Associate Professor, UNM College of Phar macy jeconklin@salud.unm.edu Luis Gonzales, PharmD, PhC UNM
What s New in Type 2 Diabetes? 2018 Diabetes Updates Jessica Conklin, PharmD, PhC, BCACP, CDE, AAHIP Associate Professor, UNM College of Phar macy jeconklin@salud.unm.edu Luis Gonzales, PharmD, PhC UNM
Diabetic Management of the Cardiac Patient
 Diabetic Management of the Cardiac Patient Dr Peter A Senior BMedSci MBBS PhD FRCP(E) Associate Professor, Director Division of Endocrinology, University of Alberta Disclosures Grants/Research Support:
Diabetic Management of the Cardiac Patient Dr Peter A Senior BMedSci MBBS PhD FRCP(E) Associate Professor, Director Division of Endocrinology, University of Alberta Disclosures Grants/Research Support:
PHARMACOLOGIC APPROACH TO ACHIEVE GLYCEMIC GOAL
 Dr Aurora Alcantara Endocrinology PHARMACOLOGIC APPROACH TO ACHIEVE GLYCEMIC GOAL SPED Convention and Diabetes Postgraduate Course May26-29 Wyndham Grand Rio Mar, PR DISCLOSURES Speaker for the following
Dr Aurora Alcantara Endocrinology PHARMACOLOGIC APPROACH TO ACHIEVE GLYCEMIC GOAL SPED Convention and Diabetes Postgraduate Course May26-29 Wyndham Grand Rio Mar, PR DISCLOSURES Speaker for the following
Navigating the New Options for the Management of Type 2 Diabetes
 Navigating the New Options for the Management of Type 2 Diabetes Clinical Associate Professor Mark Kennedy Department of General Practice, University of Melbourne Chair, Primary Care Diabetes Society of
Navigating the New Options for the Management of Type 2 Diabetes Clinical Associate Professor Mark Kennedy Department of General Practice, University of Melbourne Chair, Primary Care Diabetes Society of
TABLE 1A : Formulary Coverage of Insulin Therapies & Indications for Use in Various Populations
 177 TABLE 1A : Formulary Coverage of Insulin Therapies & Indications for Use in Various Populations Formulary Coverage Indication for use with: INSULIN THERAPY NS NB NL PE ADULTS PEDIATRICS PREGNANCY BOLUS
177 TABLE 1A : Formulary Coverage of Insulin Therapies & Indications for Use in Various Populations Formulary Coverage Indication for use with: INSULIN THERAPY NS NB NL PE ADULTS PEDIATRICS PREGNANCY BOLUS
Update on Diabetes Cardiovascular Outcome Trials
 Update on Diabetes Cardiovascular Outcome Trials Jay S. Skyler, MD, MACP Division of Endocrinology, Diabetes, and Metabolism and Diabetes Research Institute University of Miami Miller School of Medicine
Update on Diabetes Cardiovascular Outcome Trials Jay S. Skyler, MD, MACP Division of Endocrinology, Diabetes, and Metabolism and Diabetes Research Institute University of Miami Miller School of Medicine
Diabetes Management in CAD Patients. Stuart R. Chipkin, MD Research Professor School of Public Health and Health Sciences University of Massachusetts
 Diabetes Management in CAD Patients Stuart R. Chipkin, MD Research Professor School of Public Health and Health Sciences University of Massachusetts Disclosure Stuart R. Chipkin, MD, FACE Nothing to disclose
Diabetes Management in CAD Patients Stuart R. Chipkin, MD Research Professor School of Public Health and Health Sciences University of Massachusetts Disclosure Stuart R. Chipkin, MD, FACE Nothing to disclose
What s New in Diabetes Medications. Jena Torpin, PharmD
 What s New in Diabetes Medications Jena Torpin, PharmD 1 Objectives Discuss new medications in the management of diabetes Understand the mechanism of the medications discussed Understand the side effects
What s New in Diabetes Medications Jena Torpin, PharmD 1 Objectives Discuss new medications in the management of diabetes Understand the mechanism of the medications discussed Understand the side effects
6/1/2018. Lou Haenel, IV, DO, FACE, FACOI Endocrinology Roper St Francis Charleston, SC THE OMINOUS OCTET: HOW PATHOPHYSIOLOGY AND THERAPY MERGE
 Lou Haenel, IV, DO, FACE, FACOI Endocrinology Roper St Francis Charleston, SC THE OMINOUS OCTET: HOW PATHOPHYSIOLOGY AND THERAPY MERGE 1 2 3 Sulfonylureas Glipizide Glyburide Glimeperide 4 Metformin Gold
Lou Haenel, IV, DO, FACE, FACOI Endocrinology Roper St Francis Charleston, SC THE OMINOUS OCTET: HOW PATHOPHYSIOLOGY AND THERAPY MERGE 1 2 3 Sulfonylureas Glipizide Glyburide Glimeperide 4 Metformin Gold
Cardiovascular Impact of Medications for Treating Type 2 Diabetes
 Friday CME Breakfast Lecture Cardiovascular Impact of Medications for Treating Type 2 Diabetes Thomas Blevins, MD Endocrinologist, Private Practice Texas Diabetes and Endocrinology Austin, Texas Educational
Friday CME Breakfast Lecture Cardiovascular Impact of Medications for Treating Type 2 Diabetes Thomas Blevins, MD Endocrinologist, Private Practice Texas Diabetes and Endocrinology Austin, Texas Educational
TABLE 1A: Formulary Coverage of Insulin Therapies & Indications for Use in Various Populations
 177 TABLE 1A: Formulary Coverage of Insulin Therapies & Indications for Use in Various Populations TABLE 1A : Formulary Coverage of Insulin Therapies & Indications for Use in Various Populations Formulary
177 TABLE 1A: Formulary Coverage of Insulin Therapies & Indications for Use in Various Populations TABLE 1A : Formulary Coverage of Insulin Therapies & Indications for Use in Various Populations Formulary
Management of Diabetes Mellitus: A Primary Care Perspective. Screening for Diabetes Advantages of HbA1c as a Diagnostic Test
 Management of Diabetes Mellitus: A Primary Care Perspective Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest Screening
Management of Diabetes Mellitus: A Primary Care Perspective Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest Screening
Management of Type 2 Diabetes Cardiovascular Outcomes Trials Tom Blevins MD Texas Diabetes and Endocrinology Austin, Texas
 Management of Type 2 Diabetes Cardiovascular Outcomes Trials 2018 Tom Blevins MD Texas Diabetes and Endocrinology Austin, Texas Speaker Disclosure Dr. Blevins has disclosed that he has received grant support
Management of Type 2 Diabetes Cardiovascular Outcomes Trials 2018 Tom Blevins MD Texas Diabetes and Endocrinology Austin, Texas Speaker Disclosure Dr. Blevins has disclosed that he has received grant support
Management of Type 2 Diabetes Mellitus. Heather Corn, MD, MS Endocrinology, Diabetes, and Metabolism
 Management of Type 2 Diabetes Mellitus Heather Corn, MD, MS Endocrinology, Diabetes, and Metabolism Disclosures Working for Intermountain Healthcare Some of the views represented are the opinion of ABIM-certified
Management of Type 2 Diabetes Mellitus Heather Corn, MD, MS Endocrinology, Diabetes, and Metabolism Disclosures Working for Intermountain Healthcare Some of the views represented are the opinion of ABIM-certified
Objectives. Recognize all available medical treatment options for diabetes. Individualize treatment and glycemic target based on patient factors
 No disclosure Objectives Recognize all available medical treatment options for diabetes Individualize treatment and glycemic target based on patient factors Should be able to switch to more affordable
No disclosure Objectives Recognize all available medical treatment options for diabetes Individualize treatment and glycemic target based on patient factors Should be able to switch to more affordable
Learning and Earning with Gateway Professional Education CME/CEU Webinar Series. Diabetes Update July 6, :00pm 1:00pm
 Learning and Earning with Gateway Professional Education CME/CEU Webinar Series Diabetes Update July 6, 2017 12:00pm 1:00pm Jennifer Pennock Holst, MD Endocrinology, Diabetes & Metabolism AHN Center for
Learning and Earning with Gateway Professional Education CME/CEU Webinar Series Diabetes Update July 6, 2017 12:00pm 1:00pm Jennifer Pennock Holst, MD Endocrinology, Diabetes & Metabolism AHN Center for
Dept of Diabetes Main Desk
 Dept of Diabetes Main Desk 01202 448060 Glucose management in Type 2 Diabetes in Adults The natural history of type 2 diabetes is for HbA1c to deteriorate with time. A stepwise approach to treatment is
Dept of Diabetes Main Desk 01202 448060 Glucose management in Type 2 Diabetes in Adults The natural history of type 2 diabetes is for HbA1c to deteriorate with time. A stepwise approach to treatment is
Pharmacology Update for the Adult Patient - Newer Oral Medications for Diabetes
 Pharmacology Update for the Adult Patient - Newer Oral Medications for Diabetes Brooke Hudspeth, PharmD, CDE, MLDE Director of Diabetes Prevention, Kroger Pharmacy Adjunct Assistant Professor, University
Pharmacology Update for the Adult Patient - Newer Oral Medications for Diabetes Brooke Hudspeth, PharmD, CDE, MLDE Director of Diabetes Prevention, Kroger Pharmacy Adjunct Assistant Professor, University
Can We Reduce Heart Failure by Treating Diabetes? CVOT Data on SGLT2 Inhibitors and GLP-1Receptor Agonists
 Can We Reduce Heart Failure by Treating Diabetes? CVOT Data on SGLT2 Inhibitors and GLP-1Receptor Agonists Robert R. Henry, MD Professor of Medicine University of California, San Diego Relevant Conflict
Can We Reduce Heart Failure by Treating Diabetes? CVOT Data on SGLT2 Inhibitors and GLP-1Receptor Agonists Robert R. Henry, MD Professor of Medicine University of California, San Diego Relevant Conflict
Alia Gilani Health Inequalities Pharmacist
 Alia Gilani Health Inequalities Pharmacist THE SOUTH ASIAN HEALTH FOUNDATION (U.K.) (Registered Charity No. 1073178) 1. Case Study 2. Factors influencing prescribing 3. Special Considerations 4. Prescribing
Alia Gilani Health Inequalities Pharmacist THE SOUTH ASIAN HEALTH FOUNDATION (U.K.) (Registered Charity No. 1073178) 1. Case Study 2. Factors influencing prescribing 3. Special Considerations 4. Prescribing
CURRENT ISSUES IN DIABETES MANAGEMENT. Screening for Diabetes Advantages of HbA1c as a Diagnostic Test. Diagnosis of Diabetes 2013
 CURRENT ISSUES IN DIABETES MANAGEMENT Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest Screening for Diabetes 2013 BMI
CURRENT ISSUES IN DIABETES MANAGEMENT Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest Screening for Diabetes 2013 BMI
3. Cardiovascular Disease?
 Swiss recommendations 2016 Swiss Society of Endocrinology and Diabetology 1. Deficiency? Basal Premixed- Basal + GLP-1 RA (Xultophy ) or Basal Bolus 2. egfr < 30 ml/min? 3. Cardiovascular Disease? 4. Heart
Swiss recommendations 2016 Swiss Society of Endocrinology and Diabetology 1. Deficiency? Basal Premixed- Basal + GLP-1 RA (Xultophy ) or Basal Bolus 2. egfr < 30 ml/min? 3. Cardiovascular Disease? 4. Heart
Management of Diabetes Mellitus: A Primary Care Perspective
 Management of Diabetes Mellitus: A Primary Care Perspective Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest Screening
Management of Diabetes Mellitus: A Primary Care Perspective Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest Screening
Type 2 Diabetes Mellitus hypoglycaemic agents
 Type 2 Diabetes Mellitus hypoglycaemic agents Name Metformin Drug Name (eg brand name) Metformin (Diaformin Diabex) Cost / PBS per 28d mth $10.24 (1.5g dly) 1000mg+500mg / $4.44+$5.80 Concerns? Lactic
Type 2 Diabetes Mellitus hypoglycaemic agents Name Metformin Drug Name (eg brand name) Metformin (Diaformin Diabex) Cost / PBS per 28d mth $10.24 (1.5g dly) 1000mg+500mg / $4.44+$5.80 Concerns? Lactic
IMPROVED DIAGNOSIS OF TYPE 2 DIABETES AND TAILORING MEDICATIONS
 IMPROVED DIAGNOSIS OF TYPE 2 DIABETES AND TAILORING MEDICATIONS Dr Bidhu Mohapatra, MBBS, MD, FRACP Consultant Physician Endocrinology and General Medicine Introduction 382 million people affected by diabetes
IMPROVED DIAGNOSIS OF TYPE 2 DIABETES AND TAILORING MEDICATIONS Dr Bidhu Mohapatra, MBBS, MD, FRACP Consultant Physician Endocrinology and General Medicine Introduction 382 million people affected by diabetes
Newer Diabetes Treatments Drug Class Update with New Drug Evaluation: Semaglutide and Ertugliflozin
 Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35 Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35 Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
DM Fundamentals Class 4 Meds for Type 2
 DM Fundamentals Class 4 Meds for Type 2 Beverly Thomassian, RN, MPH, BC ADM, CDE President, Diabetes Education Services Copyright 1999 2015, Diabetes Education Services, All Rights Reserved. Diabetes Meds
DM Fundamentals Class 4 Meds for Type 2 Beverly Thomassian, RN, MPH, BC ADM, CDE President, Diabetes Education Services Copyright 1999 2015, Diabetes Education Services, All Rights Reserved. Diabetes Meds
No Increased Cardiovascular Risk for Lixisenatide in ELIXA
 ON ISSUES IN THE MANAGEMENT OF TYPE 2 DIABETES JUNE 2015 Coverage of data from ADA 2015, June 5 9 in Boston, Massachusetts No Increased Cardiovascular Risk for Lixisenatide in ELIXA First Cardiovascular
ON ISSUES IN THE MANAGEMENT OF TYPE 2 DIABETES JUNE 2015 Coverage of data from ADA 2015, June 5 9 in Boston, Massachusetts No Increased Cardiovascular Risk for Lixisenatide in ELIXA First Cardiovascular
Dipeptidyl-Peptidase 4 (DPP-4) Inhibitors Drug Class Prior Authorization Protocol
 Inhibitors Drug Class Prior Authorization Protocol") Dipeptidyl-Peptidase 4 (DPP-4) Inhibitors Drug Class Prior Authorization Protocol Line of Business: Medicaid P&T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has been developed
Dipeptidyl-Peptidase 4 (DPP-4) Inhibitors Drug Class Prior Authorization Protocol Line of Business: Medicaid P&T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has been developed
Disclosure. Learning Objectives. Case. Diabetes Update: Incretin Agents in Diabetes-When to Use Them? I have no disclosures to declare
 Disclosure Diabetes Update: Incretin Agents in Diabetes-When to Use Them? I have no disclosures to declare Spring Therapeutics Update 2011 CSHP BC Branch Anar Dossa BScPharm Pharm D CDE April 20, 2011
Disclosure Diabetes Update: Incretin Agents in Diabetes-When to Use Them? I have no disclosures to declare Spring Therapeutics Update 2011 CSHP BC Branch Anar Dossa BScPharm Pharm D CDE April 20, 2011
Type 2 Diabetes Management: Case 1: Reducing Hypoglycemic Risk Case 2: Reducing Cardiovascular Risk
 Type 2 Diabetes Management M. Susan Burke, MD, FACP Clinical Associate Professor of Medicine Sidney Kimmel Medical College at Thomas Jefferson University Senior Advisor, Lankenau Medical Associates Lankenau
Type 2 Diabetes Management M. Susan Burke, MD, FACP Clinical Associate Professor of Medicine Sidney Kimmel Medical College at Thomas Jefferson University Senior Advisor, Lankenau Medical Associates Lankenau
Preventing Serious Health Consequences of Type 2 Diabetes
 Preventing Serious Health Consequences of Type 2 Diabetes The Evidence Hertzel C. Gerstein MD MSc FRCPC Professor and Population Health Institute Chair in Diabetes Research McMaster University and Hamilton
Preventing Serious Health Consequences of Type 2 Diabetes The Evidence Hertzel C. Gerstein MD MSc FRCPC Professor and Population Health Institute Chair in Diabetes Research McMaster University and Hamilton
Case Studies in Type 2 Diabetes Mellitus: Focus on Cardiovascular Outcomes Trials
 Case Studies in Type 2 Diabetes Mellitus: Focus on Cardiovascular Outcomes Trials Louis Kuritzky MD Clinical Assistant Professor Emeritus Department of Community Health and Family Medicine College of Medicine
Case Studies in Type 2 Diabetes Mellitus: Focus on Cardiovascular Outcomes Trials Louis Kuritzky MD Clinical Assistant Professor Emeritus Department of Community Health and Family Medicine College of Medicine
Newer Therapies for Type 2 Diabetes
 Newer Therapies for Type 2 Diabetes Sandra Indacochea Sobel, MD Clinical Assistant Professor of Medicine Clinical Chief of Endocrinology, UPMC Mercy Division of Endocrinology, Diabetes, and Metabolism
Newer Therapies for Type 2 Diabetes Sandra Indacochea Sobel, MD Clinical Assistant Professor of Medicine Clinical Chief of Endocrinology, UPMC Mercy Division of Endocrinology, Diabetes, and Metabolism
Drug Class Review Newer Diabetes Medications and Combinations
 Drug Class Review Newer Diabetes Medications and Combinations Final Update 2 Report July 2016 The purpose reports is to make available information regarding the comparative clinical effectiveness and harms
Drug Class Review Newer Diabetes Medications and Combinations Final Update 2 Report July 2016 The purpose reports is to make available information regarding the comparative clinical effectiveness and harms
The Many Faces of T2DM in Long-term Care Facilities
 The Many Faces of T2DM in Long-term Care Facilities Question #1 Which of the following is a risk factor for increased hypoglycemia in older patients that may suggest the need to relax hyperglycemia treatment
The Many Faces of T2DM in Long-term Care Facilities Question #1 Which of the following is a risk factor for increased hypoglycemia in older patients that may suggest the need to relax hyperglycemia treatment
01/09/2017. Outline. SGLT 2 inhibitor? Diabetes Patients: Complex and Heterogeneous. Association between diabetes and cardiovascular events
 MICROVASCULAR COMPLICATIONS Incidence of outcome g 1 Cardioprotective Effects of SGLT2s Relevant for Which T2 Diabetes Patient? SGLT 2 inhibitor? 58 year old, waist circumference 5 cm, PMH: IHD On statin,
MICROVASCULAR COMPLICATIONS Incidence of outcome g 1 Cardioprotective Effects of SGLT2s Relevant for Which T2 Diabetes Patient? SGLT 2 inhibitor? 58 year old, waist circumference 5 cm, PMH: IHD On statin,
YOU HAVE DIABETES. Angie O Connor Community Diabetes Nurse Specialist 25th September 2013
 YOU HAVE DIABETES Angie O Connor Community Diabetes Nurse Specialist 25th September 2013 Predicated 2015 figures are already met 1 in 20 have diabetes:1in8 over 60years old Definite Diagnosis is key Early
YOU HAVE DIABETES Angie O Connor Community Diabetes Nurse Specialist 25th September 2013 Predicated 2015 figures are already met 1 in 20 have diabetes:1in8 over 60years old Definite Diagnosis is key Early
CANVAS Program Independent commentary
 CANVAS Program Independent commentary Cliff Bailey Aston University, Birmingham, UK 2017 Disclosures and disclaimers Clifford J Bailey CJB has attended advisory boards, undertaken ad hoc consultancy, received
CANVAS Program Independent commentary Cliff Bailey Aston University, Birmingham, UK 2017 Disclosures and disclaimers Clifford J Bailey CJB has attended advisory boards, undertaken ad hoc consultancy, received
Content Development Committee
 1 Content Development Committee Cardiologists: Family Physicians: Shaun Goodman, MD, MSc, FRCPC, FACC, FESC, FAHA, FCCS (Chair) Associate Head, Division of Cardiology, St. Michael s Hospital Professor,
1 Content Development Committee Cardiologists: Family Physicians: Shaun Goodman, MD, MSc, FRCPC, FACC, FESC, FAHA, FCCS (Chair) Associate Head, Division of Cardiology, St. Michael s Hospital Professor,
Disclosures. Objectives. Bryan Cardiology Conference DM2 & Cardiovascular Outcome Trials 8/28/2017
 Bryan Cardiology Conference DM2 & Cardiovascular Outcome Trials Shannon Wakeley MD Complete Endocrinology 9/2/2017 Disclosures Speakers Bureau: Astra Zeneca, Sanofi, Abbvie, Boehringer-Ingelheim, Medtronic,
Bryan Cardiology Conference DM2 & Cardiovascular Outcome Trials Shannon Wakeley MD Complete Endocrinology 9/2/2017 Disclosures Speakers Bureau: Astra Zeneca, Sanofi, Abbvie, Boehringer-Ingelheim, Medtronic,
Stephen Clement M.D. CDE Medical Director, Endocrine Services Inova Fairfax Hospital
 Stephen Clement M.D. CDE Medical Director, Endocrine Services Inova Fairfax Hospital Financial Disclosures Consulting Panel for GSK on Hepatitis Vaccines Case Study BH is a 67 y/o female with T2 DM for
Stephen Clement M.D. CDE Medical Director, Endocrine Services Inova Fairfax Hospital Financial Disclosures Consulting Panel for GSK on Hepatitis Vaccines Case Study BH is a 67 y/o female with T2 DM for
Drug Class Monograph
 Drug Class Monograph Class: Sodium-Glucose Co-Transporter 2 (SGLT-2) Inhibitors Drugs: Farxiga (dapagliflozin), Invokamet (canagliflozin/metformin), Invokana (canagliflozin), Jardiance (empagliflozin),
Drug Class Monograph Class: Sodium-Glucose Co-Transporter 2 (SGLT-2) Inhibitors Drugs: Farxiga (dapagliflozin), Invokamet (canagliflozin/metformin), Invokana (canagliflozin), Jardiance (empagliflozin),
Vascular complications
 Vascular complications December 8, 2018 Faculty Disclosure Faculty: Kim Connelly, MBBS, PhD, FRACP Associate Professor of Medicine, University of Toronto Cardiologist, St. Michael s Hospital Relationships
Vascular complications December 8, 2018 Faculty Disclosure Faculty: Kim Connelly, MBBS, PhD, FRACP Associate Professor of Medicine, University of Toronto Cardiologist, St. Michael s Hospital Relationships
Top HF Trials to Impact Your Practice
 Top HF Trials to Impact Your Practice Biykem Bozkurt, MD, FACC The Mary and Gordon Cain Chair & Professor of Medicine Medical Care Line Executive, DeBakey VA Medical Center, Director, Winters Center for
Top HF Trials to Impact Your Practice Biykem Bozkurt, MD, FACC The Mary and Gordon Cain Chair & Professor of Medicine Medical Care Line Executive, DeBakey VA Medical Center, Director, Winters Center for
Type 2 diabetes & Cardiovascular disease. update. Barcelona, March 15th 2018
 Type 2 diabetes & Cardiovascular disease update Barcelona, March 15th 2018 Francesc Xavier Cos Claramunt Sant Martí de Provençals. Head of Innovation and Health in Barcelona city Assoc.ProfUniversitatAutonomade
Type 2 diabetes & Cardiovascular disease update Barcelona, March 15th 2018 Francesc Xavier Cos Claramunt Sant Martí de Provençals. Head of Innovation and Health in Barcelona city Assoc.ProfUniversitatAutonomade
Canadian Diabetes Association 2013 Clinical Practice Guidelines
 Canadian Diabetes Association 2013 Clinical Practice Guidelines The Essentials (Updated d November 2016) 2016 1 Faculty/Presenter Disclosure Faculty: Alan Bell MD CCFP Relationships with commercial and
Canadian Diabetes Association 2013 Clinical Practice Guidelines The Essentials (Updated d November 2016) 2016 1 Faculty/Presenter Disclosure Faculty: Alan Bell MD CCFP Relationships with commercial and
Medical therapy advances London/Manchester RCP February/June 2016
 Medical therapy advances London/Manchester RCP February/June 2016 Advances in medical therapies for diabetes mellitus Duality of interest: The speaker or institutions with which he is associated has received
Medical therapy advances London/Manchester RCP February/June 2016 Advances in medical therapies for diabetes mellitus Duality of interest: The speaker or institutions with which he is associated has received
DM Fundamentals Class 4 Meds for Type 2
 DM Fundamentals Class 4 Meds for Type 2 Beverly Thomassian, RN, MPH, BC ADM, CDE President, Diabetes Education Services Copyright 1999 2015, Diabetes Education Services, All Rights Reserved. Diabetes Meds
DM Fundamentals Class 4 Meds for Type 2 Beverly Thomassian, RN, MPH, BC ADM, CDE President, Diabetes Education Services Copyright 1999 2015, Diabetes Education Services, All Rights Reserved. Diabetes Meds
Type 2 Diabetes Mellitus 2011
 2011 Michael T. McDermott MD Director, Endocrinology and Diabetes Practice University of Colorado Hospital Michael.mcdermott@ucdenver.edu Diabetes Mellitus Diagnosis 2011 Diabetes Mellitus Fasting Glucose
2011 Michael T. McDermott MD Director, Endocrinology and Diabetes Practice University of Colorado Hospital Michael.mcdermott@ucdenver.edu Diabetes Mellitus Diagnosis 2011 Diabetes Mellitus Fasting Glucose
NEW DIABETES CARE MEDICATIONS
 NEW DIABETES CARE MEDICATIONS James Bonucchi DO, ECNU, FACE Adult Medicine and Endocrinology Specialists Disclosures Speakers bureau Sanofi AZ BI Diabetes Diabetes cost ADA 2017 data Ever increasing disorder.
NEW DIABETES CARE MEDICATIONS James Bonucchi DO, ECNU, FACE Adult Medicine and Endocrinology Specialists Disclosures Speakers bureau Sanofi AZ BI Diabetes Diabetes cost ADA 2017 data Ever increasing disorder.
Antihyperglycemic Agents in Diabetes. Jamie Messenger, PharmD, CPP Department of Family Medicine East Carolina University August 18, 2014
 Antihyperglycemic Agents in Diabetes Jamie Messenger, PharmD, CPP Department of Family Medicine East Carolina University August 18, 2014 Objectives Review 2014 ADA Standards of Medical Care in DM as they
Antihyperglycemic Agents in Diabetes Jamie Messenger, PharmD, CPP Department of Family Medicine East Carolina University August 18, 2014 Objectives Review 2014 ADA Standards of Medical Care in DM as they
Help the Heart. An Update on GLP-1 Agonists and SGLT2 Inhibitors. Tara Hawley, PharmD PGY1 Pharmacy Resident Mayo Clinic Health System Eau Claire
 Help the Heart An Update on GLP-1 Agonists and SGLT2 Inhibitors Tara Hawley, PharmD PGY1 Pharmacy Resident Mayo Clinic Health System Eau Claire Mayo Clinic Grand Rounds May 16, 2017 2017 MFMER slide-1
Help the Heart An Update on GLP-1 Agonists and SGLT2 Inhibitors Tara Hawley, PharmD PGY1 Pharmacy Resident Mayo Clinic Health System Eau Claire Mayo Clinic Grand Rounds May 16, 2017 2017 MFMER slide-1
Cardiovascular Outcomes With Newer Diabetes Drugs: Results From The EMPA-REG and LEADER Trials
 Cardiovascular Outcomes With Newer Diabetes Drugs: Results From The EMPA-REG and LEADER Trials Rajiv Roy, MD Endocrinology Sharp Rees-Stealy Medical Group Background Between 1990 and 2010: Incidence of
Cardiovascular Outcomes With Newer Diabetes Drugs: Results From The EMPA-REG and LEADER Trials Rajiv Roy, MD Endocrinology Sharp Rees-Stealy Medical Group Background Between 1990 and 2010: Incidence of
Drug Class Update with New Drug Evaluation: Non-insulin Diabetes Treatments (SGLT-2 Inhibitors and GLP-1 Receptor Agonists)
") Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35 Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35 Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
4/9/2018 HOW TO REGULATE DIABETES MEDICATIONS. By Sarah Froemsdorf MSN, RNC, CDE, FNP DISCLOSURES NONE. Diagnosis
 HOW TO REGULATE DIABETES MEDICATIONS By Sarah Froemsdorf MSN, RNC, CDE, FNP DISCLOSURES NONE Diagnosis 1 NORMAL BODY The normal pancreas releases one unit of insulin every hour all day. The normal pancreas
HOW TO REGULATE DIABETES MEDICATIONS By Sarah Froemsdorf MSN, RNC, CDE, FNP DISCLOSURES NONE Diagnosis 1 NORMAL BODY The normal pancreas releases one unit of insulin every hour all day. The normal pancreas
Diabetes Oral Agents Pharmacology. University of Hawai i Hilo Pre-Nursing Program NURS 203 General Pharmacology Danita Narciso Pharm D
 Diabetes Oral Agents Pharmacology University of Hawai i Hilo Pre-Nursing Program NURS 203 General Pharmacology Danita Narciso Pharm D 1 Learning Objectives Understand the role of the utilization of free
Diabetes Oral Agents Pharmacology University of Hawai i Hilo Pre-Nursing Program NURS 203 General Pharmacology Danita Narciso Pharm D 1 Learning Objectives Understand the role of the utilization of free
Glucagon-like peptide-1 (GLP-1) Agonists Drug Class Prior Authorization Protocol
 Agonists Drug Class Prior Authorization Protocol") Glucagon-like peptide-1 (GLP-1) Agonists Drug Class Prior Authorization Protocol Line of Business: Medicaid P&T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has been developed
Glucagon-like peptide-1 (GLP-1) Agonists Drug Class Prior Authorization Protocol Line of Business: Medicaid P&T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has been developed
Class Update: Sodium-glucose Cotransporter 2 (SGLT2) Inhibitors
 Inhibitors") Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35 Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35 Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
RPCC Pharmacy Forum. The Type 2 Diabetes Issue. Type 2 Diabetes: The Basics
 Nov/Dec 2015 Issue 11 RPCC Pharmacy Forum Special Interest Articles: Diabetes Medication Chart Insulin Chart Afreeza Did you know? Exanatide, marketed as Byetta, is the synthetic form of exendin-4, which
Nov/Dec 2015 Issue 11 RPCC Pharmacy Forum Special Interest Articles: Diabetes Medication Chart Insulin Chart Afreeza Did you know? Exanatide, marketed as Byetta, is the synthetic form of exendin-4, which
Updates in Diabetes Care
 Updates in Diabetes Care Disclosures Nothing to disclose Pharmacist Objectives 1. List strategies for improving diabetes care 2. Understand benefits and risks associated with newer pharmacotherapeutic
Updates in Diabetes Care Disclosures Nothing to disclose Pharmacist Objectives 1. List strategies for improving diabetes care 2. Understand benefits and risks associated with newer pharmacotherapeutic
Treatment Options for Diabetes: An Update
 Treatment Options for Diabetes: An Update A/Prof. Marg McGill Manager, Diabetes Centre Dr. Ted Wu Staff Specialist Endocrinologist Diabetes Centre Centre of Health Professional Education Education Provider
Treatment Options for Diabetes: An Update A/Prof. Marg McGill Manager, Diabetes Centre Dr. Ted Wu Staff Specialist Endocrinologist Diabetes Centre Centre of Health Professional Education Education Provider
Date of Review: September 2016 Date of Last Review: September 2015
 Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35 Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35 Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Diabetes Mellitus: Implications of New Clinical Trials and New Medications
 Diabetes Mellitus: Implications of New Clinical Trials and New Medications Estimates of Diagnosed Diabetes in Adults, 2005 Alka M. Kanaya, MD Asst. Professor of Medicine UCSF, Primary Care CME October
Diabetes Mellitus: Implications of New Clinical Trials and New Medications Estimates of Diagnosed Diabetes in Adults, 2005 Alka M. Kanaya, MD Asst. Professor of Medicine UCSF, Primary Care CME October
Glucose Control drug treatments
 Glucose Control drug treatments It should be noted that glitazones are under suspicion of precipitating acute cardiac events and current recommendations contraindicate the use of glitazones in patients
Glucose Control drug treatments It should be noted that glitazones are under suspicion of precipitating acute cardiac events and current recommendations contraindicate the use of glitazones in patients