Initiating Injectables in Type 2 Diabetes. Tara Kadis Team Leader Diabetes Nurse Specialist York Teaching Hospital
|
|
|
- Martina Snow
- 5 years ago
- Views:
Transcription

1 Initiating Injectables in Type 2 Diabetes Tara Kadis Team Leader Diabetes Nurse Specialist York Teaching Hospital

2 Increasing levels in delivery of diabetes care Complex Care support People with diabetes under 25 years of age 3.2 Initial management of type 1 diabetes 3.3 Unstable glucose control 3.4 Complex diabetes 3.5 Type 1 diabetes on complex insulin regimes; insulin pumps and complex MDI 3.6 Pregnancy 3.7 Pre-conception counselling in high risk people 3.8 Advanced renal disease 3.9 Advanced diabetic foot disease 3.10 Advanced neuropathy/autonomic neuropathy 3.11 Delivery of Type 1 structured education Referral: criteria based Community Diabetes Team support Support for people with suboptimal 2.7 Management of early glucose control neuropathy and nephropathy 2.2 Severe or recurrent minor 2.8 Diabetes and obesity when hypoglycaemia insulin being considered 2.3 Insulin/GLP1 initiation and 2.9 Nursing and residential home intensification liaison and support 2.4 Pre-pregnancy counselling 2.5 Assessment for Type 1 structured education 2.6 Delivery of Type 2 structured education Discharge: criteria based Primary Care management of diabetic patients Involvement in the prevention of Type 2 diabetes (NICE PH38) 1.2 Early detection of those at high risk 1.3 Diagnosis and categorisation of diabetes 1.4 Initial management of Type 2 diabetes 1.5 On-going management of people aged 25 and over with stable Type 1 and Type 2 diabetes 1.6 Annual complications screening and care planning 1.7 Retinal screening referral 1.8 Insulin / GLP1 initiation (if accredited) 1.9 Recognition and management of early diabetic complications 1.10 Identification and appropriate referral of diabetic emergencies 1.11 Blood glucose monitoring advice and guidance 1.12 Dietary and lifestyle advice 1.13 Managing diabetes and intercurrent illness
3 Diabetes is a progressive multi-system disease characterised by: Declining beta-cell function Insulin resistance increasing body weight Increased risk of cardiovascular disease
4 As diabetes treatments are added to improve glucose control, clinicians & patients face trade-offs such as: Hypoglycaemia Weight gain Complex treatment regimens
5 Weight gain and hypoglycaemia associated with traditional therapies Delay in progressing with medication Patients see themselves as failures due to progression of therapies
6 An Aid to Decision Making in Type 2 Diabetes
 Once weekly dulaglutide (Trulicity)")
7 GLP-1 Lixisenatide (Lyxumia) Liraglutide (Victoza) Exenatide (Byetta) Once weekly exenatide (Bydureon) Once weekly dulaglutide (Trulicity) Insulin


8 GLP-1 secreted upon the ingestion of food 5.Brain: promotes satiety and reduces appetite 4,5 2.α-cell: suppresses postprandial glucagon secretion cell: enhances glucosedependent insulin secretion in the pancreas 1 3.Liver: reduces hepatic glucose output 2 4.Stomach: slows the rate of gastric emptying 3 Adapted from 1 Nauck MA, et al. Diabetologia 1993;36: ; 2 Larsson H, et al. Acta Physiol Scand 1997;160: ; 3 Nauck MA, et al. Diabetologia 1996;39: ; 4 Flint A, et al. J Clin Invest 1998;101: ; 5 Zander et al. Lancet 2002;359:
 BMI >35.0kg/m² BMI< 35.")

9 Consider adding GLP-1 2 nd or 3 rd line if patient HbA1C 58mmol/mol (7.5%) BMI >35.0kg/m² BMI< 35.0kg/m² where insulin is unacceptable because of occupational implications or weight loss would benefit other significant obesity related co mobidities
10 Only continue GLP-1 therapy if the person has had a beneficial metabolic response a reduction of at least 1.0% (11mmol/mol) in HbA1c & weight loss of at least 3% of initial body weight at 6 months.

11 Lixisenatide Once daily injection, before breakfast 10mcgs for 2 weeks then 20mcgs thereafter 1 st choice GLP-1 Add on to insulin
 Inject at any time, independent of mealtimes (preferably same time each day) Start with 0.6mgs for 1 week increasing to 1.")
12 Prefilled, disposable pen for s.c. injection Contains 18 mg liraglutide in 3 ml 0.6 mg selected 1.2 mg selected 1.8 mg selected Once-daily s.c. injection Select dose (0.6, 1.2 or 1.8 mg) Inject at any time, independent of mealtimes (preferably same time each day) Start with 0.6mgs for 1 week increasing to 1.2 mgs thereafter Licence with basal insulin Victoza Summary of Product Characteristics

13 Bydureon Once weekly 2mgs once weekly Now in a disposable device No licence with insulin
14 Not recommended in severe renal impairment egfr <30 Pregnancy/breast feeding Type 1 Diabetes Pancreatitis Risk of hypoglycaemia in combination with sulphonylurea
15 Management of potential side effects Hypoglycaemia management? Blood glucose monitoring? Injection technique/ safe use of sharps Expectations of therapy, know when to stop
16 Considerations / barriers Weight loss Minimal titration Less considerations re driving/employment Side effects Contra Indications NICE recommendations for continuation Follow- up

17 What's next?

18 Xultophy 1mL solution = 100 units Degludec mgs Liraglutide
19 Insulin
20 When to initiate insulin. If other measures fail to keep desired HbA1c <58 mmol/mol (7.5%) Max dose of tolerated treatment usually triple therapy Consider in dual therapy when significant hyperglycaemia in preference to adding further drug to control blood glucose unless true justification not to. OHA not tolerated/contra-indicated Symptoms related to poor glycaemic control Other medication causing temporary raise in blood glucose levels. The aim of the treatment is to improve glycaemic control and quality of life.
21 Before insulin therapy Reinforce dietary advice and discuss lifestyle issues and employment i.e. smoking and physical activity Check ability to administer own insulin / carers district nurse involvement Patients should be taught home blood glucose monitoring - advise to monitor blood glucose at different times.
22 Structured programme Structured education Continuing telephone support Frequent self monitoring Dose titration to target Dietary understanding Management of hypoglycaemia Management of acute changes in glucose control
23 Which? Basal Insulin with oral hypoglycaemic agents Pre-mixed insulin with oral hypoglycaemic agents Basal Bolus Regime consider referral to Community diabetes Team to initiate this regime First line choice Overweight BMI >26 Reluctance to start insulin Unable to inject themselves HbA1c > 75 mmol/mol (9%) Regular lifestyles Symptomatic Carbohydrate consistency On daily/bd insulin regimes without optimal control Requiring flexibility due to an erratic lifestyle Shift work Regular travel across time zones Regular sport To optimise blood glucose control because of complications
24 Common options for intensifying basal insulin regimens Basal insulin Switch to twice-daily premixed insulin Intensify with an additional injection Add three times daily prandial insulin with meals (basal-bolus) Add once-daily prandial insulin with the largest meal (basal-plus) Additional prandial injections can be added Adapted from Barnett A et al (2008) Int J Clin Pract 62:
25 Basal Human Insulin NPH first line choice (NICE) Starting with a dose usually before bed Titrate in line with fasting blood glucose levels Continue with OHA to help control day time blood glucose levels May be given twice daily if blood glucose levels indicate it Associated with less weight gain and hypos
26 Basal Human Insulin Humulin I Insulatard Insuman Basal
27 Getting started Commence once daily basal insulin in the evening - 10 units start dose Continue Metformin if tolerated Consider continuing sulfonylureas Teach the patient to titrate insulin dose by 2-4 units every 3-5 days Aim for fasting blood glucose of 5 8 mmol/l
28 What are the choices? Humulin I Kwikpen Insulatard Innolet 3ml Cartridges ( Savvio Pen) 3ml Cartridges ( Novopen 4) Insuman Basal Solostar pen 3ml Cartridges (Clikstar pen)
29 Basal Analogue Lantus or Levemir Consider: If person needs assistance from a carer or healthcare professional to inject insulin and therefore reduce the frequency of injections Hypoglycaemia is a problem with NPH
30 What are the choices? Lantus Solostar 3ml Cartridges (Clikstar pen) Levemir Flexpen Innolet 3ml Cartridge ( Novopen 4)
31 Human Basal V Basal Analogue Basal Human insulin Basal analogue

32 Example algorithm for titrating human basal insulin from a randomised controlled trial Exceptions to algorithm: 1. No increase in dose if fasting plasma glucose 4 mmol/l is documented at any time in the preceding week 2. Small insulin dose decreases (2-4 unit/day per adjustment) are allowed if severe hypoglycaemia (requiring assistance) or a fasting plasma glucose of 3.1 mmol/l is documented in the preceding week Yki-Jarvinen H et al (2006) Diabetologia 49:
33 Titration guidelines Fasting blood Glucose Action mmol/l >10 Increase by 4 units 8 10 Increase by 2 units 5-7 No change 3-5 Reduce by 2 units <3 Reduce by 4 units
34 Patient 1 Breakfast Lunch Tea Bed year old man, HbA1c 71 mmol/mol, BMI 28 Lives with wife, usually quite well but symptomatic Metformin 1g BD Gliclazide 160mgs BD Sitagliptin 100mgs OD

35 An Aid to Decision Making in Type 2 Diabetes
36 Patient 1 Commence once daily Isophane insulin Humulin I Kwikpen 10 units at bed time Stop Sitagliptin Continue on Gliclazide Titrate basal dose on fasting blood glucose levels, aiming for fasting 5-7 mmols.
37 Twice Daily Biphasic Human insulin Consider if HbA1c 75mmol/mol (9%) If unable to achieve control on basal insulin Regular lifestyle Increased risk of weight gain / hypoglycaemia than with basal insulin NICE recommend Human Mixtures



38 BD Pre Mixed Human Insulin Breakfast Lunch Evening Meal Sleep
39 What are the choices? Humulin M3 Kwikpens (disposable device) 3ml cartridge Insuman comb 15 / 25 / 50 3ml cartridge Solostar pen (disposable device) 25 mix only
40 Getting started In insulin naive patients usually start with: 12 units am & 8 units pm or 16 units am & 12 units pm in very overweight patients If switching from once daily basal insulin: Consider reducing dose by 10-20% 2/3rds am 1/3 evening Need to be injected mins pre meal Continue with metformin Continue the sulfonylurea initially, but review and discontinue if hypoglycaemia occurs.
41 When to consider an analogue mix? Analogue mixtures provide a quicker onset of action and offer some advantage in people with post-prandial (after-meal) rises. May also help prevent hypoglycaemia in between meals due to shorter action of rapid insulin Injection timing an issue
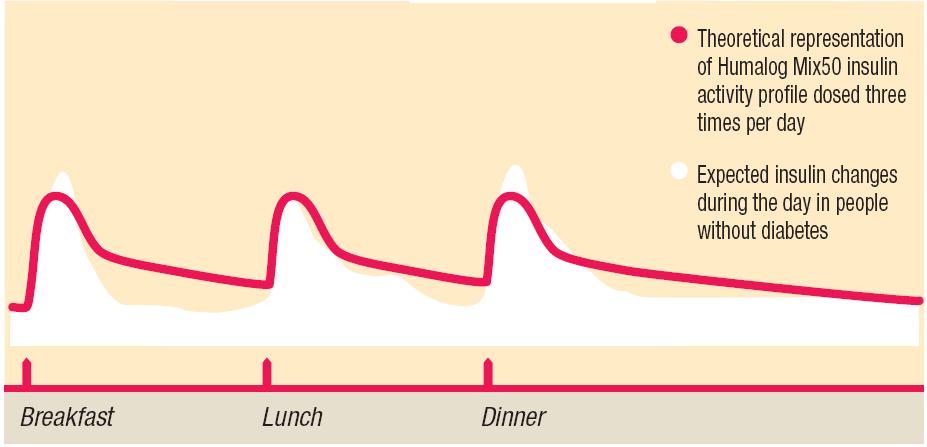
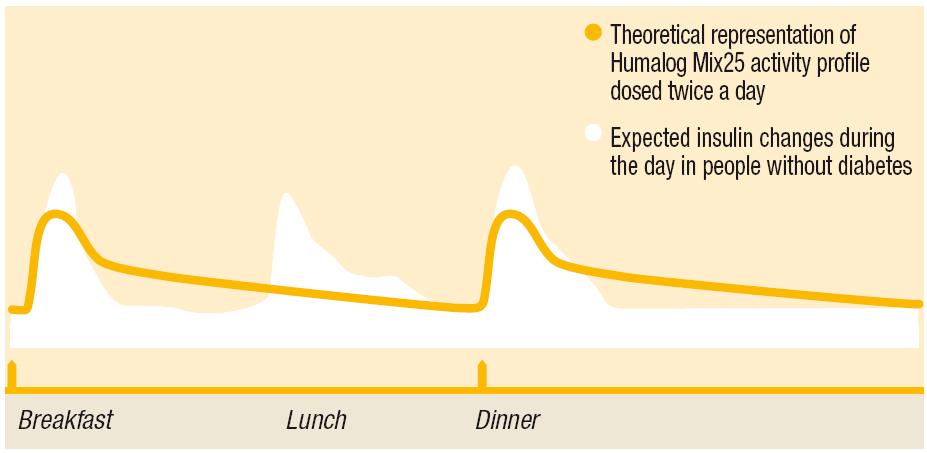
42 Insulin Analogue Mixtures Inject twice daily, within 0 to 15 minutes before or after meals. Useful in rapid post prandial rise as works quicker Humalog Mix25, Mix50 Novomix 30
43 What are the choices? Humalog Mix 25, 50 Kwik pen 3ml cartdriges ( Savvio pen) Novomix 30 Flexpen 3ml Cartridges (Novopen 4)
44 Patient 2 63 year old lady, able to give own insulin Humulin I 40 units before bed Metformin 1g BD Gliclazide 160mg BD Breakfast Lunch Tea Bed
45 Example 2 FBG satisfactory Main problem is elevation of levels during the day Review HbA1c, Consider adding a dose of Humulin I with breakfast and titrate inline with blood glucose levels during the day usually start with 10 units may need to reduce bed time dose Switch to BD Mixed insulin stop SU Reduce dose by 10% 2/3 AM, 1/3 Pm
46 TDS Insulin Mixtures Humalog mix 50 or Novomix 30 generally ones of choice Higher amount of rapid acting insulin per dose Ideal for those with a high CHO intake with meals Generally given 3 times a day with meals Don t usually use human mixed insulin due to the concerns re stacking of insulin and increased risk of hypoglycaemia
47
48 Basal plus Addition of prandial rapid acting insulin to basal insulin (Humulin I, Insuman basal, Insulatard) Give rapid dose with main meal or highest post meal blood glucose level Stepwise approach leading to injection with each meal Usual starting dose 6 units NovoRapid / Humalog / Apidra Continue on basal insulin
49 Patient 3 50 year old lady Humulin M3-36 units AM 24 units PM Metformin 1g BD Breakfast Lunch Tea Bed
50 Patient 3 Elevated levels before evening meal Review diet Consider giving TDS mix 30 / 50 so lunch is covered with the quick acting component.
51 What else do we need to know? Blood glucose monitoring Hypoglycaemia management Illness management / sick day rules Injection rotation Driving Identification / insulin passport INSULIN TITRATION guidelines.

52 Blood glucose testing - Individual assessment based on Number of injections Occupation / driving Treatment Consider post meal in patients who you suspect of post prandial hyperglycaemia. Meter standardisation in Type 2 diabetes Who to test, when to test

53 Treatment of hypoglycaemia Blood glucose below 4 mmol/l 4-5 glucotabs 100mls lucozade 3-4 jelly babies 1x mini can of coca cola. RECOVERY MINS Longer acting Carbohydrate 1 portion fruit / 2 plain biscuits / 1 slice of bread.
54 Sick day rules. Don t stop insulin Blood glucose mmol/l = 2 units extra Blood glucose mmol/l = 4 units extra Blood glucose more than 22 mmol/l 6 units extra (if on over 50 units a day double the adjustments) Increase blood glucose monitoring usually every 4 hours Drink fluids 100mL/hour prevent dehydration Managing diabetes during intercurrent illness in the community February 2013 NHS Diabetes

55 Travel Carrying insulin / frio packs Travel letter Time zones Foot care Identification Insurance

56 Needle size 4 or 5 mm needle length of choice x
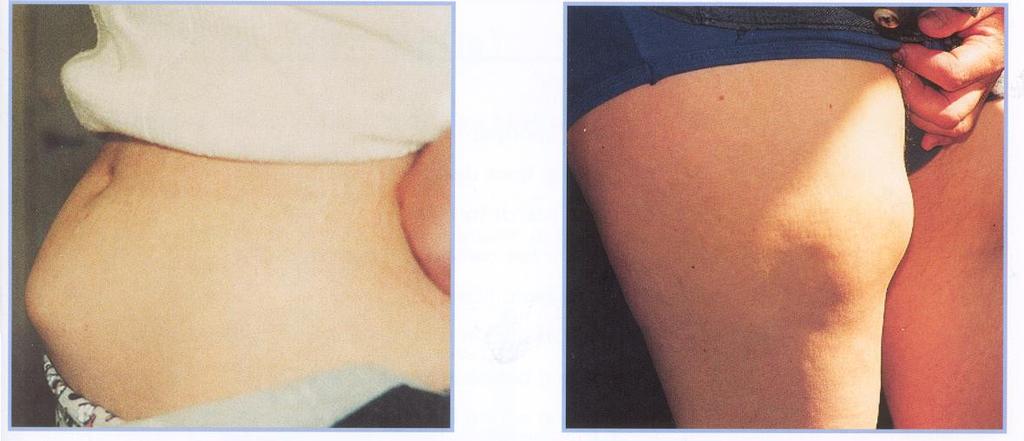
57 Lipohypertrophy
58 DVLA requirements Specific to insulin treated patients with group 1 entitlement Must have awareness of hypoglycaemia Must not have had more than one episode of hypoglycaemia requiring assistance of another person in the preceding 12 months There must be appropriate blood glucose monitoring Must not be regarded as a likely source of danger to the public while driving The visual standards for acuity and visual field must be met.
59 What to include in the annual review! Understanding of: Hypoglycaemia status and management Sick day rules Check for lipos Injection technique are they reusing needles! Sharps removal When to seek help and by whom Dietary update Driving status and DVLA recommendations ID How to titrate doses
60 Titration guidelines Fasting blood Glucose Action mmol/l >10 Increase by 4 units 8 10 Increase by 2 units 5-7 No change 3-5 Reduce by 2 units <3 Reduce by 4 units
61 Summary Consider human basal and human mixed insulin initially Analogue basal and analogue mixed insulin to be considered only when clinically indicated Take care with people taking animal insulins they are most probably on these for a reason!!! Analogues are routinely used in the management of type 1 diabetes.
62 And finally! Stepwise approach to insulin regimes Newer therapies should be considered first especially if weight / hypoglycaemia risk is an issue No one insulin regime fits all Intensification necessary in majority of patients Individual assessment on most appropriate regimen is required
63 Cost comparison based on prefilled disposable pens x5 Lilly Novo Nordisk Sanofi Aventis Basal Humulin I Insulatard Levemir Degludec Insuman Basal Lantus Biphasic Humulin M Humalog Mix 25 / Novomix Insuman Comb

64 Insulin regimens for type 2 diabetes compared Frequent blood glucose monitoring
Injectable Therapies in Diabetes
 Injectable Therapies in Diabetes Diabetes Specialist Nurse Linda Burns Learning Outcomes Understand the place of injectible therapies in diabetes Understand when patients may require insulin therapy Consider
Injectable Therapies in Diabetes Diabetes Specialist Nurse Linda Burns Learning Outcomes Understand the place of injectible therapies in diabetes Understand when patients may require insulin therapy Consider
Injectable Therapies in Diabetes
 Injectable Therapies in Diabetes Diabetes Specialist Nurse Joyce Robson Learning Outcomes Think about the place of injectible therapies in diabetes Insulin therapy GLP1 antagonists Consider commonly used
Injectable Therapies in Diabetes Diabetes Specialist Nurse Joyce Robson Learning Outcomes Think about the place of injectible therapies in diabetes Insulin therapy GLP1 antagonists Consider commonly used
Injectable Therapies in Diabetes
 Injectable Therapies in Diabetes Diabetes Specialist Nurse Joyce Robson Learning Outcomes Think about the place of injectible therapies in diabetes Think about when / why patients require insulin therapy
Injectable Therapies in Diabetes Diabetes Specialist Nurse Joyce Robson Learning Outcomes Think about the place of injectible therapies in diabetes Think about when / why patients require insulin therapy
Insulin Management. By Susan Henry Diabetes Specialist Nurse
 Insulin Management By Susan Henry Diabetes Specialist Nurse The Discovery of Insulin - 1921 - Banting & Best University Of Toronto Discovered hormone insulin in pancreatic extract of dog - Marjorie the
Insulin Management By Susan Henry Diabetes Specialist Nurse The Discovery of Insulin - 1921 - Banting & Best University Of Toronto Discovered hormone insulin in pancreatic extract of dog - Marjorie the
TYPE 2 DIABETES CRITERIA FOR REFERRAL TO LEVEL 2 OOHS
 TYPE 2 DIABETES CRITERIA FOR REFERRAL TO LEVEL 2 OOHS The aim of the Diabetes level 2 service is to provide a high quality service for safe initiation and optimization of injectable therapy within GP networks.
TYPE 2 DIABETES CRITERIA FOR REFERRAL TO LEVEL 2 OOHS The aim of the Diabetes level 2 service is to provide a high quality service for safe initiation and optimization of injectable therapy within GP networks.
TREATMENTS FOR TYPE 2 DIABETES. Susan Henry Diabetes Specialist Nurse
 TREATMENTS FOR TYPE 2 DIABETES Susan Henry Diabetes Specialist Nurse How can we improve outcomes in Type 2 diabetes? Earlier diagnosis Better patient education Stress central role of lifestyle management
TREATMENTS FOR TYPE 2 DIABETES Susan Henry Diabetes Specialist Nurse How can we improve outcomes in Type 2 diabetes? Earlier diagnosis Better patient education Stress central role of lifestyle management
Information for Patients
 Information for Patients Guidance for Diabetic Persons having an OGD or Bronchoscopy This guidance is provided to assist with your preparation for your endoscopic procedure. If you feel unclear about how
Information for Patients Guidance for Diabetic Persons having an OGD or Bronchoscopy This guidance is provided to assist with your preparation for your endoscopic procedure. If you feel unclear about how
Short-acting insulins. Biphasic insulins. Intermediate- and long-acting insulins
 Recommended Insulin Products This guideline states the Gloucestershire Joint Formulary recommended, first choice insulin products. The intention is to support the choice of treatment for new patients,
Recommended Insulin Products This guideline states the Gloucestershire Joint Formulary recommended, first choice insulin products. The intention is to support the choice of treatment for new patients,
How they work and when to take them. Diabetes Medications
 How they work and when to take them Diabetes Medications BIGUANIDES Metformin Actions Slows down the release of glucose from the liver. Helps the bodies cells become more sensitive to insulin. Pros Weight
How they work and when to take them Diabetes Medications BIGUANIDES Metformin Actions Slows down the release of glucose from the liver. Helps the bodies cells become more sensitive to insulin. Pros Weight
INJECTABLE THERAPY FOR THE TREATMENT OF DIABETES
 INJECTABLE THERAPY FOR THE TREATMENT OF DIABETES ARSHNA SANGHRAJKA DIABETES SPECIALIST PRESCRIBING PHARMACIST OBJECTIVES EXPLORE THE TYPES OF INSULIN AND INJECTABLE DIABETES TREATMENTS AND DEVICES AVAILABLE
INJECTABLE THERAPY FOR THE TREATMENT OF DIABETES ARSHNA SANGHRAJKA DIABETES SPECIALIST PRESCRIBING PHARMACIST OBJECTIVES EXPLORE THE TYPES OF INSULIN AND INJECTABLE DIABETES TREATMENTS AND DEVICES AVAILABLE
GLP-1 agonists. Ian Gallen Consultant Community Diabetologist Royal Berkshire Hospital Reading UK
 GLP-1 agonists Ian Gallen Consultant Community Diabetologist Royal Berkshire Hospital Reading UK What do GLP-1 agonists do? Physiology of postprandial glucose regulation Meal ❶ ❷ Insulin Rising plasma
GLP-1 agonists Ian Gallen Consultant Community Diabetologist Royal Berkshire Hospital Reading UK What do GLP-1 agonists do? Physiology of postprandial glucose regulation Meal ❶ ❷ Insulin Rising plasma
The principles of insulin adjustment guidance
 The principles of insulin adjustment guidance Tips for insulin titration Blood glucose (BG) monitoring is needed to help identify the efficacy of treatment in diabetes. Monitor blood glucose according
The principles of insulin adjustment guidance Tips for insulin titration Blood glucose (BG) monitoring is needed to help identify the efficacy of treatment in diabetes. Monitor blood glucose according
There have been important changes in diabetes care which may not be covered in undergraduate textbooks.
 Diabetes Clinical update There have been important changes in diabetes care which may not be covered in undergraduate textbooks. Changes in the diagnosis of diabetes a) HbA1C Since 2011, World Health Organisation
Diabetes Clinical update There have been important changes in diabetes care which may not be covered in undergraduate textbooks. Changes in the diagnosis of diabetes a) HbA1C Since 2011, World Health Organisation
Dept of Diabetes Main Desk
 Dept of Diabetes Main Desk 01202 448060 Glucose management in Type 2 Diabetes in Adults The natural history of type 2 diabetes is for HbA1c to deteriorate with time. A stepwise approach to treatment is
Dept of Diabetes Main Desk 01202 448060 Glucose management in Type 2 Diabetes in Adults The natural history of type 2 diabetes is for HbA1c to deteriorate with time. A stepwise approach to treatment is
DIABETES INDICATIONS FOR INSULIN
 DIABETES INDICATIONS FOR INSULIN 1 Introduce the likely need for insulin in the future early on as part of patient education Emphasise that it is the pancreas that fails not the patient Assess if greater
DIABETES INDICATIONS FOR INSULIN 1 Introduce the likely need for insulin in the future early on as part of patient education Emphasise that it is the pancreas that fails not the patient Assess if greater
How can we improve outcomes in Type 2 diabetes?
 How can we improve outcomes in Type 2 diabetes? Earlier diagnosis Better patient education Stress central role of lifestyle management Identify and treat all risk factors Use rational pharmacological therapy
How can we improve outcomes in Type 2 diabetes? Earlier diagnosis Better patient education Stress central role of lifestyle management Identify and treat all risk factors Use rational pharmacological therapy
Guideline for antihyperglycaemic therapy in adults with type 2 diabetes
 Guideline for antihyperglycaemic therapy in adults with type 2 diabetes Version Control Version Number Date Amendments made 1 January 2018 1.1 February 2018 Amended to reflect updated SPC advice for sitagliptin
Guideline for antihyperglycaemic therapy in adults with type 2 diabetes Version Control Version Number Date Amendments made 1 January 2018 1.1 February 2018 Amended to reflect updated SPC advice for sitagliptin
End of Life Diabetes Care
 End of Life Diabetes Care Commissioned by Diabetes UK Supplementary Documents and Flowcharts Endorsed By: Diabetes Phases of End of Life and Medications A - Blue: All From Diagnosis Stable With Year Plus
End of Life Diabetes Care Commissioned by Diabetes UK Supplementary Documents and Flowcharts Endorsed By: Diabetes Phases of End of Life and Medications A - Blue: All From Diagnosis Stable With Year Plus
Management of Type 2 Diabetes
 Management of Type 2 Diabetes Pathophysiology Insulin resistance and relative insulin deficiency/ defective secretion Not immune mediated No evidence of β cell destruction Increased risk with age, obesity
Management of Type 2 Diabetes Pathophysiology Insulin resistance and relative insulin deficiency/ defective secretion Not immune mediated No evidence of β cell destruction Increased risk with age, obesity
MANAGEMENT OF TYPE 2 DIABETES
 MANAGEMENT OF TYPE 2 DIABETES 3 Month trial of lifestyle changes. Refer to DESMOND structured education programme. Set glycaemic target HbA1c < 7.0% (53mmol/mol) or individualised If HbA1c > 53mmol/mol
MANAGEMENT OF TYPE 2 DIABETES 3 Month trial of lifestyle changes. Refer to DESMOND structured education programme. Set glycaemic target HbA1c < 7.0% (53mmol/mol) or individualised If HbA1c > 53mmol/mol
Diabetes, Type 2 Management
 CLINICAL GUIDELINE Diabetes, Type 2 Management A guideline is intended to assist healthcare professionals in the choice of disease-specific treatments. Clinical judgement should be exercised on the applicability
CLINICAL GUIDELINE Diabetes, Type 2 Management A guideline is intended to assist healthcare professionals in the choice of disease-specific treatments. Clinical judgement should be exercised on the applicability
667FM.5.1 MANAGEMENT OF TYPE 2 DIABETES: BLOOD-GLUCOSE-LOWERING THERAPY
 667FM.5.1 MANAGEMENT OF TYPE 2 DIABETES: BLOOD-GLUCOSE-LOWERING THERAPY Contents Introduction... 1 Patient Education for People with Type 2 Diabetes... 2 Dietary Advice for People with Type 2 Diabetes...
667FM.5.1 MANAGEMENT OF TYPE 2 DIABETES: BLOOD-GLUCOSE-LOWERING THERAPY Contents Introduction... 1 Patient Education for People with Type 2 Diabetes... 2 Dietary Advice for People with Type 2 Diabetes...
the person is intolerant of either metformin or a sulphonylurea, or treatment with metformin or a sulphonylurea is contraindicated, and
 Exenatide (Byetta) and Liraglutide (Victoza) prescribing guidance: Notes for initiation in primary care These incretin mimetics are given by subcutaneous injection once or twice daily. They have similar
Exenatide (Byetta) and Liraglutide (Victoza) prescribing guidance: Notes for initiation in primary care These incretin mimetics are given by subcutaneous injection once or twice daily. They have similar
Insulin Therapies: An Educational Toolkit
 University Hospitals of Leicester, Department of Diabetes and Leicester Diabetes Centre: Insulin Therapies: An Educational Toolkit This document is designed for use by those trained and competent in insulin
University Hospitals of Leicester, Department of Diabetes and Leicester Diabetes Centre: Insulin Therapies: An Educational Toolkit This document is designed for use by those trained and competent in insulin
Drugs used in Diabetes. Dr Andrew Smith
 Drugs used in Diabetes Dr Andrew Smith Plan Introduction Insulin Sensitising Drugs: Metformin Glitazones Insulin Secretagogues: Sulphonylureas Meglitinides Others: Acarbose Incretins Amylin Analogues Damaglifozin
Drugs used in Diabetes Dr Andrew Smith Plan Introduction Insulin Sensitising Drugs: Metformin Glitazones Insulin Secretagogues: Sulphonylureas Meglitinides Others: Acarbose Incretins Amylin Analogues Damaglifozin
Guidance on the Self-Monitoring of Blood Glucose in Adults with Diabetes
 Introduction Guidance on the Self-Monitoring of Blood Glucose in Adults with Diabetes This guideline is designed to offer guidance for primary and secondary care on the use of selfmonitoring of blood glucose
Introduction Guidance on the Self-Monitoring of Blood Glucose in Adults with Diabetes This guideline is designed to offer guidance for primary and secondary care on the use of selfmonitoring of blood glucose
New Treatments for Type 2 diabetes. Nandini Seevaratnam April 2016 Rushcliffe Patient Forum
 New Treatments for Type 2 diabetes Nandini Seevaratnam April 2016 Rushcliffe Patient Forum Overview Growing population of Type 2 diabetes Basic science on what goes wrong Current treatments Why there is
New Treatments for Type 2 diabetes Nandini Seevaratnam April 2016 Rushcliffe Patient Forum Overview Growing population of Type 2 diabetes Basic science on what goes wrong Current treatments Why there is
GLP-1 Receptor Agonists and SGLT-2 Inhibitors. Debbie Hicks
 GLP-1 Receptor Agonists and SGLT-2 Inhibitors Debbie Hicks Prescribing and Adverse Event reporting information is available at this meeting from the AstraZeneca representative The views expressed by the
GLP-1 Receptor Agonists and SGLT-2 Inhibitors Debbie Hicks Prescribing and Adverse Event reporting information is available at this meeting from the AstraZeneca representative The views expressed by the
KEEPING SAFE WITH INSULIN THERAPY
 KEEPING SAFE WITH INSULIN THERAPY kk WHY IS THIS LEAFLET FOR YOU? Insulin treatment improves the quality of life in many people and saves the lives of others. It is used to lower blood glucose levels.
KEEPING SAFE WITH INSULIN THERAPY kk WHY IS THIS LEAFLET FOR YOU? Insulin treatment improves the quality of life in many people and saves the lives of others. It is used to lower blood glucose levels.
New Medicine Assessment
 New Medicine Assessment Insulin degludec plus liraglutide (Xultophy ) 100 units/ml insulin degludec plus 3.6 mg/ml liraglutide solution for injection in a pre-filled pen Treatment of adults with type 2
New Medicine Assessment Insulin degludec plus liraglutide (Xultophy ) 100 units/ml insulin degludec plus 3.6 mg/ml liraglutide solution for injection in a pre-filled pen Treatment of adults with type 2
Updated August /08/2020
 Title of Guideline (must include the word Guideline (not protocol, policy, procedure etc) Contact Name and Job Title (author) Directorate & Speciality Guideline for the management of adults with diabetes
Title of Guideline (must include the word Guideline (not protocol, policy, procedure etc) Contact Name and Job Title (author) Directorate & Speciality Guideline for the management of adults with diabetes
Hypoglyceamia and Exercise
 Hypoglyceamia and Exercise Noreen Barker Diabetes Specialist Nurse May 2016 Hypoglyceamia What is a hypo? Why are we concerned? Signs and symptoms Treatments Causes Hypo unawareness Managing diabetes and
Hypoglyceamia and Exercise Noreen Barker Diabetes Specialist Nurse May 2016 Hypoglyceamia What is a hypo? Why are we concerned? Signs and symptoms Treatments Causes Hypo unawareness Managing diabetes and
EXENATIDE (BYETTA ) PROTOCOL, 5mcg and 10mcg SC injection pre-filled pens
 PROTOCOL, 5mcg and 10mcg SC injection pre-filled pens") EXENATIDE (BYETTA ) PROTOCOL, 5mcg and 10mcg SC injection pre-filled pens This document should be read in conjunction with the current Summary of Product Characteristics http://www.medicines.org.uk 1.
EXENATIDE (BYETTA ) PROTOCOL, 5mcg and 10mcg SC injection pre-filled pens This document should be read in conjunction with the current Summary of Product Characteristics http://www.medicines.org.uk 1.
Leicestershire Diabetes Guidelines: Insulin Therapy
 Endorsed by Leicestershire Medicines Strategy Group Leicestershire Diabetes Guidelines: Insulin Therapy These guidelines are designed for use by those trained and competent in insulin initiation and management
Endorsed by Leicestershire Medicines Strategy Group Leicestershire Diabetes Guidelines: Insulin Therapy These guidelines are designed for use by those trained and competent in insulin initiation and management
BEDFORDSHIRE AND LUTON JOINT PRESCRIBING COMMITTEE (JPC)
") BEDFORDSHIRE AND LUTON JOINT PRESCRIBING COMMITTEE (JPC) Overarching Shared Care Guideline for Glucagon-like peptide 1 (GLP 1) agonists, February 2017. PATIENT S NAME: PATIENT S ADDRESS: HOSPITAL NAME
BEDFORDSHIRE AND LUTON JOINT PRESCRIBING COMMITTEE (JPC) Overarching Shared Care Guideline for Glucagon-like peptide 1 (GLP 1) agonists, February 2017. PATIENT S NAME: PATIENT S ADDRESS: HOSPITAL NAME
Insulin for Adults with Type 2 Diabetes
 rth Central London Joint Formulary Committee Insulin for Adults with Type 2 Diabetes Disclaimer This guideline is registered at rth Central London (NCL) Joint Formulary Committee (JFC) and is intended
rth Central London Joint Formulary Committee Insulin for Adults with Type 2 Diabetes Disclaimer This guideline is registered at rth Central London (NCL) Joint Formulary Committee (JFC) and is intended
When and how to start insulin therapy in type 2 diabetes
 When and how to start insulin therapy in type 2 diabetes Anne Kilvert MD, FRCP Most patients with type 2 diabetes will eventually require insulin due to the progressive decline in betacell function. Dr
When and how to start insulin therapy in type 2 diabetes Anne Kilvert MD, FRCP Most patients with type 2 diabetes will eventually require insulin due to the progressive decline in betacell function. Dr
The York Diabetes Care Model
 This Session The York Diabetes Care Model The annual review what s it for and how to do it How to make the diagnosis of diabetes and who to test Categorisation of diabetes at diagnosis Basics of Insulin
This Session The York Diabetes Care Model The annual review what s it for and how to do it How to make the diagnosis of diabetes and who to test Categorisation of diabetes at diagnosis Basics of Insulin
RDNS. Injection Therapy in injection therapy in diabetes. Type 2 Diabetes
 RDNS Injection Therapy in injection therapy in diabetes Type 2 Diabetes Australian Diabetes Society (ADS) HbA1c targets for T2DM Specific Clinical Situations HbA1c General 7% Diabetes of short duration
RDNS Injection Therapy in injection therapy in diabetes Type 2 Diabetes Australian Diabetes Society (ADS) HbA1c targets for T2DM Specific Clinical Situations HbA1c General 7% Diabetes of short duration
INJECTABLE THERAPIES IN DIABETES. Barbara Ann McKee Diabetes Specialist Nurse
 INJECTABLE THERAPIES IN DIABETES Barbara Ann McKee Diabetes Specialist Nurse 1 Aims of the session Describe the different injectable agents for diabetes and when they would be used. Describe some common
INJECTABLE THERAPIES IN DIABETES Barbara Ann McKee Diabetes Specialist Nurse 1 Aims of the session Describe the different injectable agents for diabetes and when they would be used. Describe some common
Insulin Initiation and Intensification. Disclosure. Objectives
 Insulin Initiation and Intensification Neil Skolnik, M.D. Associate Director Family Medicine Residency Program Abington Memorial Hospital Professor of Family and Community Medicine Temple University School
Insulin Initiation and Intensification Neil Skolnik, M.D. Associate Director Family Medicine Residency Program Abington Memorial Hospital Professor of Family and Community Medicine Temple University School
EFFECTIVE SHARE CARE AGREEMENT. FOR THE off license use of GLP1 mimetics in combination with insulin IN DUDLEY
 Specialist details Patient identifier Name Tel: EFFECTIVE SHARE CARE AGREEMENT FOR THE off license use of GLP1 mimetics in combination with insulin IN DUDLEY The aim of Effective Shared Care Guidelines
Specialist details Patient identifier Name Tel: EFFECTIVE SHARE CARE AGREEMENT FOR THE off license use of GLP1 mimetics in combination with insulin IN DUDLEY The aim of Effective Shared Care Guidelines
Managing your diabetes: Travel Advice
 Managing your diabetes: Travel Advice Information for patients, relatives and carers For more information, please contact: Your diabetes team on telephone number 01904 726510 The York Hospital Wigginton
Managing your diabetes: Travel Advice Information for patients, relatives and carers For more information, please contact: Your diabetes team on telephone number 01904 726510 The York Hospital Wigginton
BEST 4 Diabetes. Optimisation of insulin module
 BEST 4 Diabetes Optimisation of insulin module Confidence and competence Where would you rate yourself? Why do all of our patient not achieve optimal blood glucose control? Insulin Therapy Goals and Purpose
BEST 4 Diabetes Optimisation of insulin module Confidence and competence Where would you rate yourself? Why do all of our patient not achieve optimal blood glucose control? Insulin Therapy Goals and Purpose
The first stop for professional medicines advice
 London Medicines Evaluation Network Overview: Glucagon-Like Peptide-1 receptor analogues The first stop for professional medicines advice 1 London Medicines Evaluation Network Overview: Glucagon-Like Peptide-1
London Medicines Evaluation Network Overview: Glucagon-Like Peptide-1 receptor analogues The first stop for professional medicines advice 1 London Medicines Evaluation Network Overview: Glucagon-Like Peptide-1
BEST 4 Diabetes. Optimisation of insulin module
 BEST 4 Diabetes Optimisation of insulin module Confidence and competence Where would you rate yourself? Why do all of our patient not achieve optimal blood glucose control? Insulin Therapy Goals and Purpose
BEST 4 Diabetes Optimisation of insulin module Confidence and competence Where would you rate yourself? Why do all of our patient not achieve optimal blood glucose control? Insulin Therapy Goals and Purpose
Glucose Control drug treatments
 Glucose Control drug treatments It should be noted that glitazones are under suspicion of precipitating acute cardiac events and current recommendations contraindicate the use of glitazones in patients
Glucose Control drug treatments It should be noted that glitazones are under suspicion of precipitating acute cardiac events and current recommendations contraindicate the use of glitazones in patients
Professor Rudy Bilous James Cook University Hospital
 Professor Rudy Bilous James Cook University Hospital Rate per 100 patient years Rate per 100 patient years 16 Risk of retinopathy progression 16 Risk of developing microalbuminuria 12 12 8 8 4 0 0 5 6
Professor Rudy Bilous James Cook University Hospital Rate per 100 patient years Rate per 100 patient years 16 Risk of retinopathy progression 16 Risk of developing microalbuminuria 12 12 8 8 4 0 0 5 6
Insulin Initiation, titration & Insulin switch in the Primary Care-KISS
 Insulin Initiation, titration & Insulin switch in the Primary Care-KISS Rotorua GP CME 9 June 2012 Dr Kingsley Nirmalaraj FRACP Endocrinologist, BOPDHB & Suite 9, Promed House, Tenth Ave, Tauranga Linda
Insulin Initiation, titration & Insulin switch in the Primary Care-KISS Rotorua GP CME 9 June 2012 Dr Kingsley Nirmalaraj FRACP Endocrinologist, BOPDHB & Suite 9, Promed House, Tenth Ave, Tauranga Linda
Monitoring in Type 2 Diabetes. Learning Outcomes. Type 2 Diabetes. Senga Hunter Community Diabetes Specialist Nurse
 Monitoring in Type 2 Diabetes Senga Hunter Community Diabetes Specialist Nurse Learning Outcomes Understand why blood monitoring is necessary Understand the blood tests for monitoring diabetes Understand
Monitoring in Type 2 Diabetes Senga Hunter Community Diabetes Specialist Nurse Learning Outcomes Understand why blood monitoring is necessary Understand the blood tests for monitoring diabetes Understand
Fasted and Consented but Blood Glucose 18mmol/L or How to Manage Diabetes in the Peri-Operative Period
 Fasted and Consented but Blood Glucose 18mmol/L or How to Manage Diabetes in the Peri-Operative Period Dr Ketan Dhatariya MBBS MSc MD MS FRCP Consultant in Diabetes and Endocrinology Norfolk and Norwich
Fasted and Consented but Blood Glucose 18mmol/L or How to Manage Diabetes in the Peri-Operative Period Dr Ketan Dhatariya MBBS MSc MD MS FRCP Consultant in Diabetes and Endocrinology Norfolk and Norwich
Starting Insulin in General Practice
 Starting Insulin in General Practice Timothy Kenealy GP & Assoc Prof of Integrated Care, University of Auckland Auckland DHB / my version + Counties DHB version Starting Insulin surprisingly simple, safe
Starting Insulin in General Practice Timothy Kenealy GP & Assoc Prof of Integrated Care, University of Auckland Auckland DHB / my version + Counties DHB version Starting Insulin surprisingly simple, safe
Pharmacological Glycaemic Control in Type 2 Diabetes
 Pharmacological Glycaemic Control in Type 2 Diabetes Aim(s) and Objective(s) This guideline aims to offer advice on the pharmacological management for those who require measures beyond diet and exercise
Pharmacological Glycaemic Control in Type 2 Diabetes Aim(s) and Objective(s) This guideline aims to offer advice on the pharmacological management for those who require measures beyond diet and exercise
PERIOPERATIVE DIABETES GUIDELINE
 PERIOPERATIVE DIABETES GUIDELINE This Guideline does not replace the need for the application of clinical judgment in respect to each individual patient. Background Diabetes mellitus is estimated to affect
PERIOPERATIVE DIABETES GUIDELINE This Guideline does not replace the need for the application of clinical judgment in respect to each individual patient. Background Diabetes mellitus is estimated to affect
Initiating Injectable Therapy in Type 2 Diabetes
 Initiating Injectable Therapy in Type 2 Diabetes David Doriguzzi, PA C Learning Objectives To understand current Diabetes treatment guidelines To understand how injectable medications fit into current
Initiating Injectable Therapy in Type 2 Diabetes David Doriguzzi, PA C Learning Objectives To understand current Diabetes treatment guidelines To understand how injectable medications fit into current
STEP 3: Add or Substitute with one of
 Prescribing of Hypoglycaemic Agents for Adult Patients with Type 2 Diabetes: Sunderland Refer to DESMOND Structured Education classes to promote Increased Physical Activity, Weight Loss and Calories Reduction
Prescribing of Hypoglycaemic Agents for Adult Patients with Type 2 Diabetes: Sunderland Refer to DESMOND Structured Education classes to promote Increased Physical Activity, Weight Loss and Calories Reduction
Diabetes Head to Toe May 31, 2017
 Innovations in Insulin Joanne Reid RN CDE jmreid@gbhs.on.ca Danielle Benedict RPh Outline Setting the stage Insulin as pancreas replacement therapy Commonly used insulins New insulins Case Studies Dosing
Innovations in Insulin Joanne Reid RN CDE jmreid@gbhs.on.ca Danielle Benedict RPh Outline Setting the stage Insulin as pancreas replacement therapy Commonly used insulins New insulins Case Studies Dosing
Diabetes in the UK: Update on Diabetes Treatment and Care. Why is diabetes increasing? Obesity Increased waist circumference.
 Update on Diabetes Treatment and Care Tahseen A Chowdhury Consultant Diabetologist Royal London and Mile End Hospitals Diabetes prevalence (thousands) Diabetes in the UK: 1995-21 3 25 2 15 1 5 Type 1 Type
Update on Diabetes Treatment and Care Tahseen A Chowdhury Consultant Diabetologist Royal London and Mile End Hospitals Diabetes prevalence (thousands) Diabetes in the UK: 1995-21 3 25 2 15 1 5 Type 1 Type
INSULIN INITIATION AND INTENSIFICATION WITH A FOCUS ON HYPOGLYCEMIA REDUCTION
 INSULIN INITIATION AND INTENSIFICATION WITH A FOCUS ON HYPOGLYCEMIA REDUCTION Jaiwant Rangi, MD, FACE Nov 10 th 2018 DISCLOSURES Speaker Novo Nordisk Sanofi-Aventis Boheringer Ingleheim Merck Abbvie Abbott
INSULIN INITIATION AND INTENSIFICATION WITH A FOCUS ON HYPOGLYCEMIA REDUCTION Jaiwant Rangi, MD, FACE Nov 10 th 2018 DISCLOSURES Speaker Novo Nordisk Sanofi-Aventis Boheringer Ingleheim Merck Abbvie Abbott
THIS IS A PATIENT HAND HELD DOCUMENT CARE PATHWAY FOR MANAGEMENT OF INITIATION OF INSULIN
 Worcestershire Trusts Please attach patient sticker here or record: GP Name: Consultant:. Ward: THIS IS A PATIENT HAND HELD DOCUMENT CARE PATHWAY FOR MANAGEMENT OF INITIATION OF INSULIN This Care Pathway
Worcestershire Trusts Please attach patient sticker here or record: GP Name: Consultant:. Ward: THIS IS A PATIENT HAND HELD DOCUMENT CARE PATHWAY FOR MANAGEMENT OF INITIATION OF INSULIN This Care Pathway
BEDFORDSHIRE AND LUTON JOINT PRESCRIBING COMMITTEE (JPC) Bulletin Glucagon-like peptide 1 (GLP-1) receptor agonist review
 Bulletin Glucagon-like peptide 1 (GLP-1) receptor agonist review") BEDFORDSHIRE AND LUTON JOINT PRESCRIBING COMMITTEE (JPC) February 2017 Review February 2020 Bulletin 245 - Glucagon-like peptide 1 (GLP-1) receptor agonist review JPC Recommendations:- Place in therapy
BEDFORDSHIRE AND LUTON JOINT PRESCRIBING COMMITTEE (JPC) February 2017 Review February 2020 Bulletin 245 - Glucagon-like peptide 1 (GLP-1) receptor agonist review JPC Recommendations:- Place in therapy
Guidance on the Self-Monitoring of Blood Glucose in Adults with Diabetes
 Introduction Guidance on the Self-Monitoring of Blood Glucose in Adults with Diabetes This guideline is designed to offer guidance for primary and secondary care on the use of selfmonitoring of blood glucose
Introduction Guidance on the Self-Monitoring of Blood Glucose in Adults with Diabetes This guideline is designed to offer guidance for primary and secondary care on the use of selfmonitoring of blood glucose
Arrange 3 Monthly Review Re-enforce LIFESTYLE advice and check DRUG COMPLIANCE at each visit Target HbA1c < 53mmol/mol
 Prescribing of Hypoglycaemic Agents for Adult Patients with Type 2 Diabetes: Sunderland Refer to DESMOND Structured Education classes to promote Increased Physical Activity, Weight Loss and Calories Reduction
Prescribing of Hypoglycaemic Agents for Adult Patients with Type 2 Diabetes: Sunderland Refer to DESMOND Structured Education classes to promote Increased Physical Activity, Weight Loss and Calories Reduction
Mr Rab Burtun. Dr David Kim. 8:30-10:30 WS #2: Diabetes Basic 11:00-13:00 WS #9: Diabetes Basic (Repeated)
") Dr David Kim Endocrinologist and General Physician Waitemata DHB and Apollo Specialist Clinic Albany Auckland Mr Rab Burtun Diabetes Nurse Specialist Waitemata DHB Waitakere Hospital Auckland 8:30-10:30
Dr David Kim Endocrinologist and General Physician Waitemata DHB and Apollo Specialist Clinic Albany Auckland Mr Rab Burtun Diabetes Nurse Specialist Waitemata DHB Waitakere Hospital Auckland 8:30-10:30
Peri-operative management of the surgical patient with diabetes GL059
 DT Peri-operative management of the surgical patient with diabetes GL059 Approval Approval Group Job Title, Chair of Committee Date Anaesthetics Clinical Governance Chair Anaesthetic governance Nov 2016
DT Peri-operative management of the surgical patient with diabetes GL059 Approval Approval Group Job Title, Chair of Committee Date Anaesthetics Clinical Governance Chair Anaesthetic governance Nov 2016
Glucagon-like peptide-1 (GLP-1) Agonists Drug Class Prior Authorization Protocol
 Agonists Drug Class Prior Authorization Protocol") Glucagon-like peptide-1 (GLP-1) Agonists Drug Class Prior Authorization Protocol Line of Business: Medicaid P&T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has been developed
Glucagon-like peptide-1 (GLP-1) Agonists Drug Class Prior Authorization Protocol Line of Business: Medicaid P&T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has been developed
Clinical Guidelines. Management of adult patients with diabetes undergoing endoscopic procedures
 Clinical Guidelines Management of adult patients with diabetes undergoing endoscopic s Document Detail Document type Clinical Guideline Management of adult Patients with diabetes Undergoing Document name
Clinical Guidelines Management of adult patients with diabetes undergoing endoscopic s Document Detail Document type Clinical Guideline Management of adult Patients with diabetes Undergoing Document name
Tips and Tricks for Starting and Adjusting Insulin. MC MacSween The Moncton Hospital
 Tips and Tricks for Starting and Adjusting Insulin MC MacSween The Moncton Hospital Progression of type 2 diabetes Beta cell apoptosis Natural History of Type 2 Diabetes The Burden of Treatment Failure
Tips and Tricks for Starting and Adjusting Insulin MC MacSween The Moncton Hospital Progression of type 2 diabetes Beta cell apoptosis Natural History of Type 2 Diabetes The Burden of Treatment Failure
What the Pill Looks Like. How it Works. Slows carbohydrate absorption. Reduces amount of sugar made by the liver. Increases release of insulin
 Diabetes s Oral s - Pills These are some of the pills that are currently available in Canada to treat diabetes. Each medication has benefits and side effects you should be aware of. Your diabetes team
Diabetes s Oral s - Pills These are some of the pills that are currently available in Canada to treat diabetes. Each medication has benefits and side effects you should be aware of. Your diabetes team
Selecting GLP-1 RA Treatment
 Selecting GLP-1 RA Treatment Dr Felicity Kaplan March 2017 Objectives Review the progressive nature of type 2 diabetes Understand the need for timely treatment intensification Examine the place of GLP-1
Selecting GLP-1 RA Treatment Dr Felicity Kaplan March 2017 Objectives Review the progressive nature of type 2 diabetes Understand the need for timely treatment intensification Examine the place of GLP-1
INSULIN 101: When, How and What
 INSULIN 101: When, How and What Alice YY Cheng @AliceYYCheng Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form
INSULIN 101: When, How and What Alice YY Cheng @AliceYYCheng Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form
Diabetes Update: Keeping patients safe. Victoria Ruszala MFRPSII North Bristol NHS Trust
 Diabetes Update: Keeping patients safe Victoria Ruszala MFRPSII North Bristol NHS Trust Declaration of Interests I have received funding from the following companies for providing education sessions, attending
Diabetes Update: Keeping patients safe Victoria Ruszala MFRPSII North Bristol NHS Trust Declaration of Interests I have received funding from the following companies for providing education sessions, attending
Managing Special Circumstances Key Points
 Managing Special Circumstances Key Points Hypoglycaemia Dr Arla Ogilvie Diabetes Consultant (Watford) Sick Day Rules Janet Guest Community DSN (Hertford) Preparing for Colonoscopy Carolyn Jones In-Patient
Managing Special Circumstances Key Points Hypoglycaemia Dr Arla Ogilvie Diabetes Consultant (Watford) Sick Day Rules Janet Guest Community DSN (Hertford) Preparing for Colonoscopy Carolyn Jones In-Patient
DR HJ BODANSKY MD FRCP CONSULTANT PHYSICIAN LEEDS TEACHING HOSPITALS ASSOCIATE PROFESSOR, UNIVERSITY OF LEEDS
 DR HJ BODANSKY MD FRCP CONSULTANT PHYSICIAN LEEDS TEACHING HOSPITALS ASSOCIATE PROFESSOR, UNIVERSITY OF LEEDS DIABETETES UPDATE 2015 AIMS OF THE SEMINAR Diagnosis Investigation Management When to refer
DR HJ BODANSKY MD FRCP CONSULTANT PHYSICIAN LEEDS TEACHING HOSPITALS ASSOCIATE PROFESSOR, UNIVERSITY OF LEEDS DIABETETES UPDATE 2015 AIMS OF THE SEMINAR Diagnosis Investigation Management When to refer
Agenda. Indications Different insulin preparations Insulin initiation Insulin intensification
 Insulin Therapy F. Hosseinpanah Obesity Research Center Research Institute for Endocrine sciences Shahid Beheshti University of Medical Sciences November 11, 2017 Agenda Indications Different insulin preparations
Insulin Therapy F. Hosseinpanah Obesity Research Center Research Institute for Endocrine sciences Shahid Beheshti University of Medical Sciences November 11, 2017 Agenda Indications Different insulin preparations
Dr Tahseen A. Chowdhury Royal London Hospital. New Guidelines in Diabetes: NICE or Nasty?
 Dr Tahseen A. Chowdhury Royal London Hospital New Guidelines in Diabetes: NICE or Nasty? I have no conflicts of interest I do not undertake talks / advisory bodies / research for any pharma company Consultant
Dr Tahseen A. Chowdhury Royal London Hospital New Guidelines in Diabetes: NICE or Nasty? I have no conflicts of interest I do not undertake talks / advisory bodies / research for any pharma company Consultant
Update on Therapies for Type 2 Diabetes: Angela D. Mazza, DO July 31, 2015
 Update on Therapies for Type 2 Diabetes: 2015 Angela D. Mazza, DO July 31, 2015 Objectives To present the newer available therapies for the management of T2D To discuss the advantages and disadvantages
Update on Therapies for Type 2 Diabetes: 2015 Angela D. Mazza, DO July 31, 2015 Objectives To present the newer available therapies for the management of T2D To discuss the advantages and disadvantages
Diabetes Meds Update Disclaimer and Important Info. Objectives. Page 1. Copyright , Diabetes Education Services
 Diabetes Meds Update 2016 Beverly Dyck Thomassian, RN, MPH, BC ADM, CDE President, Diabetes Education Services Disclaimer and Important Info This content is for educational purposes only. Please see Package
Diabetes Meds Update 2016 Beverly Dyck Thomassian, RN, MPH, BC ADM, CDE President, Diabetes Education Services Disclaimer and Important Info This content is for educational purposes only. Please see Package
Peri-Operative Guidelines for Management of Diabetes Patients
 Peri-Operative Guidelines for Management of Diabetes Patients Target blood glucose 6-10 mmol/l for all patients Acceptable blood glucose 4-11 mmol/l for all patients Definitions Non-Insulin Glucose Lowering
Peri-Operative Guidelines for Management of Diabetes Patients Target blood glucose 6-10 mmol/l for all patients Acceptable blood glucose 4-11 mmol/l for all patients Definitions Non-Insulin Glucose Lowering
MANAGEMENT OF DIABETES IN PREGNANCY
 MANAGEMENT OF DIABETES IN PREGNANCY Ministry of Health Malaysia Malaysian Endocrine & Metabolic Society Perinatal Society of Malaysia Family Medicine Specialists Association of Malaysia Academy of Medicine
MANAGEMENT OF DIABETES IN PREGNANCY Ministry of Health Malaysia Malaysian Endocrine & Metabolic Society Perinatal Society of Malaysia Family Medicine Specialists Association of Malaysia Academy of Medicine
TYPE 1 DIABETES AND EXERCISE. Mark W Savage
 TYPE 1 DIABETES AND EXERCISE Mark W Savage Acknowledgments Slides with a blue background are cropped and courtesy of both Eli Lilly and Company, and Dr Ian Gallen FRCP Consultant Diabetologist, Royal Berkshire
TYPE 1 DIABETES AND EXERCISE Mark W Savage Acknowledgments Slides with a blue background are cropped and courtesy of both Eli Lilly and Company, and Dr Ian Gallen FRCP Consultant Diabetologist, Royal Berkshire
24 Hour Support. Telephone Available 24 hours a day, 7 days a week
 Contents Page What is SHAIRE? 1 What is basal-bolus regimen? 2 Why do I need a basal-bolus regimen? 3 How does basal insulin work? 3 How does rapid-acting insulin work? 4 How often should I test my Blood
Contents Page What is SHAIRE? 1 What is basal-bolus regimen? 2 Why do I need a basal-bolus regimen? 3 How does basal insulin work? 3 How does rapid-acting insulin work? 4 How often should I test my Blood
Managing diabetes if you are having a colonoscopy
 Managing diabetes if you are having a colonoscopy Diabetes and Endocrinology Patient Information Leaflet Introduction This leaflet provides advice and instructions to people with diabetes who are going
Managing diabetes if you are having a colonoscopy Diabetes and Endocrinology Patient Information Leaflet Introduction This leaflet provides advice and instructions to people with diabetes who are going
Policy for the Provision of Insulin Pumps for Patients with Diabetes Mellitus
 Policy for the Provision of Insulin Pumps for Patients with Diabetes Mellitus Version No. Changes Made Version of July 2018 V0.5 Changes made to the policy following patient engagement including: - the
Policy for the Provision of Insulin Pumps for Patients with Diabetes Mellitus Version No. Changes Made Version of July 2018 V0.5 Changes made to the policy following patient engagement including: - the
insulin degludec/liraglutide 100 units/ml / 3.6mg/mL solution for injection pre-filled pen (Xultophy ) SMC No. (1088/15) Novo Nordisk A/S
 SMC No. (1088/15) Novo Nordisk A/S") insulin degludec/liraglutide 100 units/ml / 3.6mg/mL solution for injection pre-filled pen (Xultophy ) SMC No. (1088/15) Novo Nordisk A/S 4 September 2015 The Scottish Medicines Consortium (SMC) has completed
insulin degludec/liraglutide 100 units/ml / 3.6mg/mL solution for injection pre-filled pen (Xultophy ) SMC No. (1088/15) Novo Nordisk A/S 4 September 2015 The Scottish Medicines Consortium (SMC) has completed
GLP-1 (glucagon-like peptide-1) Agonists (Byetta, Bydureon, Tanzeum, Trulicity, Victoza ) Step Therapy and Quantity Limit Criteria Program Summary
 Agonists (Byetta, Bydureon, Tanzeum, Trulicity, Victoza ) Step Therapy and Quantity Limit Criteria Program Summary") OBJECTIVE The intent of the GLP-1 (glucagon-like peptide-1) s (Byetta/exenatide, Bydureon/ exenatide extended-release, Tanzeum/albiglutide, Trulicity/dulaglutide, and Victoza/liraglutide) Step Therapy
OBJECTIVE The intent of the GLP-1 (glucagon-like peptide-1) s (Byetta/exenatide, Bydureon/ exenatide extended-release, Tanzeum/albiglutide, Trulicity/dulaglutide, and Victoza/liraglutide) Step Therapy
BEDFORDSHIRE AND LUTON JOINT PRESCRIBING COMMITTEE (JPC)
") BEDFORDSHIRE AND LUTON JOINT PRESCRIBING COMMITTEE (JPC) June 2017 Review: June 2020 (earlier if required see recommendations) Bulletin 255: Insulin aspart New Formulation - Fiasp JPC Recommendations:
BEDFORDSHIRE AND LUTON JOINT PRESCRIBING COMMITTEE (JPC) June 2017 Review: June 2020 (earlier if required see recommendations) Bulletin 255: Insulin aspart New Formulation - Fiasp JPC Recommendations:
Individualising Insulin Regimens: Premixed or basal plus/bolus?
 Individualising Insulin Regimens: Premixed or basal plus/bolus? Dr. Ted Wu Director, Diabetes Centre, Hospital Sydney, Australia Turkey, April 2015 Centre of Health Professional Education Optimising insulin
Individualising Insulin Regimens: Premixed or basal plus/bolus? Dr. Ted Wu Director, Diabetes Centre, Hospital Sydney, Australia Turkey, April 2015 Centre of Health Professional Education Optimising insulin
GLP-1 receptor agonists for type 2 diabetes currently available in the U.S.
 GLP-1 receptor agonists for type 2 diabetes currently available in the U.S. GLP-1 agonists are a class of antidiabetic agents that mimic the actions of the glucagon-like peptide. GLP-1 is one of several
GLP-1 receptor agonists for type 2 diabetes currently available in the U.S. GLP-1 agonists are a class of antidiabetic agents that mimic the actions of the glucagon-like peptide. GLP-1 is one of several
Guidelines to assist General Practitioners in the Management of Type 2 Diabetes. April 2010
 Guidelines to assist General Practitioners in the Management of Type 2 Diabetes April 2010 Foreword The guidelines were devised by the Diabetes Day Centre in Beaumont Hospital in consultation with a number
Guidelines to assist General Practitioners in the Management of Type 2 Diabetes April 2010 Foreword The guidelines were devised by the Diabetes Day Centre in Beaumont Hospital in consultation with a number
Diabetes Newly Diagnosed with NO evidence of DKA
 1. DIAGNOSIS confirmed by doctor using below guidelines: (a) History of Polyuria (usually nocturia ± enuresis) Polydipsia. ± Weight Loss (b) Glycosuria (c) Blood Glucose (BG) > 11 mmol/l (confirm from
1. DIAGNOSIS confirmed by doctor using below guidelines: (a) History of Polyuria (usually nocturia ± enuresis) Polydipsia. ± Weight Loss (b) Glycosuria (c) Blood Glucose (BG) > 11 mmol/l (confirm from
Mr Gavin Hendry. Mr Rab Burtun. Prof Jim Mann. Diabetes Nurse Facilitator, Auckland. Dunedin. Human Nutrition & Medicine University of Otago, Dunedin
 Mr Rab Burtun Diabetes Nurse Facilitator, Auckland Mr Gavin Hendry Dunedin Prof Jim Mann Human Nutrition & Medicine University of Otago, Dunedin Insulin Master Class Presented by: Prof Jim Mann Gavin Hendry
Mr Rab Burtun Diabetes Nurse Facilitator, Auckland Mr Gavin Hendry Dunedin Prof Jim Mann Human Nutrition & Medicine University of Otago, Dunedin Insulin Master Class Presented by: Prof Jim Mann Gavin Hendry
Individualizing Care for Patients with Type 2 Diabetes
 Individualizing Care for Patients with Type 2 Diabetes Disclosures Speaker: AstraZeneca, Novo Nordisk, BI/Lilly, Valeritas, Takeda Advisor: Tandem Diabetes, Sanofi Objectives Develop individualized approaches
Individualizing Care for Patients with Type 2 Diabetes Disclosures Speaker: AstraZeneca, Novo Nordisk, BI/Lilly, Valeritas, Takeda Advisor: Tandem Diabetes, Sanofi Objectives Develop individualized approaches
This program applies to Commercial, GenPlus and Health Insurance Marketplace formularies.
 OBJECTIVE The intent of the GLP-1 (glucagon-like peptide-1) Agonists [Adlyxin (lixisenatide), Byetta (exenatide), Bydureon (exenatide extended-release), Tanzeum (albiglutide), Trulicity (dulaglutide),
OBJECTIVE The intent of the GLP-1 (glucagon-like peptide-1) Agonists [Adlyxin (lixisenatide), Byetta (exenatide), Bydureon (exenatide extended-release), Tanzeum (albiglutide), Trulicity (dulaglutide),
Initiation and Titration of Insulin in Diabetes Mellitus Type 2
 Initiation and Titration of Insulin in Diabetes Mellitus Type 2 Greg Doelle MD, MS April 6, 2016 Disclosure I have no actual or potential conflicts of interest in relation to the content of this lecture.
Initiation and Titration of Insulin in Diabetes Mellitus Type 2 Greg Doelle MD, MS April 6, 2016 Disclosure I have no actual or potential conflicts of interest in relation to the content of this lecture.
exenatide 2mg powder and solvent for prolonged-release suspension for injection (Bydureon ) SMC No. (748/11) Eli Lilly and Company Limited
 SMC No. (748/11) Eli Lilly and Company Limited") exenatide 2mg powder and solvent for prolonged-release suspension for injection (Bydureon ) SMC No. (748/11) Eli Lilly and Company Limited 09 December 2011 The Scottish Medicines Consortium (SMC) has completed
exenatide 2mg powder and solvent for prolonged-release suspension for injection (Bydureon ) SMC No. (748/11) Eli Lilly and Company Limited 09 December 2011 The Scottish Medicines Consortium (SMC) has completed
Scottish Medicines Consortium
 Scottish Medicines Consortium liraglutide 6mg/mL prefilled pen for injection (3mL) (Victoza ) Novo Nordisk Ltd. No. (585/09) 06 November 2009 The Scottish Medicines Consortium (SMC) has completed its assessment
Scottish Medicines Consortium liraglutide 6mg/mL prefilled pen for injection (3mL) (Victoza ) Novo Nordisk Ltd. No. (585/09) 06 November 2009 The Scottish Medicines Consortium (SMC) has completed its assessment
EAST OF ENGLAND CHILDREN AND YOUNG PEOPLE S DIABETES NETWORK. Optimising Glycaemic Control for Children and Young People with Diabetes
 EAST OF ENGLAND CHILDREN AND YOUNG PEOPLE S DIABETES NETWORK Optimising Glycaemic Control for Children and Young People with Diabetes Local diabetes teams need to take on the responsibility of ensuring
EAST OF ENGLAND CHILDREN AND YOUNG PEOPLE S DIABETES NETWORK Optimising Glycaemic Control for Children and Young People with Diabetes Local diabetes teams need to take on the responsibility of ensuring
The Wheel of Life Exercise. What s Happening? Where to start the beginning. What's in a meter- are they all the same?
 Wharfedale Hospital Otley Linda Clapham BSc Hons. RGN, SEN,Cert. Ed. The Wheel of Life Exercise An exercise to Encourage self management Work What s going on! Medication Helping patients succeed Diabetes
Wharfedale Hospital Otley Linda Clapham BSc Hons. RGN, SEN,Cert. Ed. The Wheel of Life Exercise An exercise to Encourage self management Work What s going on! Medication Helping patients succeed Diabetes