MEDICATION APPROPRIATENESS FOR THE AGING POPULATION. Building Partnerships for Successful Aging
|
|
|
- Vivian Simmons
- 5 years ago
- Views:
Transcription



1 MEDICATION APPROPRIATENESS FOR THE AGING POPULATION Building Partnerships for Successful Aging
2 Learning objectives Appreciate complexities involved in making appropriate clinical decisions in older adults with regard to stopping medications. Describe guiding principles for the care of older adults with multiple co-morbidities as relating to pharmacologic treatment. Discuss the impact of life expectancy, functional status, goals of care, and time to treat on this decision making process.
3 No Disclosures I have no financial disclosures to report.
4 Chronic Conditions Hypertension Diabetes melltius Osteoarthritis Congestive heart failure Diabetes mellitus Hyperlipidemia Osteoporosis Atrial fibrillation COPD
5 The Medication Appropriateness Index Is there an indication for the drug? Is the medication effective for the condition? Is the dosage correct? Are the directions correct? Are the directions practical? Are there clinically significant drug-drug interactions? Are there clinically significant drug-disease/condition interactions? Is there unnecessary duplication with other drugs? Is the duration of therapy acceptable? Is this drug the least expensive alternative compared with others of equal usefulness?
6 Case: Mrs. B Mrs. B is a 79-year-old woman with 5 chronic conditions of moderate severity: COPD Hypertension Diabetes mellitus Osteoporosis Osteoarthritis

7 Treatment regimen based on clinical practice guidelines

8 Potential treatment interactions
9 What should be considered appropriate prescribing for patients late in life? 1. Remaining life expectancy 2. Time until benefit 3. Goals of care 4. Treatment targets
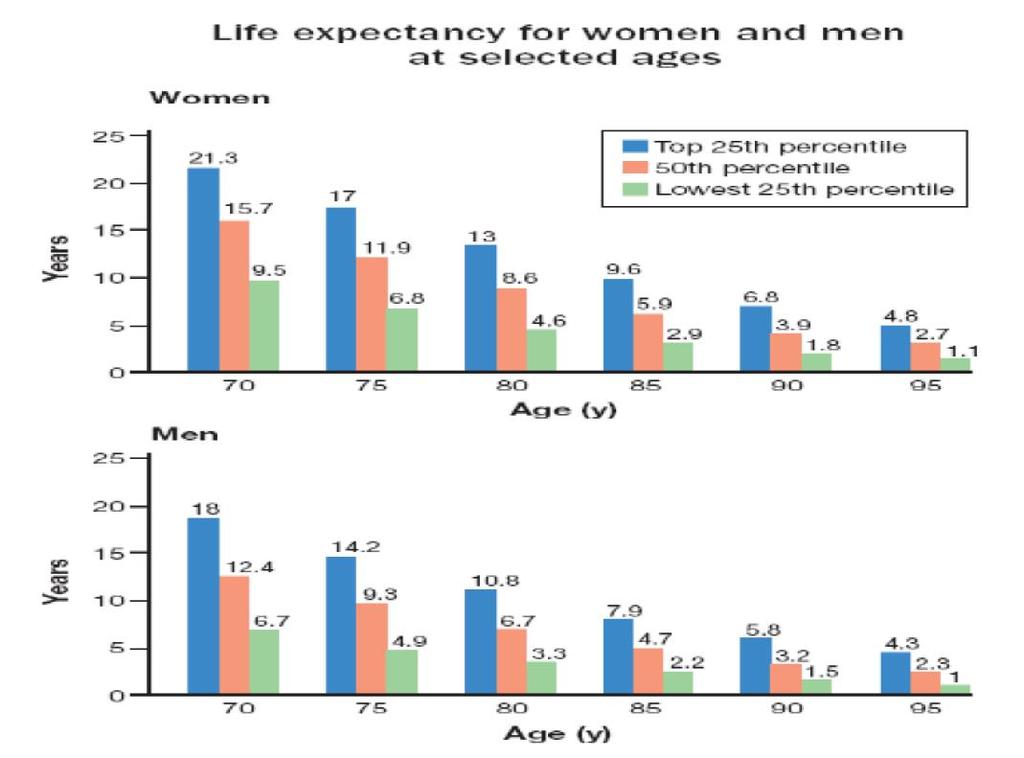
10 Life Expectancy
11 Life Expectancy
12 Time Until benefit Is the patient s life expectancy long enough that they will benefit from the drug? What is the amount of time until the medication will show a benefit?
13 Goals of Care Collaboration between physicians, patients, and families about goals of care will facilitate decisions regarding starting, stopping, and continuing medications.

14 Goals of Care
15 Treatment Targets Palliative model Life prolongation Prevention of morbidity and mortality Maintenance of current state/function and treatment of acute illness
16 Primary and Secondary Prevention Primary prevention aims to prevent disease or injury before it occurs. Secondary prevention aims to reduce the impact of a disease or injury that has already occurred.
17 Case 1 A 75-year-old Caucasian female. Past medical history: hypertension, osteoarthritis Newly diagnosed type 2 diabetes mellitus ADLs: 6/6 (independent) IADLs: 8/8 (independent ) Labs: LDL 143, Cr 1.0, GFR >60, A1c 8.7% Meds: atorvastatin, calcium, lisinopril, aspirin

18 Case 1 What is her life expectancy?

19 Case 1 This patient s life expectancy is: At least 17 years (top 25 th percentile)
20 Case 1 What is the time until benefit of the following therapies? Diabetes: 10 years to see benefit with ACE and sulfonylurea Hypertension: 2 years to see benefit with ACE Vascular events: statin can reduce risk of events after 2 years Cardiovascular events: statin can reduce risk of events after 5 years Primary prevention: aspirin reduces risk of MI after 5 years
21 Case 1 Goals of care: Patient wishes to prevent progression of her disease She wishes to maintain her excellent functional status Treatment targets: Primary and secondary prevention strategies
22 Case 2 72-year-old Caucasian male Past Medical History: Systolic CHF (NYHA class IV), emphysema ADL:3/6 IADL:3/8 VS: 84% on room air ROS: +Dyspnea at rest Meds: Metolazone, albuterol sulfate, furosemide, lisinopril, isosorbide mononitrate, ipratropium bromide, fluticasone, theophylline

23 Case 2-What is his life expectancy? This patient s life expectancy is: At least 6.7 years (lower 25 th percentile) but may be less based on organ system failure.
24 Case 2 What is time until benefit of the following therapies? CHF: relatively speaking, medications to prevent heart failure mortality such as ACE inhibitors can have a longer time to benefit than medications to treat fluid overload such as loop diuretics Emphysema: similar to CHF, inhaled corticosteroids and theophylline may have a longer time until benefit than bronchodilators
25 Case 2 Goals of care: The patient wishes to avoid further testing and hospital care Treatment targets: Palliative Analgesics, anti-anxiety, bronchodilators Consider stopping steroids and ACE inhibitors
26 Feasibility Study of a Systematic Approach for Discontinuation of Multiple Medications in Older Adults Background: Studying the feasibility of using the Good Palliative Geriatric practice algorithm (GP-GP) for drug cessation in community-dwelling older patients Methods: GP-GP was applied to 70 community dwelling patients Results: Successful discontinuation is 81% Conclusions: Feasibility of using an algorithm for trialing discontinuation of medications
 algorithm")
27 Good Palliative Geriatric Practice(GP-GP) algorithm
28 Case 3 86-year-old Caucasian male Past medical history: Hypertension, dementia, CKD stage 3, NYHA class III heart failure, hyperlipidemia ADL: 1/6 IADLs: 0/8 ROS: fatigue, generalized myalgias Medications: Furosemide, simvastatin
29 Case 3 The patient's life expectancy At least 2.2 years (top 25 th percentile) but may be less based on organ system failure.
30 Case 3 What is the time until benefit of the following therapies? CHF: relatively speaking, medications to prevent heart failure mortality such as ACE inhibitors can have a longer time to benefit than medications to treat fluid overload such as loop diuretics Hyperlipidemia: Vascular events: statin can reduce risk after 2 years Cardiovascular events: statin can reduce risk after 5 years
31 Case 3 Goals of Care: The patient wishes to avoid any invasive procedure and maintain his current status Treatment goals: Symptom control, prevention of symptoms, and to treat acute exacerbations
32 What does the research say?
33 Hypertension and Diabetes Hypertension in the very elderly trial (HYVET) showed 21% reduction in overall mortality and 31% reduction in stroke after treatment for two years. Fewer adverse affects with active treatment than placebo. For diabetes, there is a lack of clinical trials focused on the elderly but estimates from other trials show: Approximately 8 years are needed to prevent microvascular complications in new-onset diabetics Approximately 4-6 years are needed for patients with pre-existing microvascular disease ADVANCE trial: 20% reduction in albuminuria at 5 years VADT trial: improving A1c from 8.4% to 6.9% appeared to have minimal effects

34 Intensive vs. Standard Blood Pressure Control and Cardiovascular Disease Outcomes in Adults Aged > 75
35 Intensive vs. Standard Blood Pressure Control and Cardiovascular Disease Outcomes in Adults Aged > 75 Exclusion criteria: Type 2 diabetes CVA Symptomatic heart failure within 6 months Reduced EF Dementia Unexpected survival of less than 3 years Unintentional weight loss during pass 6 months (>10% of body weight) Nursing home resident SBP of less than 110 mm Hg following 1 minute of standing

36 In elderly subjects at high cardiovascular risk without established cardiovascular disease, statins significantly reduce the incident of MI and stroke, but do not significantly prolong survival in the short-term.

37 Statins reduce all-cause mortality in elderly patients and the magnitude of this effect is substantially larger than had been previously estimated.
38 Implementing the AGS glycemic control guideline for Hemoglobin A1c (HbA1c)<8% in frail older patients with diabetes led to fewer hyperglycemic episodes, but more severe hypoglycemic episodes requiring ER visits in the Early implementation period. Future glycemic control guideline implementation efforts should be coupled with close monitoring for severe hypoglycemia in the early implementation period.
39 Barriers to eliminating medications 1) Medications proven in well-designed studies 2) Contrary to their doctor s treatment 3) Computerized medical information 4) Direct-to-consumer pharmaceutical settings
40 PLEASED Do Patient or family views? Long-term benefits? Evidence of benefit Adverse effects present? Symptom control? Excessive dosage? Discontinuation feasible? DOcument, plan, share, monitor
41 Guide to stopping medications in the elderly Recognize the need to stop a medicine Reduce or stop one medicine at a time Taper medicines when appropriate Check for benefit or harm after each medicine has been stopped
42 Guide to stopping medications Anti-hypertensives Benzodiazepines Oral corticosteroids Antidepressants Acid suppressants Bisphosphonates Statins
43 Question 1 Which of the following is not a consideration with regard to appropriate prescribing of medications late in life? A. Remaining life expectancy B. Availability of generic medication C. Morbidity and mortality D. Patient expectations of treatment E. Laboratory test targets
44 Question 2 Mrs. C is a 73-year-old female with active medical conditions including diabetes mellitus, seizure disorder, CVA with late effects including left-sided hemiparesis and dysphagia, chronic kidney disease stage 4, compensated diastolic heart failure with an ejection fraction of 55%, and chronic pain due to degenerative joint disease. Her functional status is 2/6 for her ADLs (independent with feeding and continence though she does have episodes of occasional functional incontinence) and she is 0/8 for her IADLs. She resides in a long-term care facility. Her current medications include glipizide, levetiracetam, clopidogrel, aspirin, tramadol, and atorvastatin. Her last hemoglobin A1c was 5.3%. Which of the following medications should be stopped at this time? A. glipizide B. levetiracetam C. clopidogrel D. aspirin E. atorvastatin
45 Question 3 Mrs. C is a 73-year-old female with active medical conditions including diabetes mellitus, seizure disorder, CVA with late effects including leftsided hemiparesis and dysphagia, chronic kidney disease stage 4, compensated diastolic heart failure with an ejection fraction of 55%, and chronic pain due to degenerative joint disease. Her functional status is 2/6 for her ADLs (independent with feeding and continence though she does have episodes of occasional functional incontinence) and she is 0/8 for her IADLs. She resides in a long-term care facility. Her current medications include glipizide, levetiracetam, clopidogrel, aspirin, tramadol, and atorvastatin. Her last hemoglobin A1c was 5.3%. What is her estimated life expectancy? A years B years C. 9.5 years
46 References 1. Hanlon, JT Schmader, KE, Sama, GP, et. Al. A method for assessing drug therapy appropriateness. J. Clin Epidemiol. 1992;45: Boyd, et. al. JAMA 2005;294: Walter, L. C. JAMA 2001;285: Holmes, HM Hayley, DC Alexander, GC Sachs, GA, et. al. Reconsidering Medication Appropriateness for Patients Late in Life Arch Intern Med 2006;166:
PROVIDING GUIDELINEadherent
 COMMENTARY Reconsidering Medication Appropriateness for Patients Late in Life PROVIDING GUIDELINEadherent care for many medical conditions increasingly means the addition of more medications to reach disease-specific
COMMENTARY Reconsidering Medication Appropriateness for Patients Late in Life PROVIDING GUIDELINEadherent care for many medical conditions increasingly means the addition of more medications to reach disease-specific
Deconstructing Polypharmacy. Alan B. Douglass, M.D. Director
 Deconstructing Polypharmacy Alan B. Douglass, M.D. Director Recognize this patient? Mrs. Brown- 82 years young Active Medical Problems Hypertension Hyperlipidemia Type 2 Diabetes Peripheral edema Osteoarthritis
Deconstructing Polypharmacy Alan B. Douglass, M.D. Director Recognize this patient? Mrs. Brown- 82 years young Active Medical Problems Hypertension Hyperlipidemia Type 2 Diabetes Peripheral edema Osteoarthritis
Health Outcome Prioritization as a Tool for Decision Making Among Older Persons With Multiple Chronic Conditions
 Health Outcome Prioritization as a Tool for Decision Making Among Older Persons With Multiple Chronic Conditions Mary Tinetti, M.D. Canadian Geriatrics Society May, 2013 CFPC CoI Templates: Slide 1 Faculty/Presenter
Health Outcome Prioritization as a Tool for Decision Making Among Older Persons With Multiple Chronic Conditions Mary Tinetti, M.D. Canadian Geriatrics Society May, 2013 CFPC CoI Templates: Slide 1 Faculty/Presenter
Objectives. Case Ruby. 1- Warfarin. 1- Warfarin. Warfarin discontinuation 8/13/ DRUGS TO STOP GIVING HOSPICE PATIENTS
 Objectives 10 DRUGS TO STOP GIVING HOSPICE PATIENTS Richard E. Allen MD, MPH Hospice Medical Director Family Medicine Residency Director Salt Lake City, Utah 2 Recognize 10 commonly prescribed medications
Objectives 10 DRUGS TO STOP GIVING HOSPICE PATIENTS Richard E. Allen MD, MPH Hospice Medical Director Family Medicine Residency Director Salt Lake City, Utah 2 Recognize 10 commonly prescribed medications
Deprescribing Unnecessary Medications: A Four-Part Process
 Deprescribing Unnecessary Medications: A Four-Part Process Scott Endsley, MD Fam Pract Manag. 2018;25(3):28-32. Abstract and Introduction Introduction www.medscape.com Ms. Horatio is a 76-year-old patient
Deprescribing Unnecessary Medications: A Four-Part Process Scott Endsley, MD Fam Pract Manag. 2018;25(3):28-32. Abstract and Introduction Introduction www.medscape.com Ms. Horatio is a 76-year-old patient
2/11/2016. Managing Polypharmacy: Evidence-based Dissection of Pharmaceuticals. Disclosure. Objectives
 Managing Polypharmacy: Evidence-based Dissection of Pharmaceuticals Heather Veeder MD Medical Director VITAS Healthcare San Antonio, TX Adjunct Professor of Medicine University of Texas Health Science
Managing Polypharmacy: Evidence-based Dissection of Pharmaceuticals Heather Veeder MD Medical Director VITAS Healthcare San Antonio, TX Adjunct Professor of Medicine University of Texas Health Science
Finding the sweet spot: Individualized targets for older adults with Type 2 DM
 Finding the sweet spot: Individualized targets for older adults with Type 2 DM Samuel C. Durso, M.D., M.B.A. Mason F. Lord Professor of Medicine Director, Division of Geriatric Medicine and Gerontology
Finding the sweet spot: Individualized targets for older adults with Type 2 DM Samuel C. Durso, M.D., M.B.A. Mason F. Lord Professor of Medicine Director, Division of Geriatric Medicine and Gerontology
STOPP START Toolkit Supporting Medication Review in the Older Person
 STOPP START Toolkit Supporting Medication Review in the Older Person STOPP: Screening Tool of Older People s potentially inappropriate Prescriptions START: Screening Tool to Alert doctors to Right (appropriate,
STOPP START Toolkit Supporting Medication Review in the Older Person STOPP: Screening Tool of Older People s potentially inappropriate Prescriptions START: Screening Tool to Alert doctors to Right (appropriate,
Polypharmacy, Medication Nihilism, and the art of de-prescribing
 Polypharmacy, Medication Nihilism, and the art of de-prescribing Temple Family Practice Review Course Leon S. Kraybill, MD, CMD Geriatrics, Lancaster General Hospital Physicians Division Chief, LGH Division
Polypharmacy, Medication Nihilism, and the art of de-prescribing Temple Family Practice Review Course Leon S. Kraybill, MD, CMD Geriatrics, Lancaster General Hospital Physicians Division Chief, LGH Division
Management of DM in Older Adults: It s not all about sugar! Who needs treatment for DM? Peggy Odegard, Pharm.D., BCPS, CDE
 Management of DM in Older Adults: It s not all about sugar! Peggy Odegard, Pharm.D., BCPS, CDE Who needs treatment for DM? 87 year old, frail male with moderately severe dementia living in NH with persistent
Management of DM in Older Adults: It s not all about sugar! Peggy Odegard, Pharm.D., BCPS, CDE Who needs treatment for DM? 87 year old, frail male with moderately severe dementia living in NH with persistent
Guidelines for Management of Chronic Conditions
 Guidelines for Management of Chronic Conditions 1. DIABETES: If you have high blood sugar or Diabetes, the following are recommended: Goals to prevent progression of diabetes and reducing complications
Guidelines for Management of Chronic Conditions 1. DIABETES: If you have high blood sugar or Diabetes, the following are recommended: Goals to prevent progression of diabetes and reducing complications
Case 1. Case 2. What do you think about reducing or discontinuing some of the above now that his LVEF has normalized?
 Case 1 A primary care colleague inquires what to do with a patient (HFrEF in NSR) who has a digoxin level of 2.8ng/ml. Level was obtained at 10am, patient takes all medications at one time upon arising
Case 1 A primary care colleague inquires what to do with a patient (HFrEF in NSR) who has a digoxin level of 2.8ng/ml. Level was obtained at 10am, patient takes all medications at one time upon arising
Chapter 10. Learning Objectives. Learning Objectives 9/11/2012. Congestive Heart Failure
 Chapter 10 Congestive Heart Failure Learning Objectives Explain concept of polypharmacy in treatment of congestive heart failure Explain function of diuretics Learning Objectives Discuss drugs used for
Chapter 10 Congestive Heart Failure Learning Objectives Explain concept of polypharmacy in treatment of congestive heart failure Explain function of diuretics Learning Objectives Discuss drugs used for
Heart Failure Clinician Guide JANUARY 2018
 Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Heart Failure Clinician Guide JANUARY 2018 Introduction This evidence-based guideline summary is based on the 2018 National Heart Failure Guideline.
Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Heart Failure Clinician Guide JANUARY 2018 Introduction This evidence-based guideline summary is based on the 2018 National Heart Failure Guideline.
Medically Complex Older Adults: The Pharmacotherapeutic Challenge
 Medically Complex Older Adults: The Pharmacotherapeutic Challenge Bradley R. Williams, PharmD, CGP Professor, Clinical Pharmacy & Clinical Gerontology University of Southern California Presentation Objectives
Medically Complex Older Adults: The Pharmacotherapeutic Challenge Bradley R. Williams, PharmD, CGP Professor, Clinical Pharmacy & Clinical Gerontology University of Southern California Presentation Objectives
It Happens Even in Type 2! When to Start Thinking Seriously About Hypoglycemia
 It Happens Even in Type 2! When to Start Thinking Seriously About Hypoglycemia Jacqueline LaManna, PhD, ANP BC, BC ADM, CDE Holly Divine, PharmD, BCACP, CGP, CDE, FAPhA Disclosures Dr. Jacqueline LaManna
It Happens Even in Type 2! When to Start Thinking Seriously About Hypoglycemia Jacqueline LaManna, PhD, ANP BC, BC ADM, CDE Holly Divine, PharmD, BCACP, CGP, CDE, FAPhA Disclosures Dr. Jacqueline LaManna
Heart Failure Clinician Guide JANUARY 2016
 Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Heart Failure Clinician Guide JANUARY 2016 Introduction This evidence-based guideline summary is based on the 2016 National Heart Failure Guideline.
Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Heart Failure Clinician Guide JANUARY 2016 Introduction This evidence-based guideline summary is based on the 2016 National Heart Failure Guideline.
The patient with multiple chronic conditions: balancing guidelines and patient preference
 The patient with multiple chronic conditions: balancing guidelines and patient preference Sid Feldman MD CCFP FCFP Associate Professor, Department of Family and Community Medicine, University of Toronto
The patient with multiple chronic conditions: balancing guidelines and patient preference Sid Feldman MD CCFP FCFP Associate Professor, Department of Family and Community Medicine, University of Toronto
New Clinical Trends in Geriatric Medicine. April 8, 2016 Amanda Lathia, MD, MPhil Staff, Center for Geriatric Medicine
 New Clinical Trends in Geriatric Medicine April 8, 2016 Amanda Lathia, MD, MPhil Staff, Center for Geriatric Medicine Objectives Review current guidelines for blood pressure (BP) control in older adults
New Clinical Trends in Geriatric Medicine April 8, 2016 Amanda Lathia, MD, MPhil Staff, Center for Geriatric Medicine Objectives Review current guidelines for blood pressure (BP) control in older adults
Case Study #1 GUIDING PRINCIPLES FOR THE CARE OF OLDER ADULTS WITH MULTIMORBIDITY
 Case Study #1 GUIDING PRINCIPLES FOR THE CARE OF OLDER ADULTS WITH MULTIMORBIDITY Panel Moderator & Panelists: Edward Perrin, MD Banner icare Scott Bolhack, MD, MBA Sandra Brownstein, PharmD Paige Hector,
Case Study #1 GUIDING PRINCIPLES FOR THE CARE OF OLDER ADULTS WITH MULTIMORBIDITY Panel Moderator & Panelists: Edward Perrin, MD Banner icare Scott Bolhack, MD, MBA Sandra Brownstein, PharmD Paige Hector,
Disclosures. Diabetes and Cardiovascular Risk Management. Learning Objectives. Atherosclerotic Cardiovascular Disease
 Disclosures Diabetes and Cardiovascular Risk Management Tony Hampton, MD, MBA Medical Director Advocate Aurora Operating System Advocate Aurora Healthcare Downers Grove, IL No conflicts or disclosures
Disclosures Diabetes and Cardiovascular Risk Management Tony Hampton, MD, MBA Medical Director Advocate Aurora Operating System Advocate Aurora Healthcare Downers Grove, IL No conflicts or disclosures
Polypharmacy. Polypharmacy. Suboptimal Prescribing in Older Adults. Kenneth Schmader, MD Professor of Medicine-Geriatrics
 Polypharmacy Kenneth Schmader, MD Professor of Medicine-Geriatrics Polypharmacy Definition Causes Consequences Prevention/management Suboptimal Prescribing in Older Adults Overuse Polypharmacy Underuse
Polypharmacy Kenneth Schmader, MD Professor of Medicine-Geriatrics Polypharmacy Definition Causes Consequences Prevention/management Suboptimal Prescribing in Older Adults Overuse Polypharmacy Underuse
Long-Term Care Updates
 Long-Term Care Updates July 2015 By Amy Friedman Wilson, PharmD Heart failure (HF) is a clinical condition in which ventricular filling or ejection of blood is structurally or functionally impaired. 1
Long-Term Care Updates July 2015 By Amy Friedman Wilson, PharmD Heart failure (HF) is a clinical condition in which ventricular filling or ejection of blood is structurally or functionally impaired. 1
Hypertension in the very old. Objectives: Clinical Perspective
 Harvard Medical School Hypertension in the very old Ihab Hajjar, MD, MS, AGSF Associate Director, CV Research Lab Assistant Professor of Medicine, Harvard Medical School Objectives: Describe the clinical
Harvard Medical School Hypertension in the very old Ihab Hajjar, MD, MS, AGSF Associate Director, CV Research Lab Assistant Professor of Medicine, Harvard Medical School Objectives: Describe the clinical
Special thanks to the EJC Foundation for their support of Sanford Center Geriatric Specialty Clinic
 Special thanks to the EJC Foundation for their support of Sanford Center Geriatric Specialty Clinic Sanford Center for Aging 775-784-4744 med.unr.edu/aging Diabetes Management Series: From Selfmanagement
Special thanks to the EJC Foundation for their support of Sanford Center Geriatric Specialty Clinic Sanford Center for Aging 775-784-4744 med.unr.edu/aging Diabetes Management Series: From Selfmanagement
The ABCs (A1C, BP and Cholesterol) of Diabetes
 of Diabetes") The ABCs (A1C, BP and Cholesterol) of Diabetes Gregg Simonson, PhD Director, Professional Training and Consulting International Diabetes Center; Adjunct Assistant Professor, University of Minnesota Department
The ABCs (A1C, BP and Cholesterol) of Diabetes Gregg Simonson, PhD Director, Professional Training and Consulting International Diabetes Center; Adjunct Assistant Professor, University of Minnesota Department
We are delighted to have Dr. Roetzheim with us today to discuss Managing Hypertension in Older Adult Patients.
 Richard Roetzheim, MD, MSPH is Professor and Chair, Department of Family Medicine at the University of South Florida Morsani College of Medicine. Dr. Roetzheim has considerable experience leading NIH funded
Richard Roetzheim, MD, MSPH is Professor and Chair, Department of Family Medicine at the University of South Florida Morsani College of Medicine. Dr. Roetzheim has considerable experience leading NIH funded
STOPP and START criteria October 2011
 # START and STOPP are newer criteria to identify potentially inappropriate medications in elderly, including drug drug and drug disease interactions, drugs which increase risk of falls and drugs which
# START and STOPP are newer criteria to identify potentially inappropriate medications in elderly, including drug drug and drug disease interactions, drugs which increase risk of falls and drugs which
AGS Annual Meeting May Sponsored by the Polypharmacy Special Interest Group and the Pharmacists Section
 AGS Annual Meeting May 2010 Sponsored by the Polypharmacy Special Interest Group and the Pharmacists Section No financial conflicts of interest Sponsored by the Polypharmacy Special Interest Group Thanks
AGS Annual Meeting May 2010 Sponsored by the Polypharmacy Special Interest Group and the Pharmacists Section No financial conflicts of interest Sponsored by the Polypharmacy Special Interest Group Thanks
Coronary Heart Disease
 Coronary Heart Disease This document is a final specification of the PRIMIS Comparative Analysis Service (CAS) MIQUEST query set to enable analyses in support of the NSF for CHD. The specification has
Coronary Heart Disease This document is a final specification of the PRIMIS Comparative Analysis Service (CAS) MIQUEST query set to enable analyses in support of the NSF for CHD. The specification has
Individualizing Treatment Plans for Older Adults With T2DM
 Individualizing Treatment Plans for Older Adults With T2DM Key Slides from the Interactive Newsletter Hypoglycemia y in Older Adults Particularly dangerous, especially for those on insulin or secretagogues
Individualizing Treatment Plans for Older Adults With T2DM Key Slides from the Interactive Newsletter Hypoglycemia y in Older Adults Particularly dangerous, especially for those on insulin or secretagogues
Jennifer Loh, MD, FACE Chief of Endocrinology KP Hawaii AAMD of Medical Education, KP Hawaii
 Individualized Diabetes Treatment for the Elderly Jennifer Loh, MD, FACE Chief of Endocrinology KP Hawaii AAMD of Medical Education, KP Hawaii Extremely Relevant Baby Boomers are aging! ¼ of people age
Individualized Diabetes Treatment for the Elderly Jennifer Loh, MD, FACE Chief of Endocrinology KP Hawaii AAMD of Medical Education, KP Hawaii Extremely Relevant Baby Boomers are aging! ¼ of people age
Interdisciplinary detection of potential drug related problems in older people
 Interdisciplinary detection of potential drug related problems in older people Prof. dr. Mirko Petrovic Department of Internal Medicine, Ghent University Department of Geriatrics, Ghent University Hospital,
Interdisciplinary detection of potential drug related problems in older people Prof. dr. Mirko Petrovic Department of Internal Medicine, Ghent University Department of Geriatrics, Ghent University Hospital,
Diabetes Mellitus: Implications of New Clinical Trials and New Medications
 Diabetes Mellitus: Implications of New Clinical Trials and New Medications Estimates of Diagnosed Diabetes in Adults, 2005 Alka M. Kanaya, MD Asst. Professor of Medicine UCSF, Primary Care CME October
Diabetes Mellitus: Implications of New Clinical Trials and New Medications Estimates of Diagnosed Diabetes in Adults, 2005 Alka M. Kanaya, MD Asst. Professor of Medicine UCSF, Primary Care CME October
Indiana Medicaid Drug Utilization Review Board Newsletter
 Indiana Medicaid Drug Utilization Review Board Newsletter Volume 12 Issue 4 October 2009 Indiana Medicaid DUR Board Room W382 Indiana State Government Center, South 402 West Washington Street Indianapolis,
Indiana Medicaid Drug Utilization Review Board Newsletter Volume 12 Issue 4 October 2009 Indiana Medicaid DUR Board Room W382 Indiana State Government Center, South 402 West Washington Street Indianapolis,
HYPERTENSION GUIDELINES WHERE ARE WE IN 2014
 HYPERTENSION GUIDELINES WHERE ARE WE IN 2014 Donald J. DiPette MD FACP Special Assistant to the Provost for Health Affairs Distinguished Health Sciences Professor University of South Carolina University
HYPERTENSION GUIDELINES WHERE ARE WE IN 2014 Donald J. DiPette MD FACP Special Assistant to the Provost for Health Affairs Distinguished Health Sciences Professor University of South Carolina University
Update in Geriatrics: Choosing Wisely Primum Non Nocere
 Joseph G. Ouslander, M.D. Professor of Clinical Biomedical Science Senior Associate Dean for Geriatric Programs Chair, Department of Integrated Medical Science Charles E. Schmidt College of Medicine Professor
Joseph G. Ouslander, M.D. Professor of Clinical Biomedical Science Senior Associate Dean for Geriatric Programs Chair, Department of Integrated Medical Science Charles E. Schmidt College of Medicine Professor
Polypharmacy & De-prescribing In Older Adults
 Polypharmacy & De-prescribing In Older Adults Maryland Association of Osteopathic Physicians Annual Meeting September 15, 2018 Elizabeth Phung, DO Lead Clinical Associate Physician Beacham Center for Geriatric
Polypharmacy & De-prescribing In Older Adults Maryland Association of Osteopathic Physicians Annual Meeting September 15, 2018 Elizabeth Phung, DO Lead Clinical Associate Physician Beacham Center for Geriatric
Difficult to Treat Hypertension
 Difficult to Treat Hypertension According to Goldilocks JNC 8 Blood Pressure Goals (2014) BP Goal 60 years old and greater*- systolic < 150 and diastolic < 90. (Grade A)** BP Goal 18-59 years old* diastolic
Difficult to Treat Hypertension According to Goldilocks JNC 8 Blood Pressure Goals (2014) BP Goal 60 years old and greater*- systolic < 150 and diastolic < 90. (Grade A)** BP Goal 18-59 years old* diastolic
A Guidance Statement from the American College of Physicians
 Hemoglobin A1c Targets for Glycemic Control with Pharmacologic Therapy in Non-Pregnant Adults with Type 2 Diabetes Mellitus: A Guidance Statement from the American College of Physicians Timothy J. Wilt,
Hemoglobin A1c Targets for Glycemic Control with Pharmacologic Therapy in Non-Pregnant Adults with Type 2 Diabetes Mellitus: A Guidance Statement from the American College of Physicians Timothy J. Wilt,
Diabetes Mellitus in Older Adults. Presenter Disclosure Information
 Diabetes Mellitus in Older Adults Medha Munshi, M.D. Joslin Diabetes Center Beth Israel Deaconess Medical Center Harvard Medical School Presenter Disclosure Information Medha Munshi Research grant from
Diabetes Mellitus in Older Adults Medha Munshi, M.D. Joslin Diabetes Center Beth Israel Deaconess Medical Center Harvard Medical School Presenter Disclosure Information Medha Munshi Research grant from
New Lipid Guidelines. PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN: Implications of the New Guidelines for Hypertension and Lipids.
 PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN: Implications of the New Guidelines for Hypertension and Lipids Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Disclosure No relevant
PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN: Implications of the New Guidelines for Hypertension and Lipids Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Disclosure No relevant
Abbreviations DPP-IV dipeptidyl peptidase IV DREAM Diabetes REduction Assessment with ramipril and rosiglitazone
 Index Abbreviations DPP-IV dipeptidyl peptidase IV DREAM Diabetes REduction Assessment with ramipril and rosiglitazone Medication GAD glutamic acid decarboxylase GLP-1 glucagon-like peptide 1 NPH neutral
Index Abbreviations DPP-IV dipeptidyl peptidase IV DREAM Diabetes REduction Assessment with ramipril and rosiglitazone Medication GAD glutamic acid decarboxylase GLP-1 glucagon-like peptide 1 NPH neutral
There s A Pill For That (But should my patient be on it?) A Review of Tools for the Evaluation of Optimal Prescribing in Geriatric Patients
 A Review of Tools for the Evaluation of Optimal Prescribing in Geriatric Patients") There s A Pill For That (But should my patient be on it?) A Review of Tools for the Evaluation of Optimal Prescribing in Geriatric Patients Marilyn N. Bulloch, PharmD, BCPS Assistant Clinical Professor
There s A Pill For That (But should my patient be on it?) A Review of Tools for the Evaluation of Optimal Prescribing in Geriatric Patients Marilyn N. Bulloch, PharmD, BCPS Assistant Clinical Professor
Objectives. Heart failure and Hypertension. Definition & epidemiology of heart failure HEART FAILURE 3/12/2016. Kirsten Bibbins-Domingo, PhD, MD, MAS
 Objectives Heart failure and Hypertension Kirsten Bibbins-Domingo, PhD, MD, MAS Lee Goldman, MD Endowed Chair in Medicine Professor of Medicine and of Epidemiology and Biostatistics University of California,
Objectives Heart failure and Hypertension Kirsten Bibbins-Domingo, PhD, MD, MAS Lee Goldman, MD Endowed Chair in Medicine Professor of Medicine and of Epidemiology and Biostatistics University of California,
Fighting Polypharmacy - From Theory to Practice :
 Fighting Polypharmacy - From Theory to Practice : A Rational, Cost Effective Approach for Improving Drug Therapy in Disabled Elderly People Doron Garfinkel, M.D., Sara Zur-Gil, Elena Kundzinsh, M.D., Joshua
Fighting Polypharmacy - From Theory to Practice : A Rational, Cost Effective Approach for Improving Drug Therapy in Disabled Elderly People Doron Garfinkel, M.D., Sara Zur-Gil, Elena Kundzinsh, M.D., Joshua
HF-PEF: Symptoms, quality of life and mortality/morbidity
 HF-PEF: Symptoms, quality of life and mortality/morbidity May 21, 2011 John McMurray, MD Eugene Braunwald Scholar in Cardiovascular Diseases, Brigham & Women s Hospital Boston; Visiting Professor of Medicine,
HF-PEF: Symptoms, quality of life and mortality/morbidity May 21, 2011 John McMurray, MD Eugene Braunwald Scholar in Cardiovascular Diseases, Brigham & Women s Hospital Boston; Visiting Professor of Medicine,
Polypharmacy and the Older Adult. Leslie Baker, PharmD, BCGP Umanga Sharma, MD
 Polypharmacy and the Older Adult Leslie Baker, PharmD, BCGP Umanga Sharma, MD Objectives Identify what polypharmacy is Identify factors leading to polypharmacy Discuss consequences of polypharmacy Identify
Polypharmacy and the Older Adult Leslie Baker, PharmD, BCGP Umanga Sharma, MD Objectives Identify what polypharmacy is Identify factors leading to polypharmacy Discuss consequences of polypharmacy Identify
ENSURING EXCELLENCE IN PRESCRIBING FOR OLDER ADULTS
 ENSURING EXCELLENCE IN PRESCRIBING FOR OLDER ADULTS Philip J. Schneider, MS, FASHP The University of Arizona College of Pharmacy Learning Objectives: Describe the medication-use system and all interdependent
ENSURING EXCELLENCE IN PRESCRIBING FOR OLDER ADULTS Philip J. Schneider, MS, FASHP The University of Arizona College of Pharmacy Learning Objectives: Describe the medication-use system and all interdependent
Thiazolidinedione-Associated Congestive Heart Failure and Pulmonary Edema
 Search the Journal search Advanced Search > Home Current Issue Past Issues Reprints Submissions Subscriptions Permissions About Us MAYO CLIN PROC. 2003;78:1088-1091 2003 MAYO FOUNDATION FOR MEDICAL EDUCATION
Search the Journal search Advanced Search > Home Current Issue Past Issues Reprints Submissions Subscriptions Permissions About Us MAYO CLIN PROC. 2003;78:1088-1091 2003 MAYO FOUNDATION FOR MEDICAL EDUCATION
1/4/18. Heart Failure Guideline Review and Update. Disclosure. Pharmacist Objectives. Pharmacy Technician Objectives. What is Heart Failure?
 Disclosure Heart Failure Guideline Review and Update I have had no financial relationship over the past 12 months with any commercial sponsor with a vested interest in this presentation. Natalie Beiter,
Disclosure Heart Failure Guideline Review and Update I have had no financial relationship over the past 12 months with any commercial sponsor with a vested interest in this presentation. Natalie Beiter,
Overview of Current Quality Measures that can be Impacted by Ambulatory Pharmacists
 Overview of Current Quality Measures that can be Impacted by Ambulatory Pharmacists Measure Name Measure Domain Measure Focus Comment/Explanation CMS Value-based Purchasing Program (CMS VBP) AMI 30-day
Overview of Current Quality Measures that can be Impacted by Ambulatory Pharmacists Measure Name Measure Domain Measure Focus Comment/Explanation CMS Value-based Purchasing Program (CMS VBP) AMI 30-day
Let it go! Rationalising medicines for patients with life limiting illness
 Let it go! Rationalising medicines for patients with life limiting illness Inga Andrew Senior Clinical Pharmacist Northumbria Healthcare Trust E-mail: inga_andrew@northumbria-healthcare.nhs.uk Welcome
Let it go! Rationalising medicines for patients with life limiting illness Inga Andrew Senior Clinical Pharmacist Northumbria Healthcare Trust E-mail: inga_andrew@northumbria-healthcare.nhs.uk Welcome
Congestive Heart Failure: Outpatient Management
 The Chattanooga Heart Institute Cardiovascular Symposium Congestive Heart Failure: Outpatient Management E. Philip Lehman MD, MPP Disclosure No financial disclosures. Objectives Evidence-based therapy
The Chattanooga Heart Institute Cardiovascular Symposium Congestive Heart Failure: Outpatient Management E. Philip Lehman MD, MPP Disclosure No financial disclosures. Objectives Evidence-based therapy
POLYPHARMACY IN OLDER ADULTS AND BEERS CRITERIA UPDATE
 POLYPHARMACY IN OLDER ADULTS AND BEERS CRITERIA UPDATE Jeannie Kim Lee, PharmD, BCPS, CGP Clinical Pharmacy Director College of Pharmacy The University of Arizona Learning Objectives: State the risks of
POLYPHARMACY IN OLDER ADULTS AND BEERS CRITERIA UPDATE Jeannie Kim Lee, PharmD, BCPS, CGP Clinical Pharmacy Director College of Pharmacy The University of Arizona Learning Objectives: State the risks of
The Failing Heart in Primary Care
 The Failing Heart in Primary Care Hamid Ikram How fares the Heart Failure Epidemic? 4357 patients, 57% women, mean age 74 years HFSA 2010 Practice Guideline (3.1) Heart Failure Prevention A careful and
The Failing Heart in Primary Care Hamid Ikram How fares the Heart Failure Epidemic? 4357 patients, 57% women, mean age 74 years HFSA 2010 Practice Guideline (3.1) Heart Failure Prevention A careful and
1/21/2016 UPDATE ON THE AMERICAN GERIATRICS SOCIETY 2015 BEERS CRITERIA DISCLOSURE OBJECTIVES AGING GOALS BEERS CRITERIA
 UPDATE ON THE AMERICAN GERIATRICS SOCIETY 2015 BEERS CRITERIA DISCLOSURE I have no financial conflict of interest to disclose. Lacey Charbonneau, Pharm.D. PGY-1 Community Practice Resident Baptist Medical
UPDATE ON THE AMERICAN GERIATRICS SOCIETY 2015 BEERS CRITERIA DISCLOSURE I have no financial conflict of interest to disclose. Lacey Charbonneau, Pharm.D. PGY-1 Community Practice Resident Baptist Medical
2016 Internal Medicine Preferred Specialty Measure Set
 1 0059 Diabetes: Hemoglobin A1c (HbA1c) Poor Control (>9%): Percentage of patients 18-75 years of age with diabetes who had hemoglobin A1c > 9.0% during the measurement period 5 0081 Registry, EHR, 9 0105
1 0059 Diabetes: Hemoglobin A1c (HbA1c) Poor Control (>9%): Percentage of patients 18-75 years of age with diabetes who had hemoglobin A1c > 9.0% during the measurement period 5 0081 Registry, EHR, 9 0105
Disclosures. Hypertension: Nationwide Dilemma. Learning Objectives. What s Currently Recommended? Specific Concerns 3/9/2012
 How Should We ACCOMPLISH Good Blood Pressure Control In Our VETS? Disclosures No conflicts of interest to disclose Updates in the Management of HypertensionIn the Elderly Antoine T. Jenkins, Pharm.D.,
How Should We ACCOMPLISH Good Blood Pressure Control In Our VETS? Disclosures No conflicts of interest to disclose Updates in the Management of HypertensionIn the Elderly Antoine T. Jenkins, Pharm.D.,
Hypertension (JNC-8)
") Hypertension (JNC-8) Southern California University of Health Sciences Physician Assistant Program Management and Treatment of Hypertension April 17, 2018, presented by Ezra Levy, Pharm.D.! The 8 th Joint
Hypertension (JNC-8) Southern California University of Health Sciences Physician Assistant Program Management and Treatment of Hypertension April 17, 2018, presented by Ezra Levy, Pharm.D.! The 8 th Joint
Antialdosterone treatment in heart failure
 Update on the Treatment of Chronic Heart Failure 2012 Antialdosterone treatment in heart failure 전남의대윤현주 Chronic Heart Failure Prognosis of Heart failure Cecil, Text book of Internal Medicine, 22 th edition
Update on the Treatment of Chronic Heart Failure 2012 Antialdosterone treatment in heart failure 전남의대윤현주 Chronic Heart Failure Prognosis of Heart failure Cecil, Text book of Internal Medicine, 22 th edition
Diabetes and the Elderly: Medication Considerations When Determining Benefits and Risks
 Diabetes and the Elderly: Medication Considerations When Determining Benefits and Risks Gretchen M. Ray, PharmD, PhC, BCACP, CDE Associate Professor UNM College of Pharmacy September 7 th, 2018 DISCLOSURES
Diabetes and the Elderly: Medication Considerations When Determining Benefits and Risks Gretchen M. Ray, PharmD, PhC, BCACP, CDE Associate Professor UNM College of Pharmacy September 7 th, 2018 DISCLOSURES
Intelligent Polypharmacy. Professor Colin P Bradley Department of General Practice University College Cork
 Intelligent Polypharmacy Professor Colin P Bradley Department of General Practice University College Cork Polypharmacy No standard definition 2005 review the use of medications that are not clinically
Intelligent Polypharmacy Professor Colin P Bradley Department of General Practice University College Cork Polypharmacy No standard definition 2005 review the use of medications that are not clinically
American Diabetes Association 2018 Guidelines Important Notable Points
 American Diabetes Association 2018 Guidelines Important Notable Points The Standards of Medical Care in Diabetes-2018 by ADA include the most current evidencebased recommendations for diagnosing and treating
American Diabetes Association 2018 Guidelines Important Notable Points The Standards of Medical Care in Diabetes-2018 by ADA include the most current evidencebased recommendations for diagnosing and treating
Geriatric Pharmacology
 Geriatric Pharmacology Janice Scheufler R.Ph.,PharmD, FASCP Clinical Pharmacist Hospice of the Western Reserve Objectives List three risk factors for adverse drug events in the elderly Discuss two physiological
Geriatric Pharmacology Janice Scheufler R.Ph.,PharmD, FASCP Clinical Pharmacist Hospice of the Western Reserve Objectives List three risk factors for adverse drug events in the elderly Discuss two physiological
Managing Hypertension in 2016
 Managing Hypertension in 2016: Where Do We Draw the Line? Disclosure No relevant financial relationships Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine baron@medicine.ucsf.edu
Managing Hypertension in 2016: Where Do We Draw the Line? Disclosure No relevant financial relationships Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine baron@medicine.ucsf.edu
Akinbolade O, Husband A, Forrest S, Todd A. Deprescribing in advanced illness. Progress in Palliative Care 2016, 24(5),
,") Akinbolade O, Husband A, Forrest S, Todd A. Deprescribing in advanced illness. Progress in Palliative Care 2016, 24(5), 268-271 Copyright: This is an Accepted Manuscript of an article published by Taylor
Akinbolade O, Husband A, Forrest S, Todd A. Deprescribing in advanced illness. Progress in Palliative Care 2016, 24(5), 268-271 Copyright: This is an Accepted Manuscript of an article published by Taylor
Symptom Management Challenges at End-of-Life
 Symptom Management Challenges at End-of-Life Amanda Lovell, PharmD, BCGP Clinical Pharmacist- Inpatient Units Optum Hospice Pharmacy Services February 15, 2018 Hospice Pharmacy Services Objectives Identify
Symptom Management Challenges at End-of-Life Amanda Lovell, PharmD, BCGP Clinical Pharmacist- Inpatient Units Optum Hospice Pharmacy Services February 15, 2018 Hospice Pharmacy Services Objectives Identify
BLCS 1-Clinical Overview. Dr. Chris Rauscher Clinical Lead Shared Care Polypharmacy Risk Reduction Initiative
 BLCS 1-Clinical Overview Dr. Chris Rauscher Clinical Lead Shared Care Polypharmacy Risk Reduction Initiative Fraser Health Guide To Person-Centered Medication Decisions Factors to Consider When Systematically
BLCS 1-Clinical Overview Dr. Chris Rauscher Clinical Lead Shared Care Polypharmacy Risk Reduction Initiative Fraser Health Guide To Person-Centered Medication Decisions Factors to Consider When Systematically
Chronic. Outline. Congestive^ Heart Failure: Update on Effective Monitoring and Treatment. Heart Failure Epidemiology
 Chronic Congestive^ Heart Failure: Update on Effective Monitoring and Treatment Michael G. Shlipak, MD, MPH Professor of Medicine, UCSF Chief, Division of General Internal Medicine, SFVA Medical Center
Chronic Congestive^ Heart Failure: Update on Effective Monitoring and Treatment Michael G. Shlipak, MD, MPH Professor of Medicine, UCSF Chief, Division of General Internal Medicine, SFVA Medical Center
Hypertension and Cholesterol in the Elderly
 Hypertension and Cholesterol in the Elderly Angela Sanford, MD Assistant Professor of Geriatrics Saint Louis University School of Medicine I have no relevant financial disclosures Cushman WC. The burden
Hypertension and Cholesterol in the Elderly Angela Sanford, MD Assistant Professor of Geriatrics Saint Louis University School of Medicine I have no relevant financial disclosures Cushman WC. The burden
Condition/Procedure Measure Compliance Criteria Reference Attribution Method
 Premium Specialty: Cardiology Credentialed Specialties include: Cardiac Diagnostic, Cardiology, Cardiovascular Disease, Clinical Cardiac Electrophysiology, and Interventional Cardiology This document is
Premium Specialty: Cardiology Credentialed Specialties include: Cardiac Diagnostic, Cardiology, Cardiovascular Disease, Clinical Cardiac Electrophysiology, and Interventional Cardiology This document is
Oral Hypoglycemics and Risk of Adverse Cardiac Events: A Summary of the Controversy
 Oral Hypoglycemics and Risk of Adverse Cardiac Events: A Summary of the Controversy Jeffrey Boord, MD, MPH Advances in Cardiovascular Medicine Kingston, Jamaica December 7, 2012 VanderbiltHeart.com Outline
Oral Hypoglycemics and Risk of Adverse Cardiac Events: A Summary of the Controversy Jeffrey Boord, MD, MPH Advances in Cardiovascular Medicine Kingston, Jamaica December 7, 2012 VanderbiltHeart.com Outline
Three triggers that suggest that patients could benefit from a hospice palliative care approach
 Why is it important to identify people nearing the end of life? About 1% of the population dies each year. Although some deaths are unexpected, many more in fact can be predicted. This is inherently difficult,
Why is it important to identify people nearing the end of life? About 1% of the population dies each year. Although some deaths are unexpected, many more in fact can be predicted. This is inherently difficult,
Causes of death in Diabetes
 Rates of CV events in Diabetes patients Respiratory4.2 Cancer 7.6 Diabetes 1.3 CV disease 17.3 Causes of death in Diabetes 250 200 150 100 50 0 per 10,000 person-years 97 151 243 Framingham 5 X increase
Rates of CV events in Diabetes patients Respiratory4.2 Cancer 7.6 Diabetes 1.3 CV disease 17.3 Causes of death in Diabetes 250 200 150 100 50 0 per 10,000 person-years 97 151 243 Framingham 5 X increase
Association between Potentially Inappropriate Prescription (PIP) and Health Outcome Among Geriatric Home Residents
 and Health Outcome Among Geriatric Home Residents") The Egyptian Journal of Hospital Medicine (July 2018) Vol. 72 (6), Page 4660-4665 Association between Potentially Inappropriate Prescription (PIP) and Health Outcome Among Geriatric Home Residents Moatassem
The Egyptian Journal of Hospital Medicine (July 2018) Vol. 72 (6), Page 4660-4665 Association between Potentially Inappropriate Prescription (PIP) and Health Outcome Among Geriatric Home Residents Moatassem
Hypertension in 2015: SPRINT-ing ahead of JNC-8. MAJ Charles Magee, MD MPH FACP Director, WRNMMC Hypertension Clinic
 Hypertension in 2015: SPRINT-ing ahead of JNC-8 MAJ Charles Magee, MD MPH FACP Director, WRNMMC Hypertension Clinic Conflits of interest? None Disclaimer The opinions contained herein are not to be considered
Hypertension in 2015: SPRINT-ing ahead of JNC-8 MAJ Charles Magee, MD MPH FACP Director, WRNMMC Hypertension Clinic Conflits of interest? None Disclaimer The opinions contained herein are not to be considered
Rationalizing Medications. Tan Jianming Senior Pharmacist KTPH
 Rationalizing Medications Tan Jianming Senior Pharmacist KTPH + Older patients are more likely to: 2 Have multiple co-morbid diseases Have age-related physiological changes that result in a reduced tolerance
Rationalizing Medications Tan Jianming Senior Pharmacist KTPH + Older patients are more likely to: 2 Have multiple co-morbid diseases Have age-related physiological changes that result in a reduced tolerance
Shared decision making for stepdown and stopping decisions. Michael R. Gionfriddo Pharm.D, Ph.D Geisinger Center for Pharmacy Innovation and Outcomes
 Shared decision making for stepdown and stopping decisions Michael R. Gionfriddo Pharm.D, Ph.D Geisinger Center for Pharmacy Innovation and Outcomes 1 Disclosures I have had travel and lodging paid for
Shared decision making for stepdown and stopping decisions Michael R. Gionfriddo Pharm.D, Ph.D Geisinger Center for Pharmacy Innovation and Outcomes 1 Disclosures I have had travel and lodging paid for
ACCORD, ADVANCE & VADT. Now what do I do in my practice?
 ACCORD, ADVANCE & VADT Now what do I do in my practice? Richard M. Bergenstal, MD International Diabetes Center Park Nicollet Health Services University of Minnesota Minneapolis, MN richard.bergenstal@parknicollet.com
ACCORD, ADVANCE & VADT Now what do I do in my practice? Richard M. Bergenstal, MD International Diabetes Center Park Nicollet Health Services University of Minnesota Minneapolis, MN richard.bergenstal@parknicollet.com
The Diabetes Link to Heart Disease
 The Diabetes Link to Heart Disease Anthony Abe DeSantis, MD September 18, 2015 University of WA Division of Metabolism, Endocrinology and Nutrition Oswald Toosweet Case #1 68 yo M with T2DM Diagnosed DM
The Diabetes Link to Heart Disease Anthony Abe DeSantis, MD September 18, 2015 University of WA Division of Metabolism, Endocrinology and Nutrition Oswald Toosweet Case #1 68 yo M with T2DM Diagnosed DM
Managing Polypharmacy: Thinking outside the box
 Managing Polypharmacy: Thinking outside the box Martin Wilson Consultant Physician Care of the Elderly NHS Highland Clare Morrison Lead Pharmacist (North) Senior Quality Clinical Lead NHS Highland Disclosure
Managing Polypharmacy: Thinking outside the box Martin Wilson Consultant Physician Care of the Elderly NHS Highland Clare Morrison Lead Pharmacist (North) Senior Quality Clinical Lead NHS Highland Disclosure
SIGN 149 Risk estimation and the prevention of cardiovascular disease. Quick Reference Guide July Evidence
 SIGN 149 Risk estimation and the prevention of cardiovascular disease Quick Reference Guide July 2017 Evidence ESTIMATING CARDIOVASCULAR RISK R Individuals with the following risk factors should be considered
SIGN 149 Risk estimation and the prevention of cardiovascular disease Quick Reference Guide July 2017 Evidence ESTIMATING CARDIOVASCULAR RISK R Individuals with the following risk factors should be considered
Implementation of JNC- 8 Hypertension Recommendations: Combining evidence and value-based practice strategies for accountable care
 Implementation of JNC- 8 Hypertension Recommendations: Combining evidence and value-based practice strategies for accountable care Shari Bolen MD, MPH MetroHealth/Case Western Reserve University 1 Disclosure
Implementation of JNC- 8 Hypertension Recommendations: Combining evidence and value-based practice strategies for accountable care Shari Bolen MD, MPH MetroHealth/Case Western Reserve University 1 Disclosure
DISCLOSURE PHARMACIST OBJECTIVES 9/30/2014 JNC 8: A REVIEW OF THE LONG-AWAITED/MUCH-ANTICIPATED HYPERTENSION GUIDELINES. I have nothing to disclose.
 JNC 8: A REVIEW OF THE LONG-AWAITED/MUCH-ANTICIPATED HYPERTENSION GUIDELINES Tiffany Dickey, PharmD Assistant Professor, UAMS COP Clinical Pharmacy Specialist, Mercy Hospital Northwest AR DISCLOSURE I
JNC 8: A REVIEW OF THE LONG-AWAITED/MUCH-ANTICIPATED HYPERTENSION GUIDELINES Tiffany Dickey, PharmD Assistant Professor, UAMS COP Clinical Pharmacy Specialist, Mercy Hospital Northwest AR DISCLOSURE I
Changing Patterns in Medication Use with Increasing Probability of Death for Older Medicare Beneficiaries
 Changing Patterns in Medication Use with Increasing Probability of Death for Older Medicare Beneficiaries Thomas Shaffer, MHS; Linda Simoni-Wastila, PhD, Wendy Toler, PharmD, Bruce Stuart, PhD, and Jalpa
Changing Patterns in Medication Use with Increasing Probability of Death for Older Medicare Beneficiaries Thomas Shaffer, MHS; Linda Simoni-Wastila, PhD, Wendy Toler, PharmD, Bruce Stuart, PhD, and Jalpa
The Indian Polycap Study 1 & 2 (TIPS 1 & 2) and The International Polycap Study 3 & 4 (TIPS 3 & 4)
 and The International Polycap Study 3 & 4 (TIPS 3 & 4)") The Indian Polycap Study 1 & 2 (TIPS 1 & 2) and The International Polycap Study 3 & 4 (TIPS 3 & 4) Denis Xavier MD, MSc Professor and Head, Pharmacology, St. John's Medical College Coordinator, Division
The Indian Polycap Study 1 & 2 (TIPS 1 & 2) and The International Polycap Study 3 & 4 (TIPS 3 & 4) Denis Xavier MD, MSc Professor and Head, Pharmacology, St. John's Medical College Coordinator, Division
Objectives. Describe results and implications of recent landmark hypertension trials
 Hypertension Update Daniel Schwartz, MD Assistant Professor of Medicine Associate Medical Director of Heart Transplantation Temple University School of Medicine Disclosures I currently have no relationships
Hypertension Update Daniel Schwartz, MD Assistant Professor of Medicine Associate Medical Director of Heart Transplantation Temple University School of Medicine Disclosures I currently have no relationships
COPD. Breathing Made Easier
 COPD Breathing Made Easier Catherine E. Cooke, PharmD, BCPS, PAHM Independent Consultant, PosiHleath Clinical Associate Professor, University of Maryland School of Pharmacy This program has been brought
COPD Breathing Made Easier Catherine E. Cooke, PharmD, BCPS, PAHM Independent Consultant, PosiHleath Clinical Associate Professor, University of Maryland School of Pharmacy This program has been brought
JNC Evidence-Based Guidelines for the Management of High Blood Pressure in Adults
 JNC 8 2014 Evidence-Based Guidelines for the Management of High Blood Pressure in Adults Table of Contents Why Do We Treat Hypertension? Blood Pressure Treatment Goals Initial Therapy Strength of Recommendation
JNC 8 2014 Evidence-Based Guidelines for the Management of High Blood Pressure in Adults Table of Contents Why Do We Treat Hypertension? Blood Pressure Treatment Goals Initial Therapy Strength of Recommendation
Older people with diabetes avoiding hospitalization
 Diabetes Management Older people with diabetes avoiding hospitalization Ahmed H Abdelhafiz*,1,2, Joanne J Russell 1, Andrew Key 1 & Alan J Sinclair 3 Practice points The prevalence of diabetes in older
Diabetes Management Older people with diabetes avoiding hospitalization Ahmed H Abdelhafiz*,1,2, Joanne J Russell 1, Andrew Key 1 & Alan J Sinclair 3 Practice points The prevalence of diabetes in older
Course Handouts & Disclosure
 COPD: Disease Trajectory and Hospice Eligibility Terri L. Maxwell PhD, APRN VP, Strategic Initiatives Weatherbee Resources Hospice Education Network Course Handouts & Disclosure To download presentation
COPD: Disease Trajectory and Hospice Eligibility Terri L. Maxwell PhD, APRN VP, Strategic Initiatives Weatherbee Resources Hospice Education Network Course Handouts & Disclosure To download presentation
HEART FAILURE: PHARMACOTHERAPY UPDATE
 HEART FAILURE: PHARMACOTHERAPY UPDATE 3 HEART FAILURE REVIEW 1 5.1 million x1.25 = 6.375 million 40 years old = MICHAEL F. AKERS, PHARM.D. CLINICAL PHARMACIST CENTRACARE HEALTH, ST. CLOUD HOSPITAL HF Diagnosis
HEART FAILURE: PHARMACOTHERAPY UPDATE 3 HEART FAILURE REVIEW 1 5.1 million x1.25 = 6.375 million 40 years old = MICHAEL F. AKERS, PHARM.D. CLINICAL PHARMACIST CENTRACARE HEALTH, ST. CLOUD HOSPITAL HF Diagnosis
Management of Lipid Disorders and Hypertension: Implications of the New Guidelines
 Management of Lipid Disorders and Hypertension Management of Lipid Disorders and Hypertension: Implications of the New Guidelines Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine
Management of Lipid Disorders and Hypertension Management of Lipid Disorders and Hypertension: Implications of the New Guidelines Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine
CVD Outcomes Aggregate Report Report Period: 05/01/ /30/2004
 Changes in JNC VII Blood Pressure Categories Blood Pressure Category Initial Value ¹ Latest Value ¹ Improvement ² (Based on JNC VII Guidelines) values (days) (N=271) (N = 209) Normal (SBP < 120 and DBP
Changes in JNC VII Blood Pressure Categories Blood Pressure Category Initial Value ¹ Latest Value ¹ Improvement ² (Based on JNC VII Guidelines) values (days) (N=271) (N = 209) Normal (SBP < 120 and DBP
Drugs that poison the elderly
 Drugs that poison the elderly Brent Tipping Sub-specialist Geriatrician and Specialist Physician Division of Geriatric Medicine, Department of Medicine University of the Witwatersrand To treat or not to
Drugs that poison the elderly Brent Tipping Sub-specialist Geriatrician and Specialist Physician Division of Geriatric Medicine, Department of Medicine University of the Witwatersrand To treat or not to
Diabetes Guidelines in View of Recent Clinical Trials Are They Still Applicable?
 Diabetes Guidelines in View of Recent Clinical Trials Are They Still Applicable? Jay S. Skyler, MD, MACP Division of Endocrinology, Diabetes, and Metabolism and Diabetes Research Institute University of
Diabetes Guidelines in View of Recent Clinical Trials Are They Still Applicable? Jay S. Skyler, MD, MACP Division of Endocrinology, Diabetes, and Metabolism and Diabetes Research Institute University of
Kanyini Guidelines Adherence with the Polypill (Kanyini GAP)
") Kanyini Guidelines Adherence with the Polypill (Kanyini GAP) Disclosures Funded by the National Health and Medical Research Council of Australia. Dr Reddy s Laboratories Ltd manufactured and supplied polypills
Kanyini Guidelines Adherence with the Polypill (Kanyini GAP) Disclosures Funded by the National Health and Medical Research Council of Australia. Dr Reddy s Laboratories Ltd manufactured and supplied polypills
Pharmaceutical Care for Geriatrics
 Continuing Professional Pharmacy Development Program Pharmaceutical Care for Geriatrics Presented by: Alla El-Awaisi; MPharm, MRPharmS, MSc Event Organizer: Dr. Nadir Kheir; PhD Disclaimer: PRESENTING
Continuing Professional Pharmacy Development Program Pharmaceutical Care for Geriatrics Presented by: Alla El-Awaisi; MPharm, MRPharmS, MSc Event Organizer: Dr. Nadir Kheir; PhD Disclaimer: PRESENTING
Measure Owner Designation. AMA-PCPI is the measure owner. NCQA is the measure owner. QIP/CMS is the measure owner. AMA-NCQA is the measure owner
 2011 EHR Measure Specifications The specifications listed in this document have been updated to reflect clinical practice guidelines and applicable health informatics standards that are the most current
2011 EHR Measure Specifications The specifications listed in this document have been updated to reflect clinical practice guidelines and applicable health informatics standards that are the most current