Surgical Treatment of Epilepsy
|
|
|
- Duane Ford
- 5 years ago
- Views:
Transcription
1 Presurgical Assessment and the Surgical Treatment of Epilepsy Michael C., MD Director, Rush Epilepsy Center Associate Professor and Senior Attending Neurologist Rush University Medical Center Chicago, Illinois Surgical Treatment of Epilepsy Patient selection Diagnostic evaluation for surgical treatment Types of surgical treatment Outcomes of therapy: risk/benefit Seizure freedom/cognitive function 1
2 Partial Epilepsy Goals of Therapy Render patient seizure-free Avoid neurological morbidity Improve quality of life Participating and productive member of society Epilepsy Surgery Surgical Candidates Medically refractory seizures Physically, socially disabled Localization-related epilepsy Low risk for morbidity Potential for rehabilitation 2
3 Partial Epilepsy Focal or GTC Seizures > 1 million patients in US 90% of the adult incident cases 45% have medically refractory seizures 20% have intractable epilepsy Partial Epilepsy 80% of adult partial epilepsy is of temporal lobe origin 90%: amygdalohippocampal complex origin (MTLE) 10%: lateral a temporal neocortex e origin (neocortical epilepsy) 3
4 Partial Epilepsy Comorbidity Cognitive disorder: memory loss Psychological illness: variable expression and intensity Psychosocial debilitation Increased risk of morbidity and mortality Epilepsy Surgery Misperceptions Should be of last resort Exclude the following: Bitemporal spikes GTC seizures Coexistent t psychiatric i illness Developmental delay 4
5 Evaluation of the Medically Intractable Patient: Questions Does the patient have epilepsy? Need to record with EEG the events in question Nonepileptic event Psychiatric or medical etiology Have the AEDs used been appropriate for the seizure type? Have adequate blood levels been tolerated and documented to prove that seizures are medically intractable due to lack of efficacy, not tolerability? Partial Epilepsy Treatment Old drugs (CBZ, Pb, PHT, VPA) New drugs (FBM, GBP, LEV, LTG, OXC, PGB, TGB, TPM, ZNS) Vagus nerve stimulation Epilepsy surgery 5
6 Epilepsy Efficacy of Treatment Brodie et al. Neurology 2002;58:S unselected patients newly diagnosed with epilepsy Followed for a median of 5 years Evaluate the efficacy of treatment (CBZ, VPA, LTG) Epilepsy 470 Newly Diagnosed, Untreated Seizure-free on 1 st N=222 (47%) monotherapy Seizure-free on 2nd N=61 (13%) monotherapy Seizure-free on 3rd N=6 (1%) monotherapy Brodie,
7 Epilepsy Efficacy of Treatment 63% were seizure-free the last year Only 11% who failed the 1st AED became seizure-free About 30-40% will have a difficult-tocontrol seizure disorder 0% seizure-free on > 3 AEDs Brodie, 2002 Partial Epilepsy Seizure-free on AEDs Partial epilepsy: 55% Temporal lobe epilepsy: 35% Lesional pathology: 10% Mesial temporal sclerosis: 10% 7
8 Epilepsy Surgery Historical Perspective Macroscopic pathology Extratemporal cortical resections Neurological deficits Ictal semiology Epilepsy Surgery Temporal Lobectomy: Pioneers Common operative strategy EEG localization Hippocampal resection Mesial temporal sclerosis Safe and effective procedure 8
9 Unified Theory of Epilepsy Surgery The surgical treatment of medically intractable epilepsy is to substantially disrupt a dysfunctional system But rarely do the interventions, whether resection, multiple subpial transection (MST), CCD, or VNS, completely remove or suppress the dysfunctional network Surgical Decision Making Focal resections First choice in appropriate candidates Importance of early intervention Palliative surgery (successful outcome does not always mean cure ) Vagus nerve stimulation (VNS) Corpus callosum division (CCD) Multiple subpial transection (MST) 9
10 Randomized, Controlled Trial of Surgery for TLE 80 patients randomly assigned for surgery (40 pts) or AED therapy (40 pts) for 1 year Four of the 40 pts refused surgery. Six of the 36 patients required invasive presurgical investigation Results free of seizures that impair awareness: 58% randomized to surgery 8% randomized to AED therapy 64% actually had surgery p<0.001 Wiebe S, et al NEJM Editorial Few accepted therapeutic interventions are as underutilized d as surgical treatment t t of epilepsy Two million patients suffer epilepsy in US 400, ,000 not controlled with AEDs 1990 survey: 1500 therapeutic surgical interventions Seizure-free rate: 70-90% surgical therapy Quality of life for patients with epilepsy treated surgically is related to the reoccurrence of seizures QOL higher employment/school attendance in SG Engel,
11 Practice Parameters: TLE Surgery Epilepsy: chronic neurologic disorder affects 0.5-1% of world s population In US and other industrial nations with many AEDs available, 30-40% of patients not adequately controlled WHO survey: disability from epilepsy accounts for ~1% of global burden of disease as measured by disability-adjusted adjusted life years (DALYs) This ranks third behind affective disorder and alcohol dependence among neurologic disorders. Comparable to worldwide burden due to lung and breast cancer Engel, et al Practice Parameters: TLE Surgery Surgical procedures for treatment of epilepsy p ~500 year ~1500 year ~3000 year Estimated that there are 100, ,000 potential surgical candidates in US Early intervention may prevent or reverse the psychosocial sequelae of continued seizures in children Engel, et al
12 Practice Parameters: TLE Surgery Surgical efficacy compared to results from randomized clinical trials of AEDs Same patients with intractable partial epilepsy Responder rate (50% reduction of seizure frequency) of 50% is a good response Few patients rendered seizure-free Best results: VGB 6000 mg/d: 54%RR Most AEDs lower RR Vagal Nerve Stimulator: 30-50% RR at 1 year Temporal Lobectomy Presurgical Evaluation Routine EEG MRI head seizure protocol Long-term EEG monitoring Visual perimetry Neuropsychometry Sodium amobarbital study 12

13 Temporal Lobe Epilepsy Complex Partial Seizure 13
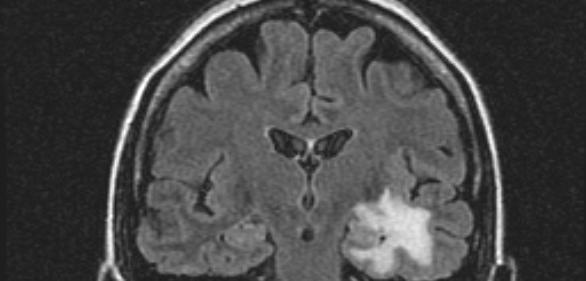
14 Imaging in Epilepsy Surgically Remediable Syndromes Lesional epilepsy: tumor, vascular anomaly, malformation of cortical development Structural MRI Medial temporal lobe epilepsy: mesial temporal poa sceoss sclerosis Structural MRI, PET CT vs MRI CT Neonate <2 yr Acute insult MRI incompatible Acute hemorrhage Ca +2 MRI Partial seizure any age Focal fixed deficit Loss of prior control Resolution/details Axis variable T2 2D GRE for Ca +2 or hemosiderin Wieshmann,



15 Standard MRI vs Epilepsy Protocol: Surgical Patients (n=90) Specificity Sensitivity % % Non-expert reader 22 _ Expert reader, standard MRI 40 _ Epilepsy protocol 89 >90 von Oertzen, et al

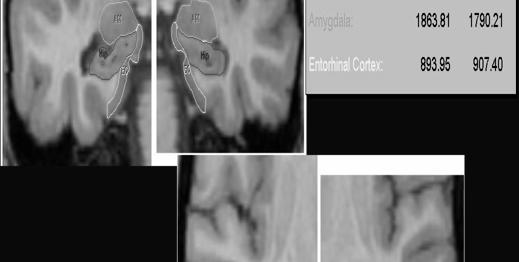
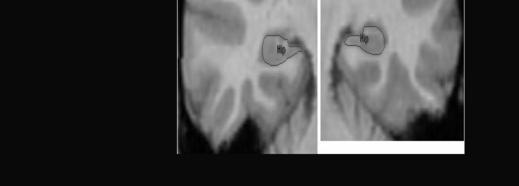

16 Amygdala Entorhinal Cortex 16


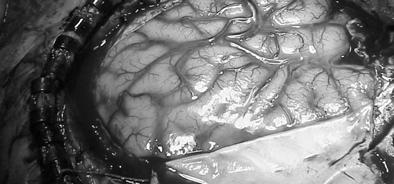

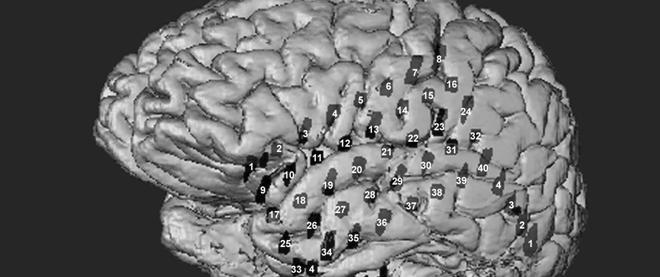
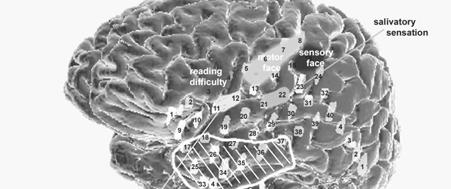

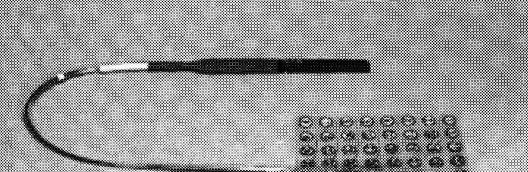
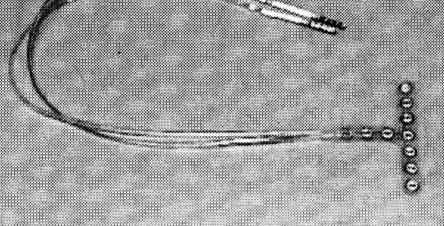
17 Long Term Intracranial Monitoring. Subdural Grid Implantation: Functional Brain Monitoring: 17


18 Location of Temporal Speech Areas Temporal Lobectomy Concordant MRI, EEG Unilateral hippocampal atrophy Unilateral epileptiform discharges 94% achieve an excellent outcome 18
19 Epilepsy Surgery Comparative Study NEJM August 2, 2001 Randomized controlled study 80 pts with TLE London, Ontario, Canada Surgery effective (p< 0.001) 001) QOL favors surgery (p< 0.001) Wiebe, et al Temporal Lobectomy Efficacy Sperling et al. (Phil., PA) JAMA 1996;276: Long-term operative outcome (5 yrs) 62 of 89 pts (70%) seizure-free 18 of 89 pts (20%) significantly improved 19
20 Temporal Lobectomy Operative Outcome Radhakrishnan et al. (Mayo) Neurology 1998;51: Excellent outcome: 134 (77%) Seizure-free: 120 (69%) Operative complication: 2 (1%) Epilepsy Surgery Extratemporal Non-lesional MRI is normal Limitations of ictal EEG Less favorable outcome Increased morbidity 20
21 Frontal Lobectomy Operative Outcome Mosewich et al. (Mayo) Epilepsia 2000;41: patients Excellent outcome: 59% Abnormal MRI: 72% Normal MRI: 41% Surgical Decision-Making Conclusions A marvelous time to treat epilepsy p So many medical and surgical treatment options The pool of truly intractable seizure patients is actually getting smaller As few as 20% of patients may not achieve complete or almost complete control with current interventions 21
22 Longer Term Follow-up and AED Drug Withdrawal Lowe, et al., Epilepsia 2004 Mar 50 consecutive patients with MTS Mean F/U = 5.8 yrs 82% seizure free at 1 year 76% seizure free at 2 yrs 64% seizure free at 5 yrs No further recurrence beyond 5 yrs 29% of recurrence associated with withdrawal of meds Quality of Life Outcome Spencer, et al Neurology, Dec 2003 Multicenter study; 396 cases Compared to pre-op baseline, at 3 months QOL, anxiety, depression improved p< QOL was highly correlated with seizure outcome 22
23 Cost-Effectiveness Wiebe, et al, Journal of Epilepsy, p patients, intention-to-treat analysis projected over 35 years By year 8, surgery was more cost-effective in direct costs than medical treatment This does not take into account the effect on QOL and indirect costs Corpus Callosum Division Corpus callosum division is a palliative procedure to improve the seizure control of patients with medically intractable epilepsy who have no localizable, single surgically resectable lesion Developed by Van Waganen in Rochester, New York, in 1939, refined by Wilson at Dartmouth in the 1970s, and others to the present 23
24 Corpus Callosum Division: Patient Outcomes % of patients with drop seizures (as a primary indication) achieve a 50% or greater reduction in seizures 21-67% of those with tonic-clonic seizures (as a primary indication) have a >50% reduction Seizure-free rates range from 2-5% Indications for Multiple Subpial Transection MST may be used alone or more commonly with cortical resection MST is used when the epileptogenic zone originates in or overlaps eloquent cortex where a resection is precluded do to the expected functional loss Eloquent cortex includes primary sensorimotor cortex and speech cortex 24
25 Technique of MST Author, Year Efficacy of MST: Worldwide No. of Patients Significant Improvement Only MST MST & RES MST Only No Worthwhile Improvement MST & RES No. of Patients Neurologic Complications Shimizu et al Sawhney et al Zonghui, a - 18 a Wyler et al Mild motor (1) Hufnagel et al Pacia, Rougier et al Patil et al Rush Epilepsy Center TOTAL MST=multiple subpial transection; RES=resection a In this study, it was not clear whether MST alone versus MST-resection was performed. Type (No. of Patients) Mild speech deficits (2); mild motor deficits (3); overt speech deficits (2) Mild dysnomia (7); moderate dysphasia (1) loss of proprioception in hand (1) Permanent (7); transient (8); sensorimotor (13) 25
 Trial Currently FDA trial ongoing at Rush Sponsored by Medtronic Vagal Nerve Stimulation (VNS): FDAapproved for adjunctive treatment of epilepsy VNS Therapy Automatic intermittent stimulation")
26 Neurostimulation for Epilepsy Responsive Neurostimulation (RNS) Trial Currently FDA trial ongoing at Rush Sponsored by Neuropace Stimulation of the Anterior Nucleus of the Thalamus for Epilepsy (SANTE) Trial Currently FDA trial ongoing at Rush Sponsored by Medtronic Vagal Nerve Stimulation (VNS): FDAapproved for adjunctive treatment of epilepsy VNS Therapy Automatic intermittent stimulation Magnet use allows patient/caregiver Mild electrical pulses applied to the left vagus nerve in the neck send signals to the brain On-demand stimulation On-demand side effect control Simple in-office programming Assured compliance 26
27 Clinical Use: VNS Maximize current load Stimulation intensity (2-3 ma) On time (30 sec) Off time (1.8 min) Delay in maximal benefit months Decrease SE by decreasing stimulation frequency from 30Hz to 20Hz Clinical Impact: VNS Rush Series over 200 patients At 6 months ~ 35% responder rate At 1 year ~ 46% responder rate Postictal state decreased in the majority Severity of seizures improved in the majority Mood improved in the majority 27
28 Future Cortical stimulation Deep brain stimulation (DBS) Gamma knife (GK) Responsive Neurostimulation: RNS Feasibility Clinical Trial Ten epilepsy p centers in US Patients who are not surgical candidates due to the presence of 2 independent epileptic foci or where the epileptic foci involves eloquent cortex that cannot be resected due to unacceptable deficits Closed-loop system that stimulates only when the recognized pre-programmed pattern is recorded; implanted brain defibrillator 28


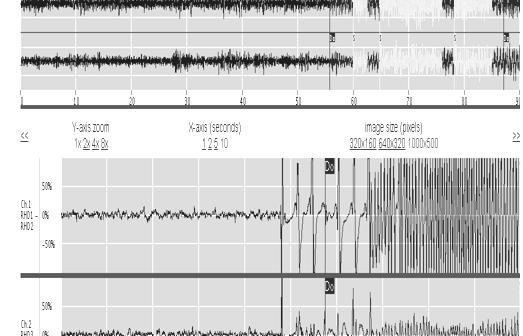
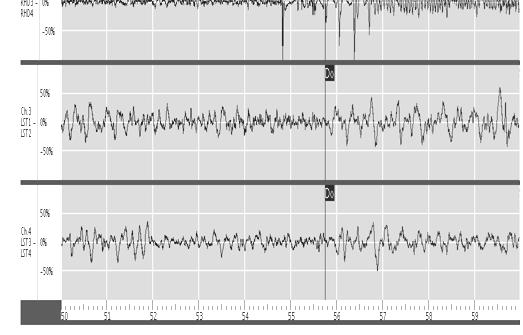
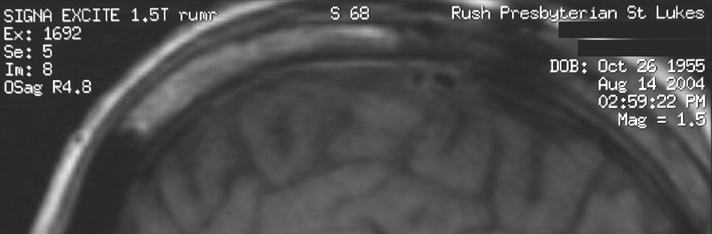
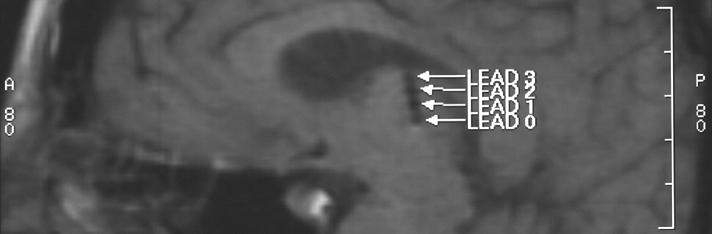
29 CT Scan Showing the Implanted Stimulator and Intracerebral Electrodes Right Sided Seizure with No Stimulation 29
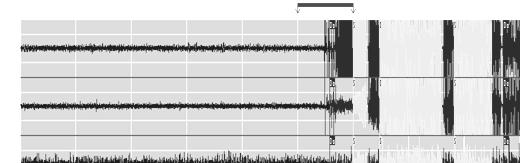
30 Left-sided seizure detected by subdural electrodes Comparison of the ictal EEG response to increased therapeutic stimulation from 2.5 to4.5 ma Response to 2.5 ma Electrographic seizure that progressed to clinical CPS then GTC Response to 4.5 ma Electrographic and clinical response to therapeutic stimulation SANTE Study Design Multi-center Prospective Randomized Double-blind Parallel design 30
31 31
32 Radiosurgical Treatment Conformal radiation directed at temporal portion of the amygdala, the anterior 2 cm of the hippocampus and adjacent parahippocampal gyrus Total volume within 50% isodose line between 5.5 and 7.5 cc Treatment isocenters: 2-6 Potential Risk of Radiosurgery for Epilepsy Risk of ongoing g seizures while waiting for radiosurgical effect (including sudden death from epilepsy) Neuropsychological deficits Language Memory Visual field defects Quadrantanopsia (relatively likely) Homonymous hemianopsia (in Europe with > 8 cc volume) 32

33 One Year Post Radiosurgery Two Years Post Radiosurgery 33
34 Typical Clinical Response Initial increase in auras with simultaneous decrease in complex partial seizures Headaches Radiological changes Conclusions Surgical treatment of epilepsy is effective and cost-effective ti in the appropriate patient t Evidenced-based data suggested that surgery is more effective than best medical care for TLE Radiosurgery appears effective for TLE Thalamic stimulation for multifocal epilepsy is being evaluated Responsive neurostimulation is an exciting novel treatment of intractable focal epilepsy when two or more foci are present; its clinical utility is being evaluated 34
Treatment of Refractory Epilepsy: Pre-surgical Evaluation, Surgical Options, and Neurostimulation
 Treatment of Refractory Epilepsy: Pre-surgical Evaluation, Surgical Options, and Neurostimulation Michael C. Smith, MD Director, Rush Epilepsy Center Professor and Senior Attending Neurologist Rush University
Treatment of Refractory Epilepsy: Pre-surgical Evaluation, Surgical Options, and Neurostimulation Michael C. Smith, MD Director, Rush Epilepsy Center Professor and Senior Attending Neurologist Rush University
PRESURGICAL EVALUATION. ISLAND OF COS Hippocrates: On the Sacred Disease. Disclosure Research-Educational Grants. Patients with seizure disorders
 PRESURGICAL EVALUATION Patients with seizure disorders Gregory D. Cascino, MD Mayo Clinic Disclosure Research-Educational Grants Mayo Foundation Neuro Pace, Inc. American Epilepsy Society American Academy
PRESURGICAL EVALUATION Patients with seizure disorders Gregory D. Cascino, MD Mayo Clinic Disclosure Research-Educational Grants Mayo Foundation Neuro Pace, Inc. American Epilepsy Society American Academy
EPILEPSY. New Ideas about an Old Disease. Gregory D. Cascino, MD
 EPILEPSY New Ideas about an Old Disease Gregory D. Cascino, MD Disclosure Research-Educational Grants Neuro Pace, Inc. American Epilepsy Society American Academy of Neurology Neurology (Associate Editor)
EPILEPSY New Ideas about an Old Disease Gregory D. Cascino, MD Disclosure Research-Educational Grants Neuro Pace, Inc. American Epilepsy Society American Academy of Neurology Neurology (Associate Editor)
Epilepsy Surgery: Who should be considered? How will patients do? Bassel Abou-Khalil, M.D.
 Epilepsy Surgery: Who should be considered? How will patients do? Bassel Abou-Khalil, M.D. Disclosures none Self-assessment questions Q1- Which qualify for drug resistance in focal epilepsy? A. Failure
Epilepsy Surgery: Who should be considered? How will patients do? Bassel Abou-Khalil, M.D. Disclosures none Self-assessment questions Q1- Which qualify for drug resistance in focal epilepsy? A. Failure
9/30/2016. Advances in Epilepsy Surgery. Epidemiology. Epidemiology
 Advances in Epilepsy Surgery George Jallo, M.D. Director, Institute for Brain Protection Sciences Johns Hopkins All Children s Hospital St Petersburg, Florida Epidemiology WHO lists it as the second most
Advances in Epilepsy Surgery George Jallo, M.D. Director, Institute for Brain Protection Sciences Johns Hopkins All Children s Hospital St Petersburg, Florida Epidemiology WHO lists it as the second most
Neuromodulation in Epilepsy. Gregory C. Mathews, M.D., Ph.D.
 Neuromodulation in Epilepsy Gregory C. Mathews, M.D., Ph.D. Disclosure There are no disclosures to share with regards to this presentation. Epilepsy Basics What is epilepsy? Partial versus generalized
Neuromodulation in Epilepsy Gregory C. Mathews, M.D., Ph.D. Disclosure There are no disclosures to share with regards to this presentation. Epilepsy Basics What is epilepsy? Partial versus generalized
Epilepsy. Hyunmi Choi, M.D., M.S. Columbia Comprehensive Epilepsy Center The Neurological Institute. Seizure
 Epilepsy Hyunmi Choi, M.D., M.S. Columbia Comprehensive Epilepsy Center The Neurological Institute Seizure Symptom Transient event Paroxysmal Temporary physiologic dysfunction Caused by self-limited, abnormal,
Epilepsy Hyunmi Choi, M.D., M.S. Columbia Comprehensive Epilepsy Center The Neurological Institute Seizure Symptom Transient event Paroxysmal Temporary physiologic dysfunction Caused by self-limited, abnormal,
Epilepsy. Seizures and Epilepsy. Buccal Midazolam vs. Rectal Diazepam for Serial Seizures. Epilepsy and Seizures 6/18/2008
 Seizures and Epilepsy Paul Garcia, M.D. UCSF Epilepsy Epileptic seizure: the physical manifestation of aberrant firing of brain cells Epilepsy: the tendency to recurrent, unprovoked epileptic seizures
Seizures and Epilepsy Paul Garcia, M.D. UCSF Epilepsy Epileptic seizure: the physical manifestation of aberrant firing of brain cells Epilepsy: the tendency to recurrent, unprovoked epileptic seizures
5/22/2009. Pediatric Neurosurgery Pediatric Neurology Neuroradiology Neurophysiology Neuropathology Neuropsychology
 Current Surgical Treatment Strategies for the Management of Pediatric Epilepsy University of California, San Francisco Department of Neurological Surgery San Francisco, California Kurtis Ian Auguste, M.D.
Current Surgical Treatment Strategies for the Management of Pediatric Epilepsy University of California, San Francisco Department of Neurological Surgery San Francisco, California Kurtis Ian Auguste, M.D.
Treatment of Epilepsy with Implanted Devices: What Are Indications and Benefits? 11/30/2012
 Treatment of Epilepsy with Implanted Devices: What Are Indications and Benefits? 11/30/2012 Barbara C. Jobst, MD Dartmouth-Hitchcock Epilepsy Center Geisel School of Medicine at Dartmouth American Epilepsy
Treatment of Epilepsy with Implanted Devices: What Are Indications and Benefits? 11/30/2012 Barbara C. Jobst, MD Dartmouth-Hitchcock Epilepsy Center Geisel School of Medicine at Dartmouth American Epilepsy
Surgical Modalities for Epilepsy Treatment. C.J. Bui, MD, FAANS Ochsner Neuroscience Symposium 2016
 Surgical Modalities for Epilepsy Treatment C.J. Bui, MD, FAANS Ochsner Neuroscience Symposium 2016 Conflict of Interest Nothing to disclose Surgical Modalities Diagnostic Subdural Grids Depth Electrodes
Surgical Modalities for Epilepsy Treatment C.J. Bui, MD, FAANS Ochsner Neuroscience Symposium 2016 Conflict of Interest Nothing to disclose Surgical Modalities Diagnostic Subdural Grids Depth Electrodes
High Resolution Ictal SPECT: Enhanced Epileptic Source Targeting?
 High Resolution Ictal SPECT: Enhanced Epileptic Source Targeting? Marvin A Rossi MD, PhD RUSH Epilepsy Center Research Lab http://www.synapticom.net Chicago, IL USA Medically-Refractory Epilepsy 500,000-800,000
High Resolution Ictal SPECT: Enhanced Epileptic Source Targeting? Marvin A Rossi MD, PhD RUSH Epilepsy Center Research Lab http://www.synapticom.net Chicago, IL USA Medically-Refractory Epilepsy 500,000-800,000
Accepted Manuscript. Editorial. Responsive neurostimulation for epilepsy: more than stimulation. Jayant N. Acharya
 Accepted Manuscript Editorial Responsive neurostimulation for epilepsy: more than stimulation Jayant N. Acharya PII: S2467-981X(18)30022-2 DOI: https://doi.org/10.1016/j.cnp.2018.06.002 Reference: CNP
Accepted Manuscript Editorial Responsive neurostimulation for epilepsy: more than stimulation Jayant N. Acharya PII: S2467-981X(18)30022-2 DOI: https://doi.org/10.1016/j.cnp.2018.06.002 Reference: CNP
Epilepsy surgery. Loránd Eross. National Institute of Clinical Neurosciences. Semmelweis University, 2018.
 Epilepsy surgery Loránd Eross National Institute of Clinical Neurosciences Semmelweis University, 2018. Epilepsy surgery Medicaltreatment Seizure free:70% Surgical treatment Seizure fee:15% Neuromodulation
Epilepsy surgery Loránd Eross National Institute of Clinical Neurosciences Semmelweis University, 2018. Epilepsy surgery Medicaltreatment Seizure free:70% Surgical treatment Seizure fee:15% Neuromodulation
Surgery for Medically Refractory Focal Epilepsy
 Surgery for Medically Refractory Focal Epilepsy Seth F Oliveria, MD PhD The Oregon Clinic Neurosurgery Director of Functional Neurosurgery: Providence Brain and Spine Institute Portland, OR Providence
Surgery for Medically Refractory Focal Epilepsy Seth F Oliveria, MD PhD The Oregon Clinic Neurosurgery Director of Functional Neurosurgery: Providence Brain and Spine Institute Portland, OR Providence
EMG, EEG, and Neurophysiology in Clinical Practice
 Mayo School of Continuous Professional Development EMG, EEG, and Neurophysiology in Clinical Practice Matthew T. Hoerth, M.D. Ritz-Carlton, Amelia Island, Florida January 29-February 4, 2017 2016 MFMER
Mayo School of Continuous Professional Development EMG, EEG, and Neurophysiology in Clinical Practice Matthew T. Hoerth, M.D. Ritz-Carlton, Amelia Island, Florida January 29-February 4, 2017 2016 MFMER
Candidates for Epilepsy Surgery. Presurgical Evaluation. Presurgical Evaluation. Presurgical Evaluation. Presurgical Evaluation 8/27/2017
 PresurgicalEpilepsy Eval: A multidisciplinary approach to intractable epilepsy Tayard Desudchit MD Faculty Of Medicine Chulalongkorn U. Candidates for Epilepsy Surgery Persistent seizures despite appropriate
PresurgicalEpilepsy Eval: A multidisciplinary approach to intractable epilepsy Tayard Desudchit MD Faculty Of Medicine Chulalongkorn U. Candidates for Epilepsy Surgery Persistent seizures despite appropriate
Epilepsy: diagnosis and treatment. Sergiusz Jóźwiak Klinika Neurologii Dziecięcej WUM
 Epilepsy: diagnosis and treatment Sergiusz Jóźwiak Klinika Neurologii Dziecięcej WUM Definition: the clinical manifestation of an excessive excitation of a population of cortical neurons Neurotransmitters:
Epilepsy: diagnosis and treatment Sergiusz Jóźwiak Klinika Neurologii Dziecięcej WUM Definition: the clinical manifestation of an excessive excitation of a population of cortical neurons Neurotransmitters:
Neuromodulation in Dravet Syndrome. Eric BJ Segal, MD Director of Pediatric Epilepsy Northeast Regional Epilepsy Group Hackensack, New Jersey
 Neuromodulation in Dravet Syndrome Eric BJ Segal, MD Director of Pediatric Epilepsy Northeast Regional Epilepsy Group Hackensack, New Jersey What is neuromodulation? Seizures are caused by synchronized
Neuromodulation in Dravet Syndrome Eric BJ Segal, MD Director of Pediatric Epilepsy Northeast Regional Epilepsy Group Hackensack, New Jersey What is neuromodulation? Seizures are caused by synchronized
Responsive Neurostimulation for the Treatment of Refractory Partial Epilepsy. Summary
 Page: 1 of 12 Last Review Status/Date: March 2015 Refractory Partial Epilepsy Summary Responsive neurostimulation (RNS) for the treatment of epilepsy involves the use of 1 or more implantable electric
Page: 1 of 12 Last Review Status/Date: March 2015 Refractory Partial Epilepsy Summary Responsive neurostimulation (RNS) for the treatment of epilepsy involves the use of 1 or more implantable electric
Approximately 70% of childhood SURGICAL TREATMENTS FOR PEDIATRIC EPILEPSY PROCEEDINGS. Ronald P. Lesser, MD KEY POINTS
 ASIM May p153-158 5/14/01 9:19 AM Page 153 SURGICAL TREATMENTS FOR PEDIATRIC EPILEPSY Ronald P. Lesser, MD KEY POINTS Most children with epilepsy refractory to drugs can improve with surgery Temporal lobe
ASIM May p153-158 5/14/01 9:19 AM Page 153 SURGICAL TREATMENTS FOR PEDIATRIC EPILEPSY Ronald P. Lesser, MD KEY POINTS Most children with epilepsy refractory to drugs can improve with surgery Temporal lobe
EPILEPSY SURGERY- SURGICAL PROCEDURES
 EPILEPSY SURGERY- SURGICAL PROCEDURES When to consider epilepsy surgery? Persistent Seizures despite adequate pharmacological treatment Drug resistant epilepsy may be defined as failure of adequate trials
EPILEPSY SURGERY- SURGICAL PROCEDURES When to consider epilepsy surgery? Persistent Seizures despite adequate pharmacological treatment Drug resistant epilepsy may be defined as failure of adequate trials
The Changing Surgical Landscape in Kids
 The Changing Surgical Landscape in Kids December 7, 2013 Howard L. Weiner, MD NYU Langone Medical Center American Epilepsy Society Annual Meeting Disclosure none American Epilepsy Society 2013 Annual Meeting
The Changing Surgical Landscape in Kids December 7, 2013 Howard L. Weiner, MD NYU Langone Medical Center American Epilepsy Society Annual Meeting Disclosure none American Epilepsy Society 2013 Annual Meeting
Epilepsy T.I.A. Cataplexy. Nonepileptic seizure. syncope. Dystonia. Epilepsy & other attack disorders Overview
 : Clinical presentation and management Markus Reuber Professor of Clinical Neurology Academic Neurology Unit University of Sheffield, Royal Hallamshire Hospital. Is it epilepsy? Overview Common attack
: Clinical presentation and management Markus Reuber Professor of Clinical Neurology Academic Neurology Unit University of Sheffield, Royal Hallamshire Hospital. Is it epilepsy? Overview Common attack
SEIZURE OUTCOME AFTER EPILEPSY SURGERY
 SEIZURE OUTCOME AFTER EPILEPSY SURGERY Prakash Kotagal, M.D. Head, Pediatric Epilepsy Cleveland Clinic Epilepsy Center LEFT TEMPORAL LOBE ASTROCYTOMA SEIZURE OUTCOME 1 YEAR AFTER EPILEPSY SURGERY IN ADULTS
SEIZURE OUTCOME AFTER EPILEPSY SURGERY Prakash Kotagal, M.D. Head, Pediatric Epilepsy Cleveland Clinic Epilepsy Center LEFT TEMPORAL LOBE ASTROCYTOMA SEIZURE OUTCOME 1 YEAR AFTER EPILEPSY SURGERY IN ADULTS
Intracranial Studies Of Human Epilepsy In A Surgical Setting
 Intracranial Studies Of Human Epilepsy In A Surgical Setting Department of Neurology David Geffen School of Medicine at UCLA Presentation Goals Epilepsy and seizures Basics of the electroencephalogram
Intracranial Studies Of Human Epilepsy In A Surgical Setting Department of Neurology David Geffen School of Medicine at UCLA Presentation Goals Epilepsy and seizures Basics of the electroencephalogram
Multimodal Imaging in Extratemporal Epilepsy Surgery
 Open Access Case Report DOI: 10.7759/cureus.2338 Multimodal Imaging in Extratemporal Epilepsy Surgery Christian Vollmar 1, Aurelia Peraud 2, Soheyl Noachtar 1 1. Epilepsy Center, Dept. of Neurology, University
Open Access Case Report DOI: 10.7759/cureus.2338 Multimodal Imaging in Extratemporal Epilepsy Surgery Christian Vollmar 1, Aurelia Peraud 2, Soheyl Noachtar 1 1. Epilepsy Center, Dept. of Neurology, University
Surgery in temporal lobe epilepsy patients without cranial MRI lateralization
 Acta neurol. belg., 2006, 106, 9-14 Surgery in temporal lobe epilepsy patients without cranial MRI lateralization Y. B. GOMCELI 1, A. ERDEM 2, E. BILIR 3, G. KUTLU 1, S. KURT 4, E. ERDEN 5,A. KARATAS 2,
Acta neurol. belg., 2006, 106, 9-14 Surgery in temporal lobe epilepsy patients without cranial MRI lateralization Y. B. GOMCELI 1, A. ERDEM 2, E. BILIR 3, G. KUTLU 1, S. KURT 4, E. ERDEN 5,A. KARATAS 2,
Paediatric Epilepsy Update N o r e e n Te a h a n canp C o l e t t e H u r l e y C N S E p i l e p s y
 Paediatric Epilepsy Update 2018 N o r e e n Te a h a n canp C o l e t t e H u r l e y C N S E p i l e p s y Epilepsy Service CUH ~550 children New diagnosis-education, support, clinic follow up Epilepsy
Paediatric Epilepsy Update 2018 N o r e e n Te a h a n canp C o l e t t e H u r l e y C N S E p i l e p s y Epilepsy Service CUH ~550 children New diagnosis-education, support, clinic follow up Epilepsy
Neuromodulation in Epilepsy. Frederick Langendorf,, MD Department of Neurology Univ of MN and Hennepin Co Medical Center June 4, 2007
 Neuromodulation in Epilepsy Frederick Langendorf,, MD Department of Neurology Univ of MN and Hennepin Co Medical Center June 4, 2007 disclosures No financial conflicts-of of-interest Epilepsy the problem
Neuromodulation in Epilepsy Frederick Langendorf,, MD Department of Neurology Univ of MN and Hennepin Co Medical Center June 4, 2007 disclosures No financial conflicts-of of-interest Epilepsy the problem
Epilepsy Research: SLATE
 Epilepsy Research: SLATE Jason M. Schwalb, MD, FAANS, FACS Clinical Associate Professor of Neurosurgery Surgical Director, Movement Disorder & Comprehensive Epilepsy Centers Research Scientist, Center
Epilepsy Research: SLATE Jason M. Schwalb, MD, FAANS, FACS Clinical Associate Professor of Neurosurgery Surgical Director, Movement Disorder & Comprehensive Epilepsy Centers Research Scientist, Center
Clinical Commissioning Policy: Deep Brain Stimulation for Refractory Epilepsy (all ages) NHS England Reference: P
 NHS England Reference: P") Clinical Commissioning Policy: Deep Brain Stimulation for Refractory Epilepsy (all ages) NHS England Reference: 1736P NHS England INFORMATION READER BOX Directorate Medical Operations and Information
Clinical Commissioning Policy: Deep Brain Stimulation for Refractory Epilepsy (all ages) NHS England Reference: 1736P NHS England INFORMATION READER BOX Directorate Medical Operations and Information
Do seizures beget seizures?
 Does MTLE cause progressive neurocognitive damage? Andrew Bleasel Westmead Do seizures beget seizures? The tendency of the disease is toward self-perpetuation; each attack facilitates occurrence of another
Does MTLE cause progressive neurocognitive damage? Andrew Bleasel Westmead Do seizures beget seizures? The tendency of the disease is toward self-perpetuation; each attack facilitates occurrence of another
Diagnosing Complicated Epilepsy: Mapping of the Epileptic Circuitry. Michael R. Sperling, M.D. Thomas Jefferson University Philadelphia, PA
 Diagnosing Complicated Epilepsy: Mapping of the Epileptic Circuitry Michael R. Sperling, M.D. Thomas Jefferson University Philadelphia, PA Overview Definition of epileptic circuitry Methods of mapping
Diagnosing Complicated Epilepsy: Mapping of the Epileptic Circuitry Michael R. Sperling, M.D. Thomas Jefferson University Philadelphia, PA Overview Definition of epileptic circuitry Methods of mapping
EPILEPSY SURGERY EVALUATION IN ADULTS WITH SCALP VIDEO-EEG MONITORING. Meriem Bensalem-Owen, MD University of Kentucky
 EPILEPSY SURGERY EVALUATION IN ADULTS WITH SCALP VIDEO-EEG MONITORING Meriem Bensalem-Owen, MD University of Kentucky DISCLOSURES Received grants for sponsored research as investigator from: UCB Eisai
EPILEPSY SURGERY EVALUATION IN ADULTS WITH SCALP VIDEO-EEG MONITORING Meriem Bensalem-Owen, MD University of Kentucky DISCLOSURES Received grants for sponsored research as investigator from: UCB Eisai
Early seizure propagation from the occipital lobe to medial temporal structures and its surgical implication
 Original article Epileptic Disord 2008; 10 (4): 260-5 Early seizure propagation from the occipital lobe to medial temporal structures and its surgical implication Naotaka Usui, Tadahiro Mihara, Koichi
Original article Epileptic Disord 2008; 10 (4): 260-5 Early seizure propagation from the occipital lobe to medial temporal structures and its surgical implication Naotaka Usui, Tadahiro Mihara, Koichi
Nonlesional Neocortical Epilepsy: Benefits v Risk December 8, 2013
 Nonlesional Neocortical Epilepsy: Benefits v Risk December 8, 2013 Orrin Devinsky, MD NYU Langone School of Medicine American Epilepsy Society Annual Meeting Disclosure Name of Commercial Interest None
Nonlesional Neocortical Epilepsy: Benefits v Risk December 8, 2013 Orrin Devinsky, MD NYU Langone School of Medicine American Epilepsy Society Annual Meeting Disclosure Name of Commercial Interest None
The American Approach to Depth Electrode Insertion December 4, 2012
 The American Approach to Depth Electrode Insertion December 4, 2012 Jonathan Miller, MD Director, Epilepsy Surgery University Hospitals Case Medical Center/Case Western Reserve University Cleveland, Ohio
The American Approach to Depth Electrode Insertion December 4, 2012 Jonathan Miller, MD Director, Epilepsy Surgery University Hospitals Case Medical Center/Case Western Reserve University Cleveland, Ohio
Epilepsy & Functional Neurosurgery
 Epilepsy & Functional Neurosurgery An Introduction The LSU-Shreveport Department of Neurosurgery Presenting Authors: Neurosurgery Residents & Faculty Epilepsy Neurosurgery What is a seizure? continuous
Epilepsy & Functional Neurosurgery An Introduction The LSU-Shreveport Department of Neurosurgery Presenting Authors: Neurosurgery Residents & Faculty Epilepsy Neurosurgery What is a seizure? continuous
Interictal High Frequency Oscillations as Neurophysiologic Biomarkers of Epileptogenicity
 Interictal High Frequency Oscillations as Neurophysiologic Biomarkers of Epileptogenicity December 10, 2013 Joyce Y. Wu, MD Associate Professor Division of Pediatric Neurology David Geffen School of Medicine
Interictal High Frequency Oscillations as Neurophysiologic Biomarkers of Epileptogenicity December 10, 2013 Joyce Y. Wu, MD Associate Professor Division of Pediatric Neurology David Geffen School of Medicine
Presurgical Evaluation before Epilepsy Surgery
 Presurgical Evaluation before Epilepsy Surgery Epilepsy Course for Neurology Resident 2015 Kanjana Unnwongse- Wehner, MD Prasat Neurological Epilepsy Center Facts About Epilepsy & Surgery Localization-related
Presurgical Evaluation before Epilepsy Surgery Epilepsy Course for Neurology Resident 2015 Kanjana Unnwongse- Wehner, MD Prasat Neurological Epilepsy Center Facts About Epilepsy & Surgery Localization-related
ChosingPhase 2 Electrodes
 ChosingPhase 2 Electrodes ACNS Course ECoG/Invasive EEG Houston, February 4 th, 2015 Stephan Schuele, MD, MPH Comprehensive Epilepsy Center Northwestern Memorial Hospital Northwestern University, Feinberg
ChosingPhase 2 Electrodes ACNS Course ECoG/Invasive EEG Houston, February 4 th, 2015 Stephan Schuele, MD, MPH Comprehensive Epilepsy Center Northwestern Memorial Hospital Northwestern University, Feinberg
Scalp EEG Findings in Temporal Lobe Epilepsy
 Scalp EEG Findings in Temporal Lobe Epilepsy Seyed M Mirsattari M.D., Ph.D., F.R.C.P.(C) Assistant Professor Depts. of CNS, Medical Biophysics, Medical Imaging, and Psychology University of Western Ontario
Scalp EEG Findings in Temporal Lobe Epilepsy Seyed M Mirsattari M.D., Ph.D., F.R.C.P.(C) Assistant Professor Depts. of CNS, Medical Biophysics, Medical Imaging, and Psychology University of Western Ontario
The Surgical Treatment of Epilepsy
 The Surgical Treatment of Epilepsy Jeffrey S. Schweitzer, MD, PhD Kaiser Los Angeles Medical Center Division of Restorative Neurosurgery Ancient craniotomy When Cao started complaining about splitting
The Surgical Treatment of Epilepsy Jeffrey S. Schweitzer, MD, PhD Kaiser Los Angeles Medical Center Division of Restorative Neurosurgery Ancient craniotomy When Cao started complaining about splitting
Case reports functional imaging in epilepsy
 Seizure 2001; 10: 157 161 doi:10.1053/seiz.2001.0552, available online at http://www.idealibrary.com on Case reports functional imaging in epilepsy MARK P. RICHARDSON Medical Research Council Fellow, Institute
Seizure 2001; 10: 157 161 doi:10.1053/seiz.2001.0552, available online at http://www.idealibrary.com on Case reports functional imaging in epilepsy MARK P. RICHARDSON Medical Research Council Fellow, Institute
Extratemporal Nonlesional Epilepsy: Grids and Strips 11/30/2012
 Extratemporal Nonlesional Epilepsy: Grids and Strips 11/30/2012 Ashesh D. Mehta, M.D., Ph.D. Department of Neurosurgery Hofstra North Shore LIJ School of Medicine American Epilepsy Society Annual Meeting
Extratemporal Nonlesional Epilepsy: Grids and Strips 11/30/2012 Ashesh D. Mehta, M.D., Ph.D. Department of Neurosurgery Hofstra North Shore LIJ School of Medicine American Epilepsy Society Annual Meeting
Epilepsies of Childhood: An Over-view of Treatment 2 nd October 2018
 Epilepsies of Childhood: An Over-view of Treatment 2 nd October 2018 Dr Sophia Varadkar MRCPI, PhD Consultant Paediatric Neurologist and Honorary Senior Lecturer Great Ormond Street Hospital for Children
Epilepsies of Childhood: An Over-view of Treatment 2 nd October 2018 Dr Sophia Varadkar MRCPI, PhD Consultant Paediatric Neurologist and Honorary Senior Lecturer Great Ormond Street Hospital for Children
Epilepsy Surgery, Imaging, and Intraoperative Neuromonitoring: Surgical Perspective
 Epilepsy Surgery, Imaging, and Intraoperative Neuromonitoring: Surgical Perspective AC Duhaime, M.D. Director, Pediatric Neurosurgery, Massachusetts General Hospital Professor, Neurosurgery, Harvard Medical
Epilepsy Surgery, Imaging, and Intraoperative Neuromonitoring: Surgical Perspective AC Duhaime, M.D. Director, Pediatric Neurosurgery, Massachusetts General Hospital Professor, Neurosurgery, Harvard Medical
Pediatric Epilepsy Surgery. W. Donald Shields, MD Emeritus Professor of Neurology and Pediatrics David Geffen School of Medicine at UCLA
 Pediatric Epilepsy Surgery W. Donald Shields, MD Emeritus Professor of Neurology and Pediatrics David Geffen School of Medicine at UCLA PEDIATRIC EPILEPSY SURGERY A THING OF BEAUTY IF DONE RIGHT PEDIATRIC
Pediatric Epilepsy Surgery W. Donald Shields, MD Emeritus Professor of Neurology and Pediatrics David Geffen School of Medicine at UCLA PEDIATRIC EPILEPSY SURGERY A THING OF BEAUTY IF DONE RIGHT PEDIATRIC
SURGICAL MANAGEMENT OF DRUG-RESISTANT FOCAL EPILEPSY
 SURGICAL MANAGEMENT OF DRUG-RESISTANT FOCAL EPILEPSY Gregory D. Cascino, MD, FAAN Epilepsy surgery is underutilized in patients with focal seizures refractory to appropriate antiepileptic drug (AED) trials
SURGICAL MANAGEMENT OF DRUG-RESISTANT FOCAL EPILEPSY Gregory D. Cascino, MD, FAAN Epilepsy surgery is underutilized in patients with focal seizures refractory to appropriate antiepileptic drug (AED) trials
The relevance of somatosensory auras in refractory temporal lobe epilepsies
 BRIEF COMMUNICATION The relevance of somatosensory auras in refractory temporal lobe epilepsies Ghazala Perven, Ruta Yardi, Juan Bulacio, Imad Najm, William Bingaman, Jorge Gonzalez-Martinez, and Lara
BRIEF COMMUNICATION The relevance of somatosensory auras in refractory temporal lobe epilepsies Ghazala Perven, Ruta Yardi, Juan Bulacio, Imad Najm, William Bingaman, Jorge Gonzalez-Martinez, and Lara
Epilepsy 101. Overview of Treatment Georgette Smith, PhD, APRN, CPNP. American Epilepsy Society
 Epilepsy 101 Overview of Treatment Georgette Smith, PhD, APRN, CPNP American Epilepsy Society Overview of Treatment Rescue Therapies Non-Medication Therapies Epilepsy surgery Vagus nerve stimulation Dietary
Epilepsy 101 Overview of Treatment Georgette Smith, PhD, APRN, CPNP American Epilepsy Society Overview of Treatment Rescue Therapies Non-Medication Therapies Epilepsy surgery Vagus nerve stimulation Dietary
Invasive Evaluation for Epilepsy Surgery Lesional Cases NO DISCLOSURES. Mr. Johnson. Seizures at 29 Years of Age. Dileep Nair, MD Juan Bulacio, MD
 Invasive Evaluation for Epilepsy Surgery Lesional Cases NO DISCLOSURES Dileep Nair, MD Juan Bulacio, MD Mr. Johnson Seizures at 29 Years of Age Onset of seizures at 16 years of age bed wetting episodes
Invasive Evaluation for Epilepsy Surgery Lesional Cases NO DISCLOSURES Dileep Nair, MD Juan Bulacio, MD Mr. Johnson Seizures at 29 Years of Age Onset of seizures at 16 years of age bed wetting episodes
Faculty/Presenter Disclosure. Intracranial EEG Recording. Objectives. General Themes. Why invasive recordings? 6/27/2018
 CFPC CoI Templates: Slide 1 used in Faculty presentation only. Faculty/Presenter Disclosure Intracranial EEG Recording Faculty: Dr Richard S McLachlan Relationships with financial sponsors: None currently
CFPC CoI Templates: Slide 1 used in Faculty presentation only. Faculty/Presenter Disclosure Intracranial EEG Recording Faculty: Dr Richard S McLachlan Relationships with financial sponsors: None currently
Some epilepsy syndromes are known to be associated with more adverse cognitive consequences than others.
 1 Neuropsychology and Epilepsy David W. Loring, Ph.D. Departments of Neurology and Clinical & Health Psychology University of Florida Gainesville, Florida 32610-0236 0236 2 Factors Affecting Cognitive
1 Neuropsychology and Epilepsy David W. Loring, Ph.D. Departments of Neurology and Clinical & Health Psychology University of Florida Gainesville, Florida 32610-0236 0236 2 Factors Affecting Cognitive
Surgery Insight: surgical management of epilepsy
 Surgery Insight: surgical management of epilepsy Ruben Kuzniecky* and Orrin Devinsky SUMMARY Epilepsy surgery has been shown to be an effective treatment for patients with intractable epilepsy. The only
Surgery Insight: surgical management of epilepsy Ruben Kuzniecky* and Orrin Devinsky SUMMARY Epilepsy surgery has been shown to be an effective treatment for patients with intractable epilepsy. The only
Clinical Commissioning Policy: Deep Brain Stimulation for Refractory Epilepsy
 Clinical Commissioning Policy: Deep Brain Stimulation for Refractory Epilepsy Reference: NHS England xxx/x/x 1 Clinical Commissioning Policy: Deep Brain Stimulation for Refractory Epilepsy First published:
Clinical Commissioning Policy: Deep Brain Stimulation for Refractory Epilepsy Reference: NHS England xxx/x/x 1 Clinical Commissioning Policy: Deep Brain Stimulation for Refractory Epilepsy First published:
Epilepsy and EEG in Clinical Practice
 Mayo School of Professional Development Epilepsy and EEG in Clinical Practice November 10-12, 2016 Hard Rock Hotel at Universal Orlando Orlando, FL Course Directors Jeffrey Britton, MD and William Tatum,
Mayo School of Professional Development Epilepsy and EEG in Clinical Practice November 10-12, 2016 Hard Rock Hotel at Universal Orlando Orlando, FL Course Directors Jeffrey Britton, MD and William Tatum,
AMERICAN BOARD OF PSYCHIATRY AND NEUROLOGY, INC. SUBSPECIALTY CERTIFICATION EXAMINATION IN EPILEPSY MEDICINE
 SUBSPECIALTY CERTIFICATION EXAMINATION IN EPILEPSY MEDICINE 2014 Content Blueprint (November 26, 2012) Number of questions: 200 I. Classification 7 9% II. Routine EEG 16 20% III. Evaluation 22 26% IV.
SUBSPECIALTY CERTIFICATION EXAMINATION IN EPILEPSY MEDICINE 2014 Content Blueprint (November 26, 2012) Number of questions: 200 I. Classification 7 9% II. Routine EEG 16 20% III. Evaluation 22 26% IV.
Research Article Predictors of Postoperative Seizure Recurrence: A Longitudinal Study of Temporal and Extratemporal Resections
 Epilepsy Research and Treatment Volume 2016, Article ID 7982494, 7 pages http://dx.doi.org/10.1155/2016/7982494 Research Article Predictors of Postoperative Seizure Recurrence: A Longitudinal Study of
Epilepsy Research and Treatment Volume 2016, Article ID 7982494, 7 pages http://dx.doi.org/10.1155/2016/7982494 Research Article Predictors of Postoperative Seizure Recurrence: A Longitudinal Study of
Intracranial Stimulation Therapy for Epilepsy
 Neurotherapeutics: The Journal of the American Society for Experimental NeuroTherapeutics Intracranial Stimulation Therapy for Epilepsy Tara L. Skarpaas* and Martha J. Morrell* *NeuroPace, Inc., Mountain
Neurotherapeutics: The Journal of the American Society for Experimental NeuroTherapeutics Intracranial Stimulation Therapy for Epilepsy Tara L. Skarpaas* and Martha J. Morrell* *NeuroPace, Inc., Mountain
Therapeutic strategies in the choice of antiepileptic drugs
 Acta neurol. belg., 2002, 102, 6-10 Original articles Therapeutic strategies in the choice of antiepileptic drugs V. DE BORCHGRAVE, V. DELVAUX, M. DE TOURCHANINOFF, J.M. DUBRU, S. GHARIANI, Th. GRISAR,
Acta neurol. belg., 2002, 102, 6-10 Original articles Therapeutic strategies in the choice of antiepileptic drugs V. DE BORCHGRAVE, V. DELVAUX, M. DE TOURCHANINOFF, J.M. DUBRU, S. GHARIANI, Th. GRISAR,
Mesial temporal lobe epilepsy (TLE) with hippocampal
 with hippocampal") » This article has been updated from its originally published version to correct the affiliations. See the corresponding erratum notice; DOI: 10.3171/2017.5.JNS141280a. «CLINICAL ARTICLE J Neurosurg 123:1375
» This article has been updated from its originally published version to correct the affiliations. See the corresponding erratum notice; DOI: 10.3171/2017.5.JNS141280a. «CLINICAL ARTICLE J Neurosurg 123:1375
How do we evaluate patients before epilepsy surgery?
 How do we evaluate patients before epilepsy surgery? Yotin Chinvarun, MD Chaiyos Khongkhatithum, MD How do we evaluate patients before epilepsy surgery? Chaiyos Khongkhatithum, MD Division of Neurology
How do we evaluate patients before epilepsy surgery? Yotin Chinvarun, MD Chaiyos Khongkhatithum, MD How do we evaluate patients before epilepsy surgery? Chaiyos Khongkhatithum, MD Division of Neurology
Responsive Neurostimulation for the Treatment of Refractory Partial Epilepsy
 Responsive Neurostimulation for the Treatment of Refractory Partial Epilepsy Policy Number: 7.01.143 Last Review: 8/2017 Origination: 8/2015 Next Review: 8/2018 Policy Blue Cross and Blue Shield of Kansas
Responsive Neurostimulation for the Treatment of Refractory Partial Epilepsy Policy Number: 7.01.143 Last Review: 8/2017 Origination: 8/2015 Next Review: 8/2018 Policy Blue Cross and Blue Shield of Kansas
Introduction to Epilepsy Surgery ผศ.นพ.บรรพต ส ทธ นามส วรรณ สาขาว ชาประสาทศ ลยศาสตร ภาคว ชาศ ลยศาสตร คณะแพทยศาสตร ศ ร ราชพยาบาล มหาว ทยาล ยมห ดล
 Introduction to Epilepsy Surgery ผศ.นพ.บรรพต ส ทธ นามส วรรณ สาขาว ชาประสาทศ ลยศาสตร ภาคว ชาศ ลยศาสตร คณะแพทยศาสตร ศ ร ราชพยาบาล มหาว ทยาล ยมห ดล Overview Drug resistant epilepsy Cortical zones Presurgical
Introduction to Epilepsy Surgery ผศ.นพ.บรรพต ส ทธ นามส วรรณ สาขาว ชาประสาทศ ลยศาสตร ภาคว ชาศ ลยศาสตร คณะแพทยศาสตร ศ ร ราชพยาบาล มหาว ทยาล ยมห ดล Overview Drug resistant epilepsy Cortical zones Presurgical
Hamartomas and epilepsy: clinical and imaging characteristics
 Seizure 2003; 12: 307 311 doi:10.1016/s1059 1311(02)00272-8 Hamartomas and epilepsy: clinical and imaging characteristics B. DIEHL, R. PRAYSON, I. NAJM & P. RUGGIERI Departments of Neurology, Pathology
Seizure 2003; 12: 307 311 doi:10.1016/s1059 1311(02)00272-8 Hamartomas and epilepsy: clinical and imaging characteristics B. DIEHL, R. PRAYSON, I. NAJM & P. RUGGIERI Departments of Neurology, Pathology
Surgical Management of Post- Traumatic Epilepsy Complexities-Adhesions and Multifocality
 Surgical Management of Post- Traumatic Epilepsy Complexities-Adhesions and Multifocality December 2, 2012 Jeffrey P. Blount MD Division of Neurosurgery University of Alabama at Birmingham Children s of
Surgical Management of Post- Traumatic Epilepsy Complexities-Adhesions and Multifocality December 2, 2012 Jeffrey P. Blount MD Division of Neurosurgery University of Alabama at Birmingham Children s of
Neuromuscular Disease(2) Epilepsy. Department of Pediatrics Soochow University Affiliated Children s Hospital
 Epilepsy. Department of Pediatrics Soochow University Affiliated Children s Hospital") Neuromuscular Disease(2) Epilepsy Department of Pediatrics Soochow University Affiliated Children s Hospital Seizures (p130) Main contents: 1) Emphasize the clinical features of epileptic seizure and epilepsy.
Neuromuscular Disease(2) Epilepsy Department of Pediatrics Soochow University Affiliated Children s Hospital Seizures (p130) Main contents: 1) Emphasize the clinical features of epileptic seizure and epilepsy.
Pediatric Epilepsy Care in Milwaukee
 Pediatric Epilepsy Care in Milwaukee Priya Monrad, MD Assistant Professor, Pediatric Neurology and Epilepsy Children s Hospital of Wisconsin Disclosures I have no relevant financial relationships to disclose.
Pediatric Epilepsy Care in Milwaukee Priya Monrad, MD Assistant Professor, Pediatric Neurology and Epilepsy Children s Hospital of Wisconsin Disclosures I have no relevant financial relationships to disclose.
PET and SPECT in Epilepsy
 PET and SPECT in Epilepsy 12.6.2013 William H Theodore MD Chief, Clinical Epilepsy Section NINDS NIH Bethesda MD American Epilepsy Society Annual Meeting Disclosures Entity DIR NINDS NIH Elsevier Individual
PET and SPECT in Epilepsy 12.6.2013 William H Theodore MD Chief, Clinical Epilepsy Section NINDS NIH Bethesda MD American Epilepsy Society Annual Meeting Disclosures Entity DIR NINDS NIH Elsevier Individual
Level 4 comprehensive epilepsy program in Malaysia, a resource-limited country
 Neurology Asia 2017; 22(4) : 299 305 Level 4 comprehensive epilepsy program in Malaysia, a resource-limited country 1 Kheng-Seang Lim, 1 Sherrini Ahmad Bazir Ahmad, 2 Vairavan Narayanan, 3 Kartini Rahmat,
Neurology Asia 2017; 22(4) : 299 305 Level 4 comprehensive epilepsy program in Malaysia, a resource-limited country 1 Kheng-Seang Lim, 1 Sherrini Ahmad Bazir Ahmad, 2 Vairavan Narayanan, 3 Kartini Rahmat,
Cerebral MRI as an important diagnostic tool in temporal lobe epilepsy
 Cerebral MRI as an important diagnostic tool in temporal lobe epilepsy Poster No.: C-2190 Congress: ECR 2014 Type: Educational Exhibit Authors: A. Puiu, D. Negru; Iasi/RO Keywords: Neuroradiology brain,
Cerebral MRI as an important diagnostic tool in temporal lobe epilepsy Poster No.: C-2190 Congress: ECR 2014 Type: Educational Exhibit Authors: A. Puiu, D. Negru; Iasi/RO Keywords: Neuroradiology brain,
Seizures- an Update. Epileptic Seizure: Definition. When is a Seizure Epilepsy?
 Seizures- an Update Jaishree T. Narayanan Department of Neurology, NorthShore University Health System Epileptic Seizure: Definition An Epileptic Seizure is a transient occurrence of signs and symptoms
Seizures- an Update Jaishree T. Narayanan Department of Neurology, NorthShore University Health System Epileptic Seizure: Definition An Epileptic Seizure is a transient occurrence of signs and symptoms
SUBSPECIALTY CERTIFICATION EXAMINATION IN EPILEPSY MEDICINE Content Blueprint (December 21, 2015)
") SUBSPECIALTY CERTIFICATION EXAMINATION IN EPILEPSY MEDICINE 2016 Content Blueprint (December 21, 2015) Number of questions: 200 1. Classification 8-12% 2. Routine EEG 16-20% 3. Evaluation 23-27% 4. Management
SUBSPECIALTY CERTIFICATION EXAMINATION IN EPILEPSY MEDICINE 2016 Content Blueprint (December 21, 2015) Number of questions: 200 1. Classification 8-12% 2. Routine EEG 16-20% 3. Evaluation 23-27% 4. Management
Seizures in Children: Laboratory
 Article neurology Seizures in Children: Laboratory Diagnosis and Management Philippe Major, MD,* Elizabeth A. Thiele, MD, PhD* Objectives After completing this article, readers should be able to: 1. Formulate
Article neurology Seizures in Children: Laboratory Diagnosis and Management Philippe Major, MD,* Elizabeth A. Thiele, MD, PhD* Objectives After completing this article, readers should be able to: 1. Formulate
Deep brain and cortical stimulation for epilepsy(review)
") Cochrane Database of Systematic Reviews Deep brain and cortical stimulation for epilepsy(review) SprengersM,VonckK,CarretteE,MarsonAG,BoonP SprengersM,VonckK,CarretteE,MarsonAG,BoonP. Deep brain and cortical
Cochrane Database of Systematic Reviews Deep brain and cortical stimulation for epilepsy(review) SprengersM,VonckK,CarretteE,MarsonAG,BoonP SprengersM,VonckK,CarretteE,MarsonAG,BoonP. Deep brain and cortical
The EEG in focal epilepsy. Bassel Abou-Khalil, M.D. Vanderbilt University Medical Center
 The EEG in focal epilepsy Bassel Abou-Khalil, M.D. Vanderbilt University Medical Center I have no financial relationships to disclose that are relative to the content of my presentation Learning Objectives
The EEG in focal epilepsy Bassel Abou-Khalil, M.D. Vanderbilt University Medical Center I have no financial relationships to disclose that are relative to the content of my presentation Learning Objectives
21 ST CENTURY TECHNOLOGY IN PEDIATRIC NEUROLOGIC DISORDERS PEDIATRIC NEUROLOGIC DISORDERS YOUR LEARNING EXPERIENCE LEARNING OBJECTIVES
 21 ST CENTURY TECHNOLOGY IN PEDIATRIC NEUROLOGIC DISORDERS Saturday, April 30, 2016 11:00 am David J. Siegler, M.D. Board Certified American Board of Psychiatry and Neurology National Board of Physicians
21 ST CENTURY TECHNOLOGY IN PEDIATRIC NEUROLOGIC DISORDERS Saturday, April 30, 2016 11:00 am David J. Siegler, M.D. Board Certified American Board of Psychiatry and Neurology National Board of Physicians
Interview. News & Views. The importance of surgery for epilepsy. Jerome Engel Jr
 Interview The importance of surgery for epilepsy Jerome Engel Jr, MD, PhD, is the Jonathan Sinay Distinguished Professor of Neurology, Neurobiology, and Psychiatry and Biobehavioral Sciences at the David
Interview The importance of surgery for epilepsy Jerome Engel Jr, MD, PhD, is the Jonathan Sinay Distinguished Professor of Neurology, Neurobiology, and Psychiatry and Biobehavioral Sciences at the David
Toward a more accurate delimitation of the epileptic focus from a surgical perspective
 Toward a more accurate delimitation of the epileptic focus from a surgical perspective Margitta Seeck Department of Clinical Neurosciences EEG & Epilepsy Unit University Hospital of Geneva Geneva, Switzerland
Toward a more accurate delimitation of the epileptic focus from a surgical perspective Margitta Seeck Department of Clinical Neurosciences EEG & Epilepsy Unit University Hospital of Geneva Geneva, Switzerland
Neuromodulation Approaches to Treatment Resistant Depression
 1 Alternative Treatments: Neuromodulation Approaches to Treatment Resistant Depression Audrey R. Tyrka, MD, PhD Assistant Professor Brown University Department of Psychiatry Associate Chief, Mood Disorders
1 Alternative Treatments: Neuromodulation Approaches to Treatment Resistant Depression Audrey R. Tyrka, MD, PhD Assistant Professor Brown University Department of Psychiatry Associate Chief, Mood Disorders
Difficult to treat childhood epilepsy: Lessons from clinical case scenario
 Difficult to treat childhood epilepsy: Lessons from clinical case scenario Surachai Likasitwattanakul, M.D. Department of Pediatrics Faculty of Medicine, Siriraj Hospital Natural history of Epilepsy Untreated
Difficult to treat childhood epilepsy: Lessons from clinical case scenario Surachai Likasitwattanakul, M.D. Department of Pediatrics Faculty of Medicine, Siriraj Hospital Natural history of Epilepsy Untreated
Vagus nerve stimulation for refractory epilepsy
 Seizure 2001; 10: 456 460 doi:10.1053/seiz.2001.0628, available online at http://www.idealibrary.com on CASE REPORT Vagus nerve stimulation for refractory epilepsy PAUL BOON, KRISTL VONCK, JACQUES DE REUCK
Seizure 2001; 10: 456 460 doi:10.1053/seiz.2001.0628, available online at http://www.idealibrary.com on CASE REPORT Vagus nerve stimulation for refractory epilepsy PAUL BOON, KRISTL VONCK, JACQUES DE REUCK
Neurostimulation for Epilepsy: Do We Know the Best Stimulation Parameters?
 Neurostimulation for Epilepsy: Do We Know the Best Stimulation Parameters? Current Literature In Basic Science Effect of Stimulus Parameters in the Treatment of Seizures by Electrical Stimulation in the
Neurostimulation for Epilepsy: Do We Know the Best Stimulation Parameters? Current Literature In Basic Science Effect of Stimulus Parameters in the Treatment of Seizures by Electrical Stimulation in the
Case report. Epileptic Disord 2005; 7 (1): 37-41
: 37-41") Case report Epileptic Disord 2005; 7 (1): 37-41 Periodic lateralized epileptiform discharges (PLEDs) as the sole electrographic correlate of a complex partial seizure Gagandeep Singh, Mary-Anne Wright,
Case report Epileptic Disord 2005; 7 (1): 37-41 Periodic lateralized epileptiform discharges (PLEDs) as the sole electrographic correlate of a complex partial seizure Gagandeep Singh, Mary-Anne Wright,
Epilepsy. Annual Incidence. Adult Epilepsy Update
 Adult Epilepsy Update Annual Incidence J. Layne Moore, MD, MPH Associate Professor Department of Neurology and Pharmacy Director, Division of Epilepsy The Ohio State University Used by permission Health
Adult Epilepsy Update Annual Incidence J. Layne Moore, MD, MPH Associate Professor Department of Neurology and Pharmacy Director, Division of Epilepsy The Ohio State University Used by permission Health
Difficult-to-Localize Intractable Focal Epilepsy: An In-Depth Look
 Current Literature In Clinical Science Difficult-to-Localize Intractable Focal Epilepsy: An In-Depth Look Stereoelectroencephalography in the Difficult to Localize Refractory Focal Epilepsy: Early Experience
Current Literature In Clinical Science Difficult-to-Localize Intractable Focal Epilepsy: An In-Depth Look Stereoelectroencephalography in the Difficult to Localize Refractory Focal Epilepsy: Early Experience
Clinical Applications of fmri
 Clinical Applications of fmri Benjamin M. Hampstead, Ph.D., ABPP/CN Associate Professor Department of Psychiatry University of Michigan VA Ann Arbor Healthcare System No Disclosures or Conflicts Hampstead
Clinical Applications of fmri Benjamin M. Hampstead, Ph.D., ABPP/CN Associate Professor Department of Psychiatry University of Michigan VA Ann Arbor Healthcare System No Disclosures or Conflicts Hampstead
VNS use for the treatment of refractory Epilepsy. Anny Laforme Joanna Wai Ling Ma
 VNS use for the treatment of refractory Epilepsy Anny Laforme Joanna Wai Ling Ma Content of the presentation Define refractory epilepsy Overwiew of available epilepsy treatments Adjunctive treatments for
VNS use for the treatment of refractory Epilepsy Anny Laforme Joanna Wai Ling Ma Content of the presentation Define refractory epilepsy Overwiew of available epilepsy treatments Adjunctive treatments for
Seizure Duration Determined by Subdural Electrode Recordings in Adult Patients with Intractable Focal Epilepsy
 Seizure Duration Determined by Subdural Electrode Recordings in Adult Patients with Intractable Focal Epilepsy Original Article Journal of Epilepsy Research pissn 2233-6249 / eissn 2233-6257 Daeyoung Kim,
Seizure Duration Determined by Subdural Electrode Recordings in Adult Patients with Intractable Focal Epilepsy Original Article Journal of Epilepsy Research pissn 2233-6249 / eissn 2233-6257 Daeyoung Kim,
Sleep Complaints and Disorders in Epileptic Patients 순천향의대천안병원순천향의대천안병원신경과양광익
 Sleep Complaints and Disorders in Epileptic Patients 순천향의대천안병원순천향의대천안병원신경과양광익 Introduction The global physical, social and economic consequence of epilepsy are high. WHO 2000 study Improving QoL is increasingly
Sleep Complaints and Disorders in Epileptic Patients 순천향의대천안병원순천향의대천안병원신경과양광익 Introduction The global physical, social and economic consequence of epilepsy are high. WHO 2000 study Improving QoL is increasingly
Methods of epilepsy surgery
 Chapter 47 Methods of epilepsy surgery ANDREW W. McEVOY 1 and WILLIAM J.F. HARKNESS 2 1 Institute of Neurology, University College, London, National Hospital for Neurology and Neurosurgery, Queen Square,
Chapter 47 Methods of epilepsy surgery ANDREW W. McEVOY 1 and WILLIAM J.F. HARKNESS 2 1 Institute of Neurology, University College, London, National Hospital for Neurology and Neurosurgery, Queen Square,
Epilepsy at the Edges. Robert F Leroy MD Texas Epilepsy Group Neurological Clinic of Texas, PA
 Epilepsy at the Edges Robert F Leroy MD Texas Epilepsy Group Neurological Clinic of Texas, PA Epilepsy at the Edges What is the current thinking about the diagnosis and treatment of epilepsy? What will
Epilepsy at the Edges Robert F Leroy MD Texas Epilepsy Group Neurological Clinic of Texas, PA Epilepsy at the Edges What is the current thinking about the diagnosis and treatment of epilepsy? What will
Epilepsy surgery. John S Duncan. Who are candidates for epilepsy surgery? The context of epilepsy surgery ORIGINAL PAPERS
 ORIGINAL PAPERS Epilepsy surgery John S Duncan ABSTRACT If the first two or three antiepileptic drugs used do not control epilepsy, there is little chance that subsequent medications will be effective.
ORIGINAL PAPERS Epilepsy surgery John S Duncan ABSTRACT If the first two or three antiepileptic drugs used do not control epilepsy, there is little chance that subsequent medications will be effective.
Epilepsy & Behavior Case Reports
 Epilepsy & Behavior Case Reports 1 (2013) 45 49 Contents lists available at ScienceDirect Epilepsy & Behavior Case Reports journal homepage: www.elsevier.com/locate/ebcr Case Report Partial disconnection
Epilepsy & Behavior Case Reports 1 (2013) 45 49 Contents lists available at ScienceDirect Epilepsy & Behavior Case Reports journal homepage: www.elsevier.com/locate/ebcr Case Report Partial disconnection
Successful Treatment of Mesial Temporal Lobe Epilepsy with Bilateral Hippocampal Atrophy and False Temporal Scalp Ictal Onset: A case report
 Hiroshima J. Med. Sci. Vol. 61, No. 2, 37~41, June, 2012 HIJM 61 7 37 Successful Treatment of Mesial Temporal Lobe Epilepsy with Bilateral Hippocampal Atrophy and False Temporal Scalp Ictal Onset: A case
Hiroshima J. Med. Sci. Vol. 61, No. 2, 37~41, June, 2012 HIJM 61 7 37 Successful Treatment of Mesial Temporal Lobe Epilepsy with Bilateral Hippocampal Atrophy and False Temporal Scalp Ictal Onset: A case
Seizure Localization in Patients with Multiple Tubers: Presurgical Evaluation in Tuberous Sclerosis
 Seizure Localization in Patients with Multiple Tubers: Presurgical Evaluation in Tuberous Sclerosis Case Report Journal of Epilepsy Research pissn 2233-6249 / eissn 2233-6257 Pamela Song, MD 1, Eun Yeon
Seizure Localization in Patients with Multiple Tubers: Presurgical Evaluation in Tuberous Sclerosis Case Report Journal of Epilepsy Research pissn 2233-6249 / eissn 2233-6257 Pamela Song, MD 1, Eun Yeon
Introduction to seizures and epilepsy
 Introduction to seizures and epilepsy Selim R. Benbadis, M.D. Professor Departments of Neurology & Neurosurgery Director, Comprehensive Epilepsy Program Symptomatic seizures Head injury (trauma) Stroke
Introduction to seizures and epilepsy Selim R. Benbadis, M.D. Professor Departments of Neurology & Neurosurgery Director, Comprehensive Epilepsy Program Symptomatic seizures Head injury (trauma) Stroke
Coexistence of focal and idiopathic generalized epilepsy in the same patient population
 Seizure (2006) 15, 28 34 www.elsevier.com/locate/yseiz Coexistence of focal and idiopathic generalized epilepsy in the same patient population Lara E. Jeha a, *, Harold H. Morris b, Richard C. Burgess
Seizure (2006) 15, 28 34 www.elsevier.com/locate/yseiz Coexistence of focal and idiopathic generalized epilepsy in the same patient population Lara E. Jeha a, *, Harold H. Morris b, Richard C. Burgess