Prescribing issues in spasticity and dystonia. Professor Rajat Gupta Consultant Paediatric Neurologist Birmingham Children s Hospital
|
|
|
- Rudolf Atkins
- 5 years ago
- Views:
Transcription




1 Prescribing issues in spasticity and dystonia Professor Rajat Gupta Consultant Paediatric Neurologist Birmingham Children s Hospital
2 Cerebral palsy is common, affecting about 2-3 per 1000 children Surveillance of cerebral palsy in Europe, Dev Med Child Neurol 2000 About 75% of children with CP have spasticity Murphy NA, et al, Phys Med Rehabil 2002 Around 10 to 15% will have dystonia (often together with spasticity)
3 Spasticity Spasticity is a motor disorder characterized by a velocity dependent increase in tonic stretch reflexes ( muscle tone ) with exaggerated tendon jerks, resulting from hyper-excitability of the stretch reflex, as one component of the upper motor neurone syndrome Lance 1980
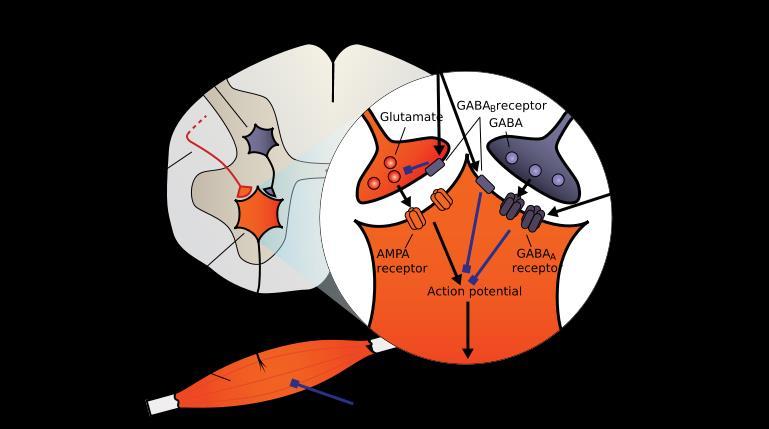
4 Spasticity results from a lack of descending impulses that normally stimulate the release of the inhibitory neurotransmitter GABA which acts presynaptically to inhibit the release of excitatory neurotransmitters
5 Dystonia Dystonia is defined as a syndrome of sustained muscle contraction that frequently causes twisting and repetitive movements or abnormal postures; it is often increased during voluntary movement Fahn S, et al, 1998
6 Dystonic movements are characterized by the co-contraction of antagonist muscles and overflow of activity into surrounding muscles resulting in an abnormal pattern of muscle activation during voluntary movement or the maintenance of posture. Dystonia originates in the basal ganglia and involves deficient inhibition at the level of the motor cortex and probably also at the levels of the brainstem and spinal cord.
7 Spasticity in under 19s management Oral drugs NICE July 2012 Consider oral diazepam or baclofen if spasticity is contributing to one or more of the following: discomfort or pain muscle spasms functional disability
8 If oral diazepam is initially used because of its rapid onset of action, consider changing to oral baclofen if long-term treatment is indicated. Continue using oral diazepam or oral baclofen if they have a clinical benefit and are well tolerated, but think about stopping the treatment whenever the child or young person's management programme is reviewed and at least every 6 months.
9 If adverse effects (such as drowsiness) occur with oral diazepam or oral baclofen, think about reducing the dose or stopping treatment. If the response to oral diazepam and oral baclofen used individually for 4 6 weeks is unsatisfactory, consider a trial of combined treatment using both drugs.
10 If a child or young person has been receiving oral diazepam and/or baclofen for several weeks, ensure that when stopping these drugs the dose is reduced in stages to avoid withdrawal symptoms. In children and young people with spasticity in whom dystonia is considered to contribute significantly to problems with posture, function and pain, consider a trial of oral drug treatment, for example with trihexyphenidyl, levodopa or baclofen.
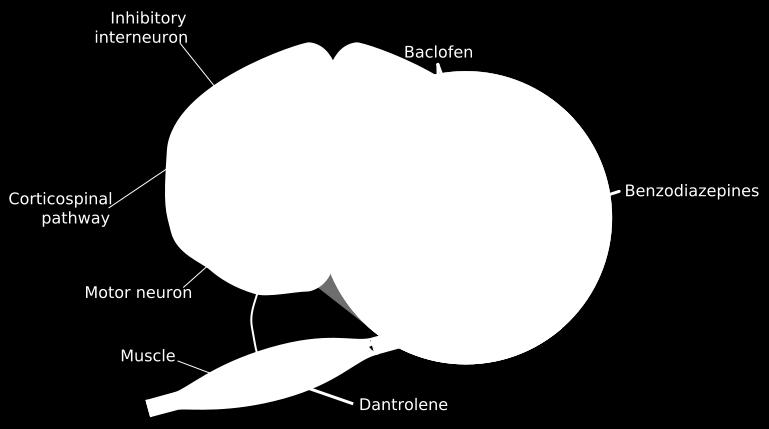
11 Baclofen Baclofen binds to GABA B receptors in Rexed laminae I to IV of the spinal cord leading to a reduction in the release of excitatory neurotransmitters (such as glutamate and aspartate), as well as substance P. Important side effects of baclofen include drowsiness, orthostatic hypotension and withdrawal symptoms such as seizures, fever, hallucinations, and rebound spasticity.
12
13 Oral baclofen has poor penetration of the bloodbrain barrier with cerebrospinal fluid (CSF) drug levels 10-fold lower than serum concentrations. Commonly oral dose escalation leads to side effects before full therapeutic efficacy is reached. Intrathecal delivery of baclofen may then be considered.
14 Benzodiazepines Benzodiazepines facilitate the binding of existing GABA to the GABA A receptor, found in high concentrations in the reticular formation and polysynaptic spinal tracts. Activation of the GABA A receptor causes an increase presynaptic inhibition and reduces monosynaptic and polysynaptic reflexes throughout the spinal cord
15
16 Different benzodiazepine compounds are available with different routes of administration and different half-lives. Oral diazepam often used. Initial dose is 250 mcg/kg tds with a maximum dose of 20 mg tds. If nocturnal spasticity is the major problem consider a single dose at night. The most important side effect is sedation. Additionally, habituation and tolerance may develop.
17 Clonidine and Tizanidine These are alpha 2, nonadrenergic receptor agonists that release excitatory neurotransmitters and inhibit supraspinal facilitatory pathways. Tizanidine is given orally and selectively decreases tone and spasm frequency in only the spastic muscles, eliminating the unwanted side effect of generalised muscle weakness.
18 Tizanidine is an imidazoline derivative similar to clonidine but without the cardiovascular effects when appropriately titrated. Potential side effects include drowsiness (particularly with tizanidine), dry mouth, dizziness, nausea and vomiting. Also hypotension with clonidine. Clonidine dose 0.5 1mcg/kg tds (max 25mcg/kg/d)
19 Dantrolene sodium Dantrolene works peripherally directly on the skeletal muscle, hindering the release of calcium from the sarcoplasmic reticulum, thereby preventing the excitation-contraction coupling mechanism. This decreases the force of muscle contraction. However, this mechanism is not selective and the resulting generalised muscle weakness may weaken respiratory muscles. It is less sedative than the other antispasticity agents
20
21 Dantrolene dosing in children 0.5 mg/kg orally once daily for 7 days, then 0.5 mg/kg three times a day for 7 days, then 1 mg/kg three times a day for 7 days, then 2 mg/kg three times a day.
22 Gabapentin The exact mechanism of action of Gabapentin is relatively unknown Thought to act at the alpha-2 δ1 subunit of voltage-dependent calcium channels, thus inhibiting calcium currents. A study by Gruenthal et al (1997) showed that using gabapentin alone, compared to a placebo, demonstrated a reduction in the Ashworth scale and in the spasticity Likert scale scores. Adverse effects include somnolence, tremor, and nystagmus
23 Gabapentin dosing 10 mg/kg once daily (max. per dose 300 mg) on day 1, then 10 mg/kg twice daily (max. per dose 300 mg) on day 2, then 10 mg/kg 3 times a day (max. per dose 300 mg) on day 3 (usual dose mg/kg daily in 3 divided doses)

24 Oral medications used to treat spasticity Levitt and Browd, 2015
25 Approach to treatment of dystonia Aetiology-specific: treatment of underlying disease Anatomy-specific: treat sensory, basal ganglia, frontal, or cerebellar origin Nonspecific: reduce stretch reflexes
26 Medicines for dystonia Medicines for spasticity will also generally improve dystonia, particularly if spasticity and dystonia co-exist in the patient. reduce stretch reflexes Baclofen, Intrathecal Baclofen, Benzodiazepines, Botulinum Toxin
27 Medicines for dystonia These include Trihexyphenidyl, Levodopa and Clonazepam Consider these when anti-spasticity medications not adequately controlling symptoms or if patient predominantly has dystonia and not spasticity
28 Approach to Treatment Anatomy-specific: treat sensory, basal ganglia, frontal, or cerebellar origin Levodopa, Trihexyphenidyl, Deep-Brain Stimulation
29 Trihexyphenidyl An anticholinergic agent. It is a muscarinic acetylcholine receptor antagonist. The therapeutic dose varies considerably. Children tend to tolerate this better than adults. Central side effects include memory loss, confusion, restlessness, insomnia, and nightmares. Children may experience chorea, or exacerbation of a pre-existing tic disorder. Peripheral side effects include blurred vision, dry mouth, constipation, and urinary retention.
30 Trihexyphenidyl dosing For Child 3 months 17 years Initially 1 2 mg daily in 1 2 divided doses, then increased in steps of 1 mg every 3 7 days, dose to be adjusted according to response and sideeffects; maximum 2 mg/kg per day (up to maximum 20mg/d)
31 Levodopa Study results with Levodopa in treating generalised dystonias have been variable. (Cloud and Jinnah, 2010). One small subset of patients with substantial improvement with levodopa is dopa-responsive dystonia (DRD), which may represent up to 5% of childhood dystonias. DRD is characterised by childhood onset, gait disturbance, muscle cramps and diurnal fluctuations. It is often misdiagnosed as cerebral palsy. Levodopa is administered in combination with the decarboxylase inhibitor carbidopa.
32 Levodopa Side effects include nausea, orthostasis, and constipation. Unlike adult patients with Parkinson s disease, children with dystonia rarely develop confusion, hallucinations, or dyskinesias. Most children with DRD will respond to low doses. But for dystonia with CP may require doses as high as 20 mg/kg/day. (Cloud and Jinnah 2010) For Child 3 months 17 years (BNFc) Initially 250 micrograms/kg 2 3 times a day, dose to be increased according to response every 2 3 days, increased if necessary up to 1 mg/kg 3 times a day.
33 Clonazepam Studies have shown Clonazepam to be effective in treating generalised and focal dystonias. (Cloud and Jinnah 2010) A typical starting dose is 0.5 mg at night. The dose is slowly increased to an average daily dose of 1 4 mg in 3 divided doses. Side effects include sedation, confusion, impaired coordination, and depression. There is also potential for dependence
34 Summary There is a lack of robust evidence to inform pharmacotherapy for dystonia and spasticity, therefore strict recommendations of first, second and third line medications are not practical. Fernandez-Alvarez E, Nardocci N, 2012 Therapeutic strategies tend to vary with individual clinician preference and experience.
35 As well as dystonia-specific therapy, identifying and treating precipitating factors is paramount. Spasticity is a common co-morbidity, and it can be difficult to differentiate between spasticity and dystonia in some children. In these cases a pragmatic approach to symptom control should be taken.
36 Medications should be reviewed periodically, addressing whether the drug has had a positive effect on quality of life and the side effects. If no improvement with second line medication, consider discussion with colleagues. As well as medication, supportive management in a multidisciplinary team including physiotherapy, occupational therapy, speech therapy and psychosocial support is essential.
37 Epidiolex may be a useful treatment on the horizon
38 Status dystonicus Status dystonicus is a potentially fatal episode of severe generalised dystonia. Complications include bulbar and respiratory compromise, and metabolic disorders such as rhabdomyolysis leading to acute renal failure. Children with status dystonicus should be managed in a hospital setting, and will often need intensive care. Important to treat complications.
39 Supportive care such as invasive ventilation and haemofiltration for rhabdomyolysis may be needed. Therapy should be aggressive, with a slow weaning process. Treatment options include benzodiazepines, clonidine, propofol, and deep sedation with barbiturates. Once the dystonia severity has lessened, a slow wean of therapy can begin.
40 Conclusion Childhood spasticity and dystonia are challenging conditions. They often co-exist. A multitude of external and internal factors often play a part in influencing dystonia. Medications have an important role in managing spasticity and dystonia. However, a pragmatic, multi-disciplinary approach to management is vital

41 ?
Overview. Spasticity. Spasticity. Oral Medications. Spasticity 3/10/2012. Medication Management of Spasticity in the Traumatic Brain Injured Patient
 Medication Management of in the Traumatic Brain Injured Patient 6 th Annual Northern Kentucky TBI Conference March 23, 2012 www.bridgesnky.org Chad Walters, D.O. Medical Director Radical Rehab Solutions
Medication Management of in the Traumatic Brain Injured Patient 6 th Annual Northern Kentucky TBI Conference March 23, 2012 www.bridgesnky.org Chad Walters, D.O. Medical Director Radical Rehab Solutions
Management of Spasticity
 Management of Spasticity Stephen P. Moran, M.D. Department of Physical Medicine and Rehabilitation Ochsner Medical Center Outline Review pathophysiology of spasticity Discuss epidemiology of spasticity
Management of Spasticity Stephen P. Moran, M.D. Department of Physical Medicine and Rehabilitation Ochsner Medical Center Outline Review pathophysiology of spasticity Discuss epidemiology of spasticity
Baclofen is a GABA-agonist, although its exact mechanism of action remains uncertain. It is known to reduce release of excitatory neurotransmitters.
 Muscle relaxants may be needed, including benzodiazepines such as diazepam (Valium). For increased muscle tone (spasticity) Baclofen (Lioresal?) is a useful drug. Baclofen is a GABA-agonist, although its
Muscle relaxants may be needed, including benzodiazepines such as diazepam (Valium). For increased muscle tone (spasticity) Baclofen (Lioresal?) is a useful drug. Baclofen is a GABA-agonist, although its
Professor Tim Anderson
 Professor Tim Anderson Neurologist University of Otago Christchurch 11:00-11:55 WS #91: Shakes Jerks and Spasms - Recognition and Differential Diagnosis 12:05-13:00 WS #102: Shakes Jerks and Spasms - Recognition
Professor Tim Anderson Neurologist University of Otago Christchurch 11:00-11:55 WS #91: Shakes Jerks and Spasms - Recognition and Differential Diagnosis 12:05-13:00 WS #102: Shakes Jerks and Spasms - Recognition
Intrathecal Baclofen for Spasticity. Dr. M. Mehra Dr. A. Kumar
 Intrathecal Baclofen for Spasticity Dr. M. Mehra Dr. A. Kumar Goals of Spasticity: Management Decrease spasticity Improve functional ability and independence Decrease pain associated with spasticity Prevent
Intrathecal Baclofen for Spasticity Dr. M. Mehra Dr. A. Kumar Goals of Spasticity: Management Decrease spasticity Improve functional ability and independence Decrease pain associated with spasticity Prevent
Professor Tim Anderson
 Professor Tim Anderson Neurologist University of Otago Christchurch 11:00-11:55 WS #91: Shakes Jerks and Spasms - Recognition and Differential Diagnosis 12:05-13:00 WS #102: Shakes Jerks and Spasms - Recognition
Professor Tim Anderson Neurologist University of Otago Christchurch 11:00-11:55 WS #91: Shakes Jerks and Spasms - Recognition and Differential Diagnosis 12:05-13:00 WS #102: Shakes Jerks and Spasms - Recognition
Dystonia. The condition can vary from very mild to severe. Dystonia may get worse over time or it may stay the same or get better.
 Dystonia What are movement disorders? Movement disorders are conditions that cause involuntary body movements. With all movement disorders, abnormal signals from the brain cause patients to have trouble
Dystonia What are movement disorders? Movement disorders are conditions that cause involuntary body movements. With all movement disorders, abnormal signals from the brain cause patients to have trouble
Role of Intrathecal Baclofen. Mr. Chirag Patel Consultant Paediatric Neurosurgeon Children s Hospital for Wales, Cardiff.
 Role of Intrathecal Baclofen Mr. Chirag Patel Consultant Paediatric Neurosurgeon Children s Hospital for Wales, Cardiff. History of Intrathecal Baclofen therapy 1978: First used in guinea pigs by Wilson.
Role of Intrathecal Baclofen Mr. Chirag Patel Consultant Paediatric Neurosurgeon Children s Hospital for Wales, Cardiff. History of Intrathecal Baclofen therapy 1978: First used in guinea pigs by Wilson.
Skeletal Muscle Relaxants. Munir Gharaibeh, MD, PhD, MHPE Faculty of Medicine, The University of Jordan March, 2014
 Skeletal Muscle Relaxants Munir Gharaibeh, MD, PhD, MHPE Faculty of Medicine, The University of Jordan March, 2014 The nicotinic Acetycholine receptor Present at the neuromuscular junction, peripheral
Skeletal Muscle Relaxants Munir Gharaibeh, MD, PhD, MHPE Faculty of Medicine, The University of Jordan March, 2014 The nicotinic Acetycholine receptor Present at the neuromuscular junction, peripheral
Psycholeptics, anti-depressants, antiepileptic, anti-ra and anti-spastic medications available at Zithulele hospital
 Psycholeptics, anti-depressants, antiepileptic, anti-ra and anti-spastic medications available at Zithulele hospital Note that with the exception of NSAIDs, none of the following medications are available
Psycholeptics, anti-depressants, antiepileptic, anti-ra and anti-spastic medications available at Zithulele hospital Note that with the exception of NSAIDs, none of the following medications are available
Spasticity. Pain and Spasticity Management in SCI Nov 23 rd, /19/17
 Pain and Spasticity Management in SCI Nov 23 rd, 2017 Phichamon Khanittanuphong, MD Rehabilitation Division Department of Orthopaedic Surgery and Physical Medicine Faculty of Medicine, Prince of Songkla
Pain and Spasticity Management in SCI Nov 23 rd, 2017 Phichamon Khanittanuphong, MD Rehabilitation Division Department of Orthopaedic Surgery and Physical Medicine Faculty of Medicine, Prince of Songkla
DRUG TREATMENT OF PARKINSON S DISEASE. Mr. D.Raju, M.pharm, Lecturer
 DRUG TREATMENT OF PARKINSON S DISEASE Mr. D.Raju, M.pharm, Lecturer PARKINSON S DISEASE (parkinsonism) is a neurodegenerative disorder which affects t h e b a s a l g a n g l i a - and is associated with
DRUG TREATMENT OF PARKINSON S DISEASE Mr. D.Raju, M.pharm, Lecturer PARKINSON S DISEASE (parkinsonism) is a neurodegenerative disorder which affects t h e b a s a l g a n g l i a - and is associated with
MOVEMENT OUTLINE. The Control of Movement: Muscles! Motor Reflexes Brain Mechanisms of Movement Mirror Neurons Disorders of Movement
 MOVEMENT 2 Dr. Steinmetz 3 OUTLINE The Control of Movement: Muscles! Motor Reflexes Brain Mechanisms of Movement Mirror Neurons Disorders of Movement Parkinson s Disease Huntington s Disease 1 4 TYPES
MOVEMENT 2 Dr. Steinmetz 3 OUTLINE The Control of Movement: Muscles! Motor Reflexes Brain Mechanisms of Movement Mirror Neurons Disorders of Movement Parkinson s Disease Huntington s Disease 1 4 TYPES
BOTULINUM TOXIN AND INTRATHECAL BACLOFEN. Spencer Cotterell DO Mercy Rehabilitation Hospital June 30, 2018
 BOTULINUM TOXIN AND INTRATHECAL BACLOFEN Spencer Cotterell DO Mercy Rehabilitation Hospital June 30, 2018 INJECTABLES MEDICAL MANAGEMENT OF SPASTICITY Leonard, J In: Botulinum toxin: 2009 A protein and
BOTULINUM TOXIN AND INTRATHECAL BACLOFEN Spencer Cotterell DO Mercy Rehabilitation Hospital June 30, 2018 INJECTABLES MEDICAL MANAGEMENT OF SPASTICITY Leonard, J In: Botulinum toxin: 2009 A protein and
Intrathecal Baclofen. Val Stevenson
 Intrathecal Baclofen Val Stevenson Plan What is it, how does it work? Who is it for? How is it done? Evidence base Pros and cons Case study Baclofen GABA derivative (inhibitory neurotransmitter) Presynaptic
Intrathecal Baclofen Val Stevenson Plan What is it, how does it work? Who is it for? How is it done? Evidence base Pros and cons Case study Baclofen GABA derivative (inhibitory neurotransmitter) Presynaptic
Objectives MANAGEMENT OF DYSTONIA AND BREAKTHROUGH SEIZURES: THE ROLE OF PALLIATIVE CARE TEAMS. Neurological Impairment (NI) 10/24/18
 10/24/18") MANAGEMENT OF DYSTONIA AND BREAKTHROUGH SEIZURES: THE ROLE OF PALLIATIVE CARE TEAMS Julie Hauer, MD Maruzza Congress 24 October 2018 Objectives Appreciate central pain as a trigger for severe movement
MANAGEMENT OF DYSTONIA AND BREAKTHROUGH SEIZURES: THE ROLE OF PALLIATIVE CARE TEAMS Julie Hauer, MD Maruzza Congress 24 October 2018 Objectives Appreciate central pain as a trigger for severe movement
Drug Management of Parkinsonism. By Prof. Mohammad Saleh M. Hassan PhD. (Pharma); MSc. (Ped.); MHPE (Ed.)
; MSc. (Ped.); MHPE (Ed.)") Drug Management of Parkinsonism By Prof. Mohammad Saleh M. Hassan PhD. (Pharma); MSc. (Ped.); MHPE (Ed.) Drug management of Parkinsonism Levodopa Ergot derivatives noamine Oxidaes Inhibitors Catechol-Omethyl
Drug Management of Parkinsonism By Prof. Mohammad Saleh M. Hassan PhD. (Pharma); MSc. (Ped.); MHPE (Ed.) Drug management of Parkinsonism Levodopa Ergot derivatives noamine Oxidaes Inhibitors Catechol-Omethyl
Long term pharmacotherapy for Alcohol Dependence: Anti Craving agents
 Long term pharmacotherapy for Alcohol Dependence: Anti Craving agents Myth or Reality? Complete Recovery means a medication-free state True or False? Treatment of Alcoholism Assessment Motivation Alcohol
Long term pharmacotherapy for Alcohol Dependence: Anti Craving agents Myth or Reality? Complete Recovery means a medication-free state True or False? Treatment of Alcoholism Assessment Motivation Alcohol
Medications and Non-Pharma Approaches to Treatment. David J. Irwin, MD Penn Frontotemporal Degeneration Center
 Medications and Non-Pharma Approaches to Treatment David J. Irwin, MD Penn Frontotemporal Degeneration Center Outline Non-Pharmacological Treatment Strategies Behavior Language Motor Supportive Care Check-points
Medications and Non-Pharma Approaches to Treatment David J. Irwin, MD Penn Frontotemporal Degeneration Center Outline Non-Pharmacological Treatment Strategies Behavior Language Motor Supportive Care Check-points
Dr Barry Snow. Neurologist Auckland District Health Board
 Dr Barry Snow Neurologist Auckland District Health Board Dystonia and Parkinson s disease Barry Snow Gowers 1888: Tetanoid chorea Dystonia a movement disorder characterized by sustained or intermittent
Dr Barry Snow Neurologist Auckland District Health Board Dystonia and Parkinson s disease Barry Snow Gowers 1888: Tetanoid chorea Dystonia a movement disorder characterized by sustained or intermittent
Best Medical Treatments for Parkinson s disease
 Best Medical Treatments for Parkinson s disease Bernadette Schöneburg, M.D. June 20 th, 2015 What is Parkinson s Disease (PD)? Progressive neurologic disorder that results from the loss of specific cells
Best Medical Treatments for Parkinson s disease Bernadette Schöneburg, M.D. June 20 th, 2015 What is Parkinson s Disease (PD)? Progressive neurologic disorder that results from the loss of specific cells
10th Medicine Review Course st July Prakash Kumar
 10th Medicine Review Course 2018 21 st July 2018 Drug Therapy for Parkinson's disease Prakash Kumar National Neuroscience Institute Singapore General Hospital Sengkang General Hospital Singhealth Duke-NUS
10th Medicine Review Course 2018 21 st July 2018 Drug Therapy for Parkinson's disease Prakash Kumar National Neuroscience Institute Singapore General Hospital Sengkang General Hospital Singhealth Duke-NUS
10/13/2017. Disclosures. Deep Brain Stimulation in the Treatment of Movement Disorders. Deep Brain Stimulation: Objectives.
 Deep Brain Stimulation in the Treatment of Movement Disorders Disclosures None Eleanor K Orehek, M.D. Movement Disorders Specialist Noran Neurological Clinic 1 2 Objectives To provide an overview of deep
Deep Brain Stimulation in the Treatment of Movement Disorders Disclosures None Eleanor K Orehek, M.D. Movement Disorders Specialist Noran Neurological Clinic 1 2 Objectives To provide an overview of deep
Drug Class Review on Skeletal Muscle Relaxants
 Drug Class Review on FINAL REPORT January 2004 This report has not been reviewed or approved by the Agency for Healthcare Research and Quality Roger Chou, MD Kim Peterson, MS Oregon Evidence-based Practice
Drug Class Review on FINAL REPORT January 2004 This report has not been reviewed or approved by the Agency for Healthcare Research and Quality Roger Chou, MD Kim Peterson, MS Oregon Evidence-based Practice
No Financial Disclosures
 Deep Brain Stimulation: A Physician and Patient Perspective Jessica McClure Warren Marks, MD Cook Children s Medical Center Cook Children s Health Foundation Endowed Chair in Neurosciences Department of
Deep Brain Stimulation: A Physician and Patient Perspective Jessica McClure Warren Marks, MD Cook Children s Medical Center Cook Children s Health Foundation Endowed Chair in Neurosciences Department of
Movement disorders in childhood: assessment and diagnosis. Lucinda Carr
 Movement disorders in childhood: assessment and diagnosis Lucinda Carr Movement disorders in childhood: Assessment Classification Causes Diagnosis Presentation of movement disorders in childhood: Concerns
Movement disorders in childhood: assessment and diagnosis Lucinda Carr Movement disorders in childhood: Assessment Classification Causes Diagnosis Presentation of movement disorders in childhood: Concerns
Reflexes. Dr. Baizer
 Reflexes Dr. Baizer 1 Learning objectives: reflexes Students will be able to describe: 1. The clinical importance of testing reflexes. 2. The essential components of spinal reflexes. 3.The stretch reflex.
Reflexes Dr. Baizer 1 Learning objectives: reflexes Students will be able to describe: 1. The clinical importance of testing reflexes. 2. The essential components of spinal reflexes. 3.The stretch reflex.
VL VA BASAL GANGLIA. FUNCTIONAl COMPONENTS. Function Component Deficits Start/initiation Basal Ganglia Spontan movements
 BASAL GANGLIA Chris Cohan, Ph.D. Dept. of Pathology/Anat Sci University at Buffalo I) Overview How do Basal Ganglia affect movement Basal ganglia enhance cortical motor activity and facilitate movement.
BASAL GANGLIA Chris Cohan, Ph.D. Dept. of Pathology/Anat Sci University at Buffalo I) Overview How do Basal Ganglia affect movement Basal ganglia enhance cortical motor activity and facilitate movement.
Parkinson s Disease Medications: Professionals Edition
 Parkinson s Disease Clinic and Research Center University of California, San Francisco 505 Parnassus Ave., Rm. 795-M, Box 0114 San Francisco, CA 94143-0114 (415) 476-9276 http://pdcenter.neurology.ucsf.edu
Parkinson s Disease Clinic and Research Center University of California, San Francisco 505 Parnassus Ave., Rm. 795-M, Box 0114 San Francisco, CA 94143-0114 (415) 476-9276 http://pdcenter.neurology.ucsf.edu
Psychobiology Handout
 Nsg 85A / Psychiatric Page 1 of 7 Psychobiology Handout STRUCTURE AND FUNCTION OF THE BRAIN Psychiatric illness and the treatment of psychiatric illness alter brain functioning. Some examples of this are
Nsg 85A / Psychiatric Page 1 of 7 Psychobiology Handout STRUCTURE AND FUNCTION OF THE BRAIN Psychiatric illness and the treatment of psychiatric illness alter brain functioning. Some examples of this are
DRUGS THAT ACT IN THE CNS
 DRUGS THAT ACT IN THE CNS Anxiolytic and Hypnotic Drugs Dr Karamallah S. Mahmood PhD Clinical Pharmacology 1 OTHER ANXIOLYTIC AGENTS/ A. Antidepressants Many antidepressants are effective in the treatment
DRUGS THAT ACT IN THE CNS Anxiolytic and Hypnotic Drugs Dr Karamallah S. Mahmood PhD Clinical Pharmacology 1 OTHER ANXIOLYTIC AGENTS/ A. Antidepressants Many antidepressants are effective in the treatment
SCI FORUM Spasticity: Part 1. The Good, The Bad, and The Not So Ugly
 SCI FORUM Spasticity: Part 1 The Good, The Bad, and The Not So Ugly Rina Reyes, MD Amy Icarangal, PT Geralyn Bertelloti, OT January 13, 2015 http://sci.washington.edu/spasticity/ Overview: Spasticity
SCI FORUM Spasticity: Part 1 The Good, The Bad, and The Not So Ugly Rina Reyes, MD Amy Icarangal, PT Geralyn Bertelloti, OT January 13, 2015 http://sci.washington.edu/spasticity/ Overview: Spasticity
What does an EEG show?
 EEG Video EEG Ambulatory EEG There s a whole lot of Shakin going on Vagus Nerve Stimulators Division of Child Neurology, Developmental Pediatrics and Genetics Intrathecal Baclofen Pumps EEG first used
EEG Video EEG Ambulatory EEG There s a whole lot of Shakin going on Vagus Nerve Stimulators Division of Child Neurology, Developmental Pediatrics and Genetics Intrathecal Baclofen Pumps EEG first used
Introduction. 1 person in 20 will have an epileptic seizure at some time in their life
 Introduction 1 person in 20 will have an epileptic seizure at some time in their life Epilepsy is diagnosed on the basis of two or more epileptic seizures. Around 450,000 people in the UK have epilepsy
Introduction 1 person in 20 will have an epileptic seizure at some time in their life Epilepsy is diagnosed on the basis of two or more epileptic seizures. Around 450,000 people in the UK have epilepsy
Margo J Nell Dept Pharmacology
 Margo J Nell Dept Pharmacology 1 The extra pyramidal system Separation of cortico-spinal system (pyramidal system, (PS)) from the basal ganglia (extra pyramidal motor system (EPS)) because they produce
Margo J Nell Dept Pharmacology 1 The extra pyramidal system Separation of cortico-spinal system (pyramidal system, (PS)) from the basal ganglia (extra pyramidal motor system (EPS)) because they produce
Antiepileptic agents
 Antiepileptic agents Excessive excitability of neurons in the CNS Abnormal function of ion channels Spread through neural networks Abnormal neural activity leads to abnormal motor activity Suppression
Antiepileptic agents Excessive excitability of neurons in the CNS Abnormal function of ion channels Spread through neural networks Abnormal neural activity leads to abnormal motor activity Suppression
SECTION 9 : MANAGEMENT OF MOVEMENT DISORDERS AND EXTRAPYRAMIDAL SIDE EFFECTS
 SECTION 9 : MANAGEMENT OF MOVEMENT DISORDERS AND EXTRAPYRAMIDAL SIDE EFFECTS Formulary and Prescribing Guidelines 9.1 Introduction Movement disorders and extrapyramidal side effects can manifest in the
SECTION 9 : MANAGEMENT OF MOVEMENT DISORDERS AND EXTRAPYRAMIDAL SIDE EFFECTS Formulary and Prescribing Guidelines 9.1 Introduction Movement disorders and extrapyramidal side effects can manifest in the
Prior Authorization with Quantity Limit Program Summary
 Gocovri (amantadine) Prior Authorization with Quantity Limit Program Summary This prior authorization applies to Commercial, NetResults A series, SourceRx and Health Insurance Marketplace formularies.
Gocovri (amantadine) Prior Authorization with Quantity Limit Program Summary This prior authorization applies to Commercial, NetResults A series, SourceRx and Health Insurance Marketplace formularies.
Source: *Dystonia facts medically edited by: Charles Patrick Davis, MD, PhD
 Source: http://www.medicinenet.com/script/main/art.asp?articlekey=349 Dystonia facts* *Dystonia facts medically edited by: Charles Patrick Davis, MD, PhD Dystonia is a disorder of muscle control; it can
Source: http://www.medicinenet.com/script/main/art.asp?articlekey=349 Dystonia facts* *Dystonia facts medically edited by: Charles Patrick Davis, MD, PhD Dystonia is a disorder of muscle control; it can
Treatment of Parkinson s Disease and of Spasticity. Satpal Singh Pharmacology and Toxicology 3223 JSMBS
 Treatment of Parkinson s Disease and of Spasticity Satpal Singh Pharmacology and Toxicology 3223 JSMBS singhs@buffalo.edu 716-829-2453 1 Disclosures NO SIGNIFICANT FINANCIAL, GENERAL, OR OBLIGATION INTERESTS
Treatment of Parkinson s Disease and of Spasticity Satpal Singh Pharmacology and Toxicology 3223 JSMBS singhs@buffalo.edu 716-829-2453 1 Disclosures NO SIGNIFICANT FINANCIAL, GENERAL, OR OBLIGATION INTERESTS
INTRATHECAL THERAPY TREATMENT OF PAIN AND SPASTICITY. Christopher S. Rumana, M.D. Tallahassee Neurological Clinic Department of Neurosurgery
 INTRATHECAL THERAPY TREATMENT OF PAIN AND SPASTICITY Christopher S. Rumana, M.D. Tallahassee Neurological Clinic Department of Neurosurgery Intrathecal Therapy Insertion of a drug into CSF space, commonly
INTRATHECAL THERAPY TREATMENT OF PAIN AND SPASTICITY Christopher S. Rumana, M.D. Tallahassee Neurological Clinic Department of Neurosurgery Intrathecal Therapy Insertion of a drug into CSF space, commonly
Motor Fluctuations Stephen Grill, MD, PHD Parkinson s and Movement Disorders Center of Maryland and Johns Hopkins University
 Motor Fluctuations Stephen Grill, MD, PHD Parkinson s and Movement Disorders Center of Maryland and Johns Hopkins University I have no financial interest with any entity producing marketing, re-selling,
Motor Fluctuations Stephen Grill, MD, PHD Parkinson s and Movement Disorders Center of Maryland and Johns Hopkins University I have no financial interest with any entity producing marketing, re-selling,
Drugs used in Parkinsonism
 Drugs used in Parkinsonism قادة فريق علم األدوية : لي التميمي & عبدالرحمن ذكري الشكر موصول ألعضاء الفريق املتميزين : جومانة القحطاني ندى الصومالي روان سعد القحطاني pharma436@outlook.com @pharma436 Your
Drugs used in Parkinsonism قادة فريق علم األدوية : لي التميمي & عبدالرحمن ذكري الشكر موصول ألعضاء الفريق املتميزين : جومانة القحطاني ندى الصومالي روان سعد القحطاني pharma436@outlook.com @pharma436 Your
Benzodiazepines. Benzodiazepines
 : History 1950s - Invented by Swiss chemists who identified its sedative effects 1950s 60s - Chlordiazepoxide (Librium) marketed as a safer alternative to barbiturates; along with newer benzodiazepines
: History 1950s - Invented by Swiss chemists who identified its sedative effects 1950s 60s - Chlordiazepoxide (Librium) marketed as a safer alternative to barbiturates; along with newer benzodiazepines
4. Causes of spasticity a. Painful stimulation 1) Urinary tract infection or kidney stones
 Urinary tract infection or kidney stones") TELE-REHABILITATION GUIDELINE Medical Management of Spasticity in Spinal Cord Injury Drafted: July 6, 2014 Peer Reviewed: Finalized: July 28, 2014 I. Definition, Assessment, Diagnosis A. Definition 1.
TELE-REHABILITATION GUIDELINE Medical Management of Spasticity in Spinal Cord Injury Drafted: July 6, 2014 Peer Reviewed: Finalized: July 28, 2014 I. Definition, Assessment, Diagnosis A. Definition 1.
Lecture 5 Skeletal muscle relaxants. Pharmacologic management of parkinsonism and other movement disorders.
 Lecture 5 Skeletal muscle relaxants. Pharmacologic management of parkinsonism and other movement disorders. I. SKELETAL MUSCLE RELAXANTS Skeletal muscle relaxants are pharmacologically active substances
Lecture 5 Skeletal muscle relaxants. Pharmacologic management of parkinsonism and other movement disorders. I. SKELETAL MUSCLE RELAXANTS Skeletal muscle relaxants are pharmacologically active substances
Nausicalm solution for injection is a clear colourless solution, presented in 1 ml ampoules.
 Nausicalm Cyclizine lactate 50 mg/ml solution for injection Presentation Nausicalm solution for injection is a clear colourless solution, presented in 1 ml ampoules. Uses Actions Cyclizine is a piperazine
Nausicalm Cyclizine lactate 50 mg/ml solution for injection Presentation Nausicalm solution for injection is a clear colourless solution, presented in 1 ml ampoules. Uses Actions Cyclizine is a piperazine
The Nervous System S P I N A L R E F L E X E S
 The Nervous System S P I N A L R E F L E X E S Reflexes Rapid, involuntary, predictable motor response to a stimulus Spinal Reflexes Spinal somatic reflexes Integration center is in the spinal cord Effectors
The Nervous System S P I N A L R E F L E X E S Reflexes Rapid, involuntary, predictable motor response to a stimulus Spinal Reflexes Spinal somatic reflexes Integration center is in the spinal cord Effectors
Antidepressants and Sedatives. David G. Standaert, M.D., Ph.D. Massachusetts General Hospital Harvard Medical School
 Antidepressants and Sedatives David G. Standaert, M.D., Ph.D. Massachusetts General Hospital Harvard Medical School Depression A frequent problem, affecting up to 5% of the population Common presentations
Antidepressants and Sedatives David G. Standaert, M.D., Ph.D. Massachusetts General Hospital Harvard Medical School Depression A frequent problem, affecting up to 5% of the population Common presentations
THE MEDICAL AND SURGICAL TREATMENT OF DYSTONIA
 THE MEDICAL AND SURGICAL TREATMENT OF DYSTONIA Samuel Frank, MD Beth Israel Deaconess Medical Center Boston, MA Dystonia may present as an isolated disorder or as part of another disease process. The clinical
THE MEDICAL AND SURGICAL TREATMENT OF DYSTONIA Samuel Frank, MD Beth Israel Deaconess Medical Center Boston, MA Dystonia may present as an isolated disorder or as part of another disease process. The clinical
What Is Cerebral Palsy?
 Disclosures Management of Tone in Cerebral Palsy Hank Chambers, MD Rady Children s Hospital Professor of Clinical Orthopedic Surgery University of California at San Diego Personal Disclosures: Consultant:
Disclosures Management of Tone in Cerebral Palsy Hank Chambers, MD Rady Children s Hospital Professor of Clinical Orthopedic Surgery University of California at San Diego Personal Disclosures: Consultant:
Dystonias. How are the dystonias classified? One way of classifying the dystonias is according to the parts of the body they affect:
 Dystonias What are the dystonias? The dystonias are movement disorders in which sustained muscle contractions cause twisting and repetitive movements or abnormal postures. The movements, which are involuntary
Dystonias What are the dystonias? The dystonias are movement disorders in which sustained muscle contractions cause twisting and repetitive movements or abnormal postures. The movements, which are involuntary
Faculty. Joseph Friedman, MD
 Faculty Claire Henchcliffe, MD, DPhil Associate Professor of Neurology Weill Cornell Medical College Associate Attending Neurologist New York-Presbyterian Hospital Director of the Parkinson s Institute
Faculty Claire Henchcliffe, MD, DPhil Associate Professor of Neurology Weill Cornell Medical College Associate Attending Neurologist New York-Presbyterian Hospital Director of the Parkinson s Institute
Introductory Clinical Pharmacology Chapter 32 Antiparkinsonism Drugs
 Introductory Clinical Pharmacology Chapter 32 Antiparkinsonism Drugs Dopaminergic Drugs: Actions Symptoms of parkinsonism are caused by depletion of dopamine in CNS Amantadine: makes more of dopamine available
Introductory Clinical Pharmacology Chapter 32 Antiparkinsonism Drugs Dopaminergic Drugs: Actions Symptoms of parkinsonism are caused by depletion of dopamine in CNS Amantadine: makes more of dopamine available
Parkinson s Disease Current Treatment Options
 Parkinson s Disease Current Treatment Options Daniel Kassicieh, D.O., FAAN Sarasota Neurology, P.A. PD: A Chronic Neurodegenerative Ds. 1 Million in USA Epidemiology 50,000 New Cases per Year Majority
Parkinson s Disease Current Treatment Options Daniel Kassicieh, D.O., FAAN Sarasota Neurology, P.A. PD: A Chronic Neurodegenerative Ds. 1 Million in USA Epidemiology 50,000 New Cases per Year Majority
Pharmacologic Treatment of Parkinson s Disease. Nicholas J. Silvestri, M.D. Assistant Professor of Neurology
 + Pharmacologic Treatment of Parkinson s Disease Nicholas J. Silvestri, M.D. Assistant Professor of Neurology + Overview n Brief review of Parkinson s disease (PD) n Clinical manifestations n Pathophysiology
+ Pharmacologic Treatment of Parkinson s Disease Nicholas J. Silvestri, M.D. Assistant Professor of Neurology + Overview n Brief review of Parkinson s disease (PD) n Clinical manifestations n Pathophysiology
Parkinson s disease Therapeutic strategies. Surat Tanprawate, MD Division of Neurology University of Chiang Mai
 Parkinson s disease Therapeutic strategies Surat Tanprawate, MD Division of Neurology University of Chiang Mai 1 Scope Modality of treatment Pathophysiology of PD and dopamine metabolism Drugs Are there
Parkinson s disease Therapeutic strategies Surat Tanprawate, MD Division of Neurology University of Chiang Mai 1 Scope Modality of treatment Pathophysiology of PD and dopamine metabolism Drugs Are there
DR. JITENDRA PATEL (MBBS, MD) Medical Educator & Researcher
 Medical Educator & Researcher") 1 DR. JITENDRA PATEL (MBBS, MD) Medical Educator & Researcher Associate Professor in Physiology Email: dr.jrpatel84@gmail.com Web: www.esphys.weebly.com 2 OUTLINE Stretch reflex overview Muscle spindle
1 DR. JITENDRA PATEL (MBBS, MD) Medical Educator & Researcher Associate Professor in Physiology Email: dr.jrpatel84@gmail.com Web: www.esphys.weebly.com 2 OUTLINE Stretch reflex overview Muscle spindle
Drug Therapy of Parkinsonism. Assistant Prof. Dr. Najlaa Saadi PhD Pharmacology Faculty of Pharmacy University of Philadelphia
 Drug Therapy of Parkinsonism Assistant Prof. Dr. Najlaa Saadi PhD Pharmacology Faculty of Pharmacy University of Philadelphia Parkinsonism is a progressive neurological disorder of muscle movement, usually
Drug Therapy of Parkinsonism Assistant Prof. Dr. Najlaa Saadi PhD Pharmacology Faculty of Pharmacy University of Philadelphia Parkinsonism is a progressive neurological disorder of muscle movement, usually
GENETICS AND TREATMENT OF DYSTONIA
 GENETICS AND TREATMENT OF DYSTONIA Oksana Suchowersky, M.D., FRCPC, FCCMG Professor of Medicine, Medical Genetics, and Psychiatry Toupin Research Chair in Neurology DYSTONIA Definition: abnormal sustained
GENETICS AND TREATMENT OF DYSTONIA Oksana Suchowersky, M.D., FRCPC, FCCMG Professor of Medicine, Medical Genetics, and Psychiatry Toupin Research Chair in Neurology DYSTONIA Definition: abnormal sustained
Anxiolytic, Sedative and Hypnotic Drugs. Assistant Prof. Dr. Najlaa Saadi PhD Pharmacology Faculty of Pharmacy University of Philadelphia
 Anxiolytic, Sedative and Hypnotic Drugs Assistant Prof. Dr. Najlaa Saadi PhD Pharmacology Faculty of Pharmacy University of Philadelphia Anxiolytics: reduce anxiety Sedatives: decrease activity, calming
Anxiolytic, Sedative and Hypnotic Drugs Assistant Prof. Dr. Najlaa Saadi PhD Pharmacology Faculty of Pharmacy University of Philadelphia Anxiolytics: reduce anxiety Sedatives: decrease activity, calming
Types of epilepsy. 1)Generalized type: seizure activity involve the whole brain, it is divided into:
Generalized type: seizure activity involve the whole brain, it is divided into:") Types of epilepsy We have different types of epilepsy, so it is not one type of seizures that the patient can suffer from; we can find some patients with generalized or partial seizure. So, there are two
Types of epilepsy We have different types of epilepsy, so it is not one type of seizures that the patient can suffer from; we can find some patients with generalized or partial seizure. So, there are two
Anxiolytic & Hypnotic Drugs. Asst Prof Dr Inam S Arif
 Anxiolytic & Hypnotic Drugs Asst Prof Dr Inam S Arif isamalhaj@yahoo.com Anxiolytic & Hpnotic Agents Anxiety: unpleasant state of tension, apprehension or uneasiness, characterised by, tachycardia, sweating,
Anxiolytic & Hypnotic Drugs Asst Prof Dr Inam S Arif isamalhaj@yahoo.com Anxiolytic & Hpnotic Agents Anxiety: unpleasant state of tension, apprehension or uneasiness, characterised by, tachycardia, sweating,
Stretch reflex and Golgi Tendon Reflex. Prof. Faten zakareia Physiology Department, College of Medicine, King Saud University 2016
 Stretch reflex and Golgi Tendon Reflex Prof. Faten zakareia Physiology Department, College of Medicine, King Saud University 2016 Objectives: Upon completion of this lecture, students should be able to
Stretch reflex and Golgi Tendon Reflex Prof. Faten zakareia Physiology Department, College of Medicine, King Saud University 2016 Objectives: Upon completion of this lecture, students should be able to
Neural Basis of Motor Control
 Neural Basis of Motor Control Central Nervous System Skeletal muscles are controlled by the CNS which consists of the brain and spinal cord. Determines which muscles will contract When How fast To what
Neural Basis of Motor Control Central Nervous System Skeletal muscles are controlled by the CNS which consists of the brain and spinal cord. Determines which muscles will contract When How fast To what
Warm-Up. Label the parts of the neuron below.
 Warm-Up Label the parts of the neuron below. A B C D E F G Warm-Up 1. One neuron transmits a nerve impulse at 40 m/s. Another conducts at the rate of 1 m/s. Which neuron has a myelinated axon? 2. List
Warm-Up Label the parts of the neuron below. A B C D E F G Warm-Up 1. One neuron transmits a nerve impulse at 40 m/s. Another conducts at the rate of 1 m/s. Which neuron has a myelinated axon? 2. List
Involuntary Movements in Children and Adolescents: Is it Seizure, Tic or Something Else?
 Involuntary Movements in Children and Adolescents: Is it Seizure, Tic or Something Else? California Association of Nurse Practitioners Monterey, March 22, 2013 Julie Sprague-McRae, MS, RN, PPCNP-BC Ruth
Involuntary Movements in Children and Adolescents: Is it Seizure, Tic or Something Else? California Association of Nurse Practitioners Monterey, March 22, 2013 Julie Sprague-McRae, MS, RN, PPCNP-BC Ruth
History Parkinson`s disease. Parkinson's disease was first formally described in 1817 by a London physician named James Parkinson
 Parkinsonismm History Parkinson`s disease Parkinson's disease was first formally described in 1817 by a London physician named James Parkinson Definition : Parkinsonism: Parkinsonism is a progressive neurological
Parkinsonismm History Parkinson`s disease Parkinson's disease was first formally described in 1817 by a London physician named James Parkinson Definition : Parkinsonism: Parkinsonism is a progressive neurological
NERVOUS SYSTEM MODULE. Academic Year Study Guide
 NERVOUS SYSTEM MODULE Academic Year 2004-2005 Study Guide CNS Objectives At the end of this course, students should recognize the followings: 1. Histological structure of the brain meninges and the supporting
NERVOUS SYSTEM MODULE Academic Year 2004-2005 Study Guide CNS Objectives At the end of this course, students should recognize the followings: 1. Histological structure of the brain meninges and the supporting
Medication Management & Strategies When the levodopa honeymoon is over
 Medication Management & Strategies When the levodopa honeymoon is over Eric J Pappert, MD Parkinson s Disease & Movement Disorders Center Neurology Associates Medication Options in Parkinson s Carbidopa/Levodopa
Medication Management & Strategies When the levodopa honeymoon is over Eric J Pappert, MD Parkinson s Disease & Movement Disorders Center Neurology Associates Medication Options in Parkinson s Carbidopa/Levodopa
This guide describes some of the important facts about Neurobloc that you need to be aware of, however, it does not replace the advice given to you
 This guide describes some of the important facts about Neurobloc that you need to be aware of, however, it does not replace the advice given to you by a healthcare professional. Further very important
This guide describes some of the important facts about Neurobloc that you need to be aware of, however, it does not replace the advice given to you by a healthcare professional. Further very important
IMPORTANT: PLEASE READ
 PART III: CONSUMER INFORMATION Pr BACLOFEN Baclofen Tablets 10 mg and 20 mg This leaflet is part III of a three-part "Product Monograph" published when BACLOFEN was approved for sale in Canada and is designed
PART III: CONSUMER INFORMATION Pr BACLOFEN Baclofen Tablets 10 mg and 20 mg This leaflet is part III of a three-part "Product Monograph" published when BACLOFEN was approved for sale in Canada and is designed
Movement disorders. Dr Rick Leventer Royal Children s Hospital
 Movement disorders Dr Rick Leventer Royal Children s Hospital richard.leventer@rch.org.au Movement disorders! conditions that affect the speed, fluency, quality, and ease of movement! usually affect TONE
Movement disorders Dr Rick Leventer Royal Children s Hospital richard.leventer@rch.org.au Movement disorders! conditions that affect the speed, fluency, quality, and ease of movement! usually affect TONE
What is dystonia? Types of dystonia
 My Dystonia Journey My Dystonia Journey My name is Liam Carbery and I suffer from generalised dystonia affecting most of my body. I hope when you are reading this, it will give you an insight into the
My Dystonia Journey My Dystonia Journey My name is Liam Carbery and I suffer from generalised dystonia affecting most of my body. I hope when you are reading this, it will give you an insight into the
NeuroPsychiatry Block
 NeuroPsychiatry Block Stretch reflex and Golgi Tendon Reflex By Prof. Faten zakareia Physiology Department, College of Medicine, King Saud University 2017 Email: Faten@ksu.edu.sa Ext:52736 NeuroPsychiatryBlock
NeuroPsychiatry Block Stretch reflex and Golgi Tendon Reflex By Prof. Faten zakareia Physiology Department, College of Medicine, King Saud University 2017 Email: Faten@ksu.edu.sa Ext:52736 NeuroPsychiatryBlock
Guidelines MANAGEMENT OF MAJOR DEPRESSIVE DISORDER (MDD)
") MANAGEMENT OF MAJOR DEPRESSIVE DISORDER (MDD) Guidelines CH Lim, B Baizury, on behalf of Development Group Clinical Practice Guidelines Management of Major Depressive Disorder A. Introduction Major depressive
MANAGEMENT OF MAJOR DEPRESSIVE DISORDER (MDD) Guidelines CH Lim, B Baizury, on behalf of Development Group Clinical Practice Guidelines Management of Major Depressive Disorder A. Introduction Major depressive
Pharmacologic Treatment of Parkinson s Disease. Nicholas J. Silvestri, M.D. Associate Professor of Neurology
 + Pharmacologic Treatment of Parkinson s Disease Nicholas J. Silvestri, M.D. Associate Professor of Neurology + Disclosures n NO SIGNIFICANT FINANCIAL, GENERAL, OR OBLIGATION INTERESTS TO REPORT + Learning
+ Pharmacologic Treatment of Parkinson s Disease Nicholas J. Silvestri, M.D. Associate Professor of Neurology + Disclosures n NO SIGNIFICANT FINANCIAL, GENERAL, OR OBLIGATION INTERESTS TO REPORT + Learning
Treatment of Parkinson s Disease: Present and Future
 Treatment of Parkinson s Disease: Present and Future Karen Blindauer, MD Professor of Neurology Director of Movement Disorders Program Medical College of Wisconsin Neuropathology: Loss of Dopamine- Producing
Treatment of Parkinson s Disease: Present and Future Karen Blindauer, MD Professor of Neurology Director of Movement Disorders Program Medical College of Wisconsin Neuropathology: Loss of Dopamine- Producing
Parkinson s Disease. Prevalence. Mark S. Baron, M.D. Cardinal Features. Clinical Characteristics. Not Just a Movement Disorder
 Prevalence Parkinson s Disease Mark S. Baron, M.D. Associate Professor of Neurology Movement Disorders Section VCU School of Medicine Common disorder Approaching 1% by 65 yrs of age, 2% by 80 yrs of age
Prevalence Parkinson s Disease Mark S. Baron, M.D. Associate Professor of Neurology Movement Disorders Section VCU School of Medicine Common disorder Approaching 1% by 65 yrs of age, 2% by 80 yrs of age
NERVOUS SYSTEM NERVOUS SYSTEM. Somatic nervous system. Brain Spinal Cord Autonomic nervous system. Sympathetic nervous system
 SYNAPTIC NERVOUS SYSTEM NERVOUS SYSTEM CENTRAL NERVOUS SYSTEM PERIPHERAL NERVOUS SYSTEM Brain Spinal Cord Autonomic nervous system Somatic nervous system Sympathetic nervous system Parasympathetic nervous
SYNAPTIC NERVOUS SYSTEM NERVOUS SYSTEM CENTRAL NERVOUS SYSTEM PERIPHERAL NERVOUS SYSTEM Brain Spinal Cord Autonomic nervous system Somatic nervous system Sympathetic nervous system Parasympathetic nervous
Program Highlights. Michael Pourfar, MD Co-Director, Center for Neuromodulation New York University Langone Medical Center New York, New York
 Program Highlights David Swope, MD Associate Professor of Neurology Mount Sinai Health System New York, New York Michael Pourfar, MD Co-Director, Center for Neuromodulation New York University Langone
Program Highlights David Swope, MD Associate Professor of Neurology Mount Sinai Health System New York, New York Michael Pourfar, MD Co-Director, Center for Neuromodulation New York University Langone
How to Effectively Manage the Motor Symptoms of HD
 How to Effectively Manage the Motor Symptoms of HD Yvette Bordelon, MD, PhD Associate Clinical Professor of Neurology David Geffen School of Medicine at UCLA The information provided by speakers in workshops,
How to Effectively Manage the Motor Symptoms of HD Yvette Bordelon, MD, PhD Associate Clinical Professor of Neurology David Geffen School of Medicine at UCLA The information provided by speakers in workshops,
Movement Disorders: A Brief Overview
 Movement Disorders: A Brief Overview Albert Hung, MD, PhD Massachusetts General Hospital Harvard Medical School August 17, 2006 Cardinal Features of Parkinsonism Tremor Rigidity Bradykinesia Postural imbalance
Movement Disorders: A Brief Overview Albert Hung, MD, PhD Massachusetts General Hospital Harvard Medical School August 17, 2006 Cardinal Features of Parkinsonism Tremor Rigidity Bradykinesia Postural imbalance
Lacosamide (Vimpat) for partial-onset epilepsy monotherapy. December 2011
 for partial-onset epilepsy monotherapy. December 2011") Lacosamide (Vimpat) for partial-onset epilepsy monotherapy This technology summary is based on information available at the time of research and a limited literature search. It is not intended to be a
Lacosamide (Vimpat) for partial-onset epilepsy monotherapy This technology summary is based on information available at the time of research and a limited literature search. It is not intended to be a
III./3.1. Movement disorders with akinetic rigid symptoms
 III./3.1. Movement disorders with akinetic rigid symptoms III./3.1.1. Parkinson s disease Parkinson s disease (PD) is the second most common neurodegenerative disorder worldwide after Alzheimer s disease.
III./3.1. Movement disorders with akinetic rigid symptoms III./3.1.1. Parkinson s disease Parkinson s disease (PD) is the second most common neurodegenerative disorder worldwide after Alzheimer s disease.
Movement Disorders Will Garrett, M.D Assistant Professor of Neurology
 Movement Disorders Will Garrett, M.D Assistant Professor of Neurology I. The Basal Ganglia The basal ganglia are composed of several structures including the caudate and putamen (collectively called the
Movement Disorders Will Garrett, M.D Assistant Professor of Neurology I. The Basal Ganglia The basal ganglia are composed of several structures including the caudate and putamen (collectively called the
Symptomatic Treatment of MS
 Symptomatic Treatment of MS Prof. Per Soelberg Sørensen Danish MS Center, Department of Neurology Copenhagen University Hospital Righospitalet, Copenhagen, Denmark Symptomatic treatment of spinal cord
Symptomatic Treatment of MS Prof. Per Soelberg Sørensen Danish MS Center, Department of Neurology Copenhagen University Hospital Righospitalet, Copenhagen, Denmark Symptomatic treatment of spinal cord
Disorders of Movement M A R T I N H A R L E Y N E U R O L O G Y
 Disorders of Movement M A R T I N H A R L E Y N E U R O L O G Y Educational Objectives Improved history taking in patients with movement disorders. Develop a systematic approach to observing and describing
Disorders of Movement M A R T I N H A R L E Y N E U R O L O G Y Educational Objectives Improved history taking in patients with movement disorders. Develop a systematic approach to observing and describing
Managing Medical Complications of Brain Injury. Katie Turpin, NP-C
 Managing Medical Complications of Brain Injury Katie Turpin, NP-C Objectives: 1. Describe the role of the medical team in a setting focused on therapy/rehabilitation. 2. Identify common disabilities or
Managing Medical Complications of Brain Injury Katie Turpin, NP-C Objectives: 1. Describe the role of the medical team in a setting focused on therapy/rehabilitation. 2. Identify common disabilities or
Goals for sedation during mechanical ventilation
 New Uses of Old Medications Gina Riggi, PharmD, BCCCP, BCPS Clinical Pharmacist Trauma ICU Jackson Memorial Hospital Disclosure I do not have anything to disclose Objectives Describe the use of ketamine
New Uses of Old Medications Gina Riggi, PharmD, BCCCP, BCPS Clinical Pharmacist Trauma ICU Jackson Memorial Hospital Disclosure I do not have anything to disclose Objectives Describe the use of ketamine
Anxiolytic and Hypnotic drugs
 Anxiolytic and Hypnotic drugs Anxiolytic and Hypnotic drugs Anxiety is unpleasant state of tension and fear that seems to arise from unknown source. The symptoms of severe anxiety are similar to those
Anxiolytic and Hypnotic drugs Anxiolytic and Hypnotic drugs Anxiety is unpleasant state of tension and fear that seems to arise from unknown source. The symptoms of severe anxiety are similar to those
Drugs Used In Management Of Pain. Dr. Aliah Alshanwani
 Drugs Used In Management Of Pain Dr. Aliah Alshanwani 1 Drugs Used In Management Of Pain A CASE OF OVERDOSE Sigmund Freud, the father of psychoanalysis His cancer of the jaw was causing him increasingly
Drugs Used In Management Of Pain Dr. Aliah Alshanwani 1 Drugs Used In Management Of Pain A CASE OF OVERDOSE Sigmund Freud, the father of psychoanalysis His cancer of the jaw was causing him increasingly
Understanding Dystonia
 Understanding Dystonia Sand Sharks Anthony Richardsen, Lindsey Rathbun, Evan Harrington, Chris Erzen The Essentials What, Why, How What is Dystonia? Dystonias are movement disorders often characterized
Understanding Dystonia Sand Sharks Anthony Richardsen, Lindsey Rathbun, Evan Harrington, Chris Erzen The Essentials What, Why, How What is Dystonia? Dystonias are movement disorders often characterized
Optimizing Clinical Communication in Parkinson s Disease:
 Optimizing Clinical Communication in Parkinson s Disease:,Strategies for improving communication between you and your neurologist PFNCA Symposium March 25, 2017 Pritha Ghosh, MD Assistant Professor of
Optimizing Clinical Communication in Parkinson s Disease:,Strategies for improving communication between you and your neurologist PFNCA Symposium March 25, 2017 Pritha Ghosh, MD Assistant Professor of
United Council for Neurologic Subspecialties Geriatric Neurology Written Examination Content Outline
 United Council for Neurologic Subspecialties Geriatric Neurology Written Examination Content Outline REV 3/24/09 The UCNS Geriatric Neurology examination was established to determine the level of competence
United Council for Neurologic Subspecialties Geriatric Neurology Written Examination Content Outline REV 3/24/09 The UCNS Geriatric Neurology examination was established to determine the level of competence
Stiff Person Syndrome
 Stiff Person Syndrome ก ก 17 2548.. ก ก ก - In summer of 1924, Iowa farmer,49 yr - Muscle stiffness and difficulty in walk - His disability had begun insidiously 4 yr earlier and become so serious that
Stiff Person Syndrome ก ก 17 2548.. ก ก ก - In summer of 1924, Iowa farmer,49 yr - Muscle stiffness and difficulty in walk - His disability had begun insidiously 4 yr earlier and become so serious that
Chapter 20. Media Directory. Amyotrophic Lateral Sclerosis. Alzheimer s Disease. Huntington s Chorea. Multiple Sclerosis
 Chapter 20 Drugs for Degenerative Diseases of the Nervous System Slide 18 Media Directory Levadopa Animation Upper Saddle River, New Jersey 07458 All rights reserved. Alzheimer s Disease Amyotrophic Lateral
Chapter 20 Drugs for Degenerative Diseases of the Nervous System Slide 18 Media Directory Levadopa Animation Upper Saddle River, New Jersey 07458 All rights reserved. Alzheimer s Disease Amyotrophic Lateral
Antidepressants: Prof. Riyadh Al_Azzawi F.R.C.Psych
 Antidepressants: Prof. Riyadh Al_Azzawi F.R.C.Psych A. Heterocyclic antidepressants: (tricyclic and tetracyclic ), e.g.amitryptaline,imipramine. B. Monoamine oxidase inhibitors(m.a.o.i), e.g.phenelzine.
Antidepressants: Prof. Riyadh Al_Azzawi F.R.C.Psych A. Heterocyclic antidepressants: (tricyclic and tetracyclic ), e.g.amitryptaline,imipramine. B. Monoamine oxidase inhibitors(m.a.o.i), e.g.phenelzine.
Presenter. Dr. Ronald Lucchino
 Adverse Drug Reactions in Adults with Down Syndrome Presenter Dr. Ronald Lucchino rvluc@comcast.net PURPOSE To increase staff awareness that older adults with DD may have higher levels of medication in
Adverse Drug Reactions in Adults with Down Syndrome Presenter Dr. Ronald Lucchino rvluc@comcast.net PURPOSE To increase staff awareness that older adults with DD may have higher levels of medication in