Warrior Personal Training Registration Packet
|
|
|
- Garry Jefferson
- 5 years ago
- Views:
Transcription
1




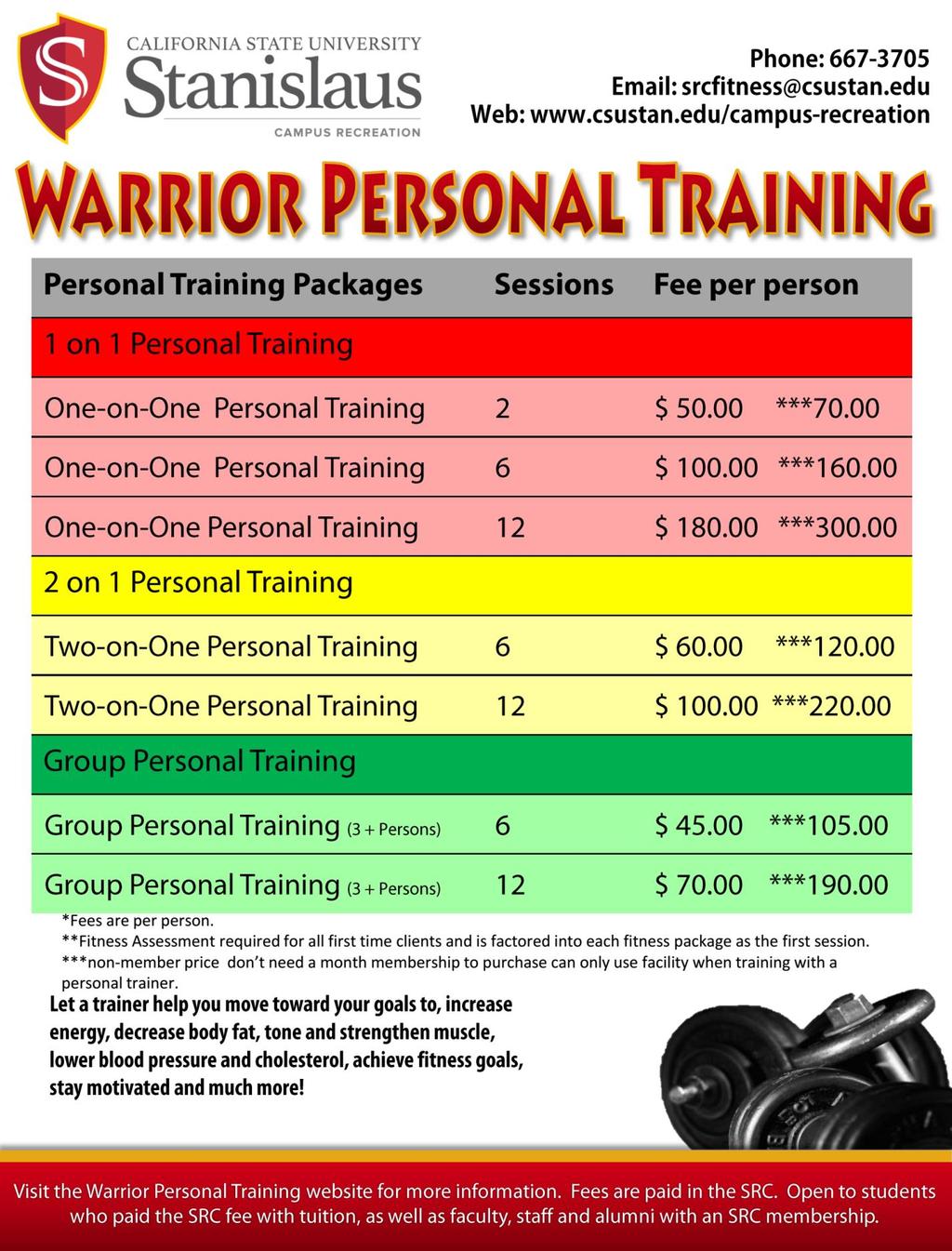
2 Warrior Personal Training Registration Packet Information and Policies This is personal training tailored to help you reach your desired fitness level. Your exercise program will be personalized to help you excel in your fitness goals. The SRC s personal trainers will discuss your exercise and health history, as well as your personal goals then prescribe an exercise regimen to fit your needs. Let a trainer help you increase energy and flexibility decrease body fat tone and strengthen muscle optimize time during workouts achieve personal fitness goals stay motivated and consistent decrease risk of injury improve cardio health & quality of life lower blood pressure and cholesterol begin exercising for the first time train like a competitive athlete learn proper biomechanics and methodology Fitness Assessment Includes body composition, cardiovascular endurance, flexibility assessment, muscular strength and endurance. The assessment is required for all first time participants. Personal Training One-on-One Personal Training An efficient workout program designed just for you to improve your health and fitness level! Must complete a Fitness Assessment Session with your chosen trainer. Two-on-One Personal Training (2 Individuals to 1 Trainer) Do you have similar training goals as a friend or maybe you want a partner to attack your fitness pursuits with the additional support and encouragement? Then hit the training floor and experience the challenge together. It is recommended that your training partner be of a similar fitness level. Requires both clients at each session. Must complete a Fitness Assessment with your chosen trainer. Group Personal Training (3+ Individuals to 1 Trainer) This is an alternative to one-on-one training and can be programmed for any style. Invite friends and clubs to join for a friendly competition. All participants required at each session. Registration and payment will need to be made as a group. Fitness Assessment recommended but not required for large group sessions. All sessions (assessments and personal training) are 60 minutes and must be purchased prior to training sessions. Only SRC Personal Trainers are allowed to conduct personal training in the Fitness Center. Cancellations & Tardiness Sessions must be cancelled 24 hours in advance to avoid being charged for a no-show. Participants will be charged for all no-show sessions. All clients and trainers are required to arrive at the scheduled time. If you are more than 15 minutes late to your session, you will be charged for the full session. Refunds & Expirations There are no refunds for sessions purchased. Refunds or credits will not be issued for unused sessions. All sessions expire by the end of the current semester/term. See the WPT website for session expiration dates. How to Sign Up Open to students who paid the SRC fee with tuition, as well as faculty, staff and alumni with an SRC membership. Complete the attached registration forms and take to the SRC to pay your fees (cash, check or Warrior Cash only). Once fees are paid you will be contacted by a trainer in 2 3 business days. Returning Clients Clients who have completed the number of sessions purchased must re-submit their registration packet. The fitness assessment does not need to be redone. I have read and understand the above Warrior Personal Training information and policies. Initials
3 Personal Information Warrior Personal Training Medical Questionnaire Check only one: Student Faculty Staff Alumni Warrior ID: Check only one: New Client Returning Client Last Name First Name Ml Address Home Phone Cell Phone Home Address City State Zip Code Emergency Contact Emergency Contact Phone Relationship to Member Gender Age of Birth (MM/DD/YYYY) Height Weight Cardiovascular Risk Please check any that apply to you: High Blood Pressure High Cholesterol Diabetes Heart Disease Bypass Surgery Stroke Do you presently smoke cigarettes? Yes No If yes, how many per day? Do you ever experience chest pains or tightness? Yes No Do you ever experience unusual shortness of breath during mild physical activity? Yes No Do you have asthma? Yes No Are you currently under doctor s care for a heart condition and need medically supervised activity? Yes No If yes, please explain: Personal History of last: Physical Exam Blood Cholesterol test Blood Pressure test Do you have any allergies? Yes No If yes, please list: Are you presently taking any medication? Yes No If so, list name and purpose: Do you ever experience dizziness during vigorous physical activity? Yes No Have you ever passed out during vigorous physical activity? Yes No If you are female, are you currently pregnant? Yes No Do you have or have had an eating disorder? Yes No Have you had any recent surgeries? Yes No If yes, describe: Do you have any other medical conditions why you should not do physical activity? Yes No If yes, please explain: Injuries Please check any of the below injuries you have had. Specify which bone, muscle, joint, etc., and year of the injury: broken bones Muscle strain/sprain Ligament, tendon, or cartilage Are you being treated for any of the above injuries? Yes No If yes, please specify the type of treatment: Joint injury or chronic pain Back injury or chronic pain Other
4 Lifestyle What is your activity level? Sedentary Moderate High Do you have a regular exercise program? Yes No If yes, please describe: Do you take any nutritional supplements or follow a special diet (vegetarian, low-calorie, gluten free, etc.)? Yes No If yes, please explain: Which meals do you consume in an average day (including snacks): Breakfast Snack Lunch Snack Dinner Snack What is your average energy level? Low High How many hours of sleep to you get on average? Goals Please check all activities you are interested in participating: Weight training Stationary bike Group Ex class Walking Running Other How much time do you want to spend working out? List any specific exercises that do not interest you or might cause you pain or discomfort: What goals do you have concerning your training and health? (i.e. weight loss, muscular growth, etc.) How ready are you to make changes to your current lifestyle? (circle one) Not Ready Extremely Ready Other How did you hear about the Personal Training program? Trainer Preference: Male Female No Preference Requested Trainer: Preferred Method of Communication (check one) Phone Either Please indicate your time preference below: Sunday Monday Tuesday Wednesday Thursday Friday Saturday Two-on-One and Large Group Sessions If you are purchasing the two-on-one or large group package you must designate one person as the primary person for contact purposes. Primary Contact: Other Participants in Group - Last Name, First Name (attach additional sheet if necessary: I have read, understood and completed this questionnaire. I have read and will comply with program information and policies. Any questions I had were answered to my full satisfaction. Member Signature Parent/Guardian Signature if under 18 years of age.
5 CALIFORNIA STATE UNIVERSITY, STANISLAUS STUDENT RECREATION COMPLEX RELEASE AND INFORMED CONSENT STATEMENT In consideration for receiving permission for use of facilities, and taking part in programs held at the Student Recreation Complex at the California State University, Stanislaus, I, for myself, my heirs, personal representative(s) and assigns hereby represent and agree as follows: 1. I understand participation is not part of the academic curriculum or job requirements of the University and are completely voluntary on my part. 2. I fully recognize and understand that there are risks and hazards, both minor and serious, associated with participation, which cannot be eliminated regardless of the care taken to avoid injury. Such risks include but are not limited to: lost, damaged or stolen personal property; cuts, scrapes, bruises, broken bones, muscle strains, pulls or tears, other bodily injuries, illness, temporary or permanent disabilities, paralysis and death. 3. I understand that physical activity requires a minimum level of fitness for safe participation. I also understand that the Student Recreation Complex advises that participants have a physical examination to determine their fitness for participation. I further understand that the Student Recreation Complex and California State University, Stanislaus do not provide medical, health or other insurance for participants. 4. Knowing the dangers, hazards and risks associated with participation in fitness and recreational activities, I voluntarily assume all responsibility and risk of loss, damage, illness and/or injury to my person or property in any way associated with my participation. 5. I agree to abide by all rules and regulations applicable to participation. 6. To the fullest extent permitted by law, I hereby release and forever discharge, and agree not to sue and to indemnify and hold harmless, the State of California, the Trustees of California State University, California State University, Stanislaus, the Student Recreation Complex, and their auxiliaries, officers, directors, agents, employees and volunteers from and against any and all liabilities, claims, demands and causes of action of any kind on account of any loss, damage, illness or injury to person or property in any way arising out of or relating to my participation in the use of the facilities or equipment, whether due to the negligence, default or other action or inaction of any person or entity. 7. I give California State University, Stanislaus, the absolute right and permission to use my photograph in its promotional materials and publicly efforts. I understand that the photographs may be used in a publication, print ad, direct-mail piece, electronic media, website, or other forms of promotion. I release the University, the photographer, their offices, employees, agents, and designees from liability for any violation of any personal or proprietary right I may have in connection with such use. I HAVE READ AND FULLY UNDERSTAND THIS RELEASE AND INFORMED CONSENT FORM, AND I SIGN IT VOLUNTARILY WITH FULL KNOWLEDGE OF ITS SIGNIFICANCE. First Name (Please Print) MI Last Name Warrior ID# Signature of Participant PARENT/GUARDIAN AGREEMENT (if under 18 years old) I am the Parent/Guardian of the above mentioned participant who is a minor child (under 18 Years old). By signing as Parent and Guardian, I agree as Parent and Guardian, on behalf of the Participant, to the entire above Release and Informed Consent Statement. Parent/Guardian Name (Print) Parent/Guardian Signature Parent/Guardian Phone Number
6 Warrior Personal Training Readiness Questionnaire Regular physical activity is fun and healthy, and increasingly more people are starting to become more active every day. Being more active is very safe for most people. However, some people should check with their doctor before they start becoming much more physically active. If you are planning to become much more physically active than you are now, start by answering the questions in the box below. If you are above the age of 15, the questionnaire will tell you if you should check with your doctor before you start. The American College of Sports Medicine (ACSM) guidelines required that men over the age of 45 and women over the age of 55 complete a Medical Authorization Form BEFORE training. Readiness Questionnaire YES NO Are you a man over the age of 45 or a woman over the age of 55 with a family history of heart disease? Has your doctor ever said that you have a heart condition and that you should only do physical activity recommended by a doctor? Do you feel pain in your chest when you do physical activity? In the past month, have you had chest pain when you were not doing physical activity? Do you lose your balance because of dizziness or do you ever lose consciousness? Do you have a bone or joint problem that could be made worse by a change in your physical activity? Is your doctor currently prescribing drugs (for example, water pills) for your blood pressure or heart condition? Do you know of any other reason why you should not do physical activity? Questionnaire Results If you answered YES to one or more questions you will need to complete the Medical Authorization Form BEFORE you start your sessions with your personal trainer or become more physically active. Tell your doctor about the Readiness Questionnaire and to which questions you answered YES. NOTE: You may be able to do any activity you want as long as you start slowly and build up gradually. Or, you may need to restrict your activities to those which are safe for you. Talk with your doctor about the kinds of activities you wish to participate in and follow his/her advice. If you answered NO (honestly) to all Readiness Questionnaire questions you can be reasonably sure that you can become more physically active and take part in a fitness appraisal/training. Other Considerations: If you are or may be pregnant talk with your doctor before you start becoming more active. If your health changes so that you then answer YES to any of the above questions, tell your fitness or health professional and discuss whether you should change your physical activity plan. I have read, understood and completed this questionnaire. Any questions I had were answered to my full satisfaction. Last Name First Name MI Member Signature Parent/Guardian Signature if under 18 years of age. Witness
7 Warrior Personal Training Readiness Questionnaire Clarifications For most people, physical activity should not pose any problem or hazard. The questionnaire has been designed to identify the small number of adults for whom physical activity might be inappropriate and those who should have medical advice concerning the type of activity most suitable. 1. Has a doctor ever said that you have a heart condition and that you should only do physical activity recommended by a doctor? Persons with known heart disease are at increased risk for cardiac complications during exercise. They should consult a physician and undergo exercise testing before starting an exercise program in order to ensure that exercise prescription follow standard guidelines for cardiac patients. Note: Medical supervision may be required during exercise training. 2. Do you feel pain in your chest when you do physical activity? See question In the past month, have you had chest pain when you were not doing physical activity? A physician should be consulted to identify the cause of chest pain, whether it occurs at rest or with exertion. If ischemic in origin, the condition should be stabilized before starting an exercise program. Exercise testing should be performed with the patient on his or her usual medication and the exercise prescription formulated in accordance with standard guidelines for cardiac patients. 4. Do you lose your balance because of dizziness or do you ever lose consciousness? A physician should be consulted to establish the cause of these symptoms, which may be related to potentially lifethreatening medical conditions. Exercise training should not be undertaken until serious cardiac disorders have been excluded. 5. Do you have a bone or joint problem that could be made worse by a change in your physical activity? Existing musculoskeletal disorders may be exacerbated by inappropriate exercise training. Persons with forms of arthritis known to be associated with a systemic component (for example, rheumatoid arthritis) may be at an increased risk for exercise-related medical complications. A physician should be consulted to determine whether any special procedures are required during exercise training. 6. Is your doctor currently prescribing drugs (for example, water pills) for your blood pressure or heart condition? See question 1. Medication effects should be considered when formulating the exercise prescription. The exercise prescription should be formulated in accordance with guidelines or the specific cardiovascular disease for which medications are being used. A physician should be consulted to determine whether the condition of factor requires special precautions during exercise training or contraindicates exercise training. 7. Do you know of any other reasons why you should not do physical activity? The exercise prescription may have to be modified in accordance with the specific reason provided.
8 California State University, Stanislaus Student Recreation Complex 1 University Circle Turlock, CA (209) Warrior Personal Training Medical Release Dear Doctor: Your patient,, wishes to start a personalized training program through the CSU Stanislaus, Student Recreation Complex Warrior Personal Training program. Exercise recommendations provided by the trainer will start easy and become progressively more intense depending on the client s goal and fitness level. If you know of any medical or other reasons why participation in the program by the client would be unwise please indicate so on this form. Physician Report I know of no reason why the applicant may not participate I believe the client can participate, but I urge caution for the following reasons: My patient is taking medications that will affect heart rate response to exercise. The effects of which are indicated below: Type of medication Effect Exercise Restrictions The client should not engage in the following activities: I recommend that the client NOT participate. Physician s Name (please print) Phone Physician s Signature
Personal Training Program Information and Policies
 Personal Training Program Information and Policies Welcome to the Student Recreation Center s (SRC) Personal Training Program! We are delighted that you chose us as a part of your commitment to health
Personal Training Program Information and Policies Welcome to the Student Recreation Center s (SRC) Personal Training Program! We are delighted that you chose us as a part of your commitment to health
Jumpstart, Fitness Assessment, & Body Composition
 Jumpstart, Fitness Assessment, & Body Composition Waiver, Release and Hold Harmless Agreement In consideration of permission granted by Purdue University allowing me to participate in Personal Training
Jumpstart, Fitness Assessment, & Body Composition Waiver, Release and Hold Harmless Agreement In consideration of permission granted by Purdue University allowing me to participate in Personal Training
Waiver, Release and Hold Harmless Agreement Personal Training Services
 Waiver, Release and Hold Harmless Agreement Personal Training Services I,, the undersigned, affirm that I am participating voluntarily in Personal Training Services. (Print name) I (together with my parent
Waiver, Release and Hold Harmless Agreement Personal Training Services I,, the undersigned, affirm that I am participating voluntarily in Personal Training Services. (Print name) I (together with my parent
CU Recreation Center
 CU Recreation Center Personal Training Congratulations on your decision to invest in yourself! Our qualified, nationally certified personal trainers will provide you with the right information and right
CU Recreation Center Personal Training Congratulations on your decision to invest in yourself! Our qualified, nationally certified personal trainers will provide you with the right information and right
New Client Reformer Session Packet
 New Client Reformer Session Packet Welcome and thank you for your interest in the Pilates Reformer program with University Recreation. You are taking the first steps towards improved health and wellness.
New Client Reformer Session Packet Welcome and thank you for your interest in the Pilates Reformer program with University Recreation. You are taking the first steps towards improved health and wellness.
FORMS 1) PAR Q & YOU:
 PAR Q & YOU:") Personal Training New Client Registration Congratulations on taking the first step to healthier and better you! The certified trainers are screened by the Vanderbilt Recreation & Wellness Center (the Rec)
Personal Training New Client Registration Congratulations on taking the first step to healthier and better you! The certified trainers are screened by the Vanderbilt Recreation & Wellness Center (the Rec)
Personal Training Registration Packet
 Personal Training Registration Packet Client Name: Date: Program Information and Policies Welcome to the UCSB Personal Training Program! We are delighted that you chose us as a part of your commitment
Personal Training Registration Packet Client Name: Date: Program Information and Policies Welcome to the UCSB Personal Training Program! We are delighted that you chose us as a part of your commitment
GEORGE MASON UNIVERSITY PERSONAL TRAINING REGISTRATION FORM NEW CLIENT
 GEORGE MASON UNIVERSITY PERSONAL TRAINING REGISTRATION FORM NEW CLIENT PLEASE PRINT, COMPLETE, AND DELIVER THIS FORM TO THE AQUATIC and FITNESS CENTER, RAC, OR SKYLINE FITNESS FRONT DESK: Ethan Carter
GEORGE MASON UNIVERSITY PERSONAL TRAINING REGISTRATION FORM NEW CLIENT PLEASE PRINT, COMPLETE, AND DELIVER THIS FORM TO THE AQUATIC and FITNESS CENTER, RAC, OR SKYLINE FITNESS FRONT DESK: Ethan Carter
FORMS 1) PAR Q & YOU:
 PAR Q & YOU:") Personal Training New Client Registration Congratulations on taking the first step to healthier and better you! The certified trainers are screened by the Vanderbilt Recreation & Wellness Center (the Rec)
Personal Training New Client Registration Congratulations on taking the first step to healthier and better you! The certified trainers are screened by the Vanderbilt Recreation & Wellness Center (the Rec)
We look forward to helping you achieve your fitness goals!
 Personal Training Congratulations on your decision to invest in yourself! Our qualified, nationally certified personal trainers will provide you with the right information and right training to help you
Personal Training Congratulations on your decision to invest in yourself! Our qualified, nationally certified personal trainers will provide you with the right information and right training to help you
PERSONAL TRAINING POLICIES
 PERSONAL TRAINING POLICIES SCHEDULING: To schedule your initial session: 1. Complete Interest Form, Health History Questionnaire, and Policies forms and return them to the Fitness Department. 2. Register
PERSONAL TRAINING POLICIES SCHEDULING: To schedule your initial session: 1. Complete Interest Form, Health History Questionnaire, and Policies forms and return them to the Fitness Department. 2. Register
Personal Training Health Screening Questionnaire
 RC Health and Fitness, LLC. 10350 Ironbridge Road Chester, VA 23831 (804)248-0222 Personal Training Health Screening Questionnaire Personal Information Today s date: Title: O DR. O Mr. O Mrs. O Ms. Name:
RC Health and Fitness, LLC. 10350 Ironbridge Road Chester, VA 23831 (804)248-0222 Personal Training Health Screening Questionnaire Personal Information Today s date: Title: O DR. O Mr. O Mrs. O Ms. Name:
Personal Training New Client Packet Personal Training/Fit for Hire
 Personal Training New Client Packet Personal Training/Fit for Hire Date / / Name Address City State Zip Phone Number Email Trainer Preference Male Female No Preference **If you would like to work with
Personal Training New Client Packet Personal Training/Fit for Hire Date / / Name Address City State Zip Phone Number Email Trainer Preference Male Female No Preference **If you would like to work with
Department of Campus Recreation: SouthFit Personal Training
 Steps to sign up Step 1: Choose the personal training package that you would like on page 2. Personal training is only available to members of the USA Student Recreation Center. Step 2: Fill out all pages
Steps to sign up Step 1: Choose the personal training package that you would like on page 2. Personal training is only available to members of the USA Student Recreation Center. Step 2: Fill out all pages
Spring 2018 Small Group Training Registration
 Spring 2018 Small Group Training Registration Small Group Training Information Packet General Information Session Dates: Monday, February 19 th - Thursday, April 20 th (8 weeks) Free class demos will be
Spring 2018 Small Group Training Registration Small Group Training Information Packet General Information Session Dates: Monday, February 19 th - Thursday, April 20 th (8 weeks) Free class demos will be
PERSONAL TRAINING CLIENT INFORMATION PACKAGE
 WEST VANCOUVER COMMUNITY CENTRE PERSONAL TRAINING PERSONAL TRAINING CLIENT INFORMATION PACKAGE At West Vancouver Community Services, our approach to health and fitness is balanced. Being healthy means
WEST VANCOUVER COMMUNITY CENTRE PERSONAL TRAINING PERSONAL TRAINING CLIENT INFORMATION PACKAGE At West Vancouver Community Services, our approach to health and fitness is balanced. Being healthy means
Weight training is based on individual needs. Beginning weights are provided. Please bring your mat or towel to lay on the floor.
 BENEFITS OF THE PROGRAM: IMPROVE MUSCLE MASS & STRENGTH REDUCE RISK OF OSTEOPOROSIS & RELATED FRACTURES REDUCE THE RISK FOR DIABETES, HEART DISEASE, DEPRESSION & OBESITY IMPROVE SELF-CONFIDENCE, SLEEP
BENEFITS OF THE PROGRAM: IMPROVE MUSCLE MASS & STRENGTH REDUCE RISK OF OSTEOPOROSIS & RELATED FRACTURES REDUCE THE RISK FOR DIABETES, HEART DISEASE, DEPRESSION & OBESITY IMPROVE SELF-CONFIDENCE, SLEEP
Personal Training Intake Form
 Personal Training Intake Form Name: Date: Cell Phone: Office Phone: E-Mail: USC Affiliation: STUDENT ALUMNI FACULTY/STAFF FACULTY/STAFF SPOUSE Sex: Male Female Age: Trainer preference (if any): How many
Personal Training Intake Form Name: Date: Cell Phone: Office Phone: E-Mail: USC Affiliation: STUDENT ALUMNI FACULTY/STAFF FACULTY/STAFF SPOUSE Sex: Male Female Age: Trainer preference (if any): How many
Personal Training Registration Packet
 Registration Packet Client name: Sessions Purchased: 3 Sessions 30 Minutes 60 Minutes 5 Sessions 10 Sessions 15 Sessions Purchase Date: General and Healthy History Questionnaire Name: Penn ID: Date of
Registration Packet Client name: Sessions Purchased: 3 Sessions 30 Minutes 60 Minutes 5 Sessions 10 Sessions 15 Sessions Purchase Date: General and Healthy History Questionnaire Name: Penn ID: Date of
P: F: balance. Some exercise equipment will be used such as treadmills, NuSteps and resistance devices.
 The Burke Rehabilitation Hospital recognizes the need to stay physically fit at all ages and functional levels. The Fit 4 Life After Stroke exercise program provides an exercise setting for people who
The Burke Rehabilitation Hospital recognizes the need to stay physically fit at all ages and functional levels. The Fit 4 Life After Stroke exercise program provides an exercise setting for people who
P: F: Session Information Sessions are held quarterly, registration is ongoing. Monday, Wednesday 2:00PM 3:00PM
 The Burke Rehabilitation Hospital recognizes the need to stay physically fit at all ages and functional levels. The Fit 4 Life After Stroke exercise program provides an exercise setting for people who
The Burke Rehabilitation Hospital recognizes the need to stay physically fit at all ages and functional levels. The Fit 4 Life After Stroke exercise program provides an exercise setting for people who
Participant Summary Information Sheet
 Participant Summary Information Sheet Name: Address: Who was your referral source? (Friend, Doctor, Newspaper, Radio - Please name source) Phone Number: Email Address: Date of Birth: Program Site: Age:
Participant Summary Information Sheet Name: Address: Who was your referral source? (Friend, Doctor, Newspaper, Radio - Please name source) Phone Number: Email Address: Date of Birth: Program Site: Age:
Trees Hall. Bellefield Hall
 Classes Begin: Monday, 5/7/2018 Classes End: Friday, 8/10/2018 No Class: Memorial Day: 5/28/2018 & Independence Day: 7/4/2018 Trees Hall Indoor Cycling 4400 Monday / Wednesday 12:00-12:55 PM HFC Indoor
Classes Begin: Monday, 5/7/2018 Classes End: Friday, 8/10/2018 No Class: Memorial Day: 5/28/2018 & Independence Day: 7/4/2018 Trees Hall Indoor Cycling 4400 Monday / Wednesday 12:00-12:55 PM HFC Indoor
The StrongWomen Program
 A National Fitness Program for Women Cooperative Extension Service 1675 C Street, #100 Anchorage, AK 99501 Leslie Shallcross, M.S., R.D., L.D. Associate Professor of Extension 907-786-6300 Name Address
A National Fitness Program for Women Cooperative Extension Service 1675 C Street, #100 Anchorage, AK 99501 Leslie Shallcross, M.S., R.D., L.D. Associate Professor of Extension 907-786-6300 Name Address
Fitness Training Services Application
 Fitness Training Services Application Thank you for your interest in one of our fitness training services with Boston College Campus Recreation. We are committed to helping Boston College students, faculty,
Fitness Training Services Application Thank you for your interest in one of our fitness training services with Boston College Campus Recreation. We are committed to helping Boston College students, faculty,
MEMBERSHIP APPLICATION
 MEMBERSHIP APPLICATION Join Date: Full Pay Draft 20/20 Membership Type: Household One Parent Household Two Adult Household Senior Household Adult Young Adult Youth Senior First Name MI Last Birth Date
MEMBERSHIP APPLICATION Join Date: Full Pay Draft 20/20 Membership Type: Household One Parent Household Two Adult Household Senior Household Adult Young Adult Youth Senior First Name MI Last Birth Date
Trees Hall. Bellefield Hall. Add a Fitness Center Membership for a small additional price!
 Classes Begin: Tuesday, 9/5/2017 Classes End: Friday, 12/8/2017 No Class: Labor Day: 9/4/2017 & Thanksgiving Break: 11/23-24/2017 Trees Hall Kettle + Conditioning Fitness Kickboxing Fitness Kickboxing
Classes Begin: Tuesday, 9/5/2017 Classes End: Friday, 12/8/2017 No Class: Labor Day: 9/4/2017 & Thanksgiving Break: 11/23-24/2017 Trees Hall Kettle + Conditioning Fitness Kickboxing Fitness Kickboxing
select class BEST VALUE! $85 $90 $55 $60 $40 $45
 Tomahawk Strong Bones Participant Registration Form Mondays and Thursdays January 9 May 25, 2017 Location: United Methodist Church (1104 School Rd, Tomahawk, WI 54487) Our Strong Bones Program follows
Tomahawk Strong Bones Participant Registration Form Mondays and Thursdays January 9 May 25, 2017 Location: United Methodist Church (1104 School Rd, Tomahawk, WI 54487) Our Strong Bones Program follows
Personal Training Information Packet
 Personal Training Information Packet Dubuque Community YMCA/YWCA 35 North Booth Street Dubuque, Iowa 52001 P 563.556.3371 F 563.556.2728 www.dubuquey.org Dear Member: Congratulations! You have just taken
Personal Training Information Packet Dubuque Community YMCA/YWCA 35 North Booth Street Dubuque, Iowa 52001 P 563.556.3371 F 563.556.2728 www.dubuquey.org Dear Member: Congratulations! You have just taken
The Strong Women Program A National Fitness Program for Women. Join the Strong Women Program Today! Sign up Now! ENROLLMENT IS LIMITED!
 Join the Strong Women Program Today! Sign up Now! ENROLLMENT IS LIMITED! Classes for new participants Friday, October 5 to Friday, January 4, 2013: 8-9 a.m. Monday, Wednesday & Friday Noon 1 p.m. Monday,
Join the Strong Women Program Today! Sign up Now! ENROLLMENT IS LIMITED! Classes for new participants Friday, October 5 to Friday, January 4, 2013: 8-9 a.m. Monday, Wednesday & Friday Noon 1 p.m. Monday,
Welcome to the CANYON WELLNESS PROGRAM!
 Welcome to the CANYON WELLNESS PROGRAM! This program is designed to allow you to continue/initiate the pursuit of your health/wellness goals. You may have just completed a course of Physical Therapy or
Welcome to the CANYON WELLNESS PROGRAM! This program is designed to allow you to continue/initiate the pursuit of your health/wellness goals. You may have just completed a course of Physical Therapy or
Client Contact Information. Training Information
 Client Contact Information Name Address (Street) (City) (State) (Zip) Home Phone ( ) Cell Phone ( ) Work Phone ( ) Email Date of Birth / / Training Information Type Personal Training - $35 Partner Training
Client Contact Information Name Address (Street) (City) (State) (Zip) Home Phone ( ) Cell Phone ( ) Work Phone ( ) Email Date of Birth / / Training Information Type Personal Training - $35 Partner Training
P: F:
 Fit 4 Life Exercise Programs provide an exercise setting for people who do not require ongoing physical therapy or occupational therapy. Fit For Life l Strength and Conditioning 1 The Strength and Conditioning
Fit 4 Life Exercise Programs provide an exercise setting for people who do not require ongoing physical therapy or occupational therapy. Fit For Life l Strength and Conditioning 1 The Strength and Conditioning
Wellness Department. Non-Resident Pool Membership Packet. Page 1
 Wellness Department Non-Resident Pool Membership Packet Page 1 Dear Non-Resident, Thank you for your inquiry into the Aquatic programs at Brethren Village. We offer the opportunity for residents in the
Wellness Department Non-Resident Pool Membership Packet Page 1 Dear Non-Resident, Thank you for your inquiry into the Aquatic programs at Brethren Village. We offer the opportunity for residents in the
Personal Training Packet
 Personal Training Packet Personal Power Small Group Partner Personal Training Waiver Personal Training Policies All cancellations must be made 24 hours in advance of your appointment time. No-shows and/or
Personal Training Packet Personal Power Small Group Partner Personal Training Waiver Personal Training Policies All cancellations must be made 24 hours in advance of your appointment time. No-shows and/or
Gym Memberships. The cost of the membership is per month, plus a one off cost of 5 for the band.
 Gym Memberships Membership Form Name: Address: Membership Start Date: Payment Details The cost of the membership is 18.50 per month, plus a one off cost of 5 for the band. This Payment should be made either
Gym Memberships Membership Form Name: Address: Membership Start Date: Payment Details The cost of the membership is 18.50 per month, plus a one off cost of 5 for the band. This Payment should be made either
COST One on One.$60.00 per hour One on One..$30.00 per half hour Small Group $40/hour/person. Thank you for your interest in our program.
 Personal Training New Client Registration Congratulations on taking the first step to healthier and better you! The certified trainers are screened by the Vanderbilt Recreation & Wellness Center (the Rec)
Personal Training New Client Registration Congratulations on taking the first step to healthier and better you! The certified trainers are screened by the Vanderbilt Recreation & Wellness Center (the Rec)
Name: Phone #: Address: Cell Phone #: Address: I d like to participate in:
 Strong Women and Strong Women Advance Program 12-Week Participant Registration Form January 8-April 2*, 2018 *Good Friday Week Schedule Changes: Strong Classes class will meet Monday (3/26) instead of
Strong Women and Strong Women Advance Program 12-Week Participant Registration Form January 8-April 2*, 2018 *Good Friday Week Schedule Changes: Strong Classes class will meet Monday (3/26) instead of
PERSONAL TRAINING AT MCGAW YMCA
 PERSONAL TRAINING AT MCGAW YMCA Welcome to personal training at the McGaw YMCA! Our personal trainers look forward to working with you and helping you meet your health and fitness goals! There are a few
PERSONAL TRAINING AT MCGAW YMCA Welcome to personal training at the McGaw YMCA! Our personal trainers look forward to working with you and helping you meet your health and fitness goals! There are a few
The University of Texas at Dallas Department of Recreational Sports Nutritional Guidance Registration Form
 The University of Texas at Dallas Department of Recreational Sports Nutritional Guidance Registration Form Directions: Please, fill out as much information as possible. If you are unsure, leave that question
The University of Texas at Dallas Department of Recreational Sports Nutritional Guidance Registration Form Directions: Please, fill out as much information as possible. If you are unsure, leave that question
ATHLETE START UP QUESTIONNAIRE The first step in the coaching process is filling out the athlete questionnaire. Once completed, back to me.
 ATHLETE START UP QUESTIONNAIRE The first step in the coaching process is filling out the athlete questionnaire. Once completed, email back to me. General/Medical 1. Name 2. Address 3. E-mail 4. Phone Best
ATHLETE START UP QUESTIONNAIRE The first step in the coaching process is filling out the athlete questionnaire. Once completed, email back to me. General/Medical 1. Name 2. Address 3. E-mail 4. Phone Best
Thank you for inquiring about our Shelly Aquatic Center at Brethren Village. We hope you will find the enclosed information helpful.
 Thank you for inquiring about our Shelly Aquatic Center at Brethren Village. We hope you will find the enclosed information helpful. Non-Resident Enrollment Policy for use of Pool Non-Resident packet includes:
Thank you for inquiring about our Shelly Aquatic Center at Brethren Village. We hope you will find the enclosed information helpful. Non-Resident Enrollment Policy for use of Pool Non-Resident packet includes:
Welcome to OPEN Gym. To book an induction please
 Welcome to OPEN Gym Induction Once you have completed your Gym Membership, Standing Order and Liability Disclaimer form as well as the Physical Activity Readiness Questionnaire (PARQ), the next thing you
Welcome to OPEN Gym Induction Once you have completed your Gym Membership, Standing Order and Liability Disclaimer form as well as the Physical Activity Readiness Questionnaire (PARQ), the next thing you
STRENGTH & CONDITIONING INFORMATION AND PRE-ACTIVITY SCREENING
 STRENGTH & CONDITIONING INFORMATION AND PRE-ACTIVITY SCREENING Please take the time to read through all the information and ensure all relevant forms are completed. The following questionnaire and waivers
STRENGTH & CONDITIONING INFORMATION AND PRE-ACTIVITY SCREENING Please take the time to read through all the information and ensure all relevant forms are completed. The following questionnaire and waivers
Join the StrongWomen Program today!
 Join the StrongWomen Program today! Dr. Miriam Nelson, a professor at Tufts University in Boston, Massachusetts, has developed a strength-training program specifically for midlife and older women. The
Join the StrongWomen Program today! Dr. Miriam Nelson, a professor at Tufts University in Boston, Massachusetts, has developed a strength-training program specifically for midlife and older women. The
YWCA LOWER CAPE FEAR 2815 S College Rd Wilmington, NC (910)
") 2815 S College Rd Wilmington, NC 28412 FLOW MOTION REGISTRATION Full Name: APPLICANT INFORMATION Last First M.I. Address: Street Address Apartment/Unit # City State ZIP Code Primary Phone: Email Mobile
2815 S College Rd Wilmington, NC 28412 FLOW MOTION REGISTRATION Full Name: APPLICANT INFORMATION Last First M.I. Address: Street Address Apartment/Unit # City State ZIP Code Primary Phone: Email Mobile
Release of Liability. Participant Signature: Participant Name (please print): Signature of Witness:
: Signature of Witness:") Release of Liability In consideration of being allowed to use NextEra Energy Health & Well-Being Fitness Center facilities and equipment, and being allowed to participate in fitness and wellness program
Release of Liability In consideration of being allowed to use NextEra Energy Health & Well-Being Fitness Center facilities and equipment, and being allowed to participate in fitness and wellness program
Client Assessment Readiness Questionnaire
 Client Assessment Readiness Questionnaire The following questions will help determine your level of readiness for change, your motivation towards reaching your goals, and identifying obstacles to your
Client Assessment Readiness Questionnaire The following questions will help determine your level of readiness for change, your motivation towards reaching your goals, and identifying obstacles to your
Fitness Training Services Application
 Fitness Training Services Application Thank you for your interest in one of our fitness training services with Boston College Campus Recreation. We are committed to helping Boston College students, faculty,
Fitness Training Services Application Thank you for your interest in one of our fitness training services with Boston College Campus Recreation. We are committed to helping Boston College students, faculty,
HEALTH/MEDICAL QUESTIONNAIRE PHYSICAL ACTIVITY READINESS QUESTIONNAIRE (PAR-Q)
") WRC Staff Use Only WRC Staff Initials Physician s Clearance received? Yes No N/A Orientation complete? Yes No Health/Medical History form signed? Yes No Assumption of Risk form signed? Yes No PAR-Q signed?
WRC Staff Use Only WRC Staff Initials Physician s Clearance received? Yes No N/A Orientation complete? Yes No Health/Medical History form signed? Yes No Assumption of Risk form signed? Yes No PAR-Q signed?
Civilian Wellness and Civilian Fitness Program (AR Health Promotion)
") Civilian Wellness and Civilian Fitness Program (AR 600-63 Health Promotion) Enrollment Packet Wellness Program Coordinators: Wendy LaRoche (wendy.laroche@us.army.mil) Celestine Beckett (celestine.beckett.civ@mail.mil)
Civilian Wellness and Civilian Fitness Program (AR 600-63 Health Promotion) Enrollment Packet Wellness Program Coordinators: Wendy LaRoche (wendy.laroche@us.army.mil) Celestine Beckett (celestine.beckett.civ@mail.mil)
ADULT PRE-EXERCISE SCREENING TOOL
 ADULT PRE-EXERCISE SCREENING TOOL This screening tool does not provide advice on a particular matter, nor does it substitute for advice from an appropriately qualified medical professional. warranty of
ADULT PRE-EXERCISE SCREENING TOOL This screening tool does not provide advice on a particular matter, nor does it substitute for advice from an appropriately qualified medical professional. warranty of
Thanks again, The BodyEvolver team Fitness Technology Partners, LLC bodyevolver.com
 Thank you for downloading this comprehensive client intake package. It is our pleasure to provide this tested document which we know will help your business. A complete on-line version of this intake package
Thank you for downloading this comprehensive client intake package. It is our pleasure to provide this tested document which we know will help your business. A complete on-line version of this intake package
Personal Training Initial Packet
 Personal Training Initial Packet ****Please complete and return to the reception desk at least 2 days prior to your scheduled Fitness Assessment**** Name: D.O.B: Today s Date: Member or Non-member (circle
Personal Training Initial Packet ****Please complete and return to the reception desk at least 2 days prior to your scheduled Fitness Assessment**** Name: D.O.B: Today s Date: Member or Non-member (circle
MEMBER PERSONAL TRAINING PACKET
 Dear YMCA Member, MEMBER PERSONAL TRAINING PACKET Congratulations on the decision to improve your health and well-being and work with one of our nationally certified personal trainers! THIS ENTIRE PACKET
Dear YMCA Member, MEMBER PERSONAL TRAINING PACKET Congratulations on the decision to improve your health and well-being and work with one of our nationally certified personal trainers! THIS ENTIRE PACKET
Personal Training Initial Packet
 Personal Training Initial Packet ****Please complete and return to the reception desk at least 2 days prior to your scheduled Fitness Assessment**** Name: D.O.B: Today s Date: Member or Non-member (circle
Personal Training Initial Packet ****Please complete and return to the reception desk at least 2 days prior to your scheduled Fitness Assessment**** Name: D.O.B: Today s Date: Member or Non-member (circle
Oxford Parks & Recreation Department. Fit After 50 Workout Center. Membership Packet
 Oxford Parks & Recreation Department Fit After 50 Workout Center Membership Packet The Fit After 50 (FA50) Workout Center Regulations have been established to make it possible for you to use the facility
Oxford Parks & Recreation Department Fit After 50 Workout Center Membership Packet The Fit After 50 (FA50) Workout Center Regulations have been established to make it possible for you to use the facility
Body Structure Medical Fitness Facility 2600 Gribbin Drive 410 Redding Rd Lexington, KY (859) General Information
 General Information") Body Structure Medical Fitness Facility 2600 Gribbin Drive 410 Redding Rd Lexington, KY 40517 (859) 268-8190 General Information Full Name Birth date / / Date / / Social Security # - - Driver s License
Body Structure Medical Fitness Facility 2600 Gribbin Drive 410 Redding Rd Lexington, KY 40517 (859) 268-8190 General Information Full Name Birth date / / Date / / Social Security # - - Driver s License
REQUIREMENTS: PROGRAM INCLUDES: IMPORTANT DATES: CHALLENGE WINNERS: HOW DO I PARTICIPATE IN AUBURN STRONG?
 REQUIREMENTS: Auburn University student, faculty or staff Physician clearance/par Q Completed registration form 3 day food log prior to nutritional assessment Nutritional Assessment Attend @ least 2 semi-private
REQUIREMENTS: Auburn University student, faculty or staff Physician clearance/par Q Completed registration form 3 day food log prior to nutritional assessment Nutritional Assessment Attend @ least 2 semi-private
Speed & Agility, Track & Field and Strength Training
 ATHLETIC SCHOLARSHIPS SPORT SCIENCE TESTING COMPETITIVE ADVANTAGE COLLEGE READINESS Speed & Agility, Track & Field and Strength Training Think of MIT training services as a strategic training partner that
ATHLETIC SCHOLARSHIPS SPORT SCIENCE TESTING COMPETITIVE ADVANTAGE COLLEGE READINESS Speed & Agility, Track & Field and Strength Training Think of MIT training services as a strategic training partner that
WAIVER AND RELEASE FROM LIABILITY
 COACHING CONTRACT I hereby contract Start-Tri.Com as my personal coach for endurance sports. I agree to pay for coaching services up front at the rate of $255/month for the Tier I package, $165/month for
COACHING CONTRACT I hereby contract Start-Tri.Com as my personal coach for endurance sports. I agree to pay for coaching services up front at the rate of $255/month for the Tier I package, $165/month for
*Your address will be added to our WODIFY system. You may receive correspondence from both WODIFT and Crossfit Toowoomba from time to time.
 Name: Date of Birth: Emergency Name and Contact No: Address: Contact Number: Email Address Occupation: Have you done Crossfit Before? Gender: If so where? *Your email address will be added to our WODIFY
Name: Date of Birth: Emergency Name and Contact No: Address: Contact Number: Email Address Occupation: Have you done Crossfit Before? Gender: If so where? *Your email address will be added to our WODIFY
The STRONGBODIES Program
 The STRONGBODIES Program Dr. Miriam Nelson, a professor at Tufts University in Boston, Massachusetts, has developed a strength-training program specifically for midlife and older men and women. The StrongBodies
The STRONGBODIES Program Dr. Miriam Nelson, a professor at Tufts University in Boston, Massachusetts, has developed a strength-training program specifically for midlife and older men and women. The StrongBodies
TEACHER TRAINING APPLICATION
 Introduction TEACHER TRAINING APPLICATION Thank you for your interest in the Hot 8 Yoga Teacher Training Program! Below you will find detailed instructions on how to apply. Please be aware that the Hot
Introduction TEACHER TRAINING APPLICATION Thank you for your interest in the Hot 8 Yoga Teacher Training Program! Below you will find detailed instructions on how to apply. Please be aware that the Hot
Training Application for
 STRENGTH Rx REAL TRAINING NO GIMMICKS HARD WORK REAL RESULTS Training Application for STRENGTH Rx Welcome to STRENGTH Rx. We offer Strength & Conditioning training for all athletes looking to improve all
STRENGTH Rx REAL TRAINING NO GIMMICKS HARD WORK REAL RESULTS Training Application for STRENGTH Rx Welcome to STRENGTH Rx. We offer Strength & Conditioning training for all athletes looking to improve all
Please complete the medical history section below so that we can be sure to respond to any
 200hr Yoga Teacher Training Application Please fill out this form and email it to teachertraining@ahamyoga.com with Teacher training application 2016 as the subject line. Any enrollments without this form
200hr Yoga Teacher Training Application Please fill out this form and email it to teachertraining@ahamyoga.com with Teacher training application 2016 as the subject line. Any enrollments without this form
APPLICATION INSTRUCTIONS
 APPLICATION INSTRUCTIONS TEACHER TRAINING PROGRAMS Application Deadlines To process your application, please send your complete application no later than one week prior to the program start date. However,
APPLICATION INSTRUCTIONS TEACHER TRAINING PROGRAMS Application Deadlines To process your application, please send your complete application no later than one week prior to the program start date. However,
Colorado Mesa University Campus Rec Services Massage Therapy Health History Questionnaire
 Colorado Mesa University Campus Rec Services Massage Therapy Health History Questionnaire Client Name: Today s : Contact Number: E-Mail: Occupation: Age: How did you hear about us? Have you ever had a
Colorado Mesa University Campus Rec Services Massage Therapy Health History Questionnaire Client Name: Today s : Contact Number: E-Mail: Occupation: Age: How did you hear about us? Have you ever had a
ENROLMENT FORM. Title: First Name: Surname: Postal Address: Postcode: Emergency Contact: Relationship: Phone: What is your main fitness goal?
 ENROLMENT FORM Personal Information Title: First Name: Surname: Date of Birth: Sex: Female Male Postal Address: Postcode: Phone: Home: Work: Mobile: Email: Preferred method of contact: Letter Phone Email
ENROLMENT FORM Personal Information Title: First Name: Surname: Date of Birth: Sex: Female Male Postal Address: Postcode: Phone: Home: Work: Mobile: Email: Preferred method of contact: Letter Phone Email
RISK REVIEW & PHYSICIAN APPROVAL FORM
 RISK REVIEW & PHYSICIAN APPROVAL FORM Burke Restorative Neurology Clinic is offering services meant to target community members with neurological impairments. The program is supervised by medical professionals
RISK REVIEW & PHYSICIAN APPROVAL FORM Burke Restorative Neurology Clinic is offering services meant to target community members with neurological impairments. The program is supervised by medical professionals
Colorado Mesa University Campus Rec Services Personal Training Request Packet
 Colorado Mesa University Campus Rec Services Personal Training Request Packet Personal Training Services are a fee-based service available to current CMU students, Faculty & Staff membership holders, as
Colorado Mesa University Campus Rec Services Personal Training Request Packet Personal Training Services are a fee-based service available to current CMU students, Faculty & Staff membership holders, as
EXTERNAL TRAINER AGREEMENT. THIS AGREEMENT dated as of the day of, 20. BETWEEN: (the External Trainer ) - and -
 - and -") EXTERNAL TRAINER AGREEMENT THIS AGREEMENT dated as of the day of, 20. BETWEEN: (the External Trainer ) - and - 2566588 Ontario Ltd. operating as Fortis Fitness West (2566588 Ontario Ltd. operating as Fortis
EXTERNAL TRAINER AGREEMENT THIS AGREEMENT dated as of the day of, 20. BETWEEN: (the External Trainer ) - and - 2566588 Ontario Ltd. operating as Fortis Fitness West (2566588 Ontario Ltd. operating as Fortis
For New Clients TO BE COMPLETED BY FRONT DESK STAFF. Date received: Payment $ Receipt# Staff Initials: TO BE COMPLETED BY SUPERVISOR
 For New Clients Client s Name: Phone: R#: Email: Age: Sex: M F Trainer Preferred: M F Name: Check all that apply: Individual Packages: **3-16 sessions must be completed in the same semester purchased 3
For New Clients Client s Name: Phone: R#: Email: Age: Sex: M F Trainer Preferred: M F Name: Check all that apply: Individual Packages: **3-16 sessions must be completed in the same semester purchased 3
EXTERNAL TRAINER AGREEMENT. THIS AGREEMENT dated as of the day of, 20. BETWEEN: (the External Trainer ) - and -
 - and -") EXTERNAL TRAINER AGREEMENT THIS AGREEMENT dated as of the day of, 20. BETWEEN: (the External Trainer ) - and - Fortis Fitness Inc. (Fortis Fitness Inc. or Fortis Fitness or the Companies ) This Agreement
EXTERNAL TRAINER AGREEMENT THIS AGREEMENT dated as of the day of, 20. BETWEEN: (the External Trainer ) - and - Fortis Fitness Inc. (Fortis Fitness Inc. or Fortis Fitness or the Companies ) This Agreement
Tidelands HealthPoint Stronger Through Movement Program Participant Information
 Tidelands HealthPoint Stronger Through Movement Program Participant Information Please Print: Name: DOB: First Middle Last Address: Phone: Street City Zip Email Address: Emergency Contact: Phone: First
Tidelands HealthPoint Stronger Through Movement Program Participant Information Please Print: Name: DOB: First Middle Last Address: Phone: Street City Zip Email Address: Emergency Contact: Phone: First
Complete enrollment packet and schedule a time to meet with Louie Morphew.
 Fitness Intake Packet (Personal Training and Adaptive Fitness Clients) Please follow the step-by-step instructions listed below. If you have any questions or concerns, please e-mail Louie Morphew at Lmorphe1@msudenver.edu.
Fitness Intake Packet (Personal Training and Adaptive Fitness Clients) Please follow the step-by-step instructions listed below. If you have any questions or concerns, please e-mail Louie Morphew at Lmorphe1@msudenver.edu.
2017 FIT FOR LIFE: 6 Week Program Stay Fit Through The Holidays Fall 2017: October 30 th December 15 th
 FOR YOUTH DEVELOPMENT FOR HEALTHY LIVING FOR SOCIAL RESPONSIBILITY 2017 FIT FOR LIFE: 6 Week Program Stay Fit Through The Holidays Fall 2017: October 30 th December 15 th Application for Participation
FOR YOUTH DEVELOPMENT FOR HEALTHY LIVING FOR SOCIAL RESPONSIBILITY 2017 FIT FOR LIFE: 6 Week Program Stay Fit Through The Holidays Fall 2017: October 30 th December 15 th Application for Participation
WEIGHT LOSS CHALLENGE: FACULTY AND STAFF. June 5th-August 2nd, 2018
 WEIGHT LOSS CHALLENGE: FACULTY AND STAFF Program overview: June 5th-August 2nd, 2018 The Faculty and Staff Weight Loss Challenge is an 8-week (16 session) program running from June 5th-August 2nd that
WEIGHT LOSS CHALLENGE: FACULTY AND STAFF Program overview: June 5th-August 2nd, 2018 The Faculty and Staff Weight Loss Challenge is an 8-week (16 session) program running from June 5th-August 2nd that
PERSONAL TRAINING. Welcome. Program policies & procedures
 Welcome PERSONAL TRAINING Welcome and thank you for your interest in personal training at Auburn University. You have taken the first step towards better overall health! We thank you for allowing our Campus
Welcome PERSONAL TRAINING Welcome and thank you for your interest in personal training at Auburn University. You have taken the first step towards better overall health! We thank you for allowing our Campus
FITNESS CONSULTATION JOURNAL
 FITNESS CONSULTATION JOURNAL 1 Table of Contents Guide to the ProFitness Program 2 Personal Information 3 Pre-Consultation Instructions 3 Personal Fitness Profile / History 4 Medical History 5-6 Injuries
FITNESS CONSULTATION JOURNAL 1 Table of Contents Guide to the ProFitness Program 2 Personal Information 3 Pre-Consultation Instructions 3 Personal Fitness Profile / History 4 Medical History 5-6 Injuries
Autism Society of Greater Orlando s 2018 Autism Walk & Family Fun Day **Annual Fundraising Event**
 Autism Society of Greater Orlando s 2018 Autism Walk & Family Fun Day **Annual Fundraising Event** The Autism Society of Greater Orlando is hosting its 13 th Annual Autism Walk & Family Fun Day inside
Autism Society of Greater Orlando s 2018 Autism Walk & Family Fun Day **Annual Fundraising Event** The Autism Society of Greater Orlando is hosting its 13 th Annual Autism Walk & Family Fun Day inside
Name: Date: Address: City: State: Zip: Birthday: / /
 PERSONAL TRAINING Name: Date: Address: City: State: Zip: Birthday: / / Sex: Male Female Name of Gym: Occupation: Phone (home): Phone (work): Body Weight: Body Fat: Height: Personal Goals 1. Primary Training
PERSONAL TRAINING Name: Date: Address: City: State: Zip: Birthday: / / Sex: Male Female Name of Gym: Occupation: Phone (home): Phone (work): Body Weight: Body Fat: Height: Personal Goals 1. Primary Training
PAR-Q & LIABILITY WAIVER
 PAR-Q & LIABILITY WAIVER Full name: Address: Post code: Mobile: Home phone: Email address: Date of Birth: Occupation: Emergency contact name: Relationship to you: Emergency contact phone number: Tara Blackaby
PAR-Q & LIABILITY WAIVER Full name: Address: Post code: Mobile: Home phone: Email address: Date of Birth: Occupation: Emergency contact name: Relationship to you: Emergency contact phone number: Tara Blackaby
Patient Information Form
 Patient Information Form Patient Name: (Last) (First) (MI) Name you prefer to be called: Mailing address: City: State: Zip: Best daytime phone: May we leave a message there? Yes No Alternate phone number:
Patient Information Form Patient Name: (Last) (First) (MI) Name you prefer to be called: Mailing address: City: State: Zip: Best daytime phone: May we leave a message there? Yes No Alternate phone number:
Eau Claire Tower Fitness Centre MEMBERSHIP APPLICATION
 Eau Claire Tower Fitness Centre MEMBERSHIP APPLICATION SHADED AREAS FOR OFFICE USE ONLY MEMBERSHIP # SECURITY CARD # START DATE DD MM YY NAME: FIRST LAST DATE DD MM YY OF BIRTH HOME ADDRESS HOME/CELL PHONE
Eau Claire Tower Fitness Centre MEMBERSHIP APPLICATION SHADED AREAS FOR OFFICE USE ONLY MEMBERSHIP # SECURITY CARD # START DATE DD MM YY NAME: FIRST LAST DATE DD MM YY OF BIRTH HOME ADDRESS HOME/CELL PHONE
DIOCESE OF HARRISBURG DIOCESAN CATHOLIC COMMITTEE ON SCOUTING
 June 2018 DCCS Retreat 2018 150 th Diocesan Anniversary! Dear Scouts, Venturers and Scouters, Join us for the 40 th Annual Diocesan Catholic Scout Retreat is the weekend of September 14, 15 & 16, 2018
June 2018 DCCS Retreat 2018 150 th Diocesan Anniversary! Dear Scouts, Venturers and Scouters, Join us for the 40 th Annual Diocesan Catholic Scout Retreat is the weekend of September 14, 15 & 16, 2018
GAH Elite Performance Adult Personal Training Registration Date:
 GAH Elite Performance Adult Personal Training Registration : Name: Address: First Middle Last Street # City State Zip of Birth: Sex (M/F) Home Phone E-mail: Emergency contact name: phone: Are you training
GAH Elite Performance Adult Personal Training Registration : Name: Address: First Middle Last Street # City State Zip of Birth: Sex (M/F) Home Phone E-mail: Emergency contact name: phone: Are you training
Talisman Therapeutic Riding, Inc. PO Box 300, Grasonville, MD
 Volunteer Application (Page 1 of 6) General Information Form - Please Print Clearly and Complete Fully (Last Name) (First Name) (Middle Initial) (Nickname) Street Address: City: State: Zip Code: Home Phone:
Volunteer Application (Page 1 of 6) General Information Form - Please Print Clearly and Complete Fully (Last Name) (First Name) (Middle Initial) (Nickname) Street Address: City: State: Zip Code: Home Phone:
*To reserve your place in the training, you must submit the completed application along with a minimum
 APPLICATION INSTRUCTIONS The Epídavros Teacher Training programs includes a vigorous two-hour asana practice. We strongly recommend that applicants have one year of consistent asana practice. If your yoga
APPLICATION INSTRUCTIONS The Epídavros Teacher Training programs includes a vigorous two-hour asana practice. We strongly recommend that applicants have one year of consistent asana practice. If your yoga
Personal Training Packet. Please complete and submit to the Fitness Center desk and you will be contacted. YMCA Mission
 HEALTH FITNESS LIFE Personal Training Packet Please complete and submit to the Fitness Center desk and you will be contacted. YMCA Mission To put Christian principles into practice through programs that
HEALTH FITNESS LIFE Personal Training Packet Please complete and submit to the Fitness Center desk and you will be contacted. YMCA Mission To put Christian principles into practice through programs that
StrongWomen Program Presented by:
 StrongWomen Program Presented by: Dr. Miriam Nelson, a professor at Tufts University in Boston, Massachusetts, has developed a strength-training program specifically for midlife and older women. The StrongWomen
StrongWomen Program Presented by: Dr. Miriam Nelson, a professor at Tufts University in Boston, Massachusetts, has developed a strength-training program specifically for midlife and older women. The StrongWomen
Physical Readiness Questionnaire
 Physical Readiness Questionnaire Date Customer Name Address City State Zip Date of Birth H Phone Cell Phone Email Sex: M F Height Weight How did you hear about this Cryo Sauna Location? FOR MINORS ONLY:
Physical Readiness Questionnaire Date Customer Name Address City State Zip Date of Birth H Phone Cell Phone Email Sex: M F Height Weight How did you hear about this Cryo Sauna Location? FOR MINORS ONLY:
Lose Dat WEIGHT LOSS/BODY COMPOSITION Challenge
 Lose Dat WEIGHT LOSS/BODY COMPOSITION Challenge is an 8-week program designed to educate all participants on how to lead a healthier lifestyle in every facet of life. This program is designed for men and
Lose Dat WEIGHT LOSS/BODY COMPOSITION Challenge is an 8-week program designed to educate all participants on how to lead a healthier lifestyle in every facet of life. This program is designed for men and
Pedaling for Parkinson s Colorado What is Pedaling for Parkinson s?
 What is Pedaling for Parkinson s? PFP is a non-profit organization focused on improving the quality of life for people with Parkinson s disease. Through a simple innovative exercise program using stationary
What is Pedaling for Parkinson s? PFP is a non-profit organization focused on improving the quality of life for people with Parkinson s disease. Through a simple innovative exercise program using stationary
Community Education. City State Zip Code. Term (please circle one) Summer 20 Fall 20 Winter 20 Spring 20
 Summer 20 Fall 20 Winter 20 Spring 20") Student ID # 1651 Lexington Ave, Astoria, OR 97103 Community Education Today s Date: Bandit Community Fitness Bandit Community Fitness offers access to the College s weight room, cardio room and running
Student ID # 1651 Lexington Ave, Astoria, OR 97103 Community Education Today s Date: Bandit Community Fitness Bandit Community Fitness offers access to the College s weight room, cardio room and running
New Patient Information
 New Patient Information First Name: Last Name: M.I.: Address: City: State: Zip Code: Mobile Phone: Home Phone: Email: Preferred method of communication: Mobile Phone Home Phone Email Date of Birth: Age:
New Patient Information First Name: Last Name: M.I.: Address: City: State: Zip Code: Mobile Phone: Home Phone: Email: Preferred method of communication: Mobile Phone Home Phone Email Date of Birth: Age:
For MWC Staff: Personal Information: Emergency Contact:
 Masonic Wellness Center and Pool Member Application 361-5699 or ext. 33783 on campus Personal Information: Name: (Mr., Mrs., Ms.) (First) (Last) (MI) Birth Date: Phone: (H): (W): Address: E-mail Address
Masonic Wellness Center and Pool Member Application 361-5699 or ext. 33783 on campus Personal Information: Name: (Mr., Mrs., Ms.) (First) (Last) (MI) Birth Date: Phone: (H): (W): Address: E-mail Address
There are a number of subscription types available to suit you and your family with annual fee or direct debit payment options available.
 Dear Prospective Member, Thank you for your enquiry regarding the facilities at Monkton Sports Club. We are delighted to offer members use of the School's outstanding sporting facilities alongside a comprehensive
Dear Prospective Member, Thank you for your enquiry regarding the facilities at Monkton Sports Club. We are delighted to offer members use of the School's outstanding sporting facilities alongside a comprehensive