Hiatal Hernias and Barrett s esophagus. Dr Sajida Ahad Mercy General Surgery
|
|
|
- Sherilyn Park
- 5 years ago
- Views:
Transcription
1 Hiatal Hernias and Barrett s esophagus Dr Sajida Ahad Mercy General Surgery
2 Objectives Identify the use of different diagnostic modalities for hiatal hernias List the different types of hiatal hernias and its significance for treatment and surgery Know the outcomes of hiatal hernia repairs and causes of morbidity and mortality associated with hiatal hernias Know the guidelines for identification, surveillance and management of Barrett s esophagus

3 What is a hiatal hernia? Hiatal hernia refers to displacement of abdominal organs, most commonly the stomach, through the esophageal hiatus of the diaphragm into the mediastinum
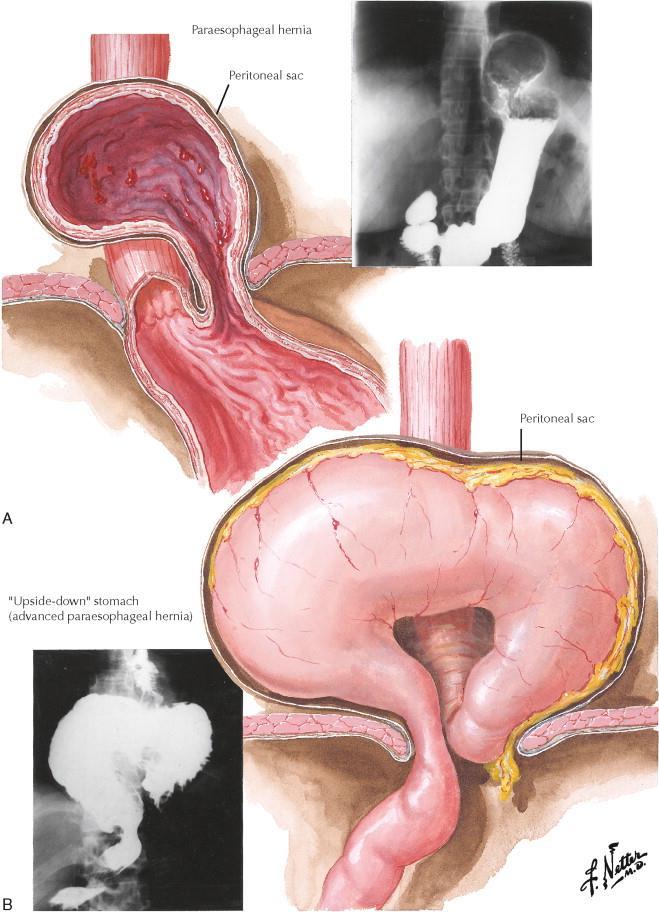
4 Types of hiatal hernias Type I sliding hiatal hernias gastroesophageal junction above the diaphragm fundus remains below the gastroesophageal junction Type II hernias are pure paraesophageal hernias (PEH) the gastroesophageal junction remains in its normal anatomic position but a portion of the fundus herniates through the diaphragmatic hiatus adjacent to the esophagus Type III hernias are a combination of Types I and II both the gastroesophageal junction and the fundus herniating through the hiatus. The fundus lies above the gastroesophageal junction. Type IV structure other than stomach, such as the omentum, colon or small bowel within the hernia sac
5 Fun facts Greater than 95% of hiatal hernias are Type I(Sliding hiatal hernias) Types II IV hernias also called paraesophageal hernias (PEH Of the paraesophageal hernias, more than 90% are Type III, and the least common is Type II Giant PEH: greater than ½ stomach in chest
6 Why Is It Important to Diagnose a Hiatal Hernia? sliding hiatal hernias are generally of no consequence and are common, particularly in older patients Large PEH can risk gastric viability hiatal hernias do not heal themselves even with significant and necessary changes in lifestyle, such as weight loss hiatal hernia will only get bigger with time, and its symptoms and associated risks will only become more profound
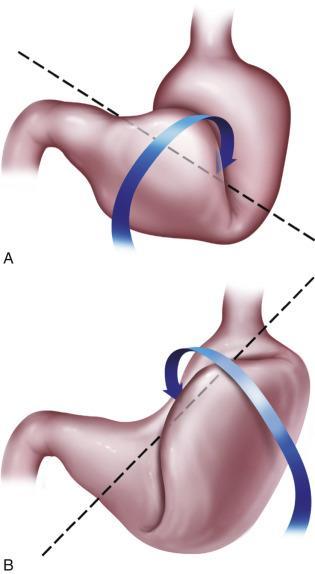
7 Risk of gastric volvulus rare condition classified according to the axis of rotation; organoaxial and mesenteroaxial it is more often diagnosed in elderly patients Acute volvulus is a surgical emergency Risk of strangulation =5% to 28% Symptoms :progressive chest pain, severe vomiting, and epigastric distention Borchardt s triad: severe epigastric pain, unproductive retching(inability to vomit), and inability to pass a nasogastric tube
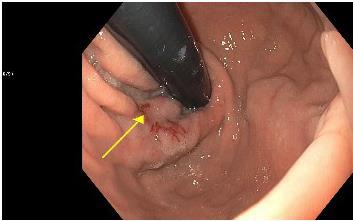
8 What Symptoms Are Associated With a Hiatal Hernia? Hiatal hernias may be asymptomatic PEH < less than 2 cm generally asymptomatic A hiatal hernia is not synonymous with gastroesophageal reflux Obstructive symptoms: dysphagia and regurgitation, aspiration pneumonia, recurring sinus infections, persistent cough, asthma, and changes in voice quality Space related symptoms: dyspnea, GERD, early satiety Cameron lesions: compromise of blood flow to or from the fundus could lead to chronic blood loss and anemia Symptoms of gastroesophageal reflux are not common; the esophageal compression associated with the paraesophageal hernia may limit concomitant gastroesophageal reflux and its associated symptoms
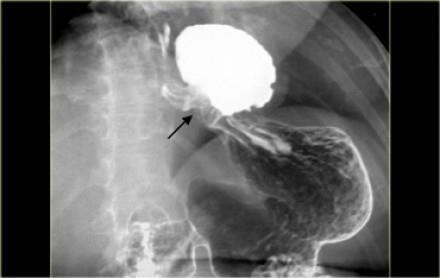
9 workup The first step in the diagnosis and evaluation of a paraesophageal hernia is to recognize its presence upper GI very helpful in establishing the diagnosis and extent of a paraesophageal hernia Non invasive Esophageal manometry Done prior to surgery Not for diagnosis but fundoplication decisions EGD To rule out other causes, assess anatomy, extent of hernia, Cameron lesions etc.
10 When to refer for surgery? All symptomatic paraesophageal hiatal hernias should be repaired operatively, particularly those that cause obstructive symptoms PEH with significant gastric distortion (e.g. an associated gastric volvulus) Operative intervention for a completely asymptomatic paraesophageal hernia must be balanced against patient age, comorbidities, BMI, operative history, size and nature of the paraesophageal hernia, complicating factors (e.g., concomitant gastroesophageal reflux disease
11 Non operative approach asymptomatic patient may require possible future intervention Focus om improvement of existing comorbidities, such as diabetes and obesity, that affect patient outcomes
12 Symptoms that are subjectively most improved after repair of a paraesophageal hernia are, in order, heartburn regurgitation dysphagia early satiety chest pain dyspnea
13 What does surgery entail? Laparoscopy abdominal approach Reduce the paraesophageal hernia (and sliding hiatal hernia, if present) to allow 6 to 8 cm of esophagus to lay in the high pressure abdominal cavity Dissect the hernia sac away from the hernia and excise of it what can be excised Reconstruct the esophageal hiatus snugly but not tightly about the esophagus Construct an antireflux fundoplication Recovery 1-2 nights in the hospital Full liquid diet, slowly advanced to regular diet over 3 to 4 weeks
14 Outcomes Failures are symptomatic or radiographic recurrences More than 90% of patients have durable, long-term symptom relief after laparoscopic paraesophageal hernia repair 40% of these same patients will have some degree of radiographic recurrence long-term dietary habits and weight control are paramount to durable outcomes
15 Conclusions Hiatal hernia can be diagnosed by various modalities. Only investigations which will alter the clinical management of the patient should be performed Repair of a type I hernia in the absence of reflux disease is not necessary All symptomatic paraesophageal hiatal hernias should be repaired,particularly those with acute obstructive symptoms or which have undergone volvulus Routine elective repair of completely asymptomatic paraesophageal hernias may not always be indicated
16 Barrett esophagus(be) acquired condition normal stratified squamous epithelium of the esophagus is replaced with metaplastic, intestinal-type columnar epithelium containing goblet cells BE in 1% to 2% of all adults in North America
17 Patients with BE have a thirtyfold increased risk of developing adenocarcinoma of the esophagus The risk of progression to esophageal adenocarcinoma arises in a stepwise fashion nondysplastic Barrett s cancer progression of 0.2% to 0.5 low-grade dysplasia of 0.7%, high-grade dysplasia of 7% per year esophageal adenocarcinoma becoming one of the fastest rising solid cancers in the Western world the overall 5-year survival remains only 17%
18 Surveillance of BE Women:lower risk of esophageal cancer in women with chronic reflux disease, screening for BE currently is not recommended Men: chronic (>5 years) and/or frequent (weekly or more) symptoms of heartburn or acid regurgitation atleast 2 risk factors for BE or EAC age over 50 years Caucasian race central obesity (waist circumference above 102 cm or waist hip ratio above 0.9) current or past history of smoking a history of BE or EAC in a first-degree relative.
19 EGD normal: no further surveillance EGD with esophagitis: treat with PPI and repeat endoscopy in 3 months BE prevalence of 9% to 12% on repeat endoscopy after treatment of esophagitis with PPI
20 BE diagnosed: the screening algorithm is determined by the presence and grade of dysplasia BE without dysplasia :surveillance endoscopy at 3-year to 5-year BE withlow-grade dysplasia (LGD) annual surveillance is recommended until two consecutive examinations are negative for dysplasia, after which the patient can return to surveillance at 3- to 5- year intervals BE with high grade dysplasia(hgd)
21 BE with high grade dysplasia(hgd) should be confirmed by a second pathologist because of the substantial interobserver variation endoscopic therapy or esophagectomy is warranted because these patients are at high risk for development of esophageal adenocarcinoma The presence of features such as ulceration, an endoscopically visible lesion, or multifocal HGD confers a higher risk of development of EAC and have been found to have an estimated risk of concurrent EAC of 60% to 78%
22 Questions?
23
24
25
26
27
Gastroesophageal Reflux Disease, Paraesophageal Hernias &
 530.81 553.3 & 530.00 43289, 43659 1043432842, MD Assistant Clinical Professor of Surgery, UH JABSOM Associate General Surgery Program Director Director of Minimally Invasive & Bariatric Surgery Programs
530.81 553.3 & 530.00 43289, 43659 1043432842, MD Assistant Clinical Professor of Surgery, UH JABSOM Associate General Surgery Program Director Director of Minimally Invasive & Bariatric Surgery Programs
ESOPHAGEAL CANCER AND GERD. Prof Salman Guraya FRCS, Masters MedEd
 ESOPHAGEAL CANCER AND GERD Prof Salman Guraya FRCS, Masters MedEd Learning objectives Esophagus anatomy and physiology Esophageal cancer Causes, presentations of esophageal cancer Diagnosis and management
ESOPHAGEAL CANCER AND GERD Prof Salman Guraya FRCS, Masters MedEd Learning objectives Esophagus anatomy and physiology Esophageal cancer Causes, presentations of esophageal cancer Diagnosis and management
Speaker disclosure. Objectives. GERD: Who and When to Treat 7/21/2015
 GERD: Who and When to Treat Eugenio J Hernandez, MD Gastrohealth, PL Assistant Professor of Clinical Medicine, FIU Herbert Wertheim School of Medicine Speaker disclosure I do not have any relevant commercial
GERD: Who and When to Treat Eugenio J Hernandez, MD Gastrohealth, PL Assistant Professor of Clinical Medicine, FIU Herbert Wertheim School of Medicine Speaker disclosure I do not have any relevant commercial
AGA SECTION. Gastroenterology 2016;150:
 Gastroenterology 2016;150:1026 1030 April 2016 AGA Section 1027 Procedural intervention (3) Upper endoscopy indications 3 6 Non-response of symptoms to a 4 8 week empiric trial of twice-daily PPI Troublesome
Gastroenterology 2016;150:1026 1030 April 2016 AGA Section 1027 Procedural intervention (3) Upper endoscopy indications 3 6 Non-response of symptoms to a 4 8 week empiric trial of twice-daily PPI Troublesome
WHAT IS GASTROESOPHAGEAL REFLUX DISEASE (GERD)?
?") WHAT IS GASTROESOPHAGEAL REFLUX DISEASE (GERD)? The term gastroesophageal reflux describes the movement (or reflux) of stomach contents back up into the esophagus, the muscular tube that extends from the
WHAT IS GASTROESOPHAGEAL REFLUX DISEASE (GERD)? The term gastroesophageal reflux describes the movement (or reflux) of stomach contents back up into the esophagus, the muscular tube that extends from the
Barrett s Esophagus. Abdul Sami Khan, M.D. Gastroenterologist Aurora Healthcare Burlington, Elkhorn, Lake Geneva, WI
 Barrett s Esophagus Abdul Sami Khan, M.D. Gastroenterologist Aurora Healthcare Burlington, Elkhorn, Lake Geneva, WI A 58 year-old, obese white man has had heartburn for more than 20 years. He read a magazine
Barrett s Esophagus Abdul Sami Khan, M.D. Gastroenterologist Aurora Healthcare Burlington, Elkhorn, Lake Geneva, WI A 58 year-old, obese white man has had heartburn for more than 20 years. He read a magazine
ACG Clinical Guideline: Diagnosis and Management of Barrett s Esophagus
 ACG Clinical Guideline: Diagnosis and Management of Barrett s Esophagus Nicholas J. Shaheen, MD, MPH, FACG 1, Gary W. Falk, MD, MS, FACG 2, Prasad G. Iyer, MD, MSc, FACG 3 and Lauren Gerson, MD, MSc, FACG
ACG Clinical Guideline: Diagnosis and Management of Barrett s Esophagus Nicholas J. Shaheen, MD, MPH, FACG 1, Gary W. Falk, MD, MS, FACG 2, Prasad G. Iyer, MD, MSc, FACG 3 and Lauren Gerson, MD, MSc, FACG
Hiatal hernias may be classified. hiatal hernia DESCRIPTION AND IDENTIFICATION. This article is the first in a twopart series about these somewhat
 paraesophagealh hiatal hernia Leslie K Browder, MD, and Alex G Little, MD DESCRIPTION AND IDENTIFICATION Hiatal hernias may be classified as four types. The most common, Type I, may present as gastroesophageal
paraesophagealh hiatal hernia Leslie K Browder, MD, and Alex G Little, MD DESCRIPTION AND IDENTIFICATION Hiatal hernias may be classified as four types. The most common, Type I, may present as gastroesophageal
Paraoesophageal Hernia
 Paraoesophageal Hernia Grand Round Adam Cichowitz Surgical Registrar Paraoesophageal Hernia Type of hiatal hernia Transdiaphragmatic migration of abdominal content gastric fundus gastric body pylorus colon
Paraoesophageal Hernia Grand Round Adam Cichowitz Surgical Registrar Paraoesophageal Hernia Type of hiatal hernia Transdiaphragmatic migration of abdominal content gastric fundus gastric body pylorus colon
GERD DIAGNOSIS & TREATMENT DISCLOSURES 4/18/2018
 GERD DIAGNOSIS & TREATMENT Subhash Chandra MBBS Assistant Professor CHI Health Clinic Gastroenterology Creighton University, School of Medicine April 28, 2018 DISCLOSURES None 1 OBJECTIVES Review update
GERD DIAGNOSIS & TREATMENT Subhash Chandra MBBS Assistant Professor CHI Health Clinic Gastroenterology Creighton University, School of Medicine April 28, 2018 DISCLOSURES None 1 OBJECTIVES Review update
Oesophageal Disorders
 Oesophageal Disorders Anatomy Upper sphincter Oesophageal body Diaphragm Lower sphincter Gastric Cardia Symptoms Of Oesophageal Disorders Dysphagia Odynophagia Heartburn Atypical Chest Pain Regurgitation
Oesophageal Disorders Anatomy Upper sphincter Oesophageal body Diaphragm Lower sphincter Gastric Cardia Symptoms Of Oesophageal Disorders Dysphagia Odynophagia Heartburn Atypical Chest Pain Regurgitation
Barrett s Esophagus: Old Dog, New Tricks
 Barrett s Esophagus: Old Dog, New Tricks Stuart Jon Spechler, M.D. Chief, Division of Gastroenterology, VA North Texas Healthcare System; Co-Director, Esophageal Diseases Center, Professor of Medicine,
Barrett s Esophagus: Old Dog, New Tricks Stuart Jon Spechler, M.D. Chief, Division of Gastroenterology, VA North Texas Healthcare System; Co-Director, Esophageal Diseases Center, Professor of Medicine,
History. Prevalence at Endoscopy. Prevalence and Reflux Sx. Prevalence at Endoscopy. Barrett s Esophagus: Controversy and Management
 Barrett s Esophagus: Controversy and Management History Norman Barrett (1950) Chronic Peptic Ulcer of the Oesophagus and Oesophagitis Allison and Johnstone (1953) The Oesophagus Lined with Gastric Mucous
Barrett s Esophagus: Controversy and Management History Norman Barrett (1950) Chronic Peptic Ulcer of the Oesophagus and Oesophagitis Allison and Johnstone (1953) The Oesophagus Lined with Gastric Mucous
Definition of GERD American College of Gastroenterology
 Definition of GERD American College of Gastroenterology GERD is defined as chronic symptoms or mucosal damage produced by the abnormal reflux of gastric contents into the esophagus DeVault et al. Am J
Definition of GERD American College of Gastroenterology GERD is defined as chronic symptoms or mucosal damage produced by the abnormal reflux of gastric contents into the esophagus DeVault et al. Am J
Paraesophageal Hernia
 Paraesophageal Hernia Inderpal (Netu) S. Sarkaria, M.D. Vice Chairman, Clinical Affairs Director, Robotic Thoracic Surgery Co-Director, Esophageal and Lung Surgery Institute Speaker/Education: Intuitive
Paraesophageal Hernia Inderpal (Netu) S. Sarkaria, M.D. Vice Chairman, Clinical Affairs Director, Robotic Thoracic Surgery Co-Director, Esophageal and Lung Surgery Institute Speaker/Education: Intuitive
Present Day Management of Barrett s Esophagus
 Slide 1 Present Day Management of Barrett s Esophagus Kinnari R. Kher, M.D. Slide 2 Goals Risk factors for development of Barrett s esophagus Risks for progression to Esophageal Adenocarcinoma Current
Slide 1 Present Day Management of Barrett s Esophagus Kinnari R. Kher, M.D. Slide 2 Goals Risk factors for development of Barrett s esophagus Risks for progression to Esophageal Adenocarcinoma Current
Hernia. emoryhealthcare.org
 Hernia Have you noticed a bulge or pain in your abdominal wall or groin? If so you may have a hernia. You may be in the process of confirming this diagnosis with your Primary Care Physician or already
Hernia Have you noticed a bulge or pain in your abdominal wall or groin? If so you may have a hernia. You may be in the process of confirming this diagnosis with your Primary Care Physician or already
Patient Presenting with Dysphagia
 Patient Presenting with Dysphagia Radiology Elective Presentation Mansur Ghani 5/18/2018 S L I D E 0 Patient Presentation 86 y/o female with a past medical history of DM type II, diabetic neuropathy, and
Patient Presenting with Dysphagia Radiology Elective Presentation Mansur Ghani 5/18/2018 S L I D E 0 Patient Presentation 86 y/o female with a past medical history of DM type II, diabetic neuropathy, and
Joel A. Ricci, MD SUNY Downstate Medical Center Department of Surgery
 Joel A. Ricci, MD SUNY Downstate Medical Center Department of Surgery Norman Barrett (1950) described the esophagus as: that part of the foregut, distal to the cricopharyngeal sphincter, which is lined
Joel A. Ricci, MD SUNY Downstate Medical Center Department of Surgery Norman Barrett (1950) described the esophagus as: that part of the foregut, distal to the cricopharyngeal sphincter, which is lined
Facing Surgery for GERD (Gastroesophageal
 Facing Surgery for GERD (Gastroesophageal Reflux Disease)? Learn about minimally invasive da Vinci Surgery The Condition GERD, Hiatal Hernia Gastroesophageal reflux disease or GERD occurs when stomach
Facing Surgery for GERD (Gastroesophageal Reflux Disease)? Learn about minimally invasive da Vinci Surgery The Condition GERD, Hiatal Hernia Gastroesophageal reflux disease or GERD occurs when stomach
Surgical Evaluation for Benign Esophageal Disease. Kimberly Howard, PA-C, MHS Duke University Medical Center April 7, 2018
 Surgical Evaluation for Benign Esophageal Disease Kimberly Howard, PA-C, MHS Duke University Medical Center April 7, 2018 Disclosures No disclosures relevant to this presentation. Objectives (for CME purposes)
Surgical Evaluation for Benign Esophageal Disease Kimberly Howard, PA-C, MHS Duke University Medical Center April 7, 2018 Disclosures No disclosures relevant to this presentation. Objectives (for CME purposes)
THORACIC SURGERY: Dysphagia. Dr. Robert Zeldin Dr. John Dickie Dr. Carmine Simone. Thoracic Surgery Toronto East General Hospital
 THORACIC SURGERY: Dysphagia Dr. Robert Zeldin Dr. John Dickie Dr. Carmine Simone Thoracic Surgery Toronto East General Hospital Objectives Definitions Common causes Investigations Treatment options Anatomy
THORACIC SURGERY: Dysphagia Dr. Robert Zeldin Dr. John Dickie Dr. Carmine Simone Thoracic Surgery Toronto East General Hospital Objectives Definitions Common causes Investigations Treatment options Anatomy
GASTROESOPHAGEAL REFLUX
 DR. PHILIP K. BLUSTEIN M.D. F.R.C.P.(C) 415 14 TH ST. NW. CALGARY AB T2N2A1 PHONE (403) 270-9555 FAX (404) 270-7479 GASTROESOPHAGEAL REFLUX DEFINITION: *MONTREAL CONSENSUS DEFINED GERD AS A CONDITION WHICH
DR. PHILIP K. BLUSTEIN M.D. F.R.C.P.(C) 415 14 TH ST. NW. CALGARY AB T2N2A1 PHONE (403) 270-9555 FAX (404) 270-7479 GASTROESOPHAGEAL REFLUX DEFINITION: *MONTREAL CONSENSUS DEFINED GERD AS A CONDITION WHICH
What s New in the Management of Esophageal Disease
 What s New in the Management of Esophageal Disease Philip O. Katz, MD Chairman, Division of Gastroenterology Einstein Medical Center Philadelphia Clinical Professor of Medicine Jefferson Medical College
What s New in the Management of Esophageal Disease Philip O. Katz, MD Chairman, Division of Gastroenterology Einstein Medical Center Philadelphia Clinical Professor of Medicine Jefferson Medical College
Gastroesophageal reflux disease Principles of GERD treatment Treatment of reflux diseases GERD
 Esophagus Anatomy/Physiology Gastroesophageal reflux disease Principles of GERD treatment Treatment of reflux diseases GERD Manometry Question 50 years old female with chest pain and dysphagia. Manometry
Esophagus Anatomy/Physiology Gastroesophageal reflux disease Principles of GERD treatment Treatment of reflux diseases GERD Manometry Question 50 years old female with chest pain and dysphagia. Manometry
Understanding GERD. & Stretta Therapy. GERD (gĕrd): Gastroesophageal Reflux Disease
: Gastroesophageal Reflux Disease") Understanding GERD & Stretta Therapy GERD (gĕrd): Gastroesophageal Reflux Disease What is GERD? When the muscle between your stomach and esophagus is weak, stomach contents like acid or bile can reflux
Understanding GERD & Stretta Therapy GERD (gĕrd): Gastroesophageal Reflux Disease What is GERD? When the muscle between your stomach and esophagus is weak, stomach contents like acid or bile can reflux
Congenital hiatus hernia: A case series. Department of Pediatric Surgery, Afyon Kocatepe University Faculty of Medicine, Afyonkarahisar, Turkey
 Orıgınal Article PEDIATRIC SURGERY North Clin Istanb 2018 doi: 10.14744/nci.2017.58672 UNCORRECTED PROOF Congenital hiatus hernia: A case series Didem Baskin Embleton, 1 Ahmet Ali Tuncer, 1 Mehmet Surhan
Orıgınal Article PEDIATRIC SURGERY North Clin Istanb 2018 doi: 10.14744/nci.2017.58672 UNCORRECTED PROOF Congenital hiatus hernia: A case series Didem Baskin Embleton, 1 Ahmet Ali Tuncer, 1 Mehmet Surhan
GERD: A linical Clinical Clinical Update Objectives
 GERD: A Clinical Update Jeff Gilbert, M.D. University i of Kentucky Gastroenterology 11/6/08 Objectives To review the basic pathophysiology underlying gastroesophageal reflux disease To highlight current
GERD: A Clinical Update Jeff Gilbert, M.D. University i of Kentucky Gastroenterology 11/6/08 Objectives To review the basic pathophysiology underlying gastroesophageal reflux disease To highlight current
Barrett s Oesophagus Information Leaflet THE DIGESTIVE SYSTEM. gutscharity.org.
 THE DIGESTIVE SYSTEM http://healthfavo.com/digestive-system-for-kids.html This factsheet is about Barrett s Oesophagus Barrett s Oesophagus is the term used for a pre-cancerous condition where the normal
THE DIGESTIVE SYSTEM http://healthfavo.com/digestive-system-for-kids.html This factsheet is about Barrett s Oesophagus Barrett s Oesophagus is the term used for a pre-cancerous condition where the normal
2 Paraesophageal Hiatus Hernia
 2 Paraesophageal Hiatus Hernia Luigi Bonavina Pearls and Pitfalls Paraesophageal (type II) hiatus hernia represents a distinct anatomic and clinic entity requiring a unique therapeutic strategy, and is
2 Paraesophageal Hiatus Hernia Luigi Bonavina Pearls and Pitfalls Paraesophageal (type II) hiatus hernia represents a distinct anatomic and clinic entity requiring a unique therapeutic strategy, and is
Paraesophageal Hernia
 THE ANNALS OF THORACIC SURGERY Journal of The Society of Thoracic Surgeons and the Southern Thoracic Surgical Association VOLUME 16 * NUMBER 6 DECEMBER 1973 Paraesophageal Hernia A Life-Threatening Disease
THE ANNALS OF THORACIC SURGERY Journal of The Society of Thoracic Surgeons and the Southern Thoracic Surgical Association VOLUME 16 * NUMBER 6 DECEMBER 1973 Paraesophageal Hernia A Life-Threatening Disease
Module 2 Heartburn Glossary
 Absorption Antacids Antibiotic Module 2 Heartburn Glossary Barrett s oesophagus Bloating Body mass index Burping Chief cells Colon Digestion Endoscopy Enteroendocrine cells Epiglottis Epithelium Absorption
Absorption Antacids Antibiotic Module 2 Heartburn Glossary Barrett s oesophagus Bloating Body mass index Burping Chief cells Colon Digestion Endoscopy Enteroendocrine cells Epiglottis Epithelium Absorption
Left diaphragmmatic eventration with gastric volvulus: Laparoscopic mesh repair of left diaphragmatic eventration
 JMSR Dr. Lakshmikanth T Case Report Left diaphragmmatic eventration with gastric volvulus: Laparoscopic mesh repair of left diaphragmatic eventration Lakshmikanth T 1 and Sanjeeva Rao K 1 1 Department
JMSR Dr. Lakshmikanth T Case Report Left diaphragmmatic eventration with gastric volvulus: Laparoscopic mesh repair of left diaphragmatic eventration Lakshmikanth T 1 and Sanjeeva Rao K 1 1 Department
GI update. Common conditions and concerns my patients frequently asked about
 GI update Common conditions and concerns my patients frequently asked about Specific conditions I ll try to cover today 1. Colon polyps, colorectal cancer and colonoscopy 2. Crohn s disease 3. Peptic ulcer
GI update Common conditions and concerns my patients frequently asked about Specific conditions I ll try to cover today 1. Colon polyps, colorectal cancer and colonoscopy 2. Crohn s disease 3. Peptic ulcer
Disclosures. Gastroesophageal Reflux Disease. Gastroesophageal Reflux Disease
 Kunal Jajoo, MD Brigham and Women s Hospital July 2012 Disclosures Spouse is a physician employed by Boston Scientific Corporation The content of this lecture equitably discusses products of multiple companies
Kunal Jajoo, MD Brigham and Women s Hospital July 2012 Disclosures Spouse is a physician employed by Boston Scientific Corporation The content of this lecture equitably discusses products of multiple companies
CASE CONFERENCE GASTRIC VOLVULUS PIKOM, MD NONGLUK, MD; RADIOLOGIST
 CASE CONFERENCE GASTRIC VOLVULUS PIKOM, MD NONGLUK, MD; RADIOLOGIST IDENTIFICATION DATA ผ ป วยเด กชายไทย อาย 13 ว น เช อชาต ไทย ส ญชาต ไทย ภ ม ล าเนา จ งหว ด อ ท ยธาน เข าร บการร กษาท รพ.มหาว ทยาล ยนเรศวรว
CASE CONFERENCE GASTRIC VOLVULUS PIKOM, MD NONGLUK, MD; RADIOLOGIST IDENTIFICATION DATA ผ ป วยเด กชายไทย อาย 13 ว น เช อชาต ไทย ส ญชาต ไทย ภ ม ล าเนา จ งหว ด อ ท ยธาน เข าร บการร กษาท รพ.มหาว ทยาล ยนเรศวรว
Learning Objectives:
 Crescent City GI Update 2018 Ochsner Clinic, NOLA Optimizing Endoscopic Evaluation of Barrett s Esophagus What Should I Do in My Practice? Gregory G. Ginsberg, M.D. Professor of Medicine University of
Crescent City GI Update 2018 Ochsner Clinic, NOLA Optimizing Endoscopic Evaluation of Barrett s Esophagus What Should I Do in My Practice? Gregory G. Ginsberg, M.D. Professor of Medicine University of
Flouroscopy CT. Principal Modality (2): Case Report # [] Date accepted: 14 May 2015
![Flouroscopy CT. Principal Modality (2): Case Report # [] Date accepted: 14 May 2015](/thumbs/85/92263701.jpg "Flouroscopy CT. Principal Modality (2): Case Report # [] Date accepted: 14 May 2015") Radiological Category: Emergency Principal Modality (1): Principal Modality (2): Flouroscopy CT Case Report # [] Submitted by: Haider Virani, M.D. Faculty reviewer: Naga Chinapuvvula, MD Date accepted:
Radiological Category: Emergency Principal Modality (1): Principal Modality (2): Flouroscopy CT Case Report # [] Submitted by: Haider Virani, M.D. Faculty reviewer: Naga Chinapuvvula, MD Date accepted:
Gastro esophageal reflux disease DR. AMMAR I. ABDUL-LATIF
 Gastro esophageal reflux disease )GERD( DR. AMMAR I. ABDUL-LATIF GERD DEFINITION EPIDEMIOLOGY CAUSES PATHOGENESIS SIGNS &SYMPTOMS COMPLICATIONS DIAGNOSIS TREATMENT Definition Montreal consensus defined
Gastro esophageal reflux disease )GERD( DR. AMMAR I. ABDUL-LATIF GERD DEFINITION EPIDEMIOLOGY CAUSES PATHOGENESIS SIGNS &SYMPTOMS COMPLICATIONS DIAGNOSIS TREATMENT Definition Montreal consensus defined
Laparoscopic Anti-Reflux (GERD) Surgery Patient Information from SAGES
 Surgery Patient Information from SAGES") SAGES Society of American Gastrointestinal and Endoscopic Surgeons https://www.sages.org Laparoscopic Anti-Reflux (GERD) Surgery Patient Information from SAGES Author : SAGES Webmaster Surgery for Heartburn
SAGES Society of American Gastrointestinal and Endoscopic Surgeons https://www.sages.org Laparoscopic Anti-Reflux (GERD) Surgery Patient Information from SAGES Author : SAGES Webmaster Surgery for Heartburn
ACG Clinical Guideline: Diagnosis and Management of Gastroesophageal Reflux Disease
 ACG Clinical Guideline: Diagnosis and Management of Gastroesophageal Reflux Disease Philip O. Katz MD 1, Lauren B. Gerson MD, MSc 2 and Marcelo F. Vela MD, MSCR 3 1 Division of Gastroenterology, Einstein
ACG Clinical Guideline: Diagnosis and Management of Gastroesophageal Reflux Disease Philip O. Katz MD 1, Lauren B. Gerson MD, MSc 2 and Marcelo F. Vela MD, MSCR 3 1 Division of Gastroenterology, Einstein
Guiding Principles. Trans-oral Incisionless Fundoplication (TIF) for GERD: When, Why & How 4/6/18
 for GERD: When, Why & How 4/6/18") Gastroesophageal Reflux Disease Shaping the Future of GERD Management Treating patients with the TIF procedure using the EsophyX device (EndoGastric Solutions) Gonzalo Pandolfi, MD Trans-oral Incisionless
Gastroesophageal Reflux Disease Shaping the Future of GERD Management Treating patients with the TIF procedure using the EsophyX device (EndoGastric Solutions) Gonzalo Pandolfi, MD Trans-oral Incisionless
Large Hiatal Hernia with Floppy Fundus: Clinical and Radiographic Findings
 Radiography of Hiatal Hernia Gastrointestinal Imaging Clinical Observations Steven Y. Huang 1 Marc S. Levine 1 Stephen E. Rubesin 1 David A. Katzka 2 Igor Laufer 1 Huang SY, Levine MS, Rubesin SE, Katzka
Radiography of Hiatal Hernia Gastrointestinal Imaging Clinical Observations Steven Y. Huang 1 Marc S. Levine 1 Stephen E. Rubesin 1 David A. Katzka 2 Igor Laufer 1 Huang SY, Levine MS, Rubesin SE, Katzka
Disclosures. Heartburn and Barrett s Esophagus. Heartburn and Barrett s Esophagus. GERD is common in the U.S. None
 Heartburn and Barrett s Esophagus None Disclosures Christian Mathy, MD University of California, San Francisco 2015 Heartburn and Barrett s Esophagus Heartburn and GERD GERD therapy Extraesophageal GERD
Heartburn and Barrett s Esophagus None Disclosures Christian Mathy, MD University of California, San Francisco 2015 Heartburn and Barrett s Esophagus Heartburn and GERD GERD therapy Extraesophageal GERD
ENDOLUMINAL THERAPIES FOR GERD. University of Colorado Department of Surgery Grand Rounds March 31st, 2008
 ENDOLUMINAL THERAPIES FOR GERD University of Colorado Department of Surgery Grand Rounds March 31st, 2008 Overview GERD Healthcare significance Definitions Treatment objectives Endoscopic options Plication
ENDOLUMINAL THERAPIES FOR GERD University of Colorado Department of Surgery Grand Rounds March 31st, 2008 Overview GERD Healthcare significance Definitions Treatment objectives Endoscopic options Plication
PeriOperative Concerns for Anti Reflux Procedure Patients
 PeriOperative Concerns for Anti Reflux Procedure Patients Kevin Gillian, M.D., F.A.C.S. VHC Heartburn Center Director GERD word association Heartburn Chest pain Spicy food Tums Purple pills How big a problem
PeriOperative Concerns for Anti Reflux Procedure Patients Kevin Gillian, M.D., F.A.C.S. VHC Heartburn Center Director GERD word association Heartburn Chest pain Spicy food Tums Purple pills How big a problem
Early View Article: Online published version of an accepted article before publication in the final form.
 Early View Article: Online published version of an accepted article before publication in the final form. Journal Name: Journal of Case Reports and Images in Surgery Type of Article: Case Report Title:
Early View Article: Online published version of an accepted article before publication in the final form. Journal Name: Journal of Case Reports and Images in Surgery Type of Article: Case Report Title:
ACG Clinical Guideline: Diagnosis and Management of Barrett s Esophagus
 30 PRACTICE GUIDELINES nature publishing group CME ACG Clinical Guideline: Diagnosis and Management of Barrett s Esophagus Nicholas J. Shaheen, MD, MPH, FACG 1, Gary W. Falk, MD, MS, FACG 2, Prasad G.
30 PRACTICE GUIDELINES nature publishing group CME ACG Clinical Guideline: Diagnosis and Management of Barrett s Esophagus Nicholas J. Shaheen, MD, MPH, FACG 1, Gary W. Falk, MD, MS, FACG 2, Prasad G.
Medical Policy Manual. Topic: Gastric Reflux Surgery Date of Origin: November Section: Surgery Last Reviewed Date: March 2014
 Medical Policy Manual Topic: Gastric Reflux Surgery Date of Origin: November 2012 Section: Surgery Last Reviewed Date: March 2014 Policy No: 186 Effective Date: May 1, 2014 IMPORTANT REMINDER Medical Policies
Medical Policy Manual Topic: Gastric Reflux Surgery Date of Origin: November 2012 Section: Surgery Last Reviewed Date: March 2014 Policy No: 186 Effective Date: May 1, 2014 IMPORTANT REMINDER Medical Policies
Putting Chronic Heartburn On Ice
 Putting Chronic Heartburn On Ice Over the years, gastroesophageal reflux disease has proven to be one of the most common complaints facing family physicians. With quicker diagnosis, this pesky ailment
Putting Chronic Heartburn On Ice Over the years, gastroesophageal reflux disease has proven to be one of the most common complaints facing family physicians. With quicker diagnosis, this pesky ailment
Quiz Adenocarcinoma of the distal stomach has been increasing in the last 20 years. a. True b. False
 Quiz 1 1. Which of the following are risk factors for esophagus cancer. a. Obesity b. Gastroesophageal reflux c. Smoking and Alcohol d. All of the above 2. Adenocarcinoma of the distal stomach has been
Quiz 1 1. Which of the following are risk factors for esophagus cancer. a. Obesity b. Gastroesophageal reflux c. Smoking and Alcohol d. All of the above 2. Adenocarcinoma of the distal stomach has been
Facing Surgery for GERD (Gastroesophageal
 Facing Surgery for GERD (Gastroesophageal Reflux Disease)? Learn about minimally invasive da Vinci Surgery The Conditions: GERD, Hiatal Hernia Gastroesophageal reflux disease or GERD is a common digestive
Facing Surgery for GERD (Gastroesophageal Reflux Disease)? Learn about minimally invasive da Vinci Surgery The Conditions: GERD, Hiatal Hernia Gastroesophageal reflux disease or GERD is a common digestive
Barrett's Esophagus and Indications for Anti-reflux Procedures. Gamal Marey SUNY Downstate Medical Center (RUMC) 7/3/2014
 7/3/2014") Barrett's Esophagus and Indications for Anti-reflux Procedures Gamal Marey SUNY Downstate Medical Center (RUMC) 7/3/2014 History 46 y/o. female, 109 lbs, with PMH significant for long standing acid reflux
Barrett's Esophagus and Indications for Anti-reflux Procedures Gamal Marey SUNY Downstate Medical Center (RUMC) 7/3/2014 History 46 y/o. female, 109 lbs, with PMH significant for long standing acid reflux
Barrett s Esophagus. lining of the lower esophagus that bears his name (i.e., Barrett's esophagus). We now
. We now") Shamika Johnson Anatomy & Physiology 206 April 20, 2010 Barrett s Esophagus What is Barrett s Esophagus? Norman Barrett was a pathologist. In 1950, he described an abnormality in the lining of the lower
Shamika Johnson Anatomy & Physiology 206 April 20, 2010 Barrett s Esophagus What is Barrett s Esophagus? Norman Barrett was a pathologist. In 1950, he described an abnormality in the lining of the lower
GERD. Gastroesophageal reflux disease, or GERD, occurs when acid from the. stomach backs up into the esophagus. Normally, food travels from the
 GERD What is GERD? Gastroesophageal reflux disease, or GERD, occurs when acid from the stomach backs up into the esophagus. Normally, food travels from the mouth, down through the esophagus and into the
GERD What is GERD? Gastroesophageal reflux disease, or GERD, occurs when acid from the stomach backs up into the esophagus. Normally, food travels from the mouth, down through the esophagus and into the
Disclosures. GI Motility Disorders. Gastrointestinal Motility Disorders & Irritable Bowel Syndrome
 Gastrointestinal Motility Disorders & Irritable Bowel Syndrome None Disclosures Jasmine Zia, MD Acting Assistant Professor Division of Gastroenterology, University of Washington 6 th Asian Health Symposium
Gastrointestinal Motility Disorders & Irritable Bowel Syndrome None Disclosures Jasmine Zia, MD Acting Assistant Professor Division of Gastroenterology, University of Washington 6 th Asian Health Symposium
GENERAL SURGERY GRAND ROUNDS DEC 12, 2012
 GENERAL SURGERY GRAND ROUNDS DEC 12, 2012 CASE I- WT 62 yo retired veteran; tx care to VHAMEM June 2012. Hx Barrett s esophagus with high grade dysplasia. Beside GERD, had PTSD and some drug issuesmarijuana,
GENERAL SURGERY GRAND ROUNDS DEC 12, 2012 CASE I- WT 62 yo retired veteran; tx care to VHAMEM June 2012. Hx Barrett s esophagus with high grade dysplasia. Beside GERD, had PTSD and some drug issuesmarijuana,
Gastroesophageal Reflux Disease in Infants and Children
 Gastroesophageal Reflux Disease in Infants and Children 4 Marzo 2017 Drssa Chiara Leoni Drssa Valentina Giorgio pediatriagastro@gmail.com valentinagiorgio1@gmail.com Definitions: GER GER is the passage
Gastroesophageal Reflux Disease in Infants and Children 4 Marzo 2017 Drssa Chiara Leoni Drssa Valentina Giorgio pediatriagastro@gmail.com valentinagiorgio1@gmail.com Definitions: GER GER is the passage
Management of Barrett s Esophagus. Case Presentation
 Management of Barrett s Esophagus Lauren B. Gerson MD, MSc Associate Clinical Professor, UCSF Director of Clinical Research Gastroenterology Fellowship Program California Pacific Medical Center San Francisco,
Management of Barrett s Esophagus Lauren B. Gerson MD, MSc Associate Clinical Professor, UCSF Director of Clinical Research Gastroenterology Fellowship Program California Pacific Medical Center San Francisco,
The Physician as Medical Illustrator
 The Physician as Medical Illustrator Francois Luks Arlet Kurkchubasche Division of Pediatric Surgery Wednesday, December 9, 2015 Week 5 A good picture is worth a 1,000 bad ones How to illustrate an operation
The Physician as Medical Illustrator Francois Luks Arlet Kurkchubasche Division of Pediatric Surgery Wednesday, December 9, 2015 Week 5 A good picture is worth a 1,000 bad ones How to illustrate an operation
What causes GER? How is GERD treated? It is necessary to take these consecutive steps: a) Changes in your lifestyle b) Drug treatment c) Surgery
 Changes in your lifestyle b) Drug treatment c) Surgery") When Gastric acids ascend the esophagus, they produce heartburn behind the sternum that can even reach the throat. Other symptoms are chronic cough, frequent vomits, and chronic affectation to the throat
When Gastric acids ascend the esophagus, they produce heartburn behind the sternum that can even reach the throat. Other symptoms are chronic cough, frequent vomits, and chronic affectation to the throat
The normal esophagus is lined with squamous epithelium.
 .. ALAN J. CAMERON, M.D. In Barrett's esophagus, the squamous lining of the lower esophagus is replaced by columnar epithelium. Barrett's esophagus is associated with gastroesophageal reflux and an increased
.. ALAN J. CAMERON, M.D. In Barrett's esophagus, the squamous lining of the lower esophagus is replaced by columnar epithelium. Barrett's esophagus is associated with gastroesophageal reflux and an increased
Clinical Payment and Coding Policy Committee Approval Date: 02/23/2018
 In the event of a conflict between a Clinical Payment and Coding Policy and any plan document under which a member is entitled to Covered Services, the plan document will govern. Plan documents include,
In the event of a conflict between a Clinical Payment and Coding Policy and any plan document under which a member is entitled to Covered Services, the plan document will govern. Plan documents include,
Chapter 14: Training in Radiology. DDSEP Chapter 1: Question 12
 DDSEP Chapter 1: Question 12 A 52-year-old white male presents for evaluation of sudden onset of abdominal pain and shoulder pain. His past medical history is notable for a history of coronary artery disease,
DDSEP Chapter 1: Question 12 A 52-year-old white male presents for evaluation of sudden onset of abdominal pain and shoulder pain. His past medical history is notable for a history of coronary artery disease,
Clinical Payment and Coding Policy Committee Approval Date: 02/23/2018
 In the event of conflict between a Clinical Payment and Coding Policy and any plan document under which a member is entitled to Covered Services, the plan document will govern. Plan documents include,
In the event of conflict between a Clinical Payment and Coding Policy and any plan document under which a member is entitled to Covered Services, the plan document will govern. Plan documents include,
4/24/2015. History of Reflux Surgery. Recent Innovations in the Surgical Treatment of Reflux
 Recent Innovations in the Surgical Treatment of Reflux Scott Carpenter, DO, FACOS, FACS Mercy Hospital Ardmore Ardmore, OK History of Reflux Surgery - 18 th century- first use of term heartburn - 1934-
Recent Innovations in the Surgical Treatment of Reflux Scott Carpenter, DO, FACOS, FACS Mercy Hospital Ardmore Ardmore, OK History of Reflux Surgery - 18 th century- first use of term heartburn - 1934-
HIATAL HERNIA, DIVERTICULITIS AND VARICOSE VEINS: Three Peas In A Pod By Evan Almeda READ ONLINE
 HIATAL HERNIA, DIVERTICULITIS AND VARICOSE VEINS: Three Peas In A Pod By Evan Almeda READ ONLINE What is a hiatal hernia? Unlike ventral hernias, which protrude through the abdominal wall, The good news
HIATAL HERNIA, DIVERTICULITIS AND VARICOSE VEINS: Three Peas In A Pod By Evan Almeda READ ONLINE What is a hiatal hernia? Unlike ventral hernias, which protrude through the abdominal wall, The good news
Histopathology of Endoscopic Resection Specimens from Barrett's Esophagus
 Histopathology of Endoscopic Resection Specimens from Barrett's Esophagus Br J Surg 38 oct. 1950 Definition of Barrett's esophagus A change in the esophageal epithelium of any length that can be recognized
Histopathology of Endoscopic Resection Specimens from Barrett's Esophagus Br J Surg 38 oct. 1950 Definition of Barrett's esophagus A change in the esophageal epithelium of any length that can be recognized
Effective Health Care
 Effective Health Care Comparative Effectiveness of Management Strategies for Gastroesophageal Reflux Disease Executive Summary Background Gastroesophageal reflux disease (GERD), defined as weekly heartburn
Effective Health Care Comparative Effectiveness of Management Strategies for Gastroesophageal Reflux Disease Executive Summary Background Gastroesophageal reflux disease (GERD), defined as weekly heartburn
Paraesophageal hiatal hernias (type II, III, IV) are. Effect of Paraesophageal Hernia Repair on Pulmonary Function
 are. Effect of Paraesophageal Hernia Repair on Pulmonary Function") Effect of Paraesophageal Hernia Repair on Pulmonary Function Donald E. Low, MD, and Eric J. Simchuk, MD Section of General Thoracic Surgery, Virginia Mason Medical Center, Seattle, Washington Background.
Effect of Paraesophageal Hernia Repair on Pulmonary Function Donald E. Low, MD, and Eric J. Simchuk, MD Section of General Thoracic Surgery, Virginia Mason Medical Center, Seattle, Washington Background.
INTRODUCTION TO UPPER ENDOSCOPY
 INTRODUCTION TO UPPER ENDOSCOPY Satish Nagula, MD Associate Professor of Medicine Icahn School of Medicine at Mount Sinai NYSGE First Year Fellows Course July 14, 2018 Early endoscopes 1805: Bozzini Lichtleiter
INTRODUCTION TO UPPER ENDOSCOPY Satish Nagula, MD Associate Professor of Medicine Icahn School of Medicine at Mount Sinai NYSGE First Year Fellows Course July 14, 2018 Early endoscopes 1805: Bozzini Lichtleiter
01/26/2010 GENERAL SURGERY ABSITE ANATOMY ANATOMY. Yvonne M. Carter, MD Georgetown University Medical Center. Layers. mucosa. squamous epithelium
 GENERAL SURGERY ABSITE REVIEW: ESOPHAGUS Yvonne M. Carter, MD Georgetown University Medical Center ANATOMY Layers mucosa muscle squamous epithelium columnar epithelium (distal 2cm) inner = circular outer
GENERAL SURGERY ABSITE REVIEW: ESOPHAGUS Yvonne M. Carter, MD Georgetown University Medical Center ANATOMY Layers mucosa muscle squamous epithelium columnar epithelium (distal 2cm) inner = circular outer
New Developments in the Endoscopic Diagnosis and Management of Barrett s Esophagus
 New Developments in the Endoscopic Diagnosis and Management of Barrett s Esophagus Prateek Sharma, MD Key Clinical Management Points: Endoscopic recognition of a columnar lined distal esophagus is crucial
New Developments in the Endoscopic Diagnosis and Management of Barrett s Esophagus Prateek Sharma, MD Key Clinical Management Points: Endoscopic recognition of a columnar lined distal esophagus is crucial
Esophageal Cancer. What is esophageal cancer? What is the esophagus?
 Jeff Stemberger was committed to his family and his faith. He was dedicated to his fast-paced career, but made time to enjoy the simple things in life with his wife and children, stay close to his mom
Jeff Stemberger was committed to his family and his faith. He was dedicated to his fast-paced career, but made time to enjoy the simple things in life with his wife and children, stay close to his mom
Everything Esophagus: Barrett s Esophagus. Nicholas Shaheen, MD, MPH Center for Esophageal Diseases and Swallowing University of North Carolina
 Everything Esophagus: Barrett s Esophagus Nicholas Shaheen, MD, MPH Center for Esophageal Diseases and Swallowing University of North Carolina The Most Important Thing Stayed the Same Adenocarcinoma A
Everything Esophagus: Barrett s Esophagus Nicholas Shaheen, MD, MPH Center for Esophageal Diseases and Swallowing University of North Carolina The Most Important Thing Stayed the Same Adenocarcinoma A
The STRETTA Procedure
 THE HEARTBURN AND REFLUX STUDY CENTER The STRETTA Procedure Introduction The STRETTA procedure is an advanced state-of-the-art endoscopic technique for the correction of all forms of reflux disease including:
THE HEARTBURN AND REFLUX STUDY CENTER The STRETTA Procedure Introduction The STRETTA procedure is an advanced state-of-the-art endoscopic technique for the correction of all forms of reflux disease including:
Clinical Study Congenital Paraesophageal Hernia with Intrathoracic Gastric Volvolus in Two Sisters
 International Scholarly Research Network ISRN Surgery Volume 2011, Article ID 856568, 5 pages doi:10.5402/2011/856568 Clinical Study Congenital Paraesophageal Hernia with Intrathoracic Gastric Volvolus
International Scholarly Research Network ISRN Surgery Volume 2011, Article ID 856568, 5 pages doi:10.5402/2011/856568 Clinical Study Congenital Paraesophageal Hernia with Intrathoracic Gastric Volvolus
LINX. A new, FDA approved treatment for GERD
 LINX A new, FDA approved treatment for GERD What Causes Reflux? Gastroesophageal reflux disease (GERD), also called reflux, is a chronic, often progressive disease caused by a weak lower esophageal sphincter
LINX A new, FDA approved treatment for GERD What Causes Reflux? Gastroesophageal reflux disease (GERD), also called reflux, is a chronic, often progressive disease caused by a weak lower esophageal sphincter
Correspondence should be addressed to Saptarshi Biswas;
 Hindawi Case Reports in Surgery Volume 2017, Article ID 8412927, 4 pages https://doi.org/10.1155/2017/8412927 Case Report Jejunal Diverticular Perforation Causing Small Bowel Obstruction in a Type 4 Hiatal
Hindawi Case Reports in Surgery Volume 2017, Article ID 8412927, 4 pages https://doi.org/10.1155/2017/8412927 Case Report Jejunal Diverticular Perforation Causing Small Bowel Obstruction in a Type 4 Hiatal
DISCLAIMER. No Conflict of Interest
 DISCLAIMER No Conflict of Interest EXCLAIMER No Interest in Conflict GORD IS SURGICAL John Dunn, FRACS Laparoscopy Auckland GOD IS SURGICAL He taua ano ta te kai (Even food can attack) PATHOGENESIS Failure
DISCLAIMER No Conflict of Interest EXCLAIMER No Interest in Conflict GORD IS SURGICAL John Dunn, FRACS Laparoscopy Auckland GOD IS SURGICAL He taua ano ta te kai (Even food can attack) PATHOGENESIS Failure
The Combined Collis-Nissen Operation: Early Assessment of Reflwx Control
 ORIGINAL ARTICLES The Combined Collis-Nissen Operation: Early Assessment of Reflwx Control Mark B. Orringer, M.D., and Jay S. Orringer, M.D. ABSTRACT This report summarizes the clinical experience with
ORIGINAL ARTICLES The Combined Collis-Nissen Operation: Early Assessment of Reflwx Control Mark B. Orringer, M.D., and Jay S. Orringer, M.D. ABSTRACT This report summarizes the clinical experience with
Early View Article: Online published version of an accepted article before publication in the final form.
 : Online published version of an accepted article before publication in the final form. Journal Name: Journal of Case Reports and Images in Surgery Type of Article: Case Report Title: A rare case of Type
: Online published version of an accepted article before publication in the final form. Journal Name: Journal of Case Reports and Images in Surgery Type of Article: Case Report Title: A rare case of Type
Case Scenario year-old white male presented to personal physician with dyspepsia with reflux.
 Case Scenario 1 57-year-old white male presented to personal physician with dyspepsia with reflux. 7/12 EGD: In the gastroesophageal junction we found an exophytic tumor. The tumor occupies approximately
Case Scenario 1 57-year-old white male presented to personal physician with dyspepsia with reflux. 7/12 EGD: In the gastroesophageal junction we found an exophytic tumor. The tumor occupies approximately
A Multidisciplinary Approach to Esophageal Dysphagia: Role of the SLP. Darlene Graner, M.A., CCC-SLP, BRS-S Sharon Burton, M.D.
 A Multidisciplinary Approach to Esophageal Dysphagia: Role of the SLP Darlene Graner, M.A., CCC-SLP, BRS-S Sharon Burton, M.D. What is the role of the SLP? Historically SLPs the preferred providers for
A Multidisciplinary Approach to Esophageal Dysphagia: Role of the SLP Darlene Graner, M.A., CCC-SLP, BRS-S Sharon Burton, M.D. What is the role of the SLP? Historically SLPs the preferred providers for
What Is Barrett s Esophagus?
 What Is Barrett s Esophagus? Having Barrett s esophagus means the cells lining the esophagus (the tube that links the mouth and the stomach) have changed into types of intestinal cells that are not normal
What Is Barrett s Esophagus? Having Barrett s esophagus means the cells lining the esophagus (the tube that links the mouth and the stomach) have changed into types of intestinal cells that are not normal
Esophageal Cancer. Source: National Cancer Institute
 Esophageal Cancer Esophageal cancer forms in the tissues that line the esophagus, or the long, hollow tube that connects the mouth and stomach. Food and drink pass through the esophagus to be digested.
Esophageal Cancer Esophageal cancer forms in the tissues that line the esophagus, or the long, hollow tube that connects the mouth and stomach. Food and drink pass through the esophagus to be digested.
Anatomy: From cricoid cartilage to diaphragm 25 Cms. 4 portions: Cervical 5 cms. Thoracic 25 cms. Abdominal 2 cms. Blood supply Lymphatic spread
 Esophagus Anatomy: From cricoid cartilage to diaphragm 25 Cms. 4 portions: Cervical 5 cms. Thoracic 25 cms. Abdominal 2 cms. Blood supply Lymphatic spread Upper 2/3 Cephalad Lower 1/3 Caudad Physiology:
Esophagus Anatomy: From cricoid cartilage to diaphragm 25 Cms. 4 portions: Cervical 5 cms. Thoracic 25 cms. Abdominal 2 cms. Blood supply Lymphatic spread Upper 2/3 Cephalad Lower 1/3 Caudad Physiology:
https://www.uptodate.com/contents/acid-reflux-gastroesophageal-reflux-disease-in-adults-...
 Page 1 of 10 Official reprint from UpToDate www.uptodate.com 2017 UpToDate The content on the UpToDate website is not intended nor recommended as a substitute for medical advice, diagnosis, or treatment.
Page 1 of 10 Official reprint from UpToDate www.uptodate.com 2017 UpToDate The content on the UpToDate website is not intended nor recommended as a substitute for medical advice, diagnosis, or treatment.
Gastrointestinal pathology 2018 lecture 2. Dr Heyam Awad FRCPath
 Gastrointestinal pathology 2018 lecture 2 Dr Heyam Awad FRCPath Eosinophilic esophagitis Incidence of eosinophilic gastritis is increasing. Symptoms: food impaction and dysphagia. Histology: infiltration
Gastrointestinal pathology 2018 lecture 2 Dr Heyam Awad FRCPath Eosinophilic esophagitis Incidence of eosinophilic gastritis is increasing. Symptoms: food impaction and dysphagia. Histology: infiltration
Combined Experience of Two European Centers
 Minimally Invasive Surgery for Achalasia: Combined Experience of Two European Centers Garzi A, Valla JS*, Molinaro F, Amato G, Messina M. Unit of Pediatric Surgery, University of Siena (Italy) *Lenval
Minimally Invasive Surgery for Achalasia: Combined Experience of Two European Centers Garzi A, Valla JS*, Molinaro F, Amato G, Messina M. Unit of Pediatric Surgery, University of Siena (Italy) *Lenval
Chapter 2 Complications of Gastroesophageal Reflux Disease
 Chapter 2 Complications of Gastroesophageal Reflux Disease Patrick Yachimski Acute esophageal exposure to gastric and/or duodenal refluxate can result in pyrosis and symptomatic gastroesophageal reflux
Chapter 2 Complications of Gastroesophageal Reflux Disease Patrick Yachimski Acute esophageal exposure to gastric and/or duodenal refluxate can result in pyrosis and symptomatic gastroesophageal reflux
EGD. John M. Wo, M.D. University of Louisville July 3, 2008
 EGD John M. Wo, M.D. University of Louisville July 3, 2008 Different Ways to do an EGD Which scope? Pediatric, regular, jumbo EGD endoscope or pediatric colonoscope Transnasal vs. transoral insertion Sedation
EGD John M. Wo, M.D. University of Louisville July 3, 2008 Different Ways to do an EGD Which scope? Pediatric, regular, jumbo EGD endoscope or pediatric colonoscope Transnasal vs. transoral insertion Sedation
June By: Reza Gholami
 ACG/CAG guideline on Management of Dyspepsia June 2017 By: Reza Gholami DEFINITION OF DYSPEPSIA AND SCOPE OF THE GUIDELINE Dyspepsia was originally defined as any symptoms referable to the upper gastrointestinal
ACG/CAG guideline on Management of Dyspepsia June 2017 By: Reza Gholami DEFINITION OF DYSPEPSIA AND SCOPE OF THE GUIDELINE Dyspepsia was originally defined as any symptoms referable to the upper gastrointestinal
Medical Illustration PLME 0400
 Introduction to Medical Illustration PLME 0400 October 17 From sketch to narrative From Sketch to Sketch: Point of view Degree of detail Visible and invisble parts Landmarks : Plan your moves The IKEA
Introduction to Medical Illustration PLME 0400 October 17 From sketch to narrative From Sketch to Sketch: Point of view Degree of detail Visible and invisble parts Landmarks : Plan your moves The IKEA
Faculty Disclosure. Objectives. State of the Art #3: Referrals for Gastroscopy (focus on common esophagus problems) 24/11/2014
 24/11/2014") State of the Art #3: Referrals for Gastroscopy (focus on common esophagus problems) Dr. Amy Morse November 2014 Faculty: Amy Morse Faculty Disclosure Relationships with commercial interests: Grants/Research
State of the Art #3: Referrals for Gastroscopy (focus on common esophagus problems) Dr. Amy Morse November 2014 Faculty: Amy Morse Faculty Disclosure Relationships with commercial interests: Grants/Research
Treating Achalasia. When to consider surgery and New options for therapy
 Treating Achalasia When to consider surgery and New options for therapy James B. Wooldridge,Jr., MD Ochsner Medical Center Senior Staff Surgeon General, Laparoscopic, and Bariatric Surgery Disclosures
Treating Achalasia When to consider surgery and New options for therapy James B. Wooldridge,Jr., MD Ochsner Medical Center Senior Staff Surgeon General, Laparoscopic, and Bariatric Surgery Disclosures
GASTROINTESTINAL TRACT
 GASTROINTESTINAL TRACT ESOPHAGUS Clinical manifestations: 1-Dysphagia (difficulty in swallowing), which is attributed either to deranged esophageal motor function or to narrowing or obstruction of the
GASTROINTESTINAL TRACT ESOPHAGUS Clinical manifestations: 1-Dysphagia (difficulty in swallowing), which is attributed either to deranged esophageal motor function or to narrowing or obstruction of the
Laparoscopic Management of Giant Paraesophageal Herniation
 Laparoscopic Management of Giant Paraesophageal Herniation Robert J. Wiechmann, MD, Mark K. Ferguson, MD, Keith S. Naunheim, MD, Paul McKesey, Steven J. Hazelrigg, MD, Tibetha S. Santucci, RN, Robin S.
Laparoscopic Management of Giant Paraesophageal Herniation Robert J. Wiechmann, MD, Mark K. Ferguson, MD, Keith S. Naunheim, MD, Paul McKesey, Steven J. Hazelrigg, MD, Tibetha S. Santucci, RN, Robin S.
Hernia Symptoms And Signs
 Hernia Symptoms And Signs 1 / 6 2 / 6 3 / 6 Hernia Symptoms And Signs The signs and symptoms of a hernia can range from noticing a painless lump to the severely painful, tender, swollen protrusion of tissue
Hernia Symptoms And Signs 1 / 6 2 / 6 3 / 6 Hernia Symptoms And Signs The signs and symptoms of a hernia can range from noticing a painless lump to the severely painful, tender, swollen protrusion of tissue
Barrett s Esophagus: State of the Art Management
 In the Name of God Barrett s Esophagus: State of the Art Management Siavosh Nasseri-Moghaddam MD, MPH, AGAF Associate Professor of Medicine Digestive Disease Research Center, Shariati Hospital, TUMS IAGH
In the Name of God Barrett s Esophagus: State of the Art Management Siavosh Nasseri-Moghaddam MD, MPH, AGAF Associate Professor of Medicine Digestive Disease Research Center, Shariati Hospital, TUMS IAGH