Barrett s Esophagus: State of the Art Management
|
|
|
- Samson Strickland
- 5 years ago
- Views:
Transcription
 sianm@ams.ac.")
1 In the Name of God Barrett s Esophagus: State of the Art Management Siavosh Nasseri-Moghaddam MD, MPH, AGAF Associate Professor of Medicine Digestive Disease Research Center, Shariati Hospital, TUMS IAGH monthly meeting, Bahman 1393 (Feb 2015) sianm@ams.ac.ir
2 Hx First described in 1950 by two surgeons, Norman Barrett in the United Kingdom and Jean-Louis Lortat-Jacob in France

3 Norman Barrett (1903)
4 What is Barrett s Esophagus? Esophagus lined by Columnar mucosa (Columnar lined epithelium, CLE) Specialized intestinal metaplasia (SIM) present on histological examination
5

6

7


8 Metaplastic Columnar Epithelium Stratified Squamous Epithelium Barrett s Esophagus The condition in which a metaplastic columnar epithelium that predisposes to cancer development replaces the stratified squamous epithelium that normally lines the distal esophagus Affects 5.6% of adult Americans AGA Medical Position Statement. Gastroenterology 2011;140:1084.
9 What is the significance of BE? By itself: nothing! The chances of development of dysplasia in this metaplastic tissue is what makes it apparently important What are these chances Initially estimated at 1%/year or less Later 0.45%/year Now: %/year

10 Estimates of Cancer Risk for Individual Patients with Non-Dysplastic Barrett s Have Been Falling 1990s Estimate: 1% per year 1 in 100 patients per year Drewitz. Am J Gastroenterol 1997;92: s Estimate: 0.5% per year 1 in 200 patients per year Shaheen. Gastroenterology 2000;119: Estimate: 0.25% per year 1 in 400 patients per year
11 The absolute risk of esophageal adenocarcinoma developing in a person 50 years of age or older is approximately 0.025% per year. However, up to 40% (in some reports over 50%) of all patients with esophageal cancer do not report GERD symptoms % of esophageal adenocas are seen in pts without known Barrett esophagus
12
13 Hypothetical scenario In the US 77million over 50 Y/O If 14% weekly GERD & BE prevalence 14% about 10 million BEs If all adenocas arise in BE 6500 will develop adenoca Annual Ca incidence rate: If 50% of adenocas rise in GERD pts: If 20% of adenoca rise in GERD pts: The figure in Iran is much lower because BE is much less infrequent (probably 1/10 th or less: ) Annual incidence rate of serious injury/death due to car accidents in Iran: So driving in Iran or simply crossing the streets is at least 125x more dangerous than developing esophageal adenoca if you have BE!
14 Guidelines for Endoscopy in GERD Upper endoscopy is indicated in men and women with heartburn and alarm symptoms (dysphagia, bleeding, anemia, weight loss, and recurrent vomiting). ACP Guidelines. Ann Intern Med 2012;157:808. Upper endoscopy is indicated in men and women with typical GERD symptoms that persist despite a therapeutic trial of 4 to 8 weeks of twice-daily proton pump inhibitor therapy. Upper endoscopy is not required in the presence of typical GERD symptoms. Endoscopy is recommended in the presence of alarm symptoms and for screening of patients at high risk for complications [Barrett s esophagus]. ACG Guidelines. Katz et al. AJG 2013;108:308.

15 AGA Medical Position Statement on Endoscopic Screening for Barrett s Esophagus We recommend against screening the general population with GERD for Barrett s esophagus. In patients with multiple risk factors associated with esophageal adenocarcinoma, we suggest screening for Barrett s esophagus. Norman Barrett Chronic GERD, hiatal hernia, age 50, male gender, white race, elevated BMI, intraabdominal body fat distribution Spechler et al. Gastroenterology 2011;140:1084.
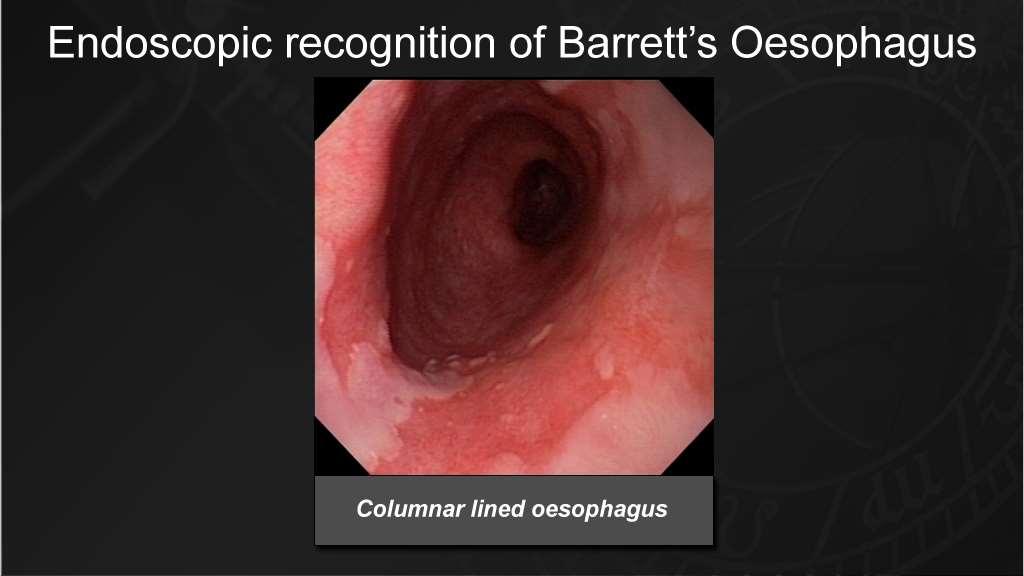
16 How is BE diagnosed? In a relaxed patient undergoing UGIE During scope withdrawal while the esophagus is partially deflated Finding columnar lined mucosa in the distal esophagus (above the proximal end of gastric folds) Confirm presence of SIM by histological examiantion NOTE: Please DO NOT report Barrett s Esophagus in your endoscopy notes. Just report columnar lined mucosa.


17 Proposed Endoscopic Landmark for GEJ Proximal extent of gastric folds Columnar Lined Esophagus GEJ McClave. Gastrointest Endosc 1987;33:413.

18

19
20 How is it reported or categorized? Prague classification In a relaxed patient while withdrawing the scope locate the proximal end of gastric folds as distance (cm) from incisors Pull back and locate the most proximal end of circumferential columnar lined esophagus (distance from incisors, cm) Pull back and locate the proximal end of tongues of columnar lined esophagus (distance from incisors, cm) Report as: Columnar lined esophagus: CxMy
21

22
23 CLE detected on EGD Four quadrant bx every 1-2cm SIM+, No Dysplasia - repeat q3-5y SIM+, LGD+ SIM+, HGD+ Pathologist repeat q6-12m or ablation confirmed by SECOND Intervention
24 What is dsyplasia and how is it diagnosed?

25 Histological Features of Dysplasia in Barrett s Esophagus Nuclei: enlargement, pleomorphism, hyperchromatism, stratification, atypical mitoses No Dysplasia Dysplasia Villiform surfaces and tubules show crowding
26 How is dysplasia classified? High grade dysplasia (HGD) vs Low Grade Dysplasia (LGD) What is the difference? What is their significance?


27 Illustrations of Barrett s dysplasias in a new GI pathology textbook Low-grade High-grade These don t look alike. Any fool can tell the differences between them. Where does LGD end and HGD begin?
28 Follow Highest LGD Lowest HGD Treat Neg Indef LGD HGD The standard diagnoses used for biopsies of Barrett s mucosa
29 How concordant are pathologists in diagnosing dysplasia? Concordance for LGD: 0.33% Concordance for HGD: 0.67%
30
31 Endoscopic Surveillance Might Not Decrease Mortality from Esophageal Adenocarcinoma 8,272 pts. with Barrett s esophagus (BE) Surveillance 351 pts. with endoscopy esophageal within adenocarcinoma 3 years was (EAC) NOT associated with decreased risk of death from 70 EAC in pts. with prior diagnosis of BE ( 6 months) esophageal cancer (adjusted odds ratio 0.99; 95% CI ) Cases 8 pts. with confirmed death from esophageal cancer Controls 101 living Barrett s pts. matched for age, sex, follow-up duration 55% surveillance endoscopy performed within 3 years 60% surveillance endoscopy performed within 3 years Corley DA. Gastroenterology 2013;145:312
32 Randomized Trial of RFA vs. Surveillance for Low- Grade Dysplasia (LGD) in Barrett s Esophagus Data 136 & patients Safety with Monitoring LGD confirmed Board early by termination: expert pathologist RFA superior to surveillance for preventing neoplastic Randomized to RFA progression (68 pts.) or surveillance (68 pts.) Potential for patient safety issues if trial continued Progression to high-grade dysplasia or cancer at 3 years 1.5% RFA group 26.5% surveillance group 25% risk of progression (95% CI %, P<.001) Progression to cancer at 3 years 1.5% RFA group 8.8% surveillance group 7.4% risk of cancer (95% CI %, P=.03) Phoa KN. JAMA 2014;311:120



33 Endoscopic Eradication Therapy for Mucosal Neoplasia in Barrett s Esophagus EMR of mucosal 2015 irregularities for staging and therapy Ablate the remaining Barrett s metaplasia to minimize metachronous neoplasia

34 Subsquamous Intestinal Metaplasia (SSIM) Protected from destruction by RFA? Squamous Epithelium Hidden from endoscopist Intestinal Metaplasia
35
36 Is Barrett Esophagus a Complication of GERD?

37 1950: 38:
38

39 Painting to show the characteristic appearances of ' reflux usoohanitis ' and ' oeotic ulcer of the esophagus' as seen at endoscopy

40 I submit that most of these cases are in truth examples of congenital short esophagus, in which there is neither general Inflammation nor stricture formation, but in which a part of the stomach extends upwards into the mediastinum -or even to the neck-and that in this stomach a typical chronic GU can form. I urge that, as accurate surgery must rest upon accurate pathology, we must distinguish between gastric and esophageal ulcers.
41 Peptic oesophagitis and peptic ulceration of the squamous epithelium of the oesophagus are secondary to regurgitation of digestive juices, are most commonly found in those patients where the competence of the cardia has been lost through herniation of the stomach into the mediastinum, and have been aptly named by Barrett (1950) " reflux oesophagitis."
42 Allison and Johnstone 1953 It describes accurately in two words the pathology and aetiology of a condition which is a common cause of digestive disorder. In the same paper Barrett for the first time drew a sharp distinction between the above and lesions which had previously been described by pathologists as peptic ulcers of the oesophagus, but which in fact were gastric ulcers occurring in gastric mucous membrane lining a viscus which, from the outside, looked like oesophagus.
43 Reflux esophagitis ulcer (peptic ulcer of the esophagus): Dense submucosal fibrosis Superficial ulcer (missed easily) May ooze, rarely bleeds Does not perforate Trivial findings on necropsy Nothing interesting to keep in museum Allison and Johnstone 1953 Ulcer in the esophagus with a gastric lining: Behaves like an ulcer in the abdominal stomach Causes stricture May bleed profusely May perforate Easily found at necropsy Kept in museum
44 Allison and Johnstone 1953 The result has been that pathologists have been describing one thing and clinicians another, and they have had the same name. The clarification of this point has been so important, and the description of a gastric ulcer in the oesophagus so confusing, that it would seem to be justifiable to refer to the latter as Barrett's ulcer. The use of the eponym does not imply agreement with Barrett's description of an oesophagus lined with gastric mucous membrane as " stomach." Such a usage merely replaces one confusion by another.
45 Allison and Johnstone 1953 A variable amount of the oesophagus below the aortic arch may be lined by gastric mucosa of cardiac type. This is presumably, but not necessarily in every case, a congenital abnormality, and in the series presented has always been associated with herniation of the true stomach through the diaphragmatic hiatus, with the cardia lying in the mediastinum.
46 Barrett, N. R The lower esophagus lined by columnar epithelium. Surgery 41: Barrett accepted this view
47 Heterotopic mucosa, a common finding in the "normal" esophagus, may take one or more forms 1. During early fetal life, the lining of the esophagus is derived from the simple columnar epithelium of the primitive foregut. 1. In the 5th or 6th month epidermoid mucosa begins to replace the cylindrical cells. 2. This process originates in the midesophagus and extends caudally and orally so that by the end of gestation the fetal esophagus is covered by squamous epithelium. 3. At birth, persisting islands of columnar mucosa may be found in the cervical esophagus, which is the last portion to become stratified. 2. By the 7th week of fetal life, caudal descent of the stomach has been completed. 1. When clusters of potentially gastric cells remain within the esophagus, characteristic nests of ectopic gastric fundic epithelium may occur after birth at any level of the esophagus. 3. The superficial cardiac glands of the lamina propria may also represent true gastric rests. Although general agreement on this point is lacking.
48
49 M 18 Y/O in 1946 Daily nausea/self-induced vomiting 1960: Heartburn/black stool antacids/sedatives 1961: admission for heartburn, pp abd pain, hematemesis XR: duodenal deformity, small SHH, questionable esophagitis Esophagoscopy: slight redness of the distal esophagus Bx

50 Squamous epithelium (1961)
51 Anticholinergics, antacids, head of bed elevation persistent SS 1962: Admisison for heartburn, mid-dorsal pain, regurgitation, and melena Cinefluorography: ulcer in posterior wall of the esophagus about 5 cm above the cardioesophageal junction. At this point the esophagus was dilated and the ulcer appeared to lie within an intraluminal filling defect. The radiological diagnosis was "probable ulceration in a leiomyoma but carcinoma cannot be excluded." Esophagoscopy: reddened esophageal mucosa distal to 37 cm and a normally located esophagogastric junction at 40 cm from the incisor teeth. At 38 cm a deep, posterior wall crater was seen. Bx of the superior margin of the ulcer

52 acute and chronic inflammation in gastric mucosa
53 2 m later admitted again: Hematemesis WN man, mild epigastric tenderness and tarry stool (guaiac, 4+) in the rectum BP: 120/80 mm Hg; PR: 136/min; RR: 20/min; and T: 99 F. Hb: 8.6 g/100 ml; WBC: 21,800/mm3,; BUN: 37mg/l00 ml; BS: 102mg/l00 ml; and U/A: negative. NG tube: black, guaiac-positive material After 2 units of whole blood, Hb increased to 10.3 g/l00 ml

54 large ulcer approximately 2 cm above a sliding esophageal hiatal hernia
55 Esophagoscopy: red, friable, bleeding esophageal mucosa starting at 20 cm from the incisor teeth and extending to the gastroesophageal junction (40 cm). A mass of heaped-up mucosa at 37cm

56 Columnar epithelium lining the esophagus (at 22, 30, & 37cm)

57 Squamous epithelium at 18cm
58 1 week later vagotomy/pyloropolasty Since surgery: no recurrence of SS His daily episodes of vomiting ceased Esophagogram, 6 months later: negative except for a small, residual hiatal hernia
59 There are animal models where induced severe esophagitis heals with columnar metaplasia Most esophagitis episodes heal with squamous epithelium The otigin of the columnar cells is not clear: Esophagus, Cardia, Bone marrow
60 Good epidemiologic evidence to link GERD and increased EAC prevalence Little evidence to link GERD and BE causally
61 Take home message Barrett esophagus is an endoscopic AND histopathologic Dx The risk of Ca is extremely low in nondysplastic BE tissue Prevalence of BE is much lower in Iran than that reported in the west Although surveillance for dysplasia in BE is recommended by most international societies, its efficacy is in serious question The problems with sampling and histopathologic Dx

62 The patient with Barrett Esophagus will get relieved when his/her endoscopist dies!

63

64
65 Natural Hx of BE Longitudinal studies: most cases of BE do not progress beyond nondysplastic intestinal metaplasia or transient lowgrade dysplasia Sharma P, et al. Clin Gastroenterol Hepatol 2006;4: Yousef F et al. Am J Epidemiol Aug 1;168(3): In cases of progression to HGD: A meta-analysis, 4 studies, 236 pts, 1234 pt/yr FU, 69 adenoca 6 per 100 patient-years during the first few years of follow-up Rastogi A et al. Gastrointest Endosc 2008;67:394-8.
66 How is natural hx affected by ablative Rx? SR & Meta-analysis, Wani S, et al. AJG 2009 Feb;104(2): Patients: nondysplastic BE (NDBE), low-grade dysplasia (LGD), or high-grade dysplasia (HGD) and follow-up of at least 6 m The rate of cancer in patients undergoing ablation and from the natural history data was calculated using weighted-average incidence rates (WIR) RESULTS: 53 articles met the inclusion criteria for the natural history data. Cancer incidence of: 5.98/1,000 patient-years (95% CI ) in NDBE; 16.98/1,000 patient-years (95% CI ) in LGD; 65.8/1,000 patient-years (95% CI ) in HGD patients 65 articles met the inclusion criteria for BE pts undergoing ablation (1,457 patients, NDBE; 239 patients, LGD; and 611 patients, HGD). The WIR for cancer was: NDBE: 1.63/1,000 pt-yr (95% CI ) LGD: 1.58/1,000 pt-yr (95% CI ) HGD: 16.76/1,000 pt-yr (95% CI ) CONCLUSIONS: Compared to historical reports of the natural history of BE, ablation may be associated with a reduction in cancer incidence, although such a comparison is limited by likely heterogeneity between treatment and natural history studies. The greatest benefit of ablation was observed in BE patients with HGD.
67 Shaheen et al NEJM 2009: ablation session in 84 pts (3.5/pt) 1 UGIB Endoscopic Rx 5 strictures Endoscopic dilatation (2.6/pt) Over 12 m, 13,573 bx (9517 ablations, 4056 controls) 1260 bx from LGD pts+ablation: 97.5% free of SIM at 12m vs. 56.9% in controls 1464 bx HGD pts+ablation: 98.5% free of SIM at 12m vs 58.6% in the controls

68 Shaheen et al NEJM % 81% 22.7% 19.0% Our findings should be viewed with caution: Cancers occurred in only 5 patients (1/84 with ablation & 4/43 in controls So the shift of a single incident cancer would have resulted in a loss of statistical significance.
69 What other options? Surgery: Curative mean mortality: 2.7% (up to 14%) 28% morbidity (anastomotic leaks, strictures, wound dehiscence, recurrent aspiration pneumonias) may require a second operation One of the longest F/U (BMJ 2000): 143 BE patients Followed for a mean of 4.4 years (up to 10 y) Regular surveillance Only 1 adenoca found He died of surgery not of the Ca
70 EMR, ESD Laborious Complications are real Recurrence happens even beneath a now normal looking mucosa
71 Cost-Utility Analysis R Garside et al Health Technology Assessment 2006; Vol. 10: No. 8 Cost utility model Markov model Base case scenario: endoscopic surveillance of BE q3y LGD q1y HGD q3m Does more harm than good when compared with no surveillance Surveillance produces: fewer quality-adjusted life-years (QALYs) for higher cost than no surveillance, The cost per cancer identified: ~ 45,000 in the surveillance arm with no apparent survival advantage owing to high recurrence rates and increased mortality due to more surgical interventions (i.e. oesophagectomies) in this arm.
72 Cost-Utility Analysis R Garside et al Health Technology Assessment 2006; Vol. 10: No. 8 The input parameters to which the model is most sensitive: the rate of recurrence of adenocarcinoma after oesophagectomy in the surveillance compared with the no surveillance arm the rate at which adenocarcinoma becomes symptomatic once it has developed the utility value (quality of life) attached to the health states for Barrett s oesophagus. One-way sensitivity analyses (for 3-yearly surveillance to become costeffective at usual levels of willingness to pay 30,000 per QALY): rate of recurrence of AC post-op reduces to 4.5% in the surveillance arm (from the base case of 9.3%) rate of recurrence of AC post-op reduces to 7% in the non-surveillance arm (from the base case of 26%) progression from undetected to symptomatic AC increases to at least 23% per year (from the base case of 14.3%) utility values for Barrett s oesophagus health states fall to 0.63 (from the base case of 0.81)
 for 1 cm circumferential length Sensitivity: 90.0% (55.5-99.7%) Specificity: 93.5% (90.9-95.")
73 New techniques for detection Compared with gastroscopy: Sensitivity: 73.3% (95%CI %) Specificity: 93.8% (95%CI %) for 1 cm circumferential length Sensitivity: 90.0% ( %) Specificity: 93.5% ( %) For segments 2 cm Kadri SR et al, BMJ 2010;341:c4372 doi: /bmj.c4372
74 Take Home Message Barrett s Esophagus is defined endoscopically AND histologically Columnar lined esophagus can be reported but NOT Barrett s esophagus Prague classification for CLE reporting Most patients with BE never die from it Current guidelines are far from perfect Dysplasia Dx is not consistent between pathologists Current Rx modalities are far from perfect (serious mortality/morbidity) Cost-utility analyses do not suggest any benefit (even may be harmful Only high risk patients (male, white, older, fat) may benefit from current surveillance/interventions
75

76 The BE patient is relieved only when his/her Endoscopist is dead!
Barrett s Esophagus. Abdul Sami Khan, M.D. Gastroenterologist Aurora Healthcare Burlington, Elkhorn, Lake Geneva, WI
 Barrett s Esophagus Abdul Sami Khan, M.D. Gastroenterologist Aurora Healthcare Burlington, Elkhorn, Lake Geneva, WI A 58 year-old, obese white man has had heartburn for more than 20 years. He read a magazine
Barrett s Esophagus Abdul Sami Khan, M.D. Gastroenterologist Aurora Healthcare Burlington, Elkhorn, Lake Geneva, WI A 58 year-old, obese white man has had heartburn for more than 20 years. He read a magazine
Barrett s Esophagus: Old Dog, New Tricks
 Barrett s Esophagus: Old Dog, New Tricks Stuart Jon Spechler, M.D. Chief, Division of Gastroenterology, VA North Texas Healthcare System; Co-Director, Esophageal Diseases Center, Professor of Medicine,
Barrett s Esophagus: Old Dog, New Tricks Stuart Jon Spechler, M.D. Chief, Division of Gastroenterology, VA North Texas Healthcare System; Co-Director, Esophageal Diseases Center, Professor of Medicine,
AGA SECTION. Gastroenterology 2016;150:
 Gastroenterology 2016;150:1026 1030 April 2016 AGA Section 1027 Procedural intervention (3) Upper endoscopy indications 3 6 Non-response of symptoms to a 4 8 week empiric trial of twice-daily PPI Troublesome
Gastroenterology 2016;150:1026 1030 April 2016 AGA Section 1027 Procedural intervention (3) Upper endoscopy indications 3 6 Non-response of symptoms to a 4 8 week empiric trial of twice-daily PPI Troublesome
History. Prevalence at Endoscopy. Prevalence and Reflux Sx. Prevalence at Endoscopy. Barrett s Esophagus: Controversy and Management
 Barrett s Esophagus: Controversy and Management History Norman Barrett (1950) Chronic Peptic Ulcer of the Oesophagus and Oesophagitis Allison and Johnstone (1953) The Oesophagus Lined with Gastric Mucous
Barrett s Esophagus: Controversy and Management History Norman Barrett (1950) Chronic Peptic Ulcer of the Oesophagus and Oesophagitis Allison and Johnstone (1953) The Oesophagus Lined with Gastric Mucous
Management of Barrett s Esophagus. Case Presentation
 Management of Barrett s Esophagus Lauren B. Gerson MD, MSc Associate Clinical Professor, UCSF Director of Clinical Research Gastroenterology Fellowship Program California Pacific Medical Center San Francisco,
Management of Barrett s Esophagus Lauren B. Gerson MD, MSc Associate Clinical Professor, UCSF Director of Clinical Research Gastroenterology Fellowship Program California Pacific Medical Center San Francisco,
Joel A. Ricci, MD SUNY Downstate Medical Center Department of Surgery
 Joel A. Ricci, MD SUNY Downstate Medical Center Department of Surgery Norman Barrett (1950) described the esophagus as: that part of the foregut, distal to the cricopharyngeal sphincter, which is lined
Joel A. Ricci, MD SUNY Downstate Medical Center Department of Surgery Norman Barrett (1950) described the esophagus as: that part of the foregut, distal to the cricopharyngeal sphincter, which is lined
Definition of GERD American College of Gastroenterology
 Definition of GERD American College of Gastroenterology GERD is defined as chronic symptoms or mucosal damage produced by the abnormal reflux of gastric contents into the esophagus DeVault et al. Am J
Definition of GERD American College of Gastroenterology GERD is defined as chronic symptoms or mucosal damage produced by the abnormal reflux of gastric contents into the esophagus DeVault et al. Am J
THE COLUMNAR-LINED ESOPHAGUS (BARRETT ACQUIRED CONDITION?
 GASTROENTEROLOGY Copyright 1966 by The Williams & Wilkins Co. Vol. 50, No.5 Printed in U.S.A. THE COLUMNAR-LINED ESOPHAGUS (BARRETT ACQUIRED CONDITION? S Y N D R O M E ) ~ A N SANFORD M. MOSSBERG, M.D.
GASTROENTEROLOGY Copyright 1966 by The Williams & Wilkins Co. Vol. 50, No.5 Printed in U.S.A. THE COLUMNAR-LINED ESOPHAGUS (BARRETT ACQUIRED CONDITION? S Y N D R O M E ) ~ A N SANFORD M. MOSSBERG, M.D.
New Developments in the Endoscopic Diagnosis and Management of Barrett s Esophagus
 New Developments in the Endoscopic Diagnosis and Management of Barrett s Esophagus Prateek Sharma, MD Key Clinical Management Points: Endoscopic recognition of a columnar lined distal esophagus is crucial
New Developments in the Endoscopic Diagnosis and Management of Barrett s Esophagus Prateek Sharma, MD Key Clinical Management Points: Endoscopic recognition of a columnar lined distal esophagus is crucial
Gregory G. Ginsberg, M.D.
 Radiofrequency Ablation for Barrett s Esophagus with HGD Gregory G. Ginsberg, M.D. Professor of Medicine University of Pennsylvania School of Medicine Abramson Cancer Center Gastroenterology Division Executive
Radiofrequency Ablation for Barrett s Esophagus with HGD Gregory G. Ginsberg, M.D. Professor of Medicine University of Pennsylvania School of Medicine Abramson Cancer Center Gastroenterology Division Executive
Present Day Management of Barrett s Esophagus
 Slide 1 Present Day Management of Barrett s Esophagus Kinnari R. Kher, M.D. Slide 2 Goals Risk factors for development of Barrett s esophagus Risks for progression to Esophageal Adenocarcinoma Current
Slide 1 Present Day Management of Barrett s Esophagus Kinnari R. Kher, M.D. Slide 2 Goals Risk factors for development of Barrett s esophagus Risks for progression to Esophageal Adenocarcinoma Current
Barrett s Esophagus: What to Do for No Dysplasia, LGD, and HGD?
 Barrett s Esophagus: What to Do for No Dysplasia, LGD, and HGD? Nicholas Shaheen, MD, MPH Center for Esophageal Diseases and Swallowing University of North Carolina 1 Outline What are the risks of progression
Barrett s Esophagus: What to Do for No Dysplasia, LGD, and HGD? Nicholas Shaheen, MD, MPH Center for Esophageal Diseases and Swallowing University of North Carolina 1 Outline What are the risks of progression
Everything Esophagus: Barrett s Esophagus. Nicholas Shaheen, MD, MPH Center for Esophageal Diseases and Swallowing University of North Carolina
 Everything Esophagus: Barrett s Esophagus Nicholas Shaheen, MD, MPH Center for Esophageal Diseases and Swallowing University of North Carolina The Most Important Thing Stayed the Same Adenocarcinoma A
Everything Esophagus: Barrett s Esophagus Nicholas Shaheen, MD, MPH Center for Esophageal Diseases and Swallowing University of North Carolina The Most Important Thing Stayed the Same Adenocarcinoma A
Barrett s esophagus. Barrett s neoplasia treatment trends
 Options for endoscopic treatment of Barrett s esophagus Patrick S. Yachimski, MD MPH Director of Pancreatobiliary Endoscopy Assistant Professor of Medicine Division of Gastroenterology, Hepatology & Nutrition
Options for endoscopic treatment of Barrett s esophagus Patrick S. Yachimski, MD MPH Director of Pancreatobiliary Endoscopy Assistant Professor of Medicine Division of Gastroenterology, Hepatology & Nutrition
Hiatal Hernias and Barrett s esophagus. Dr Sajida Ahad Mercy General Surgery
 Hiatal Hernias and Barrett s esophagus Dr Sajida Ahad Mercy General Surgery Objectives Identify the use of different diagnostic modalities for hiatal hernias List the different types of hiatal hernias
Hiatal Hernias and Barrett s esophagus Dr Sajida Ahad Mercy General Surgery Objectives Identify the use of different diagnostic modalities for hiatal hernias List the different types of hiatal hernias
Management of Barrett s: From Imaging to Resection
 Management of Barrett s: From Imaging to Resection Michael Wallace, MD, MPH, FACG Professor of Medicine Mayo Clinic Florida Goals of Endoscopic Evaluation in Barrett s Detect Barrett s and dysplasia Reduce/eliminate
Management of Barrett s: From Imaging to Resection Michael Wallace, MD, MPH, FACG Professor of Medicine Mayo Clinic Florida Goals of Endoscopic Evaluation in Barrett s Detect Barrett s and dysplasia Reduce/eliminate
Barrett's Esophagus: Sorting Out the Controversy
 Barrett's Esophagus: Sorting Out the Controversy Learning Objectives 1. Identify the challenges in screening for Barrett s esophagus 2. Demonstrate comprehension of the risk of progression of Barrett s
Barrett's Esophagus: Sorting Out the Controversy Learning Objectives 1. Identify the challenges in screening for Barrett s esophagus 2. Demonstrate comprehension of the risk of progression of Barrett s
Barrett s Esophagus: Ablate Everyone?
 Nicholas J. Shaheen, MD, MPH, FACG Barrett s Esophagus: Ablate Everyone? Nicholas J. Shaheen, MD, MPH, FACG Center for Esophageal Diseases and Swallowing University of North Carolina Greetings from UNC,
Nicholas J. Shaheen, MD, MPH, FACG Barrett s Esophagus: Ablate Everyone? Nicholas J. Shaheen, MD, MPH, FACG Center for Esophageal Diseases and Swallowing University of North Carolina Greetings from UNC,
Changes to the diagnosis and management of Barrett s Oesophagus
 Changes to the diagnosis and management of Barrett s Oesophagus A review of the new BSG and NICE guidelines and best practice Anjan Dhar DM, MD, FRCPE, AGAF, MBBS (Hons.), Cert. Med. Ed Senior Lecturer
Changes to the diagnosis and management of Barrett s Oesophagus A review of the new BSG and NICE guidelines and best practice Anjan Dhar DM, MD, FRCPE, AGAF, MBBS (Hons.), Cert. Med. Ed Senior Lecturer
MANAGEMENT OF BARRETT S RELATED NEOPLASIA IN 2018
 MANAGEMENT OF BARRETT S RELATED NEOPLASIA IN 2018 Sachin Wani Medical Director Esophageal and Gastric Center Division of Gastroenterology and Hepatology University of Colorado Anschutz Medical Campus DISCLOSURES
MANAGEMENT OF BARRETT S RELATED NEOPLASIA IN 2018 Sachin Wani Medical Director Esophageal and Gastric Center Division of Gastroenterology and Hepatology University of Colorado Anschutz Medical Campus DISCLOSURES
ACG Clinical Guideline: Diagnosis and Management of Barrett s Esophagus
 ACG Clinical Guideline: Diagnosis and Management of Barrett s Esophagus Nicholas J. Shaheen, MD, MPH, FACG 1, Gary W. Falk, MD, MS, FACG 2, Prasad G. Iyer, MD, MSc, FACG 3 and Lauren Gerson, MD, MSc, FACG
ACG Clinical Guideline: Diagnosis and Management of Barrett s Esophagus Nicholas J. Shaheen, MD, MPH, FACG 1, Gary W. Falk, MD, MS, FACG 2, Prasad G. Iyer, MD, MSc, FACG 3 and Lauren Gerson, MD, MSc, FACG
Faculty Disclosure. Objectives. State of the Art #3: Referrals for Gastroscopy (focus on common esophagus problems) 24/11/2014
 24/11/2014") State of the Art #3: Referrals for Gastroscopy (focus on common esophagus problems) Dr. Amy Morse November 2014 Faculty: Amy Morse Faculty Disclosure Relationships with commercial interests: Grants/Research
State of the Art #3: Referrals for Gastroscopy (focus on common esophagus problems) Dr. Amy Morse November 2014 Faculty: Amy Morse Faculty Disclosure Relationships with commercial interests: Grants/Research
Oesophagus and Stomach update dysplasia and early cancer
 Oesophagus and Stomach update dysplasia and early cancer Dr Tim Bracey STR teaching 13/4/16 Please check pathkids.com for previous talks One of the biggest units in the country (100 major resections per
Oesophagus and Stomach update dysplasia and early cancer Dr Tim Bracey STR teaching 13/4/16 Please check pathkids.com for previous talks One of the biggest units in the country (100 major resections per
Learning Objectives:
 Crescent City GI Update 2018 Ochsner Clinic, NOLA Optimizing Endoscopic Evaluation of Barrett s Esophagus What Should I Do in My Practice? Gregory G. Ginsberg, M.D. Professor of Medicine University of
Crescent City GI Update 2018 Ochsner Clinic, NOLA Optimizing Endoscopic Evaluation of Barrett s Esophagus What Should I Do in My Practice? Gregory G. Ginsberg, M.D. Professor of Medicine University of
Barrett s Esophagus: State of the Art. Food Getting Stuck
 Barrett s Esophagus: State of the Art Nicholas J. Shaheen, MD, MPH Center for Esophageal Diseases and Swallowing University of North Carolina SOM Food Getting Stuck 73-year-old retired Wilmington police
Barrett s Esophagus: State of the Art Nicholas J. Shaheen, MD, MPH Center for Esophageal Diseases and Swallowing University of North Carolina SOM Food Getting Stuck 73-year-old retired Wilmington police
Ablation for Barrett s Esophagus: Burn or Freeze
 Ablation for Barrett s Esophagus: Burn or Freeze John R. Saltzman MD Director of Endoscopy Brigham and Women s Hospital Professor of Medicine Harvard Medical School Disclosures No relevant disclosures
Ablation for Barrett s Esophagus: Burn or Freeze John R. Saltzman MD Director of Endoscopy Brigham and Women s Hospital Professor of Medicine Harvard Medical School Disclosures No relevant disclosures
What s New in the Management of Esophageal Disease
 What s New in the Management of Esophageal Disease Philip O. Katz, MD Chairman, Division of Gastroenterology Einstein Medical Center Philadelphia Clinical Professor of Medicine Jefferson Medical College
What s New in the Management of Esophageal Disease Philip O. Katz, MD Chairman, Division of Gastroenterology Einstein Medical Center Philadelphia Clinical Professor of Medicine Jefferson Medical College
Barrett s Oesophagus Information Leaflet THE DIGESTIVE SYSTEM. gutscharity.org.
 THE DIGESTIVE SYSTEM http://healthfavo.com/digestive-system-for-kids.html This factsheet is about Barrett s Oesophagus Barrett s Oesophagus is the term used for a pre-cancerous condition where the normal
THE DIGESTIVE SYSTEM http://healthfavo.com/digestive-system-for-kids.html This factsheet is about Barrett s Oesophagus Barrett s Oesophagus is the term used for a pre-cancerous condition where the normal
Disclosures. Gastroesophageal Reflux Disease. Gastroesophageal Reflux Disease
 Kunal Jajoo, MD Brigham and Women s Hospital July 2012 Disclosures Spouse is a physician employed by Boston Scientific Corporation The content of this lecture equitably discusses products of multiple companies
Kunal Jajoo, MD Brigham and Women s Hospital July 2012 Disclosures Spouse is a physician employed by Boston Scientific Corporation The content of this lecture equitably discusses products of multiple companies
Speaker disclosure. Objectives. GERD: Who and When to Treat 7/21/2015
 GERD: Who and When to Treat Eugenio J Hernandez, MD Gastrohealth, PL Assistant Professor of Clinical Medicine, FIU Herbert Wertheim School of Medicine Speaker disclosure I do not have any relevant commercial
GERD: Who and When to Treat Eugenio J Hernandez, MD Gastrohealth, PL Assistant Professor of Clinical Medicine, FIU Herbert Wertheim School of Medicine Speaker disclosure I do not have any relevant commercial
Endoscopic Management of Barrett s Esophagus
 Endoscopic Management of Barrett s Esophagus Sammy Ho, MD Director of Pancreaticobiliary Services and Endoscopic Ultrasound Montefiore Medical Center Barrett s Esophagus Consequence of chronic GERD Mean
Endoscopic Management of Barrett s Esophagus Sammy Ho, MD Director of Pancreaticobiliary Services and Endoscopic Ultrasound Montefiore Medical Center Barrett s Esophagus Consequence of chronic GERD Mean
American Journal of Gastroenterology. Volumetric Laser Endomicroscopy Detects Subsquamous Barrett s Adenocarcinoma
 Volumetric Laser Endomicroscopy Detects Subsquamous Barrett s Adenocarcinoma Journal: Manuscript ID: AJG-13-1412.R1 Manuscript Type: Letter to the Editor Keywords: Barrett-s esophagus, Esophagus, Endoscopy
Volumetric Laser Endomicroscopy Detects Subsquamous Barrett s Adenocarcinoma Journal: Manuscript ID: AJG-13-1412.R1 Manuscript Type: Letter to the Editor Keywords: Barrett-s esophagus, Esophagus, Endoscopy
The Pathologist s Role in the Diagnosis and Management of Neoplasia in Barrett s Oesophagus Cian Muldoon, St. James s Hospital, Dublin
 The Pathologist s Role in the Diagnosis and Management of Neoplasia in Barrett s Oesophagus Cian Muldoon, St. James s Hospital, Dublin 24.06.15 Norman Barrett Smiles [A brief digression - Chair becoming
The Pathologist s Role in the Diagnosis and Management of Neoplasia in Barrett s Oesophagus Cian Muldoon, St. James s Hospital, Dublin 24.06.15 Norman Barrett Smiles [A brief digression - Chair becoming
Barrett s Esophagus: Are We Making any Progress?
 3/22/217 arrett s Esophagus: re We Making any Progress? Stuart Jon Spechler, M.D. hief, Division of Gastroenterology, V North Texas Healthcare System; o-director, Esophageal Diseases enter, Professor of
3/22/217 arrett s Esophagus: re We Making any Progress? Stuart Jon Spechler, M.D. hief, Division of Gastroenterology, V North Texas Healthcare System; o-director, Esophageal Diseases enter, Professor of
Is Radiofrequency Ablation Effective In Treating Barrett s Esophagus Patients with High-Grade Dysplasia?
 Philadelphia College of Osteopathic Medicine DigitalCommons@PCOM PCOM Physician Assistant Studies Student Scholarship Student Dissertations, Theses and Papers 12-2016 Is Radiofrequency Ablation Effective
Philadelphia College of Osteopathic Medicine DigitalCommons@PCOM PCOM Physician Assistant Studies Student Scholarship Student Dissertations, Theses and Papers 12-2016 Is Radiofrequency Ablation Effective
Histopathology of Endoscopic Resection Specimens from Barrett's Esophagus
 Histopathology of Endoscopic Resection Specimens from Barrett's Esophagus Br J Surg 38 oct. 1950 Definition of Barrett's esophagus A change in the esophageal epithelium of any length that can be recognized
Histopathology of Endoscopic Resection Specimens from Barrett's Esophagus Br J Surg 38 oct. 1950 Definition of Barrett's esophagus A change in the esophageal epithelium of any length that can be recognized
ESOPHAGEAL CANCER AND GERD. Prof Salman Guraya FRCS, Masters MedEd
 ESOPHAGEAL CANCER AND GERD Prof Salman Guraya FRCS, Masters MedEd Learning objectives Esophagus anatomy and physiology Esophageal cancer Causes, presentations of esophageal cancer Diagnosis and management
ESOPHAGEAL CANCER AND GERD Prof Salman Guraya FRCS, Masters MedEd Learning objectives Esophagus anatomy and physiology Esophageal cancer Causes, presentations of esophageal cancer Diagnosis and management
Gastroesophageal Reflux Disease, Paraesophageal Hernias &
 530.81 553.3 & 530.00 43289, 43659 1043432842, MD Assistant Clinical Professor of Surgery, UH JABSOM Associate General Surgery Program Director Director of Minimally Invasive & Bariatric Surgery Programs
530.81 553.3 & 530.00 43289, 43659 1043432842, MD Assistant Clinical Professor of Surgery, UH JABSOM Associate General Surgery Program Director Director of Minimally Invasive & Bariatric Surgery Programs
Barrett s Esophagus: Review of Diagnostic Issues and Pre- Neoplastic Lesions
 Barrett s Esophagus: Review of Diagnostic Issues and Pre- Neoplastic Lesions Robert Odze, MD, FRCPC Chief, Gastrointestinal Pathology Associate Professor of Pathology Brigham and Women s Hospital Harvard
Barrett s Esophagus: Review of Diagnostic Issues and Pre- Neoplastic Lesions Robert Odze, MD, FRCPC Chief, Gastrointestinal Pathology Associate Professor of Pathology Brigham and Women s Hospital Harvard
Barrett s Esophagus. Radiofrequency Ablation with the HALO Technology A Reference Book
 Radiofrequency Ablation with the HALO Technology A Reference Book 540 Oakmead Parkway, Sunnyvale, CA 94085 What is Barrett s esophagus? Barrett s esophagus is a change that occurs within the cellular lining
Radiofrequency Ablation with the HALO Technology A Reference Book 540 Oakmead Parkway, Sunnyvale, CA 94085 What is Barrett s esophagus? Barrett s esophagus is a change that occurs within the cellular lining
Disclosures. Heartburn and Barrett s Esophagus. Heartburn and Barrett s Esophagus. GERD is common in the U.S. None
 Heartburn and Barrett s Esophagus None Disclosures Christian Mathy, MD University of California, San Francisco 2015 Heartburn and Barrett s Esophagus Heartburn and GERD GERD therapy Extraesophageal GERD
Heartburn and Barrett s Esophagus None Disclosures Christian Mathy, MD University of California, San Francisco 2015 Heartburn and Barrett s Esophagus Heartburn and GERD GERD therapy Extraesophageal GERD
Sixteen-year follow-up of Barrett s esophagus, endoscopically treated with argon plasma coagulation
 Original Article Sixteen-year of Barrett s esophagus, endoscopically treated with argon plasma coagulation United European Gastroenterology Journal 2014, Vol. 2(5) 367 373! Author(s) 2014 Reprints and
Original Article Sixteen-year of Barrett s esophagus, endoscopically treated with argon plasma coagulation United European Gastroenterology Journal 2014, Vol. 2(5) 367 373! Author(s) 2014 Reprints and
The normal esophagus is lined with squamous epithelium.
 .. ALAN J. CAMERON, M.D. In Barrett's esophagus, the squamous lining of the lower esophagus is replaced by columnar epithelium. Barrett's esophagus is associated with gastroesophageal reflux and an increased
.. ALAN J. CAMERON, M.D. In Barrett's esophagus, the squamous lining of the lower esophagus is replaced by columnar epithelium. Barrett's esophagus is associated with gastroesophageal reflux and an increased
This medical position statement considers a series of
 GASTROENTEROLOGY 2011;140:1084 1091 American Gastroenterological Association Medical Position Statement on the Management of Barrett s Esophagus The Institute Medical Position Panel consisted of the authors
GASTROENTEROLOGY 2011;140:1084 1091 American Gastroenterological Association Medical Position Statement on the Management of Barrett s Esophagus The Institute Medical Position Panel consisted of the authors
In 1998, the American College of Gastroenterology issued ALIMENTARY TRACT
 CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2012;10:1232 1236 ALIMENTARY TRACT Effects of Dropping the Requirement for Goblet Cells From the Diagnosis of Barrett s Esophagus MARIA WESTERHOFF,* LINDSEY HOVAN,
CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2012;10:1232 1236 ALIMENTARY TRACT Effects of Dropping the Requirement for Goblet Cells From the Diagnosis of Barrett s Esophagus MARIA WESTERHOFF,* LINDSEY HOVAN,
Gastrointestinal pathology 2018 lecture 2. Dr Heyam Awad FRCPath
 Gastrointestinal pathology 2018 lecture 2 Dr Heyam Awad FRCPath Eosinophilic esophagitis Incidence of eosinophilic gastritis is increasing. Symptoms: food impaction and dysphagia. Histology: infiltration
Gastrointestinal pathology 2018 lecture 2 Dr Heyam Awad FRCPath Eosinophilic esophagitis Incidence of eosinophilic gastritis is increasing. Symptoms: food impaction and dysphagia. Histology: infiltration
Oesophageal Disorders
 Oesophageal Disorders Anatomy Upper sphincter Oesophageal body Diaphragm Lower sphincter Gastric Cardia Symptoms Of Oesophageal Disorders Dysphagia Odynophagia Heartburn Atypical Chest Pain Regurgitation
Oesophageal Disorders Anatomy Upper sphincter Oesophageal body Diaphragm Lower sphincter Gastric Cardia Symptoms Of Oesophageal Disorders Dysphagia Odynophagia Heartburn Atypical Chest Pain Regurgitation
Gastrooesophageal reflux disease. Jera Jeruc Institute of pathology, Faculty of Medicine, Ljubljana, Slovenia
 Gastrooesophageal reflux disease Jera Jeruc Institute of pathology, Faculty of Medicine, Ljubljana, Slovenia Reflux esophagitis (RE) GERD: a spectrum of clinical conditions and histologic alterations resulting
Gastrooesophageal reflux disease Jera Jeruc Institute of pathology, Faculty of Medicine, Ljubljana, Slovenia Reflux esophagitis (RE) GERD: a spectrum of clinical conditions and histologic alterations resulting
ACG Clinical Guideline: Diagnosis and Management of Barrett s Esophagus
 30 PRACTICE GUIDELINES nature publishing group CME ACG Clinical Guideline: Diagnosis and Management of Barrett s Esophagus Nicholas J. Shaheen, MD, MPH, FACG 1, Gary W. Falk, MD, MS, FACG 2, Prasad G.
30 PRACTICE GUIDELINES nature publishing group CME ACG Clinical Guideline: Diagnosis and Management of Barrett s Esophagus Nicholas J. Shaheen, MD, MPH, FACG 1, Gary W. Falk, MD, MS, FACG 2, Prasad G.
EGD. John M. Wo, M.D. University of Louisville July 3, 2008
 EGD John M. Wo, M.D. University of Louisville July 3, 2008 Different Ways to do an EGD Which scope? Pediatric, regular, jumbo EGD endoscope or pediatric colonoscope Transnasal vs. transoral insertion Sedation
EGD John M. Wo, M.D. University of Louisville July 3, 2008 Different Ways to do an EGD Which scope? Pediatric, regular, jumbo EGD endoscope or pediatric colonoscope Transnasal vs. transoral insertion Sedation
Chapter 2 Complications of Gastroesophageal Reflux Disease
 Chapter 2 Complications of Gastroesophageal Reflux Disease Patrick Yachimski Acute esophageal exposure to gastric and/or duodenal refluxate can result in pyrosis and symptomatic gastroesophageal reflux
Chapter 2 Complications of Gastroesophageal Reflux Disease Patrick Yachimski Acute esophageal exposure to gastric and/or duodenal refluxate can result in pyrosis and symptomatic gastroesophageal reflux
Current Management: Role of Radiofrequency Ablation
 Esophageal Adenocarcinoma And Barrett s Esophagus: Current Management: Role of Radiofrequency Ablation Ketan Kulkarni, MD Regional Gastroenterology Associates of Lancaster INTRODUCTION The prognosis of
Esophageal Adenocarcinoma And Barrett s Esophagus: Current Management: Role of Radiofrequency Ablation Ketan Kulkarni, MD Regional Gastroenterology Associates of Lancaster INTRODUCTION The prognosis of
Case Scenario 1. The patient has now completed his neoadjuvant chemoradiation and has been cleared for surgery.
 Case Scenario 1 July 10, 2010 A 67-year-old male with squamous cell carcinoma of the mid thoracic esophagus presents for surgical resection. The patient has completed preoperative chemoradiation. This
Case Scenario 1 July 10, 2010 A 67-year-old male with squamous cell carcinoma of the mid thoracic esophagus presents for surgical resection. The patient has completed preoperative chemoradiation. This
From reflux to esophageal cancer. Josh Boys, MD TCV 2 nd year indentured servant
 From reflux to esophageal cancer Josh Boys, MD TCV 2 nd year indentured servant The Pathway Esophageal Squamous epithelium+reflux Columnar lined esophagus (CLE) or Cardiac mucosa Intestinal Metaplasia
From reflux to esophageal cancer Josh Boys, MD TCV 2 nd year indentured servant The Pathway Esophageal Squamous epithelium+reflux Columnar lined esophagus (CLE) or Cardiac mucosa Intestinal Metaplasia
Endoscopic Radiofrequency Ablation or Cryoablation for Barrett Esophagus
 Endoscopic Radiofrequency Ablation or Cryoablation for Barrett Esophagus Policy Number: Original Effective Date: MM.02.005 09/01/2010 Line(s) of Business: Current Effective Date: PPO; HMO; QUEST Integration
Endoscopic Radiofrequency Ablation or Cryoablation for Barrett Esophagus Policy Number: Original Effective Date: MM.02.005 09/01/2010 Line(s) of Business: Current Effective Date: PPO; HMO; QUEST Integration
Barrett Esophagus - RadioFrequency Ablation (BE-RFA) - Project manual + FAQ
 - Project manual + FAQ") Barrett Esophagus - RadioFrequency Ablation (BE-RFA) - Project manual + FAQ Table of contents 1 General project information...3 1.1 Inclusion criteria...3 1.2 Registration time points...3 1.3 Project variable
Barrett Esophagus - RadioFrequency Ablation (BE-RFA) - Project manual + FAQ Table of contents 1 General project information...3 1.1 Inclusion criteria...3 1.2 Registration time points...3 1.3 Project variable
Screening of Barrett: Is it cost-effective? Is there a high-risk population? T Ponchon Ed. Herriot Hospital Lyon, France
 Screening of Barrett: Is it cost-effective? Is there a high-risk population? T Ponchon Ed. Herriot Hospital Lyon, France Barrett s esophagus (BE) is an acquired condition in which the normal squamous epithelium
Screening of Barrett: Is it cost-effective? Is there a high-risk population? T Ponchon Ed. Herriot Hospital Lyon, France Barrett s esophagus (BE) is an acquired condition in which the normal squamous epithelium
Medicare Advantage Medical Policy
 Medicare Advantage Medical Policy Current Policy Effective Date: 1/1/18 Title: Endoscopic Radiofrequency Ablation or Cryoablation for Barrett Esophagus Description/Background Barrett Esophagus and the
Medicare Advantage Medical Policy Current Policy Effective Date: 1/1/18 Title: Endoscopic Radiofrequency Ablation or Cryoablation for Barrett Esophagus Description/Background Barrett Esophagus and the
RFA and Cyrotherapy for Esophageal Disease
 RFA and Cyrotherapy for Esophageal Disease Daniel L. Miller MD Chief, General Thoracic Surgery WellStar Healthcare System/ Mayo Clinic Care Network Clinical Professor of Surgery Medical College of Georgia/
RFA and Cyrotherapy for Esophageal Disease Daniel L. Miller MD Chief, General Thoracic Surgery WellStar Healthcare System/ Mayo Clinic Care Network Clinical Professor of Surgery Medical College of Georgia/
Accepted Manuscript. CGH Editorial: Sound the Alarm for Barrett s Screening! Tarek Sawas, M.D., M.P.H., David A. Katzka, M.D
 Accepted Manuscript CGH Editorial: Sound the Alarm for Barrett s Screening! Tarek Sawas, M.D., M.P.H., David A. Katzka, M.D PII: S1542-3565(18)31093-0 DOI: 10.1016/j.cgh.2018.10.010 Reference: YJCGH 56132
Accepted Manuscript CGH Editorial: Sound the Alarm for Barrett s Screening! Tarek Sawas, M.D., M.P.H., David A. Katzka, M.D PII: S1542-3565(18)31093-0 DOI: 10.1016/j.cgh.2018.10.010 Reference: YJCGH 56132
Endoscopic Radiofrequency Ablation or Cryoablation for Barrett s Esophagus
 Endoscopic Radiofrequency Ablation or Cryoablation for Barrett s Esophagus Policy Number: 2.01.80 Last Review: 6/2018 Origination: 6/2012 Next Review: 6/2019 Policy Blue Cross and Blue Shield of Kansas
Endoscopic Radiofrequency Ablation or Cryoablation for Barrett s Esophagus Policy Number: 2.01.80 Last Review: 6/2018 Origination: 6/2012 Next Review: 6/2019 Policy Blue Cross and Blue Shield of Kansas
Radiofrequency Ablation: Stepwise circumferential and focal RFA of Barrett s s esophagus using the HALO System
 Radiofrequency Ablation: Stepwise circumferential and focal RFA of Barrett s s esophagus using the HALO System Used abbreviations BE: Barrett s esophagus EC: Early cancer ER: Endoscopic resection HGD:
Radiofrequency Ablation: Stepwise circumferential and focal RFA of Barrett s s esophagus using the HALO System Used abbreviations BE: Barrett s esophagus EC: Early cancer ER: Endoscopic resection HGD:
Relative risk of dysplasia for patients with intestinal metaplasia in the distal oesophagus and in the gastric cardia
 Gut 2000;46:9 13 9 PAPERS Division of Gastroenterology, University of Kansas, VA Medical Center, Kansas City, Missouri, USA P Sharma A P Weston Department of Pathology, VA Medical Center, Kansas M Topalovski
Gut 2000;46:9 13 9 PAPERS Division of Gastroenterology, University of Kansas, VA Medical Center, Kansas City, Missouri, USA P Sharma A P Weston Department of Pathology, VA Medical Center, Kansas M Topalovski
Is intestinal metaplasia a necessary precursor lesion for adenocarcinomas of the distal esophagus, gastroesophageal junction and gastric cardia?
 Diseases of the Esophagus (2007) 20, 36 41 DOI: 10.1111/j.1442-2050.2007.00638.x Blackwell Publishing Asia Original article Is intestinal metaplasia a necessary precursor lesion for adenocarcinomas of
Diseases of the Esophagus (2007) 20, 36 41 DOI: 10.1111/j.1442-2050.2007.00638.x Blackwell Publishing Asia Original article Is intestinal metaplasia a necessary precursor lesion for adenocarcinomas of
Evaluating Treatments of Barrett s Esophagus That Shows High-Grade Dysplasia
 ...PRESENTATIONS... Evaluating Treatments of Barrett s Esophagus That Shows High-Grade Dysplasia Based on a presentation by Bergein F. Overholt, MD Presentation Summary Thermal ablation and surgery are
...PRESENTATIONS... Evaluating Treatments of Barrett s Esophagus That Shows High-Grade Dysplasia Based on a presentation by Bergein F. Overholt, MD Presentation Summary Thermal ablation and surgery are
Barrett esophagus. Bible class Inselspital
 Barrett esophagus Bible class Inselspital 2015.08.10 Guidelines Definition? BSG: ACG: Definition? BSG: ACG: What are the arguments for and against IM as prerequisite for the Dg? What are the arguments
Barrett esophagus Bible class Inselspital 2015.08.10 Guidelines Definition? BSG: ACG: Definition? BSG: ACG: What are the arguments for and against IM as prerequisite for the Dg? What are the arguments
Chapter 14: Training in Radiology. DDSEP Chapter 1: Question 12
 DDSEP Chapter 1: Question 12 A 52-year-old white male presents for evaluation of sudden onset of abdominal pain and shoulder pain. His past medical history is notable for a history of coronary artery disease,
DDSEP Chapter 1: Question 12 A 52-year-old white male presents for evaluation of sudden onset of abdominal pain and shoulder pain. His past medical history is notable for a history of coronary artery disease,
CLINICAL GUIDELINE FOR THE MANAGEMENT OF BARRETT S OESOPHAGUS Summary.
 CLINICAL GUIDELINE FOR THE MANAGEMENT OF BARRETT S OESOPHAGUS Summary. Page 1 of 12 Recurrent LGD at any point- discuss at MDT And consider RFA Patients with LGD should have a repeat endoscopy in 6 months.
CLINICAL GUIDELINE FOR THE MANAGEMENT OF BARRETT S OESOPHAGUS Summary. Page 1 of 12 Recurrent LGD at any point- discuss at MDT And consider RFA Patients with LGD should have a repeat endoscopy in 6 months.
Barrett s Esophagus. lining of the lower esophagus that bears his name (i.e., Barrett's esophagus). We now
. We now") Shamika Johnson Anatomy & Physiology 206 April 20, 2010 Barrett s Esophagus What is Barrett s Esophagus? Norman Barrett was a pathologist. In 1950, he described an abnormality in the lining of the lower
Shamika Johnson Anatomy & Physiology 206 April 20, 2010 Barrett s Esophagus What is Barrett s Esophagus? Norman Barrett was a pathologist. In 1950, he described an abnormality in the lining of the lower
In the Name of God. Refractory GERD
 In the Name of God Refractory GERD S Nasseri-Moghaddam MD, MPH, AGAF Associate Professor of Medicine Digestive Disease Research Institute Shariati Hospital, TUMS sianasseri@yahoo.com IAGH meeting, Ordibehesht
In the Name of God Refractory GERD S Nasseri-Moghaddam MD, MPH, AGAF Associate Professor of Medicine Digestive Disease Research Institute Shariati Hospital, TUMS sianasseri@yahoo.com IAGH meeting, Ordibehesht
Cryospray ablation using pressurized CO 2 for ablation of Barrett s esophagus with early neoplasia: early termination of a prospective series
 E17 Cryospray ablation using pressurized CO 2 for ablation of Barrett s esophagus with early neoplasia: early termination of a prospective series Authors Romy E. Verbeek 1, Frank P. Vleggaar 1, Fiebo J.
E17 Cryospray ablation using pressurized CO 2 for ablation of Barrett s esophagus with early neoplasia: early termination of a prospective series Authors Romy E. Verbeek 1, Frank P. Vleggaar 1, Fiebo J.
Citation for published version (APA): Phoa, K. Y. N. (2014). Endoscopic management of Barrett s esophagus with dysplasia
: Phoa, K. Y. N. (2014). Endoscopic management of Barrett s esophagus with dysplasia") UvA-DARE (Digital Academic Repository) Endoscopic management of Barrett s esophagus with dysplasia Phoa, Nadine Link to publication Citation for published version (APA): Phoa, K. Y. N. (2014). Endoscopic
UvA-DARE (Digital Academic Repository) Endoscopic management of Barrett s esophagus with dysplasia Phoa, Nadine Link to publication Citation for published version (APA): Phoa, K. Y. N. (2014). Endoscopic
Esophageal submucosal mass icd 10
 Esophageal submucosal mass icd 10 Search 6-6-2011 ICD-10; Risk Adjustment / HCC; Evaluation & Management (E/M). I'm hoping someone can help me with this DX, "soft tissue mass in. Upper gastrointestinal
Esophageal submucosal mass icd 10 Search 6-6-2011 ICD-10; Risk Adjustment / HCC; Evaluation & Management (E/M). I'm hoping someone can help me with this DX, "soft tissue mass in. Upper gastrointestinal
Gastric Polyps. Bible class
 Gastric Polyps Bible class 29.08.2018 Starting my training in gastroenterology, some decades ago, my first chief always told me that colonoscopy may seem technically more challenging but gastroscopy has
Gastric Polyps Bible class 29.08.2018 Starting my training in gastroenterology, some decades ago, my first chief always told me that colonoscopy may seem technically more challenging but gastroscopy has
Henry Moon was one of the giants in academic pathology during my early years.
 Henry Moon was one of the giants in academic pathology during my early years. Controversial stuff that occurs slightly above, within or slightly below the gastroesophageal junction, including Barrett s
Henry Moon was one of the giants in academic pathology during my early years. Controversial stuff that occurs slightly above, within or slightly below the gastroesophageal junction, including Barrett s
National Oesophago-Gastric Cancer Audit New Patient Registration sheet Patients with Oesophageal High Grade Glandular Dysplasia
 National Oesophago-Gastric Cancer Audit New Patient Registration sheet Patients with Oesophageal High Grade Glandular Dysplasia Patient Details Surname: NHS number: Forename: Postcode: Sex: Male Female
National Oesophago-Gastric Cancer Audit New Patient Registration sheet Patients with Oesophageal High Grade Glandular Dysplasia Patient Details Surname: NHS number: Forename: Postcode: Sex: Male Female
Treat Barrett s, Remove the Risk. HALO System
 Treat Barrett s, Remove the Risk HALO System The HALO 360 System Advanced Ablation Technology for Barrett s Esophagus The HALO 360 System is designed to remove the Barrett s epithelium in a short, well-tolerated
Treat Barrett s, Remove the Risk HALO System The HALO 360 System Advanced Ablation Technology for Barrett s Esophagus The HALO 360 System is designed to remove the Barrett s epithelium in a short, well-tolerated
DISCLOSURES. This program meets the requirements for GI specific Category 1 contact hours. M
 DISCLOSURES Educational Dimensions is accredited as a provider of continuing nursing education by the American Nurses Credentialing Center s Commission on Accreditation. Successful completion: Participants
DISCLOSURES Educational Dimensions is accredited as a provider of continuing nursing education by the American Nurses Credentialing Center s Commission on Accreditation. Successful completion: Participants
Endoscopic Radiofrequency Ablation or Cryoablation for Barrett`s Esophagus. Original Policy Date
 MP 2.01.52 Endoscopic Radiofrequency Ablation or Cryoablation for Barrett`s Esophagus Medical Policy Section Medicine Issue 12:2013 Original Policy Date 12:2013 Last Review Status/Date Reviewed with literature
MP 2.01.52 Endoscopic Radiofrequency Ablation or Cryoablation for Barrett`s Esophagus Medical Policy Section Medicine Issue 12:2013 Original Policy Date 12:2013 Last Review Status/Date Reviewed with literature
Peptic ulcer disease Disorders of the esophagus
 Peptic ulcer disease Disorders of the esophagus Peptic ulcer disease Burning epigastric pain Exacerbated by fasting Improved with meals Ulcer: disruption of mucosal integrity >5 mm in size, with depth
Peptic ulcer disease Disorders of the esophagus Peptic ulcer disease Burning epigastric pain Exacerbated by fasting Improved with meals Ulcer: disruption of mucosal integrity >5 mm in size, with depth
Quiz Adenocarcinoma of the distal stomach has been increasing in the last 20 years. a. True b. False
 Quiz 1 1. Which of the following are risk factors for esophagus cancer. a. Obesity b. Gastroesophageal reflux c. Smoking and Alcohol d. All of the above 2. Adenocarcinoma of the distal stomach has been
Quiz 1 1. Which of the following are risk factors for esophagus cancer. a. Obesity b. Gastroesophageal reflux c. Smoking and Alcohol d. All of the above 2. Adenocarcinoma of the distal stomach has been
Vital staining and Barrett s esophagus
 Marcia Irene Canto, MD, MHS Baltimore, Maryland Vital staining or chromoendoscopy refers to staining of endoscopic tissue or topical application of chemical stains or pigments to alter tissue appearances
Marcia Irene Canto, MD, MHS Baltimore, Maryland Vital staining or chromoendoscopy refers to staining of endoscopic tissue or topical application of chemical stains or pigments to alter tissue appearances
Anatomy: From cricoid cartilage to diaphragm 25 Cms. 4 portions: Cervical 5 cms. Thoracic 25 cms. Abdominal 2 cms. Blood supply Lymphatic spread
 Esophagus Anatomy: From cricoid cartilage to diaphragm 25 Cms. 4 portions: Cervical 5 cms. Thoracic 25 cms. Abdominal 2 cms. Blood supply Lymphatic spread Upper 2/3 Cephalad Lower 1/3 Caudad Physiology:
Esophagus Anatomy: From cricoid cartilage to diaphragm 25 Cms. 4 portions: Cervical 5 cms. Thoracic 25 cms. Abdominal 2 cms. Blood supply Lymphatic spread Upper 2/3 Cephalad Lower 1/3 Caudad Physiology:
Current Management of Low-Grade Dysplasia in Barrett Esophagus
 Current Management of Low-Grade Dysplasia in Barrett Esophagus Gary W. Falk, MD, MS Dr Falk is a professor of medicine in the Division of Gastroenterology at the University of Pennsylvania Perelman School
Current Management of Low-Grade Dysplasia in Barrett Esophagus Gary W. Falk, MD, MS Dr Falk is a professor of medicine in the Division of Gastroenterology at the University of Pennsylvania Perelman School
Volumetric laser endomicroscopy can target neoplasia not detected by conventional endoscopic measures in long segment Barrett s esophagus
 E318 Volumetric laser endomicroscopy can target neoplasia not detected by conventional endoscopic measures in long segment esophagus Authors Institution Arvind J. Trindade, Benley J. George, Joshua Berkowitz,
E318 Volumetric laser endomicroscopy can target neoplasia not detected by conventional endoscopic measures in long segment esophagus Authors Institution Arvind J. Trindade, Benley J. George, Joshua Berkowitz,
GASTROINTESTINAL TRACT
 GASTROINTESTINAL TRACT A 40 yr old man complains of difficulty of swallowing & a tendency to regurgitate his food--------- YOUR DIAGNOSIS IS-------- ESOPHAGUS Clinical manifestations: 1-Dysphagia (difficulty
GASTROINTESTINAL TRACT A 40 yr old man complains of difficulty of swallowing & a tendency to regurgitate his food--------- YOUR DIAGNOSIS IS-------- ESOPHAGUS Clinical manifestations: 1-Dysphagia (difficulty
Chapter 12: Training in Pathology. DDSEP Chapter 13: Question 19
 DDSEP Chapter 13: Question 19 A 70 year-old male with a history of celiac disease diagnosed in his forties reports abdominal pain, dark stools, and 20-pound weight loss. He reports complete compliance
DDSEP Chapter 13: Question 19 A 70 year-old male with a history of celiac disease diagnosed in his forties reports abdominal pain, dark stools, and 20-pound weight loss. He reports complete compliance
SAM PROVIDER TOOLKIT
 THE AMERICAN BOARD OF PATHOLOGY Maintenance of Certification (MOC) Program SAM PROVIDER TOOLKIT Developing Self-Assessment Modules (SAMs) www.abpath.org The American Board of Pathology (ABP) approves educational
THE AMERICAN BOARD OF PATHOLOGY Maintenance of Certification (MOC) Program SAM PROVIDER TOOLKIT Developing Self-Assessment Modules (SAMs) www.abpath.org The American Board of Pathology (ABP) approves educational
Slide 1. Slide 2. Slide 3 DISCLOSURES EXPECTED OUTCOMES DIAGNOSIS AND TREATMENT
 Slide 1 DIAGNOSIS AND TREATMENT 1 Slide 2 DISCLOSURES Successful completion: Participants must attend the entire program, including any resulting Q & A, and submit required documentation. Conflict of interest:
Slide 1 DIAGNOSIS AND TREATMENT 1 Slide 2 DISCLOSURES Successful completion: Participants must attend the entire program, including any resulting Q & A, and submit required documentation. Conflict of interest:
MECHANISMS OF HUMAN DISEASE: LABORATORY SESSIONS GASTROINTESTINAL (GI) PATHOLOGY LAB #1. January 06, 2012
 PATHOLOGY LAB #1. January 06, 2012") MECHANISMS OF HUMAN DISEASE: LABORATORY SESSIONS GASTROINTESTINAL (GI) PATHOLOGY LAB #1 GOAL: January 06, 2012 Faculty Copy 1. Describe the basis morphologic and pathophysiologic changes which occur in
MECHANISMS OF HUMAN DISEASE: LABORATORY SESSIONS GASTROINTESTINAL (GI) PATHOLOGY LAB #1 GOAL: January 06, 2012 Faculty Copy 1. Describe the basis morphologic and pathophysiologic changes which occur in
Gastrointestinal Disorders. Disorders of the Esophagus 3/7/2013. Congenital Abnormalities. Achalasia. Not an easy repair. Types
 Gastrointestinal Disorders Congenital Abnormalities Disorders of the Esophagus Types Stenosis Atresia Fistula Newborn aspirates while feeding. Pneumonia Not an easy repair Achalasia Lack of relaxation
Gastrointestinal Disorders Congenital Abnormalities Disorders of the Esophagus Types Stenosis Atresia Fistula Newborn aspirates while feeding. Pneumonia Not an easy repair Achalasia Lack of relaxation
A Multidisciplinary Approach to Esophageal Dysphagia: Role of the SLP. Darlene Graner, M.A., CCC-SLP, BRS-S Sharon Burton, M.D.
 A Multidisciplinary Approach to Esophageal Dysphagia: Role of the SLP Darlene Graner, M.A., CCC-SLP, BRS-S Sharon Burton, M.D. What is the role of the SLP? Historically SLPs the preferred providers for
A Multidisciplinary Approach to Esophageal Dysphagia: Role of the SLP Darlene Graner, M.A., CCC-SLP, BRS-S Sharon Burton, M.D. What is the role of the SLP? Historically SLPs the preferred providers for
Adenocarcinoma of the distal esophagus is a recognized
 ORIGINAL ARTICLE Adenocarcinomas of the Distal Esophagus and Gastric Cardia Are Predominantly Esophageal Carcinomas Parakrama Chandrasoma, MD, Kumari Wickramasinghe, MD, PhD, Yanling Ma, MD, and Tom DeMeester,
ORIGINAL ARTICLE Adenocarcinomas of the Distal Esophagus and Gastric Cardia Are Predominantly Esophageal Carcinomas Parakrama Chandrasoma, MD, Kumari Wickramasinghe, MD, PhD, Yanling Ma, MD, and Tom DeMeester,
Myogenic Control. Esophageal Motility. Enteric Nervous System. Alimentary Tract Motility. Determinants of GI Tract Motility.
 Myogenic Control Esophageal Motility David Markowitz, MD Columbia University, College of Physicians and Surgeons Basic Electrical Rythym: intrinsic rhythmic fluctuation of smooth muscle membrane potential
Myogenic Control Esophageal Motility David Markowitz, MD Columbia University, College of Physicians and Surgeons Basic Electrical Rythym: intrinsic rhythmic fluctuation of smooth muscle membrane potential
Esophageal Motility. Alimentary Tract Motility
 Esophageal Motility David Markowitz, MD Columbia University, College of Physicians and Surgeons Alimentary Tract Motility Propulsion Movement of food and endogenous secretions Mixing Allows for greater
Esophageal Motility David Markowitz, MD Columbia University, College of Physicians and Surgeons Alimentary Tract Motility Propulsion Movement of food and endogenous secretions Mixing Allows for greater
EGD Data Collection Form
 Sociodemographic Information Type Zip Code Gender Height (in inches) Race Ethnicity Inpatient Outpatient Male Female Birth Date Weight (in pounds) American Indian (Native American) or Alaska Native Asian
Sociodemographic Information Type Zip Code Gender Height (in inches) Race Ethnicity Inpatient Outpatient Male Female Birth Date Weight (in pounds) American Indian (Native American) or Alaska Native Asian
The increasing incidence of esophageal adenocarcinoma
 GASTROENTEROLOGY 2004;127:310 330 A Critical Review of the Diagnosis and Management of Barrett s Esophagus: The AGA Chicago Workshop PRATEEK SHARMA,* KENNETH MCQUAID, JOHN DENT, M. BRIAN FENNERTY, RICHARD
GASTROENTEROLOGY 2004;127:310 330 A Critical Review of the Diagnosis and Management of Barrett s Esophagus: The AGA Chicago Workshop PRATEEK SHARMA,* KENNETH MCQUAID, JOHN DENT, M. BRIAN FENNERTY, RICHARD
GI update. Common conditions and concerns my patients frequently asked about
 GI update Common conditions and concerns my patients frequently asked about Specific conditions I ll try to cover today 1. Colon polyps, colorectal cancer and colonoscopy 2. Crohn s disease 3. Peptic ulcer
GI update Common conditions and concerns my patients frequently asked about Specific conditions I ll try to cover today 1. Colon polyps, colorectal cancer and colonoscopy 2. Crohn s disease 3. Peptic ulcer
Gastroesophageal reflux disease Principles of GERD treatment Treatment of reflux diseases GERD
 Esophagus Anatomy/Physiology Gastroesophageal reflux disease Principles of GERD treatment Treatment of reflux diseases GERD Manometry Question 50 years old female with chest pain and dysphagia. Manometry
Esophagus Anatomy/Physiology Gastroesophageal reflux disease Principles of GERD treatment Treatment of reflux diseases GERD Manometry Question 50 years old female with chest pain and dysphagia. Manometry
David Markowitz, MD. Physicians and Surgeons
 Esophageal Motility David Markowitz, MD Columbia University, College of Columbia University, College of Physicians and Surgeons Alimentary Tract Motility Propulsion Movement of food and endogenous secretions
Esophageal Motility David Markowitz, MD Columbia University, College of Columbia University, College of Physicians and Surgeons Alimentary Tract Motility Propulsion Movement of food and endogenous secretions