Venous thrombosis is common and often occurs spontaneously, but it also frequently accompanies medical and surgical conditions, both in the community
|
|
|
- Jessie Carroll
- 5 years ago
- Views:
Transcription

1 Venous Thrombosis


2
3 Venous Thrombosis It occurs mainly in the deep veins of the leg (deep vein thrombosis, DVT), from which parts of the clot frequently embolize to the lungs (pulmonary embolism, PE). Fewer than 5% of all venous thromboses occur at other sites
4 Venous thrombosis is common and often occurs spontaneously, but it also frequently accompanies medical and surgical conditions, both in the community and the hospital
5 Major complications of thrombosis include a disabling post-thrombotic syndrome and death due to fatal PE
6 Many risk factors for thrombosis are known, all of them related either to immobilization or to hypercoagulability. While it has no utility to assess the risk factor status after thrombosis has occurred, several acquired risk factors are so strong that they warrant prophylactic anticoagulation, in both those with and without a history of thrombosis. Detailed guidelines for primary prevention are available.
7 The incidence of a first venous thrombosis is 1 3 per 1000 persons per year. Around two-thirds manifest as DVT of the leg, and one-third as PE. Up to half of patients with PE have no signs of DVT. From 1 10% of venous thromboses prove fatal,
8 The recurrence rate of venous thrombosis is 3 10% per year.
9 Venous thrombosis is a multicausal disease that occurs when several risk factors are present simultaneously in a particular combination
10 Acquired Orthopedic surgery Neurosurgery Major abdominal surgery Major trauma Central venous catheters Malignancy Antiphospholipid syndrome Puerperium Prolonged bed rest Pregnancy Obesity Plaster cast Oral contraceptives Hormonal replacement therapy Myeloproliferative disorders Polycythemia vera Long-haul travel Age
11 Inherited Antithrombin deficiency Protein C deficiency Protein S deficiency Factor V Leiden (FVL) Prothrombin 20210A Non-O blood group Dysfibrinogenemia Factor XIII 34val
12 Pathobiology Virchow's triad of hypercoagulability, venous stasis, and injury to the vessel wall provides a useful model for understanding many of the risk factors that lead to the formation of thrombosis.
13 Clinical Manifestations leg pain, tenderness, swelling palpable cord, discoloration, venous distention, prominence of the superficial veins, and cyanosis
14 In most patients in whom DVT is clinically suspected, the symptoms and signs are nonspecific; in more than 50% of these patients, the clinical suspicion of DVT is not confirmed by objective testing. Conversely, patients with relatively minor symptoms and signs may have extensive DVT.


15
16 In some patients, DVT may be asymptomatic, but the patient will present with pulmonary embolism. Conversely, pulmonary embolism occurs in 50% of patients with objectively documented proximal leg vein thrombosis, but many of the emboli are asymptomatic.
17 Usually, only part of the thrombus embolizes,
18 Clinical Characteristic Score Active cancer (treatment ongoing within previous 6 months or palliative) 1 Paralysis, paresis, or recent plaster immobilization of the lower extremities 1 Recent bedrest >3 days or major surgery within 3 months requiring anesthesia 1 Localized tenderness of the deep veins of the leg 1 Entire leg swollen 1 Calf swelling >3 cm larger than asymptomatic side measured 10 cm below tibial tuberosity 1 Pitting edema confined to the symptomatic leg 1 Collateral superficial veins (not varicosed) 1 Previously documented DVT 1 Alternative diagnosis as likely as or more likely than DVT -2
19 Lancet 1997;350: A score of 0 or less indicates low probability, 1 or 2 indicates moderate probability, and 3 or more indicates high probability.
 and D-dimer testing to complement")
20 Diagnostic algorithm for suspected deep venous thrombosis. This algorithm uses evaluation of pretest probability based on a clinical prediction rule (see Table 81-1 ) and D-dimer testing to complement compression ultrasonography (CUS). The asterisk indicates use of a highly sensitive (>95%) D-dimer.
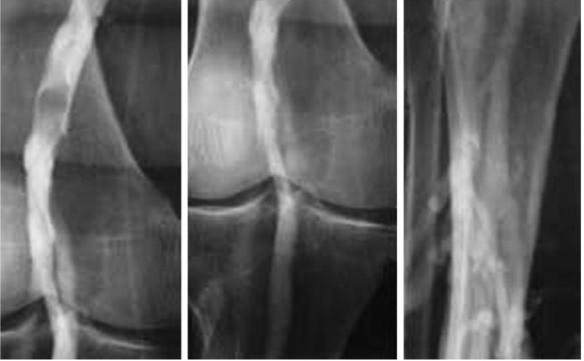
21 Imaging Contrast Venography Ascending contrast venography remains the gold standard for diagnosis, but because of its expense, discomfort to the patient, and potential for adverse experiences, venography is currently indicated in symptomatic patients only when diagnostic uncertainty persists after noninvasive testing or if noninvasive testing is unavailable.

22 Imaging
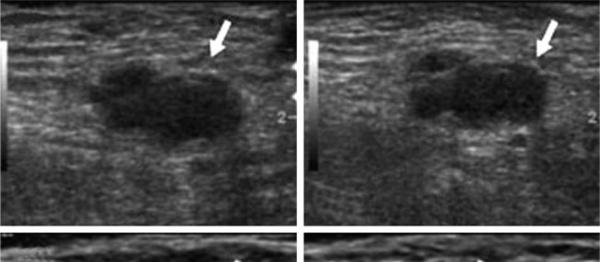
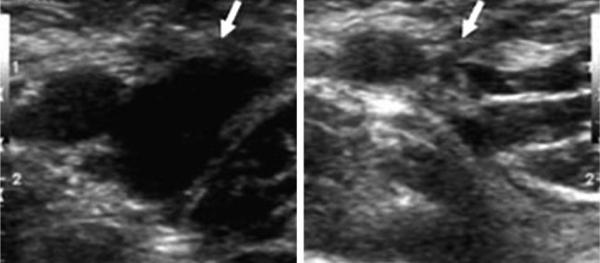
23 Compression Ultrasonography Compression venous ultrasonography is currently the most widely used noninvasive test for suspected DVT because of its accuracy in detection of thrombus involving the popliteal or more proximal veins;
24 absence of compressibility of the proximal leg veins on ultrasonography has a sensitivity of 97% and a specificity of 96% for symptomatic patients with suspected DVT
25 Thus, the finding of a noncompressible venous segment, particularly in the popliteal or common femoral vein, has a high positive predictive value for DVT in symptomatic patients and is an indication for treatment.
26 Of patients with symptoms suggestive of DVT but with normal findings on initial ultrasound examination of the proximal veins, about 15% will have undetected isolated calf DVT
27 progression into the proximal veins occurs in a minority of patients, usually within a week of presentation
28 Isolated calf DVT that does not extend into the proximal veins is rarely if ever associated with clinically important pulmonary embolus. The sensitivity of ultrasonography for calf DVT is well below 90%, with a wide range of accuracies reported for different populations of patients.
29
30 Imaging of the calf veins is timeconsuming, potentially inaccurate, and generally not recommended.
31 two-point (common femoral and popliteal) or three-point (two-point plus the calf trifurcation ) ultrasonography should be performed and, if the results are normal, repeated in 1 week after the initial examination. This approach will identify the 20 to 25% of patients who have had proximal extension of distal clot in the calf veins. If the repeated ultrasound examination is normal, further investigation and therapy can be safely withheld.
32 In centers with highly skilled operators, however, normal ultrasonography of the proximal and calf veins at presentation may be sufficiently accurate to exclude clinically important DVT;
33 D-Dimer measurement of D-dimer levels is a sensitive test for recent DVT and pulmonary emboli. Unfortunately, numerous nonthrombotic conditions, including sepsis, pregnancy, surgery, and cardiac or renal failure, can also cause elevated levels. As a result of this nonspecificity, the role of Ddimer assays is limited to helping exclude VTE when levels are not raised.


34
35 Highly sensitive tests, consisting of new rapid ELISA or immunoturbidimetric assays, have sensitivities of 95 to 100% for acute VTE but in general have low specificities (20 to 50%).
36 but clinicians must be aware of the accuracy of the assay in their institution before using the D-dimer assay to make management decisions.
37 ALTERNATIVE DIAGNOSES Diagnosis Patients (%) Muscle strain 24 Direct twisting injury to the leg 10 Leg swelling in paralyzed limb 9 Lymphangitis, lymphatic obstruction 7 Venous reflux 7 Muscle tear 6 Baker's cyst 5 Cellulitis 3 Internal abnormality of the knee 2 Unknown 26
38 Patients with a high pretest probability require ultrasonography regardless of the D-dimer result. A normal D-dimer result with use of either a moderately or highly sensitive assay can safely obviate the need for repeated imaging in patients with normal findings on initial ultrasound examination
39 Recurrent Deep Venous Thrombosis Approximately 10% of patients with unprovoked VTE will experience recurrent thromboembolism in the first year after ceasing anticoagulant therapy. In addition, many patients will have positional leg swelling and pain early during treatment as a result of venous outflow obstruction of the post-thrombotic syndrome when venous valvar incompetence is manifested
40 comparison with previous ultrasound images is required in patients with suspected recurrence. A normal D-dimer test result is useful in excluding recurrent DVT.
41 Pregnancy objective testing is needed to diagnose VTE. As in nonpregnant patients, compression ultrasonography is the initial test of choice
42
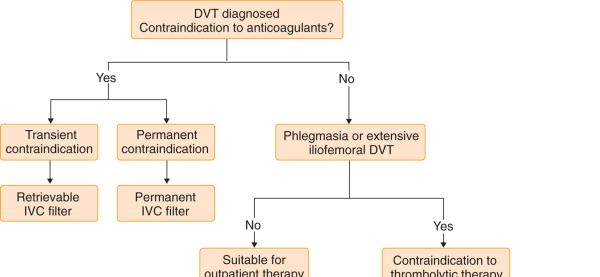
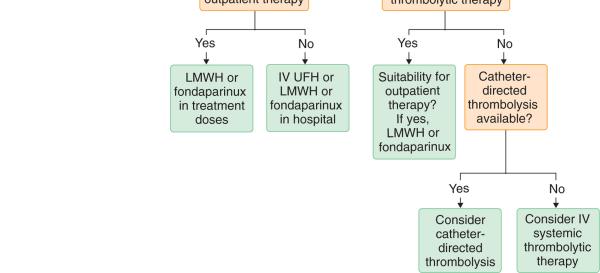
43 Anticoagulant therapy, which is the treatment of choice in most patients with VTE, Coumarin derivatives (e.g., warfarin) are usually the drugs of choice for long-term anticoagulant therapy, but such drugs have a delayed onset of anticoagulant effect
44 Therefore, initial short-term therapy with a rapid-acting heparin or heparin derivative for approximately 1 week is necessary to provide an immediate antithrombotic effect and to reduce the risk of thrombus growth or embolization in patients with acute DVT
45 LMWH or fondaparinux is preferred to inpatient treatment with intravenous unfractionated heparin whenever feasible in patients with DVT
46 The reduced size of LMWH also decreases charge-related nonspecific protein binding, thereby resulting in improved subcutaneous bioavailability, more predictable anticoagulant response, and predominantly dose-independent renal clearance.
47 once-daily administration of LMWH is thought to be as safe and effective as twice-daily administration.
48 three populations of patients in whom anti factor Xa monitoring should be considered: (1) patients with renal insufficiency (calculated creatinine clearance of less than 30 ml/min); (2) obese patients, in whom the volume of distribution of LMWH might be different, so weight-adjusted dosing might not be appropriate; and (3) pregnant women, in whom it is unclear whether the dose should be adjusted according to the woman's weight change.
49 Fondaparinux is a synthetic analogue of the critical pentasaccharide sequence required for binding of heparin molecules to antithrombin fondaparinux demonstrates 100% bioavailability, with peak plasma concentrations occurring 1.7 hours after dosing. Once-daily subcutaneous administration of fondaparinux (5.0 mg daily if weight is less than 50 kg; 7.5 mg daily if weight is 50 to 100 kg; 10 mg daily if weight is more than 100 kg) is an effective and safe alternative to LMWH for the initial 5 to 10 days of treatment of DVT
50 Clearance is predominantly renal
51 Unfractionated Heparin Up to 25% of patients with acute VTE have resistance to heparin, defined as a requirement for greater than expected doses of unfractionated heparin to achieve a therapeutic aptt. If it is available, anti factor Xa monitoring is recommended in patients with heparin resistance.
52 Warfarin the drug should be started within 24 to 48 hours of initiation of heparin with a goal of achieving international normalized ratio (INR) results between 2.0 and 3.0
53 Warfarin The dose is empirical, but a starting dose of 5 to 10 mg is suitable for most patients doses are adjusted according to the prothrombin time, expressed as the INR, performed daily or every other day until the results are in the therapeutic range for at least 24 hours.
54 Side Effects of Anticoagulants Bleeding is the most common side effect of anticoagulant therapy in approximately 2% of patients Factors such as recent surgery, trauma, and concurrent aspirin or thrombolytic therapy increase the risk of bleeding.
55 The risk of major bleeding increases according to individual characteristics, such as older age, the presence of comorbid conditions (e.g., diabetes, hypertension, renal insufficiency, previous gastrointestinal bleeding, or cancer), and the use of concomitant drugs, in particular antiplatelet therapy.
56 Heparin-induced thrombocytopenia manifested typically with thrombocytopenia and new thrombosis Monitoring of the platelet count is recommended every other day until day 14 in patients receiving therapeutic unfractionated heparin but is not routinely recommended with LMWH or fondaparinux because of the extremely low risk with these newer medications
57 The decision to prolong or to stop anticoagulation should be individualized, and a patient's preferences should be considered
58 Three months of treatment is associated with a 10 to 27% risk of recurrence whereas 6 months,,the risk of recurrence in the first year after stopping = 10%


59
60 Indications VTE suspected Guidelines Obtain baseline aptt, PT, CBC Check for contraindication to heparin therapy Order imaging study; consider giving IV unfractionated heparin (5000 IU) or LMWH VTE confirmed Give LMWH (dalteparin,[*] enoxaparin,[ ] nadroparin,[ ] tinzaparin,[ ] fondaparinux[**]) Start warfarin therapy on day 1 at 5 mg and adjust the subsequent daily dose according to INR Check platelet count between days 3 and 5 Stop LMWH therapy after at least 4 or 5 days of combined therapy when the INR is >2 Anticoagulate with warfarin for at least 3 months at an INR of 2.5, range of 2 3
61 WEIGHT-BASED NOMOGRAM FOR INITIAL INTRAVENOUS HEPARIN THERAPY aptt Dose (IU/kg) Initial dose 80 bolus, then 18/hr <35 sec (<1.2 )[*] 80 bolus, then 4/hr sec ( ) 40 bolus, then 2/hr sec ( ) No change sec (2.3 3 ) Decrease infusion rate by 2/hr >90 sec (>3 ) Hold infusion 1 hr, then decrease infusion rate by 3/hr
62 VTE in different populations of patients Management of Deep Venous Thrombosis in Pregnancy :
63 VTE in different populations of patients LMWH can simply be adjusted periodically on the basis of the woman's weight. Unfractionated heparin is less attractive than LMWH because it is associated with a greater reduction of bone density and a higher risk of heparin-induced thrombocytopenia.
64 Pregnant women with a DVT should probably be treated for the duration of pregnancy and for at least 6 weeks post partum. If the DVT occurs in the latter part of the third trimester, intravenous heparin should be administered by continuous infusion until approximately 6 hours before the expected time of delivery
65 Venous Thrombosis of the Upper Extremities Etiology : central venous catheters, acquired or hereditary thrombophilias, and anatomic (cervical rib) and physiologic (muscular individuals) impingement of the vein.
66 Upper extremity DVT can cause pulmonary emboli, although the exact frequency is not known.
67 anticoagulant therapy should be given in all patients with upper extremity DVT, with medications, doses, regimens, and durations identical to those for treatment of DVT of the leg
68 SUPERFICIAL THROMBOPHLEBITIS Superficial thrombophlebitis usually presents with pain, swelling, redness, and tenderness of superficial veins. Varicose veins can be red, warm, and clustered in a circumscribed area
69 SUPERFICIAL THROMBOPHLEBITIS it is reasonable to use moderate doses of LMWH for the initial treatment of acute, symptomatic superficial thrombophlebitis. Alternatively, and particularly for intravenous catheter induced superficial thrombophlebitis, a nonsteroidal antiinflammatory drug can be tried


70 Varicose veins are a risk factor for deep venous thrombosis and may result from it.
71 post-thrombotic syndrome develops in up to 50% of patients with proximal DVT, usually within the first 1 to 2 years after DVT. The syndrome is often a chronic, progressive disease with pain, swelling, and occasionally ulceration of the leg in patients with previous DVT.
72 Graduated compression stockings reduce the risk of the post-thrombotic syndrome by about 50%.


73
74
75
CHAPTER 2 VENOUS THROMBOEMBOLISM
 CHAPTER 2 VENOUS THROMBOEMBOLISM Objectives Venous Thromboembolism (VTE) Prevalence Patho-physiology Risk Factors Diagnosis Pulmonary Embolism (PE) Management of DVT/PE Prevention VTE Patho-physiology
CHAPTER 2 VENOUS THROMBOEMBOLISM Objectives Venous Thromboembolism (VTE) Prevalence Patho-physiology Risk Factors Diagnosis Pulmonary Embolism (PE) Management of DVT/PE Prevention VTE Patho-physiology
DEEP VEIN THROMBOSIS (DVT): TREATMENT
: TREATMENT") DEEP VEIN THROMBOSIS (DVT): TREATMENT OBJECTIVE: To provide an evidence-based approach to treatment of patients presenting with deep vein thrombosis (DVT). BACKGROUND: An estimated 45,000 patients in Canada
DEEP VEIN THROMBOSIS (DVT): TREATMENT OBJECTIVE: To provide an evidence-based approach to treatment of patients presenting with deep vein thrombosis (DVT). BACKGROUND: An estimated 45,000 patients in Canada
Mabel Labrada, MD Miami VA Medical Center
 Mabel Labrada, MD Miami VA Medical Center *1-Treatment for acute DVT with underlying malignancy is for 3 months. *2-Treatment of provoked acute proximal DVT can be stopped after 3months of treatment and
Mabel Labrada, MD Miami VA Medical Center *1-Treatment for acute DVT with underlying malignancy is for 3 months. *2-Treatment of provoked acute proximal DVT can be stopped after 3months of treatment and
DVT - initial management NSCCG
 Background information Information resources for patients and carers Updates to this care map Synonyms Below knee DVT and bleeding risks Patient with confirmed DVT Scan confirms superficial thrombophlebitis
Background information Information resources for patients and carers Updates to this care map Synonyms Below knee DVT and bleeding risks Patient with confirmed DVT Scan confirms superficial thrombophlebitis
Dr. Riaz JanMohamed Consultant Haematologist The Hillingdon Hospital Foundation Trust
 MANAGEMENT OF PATIENTS WITH DEEP VEIN THROMBOSIS (DVT) IN THE COMMUNITY SETTING & ANTICOAGULATION CLINICS THE PAST, PRESENT AND THE FUTURE Dr. Riaz JanMohamed Consultant Haematologist The Hillingdon Hospital
MANAGEMENT OF PATIENTS WITH DEEP VEIN THROMBOSIS (DVT) IN THE COMMUNITY SETTING & ANTICOAGULATION CLINICS THE PAST, PRESENT AND THE FUTURE Dr. Riaz JanMohamed Consultant Haematologist The Hillingdon Hospital
Suspected Deep Vein Thrombosis (DVT) Pathway for Non Pregnant patients Updated November 2016, with new D-dimer reference range
 Pathway for Non Pregnant patients Updated November 2016, with new D-dimer reference range") Suspected Deep Vein Thrombosis (DVT) Pathway for Non Pregnant patients Updated November 2016, with new D-dimer reference range Suspect a DVT? Complete a Two-level DVT Wells score on ICE system (see page
Suspected Deep Vein Thrombosis (DVT) Pathway for Non Pregnant patients Updated November 2016, with new D-dimer reference range Suspect a DVT? Complete a Two-level DVT Wells score on ICE system (see page
Suspected Deep Vein Thrombosis (DVT) Assessment
 Assessment") CHI no... First name... DOB... /... /... Last name... Sex: c M c F Address...... Telephone... or attach addressograph label here Hospital/Location: c Hairmyres c Monklands c Wishaw Other (specify)... Ward/Base...
CHI no... First name... DOB... /... /... Last name... Sex: c M c F Address...... Telephone... or attach addressograph label here Hospital/Location: c Hairmyres c Monklands c Wishaw Other (specify)... Ward/Base...
Slide 1. Slide 2. Slide 3. Outline of This Presentation
 Slide 1 Current Approaches to Venous Thromboembolism Prevention in Orthopedic Patients Hujefa Vora, MD Maria Fox, RN June 9, 2017 Slide 2 Slide 3 Outline of This Presentation Pathophysiology of venous
Slide 1 Current Approaches to Venous Thromboembolism Prevention in Orthopedic Patients Hujefa Vora, MD Maria Fox, RN June 9, 2017 Slide 2 Slide 3 Outline of This Presentation Pathophysiology of venous
Disclosures. DVT: Diagnosis and Treatment. Questions To Ask. Dr. Susanna Shin - DVT: Diagnosis and Treatment. Acute Venous Thromboembolism (VTE) None
 None") Disclosures DVT: Diagnosis and Treatment None Susanna Shin, MD, FACS Assistant Professor University of Washington Acute Venous Thromboembolism (VTE) Deep Venous Thrombosis (DVT) Pulmonary Embolism (PE)
Disclosures DVT: Diagnosis and Treatment None Susanna Shin, MD, FACS Assistant Professor University of Washington Acute Venous Thromboembolism (VTE) Deep Venous Thrombosis (DVT) Pulmonary Embolism (PE)
Proper Diagnosis of Venous Thromboembolism (VTE)
") Proper Diagnosis of Venous Thromboembolism (VTE) Whal Lee, M.D. Seoul National University Hospital Department of Radiology 2 nd EFORT Asia Symposium, 3 rd November 2010, Taipei DVT - Risk Factors Previous
Proper Diagnosis of Venous Thromboembolism (VTE) Whal Lee, M.D. Seoul National University Hospital Department of Radiology 2 nd EFORT Asia Symposium, 3 rd November 2010, Taipei DVT - Risk Factors Previous
Approach to Thrombosis
 Approach to Thrombosis Theera Ruchutrakool, M.D. Division of Hematology Department of Medicine Siriraj Hospital Faculty of Medicine Mahidol University Approach to Thrombosis Thrombosis: thrombus formation
Approach to Thrombosis Theera Ruchutrakool, M.D. Division of Hematology Department of Medicine Siriraj Hospital Faculty of Medicine Mahidol University Approach to Thrombosis Thrombosis: thrombus formation
PULMONARY EMBOLISM (PE): DIAGNOSIS AND TREATMENT
: DIAGNOSIS AND TREATMENT") PULMONARY EMBOLISM (PE): DIAGNOSIS AND TREATMENT OBJECTIVE: To provide a diagnostic algorithm and treatment options for patients with acute pulmonary embolism (PE). BACKGROUND: Venous thromboembolism (VTE)
PULMONARY EMBOLISM (PE): DIAGNOSIS AND TREATMENT OBJECTIVE: To provide a diagnostic algorithm and treatment options for patients with acute pulmonary embolism (PE). BACKGROUND: Venous thromboembolism (VTE)
DVT PROPHYLAXIS IN HOSPITALIZED MEDICAL PATIENTS SAURABH MAJI SR (PULMONARY,MEDICINE)
") DVT PROPHYLAXIS IN HOSPITALIZED MEDICAL PATIENTS SAURABH MAJI SR (PULMONARY,MEDICINE) Introduction VTE (DVT/PE) is an important complication in hospitalized patients Hospitalization for acute medical illness
DVT PROPHYLAXIS IN HOSPITALIZED MEDICAL PATIENTS SAURABH MAJI SR (PULMONARY,MEDICINE) Introduction VTE (DVT/PE) is an important complication in hospitalized patients Hospitalization for acute medical illness
Objectives. Venous Thromboembolism (VTE) Prophylaxis. Case VTE WHY DO IT? Question: Who Is At Risk?
 Prophylaxis. Case VTE WHY DO IT? Question: Who Is At Risk?") Objectives Venous Thromboembolism (VTE) Prophylaxis Rishi Garg, MD Department of Medicine Identify patients at risk for VTE Options for VTE prophylaxis Current Recommendations (based on The Seventh ACCP
Objectives Venous Thromboembolism (VTE) Prophylaxis Rishi Garg, MD Department of Medicine Identify patients at risk for VTE Options for VTE prophylaxis Current Recommendations (based on The Seventh ACCP
PE and DVT. Dr Anzo William Adiga WatsApp or Call Medical Officer/RHEMA MEDICAL GROUP
 PE and DVT Dr Anzo William Adiga WatsApp or Call +256777363201 Medical Officer/RHEMA MEDICAL GROUP OBJECTIVES DEFINE DVT AND P.E PATHOPHYSIOLOGY OF DVT CLINICAL PRESENTATION OF DVT/PE INVESTIGATE DVT MANAGEMENT
PE and DVT Dr Anzo William Adiga WatsApp or Call +256777363201 Medical Officer/RHEMA MEDICAL GROUP OBJECTIVES DEFINE DVT AND P.E PATHOPHYSIOLOGY OF DVT CLINICAL PRESENTATION OF DVT/PE INVESTIGATE DVT MANAGEMENT
CURRENT & FUTURE THERAPEUTIC MANAGEMENT OF VENOUS THROMBOEMBOLISM. Gordon Lowe Professor of Vascular Medicine University of Glasgow
 CURRENT & FUTURE THERAPEUTIC MANAGEMENT OF VENOUS THROMBOEMBOLISM Gordon Lowe Professor of Vascular Medicine University of Glasgow VENOUS THROMBOEMBOLISM Common cause of death and disability 50% hospital-acquired
CURRENT & FUTURE THERAPEUTIC MANAGEMENT OF VENOUS THROMBOEMBOLISM Gordon Lowe Professor of Vascular Medicine University of Glasgow VENOUS THROMBOEMBOLISM Common cause of death and disability 50% hospital-acquired
Diagnosis and Treatment of Deep Venous Thrombosis and Pulmonary Embolism
 Agency for Healthcare Research and Quality Evidence Report/Technology Assessment Diagnosis and Treatment of Deep Venous Thrombosis and Pulmonary Embolism Summary Number 68 Overview Venous thromboembolism
Agency for Healthcare Research and Quality Evidence Report/Technology Assessment Diagnosis and Treatment of Deep Venous Thrombosis and Pulmonary Embolism Summary Number 68 Overview Venous thromboembolism
Venous Thromboembolism Prophylaxis
 Approved by: Venous Thromboembolism Prophylaxis Vice President and Chief Medical Officer; and Vice President and Chief Operating Officer Corporate Policy & Procedures Manual Number: Date Approved January
Approved by: Venous Thromboembolism Prophylaxis Vice President and Chief Medical Officer; and Vice President and Chief Operating Officer Corporate Policy & Procedures Manual Number: Date Approved January
Deep vein thrombosis: diagnosis, prevention and treatment
 Deep vein thrombosis: diagnosis, prevention and treatment Catherine Bagot BSc, MD, MRCP, FRCPath and Campbell Tait BSc, FRCP, FRCPath Deep vein thrombosis can lead to significant morbidity and has well-recognised
Deep vein thrombosis: diagnosis, prevention and treatment Catherine Bagot BSc, MD, MRCP, FRCPath and Campbell Tait BSc, FRCP, FRCPath Deep vein thrombosis can lead to significant morbidity and has well-recognised
How long to continue anticoagulation after DVT?
 How long to continue anticoagulation after DVT? Dr. Nihar Ranjan Pradhan M.S., DNB (Vascular Surgery), FVES(UK) Consultant Vascular Surgeon Apollo Hospital, Jubilee Hills, Hyderabad (Formerly Faculty in
How long to continue anticoagulation after DVT? Dr. Nihar Ranjan Pradhan M.S., DNB (Vascular Surgery), FVES(UK) Consultant Vascular Surgeon Apollo Hospital, Jubilee Hills, Hyderabad (Formerly Faculty in
Prevention and treatment of venous thromboembolic disease
 REVIEW Prevention and treatment of venous thromboembolic disease SUSAN McNEILL AND CATHERINE BAGOT Awareness of the risk factors for venous thromboembolic (VTE) disease and timely administration of thromboprophylaxis
REVIEW Prevention and treatment of venous thromboembolic disease SUSAN McNEILL AND CATHERINE BAGOT Awareness of the risk factors for venous thromboembolic (VTE) disease and timely administration of thromboprophylaxis
With All the New Drugs, This is How I Treat Acute DVT and Superficial Phlebitis
 BRIGHAM AND WOMEN S HOSPITAL With All the New Drugs, This is How I Treat Acute DVT and Superficial Phlebitis Gregory Piazza, MD, MS Division of Cardiovascular Medicine Brigham and Women s Hospital April
BRIGHAM AND WOMEN S HOSPITAL With All the New Drugs, This is How I Treat Acute DVT and Superficial Phlebitis Gregory Piazza, MD, MS Division of Cardiovascular Medicine Brigham and Women s Hospital April
THROMBOSIS RISK FACTOR ASSESSMENT
 Name: Procedure: Doctor: Date: THROMBOSIS RISK FACTOR ASSESSMENT CHOOSE ALL THAT APPLY EACH RISK FACTOR REPRESENTS 1 POINT Age 41 60 years Minor Surgery Planned History of Prior Major Surgery (< 1 month)
Name: Procedure: Doctor: Date: THROMBOSIS RISK FACTOR ASSESSMENT CHOOSE ALL THAT APPLY EACH RISK FACTOR REPRESENTS 1 POINT Age 41 60 years Minor Surgery Planned History of Prior Major Surgery (< 1 month)
Prevention and management of deep venous thrombosis (DVT) John Fletcher Wound Care Association of New South Wales
 John Fletcher Wound Care Association of New South Wales") Prevention and management of deep venous thrombosis (DVT) John Fletcher Wound Care Association of New South Wales Merimbula, 6 th November 2010 University of Sydney Department of Surgery Westmead Hospital
Prevention and management of deep venous thrombosis (DVT) John Fletcher Wound Care Association of New South Wales Merimbula, 6 th November 2010 University of Sydney Department of Surgery Westmead Hospital
Disclosures. What is a Specialty Vein Clinic? Prevalence of Venous Disease. Management of Venous Disease: an evidence based approach.
 Management of Venous Disease: an evidence based approach Disclosures Ed Boyle, MD Andrew Jones, MD Dr. Ed Boyle and Dr. Andrew Jones disclose Grants/research support: Medtronic, BTG International, Clearflow,
Management of Venous Disease: an evidence based approach Disclosures Ed Boyle, MD Andrew Jones, MD Dr. Ed Boyle and Dr. Andrew Jones disclose Grants/research support: Medtronic, BTG International, Clearflow,
Dr. Rami M. Adil Al-Hayali Assistant Professor in Medicine
 Dr. Rami M. Adil Al-Hayali Assistant Professor in Medicine Venous thromboembolism: pulmonary embolism (PE) deep vein thrombosis (DVT) 1% of all patients admitted to hospital 5% of in-hospital mortality
Dr. Rami M. Adil Al-Hayali Assistant Professor in Medicine Venous thromboembolism: pulmonary embolism (PE) deep vein thrombosis (DVT) 1% of all patients admitted to hospital 5% of in-hospital mortality
Misunderstandings of Venous thromboembolism prophylaxis
 Misunderstandings of Venous thromboembolism prophylaxis Veerendra Chadachan Senior Consultant Dept of General Medicine (Vascular Medicine and Hypertension) Tan Tock Seng Hospital, Singapore Case scenario
Misunderstandings of Venous thromboembolism prophylaxis Veerendra Chadachan Senior Consultant Dept of General Medicine (Vascular Medicine and Hypertension) Tan Tock Seng Hospital, Singapore Case scenario
This chapter will describe the effectiveness of antithrombotic
 Antithrombotic Therapy for Venous Thromboembolic Disease The Seventh ACCP Conference on Antithrombotic and Thrombolytic Therapy Harry R. Büller, MD, Chair; Giancarlo Agnelli, MD; Russel D. Hull, MBBS,
Antithrombotic Therapy for Venous Thromboembolic Disease The Seventh ACCP Conference on Antithrombotic and Thrombolytic Therapy Harry R. Büller, MD, Chair; Giancarlo Agnelli, MD; Russel D. Hull, MBBS,
INDICATIONS FOR THROMBO-PROPHYLAXIS AND WHEN TO STOP ANTICOAGULATION BEFORE ELECTIVE SURGERY
 INDICATIONS FOR THROMBO-PROPHYLAXIS AND WHEN TO STOP ANTICOAGULATION BEFORE ELECTIVE SURGERY N.E. Pearce INTRODUCTION Preventable death Cause of morbidity and mortality Risk factors Pulmonary embolism
INDICATIONS FOR THROMBO-PROPHYLAXIS AND WHEN TO STOP ANTICOAGULATION BEFORE ELECTIVE SURGERY N.E. Pearce INTRODUCTION Preventable death Cause of morbidity and mortality Risk factors Pulmonary embolism
DEEP VENOUS THROMBOSIS A PRACTICAL APPROACH TO IMPROVING CLINICAL OUTCOMES
 DEEP VENOUS THROMBOSIS A PRACTICAL APPROACH TO IMPROVING CLINICAL OUTCOMES Jose M. Borromeo M.D. Vascular Surgeon Iowa Heart Center Disclosures: AstraZeneca Pharmaceuticals Cook CVRx LeMaitre Vascular,
DEEP VENOUS THROMBOSIS A PRACTICAL APPROACH TO IMPROVING CLINICAL OUTCOMES Jose M. Borromeo M.D. Vascular Surgeon Iowa Heart Center Disclosures: AstraZeneca Pharmaceuticals Cook CVRx LeMaitre Vascular,
Diagnostic Algorithms in VTE
 Diagnostic Algorithms in VTE Mark H. Meissner, MD Department of Surgery University of Washington School of Medicine Overutilization of Venous Duplex U/S 1983-1993 (Zweibel et al, Australasian Rad, 1995)
Diagnostic Algorithms in VTE Mark H. Meissner, MD Department of Surgery University of Washington School of Medicine Overutilization of Venous Duplex U/S 1983-1993 (Zweibel et al, Australasian Rad, 1995)
Cancer and Thrombosis
 Cancer and Thrombosis The close relationship between venous thromboembolism and cancer has been known since at least the 19th century by Armand Trousseau. Thrombosis is a major cause of morbidity and mortality
Cancer and Thrombosis The close relationship between venous thromboembolism and cancer has been known since at least the 19th century by Armand Trousseau. Thrombosis is a major cause of morbidity and mortality
DVT Pathophysiology and Prophylaxis in Medically Hospitalized Patients. David Liff MD Oklahoma Heart Institute Vascular Center
 DVT Pathophysiology and Prophylaxis in Medically Hospitalized Patients David Liff MD Oklahoma Heart Institute Vascular Center Overview Pathophysiology of DVT Epidemiology and risk factors for DVT in the
DVT Pathophysiology and Prophylaxis in Medically Hospitalized Patients David Liff MD Oklahoma Heart Institute Vascular Center Overview Pathophysiology of DVT Epidemiology and risk factors for DVT in the
What You Should Know
 1 New 2018 ASH Clinical Practice Guidelines on Venous Thromboembolism: What You Should Know New 2018 ASH Clinical Practice Guidelines on Venous Thromboembolism: What You Should Know The American Society
1 New 2018 ASH Clinical Practice Guidelines on Venous Thromboembolism: What You Should Know New 2018 ASH Clinical Practice Guidelines on Venous Thromboembolism: What You Should Know The American Society
CANCER ASSOCIATED THROMBOSIS. Pankaj Handa Department of General Medicine Tan Tock Seng Hospital
 CANCER ASSOCIATED THROMBOSIS Pankaj Handa Department of General Medicine Tan Tock Seng Hospital My Talk Today 1.Introduction 2. Are All Cancer Patients at Risk of VTE? 3. Should All VTE Patients Be Screened
CANCER ASSOCIATED THROMBOSIS Pankaj Handa Department of General Medicine Tan Tock Seng Hospital My Talk Today 1.Introduction 2. Are All Cancer Patients at Risk of VTE? 3. Should All VTE Patients Be Screened
HEPARIN-INDUCED THROMBOCYTOPENIA (HIT)
") HEPARIN-INDUCED THROMBOCYTOPENIA (HIT) OBJECTIVE: To assist clinicians with the investigation and management of suspected and documented heparin-induced thrombocytopenia (HIT). BACKGROUND: HIT is a transient,
HEPARIN-INDUCED THROMBOCYTOPENIA (HIT) OBJECTIVE: To assist clinicians with the investigation and management of suspected and documented heparin-induced thrombocytopenia (HIT). BACKGROUND: HIT is a transient,
10/8/2012. Disclosures. Making Sense of AT9: Review of the 2012 ACCP Antithrombotic Guidelines. Goals and Objectives. Outline
 Disclosures Making Sense of AT9: Review of the 2012 ACCP Antithrombotic Guidelines No relevant conflicts of interest related to the topic presented. Cyndy Brocklebank, PharmD, CDE Chronic Disease Management
Disclosures Making Sense of AT9: Review of the 2012 ACCP Antithrombotic Guidelines No relevant conflicts of interest related to the topic presented. Cyndy Brocklebank, PharmD, CDE Chronic Disease Management
Jessica Bryan, Natalia Evans, Karlyn Henderson, & Whitney Parks
 Jessica Bryan, Natalia Evans, Karlyn Henderson, & Whitney Parks 1. What is the most common cause of death in hospitalized patients? 1. Hospital-acquired infection 2. Pulmonary embolism 3. Myocardial infarction
Jessica Bryan, Natalia Evans, Karlyn Henderson, & Whitney Parks 1. What is the most common cause of death in hospitalized patients? 1. Hospital-acquired infection 2. Pulmonary embolism 3. Myocardial infarction
Challenges in Anticoagulation and Thromboembolism
 Challenges in Anticoagulation and Thromboembolism Ethan Cumbler M.D. Assistant Professor of Medicine Hospitalist Medicine Section University of Colorado Denver May 2010 No Conflicts of Interest Objectives
Challenges in Anticoagulation and Thromboembolism Ethan Cumbler M.D. Assistant Professor of Medicine Hospitalist Medicine Section University of Colorado Denver May 2010 No Conflicts of Interest Objectives
Jordan M. Garrison, MD FACS, FASMBS
 Jordan M. Garrison, MD FACS, FASMBS Peripheral Arterial Disease (PAD) Near or Complete obstruction of > 1 Peripheral Artery Peripheral Venous reflux Disease Varicose Veins Chronic Venous Stasis Ulcer Disease
Jordan M. Garrison, MD FACS, FASMBS Peripheral Arterial Disease (PAD) Near or Complete obstruction of > 1 Peripheral Artery Peripheral Venous reflux Disease Varicose Veins Chronic Venous Stasis Ulcer Disease
Dave Duddleston, MD VP and Medical Director Southern Farm Bureau Life
 Dave Duddleston, MD VP and Medical Director Southern Farm Bureau Life Sources of Risk for Venous Diseases Pulmonary embolism (thrombus) Bleeding from anticoagulation Mortality from underlying disease Chronic
Dave Duddleston, MD VP and Medical Director Southern Farm Bureau Life Sources of Risk for Venous Diseases Pulmonary embolism (thrombus) Bleeding from anticoagulation Mortality from underlying disease Chronic
DVT and Pulmonary Embolus. Dr Piers Blombery BSc(Biomed), MBBS (Hons), FRACP, FRCPA Consultant Haematologist Peter MacCallum Cancer Centre
, MBBS (Hons), FRACP, FRCPA Consultant Haematologist Peter MacCallum Cancer Centre") DVT and Pulmonary Embolus Dr Piers Blombery BSc(Biomed), MBBS (Hons), FRACP, FRCPA Consultant Haematologist Peter MacCallum Cancer Centre Overview Structure of deep and superficial venous system of upper
DVT and Pulmonary Embolus Dr Piers Blombery BSc(Biomed), MBBS (Hons), FRACP, FRCPA Consultant Haematologist Peter MacCallum Cancer Centre Overview Structure of deep and superficial venous system of upper
Diagnosis of Venous Thromboembolism
 Diagnosis of Venous Thromboembolism An Educational Slide Set American Society of Hematology 2018 Guidelines for Management of Venous Thromboembolism Slide set authors: Eric Tseng MD MScCH, University of
Diagnosis of Venous Thromboembolism An Educational Slide Set American Society of Hematology 2018 Guidelines for Management of Venous Thromboembolism Slide set authors: Eric Tseng MD MScCH, University of
NOTE: The first appearance of terms in bold in the body of this document (except titles) are defined terms please refer to the Definitions section.
 are defined terms please refer to the Definitions section.") TITLE VENOUS THROMBOEMBOLISM PROPHYLAXIS SCOPE Provincial Acute and Sub-Acute Care Facilities APPROVAL AUTHORITY Alberta Health Services Executive Committee SPONSOR Vice President, Quality and Chief Medical
TITLE VENOUS THROMBOEMBOLISM PROPHYLAXIS SCOPE Provincial Acute and Sub-Acute Care Facilities APPROVAL AUTHORITY Alberta Health Services Executive Committee SPONSOR Vice President, Quality and Chief Medical
Deep Vein Thrombosis and Pulmonary Embolism in the Perioperative Patient
 ...PRESENTATIONS... Deep Vein Thrombosis and Pulmonary Embolism in the Perioperative Patient Based on a presentation by James E. Muntz, MD Presentation Summary Approximately 500,000 cases of deep vein
...PRESENTATIONS... Deep Vein Thrombosis and Pulmonary Embolism in the Perioperative Patient Based on a presentation by James E. Muntz, MD Presentation Summary Approximately 500,000 cases of deep vein
General. Recommendations. Guideline Title. Bibliographic Source(s) Guideline Status. Major Recommendations
 Guideline Status. Major Recommendations") General Guideline Title Prevention of deep vein thrombosis and pulmonary embolism. Bibliographic Source(s) American College of Obstetricians and Gynecologists (ACOG). Prevention of deep vein thrombosis
General Guideline Title Prevention of deep vein thrombosis and pulmonary embolism. Bibliographic Source(s) American College of Obstetricians and Gynecologists (ACOG). Prevention of deep vein thrombosis
Deep vein thrombosis (DVT) and pulmonary embolism (PE) advice for ophthalmic surgery patients
 and pulmonary embolism (PE) advice for ophthalmic surgery patients") Deep vein thrombosis (DVT) and pulmonary embolism (PE) advice for ophthalmic surgery patients What is a deep vein thrombosis (DVT)? A DVT is a blood clot that forms within a vein deep in the leg but can
Deep vein thrombosis (DVT) and pulmonary embolism (PE) advice for ophthalmic surgery patients What is a deep vein thrombosis (DVT)? A DVT is a blood clot that forms within a vein deep in the leg but can
Deep Vein Thrombosis
 Deep Vein Thrombosis from NHS (UK) guidelines Introduction Deep vein thrombosis (DVT) is a blood clot in one of the deep veins in the body. Blood clots that develop in a vein are also known as venous thrombosis.
Deep Vein Thrombosis from NHS (UK) guidelines Introduction Deep vein thrombosis (DVT) is a blood clot in one of the deep veins in the body. Blood clots that develop in a vein are also known as venous thrombosis.
Implications from the ACCP 2012 Consensus Guidelines for the Management of Thrombosis: a case based approach
 Implications from the ACCP 2012 Consensus Guidelines for the Management of Thrombosis: a case based approach Prof. I. Baumgartner Head Clinical and Interventional Angiology About the ACCP guidelines Widely
Implications from the ACCP 2012 Consensus Guidelines for the Management of Thrombosis: a case based approach Prof. I. Baumgartner Head Clinical and Interventional Angiology About the ACCP guidelines Widely
Reducing the risk of venous thrombo-embolism (VTE) in hospital and after discharge
 in hospital and after discharge") Reducing the risk of venous thrombo-embolism (VTE) in hospital and after discharge What is a venous thromboembolism (VTE)? This is a medical term that describes a blood clot that develops in a deep vein
Reducing the risk of venous thrombo-embolism (VTE) in hospital and after discharge What is a venous thromboembolism (VTE)? This is a medical term that describes a blood clot that develops in a deep vein
Preventing Blood Clots in Adult Patients
 Manchester Royal Eye Hospital Surgical Services Information for Patients Preventing Blood Clots in Adult Patients This leaflet will give you information on how to reduce the risk of developing blood clots
Manchester Royal Eye Hospital Surgical Services Information for Patients Preventing Blood Clots in Adult Patients This leaflet will give you information on how to reduce the risk of developing blood clots
Thrombophilia. Diagnosis and Management. Kevin P. Hubbard, DO, FACOI
 Thrombophilia Diagnosis and Management Kevin P. Hubbard, DO, FACOI Clinical Professor of Medicine Kansas City University of Medicine and Biosciences-College of Osteopathic Medicine Kansas City, Missouri
Thrombophilia Diagnosis and Management Kevin P. Hubbard, DO, FACOI Clinical Professor of Medicine Kansas City University of Medicine and Biosciences-College of Osteopathic Medicine Kansas City, Missouri
Pulmonary Embolism. Pulmonary Embolism. Pulmonary Embolism. PE - Clinical
 Pulmonary embolus - a practical approach to investigation and treatment Sam Janes Wellcome Senior Fellow and Respiratory Physician, University College London Background Diagnosis Treatment Common: 50 cases
Pulmonary embolus - a practical approach to investigation and treatment Sam Janes Wellcome Senior Fellow and Respiratory Physician, University College London Background Diagnosis Treatment Common: 50 cases
Lower Limb Venous Ultrasound. Colin P. Griffin MSc, BSc (Hons)
") Lower Limb Venous Ultrasound Colin P. Griffin MSc, BSc (Hons) Peripheral Vessels Lower Limb Peripheral Vessels Lower Limb Venous Deep System Common Iliac External/Internal Iliac Common Femoral Femoral
Lower Limb Venous Ultrasound Colin P. Griffin MSc, BSc (Hons) Peripheral Vessels Lower Limb Peripheral Vessels Lower Limb Venous Deep System Common Iliac External/Internal Iliac Common Femoral Femoral
Pulmonary Thromboembolism
 Pulmonary Thromboembolism James Allen, MD Epidemiology of Pulmonary Embolism 1,500,000 new cases per year in the United States Often asymptomatic 300,000 deaths per year DVT or PE present in 10% of ICU
Pulmonary Thromboembolism James Allen, MD Epidemiology of Pulmonary Embolism 1,500,000 new cases per year in the United States Often asymptomatic 300,000 deaths per year DVT or PE present in 10% of ICU
VTE Management in Surgical Patients: Optimizing Prophylaxis Strategies
 VTE Management in Surgical Patients: Optimizing Prophylaxis Strategies VTE in Surgical Patients: Recognizing the Patients at Risk Pathogenesis of thrombosis: Virchow s triad and VTE Risk Hypercoagulability
VTE Management in Surgical Patients: Optimizing Prophylaxis Strategies VTE in Surgical Patients: Recognizing the Patients at Risk Pathogenesis of thrombosis: Virchow s triad and VTE Risk Hypercoagulability
VENOUS THROMBOEMBOLISM: DURATION OF TREATMENT
 VENOUS THROMBOEMBOLISM: DURATION OF TREATMENT OBJECTIVE: To provide guidance on the recommended duration of anticoagulant therapy for venous thromboembolism (VTE). BACKGROUND: Recurrent episodes of VTE
VENOUS THROMBOEMBOLISM: DURATION OF TREATMENT OBJECTIVE: To provide guidance on the recommended duration of anticoagulant therapy for venous thromboembolism (VTE). BACKGROUND: Recurrent episodes of VTE
Risk factors for DVT. Venous thrombosis & pulmonary embolism. Anticoagulation (cont d) Diagnosis 1/5/2018. Ahmed Mahmoud, MD
 Diagnosis 1/5/2018. Ahmed Mahmoud, MD") Risk factors for DVT Venous thrombosis & pulmonary embolism Ahmed Mahmoud, MD Surgery ; post op especially for long cases, pelvic operations (THR), Trauma ; long bone fractures, pelvic fractures (posterior
Risk factors for DVT Venous thrombosis & pulmonary embolism Ahmed Mahmoud, MD Surgery ; post op especially for long cases, pelvic operations (THR), Trauma ; long bone fractures, pelvic fractures (posterior
Venous thrombosis & pulmonary embolism. Ahmed Mahmoud, MD
 Venous thrombosis & pulmonary embolism Ahmed Mahmoud, MD Risk factors for DVT Surgery ; post op especially for long cases, pelvic operations (THR), Trauma ; long bone fractures, pelvic fractures (posterior
Venous thrombosis & pulmonary embolism Ahmed Mahmoud, MD Risk factors for DVT Surgery ; post op especially for long cases, pelvic operations (THR), Trauma ; long bone fractures, pelvic fractures (posterior
Mutidisciplinary cooperation on VTE prevention and managment
 Mutidisciplinary cooperation on VTE prevention and managment TAO YANG Dpartment of vascular surgery Shanxi DAYI Hospita Tai yuan Shanxi China Disclosure Speaker name: Tao Yang... I have the following potential
Mutidisciplinary cooperation on VTE prevention and managment TAO YANG Dpartment of vascular surgery Shanxi DAYI Hospita Tai yuan Shanxi China Disclosure Speaker name: Tao Yang... I have the following potential
Guideline Quick View: Venous Thromboembolism
 Guideline Quick View: Venous Thromboembolism The AORN Guideline Quick View is a key component of Guideline Essentials, a suite of online implementation tools designed to help the perioperative team translate
Guideline Quick View: Venous Thromboembolism The AORN Guideline Quick View is a key component of Guideline Essentials, a suite of online implementation tools designed to help the perioperative team translate
Interventional Treatment VTE: Radiologic Approach
 Interventional Treatment VTE: Radiologic Approach Hae Giu Lee, MD Professor, Dept of Radiology Seoul St. Mary s Hospital The Catholic University of Korea Introduction Incidence High incidence: 250,000-1,000,000/year
Interventional Treatment VTE: Radiologic Approach Hae Giu Lee, MD Professor, Dept of Radiology Seoul St. Mary s Hospital The Catholic University of Korea Introduction Incidence High incidence: 250,000-1,000,000/year
Outpatient Treatment of Deep Vein Thrombosis with Low Molecular Weight Heparin (LMWH) Clinical Practice Guideline August 2015
 Clinical Practice Guideline August 2015") Outpatient Treatment of Deep Vein Thrombosis with Low Molecular Weight Heparin (LMWH) Clinical Practice Guideline August 2015 General Principles: There is compelling data in the medical literature to support
Outpatient Treatment of Deep Vein Thrombosis with Low Molecular Weight Heparin (LMWH) Clinical Practice Guideline August 2015 General Principles: There is compelling data in the medical literature to support
Shared Care Protocol for the Prescription and Supply of Low Molecular Weight Heparins
 Tameside Hospital NHS Foundation Trust and NHS Tameside and Glossop Shared Care Protocol for the Prescription and Supply of Low Molecular Weight Heparins Version 5.2 Version: 5.2 Authorised by: Joint Medicines
Tameside Hospital NHS Foundation Trust and NHS Tameside and Glossop Shared Care Protocol for the Prescription and Supply of Low Molecular Weight Heparins Version 5.2 Version: 5.2 Authorised by: Joint Medicines
Low Molecular Weight Heparin for Prevention and Treatment of Venous Thromboembolic Disorders
 SURGICAL GRAND ROUNDS March 17 th, 2007 Low Molecular Weight Heparin for Prevention and Treatment of Venous Thromboembolic Disorders Guillermo Escobar, M.D. LMWH vs UFH Jayer s sales pitch: FALSE LMW is
SURGICAL GRAND ROUNDS March 17 th, 2007 Low Molecular Weight Heparin for Prevention and Treatment of Venous Thromboembolic Disorders Guillermo Escobar, M.D. LMWH vs UFH Jayer s sales pitch: FALSE LMW is
Pulmonary embolism. Paweł Balsam
 Pulmonary embolism Paweł Balsam Venous thromboembolism (VTE) Pulmonary embolism (PE) and deep vein thrombosis (DVT) are two clinical presentations of veonus thromboembolism Pulmonary embolism A pulmonary
Pulmonary embolism Paweł Balsam Venous thromboembolism (VTE) Pulmonary embolism (PE) and deep vein thrombosis (DVT) are two clinical presentations of veonus thromboembolism Pulmonary embolism A pulmonary
Obesity, renal failure, HIT: which anticoagulant to use?
 Obesity, renal failure, HIT: which anticoagulant to use? Mark Crowther with thanks to Dr David Garcia and others. This Photo by Unknown Author is licensed under CC BY-SA 1 2 Drug choices The DOACs have
Obesity, renal failure, HIT: which anticoagulant to use? Mark Crowther with thanks to Dr David Garcia and others. This Photo by Unknown Author is licensed under CC BY-SA 1 2 Drug choices The DOACs have
Is Oral Rivaroxaban Safe and Effective in the Treatment of Patients with Symptomatic DVT?
 Philadelphia College of Osteopathic Medicine DigitalCommons@PCOM PCOM Physician Assistant Studies Student Scholarship Student Dissertations, Theses and Papers 1-1-2013 Is Oral Rivaroxaban Safe and Effective
Philadelphia College of Osteopathic Medicine DigitalCommons@PCOM PCOM Physician Assistant Studies Student Scholarship Student Dissertations, Theses and Papers 1-1-2013 Is Oral Rivaroxaban Safe and Effective
Anticoagulation for prevention of venous thromboembolism
 Anticoagulation for prevention of venous thromboembolism Original article by: Michael Tam Note: updated in June 2009 with the eighth edition (from the seventh) evidence-based clinical practice guidelines
Anticoagulation for prevention of venous thromboembolism Original article by: Michael Tam Note: updated in June 2009 with the eighth edition (from the seventh) evidence-based clinical practice guidelines
Deep Vein Thrombosis and Pulmonary Embolism: Patient Information
 Deep Vein Thrombosis and Pulmonary Embolism: Patient Information A Deep Vein Thrombosis (DVT) and a Pulmonary Embolism (PE) are both disorders of unwanted blood clotting. Unwanted blood clots can occur
Deep Vein Thrombosis and Pulmonary Embolism: Patient Information A Deep Vein Thrombosis (DVT) and a Pulmonary Embolism (PE) are both disorders of unwanted blood clotting. Unwanted blood clots can occur
Early Ambulation Reduces the Risk of Venous Thromboembolism After Total Knee Replacement. Marilyn Szekendi, PhD, RN
 Early Ambulation Reduces the Risk of Venous Thromboembolism After Total Knee Replacement Marilyn Szekendi, PhD, RN ANA 7 th Annual Nursing Quality Conference, February 2013 Research Team Banafsheh Sadeghi,
Early Ambulation Reduces the Risk of Venous Thromboembolism After Total Knee Replacement Marilyn Szekendi, PhD, RN ANA 7 th Annual Nursing Quality Conference, February 2013 Research Team Banafsheh Sadeghi,
Trombosi venose superficiali e trombosi venose distali
 XXIV Congresso Nazionale SISET Abano 9-12 Novembre 2016 Trombosi venose superficiali e trombosi venose distali Gualtiero Palareti / Benilde Cosmi Università di Bologna Superficial vein thrombosis (SVT):
XXIV Congresso Nazionale SISET Abano 9-12 Novembre 2016 Trombosi venose superficiali e trombosi venose distali Gualtiero Palareti / Benilde Cosmi Università di Bologna Superficial vein thrombosis (SVT):
ED Diagnosis of DVT or tools to rule out DVT in your ED
 ED Diagnosis of DVT or tools to rule out DVT in your ED Ralph Wang UCSF Department of Emergency Medicine 53 yo f c/o left leg swelling recent cholecystectomy its midnight how do you manage this patient?
ED Diagnosis of DVT or tools to rule out DVT in your ED Ralph Wang UCSF Department of Emergency Medicine 53 yo f c/o left leg swelling recent cholecystectomy its midnight how do you manage this patient?
NICE Guidance: Venous thromboembolism (deep vein thrombosis and pulmonary embolism) in patients admitted to hospital 1
 in patients admitted to hospital 1") The College of Emergency Medicine Patron: HRH The Princess Royal Churchill House Tel +44 (0)207 404 1999 35 Red Lion Square Fax +44 (0)207 067 1267 London WC1R 4SG www.collemergencymed.ac.uk CLINICAL EFFECTIVENESS
The College of Emergency Medicine Patron: HRH The Princess Royal Churchill House Tel +44 (0)207 404 1999 35 Red Lion Square Fax +44 (0)207 067 1267 London WC1R 4SG www.collemergencymed.ac.uk CLINICAL EFFECTIVENESS
PULMONARY EMBOLISM -CASE REPORT-
 University Goce Delcev, Faculty of Medical sciences, Stip University Clinic of Cardiology, Skopje R. Of Macedonia PULMONARY EMBOLISM -CASE REPORT- Gordana Kamceva MD mr.sci Acknowledgment Marija Vavlukis
University Goce Delcev, Faculty of Medical sciences, Stip University Clinic of Cardiology, Skopje R. Of Macedonia PULMONARY EMBOLISM -CASE REPORT- Gordana Kamceva MD mr.sci Acknowledgment Marija Vavlukis
Handbook for Venous Thromboembolism
 Handbook for Venous Thromboembolism Gregory Piazza Benjamin Hohlfelder Samuel Z. Goldhaber Handbook for Venous Thromboembolism Gregory Piazza Cardiovascular Division Harvard Medical School Brigham and
Handbook for Venous Thromboembolism Gregory Piazza Benjamin Hohlfelder Samuel Z. Goldhaber Handbook for Venous Thromboembolism Gregory Piazza Cardiovascular Division Harvard Medical School Brigham and
PREVENTION AND TREATMENT OF VENOUS THROMBOEMBOLISM
 PREVENTION AND TREATMENT OF VENOUS THROMBOEMBOLISM International Consensus Statement 2013 Guidelines According to Scientific Evidence Developed under the auspices of the: Cardiovascular Disease Educational
PREVENTION AND TREATMENT OF VENOUS THROMBOEMBOLISM International Consensus Statement 2013 Guidelines According to Scientific Evidence Developed under the auspices of the: Cardiovascular Disease Educational
Updates in Medical Management of Pulmonary Embolism and Deep Vein Thrombosis. By: Justin Youtsey, Elliott Reiff, William Montgomery, Grant Finlan
 Updates in Medical Management of Pulmonary Embolism and Deep Vein Thrombosis By: Justin Youtsey, Elliott Reiff, William Montgomery, Grant Finlan Objectives Describe the prevalence of PE and DVT as it relates
Updates in Medical Management of Pulmonary Embolism and Deep Vein Thrombosis By: Justin Youtsey, Elliott Reiff, William Montgomery, Grant Finlan Objectives Describe the prevalence of PE and DVT as it relates
PULMONARY EMBOLISM MANAGEMENT GUIDELINES
 PULMONARY EMBOLISM MANAGEMENT GUIDELINES This document is adapted from the NICE guidelines titled Venous thromboembolic diseases: the management of venous thromboembolic diseases and the role of thrombophilia
PULMONARY EMBOLISM MANAGEMENT GUIDELINES This document is adapted from the NICE guidelines titled Venous thromboembolic diseases: the management of venous thromboembolic diseases and the role of thrombophilia
PULMONARY EMBOLISM/VTE CARE PROCESS MODEL
 PULMONARY EMBOLISM/VTE CARE PROCESS MODEL IMCP FALL CONFERENCE 2017 Scott Stevens, MD Co-Director, Thrombosis Clinic & Thrombosis Research Group Intermountain Medical Center Professor of Clinical Medicine
PULMONARY EMBOLISM/VTE CARE PROCESS MODEL IMCP FALL CONFERENCE 2017 Scott Stevens, MD Co-Director, Thrombosis Clinic & Thrombosis Research Group Intermountain Medical Center Professor of Clinical Medicine
Treatment Options and How They Work
 Treatment Options and How They Work Robin Offord Director of Clinical Pharmacy UCL Hospitals NHS Foundation Trust robin.offord@uclh.nhs.uk Introducing the term anticoagulant... What they do Inhibit the
Treatment Options and How They Work Robin Offord Director of Clinical Pharmacy UCL Hospitals NHS Foundation Trust robin.offord@uclh.nhs.uk Introducing the term anticoagulant... What they do Inhibit the
Simplified approach to investigation of suspected VTE
 Simplified approach to investigation of suspected VTE Diagnosis of DVT and PE THSNA 2016, Chicago 15 April 2016 Clive Kearon, McMaster University, Canada Relevant Disclosures Research Support/P.I. Employee
Simplified approach to investigation of suspected VTE Diagnosis of DVT and PE THSNA 2016, Chicago 15 April 2016 Clive Kearon, McMaster University, Canada Relevant Disclosures Research Support/P.I. Employee
What is the real place of venous echo Doppler in aircrew member flying rehabilitation after a thromboembolism event?
 89 th ASMA ANNUAL SCIENTIFIC MEETING DALLAS- May 6-10, 2018 What is the real place of venous echo Doppler in aircrew member flying rehabilitation after a thromboembolism event? S BISCONTE (1), V MARICOURT
89 th ASMA ANNUAL SCIENTIFIC MEETING DALLAS- May 6-10, 2018 What is the real place of venous echo Doppler in aircrew member flying rehabilitation after a thromboembolism event? S BISCONTE (1), V MARICOURT
Prevention of Venous Thromboembolism
 Prevention of Venous Thromboembolism Surgical Care Improvement Project Dale W. Bratzler, DO, MPH President and CEO Dale W. Bratzler, DO, MPH Oklahoma Foundation for Medical Quality QIOSC Medical Director
Prevention of Venous Thromboembolism Surgical Care Improvement Project Dale W. Bratzler, DO, MPH President and CEO Dale W. Bratzler, DO, MPH Oklahoma Foundation for Medical Quality QIOSC Medical Director
DVT Diagnosis. Reference methods. Whole leg Ultrasonography. Predictive values. Page 1. Diagnosis of 1 st time symptomatic DVT.
 DVT Diagnosis Ulf Nyman Associate Professor Lund University Department of Radiology East Division (Kristianstad, HässleholmH Trelleborg, Ystad) Sweden Diagnosis of 1 st time symptomatic DVT Scientific
DVT Diagnosis Ulf Nyman Associate Professor Lund University Department of Radiology East Division (Kristianstad, HässleholmH Trelleborg, Ystad) Sweden Diagnosis of 1 st time symptomatic DVT Scientific
TRANSPARENCY COMMITTEE OPINION. 18 April 2007
 The legally binding text is the original French version TRANSPARENCY COMMITTEE OPINION 18 April 2007 ARIXTRA 2.5 mg/0.5 ml, solution for injection in prefilled syringe Pack of 2 (CIP: 359 225-4) Pack of
The legally binding text is the original French version TRANSPARENCY COMMITTEE OPINION 18 April 2007 ARIXTRA 2.5 mg/0.5 ml, solution for injection in prefilled syringe Pack of 2 (CIP: 359 225-4) Pack of
Management of Post-Thrombotic Syndrome
 Management of Post-Thrombotic Syndrome Thanainit Chotanaphuti Phramongkutklao College of Medicine Bangkok, Thailand President of CAOS Asia President of Thai Hip & Knee Society President of ASEAN Arthroplasty
Management of Post-Thrombotic Syndrome Thanainit Chotanaphuti Phramongkutklao College of Medicine Bangkok, Thailand President of CAOS Asia President of Thai Hip & Knee Society President of ASEAN Arthroplasty
DVT Primary Care Prescribing Pathway
 DVT Primary Care Prescribing Pathway Scope Classification Author Health Economy Wide Guideline East Lancashire Medicines Management Board (Reviewed December 207) Authorised by ELMMB Date February 208 Reviewed
DVT Primary Care Prescribing Pathway Scope Classification Author Health Economy Wide Guideline East Lancashire Medicines Management Board (Reviewed December 207) Authorised by ELMMB Date February 208 Reviewed
DOPPLER ULTRASOUND OF DEEP VENOUS THROMBOSIS
 TOKUDA HOSPITAL SOFIA DOPPLER ULTRASOUND OF DEEP VENOUS THROMBOSIS MILENA STANEVA, MD, PhD Department of vascular surgery and angiology Venous thromboembolic disease continues to cause significant morbidity
TOKUDA HOSPITAL SOFIA DOPPLER ULTRASOUND OF DEEP VENOUS THROMBOSIS MILENA STANEVA, MD, PhD Department of vascular surgery and angiology Venous thromboembolic disease continues to cause significant morbidity
Duration of anticoagulation
 Duration of anticoagulation P. Fontana Service d angiologie et d hémostase Hôpitaux Universitaires de Genève Pomeriggio formativo in coagulazione, Bellinzona, 19.10.2017 Conflict of interest AstraZeneca,
Duration of anticoagulation P. Fontana Service d angiologie et d hémostase Hôpitaux Universitaires de Genève Pomeriggio formativo in coagulazione, Bellinzona, 19.10.2017 Conflict of interest AstraZeneca,
Pulmonary Embolism Pathway
 Pulmonary Embolism Pathway Ambulatory Care Pathway Dr. A. Zafar, Dr. A. Rehman, Dr. T. Malik September, 2011. Patient Identification Label Pulmonary Embolism Pathway Clinical History Comments Hospital
Pulmonary Embolism Pathway Ambulatory Care Pathway Dr. A. Zafar, Dr. A. Rehman, Dr. T. Malik September, 2011. Patient Identification Label Pulmonary Embolism Pathway Clinical History Comments Hospital
Thromboembolic prophylaxis
 .6 1 General topics Vein thrombosis in orthopedic trauma surgery 35 1.1 Introduction 35 1.2 History 35 2 Clinically important outcomes 35 2.1 Deep vein thrombosis (DVT) 35 2.2 Pulmonary embolism (PE) 35
.6 1 General topics Vein thrombosis in orthopedic trauma surgery 35 1.1 Introduction 35 1.2 History 35 2 Clinically important outcomes 35 2.1 Deep vein thrombosis (DVT) 35 2.2 Pulmonary embolism (PE) 35
Venous Thromboembolic Disease Update
 Canadian Society of Internal Medicine Annual Meeting Calgary, Alberta, October 2014 Venous Thromboembolic Disease Update Benjamin Bell, MD FRCPC James Douketis, MD FRCPC On Behalf of Thrombosis Canada
Canadian Society of Internal Medicine Annual Meeting Calgary, Alberta, October 2014 Venous Thromboembolic Disease Update Benjamin Bell, MD FRCPC James Douketis, MD FRCPC On Behalf of Thrombosis Canada
Venous thromboembolic diseases: diagnosis, management and thrombophilia testing (2012) NICE guideline CG144
 NICE guideline CG144") Venous thromboembolic diseases: diagnosis, management and thrombophilia testing (2012) NICE guideline CG144 Appendix A: Summary of new evidence from Summary of evidence from previous year Diagnosis Diagnostic
Venous thromboembolic diseases: diagnosis, management and thrombophilia testing (2012) NICE guideline CG144 Appendix A: Summary of new evidence from Summary of evidence from previous year Diagnosis Diagnostic
Pulmonary embolism. Paweł Balsam MD, PhD
 Pulmonary embolism Paweł Balsam MD, PhD Venous thromboembolism (VTE) Pulmonary embolism (PE) and deep vein thrombosis (DVT) are two clinical presentations of veonus thromboembolism Pulmonary embolism A
Pulmonary embolism Paweł Balsam MD, PhD Venous thromboembolism (VTE) Pulmonary embolism (PE) and deep vein thrombosis (DVT) are two clinical presentations of veonus thromboembolism Pulmonary embolism A
Cover Page. The handle holds various files of this Leiden University dissertation.
 Cover Page The handle http://hdl.handle.net/1887/19768 holds various files of this Leiden University dissertation. Author: Langevelde, Kirsten van Title: Are pulmonary embolism and deep-vein thrombosis
Cover Page The handle http://hdl.handle.net/1887/19768 holds various files of this Leiden University dissertation. Author: Langevelde, Kirsten van Title: Are pulmonary embolism and deep-vein thrombosis
Low-Molecular-Weight Heparin
 Low-Molecular-Weight Heparin Policy Number: Original Effective Date: MM.04.019 10/15/2007 Line(s) of Business: Current Effective Date: HMO; PPO; QUEST Integration 05/01/2016 Section: Prescription Drugs
Low-Molecular-Weight Heparin Policy Number: Original Effective Date: MM.04.019 10/15/2007 Line(s) of Business: Current Effective Date: HMO; PPO; QUEST Integration 05/01/2016 Section: Prescription Drugs
Venous Thromboembolism. Prevention
 Venous Thromboembolism Prevention August 2010 Venous Thromboembloism Prevention 1 1 Expected Practice Assess all patients upon admission to the ICU for risk factors of venous thromboembolism (VTE) and
Venous Thromboembolism Prevention August 2010 Venous Thromboembloism Prevention 1 1 Expected Practice Assess all patients upon admission to the ICU for risk factors of venous thromboembolism (VTE) and
DISORDERS OF VENOUS SYSTEM
 DISORDERS OF VENOUS SYSTEM Varicose Veins Any dilated, elongated and tortuous vein irrespective of size Varicose veins are common in the superficial veins of the leg which are subject to high pressure
DISORDERS OF VENOUS SYSTEM Varicose Veins Any dilated, elongated and tortuous vein irrespective of size Varicose veins are common in the superficial veins of the leg which are subject to high pressure
Medical Patients: A Population at Risk
 Case Vignette A 68-year-old woman with obesity was admitted to the Medical Service with COPD and pneumonia and was treated with oral corticosteroids, bronchodilators, and antibiotics. She responded well
Case Vignette A 68-year-old woman with obesity was admitted to the Medical Service with COPD and pneumonia and was treated with oral corticosteroids, bronchodilators, and antibiotics. She responded well