Ocular Injuries in Sports. Rance McClain, D.O. Associate Dean, Clinical Sciences William Carey University FM/NMM-OMM/Sports Medicine
|
|
|
- Edwin Bryan
- 5 years ago
- Views:
Transcription
1 Ocular Injuries in Sports Rance McClain, D.O. Associate Dean, Clinical Sciences William Carey University FM/NMM-OMM/Sports Medicine

2
3 Learning Objectives 1. Know the sport classification and risk of ocular injury 2. Discuss the most common mechanisms of ocular trauma in sports 3. Know the prevention and treatment of sports related ocular injuries 4. Be able to conduct an on site evaluation of ocular injuries (Workshop material)
4
5 Background 40,000+ sports related ocular injuries annually seen in the emergency department 90% are considered preventable 30% of eye injuries in those under 16 years of age are related to sports participation 5-14 years old = baseball years old = basketball
6 Sport Classification Collision football, rugby, hockey, lacrosse Contact baseball, soccer, basketball, wrestling Noncontact cross-country running, track, tennis, crew, swimming Other bowling, golf, archery, field events
7 Sport Classification Misleading when used in the context of possible ocular injuries Hockey has lower incidence due to the use of proper protective equipment Golf and racquet sports are at higher risk for injury
8 Sport Classification Eye Risk Low risk no use of ball, puck, bat, stick, or racquet and no contact track/field, swimming, gymnastics, and cycling High risk baseball, hockey, football, basketball, lacrosse, racquet sports, tennis, fencing, golf, and water polo
9 Sport Classification Eye Risk Very high risk boxing, wrestling, and contact martial arts Frequent high impact trauma to the eye and no eye protection typically worn
10 Functionally One-Eyed Athletes Considered monocular when best corrected vision in weakest eye is 20/40 Must wear eye protection which meets ASTM (American Society for Testing and Materials) racquet sports standards when participating in events Under face mask in sports requiring such equipment Recommend protective lens use at ALL times
11 Functionally One-Eyed Athletes Very high risk sports are contraindicated due to lack of proper protective equipment ASTM has multiple classifications for different sports DO NOT confuse ASTM ratings with ANSI (American National Standards Institute) which do not write standards for sports eyewear, but do write standards for other protective eyewear
12 ASTM Standards Eye protectors must shift impact from the eyes and the face to the skull without causing intracranial injury May be necessary to integrate into helmet Hockey, football, baseball and lacrosse Must be acceptable to the athlete, not change the appeal of the game, and not generate unacceptable liability

13
14 ASTM Standards Polycarbonate Highly impact-resistant plastic 2mm thickness in low risk sports 3mm thickness in high risk sports Withstand ball at 45mph-youth, 55-mid, 85-adult Capable of absorbing ultraviolet light Available in prescription and nonprescription lenses Multiple standards for particular sports
15 Injury Mechanisms Blunt trauma Most common mechanism Examples Blowout fracture, contusions, iris injury, ruptured globe, traumatic iritis, subconjunctival hemorrhage, hyphema, retinal hemorrhage, commotio retinae, vitreous hemorrhage, choroidal rupture, retinal tears, and retinal detachment
16 Injury Mechanisms Blunt Trauma Damage depends on size, hardness and velocity of the blunt object and the force imparted directly to the eye Objects smaller than the orbital opening cause rapid AP compression and dilation of the middle globe, transferring force to the internal structures Objects larger than the orbital opening exert force on the floor of the orbit or medial wall and cause fracture of the thin bones Prevents rupture of the globe


17 Blunt Trauma Minor external trauma in the presence of severe ocular injury. The eye of the patient in the top view had no light perception and a large afferent pupillary defect from an avulsed optic nerve


18 Blunt Trauma Ruptured globe caused by golf ball The patient has transmarginal eyelid lacerations, a corneascleral laceration, and prolapsed uvea on the eyelid.


19 Blunt Trauma Extensive subconjunctival hemorrhage can be a sign of occult globe rupture Hyphema


20 Blunt Trauma Commotio retinae, seen as a whitish change in the retina after blunt trauma. This is believed to be caused by disorganization at the photoreceptor level Choroidal rupture resulting from blunt trauma. A late complication, choroidal neovascular membrane (dark area surrounding the rupture) can affect vision.
21 Penetrating Injuries Relatively uncommon Can occur with large projectiles Eye glass breakage from improper eyewear Fishing hooks Canalicular lacerations usually occur because of trauma from a fellow player's finger in the area of the medial canthus


22 Penetrating Injuries Fishing hook in the left eye. The hook was appropriately taped to the patient's forehead, a shield was placed, and immediate ophthalmologic referral was obtained Corneal abrasion with fluorescein stain
23 Radiation Injuries Result of exposure to ultraviolet light in snow skiing, water skiing, and other water sports Pinguecula: They are yellow-white, amorphous, subepithelial deposits of abnormal collagen at the interpalpebral limbus, which may be calcified Pterygium: raised, wedge-shaped growth of the conjunctiva. Grows over the central cornea and affects the vision. As the pterygium develops, it may alter the shape of the cornea, causing astigmatism. If the pterygium invades the central cornea, it is removed surgically


24 Radiation Injuries Pinguecula Pterygium
25 Immediate Referral Sudden decrease in or loss of vision Loss of field of vision Pain on movement of the eye Photophobia Diplopia Proptosis of the eye Light flashes or floaters Irregularly shaped pupil Suspected globe perforation Foreign-body sensation/embedded foreign body Red and inflamed eye Hyphema (blood in anterior chamber) Halos around lights (corneal edema) Laceration of the lid margin or near medial canthus Subconjunctival hemorrhage Broken contact lens or shattered eyeglasses
26 Hands on workshop for ocular evaluation and injuries
27 Ocular Sports Examination During the workshop we will cover Ocular preparticipation history Standard aspects of the PPE examination Special vision testing for athletes What equipment can/should be in your bag On field techniques and care
28 Preparticipation Examination Ocular history (simple) Problems with eyes or vision? Wear glasses or contacts? Wear protective eyewear? Ocular history (more in depth) Hyperopia/myopia, surgical aphakia (loss of lens), retinal detachment, eye surgery, and injury or infection Family history of retinal detachment, retinal tears, and diabetic retinopathy
29 Preparticipation Examination Complete eye exam Acuity Visual fields Motor control External exam Anisocoria (unequal pupils) Funduscopic exam *Testing for color blindness
30
31 Ocular First Aid List for Team Physician Bag
32 On Site Evaluation History Mechanism of injury Object Force Direction of impact Best-corrected visual acuity pre-injury if known Visual field Defects suggest a retinal, optic nerve, or central nervous system injury
33 On Site Evaluation Pupil examination Anisocoria, light reflex and consensual light reflex Pupil irregularity is almost always pathologic A deafferented pupil constricts consensually, but not to direct light, paradoxically enlarging when the light is quickly brought from the unaffected side (Marcus Gunn pupil). An efferent lesion prevents direct and consensual constriction while the unaffected eye maintains both.

34 On Site Evaluation Penlight examination of the anterior chamber Foreign bodies Hyphema Abrasions Lacerations
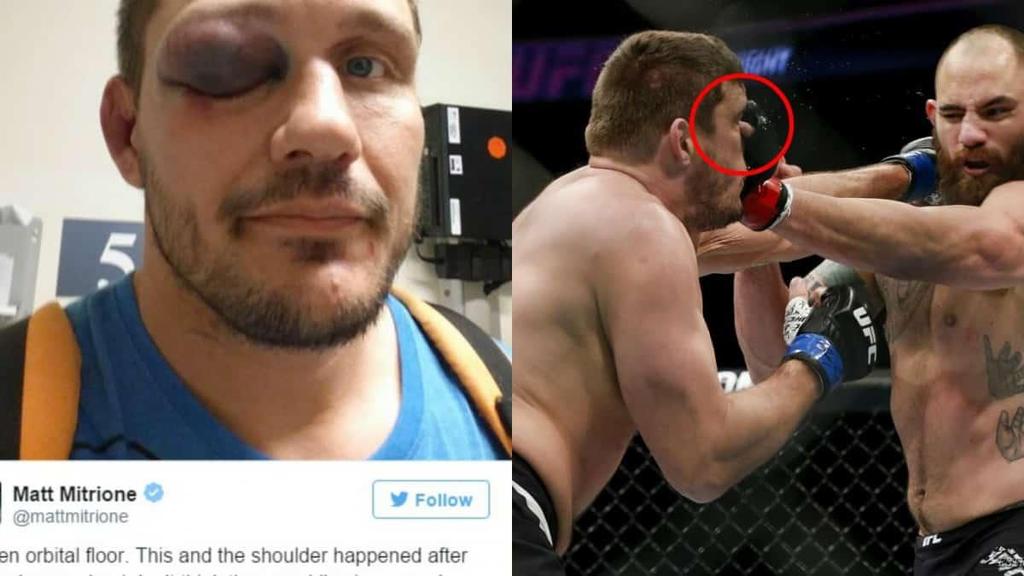
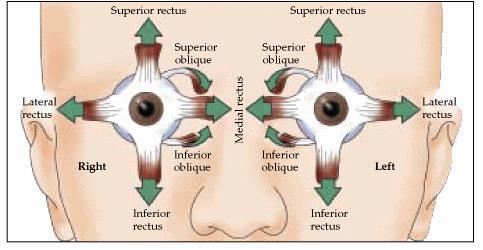
35 On Site Evaluation Both eyes should have full motility in all positions of gaze. Elevation of gaze may be limited by an orbital floor fracture. Double vision in any gaze position suggests significant injury in one or both eyes
36 On Site Evaluation External examination Periorbital ecchymosis, edema, proptosis, and bony step-off of the orbital rim. Trismus, or pain when opening the mouth, often occurs with fractures of the lateral wall of the orbit. Paresthesia in the CN V2 (infraorbital) distribution of the trigeminal nerve suggests a fracture of the orbital floor

37
38 On Site Evaluation Funduscopic examination Evaluate the red reflex Even modest bleeding into the ocular media can alter or obscure This may be the only sign of occult rupture of the globe Any alteration of the red reflex requires immediate ophthalmologic referral
39 Treatment Corneal abrasion fluorescent exam with cobalt blue light antibiotic ointment 24 hour ophthalmologic followup Superficial corneal foreign body sterile irrigating solution or moistened sterile cotton swab antibiotic ointment 24 hour ophthalmologic followup
40 Treatment Concealed foreign object suggested by vertical linear corneal abrasions Evert upper eyelid Sterile irrigating solution or moistened sterile cotton swab Follow Corneal abrasion guidelines
41 Treatment Superficial eyelid laceration Rule out globe injury Reapproximate superficial lacerations not involving lid margins Full thickness lacerations, especially involving the lid margin, warrant immediate referral Hyphema Shield the eye and refer immediately
42 Treatment Burns Classic signs of UV burn are intense pain, photophobia, and delay in symptom onset Fine punctate staining with fluorescein is characteristic. Treat with systemic analgesics and topical antibiotic. Refer if epithelial defect is present
43 Treatment Blunt Trauma Look for facial fractures and globe injuries If no signs of orbital fracture or optic neuropathy are present, use rest, analgesics, and cold compresses to control further edema and discomfort
44 Return To Play In patients with significant ocular injury, a full examination and clearance by an ophthalmologist are required. The injured eye should feel comfortable and have adequate return of vision. Eye protectors must be worn.
45 Return To Play During the game, immediate return to play depends on the athlete's symptoms and the nature of the injury as determined by the team physician. Athletes should never be allowed to use topical anesthetics to prolong play
46 References 1. Prevention and Treatment of Common Eye Injuries in Sports. American Family Physician Volume 67, Number 7 / April 1, Standard Specification for Eye Protectors for Selected Sports. American Society for Testing and Materials. ASTM Standard F803-11, ASTM International, West Conshohocken, PA, DOI: /F The Physician and Sportsmedicine Volume 28, Number 6 / June Preparticipation Physical Evaluation (AAP)- 4 th edition
47 Thank you and May the Force be with you!
EYE INJURIES OBJECTIVES COMMON EYE EMERGENCIES 7/19/2017 IMPROVE ASSESSMENT OF EYE INJURIES
 EYE INJURIES BRITTA ANDERSON D.O. DMC PRIMARY CARE SPORTS MEDICINE ASSOCIATE TEAM PHYSICIAN DETROIT TIGERS OBJECTIVES IMPROVE ASSESSMENT OF EYE INJURIES UNDERSTAND WHAT IS CONSIDERED AN EMERGENCY DEVELOP
EYE INJURIES BRITTA ANDERSON D.O. DMC PRIMARY CARE SPORTS MEDICINE ASSOCIATE TEAM PHYSICIAN DETROIT TIGERS OBJECTIVES IMPROVE ASSESSMENT OF EYE INJURIES UNDERSTAND WHAT IS CONSIDERED AN EMERGENCY DEVELOP
Ocular and Periocular Trauma. Tina Rutar, MD. Assistant Professor of Ophthalmology and Pediatrics. Director, Visual Center for the Child
 Ocular and Periocular Trauma Tina Rutar, MD Assistant Professor of Ophthalmology and Pediatrics Director, Visual Center for the Child University of California, San Francisco Phone: 415-353-2560 Fax: 415-353-2468
Ocular and Periocular Trauma Tina Rutar, MD Assistant Professor of Ophthalmology and Pediatrics Director, Visual Center for the Child University of California, San Francisco Phone: 415-353-2560 Fax: 415-353-2468
Ocular and periocular trauma
 Ocular and periocular trauma No financial disclosures. Tina Rutar M.D. Assistant Professor of Clinical Ophthalmology and Pediatrics Director, Visual Center for the Child University of California San Francisco
Ocular and periocular trauma No financial disclosures. Tina Rutar M.D. Assistant Professor of Clinical Ophthalmology and Pediatrics Director, Visual Center for the Child University of California San Francisco
EYE TRAUMA: INCIDENCE
 Introduction EYE TRAUMA: INCIDENCE 2.5 million eye injuries per year in U.S. 40,000 60,000 of eye injuries lead to visual loss Introduction Final visual outcome of many ocular emergencies depends on prompt,
Introduction EYE TRAUMA: INCIDENCE 2.5 million eye injuries per year in U.S. 40,000 60,000 of eye injuries lead to visual loss Introduction Final visual outcome of many ocular emergencies depends on prompt,
MRI masterfile Part 5 WM Heme Strokes.ppt 1
 Ocular and Orbital Trauma Eye Trauma: Incidence 1.3 million eye injuries in the US per year. 40,000 of these injuries lead to blindness in the US. Patrick Sibony, MD March 23, 2013 Ophthalmic Emergencies
Ocular and Orbital Trauma Eye Trauma: Incidence 1.3 million eye injuries in the US per year. 40,000 of these injuries lead to blindness in the US. Patrick Sibony, MD March 23, 2013 Ophthalmic Emergencies
UC SF. g h. Eye Trauma. Martha Neighbor, MD Emergency Services San Francisco General Hospital University of California
 UC SF Eye Trauma sf g h Martha Neighbor, MD Emergency Services San Francisco General Hospital University of California Goals Recognize vision threatening eye emergencies Treat them when we can Know when
UC SF Eye Trauma sf g h Martha Neighbor, MD Emergency Services San Francisco General Hospital University of California Goals Recognize vision threatening eye emergencies Treat them when we can Know when
Assessment and Management of Ocular Trauma. Disclosure I have no direct financial interests in today s subject matter. 3/25/2019. Normal Eye Anatomy
 Assessment and Management of Ocular Trauma Samiksha Fouzdar Jain, MD,FRCS Department of Ophthalmology & Visual Sciences Truhlsen Eye Institute Disclosure I have no direct financial interests in today s
Assessment and Management of Ocular Trauma Samiksha Fouzdar Jain, MD,FRCS Department of Ophthalmology & Visual Sciences Truhlsen Eye Institute Disclosure I have no direct financial interests in today s
Ophthalmic Trauma Update
 Ophthalmic Trauma Update Richard S. Davidson, M.D. Professor of Ophthalmology Vice Chair for Quality and Clinical Affairs UCHealth Eye Center University of Colorado School of Medicine August 5, 2017 Financial
Ophthalmic Trauma Update Richard S. Davidson, M.D. Professor of Ophthalmology Vice Chair for Quality and Clinical Affairs UCHealth Eye Center University of Colorado School of Medicine August 5, 2017 Financial
MRI masterfile Part 5 WM Heme Strokes.ppt 2
 Imaging of Orbital Trauma Corneal Abrasion CT scan is preferable to MRI Bone, Rapid, Easy to monitor patient Foreign bodies, air, hemorrhage Fractures Cost Needed for an MRI MRI Globe and intraocular injuries
Imaging of Orbital Trauma Corneal Abrasion CT scan is preferable to MRI Bone, Rapid, Easy to monitor patient Foreign bodies, air, hemorrhage Fractures Cost Needed for an MRI MRI Globe and intraocular injuries
Management of specific eye problems in the ED
 of specific eye problems in the ED CORNEAL ABRASION Causes Foreign bodies Tangential shearing injuries, e.g. poking finger into eye Exact cause of injury (Remember to exclude possibility of intraocular
of specific eye problems in the ED CORNEAL ABRASION Causes Foreign bodies Tangential shearing injuries, e.g. poking finger into eye Exact cause of injury (Remember to exclude possibility of intraocular
2/5/2018. Trauma. Subdivided into two main categories: Closed globe Open Globe
 1 2 3 4 5 Ocular Trauma Guide for Eye Care Office Staff Winter Thaw 2018 Aaron Yatskevich OD Definition A broad term used to describe a physical or chemical wound to the eye or eye socket. Ocular trauma
1 2 3 4 5 Ocular Trauma Guide for Eye Care Office Staff Winter Thaw 2018 Aaron Yatskevich OD Definition A broad term used to describe a physical or chemical wound to the eye or eye socket. Ocular trauma
Ocular Urgencies and Emergencies
 Ocular Urgencies and Emergencies Pam Boyce, O.D., F.A.A.O. Boyce Family Eye Care, Ltd. 528 Devon Ave. Park Ridge, IL 60068 847-518-0303 Somebody s going to lose an eye Epidemiology 2.4 million ocular and
Ocular Urgencies and Emergencies Pam Boyce, O.D., F.A.A.O. Boyce Family Eye Care, Ltd. 528 Devon Ave. Park Ridge, IL 60068 847-518-0303 Somebody s going to lose an eye Epidemiology 2.4 million ocular and
ation is essential. Whether on the playing it is important to keep in mind that severe
 JENNIFER LAIO, MD, and BRUCE M. ZAGELBAUM, MD NYU School of Medicine, Manhasset, NY North Shore University Hospital, Eye injuries sustained in sports and recreational activities are common in the United
JENNIFER LAIO, MD, and BRUCE M. ZAGELBAUM, MD NYU School of Medicine, Manhasset, NY North Shore University Hospital, Eye injuries sustained in sports and recreational activities are common in the United
Acute Eyes for ED. Enis Kocak. The Alfred Ophthalmology
 Acute Eyes for ED Enis Kocak The Alfred Ophthalmology The problem with eyes Things to cover Ocular anatomy Basic assessment Common presentations Eye first aid and procedures Ophthalmic emergencies What
Acute Eyes for ED Enis Kocak The Alfred Ophthalmology The problem with eyes Things to cover Ocular anatomy Basic assessment Common presentations Eye first aid and procedures Ophthalmic emergencies What
OPHTHALMOLOGY REFERRAL GUIDE FOR GPS
 OPHTHALMOLOGY REFERRAL GUIDE FOR GPS A guidebook to support general practitioners in the management and referral of a range of common eye problems. Contents 3 Introduction 4 Ophthalmic Workup 6 Acute Visual
OPHTHALMOLOGY REFERRAL GUIDE FOR GPS A guidebook to support general practitioners in the management and referral of a range of common eye problems. Contents 3 Introduction 4 Ophthalmic Workup 6 Acute Visual
5/2/2016 EYE EMERGENCIES. Nathaniel Pelsor, O.D., FAAO Talley Medical-Surgical Eye Care Associates. Anatomy. Tools
 EYE EMERGENCIES Nathaniel Pelsor, O.D., FAAO Talley Medical-Surgical Eye Care Associates Anatomy Tools 1 Contact dermatitis Blepharitis HSV Preseptal Cellulitis Anterior Chamber Subconjunctival hemorrhage
EYE EMERGENCIES Nathaniel Pelsor, O.D., FAAO Talley Medical-Surgical Eye Care Associates Anatomy Tools 1 Contact dermatitis Blepharitis HSV Preseptal Cellulitis Anterior Chamber Subconjunctival hemorrhage
Ocular Emergencies. What is an emergency to the patient is not necessarily an emergency to the staff
 OCULAR EMERGENCIES Ophthalmic Photographers Society November 15, 2013 Michael A. DellaVecchia MD PhD FACS Wills Eye Emergency Department Philadelphia PA Ocular Emergencies What is an emergency to the patient
OCULAR EMERGENCIES Ophthalmic Photographers Society November 15, 2013 Michael A. DellaVecchia MD PhD FACS Wills Eye Emergency Department Philadelphia PA Ocular Emergencies What is an emergency to the patient
PEDIATRIC OCULAR INJURIES. Sapna Tibrewal MD
 PEDIATRIC OCULAR INJURIES Sapna Tibrewal MD 1 Learning Objectives Learn to recognize the common pediatric ocular injuries Immediate management tips to be instituted in your office/ ER Know when to call
PEDIATRIC OCULAR INJURIES Sapna Tibrewal MD 1 Learning Objectives Learn to recognize the common pediatric ocular injuries Immediate management tips to be instituted in your office/ ER Know when to call
PENETRATING EYE INJUIRES
 PENETRATING EYE INJUIRES King Harold receives a mortal penetrating injury to the eye at the Battle of Hastings 1066, Detail Bayeux Tapestry, Eleventh century. Then Earl William came from Normandy into
PENETRATING EYE INJUIRES King Harold receives a mortal penetrating injury to the eye at the Battle of Hastings 1066, Detail Bayeux Tapestry, Eleventh century. Then Earl William came from Normandy into
Clues of a Ruptured Globe
 Definition any eye that has sustained a full thickness traumatic disruption of the cornea or sclera Overwhelmingly, rupture accidents occur in young men, small children and the elderly Corneal laceration
Definition any eye that has sustained a full thickness traumatic disruption of the cornea or sclera Overwhelmingly, rupture accidents occur in young men, small children and the elderly Corneal laceration
LECTURE # 7 EYECARE REVIEW: PART III
 LECTURE # 7 EYECARE REVIEW: PART III HOW TO TRIAGE EYE EMERGENCIES STEVE BUTZON, O.D. EYECARE REVIEW: HOW TO TRIAGE EYE EMERGENCIES FOR PRIMARY CARE PHYSICIANS Steve Butzon, O.D. Member Director IDOC President
LECTURE # 7 EYECARE REVIEW: PART III HOW TO TRIAGE EYE EMERGENCIES STEVE BUTZON, O.D. EYECARE REVIEW: HOW TO TRIAGE EYE EMERGENCIES FOR PRIMARY CARE PHYSICIANS Steve Butzon, O.D. Member Director IDOC President
Ocular Lecture. Sue Bednar NP Ali Atwater PA-C
 Ocular Lecture Sue Bednar NP Ali Atwater PA-C Triaging Ocular Complaints Painful Eye/Red eye +/-blurry vision +/-visual loss +/-floaters +/-fevers If any of the above findings exist, pt is likely to have
Ocular Lecture Sue Bednar NP Ali Atwater PA-C Triaging Ocular Complaints Painful Eye/Red eye +/-blurry vision +/-visual loss +/-floaters +/-fevers If any of the above findings exist, pt is likely to have
Eye Trauma. Lid Laceration. Orbital Fracture
 Eye Trauma Lid Laceration The presence of a lid laceration, however insignificant, mandates careful exploration of the wound and examination of the globe. 1. Superficial lacerations parallel to the lid
Eye Trauma Lid Laceration The presence of a lid laceration, however insignificant, mandates careful exploration of the wound and examination of the globe. 1. Superficial lacerations parallel to the lid
Sepideh Tara Rousta, MD FAAO Robert Wood Johnson University Hospital Saint Peter s University Hospital Wills Eye Hospital
 Sepideh Tara Rousta, MD FAAO Robert Wood Johnson University Hospital Saint Peter s University Hospital Wills Eye Hospital 14 mo old w R eye cross (parents) 9 mo old R eye crossing getting worse for past
Sepideh Tara Rousta, MD FAAO Robert Wood Johnson University Hospital Saint Peter s University Hospital Wills Eye Hospital 14 mo old w R eye cross (parents) 9 mo old R eye crossing getting worse for past
Examining Children s Eyes
 Paediatric Ophthalmology What to refer & when? Aims Tips for assessing a child s eyes in general practice Common paediatric ophthalmology symptoms and signs What needs to be referred and when? MISS FARIHA
Paediatric Ophthalmology What to refer & when? Aims Tips for assessing a child s eyes in general practice Common paediatric ophthalmology symptoms and signs What needs to be referred and when? MISS FARIHA
SILA THONGLAI MD. Bangkok Eye center Bangkok Hospital Thailand
 SILA THONGLAI MD. Bangkok Eye center Bangkok Hospital Thailand Ocular Anatomy Bony Components of Orbit 1 1. Frontal bone 4 5 7 6 2. Zygomatic bone 3. Maxillary bone 4. Sphenoid bone 5. Ethmoid bone 2 3
SILA THONGLAI MD. Bangkok Eye center Bangkok Hospital Thailand Ocular Anatomy Bony Components of Orbit 1 1. Frontal bone 4 5 7 6 2. Zygomatic bone 3. Maxillary bone 4. Sphenoid bone 5. Ethmoid bone 2 3
Telephone Triage Urgency or Emergency? Mary E. Schmidt, ABOC, CPO
 Telephone Triage Urgency or Emergency? www.eyesystems.info Mary E. Schmidt, ABOC, CPO mary@eyesystems.info Definition of Triage The sorting of patient and allocation of care or treatment according to the
Telephone Triage Urgency or Emergency? www.eyesystems.info Mary E. Schmidt, ABOC, CPO mary@eyesystems.info Definition of Triage The sorting of patient and allocation of care or treatment according to the
THE 35 GOLDEN EYE RULES
 THE 35 GOLDEN EYE RULES The Sense of Sight, from La Dame a la Licorne, The Lady and the Unicorn Tapestries, Late 15th Century Flemish Tapestry in wool and silk, Musée Nationale du Moyen Age, Paris. 1.
THE 35 GOLDEN EYE RULES The Sense of Sight, from La Dame a la Licorne, The Lady and the Unicorn Tapestries, Late 15th Century Flemish Tapestry in wool and silk, Musée Nationale du Moyen Age, Paris. 1.
Focusing on A&E. By Sandy Cooper, (Ophthalmic Nurse Practitioner), Tel
, Tel") Focusing on A&E By Sandy Cooper, (Ophthalmic Nurse Practitioner), Tel 01752 439331 Email sandra.cooper5@nhs.net sandracooper041@btinternet.com THINGS TO WORRY ABOUT WITH ANY EYE PROBLEM CHANGES IN VISION
Focusing on A&E By Sandy Cooper, (Ophthalmic Nurse Practitioner), Tel 01752 439331 Email sandra.cooper5@nhs.net sandracooper041@btinternet.com THINGS TO WORRY ABOUT WITH ANY EYE PROBLEM CHANGES IN VISION
Entire Staff Needs To Be Trained. Ocular Emergencies 101. Injury Types. 3 Things to always remember. Rule #1 7/1/2017
 Ocular Emergencies 101 Lynn E. Lawrence, CPOT, ABOC, COA, OSC This lecture is graphic! Injury Types Rule #1 Entire Staff Needs To Be Trained 3 Things to always remember Everyone must be trained in emergencies!
Ocular Emergencies 101 Lynn E. Lawrence, CPOT, ABOC, COA, OSC This lecture is graphic! Injury Types Rule #1 Entire Staff Needs To Be Trained 3 Things to always remember Everyone must be trained in emergencies!
Everyday Practice. Eye trauma: Primary care for general physicians
 VOL.. 15, NO.2, 85 2002 Everyday Practice Eye trauma: Primary care for general physicians H. K. TEWARI, ATUL KUMAR, GUNJAN PRAKASH INTRODUCTION The understanding of ocular trauma is important for the primary
VOL.. 15, NO.2, 85 2002 Everyday Practice Eye trauma: Primary care for general physicians H. K. TEWARI, ATUL KUMAR, GUNJAN PRAKASH INTRODUCTION The understanding of ocular trauma is important for the primary
Ocular Emergencies. Pisit Preechawat, MD Department of Ophthalmology, Ramathibodi Hospital
 Ocular Emergencies Pisit Preechawat, MD Department of Ophthalmology, Ramathibodi Hospital Ocular Anatomy Bony Components of Orbit 1 1. Frontal bone 4 5 7 6 2. Zygomatic bone 3. Maxillary bone 4. Sphenoid
Ocular Emergencies Pisit Preechawat, MD Department of Ophthalmology, Ramathibodi Hospital Ocular Anatomy Bony Components of Orbit 1 1. Frontal bone 4 5 7 6 2. Zygomatic bone 3. Maxillary bone 4. Sphenoid
Ears. Mouth. Jowls 6 Major Bones of the Face Nasal bone Two
 1 2 3 4 5 Chapter 25 Injuries to the Face, Neck, and Eyes Injuries to the Face and Neck Face and neck are to injury Relatively unprotected positions on body Some injuries are life-threatening. trauma to
1 2 3 4 5 Chapter 25 Injuries to the Face, Neck, and Eyes Injuries to the Face and Neck Face and neck are to injury Relatively unprotected positions on body Some injuries are life-threatening. trauma to
By Darlene Jones, Nurse. May 2017
 By Darlene Jones, Nurse May 2017 Disclosure of potential conflict of interest Darlene Jones, Nurse I have no conflict of interest Course objectives Become familiar with the different pathologies in ophthalmology
By Darlene Jones, Nurse May 2017 Disclosure of potential conflict of interest Darlene Jones, Nurse I have no conflict of interest Course objectives Become familiar with the different pathologies in ophthalmology
Faculty Financial Disclosure. Learning Objectives: Office Ophthalmology. Basic Eye Exam: What s in your pocket/office? Office Ophthalmology
 Faculty Financial Disclosure Office Ophthalmology Lynn K. Gordon, MD, PhD, has no financial relationships to disclose. Lynn K. Gordon, MD, PhD Professor and Vernon O Underwood Family Chair Department of
Faculty Financial Disclosure Office Ophthalmology Lynn K. Gordon, MD, PhD, has no financial relationships to disclose. Lynn K. Gordon, MD, PhD Professor and Vernon O Underwood Family Chair Department of
Eyes, ears, teeth and everything in between
 Eyes, ears, teeth and everything in between E M E R G E N C Y D E P A R T M E N T J U N I O R T E A C H created 14/11/10 by S.R. Bruijns, version 1.0 Objectives Eyes Ears Teeth Maxilla- facial EYES Approaching
Eyes, ears, teeth and everything in between E M E R G E N C Y D E P A R T M E N T J U N I O R T E A C H created 14/11/10 by S.R. Bruijns, version 1.0 Objectives Eyes Ears Teeth Maxilla- facial EYES Approaching
Ophthalmology. Corneal Abrasion. History
 Ophthalmology Corneal Abrasion - Usually clear history of very recent trauma - Foreign Body Sensation - Pain +++ - Lacrimation - Photophobia Fig. 1 Corneal Abrasion - Abrasion stains yellow / green with
Ophthalmology Corneal Abrasion - Usually clear history of very recent trauma - Foreign Body Sensation - Pain +++ - Lacrimation - Photophobia Fig. 1 Corneal Abrasion - Abrasion stains yellow / green with
Injury. Contusion Lamellar Laceration Laceration Rupture. Penetrating IOFB. Perforating
 Mechanical Ocular Trauma Došková Hana, MD. Department of Ophthalmology Medicine Faculty of Masaryk University Brno General Considerations Ocular trauma constitude about 6% of all injuries, but eyes set
Mechanical Ocular Trauma Došková Hana, MD. Department of Ophthalmology Medicine Faculty of Masaryk University Brno General Considerations Ocular trauma constitude about 6% of all injuries, but eyes set
OPHTHALMOLOGIC PEARLS FOR THE NON- OPHTHALMOLOGIST. David G. Gross D.O. Deen-Gross Eye Centers Merrillville-Hobart Deengrosseye.
 OPHTHALMOLOGIC PEARLS FOR THE NON- OPHTHALMOLOGIST David G. Gross D.O. Deen-Gross Eye Centers Merrillville-Hobart Deengrosseye.com A FEW OF THE AREAS WE WILL DISCUSS Red Eye Glaucoma Neuro ophthalmic tid
OPHTHALMOLOGIC PEARLS FOR THE NON- OPHTHALMOLOGIST David G. Gross D.O. Deen-Gross Eye Centers Merrillville-Hobart Deengrosseye.com A FEW OF THE AREAS WE WILL DISCUSS Red Eye Glaucoma Neuro ophthalmic tid
Maxillofacial and Ocular Injuries
 Maxillofacial and Ocular Injuries Objectives At the conclusion of this presentation the participant will be able to: Identify the key anatomical structures of the face and eye and the impact of force on
Maxillofacial and Ocular Injuries Objectives At the conclusion of this presentation the participant will be able to: Identify the key anatomical structures of the face and eye and the impact of force on
Ocular Trauma. Breaking Down Blunt. Blunt ocular trauma occurs frequently in sporting
 Focus on CME at the University of Saskatchewan Breaking Down Blunt Ocular Trauma By Dan Ash, MD, BA, FRCSC, FACS, FAAO Blunt ocular trauma occurs frequently in sporting activities, as well as in industrial
Focus on CME at the University of Saskatchewan Breaking Down Blunt Ocular Trauma By Dan Ash, MD, BA, FRCSC, FACS, FAAO Blunt ocular trauma occurs frequently in sporting activities, as well as in industrial
Ocular Trauma. Authors Dr Shrinkhal 1, Dr Kamya Sharma 2
 International Journal of Emerging Trends in Science and Technology IC Value: 76.89 (Index Copernicus) Impact Factor: 2.838 DOI: https://dx.doi.org/10.18535/ijetst/v3i12.01 Ocular Trauma Authors Dr Shrinkhal
International Journal of Emerging Trends in Science and Technology IC Value: 76.89 (Index Copernicus) Impact Factor: 2.838 DOI: https://dx.doi.org/10.18535/ijetst/v3i12.01 Ocular Trauma Authors Dr Shrinkhal
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Abdominal injuries, abdominal wall muscle injury, 212 213 diaphragmatic spasm, 212 liver injury, 213 214 pancreatic injury, 216 rectus
Index Note: Page numbers of article titles are in boldface type. A Abdominal injuries, abdominal wall muscle injury, 212 213 diaphragmatic spasm, 212 liver injury, 213 214 pancreatic injury, 216 rectus
10/4/2013. Bruce K.Williams, MSN, RN,ACNP-BC Sisters of Charity Providence Hospitals. What is the worst thing that can go wrong with an eye?
 Red Eyes, Red Alert! Bruce K.Williams, MSN, RN,ACNP-BC Sisters of Charity Providence Hospitals Red Eyes, Red Alert! Red Eyes, Red Alert! What is the worst thing that can go wrong with an eye? 1 Red Eyes,
Red Eyes, Red Alert! Bruce K.Williams, MSN, RN,ACNP-BC Sisters of Charity Providence Hospitals Red Eyes, Red Alert! Red Eyes, Red Alert! What is the worst thing that can go wrong with an eye? 1 Red Eyes,
Test Bank for Medical Surgical Nursing An Integrated Approach 3rd Edition by White
 Test Bank for Medical Surgical Nursing An Integrated Approach 3rd Edition by White Link full download : http://testbankair.com/download/test-bank-for-medical-surgical-nursing-anintegrated-approach-3rd-edition-by-white/
Test Bank for Medical Surgical Nursing An Integrated Approach 3rd Edition by White Link full download : http://testbankair.com/download/test-bank-for-medical-surgical-nursing-anintegrated-approach-3rd-edition-by-white/
Ocular Injuries. Chapter 14
 Ocular Injuries Chapter 14 Ocular Injuries Introduction The preservation of the eyes and eyesight of service personnel is an extremely important goal. Despite comprising as little as 0.1% of the total
Ocular Injuries Chapter 14 Ocular Injuries Introduction The preservation of the eyes and eyesight of service personnel is an extremely important goal. Despite comprising as little as 0.1% of the total
TRAUMA, TRAUMA A YOUNG PARENT WOULD HAVE HEARD THE TITLE AND IMMEDIATELY THOUGHT 10/24/2018 JAMES LEE, M.D., ASSISTANT PROFESSOR TECHNICIAN CONFERENCE
 TRAUMA, TRAUMA JAMES LEE, M.D., ASSISTANT PROFESSOR TECHNICIAN CONFERENCE OCT 26, 2018 A YOUNG PARENT WOULD HAVE HEARD THE TITLE AND IMMEDIATELY THOUGHT 1 GROSS PICTURES LET S START WITH EYELIDS Lacerations
TRAUMA, TRAUMA JAMES LEE, M.D., ASSISTANT PROFESSOR TECHNICIAN CONFERENCE OCT 26, 2018 A YOUNG PARENT WOULD HAVE HEARD THE TITLE AND IMMEDIATELY THOUGHT 1 GROSS PICTURES LET S START WITH EYELIDS Lacerations
Imaging Orbit/Periorbital Injury
 Imaging Orbit/Periorbital Injury 9 th Nordic Trauma Radiology Course 2016 Stuart E. Mirvis, M.D., FACR Department of Radiology University of Maryland School of Medicine Fireworks Topics to Cover Struts
Imaging Orbit/Periorbital Injury 9 th Nordic Trauma Radiology Course 2016 Stuart E. Mirvis, M.D., FACR Department of Radiology University of Maryland School of Medicine Fireworks Topics to Cover Struts
The Emergent Eye in the Acute Setting
 The Emergent Eye in the Acute Setting Todd P. Margolis MD, PhD Professor of Ophthalmology & Director of the F.I. Proctor Foundation UCSF Physical Exam-- Visual Acuity Essential Corrected visual acuity
The Emergent Eye in the Acute Setting Todd P. Margolis MD, PhD Professor of Ophthalmology & Director of the F.I. Proctor Foundation UCSF Physical Exam-- Visual Acuity Essential Corrected visual acuity
Around The Globe in 60 Minutes
 Around The Globe in 60 Minutes Around the GLOBE in Sixty Minutes Basic Ocular Anatomy, Examination, and Diagnostic Techniques Introduction Focusing on canine and feline ocular anatomy and basic examination
Around The Globe in 60 Minutes Around the GLOBE in Sixty Minutes Basic Ocular Anatomy, Examination, and Diagnostic Techniques Introduction Focusing on canine and feline ocular anatomy and basic examination
Entire Staff Needs To Be Trained
 Ocular Emergencies 101 Lynn E. Lawrence, CPOT, ABOC, COA This lecture is graphic! Rule #1 Entire Staff Needs To Be Trained 3 Things to always remember Everyone must be trained in emergencies! training
Ocular Emergencies 101 Lynn E. Lawrence, CPOT, ABOC, COA This lecture is graphic! Rule #1 Entire Staff Needs To Be Trained 3 Things to always remember Everyone must be trained in emergencies! training
Phone Triage for Optometric Staff ???????? CHEMICAL BURN CHEMICAL BURN
 Phone Triage for Optometric Staff There are very few ocular emergencies that you will have to deal with in practice, but it is imperative that you be able to Michelle Welch, O.D. NSU Oklahoma College of
Phone Triage for Optometric Staff There are very few ocular emergencies that you will have to deal with in practice, but it is imperative that you be able to Michelle Welch, O.D. NSU Oklahoma College of
OCT : retinal layers. Extraocular muscles. History. Central vs Peripheral vision. History: Temporal course. Optical Coherence Tomography (OCT)
") Optical Coherence Tomography (OCT) OCT : retinal layers 7 Central vs Peripheral vision Extraocular muscles RPE E Peripheral Vision: Rods (95 million) 30% Ganglion cells Central Vision: Cones (5 million)
Optical Coherence Tomography (OCT) OCT : retinal layers 7 Central vs Peripheral vision Extraocular muscles RPE E Peripheral Vision: Rods (95 million) 30% Ganglion cells Central Vision: Cones (5 million)
Dr Jo-Anne Pon. Dr Sean Every. 8:30-9:25 WS #70: Eye Essentials for GPs 9:35-10:30 WS #80: Eye Essentials for GPs (Repeated)
") Dr Sean Every Ophthalmologist Southern Eye Specialists Christchurch Dr Jo-Anne Pon Ophthalmologist Southern Eye Specialists, Christchurch Hospital, Christchurch 8:30-9:25 WS #70: Eye Essentials for GPs
Dr Sean Every Ophthalmologist Southern Eye Specialists Christchurch Dr Jo-Anne Pon Ophthalmologist Southern Eye Specialists, Christchurch Hospital, Christchurch 8:30-9:25 WS #70: Eye Essentials for GPs
Joint Theater Trauma System Clinical Practice Guideline
 INITIAL CARE OF OCULAR AND ADNEXAL INJURIES BY NON- OPHTHALMOLOGISTS AT ROLE 1, ROLE 2, and NON-OPHTHALMIC ROLE 3 FACILITIES Original Release/Approval 1 Aug 2007 Note: This CPG requires an annual review.
INITIAL CARE OF OCULAR AND ADNEXAL INJURIES BY NON- OPHTHALMOLOGISTS AT ROLE 1, ROLE 2, and NON-OPHTHALMIC ROLE 3 FACILITIES Original Release/Approval 1 Aug 2007 Note: This CPG requires an annual review.
DISCLOSURES. PEDIATRIC RED EYES Rachel M. Smith, OD, FCOVD HISTORY, HISTORY, HISTORY WHY RED EYES? EXAMINE THE EYE RED FLAGS TO REFER 3/25/2019
 DISCLOSURES Consultant/Speakers bureaus Research funding PEDIATRIC RED EYES Rachel M. Smith, OD, FCOVD Pediatric Optometrist Children s Hospital & Medical Center Stock ownership/corporate boards employment
DISCLOSURES Consultant/Speakers bureaus Research funding PEDIATRIC RED EYES Rachel M. Smith, OD, FCOVD Pediatric Optometrist Children s Hospital & Medical Center Stock ownership/corporate boards employment
The Epidemiology and Incidence of Visual Deficits Following Ocular Trauma in Pediatric Patients
 Yale University EliScholar A Digital Platform for Scholarly Publishing at Yale Yale Medicine Thesis Digital Library School of Medicine 3-25-2008 The Epidemiology and Incidence of Visual Deficits Following
Yale University EliScholar A Digital Platform for Scholarly Publishing at Yale Yale Medicine Thesis Digital Library School of Medicine 3-25-2008 The Epidemiology and Incidence of Visual Deficits Following
Case #1: 68 M with floaters OS
 Case #1: 68 M with floaters OS Point-of-Care Ocular Sonography for the Emergency Department Nate Teismann MD Dept of Emergency Medicine, UCSF Topics in EM 2012 Acute onset of dark spots in L eye 2 days
Case #1: 68 M with floaters OS Point-of-Care Ocular Sonography for the Emergency Department Nate Teismann MD Dept of Emergency Medicine, UCSF Topics in EM 2012 Acute onset of dark spots in L eye 2 days
Probe Selection A high frequency (7-12 MHz) linear array transducer should be used to visualize superficial structures (Image 1).
 linear array transducer should be used to visualize superficial structures (Image 1).") ! Teresa S. Wu, MD, FACEP Director, Emergency Ultrasound Program & Fellowships Co-Director, Women s Imaging Fellowship Maricopa Medical Center Associate Professor, Emergency Medicine Director, Simulation
! Teresa S. Wu, MD, FACEP Director, Emergency Ultrasound Program & Fellowships Co-Director, Women s Imaging Fellowship Maricopa Medical Center Associate Professor, Emergency Medicine Director, Simulation
Ocular Injuries. Chapter 14
 Ocular Injuries Chapter 14 Ocular Injuries Introduction The preservation of the eyes and eyesight of service personnel is an extremely important goal. Despite comprising as little as 0.1% of the total
Ocular Injuries Chapter 14 Ocular Injuries Introduction The preservation of the eyes and eyesight of service personnel is an extremely important goal. Despite comprising as little as 0.1% of the total
Identify the choice that best completes the statement or answers the question.
 Chapter 5. The Eye Multiple Choice Identify the choice that best completes the statement or answers the question. 1. The most common type of eye disorder is: A. Refractive errors B. Macular conditions
Chapter 5. The Eye Multiple Choice Identify the choice that best completes the statement or answers the question. 1. The most common type of eye disorder is: A. Refractive errors B. Macular conditions
Pediatric Ophthalmic Infections and Injuries Honey Herce, MD
 Pediatric Ophthalmic Infections and Injuries Honey Herce, MD Assistant Professor in the Department of Ophthalmology Texas Children's Hospital Baylor College of Medicine Pediatric Ophthalmic Infections
Pediatric Ophthalmic Infections and Injuries Honey Herce, MD Assistant Professor in the Department of Ophthalmology Texas Children's Hospital Baylor College of Medicine Pediatric Ophthalmic Infections
Facial Sports Injuries
 Facial Sports Injuries Playing catch, shooting hoops, bicycling on a scenic path or just kicking around a soccer ball have more in common than you may think. On the up side, these activities are good exercise
Facial Sports Injuries Playing catch, shooting hoops, bicycling on a scenic path or just kicking around a soccer ball have more in common than you may think. On the up side, these activities are good exercise
Anatomy: There are 6 muscles that move your eye.
 Thyroid Eye Disease Your doctor thinks you have thyroid orbitopathy. This is an autoimmune condition where your body's immune system is producing factors that stimulate enlargement of the muscles that
Thyroid Eye Disease Your doctor thinks you have thyroid orbitopathy. This is an autoimmune condition where your body's immune system is producing factors that stimulate enlargement of the muscles that
Paediatric acute ophthalmology. Harry Bradshaw
 Paediatric acute ophthalmology Harry Bradshaw Approach Red eye Leukocoria Neurological Trauma Visual loss Red eye Orbital Eyelid Conjunctiva Cornea Uvea Orbital Orbit fixed volume Contiguous with sinuses,
Paediatric acute ophthalmology Harry Bradshaw Approach Red eye Leukocoria Neurological Trauma Visual loss Red eye Orbital Eyelid Conjunctiva Cornea Uvea Orbital Orbit fixed volume Contiguous with sinuses,
Preview. Ophthalmology for Primary Care Providers. Useful references. How the eye works
 Preview Ophthalmology for Primary Care Providers Bob Avery, MD, PhD How the eye works The red eye Acute eye conditions Chronic vision loss Basic eye exam Ophthalmology/Surgery University of New Mexico
Preview Ophthalmology for Primary Care Providers Bob Avery, MD, PhD How the eye works The red eye Acute eye conditions Chronic vision loss Basic eye exam Ophthalmology/Surgery University of New Mexico
Ophthalmology for Primary Care Providers
 Ophthalmology for Primary Care Providers Bob Avery, MD, PhD Ophthalmology/Surgery University of New Mexico School of Medicine bavery@salud.unm.edu Preview How the eye works Basic eye exam The red eye Acute
Ophthalmology for Primary Care Providers Bob Avery, MD, PhD Ophthalmology/Surgery University of New Mexico School of Medicine bavery@salud.unm.edu Preview How the eye works Basic eye exam The red eye Acute
For details on measurement and recording of visual acuity, refer to Annex 1. VISION INTERPRETING RESULTS ABSTRACT
 management update on functional decline in older adults 2012 Unit No. 5 VISION Dr Au Eong Kah Guan, Ms Yulianti, Ms Fifiana ABSTRACT Among Singaporean adults of Chinese origin aged 40 to 79 years old,
management update on functional decline in older adults 2012 Unit No. 5 VISION Dr Au Eong Kah Guan, Ms Yulianti, Ms Fifiana ABSTRACT Among Singaporean adults of Chinese origin aged 40 to 79 years old,
Andrew J. Hendershot, MD Havener Eye Institute The Ohio State University s Wexner Medical Center
 Ocular Trauma for the Primary Care Physician Andrew J. Hendershot, MD Havener Eye Institute The Ohio State University s Wexner Medical Center Relevance Often those with minor eye injuries will first seek
Ocular Trauma for the Primary Care Physician Andrew J. Hendershot, MD Havener Eye Institute The Ohio State University s Wexner Medical Center Relevance Often those with minor eye injuries will first seek
Dr. Esam Ahmad Z. Omar BDS, MSc-OMFS, FFDRCSI. Monitor the vital signs. Monitor the vital signs. Complications of Facial Traumas.
 Complications of Facial Traumas 1) Immediate Complications 2) Late Complications Dr. Esam Ahmad Z. Omar BDS, MSc-OMFS, FFDRCSI Assistant Professor Oral & Maxillofacial Surgeon Taibah University Monitor
Complications of Facial Traumas 1) Immediate Complications 2) Late Complications Dr. Esam Ahmad Z. Omar BDS, MSc-OMFS, FFDRCSI Assistant Professor Oral & Maxillofacial Surgeon Taibah University Monitor
Wildlife Ophthalmology D R. H E A T H E R R E I D T O R O N T O W I L D L I F E C E N T R E T O R O N T O, O N C A N A D A
 Wildlife Ophthalmology D R. H E A T H E R R E I D T O R O N T O W I L D L I F E C E N T R E T O R O N T O, O N C A N A D A Why understand eyes? Wildlife need to have excellent vision to survive in the
Wildlife Ophthalmology D R. H E A T H E R R E I D T O R O N T O W I L D L I F E C E N T R E T O R O N T O, O N C A N A D A Why understand eyes? Wildlife need to have excellent vision to survive in the
Developed by Bradford J. Shingleton, MD, in conjunction with the Ophthalmology Liaisons Committee of the American Academy of Ophthalmology
 Developed by Bradford J. Shingleton, MD, in conjunction with the Ophthalmology Liaisons Committee of the American Academy of Ophthalmology Reviewer, 2009 Revision Mary A. O'Hara, MD Executive Editor, 2009
Developed by Bradford J. Shingleton, MD, in conjunction with the Ophthalmology Liaisons Committee of the American Academy of Ophthalmology Reviewer, 2009 Revision Mary A. O'Hara, MD Executive Editor, 2009
REFERRAL GUIDELINES: OPHTHALMOLOGY
 Outpatient Referral Guidelines Page 1 1 REFERRAL GUIDELINES: OPHTHALMOLOGY Date of birth Demographic Contact details (including mobile phone) Clinical Reason for referral Duration of symptoms Essential
Outpatient Referral Guidelines Page 1 1 REFERRAL GUIDELINES: OPHTHALMOLOGY Date of birth Demographic Contact details (including mobile phone) Clinical Reason for referral Duration of symptoms Essential
Ocular trauma. Abstract. Introduction. Approach to the patient. CPD Article: Ocular trauma
 Ocular trauma Abstract Mustak H, MBChB, DipOphth(SA), Registrar Division of Ophthalmology, Groote Schuur Hospital; University of Cape Town Du Toit N, MBChB, DipOphth(SA), FRCS(Ed), FCOphth(SA), MMed, Consultant
Ocular trauma Abstract Mustak H, MBChB, DipOphth(SA), Registrar Division of Ophthalmology, Groote Schuur Hospital; University of Cape Town Du Toit N, MBChB, DipOphth(SA), FRCS(Ed), FCOphth(SA), MMed, Consultant
NEPTUNE RED BANK BRICK
 NEPTUNE RED BANK BRICK Diabetes & The Eye Diabetics are more likely to develop Cataracts at a younger age. Diabetics are twice as likely to develop Glaucoma when compared to non-diabetics. The primary
NEPTUNE RED BANK BRICK Diabetes & The Eye Diabetics are more likely to develop Cataracts at a younger age. Diabetics are twice as likely to develop Glaucoma when compared to non-diabetics. The primary
ALTERNATIVES TO PHAKIC IMPLANT SURGERY
 Visian ICL Consent INTRODUCTION This information is being provided to you so that you can make an informed decision about having eye surgery to reduce or eliminate your nearsightedness. Only you and your
Visian ICL Consent INTRODUCTION This information is being provided to you so that you can make an informed decision about having eye surgery to reduce or eliminate your nearsightedness. Only you and your
LASER REFRACTIVE CENTER INFORMED CONSENT DOCUMENT PERIPHERAL CORNEAL RELAXING INCISION (PCRI)
") INTRODUCTION The purpose of this document is to provide written information regarding the risks, benefits and alternatives of Peripheral Relaxing Corneal Incision. This material serves as a supplement
INTRODUCTION The purpose of this document is to provide written information regarding the risks, benefits and alternatives of Peripheral Relaxing Corneal Incision. This material serves as a supplement
EYE ASSESSMENT - ADULT
 For more information or to provide feedback on this or any other decision support tool, email certifiedpractice@crnbc.ca EYE ASSESSMENT - ADULT Nurses with RN First Call Certified Practice designation
For more information or to provide feedback on this or any other decision support tool, email certifiedpractice@crnbc.ca EYE ASSESSMENT - ADULT Nurses with RN First Call Certified Practice designation
THE RED EYE Cynthia McNamara, MD Week 25
 THE RED EYE Cynthia McNamara, MD Week 25 Educational Objectives: 1. Know the differential diagnosis and presentation of specific etiologies of the red eye 2. Be able to evaluate patients presenting with
THE RED EYE Cynthia McNamara, MD Week 25 Educational Objectives: 1. Know the differential diagnosis and presentation of specific etiologies of the red eye 2. Be able to evaluate patients presenting with
Neuro-ophthalmologyophthalmology. Marek Michalec, MD.
 Neuro-ophthalmologyophthalmology Marek Michalec, MD. Neuro-ophthalmology Study integrating ophthalmology and neurology Disorders affecting parts of CNS devoted to vision or eye: Afferent system (visual
Neuro-ophthalmologyophthalmology Marek Michalec, MD. Neuro-ophthalmology Study integrating ophthalmology and neurology Disorders affecting parts of CNS devoted to vision or eye: Afferent system (visual
Bleeding in the anterior chamber, obstructing vision Caused by surgery, injury, coagulopathy, sickle cell or idiopathic Needs urgent care to prevent
 Bleeding in the anterior chamber, obstructing vision Caused by surgery, injury, coagulopathy, sickle cell or idiopathic Needs urgent care to prevent long-term vision loss TX by elevating head of bed, reducing
Bleeding in the anterior chamber, obstructing vision Caused by surgery, injury, coagulopathy, sickle cell or idiopathic Needs urgent care to prevent long-term vision loss TX by elevating head of bed, reducing
CORNEAL CONDITIONS CORNEAL TRANSPLANTATION
 GENERAL INFORMATION CORNEAL CONDITIONS CORNEAL TRANSPLANTATION WHAT ARE CORNEAL CONDITIONS? The cornea is the clear outer layer of the eye. Shaped like a dome, it helps to protect the eye from foreign
GENERAL INFORMATION CORNEAL CONDITIONS CORNEAL TRANSPLANTATION WHAT ARE CORNEAL CONDITIONS? The cornea is the clear outer layer of the eye. Shaped like a dome, it helps to protect the eye from foreign
Ocular warning signs in GP practice: Paediatric Eye Pointers
 Ocular warning signs in GP practice: Paediatric Eye Pointers Dr Benjamin Chang MB, BCh, BAO, MMedSci, FRCS(Irel), FRCS(Edin), FRCOphth(Lond) Senior Consultant Ophthalmology and Visual Sciences Khoo Teck
Ocular warning signs in GP practice: Paediatric Eye Pointers Dr Benjamin Chang MB, BCh, BAO, MMedSci, FRCS(Irel), FRCS(Edin), FRCOphth(Lond) Senior Consultant Ophthalmology and Visual Sciences Khoo Teck
Aristotle University Thessaloniki Medical School I. & II. Departments of Ophthalmology 90 DIAGNOSTIC & THERAPEUTIC APPROACHES IN OPHTHALMOLOGY
 Aristotle University Thessaloniki Medical School I. & II. Departments of Ophthalmology 90 DIAGNOSTIC & THERAPEUTIC APPROACHES IN OPHTHALMOLOGY The medical student should be able to... I. Pathophysiology
Aristotle University Thessaloniki Medical School I. & II. Departments of Ophthalmology 90 DIAGNOSTIC & THERAPEUTIC APPROACHES IN OPHTHALMOLOGY The medical student should be able to... I. Pathophysiology
OPHTHALMOLOGY DEPARTMENT Primary care referral guidelines
 OPHTHALMOLOGY DEPARTMENT Primary care referral guidelines Contents REFERRAL CATEGIES... 2 Emergency... 2 Urgent... 2 Semi urgent/routine... 2 Not accepted... 2 OPHTHALMOLOGY CONDITIONS NOT ACCEPTED...
OPHTHALMOLOGY DEPARTMENT Primary care referral guidelines Contents REFERRAL CATEGIES... 2 Emergency... 2 Urgent... 2 Semi urgent/routine... 2 Not accepted... 2 OPHTHALMOLOGY CONDITIONS NOT ACCEPTED...
ASSESSING THE EYES. Structures. Eyelids Extraocularmuscles Eyelashes Lacrimal glands: Lacrimal ducts Cornea Conjunctiva Sclera Pupils Iris.
 ASSESSING THE EYES Structures External Eyelids Extraocularmuscles Eyelashes Lacrimal glands: Lacrimal ducts Cornea Conjunctiva Sclera Pupils Iris 1 2 Structures Internal Optic disc Physiological cup Retinal
ASSESSING THE EYES Structures External Eyelids Extraocularmuscles Eyelashes Lacrimal glands: Lacrimal ducts Cornea Conjunctiva Sclera Pupils Iris 1 2 Structures Internal Optic disc Physiological cup Retinal
DEFINITION Corneal abrasion is a defect in the corneal surface epithelium due to scraping or rubbing of the corneal epithelium.
 DEFINITION Corneal abrasion is a defect in the corneal surface epithelium due to scraping or rubbing of the corneal epithelium. IMMEDIATE CONSULTATION REQUIRED IN THE FOLLOWING SITUATIONS Dendritic pattern
DEFINITION Corneal abrasion is a defect in the corneal surface epithelium due to scraping or rubbing of the corneal epithelium. IMMEDIATE CONSULTATION REQUIRED IN THE FOLLOWING SITUATIONS Dendritic pattern
02/03/2014. Average Length: 23mm (Infant ~16mm) Approximately the size of a quarter Volume: ~5mL
 Approximately the size of a quarter Volume: ~5mL") Identify the anatomy of the eye. Explain the basic physiology of the parts of the eye. Briefly discuss various surgeries related to different parts of the anatomy. Average Length: 23mm (Infant ~16mm) Approximately
Identify the anatomy of the eye. Explain the basic physiology of the parts of the eye. Briefly discuss various surgeries related to different parts of the anatomy. Average Length: 23mm (Infant ~16mm) Approximately
Differential Diagnosis of Conjunctivitis and Keratoconjunctivitis
 Differential Diagnosis of Conjunctivitis and Keratoconjunctivitis Dr. Victor Malinovsky 2006 Mechanical-Physical Trauma Corneal Abrasions Abrasions (interpalpebral/variable): a focal loss of epithelium
Differential Diagnosis of Conjunctivitis and Keratoconjunctivitis Dr. Victor Malinovsky 2006 Mechanical-Physical Trauma Corneal Abrasions Abrasions (interpalpebral/variable): a focal loss of epithelium
Emergency Ophthalmology Lawrence B. Stack, MD Handout can be found on lbstack.com/students/eye-handout.pdf
 Emergency Ophthalmology Lawrence B. Stack, MD Handout can be found on lbstack.com/students/eye-handout.pdf Summary Points: 1. Consult Ophthalmology if you can not account for change in visual acuity 2.
Emergency Ophthalmology Lawrence B. Stack, MD Handout can be found on lbstack.com/students/eye-handout.pdf Summary Points: 1. Consult Ophthalmology if you can not account for change in visual acuity 2.
HANDBOOK FOR JUNIOR RESIDENTS AND MEDICAL STUDENTS LEARNING EMERGENCY OPHTHALMOLOGY
 HANDBOOK FOR JUNIOR RESIDENTS AND MEDICAL STUDENTS LEARNING EMERGENCY OPHTHALMOLOGY Compiled by The Task Force on Undergraduate Teaching in Ophthalmology of the International Council of Ophthalmology and
HANDBOOK FOR JUNIOR RESIDENTS AND MEDICAL STUDENTS LEARNING EMERGENCY OPHTHALMOLOGY Compiled by The Task Force on Undergraduate Teaching in Ophthalmology of the International Council of Ophthalmology and
Disclosure Ocular Anatomy and Motility
 Disclosure Ocular Anatomy and Motility Jenean Carlton BA, ABOC, NCLC President, Carlton & Associates, LLC Carlton and Associates, LLC provides communications and educational materials for the optical industry
Disclosure Ocular Anatomy and Motility Jenean Carlton BA, ABOC, NCLC President, Carlton & Associates, LLC Carlton and Associates, LLC provides communications and educational materials for the optical industry
Assisting in Ophthalmology. Copyright 2011, 2007, 2003, 1999 by Saunders, an imprint of Elsevier Inc. All rights reserved.
 Assisting in Ophthalmology Learning Objectives Define, spell, and pronounce the terms listed in the vocabulary. Apply critical thinking skills in performing patient assessment and care. Explain the differences
Assisting in Ophthalmology Learning Objectives Define, spell, and pronounce the terms listed in the vocabulary. Apply critical thinking skills in performing patient assessment and care. Explain the differences
Cairo University Faculty of Medicine. Course Specifications Course title: Ophthalmology (Code): OPH-409. Department of Ophthalmology
: OPH-409. Department of Ophthalmology") Cairo University Faculty of Medicine Department of Ophthalmology Course Specifications Course title: Ophthalmology (Code): OPH-409 Department of Ophthalmology Fourth academic year of M.B.B.Ch. program
Cairo University Faculty of Medicine Department of Ophthalmology Course Specifications Course title: Ophthalmology (Code): OPH-409 Department of Ophthalmology Fourth academic year of M.B.B.Ch. program
CNS 2 Physiology lab
 It should be noted that the doctor emphasized that this material is also considered as continuation of the theory material and is INCLUDED IN THE THEORY EXAM. Presbiopia: is decrease in accommodation of
It should be noted that the doctor emphasized that this material is also considered as continuation of the theory material and is INCLUDED IN THE THEORY EXAM. Presbiopia: is decrease in accommodation of
Ocular Anatomy for the Paraoptometric
 Ocular Anatomy for the Paraoptometric Minnesota Optometric Association Paraoptometric CE Friday September 30, 2016 Lindsay A. Sicks, OD, FAAO Assistant Professor, Illinois College of Optometry lsicks@ico.edu
Ocular Anatomy for the Paraoptometric Minnesota Optometric Association Paraoptometric CE Friday September 30, 2016 Lindsay A. Sicks, OD, FAAO Assistant Professor, Illinois College of Optometry lsicks@ico.edu
PREAMBLE TO MSC PAYMENT SCHEDULE: OPTOMETRY SERVICES
 PREAMBLE TO MSC PAYMENT SCHEDULE: OPTOMETRY SERVICES A. GENERAL PROVISIONS 1. Eye Examination Benefits Optometric benefits are services defined in Section 23 of the Medical and Health Care Services Regulations,
PREAMBLE TO MSC PAYMENT SCHEDULE: OPTOMETRY SERVICES A. GENERAL PROVISIONS 1. Eye Examination Benefits Optometric benefits are services defined in Section 23 of the Medical and Health Care Services Regulations,
Year 2 MBChB Clinical Skills Session Ophthalmoscopy. Reviewed & ratified by: Mr M Batterbury Consultant Ophthalmologist
 Year 2 MBChB Clinical Skills Session Ophthalmoscopy Reviewed & ratified by: o Mr M Batterbury Consultant Ophthalmologist Learning objectives o To understand the anatomy and physiology of the external and
Year 2 MBChB Clinical Skills Session Ophthalmoscopy Reviewed & ratified by: o Mr M Batterbury Consultant Ophthalmologist Learning objectives o To understand the anatomy and physiology of the external and
Informed IntraLASIK Consent
 9201 Sunset Boulevard Suite 709 West Hollywood, CA 90069 Informed Intra Consent Phone 310. 275. 5533 Fax 310. 275. 5523 info@benjamineye.com www.benjamineye.com For the Correction of Nearsightedness, Farsightedness,
9201 Sunset Boulevard Suite 709 West Hollywood, CA 90069 Informed Intra Consent Phone 310. 275. 5533 Fax 310. 275. 5523 info@benjamineye.com www.benjamineye.com For the Correction of Nearsightedness, Farsightedness,