Shock and Vasopressors. Nina E. Glass, MD TACS Fellow SICU Didactic Curriculum 9/24/14
|
|
|
- Christian Morris
- 5 years ago
- Views:
Transcription
1 Shock and Vasopressors Nina E. Glass, MD TACS Fellow SICU Didactic Curriculum 9/24/14
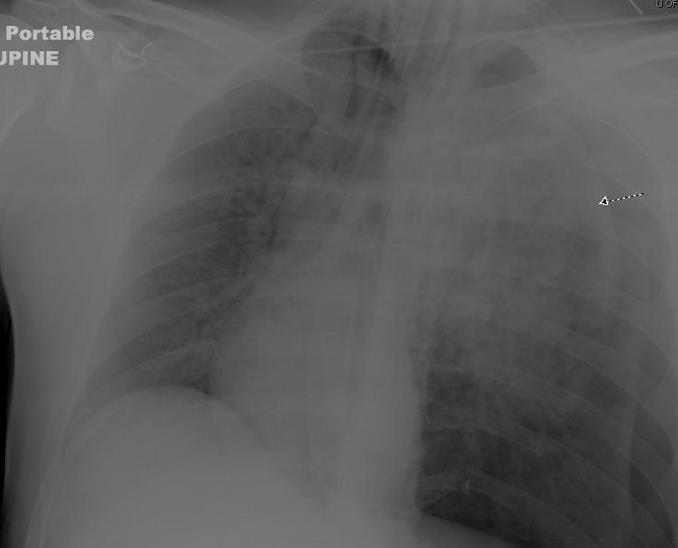
2 Review Question Unilaterally diminished breath sounds A. Figure 1 B. Figure 2 C. Both D. Neither

3 Related Specialties 39
4 Review Question Jugular venous distension A. Figure 1 B. Figure 2 C. Both D. Neither
5 Review Question Muffled heart sounds A. Figure 1 B. Figure 2 C. Both D. Neither
6 Review Question Typically does not require operative intervention A. Figure 1 B. Figure 2 C. Both D. Neither
7 Review Question Which of the following statements about blunt cardiac injuries is TRUE? A. Echocardiography is indicated in patients with hemodynamic instability. B. Bradycardia is a common finding. C. Depressed ST segents on electrocardiogram are pathognomonic. D. Troponin levels should be monitored routinely for 24 hours. E. Chest pain is an indication for hours of monitoring by telemetry.
8 Review Question A 70-year-old man is postoperative day 1 from an omental patch placement for a perforated duodenal ulcer. His lactate is 5 mmol/l, his blood pressure is 90/60 mm Hg, his heart rate is 90 beats per minute, his cardiac index is 2.4 L/min/m2, his pulmonary wedge pressure is 4 cm of H2O, and his central venous pressure is 1 cm of H2O. Which of the following statements is TRUE? A. He is in cardiogenic shock. B. He should be given a crystalloid fluid bolus. C. He should be started on a vasopressin drip. D. He should be started on a phenylephrine drip. E. He should be started on an epinephrine drip.
9 Review Quesiton A 70-year-old diabetic woman is admitted to the intensive care unit in septic shock after an open cholecystectomy for gangrenous cholecystitis. She has refractory hypotension despite aggressive fluid resuscitation and high-dose norepinephrine infusion. Which of the following vasopressive agents is most appropriate to start in this patient? A. Phenylephrine B. Vasopressin C. Ephedrine D. Midodrine E. Dopamine
10 Review Question A 26-year-old man is transported to your hospital after a skiing accident. Chest and pelvis radiographs at the outside hospital are normal, but his lateral cervical spine film shows a subluxation at C6-7. He is alert, responsive, and not hypoxic. On physical exam, he has no sensation or movement beneath the clavicles, no rectal tone, and evidence of priapism. Despite 2-L crystalloid infusion, he has a blood pressure of 75/40 mm Hg and a pulse of 85 beats per minute. Which of the following is the next most appropriate step in this patient s management? A. Norepinephrine infusion B. Dopamine infusion C. CT scan of the spine, chest, abdomen, and eplvis D. MRI of the cervical and thoracic spine E. Focused assessment with sonography for trauma (FAST) exam
11 Review Question A 20-year-old woman is involved in a motor vehicle crash and is unable to move her extremities on admission to the emergency department. She is initially hypotensive but responds to fluid administration. CT scans reveal a cervical spine subluxation injury at C5-C6. Her only other injury is a nondisplaced pubic ramus fracture. No other injuries are seen on the scans of her head, chest, abdomen, and pelvis, and she has no long bone fractures or significant soft tissue injuries. When she arrives at the intensive care unit, her blood pressure falls to 80/50 mm Hg with a pulse of 55 beats per minute and O2 saturation of 99%. With further volume resuscitation, her O2 saturation falls to 88%, but her other vital signs do not change. Pulmonary auscultation reveals rales. Her extremities appear wellperfused with brisk capillary refill. Which of the following is the best treatment for her hypotension? A. Exploratory laparotomy B. Pelvic wrap C. Steroids D. Pressors E. Blood products in a 1:1:1 ratio (red cells:plasma:platelets)

12
13 Pharmacotherapy in shock Vasopressors Norepinephrine Epinephrine Dopamine Phenylephrine Inotropes Dobutamine Dopexamine Isoproterenol Milrinone Levosimendan Miscellaneous Vasopressin Terlipressin Steroids (Drotrecogin Alfa)
14 Overview of pharmacotherapy Goals of therapy: Raise blood pressure Raise heart rate Improve cardiac output Improve tissue perfusion Side effects of therapy Arrhythmias Vasoconstriction
15 Vasopressors
16 Norepinephrine Naturally occurring Potent α-adrenergic effects Less potent β 1 stimulation Indications First line treatment in septic shock May be used for acute hypotension from any cause Moderately arrhythmogenic Peripheral vasoconstriction Leave em Dead Enhances renal function in sepsis
17 Review Question A 54-year-old woman is undergoing a lumpectomy and sentinel node biopsy. Shortly after induction, while the surgeon is injecting isosulfan blue into the breast, the patient becomes hypotensive and flushed, and she becomes difficult to ventilate. From the following agents that the patient received, which is most likely to be the cause of the anaphylactic reaction? A. Isosulfan blue B. Succinylcholine C. Propofol D. Cefazolin E. Lidocaine
18 Epinephrine Major physiologic adrenergic hormone of the adrenal medulla Potently stimulates α 1 receptors Β effects (1 and 2) Chronotropic and inotropic Vasodilation less MAP than Norepinephrine Dose-dependent response Indications Anaphylaxis (β 2 blunts mast cell response) Cardiac arrest/other refractory conditions
19 Dopamine Hormone precursor of norepinephrine and epinephrine Dose dependent α, β, and dopaminergic receptors Renal dose, 0-5μg/kg/min, dopa Middle dose, 5-10μg/kg/min, β High dose, 10-20μg/kg/min, α Arrhythmogenic (particularly lower doses) Indications...
20 Review Question Therapy for a 30-year-old intubated man after fall from 20 feet who is in the intensive care unit with pelvic and thoracic spine fractures, flaccid, warm bilateral lower extremities, bradycardia, hypotension, and negative thoracic, abdominal, and pelvic computed tomography. A. Intravenous dobutamine B. Intravenous phenylephrine C. Transfusion packed red blood cells D. Intravenous corticosteroids E. Intravenous antibiotics
21 Phenylephrine Rapid/short duration Pure α 1 stimulation Increases SVR to increase MAP Reflex bradycardia Impairs cardiac output by increasing afterload Indications Distributive shock with tachyarrhythmia Pregnant patient with shock
22 Review Question Selective alpha-1 adrenergic receptor agonist, potent vasoconstrictor A. Norepinephrine B. Epinephrine C. Phenylephrine D. Vasopressin E. Dobutamine
23 Review Question Alpha and beta-1 adrenergic receptor agonist, used in septic shock A. Norepinephrine B. Epinephrine C. Phenylephrine D. Vasopressin E. Dobutamine
24 Review Question Alpha, beta-1, and beta-2 receptor agonist, produced in the adrenal medulla A. Norepinephrine B. Epinephrine C. Phenylephrine D. Vasopressin E. Dobutamine
25 Inotropes
26 Dobutamine Synthetic adrenergic agent L-isomer α 1 ; D-isomer β 1 /β 2 Indications Pulmonary edema with marginal blood pressure
27 Dopexamine Synthetic catecholamine Dopa/Β 2 >>β 1 causing vasodilation and positive inotropy via afterload decrease; also inhibits Norepi reuptake Improved splanchnic perfusion Indication Compared to dobutamine/dopamine
28 Isoproterenol Pure β agonist May lead to cardiac ischemia Indications β-blocker overdose Atropine-resistant transplanted heart
29 Milrinone Synthetic phosphodiesterase III inhibitor Increases camp Modulates myocardial contractility Vasodilation Indications Cardiogenic shock/cardiac failure Acutely decompensated CHF
30 Levosimendan Increases sensitivity of troponin C for calcium without enhancing nflux of calcium Indications Currently used perioperatiely in cardiac surgery patients Under investigation for use in septic shock, etc.
31 Other pharmacologic therapy
32 Vasopressin Hormone V1 receptors Indications Septic shock (adjunct to norepinephrine) ACLS (along with steroids)
33 Terlipressin Analogue of vasopressin Long half life
34 Review Question Therapy for a 55-year-old woman with severe rheumatoid arthritis in the intensive care unit with tachycardia, hypotension, and fever after recent negative exploratory laparotomy. A. Intravenous dobutamine B. Intravenous phenylephrine C. Transfusion packed red blood cells D. Intravenous corticosteroids E. Intravenous antibiotics
35 Steroids Indications Stress-dose steroids Adrenal insufficiency
36 Drotrecogin Alfa Recombinant Activated protein C Down-regulates proinflammatory state (including anticoagulant/enhance fibrinolysis/opens microcirculation) Off market
37 In Summary, a few recommendations...
38 Recommendations (1) Smaller combined doses of inotropes and vasopressors may be advantageous over a single agent used at higher doses to avoid doserelated adverse effects. Christopher B. Overgaard and Vladimír Džavík. Inotropes and Vasopressors. Circulation; Volume 118(10): September 2, 2008
39 Recommendations (2) The use of vasopressin at low to moderate doses may allow catecholamine sparing, and it may be particularly useful in settings of catecholamine hyposensitivity and after prolonged critical illness. Christopher B. Overgaard and Vladimír Džavík. Inotropes and Vasopressors. Circulation; Volume 118(10): September 2, 2008
40 Recommendations (3) In cardiogenic shock complicating AMI, current guidelines based on expert opinion recommended dopamine or dobutamine as first-line agents with moderate hypotension (systolic blood pressure mm Hg) and norepinephrine as the preferred therapy for severe hypotension (systolic blood pressure Christopher <70 B. Overgaard mmhg). and Vladimír Džavík. Inotropes and Vasopressors. Circulation; Volume 118(10): September 2, 2008
41 Recommendations (4) Routine inotropic use is not recommended for end-stage heart failure. When such use is essential, every effort should be made to either reinstitute stable oral therapy as quickly as possible or use destination therapy such as cardiac transplantation or LV assist device support. Christopher B. Overgaard and Vladimír Džavík. Inotropes and Vasopressors. Circulation; Volume 118(10): September 2, 2008
42 Recommendations (5) Large randomized trials focusing on clinical outcomes are needed to better assess the clinical efficacy of these agents. Christopher B. Overgaard and Vladimír Džavík. Inotropes and Vasopressors. Circulation; Volume 118(10): September 2, 2008
43 Surgical Critical Care I.36 Phosphodiesterase inhibitor A. Phenylephrine B. Fenoldopam C. Amrinone D. Vasopressin E. Nitroglycerin
44 Surgical Critical Care I.37 Pure alpha-agonist A. Phenylephrine B. Fenoldopam C. Amrinone D. Vasopressin E. Nitroglycerin
45 Surgical Critical Care I.38 Antidiuretic A. Phenylephrine B. Fenoldopam C. Amrinone D. Vasopressin E. Nitroglycerin
46 Surgical Critical Care I.39 Dopaminergic receptor agonist A. Phenylephrine B. Fenoldopam C. Amrinone D. Vasopressin E. Nitroglycerin
47 Surgical Critical Care I.40 Venodilator A. Phenylephrine B. Fenoldopam C. Amrinone D. Vasopressin E. Nitroglycerin
48 Surgical Critical Care II.38 Potent alpha-adrenergic activity; no affinity for beta-adrenergic receptors; minimal direct effect on heart rate A. Dopamine B. Dobutamine C. Norepinephrine D. Epinephrine E. Phenylephrine
49 Surgical Critical Care II.39 Affinity for both beta-1 and beta-2 adrenergic receptors; mild vasodilator effects A. Dopamine B. Dobutamine C. Norepinephrine D. Epinephrine E. Phenylephrine
50 Surgical Critical Care II.40 Dose-dependent alpha- and betareceptor affinity; increases cardiac contractility and heart rate A. Dopamine B. Dobutamine C. Norepinephrine D. Epinephrine E. Phenylephrine
51 Summary
Titrating Critical Care Medications
 Titrating Critical Care Medications Chad Johnson, MSN (NED), RN, CNCC(C), CNS-cc Clinical Nurse Specialist: Critical Care and Neurosurgical Services E-mail: johnsoc@tbh.net Copyright 2017 1 Learning Objectives
Titrating Critical Care Medications Chad Johnson, MSN (NED), RN, CNCC(C), CNS-cc Clinical Nurse Specialist: Critical Care and Neurosurgical Services E-mail: johnsoc@tbh.net Copyright 2017 1 Learning Objectives
Introduction. Invasive Hemodynamic Monitoring. Determinants of Cardiovascular Function. Cardiovascular System. Hemodynamic Monitoring
 Introduction Invasive Hemodynamic Monitoring Audis Bethea, Pharm.D. Assistant Professor Therapeutics IV January 21, 2004 Hemodynamic monitoring is necessary to assess and manage shock Information obtained
Introduction Invasive Hemodynamic Monitoring Audis Bethea, Pharm.D. Assistant Professor Therapeutics IV January 21, 2004 Hemodynamic monitoring is necessary to assess and manage shock Information obtained
HYPOTENSION IS DANGEROUS C. R Y A N K E A Y, M D, F A C E P 1 6 M A R C H
 HYPOTENSION IS DANGEROUS C. R Y A N K E A Y, M D, F A C E P 1 6 M A R C H 2 0 1 8 OBJECTIVES Case-based overview of pressors Debunking pressor myths Utilizing push-dose pressors CASE 1 82-year old male,
HYPOTENSION IS DANGEROUS C. R Y A N K E A Y, M D, F A C E P 1 6 M A R C H 2 0 1 8 OBJECTIVES Case-based overview of pressors Debunking pressor myths Utilizing push-dose pressors CASE 1 82-year old male,
Vasoactive drugs. Dr. Zohair Alaseri, MD
 Vasoactive drugs Dr. Zohair Alaseri, MD FRCPc, Emergency Medicine FRCPc, Critical Care Medicine Intensivest and Emergency Medicine Consultant Chairman, Department of Emergency Medicine King Saud University
Vasoactive drugs Dr. Zohair Alaseri, MD FRCPc, Emergency Medicine FRCPc, Critical Care Medicine Intensivest and Emergency Medicine Consultant Chairman, Department of Emergency Medicine King Saud University
Pharmacology of inotropes and vasopressors
 Pharmacology of inotropes and vasopressors Curriculum 3.3 Recognises and manages the patient with circulatory failure 4.4 Uses fluids and vasoactive / inotropic drugs to support the circulation PR_BK_41
Pharmacology of inotropes and vasopressors Curriculum 3.3 Recognises and manages the patient with circulatory failure 4.4 Uses fluids and vasoactive / inotropic drugs to support the circulation PR_BK_41
Case year old female nursing home resident with a hx CAD, PUD, recent hip fracture Transferred to ED with decreased mental status BP in ED 80/50
 Case 1 65 year old female nursing home resident with a hx CAD, PUD, recent hip fracture Transferred to ED with decreased mental status BP in ED 80/50 Case 1 65 year old female nursing home resident with
Case 1 65 year old female nursing home resident with a hx CAD, PUD, recent hip fracture Transferred to ED with decreased mental status BP in ED 80/50 Case 1 65 year old female nursing home resident with
The Pharmacology of Hypotension: Vasopressor Choices for HIE patients. Keliana O Mara, PharmD August 4, 2018
 The Pharmacology of Hypotension: Vasopressor Choices for HIE patients Keliana O Mara, PharmD August 4, 2018 Objectives Review the pathophysiology of hypotension in neonates Discuss the role of vasopressors
The Pharmacology of Hypotension: Vasopressor Choices for HIE patients Keliana O Mara, PharmD August 4, 2018 Objectives Review the pathophysiology of hypotension in neonates Discuss the role of vasopressors
Vasoactive Medications. Matthew J. Korobey Pharm.D., BCCCP Critical Care Clinical Specialist Mercy St. Louis
 Vasoactive Medications Matthew J. Korobey Pharm.D., BCCCP Critical Care Clinical Specialist Mercy St. Louis Objectives List components of physiology involved in blood pressure Review terminology related
Vasoactive Medications Matthew J. Korobey Pharm.D., BCCCP Critical Care Clinical Specialist Mercy St. Louis Objectives List components of physiology involved in blood pressure Review terminology related
VASOPRESSORS AND INOTROPES CLINICAL PROFESSOR ANDREW BEZZINA FACEM MAY 2017
 VASOPRESSORS AND INOTROPES CLINICAL PROFESSOR ANDREW BEZZINA FACEM MAY 2017 CONFLICTS OF INTEREST OVERVIEW Why? When? What? How? WHY? Circulation WHY? - SHOCK!!! Pump (Heart) HYPOVOLAEMIC the pipes have
VASOPRESSORS AND INOTROPES CLINICAL PROFESSOR ANDREW BEZZINA FACEM MAY 2017 CONFLICTS OF INTEREST OVERVIEW Why? When? What? How? WHY? Circulation WHY? - SHOCK!!! Pump (Heart) HYPOVOLAEMIC the pipes have
การอบรมว ทยาศาสตร พ นฐานทางศ ลยศาสตร เร อง นพ.ส ณฐ ต โมราก ล ภาคว ชาว ส ญญ ว ทยา คณะแพทยศาสตร โรงพยาบาลรามาธ บด มหาวทยาลยมหดล
 การอบรมว ทยาศาสตร พ นฐานทางศ ลยศาสตร เร อง นพ.ส ณฐ ต โมราก ล ภาคว ชาว ส ญญ ว ทยา คณะแพทยศาสตร โรงพยาบาลรามาธ บด มหาวทยาลยมหดล Distributive shock Severe sepsis and Septic shock Anaphylactic shock Neurogenic
การอบรมว ทยาศาสตร พ นฐานทางศ ลยศาสตร เร อง นพ.ส ณฐ ต โมราก ล ภาคว ชาว ส ญญ ว ทยา คณะแพทยศาสตร โรงพยาบาลรามาธ บด มหาวทยาลยมหดล Distributive shock Severe sepsis and Septic shock Anaphylactic shock Neurogenic
Swans and Pressors. Vanderbilt Surgery Summer School Ricky Shinall
 Swans and Pressors Vanderbilt Surgery Summer School Ricky Shinall Shock, Swans, Pressors in 15 minutes 4 Reasons for Shock 4 Swan numbers to know 7 Pressors =15 things to know 4 Reasons for Shock Not enough
Swans and Pressors Vanderbilt Surgery Summer School Ricky Shinall Shock, Swans, Pressors in 15 minutes 4 Reasons for Shock 4 Swan numbers to know 7 Pressors =15 things to know 4 Reasons for Shock Not enough
Swans and Pressors. Vanderbilt Surgery Summer School Ricky Shinall
 Swans and Pressors Vanderbilt Surgery Summer School Ricky Shinall SHOCK Hypotension SHOCK Hypotension SHOCK=Reduction of systemic tissue perfusion, resulting in decreased oxygen delivery to the tissues.
Swans and Pressors Vanderbilt Surgery Summer School Ricky Shinall SHOCK Hypotension SHOCK Hypotension SHOCK=Reduction of systemic tissue perfusion, resulting in decreased oxygen delivery to the tissues.
Utilizing Vasopressors:
 Utilizing Vasopressors: Critical Care Advances in the Emergency Department José A. Rubero, MD, FACEP, FAAEM Associate Program Director University of Central Florida/HCA GME Consortium Emergency Medicine
Utilizing Vasopressors: Critical Care Advances in the Emergency Department José A. Rubero, MD, FACEP, FAAEM Associate Program Director University of Central Florida/HCA GME Consortium Emergency Medicine
SHOCK. Emergency pediatric PICU division Pediatric Department Medical Faculty, University of Sumatera Utara H. Adam Malik Hospital
 SHOCK Emergency pediatric PICU division Pediatric Department Medical Faculty, University of Sumatera Utara H. Adam Malik Hospital 1 Definition Shock is an acute, complex state of circulatory dysfunction
SHOCK Emergency pediatric PICU division Pediatric Department Medical Faculty, University of Sumatera Utara H. Adam Malik Hospital 1 Definition Shock is an acute, complex state of circulatory dysfunction
DIAGNOSIS AND MANAGEMENT OF ACUTE HEART FAILURE
 DIAGNOSIS AND MANAGEMENT OF ACUTE HEART FAILURE Mefri Yanni, MD Bagian Kardiologi dan Kedokteran Vaskular RS.DR.M.Djamil Padang The 3rd Symcard Padang, Mei 2013 Outline Diagnosis Diagnosis Treatment options
DIAGNOSIS AND MANAGEMENT OF ACUTE HEART FAILURE Mefri Yanni, MD Bagian Kardiologi dan Kedokteran Vaskular RS.DR.M.Djamil Padang The 3rd Symcard Padang, Mei 2013 Outline Diagnosis Diagnosis Treatment options
Nothing to Disclose. Severe Pulmonary Hypertension
 Severe Ronald Pearl, MD, PhD Professor and Chair Department of Anesthesiology Stanford University Rpearl@stanford.edu Nothing to Disclose 65 year old female Elective knee surgery NYHA Class 3 Aortic stenosis
Severe Ronald Pearl, MD, PhD Professor and Chair Department of Anesthesiology Stanford University Rpearl@stanford.edu Nothing to Disclose 65 year old female Elective knee surgery NYHA Class 3 Aortic stenosis
MANAGEMENT OF CIRCULATORY FAILURE
 MANAGEMENT OF CIRCULATORY FAILURE BACKGROUND AND DEFINITION There is no consensus on the definition of circulatory failure or shock in newborns; it can be defined as global tissue hypoxia secondary to
MANAGEMENT OF CIRCULATORY FAILURE BACKGROUND AND DEFINITION There is no consensus on the definition of circulatory failure or shock in newborns; it can be defined as global tissue hypoxia secondary to
Evidence-Based. Management of Severe Sepsis. What is the BP Target?
 Evidence-Based Management of Severe Sepsis Michael A. Gropper, MD, PhD Professor and Vice Chair of Anesthesia Director, Critical Care Medicine Chair, Quality Improvment University of California San Francisco
Evidence-Based Management of Severe Sepsis Michael A. Gropper, MD, PhD Professor and Vice Chair of Anesthesia Director, Critical Care Medicine Chair, Quality Improvment University of California San Francisco
When Fluids are Not Enough: Inopressor Therapy
 When Fluids are Not Enough: Inopressor Therapy Problems in Neonatology Neonatal problem: hypoperfusion Severe sepsis Hallmark of septic shock Secondary to neonatal encephalopathy Vasoplegia Syndrome??
When Fluids are Not Enough: Inopressor Therapy Problems in Neonatology Neonatal problem: hypoperfusion Severe sepsis Hallmark of septic shock Secondary to neonatal encephalopathy Vasoplegia Syndrome??
Utilizing Vasopressors:
 Utilizing Vasopressors: Critical Care Advances in the Emergency Department José A. Rubero, MD, FACEP, FAAEM Associate Program Director University of Central Florida/HCA GME Consortium Emergency Medicine
Utilizing Vasopressors: Critical Care Advances in the Emergency Department José A. Rubero, MD, FACEP, FAAEM Associate Program Director University of Central Florida/HCA GME Consortium Emergency Medicine
Useful diagnostic measures: chest x ray to check pulmonary edema, ECG and ECHO to detect cardiac abnormalities (1).
.") Cardiogenic shock Etiology The most common cause of cardiogenic shock is LV dysfunction and necrosis as a result of acute myocardial infarction (AMI) (1). Acute valvular insufficiency or stenosis prevents
Cardiogenic shock Etiology The most common cause of cardiogenic shock is LV dysfunction and necrosis as a result of acute myocardial infarction (AMI) (1). Acute valvular insufficiency or stenosis prevents
Disclosures. Objectives 10/11/17. Short Term Mechanical Circulatory Support for Advanced Cardiogenic Shock. I have no disclosures to report
 Short Term Mechanical Circulatory Support for Advanced Cardiogenic Shock Christopher K. Gordon MSN, ACNP-BC Disclosures I have no disclosures to report 1. Pathophysiology 2. Epidemiology 3. Assessment
Short Term Mechanical Circulatory Support for Advanced Cardiogenic Shock Christopher K. Gordon MSN, ACNP-BC Disclosures I have no disclosures to report 1. Pathophysiology 2. Epidemiology 3. Assessment
Dilemmas in Septic Shock
 Dilemmas in Septic Shock William Janssen, M.D. Assistant Professor of Medicine National Jewish Health University of Colorado Denver Health Sciences Center A 62 year-old female presents to the ED with fever,
Dilemmas in Septic Shock William Janssen, M.D. Assistant Professor of Medicine National Jewish Health University of Colorado Denver Health Sciences Center A 62 year-old female presents to the ED with fever,
Medical Treatment for acute Decompensated Heart Failure. Vlasis Ninios Cardiologist St. Luke s s Hospital Thessaloniki 2011
 Medical Treatment for acute Decompensated Heart Failure Vlasis Ninios Cardiologist St. Luke s s Hospital Thessaloniki 2011 2010 HFSA guidelines for ADHF 2009 focused update of the 2005 American College
Medical Treatment for acute Decompensated Heart Failure Vlasis Ninios Cardiologist St. Luke s s Hospital Thessaloniki 2011 2010 HFSA guidelines for ADHF 2009 focused update of the 2005 American College
HOW LOW CAN YOU GO? HYPOTENSION AND THE ANESTHETIZED PATIENT.
 HOW LOW CAN YOU GO? HYPOTENSION AND THE ANESTHETIZED PATIENT. Donna M. Sisak, CVT, LVT, VTS (Anesthesia/Analgesia) Seattle Veterinary Specialists Kirkland, WA dsisak@svsvet.com THE ANESTHETIZED PATIENT
HOW LOW CAN YOU GO? HYPOTENSION AND THE ANESTHETIZED PATIENT. Donna M. Sisak, CVT, LVT, VTS (Anesthesia/Analgesia) Seattle Veterinary Specialists Kirkland, WA dsisak@svsvet.com THE ANESTHETIZED PATIENT
4/5/2018. Update on Sepsis NIKHIL JAGAN PULMONARY AND CRITICAL CARE CREIGHTON UNIVERSITY. I have no financial disclosures
 Update on Sepsis NIKHIL JAGAN PULMONARY AND CRITICAL CARE CREIGHTON UNIVERSITY I have no financial disclosures 1 Objectives Why do we care about sepsis Understanding the core measures by Centers for Medicare
Update on Sepsis NIKHIL JAGAN PULMONARY AND CRITICAL CARE CREIGHTON UNIVERSITY I have no financial disclosures 1 Objectives Why do we care about sepsis Understanding the core measures by Centers for Medicare
The Art and Science of Infusion Nursing John M. Allen, PharmD, BCPS. Understanding Vasoactive Medications
 The Art and Science of Infusion Nursing John M. Allen, PharmD, BCPS Understanding Vasoactive Medications Focus on Pharmacology and Effective Titration ABSTRACT In the care of the critically ill patient,
The Art and Science of Infusion Nursing John M. Allen, PharmD, BCPS Understanding Vasoactive Medications Focus on Pharmacology and Effective Titration ABSTRACT In the care of the critically ill patient,
Pediatric Septic Shock. Geoffrey M. Fleming M.D. Division of Pediatric Critical Care Vanderbilt University School of Medicine Nashville, Tennessee
 Pediatric Septic Shock Geoffrey M. Fleming M.D. Division of Pediatric Critical Care Vanderbilt University School of Medicine Nashville, Tennessee Case 4 year old male with a history of gastroschesis repaired
Pediatric Septic Shock Geoffrey M. Fleming M.D. Division of Pediatric Critical Care Vanderbilt University School of Medicine Nashville, Tennessee Case 4 year old male with a history of gastroschesis repaired
Intravenous Inotropic Support an Overview
 Intravenous Inotropic Support an Overview Shaul Atar, MD Western Galilee Medical Center, Nahariya Affiliated with the Faculty of Medicine of the Galilee, Safed, Israel INOTROPES in Acute HF (not vasopressors)
Intravenous Inotropic Support an Overview Shaul Atar, MD Western Galilee Medical Center, Nahariya Affiliated with the Faculty of Medicine of the Galilee, Safed, Israel INOTROPES in Acute HF (not vasopressors)
The Hypotensive Poisoned Patient. Robert S. Hoffman, MD Director, NYC PCC
 The Hypotensive Poisoned Patient Robert S. Hoffman, MD Director, NYC PCC Some Definitions Hypotension = Low blood pressure Failure of macrocirculation Shock = Poor tissue perfusion Failure of microcirculation
The Hypotensive Poisoned Patient Robert S. Hoffman, MD Director, NYC PCC Some Definitions Hypotension = Low blood pressure Failure of macrocirculation Shock = Poor tissue perfusion Failure of microcirculation
7/21/2017. Learning Objectives. Current Cardiovascular Pharmacology. Epinephrine. Cardiotonic Agents. Epinephrine. Epinephrine. Arthur Jones, EdD, RRT
 Learning Objectives Current Cardiovascular Pharmacology Arthur Jones, EdD, RRT Explain the actions, effects, indications, adverse effects, & precautions for agents from the following drug categories Cardiotonic
Learning Objectives Current Cardiovascular Pharmacology Arthur Jones, EdD, RRT Explain the actions, effects, indications, adverse effects, & precautions for agents from the following drug categories Cardiotonic
Percutaneous Mechanical Circulatory Support for Cardiogenic Shock. 24 th Annual San Diego Heart Failure Symposium Ryan R Reeves, MD FSCAI
 Percutaneous Mechanical Circulatory Support for Cardiogenic Shock 24 th Annual San Diego Heart Failure Symposium Ryan R Reeves, MD FSCAI The Need for Circulatory Support Basic Pathophysiologic Problems:
Percutaneous Mechanical Circulatory Support for Cardiogenic Shock 24 th Annual San Diego Heart Failure Symposium Ryan R Reeves, MD FSCAI The Need for Circulatory Support Basic Pathophysiologic Problems:
Agenda เอกราช อร ยะช ยพาณ ชย. - Cardiac physiology - Pathophysiology of shock - Pathophysiology of heart failure 9/6/2016
 6 September 2016 เอกราช อร ยะช ยพาณ ชย Heart Failure and Transplant Cardiology aekarach.a@chula.ac.th Agenda - Cardiac physiology - Pathophysiology of shock - Pathophysiology of heart failure http://fullpulse.weebly.com/conversation
6 September 2016 เอกราช อร ยะช ยพาณ ชย Heart Failure and Transplant Cardiology aekarach.a@chula.ac.th Agenda - Cardiac physiology - Pathophysiology of shock - Pathophysiology of heart failure http://fullpulse.weebly.com/conversation
Medical Management of Acute Heart Failure
 Critical Care Medicine and Trauma Medical Management of Acute Heart Failure Mary O. Gray, MD, FAHA Associate Professor of Medicine University of California, San Francisco Staff Cardiologist and Training
Critical Care Medicine and Trauma Medical Management of Acute Heart Failure Mary O. Gray, MD, FAHA Associate Professor of Medicine University of California, San Francisco Staff Cardiologist and Training
Medical Management of Acutely Decompensated Heart Failure. William T. Abraham, MD Director, Division of Cardiovascular Medicine
 Medical Management of Acutely Decompensated Heart Failure William T. Abraham, MD Director, Division of Cardiovascular Medicine Orlando, Florida October 7-9, 2011 Goals of Acute Heart Failure Therapy Alleviate
Medical Management of Acutely Decompensated Heart Failure William T. Abraham, MD Director, Division of Cardiovascular Medicine Orlando, Florida October 7-9, 2011 Goals of Acute Heart Failure Therapy Alleviate
ACUTE HEART FAILURE. Julie Gorchynski MD, MSc, FACEP, FAAEM. Department of Emergency Medicine Emergency Residency Program UTHSC, San Antonio TCEP 2014
 ACUTE HEART FAILURE Julie Gorchynski MD, MSc, FACEP, FAAEM Department of Emergency Medicine Emergency Residency Program UTHSC, San Antonio TCEP 2014 No disclosures Objectives Overview Cases Current Therapy
ACUTE HEART FAILURE Julie Gorchynski MD, MSc, FACEP, FAAEM Department of Emergency Medicine Emergency Residency Program UTHSC, San Antonio TCEP 2014 No disclosures Objectives Overview Cases Current Therapy
Intravenous Infusions
 Intravenous Infusions 1) An IV insulin infusion can be used for patients: a) with out of control diabetes b) with DKA (Diabetic Ketoacidosis) c) after a heart attack 2) Hyperglycemia is an adaptive response
Intravenous Infusions 1) An IV insulin infusion can be used for patients: a) with out of control diabetes b) with DKA (Diabetic Ketoacidosis) c) after a heart attack 2) Hyperglycemia is an adaptive response
Surviving Sepsis Campaign Guidelines 2012 & Update for David E. Tannehill, DO Critical Care Medicine Mercy Hospital St.
 Surviving Sepsis Campaign Guidelines 2012 & Update for 2015 David E. Tannehill, DO Critical Care Medicine Mercy Hospital St. Louis Be appropriately aggressive the longer one delays aggressive metabolic
Surviving Sepsis Campaign Guidelines 2012 & Update for 2015 David E. Tannehill, DO Critical Care Medicine Mercy Hospital St. Louis Be appropriately aggressive the longer one delays aggressive metabolic
Index. Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type. A Abdomen, and aorta, as causes of shock, point-of-care ultrasonography in assessment of, 915 917 Abdominal compartment syndrome, trauma patient
Note: Page numbers of article titles are in boldface type. A Abdomen, and aorta, as causes of shock, point-of-care ultrasonography in assessment of, 915 917 Abdominal compartment syndrome, trauma patient
7/4/2015. Titrating Vasoactive Drips
 Leanna R. Miller RN, MN, CCRN-CMC, PCCN-CSC, CEN, NP LRM Consulting Vasoactive medications are indicated when the SBP has a decrease of > 30mmHg from the baseline or a MAP < 60mmHg and when either condition
Leanna R. Miller RN, MN, CCRN-CMC, PCCN-CSC, CEN, NP LRM Consulting Vasoactive medications are indicated when the SBP has a decrease of > 30mmHg from the baseline or a MAP < 60mmHg and when either condition
Sepsis Bundle Project (SEP) Kathy Wonderly RN, MSEd, CPHQ Consultant Developed: April 2015 Most recent Revision: December 2018
 Kathy Wonderly RN, MSEd, CPHQ Consultant Developed: April 2015 Most recent Revision: December 2018") Sepsis Bundle Project (SEP) Kathy Wonderly RN, MSEd, CPHQ Consultant Developed: April 2015 Most recent Revision: December 2018 Objectives 1. To identify the symptom of severe sepsis and septic shock syndrome.
Sepsis Bundle Project (SEP) Kathy Wonderly RN, MSEd, CPHQ Consultant Developed: April 2015 Most recent Revision: December 2018 Objectives 1. To identify the symptom of severe sepsis and septic shock syndrome.
John Park, MD Assistant Professor of Medicine
 John Park, MD Assistant Professor of Medicine Faculty photo will be placed here park.john@mayo.edu 2015 MFMER 3543652-1 Sepsis Out with the Old, In with the New Mayo School of Continuous Professional Development
John Park, MD Assistant Professor of Medicine Faculty photo will be placed here park.john@mayo.edu 2015 MFMER 3543652-1 Sepsis Out with the Old, In with the New Mayo School of Continuous Professional Development
When Fluids are Not Enough: Inopressor Therapy
 When Fluids are Not Enough: Inopressor Therapy Problems in Neonatology Neonatal problem: hypoperfusion Severe sepsis Hallmark of septic shock Secondary to neonatal encephalopathy Vasoplegia Syndrome??
When Fluids are Not Enough: Inopressor Therapy Problems in Neonatology Neonatal problem: hypoperfusion Severe sepsis Hallmark of septic shock Secondary to neonatal encephalopathy Vasoplegia Syndrome??
Post Cardiac Arrest Care 2015 American Heart Association Guideline Update for CPR and Emergency Cardiovascular Care
 Post Cardiac Arrest Care 2015 American Heart Association Guideline Update for CPR and Emergency Cardiovascular Care รศ.ดร.พญ.ต นหยง พ พานเมฆาภรณ ภาคว ชาว ส ญญ ว ทยา คณะแพทยศาสตร มหาว ทยาล ยเช ยงใหม System
Post Cardiac Arrest Care 2015 American Heart Association Guideline Update for CPR and Emergency Cardiovascular Care รศ.ดร.พญ.ต นหยง พ พานเมฆาภรณ ภาคว ชาว ส ญญ ว ทยา คณะแพทยศาสตร มหาว ทยาล ยเช ยงใหม System
12/1/2009. Chapter 19: Hemorrhage. Hemorrhage and Shock Occurs when there is a disruption or leak in the vascular system Internal hemorrhage
 Chapter 19: Hemorrhage Hemorrhage and Shock Occurs when there is a disruption or leak in the vascular system External hemorrhage Internal hemorrhage Associated with higher morbidity and mortality than
Chapter 19: Hemorrhage Hemorrhage and Shock Occurs when there is a disruption or leak in the vascular system External hemorrhage Internal hemorrhage Associated with higher morbidity and mortality than
SHOCK. May 12, 2011 Body and Disease
 SHOCK May 12, 2011 Body and Disease Shock Definition of shock Pathophysiology Types of shock Management of shock Shock Definition? Shock What the Duke Community would have experienced if Gordon Hayward
SHOCK May 12, 2011 Body and Disease Shock Definition of shock Pathophysiology Types of shock Management of shock Shock Definition? Shock What the Duke Community would have experienced if Gordon Hayward
Sepsis: Identification and Management in an Acute Care Setting
 Sepsis: Identification and Management in an Acute Care Setting Dr. Barbara M. Mills DNP Director Rapid Response Team/ Code Resuscitation Stony Brook University Medical Center SEPSIS LECTURE NPA 2018 OBJECTIVES
Sepsis: Identification and Management in an Acute Care Setting Dr. Barbara M. Mills DNP Director Rapid Response Team/ Code Resuscitation Stony Brook University Medical Center SEPSIS LECTURE NPA 2018 OBJECTIVES
Cardiovascular Active Medications
 Co-assistenten les 2017-2018 L. Al tmimi, MD, PhD Student Department of Anesthesia University hospitals Leuven Many drugs are used to manage hemodynamic before, during and after any operation Drug errors
Co-assistenten les 2017-2018 L. Al tmimi, MD, PhD Student Department of Anesthesia University hospitals Leuven Many drugs are used to manage hemodynamic before, during and after any operation Drug errors
SHOCK in Paediatric Trauma
 SHOCK in Paediatric Trauma Speaker: Tang Sze Kit, (Fellow, Hong Kong College of Paediatric Nursing, MSc, MN, BN) Date: 26/4/2016 Time: 18:30-19:30 Venue: Paediatrics & Adolescent Ambulatory Centre, G/F,
SHOCK in Paediatric Trauma Speaker: Tang Sze Kit, (Fellow, Hong Kong College of Paediatric Nursing, MSc, MN, BN) Date: 26/4/2016 Time: 18:30-19:30 Venue: Paediatrics & Adolescent Ambulatory Centre, G/F,
Δακτυλίτιδα και Ινότροπα Φάρμακα στην Καρδιακή Ανεπάρκεια. Ι.Κανονίδης
 Δακτυλίτιδα και Ινότροπα Φάρμακα στην Καρδιακή Ανεπάρκεια Ι.Κανονίδης Cardiac Glycosides Chronic Congestive Heart Failure DIGOXIN Na-K ATPase Na + K + Na-Ca Exchange Na + Ca ++ Ca ++ K + Na + Myofilaments
Δακτυλίτιδα και Ινότροπα Φάρμακα στην Καρδιακή Ανεπάρκεια Ι.Κανονίδης Cardiac Glycosides Chronic Congestive Heart Failure DIGOXIN Na-K ATPase Na + K + Na-Ca Exchange Na + Ca ++ Ca ++ K + Na + Myofilaments
Cardiovascular Active Medications
 Co-assistenten 2015-2016 L. Al tmimi, MD, PhD Student Department of Anesthesia University hospitals Leuven Introduction Many drugs are used to manage hemodynamic before, during and after any operation
Co-assistenten 2015-2016 L. Al tmimi, MD, PhD Student Department of Anesthesia University hospitals Leuven Introduction Many drugs are used to manage hemodynamic before, during and after any operation
Cardiovascular Management of Septic Shock
 Cardiovascular Management of Septic Shock R. Phillip Dellinger, MD Professor of Medicine Robert Wood Johnson Medical School/UMDNJ Director, Critical Care Medicine and Med/Surg ICU Cooper University Hospital
Cardiovascular Management of Septic Shock R. Phillip Dellinger, MD Professor of Medicine Robert Wood Johnson Medical School/UMDNJ Director, Critical Care Medicine and Med/Surg ICU Cooper University Hospital
Tissue oxygenation is dependent upon, cardiac output, hemoglobin saturation and peripheral micro circulation.
 Editorial Shock occurs when there is circulatory failure that results in inadequate cellular oxygen, that is arterial blood flow is inadequate to meet tissue metabolic needs. Tissue oxygenation is dependent
Editorial Shock occurs when there is circulatory failure that results in inadequate cellular oxygen, that is arterial blood flow is inadequate to meet tissue metabolic needs. Tissue oxygenation is dependent
Blanchard Valley Hospital Pharmacy Code Blue Overview
 Blanchard Valley Hospital Pharmacy Code Blue Overview Adapted from Gary Spanik, RPh Edited by Kate Reeves, Pharm D, RPh Jon Manocchio, Pharm D, RPh Pharmacist Responsibilities Be aware of basic ACLS tenets
Blanchard Valley Hospital Pharmacy Code Blue Overview Adapted from Gary Spanik, RPh Edited by Kate Reeves, Pharm D, RPh Jon Manocchio, Pharm D, RPh Pharmacist Responsibilities Be aware of basic ACLS tenets
Objectives. Epidemiology of Sepsis. Review Guidelines for Resuscitation. Tx: EGDT, timing/choice of abx, activated
 Update on Surviving Sepsis 2008 Objectives Epidemiology of Sepsis Definition of Sepsis and Septic Shock Review Guidelines for Resuscitation Dx: Lactate, t cultures, SVO2 Tx: EGDT, timing/choice of abx,
Update on Surviving Sepsis 2008 Objectives Epidemiology of Sepsis Definition of Sepsis and Septic Shock Review Guidelines for Resuscitation Dx: Lactate, t cultures, SVO2 Tx: EGDT, timing/choice of abx,
Cardiovascular Active Medications
 Co-assistenten 2014-2015 L. Al tmimi, MD Department of Anesthesia University hospitals Of Leuven Introduction Many drugs are used to manage hemodynamic before, during and after any operation Drug errors
Co-assistenten 2014-2015 L. Al tmimi, MD Department of Anesthesia University hospitals Of Leuven Introduction Many drugs are used to manage hemodynamic before, during and after any operation Drug errors
เอกราช อร ยะช ยพาณ ชย
 25 September 2017 เอกราช อร ยะช ยพาณ ชย Heart Failure and Transplant Cardiology aekarach.a@chula.ac.th Presentation at 1 Agenda Physiology of the heart Pathophysiology of shock Pathophysiology of heart
25 September 2017 เอกราช อร ยะช ยพาณ ชย Heart Failure and Transplant Cardiology aekarach.a@chula.ac.th Presentation at 1 Agenda Physiology of the heart Pathophysiology of shock Pathophysiology of heart
Vasopressors for shock
 Vasopressors for shock Background Reviews and Observational Studies Holler 2015. Nontraumatic Hypotension and Shock in the Emergency Department and Prehospital Setting Prevalence, Etiology and Mortality:
Vasopressors for shock Background Reviews and Observational Studies Holler 2015. Nontraumatic Hypotension and Shock in the Emergency Department and Prehospital Setting Prevalence, Etiology and Mortality:
Resuscitation Before Emergency Surgeries FEIRAN LOU SUNY DOWNSTATE MEDICAL CENTER KINGS COUNTY HOSPITAL
 Resuscitation Before Emergency Surgeries FEIRAN LOU SUNY DOWNSTATE MEDICAL CENTER KINGS COUNTY HOSPITAL Case 73 yo woman h/o HTN three days abdominal pain and nausea. The pain was diffuse, cramp-like,
Resuscitation Before Emergency Surgeries FEIRAN LOU SUNY DOWNSTATE MEDICAL CENTER KINGS COUNTY HOSPITAL Case 73 yo woman h/o HTN three days abdominal pain and nausea. The pain was diffuse, cramp-like,
-Cardiogenic: shock state resulting from impairment or failure of myocardium
 Shock chapter Shock -Condition in which tissue perfusion is inadequate to deliver oxygen, nutrients to support vital organs, cellular function -Affects all body systems -Classic signs of early shock: Tachycardia,tachypnea,restlessness,anxiety,
Shock chapter Shock -Condition in which tissue perfusion is inadequate to deliver oxygen, nutrients to support vital organs, cellular function -Affects all body systems -Classic signs of early shock: Tachycardia,tachypnea,restlessness,anxiety,
Staging Sepsis for the Emergency Department: Physician
 Staging Sepsis for the Emergency Department: Physician Sepsis Continuum 1 Sepsis Continuum SIRS = 2 or more clinical criteria, resulting in Systemic Inflammatory Response Syndrome Sepsis = SIRS + proven/suspected
Staging Sepsis for the Emergency Department: Physician Sepsis Continuum 1 Sepsis Continuum SIRS = 2 or more clinical criteria, resulting in Systemic Inflammatory Response Syndrome Sepsis = SIRS + proven/suspected
SEPSIS SYNDROME
 INTRODUCTION Sepsis has been defined as a life threatening condition that arises when the body s response to an infection injures its own tissues and organs. Sepsis may lead to shock, multiple organ failure
INTRODUCTION Sepsis has been defined as a life threatening condition that arises when the body s response to an infection injures its own tissues and organs. Sepsis may lead to shock, multiple organ failure
Identification & Treatment of Sepsis for the Pediatric Population
 Identification & Treatment of Sepsis for the Pediatric Population Priya Narang, PharmD, MS PGY-1 Pharmacy Practice Resident A presentation for HealthTrust Members March 13, 2018 Disclosures This program
Identification & Treatment of Sepsis for the Pediatric Population Priya Narang, PharmD, MS PGY-1 Pharmacy Practice Resident A presentation for HealthTrust Members March 13, 2018 Disclosures This program
Dr Nick Taylor Visiting Emergency Specialist Teaching Hospital Karapitiya
 Dr Nick Taylor Visiting Emergency Specialist Teaching Hospital Karapitiya Senior Specialist and Director ED Training Clinical Lecturer, Australian National University Canberra Hospital, Australia Inotropes
Dr Nick Taylor Visiting Emergency Specialist Teaching Hospital Karapitiya Senior Specialist and Director ED Training Clinical Lecturer, Australian National University Canberra Hospital, Australia Inotropes
Impedance Cardiography (ICG) Application of ICG in Intensive Care and Emergency
 Application of ICG in Intensive Care and Emergency") Impedance Cardiography (ICG) Application of ICG in Intensive Care and Emergency Aim of haemodynamic monitoring in ICU and ED Detection and therapy of insufficient organ perfusion Answers to common cardiovascular
Impedance Cardiography (ICG) Application of ICG in Intensive Care and Emergency Aim of haemodynamic monitoring in ICU and ED Detection and therapy of insufficient organ perfusion Answers to common cardiovascular
VASOACTIVE DRUGS AND THEIR USE IN SHOCK. Learning Objectives. Shock 10/5/2016
 VASOACTIVE DRUGS AND THEIR USE IN SHOCK October 13, 2016 David Castillo, PharmD, BCPS Emergency Department Lead Clinical Pharmacist Peacehealth Southwest Medical Center DCastillo@peacehealth.org Learning
VASOACTIVE DRUGS AND THEIR USE IN SHOCK October 13, 2016 David Castillo, PharmD, BCPS Emergency Department Lead Clinical Pharmacist Peacehealth Southwest Medical Center DCastillo@peacehealth.org Learning
Hypotension in the Neonate
 Neonatal Nursing Education Brief: Hypotension in the Neonate http://www.seattlechildrens.org/healthcare-professionals/education/continuing-medicalnursing-education/neonatal-nursing-education-briefs/ Neonatal
Neonatal Nursing Education Brief: Hypotension in the Neonate http://www.seattlechildrens.org/healthcare-professionals/education/continuing-medicalnursing-education/neonatal-nursing-education-briefs/ Neonatal
Sepsis is a complicated infectious process that propagates. Use of Vasopressors in Septic Shock. Clinical review
 Use of Vasopressors in Septic Shock Megan A. Rech, PharmD, Megan Prasse, PharmD, and Gourang Patel, PharmD, MSc Abstract Objective: To review the latest findings on the use of vasopressor agents in septic
Use of Vasopressors in Septic Shock Megan A. Rech, PharmD, Megan Prasse, PharmD, and Gourang Patel, PharmD, MSc Abstract Objective: To review the latest findings on the use of vasopressor agents in septic
Neonatal Shock. Imbalance between tissue oxygen delivery and oxygen consumption
 Neonatal Shock Moira Crowley, MD Assistant Professor, Pediatrics Co-director, Neonatal ECMO Program Rainbow Babies and Children s Hospital Case Western Resverve University School of Medicine 1 Objectives
Neonatal Shock Moira Crowley, MD Assistant Professor, Pediatrics Co-director, Neonatal ECMO Program Rainbow Babies and Children s Hospital Case Western Resverve University School of Medicine 1 Objectives
Printed copies of this document may not be up to date, obtain the most recent version from
 Children s Acute Transport Service Clinical Guidelines Septic Shock Document Control Information Author Shruti Dholakia L Chigaru Author Position Fellow CATS Consultant Document Owner E. Polke Document
Children s Acute Transport Service Clinical Guidelines Septic Shock Document Control Information Author Shruti Dholakia L Chigaru Author Position Fellow CATS Consultant Document Owner E. Polke Document
PHARMACOLOGICAL MANAGEMENT OF CARDIOGENIC SHOCK
 PHARMACOLOGICAL MANAGEMENT OF CARDIOGENIC SHOCK Doron Zahger, MD Department of Cardiology, Soroka University Medical Center, Faculty of Health Sciences, Ben Gurion University of the Negev, Beer Sheva,
PHARMACOLOGICAL MANAGEMENT OF CARDIOGENIC SHOCK Doron Zahger, MD Department of Cardiology, Soroka University Medical Center, Faculty of Health Sciences, Ben Gurion University of the Negev, Beer Sheva,
Haemodynamic Support. (getting the blood to go round and round) philippelefevre.com
 philippelefevre.com") Haemodynamic Support (getting the blood to go round and round) philippelefevre.com Haemodynamic Support Whats wrong with your patient? What can we do about it? Volume expansion Inotropes, Chronotropes
Haemodynamic Support (getting the blood to go round and round) philippelefevre.com Haemodynamic Support Whats wrong with your patient? What can we do about it? Volume expansion Inotropes, Chronotropes
Cardiogenic shock: Current management
 Cardiogenic shock: Current management Janine Pöss Universitätsklinikum des Saarlandes Klinik für Innere Medizin III Kardiologie, Angiologie und internistische Intensivmedizin Homburg/Saar I have nothing
Cardiogenic shock: Current management Janine Pöss Universitätsklinikum des Saarlandes Klinik für Innere Medizin III Kardiologie, Angiologie und internistische Intensivmedizin Homburg/Saar I have nothing
Bolus (Push Dose) Pressors: Good Idea or a bit Much?
 Pressors: Good Idea or a bit Much?") Bolus (Push Dose) Pressors: Good Idea or a bit Much? Robert Katzer MD MBA FACEP FAEMS Associate Professor, Emergency Medicine University of California, Irvine Pressors: Which Ones Are Out There, What Do
Bolus (Push Dose) Pressors: Good Idea or a bit Much? Robert Katzer MD MBA FACEP FAEMS Associate Professor, Emergency Medicine University of California, Irvine Pressors: Which Ones Are Out There, What Do
Surviving Sepsis Campaign. Guidelines for Management of Severe Sepsis/Septic Shock. An Overview
 Surviving Sepsis Campaign Guidelines for Management of Severe Sepsis/Septic Shock An Overview Mechanical Ventilation of Sepsis-Induced ALI/ARDS ARDSnet Mechanical Ventilation Protocol Results: Mortality
Surviving Sepsis Campaign Guidelines for Management of Severe Sepsis/Septic Shock An Overview Mechanical Ventilation of Sepsis-Induced ALI/ARDS ARDSnet Mechanical Ventilation Protocol Results: Mortality
Review of Cardiac Mechanics & Pharmacology 10/23/2016. Brent Dunworth, CRNA, MSN, MBA 1. Learning Objectives
 Brent Dunworth, CRNA, MSN, MBA Associate Director of Advanced Practice Division Chief, Nurse Anesthesia Vanderbilt University Medical Center Nashville, Tennessee Learning Objectives Review the principles
Brent Dunworth, CRNA, MSN, MBA Associate Director of Advanced Practice Division Chief, Nurse Anesthesia Vanderbilt University Medical Center Nashville, Tennessee Learning Objectives Review the principles
Protocol Identifier Subject Identifier Visit Description. [Y] Yes [N] No. [Y] Yes [N] N. If Yes, admission date and time: Day Month Year
![Protocol Identifier Subject Identifier Visit Description. [Y] Yes [N] No. [Y] Yes [N] N. If Yes, admission date and time: Day Month Year](/thumbs/76/74263761.jpg "Protocol Identifier Subject Identifier Visit Description. [Y] Yes [N] No. [Y] Yes [N] N. If Yes, admission date and time: Day Month Year") PAST MEDICAL HISTORY Has the subject had a prior episode of heart failure? o Does the subject have a prior history of exposure to cardiotoxins, such as anthracyclines? URGENT HEART FAILURE VISIT Did heart
PAST MEDICAL HISTORY Has the subject had a prior episode of heart failure? o Does the subject have a prior history of exposure to cardiotoxins, such as anthracyclines? URGENT HEART FAILURE VISIT Did heart
Objectives. Management of Septic Shock. Definitions Progression of sepsis. Epidemiology of severe sepsis. Major goals of therapy
 Objectives Management of Septic Shock Review of the Evidence and Implementation of Pediatric Guidelines at Christus Santa Rosa Manish Desai, M.D. PL 5 2 nd year Pediatric Critical Care Fellow Review of
Objectives Management of Septic Shock Review of the Evidence and Implementation of Pediatric Guidelines at Christus Santa Rosa Manish Desai, M.D. PL 5 2 nd year Pediatric Critical Care Fellow Review of
Rounds in the ICU. Eran Segal, MD Director General ICU Sheba Medical Center
 Rounds in the ICU Eran Segal, MD Director General ICU Sheba Medical Center Real Clinical cases (including our mistakes) Emphasis on hemodynamic monitoring Usually no single correct answer We will conduct
Rounds in the ICU Eran Segal, MD Director General ICU Sheba Medical Center Real Clinical cases (including our mistakes) Emphasis on hemodynamic monitoring Usually no single correct answer We will conduct
Pediatric Code Blue. Goals of Resuscitation. Focus Conference November Ensure organ perfusion
 Pediatric Code Blue Focus Conference November 2015 Duane C. Williams, MD Pediatric Critical Care Department of Pediatrics Children s Hospital of Richmond at VCU Goals of Resuscitation Ensure organ perfusion
Pediatric Code Blue Focus Conference November 2015 Duane C. Williams, MD Pediatric Critical Care Department of Pediatrics Children s Hospital of Richmond at VCU Goals of Resuscitation Ensure organ perfusion
Sepsis overview. Dr. Tsang Hin Hung MBBS FHKCP FRCP
 Sepsis overview Dr. Tsang Hin Hung MBBS FHKCP FRCP Epidemiology Sepsis, severe sepsis, septic shock Pathophysiology of sepsis Recent researches and advances From bench to bedside Sepsis bundle Severe sepsis
Sepsis overview Dr. Tsang Hin Hung MBBS FHKCP FRCP Epidemiology Sepsis, severe sepsis, septic shock Pathophysiology of sepsis Recent researches and advances From bench to bedside Sepsis bundle Severe sepsis
Adenosine. poison/drug induced. flushing, chest pain, transient asystole. Precautions: tachycardia. fibrillation, atrial flutter. Indications: or VT
 Adenosine Indications: 1. Narrow complex PSVT 2. Does not convert atrial fibrillation, atrial flutter or VT 1. Side effects include flushing, chest pain, transient asystole 2. May deteriorate widecomplex
Adenosine Indications: 1. Narrow complex PSVT 2. Does not convert atrial fibrillation, atrial flutter or VT 1. Side effects include flushing, chest pain, transient asystole 2. May deteriorate widecomplex
Pediatric Sepsis Treatment:
 Disclosures Pediatric Sepsis Treatment: (treat) Early & (reevaluate) Often None June 11, 2018 Leslie Dervan, MD MS Pacific Northwest Sepsis Conference 1 Agenda Sepsis: pathophysiology at-a-glance Pediatric
Disclosures Pediatric Sepsis Treatment: (treat) Early & (reevaluate) Often None June 11, 2018 Leslie Dervan, MD MS Pacific Northwest Sepsis Conference 1 Agenda Sepsis: pathophysiology at-a-glance Pediatric
Frank Sebat, MD - June 29, 2006
 Types of Shock Hypovolemic Shock Low blood volume decreasing cardiac output. AN INTEGRATED SYSTEM OF CARE FOR PATIENTS AT RISK SHOCK TEAM and RAPID RESPONSE TEAM Septic or Distributive Shock Decrease in
Types of Shock Hypovolemic Shock Low blood volume decreasing cardiac output. AN INTEGRATED SYSTEM OF CARE FOR PATIENTS AT RISK SHOCK TEAM and RAPID RESPONSE TEAM Septic or Distributive Shock Decrease in
Post-Cardiac Surgery Evaluation
 Post-Cardiac Surgery Evaluation 20th Annual Heart Conference October 15, 2016 Gary A Mayman PROFESSOR PEDIATRICS UNIVERSITY OF NEVADA Look Touch Listen Temperature, pulse, respiratory rate, & blood pressure
Post-Cardiac Surgery Evaluation 20th Annual Heart Conference October 15, 2016 Gary A Mayman PROFESSOR PEDIATRICS UNIVERSITY OF NEVADA Look Touch Listen Temperature, pulse, respiratory rate, & blood pressure
Emergency Cardiovascular Care: EMT-Intermediate Treatment Algorithms. Introduction to the Algorithms
 Emergency Cardiovascular Care: EMT-Intermediate Treatment Algorithms Introduction to the Algorithms Cardiac Arrest Algorithms Prehospital Medication Profiles Perspective regarding the EMT- Intermediate
Emergency Cardiovascular Care: EMT-Intermediate Treatment Algorithms Introduction to the Algorithms Cardiac Arrest Algorithms Prehospital Medication Profiles Perspective regarding the EMT- Intermediate
Anaesthesia. Cardiovascular. Update in. Inotropes and vasopressors in critical care
 Update in Anaesthesia Inotropes and vasopressors in critical care Hannah Dodwell and Bruce McCormick Correspondence Email: hannah.dodwell@doctors.net.uk INTRODUCTION Shock is present in many patients requiring
Update in Anaesthesia Inotropes and vasopressors in critical care Hannah Dodwell and Bruce McCormick Correspondence Email: hannah.dodwell@doctors.net.uk INTRODUCTION Shock is present in many patients requiring
Chapter 9. Learning Objectives. Learning Objectives 9/11/2012. Cardiac Arrhythmias. Define electrical therapy
 Chapter 9 Cardiac Arrhythmias Learning Objectives Define electrical therapy Explain why electrical therapy is preferred initial therapy over drug administration for cardiac arrest and some arrhythmias
Chapter 9 Cardiac Arrhythmias Learning Objectives Define electrical therapy Explain why electrical therapy is preferred initial therapy over drug administration for cardiac arrest and some arrhythmias
PULMONARY AND CRITICAL CARE BULLETIN
 The Chest Health Care, Education & Research Trust Chandigarh PULMONARY AND CRITICAL CARE BULLETIN Vol. XI, No. 2, April 15, 2005 Website : www.indiachest.org (p. 9-20) IN THIS ISSUE : 1. CARDIOVASCULAR
The Chest Health Care, Education & Research Trust Chandigarh PULMONARY AND CRITICAL CARE BULLETIN Vol. XI, No. 2, April 15, 2005 Website : www.indiachest.org (p. 9-20) IN THIS ISSUE : 1. CARDIOVASCULAR
We have reviewed this material in accordance with U.S. Copyright Law and have tried to maximize your ability to
 Author(s): Patrick Carter, Daniel Wachter, Rockefeller Oteng, Carl Seger, 2009-2010. License: Unless otherwise noted, this material is made available under the terms of the Creative Commons Attribution
Author(s): Patrick Carter, Daniel Wachter, Rockefeller Oteng, Carl Seger, 2009-2010. License: Unless otherwise noted, this material is made available under the terms of the Creative Commons Attribution
Taking the shock factor out of shock
 Taking the shock factor out of shock Julie Antonellis, BS, LVT, VTS (ECC) Northern Virginia Regional Director for the VALVT Technician Supervisor VCA Animal Emergency Critical Care Business owner Antonellis
Taking the shock factor out of shock Julie Antonellis, BS, LVT, VTS (ECC) Northern Virginia Regional Director for the VALVT Technician Supervisor VCA Animal Emergency Critical Care Business owner Antonellis
Vasoactive Drugs Do I have to choose? Dr. Vandewiele Bert 20 February 2012
 Vasoactive Drugs Do I have to choose? Dr. Vandewiele Bert 20 February 2012 What is what? Inotrope A substance that alters the force of muscular contraction (positive/negative) Vasopressor An agent producing
Vasoactive Drugs Do I have to choose? Dr. Vandewiele Bert 20 February 2012 What is what? Inotrope A substance that alters the force of muscular contraction (positive/negative) Vasopressor An agent producing
Patient Safety Safe Table Webcast: Sepsis (Part III and IV) December 17, 2014
 December 17, 2014") Patient Safety Safe Table Webcast: Sepsis (Part III and IV) December 17, 2014 Presenters Mark Blaney, RN Regional Nurse Educator CHI Franciscan Health Karen Lautermilch Director, Quality & Performance
Patient Safety Safe Table Webcast: Sepsis (Part III and IV) December 17, 2014 Presenters Mark Blaney, RN Regional Nurse Educator CHI Franciscan Health Karen Lautermilch Director, Quality & Performance
INTENSIVE CARE MEDICINE CPD EVENING. Dr Alastair Morgan Wednesday 13 th September 2017
 INTENSIVE CARE MEDICINE CPD EVENING Dr Alastair Morgan Wednesday 13 th September 2017 WHAT IS NEW IN ICU? (RELEVANT TO ANAESTHETISTS) Not much! SURVIVING SEPSIS How many deaths in England were thought
INTENSIVE CARE MEDICINE CPD EVENING Dr Alastair Morgan Wednesday 13 th September 2017 WHAT IS NEW IN ICU? (RELEVANT TO ANAESTHETISTS) Not much! SURVIVING SEPSIS How many deaths in England were thought
Heart Failure (HF) Treatment
 Treatment") Heart Failure (HF) Treatment Heart Failure (HF) Complex, progressive disorder. The heart is unable to pump sufficient blood to meet the needs of the body. Its cardinal symptoms are dyspnea, fatigue, and
Heart Failure (HF) Treatment Heart Failure (HF) Complex, progressive disorder. The heart is unable to pump sufficient blood to meet the needs of the body. Its cardinal symptoms are dyspnea, fatigue, and
Critical Care Treatment Guidelines
 Critical Care Treatment Guidelines West Virginia Office of Emergency Medical Services CCT Guidelines CCT Guidelines TABLE OF CONTENTS Preface Acknowledgments Using the Guidelines INITIAL TREATMENT / UNIVERSAL
Critical Care Treatment Guidelines West Virginia Office of Emergency Medical Services CCT Guidelines CCT Guidelines TABLE OF CONTENTS Preface Acknowledgments Using the Guidelines INITIAL TREATMENT / UNIVERSAL
The Septic Patient. Dr Arunraj Navaratnarajah. Renal SpR Imperial College NHS Healthcare Trust
 The Septic Patient Dr Arunraj Navaratnarajah Renal SpR Imperial College NHS Healthcare Trust Objectives of this session Define SIRS / sepsis / severe sepsis / septic shock Early recognition of Sepsis The
The Septic Patient Dr Arunraj Navaratnarajah Renal SpR Imperial College NHS Healthcare Trust Objectives of this session Define SIRS / sepsis / severe sepsis / septic shock Early recognition of Sepsis The
Daniel A. Beals MD, FACS, FAAP Pediatric Surgery and Urology Community Medical Center Associate Professor of Surgery and Pediatrics University of
 Daniel A. Beals MD, FACS, FAAP Pediatric Surgery and Urology Community Medical Center Associate Professor of Surgery and Pediatrics University of Washington Seattle Children s Hospital Objectives Define
Daniel A. Beals MD, FACS, FAAP Pediatric Surgery and Urology Community Medical Center Associate Professor of Surgery and Pediatrics University of Washington Seattle Children s Hospital Objectives Define
WHAT DO YOU SEE WHEN YOU STIMULATE BETA
 CARDIAC DRUG REVIEW WHAT DO YOU SEE WHEN YOU STIMULATE BETA VASODILATE BRONCHODILATE +CHRONOTROPE +INOTROPE EPI S OTHER NAME? ADRENALIN WHAT DOES EPI DO THAT NOREPI AND DOPAMINE DO NOT DO? BETA 2 BRONCHODILATOR
CARDIAC DRUG REVIEW WHAT DO YOU SEE WHEN YOU STIMULATE BETA VASODILATE BRONCHODILATE +CHRONOTROPE +INOTROPE EPI S OTHER NAME? ADRENALIN WHAT DOES EPI DO THAT NOREPI AND DOPAMINE DO NOT DO? BETA 2 BRONCHODILATOR
SEPSIS RAPID RESPONSE
 SEPSIS RAPID RESPONSE Sepsis kills up to 50% of those infected. How many deaths will you prevent this year? 1 SEPSIS Back ground: According to the Institute for Health Improvement and the Surviving Sepsis
SEPSIS RAPID RESPONSE Sepsis kills up to 50% of those infected. How many deaths will you prevent this year? 1 SEPSIS Back ground: According to the Institute for Health Improvement and the Surviving Sepsis