Neonatal Shock. Imbalance between tissue oxygen delivery and oxygen consumption
|
|
|
- George Lamb
- 6 years ago
- Views:
Transcription


1 Neonatal Shock Moira Crowley, MD Assistant Professor, Pediatrics Co-director, Neonatal ECMO Program Rainbow Babies and Children s Hospital Case Western Resverve University School of Medicine 1
2 Objectives Review the initial evaluation and differential diagnosis of neonatal shock Review the pharmacology of treatment of shock Apply the above information to a clinical case 2
3 Neonatal Shock Imbalance between tissue oxygen delivery and oxygen consumption Syndrome with diverse group of life threatening and multifactorial conditions Not regarded as a single pathologic entity
4 Oxygen Delivery and Consumption Normal Physiology Anaerobic Metabolism Oxygen Delivery must remain > 2 3 times consumption 4
5 Blood Pressure
6 Hypotension Associated risks preterm > term infants Inability to regulate cerebral blood flow (CBF) Paucity of data on reference values for arterial blood pressure in newborns Mean arterial blood pressure GA (weeks) BP tends to increase with: Advancing GA Birth weight Postnatal age (esp within first 5 days of life) 6
7 Normal Blood Pressure Ranges Nuntnarumit et al, Clin Perinatol: Dec
8 Blood Pressure Rule of Thumb Lower acceptable mean blood pressure (mmhg) on DOL 1 should be GA wks DOL 2-3 increases by ~ 5-7mmHg By DOL 3, 90% infants wks GA will have mean blood pressure >30mmHg Nuntnarumit et al, Clin Perinatol: Dec
9 Cerebral Blood Flow and Autoregulation 9
10 Shock 10
11 Case 4.1kg 39 wk male born via c-section for failure to progress Pregnancy complicated by gestation DM on glyburide, screens negative including GBS Floppy, poor respiratory effort PPV CPAP Inability to obtain pulse oximetry and pale APGARs: 2, 5, 6 Vital signs: HR 171; RR 31; Sat 85%; Blood Pressure unable to register 11
12 Is this baby in shock? If so, which phase of shock? What type of shock? 12
13 Phases of Neonatal Shock Compensated Uncompensated Irreversible 13
14 Phase 1: Compensated Shock Vital organ function maintained Neurohormonal compensatory mechanism Redistribute blood flow to heart, brain and adrenals Decreased: stroke volume, central venous pressure and urine output Normal blood pressure Increased myocardial contractility and HR so CO remains ~normal 14
15 Compensated Shock, cont. * *Blood pressure may not always appropriately reflect status of organ blood flow 15
16 Phase 2: Uncompensated Shock Failure of intrinsic neurohormonal compensatory mechanisms Decreased: microvascular perfusion myocardial contractility stroke volume blood pressure Decreased tissue perfusion lactic acidosis Multiorgan failure if untreated 16

17 Uncompensated Shock, cont. 17
18 Phase 3: Irreversible Phase Cellular damage complete organ failure Death invariably 18
19 Cellular and Molecular Pathophysiology of Shock Reactive oxygen species cell injury Nitric oxide overproduction hypotension Eicosanoids vasomediators and inflammatory mediators K ATP channels vascular smooth muscle tone 19
20 Down-Regulatrion of Adrenergic Receptors Occurs with critical illness and exogenous catecholamine administration Absolute or relative adrenal insuficiency Leads to pressor-resistant shock Glucocorticoids 20
21 Back to our case Intubated, lines placed Code event requiring epinephrine and compressions during placement VBG: <6.8/37/113 Lactate 13.8 Hct 24 NS bolus and PRBCs Oscillator, 100% oxygen, ino 20 Saturations now mid 90s, HR 140s Echocardiogram done 21
22 Echocardiogram 22
23 Types of Shock Hypovolemic Cardiogenic Distributive More than one type may be involved 23
24 Hypovolemic Shock Uncommon primary cause of neonatal shock Hypovolemia low CO and preload BP Causes Fetomaternal hemorrhage Massive hemorrage Inappropriate increase in vascular capacitance Surgical/GI losses (gastroschisis) Decreased venous return (air leaks, PEEP) DIC Dehydration (insensible losses/polyuria) 24
25 Cardiogenic Shock Neonate have immature myocardial structure and function Greater dependence on extracellular [Ca 2+ ] Greater sensitivity to increased afterload ELBW seem to be more sensitive 25

26 Immature Myocyte Ca 2+ Ca 2+ NCX Ca 2+ Ca 2+ SR Ca 2+ SR Ca 2+? Ca 2+ Ca 2+ Ca 2+ Ca 2+ Na + Mito ATP Ca 2+ NCX Na +
27 Cardiogenic Shock, cont. Increase in afterload myocardial dysfunction and decreased cardiac output Transitional circulation Placenta low resistance cut the cord immediate increase in SVR Can lead to increased LV afterload Decrease in cardiac output Development of shock 27
28 Other Causes of Cardiogenic Shock Perinatal asphyxia Prolonged septic shock PDA ligation Cardiomyopathies Myocarditis Ductal-dependent heart defects Arrhythmias 28
29 Distributive Shock Most common cause of early neonatal shock Impaired regulation of vascular tone +/- myocardial dysfunction SEPSIS Inflammatory mediators (TNF-α) 29
30 Distributive Shock, cont. Two hemodynamic patterns Warm shock Loss of vascular tone Increased systemic blood flow Hypotension Cold shock Increased vascular tone Low systemic blood flow Falling blood pressure 30
31 Pressor-Resistant Systemic Hypotension Normal to high systemic blood flow? Supranormal cardiac output More likely to be 27wks gestation or critically ill or perinatal asphyxia Down-regulation of cardiovascular adrenergic receptors, cytokine release, excess NO synthesis Exacerbated by immaturity, relative adrenal insuficiency 31
32 Returning to Our Case What do we do next? Echo demonstrating small ventricles (decreased preload) Poor function Mean arterial blood pressure 31mmHg Lactic acidosis 32
33 Treatment of Neonatal Shock 33
34 Treatment Modalities Volume Cardiovascular pharmacologic therapies Corticosteroids Tailored to primary cause and effect 34
35 Volume Relatively uncommon in 1 st day Replace the fluid that is lost Excessive volume worsen status if myocardial dysfuntion Morbidities: PDA, lung dysfuntion,?ivh 35
36 Indications for Volume Resuscitation Known blood loss Insensible losses Declining central venous pressure Volume repletion in distributive shock Before starting pharmacologic support 10mL/kg Normal Saline over ~30 minutes May repeat 36
37 Crystalloid vs. Colloid? Oca, et al. J Perinatol 2003 Randomized hypotensive preterm and term to normal saline vs. 5% albumin No difference in magnitude of BP response No difference in need for 2 nd bolus NS is safe, readily available, cheaper NS better than albumin 37
38 Crystalloid vs. Colloid? So, et al. Arch Dis Child 1997 Randomized hypotensive preterm infants to NS vs. 5% albumin No difference in BP response No difference in need for inotropic support NS just as effective as albumin 38
39 Volume Expansion Normal saline first choice Unless known anemia/blood loss 39
40 Pharmacologic Therapies Inotropes - drugs that improve myocardia contractility Increase peak force of contraction under isometric conditions Chronotropes drugs that increase HR Lusitropes drugs that increases the rate of myocardial relaxation Limited evidence as to which to use, doses and monitoring 40
41 Inotropes Stimulate myocardial α-adrenergic receptors β-adrenergic receptors Dopaminergic receptors 41
42 Mechanisms of Action 42
43 α- and β-receptor Stimulation

44 Properties of Receptors 44
45
46 Trends in Neonatal Hypotension All Infants ELBW Infants J Pediatr 2014;165: Arch Dis Child Fetal Neonatal Ed 2006;91:F213-F220.
47 Receptor Activity Drug α 1 β 1 β 2 DA 1 Dopamine Epinephrine Norepinephrine Dobutamine Milrinone
48 Hemodynamic Effects Drug HR MAP CI SVR Dopamine / Epinephrine - - / Norepinephrine 0-0 / / Dobutamine 0 - / 0 / Milrinone 0 / /
49 Dopamine Most commonly used in NICU Stimulates α- and β-adrenergic, dopaminergic and serotinergic receptors Maturational differences in α- and β- adrenergic receptors and thus dosedependent responses Effective in shock due to myocardial dysfunction and shock due to altered vasoregulation 49
50 50
51 Thoughts Hemodynamic effects and response altered by downregulation of adrenergic receptors Prolonged endogenous and exogenous receptor stimulation May see attenuated response 51
52 Dobutamine Relatively cardioselective 2 enantiomers with different affinity for adrenergic receptors Negative isomer α 1 -receptor agonist Increases myocardial contractility and SVR Positive isomer β 1 - and β 2 -receptor agonist Increases myocardial contractility, HR and conduction velocity, decreases SVR Net effect increase myocardial contractility, HR (lesser extent), no effect or decrease SVR 52
53 53
54 Cardiovascular Effects Myocardial dysfunction, normal SVR drug of choice Increases CO (more effective than dopamine) Example: Asphyxia Not appropriate 1 st line if vasodilatory shock is primary cause (low SVR) May add to dopamine 54
55 Dopamine vs. Dobutamine? If BP is low, dopamine better than dobutamine in increasing SVR Dobutamine without an α 1 -adrenergic agonist may worsen hypotension If impaired myocardial function adding dobutamine may be beneficial 55
56 Dopamine vs. Dobutamine Randomized, double-blind, crossover trial Preterm infants < 32 weeks (N = 20) Dopamine Median dose 12.5 mcg/kg/min 100% achieved MAP > 30 mmhg Increased SVR while maintaining SV Dobutamine Median dose 20 mcg/kg/min 40% achieved MAP > 30 mmhg Dobutamine increased CO, less impact on MAP Roze et al. Arch Dis Child 1993;69:59-63.
57 Dopamine vs. Dobutamine
58 Epinephrine Dose dependent stimulation of α- and β- adrenergic receptors Net effects Significant increase in BP Increases systemic blood flow by increasing SVR and CO 100-fold more potent than dopamine or dobutamine as inotrope 58
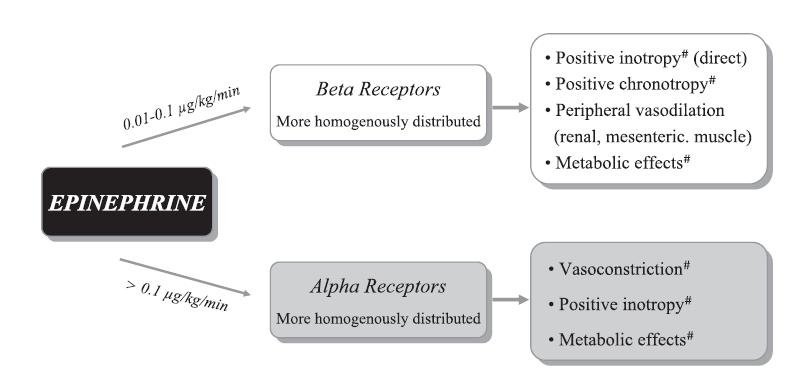
59 59
60 Epinephrine Clinical Use Refractory shock, second line agent Hyperglycemia Renal vasoconstriction Free from myocardial damage and ischemia Potent β- activity Direct cardiac toxicity Damage to arterial walls Myocardial contraction band necrosis Myocyte apoptosis
61 Norepinephrine Potent vasopressor Increases HR Increases myocardial contractility Increases SVR 100-fold more potent than dopamine or dobutamine as inotrope Lacks β 2 effects Use if diastolic pressure low If systolic pressure low, epinephrine 61
62 Milrinone Lusitope aiding in diastolic relaxation Prevents degredation of camp improves myocardial contractility, decreases PVR and SVR Inotropy : vasoldilation = 1:20 Limited studies in neonates Benefit when added to epi or norepi Caution with renal failure 62
63 Circulation 2008;118: Milrinone Phosphodiesterase 3 Inhibitor
64 Corticosteroids Relative or absolute adrenal insufficiency Especially sick preterm infants Glucocorticoids involved in regulating expression of cardiovascular adrenergic receptors If not enough receptors decreased response to vasopressors 64
65 Adrenocortical Function wk GA inverse relationship between GA and [cortisol] Illness has significant negative effect on [cortisol] ELBW requiring more respiratory support and inotropic support had lower cortisol levels Several studies shown that many stressed newborns fail to synthesize cortisol, have low levels Scott and Waterberg 65
66 Adrenocortical Function in VLBW Infants Ng et al. 66
67 How Does Hydrocortisone Increase BP? Non-genomic effects: Inhibits rate limiting enzyme in catecholamine break down Decreases NE reuptake at nerve endings Increases cytosolic Ca 2+ availability Inhibits vasodilatory effects of inflammatory response Improves capillary integrity 1-2 hrs Seri and Evans 67
68 How Does Hydrocortisone Increase BP?, cont. Genomic Effects: Upregulation of cardiovascular adrenergic receptors Induction of second messenger systems Synthesis and membrane assembly of new receptor proteins Requires 8-12 hrs Seri and Evans 68
69 Preterm Infants Response to Hydrocortisone Seri and Evans, Pediatrics; May
70 What About Late Preterm and Term Infants? Not well studied in term infants Used frequently with paucity of evidence Currently being studied through NRN RCT evaluating the effects of a course of hydrocortisone therapy on morbidity and cardiovascular function and long-term neurodevelopment and mortality of ill term and late preterm infants diagnosed with cardiovascular insufficiency Clinical trials.gov: NCT
71 ECMO Refractory hypotension Failure of medical therapy 71
72 Back to Our Case Continued to fluid resuscitate NS, blood products (coagulopathy) Started dopamine Acute hypotensive episode with desaturation More fluid, increased dopamine and added hydrocortisone Repeated echocardiogram 72
73 Repeat Echocardiogram 73
74 Case Conclusion Once intravascular volume improved, cardiac function improved oxygenation improved, lactatic acidosis started to improve Able to wean off support over then next few days 74
75 Conclusions Early recognition of neonatal shock is imperative Remember low BP low organ perfusion Volume resuscitation may not be indicated in preterm infant unless known cause for hypovolemia Normal saline is preferred unless blood loss 75
76 Conclusions, cont. Pharmacologic therapies may be necessary Dopamine is most common inotrope used by neonatologist, but depending on etiology of hypotension, others may be more appropriate Glucocorticoid therapy should be considered More data is needed to determine efficacy and long term outcomes 76

77 Thank You 77
78 Selected References Noori, et al. Fetal and Neonatal Physiology. 4 th Edition. Eds: Polin, Fox, Abman. Chapter 77. Noori and Seri. Neonatal Blood Pressure Support: The use of Inotropes, Lusitropes, and Other Vasopressor Agents. Clin Perinatology, Patwardhan. Inotropes in term neonates. Infant, Evans. Which inotrope for which baby? Arch Dis Child Fetal Neonatal Ed, 2006 F Special thanks to J McClary, PharmD and M. Auslender, MD for 78
The Pharmacology of Hypotension: Vasopressor Choices for HIE patients. Keliana O Mara, PharmD August 4, 2018
 The Pharmacology of Hypotension: Vasopressor Choices for HIE patients Keliana O Mara, PharmD August 4, 2018 Objectives Review the pathophysiology of hypotension in neonates Discuss the role of vasopressors
The Pharmacology of Hypotension: Vasopressor Choices for HIE patients Keliana O Mara, PharmD August 4, 2018 Objectives Review the pathophysiology of hypotension in neonates Discuss the role of vasopressors
SHOCK. Emergency pediatric PICU division Pediatric Department Medical Faculty, University of Sumatera Utara H. Adam Malik Hospital
 SHOCK Emergency pediatric PICU division Pediatric Department Medical Faculty, University of Sumatera Utara H. Adam Malik Hospital 1 Definition Shock is an acute, complex state of circulatory dysfunction
SHOCK Emergency pediatric PICU division Pediatric Department Medical Faculty, University of Sumatera Utara H. Adam Malik Hospital 1 Definition Shock is an acute, complex state of circulatory dysfunction
Hypotension in the Neonate
 Neonatal Nursing Education Brief: Hypotension in the Neonate http://www.seattlechildrens.org/healthcare-professionals/education/continuing-medicalnursing-education/neonatal-nursing-education-briefs/ Neonatal
Neonatal Nursing Education Brief: Hypotension in the Neonate http://www.seattlechildrens.org/healthcare-professionals/education/continuing-medicalnursing-education/neonatal-nursing-education-briefs/ Neonatal
MANAGEMENT OF CIRCULATORY FAILURE
 MANAGEMENT OF CIRCULATORY FAILURE BACKGROUND AND DEFINITION There is no consensus on the definition of circulatory failure or shock in newborns; it can be defined as global tissue hypoxia secondary to
MANAGEMENT OF CIRCULATORY FAILURE BACKGROUND AND DEFINITION There is no consensus on the definition of circulatory failure or shock in newborns; it can be defined as global tissue hypoxia secondary to
Case year old female nursing home resident with a hx CAD, PUD, recent hip fracture Transferred to ED with decreased mental status BP in ED 80/50
 Case 1 65 year old female nursing home resident with a hx CAD, PUD, recent hip fracture Transferred to ED with decreased mental status BP in ED 80/50 Case 1 65 year old female nursing home resident with
Case 1 65 year old female nursing home resident with a hx CAD, PUD, recent hip fracture Transferred to ED with decreased mental status BP in ED 80/50 Case 1 65 year old female nursing home resident with
Vasoactive Medications. Matthew J. Korobey Pharm.D., BCCCP Critical Care Clinical Specialist Mercy St. Louis
 Vasoactive Medications Matthew J. Korobey Pharm.D., BCCCP Critical Care Clinical Specialist Mercy St. Louis Objectives List components of physiology involved in blood pressure Review terminology related
Vasoactive Medications Matthew J. Korobey Pharm.D., BCCCP Critical Care Clinical Specialist Mercy St. Louis Objectives List components of physiology involved in blood pressure Review terminology related
Introduction. Invasive Hemodynamic Monitoring. Determinants of Cardiovascular Function. Cardiovascular System. Hemodynamic Monitoring
 Introduction Invasive Hemodynamic Monitoring Audis Bethea, Pharm.D. Assistant Professor Therapeutics IV January 21, 2004 Hemodynamic monitoring is necessary to assess and manage shock Information obtained
Introduction Invasive Hemodynamic Monitoring Audis Bethea, Pharm.D. Assistant Professor Therapeutics IV January 21, 2004 Hemodynamic monitoring is necessary to assess and manage shock Information obtained
Physiologic Based Management of Circulatory Shock Kuwait 2018
 Physiologic Based Management of Circulatory Shock Kuwait 2018 Dr. Yasser Elsayed, MD, PhD Director of the Targeted Neonatal Echocardiography, Point of Care and Hemodynamics Program Staff Neonatologist
Physiologic Based Management of Circulatory Shock Kuwait 2018 Dr. Yasser Elsayed, MD, PhD Director of the Targeted Neonatal Echocardiography, Point of Care and Hemodynamics Program Staff Neonatologist
When Fluids are Not Enough: Inopressor Therapy
 When Fluids are Not Enough: Inopressor Therapy Problems in Neonatology Neonatal problem: hypoperfusion Severe sepsis Hallmark of septic shock Secondary to neonatal encephalopathy Vasoplegia Syndrome??
When Fluids are Not Enough: Inopressor Therapy Problems in Neonatology Neonatal problem: hypoperfusion Severe sepsis Hallmark of septic shock Secondary to neonatal encephalopathy Vasoplegia Syndrome??
I intend to discuss an unapproved/investigative use of a commercial product/device in my presentation
 Istvan Seri MD PhD Center for Fetal and Neonatal Medicine USC Division of Neonatal Medicine Children Hospital Los Angeles and LAC+USC Medical Center Keck School of Medicine University of Southern California
Istvan Seri MD PhD Center for Fetal and Neonatal Medicine USC Division of Neonatal Medicine Children Hospital Los Angeles and LAC+USC Medical Center Keck School of Medicine University of Southern California
Advanced Monitoring of Cardiovascular and Respiratory Systems in Infants Kuwait 2018 Dr. Yasser Elsayed, MD, PhD Director of the Targeted Neonatal
 Advanced Monitoring of Cardiovascular and Respiratory Systems in Infants Kuwait 2018 Dr. Yasser Elsayed, MD, PhD Director of the Targeted Neonatal Echocardiography, Point of Care and Hemodynamics Program
Advanced Monitoring of Cardiovascular and Respiratory Systems in Infants Kuwait 2018 Dr. Yasser Elsayed, MD, PhD Director of the Targeted Neonatal Echocardiography, Point of Care and Hemodynamics Program
9/16/2012. Progression of Shock. Blood pressure: Pathophysiology & Clinical Management
 Mean BP (mm Hg) 9/16/212 September 2, 14: 6 min Blood pressure: Pathophysiology & Clinical Management Shahab Noori, MD Associate Professor of Pediatrics Division of Neonatology Progression of Shock BP
Mean BP (mm Hg) 9/16/212 September 2, 14: 6 min Blood pressure: Pathophysiology & Clinical Management Shahab Noori, MD Associate Professor of Pediatrics Division of Neonatology Progression of Shock BP
Pediatric Septic Shock. Geoffrey M. Fleming M.D. Division of Pediatric Critical Care Vanderbilt University School of Medicine Nashville, Tennessee
 Pediatric Septic Shock Geoffrey M. Fleming M.D. Division of Pediatric Critical Care Vanderbilt University School of Medicine Nashville, Tennessee Case 4 year old male with a history of gastroschesis repaired
Pediatric Septic Shock Geoffrey M. Fleming M.D. Division of Pediatric Critical Care Vanderbilt University School of Medicine Nashville, Tennessee Case 4 year old male with a history of gastroschesis repaired
Objectives. Management of Septic Shock. Definitions Progression of sepsis. Epidemiology of severe sepsis. Major goals of therapy
 Objectives Management of Septic Shock Review of the Evidence and Implementation of Pediatric Guidelines at Christus Santa Rosa Manish Desai, M.D. PL 5 2 nd year Pediatric Critical Care Fellow Review of
Objectives Management of Septic Shock Review of the Evidence and Implementation of Pediatric Guidelines at Christus Santa Rosa Manish Desai, M.D. PL 5 2 nd year Pediatric Critical Care Fellow Review of
Swans and Pressors. Vanderbilt Surgery Summer School Ricky Shinall
 Swans and Pressors Vanderbilt Surgery Summer School Ricky Shinall Shock, Swans, Pressors in 15 minutes 4 Reasons for Shock 4 Swan numbers to know 7 Pressors =15 things to know 4 Reasons for Shock Not enough
Swans and Pressors Vanderbilt Surgery Summer School Ricky Shinall Shock, Swans, Pressors in 15 minutes 4 Reasons for Shock 4 Swan numbers to know 7 Pressors =15 things to know 4 Reasons for Shock Not enough
Swans and Pressors. Vanderbilt Surgery Summer School Ricky Shinall
 Swans and Pressors Vanderbilt Surgery Summer School Ricky Shinall SHOCK Hypotension SHOCK Hypotension SHOCK=Reduction of systemic tissue perfusion, resulting in decreased oxygen delivery to the tissues.
Swans and Pressors Vanderbilt Surgery Summer School Ricky Shinall SHOCK Hypotension SHOCK Hypotension SHOCK=Reduction of systemic tissue perfusion, resulting in decreased oxygen delivery to the tissues.
DIAGNOSIS AND MANAGEMENT OF ACUTE HEART FAILURE
 DIAGNOSIS AND MANAGEMENT OF ACUTE HEART FAILURE Mefri Yanni, MD Bagian Kardiologi dan Kedokteran Vaskular RS.DR.M.Djamil Padang The 3rd Symcard Padang, Mei 2013 Outline Diagnosis Diagnosis Treatment options
DIAGNOSIS AND MANAGEMENT OF ACUTE HEART FAILURE Mefri Yanni, MD Bagian Kardiologi dan Kedokteran Vaskular RS.DR.M.Djamil Padang The 3rd Symcard Padang, Mei 2013 Outline Diagnosis Diagnosis Treatment options
Pediatric Sepsis Treatment:
 Disclosures Pediatric Sepsis Treatment: (treat) Early & (reevaluate) Often None June 11, 2018 Leslie Dervan, MD MS Pacific Northwest Sepsis Conference 1 Agenda Sepsis: pathophysiology at-a-glance Pediatric
Disclosures Pediatric Sepsis Treatment: (treat) Early & (reevaluate) Often None June 11, 2018 Leslie Dervan, MD MS Pacific Northwest Sepsis Conference 1 Agenda Sepsis: pathophysiology at-a-glance Pediatric
HOW LOW CAN YOU GO? HYPOTENSION AND THE ANESTHETIZED PATIENT.
 HOW LOW CAN YOU GO? HYPOTENSION AND THE ANESTHETIZED PATIENT. Donna M. Sisak, CVT, LVT, VTS (Anesthesia/Analgesia) Seattle Veterinary Specialists Kirkland, WA dsisak@svsvet.com THE ANESTHETIZED PATIENT
HOW LOW CAN YOU GO? HYPOTENSION AND THE ANESTHETIZED PATIENT. Donna M. Sisak, CVT, LVT, VTS (Anesthesia/Analgesia) Seattle Veterinary Specialists Kirkland, WA dsisak@svsvet.com THE ANESTHETIZED PATIENT
Evidence-Based. Management of Severe Sepsis. What is the BP Target?
 Evidence-Based Management of Severe Sepsis Michael A. Gropper, MD, PhD Professor and Vice Chair of Anesthesia Director, Critical Care Medicine Chair, Quality Improvment University of California San Francisco
Evidence-Based Management of Severe Sepsis Michael A. Gropper, MD, PhD Professor and Vice Chair of Anesthesia Director, Critical Care Medicine Chair, Quality Improvment University of California San Francisco
SHOCK Susanna Hilda Hutajulu, MD, PhD
 SHOCK Susanna Hilda Hutajulu, MD, PhD Div Hematology and Medical Oncology Department of Internal Medicine Universitas Gadjah Mada Yogyakarta Outline Definition Epidemiology Physiology Classes of Shock
SHOCK Susanna Hilda Hutajulu, MD, PhD Div Hematology and Medical Oncology Department of Internal Medicine Universitas Gadjah Mada Yogyakarta Outline Definition Epidemiology Physiology Classes of Shock
Pediatric Shock. National Pediatric Nighttime Curriculum Written by Julia M. Gabhart, M.D. Lucile Packard Children s Hospital at Stanford
 Pediatric Shock National Pediatric Nighttime Curriculum Written by Julia M. Gabhart, M.D. Lucile Packard Children s Hospital at Stanford Pre-Topic Questions 1. Why is it important to identify the stage
Pediatric Shock National Pediatric Nighttime Curriculum Written by Julia M. Gabhart, M.D. Lucile Packard Children s Hospital at Stanford Pre-Topic Questions 1. Why is it important to identify the stage
การอบรมว ทยาศาสตร พ นฐานทางศ ลยศาสตร เร อง นพ.ส ณฐ ต โมราก ล ภาคว ชาว ส ญญ ว ทยา คณะแพทยศาสตร โรงพยาบาลรามาธ บด มหาวทยาลยมหดล
 การอบรมว ทยาศาสตร พ นฐานทางศ ลยศาสตร เร อง นพ.ส ณฐ ต โมราก ล ภาคว ชาว ส ญญ ว ทยา คณะแพทยศาสตร โรงพยาบาลรามาธ บด มหาวทยาลยมหดล Distributive shock Severe sepsis and Septic shock Anaphylactic shock Neurogenic
การอบรมว ทยาศาสตร พ นฐานทางศ ลยศาสตร เร อง นพ.ส ณฐ ต โมราก ล ภาคว ชาว ส ญญ ว ทยา คณะแพทยศาสตร โรงพยาบาลรามาธ บด มหาวทยาลยมหดล Distributive shock Severe sepsis and Septic shock Anaphylactic shock Neurogenic
SHOCK. May 12, 2011 Body and Disease
 SHOCK May 12, 2011 Body and Disease Shock Definition of shock Pathophysiology Types of shock Management of shock Shock Definition? Shock What the Duke Community would have experienced if Gordon Hayward
SHOCK May 12, 2011 Body and Disease Shock Definition of shock Pathophysiology Types of shock Management of shock Shock Definition? Shock What the Duke Community would have experienced if Gordon Hayward
Utilizing Vasopressors:
 Utilizing Vasopressors: Critical Care Advances in the Emergency Department José A. Rubero, MD, FACEP, FAAEM Associate Program Director University of Central Florida/HCA GME Consortium Emergency Medicine
Utilizing Vasopressors: Critical Care Advances in the Emergency Department José A. Rubero, MD, FACEP, FAAEM Associate Program Director University of Central Florida/HCA GME Consortium Emergency Medicine
เอกราช อร ยะช ยพาณ ชย
 25 September 2017 เอกราช อร ยะช ยพาณ ชย Heart Failure and Transplant Cardiology aekarach.a@chula.ac.th Presentation at 1 Agenda Physiology of the heart Pathophysiology of shock Pathophysiology of heart
25 September 2017 เอกราช อร ยะช ยพาณ ชย Heart Failure and Transplant Cardiology aekarach.a@chula.ac.th Presentation at 1 Agenda Physiology of the heart Pathophysiology of shock Pathophysiology of heart
SHOCK AETIOLOGY OF SHOCK (1) Inadequate circulating blood volume ) Loss of Autonomic control of the vasculature (3) Impaired cardiac function
 Inadequate circulating blood volume ) Loss of Autonomic control of the vasculature (3) Impaired cardiac function") SHOCK Shock is a condition in which the metabolic needs of the body are not met because of an inadequate cardiac output. If tissue perfusion can be restored in an expeditious fashion, cellular injury may
SHOCK Shock is a condition in which the metabolic needs of the body are not met because of an inadequate cardiac output. If tissue perfusion can be restored in an expeditious fashion, cellular injury may
Sepsis: Identification and Management in an Acute Care Setting
 Sepsis: Identification and Management in an Acute Care Setting Dr. Barbara M. Mills DNP Director Rapid Response Team/ Code Resuscitation Stony Brook University Medical Center SEPSIS LECTURE NPA 2018 OBJECTIVES
Sepsis: Identification and Management in an Acute Care Setting Dr. Barbara M. Mills DNP Director Rapid Response Team/ Code Resuscitation Stony Brook University Medical Center SEPSIS LECTURE NPA 2018 OBJECTIVES
Staging Sepsis for the Emergency Department: Physician
 Staging Sepsis for the Emergency Department: Physician Sepsis Continuum 1 Sepsis Continuum SIRS = 2 or more clinical criteria, resulting in Systemic Inflammatory Response Syndrome Sepsis = SIRS + proven/suspected
Staging Sepsis for the Emergency Department: Physician Sepsis Continuum 1 Sepsis Continuum SIRS = 2 or more clinical criteria, resulting in Systemic Inflammatory Response Syndrome Sepsis = SIRS + proven/suspected
1
 1 2 3 RIFAI 5 6 Dublin cohort, retrospective review. Milrinone was commenced at an initial dose of 0.50 μg/kg/minute up to 0.75 μg/kg/minute and was continued depending on clinical response. No loading
1 2 3 RIFAI 5 6 Dublin cohort, retrospective review. Milrinone was commenced at an initial dose of 0.50 μg/kg/minute up to 0.75 μg/kg/minute and was continued depending on clinical response. No loading
Taking the shock factor out of shock
 Taking the shock factor out of shock Julie Antonellis, BS, LVT, VTS (ECC) Northern Virginia Regional Director for the VALVT Technician Supervisor VCA Animal Emergency Critical Care Business owner Antonellis
Taking the shock factor out of shock Julie Antonellis, BS, LVT, VTS (ECC) Northern Virginia Regional Director for the VALVT Technician Supervisor VCA Animal Emergency Critical Care Business owner Antonellis
Titrating Critical Care Medications
 Titrating Critical Care Medications Chad Johnson, MSN (NED), RN, CNCC(C), CNS-cc Clinical Nurse Specialist: Critical Care and Neurosurgical Services E-mail: johnsoc@tbh.net Copyright 2017 1 Learning Objectives
Titrating Critical Care Medications Chad Johnson, MSN (NED), RN, CNCC(C), CNS-cc Clinical Nurse Specialist: Critical Care and Neurosurgical Services E-mail: johnsoc@tbh.net Copyright 2017 1 Learning Objectives
Cardiovascular Management of Septic Shock
 Cardiovascular Management of Septic Shock R. Phillip Dellinger, MD Professor of Medicine Robert Wood Johnson Medical School/UMDNJ Director, Critical Care Medicine and Med/Surg ICU Cooper University Hospital
Cardiovascular Management of Septic Shock R. Phillip Dellinger, MD Professor of Medicine Robert Wood Johnson Medical School/UMDNJ Director, Critical Care Medicine and Med/Surg ICU Cooper University Hospital
State of Florida Systemic Supportive Care Guidelines. Michael D. Weiss, M.D. Associate Professor of Pediatrics Division of Neonatology
 State of Florida Systemic Supportive Care Guidelines Michael D. Weiss, M.D. Associate Professor of Pediatrics Division of Neonatology I. FEN 1. What intravenous fluids should be initiated upon admission
State of Florida Systemic Supportive Care Guidelines Michael D. Weiss, M.D. Associate Professor of Pediatrics Division of Neonatology I. FEN 1. What intravenous fluids should be initiated upon admission
HYPOTENSION IS DANGEROUS C. R Y A N K E A Y, M D, F A C E P 1 6 M A R C H
 HYPOTENSION IS DANGEROUS C. R Y A N K E A Y, M D, F A C E P 1 6 M A R C H 2 0 1 8 OBJECTIVES Case-based overview of pressors Debunking pressor myths Utilizing push-dose pressors CASE 1 82-year old male,
HYPOTENSION IS DANGEROUS C. R Y A N K E A Y, M D, F A C E P 1 6 M A R C H 2 0 1 8 OBJECTIVES Case-based overview of pressors Debunking pressor myths Utilizing push-dose pressors CASE 1 82-year old male,
Fluids in Sepsis: How much and what type? John Fowler, MD, FACEP Kent Hospital, İzmir Eisenhower Medical Center, USA American Hospital Dubai, UAE
 Fluids in Sepsis: How much and what type? John Fowler, MD, FACEP Kent Hospital, İzmir Eisenhower Medical Center, USA American Hospital Dubai, UAE In critically ill patients: too little fluid Low preload,
Fluids in Sepsis: How much and what type? John Fowler, MD, FACEP Kent Hospital, İzmir Eisenhower Medical Center, USA American Hospital Dubai, UAE In critically ill patients: too little fluid Low preload,
Does Targeted Neonatal Echocardiography(TnECHO) can help prevent Postoperative Cardiorespiratory instability following PDA ligation?
 can help prevent Postoperative Cardiorespiratory instability following PDA ligation?") Does Targeted Neonatal Echocardiography(TnECHO) can help prevent Postoperative Cardiorespiratory instability following PDA ligation? Amish Jain, Mohit Sahni, Afif El Khuffash, Arvind Sehgal, Patrick J
Does Targeted Neonatal Echocardiography(TnECHO) can help prevent Postoperative Cardiorespiratory instability following PDA ligation? Amish Jain, Mohit Sahni, Afif El Khuffash, Arvind Sehgal, Patrick J
When Fluids are Not Enough: Inopressor Therapy
 When Fluids are Not Enough: Inopressor Therapy Problems in Neonatology Neonatal problem: hypoperfusion Severe sepsis Hallmark of septic shock Secondary to neonatal encephalopathy Vasoplegia Syndrome??
When Fluids are Not Enough: Inopressor Therapy Problems in Neonatology Neonatal problem: hypoperfusion Severe sepsis Hallmark of septic shock Secondary to neonatal encephalopathy Vasoplegia Syndrome??
Agenda เอกราช อร ยะช ยพาณ ชย. - Cardiac physiology - Pathophysiology of shock - Pathophysiology of heart failure 9/6/2016
 6 September 2016 เอกราช อร ยะช ยพาณ ชย Heart Failure and Transplant Cardiology aekarach.a@chula.ac.th Agenda - Cardiac physiology - Pathophysiology of shock - Pathophysiology of heart failure http://fullpulse.weebly.com/conversation
6 September 2016 เอกราช อร ยะช ยพาณ ชย Heart Failure and Transplant Cardiology aekarach.a@chula.ac.th Agenda - Cardiac physiology - Pathophysiology of shock - Pathophysiology of heart failure http://fullpulse.weebly.com/conversation
Fluid Boluses in Preterm Babies with Poor Perfusion: A Hot Potato. Win Tin The James Cook University Hospital University of Durham
 Fluid Boluses in Preterm Babies with Poor Perfusion: A Hot Potato Win Tin The James Cook University Hospital University of Durham Introduction Fluid Bolus/es (Intravascular Volume Expansion) - One of the
Fluid Boluses in Preterm Babies with Poor Perfusion: A Hot Potato Win Tin The James Cook University Hospital University of Durham Introduction Fluid Bolus/es (Intravascular Volume Expansion) - One of the
Goal-directed vs Flow-guidedresponsive
 Goal-directed vs Flow-guidedresponsive therapy S Magder Department of Critical Care, McGill University Health Centre Flow-directed vs goal directed strategy for management of hemodynamics S Magder Curr
Goal-directed vs Flow-guidedresponsive therapy S Magder Department of Critical Care, McGill University Health Centre Flow-directed vs goal directed strategy for management of hemodynamics S Magder Curr
Surviving Sepsis Campaign Guidelines 2012 & Update for David E. Tannehill, DO Critical Care Medicine Mercy Hospital St.
 Surviving Sepsis Campaign Guidelines 2012 & Update for 2015 David E. Tannehill, DO Critical Care Medicine Mercy Hospital St. Louis Be appropriately aggressive the longer one delays aggressive metabolic
Surviving Sepsis Campaign Guidelines 2012 & Update for 2015 David E. Tannehill, DO Critical Care Medicine Mercy Hospital St. Louis Be appropriately aggressive the longer one delays aggressive metabolic
-Cardiogenic: shock state resulting from impairment or failure of myocardium
 Shock chapter Shock -Condition in which tissue perfusion is inadequate to deliver oxygen, nutrients to support vital organs, cellular function -Affects all body systems -Classic signs of early shock: Tachycardia,tachypnea,restlessness,anxiety,
Shock chapter Shock -Condition in which tissue perfusion is inadequate to deliver oxygen, nutrients to support vital organs, cellular function -Affects all body systems -Classic signs of early shock: Tachycardia,tachypnea,restlessness,anxiety,
Shock and hemodynamic monitorization. Nilüfer Yalındağ Öztürk Marmara University Pendik Research and Training Hospital
 Shock and hemodynamic monitorization Nilüfer Yalındağ Öztürk Marmara University Pendik Research and Training Hospital Shock Leading cause of morbidity and mortality Worldwide: dehydration and hypovolemic
Shock and hemodynamic monitorization Nilüfer Yalındağ Öztürk Marmara University Pendik Research and Training Hospital Shock Leading cause of morbidity and mortality Worldwide: dehydration and hypovolemic
The Septic Patient. Dr Arunraj Navaratnarajah. Renal SpR Imperial College NHS Healthcare Trust
 The Septic Patient Dr Arunraj Navaratnarajah Renal SpR Imperial College NHS Healthcare Trust Objectives of this session Define SIRS / sepsis / severe sepsis / septic shock Early recognition of Sepsis The
The Septic Patient Dr Arunraj Navaratnarajah Renal SpR Imperial College NHS Healthcare Trust Objectives of this session Define SIRS / sepsis / severe sepsis / septic shock Early recognition of Sepsis The
NE refractoriness: From Definition To Treatment... Prof. Alain Combes
 NE refractoriness: From Definition To Treatment... Prof. Alain Combes Service de Réanimation ican, Institute of Cardiometabolism and Nutrition Hôpital Pitié-Salpêtrière, AP-HP, Paris Université Pierre
NE refractoriness: From Definition To Treatment... Prof. Alain Combes Service de Réanimation ican, Institute of Cardiometabolism and Nutrition Hôpital Pitié-Salpêtrière, AP-HP, Paris Université Pierre
SHOCK. Pathophysiology
 SHOCK Dr. Ahmed Saleem FICMS TUCOM / 3rd Year / 2015 Shock is the most common and therefore the most important cause of death of surgical patients. Death may occur rapidly due to a profound state of shock,
SHOCK Dr. Ahmed Saleem FICMS TUCOM / 3rd Year / 2015 Shock is the most common and therefore the most important cause of death of surgical patients. Death may occur rapidly due to a profound state of shock,
Patient Safety Safe Table Webcast: Sepsis (Part III and IV) December 17, 2014
 December 17, 2014") Patient Safety Safe Table Webcast: Sepsis (Part III and IV) December 17, 2014 Presenters Mark Blaney, RN Regional Nurse Educator CHI Franciscan Health Karen Lautermilch Director, Quality & Performance
Patient Safety Safe Table Webcast: Sepsis (Part III and IV) December 17, 2014 Presenters Mark Blaney, RN Regional Nurse Educator CHI Franciscan Health Karen Lautermilch Director, Quality & Performance
Useful diagnostic measures: chest x ray to check pulmonary edema, ECG and ECHO to detect cardiac abnormalities (1).
.") Cardiogenic shock Etiology The most common cause of cardiogenic shock is LV dysfunction and necrosis as a result of acute myocardial infarction (AMI) (1). Acute valvular insufficiency or stenosis prevents
Cardiogenic shock Etiology The most common cause of cardiogenic shock is LV dysfunction and necrosis as a result of acute myocardial infarction (AMI) (1). Acute valvular insufficiency or stenosis prevents
Case Scenario 3: Shock and Sepsis
 Name: Molly Boyle 1. Define the term shock (Lewis textbook): Shock is a syndrome characterized by decreased perfusion and impaired metabolism. Shock can have a number of causes that result in damage to
Name: Molly Boyle 1. Define the term shock (Lewis textbook): Shock is a syndrome characterized by decreased perfusion and impaired metabolism. Shock can have a number of causes that result in damage to
Review of Cardiac Mechanics & Pharmacology 10/23/2016. Brent Dunworth, CRNA, MSN, MBA 1. Learning Objectives
 Brent Dunworth, CRNA, MSN, MBA Associate Director of Advanced Practice Division Chief, Nurse Anesthesia Vanderbilt University Medical Center Nashville, Tennessee Learning Objectives Review the principles
Brent Dunworth, CRNA, MSN, MBA Associate Director of Advanced Practice Division Chief, Nurse Anesthesia Vanderbilt University Medical Center Nashville, Tennessee Learning Objectives Review the principles
Vasopressors in Septic Shock. Keith R. Walley, MD St. Paul s Hospital University of British Columbia Vancouver, Canada
 Vasopressors in Septic Shock Keith R. Walley, MD St. Paul s Hospital University of British Columbia Vancouver, Canada Echocardiogram: EF=25% 57 y.o. female, pneumonia, shock Echocardiogram: EF=25% 57 y.o.
Vasopressors in Septic Shock Keith R. Walley, MD St. Paul s Hospital University of British Columbia Vancouver, Canada Echocardiogram: EF=25% 57 y.o. female, pneumonia, shock Echocardiogram: EF=25% 57 y.o.
Shock and Vasopressors. Nina E. Glass, MD TACS Fellow SICU Didactic Curriculum 9/24/14
 Shock and Vasopressors Nina E. Glass, MD TACS Fellow SICU Didactic Curriculum 9/24/14 Review Question Unilaterally diminished breath sounds A. Figure 1 B. Figure 2 C. Both D. Neither Related Specialties
Shock and Vasopressors Nina E. Glass, MD TACS Fellow SICU Didactic Curriculum 9/24/14 Review Question Unilaterally diminished breath sounds A. Figure 1 B. Figure 2 C. Both D. Neither Related Specialties
VASOPRESSORS AND INOTROPES CLINICAL PROFESSOR ANDREW BEZZINA FACEM MAY 2017
 VASOPRESSORS AND INOTROPES CLINICAL PROFESSOR ANDREW BEZZINA FACEM MAY 2017 CONFLICTS OF INTEREST OVERVIEW Why? When? What? How? WHY? Circulation WHY? - SHOCK!!! Pump (Heart) HYPOVOLAEMIC the pipes have
VASOPRESSORS AND INOTROPES CLINICAL PROFESSOR ANDREW BEZZINA FACEM MAY 2017 CONFLICTS OF INTEREST OVERVIEW Why? When? What? How? WHY? Circulation WHY? - SHOCK!!! Pump (Heart) HYPOVOLAEMIC the pipes have
CrackCast Episode 6 Shock
 CrackCast Episode 6 Shock Episode overview: 1) List, define and explain the 5 causes of shock 2) What is the utility of lactate and base deficit in the management of shock? 3) Define: SIRS, Sepsis, Severe
CrackCast Episode 6 Shock Episode overview: 1) List, define and explain the 5 causes of shock 2) What is the utility of lactate and base deficit in the management of shock? 3) Define: SIRS, Sepsis, Severe
Printed copies of this document may not be up to date, obtain the most recent version from
 Children s Acute Transport Service Clinical Guidelines Septic Shock Document Control Information Author Claire Fraser P.Ramnarayan Author Position tanp CATS Consultant Document Owner E. Polke Document
Children s Acute Transport Service Clinical Guidelines Septic Shock Document Control Information Author Claire Fraser P.Ramnarayan Author Position tanp CATS Consultant Document Owner E. Polke Document
UPMC Critical Care
 UPMC Critical Care www.ccm.pitt.edu Shock and Monitoring Samuel A. Tisherman, MD, FACS, FCCM Professor Departments of CCM and Surgery University of Pittsburgh Shock Anaerobic metabolism Lactic acidosis
UPMC Critical Care www.ccm.pitt.edu Shock and Monitoring Samuel A. Tisherman, MD, FACS, FCCM Professor Departments of CCM and Surgery University of Pittsburgh Shock Anaerobic metabolism Lactic acidosis
Written 01/09/17 Rewritten 3/29/17 for Interior Regional EMS Symposium
 Written 01/09/17 Rewritten 3/29/17 for Interior Regional EMS Symposium MARIA E. MANDICH MD Fairbanks Memorial Hospital Emergency Department Attending Physician Interior Region EMS Council Medical Director
Written 01/09/17 Rewritten 3/29/17 for Interior Regional EMS Symposium MARIA E. MANDICH MD Fairbanks Memorial Hospital Emergency Department Attending Physician Interior Region EMS Council Medical Director
PEDIATRIC SHOCK 10/9/2014. Objectives. What is shock? By the end of this presentation, the learner will be able to:
 PEDIATRIC SHOCK Leanna R. Miller, RN, MN, CCRN-CMC, PCCN-CMS, CEN, CNRN, CPNP Education Specialist-LRM Consulting Nashville, TN Objectives By the end of this presentation, the learner will be able to:
PEDIATRIC SHOCK Leanna R. Miller, RN, MN, CCRN-CMC, PCCN-CMS, CEN, CNRN, CPNP Education Specialist-LRM Consulting Nashville, TN Objectives By the end of this presentation, the learner will be able to:
During the stabilization period, immediately
 ROBIN BISSINGER, PHD, NNP-BC Section Editor Management of Hypotension in the Very Low-Birth-Weight Infant During the Golden Hour Margaret Conway-Orgel, MSN, NNP-BC 2.5 HOURS Continuing Education ABSTRACT
ROBIN BISSINGER, PHD, NNP-BC Section Editor Management of Hypotension in the Very Low-Birth-Weight Infant During the Golden Hour Margaret Conway-Orgel, MSN, NNP-BC 2.5 HOURS Continuing Education ABSTRACT
HYPOVOLEMIA AND HEMORRHAGE UPDATE ON VOLUME RESUSCITATION HEMORRHAGE AND HYPOVOLEMIA DISTRIBUTION OF BODY FLUIDS 11/7/2015
 UPDATE ON VOLUME RESUSCITATION HYPOVOLEMIA AND HEMORRHAGE HUMAN CIRCULATORY SYSTEM OPERATES WITH A SMALL VOLUME AND A VERY EFFICIENT VOLUME RESPONSIVE PUMP. HOWEVER THIS PUMP FAILS QUICKLY WITH VOLUME
UPDATE ON VOLUME RESUSCITATION HYPOVOLEMIA AND HEMORRHAGE HUMAN CIRCULATORY SYSTEM OPERATES WITH A SMALL VOLUME AND A VERY EFFICIENT VOLUME RESPONSIVE PUMP. HOWEVER THIS PUMP FAILS QUICKLY WITH VOLUME
Early Goal-Directed Therapy
 Early Goal-Directed Therapy Where do we stand? Jean-Daniel Chiche, MD PhD MICU & Dept of Host-Pathogen Interaction Hôpital Cochin & Institut Cochin, Paris-F Resuscitation targets in septic shock 1 The
Early Goal-Directed Therapy Where do we stand? Jean-Daniel Chiche, MD PhD MICU & Dept of Host-Pathogen Interaction Hôpital Cochin & Institut Cochin, Paris-F Resuscitation targets in septic shock 1 The
Resuscitation Before Emergency Surgeries FEIRAN LOU SUNY DOWNSTATE MEDICAL CENTER KINGS COUNTY HOSPITAL
 Resuscitation Before Emergency Surgeries FEIRAN LOU SUNY DOWNSTATE MEDICAL CENTER KINGS COUNTY HOSPITAL Case 73 yo woman h/o HTN three days abdominal pain and nausea. The pain was diffuse, cramp-like,
Resuscitation Before Emergency Surgeries FEIRAN LOU SUNY DOWNSTATE MEDICAL CENTER KINGS COUNTY HOSPITAL Case 73 yo woman h/o HTN three days abdominal pain and nausea. The pain was diffuse, cramp-like,
How and why I give IV fluid Disclosures SCA Fluids and public health 4/1/15. Andrew Shaw MB FRCA FCCM FFICM
 How and why I give IV fluid Andrew Shaw MB FRCA FCCM FFICM Professor and Chief Cardiothoracic Anesthesiology Vanderbilt University Medical Center 2015 Disclosures Consultant for Grifols manufacturer of
How and why I give IV fluid Andrew Shaw MB FRCA FCCM FFICM Professor and Chief Cardiothoracic Anesthesiology Vanderbilt University Medical Center 2015 Disclosures Consultant for Grifols manufacturer of
Pharmacology of inotropes and vasopressors
 Pharmacology of inotropes and vasopressors Curriculum 3.3 Recognises and manages the patient with circulatory failure 4.4 Uses fluids and vasoactive / inotropic drugs to support the circulation PR_BK_41
Pharmacology of inotropes and vasopressors Curriculum 3.3 Recognises and manages the patient with circulatory failure 4.4 Uses fluids and vasoactive / inotropic drugs to support the circulation PR_BK_41
Failure of the circulation to maintain Tissue cellular. Tissue hypoperfusion Cellular hypoxia SHOCK. Perfusion
 Shock SHOCK Failure of the circulation to maintain Tissue cellular Perfusion Organs Syndrome RR
Shock SHOCK Failure of the circulation to maintain Tissue cellular Perfusion Organs Syndrome RR
Objectives. Epidemiology of Sepsis. Review Guidelines for Resuscitation. Tx: EGDT, timing/choice of abx, activated
 Update on Surviving Sepsis 2008 Objectives Epidemiology of Sepsis Definition of Sepsis and Septic Shock Review Guidelines for Resuscitation Dx: Lactate, t cultures, SVO2 Tx: EGDT, timing/choice of abx,
Update on Surviving Sepsis 2008 Objectives Epidemiology of Sepsis Definition of Sepsis and Septic Shock Review Guidelines for Resuscitation Dx: Lactate, t cultures, SVO2 Tx: EGDT, timing/choice of abx,
SHOCK IN THE NEONATE. Developed by - Lisa Fikac, MSN, RNC-NIC. Expiration Date - 8/19/17
 SHOCK IN THE NEONATE Developed by - Lisa Fikac, MSN, RNC-NIC Expiration Date - 8/19/17 This continuing education activity is provided by Cape Fear Valley Health System, Training and Development Department,
SHOCK IN THE NEONATE Developed by - Lisa Fikac, MSN, RNC-NIC Expiration Date - 8/19/17 This continuing education activity is provided by Cape Fear Valley Health System, Training and Development Department,
Intravenous Inotropic Support an Overview
 Intravenous Inotropic Support an Overview Shaul Atar, MD Western Galilee Medical Center, Nahariya Affiliated with the Faculty of Medicine of the Galilee, Safed, Israel INOTROPES in Acute HF (not vasopressors)
Intravenous Inotropic Support an Overview Shaul Atar, MD Western Galilee Medical Center, Nahariya Affiliated with the Faculty of Medicine of the Galilee, Safed, Israel INOTROPES in Acute HF (not vasopressors)
Special features of cardiogenic failure in sepsis. Krisztina Madách
 Special features of cardiogenic failure in sepsis Krisztina Madách The problem in focus Incidence of sepsis is increasing Severe sepsis and septic shock are leading cause of death in ICU Septic patients
Special features of cardiogenic failure in sepsis Krisztina Madách The problem in focus Incidence of sepsis is increasing Severe sepsis and septic shock are leading cause of death in ICU Septic patients
NEONATAL CLINICAL PRACTICE GUIDELINE
 NEONATAL CLINICAL PRACTICE GUIDELINE Title: Brain Oxygen Monitoring in Newborns Using Near Infrared Spectroscopy (NIRS) Approval Date: Pages: June 2016 Approved by: Neonatal Patient Care Teams, HSC & SBH
NEONATAL CLINICAL PRACTICE GUIDELINE Title: Brain Oxygen Monitoring in Newborns Using Near Infrared Spectroscopy (NIRS) Approval Date: Pages: June 2016 Approved by: Neonatal Patient Care Teams, HSC & SBH
Circulatory shock. Types, Etiology, Pathophysiology. Physiology of Circulation: The Vessels. 600,000 miles of vessels containing 5-6 liters of blood
 Circulatory shock Types, Etiology, Pathophysiology Blagoi Marinov, MD, PhD Pathophysiology Dept. Physiology of Circulation: The Vessels 600,000 miles of vessels containing 5-6 liters of blood Vessel tone
Circulatory shock Types, Etiology, Pathophysiology Blagoi Marinov, MD, PhD Pathophysiology Dept. Physiology of Circulation: The Vessels 600,000 miles of vessels containing 5-6 liters of blood Vessel tone
I have no relevant financial relationships with the manufacturers of any. commercial products and/or provider of commercial services discussed in
 I have no relevant financial relationships with the manufacturers of any commercial products and/or provider of commercial services discussed in this activity I do intend to discuss an unapproved/investigative
I have no relevant financial relationships with the manufacturers of any commercial products and/or provider of commercial services discussed in this activity I do intend to discuss an unapproved/investigative
SHOCK in Paediatric Trauma
 SHOCK in Paediatric Trauma Speaker: Tang Sze Kit, (Fellow, Hong Kong College of Paediatric Nursing, MSc, MN, BN) Date: 26/4/2016 Time: 18:30-19:30 Venue: Paediatrics & Adolescent Ambulatory Centre, G/F,
SHOCK in Paediatric Trauma Speaker: Tang Sze Kit, (Fellow, Hong Kong College of Paediatric Nursing, MSc, MN, BN) Date: 26/4/2016 Time: 18:30-19:30 Venue: Paediatrics & Adolescent Ambulatory Centre, G/F,
4/5/2018. Update on Sepsis NIKHIL JAGAN PULMONARY AND CRITICAL CARE CREIGHTON UNIVERSITY. I have no financial disclosures
 Update on Sepsis NIKHIL JAGAN PULMONARY AND CRITICAL CARE CREIGHTON UNIVERSITY I have no financial disclosures 1 Objectives Why do we care about sepsis Understanding the core measures by Centers for Medicare
Update on Sepsis NIKHIL JAGAN PULMONARY AND CRITICAL CARE CREIGHTON UNIVERSITY I have no financial disclosures 1 Objectives Why do we care about sepsis Understanding the core measures by Centers for Medicare
Sepsis Management: Past, Present, and Future
 Sepsis Management: Past, Present, and Future Benjamin Ferrell, MD Tennessee ACP Meeting October 28, 2017 Learning Objectives Identify the most updated definition and clinical criteria for sepsis Describe
Sepsis Management: Past, Present, and Future Benjamin Ferrell, MD Tennessee ACP Meeting October 28, 2017 Learning Objectives Identify the most updated definition and clinical criteria for sepsis Describe
Sepsis Awareness and Education
 Sepsis Awareness and Education Meets the updated New York State Department of Health (NYSDOH) requirements for Infection Control and Barrier Precautions coursework Element VII: Sepsis Awareness and Education
Sepsis Awareness and Education Meets the updated New York State Department of Health (NYSDOH) requirements for Infection Control and Barrier Precautions coursework Element VII: Sepsis Awareness and Education
Irreversible shock can defined as last phase of shock where despite correcting the initial insult leading to shock and restoring circulation there is
 R. Siebert Irreversible shock can defined as last phase of shock where despite correcting the initial insult leading to shock and restoring circulation there is a progressive decline in blood pressure
R. Siebert Irreversible shock can defined as last phase of shock where despite correcting the initial insult leading to shock and restoring circulation there is a progressive decline in blood pressure
What works in sepsis. Topics. EGDT: Severe Sepsis/ Shock. Sepsis
 What works in sepsis Eric Schmidt, MD Denver Health Medical Center University of Colorado School of Medicine Topics Understanding and implemen@ng early goal directed therapy (EGDT) Ac@vated Protein C should
What works in sepsis Eric Schmidt, MD Denver Health Medical Center University of Colorado School of Medicine Topics Understanding and implemen@ng early goal directed therapy (EGDT) Ac@vated Protein C should
Disclosures. ICU Management of Advanced Lung Disease 5/9/2015. No Disclosures. All pictures from commercial sources
 Disclosures ICU Management of Advanced Lung Disease No Disclosures All pictures from commercial sources Lundy J. Campbell, MD UCSF Department of Anesthesia and Perioperative Care Division of Critical Care
Disclosures ICU Management of Advanced Lung Disease No Disclosures All pictures from commercial sources Lundy J. Campbell, MD UCSF Department of Anesthesia and Perioperative Care Division of Critical Care
Dilemmas in Septic Shock
 Dilemmas in Septic Shock William Janssen, M.D. Assistant Professor of Medicine National Jewish Health University of Colorado Denver Health Sciences Center A 62 year-old female presents to the ED with fever,
Dilemmas in Septic Shock William Janssen, M.D. Assistant Professor of Medicine National Jewish Health University of Colorado Denver Health Sciences Center A 62 year-old female presents to the ED with fever,
Department of Intensive Care Medicine UNDERSTANDING CIRCULATORY FAILURE IN SEPSIS
 Department of Intensive Care Medicine UNDERSTANDING CIRCULATORY FAILURE IN SEPSIS UNDERSTANDING CIRCULATORY FAILURE IN SEPSIS a mismatch between tissue perfusion and metabolic demands the heart, the vasculature
Department of Intensive Care Medicine UNDERSTANDING CIRCULATORY FAILURE IN SEPSIS UNDERSTANDING CIRCULATORY FAILURE IN SEPSIS a mismatch between tissue perfusion and metabolic demands the heart, the vasculature
12/1/2009. Chapter 19: Hemorrhage. Hemorrhage and Shock Occurs when there is a disruption or leak in the vascular system Internal hemorrhage
 Chapter 19: Hemorrhage Hemorrhage and Shock Occurs when there is a disruption or leak in the vascular system External hemorrhage Internal hemorrhage Associated with higher morbidity and mortality than
Chapter 19: Hemorrhage Hemorrhage and Shock Occurs when there is a disruption or leak in the vascular system External hemorrhage Internal hemorrhage Associated with higher morbidity and mortality than
Ruminations about the Past, Present, and Future
 Ruminations about the Past, Present, and Future Raymond L. Fowler, MD, FACEP, DABEMS Professor and Chief Division of Emergency Medical Services Department of Emergency Medicine UT Southwestern Medical
Ruminations about the Past, Present, and Future Raymond L. Fowler, MD, FACEP, DABEMS Professor and Chief Division of Emergency Medical Services Department of Emergency Medicine UT Southwestern Medical
Heart Failure (HF) Treatment
 Treatment") Heart Failure (HF) Treatment Heart Failure (HF) Complex, progressive disorder. The heart is unable to pump sufficient blood to meet the needs of the body. Its cardinal symptoms are dyspnea, fatigue, and
Heart Failure (HF) Treatment Heart Failure (HF) Complex, progressive disorder. The heart is unable to pump sufficient blood to meet the needs of the body. Its cardinal symptoms are dyspnea, fatigue, and
Shock Management. Seyed Tayeb Moradian MSc, Critical Care Nursing Ph.D Candidate. PDF created with pdffactory Pro trial version
 Shock Management Seyed Tayeb Moradian MSc, Critical Care Nursing Ph.D Candidate Definition of Shock The definition of shock does not involve low blood pressure, rapid pulse or cool clammy skin - these
Shock Management Seyed Tayeb Moradian MSc, Critical Care Nursing Ph.D Candidate Definition of Shock The definition of shock does not involve low blood pressure, rapid pulse or cool clammy skin - these
CARDIOGENIC SHOCK. Antonio Pesenti. Università degli Studi di Milano Bicocca Azienda Ospedaliera San Gerardo Monza (MI)
") CARDIOGENIC SHOCK Antonio Pesenti Università degli Studi di Milano Bicocca Azienda Ospedaliera San Gerardo Monza (MI) Primary myocardial dysfunction resulting in the inability of the heart to mantain an
CARDIOGENIC SHOCK Antonio Pesenti Università degli Studi di Milano Bicocca Azienda Ospedaliera San Gerardo Monza (MI) Primary myocardial dysfunction resulting in the inability of the heart to mantain an
9/13/2015. Laboratory. HPI and PE
 Critical Care HPI and PE 74 yo male confused SBP 90/20 MAP50, P 122, RR 34 Ox1 w/o nuchal rigidity S1S2 wo m RLL reduced breath sounds Skin warm dry Laboratory» WBC 15,600 Hgb 8.4 HCt 23%, Plts 95000,
Critical Care HPI and PE 74 yo male confused SBP 90/20 MAP50, P 122, RR 34 Ox1 w/o nuchal rigidity S1S2 wo m RLL reduced breath sounds Skin warm dry Laboratory» WBC 15,600 Hgb 8.4 HCt 23%, Plts 95000,
PULMONARY AND CRITICAL CARE BULLETIN
 The Chest Health Care, Education & Research Trust Chandigarh PULMONARY AND CRITICAL CARE BULLETIN Vol. XI, No. 2, April 15, 2005 Website : www.indiachest.org (p. 9-20) IN THIS ISSUE : 1. CARDIOVASCULAR
The Chest Health Care, Education & Research Trust Chandigarh PULMONARY AND CRITICAL CARE BULLETIN Vol. XI, No. 2, April 15, 2005 Website : www.indiachest.org (p. 9-20) IN THIS ISSUE : 1. CARDIOVASCULAR
Percutaneous Mechanical Circulatory Support for Cardiogenic Shock. 24 th Annual San Diego Heart Failure Symposium Ryan R Reeves, MD FSCAI
 Percutaneous Mechanical Circulatory Support for Cardiogenic Shock 24 th Annual San Diego Heart Failure Symposium Ryan R Reeves, MD FSCAI The Need for Circulatory Support Basic Pathophysiologic Problems:
Percutaneous Mechanical Circulatory Support for Cardiogenic Shock 24 th Annual San Diego Heart Failure Symposium Ryan R Reeves, MD FSCAI The Need for Circulatory Support Basic Pathophysiologic Problems:
Tissue oxygenation is dependent upon, cardiac output, hemoglobin saturation and peripheral micro circulation.
 Editorial Shock occurs when there is circulatory failure that results in inadequate cellular oxygen, that is arterial blood flow is inadequate to meet tissue metabolic needs. Tissue oxygenation is dependent
Editorial Shock occurs when there is circulatory failure that results in inadequate cellular oxygen, that is arterial blood flow is inadequate to meet tissue metabolic needs. Tissue oxygenation is dependent
Sepsis Combine experience and Evidence. Eran Segal, MD Director General ICU, Sheba Medical Center, Israel
 Sepsis Combine experience and Evidence Eran Segal, MD Director General ICU, Sheba Medical Center, Israel The Science of Sepsis A complex and diverse clinical entity Outcome is affected by: Infecting organism
Sepsis Combine experience and Evidence Eran Segal, MD Director General ICU, Sheba Medical Center, Israel The Science of Sepsis A complex and diverse clinical entity Outcome is affected by: Infecting organism
Acute Liver Failure: Supporting Other Organs
 Acute Liver Failure: Supporting Other Organs Michael A. Gropper, MD, PhD Professor of Anesthesia and Physiology Director, Critical Care Medicine University of California San Francisco Acute Liver Failure
Acute Liver Failure: Supporting Other Organs Michael A. Gropper, MD, PhD Professor of Anesthesia and Physiology Director, Critical Care Medicine University of California San Francisco Acute Liver Failure
Low Cardiac Output in the Pediatric Patient
 Low Cardiac Output in the Pediatric Patient Jeffrey Burns, M.D., M.P.H. Chief, Division of Critical Care Medicine Children s Hospital Boston Associate Professor of Anesthesia and Pediatrics Harvard Medical
Low Cardiac Output in the Pediatric Patient Jeffrey Burns, M.D., M.P.H. Chief, Division of Critical Care Medicine Children s Hospital Boston Associate Professor of Anesthesia and Pediatrics Harvard Medical
DO 2 > VO 2. The amount of oxygen delivered is a product of cardiac output (L/min) and the amount of oxygen in the arterial blood (ml/dl).
 and the amount of oxygen in the arterial blood (ml/dl).") Shock (Part 1): Review and Diagnostic Approach Jeffrey M. Todd, DVM, DACVECC University of Minnesota, St. Paul, MN Overview Shock is the clinical presentation of inadequate oxygen utilization, typically
Shock (Part 1): Review and Diagnostic Approach Jeffrey M. Todd, DVM, DACVECC University of Minnesota, St. Paul, MN Overview Shock is the clinical presentation of inadequate oxygen utilization, typically
BIPN100 F15 Human Physiol I (Kristan) Lecture 14 Cardiovascular control mechanisms p. 1
 Lecture 14 Cardiovascular control mechanisms p. 1") BIPN100 F15 Human Physiol I (Kristan) Lecture 14 Cardiovascular control mechanisms p. 1 Terms you should understand: hemorrhage, intrinsic and extrinsic mechanisms, anoxia, myocardial contractility, residual
BIPN100 F15 Human Physiol I (Kristan) Lecture 14 Cardiovascular control mechanisms p. 1 Terms you should understand: hemorrhage, intrinsic and extrinsic mechanisms, anoxia, myocardial contractility, residual
Printed copies of this document may not be up to date, obtain the most recent version from
 Children s Acute Transport Service Clinical Guidelines Septic Shock Document Control Information Author Shruti Dholakia L Chigaru Author Position Fellow CATS Consultant Document Owner E. Polke Document
Children s Acute Transport Service Clinical Guidelines Septic Shock Document Control Information Author Shruti Dholakia L Chigaru Author Position Fellow CATS Consultant Document Owner E. Polke Document
Neonatal Life Support Provider (NLSP) Certification Preparatory Materials
 Certification Preparatory Materials") Neonatal Life Support Provider (NLSP) Certification Preparatory Materials NEONATAL LIFE SUPPORT PROVIDER (NRP) CERTIFICATION TABLE OF CONTENTS NEONATAL FLOW ALGORITHM.2 INTRODUCTION 3 ANTICIPATION OF RESUSCITATION
Neonatal Life Support Provider (NLSP) Certification Preparatory Materials NEONATAL LIFE SUPPORT PROVIDER (NRP) CERTIFICATION TABLE OF CONTENTS NEONATAL FLOW ALGORITHM.2 INTRODUCTION 3 ANTICIPATION OF RESUSCITATION
Presented by: Indah Dwi Pratiwi
 Presented by: Indah Dwi Pratiwi Normal Fluid Requirements Resuscitation Fluids Goals of Resuscitation Maintain normal body temperature In most cases, elevate the feet and legs above the level of the heart
Presented by: Indah Dwi Pratiwi Normal Fluid Requirements Resuscitation Fluids Goals of Resuscitation Maintain normal body temperature In most cases, elevate the feet and legs above the level of the heart
John Park, MD Assistant Professor of Medicine
 John Park, MD Assistant Professor of Medicine Faculty photo will be placed here park.john@mayo.edu 2015 MFMER 3543652-1 Sepsis Out with the Old, In with the New Mayo School of Continuous Professional Development
John Park, MD Assistant Professor of Medicine Faculty photo will be placed here park.john@mayo.edu 2015 MFMER 3543652-1 Sepsis Out with the Old, In with the New Mayo School of Continuous Professional Development