Cardiac Protection across the cardiac continuum. Dong-Ju Choi, MD, PhD College of Medicine Seoul National University
|
|
|
- Myles Byrd
- 5 years ago
- Views:
Transcription
1 Cardiac Protection across the cardiac continuum Dong-Ju Choi, MD, PhD College of Medicine Seoul National University
2 Renin Angiotensin Cascade Nitric oxide (NO) Bradykinin Degradation products ACE ACEI site of action Angiotensinogen Renin A I A II CAGE Cathepsin G Chymase t-pa Cathepsin G Tonin AT 1 receptor AT 2 receptor Hypertrophy/proliferation Vasoconstriction Aldosterone release Antidiuretic hormone release Antiproliferation NO Release Differentiation Vasodilation de Gasparo M, et al. Hypertension. Pathophysiology, Diagnosis, and Management. 2nd ed. New York, NY: Raven Press; 1995: Dzau VJ. J Hypertens. 1989;7:

3 Pathophysiologic Effects of Angiotensin II Contractility Abnormal vasoconstriction PAI-1/ thrombosis Platelet aggregation Activate SNS Aldosterone Vasopressin Angiotensin II Superoxide production Vascular smooth muscle growth Endothelin Collagen Myocyte growth Burnier M, Brunner HR. Lancet. 2000;355:
4 Adverse Effects of RAS on CV System Vascular change 1. Vascular remodeling 2. Endothelial dysfunction 3. Inflammation Myocardial damage 1. Myocyte sequestration 2. Myocyte isolation
5 Increase BP Ang II
6 Vascular Remodeling
 Infiltration of leukocytes, and 3) Tissue remodeling.")
7 AngII-induced Inflammation The inflammatory response by AngII: 1) Increase in vascular permeability, 2) Infiltration of leukocytes, and 3) Tissue remodeling.




8 Myocardial Damage by RAS 1. Myocyte sequestration Hypertrophy Apoptosis Necrosis 2. Myocyte isolation Interstitial fibrosis Conduction disturbance
9 Blocking RAS is critical to prevent 1. Vascular change (Vascular remodeling, endothelial dysfunction and inflammation) and 2. Myocardial damage (Myocyte sequestration and myocyte isolation)
10 The Cardiovascular Continuum: Mechanisms and Mediators Oxidative Stress/Endothelial Dysfunction Vascular CAD Disease Myocardial Tissue Injury Infarction Pathological Tissue Loss Remodeling Target Ventricular Organ Dysfunction Enlargement Target Organ Damage Atherosclerosis Vascular Dysfunction Hypertrophy Risk Factors: ANGIOTENSIN II Heart End-stage Failure Organ Failure Death
11 Clinical Trials with ACE inhibitors MI Vascular and CAD HOPE, QUIET, EUROPA, PEACE CONSENSUS, ISIS-4, GISSI-3 SMILE, SAVE AIRE, TRACE Myocardial Infarction Pathological Remodeling CAD Atherosclerosis Hypertrophy Hypertension HF Ventricular Enlargement Heart Failure Risk Factors: Diabetes Hypertension Hyperlipdemia CAPPP, ALLHAT DM ABCD, REIN, AASK SOLVD V-HeFT II SAVE, Death ATLAS

12 Clinical Trials with ARB DM/Renal RENAAL, IDNT IRMAII, ARVAL ABCD-2V, NAVIGATOR Post-MI VALIANT, OPTIMAL VAL-PREST CAD, Nephropathy Atherosclerosis Hypertrophy Myocardial Infarction Pathological Remodeling Ventricular Enlargement Heart Failure Risk Factors: Diabetes Hypertension Hyperlipdemia Hypertension SCOPE, VALUE, TROPHY, LIFE HF ELITE I&II Val-HeFT CHARM Death
13 Val-Syst Trial: Powerful Double-digit BP Reductions with Valsartan-based Therapy in Patients with ISH Aged Randomised, double-blind, titration to effect study of patients (aged years) with ISH: 24 weeks treatment SBP Mean change in BP (mmhg) DIOVANbased (n=166) Amlodipinebased (n=163) NS Val-Syst: Valsartan in Isolated Systolic Hypertension (ISH); Per protocol population data shown; NS = not significant DIOVANbased (n=166) 6.0 DBP NS Amlodipinebased (n=163) 6.5 Patients were randomised to DIOVAN 80 mg or amlodipine 5 mg After 8 weeks, patients with SBP 140 mmhg were titrated to DIOVAN 160 mg/d or amlodipine 10 mg After an additional 8 weeks, HCTZ 12.5 mg was added to treatment in patients with SBP 140 mmhg Clin Ther 2003;25:
14 Time Course of Morning BP Changes Mediated by ARBs Morning home BP 165 Patients with essential hypertension: 4 weeks treatment SBP (mmhg) Start of treatment Day Valsartan mg (n=18) Telmisartan mg (n=18) Losartan mg (n=18) Candesartan 2 12 mg (n=18) Clin Exp Hypertens 2005;27:477 89
15 The role of arterial stiffness The role of arterial stiffness as the major cause of cardiovascular risk can be seen in recent outcome data. Pulse Wave Velocity aortic pulse wave velocity on entry was used to stratify arterial stiffness in a cohort of ESRD patients into tertiles 1st tertile has almost normal results; 3rd tertile has 6x risk of all cause mortality Clin Exp Hypertens Oct-Nov;26(7-8):689-99
16 Reduces Arterial Stiffness Randomised study of patients with hypertension: 3 months treatment Brachial ankle PWV* (cm/sec) Nifedipine 20 mg (n=20) 69 p=0.02 Diovan 80 mg (n=21) 195 *Brachial-ankle pulse wave velocity (PWV), a measure for systemic arterial stiffness Am J Hypertens 2004;17:1050 5
17 Reduces Arterial Stiffness Randomised, double-blind, parallel-group design study of patients with essential hypertension: 6 weeks treatment Change in AIx from baseline Diovan 80 mg HCTZ 25 mg Placebo 21.7* (n=20) 3.2 (n=20) 0.3 (n=20) Diovan improves arterial compliance in patients with hypertension Effects are independent of BP reduction (BP reductions similar for Diovan and HCTZ) Augmentation index (AIx), a measure of arterial function * p<0.01 vs HCTZ and vs placebo J Hypertens 2002;20:2423 8
18 DETECTIV : Valsartan Increases Small Artery Elasticity in Asymptomatic Risk Patients with High CV Risk Results from a 12-month study in 76 asymptomatic patients # with RDS 6 and controlled BP and cholesterol levels (DETECTIV study) Change in small artery elasticity from baseline (ml/mmhg x100) % increase* months 12 months Change in RDS from baseline months 12 months % reduction* Placebo DIOVAN 160 mg od for 6 months DIOVAN 160 mg od for 12 months # Individuals completing the study with or without antihypertensive or lipid lowering medications, BP <140/90 mmhg; *p<0.000; RDS=Rasmussen Disease Score Duprez et al. JACC 2007;50:published online
19 Val-MARC: Managing BP Aggressively and Evaluating Reductions in hscrp Multicentre, open-label, randomised, parallel-group study of patients with Stage II hypertension Objectives, to determine: If BP reduction with DIOVAN/Co-DIOVAN is effective at reducing hscrp levels If there is a difference between moderate and aggressive BP reduction in terms of hscrp change Primary endpoints: Change in SBP from baseline to Week 6 with DIOVAN vs Co-DIOVAN Change in hscrp from baseline to Week 6 with DIOVAN vs Co-DIOVAN Change in hscrp from baseline to Week 12 in the overall group Screening 0 7 days DIOVAN 160 mg (n=836) Co-DIOVAN 160/12.5 mg (n=832) DIOVAN 320 mg (n=807) Co-DIOVAN 320/12.5 mg (n=808) DIOVAN 320 mg (plus optional HCTZ 12.5 mg) Co-DIOVAN 320/12.5mg (or optional Co-DIOVAN 320/25mg) Week 0 Visit 1 (randomisation) Week 2 Visit 2 Week 6 Visit 3 Week 12 Visit 4 (End of study) Hypertension 2006;48:73-79
20 Val-MARC : DIOVAN Reduces hscrp Levels Independent of Blood Pressure Reduction Results from a 6-week study* in 1,615 patients with stage II HTN # (Val-MARC study) Change in hscrp plasma level (%) from baseline to 6 weeks* % DIOVAN mg od (n=807, median change -0.12) 4.4% Co-DIOVAN 160/ /12.5 mg od (n=808, median change +0.05) # SBP 160 mmhg or DBP 100 mmhg, patients completing the study; *Study duration 12 weeks, after 6 weeks of treatment, HCTZ 12.5 mg/day allowed at discretion in both groups to reach BP <140/90 mmhg); p<0.001 for DIOVAN vs. Co-DIOVAN Ridker et al. Hypertension 2006;48:73-79
21 VALUE: Elective Titration to Target BP(<140/90 mmhg) Patients aged 50 years, with treated or untreated hypertension and at high risk of CV events DIOVAN-based regimen DIOVAN 80 mg Rollover from previous therapy (92%) Amlodipinebased regimen Amlo 5 mg DIOVAN 160 mg Amlo 10 mg Co-DIOVAN 160/12.5 mg Amlo 10 mg + HCTZ 12.5 mg Co-DIOVAN 160/25 mg DIOVAN 160 mg + HCTZ 25 mg + Free add-on Amlo 10 mg + HCTZ 25 mg Amlo 10 mg + HCTZ 25 mg + Free add-on Month * 72 Screening Randomisation End of treatment adjustment period *Patient visits every 6 months for Months 6 72; Amlo = amlodipine Lancet 2004;363:
22 VALUE: Rate of Cardiac Events Did not Differ Between the Vasarta and Amlodipine Groups Proportion of patients with first event (%) DIOVAN-based regimen Amlodipine-based regimen HR=1.03; 95% CI= ; p=0.49 Number at risk Time (months) DIOVAN 7,649 7,459 7,407 7,250 7,085 6,906 6,732 6,536 6,349 5,911 3,765 1,474 Amlodipine 7,596 7,469 7,424 7,267 7,117 6,955 6,772 6,576 6,391 5,959 3,725 1,474 Lancet 2004;363:
23 LIFE : The Losartan Intervention For Endpoint Reduction in Hypertension Study Patients aged 55 years, with treated or untreated hypertensionand at high risk of CV events * Titration to target blood pressure: <140 / 90 mmhg Losartan 100 mg + HCTZ mg + others** Losartan 100 mg + HCTZ 12.5 mg* Losartan 50 mg + HCTZ 12.5 mg* Placebo Losartan 50 mg Atenolol 50 mg Atenolol 50 mg + HCTZ 12.5 mg* Atenolol 100 mg + HCTZ 12.5 mg* Atenolol 100 mg + HCTZ mg + others** Day 14 Day 7 Day 1 Mth 1 Mth 2 Mth 4 Mth 6 Yr 1 Yr 1.5 Yr 2 Yr 2.5 Yr 3 Yr 3.5 Yr 4 Yr 5 * Titration encouraged if SiDBP >90 mmhg or SiSBP >140 mmhg but was mandatory if SiBP >160 / 95 mmhg **Other antihypertensives excluding ACEIs, A II antagonists, beta blockers Lancet 2002;359;
24 LIFE : BP reductions Atenolol Losartan 140 Systolic mmhg Mean arterial 80 Diastolic Time (months) Lancet 2002;359;
25 LIFE : Primary Composite Endpoint Intention-to-Treat Atenolol Endpoint Rate Losartan Adjusted Risk Reduction 13 0%, p=0 021 Unadjusted Risk Reduction 14 6%, p= Study Day Study Month Losartan (n) Atenolol (n) Lancet 2002;359;
26 Atrial fibrillation accounts for 1/3 of all patients discharges with arrhythmia as principal diagnosis 6% PVCs 4% Atrial Flutter 6% PSVT 9% SSS 18% Unspecified 34% Atrial Fibrillation 8% Conduction Disease 3% SCD 10% VT 2% VF J Am Coll Cardiol. 1992;19(3):41A.
27 Relative Risk of Stroke and Mortality in Patients with AF vs. without AF Relative Risk (times) Stroke Mortality 0 Framingham Whitehall Regional Heart Study Whitehall Framingham (no Heart Disease) Framingham (overall) Manitoba Stroke rate in Non-Rheumatic HD with AF : 5% / year (Patients without AF) Lancet 1987;1:526 Am Heart J 1983;106:389 Am J Med 1995;98:476
28 VALUE - AF : Reduces the risk of new onset AF by 16% DIOVAN significantly reduces the risk of new-onset AF by 16% compared with amlodipine DIOVAN significantly reduces the risk of persistent AF by 32% compared with amlodipine J Hypertens 2008, 26:
29 VALIANT: Study Design and Inclusion Criteria days after acute MI SAVE, AIRE or TRACE eligible (either clinical/radiological signs of HF or LVSD) Major exclusion criteria Serum creatinine >2.5 mg/dl DBP <100 mmhg Prior intolerance of an ARB or ACE-I Double-blind active-controlled, stepwise titration Captopril 50 mg tid (n=4,909) DIOVAN 160 mg bid (n=4,909) Captopril 50 mg tid + DIOVAN 80 mg bid (n=4,885) Median duration: 24.7 months Event-driven Primary endpoint: Secondary endpoints: Other endpoints: All-cause mortality CV morbidity and mortality Safety and tolerability Am Heart J 2000;140: N Engl J Med 2003;349:
30 VALIANT: Risk of Mortality is Similarly Reduced with Valsartan and Captopril Patients with acute MI complicated by either HF or LVSD Probability of death from any cause Captopril 50 mg tid* (n=4,909) DIOVAN 160 mg bid* (n=4,909) DIOVAN 80 mg bid + captopril 50 mg tid* (n=4,885) *titration to target dose DIOVAN vs captopril: HR=1.00; p=0.98 DIOVAN + captopril vs captopril: HR=0.98; p= Time (months) Captopril 4,909 4,428 4,241 4,018 2,635 1, Diovan 4,909 4,464 4,272 4,007 2,648 1, Diovan + captopril 4,885 4,414 4,265 3,994 2,648 1, LVSD = left ventricular systolic dysfunction HF = heart failure N Engl J Med 2003;349:
31 OPTIMAAL(Optimal Trial in Myocardial Infarction with the Angiotensin II Antagonist Losartan) 50 years of age AMI-patients with heart failure or anterior Q-wave AMI 31,738 assessed 26,261 excluded 5,477 randomised 2,744 Losartan 2,733 Captopril 459 discont d 424 discont d 2,744 analysed 2,733 analysed Lancet 2002;360:752 60
32 OPTIMAAL: No Difference in Mortality Risk Between Losartan and Captopril Endpoint rate (%) Losartan (n= 2,744) Captopril (n=2,733) Relative risk 1.13 (85% CI ) p= Months Lancet 2002;360:752 60
33 Val-HeFT (The Valsartan in Heart Failure Trial ) 5,010 patients with HF 18 years; EF <40%; NYHA II IV; LVIDd >2.9 cm/m 2 ACE-I (93%), diuretics (86%), digoxin (67%), beta-blockers (36%) Randomised to Receiving standard therapy DIOVAN 40 mg bid titrated to 160 mg bid Placebo Two primary endpoints: 1) Mortality 2) Combined endpoint of mortality and morbidity EF = ejection fraction NYHA = New York Heart Association LVIDd = left-ventricular internal diastolic diameter N Engl J Med 2001;345:
34 Val-HeFT: Improves CV Outcomes* in CHF Results from a 23-month mean follow-up study in 5,010 patients with CHF on standard therapy (Val-HeFT study) 100 Event-free probability (%) DIOVAN (n=2,511) Placebo (n=2,499) RR=0.87; 97.5% CI: Time (months) 13.2% risk reduction *Combined 1 endpoint: all-cause mortality, cardiac arrest with resuscitation, hospitalization for worsening HF, or therapy with intravenous inotropes or vasodilators; p=0.009 vs. placebo; 1 endpoint of mortality was not significantly different between valsartan and placebo; DIOVAN regimen started at 40 mg bid after placebo run-in, doubled every 2 weeks to target 160 mg bid Cohn et al. N Engl J Med 2001;345:
35 ELITE II :Evaluation of Losartan in the Elderly Study Randomised trial of losartan versus captopril in patients over 65 with heart failure 60 yrs; NYHA II - IV; EF 40 % ACEI naive or < 7 days in 3 months prior to entry Standard Rx ( ± Dig / Diuretics ), ß - blocker stratification Captopril 50 mg 3 times daily n = 1574 Event Driven Targeting 510 deaths estimate 2 yrs median follow-up 555 days Losartan 50 mg daily n = 1578 Primary Endpoint : All-cause Mortality Secondary Endpoint : Sudden cardiac death and/or Resuscitated Arrest Other : All-cause Mortality / Hospitalizations Safety and Tolerability Lancet 2000;355:
36 ELITE II: 1.0 Risk of All-cause Mortality or Hospital Admission is Similarly Reduced with Losartan and Captopril Event-free probability p=0.18 Losartan (n=1578) Captopril (n=1574) Follow-up (days) Lancet 2000;355:
37 JIKEI HEART : Valsartan-based Therapy Improved Outcomes in Japanese Patients with HT and/or Coronary Heart Disease and/or HF Valsartan-based therapy group (n=1541) Run-in Conventional treatment (non-arb) + valsartan mg daily + valsartan mg daily + non-arb treatment Conventional treatment (non-arb) + non-arb Non-ARB treatment arm (n=1540) + non-arb + non-arb 4 Randomisation 0 Titration 8 12 Weeks Titration End of study (median follow-up was 3.1 years) Mochizuki et al. Lancet 2007;369:1431 9
38 JIKEI HEART 0 CV mortality and morbidity Stroke/TIA Hospitalisation for HF Hospitalisation for angina Risk reduction (%) * p= * p= * p= * p= TIA = transient ischemic attack *With DIOVAN-based therapy compared with non-arb therapy; primary endpoint Lancet 2007;369:1431 9
39 Mortality and Morbidity Endpoint Trials with ARB 60,000 VALUE 1 ONTARGET 8 CHARM 14 50,345 VALIANT 2 TRANSEND 8 SCOPE 15 50,000 NAVIGATOR 3 LIFE 9 SCAST* 16 Val-HeFT 4 OPTIMAAL 10 CASE-J 17 Number of patients 40,000 30,000 20,000 29,400 JIKEI HEART 5,6 KYOTO HEART* 7 22,991 19,768 ELITE II 11 RENAAL 12 NCT * 13 14,815 I-Preserve 18 IDNT 19 ACTIVE* 20 SUPPORT* 21 MOSES 22 10,000 1,000 1,405 0 DIOVAN Telmisartan Losartan Candesartan Irbesartan Olmesartan Eprosartan 1 Julius et al. Lancet 2004;363: ; 2 Pfeffer et al. NEJM 2003;349: ; Cohn et al. NEJM 2001;345: ; 5 Mochizuki et al. J Hypertens 2006;24(Suppl. 4):S31; 6 Mochizuki et al. Cardiovasc Drugs Ther 2004;18:305 9; 7 (NCT ) Dahlof et al. Lancet 2002;359: ; 10 Dickstein et al. Lancet 2002;360:752 60; 11 Pitt et al. Lancet 2000;355:1582 7; 12 Brenner et al. NEJM 2001;345:861 9; 13 (NCT ) Papademetriou et al. J Am Coll Cardiol 2004;44: ; 16 (NCT ); 17 Ogihara J Hypertens 2006;24(Suppl. 4):S30; 18 Carson et al. J Card Fail 2005;11:576 85; 19 Lewis et al. NEJM 2001;345:851 60; 20 (NCT ); 21 (NCT ); 22 Schrader et al. Stroke 2005;36: *Expected enrolment

40
41
42
43
44 Summary: To protect and improve vascular and cardiac structure/function understanding the effects of angiotensin II is an important issue in HT. Blocking the negative effects of angiotensin II at the AT 1 receptor improves endothelial function, improves inflammation, reduces oxidative stress improves left ventricular remodeling and function ARB has proven clinical benefits from HT to HF patients in the spectrum of CV continuum. ARB provides proven cardioprotective benefits.
ARBs in Cardiovascular Disease
 ARBs in Cardiovascular Disease Yong-Jin Kim, MD Seoul National University Hospital Cardiovascular Continuum Ventricular remodelling Remodelling Myocardial infarction Myocardial infarction Ventricular dilation
ARBs in Cardiovascular Disease Yong-Jin Kim, MD Seoul National University Hospital Cardiovascular Continuum Ventricular remodelling Remodelling Myocardial infarction Myocardial infarction Ventricular dilation
Optimal blockade of the Renin- Angiotensin-Aldosterone. in chronic heart failure
 Optimal blockade of the Renin- Angiotensin-Aldosterone Aldosterone- (RAA)-System in chronic heart failure Jan Östergren Department of Medicine Karolinska University Hospital Stockholm, Sweden Key Issues
Optimal blockade of the Renin- Angiotensin-Aldosterone Aldosterone- (RAA)-System in chronic heart failure Jan Östergren Department of Medicine Karolinska University Hospital Stockholm, Sweden Key Issues
ACE inhibitors: still the gold standard?
 ACE inhibitors: still the gold standard? Session: Twenty-five years after CONSENSUS What have we learnt about the RAAS in heart failure? Lars Køber, MD, D.Sci Department of Cardiology Rigshospitalet University
ACE inhibitors: still the gold standard? Session: Twenty-five years after CONSENSUS What have we learnt about the RAAS in heart failure? Lars Køber, MD, D.Sci Department of Cardiology Rigshospitalet University
Understanding and Development of New Therapies for Heart Failure - Lessons from Recent Clinical Trials -
 Understanding and Development of New Therapies for Heart Failure - Lessons from Recent Clinical Trials - Clinical trials Evidence-based medicine, clinical practice Impact upon Understanding pathophysiology
Understanding and Development of New Therapies for Heart Failure - Lessons from Recent Clinical Trials - Clinical trials Evidence-based medicine, clinical practice Impact upon Understanding pathophysiology
The Therapeutic Potential of Novel Approaches to RAAS. Professor of Medicine University of California, San Diego
 The Therapeutic Potential of Novel Approaches to RAAS Inhibition in Heart Failure Barry Greenberg, M.D. Professor of Medicine University of California, San Diego Chain of Events Leading to End-Stage Heart
The Therapeutic Potential of Novel Approaches to RAAS Inhibition in Heart Failure Barry Greenberg, M.D. Professor of Medicine University of California, San Diego Chain of Events Leading to End-Stage Heart
Rationale for the use of Single Pill Combination (SPC) and Asian data of ARB/CCB SPC
 and Asian data of ARB/CCB SPC") Rationale for the use of Single Pill Combination (SPC) and Asian data of ARB/CCB SPC Seung Woo Park, MD Samsung Medical Center BP Control Rates in Asia BP controlled BP uncontrolled 24.3% 36.6% 19% Turkey
Rationale for the use of Single Pill Combination (SPC) and Asian data of ARB/CCB SPC Seung Woo Park, MD Samsung Medical Center BP Control Rates in Asia BP controlled BP uncontrolled 24.3% 36.6% 19% Turkey
Comprehensive Cardiovascular & Metabolic Protection Liking Scientific Advances to Clinical Practice 인제의대상계백병원 당뇨병센터 고경수
 Comprehensive Cardiovascular & Metabolic Protection Liking Scientific Advances to Clinical Practice 인제의대상계백병원 당뇨병센터 고경수 Cardiovascular & metabolic risk factors The importance of BP management for HTN patients
Comprehensive Cardiovascular & Metabolic Protection Liking Scientific Advances to Clinical Practice 인제의대상계백병원 당뇨병센터 고경수 Cardiovascular & metabolic risk factors The importance of BP management for HTN patients
heart failure John McMurray University of Glasgow.
 A to Z of RAAS blockade in heart failure John McMurray BHF Cardiovascular Research Centre University of Glasgow. RAAS inhibition in CHF ACE inhibition in patients with low LVEF CHF CONSENSUS Enalapril
A to Z of RAAS blockade in heart failure John McMurray BHF Cardiovascular Research Centre University of Glasgow. RAAS inhibition in CHF ACE inhibition in patients with low LVEF CHF CONSENSUS Enalapril
VALUE OF ACEI IN THE MANAGEMENT OF HYPERTENSION
 VALUE OF ACEI IN THE MANAGEMENT OF HYPERTENSION Dr Catherine BESEME Paris 6 th December 2005 6 th International Congress of Bangladesh Society of Medicine Hypertension is a risk factor at the source, with
VALUE OF ACEI IN THE MANAGEMENT OF HYPERTENSION Dr Catherine BESEME Paris 6 th December 2005 6 th International Congress of Bangladesh Society of Medicine Hypertension is a risk factor at the source, with
Should All Patients Be Treated with Ace-inh /ARB after STEMI with Preserved LV Function?
 Should All Patients Be Treated with Ace-inh /ARB after STEMI with Preserved LV Function? Avi Shimony, MD, FESC Cardiology Division Soroka University Medical Center Ben-Gurion University, Beer-Sheva Disclosure
Should All Patients Be Treated with Ace-inh /ARB after STEMI with Preserved LV Function? Avi Shimony, MD, FESC Cardiology Division Soroka University Medical Center Ben-Gurion University, Beer-Sheva Disclosure
RAS Blockade Across the CV Continuum
 A Summary of Recent International Meetings RAS Blockade Across the CV Continuum Copyright New Evidence Presented at the 2009 Congress of the European Society of Cardiology (August 29-September 2, Barcelona)
A Summary of Recent International Meetings RAS Blockade Across the CV Continuum Copyright New Evidence Presented at the 2009 Congress of the European Society of Cardiology (August 29-September 2, Barcelona)
The Beneficial Role of Angiotensin- Converting Enzyme Inhibitor in Acute Myocardial Infarction
 The Beneficial Role of Angiotensin- Converting Enzyme Inhibitor in Acute Myocardial Infarction Cardiovascular Center, Korea University Guro Hospital 2007. 4. 20 Seung-Woon Rha, MD, PhD Introduction 1.
The Beneficial Role of Angiotensin- Converting Enzyme Inhibitor in Acute Myocardial Infarction Cardiovascular Center, Korea University Guro Hospital 2007. 4. 20 Seung-Woon Rha, MD, PhD Introduction 1.
Hypertension Management Focus on new RAAS blocker. Disclosure
 Hypertension Management Focus on new RAAS blocker Rameshkumar Raman M.D Endocrine Associates of The Quad Cities Disclosure Speaker bureau Abbott, Eli Lilly, Novo Nordisk, Novartis, Takeda, Merck, Solvay
Hypertension Management Focus on new RAAS blocker Rameshkumar Raman M.D Endocrine Associates of The Quad Cities Disclosure Speaker bureau Abbott, Eli Lilly, Novo Nordisk, Novartis, Takeda, Merck, Solvay
A Fresh Look at ARBs : Focus on HF survival data
 A Fresh Look at ARBs : Focus on HF survival data Seok-Min Kang, MD, Ph D. Division of Cardiology, Severance Cardiovascular Hospital, Yonsei University College of Medicine, Seoul, Korea HF specialists ARBs,
A Fresh Look at ARBs : Focus on HF survival data Seok-Min Kang, MD, Ph D. Division of Cardiology, Severance Cardiovascular Hospital, Yonsei University College of Medicine, Seoul, Korea HF specialists ARBs,
ESC Guidelines for the Diagnosis and Treatment of Chronic Heart Failure
 ESC Guidelines for the Diagnosis and Treatment of Chronic Heart Failure - 2005 Karl Swedberg Professor of Medicine Department of Medicine Sahlgrenska University Hospital/Östra Göteborg University Göteborg
ESC Guidelines for the Diagnosis and Treatment of Chronic Heart Failure - 2005 Karl Swedberg Professor of Medicine Department of Medicine Sahlgrenska University Hospital/Östra Göteborg University Göteborg
Cardiovascular Protection and the RAS
 Cardiovascular Protection and the RAS Katalin Kauser, MD, PhD, DSc Senior Associate Director, Boehringer Ingelheim Pharmaceutical Inc. Micardis Product Pipeline Scientific Support Ridgefield, CT, USA Cardiovascular
Cardiovascular Protection and the RAS Katalin Kauser, MD, PhD, DSc Senior Associate Director, Boehringer Ingelheim Pharmaceutical Inc. Micardis Product Pipeline Scientific Support Ridgefield, CT, USA Cardiovascular
LXIV: DRUGS: 4. RAS BLOCKADE
 LXIV: DRUGS: 4. RAS BLOCKADE ACE Inhibitors Components of RAS Actions of Angiotensin i II Indications for ACEIs Contraindications RAS blockade in hypertension RAS blockade in CAD RAS blockade in HF Limitations
LXIV: DRUGS: 4. RAS BLOCKADE ACE Inhibitors Components of RAS Actions of Angiotensin i II Indications for ACEIs Contraindications RAS blockade in hypertension RAS blockade in CAD RAS blockade in HF Limitations
Rationale for the use of Single Pill Combination. Yong Jin Kim, MD Seoul National University Hospital
 Rationale for the use of Single Pill Combination Yong Jin Kim, MD Seoul National University Hospital Unmet Need of Hypertension Treatment Hypertension # 1 Risk Factor for Global Mortality 0 1 2 3 4 5 6
Rationale for the use of Single Pill Combination Yong Jin Kim, MD Seoul National University Hospital Unmet Need of Hypertension Treatment Hypertension # 1 Risk Factor for Global Mortality 0 1 2 3 4 5 6
Ferrari R, Fox K, Bertrand M, Mourad J.J, Akkerhuis KM, Van Vark L, Boersma E.
 Effect of angiotensin-converting enzyme inhibitors and angiotensin II receptor blockers on cardiovascular mortality in hypertension: a meta-analysis of randomized controlled trials Ferrari R, Fox K, Bertrand
Effect of angiotensin-converting enzyme inhibitors and angiotensin II receptor blockers on cardiovascular mortality in hypertension: a meta-analysis of randomized controlled trials Ferrari R, Fox K, Bertrand
State of the art treatment of hypertension: established and new drugs. Prof. M. Burnier Service of Nephrology and Hypertension Lausanne, Switzerland
 State of the art treatment of hypertension: established and new drugs Prof. M. Burnier Service of Nephrology and Hypertension Lausanne, Switzerland First line therapies in hypertension ACE inhibitors AT
State of the art treatment of hypertension: established and new drugs Prof. M. Burnier Service of Nephrology and Hypertension Lausanne, Switzerland First line therapies in hypertension ACE inhibitors AT
Hypertension Update 2009
 Hypertension Update 2009 New Drugs, New Goals, New Approaches, New Lessons from Clinical Trials Timothy C Fagan, MD, FACP Professor Emeritus University of Arizona New Drugs Direct Renin Inhibitors Endothelin
Hypertension Update 2009 New Drugs, New Goals, New Approaches, New Lessons from Clinical Trials Timothy C Fagan, MD, FACP Professor Emeritus University of Arizona New Drugs Direct Renin Inhibitors Endothelin
Therapeutic Targets and Interventions
 Therapeutic Targets and Interventions Ali Valika, MD, FACC Advanced Heart Failure and Pulmonary Hypertension Advocate Medical Group Midwest Heart Foundation Disclosures: 1. Novartis: Speaker Honorarium
Therapeutic Targets and Interventions Ali Valika, MD, FACC Advanced Heart Failure and Pulmonary Hypertension Advocate Medical Group Midwest Heart Foundation Disclosures: 1. Novartis: Speaker Honorarium
ACE inhibitors vs ARBs Myths and Facts
 ACE inhibitors vs ARBs Myths and Facts Prof. Dr. med. Frank Ruschitzka, FRCP (Edinburgh) Director Heart Failure/Transplantation Clinic University Clinic Zurich Switzerland Conflict of interest: Bayer,
ACE inhibitors vs ARBs Myths and Facts Prof. Dr. med. Frank Ruschitzka, FRCP (Edinburgh) Director Heart Failure/Transplantation Clinic University Clinic Zurich Switzerland Conflict of interest: Bayer,
Amlodipine/Valsartan (Exforge ) Changing the Landscape of BP Management
 Changing the Landscape of BP Management") Amlodipine/Valsartan (Exforge ) Changing the Landscape of BP Management Bum-Kee Hong Yongdong Severance Hospital Yonsei University College of Medicine Rationale for Multiple-Mechanism Therapy Inadequacy
Amlodipine/Valsartan (Exforge ) Changing the Landscape of BP Management Bum-Kee Hong Yongdong Severance Hospital Yonsei University College of Medicine Rationale for Multiple-Mechanism Therapy Inadequacy
Aldosterone Antagonism in Heart Failure: Now for all Patients?
 Aldosterone Antagonism in Heart Failure: Now for all Patients? Inder Anand, MD, FRCP, D Phil (Oxon.) Professor of Medicine, University of Minnesota, Director Heart Failure Program, VA Medical Center 111C
Aldosterone Antagonism in Heart Failure: Now for all Patients? Inder Anand, MD, FRCP, D Phil (Oxon.) Professor of Medicine, University of Minnesota, Director Heart Failure Program, VA Medical Center 111C
Since the initial description of angiotensin II mediated
 CLINICAL CARDIOLOGY: PHYSICIAN UPDATE Manipulation of the Renin-Angiotensin System Michael M. Givertz, MD Since the initial description of angiotensin II mediated hypertension 40 years ago, basic and clinical
CLINICAL CARDIOLOGY: PHYSICIAN UPDATE Manipulation of the Renin-Angiotensin System Michael M. Givertz, MD Since the initial description of angiotensin II mediated hypertension 40 years ago, basic and clinical
ESC Guidelines for the Diagnosis and Treatment of Acute and Chronic Heart Failure
 Patients t with acute heart failure frequently develop chronic heart failure Patients with chronic heart failure frequently decompensate acutely ESC Guidelines for the Diagnosis and A clinical response
Patients t with acute heart failure frequently develop chronic heart failure Patients with chronic heart failure frequently decompensate acutely ESC Guidelines for the Diagnosis and A clinical response
Prevention of Atrial Fibrillation and Heart Failure in the Hypertensive Patient
 Prevention of Atrial Fibrillation and Heart Failure in the Hypertensive Patient The Issue of Primary Prevention of A.Fib. (and Heart Failure) and not the Prevention of Recurrent A.Fib. after Electroconversion
Prevention of Atrial Fibrillation and Heart Failure in the Hypertensive Patient The Issue of Primary Prevention of A.Fib. (and Heart Failure) and not the Prevention of Recurrent A.Fib. after Electroconversion
Drugs acting on the reninangiotensin-aldosterone
 Drugs acting on the reninangiotensin-aldosterone system John McMurray Eugene Braunwald Scholar in Cardiovascular Diseases, Brigham and Women s Hospital, Boston & Visiting Professor, Harvard Medical School
Drugs acting on the reninangiotensin-aldosterone system John McMurray Eugene Braunwald Scholar in Cardiovascular Diseases, Brigham and Women s Hospital, Boston & Visiting Professor, Harvard Medical School
I know the trials in heart failure but how do I manage my patient? Dosing of neurohormones antagonists
 I know the trials in heart failure but how do I manage my patient? Dosing of neurohormones antagonists Alessandro Fucili (Ferrara, IT) Massimo F Piepoli (Piacenza, IT) Clinical Case: 82 year old woman
I know the trials in heart failure but how do I manage my patient? Dosing of neurohormones antagonists Alessandro Fucili (Ferrara, IT) Massimo F Piepoli (Piacenza, IT) Clinical Case: 82 year old woman
The Road to Renin System Optimization: Renin Inhibitor
 The Road to Renin System Optimization: Renin Inhibitor A New Perspective on the Renin-Angiotensin System (RAS) Yong-Jin Kim, MD Seoul National University Hospital Human and Economic Costs of Hypertension
The Road to Renin System Optimization: Renin Inhibitor A New Perspective on the Renin-Angiotensin System (RAS) Yong-Jin Kim, MD Seoul National University Hospital Human and Economic Costs of Hypertension
How clinically important are the results of the large trials in hypertension?
 How clinically important are the results of the large trials in hypertension? Stéphane LAURENT, MD, PhD, FESC Pharmacology Department and PARCC / INSERM U970 Hôpital Européen Georges Pompidou, Université
How clinically important are the results of the large trials in hypertension? Stéphane LAURENT, MD, PhD, FESC Pharmacology Department and PARCC / INSERM U970 Hôpital Européen Georges Pompidou, Université
Cedars Sinai Diabetes. Michael A. Weber
 Cedars Sinai Diabetes Michael A. Weber Speaker Disclosures I disclose that I am a Consultant for: Ablative Solutions, Boston Scientific, Boehringer Ingelheim, Eli Lilly, Forest, Medtronics, Novartis, ReCor
Cedars Sinai Diabetes Michael A. Weber Speaker Disclosures I disclose that I am a Consultant for: Ablative Solutions, Boston Scientific, Boehringer Ingelheim, Eli Lilly, Forest, Medtronics, Novartis, ReCor
Preventing the cardiovascular complications of hypertension
 European Heart Journal Supplements (2004) 6 (Supplement H), H37 H42 Preventing the cardiovascular complications of hypertension Peter Trenkwalder* Department of Internal Medicine, Starnberg Hospital, Ludwig
European Heart Journal Supplements (2004) 6 (Supplement H), H37 H42 Preventing the cardiovascular complications of hypertension Peter Trenkwalder* Department of Internal Medicine, Starnberg Hospital, Ludwig
Renin Angiotensin System Current and Potential Targets
 Renin Angiotensin System Current and Potential Targets Dae Suk Han, MD. Seung Hyeok Han, MD. Department of Internal Medicine Division of Nephrology Yonsei University College of Medicine Renin The First
Renin Angiotensin System Current and Potential Targets Dae Suk Han, MD. Seung Hyeok Han, MD. Department of Internal Medicine Division of Nephrology Yonsei University College of Medicine Renin The First
Hypertension Guidelines: Are We Pressured to Change? Oregon Cardiovascular Symposium Portland, Oregon June 6, Financial Disclosures
 Hypertension Guidelines: Are We Pressured to Change? Oregon Cardiovascular Symposium Portland, Oregon June 6, 2015 William C. Cushman, MD Professor, Preventive Medicine, Medicine, and Physiology University
Hypertension Guidelines: Are We Pressured to Change? Oregon Cardiovascular Symposium Portland, Oregon June 6, 2015 William C. Cushman, MD Professor, Preventive Medicine, Medicine, and Physiology University
Heart Failure: Combination Treatment Strategies
 Heart Failure: Combination Treatment Strategies M. McDonald MD, FRCP State of the Heart Symposium May 28, 2011 None Disclosures Case 69 F, prior MIs (LV ejection fraction 25%), HTN No demonstrable ischemia
Heart Failure: Combination Treatment Strategies M. McDonald MD, FRCP State of the Heart Symposium May 28, 2011 None Disclosures Case 69 F, prior MIs (LV ejection fraction 25%), HTN No demonstrable ischemia
Treating Hypertension in Individuals with Diabetes
 Treating Hypertension in Individuals with Diabetes Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any
Treating Hypertension in Individuals with Diabetes Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any
Combination of renin-angiotensinaldosterone. how to choose?
 Combination of renin-angiotensinaldosterone system inhibitors how to choose? Karl Swedberg Professor of Medicine Sahlgrenska Academy University of Gothenburg karl.swedberg@gu.se Disclosures Research grants
Combination of renin-angiotensinaldosterone system inhibitors how to choose? Karl Swedberg Professor of Medicine Sahlgrenska Academy University of Gothenburg karl.swedberg@gu.se Disclosures Research grants
Mayo Clin Proc, March 2003, Vol 78 Role of ARBs in Treatment of Heart Failure 335 system, tissue-based RAS has long-term effects that can modify cardi
 334 Concise Review for Clinicians Therapeutic Role of Angiotensin II Receptor Blockers in the Treatment of Heart Failure Concise Review for Clinicians PRERANA MANOHAR, MD, AND ILEANA L. PIÑA, MD Angiotensin
334 Concise Review for Clinicians Therapeutic Role of Angiotensin II Receptor Blockers in the Treatment of Heart Failure Concise Review for Clinicians PRERANA MANOHAR, MD, AND ILEANA L. PIÑA, MD Angiotensin
T. Suithichaiyakul Cardiomed Chula
 T. Suithichaiyakul Cardiomed Chula The cardiovascular (CV) continuum: role of risk factors Endothelial Dysfunction Atherosclerosis and left ventricular hypertrophy Myocardial infarction & stroke Endothelial
T. Suithichaiyakul Cardiomed Chula The cardiovascular (CV) continuum: role of risk factors Endothelial Dysfunction Atherosclerosis and left ventricular hypertrophy Myocardial infarction & stroke Endothelial
RENAAL, IRMA-2 and IDNT. Three featured trials linking a disease spectrum IDNT RENAAL. Death IRMA 2
 Treatment of Diabetic Nephropathy and Proteinuria Background End stage renal disease is a major cause of death and disability among diabetics BP reduction is important to slow the progression of diabetic
Treatment of Diabetic Nephropathy and Proteinuria Background End stage renal disease is a major cause of death and disability among diabetics BP reduction is important to slow the progression of diabetic
Managing Hypertension in Diabetes Sean Stewart, PharmD, BCPS, BCACP, CLS Internal Medicine Park Nicollet Clinic St Louis Park.
 Managing Hypertension in Diabetes 2015 Sean Stewart, PharmD, BCPS, BCACP, CLS Internal Medicine Park Nicollet Clinic St Louis Park Case Scenario Mike M is a 59 year old man with type 2 diabetes managed
Managing Hypertension in Diabetes 2015 Sean Stewart, PharmD, BCPS, BCACP, CLS Internal Medicine Park Nicollet Clinic St Louis Park Case Scenario Mike M is a 59 year old man with type 2 diabetes managed
Antihypertensive Trial Design ALLHAT
 1 U.S. Department of Health and Human Services Major Outcomes in High Risk Hypertensive Patients Randomized to Angiotensin-Converting Enzyme Inhibitor or Calcium Channel Blocker vs Diuretic National Institutes
1 U.S. Department of Health and Human Services Major Outcomes in High Risk Hypertensive Patients Randomized to Angiotensin-Converting Enzyme Inhibitor or Calcium Channel Blocker vs Diuretic National Institutes
Are all Antihypertensives the same?
 Are all Antihypertensives the same? Athanasios J. Manolis MD, FACC, FESC, FAHA Director of Cardiology Dept, Asklepeion General Hospital, Athens Greece. Adj. Ass. Professor, Hypertension Section, Boston
Are all Antihypertensives the same? Athanasios J. Manolis MD, FACC, FESC, FAHA Director of Cardiology Dept, Asklepeion General Hospital, Athens Greece. Adj. Ass. Professor, Hypertension Section, Boston
Angiotensin Receptor Blockers: Novel Role in High-Risk Patients
 Angiotensin Receptor Blockers: Novel Role in High-Risk Patients UsmanJaved, MD a, Prakash C. Deedwania, MD, FACC, FACP, FCCP, FAHA a,b, * KEYWORDS Angiotensin receptor blockers RAAS blockade Cardioprotection
Angiotensin Receptor Blockers: Novel Role in High-Risk Patients UsmanJaved, MD a, Prakash C. Deedwania, MD, FACC, FACP, FCCP, FAHA a,b, * KEYWORDS Angiotensin receptor blockers RAAS blockade Cardioprotection
Φαρμακευτική θεραπεία της μετεμφραγματικής καρδιακής ανεπάρκειας. Α. Καραβίδας Υπεύθυνος ιατρείου καρδιακής ανεπάρκειας Γ.Ν.Α Γ.
 Φαρμακευτική θεραπεία της μετεμφραγματικής καρδιακής ανεπάρκειας Α. Καραβίδας Υπεύθυνος ιατρείου καρδιακής ανεπάρκειας Γ.Ν.Α Γ.Γεννηματάς Clinical Trials on Fibrinolysis N = 61.41 AMI pts, ( GUSTO I, GUSTOIIb,
Φαρμακευτική θεραπεία της μετεμφραγματικής καρδιακής ανεπάρκειας Α. Καραβίδας Υπεύθυνος ιατρείου καρδιακής ανεπάρκειας Γ.Ν.Α Γ.Γεννηματάς Clinical Trials on Fibrinolysis N = 61.41 AMI pts, ( GUSTO I, GUSTOIIb,
Blood Pressure Targets: Where are We Now?
 Blood Pressure Targets: Where are We Now? Diana Cao, PharmD, BCPS-AQ Cardiology Assistant Professor Department of Clinical & Administrative Sciences California Northstate University College of Pharmacy
Blood Pressure Targets: Where are We Now? Diana Cao, PharmD, BCPS-AQ Cardiology Assistant Professor Department of Clinical & Administrative Sciences California Northstate University College of Pharmacy
Faiez Zannad. Institut Lorrain du Coeur et des Vaisseaux. CIC - Inserm
 Faiez Zannad Institut Lorrain du Coeur et des Vaisseaux CIC - Inserm Disclosure Faiez Zannad Grants BG Medicine, Roche Diagnostics. Consultant/Steering committees/event committees/ Data safety Monitoring
Faiez Zannad Institut Lorrain du Coeur et des Vaisseaux CIC - Inserm Disclosure Faiez Zannad Grants BG Medicine, Roche Diagnostics. Consultant/Steering committees/event committees/ Data safety Monitoring
Antihypertensive efficacy of olmesartan compared with other antihypertensive drugs
 (2002) 16 (Suppl 2), S24 S28 2002 Nature Publishing Group All rights reserved 0950-9240/02 $25.00 www.nature.com/jhh compared with other antihypertensive drugs University Clinic Bonn, Department of Internal
(2002) 16 (Suppl 2), S24 S28 2002 Nature Publishing Group All rights reserved 0950-9240/02 $25.00 www.nature.com/jhh compared with other antihypertensive drugs University Clinic Bonn, Department of Internal
BLOOD PRESSURE-LOWERING TREATMENT
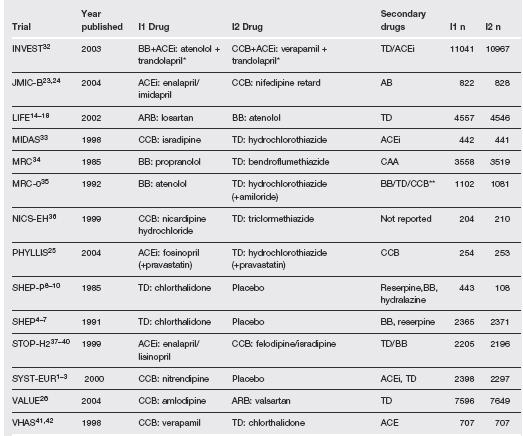
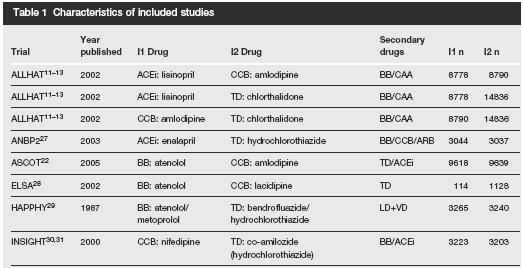
 BLOOD PRESSURE-LOWERING TRIALS NUMBER OF PARTICIPANTS NUMBER OF PERCENTAGE OF MEAN AGE MEAN - (YEARS) TRIALS WITH ANALYSIS BY GENDER N, (%) 69,473 28,008 40.3% 70.2 3.2 3/5 (60%) APPENDIX 2 1 BLOOD PRESSURE-LOWERING
BLOOD PRESSURE-LOWERING TRIALS NUMBER OF PARTICIPANTS NUMBER OF PERCENTAGE OF MEAN AGE MEAN - (YEARS) TRIALS WITH ANALYSIS BY GENDER N, (%) 69,473 28,008 40.3% 70.2 3.2 3/5 (60%) APPENDIX 2 1 BLOOD PRESSURE-LOWERING
Management of The Patients with Hypertension and High Risk Cardiovascular Disease
 Management of The Patients with Hypertension and High Risk Cardiovascular Disease Songsak Kiatchoosakun, MD. Cardiology, Medicine Khon Kaen University CVD and Hypertension: Worldwide Morbidity and Mortality
Management of The Patients with Hypertension and High Risk Cardiovascular Disease Songsak Kiatchoosakun, MD. Cardiology, Medicine Khon Kaen University CVD and Hypertension: Worldwide Morbidity and Mortality
Clinical Updates in the Treatment of Hypertension JNC 7 vs. JNC 8. Lauren Thomas, PharmD PGY1 Pharmacy Practice Resident South Pointe Hospital
 Clinical Updates in the Treatment of Hypertension JNC 7 vs. JNC 8 Lauren Thomas, PharmD PGY1 Pharmacy Practice Resident South Pointe Hospital Objectives Review the Eighth Joint National Committee (JNC
Clinical Updates in the Treatment of Hypertension JNC 7 vs. JNC 8 Lauren Thomas, PharmD PGY1 Pharmacy Practice Resident South Pointe Hospital Objectives Review the Eighth Joint National Committee (JNC
The Role of ACEI and ARBs in AF prevention
 The Role of ACEI and ARBs in AF prevention Dr. Sameh Shaheen MD, FESC Prof. of cardiology Ain-Shams university Time course of atrial substrate remodeling in relation to the clinical appearance of AF and
The Role of ACEI and ARBs in AF prevention Dr. Sameh Shaheen MD, FESC Prof. of cardiology Ain-Shams university Time course of atrial substrate remodeling in relation to the clinical appearance of AF and
Hypertension in Geriatrics. Dr. Allen Liu Consultant Nephrologist 10 September 2016
 Hypertension in Geriatrics Dr. Allen Liu Consultant Nephrologist 10 September 2016 Annual mortality (%) Cardiovascular Mortality Rates are Higher among Dialysis Patients 100 10 1 0.1 0.01 0.001 25-34
Hypertension in Geriatrics Dr. Allen Liu Consultant Nephrologist 10 September 2016 Annual mortality (%) Cardiovascular Mortality Rates are Higher among Dialysis Patients 100 10 1 0.1 0.01 0.001 25-34
New evidences in heart failure: the GISSI-HF trial. Aldo P Maggioni, MD ANMCO Research Center Firenze, Italy
 New evidences in heart failure: the GISSI-HF trial Aldo P Maggioni, MD ANMCO Research Center Firenze, Italy % Improving survival in chronic HF and LV systolic dysfunction: 1 year all-cause mortality 20
New evidences in heart failure: the GISSI-HF trial Aldo P Maggioni, MD ANMCO Research Center Firenze, Italy % Improving survival in chronic HF and LV systolic dysfunction: 1 year all-cause mortality 20
Where are we with RAS blockade? New Targets.
 Where are we with RAS blockade? New Targets. Pr. M. Burnier Service of Nephrology and Hypertension Consultation Centre Hospitalier Universitaire Vaudois Lausanne, Switzerland Introduction of new antihypertensive
Where are we with RAS blockade? New Targets. Pr. M. Burnier Service of Nephrology and Hypertension Consultation Centre Hospitalier Universitaire Vaudois Lausanne, Switzerland Introduction of new antihypertensive
Causes of Poor BP control Rates
 Goals Of Hypertension Management in Clinical Practice World Hypertension League (WHL) Meeting Adel E. Berbari, MD, FAHA, FACP Professor of Medicine and Physiology Head, Division of Hypertension and Vascular
Goals Of Hypertension Management in Clinical Practice World Hypertension League (WHL) Meeting Adel E. Berbari, MD, FAHA, FACP Professor of Medicine and Physiology Head, Division of Hypertension and Vascular
Hypertension Update Warwick Jaffe Interventional Cardiologist Ascot Hospital
 Hypertension Update 2008 Warwick Jaffe Interventional Cardiologist Ascot Hospital Definition of Hypertension Continuous variable At some point the risk becomes high enough to justify treatment Treatment
Hypertension Update 2008 Warwick Jaffe Interventional Cardiologist Ascot Hospital Definition of Hypertension Continuous variable At some point the risk becomes high enough to justify treatment Treatment
Η θέση της αντισπερτασικής αγωγής στην πρόληψη της κολπικής μαρμαρσγής. Ανδρέας Πιηηαράς. Σεμινάριο ΟΕ ΕΚΕ Θεζζαλονίκη 2012
 Η θέση της αντισπερτασικής αγωγής στην πρόληψη της κολπικής μαρμαρσγής Ανδρέας Πιηηαράς Σεμινάριο ΟΕ ΕΚΕ Θεζζαλονίκη 2012 AF May Present with a Wide Range of Symptoms LIGHT- HEADEDNESS PALPITATIONS SYNCOPE
Η θέση της αντισπερτασικής αγωγής στην πρόληψη της κολπικής μαρμαρσγής Ανδρέας Πιηηαράς Σεμινάριο ΟΕ ΕΚΕ Θεζζαλονίκη 2012 AF May Present with a Wide Range of Symptoms LIGHT- HEADEDNESS PALPITATIONS SYNCOPE
Entresto Development of sacubitril/valsartan (LCZ696) for the treatment of heart failure with reduced ejection fraction
 for the treatment of heart failure with reduced ejection fraction") Cardio-Metabolic Franchise Entresto Development of sacubitril/valsartan (LCZ696) for the treatment of heart failure with reduced ejection fraction Randy L Webb, PhD Rutgers Workshop October 21, 2016 Heart
Cardio-Metabolic Franchise Entresto Development of sacubitril/valsartan (LCZ696) for the treatment of heart failure with reduced ejection fraction Randy L Webb, PhD Rutgers Workshop October 21, 2016 Heart
Treating HF Patients with ARNI s Why, When and How?
 Treating HF Patients with ARNI s Why, When and How? 19 th Annual San Diego Heart Failure Symposium for Primary Care Physicians January 11-12, 2019 La Jolla, CA Barry Greenberg M.D. Distinguished Professor
Treating HF Patients with ARNI s Why, When and How? 19 th Annual San Diego Heart Failure Symposium for Primary Care Physicians January 11-12, 2019 La Jolla, CA Barry Greenberg M.D. Distinguished Professor
Metabolic Consequences of Anti Hypertensives: Is It Clinically Important?
 Metabolic Consequences of Anti Hypertensives: Is It Clinically Important?,FACA,FICA,MASH,FVBWG,MISCP CONSULTANT OF CARDIOLOGY DIRECTOR OF PORT-FOUAD HOSPITAL CCU Consideration of antihypertensive agents
Metabolic Consequences of Anti Hypertensives: Is It Clinically Important?,FACA,FICA,MASH,FVBWG,MISCP CONSULTANT OF CARDIOLOGY DIRECTOR OF PORT-FOUAD HOSPITAL CCU Consideration of antihypertensive agents
JNC 8 -Controversies. Sagren Naidoo Nephrologist CMJAH
 JNC 8 -Controversies Sagren Naidoo Nephrologist CMJAH Joint National Committee (JNC) Panel appointed by the National Heart, Lung, and Blood Institute (NHLBI) First guidelines (JNC-1) published in 1977
JNC 8 -Controversies Sagren Naidoo Nephrologist CMJAH Joint National Committee (JNC) Panel appointed by the National Heart, Lung, and Blood Institute (NHLBI) First guidelines (JNC-1) published in 1977
HF-PEF: Symptoms, quality of life and mortality/morbidity
 HF-PEF: Symptoms, quality of life and mortality/morbidity May 21, 2011 John McMurray, MD Eugene Braunwald Scholar in Cardiovascular Diseases, Brigham & Women s Hospital Boston; Visiting Professor of Medicine,
HF-PEF: Symptoms, quality of life and mortality/morbidity May 21, 2011 John McMurray, MD Eugene Braunwald Scholar in Cardiovascular Diseases, Brigham & Women s Hospital Boston; Visiting Professor of Medicine,
Stříbrná svatba srdečního selhání a blokády systému RAAS
 Stříbrná svatba srdečního selhání a blokády systému RAAS Jiří Vítovec LF MU a ICRC FN u sv.anny Patofysiologický efekt angiotensinu II Vasokonstrikce Kontraktilita Aktivace SNS Aldosteron PAI-1/ trombosa
Stříbrná svatba srdečního selhání a blokády systému RAAS Jiří Vítovec LF MU a ICRC FN u sv.anny Patofysiologický efekt angiotensinu II Vasokonstrikce Kontraktilita Aktivace SNS Aldosteron PAI-1/ trombosa
ANGIOTENSIN II RECEPTOR BLOCKERS: MORE THAN THE ALTERNATIVE PRESENTATION BY: PATRICK HO, USC PHARM D. CANDIDATE OF 2017 MENTOR: DR.
 ANGIOTENSIN II RECEPTOR BLOCKERS: MORE THAN THE ALTERNATIVE PRESENTATION BY: PATRICK HO, USC PHARM D. CANDIDATE OF 2017 MENTOR: DR. CRAIG STERN, PHARMD, MBA, RPH, FASCP, FASHP, FICA, FLMI, FAMCP RENIN-ANGIOTENSIN
ANGIOTENSIN II RECEPTOR BLOCKERS: MORE THAN THE ALTERNATIVE PRESENTATION BY: PATRICK HO, USC PHARM D. CANDIDATE OF 2017 MENTOR: DR. CRAIG STERN, PHARMD, MBA, RPH, FASCP, FASHP, FICA, FLMI, FAMCP RENIN-ANGIOTENSIN
ALLHAT Role of Diuretics in the Prevention of Heart Failure - The Antihypertensive and Lipid- Lowering Treatment to Prevent Heart Attack Trial
 1 ALLHAT Role of Diuretics in the Prevention of Heart Failure - The Antihypertensive and Lipid- Lowering Treatment to Prevent Heart Attack Trial Davis BR, Piller LB, Cutler JA, et al. Circulation 2006.113:2201-2210.
1 ALLHAT Role of Diuretics in the Prevention of Heart Failure - The Antihypertensive and Lipid- Lowering Treatment to Prevent Heart Attack Trial Davis BR, Piller LB, Cutler JA, et al. Circulation 2006.113:2201-2210.
Hypertension Update Clinical Controversies Regarding Age and Race
 Hypertension Update Clinical Controversies Regarding Age and Race Allison Helmer, PharmD, BCACP Assistant Clinical Professor Auburn University Harrison School of Pharmacy July 22, 2017 DISCLOSURE/CONFLICT
Hypertension Update Clinical Controversies Regarding Age and Race Allison Helmer, PharmD, BCACP Assistant Clinical Professor Auburn University Harrison School of Pharmacy July 22, 2017 DISCLOSURE/CONFLICT
Women s Heart Health: Holistic Approaches Throughout the Lifetime - Key Differences in Heart Failure in Women
 Women s Heart Health: Holistic Approaches Throughout the Lifetime - Key Differences in Heart Failure in Women C. Noel Bairey Merz MD Medical Director and Barbra Streisand Women s Heart Center Preventive
Women s Heart Health: Holistic Approaches Throughout the Lifetime - Key Differences in Heart Failure in Women C. Noel Bairey Merz MD Medical Director and Barbra Streisand Women s Heart Center Preventive
Combination Therapy for Hypertension
 Combination Therapy for Hypertension Se-Joong Rim, MD Cardiology Division, Yonsei University College of Medicine, Seoul, Korea Goals of Therapy Reduce CVD and renal morbidity and mortality. Treat to BP
Combination Therapy for Hypertension Se-Joong Rim, MD Cardiology Division, Yonsei University College of Medicine, Seoul, Korea Goals of Therapy Reduce CVD and renal morbidity and mortality. Treat to BP
New Lipid Guidelines. PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN: Implications of the New Guidelines for Hypertension and Lipids.
 PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN: Implications of the New Guidelines for Hypertension and Lipids Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Disclosure No relevant
PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN: Implications of the New Guidelines for Hypertension and Lipids Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Disclosure No relevant
Disclosure of Relationships
 Disclosure of Relationships Over the past 12 months Dr Ruilope has served as Consultant and Speakers Bureau member of Astra-Zeneca, Bayer, Daiichi-Sankyo, Menarini, Novartis, Otsuka, Pfizer, Relypsa, Servier
Disclosure of Relationships Over the past 12 months Dr Ruilope has served as Consultant and Speakers Bureau member of Astra-Zeneca, Bayer, Daiichi-Sankyo, Menarini, Novartis, Otsuka, Pfizer, Relypsa, Servier
Outcomes and Perspectives of Single-Pill Combination Therapy for the modern management of hypertension
 Outcomes and Perspectives of Single-Pill Combination Therapy for the modern management of hypertension Prof. Massimo Volpe, MD, FAHA, FESC, Chair of Cardiology, Department of Clinical and Molecular Medicine
Outcomes and Perspectives of Single-Pill Combination Therapy for the modern management of hypertension Prof. Massimo Volpe, MD, FAHA, FESC, Chair of Cardiology, Department of Clinical and Molecular Medicine
HFpEF. April 26, 2018
 HFpEF April 26, 2018 (J Am Coll Cardiol 2017;70:2476 86) HFpEF 50% or more (40-71%) of patients with CHF have preserved LV systolic function. HFpEF is an increasingly frequent hospital discharge. Outcomes
HFpEF April 26, 2018 (J Am Coll Cardiol 2017;70:2476 86) HFpEF 50% or more (40-71%) of patients with CHF have preserved LV systolic function. HFpEF is an increasingly frequent hospital discharge. Outcomes
HYPERTENSION GUIDELINES WHERE ARE WE IN 2014
 HYPERTENSION GUIDELINES WHERE ARE WE IN 2014 Donald J. DiPette MD FACP Special Assistant to the Provost for Health Affairs Distinguished Health Sciences Professor University of South Carolina University
HYPERTENSION GUIDELINES WHERE ARE WE IN 2014 Donald J. DiPette MD FACP Special Assistant to the Provost for Health Affairs Distinguished Health Sciences Professor University of South Carolina University
The CARI Guidelines Caring for Australasians with Renal Impairment. Blood Pressure Control role of specific antihypertensives
 Blood Pressure Control role of specific antihypertensives Date written: May 2005 Final submission: October 2005 Author: Adrian Gillian GUIDELINES a. Regimens that include angiotensin-converting enzyme
Blood Pressure Control role of specific antihypertensives Date written: May 2005 Final submission: October 2005 Author: Adrian Gillian GUIDELINES a. Regimens that include angiotensin-converting enzyme
DIASTOLIC HEART FAILURE
 DIASTOLIC HEART FAILURE M Mohsen Ibrahim, MD Alexandria, Proposed Criteria for Diastolic Heart Failure ESC Working Group (EHJ 1998) CHF signs/symptoms EF 45% Hemodynamic or echo evidence of diastolic dysfunction
DIASTOLIC HEART FAILURE M Mohsen Ibrahim, MD Alexandria, Proposed Criteria for Diastolic Heart Failure ESC Working Group (EHJ 1998) CHF signs/symptoms EF 45% Hemodynamic or echo evidence of diastolic dysfunction
Management of Lipid Disorders and Hypertension: Implications of the New Guidelines
 Management of Lipid Disorders and Hypertension Management of Lipid Disorders and Hypertension: Implications of the New Guidelines Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine
Management of Lipid Disorders and Hypertension Management of Lipid Disorders and Hypertension: Implications of the New Guidelines Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine
Angiotensin receptor blockers in the treatment of heart failure
 Heart Failure: Pharmacologic Management Edited by Arthur M. Feldman Copyright 2006 by Blackwell Publishing 4 CHAPTER 4 Angiotensin receptor blockers in the treatment of heart failure Anita Deswal, MD,
Heart Failure: Pharmacologic Management Edited by Arthur M. Feldman Copyright 2006 by Blackwell Publishing 4 CHAPTER 4 Angiotensin receptor blockers in the treatment of heart failure Anita Deswal, MD,
Heart Failure Management Update
 Heart Failure Management Update Rafique Ahmed, MD, PhD, FACC, FCPS Consultant Cardiac Electrophysiologist Baltimore, Maryland, USA Heart Failure - Definition The situation when the heart is incapable of
Heart Failure Management Update Rafique Ahmed, MD, PhD, FACC, FCPS Consultant Cardiac Electrophysiologist Baltimore, Maryland, USA Heart Failure - Definition The situation when the heart is incapable of
Cardiovascular Diseases in CKD
 1 Cardiovascular Diseases in CKD Hung-Chun Chen, MD, PhD. Kaohsiung Medical University Taiwan Society of Nephrology 1 2 High Prevalence of CVD in CKD & ESRD Foley RN et al, AJKD 1998; 32(suppl 3):S112-9
1 Cardiovascular Diseases in CKD Hung-Chun Chen, MD, PhD. Kaohsiung Medical University Taiwan Society of Nephrology 1 2 High Prevalence of CVD in CKD & ESRD Foley RN et al, AJKD 1998; 32(suppl 3):S112-9
New updates on Hypertension and Heart Failure 2015 Yiu Kai Hang
 New updates on Hypertension and Heart Failure 2015 Yiu Kai Hang MD, MBBS, MRCP, FHKCP, FHKAM, FRCP (Edin) Clinical Associate Professor Cardiology Division, Department of Medicine, HKU Honorary Consultant,
New updates on Hypertension and Heart Failure 2015 Yiu Kai Hang MD, MBBS, MRCP, FHKCP, FHKAM, FRCP (Edin) Clinical Associate Professor Cardiology Division, Department of Medicine, HKU Honorary Consultant,
Antialdosterone treatment in heart failure
 Update on the Treatment of Chronic Heart Failure 2012 Antialdosterone treatment in heart failure 전남의대윤현주 Chronic Heart Failure Prognosis of Heart failure Cecil, Text book of Internal Medicine, 22 th edition
Update on the Treatment of Chronic Heart Failure 2012 Antialdosterone treatment in heart failure 전남의대윤현주 Chronic Heart Failure Prognosis of Heart failure Cecil, Text book of Internal Medicine, 22 th edition
Caring for Australians with Renal Impairment. BP lowering and CVD
 Caring for Australians with Renal Impairment BP lowering and CVD Questions: Conflicts of Interest: RH, TN, HHL- no conflict VP- level II conflict Speakers fees: Abbott, Astra Zeneca, Roche, Servier Grant
Caring for Australians with Renal Impairment BP lowering and CVD Questions: Conflicts of Interest: RH, TN, HHL- no conflict VP- level II conflict Speakers fees: Abbott, Astra Zeneca, Roche, Servier Grant
ALLHAT. Major Outcomes in High Risk Hypertensive Patients Randomized to Angiotensin-Converting Enzyme Inhibitor or Calcium Channel Blocker vs Diuretic
 1 U.S. Department of Health and Human Services National Institutes of Health Major Outcomes in High Risk Hypertensive Patients Randomized to Angiotensin-Converting Enzyme Inhibitor or Calcium Channel Blocker
1 U.S. Department of Health and Human Services National Institutes of Health Major Outcomes in High Risk Hypertensive Patients Randomized to Angiotensin-Converting Enzyme Inhibitor or Calcium Channel Blocker
Hypertension: What s new since JNC 7. Harold M. Szerlip, MD, FACP, FCCP, FASN, FNKF
 Hypertension: What s new since JNC 7 Harold M. Szerlip, MD, FACP, FCCP, FASN, FNKF Disclosures Spectral Diagnostics Site investigator Eli Lilly Site investigator ACP IM ITE writing committee NBME Step
Hypertension: What s new since JNC 7 Harold M. Szerlip, MD, FACP, FCCP, FASN, FNKF Disclosures Spectral Diagnostics Site investigator Eli Lilly Site investigator ACP IM ITE writing committee NBME Step
Modern Management of Hypertension
 Modern Management of Hypertension Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Current Status of Hypertension Prevalence
Modern Management of Hypertension Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Current Status of Hypertension Prevalence
Heart Failure Treatments
 Heart Failure Treatments Past & Present www.philippelefevre.com Background Background Chronic heart failure Drugs Mechanical Electrical Background Chronic heart failure Drugs Mechanical Electrical Sudden
Heart Failure Treatments Past & Present www.philippelefevre.com Background Background Chronic heart failure Drugs Mechanical Electrical Background Chronic heart failure Drugs Mechanical Electrical Sudden
Hypertension. Does it Matter What Medications We Use? Nishant K. Sekaran, M.D. M.Sc. Intermountain Heart Institute
 Hypertension Does it Matter What Medications We Use? Nishant K. Sekaran, M.D. M.Sc. Intermountain Heart Institute Hypertension 2017 Classification BP Category Systolic Diastolic Normal 120 and 80 Elevated
Hypertension Does it Matter What Medications We Use? Nishant K. Sekaran, M.D. M.Sc. Intermountain Heart Institute Hypertension 2017 Classification BP Category Systolic Diastolic Normal 120 and 80 Elevated
Valsartan Amlodipine HCT Combination: Control To Goal. Dr. Sameh Shaheen M.B.B.Ch, MSc, MD, FESC, FSCAI. Prof of cardiology Ain Shams University
 Valsartan Amlodipine HCT Combination: Control To Goal Dr. Sameh Shaheen M.B.B.Ch, MSc, MD, FESC, FSCAI Prof of cardiology Ain Shams University Sonesta Hotel Cairo Egypt December 4 th 5 th ; 213 Hypertension
Valsartan Amlodipine HCT Combination: Control To Goal Dr. Sameh Shaheen M.B.B.Ch, MSc, MD, FESC, FSCAI Prof of cardiology Ain Shams University Sonesta Hotel Cairo Egypt December 4 th 5 th ; 213 Hypertension
Management of Hypertension
 Clinical Practice Guidelines Management of Hypertension Definition and classification of blood pressure levels (mmhg) Category Systolic Diastolic Normal
Clinical Practice Guidelines Management of Hypertension Definition and classification of blood pressure levels (mmhg) Category Systolic Diastolic Normal
Heart Failure Clinician Guide JANUARY 2018
 Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Heart Failure Clinician Guide JANUARY 2018 Introduction This evidence-based guideline summary is based on the 2018 National Heart Failure Guideline.
Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Heart Failure Clinician Guide JANUARY 2018 Introduction This evidence-based guideline summary is based on the 2018 National Heart Failure Guideline.
Pharmacological Treatment for Chronic Heart Failure. Dr Elaine Chau HK Sanatorium & Hospital, Hong Kong 3 August 2014
 Pharmacological Treatment for Chronic Heart Failure Dr Elaine Chau HK Sanatorium & Hospital, Hong Kong 3 August 2014 1 ACC/AHA 2005 guideline update for Diagnosis & management of CHF in the Adult -SA Hunt
Pharmacological Treatment for Chronic Heart Failure Dr Elaine Chau HK Sanatorium & Hospital, Hong Kong 3 August 2014 1 ACC/AHA 2005 guideline update for Diagnosis & management of CHF in the Adult -SA Hunt
Online Appendix (JACC )
") Beta blockers in Heart Failure Collaborative Group Online Appendix (JACC013117-0413) Heart rate, heart rhythm and prognostic effect of beta-blockers in heart failure: individual-patient data meta-analysis
Beta blockers in Heart Failure Collaborative Group Online Appendix (JACC013117-0413) Heart rate, heart rhythm and prognostic effect of beta-blockers in heart failure: individual-patient data meta-analysis
Joo-Yong Hahn, MD/PhD
 Sungkyunkwan University School of Medicine Joo-Yong Hahn, MD/PhD Heart Vascular Stork Institute, Samsung Medical Center Sungkyunkwan University School of Medicine Grant support Korean Society of Interventional
Sungkyunkwan University School of Medicine Joo-Yong Hahn, MD/PhD Heart Vascular Stork Institute, Samsung Medical Center Sungkyunkwan University School of Medicine Grant support Korean Society of Interventional
Modern Management of Hypertension: Where Do We Draw the Line?
 Modern Management of Hypertension: Where Do We Draw the Line? Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Blood Pressure
Modern Management of Hypertension: Where Do We Draw the Line? Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Blood Pressure
Explore the Rationale for the Dual Mechanism CCB/ARB Approach in Hypertension Management
 Explore the Rationale for the Dual Mechanism CCB/ARB Approach in Hypertension Management Jeong Bae Park, MD,PhD Dept of Med/Cardiology, Cheil General Hospital, Kwandong University College of Medicine Apr
Explore the Rationale for the Dual Mechanism CCB/ARB Approach in Hypertension Management Jeong Bae Park, MD,PhD Dept of Med/Cardiology, Cheil General Hospital, Kwandong University College of Medicine Apr
Hypertension Management Controversies in the Elderly Patient
 Hypertension Management Controversies in the Elderly Patient Juan Bowen, MD Geriatric Update for the Primary Care Provider November 17, 2016 2016 MFMER slide-1 Disclosure No financial relationships No
Hypertension Management Controversies in the Elderly Patient Juan Bowen, MD Geriatric Update for the Primary Care Provider November 17, 2016 2016 MFMER slide-1 Disclosure No financial relationships No
Diabetes and Hypertension
 Diabetes and Hypertension William C. Cushman, MD, FAHA, FACP, FASH Chief, Preventive Medicine, Veterans Affairs Medical Center Professor, Preventive Medicine, Medicine, and Physiology University of Tennessee
Diabetes and Hypertension William C. Cushman, MD, FAHA, FACP, FASH Chief, Preventive Medicine, Veterans Affairs Medical Center Professor, Preventive Medicine, Medicine, and Physiology University of Tennessee