INTRODUCTION. Acute respiratory distress syndrome (ARDS) is a common complication of critical illness
|
|
|
- Easter Gordon
- 5 years ago
- Views:
Transcription
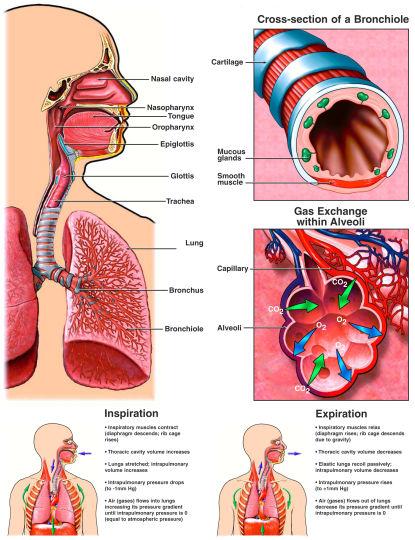
1 Breanna Keller NDFS 356 Acute Respiratory Distress Syndrome INTRODUCTION Acute respiratory distress syndrome (ARDS) is a common complication of critical illness and results in the sudden failure of the respiratory system. ARDS occurs when fluid builds up in the lungs and prevents normal gas exchange. The build up of fluid prevents oxygen from passing through to the bloodstream and can cause rapid, difficult breathing, low blood pressure, and organ failure. ARDS patients are often critically ill with coexisting conditions such as sepsis and multiple organ failure and require ventilator and fluid management support. Despite progress in understanding ARDS pathophysiology and treatment practices, mortality rates are still as high as 40-46% (1) and quality of life post ARDS is subpar. DISEASE DESCRIPTION ARDS is the acute onset of clinically significant hypoxemia with presence of diffuse pulmonary edema resulting from increased pulmonary vascular permeability (2). ARDS is used to describe worsened conditions of severe hypoxemia in acute lung injury (ALI). Diagnostic criteria for ALI and ARDS are the same except for oxygenation standards. Partial arterial pressure of oxygen (PaO 2 )/fractional concentration of oxygen in inspired air (FiO 2 ) in ALI is <300 mg Hg, whereas (PaO 2 )/(FiO 2 ) in ARDS <200 mg Hg. ALI and ARDS are both characterized to have <18 mm Hg pulmonary acute wedge pressure with no signs of left arterial hypertension or fluid overload (3). ARDS is a leading cause of prolonged intensive care unit (ICU) stays and has been a subject of great interest.
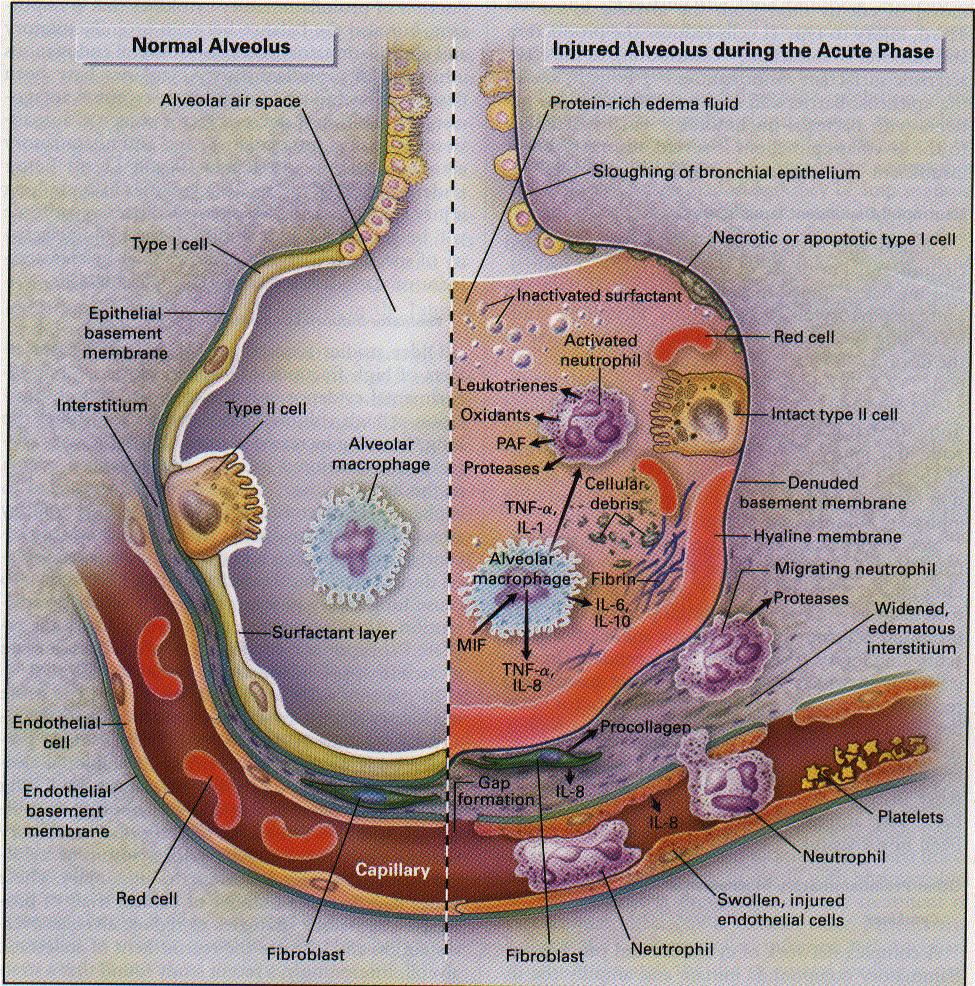
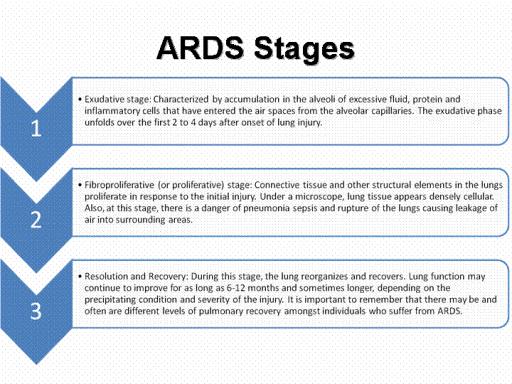
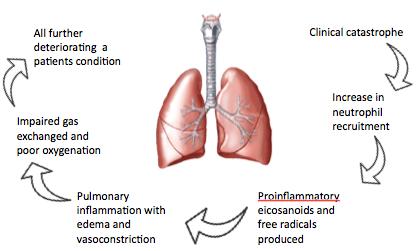
2 ETIOLOGY ALI/ARDS is the result of direct injury or indirect injury to the lungs. Direct injuries may be related to pneumonia, gastric aspiration, drowning, fat and amniotic-fluid embolism, pulmonary contusion, alveolar hemorrhage, smoke and toxic gas inhalation, reperfusion, and unilateral lung re-implantation. Indirect injuries include severe sepsis, transfusions, shock, narcotic overdose, and pancreatitis (2). Factors that appear to increase the risk of developing ALI/ARDS include advanced age, cigarette smoking, alcohol use, and gender (female) indicated during trauma cases. Recent studies suggest a genetic link between variations of the FAS gene and ALI susceptibility (4). Further research is needed to understand causes of ALI/ARDS. PATHOPHYSIOLOGY Acute Exudative Phase ARDS occurs in two stages: the acute exudative phase and fibroproliferative phase. Early histologic changes in the acute exudative phase are characterized by disruption of the capillary endothelium-alveolar epithelium interface, protein-rich pulmonary edema, and increased neutrophilic alveolar infiltrates (3). Direct or indirect injury to the capillary endothelium-alveolar epithelium interface allows protein-rich fluids to leak into the interstitium and alveolar space. Initial injury and presence of pulmonary edema causes diffuse alveolar damage, and stimulates an inflammatory response to release cytokines (e.g. TNF, IL-1, IL-6) and attract neutrophils to the lungs. Neutrophilic activity produces reactive oxygen species and proteases and causes oxidative cell damage. Oxidative stress and protease activity reduce surfactant activity as well as inactivate remaining surfactant
3 promoting diffuse atelectasis (2). Additionally, protease or elastase activity damages the structural framework of the lung and increased permeability exacerbates pulmonary edema. The presence of excess fluid and atelectasis leads to ventilation-perfusion mismatch and reduced lung compliance, as evidenced by hypoxemic vasoconstriction (3). Sustained pulmonary artery pressures may lead to right heart failure. Oxygen demands will eventually exceed the lungs ability to perform normal gas exchange and result in hypoxemic, hypercarbic respiratory failure. Fibroproliferative Phase The initial phase of fluid accumulation is followed by a proliferation phase. Chronic inflammation, fibrosis, and neovascularization occur during the fibroproliferative phase. However, time is the only feature used to distinguish between the exudative phase and fibroproliferative phase (2). The proliferation phase begins within 72 hours and lasts for more than 7 days. Noted activity during this phase includes proliferation of type II alveolar cells, fibroblast activity, and new matrix deposition (1). Type I alveolar cells provide surface area for gas exchange to occur. Type II alveolar cells act as progenitor cells for both type I and II alveolar cells, as well as synthesize, store, and release surfactant in order to maximize gas exchange (5). Fibroblast activity synthesizes collagen, the structural framework for connective tissue and promotes scarring. During the proliferation phase, type II cells proliferate with some alveolar epithelial cell regeneration and fibroblastic remodeling (6). It is not completely understood what factors influence progression into the proliferation phase or recovery. However, those who develop fibrosis have decreased lung compliance, as well as increased hypoxemia and risk of mortality (1).
4 METHODS OF MEDICAL DIAGNOSIS There is no specific method for diagnosing ARDS. ARDS is diagnosed by ruling out other diseases or conditions that produce similar symptoms. Imaging A chest x-ray is a non-invasive test that creates pictures of the chest, heart, lungs, large arteries, ribs, and diaphragm using electromagnetic waves. Computerized tomography (CT) scan combines x-ray images taken from different cross-sectional views to provide information about structures within the heart and lungs. ARDS patients are diagnosed with bilateral pulmonary infiltrates seen on a front chest radiograph. Lab Tests Tests used to diagnose ARDS include arterial blood gas, CBC to indicate low oxygen levels or hypoxemic conditions, and tests for possible infections. Sputum cultures can be collected and analyzed to determine type of lung infection. Heart Tests ARDS is diagnosed by excluding cardiogenic pulmonary edema and other causes of hypoxemic respiratory failure. Electrocardiogram and echocardiogram are used because signs and symptoms of ARDS are similar to those of heart problems. For instance, an echocardiogram is used to rule out congestive heart failure, which can look similar to ARDS on a chest x-ray (7). CURRENT MEDICAL THERAPIES Currently there are no specific treatments for ARDS. Better understanding of the pathogenesis of ARDS and technological advancements has improved therapeutic
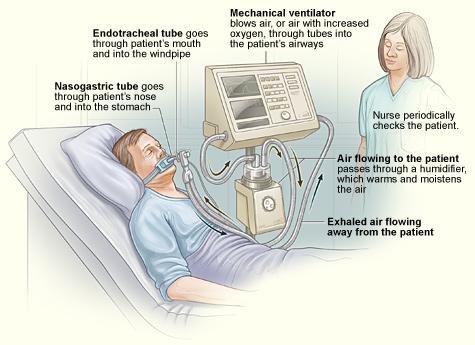
5 practices. Supportive care looks to treat the underlying cause of ARDS, as well as maintain adequate oxygenation and avoid iatrogenic complications (2). ICU patient beds will raise the head of bed 30 degrees to reduce risks of hospital-acquired pneumonia and aspiration. Mechanical Ventilation Mechanical ventilation relieves the respiratory muscles of their work by using supplying supplemental oxygen and pressure to expand atelectatic alveoli and assist with impaired gas exchange. The traditional approach of ventilation was to achieve near normal arterial blood gases, even if high tidal volumes and volume-cycled ventilation were used. It became apparent that high tidal volumes and increased extrinsic positive end expiratory pressure (PEEP) leads to over-distention and injury of compliant alveoli, as well as exacerbates the existing injury and inflammatory response (2). Current practices take a pressure and volume-limited approach with permissive hypercapnia. Low Tidal Volume Ventilation Tidal volume represents the volume of air displaced between inspiration and expiration. Studies show large tidal volumes and high inspiratory pressures results in development of hyaline membranes and exacerbates the inflammatory response (1). The National Heart Lung and Blood Institute (NHLBI) ARDS Network conducted a randomized controlled trial that compared low versus high tidal volume ventilated patients. Low tidal volume had higher survival rates and higher rates of weaning from mechanical ventilation (8). Current recommendations are to use 6 ml/kg predicted bodyweight tidal volume.
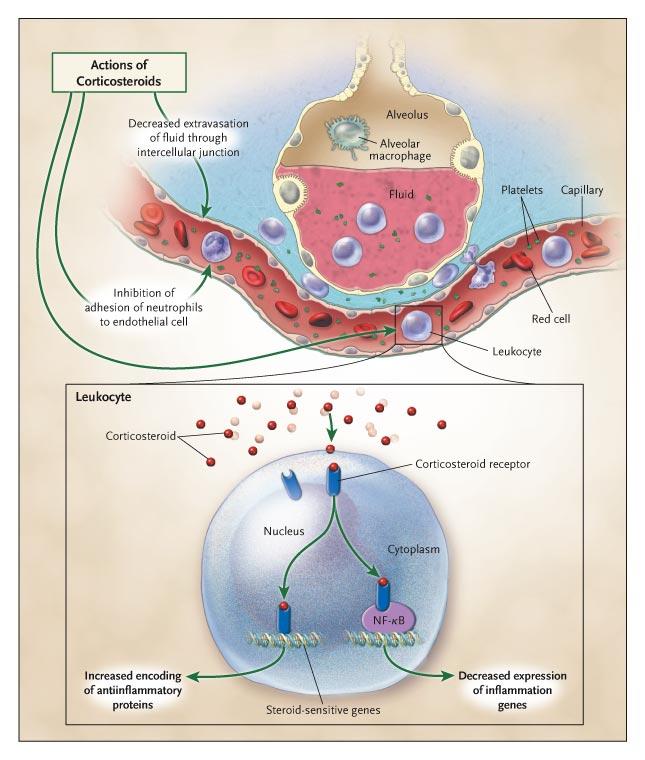
6 PEEP Positive end expiratory pressure (PEEP) is the alveolar pressure that exists at the end of expiration. PEEP provides pressure support in atelectatic alveoli, increases functional residual capacity, and improves oxygenation. High PEEP levels could increase edema, over-distend compliant alveoli, worsen ventilation-perfusion matching, and cause hypotension. Research suggests higher PEEP levels are not harmful but pressure-limited mode of ventilation be used rather than volume-cycled ventilation (2). Current recommendations are to use the lowest PEEP-F i O 2 that produces acceptable oxygenation 88%-95%. Weaning As soon as the condition that caused respiratory failure has started to improve, weaning from ventilation may begin (9). The transition requires patients to be hemodynamically stable, able to take spontaneous breaths, and need <50% supplemental O 2 and <8 cm H 2 O PEEP (2). Prone Positioning Improved oxygenation has been reported in ARDS patients when in the prone position. Proposed benefits from prone positioning include increased chest wall elastance, improved ventilation due to decreased ventilation-perfusion mismatch, and reduced ventilator-associated lung injury (1). However, evidence does not support routine use of the prone position in improving survival rates (10). Corticosteroids Corticosteroids are used to regulate the inflammatory response through increased
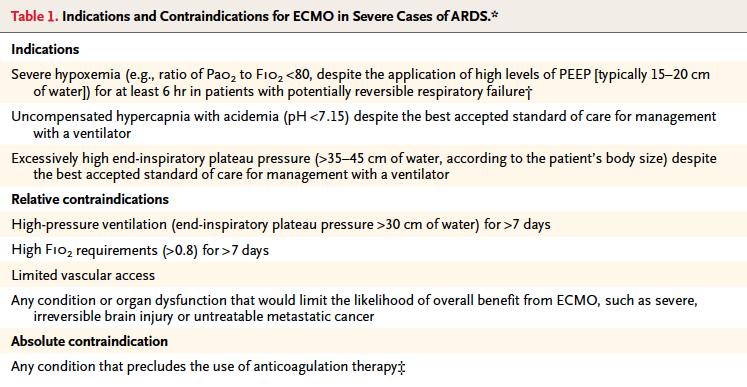
7 encoding for anti-inflammatory proteins and decreased expression of inflammation genes. Evidence for the use of corticosteroids to prevent or treat early ALI is inconclusive, but may be beneficial in late persistent ALI (2). Fluid Management Increased lung capillary permeability leads to an accumulation of fluids in the interstitium and alveolar space. The NHLBI ARDS network recommends conservative fluid administration to improve lung function and shorten duration of mechanical ventilation (1). Fluid restrictions and diuretic use help to alleviate pulmonary edema seen in ARDS. Vasodilators Pulmonary hypoxemic vasoconstriction is part of ARDS pathophysiology and selective vasodilation helps to improve blood flow and gas exchange in ARDS patients. Although oxygenation and pulmonary resistance are improved, evidence does not indicate better clinical outcomes (2). Extracorporeal Support An extracorporeal membrane oxygenator (ECMO) is a device used to provide respiratory support by circulating blood through an artificial lung, then returning the blood to the patient s circulatory system (11). ECMO uses a blood-gas interface for the diffusion of gas exchange. Extracorporeal support provides temporary improvement in those with severe ARDS, but does not seem to affect clinical outcomes (1). APPROPRIATE TOOLS IN NUTRITION ASSESSMENT Nutrition support is essential to meet energy requirements and maintain muscle strength.
8 An accurate assessment of needs is important in ALI/ARDS. Underfeeding can prevent unsuccessful ventilator weaning and increase susceptibility of infection, whereas overfeeding can lead to hypercapnea and delay ventilator weaning (3). Indirect calorimetry (IC) should be used to obtain initial needs assessment and repeated during length of stay. MNT Basic medical nutrition therapy goals are to meet basic nutritional requirements, preserve lean body mass, restore respiratory muscle mass and strength, maintain fluid balance, improve resistance to infection, and facilitate weaning from oxygen support and mechanical ventilation by providing energy substrates without exceeding the capacity of the respiratory system to clear CO2 (12). Nutritional implications of hypoxemic state as a result of ARDS condition include anorexia, early satiety, malaise, bloating, constipation and diarrhea. A person with respiratory failure can burn more calories breathing than a healthy person does. It is easy to lose weight without trying. Obesity and Underfeeding In obese patients, caloric restriction can reduce the hypercapnea and fluid retention that is seen in ARDS. Protein provision should be a priority as it promotes fat oxidation and prevents further muscle wasting. It is recommended to provide 60-70% of target or kcal/kg and g/kg of protein (3). Hypercapnea and Overfeeding Permissive hypercapnia from mechanical ventilator support has nutritional implications. Carbohydrates have high CO 2 production during metabolism. In order to achieve a respiratory quotient of ~.7, ARDS patients should consume a high fat diet. Overfeeding
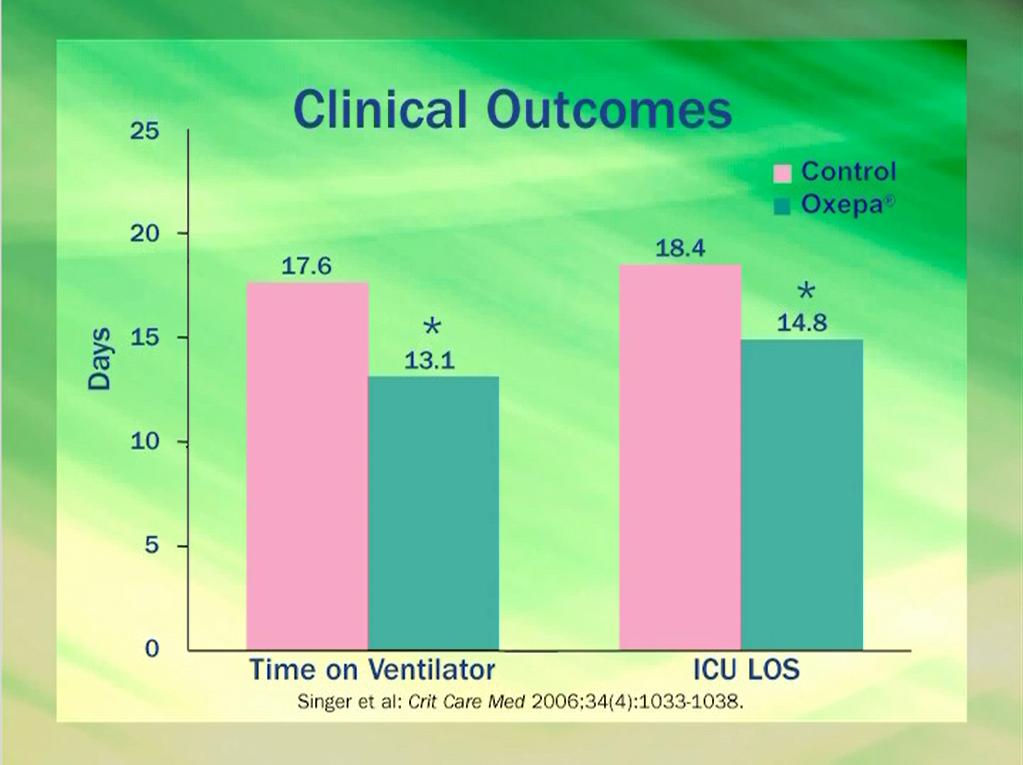
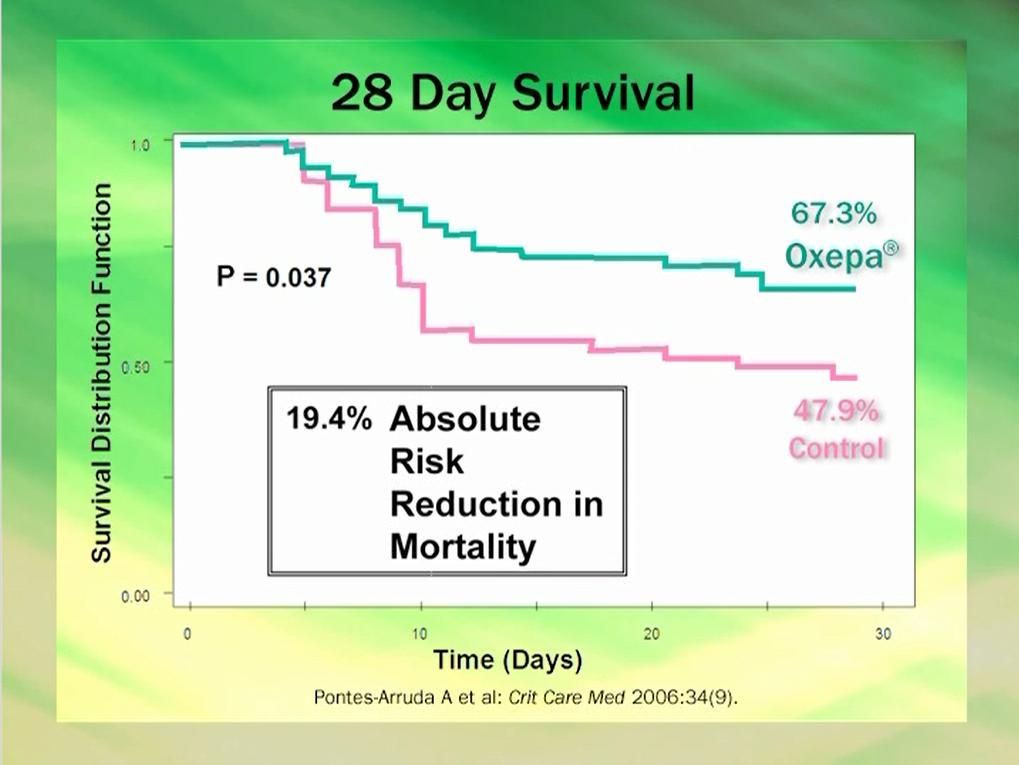
9 increases lipogenesis, increases glucose levels, leads to hepatic dysfunction and the inability to wean from the ventilator (3). Constant assessment of nutritional needs is important to prevent overfeeding. Oxepa Oxepa is the recommended formula for ARDS patients on nutrition support. Oxepa contains fatty acids, vitamins A, C, and E, and is volume reduced. Lipids reduce carbohydrate load and are increasingly used in immunonutrition. Oxepa decreases pulmonary inflammation and edema, facilitates pulmonary vasodilation, improves oxygenation, decreases time on a ventilator, reduces new organ failures, decreases ICU length and stay, lowers mortality rates, and is less expensive (13). Post ICU After weaning from ventilator support/en support it is important to eat a calorically dense diet including a variety of foods. Eating several small meals a day of favorite foods will help to consume necessary amount of calories without feeling uncomfortable. LONG TERM PROGNOSIS Several different pathways are involved in the development of ARDS, and there isn t a single biomarker that can predict the outcome of ARDS patients. Multiple Organ Dysfunction Syndrome (MODS) is the leading cause of death in ARDS (1). Post ICU patient survivors reported reduced physical function and quality of life despite normal or almost normal pulmonary function.
10 CONCLUSION ALI/ARDS continues to affect morbidity and mortality rates in critically ill patients. Treatment of the underlying cause of ARDS and as well as mechanical ventilation support can help to attenuate conditions of respiratory failure. Early nutrition support is critical to meet increased energy and protein needs related to hypoxemia and muscle wasting. Fluid management and proper MNT help to shorten time on ventilator support and reduce ICU length of stay.
11 REFERENCES (1) Pierrakos C, Karanikolas M, Scolletta S, Karamouzos V, Velissaris D. Acute respiratory distress syndrome: Pathophysiology and therapeutic options. J Clin Med Res. 2011;4(1):7-16. (2) Wheeler P, Bernard GR. Acute lung injury and the acute respiratory distress syndrome: A clinical review. Lancet. 2007;369: (3) Turner KL, Moore FA, Martindale R. Nutrition support for the acute lung injury/adult respiratory distress syndrome patine: A review. Nutr Clin Pract. 2011; 26(1): (4) Harmon EM, Pinsky MR. Acute respiratory distress syndrome. Available at Accessed March 6, (5) Ward HE, Nicholas TE. Alveolar type I and type II cells. Aust N Z J Med. 1984;14: (6) Hudson K. ARDS: Acute respiratory distress syndrome. Available at Accessed March 6, (7) Times Health Guide. Acute respiratory distress syndrome. Available at Accessed March 13, (8) The Acute Respiratory Distress Syndrome Network. Ventilation with lower tidal volumes as compared with traditional tidal volumes for acute lung injury and the acute respiratory distress syndrome. N Engl J Med. 2000;342: (9) McConville JF, Kress JP. Weaning patients from the ventilator. N Engl J Med. 2012;367: (10) Bloomfield R, Noble DW, Webster NR. Prone position for acute respiratory failure in adults. Cochrane Database of Systematic Reviews. 2009(4). (11) Leonard PC. Building a Medical Vocabulary. 8 th ed. St. Louis County, MO: Elsevier Inc; 2012 (12) Mahan KL, Escott-Stump S, Raymond JL. Krause s Food and the Nutrition Care Process. 13 th ed. St. Louis, MO: Elsevier Inc; (13) Oxepa: Advanced technology, advanced therapy. Therapeutic Nutrition for modulating inflammation in sepsis, ARDS, and ALI. Abbott Laboratories, Inc
12 Acute Respiratory Distress Syndrome (ARDS) BREANNA KELLER
13 ARDS ARDS: a life-threatening condition characterized by severe hypoxia, bilateral pulmonary fluid infiltration, and decreased lung compliance; usually occurring without prior lung disease but secondary to catastrophic illness
14 Etiology The most common underlying causes of ARDS include: Sepsis Inhalation of harmful substances Severe pneumonia Head or chest injury
15 Risk Factors Direct lung injury Pneumonia, gastric aspiration, drowning, fat and amnioticfluid embolism, pulmonary contusion, alveolar hemorrhage, smoke and toxic gas inhalation, reperfusion, and unilateral lung re-implantation Indirect lung injury Severe sepsis, transfusions, shock, narcotic overdose, and pancreatitis
16 Risk Factors Cont. Several risk factors appear to increase the risk of ARDS after an inciting event including: Advanced age Female sex (noted only in trauma cases) Cigarette smoking Alcohol use
17 Diagnosis There is no specific test to identify ARDS Diagnosis is reached by ruling out other diseases and conditions

18 ARDS Diagnosis
19 Imaging Bilateral pulmonary infiltrates detected Chest X-rays A chest X-ray can reveal which parts of the lungs have fluid in them and whether the heart is enlarged CT Scan A CT scan can provide detailed information about the structure within the heart and lungs
20 Lab Tests Blood testing Arterial blood gas, CBC to indicate low oxygen levels or hypoxemic conditions, and tests for possible infections Sputum cultures Collected and analyzed to determine type of lung infection
21 Heart Tests Signs and symptoms of ARDS are similar to cardiogenic pulmonary edema and other causes of hypoxemic respiratory failure An objective assessment meaning an echocardiogram should be preformed if there is no clear risk factor present like trauma or sepsis
22 Pathology SCIENTIFIC STUDY OF THE NATURE OF DISEASE AND ITS CAUSES, PROCESSES, DEVELOPMENT, AND CONSEQUENCES.
23

24 Histopathology Diffuse alveolar damage characterized by: Neutrophilic alveolar infiltrates Hemorrhage Protein-rich pulmonary edema
25 Acute Exudative Phase Cytokines (e.g. TNF, IL-I, IL-8) à inflammatory response Oxidative stress & protease activity Reduces surfactant activity, inactivates remaining surfactant à atelectasis Damage of structural framework Increased permeability exacerbates alveolar edema Capillary thrombosis
26 Fibroproliferative Phase Chronic inflammation Pulmonary fibrosis Neovascularization
27
28
29 Pathophysiology Inflammatory infiltrates, edema, atelectasis lead to: Ventilation-perfusion mismatch à hypoxemia Reduced lung compliance Hypoxemic vasoconstriction, capillary damage Increases pulmonary-artery pressures Sustained pressures à cor pulmonale
30 Pathophysiology Cont. Increased efforts of breathing Oxygen demands exceed respiratory capability à hypoxemic, hypercarbic respiratory failure
31 Treatment No specific treatment Supportive care Avoid iatrogenic complications Treat underlying cause Maintain adequate oxygenation Mechanical ventilation Reduces airway pressure
32 Supportive Care Treat underlying cause of ARDS Prevent deep vein thrombosis, GI bleeding, pressure ulcers Bed head raised 30 degrees Reduce risk of hospital-acquired pneumonia Enteral nutrition Glucose control
33

34 Mechanical Ventilation, Oxygen, PEEP Lung capacity affected by age, gender, height Mechanical ventilation used to relieve respiratory muscles of their work Usually tracheal-tubedelivered ventilation
35 Mechanical Ventilation, Oxygen, PEEP High tidal volume ventilation Over-distention and injury of compliant alveoli Exacerbate existing injury Local, systemic inflammation Positive-pressure ventilation Supplemental oxygen PEEP
36 Mechanical Ventilation, Oxygen, PEEP PEEP Pressure support in atelectic alveoli, increases functional residual capacity, improves oxygenation Could increase edema, over-distend compliant alveoli, worsen ventilation-perfusion matching, cause hypotension Pressure-limited mode of ventilation better than volume-cycled ventilation
37 Recommendations Pressure and volume-limited approach with permissive hypercapnia 6 ml/kg adjusted bodyweight tidal volume Lowest PEEP-F i O 2 that produces acceptable oxygenation 88%-95%
38 Weaning from ventilators Hemodynamically stable Spontaneous breaths <50% supplemental O 2, <8 cm H 2 O PEEP Modify inflammation, change mechanical properties of lungs No conclusive evidence
39 Treatment cont. Prone Positioning Corticosteroids Fluid management Diuretic use to reduce lung water Vasodilators Extracorporeal support
40
41 Extracorporeal Support (ECMO) Oxygenates and removes CO 2 from the blood Blood withdrawn into oxygenator, returned Blood-gas interface for diffusion of gases

42
43
44 Basic MNT Goals Meet basic nutritional requirements Preserve lean body mass Restore respiratory muscle mass and strength Maintain fluid balance Improve resistance to infection Facilitate weaning from oxygen support and mechanical ventilation by providing energy substrates without exceeding the capacity of the respiratory system to clear CO2
45 MNT Cont. Negative Nitrogen balance Protein (1.5-2 g/kg) Pulmonary rehabilitation programs Small portions Favorite foods Inadequate oxygen Anorexia Early satiety Malaise Bloating Constipation Diarrhea
46 Obesity and Underfeeding Underfeeding delays ventilator weaning Factors associated with obesity: Chest physiology Reduced functional reserve capacities Smaller lung volumes Hypercapnea Glucose resistance Mobilization of fat stores
47 Obesity and Underfeeding Protein provision Promotes endogenous fat oxidation Shifts from utilization of muscle stores Caloric restriction Improves glycemic control Reduces hypercapnea and fluid retention Endorse hypocaloric feeding for obese patient with goals of: 60-70% of target or kcal/g with g/kg of protein
48 Hypercapnia and Overfeeding Limit tidal volumes to prevent further inflammation and barotrauma Increases CO2 production Can lead to: Increased lipogenesis Increased glucose levels Hepatic dysfunction Inability to wean from the ventilator
49 Lipids in ARDS Anti-inflammatory lipid substrates Omega-3 fatty acids Fish oils (DHA and EPA) Resolvins Neuroprotectin
50 EN EN Always given when gut is functional Early EN ( within hours of arrival) Feed directly into small bowel Supplementation with vitamins A, C, E Phosphate
51 PN Shock Nonfunctional gut Peritonitis A marker for severity of disease
52 Pulmonary Inflammation

53 How Oxepa Works

54 Benefits of Oxepa
55
56

57 Cost of Care
 Adult 25 kcal/kg diet for")
58 Enteral Feedings in ARDS Oxepa for 60kg(132lb) Adult 25 kcal/kg diet for 24hrs.
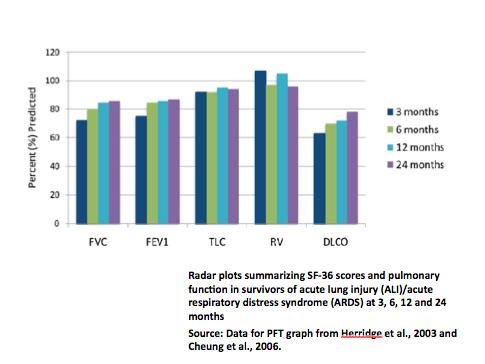
59 Quality of Life Health-related quality of life (HRQL) - a self-reported measure of one s own physical, mental, and social wellbeing Short Form-36 (SF-36) health survey - The most commonly used and best-validated tool to measure HRQL Nottingham Health Profile (NHP) - NHP gives more coverage to emotional reaction, pain, and physical mobility and unlike SF-36, NHP includes problems of sleep disturbance distance walked in 6 minutes with continuous oximetry (6MWD)
60 One-year post-icu in ARDS 104 patients 6MWD improved over first year post-icu All domains of SF-36 improved from 3 to 12 months and physical role and physical functioning domains showed greatest improvement when they were compared to general population at 1 year, all domains except emotional role were reduced
61
62
63
64 4 years and 5.5 years post-icu in ARDS 50 patients 54% survivors had normal lung function at 5.5 years Survivors had impairment of all domains SF-36 with 25% reduction physical functioning and physical role function
65 5 years post - ICU 81% Survived Only 86% of survivors available for follow-up at 5 years Also showed that both physical function and quality of life indices were reduced despite normal or almost normal pulmonary function.
66 Future Research Focus Strong relationship between the overall HRQL encountered at 1 month and at 6 months after ARDS, which indicates that identification of patients who will have a poor long-term quality of life is possible at an early time point Impaired HRQL has little to do with pulmonary function per se, as symptoms are a result of impaired recovery of strength, immobilization, critically illness polyneuropathy, and entrapment neuropathies Early intervention strategies to prevent or ameliorate physical morbidity may prove important for treating survivors of critical illness
67
68 Case Study Daishi Hayato 65yrs old male, lives with wife (62yrs old) My husband had emphysema for many years. He was working in the yard today and got really short of breath. I called our doctor, and she said to go straight to the emergency room.
69 Case Study Cont. Long- standing history of COPD due to tobacco use 2PPD for 50 yrs Dyspnea, swelling in lower extremiles, pneumothorax, intermiment claudicalon Meds: Combivent, Lasix,O2 via nasal cannula at night nutrilon Hx - AppeLte has been decreased for past several weeks.
70 Case Study Cont. Ht 5 4, Wt 122 lbs, UBW 135LBS HDL C 32mg/dL - low LDL 132 MG/dL - high
71 Case Study Cont. PES statement Increased nutrient needs related to long standing history of COPD and nutrient deprivation from Acute Respiratory Distress Syndrome as evidenced by decreased dietary intake and low body weight.
72 Acute Respiratory Distress Syndrome (ARDS) What is acute respiratory distress syndrome? Acute respiratory distress syndrome (ARDS) is the sudden failure of the respiratory system. It can occur in anyone over the age of one who is critically ill. ARDS can be life- threatening because normal gas exchange does not take place due to severe fluid buildup in both lungs. The condition is characterized by rapid breathing, difficulty getting enough air into the lungs and low blood oxygen levels. Who has ARDS? The incidence of ARDS has been difficult to determine partly because of the variety of causes, clinical manifestations and differing criteria used to define it. Various published estimates have ranged from 1.5 to 75 cases per 100,000 persons. In 2007, the National Heart, Lung and Blood Institute estimated that approximately 190,000 Americans are affected by ARDS annually. What is the health impact of ARDS? Lung function in most survivors of ARDS will return to normal or near normal within several months; however some will have lasting damage to their lungs or to areas outside the lungs. A study found that one year after discharge from the intensive care unit, ARDS survivors may still suffer side effects, mostly persistent muscle wasting and weakness. Quality of life in these survivors is compromised with poor mental and physical health outcomes. Food plan for ARDS Calorie intake to meet energy needs A person with respiratory failure can burn more calories breathing than a healthy person does. They find that they lose weight without trying. Therefore, it is important for the patient to eat a calorically dense diet including a variety of foods. Timing of meals Eating several small meals a day instead of two or three large ones can help you eat well and not feel uncomfortable. Try dividing your day s food into 4 to 6 small meals. You can eat a small breakfast, lunch, and dinner. Then get the rest of your nutritional needs for the day by eating two or three between-meal snacks.
Acute Respiratory Distress Syndrome
 Acute Respiratory Distress Syndrome ARDS Lung complication resulting in dangerously low blood oxygen ARDS is often a result of other health complications Clinical Manifestations Related to systemic inflammatory
Acute Respiratory Distress Syndrome ARDS Lung complication resulting in dangerously low blood oxygen ARDS is often a result of other health complications Clinical Manifestations Related to systemic inflammatory
MEDICAL NUTRITION THERAPY
 MEDICAL NUTRITION THERAPY Goals of Nutritional Care Meet basic nutrient requirements Preserve LBM Restore respiratory muscle mass and strength Maintain fluid balance Improve resistance to infection Facilitate
MEDICAL NUTRITION THERAPY Goals of Nutritional Care Meet basic nutrient requirements Preserve LBM Restore respiratory muscle mass and strength Maintain fluid balance Improve resistance to infection Facilitate
ACUTE RESPIRATORY DISTRESS SYNDROME
 ACUTE RESPIRATORY DISTRESS SYNDROME Angel Coz MD, FCCP, DCE Assistant Professor of Medicine UCSF Fresno November 4, 2017 No disclosures OBJECTIVES Identify current trends and risk factors of ARDS Describe
ACUTE RESPIRATORY DISTRESS SYNDROME Angel Coz MD, FCCP, DCE Assistant Professor of Medicine UCSF Fresno November 4, 2017 No disclosures OBJECTIVES Identify current trends and risk factors of ARDS Describe
7/4/2015. diffuse lung injury resulting in noncardiogenic pulmonary edema due to increase in capillary permeability
 Leanna R. Miller, RN, MN, CCRN-CMC, PCCN-CSC, CEN, CNRN, CMSRN, NP Education Specialist LRM Consulting Nashville, TN Objectives Identify the 5 criteria for the diagnosis of ARDS. Discuss the common etiologies
Leanna R. Miller, RN, MN, CCRN-CMC, PCCN-CSC, CEN, CNRN, CMSRN, NP Education Specialist LRM Consulting Nashville, TN Objectives Identify the 5 criteria for the diagnosis of ARDS. Discuss the common etiologies
ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) Rv
 Rv") ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) Rv.8.18.18 ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) SUDDEN PROGRESSIVE FORM OF ACUTE RESPIRATORY FAILURE ALVEOLAR CAPILLARY MEMBRANE BECOMES DAMAGED AND MORE
ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) Rv.8.18.18 ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) SUDDEN PROGRESSIVE FORM OF ACUTE RESPIRATORY FAILURE ALVEOLAR CAPILLARY MEMBRANE BECOMES DAMAGED AND MORE
Acute Respiratory Distress Syndrome (ARDS) An Update
 An Update") Acute Respiratory Distress Syndrome (ARDS) An Update Prof. A.S.M. Areef Ahsan FCPS(Medicine) MD(Critical Care Medicine) MD ( Chest) Head, Dept. of Critical Care Medicine BIRDEM General Hospital INTRODUCTION
Acute Respiratory Distress Syndrome (ARDS) An Update Prof. A.S.M. Areef Ahsan FCPS(Medicine) MD(Critical Care Medicine) MD ( Chest) Head, Dept. of Critical Care Medicine BIRDEM General Hospital INTRODUCTION
THE ACUTE RESPIRATORY DISTRESS SYNDROME. Daniel Brockman, DO
 THE ACUTE RESPIRATORY DISTRESS SYNDROME Daniel Brockman, DO Objectives Describe the history and evolution of the diagnosis of ARDS Review the diagnostic criteria for ARDS Discuss the primary interventions
THE ACUTE RESPIRATORY DISTRESS SYNDROME Daniel Brockman, DO Objectives Describe the history and evolution of the diagnosis of ARDS Review the diagnostic criteria for ARDS Discuss the primary interventions
Author: Thomas Sisson, MD, 2009
 Author: Thomas Sisson, MD, 2009 License: Unless otherwise noted, this material is made available under the terms of the Creative Commons Attribution Non-commercial Share Alike 3.0 License: http://creativecommons.org/licenses/by-nc-sa/3.0/
Author: Thomas Sisson, MD, 2009 License: Unless otherwise noted, this material is made available under the terms of the Creative Commons Attribution Non-commercial Share Alike 3.0 License: http://creativecommons.org/licenses/by-nc-sa/3.0/
Clinical syndrome of severe dyspnea of rapid onset, hypoxemia, and diffuse pulmonary infiltrates leading to respiratory failure.
 Yuanlin Song, M.D. Clinical syndrome of severe dyspnea of rapid onset, hypoxemia, and diffuse pulmonary infiltrates leading to respiratory failure. Pneumonia Trauma SARS PaO2/fiO2
Yuanlin Song, M.D. Clinical syndrome of severe dyspnea of rapid onset, hypoxemia, and diffuse pulmonary infiltrates leading to respiratory failure. Pneumonia Trauma SARS PaO2/fiO2
Breathing life into new therapies: Updates on treatment for severe respiratory failure. Whitney Gannon, MSN ACNP-BC
 Breathing life into new therapies: Updates on treatment for severe respiratory failure Whitney Gannon, MSN ACNP-BC Overview Definition of ARDS Clinical signs and symptoms Causes Pathophysiology Management
Breathing life into new therapies: Updates on treatment for severe respiratory failure Whitney Gannon, MSN ACNP-BC Overview Definition of ARDS Clinical signs and symptoms Causes Pathophysiology Management
ICU NUTRITION UPDATE : ESPEN GUIDELINES Mirey Karavetian Assistant Professor Zayed University
 ICU NUTRITION UPDATE : ESPEN GUIDELINES 2018 Mirey Karavetian Assistant Professor Zayed University http://www.espen.org/files/espen- Guidelines/ESPEN_Guideline_on_clinical_nutrition_in_-ICU.pdf Medical
ICU NUTRITION UPDATE : ESPEN GUIDELINES 2018 Mirey Karavetian Assistant Professor Zayed University http://www.espen.org/files/espen- Guidelines/ESPEN_Guideline_on_clinical_nutrition_in_-ICU.pdf Medical
Pulmonary Pathophysiology
 Pulmonary Pathophysiology 1 Reduction of Pulmonary Function 1. Inadequate blood flow to the lungs hypoperfusion 2. Inadequate air flow to the alveoli - hypoventilation 2 Signs and Symptoms of Pulmonary
Pulmonary Pathophysiology 1 Reduction of Pulmonary Function 1. Inadequate blood flow to the lungs hypoperfusion 2. Inadequate air flow to the alveoli - hypoventilation 2 Signs and Symptoms of Pulmonary
Steroids in ARDS: if, when, how much? John Fowler, MD, FACEP Dept. of Emergency Medicine Kent Hospital, İzmir, Türkiye
 Steroids in ARDS: if, when, how much? John Fowler, MD, FACEP Dept. of Emergency Medicine Kent Hospital, İzmir, Türkiye Steroids in ARDS: conclusion Give low-dose steroids if indicated for another problem
Steroids in ARDS: if, when, how much? John Fowler, MD, FACEP Dept. of Emergency Medicine Kent Hospital, İzmir, Türkiye Steroids in ARDS: conclusion Give low-dose steroids if indicated for another problem
RESPIRATORY COMPLICATIONS AFTER SCI
 SHEPHERD.ORG RESPIRATORY COMPLICATIONS AFTER SCI NORMA I RIVERA, RRT, RCP RESPIRATORY EDUCATOR SHEPHERD CENTER 2020 Peachtree Road, NW, Atlanta, GA 30309-1465 404-352-2020 DISCLOSURE STATEMENT I have no
SHEPHERD.ORG RESPIRATORY COMPLICATIONS AFTER SCI NORMA I RIVERA, RRT, RCP RESPIRATORY EDUCATOR SHEPHERD CENTER 2020 Peachtree Road, NW, Atlanta, GA 30309-1465 404-352-2020 DISCLOSURE STATEMENT I have no
Landmark articles on ventilation
 Landmark articles on ventilation Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity ARDS AECC DEFINITION-1994 ALI Acute onset Bilateral chest infiltrates PCWP
Landmark articles on ventilation Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity ARDS AECC DEFINITION-1994 ALI Acute onset Bilateral chest infiltrates PCWP
Index. Note: Page numbers of article titles are in boldface type
 Index Note: Page numbers of article titles are in boldface type A Acute coronary syndrome, perioperative oxygen in, 599 600 Acute lung injury (ALI). See Lung injury and Acute respiratory distress syndrome.
Index Note: Page numbers of article titles are in boldface type A Acute coronary syndrome, perioperative oxygen in, 599 600 Acute lung injury (ALI). See Lung injury and Acute respiratory distress syndrome.
DAILY SCREENING FORM
 DAILY SCREENING FORM Patient s initials: Date of admission: Time of admission: Gender: M F Year of Birth: Type of admission: Medical/Surgical/Postoperative (elective) Days Date Mechanical ventilation Lung
DAILY SCREENING FORM Patient s initials: Date of admission: Time of admission: Gender: M F Year of Birth: Type of admission: Medical/Surgical/Postoperative (elective) Days Date Mechanical ventilation Lung
ECMO for Severe Hypoxemic Respiratory Failure: Pro-Con Debate. Carolyn Calfee, MD MAS Mark Eisner, MD MPH
 ECMO for Severe Hypoxemic Respiratory Failure: Pro-Con Debate Carolyn Calfee, MD MAS Mark Eisner, MD MPH June 3, 2010 Case Presentation Setting: Community hospital, November 2009 29 year old woman with
ECMO for Severe Hypoxemic Respiratory Failure: Pro-Con Debate Carolyn Calfee, MD MAS Mark Eisner, MD MPH June 3, 2010 Case Presentation Setting: Community hospital, November 2009 29 year old woman with
ARDS: an update 6 th March A. Hakeem Al Hashim, MD, FRCP SQUH
 ARDS: an update 6 th March 2017 A. Hakeem Al Hashim, MD, FRCP SQUH 30M, previously healthy Hx: 1 week dry cough Gradually worsening SOB No travel Hx Case BP 130/70, HR 100/min ph 7.29 pco2 35 po2 50 HCO3
ARDS: an update 6 th March 2017 A. Hakeem Al Hashim, MD, FRCP SQUH 30M, previously healthy Hx: 1 week dry cough Gradually worsening SOB No travel Hx Case BP 130/70, HR 100/min ph 7.29 pco2 35 po2 50 HCO3
INTRODUCTION The effect of CPAP works on lung mechanics to improve oxygenation (PaO 2
 2 Effects of CPAP INTRODUCTION The effect of CPAP works on lung mechanics to improve oxygenation (PaO 2 ). The effect on CO 2 is only secondary to the primary process of improvement in lung volume and
2 Effects of CPAP INTRODUCTION The effect of CPAP works on lung mechanics to improve oxygenation (PaO 2 ). The effect on CO 2 is only secondary to the primary process of improvement in lung volume and
Recent Advances in Respiratory Medicine
 Recent Advances in Respiratory Medicine Dr. R KUMAR Pulmonologist Non Invasive Ventilation (NIV) NIV Noninvasive ventilation (NIV) refers to the administration of ventilatory support without using an invasive
Recent Advances in Respiratory Medicine Dr. R KUMAR Pulmonologist Non Invasive Ventilation (NIV) NIV Noninvasive ventilation (NIV) refers to the administration of ventilatory support without using an invasive
Acute Respiratory Failure. Respiratory Failure. Respiratory Failure. Acute Respiratory Failure. Ventilatory Failure. Type 1 Respiratory Failure
 Acute Respiratory Failure Physiologic Classification Acute Respiratory Failure Type 1 Hypoxemic Type 2 Ventilatory Type 3 Post-op Type 4 Shock Mechanism Shunt Va Atelectasis Cardiac Output Phil Factor,
Acute Respiratory Failure Physiologic Classification Acute Respiratory Failure Type 1 Hypoxemic Type 2 Ventilatory Type 3 Post-op Type 4 Shock Mechanism Shunt Va Atelectasis Cardiac Output Phil Factor,
Surviving Sepsis Campaign. Guidelines for Management of Severe Sepsis/Septic Shock. An Overview
 Surviving Sepsis Campaign Guidelines for Management of Severe Sepsis/Septic Shock An Overview Mechanical Ventilation of Sepsis-Induced ALI/ARDS ARDSnet Mechanical Ventilation Protocol Results: Mortality
Surviving Sepsis Campaign Guidelines for Management of Severe Sepsis/Septic Shock An Overview Mechanical Ventilation of Sepsis-Induced ALI/ARDS ARDSnet Mechanical Ventilation Protocol Results: Mortality
Oxygenation. Chapter 45. Re'eda Almashagba 1
 Oxygenation Chapter 45 Re'eda Almashagba 1 Respiratory Physiology Structure and function Breathing: inspiration, expiration Lung volumes and capacities Pulmonary circulation Respiratory gas exchange: oxygen,
Oxygenation Chapter 45 Re'eda Almashagba 1 Respiratory Physiology Structure and function Breathing: inspiration, expiration Lung volumes and capacities Pulmonary circulation Respiratory gas exchange: oxygen,
The new ARDS definitions: what does it mean?
 The new ARDS definitions: what does it mean? Richard Beale 7 th September 2012 METHODS ESICM convened an international panel of experts, with representation of ATS and SCCM The objectives were to update
The new ARDS definitions: what does it mean? Richard Beale 7 th September 2012 METHODS ESICM convened an international panel of experts, with representation of ATS and SCCM The objectives were to update
Chronic Obstructive Pulmonary Disease
 136 PHYSIOLOGY CASES AND PROBLEMS Case 24 Chronic Obstructive Pulmonary Disease Bernice Betweiler is a 73-year-old retired seamstress who has never been married. She worked in the alterations department
136 PHYSIOLOGY CASES AND PROBLEMS Case 24 Chronic Obstructive Pulmonary Disease Bernice Betweiler is a 73-year-old retired seamstress who has never been married. She worked in the alterations department
Objectives. Health care significance of ARF 9/10/15 TREATMENT OF ACUTE RESPIRATORY FAILURE OF VARIABLE CAUSES: INVASIVE VS. NON- INVASIVE VENTILATION
 TREATMENT OF ACUTE RESPIRATORY FAILURE OF VARIABLE CAUSES: INVASIVE VS. NON- INVASIVE VENTILATION Louisa Chika Ikpeama, DNP, CCRN, ACNP-BC Objectives Identify health care significance of acute respiratory
TREATMENT OF ACUTE RESPIRATORY FAILURE OF VARIABLE CAUSES: INVASIVE VS. NON- INVASIVE VENTILATION Louisa Chika Ikpeama, DNP, CCRN, ACNP-BC Objectives Identify health care significance of acute respiratory
Paramedic Rounds. Pre-Hospital Continuous Positive Airway Pressure (CPAP)
") Paramedic Rounds Pre-Hospital Continuous Positive Airway Pressure (CPAP) Morgan Hillier MD Class of 2011 Dr. Mike Peddle Assistant Medical Director SWORBHP Objectives Outline evidence for pre-hospital
Paramedic Rounds Pre-Hospital Continuous Positive Airway Pressure (CPAP) Morgan Hillier MD Class of 2011 Dr. Mike Peddle Assistant Medical Director SWORBHP Objectives Outline evidence for pre-hospital
Chronic Obstructive Pulmonary Disease (COPD) Copyright 2014 by Mosby, an imprint of Elsevier Inc.
 Copyright 2014 by Mosby, an imprint of Elsevier Inc.") Chronic Obstructive Pulmonary Disease () 8.18.18 Copyright 2014 by Mosby, an imprint of Elsevier Inc. Description Airflow limitation not fully reversible progressive Abnormal inflammatory response of lungs
Chronic Obstructive Pulmonary Disease () 8.18.18 Copyright 2014 by Mosby, an imprint of Elsevier Inc. Description Airflow limitation not fully reversible progressive Abnormal inflammatory response of lungs
NON-INVASIVE VENTILATION. Lijun Ding 23 Jan 2018
 NON-INVASIVE VENTILATION Lijun Ding 23 Jan 2018 Learning objectives What is NIV The difference between CPAP and BiPAP The indication of the use of NIV Complication of NIV application Patient monitoring
NON-INVASIVE VENTILATION Lijun Ding 23 Jan 2018 Learning objectives What is NIV The difference between CPAP and BiPAP The indication of the use of NIV Complication of NIV application Patient monitoring
Pulmonary & Extra-pulmonary ARDS: FIZZ or FUSS?
 Pulmonary & Extra-pulmonary ARDS: FIZZ or FUSS? Dr. Rajagopala Srinivas Senior Resident, Dept. Pulmonary Medicine, PGIMER, Chandigarh. The beginning.. "The etiology of this respiratory distress syndrome
Pulmonary & Extra-pulmonary ARDS: FIZZ or FUSS? Dr. Rajagopala Srinivas Senior Resident, Dept. Pulmonary Medicine, PGIMER, Chandigarh. The beginning.. "The etiology of this respiratory distress syndrome
Ron Hosp, MS-HSA, RRT Regional Respiratory Specialist. This program has been approved for 1 hour of continuing education credit.
 Ron Hosp, MS-HSA, RRT Regional Respiratory Specialist This program has been approved for 1 hour of continuing education credit. Course Objectives Identify at least four goals of home NIV Identify candidates
Ron Hosp, MS-HSA, RRT Regional Respiratory Specialist This program has been approved for 1 hour of continuing education credit. Course Objectives Identify at least four goals of home NIV Identify candidates
Wet Lungs Dry lungs Impact on Outcome in ARDS. Charlie Phillips MD Division of PCCM OHSU 2009
 Wet Lungs Dry lungs Impact on Outcome in ARDS Charlie Phillips MD Division of PCCM OHSU 2009 Today s talk Pathophysiology of ARDS The case for dry Targeting EVLW Disclosures Advisor for Pulsion Medical
Wet Lungs Dry lungs Impact on Outcome in ARDS Charlie Phillips MD Division of PCCM OHSU 2009 Today s talk Pathophysiology of ARDS The case for dry Targeting EVLW Disclosures Advisor for Pulsion Medical
Outcomes From Severe ARDS Managed Without ECMO. Roy Brower, MD Johns Hopkins University Critical Care Canada Forum Toronto November 1, 2016
 Outcomes From Severe ARDS Managed Without ECMO Roy Brower, MD Johns Hopkins University Critical Care Canada Forum Toronto November 1, 2016 Severe ARDS Berlin Definition 2012 P:F ratio 100 mm Hg Prevalence:
Outcomes From Severe ARDS Managed Without ECMO Roy Brower, MD Johns Hopkins University Critical Care Canada Forum Toronto November 1, 2016 Severe ARDS Berlin Definition 2012 P:F ratio 100 mm Hg Prevalence:
Management of refractory ARDS. Saurabh maji
 Management of refractory ARDS Saurabh maji Refractory hypoxemia as PaO2/FIO2 is less than 100 mm Hg, inability to keep plateau pressure below 30 cm H2O despite a VT of 4 ml/kg development of barotrauma
Management of refractory ARDS Saurabh maji Refractory hypoxemia as PaO2/FIO2 is less than 100 mm Hg, inability to keep plateau pressure below 30 cm H2O despite a VT of 4 ml/kg development of barotrauma
9/5/2018. Conflicts of Interests. Pediatric Acute Respiratory Distress Syndrome. Objectives ARDS ARDS. Definitions. None
 Pediatric Acute Respiratory Distress Syndrome Conflicts of Interests Diane C Lipscomb, MD Director Inpatient Pediatric Medical Director Mercy Springfield Associate Clerkship Clinical Director University
Pediatric Acute Respiratory Distress Syndrome Conflicts of Interests Diane C Lipscomb, MD Director Inpatient Pediatric Medical Director Mercy Springfield Associate Clerkship Clinical Director University
Ventilation in Paediatric ARDS: extrapolate from adult studies?
 Ventilation in Paediatric ARDS: extrapolate from adult studies? ASMIC 2014 Dr Adrian Plunkett Consultant Paediatric Intensivist Birmingham Children s Hospital, UK Aims of the presentation Ventilation
Ventilation in Paediatric ARDS: extrapolate from adult studies? ASMIC 2014 Dr Adrian Plunkett Consultant Paediatric Intensivist Birmingham Children s Hospital, UK Aims of the presentation Ventilation
EVALUATE DATA IN THE PATIENT RECORD
 EVALUATE DATA IN THE PATIENT RECORD Shawna Strickland, PhD, RRT-NPS, AE-C, FAARC Objectives At the end of this module, the learner will be able to identify the pertinent data from the patient chart for
EVALUATE DATA IN THE PATIENT RECORD Shawna Strickland, PhD, RRT-NPS, AE-C, FAARC Objectives At the end of this module, the learner will be able to identify the pertinent data from the patient chart for
The ARDS is characterized by increased permeability. Incidence of ARDS in an Adult Population of Northeast Ohio*
 Incidence of ARDS in an Adult Population of Northeast Ohio* Alejandro C. Arroliga, MD, FCCP; Ziad W. Ghamra, MD; Alejandro Perez Trepichio, MD; Patricia Perez Trepichio, RRT; John J. Komara Jr., BA, RRT;
Incidence of ARDS in an Adult Population of Northeast Ohio* Alejandro C. Arroliga, MD, FCCP; Ziad W. Ghamra, MD; Alejandro Perez Trepichio, MD; Patricia Perez Trepichio, RRT; John J. Komara Jr., BA, RRT;
Introduction and Overview of Acute Respiratory Failure
 Introduction and Overview of Acute Respiratory Failure Definition: Acute Respiratory Failure Failure to oxygenate Inadequate PaO 2 to saturate hemoglobin PaO 2 of 60 mm Hg ~ SaO 2 of 90% PaO 2 of 50 mm
Introduction and Overview of Acute Respiratory Failure Definition: Acute Respiratory Failure Failure to oxygenate Inadequate PaO 2 to saturate hemoglobin PaO 2 of 60 mm Hg ~ SaO 2 of 90% PaO 2 of 50 mm
What is the next best step?
 Noninvasive Ventilation William Janssen, M.D. Assistant Professor of Medicine National Jewish Health University of Colorado Denver Health Sciences Center What is the next best step? 65 year old female
Noninvasive Ventilation William Janssen, M.D. Assistant Professor of Medicine National Jewish Health University of Colorado Denver Health Sciences Center What is the next best step? 65 year old female
1. When a patient fails to ventilate or oxygenate adequately, the problem is caused by pathophysiological factors such as hyperventilation.
 Chapter 1: Principles of Mechanical Ventilation TRUE/FALSE 1. When a patient fails to ventilate or oxygenate adequately, the problem is caused by pathophysiological factors such as hyperventilation. F
Chapter 1: Principles of Mechanical Ventilation TRUE/FALSE 1. When a patient fails to ventilate or oxygenate adequately, the problem is caused by pathophysiological factors such as hyperventilation. F
Prepared by : Bayan Kaddourah RN,MHM. GICU Clinical Instructor
 Mechanical Ventilation Prepared by : Bayan Kaddourah RN,MHM. GICU Clinical Instructor 1 Definition Is a supportive therapy to facilitate gas exchange. Most ventilatory support requires an artificial airway.
Mechanical Ventilation Prepared by : Bayan Kaddourah RN,MHM. GICU Clinical Instructor 1 Definition Is a supportive therapy to facilitate gas exchange. Most ventilatory support requires an artificial airway.
An Overview of Bronchopulmonary Dysplasia and Chronic Lung Disease in Infancy
 An Overview of Bronchopulmonary Dysplasia and Chronic Lung Disease in Infancy Housekeeping: I have no financial disclosures Learning objectives: Develop an understanding of bronchopulmonary dysplasia (BPD)
An Overview of Bronchopulmonary Dysplasia and Chronic Lung Disease in Infancy Housekeeping: I have no financial disclosures Learning objectives: Develop an understanding of bronchopulmonary dysplasia (BPD)
Basic mechanisms disturbing lung function and gas exchange
 Basic mechanisms disturbing lung function and gas exchange Blagoi Marinov, MD, PhD Pathophysiology Department, Medical University of Plovdiv Respiratory system 1 Control of breathing Structure of the lungs
Basic mechanisms disturbing lung function and gas exchange Blagoi Marinov, MD, PhD Pathophysiology Department, Medical University of Plovdiv Respiratory system 1 Control of breathing Structure of the lungs
Fluid restriction is superior in acute lung injury and ARDS
 TAKE-HOME POINTS FROM LECTURES BY CLEVELAND CLINIC AND VISITING FACULTY MEDICAL GRAND ROUNDS CME CREDIT HERBERT P. WIEDEMANN, MD Chairman, Department of Pulmonary, Allergy, and Critical Care Medicine,
TAKE-HOME POINTS FROM LECTURES BY CLEVELAND CLINIC AND VISITING FACULTY MEDICAL GRAND ROUNDS CME CREDIT HERBERT P. WIEDEMANN, MD Chairman, Department of Pulmonary, Allergy, and Critical Care Medicine,
Acute Respiratory Distress Syndrome
 Colloquium series on Integrated Systems Physiology: from molecule to function to disease Series Editors: D. Neil Granger & Joey Granger Acute Respiratory Distress Syndrome Marie Carmelle Elie Donna Carden
Colloquium series on Integrated Systems Physiology: from molecule to function to disease Series Editors: D. Neil Granger & Joey Granger Acute Respiratory Distress Syndrome Marie Carmelle Elie Donna Carden
NON INVASIVE LIFE SAVERS. Non Invasive Ventilation (NIV)
") Table 1. NIV: Mechanisms Of Action Decreases work of breathing Increases functional residual capacity Recruits collapsed alveoli Improves respiratory gas exchange Reverses hypoventilation Maintains upper
Table 1. NIV: Mechanisms Of Action Decreases work of breathing Increases functional residual capacity Recruits collapsed alveoli Improves respiratory gas exchange Reverses hypoventilation Maintains upper
ARDS - a must know. Page 1 of 14
 ARDS - a must know Poster No.: C-1683 Congress: ECR 2016 Type: Authors: Keywords: DOI: Educational Exhibit M. Cristian; Turda/RO Education and training, Edema, Acute, Localisation, Education, Digital radiography,
ARDS - a must know Poster No.: C-1683 Congress: ECR 2016 Type: Authors: Keywords: DOI: Educational Exhibit M. Cristian; Turda/RO Education and training, Edema, Acute, Localisation, Education, Digital radiography,
ARDS and Ventilators PG26 Update in Surgical Critical Care October 9, 2013
 ARDS and Ventilators PG26 Update in Surgical Critical Care October 9, 2013 Pauline K. Park MD, FACS, FCCM University of Michigan School of Medicine Ann Arbor, MI OVERVIEW New Berlin definition of ARDS
ARDS and Ventilators PG26 Update in Surgical Critical Care October 9, 2013 Pauline K. Park MD, FACS, FCCM University of Michigan School of Medicine Ann Arbor, MI OVERVIEW New Berlin definition of ARDS
Case discussion Acute severe asthma during pregnancy. J.G. van der Hoeven
 Case discussion Acute severe asthma during pregnancy J.G. van der Hoeven Case (1) 32-year-old female - gravida 3 - para 2 Previous medical history - asthma Pregnant (33 w) Acute onset fever with wheezing
Case discussion Acute severe asthma during pregnancy J.G. van der Hoeven Case (1) 32-year-old female - gravida 3 - para 2 Previous medical history - asthma Pregnant (33 w) Acute onset fever with wheezing
New Strategies in the Management of Patients with Severe Sepsis
 New Strategies in the Management of Patients with Severe Sepsis Michael Zgoda, MD, MBA President, Medical Staff Medical Director, ICU CMC-University, Charlotte, NC Factors of increases in the dx. of severe
New Strategies in the Management of Patients with Severe Sepsis Michael Zgoda, MD, MBA President, Medical Staff Medical Director, ICU CMC-University, Charlotte, NC Factors of increases in the dx. of severe
Competency Title: Continuous Positive Airway Pressure
 Competency Title: Continuous Positive Airway Pressure Trainee Name: ------------------------------------------------------------- Title: ---------------------------------------------------------------
Competency Title: Continuous Positive Airway Pressure Trainee Name: ------------------------------------------------------------- Title: ---------------------------------------------------------------
Lecture Notes. Chapter 9: Smoke Inhalation Injury and Burns
 Lecture Notes Chapter 9: Smoke Inhalation Injury and Burns Objectives List the factors that influence mortality rate Describe the nature of smoke inhalation and the fire environment Recognize the pulmonary
Lecture Notes Chapter 9: Smoke Inhalation Injury and Burns Objectives List the factors that influence mortality rate Describe the nature of smoke inhalation and the fire environment Recognize the pulmonary
Hyaline membrane disease. By : Dr. Ch Sarishma Peadiatric Pg
 Hyaline membrane disease By : Dr. Ch Sarishma Peadiatric Pg Also called Respiratory distress syndrome. It occurs primarily in premature infants; its incidence is inversely related to gestational age and
Hyaline membrane disease By : Dr. Ch Sarishma Peadiatric Pg Also called Respiratory distress syndrome. It occurs primarily in premature infants; its incidence is inversely related to gestational age and
Restrictive Pulmonary Diseases
 Restrictive Pulmonary Diseases Causes: Acute alveolo-capillary sysfunction Interstitial disease Pleural disorders Chest wall disorders Neuromuscular disease Resistance Pathophysiology Reduced compliance
Restrictive Pulmonary Diseases Causes: Acute alveolo-capillary sysfunction Interstitial disease Pleural disorders Chest wall disorders Neuromuscular disease Resistance Pathophysiology Reduced compliance
PATHOPHYSIOLOGICAL PROCESS TEMPLATE
 1 PATHOPHYSIOLOGICAL PROCESS TEMPLATE DISEASE: Chronic obstructive pulmonary disease (COPD) DEFINITION: COPD can be defined as a disease in which there is a significant damage to the lungs thus reducing
1 PATHOPHYSIOLOGICAL PROCESS TEMPLATE DISEASE: Chronic obstructive pulmonary disease (COPD) DEFINITION: COPD can be defined as a disease in which there is a significant damage to the lungs thus reducing
Lecture Notes. Chapter 4: Chronic Obstructive Pulmonary Disease (COPD)
") Lecture Notes Chapter 4: Chronic Obstructive Pulmonary Disease (COPD) Objectives Define COPD Estimate incidence of COPD in the US Define factors associated with onset of COPD Describe the clinical features
Lecture Notes Chapter 4: Chronic Obstructive Pulmonary Disease (COPD) Objectives Define COPD Estimate incidence of COPD in the US Define factors associated with onset of COPD Describe the clinical features
RESPIRATORY FAILURE. Dr Graeme McCauley KGH
 RESPIRATORY FAILURE Dr Graeme McCauley KGH Definitions Failure to oxygenate-pao2 < 60 Failure to clear CO2-PaCO2 > 50 Acute vs Chronic Hypoxemic failure- type l Hypercapneic failure- type ll Causes of
RESPIRATORY FAILURE Dr Graeme McCauley KGH Definitions Failure to oxygenate-pao2 < 60 Failure to clear CO2-PaCO2 > 50 Acute vs Chronic Hypoxemic failure- type l Hypercapneic failure- type ll Causes of
Acute Respiratory Distress Syndrome. By Sydney Hunter. March 6, 2014 NDFS 356
 Acute Respiratory Distress Syndrome By Sydney Hunter March 6, 2014 NDFS 356 1 Introduction The onset of acute respiratory distress syndrome occurs as a result of previous trauma, stress, or shock. It can
Acute Respiratory Distress Syndrome By Sydney Hunter March 6, 2014 NDFS 356 1 Introduction The onset of acute respiratory distress syndrome occurs as a result of previous trauma, stress, or shock. It can
Case Study BMIs in the range of are considered overweight. Therefore, F.V. s usual BMI indicates that she was overweight.
 Morgan McFarlane February 26 th, 2013 HHP 439 Professor White Case Study 7.10 1. What is your interpretation of F.V. s clinical data? F.V. s clinical data includes chronic abdominal pain, loose stools,
Morgan McFarlane February 26 th, 2013 HHP 439 Professor White Case Study 7.10 1. What is your interpretation of F.V. s clinical data? F.V. s clinical data includes chronic abdominal pain, loose stools,
The use of proning in the management of Acute Respiratory Distress Syndrome
 Case 3 The use of proning in the management of Acute Respiratory Distress Syndrome Clinical Problem This expanded case summary has been chosen to explore the rationale and evidence behind the use of proning
Case 3 The use of proning in the management of Acute Respiratory Distress Syndrome Clinical Problem This expanded case summary has been chosen to explore the rationale and evidence behind the use of proning
Cor pulmonale. Dr hamid reza javadi
 1 Cor pulmonale Dr hamid reza javadi 2 Definition Cor pulmonale ;pulmonary heart disease; is defined as dilation and hypertrophy of the right ventricle (RV) in response to diseases of the pulmonary vasculature
1 Cor pulmonale Dr hamid reza javadi 2 Definition Cor pulmonale ;pulmonary heart disease; is defined as dilation and hypertrophy of the right ventricle (RV) in response to diseases of the pulmonary vasculature
Nutrition and Sepsis
 Nutrition and Sepsis Todd W. Rice, MD, MSc Associate Professor of Medicine Vanderbilt University 2017 DNS Symposium June 2, 2017 Case 55 y.o. male COPD, DM, HTN, presents with pneumonia and septic shock.
Nutrition and Sepsis Todd W. Rice, MD, MSc Associate Professor of Medicine Vanderbilt University 2017 DNS Symposium June 2, 2017 Case 55 y.o. male COPD, DM, HTN, presents with pneumonia and septic shock.
ARDS A Brief Overview. Lucas Pitts, M.D. Assistant Professor of Medicine Pulmonary and Critical Care Medicine University of Kansas School of Medicine
 ARDS A Brief Overview Lucas Pitts, M.D. Assistant Professor of Medicine Pulmonary and Critical Care Medicine University of Kansas School of Medicine Outline Definition of ARDS Epidemiology of ARDS Pathophysiology
ARDS A Brief Overview Lucas Pitts, M.D. Assistant Professor of Medicine Pulmonary and Critical Care Medicine University of Kansas School of Medicine Outline Definition of ARDS Epidemiology of ARDS Pathophysiology
Restrictive lung diseases
 Restrictive lung diseases Restrictive lung diseases are diseases that affect the interstitium of the lung. Interstitium of the lung is the very thin walls surrounding the alveoli, it s formed of epithelium
Restrictive lung diseases Restrictive lung diseases are diseases that affect the interstitium of the lung. Interstitium of the lung is the very thin walls surrounding the alveoli, it s formed of epithelium
Oklahoma Dietetic Association. Ainsley Malone, MS, RD, LD, CNSD April, 16, 2008 Permissive Underfeeding: What, Where and Why? Mt.
 The What, Why and When of Permissive Ainsley Malone, MS, RD, CNSD Nutrition Support Team Mt. Carmel West Hospital Mt. Carmel West 500 bed academic center Non-physician based NST Dietitian, pharmacist and
The What, Why and When of Permissive Ainsley Malone, MS, RD, CNSD Nutrition Support Team Mt. Carmel West Hospital Mt. Carmel West 500 bed academic center Non-physician based NST Dietitian, pharmacist and
Veno-Venous ECMO Support. Chris Cropsey, MD Sept. 21, 2015
 Veno-Venous ECMO Support Chris Cropsey, MD Sept. 21, 2015 Objectives List indications and contraindications for ECMO Describe hemodynamics and oxygenation on ECMO Discuss evidence for ECMO outcomes Identify
Veno-Venous ECMO Support Chris Cropsey, MD Sept. 21, 2015 Objectives List indications and contraindications for ECMO Describe hemodynamics and oxygenation on ECMO Discuss evidence for ECMO outcomes Identify
Steroids for ARDS. Clinical Problem. Management
 Steroids for ARDS James Beck Clinical Problem A 60 year old lady re-presented to ICU with respiratory failure. She had previously been admitted for fluid management and electrolyte correction having presented
Steroids for ARDS James Beck Clinical Problem A 60 year old lady re-presented to ICU with respiratory failure. She had previously been admitted for fluid management and electrolyte correction having presented
DISEASES OF THE RESPIRATORY SYSTEM 2017 DR HEYAM AWAD LECTURE 1: RESPIRATORY DISTRESS SYNDROMES
 DISEASES OF THE RESPIRATORY SYSTEM 2017 DR HEYAM AWAD LECTURE 1: RESPIRATORY DISTRESS SYNDROMES This lecture covers two topics: neonatal respiratory distress syndrome (neonatal RDS) and adult respiratory
DISEASES OF THE RESPIRATORY SYSTEM 2017 DR HEYAM AWAD LECTURE 1: RESPIRATORY DISTRESS SYNDROMES This lecture covers two topics: neonatal respiratory distress syndrome (neonatal RDS) and adult respiratory
Handling Common Problems & Pitfalls During. Oxygen desaturation in patients receiving mechanical ventilation ACUTE SEVERE RESPIRATORY FAILURE
 Handling Common Problems & Pitfalls During ACUTE SEVERE RESPIRATORY FAILURE Pravit Jetanachai, MD QSNICH Oxygen desaturation in patients receiving mechanical ventilation Causes of oxygen desaturation 1.
Handling Common Problems & Pitfalls During ACUTE SEVERE RESPIRATORY FAILURE Pravit Jetanachai, MD QSNICH Oxygen desaturation in patients receiving mechanical ventilation Causes of oxygen desaturation 1.
Lecture Notes. Chapter 2: Introduction to Respiratory Failure
 Lecture Notes Chapter 2: Introduction to Respiratory Failure Objectives Define respiratory failure, ventilatory failure, and oxygenation failure List the causes of respiratory failure Describe the effects
Lecture Notes Chapter 2: Introduction to Respiratory Failure Objectives Define respiratory failure, ventilatory failure, and oxygenation failure List the causes of respiratory failure Describe the effects
ENTERAL NUTRITION IN THE CRITICALLY ILL
 ENTERAL NUTRITION IN THE CRITICALLY ILL 1 Ebb phase Flow phase acute response (catabolic) adoptive response (anabolic) 2 3 Metabolic Response to Stress (catabolic phase) Glucose and Protein Metabolism
ENTERAL NUTRITION IN THE CRITICALLY ILL 1 Ebb phase Flow phase acute response (catabolic) adoptive response (anabolic) 2 3 Metabolic Response to Stress (catabolic phase) Glucose and Protein Metabolism
Questions 1-3 refer to the following diagram. Indicate the plane labeled by the corresponding question number.
 Name: Grade: ANATOMY TEST Questions 1-3 refer to the following diagram. Indicate the plane labeled by the corresponding question number. 1. Plane #1 is the... 2. Plane #2 is the... 3. Plane #3 is the...
Name: Grade: ANATOMY TEST Questions 1-3 refer to the following diagram. Indicate the plane labeled by the corresponding question number. 1. Plane #1 is the... 2. Plane #2 is the... 3. Plane #3 is the...
Non-invasive Positive Pressure Mechanical Ventilation: NIPPV: CPAP BPAP IPAP EPAP. My Real Goals. What s new in 2018? OMG PAP?
 Non-invasive Positive Pressure Mechanical Ventilation: What s new in 2018? Geoffrey R. Connors, MD, FACP Associate Professor of Medicine University of Colorado School of Medicine Division of Pulmonary
Non-invasive Positive Pressure Mechanical Ventilation: What s new in 2018? Geoffrey R. Connors, MD, FACP Associate Professor of Medicine University of Colorado School of Medicine Division of Pulmonary
Disclosures. None. Enteral Nutrition and Vasoactive Therapy! But actually.. Stocks Advisory boards Grants Speakers Bureau. Paul Marik, MD,FCCM,FCCP
 Enteral Nutrition and Vasoactive Therapy! Paul Marik, MD,FCCM,FCCP Disclosures Stocks Advisory boards Grants Speakers Bureau None But actually.. 1 We suggest a determination of nutrition risk (NUTRIC score)
Enteral Nutrition and Vasoactive Therapy! Paul Marik, MD,FCCM,FCCP Disclosures Stocks Advisory boards Grants Speakers Bureau None But actually.. 1 We suggest a determination of nutrition risk (NUTRIC score)
Acute respiratory distress syndrome
 20 Acute respiratory distress syndrome Introduction i Key points Acute respiratory distress syndrome is triggered by injury to the alveolar capillary barrier from any of a variety of causes, resulting
20 Acute respiratory distress syndrome Introduction i Key points Acute respiratory distress syndrome is triggered by injury to the alveolar capillary barrier from any of a variety of causes, resulting
RESPIRATORY PHYSIOLOGY Pre-Lab Guide
 RESPIRATORY PHYSIOLOGY Pre-Lab Guide NOTE: A very useful Study Guide! This Pre-lab guide takes you through the important concepts that where discussed in the lab videos. There will be some conceptual questions
RESPIRATORY PHYSIOLOGY Pre-Lab Guide NOTE: A very useful Study Guide! This Pre-lab guide takes you through the important concepts that where discussed in the lab videos. There will be some conceptual questions
INDICATIONS FOR RESPIRATORY ASSISTANCE A C U T E M E D I C I N E U N I T P - Y E A R M B B S 4
 INDICATIONS FOR RESPIRATORY ASSISTANCE A C U T E M E D I C I N E U N I T P - Y E A R M B B S 4 RESPIRATORY FAILURE Acute respiratory failure is defined by hypoxemia with or without hypercapnia. It is one
INDICATIONS FOR RESPIRATORY ASSISTANCE A C U T E M E D I C I N E U N I T P - Y E A R M B B S 4 RESPIRATORY FAILURE Acute respiratory failure is defined by hypoxemia with or without hypercapnia. It is one
Respiratory Failure. Causes of Acute Respiratory Failure (ARF): a- Intrapulmonary:
: a- Intrapulmonary:") Respiratory failure exists whenever the exchange of O 2 for CO 2 in the lungs cannot keep up with the rate of O 2 consumption & CO 2 production in the cells of the body. This results in a fall in arterial
Respiratory failure exists whenever the exchange of O 2 for CO 2 in the lungs cannot keep up with the rate of O 2 consumption & CO 2 production in the cells of the body. This results in a fall in arterial
Replacement of air with fluid, inflammatory. cells or cellular debris. Parenchymal, Interstitial (Restrictive) and Vascular Diseases.
 and Vascular Diseases.") Parenchymal, Interstitial (Restrictive) and Vascular Diseases Alain C. Borczuk, M.D. Dept of Pathology Replacement of air with fluid, inflammatory cells Pulmonary Edema Pneumonia Hemorrhage Diffuse alveolar
Parenchymal, Interstitial (Restrictive) and Vascular Diseases Alain C. Borczuk, M.D. Dept of Pathology Replacement of air with fluid, inflammatory cells Pulmonary Edema Pneumonia Hemorrhage Diffuse alveolar
ARDS and Lung Protection
 ARDS and Lung Protection Kristina Sullivan, MD Associate Professor University of California, San Francisco Department of Anesthesia and Perioperative Care Division of Critical Care Medicine Overview Low
ARDS and Lung Protection Kristina Sullivan, MD Associate Professor University of California, San Francisco Department of Anesthesia and Perioperative Care Division of Critical Care Medicine Overview Low
Bronchoalveolar lavage (BAL) with surfactant in pediatric ARDS
 with surfactant in pediatric ARDS") Bronchoalveolar lavage (BAL) with surfactant in pediatric ARDS M. Luchetti, E. M. Galassini, A. Galbiati, C. Pagani,, F. Silla and G. A. Marraro gmarraro@picu.it www.picu.it Anesthesia and Intensive Care
Bronchoalveolar lavage (BAL) with surfactant in pediatric ARDS M. Luchetti, E. M. Galassini, A. Galbiati, C. Pagani,, F. Silla and G. A. Marraro gmarraro@picu.it www.picu.it Anesthesia and Intensive Care
ARDS: MANAGEMENT UPDATE
 ARDS: MANAGEMENT UPDATE Tanıl Kendirli, Assoc. Prof. Ankara University School of Medicine, Pediatric Critical Care Medicine The AECC Definition Timing Acute onset, within 48-72 hours Oxygenation ALI PaO2/FiO2
ARDS: MANAGEMENT UPDATE Tanıl Kendirli, Assoc. Prof. Ankara University School of Medicine, Pediatric Critical Care Medicine The AECC Definition Timing Acute onset, within 48-72 hours Oxygenation ALI PaO2/FiO2
Charisma High-flow CPAP solution
 Charisma High-flow CPAP solution Homecare PNEUMOLOGY Neonatology Anaesthesia INTENSIVE CARE VENTILATION Sleep Diagnostics Service Patient Support charisma High-flow CPAP solution Evidence CPAP therapy
Charisma High-flow CPAP solution Homecare PNEUMOLOGY Neonatology Anaesthesia INTENSIVE CARE VENTILATION Sleep Diagnostics Service Patient Support charisma High-flow CPAP solution Evidence CPAP therapy
Test Bank Pilbeam's Mechanical Ventilation Physiological and Clinical Applications 6th Edition Cairo
 Instant dowload and all chapters Test Bank Pilbeam's Mechanical Ventilation Physiological and Clinical Applications 6th Edition Cairo https://testbanklab.com/download/test-bank-pilbeams-mechanical-ventilation-physiologicalclinical-applications-6th-edition-cairo/
Instant dowload and all chapters Test Bank Pilbeam's Mechanical Ventilation Physiological and Clinical Applications 6th Edition Cairo https://testbanklab.com/download/test-bank-pilbeams-mechanical-ventilation-physiologicalclinical-applications-6th-edition-cairo/
NIV use in ED. Dr. Khalfan AL Amrani Emergency Resuscitation Symposium 2 nd May 2016 SQUH
 NIV use in ED Dr. Khalfan AL Amrani Emergency Resuscitation Symposium 2 nd May 2016 SQUH Outline History & Introduction Overview of NIV application Review of proven uses of NIV History of Ventilation 1940
NIV use in ED Dr. Khalfan AL Amrani Emergency Resuscitation Symposium 2 nd May 2016 SQUH Outline History & Introduction Overview of NIV application Review of proven uses of NIV History of Ventilation 1940
Adult Respiratory Distress Syndrome
 Critical Care Medicine Adult Respiratory Distress Syndrome Leonard J. Sonne, MD, FACP, FCCP* *Chief, Division of Pulmonary Physiology and Medicine, Department of Medicine, King Faisal Specialist Hospital
Critical Care Medicine Adult Respiratory Distress Syndrome Leonard J. Sonne, MD, FACP, FCCP* *Chief, Division of Pulmonary Physiology and Medicine, Department of Medicine, King Faisal Specialist Hospital
Critical Care in Obstetrics: An Innovative and Integrated Model for Learning the Essentials
 Critical Care in Obstetrics: An Innovative and Integrated Model for Learning the Essentials Respiratory Distress Syndrome and Pulmonary Edema Sonya S. Abdel-Razeq, MD Maternal-Fetal Medicine Surgical Critical
Critical Care in Obstetrics: An Innovative and Integrated Model for Learning the Essentials Respiratory Distress Syndrome and Pulmonary Edema Sonya S. Abdel-Razeq, MD Maternal-Fetal Medicine Surgical Critical
HYPEREMIA AND CONGESTION
 HYPEREMIA AND CONGESTION Learning Objectives Define congestion and hyperemia Differentiate between the two with regard to: Mechanisms / underlying causes Appearance (gross and histologic) Effects Differentiate
HYPEREMIA AND CONGESTION Learning Objectives Define congestion and hyperemia Differentiate between the two with regard to: Mechanisms / underlying causes Appearance (gross and histologic) Effects Differentiate
2
 1 2 Although the term "cardiomyopathy" could theoretically apply to almost any disease affecting the heart, it is usually reserved for "severe myocardial disease leading to heart failure".cardiomyopathy
1 2 Although the term "cardiomyopathy" could theoretically apply to almost any disease affecting the heart, it is usually reserved for "severe myocardial disease leading to heart failure".cardiomyopathy
SESSION IV: MECHANISMS OF HUMAN DISEASE: LABORATORY SESSIONS PULMONARY PATHOLOGY I. December 5, 2012
 SESSION IV: MECHANISMS OF HUMAN DISEASE: LABORATORY SESSIONS PULMONARY PATHOLOGY I December 5, 2012 FACULTY COPY GOAL: Describe the basic morphologic and pathophysiologic changes in various conditions
SESSION IV: MECHANISMS OF HUMAN DISEASE: LABORATORY SESSIONS PULMONARY PATHOLOGY I December 5, 2012 FACULTY COPY GOAL: Describe the basic morphologic and pathophysiologic changes in various conditions
2/4/2019. GOLD Objectives. GOLD 2019 Report: Chapters
 GOLD Objectives To provide a non biased review of the current evidence for the assessment, diagnosis and treatment of patients with COPD. To highlight short term and long term treatment objectives organized
GOLD Objectives To provide a non biased review of the current evidence for the assessment, diagnosis and treatment of patients with COPD. To highlight short term and long term treatment objectives organized
Respiratory Disease. Dr Amal Damrah consultant Neonatologist and Paediatrician
 Respiratory Disease Dr Amal Damrah consultant Neonatologist and Paediatrician Signs and Symptoms of Respiratory Diseases Cardinal Symptoms Cough Sputum Hemoptysis Dyspnea Wheezes Chest pain Signs and Symptoms
Respiratory Disease Dr Amal Damrah consultant Neonatologist and Paediatrician Signs and Symptoms of Respiratory Diseases Cardinal Symptoms Cough Sputum Hemoptysis Dyspnea Wheezes Chest pain Signs and Symptoms
Respiratory Diseases and Disorders
 Chapter 9 Respiratory Diseases and Disorders Anatomy and Physiology Chest, lungs, and conducting airways Two parts: Upper respiratory system consists of nose, mouth, sinuses, pharynx, and larynx Lower
Chapter 9 Respiratory Diseases and Disorders Anatomy and Physiology Chest, lungs, and conducting airways Two parts: Upper respiratory system consists of nose, mouth, sinuses, pharynx, and larynx Lower
Course Handouts & Disclosure
 COPD: Disease Trajectory and Hospice Eligibility Terri L. Maxwell PhD, APRN VP, Strategic Initiatives Weatherbee Resources Hospice Education Network Course Handouts & Disclosure To download presentation
COPD: Disease Trajectory and Hospice Eligibility Terri L. Maxwell PhD, APRN VP, Strategic Initiatives Weatherbee Resources Hospice Education Network Course Handouts & Disclosure To download presentation
Case Study #2. Case Study #1 cont 9/28/2011. CAPA 2011 Christy Wilson PA C. LH is 78 yowf with PMHx of metz breast CA presents
 Case Study #1 CAPA 2011 Christy Wilson PA C 46 yo female presents with community acquired PNA (CAP). Her condition worsened and she was transferred to the ICU and placed on mechanical ventilation. Describe
Case Study #1 CAPA 2011 Christy Wilson PA C 46 yo female presents with community acquired PNA (CAP). Her condition worsened and she was transferred to the ICU and placed on mechanical ventilation. Describe
Biochemistry of Lungs. Lecture # 35 Lecturer: Alexander Koval
 Biochemistry of Lungs Lecture # 35 Lecturer: Alexander Koval Introduction Biochemistry of lungs Overview of substances produced (surfactant, mucus, collagen), inactivated (ROS, kinins, serotonin, catecholamines)
Biochemistry of Lungs Lecture # 35 Lecturer: Alexander Koval Introduction Biochemistry of lungs Overview of substances produced (surfactant, mucus, collagen), inactivated (ROS, kinins, serotonin, catecholamines)
APRV Ventilation Mode
 APRV Ventilation Mode Airway Pressure Release Ventilation A Type of CPAP Continuous Positive Airway Pressure (CPAP) with an intermittent release phase. Patient cycles between two levels of CPAP higher
APRV Ventilation Mode Airway Pressure Release Ventilation A Type of CPAP Continuous Positive Airway Pressure (CPAP) with an intermittent release phase. Patient cycles between two levels of CPAP higher