Υπέρταση στις γυναίκες
|
|
|
- Joel Copeland
- 5 years ago
- Views:
Transcription
1 Υπέρταση στις γυναίκες Ελένη Τριανταφυλλίδη Διευθύντρια ΕΣΥ Καρδιολογίας Υπεύθυνη Αντιυπερτασικού Ιατρείου Β Πανεπιστημιακή Καρδιολογική Κλινική Νοσοκομείο ΑΤΤΙΚΟΝ
2 Cardiovascular disease is the Europe s No. 1 killer Main cause of disease More than 4.3 million deaths/year 48% of all deaths Coronary heart disease most common cause of death in Europe (1.9 million deaths/year) Stroke more than 500,000 deaths/year Cost to EU estimated at 192 billion/year Allender et al. European Heart Network 2008

3 54% of strokes and 47% of IHD attributable to untreated hypertension
4 Blood Pressure and CAD/Stroke Mortality

5 Heart: Aortic Aneurysms Atrial fibrillation Arteries: Peripheral artery disease Sexual dysfunction

6

7 Εκτίμηση καρδιαγγειακού κινδύνου
8
9 Compliance with antihypertensive therapy Compliance equal to 25-85% depending on series with a 53% as a mean value Risk factors for non-compliance: 1. young age 5. cost for medications 2. female sex 6. drug class-side effects 3. single persons 7. lack of symptoms 4. comorbidities 8. ineffective consultation

10 During early adulthood mean systolic BP is higher in men than women, but the subsequent rate of rise in BP is steeper for women than men. Prevalence and severity of hypertension increase markedly with advancing age in women, such that a higher percentage of women than men have high BP after 65 years

11 Aging of world population by a n d l o n g e r l i f e expectancies in women than in men are possibly related to the greater increases in the prevalence of hypertension among women.
12 Data from the Framingham Heart Study showed gender differences in BP control rates and in the pattern of antihypertensive medications prescribed. An age-related decrease in BP control rates were more pronounced in women than in men. Among the oldest participants with hypertension, only 23% of women (vs. 38% of men) were controlled to BP <140/90 mmhg. Treatment with thiazide diuretics was also more frequent among women than men (38 vs. 23%, respectively) while ACE-I prescription less common. It is unknown whether the age-related decline in BP control among women is related to true treatment resistance because of biological factors or to inappropriate therapeutic choices in the clinical setting (drug selection, inadequate intensity of treatment, lack of compliance). Lloyd-Jones DM, Evans JC, Levy D. Hypertension in adults across the age spectrum: current outcomes and control in the community. JAMA 2005; 294:


13 Hypertension control in w o m e n r e m a i n s p o o r, especially among elderly women. R a t e s o f u n c o n t r o l l e d hypertension were positively related with age with only 29% of hypertensive women aged years having clinic BP <140/90mmHg. An increased prevalence of concomitant CV factors, including central obesity, elevated total cholesterol and low HDL-C levels are likely to contribute to poor BP control in elderly women.
14 Data from the Framingham Heart Study showed gender differences in BP control rates and in the pattern of antihypertensive medications prescribed. An age-related decrease in BP control rates were more pronounced in women than in men. Among the oldest participants with hypertension, only 23% of women (vs. 38% of men) were controlled to BP <140/90 mmhg. Treatment with thiazide diuretics was also more frequent among women than men (38 vs. 23%, respectively) while ACE-I prescription less common. It is unknown whether the age-related decline in BP control among women is related to true treatment resistance because of biological factors or to inappropriate therapeutic choices in the clinical setting (drug selection, inadequate intensity of treatment, lack of compliance). Lloyd-Jones DM, Evans JC, Levy D. Hypertension in adults across the age spectrum: current outcomes and control in the community. JAMA 2005; 294:

15 Estrogen induces vasodilatation, prevents vascular remodeling processes, inhibits vascular response to injury, provides reno-protection and decreases basal sympathetic tone. Progesterone induces endothelium-dependent vascular relaxation.
16 Hypertension-induced left ventricular hypertrophy is different in female and male patients, since hypertensive women are more likely to develop concentric hypertrophy while eccentric hypertrophy is more common among men. Arterial stiffness becomes more pronounced in postmenopausal women than men, leading to greater pulsatile afterload and subsequent diastolic dysfunction. Carotid plaques are more common in hypertensive men than women.
17 Fibromuscular dysplasia, a nonatherosclerotic noninflammatory vascular disease that can affect renal arteries and cause renovascular hypertension, primarily affects women aged from age 20 to 60, but can also affects men and children. Primary aldosteronism (PA), once considered being a rare condition has been demonstrated to be much more prevalent than previously thought and is probably the commonest cause of secondary hypertension. The prevalence of PA is similar in men and women, but estrogen and progesterone can affect aldosterone and renin levels and, consequently, can interfere with the investigation of PA. Screening with aldosterone renin ratio can be affected by the phase of menstrual cycle and by different forms of contraception.

18 Pregnancy
19 During early pregnancy, significant plasma volume expansion is common and frequently associated with a decrease in systemic vascular resistance, which leads to an increased cardiac output as well as a fall in mean arterial pressure. In women with mild pre-existing HTN these changes can obscure an early diagnosis of HTN. Pregnancy-associated HTN affects about 10% of all pregnancies. Preeclampsia, which is a pregnancy-specific syndrome of exaggerated vasoconstriction and reduced organ perfusion, must be differentiated from pre-existing chronic hypertension as the former can threaten the lives of both mother and fetus, and requires specialized care. Preeclampsia places women at long-term risk for CV diseases and that careful follow-up and aggressive preventive strategies are recommended.
20 Combined oral contraceptives (COCs) induce small increases in BP in the entire population of users and has been associated with a small excess risk of CV disease among women, especially in those with hypertension. Hypertension is two to three times more common among women taking oral COCs, especially in those obese and at advanced age, than in those not taking these medications. Modern preparations that contain lower doses (<30 mg) of estrogen can also lead to development of hypertension and can precipitate accelerated or malignant hypertension. Environmental characteristics (pre-existing pregnancy-induced hypertension, occult renal disease, obesity, middle age (>35 years) and duration of COC use) as well as genetic characteristics (family history of hypertension, increase susceptibility to COC-induced hypertension). Controlled prospective studies have consistently demonstrated a return of BP to pretreatment levels within 3 months of discontinuing COCs. Progestin-only contraceptives are a better choice for women with established hypertension.
21 The effect of menopause on BP is controversial and confounded by the effects of aging and clustering of other CV risk factors, such as body weight, LV hypertrophy and lipid levels. After adjustment for age and body mass index, the prevalence of hypertension in postmenopausal women is at least two fold and steeper that in premenopausal women. Changes in BP after menopause seem to be related with alterations in estrogen and progesterone levels. Both hormones have a significant impact on renal salt handling. While the BP response of premenopausal normotensive women is insensitive to dietary salt intake, BP in postmenopausal women becomes salt sensitive. However, the effects of natural estrogen and progesterone appear to be different from the synthetic preparations. Increased angiotensinogen generation has been proposed as a potential mechanism that links estrogen therapy to HTN.

22 Conflicting results have been reported by studies that evaluated the effects of hormone replacement therapy (HRT) on BP. Differences in patient populations studied, methods of measuring BP, hormone preparations and routes of administration partially explain the discrepancy between the studies. Minimal BP effects in normotensive women have been showed in most studies. HRT induces, if any, small changes in BP and should not preclude HRT use in either normotensive or hypertensive women. Nevertheless, all hypertensive women treated with HRT should have their BP measured initially and then at 3 6-month intervals depending on the difficulty of control.


23 Complications

24 In the Chicago Heart Association cohort, which was conducted in the 1960s and 1970s, high BP was the most common major risk factor in women and independently increased the risk of CHD mortality (RR 3.17)
25 Most epidemiological studies have shown that men have a higher stroke incidence than women. Such a gender difference in stroke incidence might be caused by the beneficial effects of estrogen on the brain in premenopausal women. In animal models, estrogen appeared to protect against ischemic brain damage (endothelium/neurons) Stroke incidence was increased in postmenopausal women whose serum estradiol level was the same/ less than the level in men. Estrogen treatment after menopause increases the risk of stroke and venous thromboembolic disease. Therefore, the effect of estrogen is not a simple answer for explaining the gender difference in stroke incidence..

26 The rates of ischemic stroke were reduced in both men and women owing to better management of hypertension for the past 40 years; however, there was a dramatic change in stroke subtypes. Women suffer more from lacunar infarctions and less from atherothrombotic infarctions compared to men. Interestingly, in women more Silent Brain Infarctions (x3 risk for clinical stroke) appear in brain imaging than in men. * Hypertens Res 2010; 33:
27 Males have a faster decline of renal function with age than females; however, this gender association is reversed in older age and postmenopausal women experience a more rapid deterioration of renal function than male individuals. Natural estrogen seems to exert beneficial actions on renal function. Contradictory findings exist regarding the impact of gender on the prevalence of chronic kidney disease. The prevalence of chronic kidney disease in women was found lower, similar, or higher than in men in different population cohorts. Women compared to men with incident hypertension were significantly less likely to suffer from myocardial infarction and stroke or die from any cause, while they were significantly more likely to develop chronic kidney disease. J Hypertens. 2013;31:271 7.

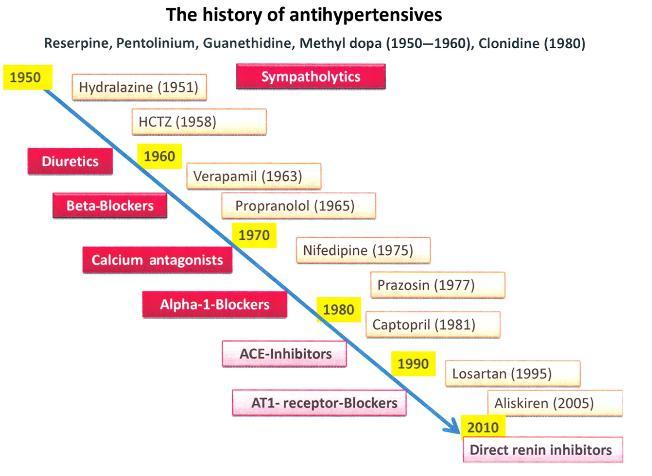
28 Treatment
29 Early clinical trials of treating mild-to-moderate HTN were primarily conducted on a middle-aged male population, and most decisions regarding hypertensive treatment for women prior to the 1990s were based on data obtained from these trials. Within the last two decades, women have been included in major outcome trials of antihypertensive treatment, which have generally shown comparable benefit in both women and men. Therefore, treatment recommendations remain the same for women and men.
 from the body.")
30 Pharmacokinetics is a term that describes the kinetics of the processes undergone by drugs in the body. It comprises main four steps: absorption, distribution, metabolism and clearance (Cl) from the body. Distribution: Women have a higher percent body fat than men, which can affect the volume of distribution of certain drugs. Metabolism: Sex-specific differences in activities of cytochrome P450 (CYP), transporters, uridine diphosphate glucuronosyltransferase enzymes, and renal excretion will result in differences in Cl. Clearence: Renal Cl of unchanged drugs is decreased in women because of a lower rate of glomerular filtration. However, clinically significant differences in therapeutic response resulting from sex-specific disparities in pharmacokinetics seem to be rare. It is important to take into account body weight and age, as well as comorbidity in determining the appropriate drug regimen for both men and women.
31 Gender differences in both benefit and adverse effects of treatment. In the VALUE study, women, but not men, assigned to valsartan-based treatment presented a relative increased risk of the primary endpoint of cardiac mortality and morbidity compared with those who received amlodipine-based treatment. Furthermore, the trend toward less congestive heart failure with valsartanbased treatment was not statistically significant in women. The ALLHAT Trial showed a slightly greater BP response to amlodipine compared with lisinopril in women, and this finding was associated with a more pronounced reduction in stroke. In the LIFE study despite similar BP reduction fewer events occurred in women than in men.
32 The Blood Pressure Lowering Treatment Trialists Collaboration reviewed 31 randomized trials that included women and men. Despite baseline BP levels were slightly higher among women than men, there was no evidence that women and men present different levels of protection from BP lowering regarding : total major CV events (stroke, coronary heart disease events, heart failure and other CV death). specific events as coronary heart disease, heart failure, CV death or total mortality. Treatment regimens based on calcium antagonists conferred marginally greater protection than regimens based on angiotensin-converting enzyme inhibitors in women compared with men. Treatment with beta blockers or diuretics showed similar benefit to other drug classes for either gender. Lancet 2014; (384) : p

33 Adverse events
34 Epidemiologic population studies have suggested that lowering BP, while reducing risks of stroke and vascular complications, might increase mortality or adverse events among the elderly (>80 years of age). These observations were particularly striking in older men. After adjustment for baseline BP, a decrease in diastolic pressure of >5mmHg was associated with higher all-cause mortality. In women, a decrease in either diastolic or systolic BP was not associated with poorer survival. Lancet 1999; 353:793-96
35 Biochemical responses to drugs appear to be gender dependent. Angiotensin-converting enzyme inhibitor induced cough is two to three times more common in women than in men. ACE-I and ARBs are contraindicated in women with family plan. Women are more likely to complain of calcium channel blocker-related peripheral edema and minoxidil-induced hirsutism. Women are more likely to develop hyponatremia or hypokalemia and men more likely to develop gout in response to diuretic therapy. However, HCTZ are particularly useful in elderly women, because their use was associated with decreased risk of hip fracture probably by reduction of urinary calcium loss. Sexual dysfunction related to antihypertensive therapy, which is more commonly discussed with men than women, seems to be a problem in women as well as in men. This effect is most often associated with centrally acting agents, b- blockers and thiazide diuretics, whereas angiotensin receptor blocker therapy may improve these symptoms.

36
37 Conclusions (1) ü Prevalence of hypertension is expected to increase more in women than men in the future. ü HTN awareness and treatment are higher in women than in men while the proportion of patients treated and controlled was higher in men than in women. It is suggested: a. raising HTN awareness and treatment for men, whereas b. controlling HTN in women.
38 Conclusions (2) ü Development of hypertension with COCs can occur and, usually, it resolves with withdrawal of the COC. ü Although the BP effects of menopause or HRT remain controversial, subsequent hypertension importantly contributes to CV morbidity and mortality in women. ü Antihypertensive treatments have comparable benefits in both women and men, but additional analyses/trials have demonstrated gender differences in both benefit/adverse effects of treatment.
HYPERTENSION GUIDELINES WHERE ARE WE IN 2014
 HYPERTENSION GUIDELINES WHERE ARE WE IN 2014 Donald J. DiPette MD FACP Special Assistant to the Provost for Health Affairs Distinguished Health Sciences Professor University of South Carolina University
HYPERTENSION GUIDELINES WHERE ARE WE IN 2014 Donald J. DiPette MD FACP Special Assistant to the Provost for Health Affairs Distinguished Health Sciences Professor University of South Carolina University
Cardiac Pathophysiology
 Cardiac Pathophysiology Evaluation Components Medical history Physical examination Routine laboratory tests Optional tests Medical History Duration and classification of hypertension. Patient history of
Cardiac Pathophysiology Evaluation Components Medical history Physical examination Routine laboratory tests Optional tests Medical History Duration and classification of hypertension. Patient history of
Hypertension. Most important public health problem in developed countries
 Hypertension Strategy for Continued Success in Treatment for the 21st Century November 15, 2005 Arnold B. Meshkov, M.D. Associate Professor of Medicine Temple University School of Medicine Philadelphia,
Hypertension Strategy for Continued Success in Treatment for the 21st Century November 15, 2005 Arnold B. Meshkov, M.D. Associate Professor of Medicine Temple University School of Medicine Philadelphia,
Antihypertensive drugs SUMMARY Made by: Lama Shatat
 Antihypertensive drugs SUMMARY Made by: Lama Shatat Diuretic Thiazide diuretics The loop diuretics Potassium-sparing Diuretics *Hydrochlorothiazide *Chlorthalidone *Furosemide *Torsemide *Bumetanide Aldosterone
Antihypertensive drugs SUMMARY Made by: Lama Shatat Diuretic Thiazide diuretics The loop diuretics Potassium-sparing Diuretics *Hydrochlorothiazide *Chlorthalidone *Furosemide *Torsemide *Bumetanide Aldosterone
Heart Failure (HF) Treatment
 Treatment") Heart Failure (HF) Treatment Heart Failure (HF) Complex, progressive disorder. The heart is unable to pump sufficient blood to meet the needs of the body. Its cardinal symptoms are dyspnea, fatigue, and
Heart Failure (HF) Treatment Heart Failure (HF) Complex, progressive disorder. The heart is unable to pump sufficient blood to meet the needs of the body. Its cardinal symptoms are dyspnea, fatigue, and
Hypertension. Does it Matter What Medications We Use? Nishant K. Sekaran, M.D. M.Sc. Intermountain Heart Institute
 Hypertension Does it Matter What Medications We Use? Nishant K. Sekaran, M.D. M.Sc. Intermountain Heart Institute Hypertension 2017 Classification BP Category Systolic Diastolic Normal 120 and 80 Elevated
Hypertension Does it Matter What Medications We Use? Nishant K. Sekaran, M.D. M.Sc. Intermountain Heart Institute Hypertension 2017 Classification BP Category Systolic Diastolic Normal 120 and 80 Elevated
Hypertension Update Warwick Jaffe Interventional Cardiologist Ascot Hospital
 Hypertension Update 2008 Warwick Jaffe Interventional Cardiologist Ascot Hospital Definition of Hypertension Continuous variable At some point the risk becomes high enough to justify treatment Treatment
Hypertension Update 2008 Warwick Jaffe Interventional Cardiologist Ascot Hospital Definition of Hypertension Continuous variable At some point the risk becomes high enough to justify treatment Treatment
M2 TEACHING UNDERSTANDING PHARMACOLOGY
 M2 TEACHING UNDERSTANDING PHARMACOLOGY USING CVS SYSTEM AS AN EXAMPLE NIGEL FONG 2 JAN 2014 TODAY S OBJECTIVE Pharmacology often seems like an endless list of mechanisms and side effects to memorize. To
M2 TEACHING UNDERSTANDING PHARMACOLOGY USING CVS SYSTEM AS AN EXAMPLE NIGEL FONG 2 JAN 2014 TODAY S OBJECTIVE Pharmacology often seems like an endless list of mechanisms and side effects to memorize. To
Management of Hypertension. M Misra MD MRCP (UK) Division of Nephrology University of Missouri School of Medicine
 Division of Nephrology University of Missouri School of Medicine") Management of Hypertension M Misra MD MRCP (UK) Division of Nephrology University of Missouri School of Medicine Disturbing Trends in Hypertension HTN awareness, treatment and control rates are decreasing
Management of Hypertension M Misra MD MRCP (UK) Division of Nephrology University of Missouri School of Medicine Disturbing Trends in Hypertension HTN awareness, treatment and control rates are decreasing
Hypertension The normal radial artery blood pressures in adults are: Systolic arterial pressure: 100 to 140 mmhg. Diastolic arterial pressure: 60 to
 Hypertension The normal radial artery blood pressures in adults are: Systolic arterial pressure: 100 to 140 mmhg. Diastolic arterial pressure: 60 to 90 mmhg. These pressures are called Normal blood pressure
Hypertension The normal radial artery blood pressures in adults are: Systolic arterial pressure: 100 to 140 mmhg. Diastolic arterial pressure: 60 to 90 mmhg. These pressures are called Normal blood pressure
ΑΡΥΙΚΗ ΠΡΟΔΓΓΙΗ ΤΠΔΡΣΑΙΚΟΤ ΑΘΔΝΟΤ. Μ.Β.Παπαβαζιλείοσ Καρδιολόγος FESC - Γιεσθύνηρια ιζμανόγλειον ΓΝΑ Clinical Hypertension Specialist ESH
 ΑΡΥΙΚΗ ΠΡΟΔΓΓΙΗ ΤΠΔΡΣΑΙΚΟΤ ΑΘΔΝΟΤ Μ.Β.Παπαβαζιλείοσ Καρδιολόγος FESC - Γιεσθύνηρια ιζμανόγλειον ΓΝΑ Clinical Hypertension Specialist ESH Hypertension Co-Morbidities HTN Commonly Clusters with Other Risk
ΑΡΥΙΚΗ ΠΡΟΔΓΓΙΗ ΤΠΔΡΣΑΙΚΟΤ ΑΘΔΝΟΤ Μ.Β.Παπαβαζιλείοσ Καρδιολόγος FESC - Γιεσθύνηρια ιζμανόγλειον ΓΝΑ Clinical Hypertension Specialist ESH Hypertension Co-Morbidities HTN Commonly Clusters with Other Risk
Η σημασία της αρτηριακής σκληρίας στην εκτίμηση της διαστολικής δυσλειτουργίας στην υπέρταση. Θεραπευτικές παρεμβάσεις
 Η σημασία της αρτηριακής σκληρίας στην εκτίμηση της διαστολικής δυσλειτουργίας στην υπέρταση. Θεραπευτικές παρεμβάσεις Ελένη Τριανταφυλλίδη Επιμελήτρια Α Β Πανεπιστημιακή Καρδιολογική Κλινική Αττικό Νοσοκομείο
Η σημασία της αρτηριακής σκληρίας στην εκτίμηση της διαστολικής δυσλειτουργίας στην υπέρταση. Θεραπευτικές παρεμβάσεις Ελένη Τριανταφυλλίδη Επιμελήτρια Α Β Πανεπιστημιακή Καρδιολογική Κλινική Αττικό Νοσοκομείο
DISCLOSURE PHARMACIST OBJECTIVES 9/30/2014 JNC 8: A REVIEW OF THE LONG-AWAITED/MUCH-ANTICIPATED HYPERTENSION GUIDELINES. I have nothing to disclose.
 JNC 8: A REVIEW OF THE LONG-AWAITED/MUCH-ANTICIPATED HYPERTENSION GUIDELINES Tiffany Dickey, PharmD Assistant Professor, UAMS COP Clinical Pharmacy Specialist, Mercy Hospital Northwest AR DISCLOSURE I
JNC 8: A REVIEW OF THE LONG-AWAITED/MUCH-ANTICIPATED HYPERTENSION GUIDELINES Tiffany Dickey, PharmD Assistant Professor, UAMS COP Clinical Pharmacy Specialist, Mercy Hospital Northwest AR DISCLOSURE I
VA/DoD Clinical Practice Guideline for the Diagnosis and Management of Hypertension - Pocket Guide Update 2004 Revision July 2005
 VA/DoD Clinical Practice Guideline for the Diagnosis and Management of Hypertension - Pocket Guide Update 2004 Revision July 2005 1 Any adult in the health care system 2 Obtain blood pressure (BP) (Reliable,
VA/DoD Clinical Practice Guideline for the Diagnosis and Management of Hypertension - Pocket Guide Update 2004 Revision July 2005 1 Any adult in the health care system 2 Obtain blood pressure (BP) (Reliable,
Management of Hypertension
 Clinical Practice Guidelines Management of Hypertension Definition and classification of blood pressure levels (mmhg) Category Systolic Diastolic Normal
Clinical Practice Guidelines Management of Hypertension Definition and classification of blood pressure levels (mmhg) Category Systolic Diastolic Normal
Estrogens vs Testosterone for cardiovascular health and longevity
 Estrogens vs Testosterone for cardiovascular health and longevity Panagiota Pietri, MD, PhD, FESC Director of Hypertension Unit Athens Medical Center Athens, Greece Women vs Men Is there a difference in
Estrogens vs Testosterone for cardiovascular health and longevity Panagiota Pietri, MD, PhD, FESC Director of Hypertension Unit Athens Medical Center Athens, Greece Women vs Men Is there a difference in
Hypertension Update Clinical Controversies Regarding Age and Race
 Hypertension Update Clinical Controversies Regarding Age and Race Allison Helmer, PharmD, BCACP Assistant Clinical Professor Auburn University Harrison School of Pharmacy July 22, 2017 DISCLOSURE/CONFLICT
Hypertension Update Clinical Controversies Regarding Age and Race Allison Helmer, PharmD, BCACP Assistant Clinical Professor Auburn University Harrison School of Pharmacy July 22, 2017 DISCLOSURE/CONFLICT
Hypertension CHAPTER-I CARDIOVASCULAR SYSTEM. Dr. K T NAIK Pharm.D Associate Professor Department of Pharm.D Krishna Teja Pharmacy College, Tirupati
 CHAPTER-I CARDIOVASCULAR SYSTEM Hypertension SUB: PHARMACOTHERAPEUTICS-I CODE:T0820006 Dr. K T NAIK Pharm.D Associate Professor Department of Pharm.D Krishna Teja Pharmacy College, Tirupati Hypertension
CHAPTER-I CARDIOVASCULAR SYSTEM Hypertension SUB: PHARMACOTHERAPEUTICS-I CODE:T0820006 Dr. K T NAIK Pharm.D Associate Professor Department of Pharm.D Krishna Teja Pharmacy College, Tirupati Hypertension
Chapter 23. Media Directory. Cardiovascular Disease (CVD) Hypertension: Classified into Three Categories
 Hypertension: Classified into Three Categories") Chapter 23 Drugs for Hypertension Slide 37 Slide 41 Media Directory Nifedipine Animation Doxazosin Animation Upper Saddle River, New Jersey 07458 All rights reserved. Cardiovascular Disease (CVD) Includes
Chapter 23 Drugs for Hypertension Slide 37 Slide 41 Media Directory Nifedipine Animation Doxazosin Animation Upper Saddle River, New Jersey 07458 All rights reserved. Cardiovascular Disease (CVD) Includes
Antihypertensive Agents Part-2. Assistant Prof. Dr. Najlaa Saadi PhD Pharmacology Faculty of Pharmacy University of Philadelphia
 Antihypertensive Agents Part-2 Assistant Prof. Dr. Najlaa Saadi PhD Pharmacology Faculty of Pharmacy University of Philadelphia Agents that block production or action of angiotensin Angiotensin-converting
Antihypertensive Agents Part-2 Assistant Prof. Dr. Najlaa Saadi PhD Pharmacology Faculty of Pharmacy University of Philadelphia Agents that block production or action of angiotensin Angiotensin-converting
By Prof. Khaled El-Rabat
 What is The Optimum? By Prof. Khaled El-Rabat Professor of Cardiology - Benha Faculty of Medicine HT. Introduction Despite major worldwide efforts over recent decades directed at diagnosing and treating
What is The Optimum? By Prof. Khaled El-Rabat Professor of Cardiology - Benha Faculty of Medicine HT. Introduction Despite major worldwide efforts over recent decades directed at diagnosing and treating
There is a striking age-dependent sexual dimorphism
 H y p e r t e n s i o n C u r r i c u l u m R e v i e w D o n a l d G. V i d t, M D, S e c t i o n E d i t o r Gender and Blood Pressure Suzanne Oparil, MD; Andrew P. Miller, MD The prevalence, impact,
H y p e r t e n s i o n C u r r i c u l u m R e v i e w D o n a l d G. V i d t, M D, S e c t i o n E d i t o r Gender and Blood Pressure Suzanne Oparil, MD; Andrew P. Miller, MD The prevalence, impact,
Prevention of Heart Failure: What s New with Hypertension
 Prevention of Heart Failure: What s New with Hypertension Ali AlMasood Prince Sultan Cardiac Center Riyadh 3ed Saudi Heart Failure conference, Jeddah, 13 December 2014 Background 20-30% of Saudi adults
Prevention of Heart Failure: What s New with Hypertension Ali AlMasood Prince Sultan Cardiac Center Riyadh 3ed Saudi Heart Failure conference, Jeddah, 13 December 2014 Background 20-30% of Saudi adults
Hypertension Management Controversies in the Elderly Patient
 Hypertension Management Controversies in the Elderly Patient Juan Bowen, MD Geriatric Update for the Primary Care Provider November 17, 2016 2016 MFMER slide-1 Disclosure No financial relationships No
Hypertension Management Controversies in the Elderly Patient Juan Bowen, MD Geriatric Update for the Primary Care Provider November 17, 2016 2016 MFMER slide-1 Disclosure No financial relationships No
Hypertension (JNC-8)
") Hypertension (JNC-8) Southern California University of Health Sciences Physician Assistant Program Management and Treatment of Hypertension April 17, 2018, presented by Ezra Levy, Pharm.D.! The 8 th Joint
Hypertension (JNC-8) Southern California University of Health Sciences Physician Assistant Program Management and Treatment of Hypertension April 17, 2018, presented by Ezra Levy, Pharm.D.! The 8 th Joint
The Failing Heart in Primary Care
 The Failing Heart in Primary Care Hamid Ikram How fares the Heart Failure Epidemic? 4357 patients, 57% women, mean age 74 years HFSA 2010 Practice Guideline (3.1) Heart Failure Prevention A careful and
The Failing Heart in Primary Care Hamid Ikram How fares the Heart Failure Epidemic? 4357 patients, 57% women, mean age 74 years HFSA 2010 Practice Guideline (3.1) Heart Failure Prevention A careful and
Amlodipine plus Lisinopril Tablets AMLOPRES-L
 Amlodipine plus Lisinopril Tablets AMLOPRES-L COMPOSITION AMLOPRES-L Each uncoated tablet contains: Amlodipine besylate equivalent to Amlodipine 5 mg and Lisinopril USP equivalent to Lisinopril (anhydrous)
Amlodipine plus Lisinopril Tablets AMLOPRES-L COMPOSITION AMLOPRES-L Each uncoated tablet contains: Amlodipine besylate equivalent to Amlodipine 5 mg and Lisinopril USP equivalent to Lisinopril (anhydrous)
Clinical Updates in the Treatment of Hypertension JNC 7 vs. JNC 8. Lauren Thomas, PharmD PGY1 Pharmacy Practice Resident South Pointe Hospital
 Clinical Updates in the Treatment of Hypertension JNC 7 vs. JNC 8 Lauren Thomas, PharmD PGY1 Pharmacy Practice Resident South Pointe Hospital Objectives Review the Eighth Joint National Committee (JNC
Clinical Updates in the Treatment of Hypertension JNC 7 vs. JNC 8 Lauren Thomas, PharmD PGY1 Pharmacy Practice Resident South Pointe Hospital Objectives Review the Eighth Joint National Committee (JNC
Therefore MAP=CO x TPR = HR x SV x TPR
 Regulation of MAP Flow = pressure gradient resistance CO = MAP TPR Therefore MAP=CO x TPR = HR x SV x TPR TPR is the total peripheral resistance: this is the combined resistance of all blood vessels (remember
Regulation of MAP Flow = pressure gradient resistance CO = MAP TPR Therefore MAP=CO x TPR = HR x SV x TPR TPR is the total peripheral resistance: this is the combined resistance of all blood vessels (remember
Younger adults with a family history of premature artherosclerotic disease should have their cardiovascular risk factors measured.
 Appendix 2A - Guidance on Management of Hypertension Measurement of blood pressure All adults from 40 years should have blood pressure measured as part of opportunistic cardiovascular risk assessment.
Appendix 2A - Guidance on Management of Hypertension Measurement of blood pressure All adults from 40 years should have blood pressure measured as part of opportunistic cardiovascular risk assessment.
RESISTENT HYPERTENSION. Dr. Helmy Bakr Professor and Head of Cardiology Dept. Mansoura University
 RESISTENT HYPERTENSION Dr. Helmy Bakr Professor and Head of Cardiology Dept. Mansoura University Resistant Hypertension Blood pressure remaining above goal in spite of concurrent use of 3 antihypertensive
RESISTENT HYPERTENSION Dr. Helmy Bakr Professor and Head of Cardiology Dept. Mansoura University Resistant Hypertension Blood pressure remaining above goal in spite of concurrent use of 3 antihypertensive
Dr Narender Goel MD (Internal Medicine and Nephrology) Financial Disclosure: None, Conflict of Interest: None
 Financial Disclosure: None, Conflict of Interest: None") Dr Narender Goel MD (Internal Medicine and Nephrology) drnarendergoel@gmail.com Financial Disclosure: None, Conflict of Interest: None 12 th December 2013, New York Visit us at: http://kidneyscience.info/
Dr Narender Goel MD (Internal Medicine and Nephrology) drnarendergoel@gmail.com Financial Disclosure: None, Conflict of Interest: None 12 th December 2013, New York Visit us at: http://kidneyscience.info/
5.2 Key priorities for implementation
 5.2 Key priorities for implementation From the full set of recommendations, the GDG selected ten key priorities for implementation. The criteria used for selecting these recommendations are listed in detail
5.2 Key priorities for implementation From the full set of recommendations, the GDG selected ten key priorities for implementation. The criteria used for selecting these recommendations are listed in detail
Chapter 10. Learning Objectives. Learning Objectives 9/11/2012. Congestive Heart Failure
 Chapter 10 Congestive Heart Failure Learning Objectives Explain concept of polypharmacy in treatment of congestive heart failure Explain function of diuretics Learning Objectives Discuss drugs used for
Chapter 10 Congestive Heart Failure Learning Objectives Explain concept of polypharmacy in treatment of congestive heart failure Explain function of diuretics Learning Objectives Discuss drugs used for
Reframe the Paradigm of Hypertension treatment Focus on Diabetes
 Reframe the Paradigm of Hypertension treatment Focus on Diabetes Paola Atallah, MD Lecturer of Clinical Medicine SGUMC EDL monthly meeting October 25,2016 Overview Physiopathology of hypertension Classification
Reframe the Paradigm of Hypertension treatment Focus on Diabetes Paola Atallah, MD Lecturer of Clinical Medicine SGUMC EDL monthly meeting October 25,2016 Overview Physiopathology of hypertension Classification
Diversity and HTN: Approaches to optimal BP control in AfricanAmericans
 Diversity and HTN: Approaches to optimal BP control in AfricanAmericans Quinn Capers, IV, MD, FACC, FSCAI Assistant Professor of Medicine Associate Dean for Admissions Do Racial Differences Really Exist
Diversity and HTN: Approaches to optimal BP control in AfricanAmericans Quinn Capers, IV, MD, FACC, FSCAI Assistant Professor of Medicine Associate Dean for Admissions Do Racial Differences Really Exist
Hypertension Pharmacotherapy: A Practical Approach
 Hypertension Pharmacotherapy: A Practical Approach Ronald Victor, MD Burns & Allen Chair in Cardiology Director, The Hypertension Center Associate Director, The Heart Institute Hypertension Center 1. 2.
Hypertension Pharmacotherapy: A Practical Approach Ronald Victor, MD Burns & Allen Chair in Cardiology Director, The Hypertension Center Associate Director, The Heart Institute Hypertension Center 1. 2.
Management of Hypertension. Ahmed El Hawary MD Suez Canal University
 Management of Hypertension Ahmed El Hawary MD Suez Canal University Minimal vs. Optimal Care Resources more than science affect type of care and level of management. what is possible (minimal care) and
Management of Hypertension Ahmed El Hawary MD Suez Canal University Minimal vs. Optimal Care Resources more than science affect type of care and level of management. what is possible (minimal care) and
Introductory Clinical Pharmacology Chapter 41 Antihypertensive Drugs
 Introductory Clinical Pharmacology Chapter 41 Antihypertensive Drugs Blood Pressure Normal = sys
Introductory Clinical Pharmacology Chapter 41 Antihypertensive Drugs Blood Pressure Normal = sys
Hypertension. Risk of cardiovascular disease beginning at 115/75 mmhg doubles with every 20/10mm Hg increase. (Grade B)
") Practice Guidelines and Principles: Guidelines and principles are intended to be flexible. They serve as reference points or recommendations, not rigid criteria. Guidelines and principles should be followed
Practice Guidelines and Principles: Guidelines and principles are intended to be flexible. They serve as reference points or recommendations, not rigid criteria. Guidelines and principles should be followed
JNC Evidence-Based Guidelines for the Management of High Blood Pressure in Adults
 JNC 8 2014 Evidence-Based Guidelines for the Management of High Blood Pressure in Adults Table of Contents Why Do We Treat Hypertension? Blood Pressure Treatment Goals Initial Therapy Strength of Recommendation
JNC 8 2014 Evidence-Based Guidelines for the Management of High Blood Pressure in Adults Table of Contents Why Do We Treat Hypertension? Blood Pressure Treatment Goals Initial Therapy Strength of Recommendation
What s In the New Hypertension Guidelines?
 American College of Physicians Ohio/Air Force Chapters 2018 Scientific Meeting Columbus, OH October 5, 2018 What s In the New Hypertension Guidelines? Max C. Reif, MD, FACP Objectives: At the end of the
American College of Physicians Ohio/Air Force Chapters 2018 Scientific Meeting Columbus, OH October 5, 2018 What s In the New Hypertension Guidelines? Max C. Reif, MD, FACP Objectives: At the end of the
Antihypertensive drugs: I. Thiazide and other diuretics:
 Clinical assessment of hypertensive patient: You have to take history regarding the presence of other risk factors for CAb like diabetes mellitus, smoking, etc. Take history whether the patient takes medications
Clinical assessment of hypertensive patient: You have to take history regarding the presence of other risk factors for CAb like diabetes mellitus, smoking, etc. Take history whether the patient takes medications
Cardiovascular Health Practice Guideline Outpatient Management of Coronary Artery Disease 2003
 Authorized By: Medical Management Guideline Committee Approval Date: 12/13/01 Revision Date: 12/11/03 Beta-Blockers Nitrates Calcium Channel Blockers MEDICATIONS Indicated in post-mi, unstable angina,
Authorized By: Medical Management Guideline Committee Approval Date: 12/13/01 Revision Date: 12/11/03 Beta-Blockers Nitrates Calcium Channel Blockers MEDICATIONS Indicated in post-mi, unstable angina,
Circulation. Blood Pressure and Antihypertensive Medications. Venous Return. Arterial flow. Regulation of Cardiac Output.
 Circulation Blood Pressure and Antihypertensive Medications Two systems Pulmonary (low pressure) Systemic (high pressure) Aorta 120 mmhg Large arteries 110 mmhg Arterioles 40 mmhg Arteriolar capillaries
Circulation Blood Pressure and Antihypertensive Medications Two systems Pulmonary (low pressure) Systemic (high pressure) Aorta 120 mmhg Large arteries 110 mmhg Arterioles 40 mmhg Arteriolar capillaries
Hypertension Update. Objectives 4/28/2015. Beverly J. Mathis, D.O. OOA May 2015
 Hypertension Update Beverly J. Mathis, D.O. OOA May 2015 Objectives Learn new recommendations for BP treatment goals Approach to hypertension in the office Use of hypertensive drugs, and how to tailor
Hypertension Update Beverly J. Mathis, D.O. OOA May 2015 Objectives Learn new recommendations for BP treatment goals Approach to hypertension in the office Use of hypertensive drugs, and how to tailor
Hypertension Management Focus on new RAAS blocker. Disclosure
 Hypertension Management Focus on new RAAS blocker Rameshkumar Raman M.D Endocrine Associates of The Quad Cities Disclosure Speaker bureau Abbott, Eli Lilly, Novo Nordisk, Novartis, Takeda, Merck, Solvay
Hypertension Management Focus on new RAAS blocker Rameshkumar Raman M.D Endocrine Associates of The Quad Cities Disclosure Speaker bureau Abbott, Eli Lilly, Novo Nordisk, Novartis, Takeda, Merck, Solvay
Outcomes and Perspectives of Single-Pill Combination Therapy for the modern management of hypertension
 Outcomes and Perspectives of Single-Pill Combination Therapy for the modern management of hypertension Prof. Massimo Volpe, MD, FAHA, FESC, Chair of Cardiology, Department of Clinical and Molecular Medicine
Outcomes and Perspectives of Single-Pill Combination Therapy for the modern management of hypertension Prof. Massimo Volpe, MD, FAHA, FESC, Chair of Cardiology, Department of Clinical and Molecular Medicine
Hypertension in the Elderly. John Puxty Division of Geriatrics Center for Studies in Aging and Health, Providence Care
 Hypertension in the Elderly John Puxty Division of Geriatrics Center for Studies in Aging and Health, Providence Care Learning Objectives Review evidence for treatment of hypertension in elderly Consider
Hypertension in the Elderly John Puxty Division of Geriatrics Center for Studies in Aging and Health, Providence Care Learning Objectives Review evidence for treatment of hypertension in elderly Consider
DISCLOSURES OUTLINE OUTLINE 9/29/2014 ANTI-HYPERTENSIVE MANAGEMENT OF CHRONIC KIDNEY DISEASE
 ANTI-HYPERTENSIVE MANAGEMENT OF CHRONIC KIDNEY DISEASE DISCLOSURES Editor-in-Chief- Nephrology- UpToDate- (Wolters Klewer) Richard J. Glassock, MD, MACP Geffen School of Medicine at UCLA 1 st Annual Internal
ANTI-HYPERTENSIVE MANAGEMENT OF CHRONIC KIDNEY DISEASE DISCLOSURES Editor-in-Chief- Nephrology- UpToDate- (Wolters Klewer) Richard J. Glassock, MD, MACP Geffen School of Medicine at UCLA 1 st Annual Internal
Hypertension. Penny Mosley MRPharmS
 Hypertension Penny Mosley MRPharmS Outline of presentation Introduction to hypertension Physiological control of arterial blood pressure What determines our bp? What determines the heart rate? What determines
Hypertension Penny Mosley MRPharmS Outline of presentation Introduction to hypertension Physiological control of arterial blood pressure What determines our bp? What determines the heart rate? What determines
7/7/ CHD/MI LVH and LV dysfunction Dysrrhythmias Stroke PVD Renal insufficiency and failure Retinopathy. Normal <120 Prehypertension
 Prevalence of Hypertension Hypertension: Diagnosis and Management T. Villela, M.D. Program Director University of California, San Francisco-San Francisco General Hospital Family and Community Medicine
Prevalence of Hypertension Hypertension: Diagnosis and Management T. Villela, M.D. Program Director University of California, San Francisco-San Francisco General Hospital Family and Community Medicine
Combination Therapy for Hypertension
 Combination Therapy for Hypertension Se-Joong Rim, MD Cardiology Division, Yonsei University College of Medicine, Seoul, Korea Goals of Therapy Reduce CVD and renal morbidity and mortality. Treat to BP
Combination Therapy for Hypertension Se-Joong Rim, MD Cardiology Division, Yonsei University College of Medicine, Seoul, Korea Goals of Therapy Reduce CVD and renal morbidity and mortality. Treat to BP
Hypertension Update Background
 Hypertension Update Background Overview Aaron J. Friedberg, MD Assistant Professor, Clinical Division of General Internal Medicine The Ohio State University Wexner Medical Center Management Guideline Comparison
Hypertension Update Background Overview Aaron J. Friedberg, MD Assistant Professor, Clinical Division of General Internal Medicine The Ohio State University Wexner Medical Center Management Guideline Comparison
Primary Prevention of Stroke
 Primary Prevention of Stroke Dr Chris Ellis Cardiologist Green Lane CVS Service, Auckland City Hospital & Auckland Heart Group, Mercy Hospital, Auckland 67 Pages Long, 735 References 29 Sub-Headings for
Primary Prevention of Stroke Dr Chris Ellis Cardiologist Green Lane CVS Service, Auckland City Hospital & Auckland Heart Group, Mercy Hospital, Auckland 67 Pages Long, 735 References 29 Sub-Headings for
Hypertension Update 2009
 Hypertension Update 2009 New Drugs, New Goals, New Approaches, New Lessons from Clinical Trials Timothy C Fagan, MD, FACP Professor Emeritus University of Arizona New Drugs Direct Renin Inhibitors Endothelin
Hypertension Update 2009 New Drugs, New Goals, New Approaches, New Lessons from Clinical Trials Timothy C Fagan, MD, FACP Professor Emeritus University of Arizona New Drugs Direct Renin Inhibitors Endothelin
Difficult to Treat Hypertension
 Difficult to Treat Hypertension According to Goldilocks JNC 8 Blood Pressure Goals (2014) BP Goal 60 years old and greater*- systolic < 150 and diastolic < 90. (Grade A)** BP Goal 18-59 years old* diastolic
Difficult to Treat Hypertension According to Goldilocks JNC 8 Blood Pressure Goals (2014) BP Goal 60 years old and greater*- systolic < 150 and diastolic < 90. (Grade A)** BP Goal 18-59 years old* diastolic
Introduction. Factors affecting blood pressure: 1-COP = HR X SV mainly affect SBP. 2-TPR = diameter of arterioles X viscosity of blood affect DBP
 Introduction Hypertension is a persistent elevation of blood pressure above 140 / 90 mmhg for more than three sitting. (0ptimal level
Introduction Hypertension is a persistent elevation of blood pressure above 140 / 90 mmhg for more than three sitting. (0ptimal level
Should beta blockers remain first-line drugs for hypertension?
 1 de 6 03/11/2008 13:23 Should beta blockers remain first-line drugs for hypertension? Maros Elsik, Cardiologist, Department of Epidemiology and Preventive Medicine, Monash University and The Alfred Hospital,
1 de 6 03/11/2008 13:23 Should beta blockers remain first-line drugs for hypertension? Maros Elsik, Cardiologist, Department of Epidemiology and Preventive Medicine, Monash University and The Alfred Hospital,
Hypertension Update. Sarah J. Payne, MS, PharmD, BCPS Assistant Professor, Department of Pharmacotherapy UNT System College of Pharmacy
 Hypertension Update Sarah J. Payne, MS, PharmD, BCPS Assistant Professor, Department of Pharmacotherapy UNT System College of Pharmacy Introduction 1/3 of US adults have HTN More prevalent in non-hispanic
Hypertension Update Sarah J. Payne, MS, PharmD, BCPS Assistant Professor, Department of Pharmacotherapy UNT System College of Pharmacy Introduction 1/3 of US adults have HTN More prevalent in non-hispanic
HYPERTENSION IN EMERGENCY MEDICINE Michael Jay Bresler, M.D., FACEP
 HYPERTENSION IN EMERGENCY MEDICINE Michael Jay Bresler, M.D., FACEP What is normal blood pressure? Prehypertension 130-139/80-90 Compared with normal BP Double the risk for developing hypertension. Lifestyle
HYPERTENSION IN EMERGENCY MEDICINE Michael Jay Bresler, M.D., FACEP What is normal blood pressure? Prehypertension 130-139/80-90 Compared with normal BP Double the risk for developing hypertension. Lifestyle
Beta 1 Beta blockers A - Propranolol,
 Pharma Lecture 3 Beta blockers that we are most interested in are the ones that target Beta 1 receptors. Beta blockers A - Propranolol, it s a non-selective competitive antagonist of beta 1 and beta 2
Pharma Lecture 3 Beta blockers that we are most interested in are the ones that target Beta 1 receptors. Beta blockers A - Propranolol, it s a non-selective competitive antagonist of beta 1 and beta 2
Hypertension Update. Aaron J. Friedberg, MD
 Hypertension Update Aaron J. Friedberg, MD Assistant Professor, Clinical Division of General Internal Medicine The Ohio State University Wexner Medical Center Background Diagnosis Management Overview Guideline
Hypertension Update Aaron J. Friedberg, MD Assistant Professor, Clinical Division of General Internal Medicine The Ohio State University Wexner Medical Center Background Diagnosis Management Overview Guideline
LCZ696 A First-in-Class Angiotensin Receptor Neprilysin Inhibitor
 The Angiotensin Receptor Neprilysin Inhibitor LCZ696 in Heart Failure with Preserved Ejection Fraction The Prospective comparison of ARNI with ARB on Management Of heart failure with preserved ejection
The Angiotensin Receptor Neprilysin Inhibitor LCZ696 in Heart Failure with Preserved Ejection Fraction The Prospective comparison of ARNI with ARB on Management Of heart failure with preserved ejection
New Hypertension Guideline Recommendations for Adults July 7, :45-9:30am
 Advances in Cardiovascular Disease 30 th Annual Convention and Reunion UERM-CMAA, Inc. Annual Convention and Scientific Meeting July 5-8, 2018 New Hypertension Guideline Recommendations for Adults July
Advances in Cardiovascular Disease 30 th Annual Convention and Reunion UERM-CMAA, Inc. Annual Convention and Scientific Meeting July 5-8, 2018 New Hypertension Guideline Recommendations for Adults July
DRUG CLASSES BETA-ADRENOCEPTOR ANTAGONISTS (BETA-BLOCKERS)
") DRUG CLASSES BETA-ADRENOCEPTOR ANTAGONISTS (BETA-BLOCKERS) Beta-blockers have been widely used in the management of angina, certain tachyarrhythmias and heart failure, as well as in hypertension. Examples
DRUG CLASSES BETA-ADRENOCEPTOR ANTAGONISTS (BETA-BLOCKERS) Beta-blockers have been widely used in the management of angina, certain tachyarrhythmias and heart failure, as well as in hypertension. Examples
In the Literature 1001 BP of 1.1 mm Hg). The trial was stopped early based on prespecified stopping rules because of a significant difference in cardi
. The trial was stopped early based on prespecified stopping rules because of a significant difference in cardi") Is Choice of Antihypertensive Agent Important in Improving Cardiovascular Outcomes in High-Risk Hypertensive Patients? Commentary on Jamerson K, Weber MA, Bakris GL, et al; ACCOMPLISH Trial Investigators.
Is Choice of Antihypertensive Agent Important in Improving Cardiovascular Outcomes in High-Risk Hypertensive Patients? Commentary on Jamerson K, Weber MA, Bakris GL, et al; ACCOMPLISH Trial Investigators.
ΥΠΕΡΤΑΣΗ ΚΑΙ ΣΤΕΦΑΝΙΑΙΑ ΝΟΣΟΣ Ι.Ε.ΚΑΝΟΝΙΔΗΣ
 ΥΠΕΡΤΑΣΗ ΚΑΙ ΣΤΕΦΑΝΙΑΙΑ ΝΟΣΟΣ Ι.Ε.ΚΑΝΟΝΙΔΗΣ CAD: Statistics CAD is the largest killer of American males and females 13 million Americans have CAD 1.1 million MI s per year Every 26 seconds an American
ΥΠΕΡΤΑΣΗ ΚΑΙ ΣΤΕΦΑΝΙΑΙΑ ΝΟΣΟΣ Ι.Ε.ΚΑΝΟΝΙΔΗΣ CAD: Statistics CAD is the largest killer of American males and females 13 million Americans have CAD 1.1 million MI s per year Every 26 seconds an American
Hypertension Clinical case scenarios for primary care
 Hypertension Clinical case scenarios for primary care Implementing NICE guidance August 2011 NICE clinical guideline 127 What this presentation covers Five clinical case scenarios, including: presentation
Hypertension Clinical case scenarios for primary care Implementing NICE guidance August 2011 NICE clinical guideline 127 What this presentation covers Five clinical case scenarios, including: presentation
MPharmProgramme. Hypertension (HTN)
") MPharmProgramme Hypertension (HTN) Slide 1 of 30 Overview Definition Prevalence Type Causes Diagnosis Management Patients perspective Slide 2 of 30 Definition It is not a disease! So what is it? What two
MPharmProgramme Hypertension (HTN) Slide 1 of 30 Overview Definition Prevalence Type Causes Diagnosis Management Patients perspective Slide 2 of 30 Definition It is not a disease! So what is it? What two
Evaluation and Management of Hypertension in Women. Vesna D. Garovic, M.D. Moscow, Russia, December 2016
 Evaluation and Management of Hypertension in Women Vesna D. Garovic, M.D. Moscow, Russia, December 2016 2016 MFMER 3508058-1 Women are not small men There is nothing as powerful as an idea whose time has
Evaluation and Management of Hypertension in Women Vesna D. Garovic, M.D. Moscow, Russia, December 2016 2016 MFMER 3508058-1 Women are not small men There is nothing as powerful as an idea whose time has
Hypertension Guidelines: Are We Pressured to Change? Oregon Cardiovascular Symposium Portland, Oregon June 6, Financial Disclosures
 Hypertension Guidelines: Are We Pressured to Change? Oregon Cardiovascular Symposium Portland, Oregon June 6, 2015 William C. Cushman, MD Professor, Preventive Medicine, Medicine, and Physiology University
Hypertension Guidelines: Are We Pressured to Change? Oregon Cardiovascular Symposium Portland, Oregon June 6, 2015 William C. Cushman, MD Professor, Preventive Medicine, Medicine, and Physiology University
Chapter 10 Worksheet Blood Pressure and Antithrombotic Agents
 Complete the following. 1. A layer of cells lines each vessel in the vascular system. This layer is a passive barrier that keeps cells and proteins from going into tissues; it also contains substances
Complete the following. 1. A layer of cells lines each vessel in the vascular system. This layer is a passive barrier that keeps cells and proteins from going into tissues; it also contains substances
1. Antihypertensive agents 2. Vasodilators & treatment of angina 3. Drugs used in heart failure 4. Drugs used in arrhythmias
 1. Antihypertensive agents 2. Vasodilators & treatment of angina 3. Drugs used in heart failure 4. Drugs used in arrhythmias Only need to know drugs discussed in class At the end of this section you should
1. Antihypertensive agents 2. Vasodilators & treatment of angina 3. Drugs used in heart failure 4. Drugs used in arrhythmias Only need to know drugs discussed in class At the end of this section you should
HYPERTENSION AND HEART FAILURE
 HYPERTENSION AND HEART FAILURE Kenya Cardiac Society Symposium Feb 2017 Dr Jeilan Mohamed No conflict of interests . Geoffrey, 45 yr old hypertensive office worker male from Nairobi, has just watched his
HYPERTENSION AND HEART FAILURE Kenya Cardiac Society Symposium Feb 2017 Dr Jeilan Mohamed No conflict of interests . Geoffrey, 45 yr old hypertensive office worker male from Nairobi, has just watched his
Functional vascular disorders
 Functional vascular disorders Raynaud s phenomenon Raynaud s phenomenon Refers to Intermittent,bilateral attacks of ischemia of the fingers or toes, and sometimes ears or nose. It clinically manifests
Functional vascular disorders Raynaud s phenomenon Raynaud s phenomenon Refers to Intermittent,bilateral attacks of ischemia of the fingers or toes, and sometimes ears or nose. It clinically manifests
Pharmacologic Management of Hypertension
 Current Concepts In Management of Fernando Vega, MD Secondary - Definition Renovascular Disease (The kidney doesn t get impressed by blood pressure) Renovascular stenosis Renal artery stenosis Fibromuscular
Current Concepts In Management of Fernando Vega, MD Secondary - Definition Renovascular Disease (The kidney doesn t get impressed by blood pressure) Renovascular stenosis Renal artery stenosis Fibromuscular
Long-Term Care Updates
 Long-Term Care Updates August 2015 By Darren Hein, PharmD Hypertension is a clinical condition in which the force of blood pushing on the arteries is higher than normal. This increases the risk for heart
Long-Term Care Updates August 2015 By Darren Hein, PharmD Hypertension is a clinical condition in which the force of blood pushing on the arteries is higher than normal. This increases the risk for heart
DRUGS USED TO TREAT HYPERTENSION BY ALI ALALAWI
 DRUGS USED TO TREAT HYPERTENSION BY ALI ALALAWI 3. Vasodilators Drugs which dilate blood vessels ( decrease peripheral vascular resistance) by acting on smooth muscle cells through non-autonomic mechanisms:
DRUGS USED TO TREAT HYPERTENSION BY ALI ALALAWI 3. Vasodilators Drugs which dilate blood vessels ( decrease peripheral vascular resistance) by acting on smooth muscle cells through non-autonomic mechanisms:
Management of Hypertension in special groups. DR-Mohammed Salah Assistant Lecturer of Cardiology Mansoura University
 Management of Hypertension in special groups BY DR-Mohammed Salah Assistant Lecturer of Cardiology Mansoura University AGENDA SPECIAL GROUPS SPECIFIC DRUDS FOR SPECIAL GROUPS TARGET BP FOR SPECIAL GROUPS:
Management of Hypertension in special groups BY DR-Mohammed Salah Assistant Lecturer of Cardiology Mansoura University AGENDA SPECIAL GROUPS SPECIFIC DRUDS FOR SPECIAL GROUPS TARGET BP FOR SPECIAL GROUPS:
How Low Do We Go? Update on Hypertension
 How Low Do We Go? Update on Beth L. Abramson, MD, FRCPC, FACC As presented at the University of Toronto s Saturday at the University Session (September 2003) Arecent World Health Organization report states
How Low Do We Go? Update on Beth L. Abramson, MD, FRCPC, FACC As presented at the University of Toronto s Saturday at the University Session (September 2003) Arecent World Health Organization report states
HYPERTENSIVE VASCULAR DISEASE
 HYPERTENSIVE VASCULAR DISEASE Cutoffs in diagnosing hypertension in clinical practice sustained diastolic pressures >90 mm Hg, or sustained systolic pressures >140 mm Hg Malignant hypertension A small
HYPERTENSIVE VASCULAR DISEASE Cutoffs in diagnosing hypertension in clinical practice sustained diastolic pressures >90 mm Hg, or sustained systolic pressures >140 mm Hg Malignant hypertension A small
Rationale for the use of Single Pill Combination (SPC) and Asian data of ARB/CCB SPC
 and Asian data of ARB/CCB SPC") Rationale for the use of Single Pill Combination (SPC) and Asian data of ARB/CCB SPC Seung Woo Park, MD Samsung Medical Center BP Control Rates in Asia BP controlled BP uncontrolled 24.3% 36.6% 19% Turkey
Rationale for the use of Single Pill Combination (SPC) and Asian data of ARB/CCB SPC Seung Woo Park, MD Samsung Medical Center BP Control Rates in Asia BP controlled BP uncontrolled 24.3% 36.6% 19% Turkey
In the name of GOD. Animal models of cardiovascular diseases: myocardial infarction & hypertension
 In the name of GOD Animal models of cardiovascular diseases: myocardial infarction & hypertension 44 Presentation outline: Cardiovascular diseases Acute myocardial infarction Animal models for myocardial
In the name of GOD Animal models of cardiovascular diseases: myocardial infarction & hypertension 44 Presentation outline: Cardiovascular diseases Acute myocardial infarction Animal models for myocardial
VALUE OF ACEI IN THE MANAGEMENT OF HYPERTENSION
 VALUE OF ACEI IN THE MANAGEMENT OF HYPERTENSION Dr Catherine BESEME Paris 6 th December 2005 6 th International Congress of Bangladesh Society of Medicine Hypertension is a risk factor at the source, with
VALUE OF ACEI IN THE MANAGEMENT OF HYPERTENSION Dr Catherine BESEME Paris 6 th December 2005 6 th International Congress of Bangladesh Society of Medicine Hypertension is a risk factor at the source, with
Renal Regulation of Sodium and Volume. Dr. Dave Johnson Associate Professor Dept. Physiology UNECOM
 Renal Regulation of Sodium and Volume Dr. Dave Johnson Associate Professor Dept. Physiology UNECOM Maintaining Volume Plasma water and sodium (Na + ) are regulated independently - you are already familiar
Renal Regulation of Sodium and Volume Dr. Dave Johnson Associate Professor Dept. Physiology UNECOM Maintaining Volume Plasma water and sodium (Na + ) are regulated independently - you are already familiar
Elements for a public summary
 VI.2 Elements for a public summary VI.2.1Overview of disease epidemiology 1 Losartan is indicated for: Treatment of essential hypertension in adults and in children and adolescent 6 18 years of age. Treatment
VI.2 Elements for a public summary VI.2.1Overview of disease epidemiology 1 Losartan is indicated for: Treatment of essential hypertension in adults and in children and adolescent 6 18 years of age. Treatment
Blood Pressure Management in Acute Ischemic Stroke
 Blood Pressure Management in Acute Ischemic Stroke Kimberly Clark, PharmD, BCCCP Clinical Pharmacy Specialist Critical Care, Greenville Health System Adjunct Assistant Professor, South Carolina College
Blood Pressure Management in Acute Ischemic Stroke Kimberly Clark, PharmD, BCCCP Clinical Pharmacy Specialist Critical Care, Greenville Health System Adjunct Assistant Professor, South Carolina College
Using the New Hypertension Guidelines
 Using the New Hypertension Guidelines Kamal Henderson, MD Department of Cardiology, Preventive Medicine, University of North Carolina School of Medicine Kotchen TA. Historical trends and milestones in
Using the New Hypertension Guidelines Kamal Henderson, MD Department of Cardiology, Preventive Medicine, University of North Carolina School of Medicine Kotchen TA. Historical trends and milestones in
Phase 3 investigation of aprocitentan for resistant hypertension management. Investor Webcast June 2018
 Phase 3 investigation of aprocitentan for resistant hypertension management Investor Webcast June 2018 The following information contains certain forward-looking statements, relating to the company s business,
Phase 3 investigation of aprocitentan for resistant hypertension management Investor Webcast June 2018 The following information contains certain forward-looking statements, relating to the company s business,
Towards a Greater Understanding of Cardiac Medications Foundational Cardiac Concepts That Must Be Understood:
 Towards a Greater Understanding of Cardiac Medications Foundational Cardiac Concepts That Must Be Understood: Cardiac Output (CO) CO=SVxHR (stroke volume x heart rate) Cardiac output: The amount of blood
Towards a Greater Understanding of Cardiac Medications Foundational Cardiac Concepts That Must Be Understood: Cardiac Output (CO) CO=SVxHR (stroke volume x heart rate) Cardiac output: The amount of blood
Heart Failure. Acute. Plasma [NE] (pg/ml) 24 Hours. Chronic
![Heart Failure. Acute. Plasma [NE] (pg/ml) 24 Hours. Chronic](/thumbs/90/103241154.jpg "Heart Failure. Acute. Plasma [NE] (pg/ml) 24 Hours. Chronic") Heart Failure Heart failure is the inability of the heart to deliver sufficient blood to the tissues to ensure adequate oxygen supply. Clinically it is characterized by signs of volume overload or symptoms
Heart Failure Heart failure is the inability of the heart to deliver sufficient blood to the tissues to ensure adequate oxygen supply. Clinically it is characterized by signs of volume overload or symptoms
Incidental Findings; Management of patients presenting with high BP. Phil Swales
 Incidental Findings; Management of patients presenting with high BP Phil Swales Consultant Physician Acute & General Medicine University Hospitals of Leicester NHS Trust Objectives The approach to an incidental
Incidental Findings; Management of patients presenting with high BP Phil Swales Consultant Physician Acute & General Medicine University Hospitals of Leicester NHS Trust Objectives The approach to an incidental
Treating Hypertension in Individuals with Diabetes
 Treating Hypertension in Individuals with Diabetes Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any
Treating Hypertension in Individuals with Diabetes Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any
Pre-ALLHAT Drug Use. Diuretics. ß-Blockers. ACE Inhibitors. CCBs. Year. % of Treated Patients on Medication. CCBs. Beta Blockers.
 Pre- Drug Use % of Treated Patients on Medication 60 50 40 30 20 10 0 1978 Diuretics ß-Blockers ACE Inhibitors Year CCBs CCBs Beta Blockers Diuretics ACE Inhibitors 1980 1982 1984 1986 1988 1990 1992 IMS
Pre- Drug Use % of Treated Patients on Medication 60 50 40 30 20 10 0 1978 Diuretics ß-Blockers ACE Inhibitors Year CCBs CCBs Beta Blockers Diuretics ACE Inhibitors 1980 1982 1984 1986 1988 1990 1992 IMS
LXIV: DRUGS: 4. RAS BLOCKADE
 LXIV: DRUGS: 4. RAS BLOCKADE ACE Inhibitors Components of RAS Actions of Angiotensin i II Indications for ACEIs Contraindications RAS blockade in hypertension RAS blockade in CAD RAS blockade in HF Limitations
LXIV: DRUGS: 4. RAS BLOCKADE ACE Inhibitors Components of RAS Actions of Angiotensin i II Indications for ACEIs Contraindications RAS blockade in hypertension RAS blockade in CAD RAS blockade in HF Limitations
ANGIOTENSIN II RECEPTOR BLOCKERS: MORE THAN THE ALTERNATIVE PRESENTATION BY: PATRICK HO, USC PHARM D. CANDIDATE OF 2017 MENTOR: DR.
 ANGIOTENSIN II RECEPTOR BLOCKERS: MORE THAN THE ALTERNATIVE PRESENTATION BY: PATRICK HO, USC PHARM D. CANDIDATE OF 2017 MENTOR: DR. CRAIG STERN, PHARMD, MBA, RPH, FASCP, FASHP, FICA, FLMI, FAMCP RENIN-ANGIOTENSIN
ANGIOTENSIN II RECEPTOR BLOCKERS: MORE THAN THE ALTERNATIVE PRESENTATION BY: PATRICK HO, USC PHARM D. CANDIDATE OF 2017 MENTOR: DR. CRAIG STERN, PHARMD, MBA, RPH, FASCP, FASHP, FICA, FLMI, FAMCP RENIN-ANGIOTENSIN
Update on Current Trends in Hypertension Management
 Friday General Session Update on Current Trends in Hypertension Management Shawna Nesbitt, MD Associate Dean, Minority Student Affairs Associate Professor, Department of Internal Medicine Office of Student
Friday General Session Update on Current Trends in Hypertension Management Shawna Nesbitt, MD Associate Dean, Minority Student Affairs Associate Professor, Department of Internal Medicine Office of Student
β adrenergic blockade, a renal perspective Prof S O McLigeyo
 β adrenergic blockade, a renal perspective Prof S O McLigeyo Carvedilol Third generation β blocker (both β 1 and β 2 ) Possesses α 1 adrenergic blocking properties. β: α blocking ratio 7:1 to 3:1 Antioxidant
β adrenergic blockade, a renal perspective Prof S O McLigeyo Carvedilol Third generation β blocker (both β 1 and β 2 ) Possesses α 1 adrenergic blocking properties. β: α blocking ratio 7:1 to 3:1 Antioxidant
Director of the Israeli Institute for Quality in Medicine Israeli Medical Association July 1st, 2016
 The differential effect of Atherosclerosis on end organ damage in adult and elderly patients with CVRF: New Algorithm for Hypertension Diagnosis and Treatment R. Zimlichman, FAHA, FASH, FESC, FESH Chief
The differential effect of Atherosclerosis on end organ damage in adult and elderly patients with CVRF: New Algorithm for Hypertension Diagnosis and Treatment R. Zimlichman, FAHA, FASH, FESC, FESH Chief