Marti McCulloch, BS, MBA, RDCS, FASE Houston, Texas
|
|
|
- Robyn Robbins
- 5 years ago
- Views:
Transcription


1 Marti McCulloch, BS, MBA, RDCS, FASE Houston, Texas Mitral Regurgitation
 Regurgitant Fraction (%) Effective Regurgitant Orifice Area (EROA cm 2 ) Cases implement what you")
2 What to Expect Review Specific Signs of Severity Supportive Signs of Severity Qualitative Parameters Structural Doppler Quantitative Parameters Vena Contracta Width Regurgitant Volume (ml/beat) Regurgitant Fraction (%) Effective Regurgitant Orifice Area (EROA cm 2 ) Cases implement what you learned!


3 Specific Signs Mild Small central jet <4 cm 2 or <20% of LA Vena contracta width <0.3cm No or minimal flow convergence Moderate Signs of MR > Mild but no criteria for severe MR Severe Vena contracta width >0.7cm Large flow convergence Systolic reversal in pulmonary veins Prominent flail MV leaflet of ruptured papillary muscle Zoghbi, et. al. JASE 2003


 Enlarged LV Enlarged LA Zoghbi, et.")
4 Supportive Signs Mild Systolic dominant flow in pulmonary veins A-wave dominant mitral inflow Soft density, parabolic CW Doppler MR signal Normal LV size Moderate Intermediate signs/findings Severe Dense, triangular CW Doppler MR jet (early peaking) E-wave dominant mitral inflow (E > 1.2 m/s) Enlarged LV Enlarged LA Zoghbi, et. al. JASE 2003
 Mild <0.")

 Mild:")

 Mild <30 Mild-Mod")
5 Quantitative Parameters EROA (cm 2 ) Mild <0.20 Mild-Mod Mod-Sev Severe >0.40 R Vol (ml/beat) Mild: <30 Mild-Mod Mod-Sev Severe >60 Regurgitant Fraction % (RF) Mild <30 Mild-Mod Mod-Sev Severe >50 Zoghbi, et. al. JASE 2003
6 Grading MR Qualitative/Supportive Methods Parameters Mild Moderate Severe Color jet area 4cm 2 or 10% LA Variable >10cm 2 or 40% LA CW Faint/parabolic Dense/para Dense/early peak Pvein flow Sys. dominance Sys. Blunting Systolic reversal MV Inflow Dominant A wave Dominant E >1.2 Quantitative Methods Parameters Mild Moderate Severe Vena Contracta < >0.7 Reg. Volume < >60 Reg. Fraction < >50 EROA (cm 2 ) < >0.40 Zoghbi, et. al. JASE 2003

7 7

8 Mitral Regurgitation

9 Vena Contracta Measurement at the narrowest portion of neck during mitral regurgitation. VC = 0.9 Optimize jet in PLAX Zoom or RES Look for flow across the valve with a neck Measurement of the vena contracta is a quick and accurate quantitative technique when properly applied. It works best on single central MR jets, but is also valuable in assessing an eccentric jet. Roberts, B and Grayburn, P. Vena Contracta: Practical Approach. J Am Soc Echocardiogr 2003;16: )

10 PISA Method Volume Flow Rate (VFR) = 2 x x r 2 x V r Effective Reg Orifice Area = VFR/V MAX Regurgitant Volume (rvol) = ERO x VTI r=0.7 Adjust baseline Scroll to midsystole Locate vena contracta Measure from vena contracta to 1 st color shift change

11 PISA Method Volume Flow Rate (VFR) = 2 x x r 2 x V r Effective Reg Orifice (ERO) = VFR/V MAX Regurgitant Volume (RVol) = ERO x VTI VFR = 6.28 x.49 x 34 VFR = 105cc/s r=0.7 ERO = VFR/V MAX ERO = 105/417.4 ERO = 0.25cm 2 RVol = ERO x VTI RVol = 0.25 x 130 Rvol = 32mL
12 Grading MR Qualitative Methods Parameters Mild Moderate Severe Color jet area 4cm 2 or 10% LA Variable >10cm 2 or 40% LA CW Faint/parabolic Dense/para Dense/early peak Pvein flow Sys. dominance Sys. Blunting Systolic reversal MV Inflow Dominant A wave Dominant E >1.2 Quantitive Methods Parameters Mild Moderate Severe Vena Contracta < >0.7 Reg. Volume < >60 Reg. Fraction < >50 EROA (cm 2 ) < >0.40 Zoghbi, et. al. JASE 2003
13 Easy PISA? If aliasing velocity cm/sec and the velocity is around 500 cm/sec ERO = ERO = 0.38 X r X r 2 X 30 cm/sec 500 cm/sec r=0.7 ERO = 0.38 x (0.7) 2 ERO = 0.38 x 0.49 ERO = 0.19 cm 2
14 Left Atrial Pressure LAP = SBP 4 X MRV 2 SBP = 140 MRV = 5 m/s LAP= X 25 LAP= LAP= 40 LAP = SBP 4 X MRV 2 SBP = 140 MRV = 4 m/s LAP = X 16 LAP = LAP = 76
15 Regurgitant Fraction % RF% = SV (Valve) SV (Systemic) / SV (Valve) VTI 25.9 cm MA ann 2.2 cm MA SV = D 2 x.785 x VTI MA SV = 2.2 x.785 x 25.9 MA SV = 98.4 ml LVOT SV = D 2 x.785 x VTI
16 Regurgitant Fraction % RF% = SV (Valve) SV (Systemic) / SV (Valve) VTI 15.8 cm LVOT 1.8 cm MA SV = D 2 x.785 x VTI MA SV = 2.2 x.785 x 25.9 MA SV = 98.4 ml LVOT SV = D 2 x.785 x VTI LVOT SV = 3.24 x.785 x 15.8 LVOT SV = 40.2 ml RF% = MA SV LV SV / MA SV RF% = / 98.4 RF% = 59%
17 Grading MR Qualitative Methods Parameters Mild Moderate Severe Color jet area 4cm 2 or 10% LA Variable >10cm 2 or 40% LA CW Faint/parabolic Dense/para Dense/early peak Pvein flow Sys. dominance Sys. Blunting Systolic reversal MV Inflow Dominant A wave Dominant E >1.2 Quantitive Methods Parameters Mild Moderate Severe Vena Contracta < >0.7 Reg. Volume < >60 Reg. Fraction < >50 EROA (cm 2 ) < >0.40 Zoghbi, et. al. JASE 2003
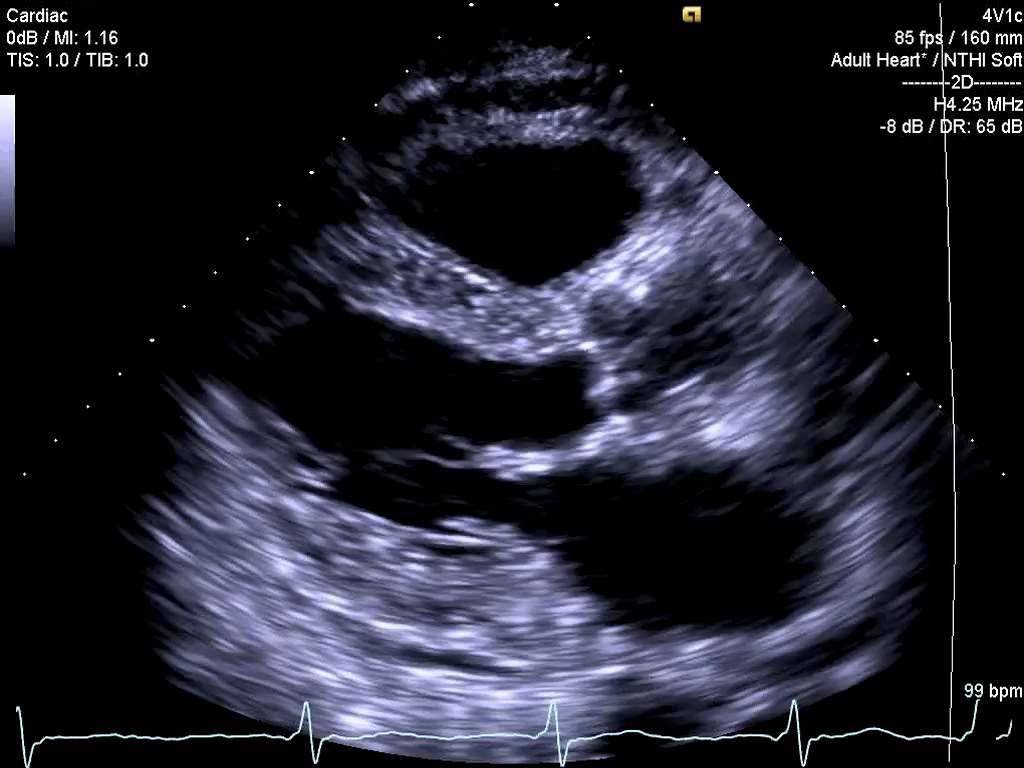
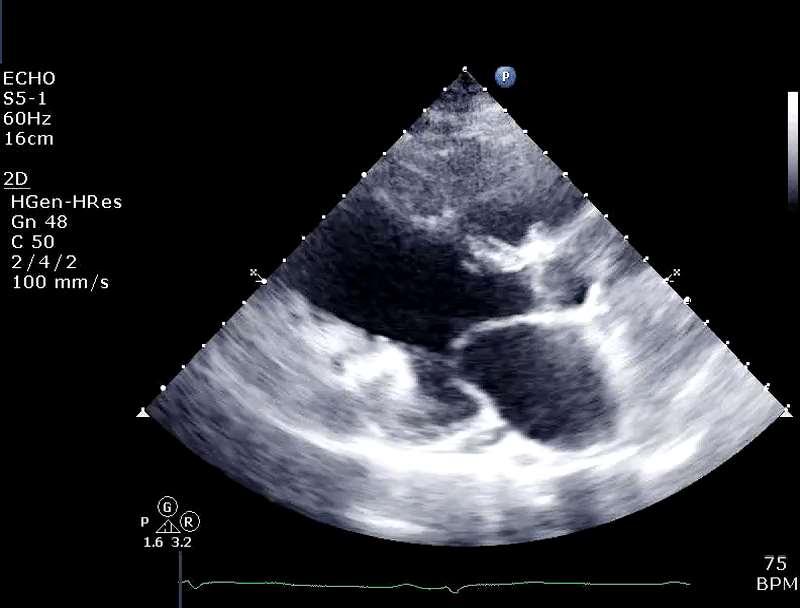
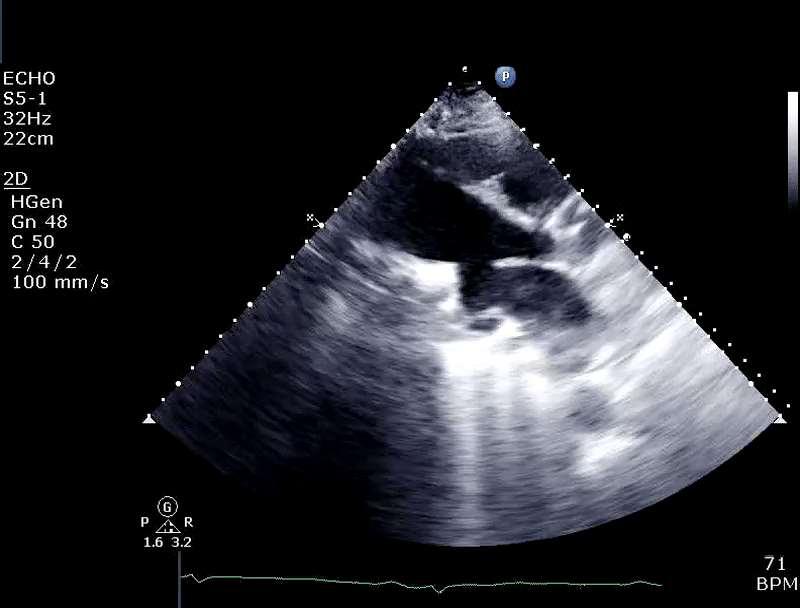
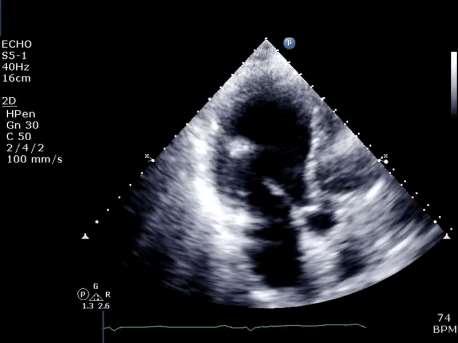
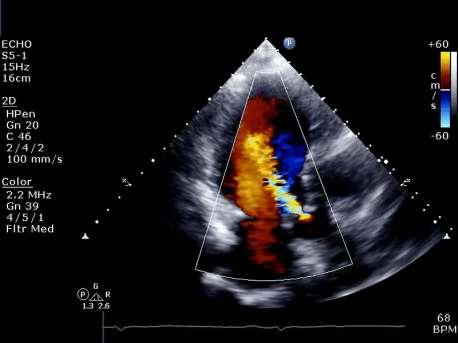
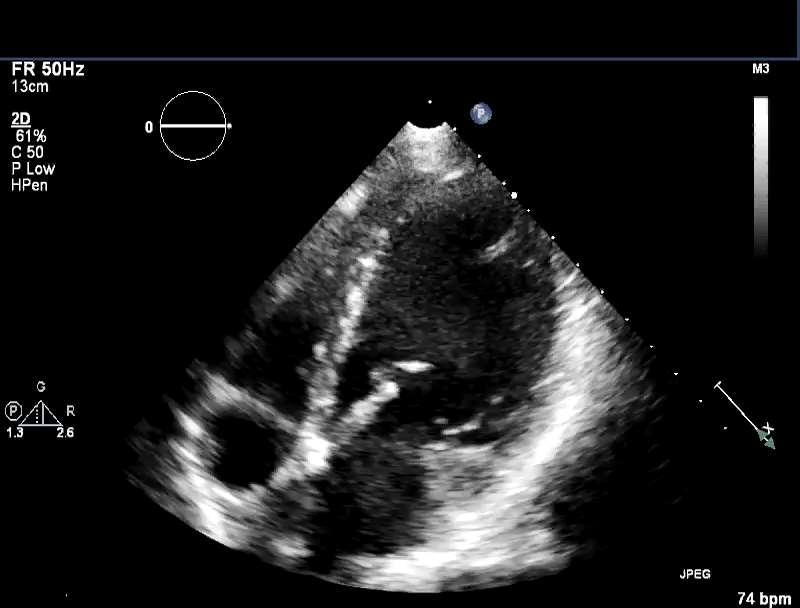
18 Case 175,425,421cn 32 y/o Vietnamese Female lb B/P 105/51 HR 68 Prior MV Repair 18

19 Case 175,425,421cn 19
20 Case 175,425,421cn 20
21 Case 175,425,421cn What kind of MV surgery? a) No surgery b) Ring repair c) Mitral Clip d) Replacement 21
22 Case 175,425,421cn What kind of MV surgery? a) No surgery b) Ring repair c) Mitral Clip d) Replacement 22
23 Case 175,425,421cn 23
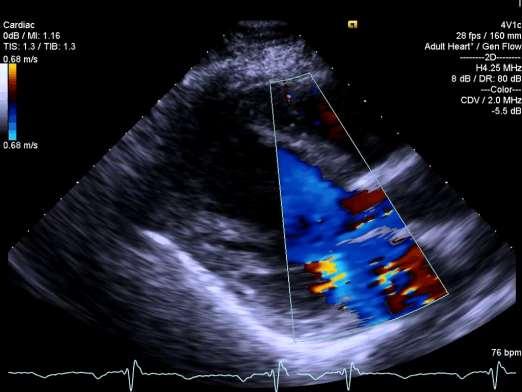
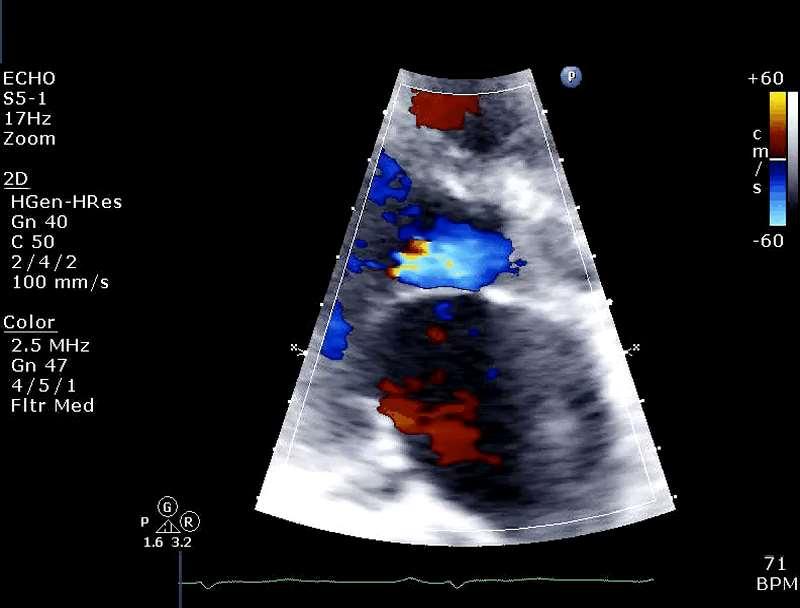
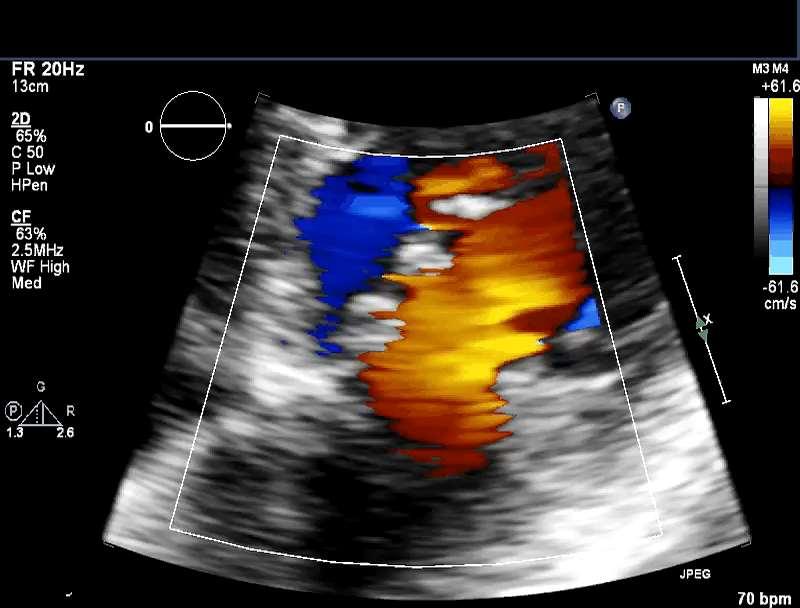
24 Case 175,425,421cn Based on info so far, what is severity? a) Mild b) Moderate c) Severe d) Low Nyquist 24
25 Case 175,425,421cn Based on info so far, what is severity? a) Mild b) Moderate c) Severe d) Low Nyquist 25
26 Case 175,425,421cn What is the estimated vena contracta? a) <0.30 b) c) >0.70 d) Poor image 26
27 Case 175,425,421cn What is the estimated vena contracta? a) < cm b) c) >0.70 d) Poor image 27
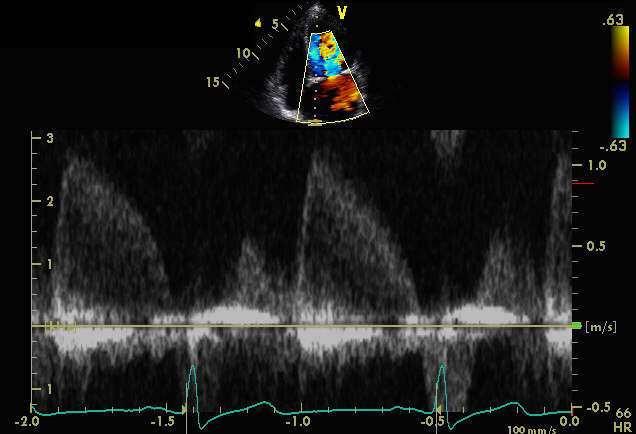
28 Case 175,425,421cn When do you measure? a) Early sys 0.5 b) Mid sys 0.9 c) Late sys
 a) Early sys 0.5 b) Mid sys 0.")
29 Case 175,425,421cn a) When do you measure? b) a) Early sys 0.5 b) Mid sys 0.9 c) c) Late sys
30 Case 175,425,421cn 30
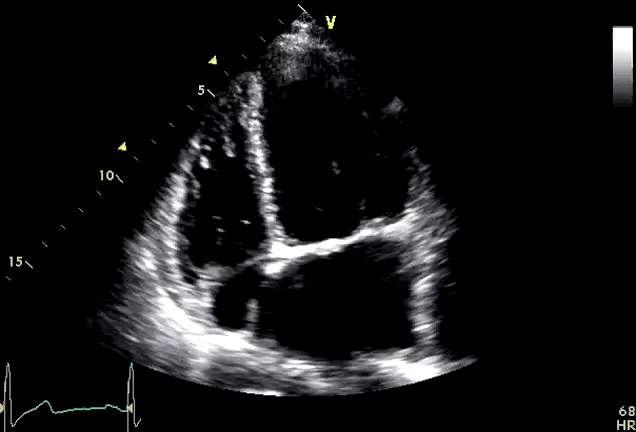
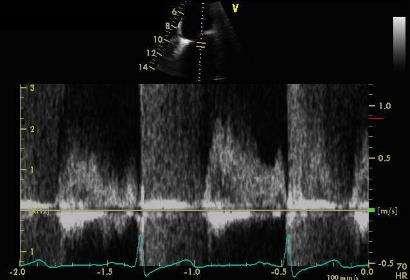
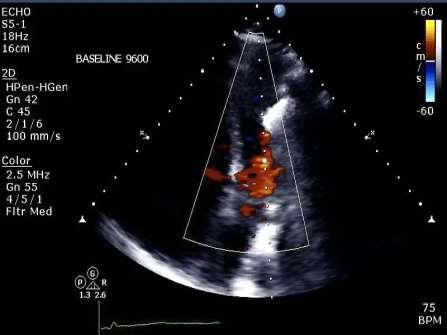
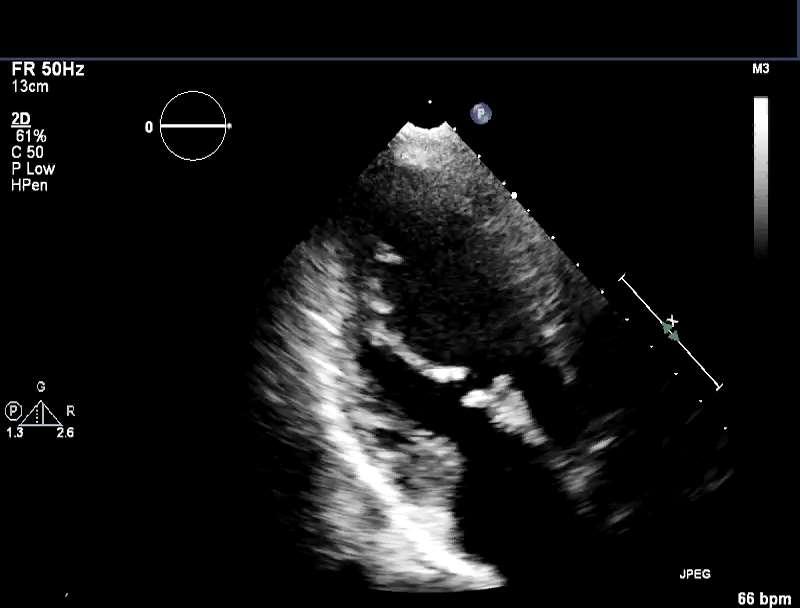
31 Case 175,425,421cn What size is the LA? 130.7ml What about density and shape of Doppler? 31
32 Case 175,425,421cn 32
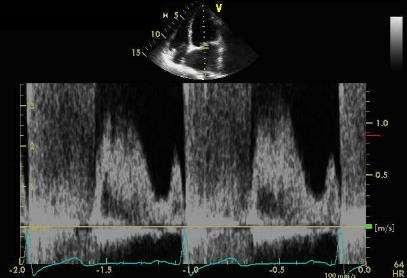
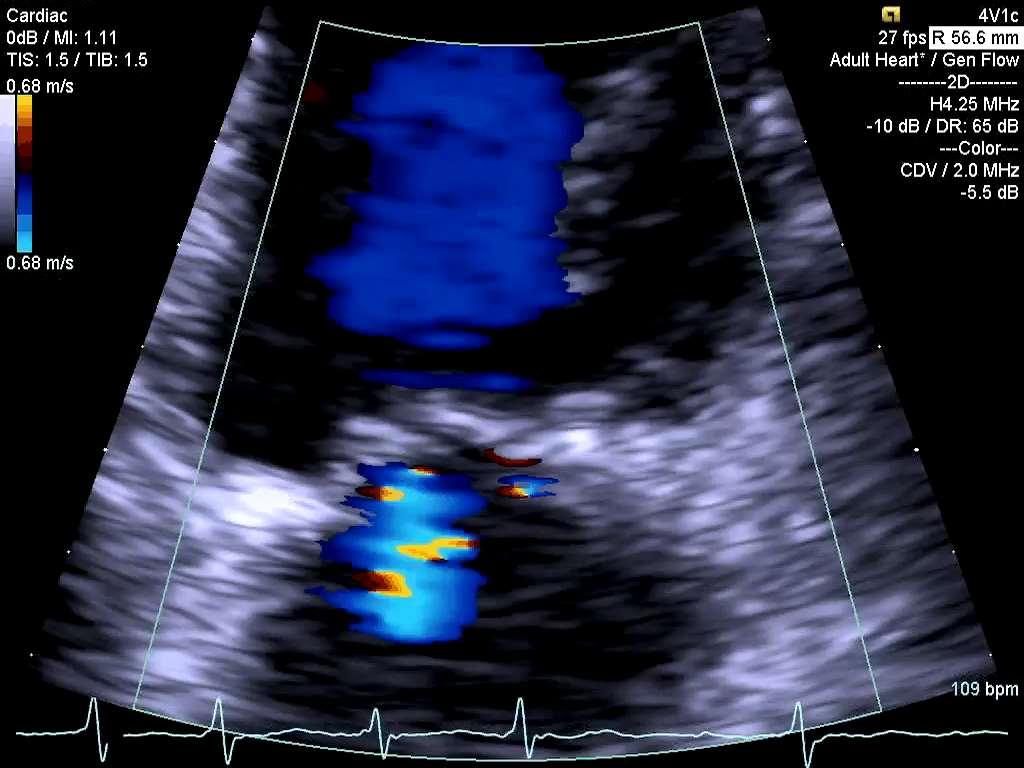
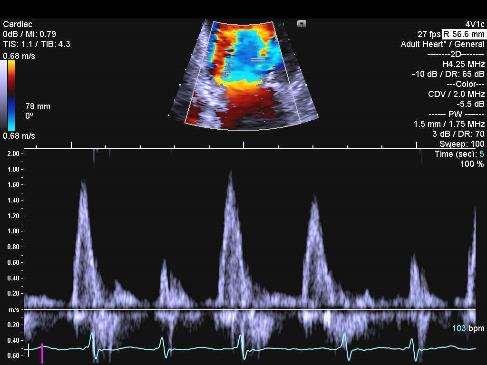
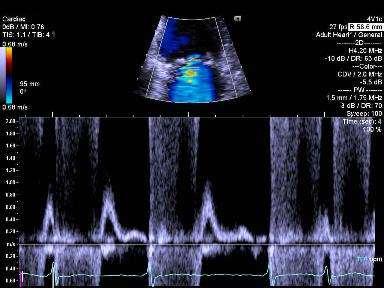
33 Case 175,425,421cn What supportive sign is noted in pulmonary vein flow for significant MR? S D A a) Dominant D wave b) Dominant S wave c) Dominant A wave d) All of the above 33
34 Case 175,425,421cn What supportive sign is noted in pulmonary vein flow for significant MR? S D A a) Dominant D wave b) Dominant S wave c) Dominant A wave d) All of the above 34

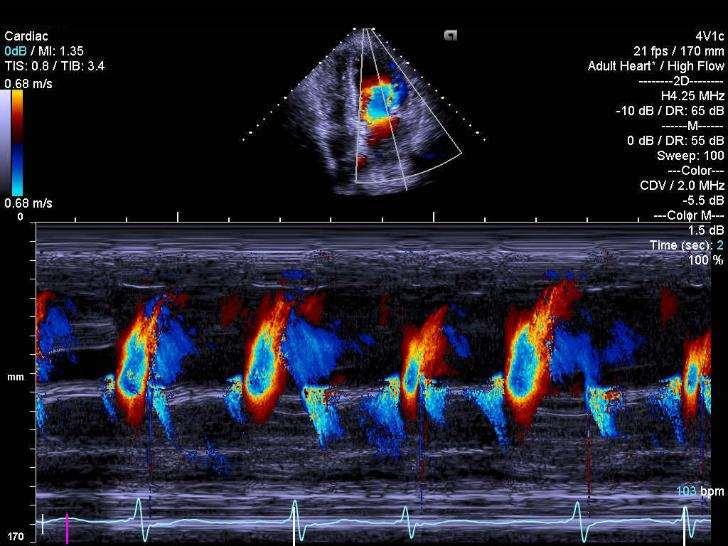
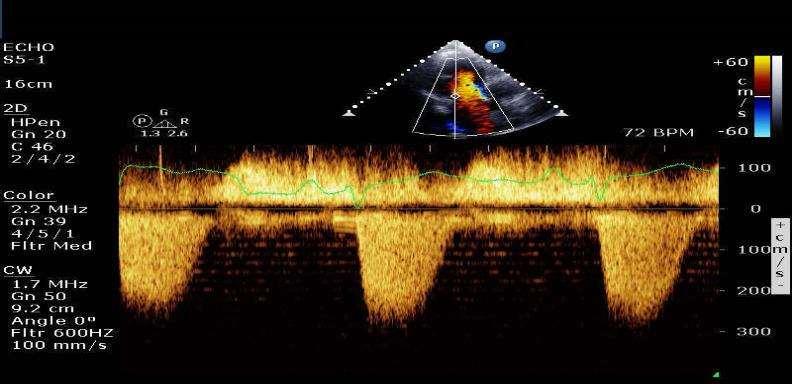
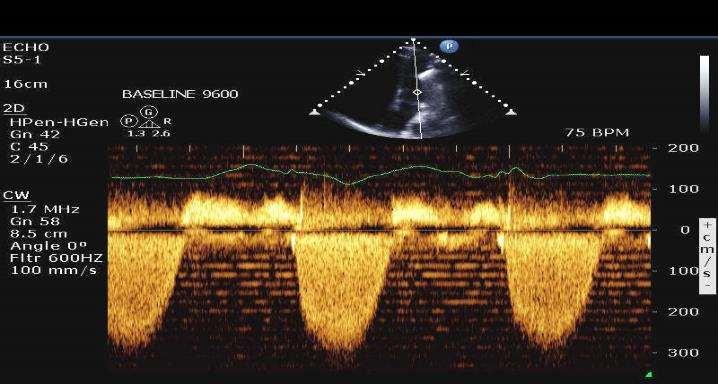
35 Case 175,425,421cn What is the LA pressure? 32 y/o Vietnamese Female lb B/P 105/51 HR 68 Prior MV Repair MV pk Vel 417.4cm/s 35
36 Left Atrial Pressure LAP = SBP 4 X MRV 2 SBP = 105 MRV = 4.2 m/s LAP= X LAP= LAP= MV pk Vel 417.4cm/s SBP = 105
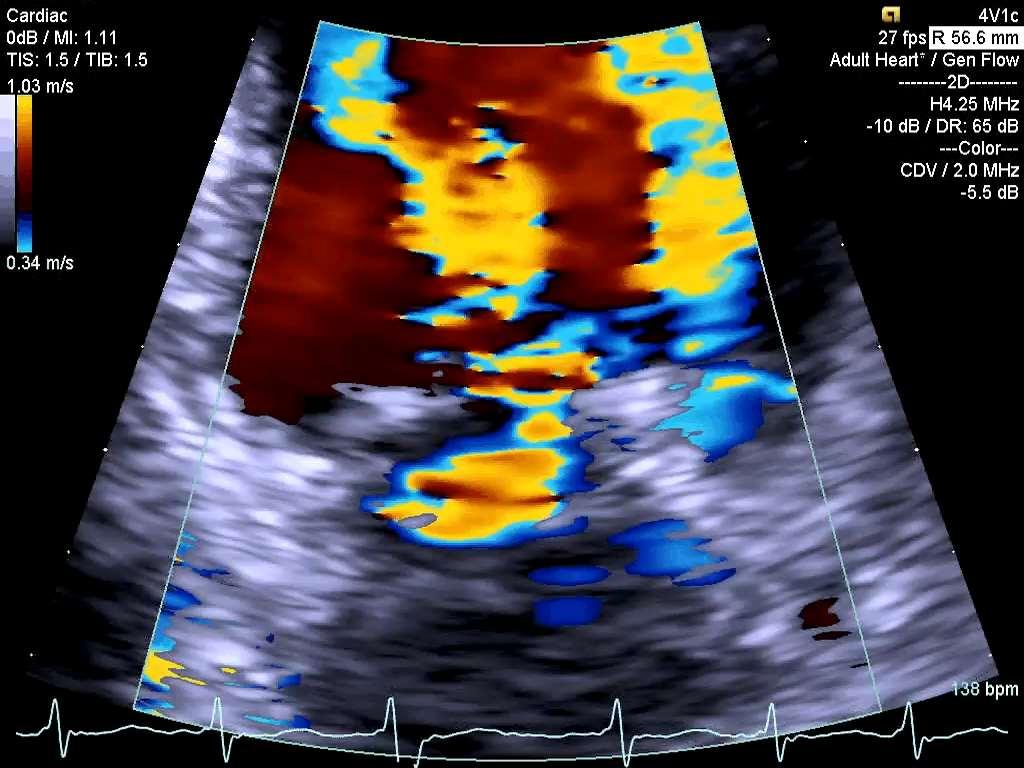
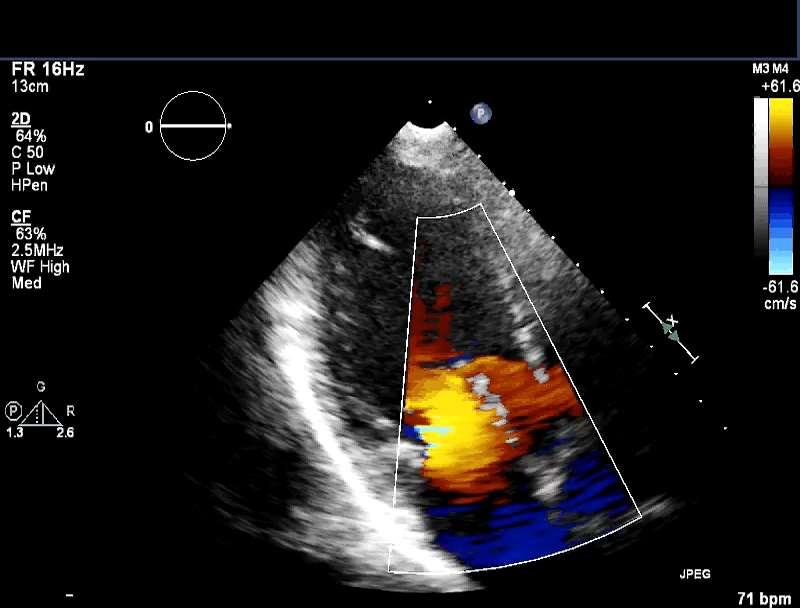
37 Case 175,425,421cn Tips for measuring flow convergence (PISA) 1. Leaflet to 1 st color shift 2. Mid systole 3. Baseline shift 4. Zoom 5. Do often 37

38 PISA Method - 4 Numbers r = 0.9 MR pk Vel = 417 cm/s V r = 38 cm/s MR TVI = 130 cm r=0.9 ERO and RVol


39 PISA Method - 4 Numbers r=0.9 VFR = 2 x x r 2 x V r VFR = 6.28 x.81 x 38 VFR = 193cc/s V MAX 4.17m/s VTI 130 ERO = VFR/V MAX ERO = 193/417.4 ERO = 0.46cm 2 RVol = ERO x VTI RVol = 0.46 x 130 Rvol = 59.8 ml
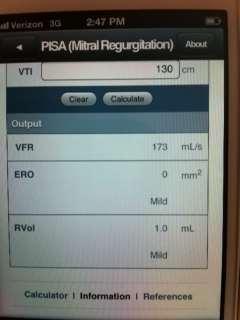



40 Case 175,425,421cn iase app Severe 54 Severe 40
41 Grading MR Qualitative Methods Parameters Mild Moderate Severe Color jet area 4cm 2 or 10% LA Variable >10cm 2 or 40% LA CW Faint/parabolic Dense/para Dense/early peak Pvein flow Sys. dominance Sys. Blunting Systolic reversal MV Inflow Dominant A wave Dominant E >1.2 Quantitive Methods Parameters Mild Moderate Severe Vena Contracta < >0.7 Reg. Volume < >60 Reg. Fraction < >50 EROA (cm 2 ) < >0.40 Zoghbi, et. al. JASE 2003


42 Case 175,425,421cn MA Stroke Volume & CO 42
43 Regurgitant Fraction % RF% = SV (Valve) SV (Systemic) / SV (Valve) VTI 15.8 cm LVOT 1.8 cm MA SV = D 2 x.785 x VTI MA SV = 2.2 x.785 x 25.9 MA SV = 98.4 ml LVOT SV = D 2 x.785 x VTI LVOT SV = 3.24 x.785 x 15.8 LVOT SV = 40.2 ml RF% = MA SV LV SV / MA SV RF% = / 98.4 RF% = 59%
44 Grading MR Qualitative Methods Parameters Mild Moderate Severe Color jet area 4cm 2 or 10% LA Variable >10cm 2 or 40% LA CW Faint/parabolic Dense/para Dense/early peak Pvein flow Sys. dominance Sys. Blunting Systolic reversal Quantitive Methods Parameters Mild Moderate Severe Vena Contracta < >0.7 Reg. Volume < >60 Reg. Fraction < >50 EROA (cm 2 ) < >0.40 Zoghbi, et. al. JASE 2003
45 Case 175,425,421cn Findings for the 32 y/o Vietnamese Female LV function normal RV normal LA Severely enlarged RA normal AV trace AI MV thickened leaflets, surgical ring, severe regurgitation with RF of 59% and estimated Rvol of 58 ml. 45
46 46
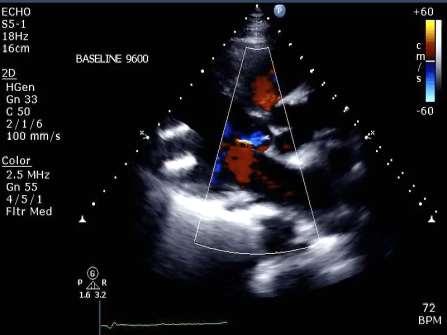
47 Case 176,298,521JH 68 y/o Female lb BSA 1.79 m 2 Primary indication Atrial Fibrillation 47
48 Case 176,298,521JH 48

49 Case 176,298,521JH 49

50 Case 176,298,521JH 50
51 Case 176,298,521JH Based on information so far, what degree is the MR? a) Mild b) Mild to Moderate c) Moderate d) Severe 51
52 Case 176,298,521JH Based on information so far, what degree is the MR? a) Mild b) Mild to Moderate c) Moderate d) Severe 52
53 Case 176,298,521JH Based on vena contracta what is the VC = 0.2 degree of MR? VC = 0.4 a) Mild b) Mild to Moderate c) Moderate d) Severe 53
54 Case 176,298,521JH Based on vena contracta what is the VC = 0.2 degree of MR? VC = 0.4 a) Mild b) Mild to Moderate c) Moderate d) Severe 54
55 Grading MR Qualitative Methods Parameters Mild Moderate Severe Color jet area 4cm 2 or 10% LA Variable >10cm 2 or 40% LA CW Faint/parabolic Dense/para Dense/early peak Pvein flow Sys. dominance Sys. Blunting Systolic reversal MV Inflow Dominant A wave Dominant E >1.2 Quantitive Methods Parameters Mild Moderate Severe Vena Contracta < >0.7 Reg. Volume < >60 Reg. Fraction < >50 EROA (cm 2 ) < >0.40 Zoghbi, et. al. JASE 2003

56 Case 176,298,521JH What size is the LA? 56
57 Case 176,298,521JH What size is the LA? 71.7 ml a) Normal b) Mildly enlarged c) Moderately big d) Severely enlarged 57
 Normal b) Mildly enlarged c) Moderately big d)")
58 Case 176,298,521JH What size is the LA? 71.7 ml a) Normal b) Mildly enlarged c) Moderately big d) Severely enlarged 58
59 Case 176,298,521JH 59
60 Case 176,298,521JH 60
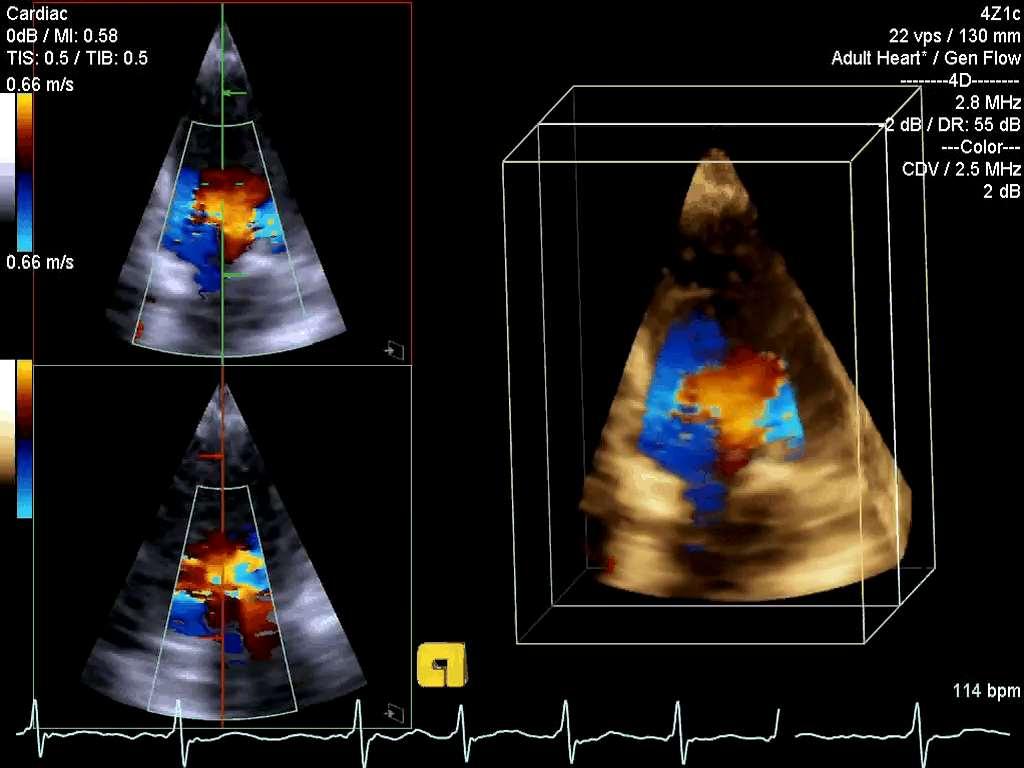
61 Case 176,298,521JH How many MR jets are there?? a) one b) two c) three d) What MR? 61
62 Case 176,298,521JH How many MR jets are there?? a) one b) two c) three d) What MR? 62

63 Case 176,298,521JH 63
64 Case 176,298,521JH 64
65 Case 176,298,521JH 65
66 Case 176,298,521JH 66
67 Case 176,298,521JH MIn Supportive signs include MR PVein S D D S a) Dominant E b) Dense parabolic Doppler c) None of the above d) A & B A 67
68 Case 176,298,521JH MIn Supportive signs include MR PVein S D D S a) Dominant E b) Dense parabolic Doppler c) None of the above d) A & B A 68
69 Grading MR Qualitative/Supportive Methods Parameters Mild Moderate Severe Color jet area 4cm 2 or 10% LA Variable >10cm 2 or 40% LA CW Faint/parabolic Dense/para Dense/early peak Pvein flow Sys. dominance Sys. Blunting Systolic reversal MV Inflow Dominant A wave Dominant E >1.2 Quantitative Methods Parameters Mild Moderate Severe Vena Contracta < >0.7 Reg. Volume < >60 Reg. Fraction < >50 EROA (cm 2 ) < >0.40 Zoghbi, et. al. JASE 2003
70 Case 176,298,521JH 70
71 Case 176,298,521JH 71


72 PISA Method - 4 Numbers r=0.4 VFR = 2 x x r 2 x V r VFR = 6.28 x.16 x 34 VFR = 34 cc/s V MAX 5 m/s ERO = VFR/V MAX ERO = 34/500 ERO = 0.068cm 2 Easy PISA = 0.38 x r 2 ERO = 0.38 X 0.16 ERO = 0.06cm 2
73 Grading MR Qualitative Methods Parameters Mild Moderate Severe Color jet area 4cm 2 or 10% LA Variable >10cm 2 or 40% LA CW Faint/parabolic Dense/para Dense/early peak Pvein flow Sys. dominance Sys. Blunting Systolic reversal MV Inflow Dominant A wave Dominant E >1.2 Quantitive Methods Parameters Mild Moderate Severe Vena Contracta < >0.7 Reg. Volume < >60 Reg. Fraction < >50 EROA (cm 2 ) < >0.40 Zoghbi, et. al. JASE 2003
74 Case 176,298,521JH Findings for the 68 y/o female LV size normal, mild/mod LVH, fx lower limits of normal RV size normal and mildly depressed LA mod to severely enlarged RA mildly enlarged Small PE AV mild calcification with trace AI MV no structural abnormalities with mild to moderate regurgitation 74
75 Case 185,425,421cj 59 y/o female Primary diagnosis CHF lb BSA 1.92 B/P 70/00 75
76 Case 185,425,421cj 76
77 Case 185,425,421cj 77
78 Case 185,425,421cj What do you think about the valves? 78
79 Case 185,425,421 79
80 Case 185,425,421 80
81 Case 185,425,421cj 59 y/o female Primary diagnosis CHF lb BSA 1.92 B/P 70/00 Heartmate II LVAD insertion 9/28/2010 LVAD misalignment 81
82 Case 185,425,421 After LVAD adjustment 82





83 Case 185,425,421 Heartmate II 83

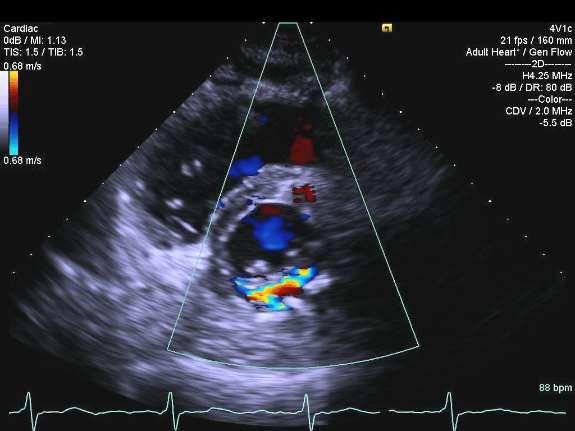
84 Case 546,222,333RR 57 y/o female Primary diagnosis mitral regurgitation 65 in 113 lb BSA 1.55 B/P 110/77 84
85 Case 546,222,333RR 85

86 Case 546,222,333RR 86
87 Case 546,222,333RR What is the estimated vena contracta? a) <0.30 b) c) >0.70 d) Too eccentric to estimate 87
88 Case 546,222,333RR What is the estimated vena contracta? VC 1.4cm a) <0.30 b) c) >0.70 d) Too eccentric to estimate 88
89 Grading MR Qualitative/Supportive Methods Parameters Mild Moderate Severe Color jet area 4cm 2 or 10% LA Variable >10cm 2 or 40% LA CW Faint/parabolic Dense/para Dense/early peak Pvein flow Sys. dominance Sys. Blunting Systolic reversal MV Inflow Dominant A wave Dominant E >1.2 Quantitative Methods Parameters Mild Moderate Severe Vena Contracta < >0.7 Reg. Volume < >60 Reg. Fraction < >50 EROA (cm 2 ) < >0.40 Zoghbi, et. al. JASE 2003
90 Case 546,222,333RR 90
91 Case 546,222,333RR 91
 Normal b) Mildly enlarged c) Moderately big d)")
92 Case 546,222,333RR What size is the LA? a) Normal b) Mildly enlarged c) Moderately big d) Severely enlarged 92
 Normal b) Mildly enlarged c) Moderately big d) Severely")
93 Case 546,222,333RR What size is the LA? LA Vol = 89.6 ml a) Normal b) Mildly enlarged c) Moderately big d) Severely enlarged 93
 Normal b) Mildly enlarged c) Moderately big d) Severely")
94 Case 546,222,333RR What size is the LA? LA Vol = 89.6 ml a) Normal b) Mildly enlarged c) Moderately big d) Severely enlarged 94
95 Case 546,222,333RR 95

96 Case 546,222,333RR 96


97 Case 546,222,333RR What do you think about these Doppler tracings? 97

98 Case 546,222,333RR What do you think about these Doppler tracings? 98
99 Grading MR Qualitative/Supportive Methods Parameters Mild Moderate Severe Color jet area 4cm 2 or 10% LA Variable >10cm 2 or 40% LA CW Faint/parabolic Dense/para Dense/early peak Pvein flow Sys. dominance Sys. Blunting Systolic reversal MV Inflow Dominant A wave Dominant E >1.2 Quantitative Methods Parameters Mild Moderate Severe Vena Contracta < >0.7 Reg. Volume < >60 Reg. Fraction < >50 EROA (cm 2 ) < >0.40 Zoghbi, et. al. JASE 2003

100 Specific Signs Mild Small central jet <4 cm 2 or <20% of LA Vena contracta width <0.3cm No or minimal flow convergence Moderate Signs of MR > Mild but no criteria for severe MR Severe Vena contracta width >0.7cm Large flow convergence Systolic reversal in pulmonary veins Prominent flail MV leaflet of ruptured papillary muscle Zoghbi, et. al. JASE 2003
101 Supportive Signs Mild Systolic dominant flow in pulmonary veins A-wave dominant mitral inflow Soft density, parabolic CW Doppler MR signal Normal LV size Moderate Intermediate signs/findings Severe Dense, triangular CW Doppler MR jet (early peaking) E-wave dominant mitral inflow (E > 1.2 m/s) Enlarged LV Enlarged LA Zoghbi, et. al. JASE 2003

102 Regurgitant Fraction % RF% = SV (Valve) SV (Systemic) / SV (Valve) MA ann 3 cm VTI 18.5 cm MA SV = D 2 x.785 x VTI MA SV = 9 x.785 x 18.5 MA SV = ml LVOT SV = D 2 x.785 x VTI

103 Regurgitant Fraction % RF% = SV (Valve) SV (Systemic) / SV (Valve) VTI 13.1 cm LVOT 2.3 cm MA SV = D 2 x.785 x VTI MA SV = 9 x.785 x 18.5 MA SV = 130 ml LVOT SV = D 2 x.785 x VTI LVOT SV = 5.3 x.785 x 13.1 LVOT SV = 54.5 ml RF% = MA SV LV SV / MA SV RF% = / 130 RF% = 58% RVol = = 76 ml
104 Grading MR Qualitative/Supportive Methods Parameters Mild Moderate Severe Color jet area 4cm 2 or 10% LA Variable >10cm 2 or 40% LA CW Faint/parabolic Dense/para Dense/early peak Pvein flow Sys. dominance Sys. Blunting Systolic reversal MV Inflow Dominant A wave Dominant E >1.2 Quantitative Methods Parameters Mild Moderate Severe Vena Contracta < >0.7 Reg. Volume < >60 Reg. Fraction < >50 EROA (cm 2 ) < >0.40 Zoghbi, et. al. JASE 2003

105 Case 546,222,333RR Findings LV size is enlarged, overall fx normal RV size is normal with normal fx LA severely enlarged RA normal MV barlows and prolapsed. Severe regurgitation with an estimated RF of 58% and a Rvol of 76ml. 105
106 Test Time What are the 2 views/images needed for PISA? a) Subcostal and parasternal b) Zoom color 4 chamber and MR cw Doppler c) Parasternal and color M-Mode d) Zoom color 4 chamber and MR cw Doppler
107 Test Time What are the 2 views/images needed for PISA? a) Subcostal and parasternal b) Zoom color 4 chamber and MR cw Doppler c) Parasternal and color M-Mode d) Zoom color 4 chamber and MR cw Doppler
108 Test Time What 4 #/measurements do you need for PISA? a) Baseline shift, lvot vel, lvot TVI, prox flow convergence b) Baseline shift, pulm vein flow, lvot TVI, prox flow convergence c) Baseline shift, MR vel, MR TVI, prox flow convergence d) Lvot diam, lvot vel, lvot TVI, prox flow convergence
109 Test Time What 4 #/measurements do you need for PISA? a) Baseline shift, lvot vel, lvot TVI, prox flow convergence b) Baseline shift, pulm vein flow, lvot TVI, prox flow convergence c) Baseline shift, MR vel, MR TVI, prox flow convergence d) Lvot diam, lvot vel, lvot TVI, prox flow convergence
110 Test Time Which of the following best describes the vena contracta? a) The vena contracta is too hard to do on a daily basis to accurately define MR b) The vena contracta is relatively simple and accurate for identifying mild and severe MR c) The vena contracta is a vasospasm in the descending vein of marshal and not related to MR d) The vena contracta is only used for PISA
111 Test Time Which of the following best describes the vena contracta? a) The vena contracta is too hard to do on a daily basis to accurately define MR b) The vena contracta is relatively simple and accurate for identifying mild and severe MR c) The vena contracta is a vasospasm in the descending vein of marshal and not related to MR d) The vena contracta is only used for PISA
112 Pearls and Pitfalls Practice, Practice, Practice Are you really good at something you only do every now and then? Specific signs in conjunction with the supportive signs renders a > 90% specificity Nyquist limit must be greater than 54cm/s The process of grading MR should be comprehensive, using clues and and measurements by Doppler echocardiography

113 Thank you!



114 Texas Medical Center 5 million pt s Pre-stress test 114

115 115
Professors Carpentier and McGoon Mechanism, resulting from the disease Severity of regurgitation, resulting from the mechanism Echo
 Professors Carpentier and McGoon Mechanism, resulting from the disease Severity of regurgitation, resulting from the mechanism Echo define the mechanism, quantify the regurgitation severity CP1293058-3
Professors Carpentier and McGoon Mechanism, resulting from the disease Severity of regurgitation, resulting from the mechanism Echo define the mechanism, quantify the regurgitation severity CP1293058-3
ASE Guidelines on Aortic Regurgitation What Do I Measure? Case Studies
 ASE Guidelines on Aortic Regurgitation What Do I Measure? Case Studies Mitral Regurgitation The New ASE Guidelines: Role of 2D/3D and CMR William A. Zoghbi MD, FASE, MACC Professor and Chairman, Department
ASE Guidelines on Aortic Regurgitation What Do I Measure? Case Studies Mitral Regurgitation The New ASE Guidelines: Role of 2D/3D and CMR William A. Zoghbi MD, FASE, MACC Professor and Chairman, Department
New 3D Quantification of Mitral Regurgitation Severity. Judy Hung, MD Cardiac Ultrasound Laboratory Massachusetts General Hospital Boston, MA
 New 3D Quantification of Mitral Regurgitation Severity Judy Hung, MD Cardiac Ultrasound Laboratory Massachusetts General Hospital Boston, MA No Financial Disclosures No off label discussion of devices
New 3D Quantification of Mitral Regurgitation Severity Judy Hung, MD Cardiac Ultrasound Laboratory Massachusetts General Hospital Boston, MA No Financial Disclosures No off label discussion of devices
Valvular Regurgitation: Can We Do Better Than Colour Doppler?
 Valvular Regurgitation: Can We Do Better Than Colour Doppler? A/Prof David Prior St Vincent s Hospital Melbourne Sports Cardiology Valvular Regurgitation Valve regurgitation volume loads the ventricles
Valvular Regurgitation: Can We Do Better Than Colour Doppler? A/Prof David Prior St Vincent s Hospital Melbourne Sports Cardiology Valvular Regurgitation Valve regurgitation volume loads the ventricles
Disclosures Rebecca T. Hahn, MD, FASE
 The New ASE Guidelines for Native Valvular Regurgitation Mitral Regurgitation The New ASE Guidelines: Role of 2D/3D and CMR (With caveats and comments from R. Hahn) William A. Zoghbi MD, FASE, MACC Professor
The New ASE Guidelines for Native Valvular Regurgitation Mitral Regurgitation The New ASE Guidelines: Role of 2D/3D and CMR (With caveats and comments from R. Hahn) William A. Zoghbi MD, FASE, MACC Professor
How to assess ischaemic MR?
 ESC 2012 How to assess ischaemic MR? Luc A. Pierard, MD, PhD, FESC, FACC Professor of Medicine Head, Department of Cardiology University Hospital Sart Tilman, Liège ESC 2012 No conflict of interest Luc
ESC 2012 How to assess ischaemic MR? Luc A. Pierard, MD, PhD, FESC, FACC Professor of Medicine Head, Department of Cardiology University Hospital Sart Tilman, Liège ESC 2012 No conflict of interest Luc
What are the best diagnostic tools to quantify aortic regurgitation?
 What are the best diagnostic tools to quantify aortic regurgitation? Agnès Pasquet, MD, PhD Pôle de Recherche Cardiovasculaire Institut de Recherche Expérimentale et Clinique Université catholique de Louvain
What are the best diagnostic tools to quantify aortic regurgitation? Agnès Pasquet, MD, PhD Pôle de Recherche Cardiovasculaire Institut de Recherche Expérimentale et Clinique Université catholique de Louvain
PISA Evaluation of Mitral Regurgitation. Raymond Graber, MD Cardiac Anesthesia Group University Hospitals Case Medical Center 4/07/2011
 PISA Evaluation of Mitral Regurgitation Raymond Graber, MD Cardiac Anesthesia Group University Hospitals Case Medical Center 4/07/2011 Introduction Evaluation of MR. What is PISA? Physiologic basis Issues
PISA Evaluation of Mitral Regurgitation Raymond Graber, MD Cardiac Anesthesia Group University Hospitals Case Medical Center 4/07/2011 Introduction Evaluation of MR. What is PISA? Physiologic basis Issues
Prof. JL Zamorano Hospital Universitario Ramón y Cajal
 Prof. JL Zamorano Hospital Universitario Ramón y Cajal Should we forget TR? Nath J et al. Impact of tricuspid regurgitation on long-term survival. J Am Coll Cardiol. 2004; 43:405-409 Why is it difficult
Prof. JL Zamorano Hospital Universitario Ramón y Cajal Should we forget TR? Nath J et al. Impact of tricuspid regurgitation on long-term survival. J Am Coll Cardiol. 2004; 43:405-409 Why is it difficult
EVALUATION OF CHRONIC MITRAL REGURGITATION: ASSESSING MECHANISMS AND QUANTIFYING SEVERITY 2018 STRUCTURAL HEART DISEASE CONFERENCE June 1, 2018
 1 EVALUATION OF CHRONIC MITRAL REGURGITATION: ASSESSING MECHANISMS AND QUANTIFYING SEVERITY 2018 STRUCTURAL HEART DISEASE CONFERENCE June 1, 2018 David A. Orsinelli, MD, FACC, FASE Professor, Internal
1 EVALUATION OF CHRONIC MITRAL REGURGITATION: ASSESSING MECHANISMS AND QUANTIFYING SEVERITY 2018 STRUCTURAL HEART DISEASE CONFERENCE June 1, 2018 David A. Orsinelli, MD, FACC, FASE Professor, Internal
Quantification of Aortic Regurgitation
 Quantification of Aortic Regurgitation ASE Review 2018 Boston Susan E Wiegers, MD, FASE, FACC Professor of Medicine And thanks to Dr. Roberto Lang Disclosure None related to this presentation 1 Objectives
Quantification of Aortic Regurgitation ASE Review 2018 Boston Susan E Wiegers, MD, FASE, FACC Professor of Medicine And thanks to Dr. Roberto Lang Disclosure None related to this presentation 1 Objectives
MR echo case. N.Koutsogiannis Department of Cardiology University Hospital Of Patras
 MR echo case N.Koutsogiannis Department of Cardiology University Hospital Of Patras Case A 35 years old male came to the echo lab for a third opinion for his valvulopathy. He reports a long standing MR
MR echo case N.Koutsogiannis Department of Cardiology University Hospital Of Patras Case A 35 years old male came to the echo lab for a third opinion for his valvulopathy. He reports a long standing MR
Echocardiography. Guidelines for Valve and Chamber Quantification. In partnership with
 Echocardiography Guidelines for Valve and Chamber Quantification In partnership with Explanatory note & references These guidelines have been developed by the Education Committee of the British Society
Echocardiography Guidelines for Valve and Chamber Quantification In partnership with Explanatory note & references These guidelines have been developed by the Education Committee of the British Society
The difficult patient with mitral regurgitation
 Clinical pathways The difficult patient with mitral regurgitation Stress echo can be the best tool Challenging cases Maria João Andrade, Lisbon PT Management of Severe Chronic Organic MR Echo Exercise
Clinical pathways The difficult patient with mitral regurgitation Stress echo can be the best tool Challenging cases Maria João Andrade, Lisbon PT Management of Severe Chronic Organic MR Echo Exercise
CHAPTER 4 AN EFFICACIOUS APPROACH FOR THE QUANTIFICATION OF MITRAL REGURGITATION USING IMAGE PROCESSING AND PROXIMAL FLOW CONVERGENCE METHOD
 CHAPTER 4 AN EFFICACIOUS APPROACH FOR THE QUANTIFICATION OF MITRAL REGURGITATION USING IMAGE PROCESSING AND PROXIMAL FLOW CONVERGENCE METHOD 4.1. Introduction Mitral Regurgitation also called Mitral Insufficiency
CHAPTER 4 AN EFFICACIOUS APPROACH FOR THE QUANTIFICATION OF MITRAL REGURGITATION USING IMAGE PROCESSING AND PROXIMAL FLOW CONVERGENCE METHOD 4.1. Introduction Mitral Regurgitation also called Mitral Insufficiency
Quantification of MR
 Valvular Regurgitation: Putting the New Guidelines into Practice James D. Thomas, MD, FACC, FASE, FESC Director, Center for Heart Valve Disease Bluhm Cardiovascular Institute Professor of Medicine, Feinberg
Valvular Regurgitation: Putting the New Guidelines into Practice James D. Thomas, MD, FACC, FASE, FESC Director, Center for Heart Valve Disease Bluhm Cardiovascular Institute Professor of Medicine, Feinberg
Echocardiography: Guidelines for Valve Quantification
 Echocardiography: Guidelines for Echocardiography: Guidelines for Chamber Quantification British Society of Echocardiography Education Committee Richard Steeds (Chair), Gill Wharton (Lead Author), Jane
Echocardiography: Guidelines for Echocardiography: Guidelines for Chamber Quantification British Society of Echocardiography Education Committee Richard Steeds (Chair), Gill Wharton (Lead Author), Jane
Quantitation of Aortic Regurgitation ASCeXAM / ReASCE Review Course
 Quantitation of Aortic Regurgitation 2017 ASCeXAM / ReASCE Review Course David Adams, ACS, RCS, RDCS, FASE Duke University Medical Center May 1, 2017 Disclosures None 1 Exam based on: Zoghbi et al. JASE
Quantitation of Aortic Regurgitation 2017 ASCeXAM / ReASCE Review Course David Adams, ACS, RCS, RDCS, FASE Duke University Medical Center May 1, 2017 Disclosures None 1 Exam based on: Zoghbi et al. JASE
LUST trial. Echocardiography USER S MANUAL
 LUST trial Echocardiography USER S MANUAL Rosa Sicari, Luna Gargani Ins1tute of Clinical Physiology Na1onal Council of Research, Pisa, Italy Parameters required (1) Aortic root Measurement of aortic root
LUST trial Echocardiography USER S MANUAL Rosa Sicari, Luna Gargani Ins1tute of Clinical Physiology Na1onal Council of Research, Pisa, Italy Parameters required (1) Aortic root Measurement of aortic root
Case Reviews: Hemodynamic Calculations in Valvular Regurgitation
 Case Reviews: Hemodynamic Calculations in Valvular Regurgitation Case 5 History: 69-year-old man with orthotopic heart transplant 15 years ago. Inferior MI several years ago. Recurrent CHF. Currently dyspneic
Case Reviews: Hemodynamic Calculations in Valvular Regurgitation Case 5 History: 69-year-old man with orthotopic heart transplant 15 years ago. Inferior MI several years ago. Recurrent CHF. Currently dyspneic
Regurgitant Lesions. Bicol Hospital, Legazpi City, Philippines July Gregg S. Pressman MD, FACC, FASE Einstein Medical Center Philadelphia, USA
 Regurgitant Lesions Bicol Hospital, Legazpi City, Philippines July 2016 Gregg S. Pressman MD, FACC, FASE Einstein Medical Center Philadelphia, USA Aortic Insufficiency Valve anatomy and function LVOT and
Regurgitant Lesions Bicol Hospital, Legazpi City, Philippines July 2016 Gregg S. Pressman MD, FACC, FASE Einstein Medical Center Philadelphia, USA Aortic Insufficiency Valve anatomy and function LVOT and
MITRAL REGURGITATION ECHO PARAMETERS TOOL
 Comprehensive assessment of qualitative and quantitative parameters, along with the use of standardized nomenclature when reporting echocardiographic findings, helps to better define a patient s MR and
Comprehensive assessment of qualitative and quantitative parameters, along with the use of standardized nomenclature when reporting echocardiographic findings, helps to better define a patient s MR and
The Doppler Examination. Katie Twomley, MD Wake Forest Baptist Health - Lexington
 The Doppler Examination Katie Twomley, MD Wake Forest Baptist Health - Lexington OUTLINE Principles/Physics Use in valvular assessment Aortic stenosis (continuity equation) Aortic regurgitation (pressure
The Doppler Examination Katie Twomley, MD Wake Forest Baptist Health - Lexington OUTLINE Principles/Physics Use in valvular assessment Aortic stenosis (continuity equation) Aortic regurgitation (pressure
Hemodynamic Assessment. Assessment of Systolic Function Doppler Hemodynamics
 Hemodynamic Assessment Matt M. Umland, RDCS, FASE Aurora Medical Group Milwaukee, WI Assessment of Systolic Function Doppler Hemodynamics Stroke Volume Cardiac Output Cardiac Index Tei Index/Index of myocardial
Hemodynamic Assessment Matt M. Umland, RDCS, FASE Aurora Medical Group Milwaukee, WI Assessment of Systolic Function Doppler Hemodynamics Stroke Volume Cardiac Output Cardiac Index Tei Index/Index of myocardial
Quantifying Aortic Regurgitation
 Quantifying Aortic Regurgitation Linda D. Gillam, MD, MPH Morristown Medical Center Dorothy and Lloyd Huck Chair Cardiovascular Medicine Atlantic Health System No Disclosures 1 Valve Dysfunction Functional
Quantifying Aortic Regurgitation Linda D. Gillam, MD, MPH Morristown Medical Center Dorothy and Lloyd Huck Chair Cardiovascular Medicine Atlantic Health System No Disclosures 1 Valve Dysfunction Functional
DOPPLER HEMODYNAMICS (1) QUANTIFICATION OF PRESSURE GRADIENTS and INTRACARDIAC PRESSURES
 QUANTIFICATION OF PRESSURE GRADIENTS and INTRACARDIAC PRESSURES") THORAXCENTRE DOPPLER HEMODYNAMICS (1) QUANTIFICATION OF PRESSURE GRADIENTS and INTRACARDIAC PRESSURES J. Roelandt DOPPLER HEMODYNAMICS Intracardiac pressures and pressure gradients Volumetric measurement
THORAXCENTRE DOPPLER HEMODYNAMICS (1) QUANTIFICATION OF PRESSURE GRADIENTS and INTRACARDIAC PRESSURES J. Roelandt DOPPLER HEMODYNAMICS Intracardiac pressures and pressure gradients Volumetric measurement
HEMODYNAMIC ASSESSMENT
 HEMODYNAMIC ASSESSMENT INTRODUCTION Conventionally hemodynamics were obtained by cardiac catheterization. It is possible to determine the same by echocardiography. Methods M-mode & 2D echo alone can provide
HEMODYNAMIC ASSESSMENT INTRODUCTION Conventionally hemodynamics were obtained by cardiac catheterization. It is possible to determine the same by echocardiography. Methods M-mode & 2D echo alone can provide
Imaging MV. Jeroen J. Bax Leiden University Medical Center The Netherlands Davos, feb 2015
 Imaging MV Jeroen J. Bax Leiden University Medical Center The Netherlands Davos, feb 2015 MV/MR: information needed on.. 1. MV anatomy 2. MR etiology - primary vs secondary 3. MR severity quantification
Imaging MV Jeroen J. Bax Leiden University Medical Center The Netherlands Davos, feb 2015 MV/MR: information needed on.. 1. MV anatomy 2. MR etiology - primary vs secondary 3. MR severity quantification
Doppler Basic & Hemodynamic Calculations
 Doppler Basic & Hemodynamic Calculations August 19, 2017 Smonporn Boonyaratavej MD Division of Cardiology, Department of Medicine Chulalongkorn University Cardiac Center, King Chulalongkorn Memorial Hospital
Doppler Basic & Hemodynamic Calculations August 19, 2017 Smonporn Boonyaratavej MD Division of Cardiology, Department of Medicine Chulalongkorn University Cardiac Center, King Chulalongkorn Memorial Hospital
Diastolic Heart Function: Applying the New Guidelines Case Studies
 Diastolic Heart Function: Applying the New Guidelines Case Studies Mitral Regurgitation The New ASE William Guidelines: A. Zoghbi Role MD, of FASE, 2D/3D MACCand CMR Professor and Chairman, Department
Diastolic Heart Function: Applying the New Guidelines Case Studies Mitral Regurgitation The New ASE William Guidelines: A. Zoghbi Role MD, of FASE, 2D/3D MACCand CMR Professor and Chairman, Department
ECHOCARDIOGRAPHY DATA REPORT FORM
 Patient ID Patient Study ID AVM - - Date of form completion / / 20 Initials of person completing the form mm dd yyyy Study period Preoperative Postoperative Operative 6-month f/u 1-year f/u 2-year f/u
Patient ID Patient Study ID AVM - - Date of form completion / / 20 Initials of person completing the form mm dd yyyy Study period Preoperative Postoperative Operative 6-month f/u 1-year f/u 2-year f/u
Ioannis Alexanian, MD, PhD Department of Cardiology General Hospital of Chest Diseases Sotiria Athens
 MITRAL REGURGITATION IN PATIENT WITH SEVERE AORTIC VALVE STENOSIS Ioannis Alexanian, MD, PhD Department of Cardiology General Hospital of Chest Diseases Sotiria Athens I HAVE NOTHING TO DECLARE Management
MITRAL REGURGITATION IN PATIENT WITH SEVERE AORTIC VALVE STENOSIS Ioannis Alexanian, MD, PhD Department of Cardiology General Hospital of Chest Diseases Sotiria Athens I HAVE NOTHING TO DECLARE Management
Guidelines in perspective?
 EuroValve 2016 Challenges in the management Secondary MR Guidelines in perspective? Luc A. Pierard, MD, PhD Professor of Medicine Head of the Department of Cardiology, Liège, Belgium Heart Valve Clinic,
EuroValve 2016 Challenges in the management Secondary MR Guidelines in perspective? Luc A. Pierard, MD, PhD Professor of Medicine Head of the Department of Cardiology, Liège, Belgium Heart Valve Clinic,
Normal TTE/TEE Examinations
 Normal TTE/TEE Examinations Geoffrey A. Rose, MD FACC FASE Sanger Heart & Vascular Institute Before you begin imaging... Obtain the patient s Height Weight BP PLAX View PLAX View Is apex @ 9-10 o clock?
Normal TTE/TEE Examinations Geoffrey A. Rose, MD FACC FASE Sanger Heart & Vascular Institute Before you begin imaging... Obtain the patient s Height Weight BP PLAX View PLAX View Is apex @ 9-10 o clock?
Titel Kardiologie-SG.ch hot topics in heart failure and mitral regurgitation
 Titel Kardiologie-SG.ch hot topics in heart failure and mitral regurgitation where and how to quantify mitral regurgitation: Echolab, Cathlab or MRI? Philipp K. Haager, St. Gallen Measuring mitral regurgitation?
Titel Kardiologie-SG.ch hot topics in heart failure and mitral regurgitation where and how to quantify mitral regurgitation: Echolab, Cathlab or MRI? Philipp K. Haager, St. Gallen Measuring mitral regurgitation?
What Degree of MR Deserves Surgical or Transcatheter Intervention, and How Should It Be Assessed?
 What Degree of MR Deserves Surgical or Transcatheter Intervention, and How Should It Be Assessed? Robert J. Siegel, M.D., FACC Nov. 14-15, 2017, Beverly Hills Director, Cardiac Non-Invasive Laboratory
What Degree of MR Deserves Surgical or Transcatheter Intervention, and How Should It Be Assessed? Robert J. Siegel, M.D., FACC Nov. 14-15, 2017, Beverly Hills Director, Cardiac Non-Invasive Laboratory
Aortic Stenosis: Spectrum of Disease, Low Flow/Low Gradient and Variants
 Aortic Stenosis: Spectrum of Disease, Low Flow/Low Gradient and Variants Martin G. Keane, MD, FASE Professor of Medicine Lewis Katz School of Medicine at Temple University Basic root structure Parasternal
Aortic Stenosis: Spectrum of Disease, Low Flow/Low Gradient and Variants Martin G. Keane, MD, FASE Professor of Medicine Lewis Katz School of Medicine at Temple University Basic root structure Parasternal
Quantification of Mitral Stenosis: Planimetry, pressure Half time, Continuity Common Errors
 Quantification of Mitral Stenosis: Planimetry, pressure Half time, Continuity Common Errors Christopher J Kramer RDCS Advanced Cardiovascular Services Aurora Health Care Milwaukee, WI No Disclosures Baumgartner,
Quantification of Mitral Stenosis: Planimetry, pressure Half time, Continuity Common Errors Christopher J Kramer RDCS Advanced Cardiovascular Services Aurora Health Care Milwaukee, WI No Disclosures Baumgartner,
Clinical Outcome of Tricuspid Regurgitation. David Messika-Zeitoun
 Clinical Outcome of Tricuspid Regurgitation David Messika-Zeitoun I have financial relationships to disclose Consultant for: Edwards, Symetis and Valtech Tricuspid Regurgitation is a Common Finding Tricuspid
Clinical Outcome of Tricuspid Regurgitation David Messika-Zeitoun I have financial relationships to disclose Consultant for: Edwards, Symetis and Valtech Tricuspid Regurgitation is a Common Finding Tricuspid
Primary Mitral Regurgitation
 EURO VALVE Madrid News from Valves Guidelines 2012: What s new and Why? Primary Mitral Regurgitation Luc A. Pierard, MD, PhD Professor of Medicine Head of the Department of Cardiology Heart Valve Clinic,
EURO VALVE Madrid News from Valves Guidelines 2012: What s new and Why? Primary Mitral Regurgitation Luc A. Pierard, MD, PhD Professor of Medicine Head of the Department of Cardiology Heart Valve Clinic,
Congenital. Unicuspid Bicuspid Quadricuspid
 David Letterman s Top 10 Aortic Stenosis The victim can be anyone: Echo is the question and the answer!!!! Hilton Head Island Echocardiography Conference 2012 Timothy E. Paterick, MD, JD, MBA Christopher
David Letterman s Top 10 Aortic Stenosis The victim can be anyone: Echo is the question and the answer!!!! Hilton Head Island Echocardiography Conference 2012 Timothy E. Paterick, MD, JD, MBA Christopher
Echo Doppler Assessment of Right and Left Ventricular Hemodynamics.
 Echo Doppler Assessment of Right and Left Ventricular Hemodynamics. Itzhak Kronzon, MD, FASE, FACC, FESC, FAHA, FACP, FCCP Northwell, Lenox Hill Hospital, New York Professor of Cardiology Hofstra University
Echo Doppler Assessment of Right and Left Ventricular Hemodynamics. Itzhak Kronzon, MD, FASE, FACC, FESC, FAHA, FACP, FCCP Northwell, Lenox Hill Hospital, New York Professor of Cardiology Hofstra University
NEW GUIDELINES. A Guideline Protocol for the Assessment of Aortic Regurgitation From the British Society of Echocardiography Education Committee
 NEW GUIDELINES A Guideline Protocol for the Assessment of Aortic Regurgitation From the British Society of Echocardiography Education Committee Gill Wharton, Prathap Kanagala (Lead Authors) Richard Steeds
NEW GUIDELINES A Guideline Protocol for the Assessment of Aortic Regurgitation From the British Society of Echocardiography Education Committee Gill Wharton, Prathap Kanagala (Lead Authors) Richard Steeds
Advanced Applica,on of Point- of- Care Echocardiography in Cri,cal Care. Dr. Mark Tutschka Dr. Rob ArnAield
 Advanced Applica,on of Point- of- Care Echocardiography in Cri,cal Care Dr. Mark Tutschka Dr. Rob ArnAield OBJECTIVES Provide an overview of common advanced echocardiographic techniques suitable for use
Advanced Applica,on of Point- of- Care Echocardiography in Cri,cal Care Dr. Mark Tutschka Dr. Rob ArnAield OBJECTIVES Provide an overview of common advanced echocardiographic techniques suitable for use
Goals of Reporting. Background of the STS/ACC TVT Registry. TVT Registry TAVR and MitraClip 10/11/ /11/2016 9:10 9:30 AM
 10/11/2016 9:10 9:30 AM Rebecca T. Hahn, MD Director of Interventional Echocardiography Columbia University Medical College Background of the STS/ACC TVT Registry The STS/ACC TVT Registry is a benchmarking
10/11/2016 9:10 9:30 AM Rebecca T. Hahn, MD Director of Interventional Echocardiography Columbia University Medical College Background of the STS/ACC TVT Registry The STS/ACC TVT Registry is a benchmarking
OPTIMIZING ECHO ACQUISTION FOR STRAIN AND DIASTOLOGY
 OPTIMIZING ECHO ACQUISTION FOR STRAIN AND DIASTOLOGY October 8, 2017 Deborah Agler, ACS, RDCS, FASE Coordinator of Education and Training Cleveland Clinic General Principles Diastology Clinical Data Heart
OPTIMIZING ECHO ACQUISTION FOR STRAIN AND DIASTOLOGY October 8, 2017 Deborah Agler, ACS, RDCS, FASE Coordinator of Education and Training Cleveland Clinic General Principles Diastology Clinical Data Heart
Tricuspid and Pulmonary Valve Disease
 Tricuspid and Pulmonary Valve Disease Lawrence Rudski MD FRCPC FACC FASE Professor of Medicine Director, Division of Cardiology Jewish General Hospital McGill University Right Sided Failure Edema Gut congestion
Tricuspid and Pulmonary Valve Disease Lawrence Rudski MD FRCPC FACC FASE Professor of Medicine Director, Division of Cardiology Jewish General Hospital McGill University Right Sided Failure Edema Gut congestion
P = 4V 2. IVC Dimensions 10/20/2014. Comprehensive Hemodynamic Evaluation by Doppler Echocardiography. The Simplified Bernoulli Equation
 Comprehensive Hemodynamic Evaluation by Doppler Echocardiography Itzhak Kronzon, MD North Shore LIJ/ Lenox Hill Hospital New York, NY Disclosure: Philips Healthcare St. Jude Medical The Simplified Bernoulli
Comprehensive Hemodynamic Evaluation by Doppler Echocardiography Itzhak Kronzon, MD North Shore LIJ/ Lenox Hill Hospital New York, NY Disclosure: Philips Healthcare St. Jude Medical The Simplified Bernoulli
Echocardiographic Evaluation of Aortic Valve Prosthesis
 Echocardiographic Evaluation of Aortic Valve Prosthesis Amr E Abbas, MD, FACC, FASE, FSCAI, FSVM, RPVI Co-Director, Echocardiography, Director, Interventional Cardiology Research, Beaumont Health System
Echocardiographic Evaluation of Aortic Valve Prosthesis Amr E Abbas, MD, FACC, FASE, FSCAI, FSVM, RPVI Co-Director, Echocardiography, Director, Interventional Cardiology Research, Beaumont Health System
Comprehensive Hemodynamics By Doppler Echocardiography. The Echocardiographic Swan-Ganz Catheter.
 Comprehensive Hemodynamics By Doppler Echocardiography. The Echocardiographic Swan-Ganz Catheter. Itzhak Kronzon, MD, FASE, FACC, FESC, FAHA, FACP, FCCP North Shore HS, LIJ/Lenox Hill Hospital, New York
Comprehensive Hemodynamics By Doppler Echocardiography. The Echocardiographic Swan-Ganz Catheter. Itzhak Kronzon, MD, FASE, FACC, FESC, FAHA, FACP, FCCP North Shore HS, LIJ/Lenox Hill Hospital, New York
Back to Basics: Common Errors In Quantitation In Everyday Practice
 Back to Basics: Common Errors In Quantitation In Everyday Practice Deborah Agler, ACS, RDCS, FASE October 9, 2017 ASE: Echo Florida Rebecca T. Hahn, MD Director of Interventional Echocardiography Professor
Back to Basics: Common Errors In Quantitation In Everyday Practice Deborah Agler, ACS, RDCS, FASE October 9, 2017 ASE: Echo Florida Rebecca T. Hahn, MD Director of Interventional Echocardiography Professor
Exercise Pulmonary Hypertension predicts the Occurrence of Symptoms in Asymptomatic Degenerative Mitral Regurgitation
 Exercise Pulmonary Hypertension predicts the Occurrence of Symptoms in Asymptomatic Degenerative Mitral Regurgitation Julien Magne, PhD, Kim O Connor, MD, Giuseppe Romano, MD, Marie Moonen, MD, Luc A.
Exercise Pulmonary Hypertension predicts the Occurrence of Symptoms in Asymptomatic Degenerative Mitral Regurgitation Julien Magne, PhD, Kim O Connor, MD, Giuseppe Romano, MD, Marie Moonen, MD, Luc A.
Who will Benefit from Percutaneous Management of Mitral Regurgitation? An Imaging Guide to Management
 Who will Benefit from Percutaneous Management of Mitral Regurgitation? An Imaging Guide to Management James D. Thomas, M.D., F.A.C.C. Department of Cardiovascular Medicine Heart and Vascular Institute
Who will Benefit from Percutaneous Management of Mitral Regurgitation? An Imaging Guide to Management James D. Thomas, M.D., F.A.C.C. Department of Cardiovascular Medicine Heart and Vascular Institute
What echo measurements are key prior to MitraClip?
 APHP CHU Bichat - Claude Bernard What echo measurements are key prior to MitraClip? Eric Brochet,MD Cardiology Department Hopital Bichat Paris France No disclosure Conflict of interest Case 69 y.o man
APHP CHU Bichat - Claude Bernard What echo measurements are key prior to MitraClip? Eric Brochet,MD Cardiology Department Hopital Bichat Paris France No disclosure Conflict of interest Case 69 y.o man
Dobutamine Stress testing In Low Flow, Low EF, Low Gradient Aortic Stenosis Case Studies
 Dobutamine Stress testing In Low Flow, Low EF, Low Gradient Aortic Stenosis Case Studies Mitral Regurgitation The New ASE Guidelines: Role of 2D/3D and CMR William A. Zoghbi MD, FASE, MACC Professor and
Dobutamine Stress testing In Low Flow, Low EF, Low Gradient Aortic Stenosis Case Studies Mitral Regurgitation The New ASE Guidelines: Role of 2D/3D and CMR William A. Zoghbi MD, FASE, MACC Professor and
LV geometric and functional changes in VHD: How to assess? Mi-Seung Shin M.D., Ph.D. Gachon University Gil Hospital
 LV geometric and functional changes in VHD: How to assess? Mi-Seung Shin M.D., Ph.D. Gachon University Gil Hospital LV inflow across MV LV LV outflow across AV LV LV geometric changes Pressure overload
LV geometric and functional changes in VHD: How to assess? Mi-Seung Shin M.D., Ph.D. Gachon University Gil Hospital LV inflow across MV LV LV outflow across AV LV LV geometric changes Pressure overload
Swan Song: Echocardiography as a Pulmonary Artery Catheter? Interdepartmental Division of Critical Care Medicine
 Swan Song: Echocardiography as a Pulmonary Artery Catheter? The swan is without spot, and it sings sweetly as it dies, that song ending its life Leonardo Da Vinci Curr Opin Anesthesiol 2016, 29:36 45 Circulation.
Swan Song: Echocardiography as a Pulmonary Artery Catheter? The swan is without spot, and it sings sweetly as it dies, that song ending its life Leonardo Da Vinci Curr Opin Anesthesiol 2016, 29:36 45 Circulation.
Direct Planimetry of Mitral Valve Regurgitation Orifice Area by Real-time 3D Transesophageal Echocardiography
 Direct Planimetry of Mitral Valve Regurgitation Orifice Area by Real-time 3D Transesophageal Echocardiography Ertunc Altiok, Sandra Hamada, Silke van Hall, Mehtap Hanenberg, Eva Grabskaya, Michael Becker,
Direct Planimetry of Mitral Valve Regurgitation Orifice Area by Real-time 3D Transesophageal Echocardiography Ertunc Altiok, Sandra Hamada, Silke van Hall, Mehtap Hanenberg, Eva Grabskaya, Michael Becker,
25 different brand names >44 different models Sizes mm
 Types of Prosthetic Valves BIOLOGIC STENTED Porcine xenograft Pericardial xenograft STENTLESS Porcine xenograft Pericardial xenograft Homograft (allograft) Autograft PERCUTANEOUS MECHANICAL Bileaflet Single
Types of Prosthetic Valves BIOLOGIC STENTED Porcine xenograft Pericardial xenograft STENTLESS Porcine xenograft Pericardial xenograft Homograft (allograft) Autograft PERCUTANEOUS MECHANICAL Bileaflet Single
British Society of Echocardiography
 British Society of Echocardiography Affiliated to the British Cardiac Society A Minimum Dataset for a Standard Adult Transthoracic Echocardiogram From the British Society of Echocardiography Education
British Society of Echocardiography Affiliated to the British Cardiac Society A Minimum Dataset for a Standard Adult Transthoracic Echocardiogram From the British Society of Echocardiography Education
Basic Approach to the Echocardiographic Evaluation of Ventricular Diastolic Function
 Basic Approach to the Echocardiographic Evaluation of Ventricular Diastolic Function J A F E R A L I, M D U N I V E R S I T Y H O S P I T A L S C A S E M E D I C A L C E N T E R S T A F F C A R D I O T
Basic Approach to the Echocardiographic Evaluation of Ventricular Diastolic Function J A F E R A L I, M D U N I V E R S I T Y H O S P I T A L S C A S E M E D I C A L C E N T E R S T A F F C A R D I O T
Diastolic Function Assessment New Guideline Update Practical Approach
 Mayo Clinic Department of Cardiovascular Diseases Mayo Clinic Echocardiography Review Course for Boards and Recertification Diastolic Function Assessment New Guideline Update Practical Approach Jae K.
Mayo Clinic Department of Cardiovascular Diseases Mayo Clinic Echocardiography Review Course for Boards and Recertification Diastolic Function Assessment New Guideline Update Practical Approach Jae K.
Tricuspid and Pulmonary Valve Disease
 Tricuspid and Pulmonary Valve Disease Lawrence Rudski MD FRCPC FACC FASE Professor of Medicine Director, Division of Cardiology Jewish General Hospital McGill University Question 1 All of the following
Tricuspid and Pulmonary Valve Disease Lawrence Rudski MD FRCPC FACC FASE Professor of Medicine Director, Division of Cardiology Jewish General Hospital McGill University Question 1 All of the following
School, The University of Texas Health Science Center at Houston, TX.
 Chapter 4: Basics of echocardiography for transcatheter interventions Adrian DaSilva-DeAbreu, MD 1, Catalin Loghin, MD 2 1 Resident, Department of Internal Medicine, McGovern Medical School, The University
Chapter 4: Basics of echocardiography for transcatheter interventions Adrian DaSilva-DeAbreu, MD 1, Catalin Loghin, MD 2 1 Resident, Department of Internal Medicine, McGovern Medical School, The University
Adel Hasanin Ahmed 1
 Adel Hasanin Ahmed 1 PERICARDIAL DISEASE The pericardial effusion ends anteriorly to the descending aorta and is best visualised in the PLAX. PSAX is actually very useful sometimes for looking at posterior
Adel Hasanin Ahmed 1 PERICARDIAL DISEASE The pericardial effusion ends anteriorly to the descending aorta and is best visualised in the PLAX. PSAX is actually very useful sometimes for looking at posterior
MAKING SENSE OF MODERATE GRADIENTS IN PATIENTS WITH SYMPTOMATIC AORTIC STENOSIS
 MAKING SENSE OF MODERATE GRADIENTS IN PATIENTS WITH SYMPTOMATIC AORTIC STENOSIS David A. Orsinelli, MD, FACC, FASE Professor, Internal Medicine Director, Structural Heart Imaging The Ohio State University
MAKING SENSE OF MODERATE GRADIENTS IN PATIENTS WITH SYMPTOMATIC AORTIC STENOSIS David A. Orsinelli, MD, FACC, FASE Professor, Internal Medicine Director, Structural Heart Imaging The Ohio State University
Prosthetic valve dysfunction: stenosis or regurgitation
 Prosthetic valve dysfunction: stenosis or regurgitation Jean G. Dumesnil MD, FRCP(C), FACC, FASE(Hon) Quebec Heart and Lung Institute, Québec, Québec No disclosures Possible Causes of High Gradients in
Prosthetic valve dysfunction: stenosis or regurgitation Jean G. Dumesnil MD, FRCP(C), FACC, FASE(Hon) Quebec Heart and Lung Institute, Québec, Québec No disclosures Possible Causes of High Gradients in
ASCeXAM / ReASCE. Practice Board Exam Questions Monday Morning
 ASCeXAM / ReASCE Practice Board Exam Questions Monday Morning Ultrasound Physics Artifacts Doppler Physics Imaging, Knobology, and Artifacts Echocardiographic Evaluation of the RV Tricuspid and Pulmonary
ASCeXAM / ReASCE Practice Board Exam Questions Monday Morning Ultrasound Physics Artifacts Doppler Physics Imaging, Knobology, and Artifacts Echocardiographic Evaluation of the RV Tricuspid and Pulmonary
Echocardiographic evaluation of mitral stenosis
 Echocardiographic evaluation of mitral stenosis Euroecho 2011 Philippe Unger, MD, FESC Erasme Hospital, ULB, Brussels, Belgium I have nothing to declare EuroHeart Survey Etiology of single native left-sided
Echocardiographic evaluation of mitral stenosis Euroecho 2011 Philippe Unger, MD, FESC Erasme Hospital, ULB, Brussels, Belgium I have nothing to declare EuroHeart Survey Etiology of single native left-sided
AIMI-HF PROCEDURE MANUAL TECHNICAL GUIDE FOR ECHOCARDIOGRAPHY. MHI Core Laboratory E. O Meara - J.C. Tardif J. Vincent, G. Grenier, C.
 AIMI-HF PROCEDURE MANUAL TECHNICAL GUIDE FOR ECHOCARDIOGRAPHY MHI Core Laboratory E. O Meara - J.C. Tardif J. Vincent, G. Grenier, C. Roy February 2016 Montreal Heart Institute HF Research Aude Turgeon,
AIMI-HF PROCEDURE MANUAL TECHNICAL GUIDE FOR ECHOCARDIOGRAPHY MHI Core Laboratory E. O Meara - J.C. Tardif J. Vincent, G. Grenier, C. Roy February 2016 Montreal Heart Institute HF Research Aude Turgeon,
PROSTHETIC VALVE BOARD REVIEW
 PROSTHETIC VALVE BOARD REVIEW The correct answer D This two chamber view shows a porcine mitral prosthesis with the typical appearance of the struts although the leaflets are not well seen. The valve
PROSTHETIC VALVE BOARD REVIEW The correct answer D This two chamber view shows a porcine mitral prosthesis with the typical appearance of the struts although the leaflets are not well seen. The valve
Prof. Patrizio LANCELLOTTI, MD, PhD Heart Valve Clinic, University of Liège, CHU Sart Tilman, Liège, BELGIUM
 The Patient with Aortic Stenosis and Mitral Regurgitation Prof. Patrizio LANCELLOTTI, MD, PhD Heart Valve Clinic, University of Liège, CHU Sart Tilman, Liège, BELGIUM Aortic Stenosis + Mitral Regurgitation?
The Patient with Aortic Stenosis and Mitral Regurgitation Prof. Patrizio LANCELLOTTI, MD, PhD Heart Valve Clinic, University of Liège, CHU Sart Tilman, Liège, BELGIUM Aortic Stenosis + Mitral Regurgitation?
HEART VALVE DISEASES. Dr. James Kadouch Medical Officer Cardiologist Delphine Labojka Method & Process Manager
 NOVEMBER 2017 SCOR inform HEART VALVE DISEASES Dr. James Kadouch Medical Officer Cardiologist Delphine Labojka Method & Process Manager Introduction Cardiac cycle and heart valve diseases 03 The aortic
NOVEMBER 2017 SCOR inform HEART VALVE DISEASES Dr. James Kadouch Medical Officer Cardiologist Delphine Labojka Method & Process Manager Introduction Cardiac cycle and heart valve diseases 03 The aortic
CHAPTER 5 EFFICIENT APPROACHES FOR QUANTIFICATION OF AORTIC REGURGITATION USING PROXIMAL ISOVELOCITY SURFACE AREA PROCESS
 CHAPTER 5 EFFICIENT APPROACHES FOR QUANTIFICATION OF AORTIC REGURGITATION USING PROXIMAL ISOVELOCITY SURFACE AREA PROCESS 5.1. Introduction Aortic Regurgitation is also known as Aortic Insufficiency (AI).
CHAPTER 5 EFFICIENT APPROACHES FOR QUANTIFICATION OF AORTIC REGURGITATION USING PROXIMAL ISOVELOCITY SURFACE AREA PROCESS 5.1. Introduction Aortic Regurgitation is also known as Aortic Insufficiency (AI).
Functional Mitral Regurgitation
 Club 35 - The best in heart valve disease - Functional Mitral Regurgitation Steven Droogmans, MD, PhD UZ Brussel, Jette, Belgium 08-12-2011 Euroecho & other Imaging Modalities 2011 No conflicts of interest
Club 35 - The best in heart valve disease - Functional Mitral Regurgitation Steven Droogmans, MD, PhD UZ Brussel, Jette, Belgium 08-12-2011 Euroecho & other Imaging Modalities 2011 No conflicts of interest
MITRAL VALVE PATHOLOGY WITH TRICUSPID REGURGITATION (AND PHT)
") UNIVERSITY OF PADUA, SCHOOL OF MEDICINE Department of Cardiac,Thoracic and Vascular Sciences Padua, Italy MITRAL VALVE PATHOLOGY WITH TRICUSPID REGURGITATION (AND PHT) Luigi P. Badano**, MD, PhD, FESC,
UNIVERSITY OF PADUA, SCHOOL OF MEDICINE Department of Cardiac,Thoracic and Vascular Sciences Padua, Italy MITRAL VALVE PATHOLOGY WITH TRICUSPID REGURGITATION (AND PHT) Luigi P. Badano**, MD, PhD, FESC,
Ref 1. Ref 2. Ref 3. Ref 4. See graph
 Ref 1 Ref 2 Ref 3 1. Ages 6-23 y/o 2. Significant LVM differences by gender 3. For males 95 th percentiles: a. LVM/BSA = 103 b. LVM/height = 100 4. For females 95 th percentiles: a. LVM/BSA = 84 b. LVM/height
Ref 1 Ref 2 Ref 3 1. Ages 6-23 y/o 2. Significant LVM differences by gender 3. For males 95 th percentiles: a. LVM/BSA = 103 b. LVM/height = 100 4. For females 95 th percentiles: a. LVM/BSA = 84 b. LVM/height
Uncommon Doppler Echocardiographic Findings of Severe Pulmonic Insufficiency
 Uncommon Doppler Echocardiographic Findings of Severe Pulmonic Insufficiency Rahul R. Jhaveri, MD, Muhamed Saric, MD, PhD, FASE, and Itzhak Kronzon, MD, FASE, New York, New York Background: Two-dimensional
Uncommon Doppler Echocardiographic Findings of Severe Pulmonic Insufficiency Rahul R. Jhaveri, MD, Muhamed Saric, MD, PhD, FASE, and Itzhak Kronzon, MD, FASE, New York, New York Background: Two-dimensional
Diastolic Function Assessment Practical Ways to Incorporate into Every Echo
 Diastolic Function Assessment Practical Ways to Incorporate into Every Echo Jae K. Oh, MD Echo Hawaii 2018 2018 MFMER 3712003-1 Learning Objectives My presentation will help you to Appreciate the importance
Diastolic Function Assessment Practical Ways to Incorporate into Every Echo Jae K. Oh, MD Echo Hawaii 2018 2018 MFMER 3712003-1 Learning Objectives My presentation will help you to Appreciate the importance
Diastolic Function Overview
 Diastolic Function Overview Richard Palma BS, RDCS, RCS, APS, FASE Director and Clinical Coordinator The Hoffman Heart and Vascular Institute School of Cardiac Ultrasound None Disclosures Learning Objectives
Diastolic Function Overview Richard Palma BS, RDCS, RCS, APS, FASE Director and Clinical Coordinator The Hoffman Heart and Vascular Institute School of Cardiac Ultrasound None Disclosures Learning Objectives
JOINT MEETING 2 Tricuspid club Chairpersons: G. Athanassopoulos, A. Avgeropoulou, M. Khoury, G. Stavridis
 JOINT MEETING 2 Tricuspid club Chairpersons: G. Athanassopoulos, A. Avgeropoulou, M. Khoury, G. Stavridis Similarities and differences in Tricuspid vs. Mitral Valve Anatomy and Imaging. Echo evaluation
JOINT MEETING 2 Tricuspid club Chairpersons: G. Athanassopoulos, A. Avgeropoulou, M. Khoury, G. Stavridis Similarities and differences in Tricuspid vs. Mitral Valve Anatomy and Imaging. Echo evaluation
Σεμινάρια Ομάδων Εργασίας 2017 Ανεπάρκεια μιτροειδούς μυξωματώδους αιτιολογίας
 Σεμινάρια Ομάδων Εργασίας 2017 Ανεπάρκεια μιτροειδούς μυξωματώδους αιτιολογίας Μυτάς Δημήτρης MD, PhD Επιμ Α ΕΣΥ Σισμανόγλειο Γενικό Νοσοκομείο Αττικής Δηλώνω υπεύθυνα ότι η παρούσα ομιλία δεν επιχορηγείται
Σεμινάρια Ομάδων Εργασίας 2017 Ανεπάρκεια μιτροειδούς μυξωματώδους αιτιολογίας Μυτάς Δημήτρης MD, PhD Επιμ Α ΕΣΥ Σισμανόγλειο Γενικό Νοσοκομείο Αττικής Δηλώνω υπεύθυνα ότι η παρούσα ομιλία δεν επιχορηγείται
Ischemic Mitral Regurgitation
 Ischemic Mitral Regurgitation Jean-Louis J. Vanoverschelde, MD, PhD Université catholique de Louvain Brussels, Belgium Definition Ischemic mitral regurgitation is mitral regurgitation due to complications
Ischemic Mitral Regurgitation Jean-Louis J. Vanoverschelde, MD, PhD Université catholique de Louvain Brussels, Belgium Definition Ischemic mitral regurgitation is mitral regurgitation due to complications
Valve Disease Board Review Questions
 Valve Disease Board Review Questions Dennis A. Tighe, MD, FASE University of Massachusetts Medical School Worcester, MA Case 1 History A 61 year-old man Presents to hospital with worsening shortness of
Valve Disease Board Review Questions Dennis A. Tighe, MD, FASE University of Massachusetts Medical School Worcester, MA Case 1 History A 61 year-old man Presents to hospital with worsening shortness of
Nancy Goldman Cutler, MD Beaumont Children s Hospital Royal Oak, Mi
 Nancy Goldman Cutler, MD Beaumont Children s Hospital Royal Oak, Mi Identify increased LV wall thickness (WT) Understand increased WT in athletes Understand hypertrophic cardiomyopathy (HCM) Enhance understanding
Nancy Goldman Cutler, MD Beaumont Children s Hospital Royal Oak, Mi Identify increased LV wall thickness (WT) Understand increased WT in athletes Understand hypertrophic cardiomyopathy (HCM) Enhance understanding
Echo in Pulmonary HTN
 Echo in Pulmonary HTN Steven A. Goldstein MD FACC FASE Professor of Medicine Georgetown University Medical Center MedStar Heart Institute Washington Hospital Center Monday, October 10, 2017 Pulmonary Artery
Echo in Pulmonary HTN Steven A. Goldstein MD FACC FASE Professor of Medicine Georgetown University Medical Center MedStar Heart Institute Washington Hospital Center Monday, October 10, 2017 Pulmonary Artery
TAVR TTE INTERROGATION BY ALAN MATTHEWS
 TAVR TTE INTERROGATION BY ALAN MATTHEWS KEYS TO ACCURATE ASSESSMENT EDWARDS SAPIEN VALVE 3 PHASES OF TAVR TTE Evaluation (Qualifying) Placement (Intraoperative) Follow-up (Post-Op) GOALS High quality TTE
TAVR TTE INTERROGATION BY ALAN MATTHEWS KEYS TO ACCURATE ASSESSMENT EDWARDS SAPIEN VALVE 3 PHASES OF TAVR TTE Evaluation (Qualifying) Placement (Intraoperative) Follow-up (Post-Op) GOALS High quality TTE
HOW IMPORTANT ARE THESE ECHO MEASUREMENTS ANYWAY?
 HOW IMPORTANT ARE THESE ECHO MEASUREMENTS ANYWAY? John D. Carroll, MD Professor, Director of Interventional Cardiology and Co-Medical Director of the Cardiac and Vascular Center, University of Colorado
HOW IMPORTANT ARE THESE ECHO MEASUREMENTS ANYWAY? John D. Carroll, MD Professor, Director of Interventional Cardiology and Co-Medical Director of the Cardiac and Vascular Center, University of Colorado
Diastolic Function: What the Sonographer Needs to Know. Echocardiographic Assessment of Diastolic Function: Basic Concepts 2/8/2012
 Diastolic Function: What the Sonographer Needs to Know Pat Bailey, RDCS, FASE Technical Director Beaumont Health System Echocardiographic Assessment of Diastolic Function: Basic Concepts Practical Hints
Diastolic Function: What the Sonographer Needs to Know Pat Bailey, RDCS, FASE Technical Director Beaumont Health System Echocardiographic Assessment of Diastolic Function: Basic Concepts Practical Hints
Blank DISCLOSURES 1/17/2017 COMPLEX VALVE CASES CHALLENGES IN EVALUATING AND MANAGING MULTIVALVULAR HEART DISEASE ECHO HAWAII 1/23/17 NONE
 Blank COMPLEX VALVE CASES ECHO HAWAII 1/23/17 1 David A. Orsinelli, MD, FACC, FASE Professor, Internal Medicine Director, Structural Heart Imaging The Ohio State University Division of Cardiovascular Medicine
Blank COMPLEX VALVE CASES ECHO HAWAII 1/23/17 1 David A. Orsinelli, MD, FACC, FASE Professor, Internal Medicine Director, Structural Heart Imaging The Ohio State University Division of Cardiovascular Medicine
Imaging Assessment of Aortic Stenosis/Aortic Regurgitation
 Imaging Assessment of Aortic Stenosis/Aortic Regurgitation Craig E Fleishman, MD FACC FASE The Heart Center at Arnold Palmer Hospital for Children, Orlando SCAI Fall Fellows Course 2014 Las Vegas Disclosure
Imaging Assessment of Aortic Stenosis/Aortic Regurgitation Craig E Fleishman, MD FACC FASE The Heart Center at Arnold Palmer Hospital for Children, Orlando SCAI Fall Fellows Course 2014 Las Vegas Disclosure
Appendix II: ECHOCARDIOGRAPHY ANALYSIS
 Appendix II: ECHOCARDIOGRAPHY ANALYSIS Two-Dimensional (2D) imaging was performed using the Vivid 7 Advantage cardiovascular ultrasound system (GE Medical Systems, Milwaukee) with a frame rate of 400 frames
Appendix II: ECHOCARDIOGRAPHY ANALYSIS Two-Dimensional (2D) imaging was performed using the Vivid 7 Advantage cardiovascular ultrasound system (GE Medical Systems, Milwaukee) with a frame rate of 400 frames
GENERAL PRINCIPLES FOR ECHO ASSESSMENT OF DIASTOLIC FUNCTION (For full recommendation refer to the Left Ventricular Diastolic Function Guideline)
") 1 THE AMERICAN SOCIETY OF ECHOCARDIOGRAPHY RECOMMENDATIONS FOR THE EVALUATION OF LEFT VENTRICULAR DIASTOLIC FUNCTION BY ECHOCARDIOGRAPHY: A QUICK REFERENCE GUIDE FROM THE ASE WORKFLOW AND LAB MANAGEMENT
1 THE AMERICAN SOCIETY OF ECHOCARDIOGRAPHY RECOMMENDATIONS FOR THE EVALUATION OF LEFT VENTRICULAR DIASTOLIC FUNCTION BY ECHOCARDIOGRAPHY: A QUICK REFERENCE GUIDE FROM THE ASE WORKFLOW AND LAB MANAGEMENT
Right Heart Hemodynamics: Echo-Cath Discrepancies
 Department of cardiac, thoracic and vascular sciences University of Padua, School of Medicine Padua, Italy Right Heart Hemodynamics: Echo-Cath Discrepancies Luigi P. Badano, MD, PhD, FESC, FACC **Dr. Badano
Department of cardiac, thoracic and vascular sciences University of Padua, School of Medicine Padua, Italy Right Heart Hemodynamics: Echo-Cath Discrepancies Luigi P. Badano, MD, PhD, FESC, FACC **Dr. Badano
Assessment of LV systolic function
 Tutorial 5 - Assessment of LV systolic function Assessment of LV systolic function A knowledge of the LV systolic function is crucial in the undertanding of and management of unstable hemodynamics or a
Tutorial 5 - Assessment of LV systolic function Assessment of LV systolic function A knowledge of the LV systolic function is crucial in the undertanding of and management of unstable hemodynamics or a
Reshape/Coapt: do we need more? Prof. J Zamorano Head of Cardiology University Hospital Ramon y Cajal, Madrid
 Reshape/Coapt: do we need more? Prof. J Zamorano Head of Cardiology University Hospital Ramon y Cajal, Madrid Patient records 76 y.o. male Hypertension. Dyslipidemia. OPLD. Smoked in the past. Diabetes
Reshape/Coapt: do we need more? Prof. J Zamorano Head of Cardiology University Hospital Ramon y Cajal, Madrid Patient records 76 y.o. male Hypertension. Dyslipidemia. OPLD. Smoked in the past. Diabetes
Relevant Financial Relationship(s) Off Label Usage. None. None
 Off Label Usage. None. None") Different Variants Amr E Abbas, MD, FACC, FSCAI, FASE, FSVM Director, Interventional Cardiology Research Beaumont Health Associate Professor of Medicine, OU/WB School of Medicine ASCeXAM/ReASCeXAM 2018
Different Variants Amr E Abbas, MD, FACC, FSCAI, FASE, FSVM Director, Interventional Cardiology Research Beaumont Health Associate Professor of Medicine, OU/WB School of Medicine ASCeXAM/ReASCeXAM 2018
TEE Zebras. Case Cardiac Anesthesia Group
 TEE Zebras Edwin G. Avery, IV, M.D., C.P.I. Chief, Division of Cardiac Anesthesia University Hospitals Case Medical Center Associate Professor of Anesthesiology Case Western Reserve University School of
TEE Zebras Edwin G. Avery, IV, M.D., C.P.I. Chief, Division of Cardiac Anesthesia University Hospitals Case Medical Center Associate Professor of Anesthesiology Case Western Reserve University School of
Introduction RECOMMENDATIONS
 European Journal of Echocardiography (2010) 11, 223 244 doi:10.1093/ejechocard/jeq030 RECOMMENDATIONS European Association of Echocardiography recommendations for the assessment of valvular regurgitation.
European Journal of Echocardiography (2010) 11, 223 244 doi:10.1093/ejechocard/jeq030 RECOMMENDATIONS European Association of Echocardiography recommendations for the assessment of valvular regurgitation.
Aortic stenosis with concomitant mitral regurgitation
 Challenges in the evaluation and management of aortic stenosis Aortic stenosis with concomitant mitral regurgitation S1 Philippe Unger, M.D., FESC Erasme Hospital - Université Libre de Bruxelles Brussels,
Challenges in the evaluation and management of aortic stenosis Aortic stenosis with concomitant mitral regurgitation S1 Philippe Unger, M.D., FESC Erasme Hospital - Université Libre de Bruxelles Brussels,