Cardiology Updates: Syncope and Stress Testing. Kathleen Morris, DO Cardiology Fellow St. Vincent Hospital
|
|
|
- Anthony James
- 5 years ago
- Views:
Transcription
1 Cardiology Updates: Syncope and Stress Testing Kathleen Morris, DO Cardiology Fellow St. Vincent Hospital
2 Disclosures NONE
3 PART ONE: Let s start with SYNCOPE Objectives: Definition of Syncope Brief review of causes and incidence Review ACC 2017 Updated Guidelines
4 Abrupt, transient, complete loss of consciousness associated with inability to maintain postural tone with rapid and spontaneous recovery. CEREBRAL HYPOPERFUSION Should NOT be other non syncope loss of consciousness such as: seizure, antecedent head trauma or apparent LOC (pseudosyncope) Definition of Syncope
5 Incidence Framingham Heart Study followed 7814 men and women Followed for 17 years 11% reported syncopal episodes Similar in men and women* 3 5% of ER visits 1% of hospital admissions
6 COST A nationally representative sample of hospital discharges and reported charges was analyzed, and costs were estimated using Medicare cost to charge ratios. A conservative estimate of total annual costs for syncope related hospitalizations was $2.4 billion (95% confidence interval [CI] $2.2 to $2.6 billion), with a mean cost of $5,400 (95% CI $5,100 to $5,600) per hospitalization. Efforts to safely decrease syncope related admissions may result in substantial costs savings.
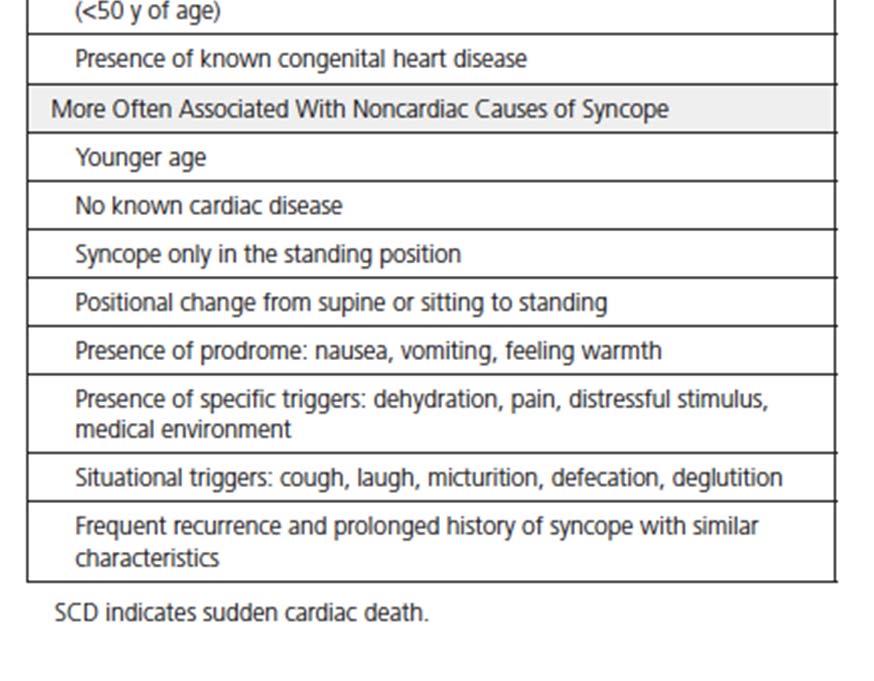
7 Etiologies of Syncope Neurally mediated 35% Vasovagal Carotid hypersensitivity Situational Cough, post micturition Orthostatic 10% Drug induced Autonomic failure Primary Secondary Syncope mimics Seizure, psychogenic (2 10%) Neurologic CVA/TIA Unknown (25 40%) Cardiac Arrhythmia 10% Bradycardia Sinus pause/arrest, AV block AV block Tachycardia VT, SVT Long QT syndrome Structural Cardiopulmonary 5% Aortic stenosis HOCM Pulmonary HTN Aortic Dissection
8


9 Let s Review the Guidelines
10 History and Physical Exam Most Important IB Recommendation History and Physical Exam History and Physical Exam History and Physical Exam

11
12 IB: Resting ECG is useful in initial evaluation. Bradyarrhythmia with sinus pauses High grade AV conduction block Ventricular tachyarrhythmias Rare causes (but do not miss!) Wolff Parkinson White Brugada Syndrome Long QT syndrome (LQTS) Hypertrophic cardiomyopathy (HCM) Arrhythmogenic right ventricular dysplasia (ARVC) Utility and prognostic value of obtaining ECG has been questioned



13 Example



14 Example


15 IB: Evaluation and cause of short and long term morbidity and mortality is recommended.


16 IIB: Risk factor scores do exist.
17 IIa: Transthoracic echocardiography can be useful in selected patients with syncope if cardiovascular disease is suspected. Clues: Abnormal ECG; if suspect valvular disease, LV systolic dysfunction, HCM or other structural HD (based on PE). Be aware of cost and necessity. On the other side: Class III recommendation: Routine cardiac imaging is NOT useful in evaluation of patients with syncope UNLESS cardiac etiology is suspected. Cardiac Imaging
18 Special Scenarios: EXERTIONAL SYNCOPE IIA: Exercise stress testing can be useful to establish the cause of syncope in selected patients who experience syncope or presyncope during exertion. Structural lesions: HCM, AS, anomalous coronary arteries, PH Channelopathies: LQTS, Catecholaminergic polymorphic ventricular tachycardia *Need to be completed with extreme caution and with experienced provider present.
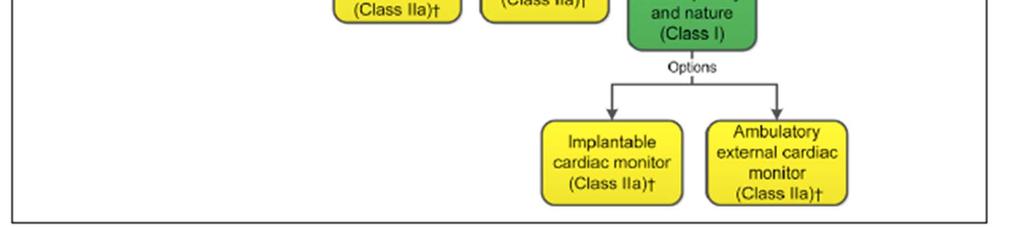
19 Cardiac Monitoring I: Choice of specific cardiac monitor should be based on frequency and nature of events hour Holter monitor Event monitor (typically 2 4 weeks) Loop recorder for more infrequent episodes MCOT monitor (continuous ECG monitoring) for 2 4 weeks I: Continuous ECG monitoring is useful for hospitalized patients for syncope of suspected cardiac etiology.
20 Electrophysiology Testing IIA: EPS can be useful for evaluation of selected patients with syncope of suspected arrhythmic etiology. Only helpful in patients who have underlying cardiac disease. Most of literature old % of patients with or without structural heart disease.
21 If diagnosis unclear after initial evaluation, tilt table testing may be useful for VVS. Tilt Table Testing (all IIA recommendations) May be useful in patients with suspected delayed OH (> 3 minutes). Reasonable to distinguish convulsive syncope from epilepsy in selected patients. Reasonable to establish diagnosis of pseudosyncope.
22 NO BENEFIT (Class III) Routine laboratory testing Routine cardiac imaging Really any ROUTINE testing should be based on overall clinical suspicion.
23 Neurologic Testing Class III: NO BENEFIT MRI and CT of the head are NOT recommended in routine evaluation of patients with syncope in absence of focal neurological findings or head injury that support further evaluation. MRI ordered in 11% and established diagnosis in 0.24% CT ordered in 57% and established diagnosis in 1% Carotid artery imaging is NOT recommended in the routine use in the absence of focal neurologic findings. Ordered in 58% and established diagnosis in 0.5%. Routine use of EEGs NOT recommended in absence of features suggesting seizure. Ordered 52% of time and established diagnosis 0.7%.

24 Warrants further evaluation

25 OVERVIEW
26 Management Recommendations For structural or inheritable arrhythmic conditions, certainly would consult cardiology. Decision making within need for ICD in parallel with management. Varies disease state by disease state. Refer to ACC/AHA guidelines for each disease state. EXAMPLE: Class I for LQTS: BB therapy (and not ICD) is recommended in patients with syncope and LQTS (Same with CPVT). VERSUS Class IIa for ARVC: ICD implantation is reasonable for syncope in ARVC. (Class I if documented sustained arrhythmia).

27 VASOVAGAL SYNCOPE

28 Orthostatic hypotension
29 Other Key Points Within guidelines, there are specific recommendations on driving restrictions depending on cause. Class I: Cardiovascular assessment by a care provider experienced in treating athletes with syncope is recommended prior to resuming competitive sports.

 use them")
30 Summary Slide 1. Be cost effective within your decision making regarding syncope work up. 2. History and Physical is everything. May require no further work up with a good thorough evaluation. 3. Take a concerning history in a young individual, particularly athlete, seriously. 4. A lot of resources are at your finger tips (risk calculators, reference of high risk features) use them to your advantage when you are unsure.


31 PART TWO: STRESS TESTING
32 CASE ONE 58 yo active male with medically treated 65% mid cx stenosis on LHC 2011 noted some chest pain while exercising at the gym. Which stress test most appropriate? Treadmill exercise Treadmill + Stress ECHO Treadmill + Nuclear myocardial perfusion scan Pharmacological nuclear myocardial perfusion imaging Dobutamine stress echocardiogram Coronary angiography
33 CASE TWO 65 yo male with HTN, HLD with atypical chest pain at rest or with exertion. Has chronic AF with slow ventricular response with PPM and underlying LBBB. Which stress test is most appropriate? Treadmill exercise Treadmill + Stress ECHO Treadmill + Nuclear myocardial perfusion scan Pharmacological nuclear myocardial perfusion imaging Dobutamine stress echocardiogram Coronary angiography
34 CASE THREE 75 yo female with DM, HTN, advanced COPD on home O2 recently seen for worsening SOB for 2 3 weeks. Which stress test most appropriate? Treadmill exercise Treadmill + Stress ECHO Treadmill + Nuclear myocardial perfusion scan Pharmacological nuclear myocardial perfusion imaging Dobutamine stress echocardiogram Coronary angiography

35 Ischemic cascade
36 Bayes Theorem The probability of a new event, or true positive stress test, depends on the pre test risk of the patient which have been derived from empiric data


37 Stress Testing= Intermediate Risk Patients CHEST PAIN FEATURES: Typical: Substernal Exertional Relieved by rest or nitroglycerin Typical 3/3 Atypical 2/3 Noncardiac 1/3
38 Within decision making, THINK: STRESS EXERCISE if able, gold standard VASODILATOR Ragadenosone (Lexiscan) Adenosine (Persantine) Beta agonist Dobutamine TEST ECG ECHOCARDIOGRAM SPECT nuclear imaging PET imaging Cardiac MRI

39 7. Cardiac MRI
40 Stress Testing Sensitivity and Specificity
41 Local availability and expertise Ability to exercise Clinical factors impacting stress test modality Resting ECG abnormalities Patient s body habitus Limited acoustic windows for echocardiography History of prior coronary revascularization Radiation exposure Need for concomitant assessment of hemodynamics or valvular disease
42 Basic Algorithm ECG uninterpretable: WPW Ventricular paced rhythm LBBB > 1 mm ST depression at rest Digoxin with ST changes LVH with ST T wave abnormalities EXERCISE ECG ECG uninterpretable or history of prior revascularization? Can the patient exercise? YES NO Active wheezing, history of advanced conduction disease History of tachyarrhythmia, severe HTN Avoid regadenoson/ adenosine Avoid Dobutamine Exercise ECG ONLY NO YES ADD IMAGING IMAGING Preference: LBBB or RV pacing > SPECT imaging may be preferred Marked obesity > PET vs. cmri (if can fit) if available Myocardial viability > PET or cmri


43 Treadmill Exercise Stress Test Protocol: Follow Bruce Protocol and achieve 85% max predicted HR (220 age) End Points: HR, BP, Exercise capacity, ECG symptoms Hold BB 24 hours prior Indications: Normal resting ECG Least expensive; provides good measure of functional capacity Prognostic value Limitations: Non diagnostic ECG: LBBB, paced, LVH, ST depression > 0.5 mm Lower sensitivity and specificity. Non localizing (unless has ST elevation)
44 Treadmill Exercise ECG Duke Treadmill Score: Unfavorable: (5% mortality) Exercise minutes (ST deviation in mm x 5) (angina index x 4) Score < 11 HIGH RISK 5 yr survival 75% Score 10 to 4+ MODERATE RISK 5 yr survival 75 95% Score > +5 LOW RISK 5 yr survival 95% Workload < 4 METS ST depression > 1 mm Failure to increased SBP > 120 Exercise induced ST elevation Angina pectoris at low exercise work Sustained or symptomatic VT



45 Why obtain imaging? LBBB Paced rhythm Abnormal ST segments at baseline LVH with repolarization WPW Patients with prior revascularization
 Less sensitive than myocardial perfusion imaging (requires")
46 Stress Echocardiogram Dobutamine OR Advantages: Direct visualization of walls, localize region of abnormality Higher specificity than perfusion imaging (3v disease, LM), higher sensitivity than treadmill NO radiation Disadvantages: May be technically difficult with poor acoustic windows (could obtain ideal images at less than MPHR) Less sensitive than myocardial perfusion imaging (requires ischemia) Subjective interpretation False negative: more common in single vessel disease (particularly circumflex)


47 SPECT nuclear imaging Vasodilator OR Advantages: Used in moderate to high pre test probability Can risk stratify, look at perfusion and function, localize disease Higher sensitivity than stress echo Limitations Expensive Decreased specificity particularly related to attenuation artifact Radiation exposure Cannot assess myocardium or valves High Risk Scan Findings: Multiple reversible defects, large perfusion defect Transient dilatation of left ventricle Depressed resting LVEF Increase RV radiotracer uptake
48 THE ISCHEMIC CASCADE Exercise ECG STRESS ECHO Nuclear MPI Sensitivity
")
 Limitations:")
49 A word about cmri within stress testing Stress Cardiac MRI Better quality images In general, cannot exercise (uses adenosine) Provides structural, perfusion, viability associated with scar pattern (which could influence risk of SCD) Limitations: Availability, cost
50 CASE ONE 58 yo active male with medically treated 65% mid cx stenosis on LHC 2011 noted some chest pain while exercising at the gym. Which stress test most appropriate? Treadmill exercise Treadmill + Stress ECHO Treadmill + Nuclear myocardial perfusion scan Pharmacological nuclear myocardial perfusion imaging Dobutamine stress echocardiogram Coronary angiography
51 CASE TWO 65 yo male with HTN, HLD with atypical chest pain at rest or with exertion. Has chronic AF with slow ventricular response with PPM and underlying LBBB. Which stress test is most appropriate? Treadmill exercise Treadmill + Stress ECHO Treadmill + Nuclear myocardial perfusion scan Pharmacological nuclear myocardial perfusion imaging Dobutamine stress echocardiogram Coronary angiography
52 CASE THREE 75 yo female with DM, HTN, advanced COPD on home O2 recently seen for worsening SOB for 2 3 weeks. Which stress test most appropriate? Treadmill exercise Treadmill + Stress ECHO Treadmill + Nuclear myocardial perfusion scan Pharmacological nuclear myocardial perfusion imaging Dobutamine stress echocardiogram Coronary angiography
53 Questions to consider when ordering What is your pre test probability of CAD? Reason for ordering stress test? Hold BB or not? Advantages and limitations of each stress modality? Ability to exercise? Normal or abnormal resting ECG? Contraindication to certain choice of agent/test (ie severe COPD on O2)? Cost/Availability Cost: Exercise ECG < Stress echo < SPECT < cmri/pet < LHC
54 Summary Appropriate for intermediate risk patients. If can exercise and has interpretable ECG, should get exercise ECG stress testing. If can exercise, do it! Provides prognostic data. Choice between Dobutamine echocardiogram vs. vasodilator SPECT imaging (part may be center dependent availability, expertise). We will start seeing more cmri and PET stress testing, particularly in those with difficult imaging, need for assessment of myocardial viability. Keep in mind that stress cmri is only available with vasodilator (adenosine) in Indianapolis (cannot get exercise data).


55 THANK YOU! QUESTIONS!?
56 References Angus S et al. The Cost Effective Evaluation of Syncope. Med Clin North AM. 2016: 100 (5): Shen et al ACC/AHA/HRS Guideline for Evaluation and Management of Patients with Syncope. Circulation. 2017: 136. Gajulapalli et al. Cardiac Stress Testing for Diagnosis and Management of Coronary Artery Disease: A reference for the Primary Care Physician. Southern Medical Journal. 2012: 105 (2):
Choosing the Appropriate Stress Test: Brett C. Stoll, MD, FACC February 24, 2018
 Choosing the Appropriate Stress Test: Brett C. Stoll, MD, FACC February 24, 2018 Choosing the Appropriate Stress Test: Does it Really Matter? Brett C. Stoll, MD, FACC February 24, 2018 Conflicts of Interest
Choosing the Appropriate Stress Test: Brett C. Stoll, MD, FACC February 24, 2018 Choosing the Appropriate Stress Test: Does it Really Matter? Brett C. Stoll, MD, FACC February 24, 2018 Conflicts of Interest
Syncope Guidelines What s new? October 19 th 2017 Mohamed Aljaabari MBBCh, FACC, FHRS Consultant Electrophysiologist - Mafraq Hospital
 Syncope Guidelines What s new? October 19 th 2017 Mohamed Aljaabari MBBCh, FACC, FHRS Consultant Electrophysiologist - Mafraq Hospital Case Presentation 35 Male presented with sudden loss of consciousness
Syncope Guidelines What s new? October 19 th 2017 Mohamed Aljaabari MBBCh, FACC, FHRS Consultant Electrophysiologist - Mafraq Hospital Case Presentation 35 Male presented with sudden loss of consciousness
My Patient Needs a Stress Test
 My Patient Needs a Stress Test Amy S. Burhanna,, MD, FACC Coastal Cardiology Cape May Court House, New Jersey Absolute and relative contraindications to exercise testing Absolute Acute myocardial infarction
My Patient Needs a Stress Test Amy S. Burhanna,, MD, FACC Coastal Cardiology Cape May Court House, New Jersey Absolute and relative contraindications to exercise testing Absolute Acute myocardial infarction
An Approach to the Patient with Syncope. Guy Amit MD, MPH Soroka University Medical Center Beer-Sheva
 An Approach to the Patient with Syncope Guy Amit MD, MPH Soroka University Medical Center Beer-Sheva Case presentation A 23 y.o. man presented with 2 episodes of syncope One during exercise,one at rest
An Approach to the Patient with Syncope Guy Amit MD, MPH Soroka University Medical Center Beer-Sheva Case presentation A 23 y.o. man presented with 2 episodes of syncope One during exercise,one at rest
Index. cardiology.theclinics.com. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Adenosine in idiopathic AV block, 445 446 Adolescent(s) syncope in, 397 409. See also Syncope, in children and adolescents AECG monitoring.
Index Note: Page numbers of article titles are in boldface type. A Adenosine in idiopathic AV block, 445 446 Adolescent(s) syncope in, 397 409. See also Syncope, in children and adolescents AECG monitoring.
Lee Chee Wan. Senior Consultant Pacing and Cardiac Electrophysiology. GP Symposium 2 nd April 2016
 Lee Chee Wan Senior Consultant Pacing and Cardiac Electrophysiology GP Symposium 2 nd April 2016 Objectives Definition of syncope Common causes of syncope & impacts How to clinically assess patient with
Lee Chee Wan Senior Consultant Pacing and Cardiac Electrophysiology GP Symposium 2 nd April 2016 Objectives Definition of syncope Common causes of syncope & impacts How to clinically assess patient with
Cardiac Conditions in Sport & Exercise. Cardiac Conditions in Sport. USA - Sudden Cardiac Death (SCD) Dr Anita Green. Sudden Cardiac Death
 Dr Anita Green. Sudden Cardiac Death") Cardiac Conditions in Sport & Exercise Dr Anita Green Cardiac Conditions in Sport Sudden Cardiac Death USA - Sudden Cardiac Death (SCD)
Cardiac Conditions in Sport & Exercise Dr Anita Green Cardiac Conditions in Sport Sudden Cardiac Death USA - Sudden Cardiac Death (SCD)
Syncope Guidelines: What s New?
 Syncope Guidelines: What s New? Dr. Samuel Asirvatham Professor of Medicine and Pediatrics Mayo Clinic College of Medicine Medical Director, Electrophysiology Laboratory Program Director, EP Fellowship
Syncope Guidelines: What s New? Dr. Samuel Asirvatham Professor of Medicine and Pediatrics Mayo Clinic College of Medicine Medical Director, Electrophysiology Laboratory Program Director, EP Fellowship
HEART CONDITIONS IN SPORT
 HEART CONDITIONS IN SPORT Dr. Anita Green CHD Risk Factors Smoking Hyperlipidaemia Hypertension Obesity Physical Inactivity Diabetes Risks are cumulative (multiplicative) Lifestyles predispose to RF One
HEART CONDITIONS IN SPORT Dr. Anita Green CHD Risk Factors Smoking Hyperlipidaemia Hypertension Obesity Physical Inactivity Diabetes Risks are cumulative (multiplicative) Lifestyles predispose to RF One
Stress Testing:Which Study is Indicated for My Patient?
 Stress Testing:Which Study is Indicated for My Patient? Cardiology-Primary Care Conference 7/14/17 Peter Casterella, MD Co-Executive Director Swedish Heart and Vascular Institute 1 Stress Testing Options
Stress Testing:Which Study is Indicated for My Patient? Cardiology-Primary Care Conference 7/14/17 Peter Casterella, MD Co-Executive Director Swedish Heart and Vascular Institute 1 Stress Testing Options
I have no financial disclosures
 Manpreet Singh MD I have no financial disclosures Exercise Treadmill Bicycle Functional capacity assessment Well validated prognostic value Ischemic assessment ECG changes ST segments Arrhythmias Hemodynamic
Manpreet Singh MD I have no financial disclosures Exercise Treadmill Bicycle Functional capacity assessment Well validated prognostic value Ischemic assessment ECG changes ST segments Arrhythmias Hemodynamic
CHRONIC CAD DIAGNOSIS
 CHRONIC CAD DIAGNOSIS Chest Pain Evaluation 1. Approach to diagnosis of CAD 2. Classification of chest pain 3. Pre-test likelihood CAD 4. Algorithm for chest pain evaluation in women 5. Indications for
CHRONIC CAD DIAGNOSIS Chest Pain Evaluation 1. Approach to diagnosis of CAD 2. Classification of chest pain 3. Pre-test likelihood CAD 4. Algorithm for chest pain evaluation in women 5. Indications for
Clinical Evaluation & Management of Syncope:UPDATE
 Clinical Evaluation & Management of Syncope:UPDATE 2017 ACC/AHA/HRS Guideline for the Evaluation and Management of Patients With Syncope Developed in Collaboration with the American College of Emergency
Clinical Evaluation & Management of Syncope:UPDATE 2017 ACC/AHA/HRS Guideline for the Evaluation and Management of Patients With Syncope Developed in Collaboration with the American College of Emergency
Exercise Test: Practice and Interpretation. Jidong Sung Division of Cardiology Samsung Medical Center Sungkyunkwan University School of Medicine
 Exercise Test: Practice and Interpretation Jidong Sung Division of Cardiology Samsung Medical Center Sungkyunkwan University School of Medicine 2 Aerobic capacity and survival Circulation 117:614, 2008
Exercise Test: Practice and Interpretation Jidong Sung Division of Cardiology Samsung Medical Center Sungkyunkwan University School of Medicine 2 Aerobic capacity and survival Circulation 117:614, 2008
Index. cardiacep.theclinics.com. Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type. A AEDs. See Automated external defibrillators (AEDs) AF. See Atrial fibrillation (AF) Age as factor in SD in marathon runners, 45 Antiarrhythmic
Note: Page numbers of article titles are in boldface type. A AEDs. See Automated external defibrillators (AEDs) AF. See Atrial fibrillation (AF) Age as factor in SD in marathon runners, 45 Antiarrhythmic
Choosing the Right Cardiac Test. Outline
 Choosing the Right Cardiac Test Atif Qasim, M.D., M.S.C.E. University of California, San Francisco Disclosures: None 2013 Outline Focus on choosing the optimal tests for coronary disease evaluation Overview
Choosing the Right Cardiac Test Atif Qasim, M.D., M.S.C.E. University of California, San Francisco Disclosures: None 2013 Outline Focus on choosing the optimal tests for coronary disease evaluation Overview
Syncope (From a Cardiologist s Perspective) Patrick Henderson, DO 118 th OOA Annual Convention Internal Medicine Specialty Track April 28 th, 2018
 Patrick Henderson, DO 118 th OOA Annual Convention Internal Medicine Specialty Track April 28 th, 2018") Syncope (From a Cardiologist s Perspective) Patrick Henderson, DO 118 th OOA Annual Convention Internal Medicine Specialty Track April 28 th, 2018 No financial disclosures to report Goals Formally define
Syncope (From a Cardiologist s Perspective) Patrick Henderson, DO 118 th OOA Annual Convention Internal Medicine Specialty Track April 28 th, 2018 No financial disclosures to report Goals Formally define
DEPARTMENT NAME PRE-PARTICIPATION SCREENING THE SPORTS PHYSICAL
 PRE-PARTICIPATION SCREENING THE SPORTS PHYSICAL Michele Krenek, MSN, RN, FNP-C TCHAPP Conference, Houston, TX April 4, 2019 PRE-PARTICIPATION SPORTS SCREENING According to the AHA the definition of the
PRE-PARTICIPATION SCREENING THE SPORTS PHYSICAL Michele Krenek, MSN, RN, FNP-C TCHAPP Conference, Houston, TX April 4, 2019 PRE-PARTICIPATION SPORTS SCREENING According to the AHA the definition of the
Case Question. Evaluation of Chest pain in the Office and Cardiac Stress Testing
 Evaluation of Chest pain in the Office and Cardiac Stress Testing Chad Link, DO FACC Sparrow Hospital Thoracic and Cardiovascular Institute Chairman- TCI Cardiology Section Disclosures Speakers Bureau
Evaluation of Chest pain in the Office and Cardiac Stress Testing Chad Link, DO FACC Sparrow Hospital Thoracic and Cardiovascular Institute Chairman- TCI Cardiology Section Disclosures Speakers Bureau
Sudden cardiac death: Primary and secondary prevention
 Sudden cardiac death: Primary and secondary prevention By Kai Chi Chan Penultimate Year Medical Student St George s University of London at UNic Sheba Medical Centre Definition Sudden cardiac arrest (SCA)
Sudden cardiac death: Primary and secondary prevention By Kai Chi Chan Penultimate Year Medical Student St George s University of London at UNic Sheba Medical Centre Definition Sudden cardiac arrest (SCA)
Stress ECG is still Viable in Suleiman M Kharabsheh, MD, FACC Consultant Invasive Cardiologist KFHI KFSHRC-Riyadh
 Stress ECG is still Viable in 2016 Suleiman M Kharabsheh, MD, FACC Consultant Invasive Cardiologist KFHI KFSHRC-Riyadh Stress ECG Do we still need stress ECG with all the advances we have in the CV field?
Stress ECG is still Viable in 2016 Suleiman M Kharabsheh, MD, FACC Consultant Invasive Cardiologist KFHI KFSHRC-Riyadh Stress ECG Do we still need stress ECG with all the advances we have in the CV field?
Syncope: Evaluation of the Weak and Dizzy
 Syncope: Evaluation of the Weak and Dizzy William M. Miles, MD, FACC, FHRS Professor of Medicine Silverstein Chair for Cardiovascular Education University of Florida College of Medicine Disclosures Medtronic,
Syncope: Evaluation of the Weak and Dizzy William M. Miles, MD, FACC, FHRS Professor of Medicine Silverstein Chair for Cardiovascular Education University of Florida College of Medicine Disclosures Medtronic,
Disclosures. I have no financial disclosures relevant to the talk
 Syncope Sachin S. Sule, MD, FACP Associate Professor of Integrated Medical Science Division of Medicine Director,Internal Medicine Residency Program Charles E. Schmidt College of Medicine, Florida Atlantic
Syncope Sachin S. Sule, MD, FACP Associate Professor of Integrated Medical Science Division of Medicine Director,Internal Medicine Residency Program Charles E. Schmidt College of Medicine, Florida Atlantic
Rapid Access Clinics for Transient Loss of Consciousness
 Rapid Access Clinics for Transient Loss of Consciousness Michael Gammage Department of Cardiovascular Medicine University of Birmingham and University Hospital Birmingham NHS Foundation Trust Those who
Rapid Access Clinics for Transient Loss of Consciousness Michael Gammage Department of Cardiovascular Medicine University of Birmingham and University Hospital Birmingham NHS Foundation Trust Those who
Cardiac Risk Factors and Noninvasive Cardiac Diagnosis-ECG, ECHO, et al. Martin C. Burke, DO, FACOI ACOI IM Board Review Course 2018
 Cardiac Risk Factors and Noninvasive Cardiac Diagnosis-ECG, ECHO, et al. Martin C. Burke, DO, FACOI ACOI IM Board Review Course 2018 No Disclosures The American Heart Association Evidence-Based Scoring
Cardiac Risk Factors and Noninvasive Cardiac Diagnosis-ECG, ECHO, et al. Martin C. Burke, DO, FACOI ACOI IM Board Review Course 2018 No Disclosures The American Heart Association Evidence-Based Scoring
Syncope: Evaluation of the Weak and Dizzy
 Syncope: Evaluation of the Weak and Dizzy William M. Miles, MD, FACC, FHRS Professor of Medicine Silverstein Chair for Cardiovascular Education University of Florida College of Medicine Disclosures Medtronic,
Syncope: Evaluation of the Weak and Dizzy William M. Miles, MD, FACC, FHRS Professor of Medicine Silverstein Chair for Cardiovascular Education University of Florida College of Medicine Disclosures Medtronic,
Syncope By Remus Popa
 Syncope By Remus Popa A 66 years old male is brought to the ED from a restaurant where he fainted while dining out with his family. He complained of nausea and stood up to go to the restroom but immediately
Syncope By Remus Popa A 66 years old male is brought to the ED from a restaurant where he fainted while dining out with his family. He complained of nausea and stood up to go to the restroom but immediately
7. Echocardiography Appropriate Use Criteria (by Indication)
") Criteria for Echocardiography 1133 7. Echocardiography Criteria (by ) Table 1. TTE for General Evaluation of Cardiac Structure and Function Suspected Cardiac Etiology General With TTE 1. Symptoms or conditions
Criteria for Echocardiography 1133 7. Echocardiography Criteria (by ) Table 1. TTE for General Evaluation of Cardiac Structure and Function Suspected Cardiac Etiology General With TTE 1. Symptoms or conditions
Severe Hypertension. Pre-referral considerations: 1. BP of arm and Leg 2. Ambulatory BP 3. Renal causes
 Severe Hypertension *Prior to making a referral, call office or Doc Halo, to speak with a Cardiologist or APP to discuss patient and possible treatment options. Please only contact the patient's cardiologist.
Severe Hypertension *Prior to making a referral, call office or Doc Halo, to speak with a Cardiologist or APP to discuss patient and possible treatment options. Please only contact the patient's cardiologist.
DECLARATION OF CONFLICT OF INTEREST
 DECLARATION OF CONFLICT OF INTEREST The Management of Syncope remains a challenge: Clues from the History Richard Sutton, DSc Emeritus Professor of Cardiology Imperial College, St Mary s Hospital, London,
DECLARATION OF CONFLICT OF INTEREST The Management of Syncope remains a challenge: Clues from the History Richard Sutton, DSc Emeritus Professor of Cardiology Imperial College, St Mary s Hospital, London,
Detailed Order Request Checklists for Cardiology
 Next Generation Solutions Detailed Order Request Checklists for Cardiology 8600 West Bryn Mawr Avenue South Tower Suite 800 Chicago, IL 60631 www.aimspecialtyhealth.com Appropriate.Safe.Affordable 2018
Next Generation Solutions Detailed Order Request Checklists for Cardiology 8600 West Bryn Mawr Avenue South Tower Suite 800 Chicago, IL 60631 www.aimspecialtyhealth.com Appropriate.Safe.Affordable 2018
9/2/2016 CARDIOLOGY TESTING WHAT TO ORDER WHEN REFERENCE OBJECTIVES
 CARDIOLOGY TESTING WHAT TO ORDER WHEN A J W A D F A R A H, M S, P A - C A S S O C I A T E D I R E C T O R O F M E D I C A L O P E R A T I O N S O F A D V A N C E D P R A C T I C E P R O V I D E R S W I
CARDIOLOGY TESTING WHAT TO ORDER WHEN A J W A D F A R A H, M S, P A - C A S S O C I A T E D I R E C T O R O F M E D I C A L O P E R A T I O N S O F A D V A N C E D P R A C T I C E P R O V I D E R S W I
Syncope Update Dr Matthew Lovell, Consultant in Cardiology
 Syncope Update Dr Matthew Lovell, Consultant in Cardiology Definition of Syncope Syncope is defined as TLOC due to cerebral hypoperfusion Characterized by a rapid onset, short duration, and spontaneous
Syncope Update Dr Matthew Lovell, Consultant in Cardiology Definition of Syncope Syncope is defined as TLOC due to cerebral hypoperfusion Characterized by a rapid onset, short duration, and spontaneous
The Value of Stress MRI in Evaluation of Myocardial Ischemia
 The Value of Stress MRI in Evaluation of Myocardial Ischemia Dr. Saeed Al Sayari, MBBS, EBCR, MBA Department of Radiology and Nuclear Medicine Mafraq Hospital, Abu Dhabi United Arab Emirates Introduction
The Value of Stress MRI in Evaluation of Myocardial Ischemia Dr. Saeed Al Sayari, MBBS, EBCR, MBA Department of Radiology and Nuclear Medicine Mafraq Hospital, Abu Dhabi United Arab Emirates Introduction
Risk Stratification for CAD for the Primary Care Provider
 Risk Stratification for CAD for the Primary Care Provider Shimoli Shah MD Assistant Professor of Medicine Directory, Ambulatory Cardiology Clinic Knight Cardiovascular Institute Oregon Health & Sciences
Risk Stratification for CAD for the Primary Care Provider Shimoli Shah MD Assistant Professor of Medicine Directory, Ambulatory Cardiology Clinic Knight Cardiovascular Institute Oregon Health & Sciences
Angina Luis Tulloch, MD 03/27/2012
 Angina Luis Tulloch, MD 03/27/2012 Acute coronary syndromes ACS STE > 1 mm, new LBBB* Increased cardiac enzymes STEMI Yes Yes NSTEMI No Yes UA No No *Recognize Wellen s sign/syndrome, posterior wall MI,
Angina Luis Tulloch, MD 03/27/2012 Acute coronary syndromes ACS STE > 1 mm, new LBBB* Increased cardiac enzymes STEMI Yes Yes NSTEMI No Yes UA No No *Recognize Wellen s sign/syndrome, posterior wall MI,
Case Discussion. Date: 2011/03/12 Reporter: FM R1 宋泓逸 Supervisor: F1 許瓅文
 Case Discussion Date: 2011/03/12 Reporter: FM R1 宋泓逸 Supervisor: F1 許瓅文 Discussion Syncope: in the emergency department References Articles from UpToDate, keyword as syncope Harrison s internal medicine,
Case Discussion Date: 2011/03/12 Reporter: FM R1 宋泓逸 Supervisor: F1 許瓅文 Discussion Syncope: in the emergency department References Articles from UpToDate, keyword as syncope Harrison s internal medicine,
Optimal testing for coronary artery disease in symptomatic and asymptomatic patients
 Optimal testing for coronary artery disease in symptomatic and asymptomatic patients Alexandre C Ferreira, MD Clinical Chief of Cardiology Jackson Health System Director, Interventional Cardiology Training
Optimal testing for coronary artery disease in symptomatic and asymptomatic patients Alexandre C Ferreira, MD Clinical Chief of Cardiology Jackson Health System Director, Interventional Cardiology Training
Risk Factors for Sudden cardiac Death
 Risk Factors for Sudden cardiac Death A. Arenal Arrhythmias in competitive sports Disclosure Conflict of interest Advisory board: Medtronic, Boston Scientific Research grants: Medtronic, Boston Scientific,
Risk Factors for Sudden cardiac Death A. Arenal Arrhythmias in competitive sports Disclosure Conflict of interest Advisory board: Medtronic, Boston Scientific Research grants: Medtronic, Boston Scientific,
ASE 2011 Appropriate Use Criteria for Echocardiography
 ASE 2011 Appropriate Use Criteria for Echocardiography Table 1. TTE for General Evaluation of Cardiac Structure and Function 1 2 Suspected Cardiac Etiology General With TTE Symptoms or conditions potentially
ASE 2011 Appropriate Use Criteria for Echocardiography Table 1. TTE for General Evaluation of Cardiac Structure and Function 1 2 Suspected Cardiac Etiology General With TTE Symptoms or conditions potentially
P F = R. Disorder of the Breast. Approach to the Patient with Chest Pain. Typical Characteristics of Angina Pectoris. Myocardial Ischemia
 Disorder of the Breast Approach to the Patient with Chest Pain Anthony J. Minisi, MD Department of Internal Medicine, Division of Cardiology Virginia Commonwealth University School of Medicine William
Disorder of the Breast Approach to the Patient with Chest Pain Anthony J. Minisi, MD Department of Internal Medicine, Division of Cardiology Virginia Commonwealth University School of Medicine William
Arrhythmias (II) Ventricular Arrhythmias. Disclosures
 Ventricular Arrhythmias. Disclosures") Arrhythmias (II) Ventricular Arrhythmias Amy Leigh Miller, MD, PhD Cardiovascular Electrophysiology, Brigham & Women s Hospital Disclosures None Rhythms and Mortality Implantable loop recorder post-mi
Arrhythmias (II) Ventricular Arrhythmias Amy Leigh Miller, MD, PhD Cardiovascular Electrophysiology, Brigham & Women s Hospital Disclosures None Rhythms and Mortality Implantable loop recorder post-mi
Syncope : What tests should I do? Boon Lim Consultant Cardiologist Clinical Lead for Imperial Syncope Unit Hammersmith Hospital
 Syncope : What tests should I do? Boon Lim Consultant Cardiologist Clinical Lead for Imperial Syncope Unit Hammersmith Hospital The most important diagnostic test is History taking Why is history taking
Syncope : What tests should I do? Boon Lim Consultant Cardiologist Clinical Lead for Imperial Syncope Unit Hammersmith Hospital The most important diagnostic test is History taking Why is history taking
Clinical Case 1 A patient with a syncope Panos E. Vardas President Elect of the ESC, Prof of Cardiology, University Hospital of Crete
 Clinical Case 1 A patient with a syncope Panos E. Vardas President Elect of the ESC, Prof. of Cardiology, University Hospital of Crete Case presentation A 64-year-old male smoker, with arterial hypertension
Clinical Case 1 A patient with a syncope Panos E. Vardas President Elect of the ESC, Prof. of Cardiology, University Hospital of Crete Case presentation A 64-year-old male smoker, with arterial hypertension
Valutazione iniziale e stratificazione del rischio
 Valutazione iniziale e stratificazione del rischio Paolo Alboni Sezione di Cardiologia Ospedale Privato Quisisana Ferrara DEFINITION OF SYNCOPE Syncope is a transient loss of consciousness due to global
Valutazione iniziale e stratificazione del rischio Paolo Alboni Sezione di Cardiologia Ospedale Privato Quisisana Ferrara DEFINITION OF SYNCOPE Syncope is a transient loss of consciousness due to global
The use of Cardiac CT and MRI in Clinical Practice
 The use of Cardiac CT and MRI in Clinical Practice Matthew W. Martinez, MD Assistant Professor of Medicine LVPG - Lehigh Valley Heart Specialists Lehigh Valley Health Network Oct. 3, 2009 DISCLOSURE Relevant
The use of Cardiac CT and MRI in Clinical Practice Matthew W. Martinez, MD Assistant Professor of Medicine LVPG - Lehigh Valley Heart Specialists Lehigh Valley Health Network Oct. 3, 2009 DISCLOSURE Relevant
21st Annual Contemporary Therapeutic Issues in Cardiovascular Disease
 21st Annual Contemporary Therapeutic Issues in Cardiovascular Disease Noninvasive Evaluation of Coronary Artery Disease: Anatomical, Functional, Clinical May 5, 2018 Mark Hansen MD FRCPC Cardiologist,
21st Annual Contemporary Therapeutic Issues in Cardiovascular Disease Noninvasive Evaluation of Coronary Artery Disease: Anatomical, Functional, Clinical May 5, 2018 Mark Hansen MD FRCPC Cardiologist,
Pearls & Pitfalls in nuclear cardiology
 Pearls & Pitfalls in nuclear cardiology Maythinee Chantadisai, MD., NM physician Division of Nuclear Medicine, Department of radiology, KCMH Principle of myocardial perfusion imaging (MPI) Radiotracer
Pearls & Pitfalls in nuclear cardiology Maythinee Chantadisai, MD., NM physician Division of Nuclear Medicine, Department of radiology, KCMH Principle of myocardial perfusion imaging (MPI) Radiotracer
Cardiac evaluation for the noncardiac. Nathaen Weitzel MD University of Colorado Denver Dept of Anesthesiology
 Cardiac evaluation for the noncardiac patient Nathaen Weitzel MD University of Colorado Denver Dept of Anesthesiology Objectives! Review ACC / AHA guidelines as updated for 2009! Discuss new recommendations
Cardiac evaluation for the noncardiac patient Nathaen Weitzel MD University of Colorado Denver Dept of Anesthesiology Objectives! Review ACC / AHA guidelines as updated for 2009! Discuss new recommendations
ECG Workshop. Nezar Amir
 ECG Workshop Nezar Amir Myocardial Ischemia ECG Infarct ECG in STEMI is dynamic & evolving Common causes of ST shift Infarct Localisation Left main artery occlusion: o diffuse ST-depression with ST elevation
ECG Workshop Nezar Amir Myocardial Ischemia ECG Infarct ECG in STEMI is dynamic & evolving Common causes of ST shift Infarct Localisation Left main artery occlusion: o diffuse ST-depression with ST elevation
EVALUATION OF THE ATHLETE. Karen Stout, MD Professor, Medicine and Pediatrics University of Washington
 EVALUATION OF THE 12 ATHLETE Karen Stout, MD Professor, Medicine and Pediatrics University of Washington NO DISCLOSURES OUTLINE Why evaluate athletes? What s the problem? What evaluation should be done?
EVALUATION OF THE 12 ATHLETE Karen Stout, MD Professor, Medicine and Pediatrics University of Washington NO DISCLOSURES OUTLINE Why evaluate athletes? What s the problem? What evaluation should be done?
Cardiac Imaging. Kimberly Delcour, DO, FACC. Mahi Ashwath, MD, FACC, FASE. Director, Cardiac CT. Director, Cardiac MRI
 Cardiac Imaging Kimberly Delcour, DO, FACC Director, Cardiac CT Mahi Ashwath, MD, FACC, FASE Director, Cardiac MRI Cardiac Imaging Discuss the clinical applications of and indications for: Cardiac CT Nuclear
Cardiac Imaging Kimberly Delcour, DO, FACC Director, Cardiac CT Mahi Ashwath, MD, FACC, FASE Director, Cardiac MRI Cardiac Imaging Discuss the clinical applications of and indications for: Cardiac CT Nuclear
Chest Pain Wave I. Making Dollars and Sense Out of Stress Testing
 Chest Pain Wave I Making Dollars and Sense Out of Stress Testing Presenters Kristin Newby, MD, FACC Michael Kontos, MD, FACC Disclosures Dr. Newby: None specifically related to this activity All RWI are
Chest Pain Wave I Making Dollars and Sense Out of Stress Testing Presenters Kristin Newby, MD, FACC Michael Kontos, MD, FACC Disclosures Dr. Newby: None specifically related to this activity All RWI are
Management of Syncope in Heart Failure. University of Iowa
 Management of Syncope in Heart Failure Brian Olshansky University of Iowa 1 Syncope Transient loss of consciousness, with rapid, usually complete, recovery, with or without prodrome A common, non-specific,
Management of Syncope in Heart Failure Brian Olshansky University of Iowa 1 Syncope Transient loss of consciousness, with rapid, usually complete, recovery, with or without prodrome A common, non-specific,
Appropriateness of Stress Echocardiography and Nuclear Stress Thallium/Sesta Mibi Testing Methods
 Appropriateness of Stress Echocardiography and Nuclear Stress Thallium/Sesta Mibi Testing Methods Review by Michael Devenport, MS, RDCS Objectives: A basic description and review of appropriate use of
Appropriateness of Stress Echocardiography and Nuclear Stress Thallium/Sesta Mibi Testing Methods Review by Michael Devenport, MS, RDCS Objectives: A basic description and review of appropriate use of
IHCP bulletin INDIANA HEALTH COVERAGE PROGRAMS BT JANUARY 24, 2012
 IHCP bulletin INDIANA HEALTH COVERAGE PROGRAMS BT201203 JANUARY 24, 2012 The IHCP to reimburse implantable cardioverter defibrillators separately from outpatient implantation Effective March 1, 2012, the
IHCP bulletin INDIANA HEALTH COVERAGE PROGRAMS BT201203 JANUARY 24, 2012 The IHCP to reimburse implantable cardioverter defibrillators separately from outpatient implantation Effective March 1, 2012, the
Syncope. A Symptom not a Diagnosis
 A Symptom not a Diagnosis Vijay Duggirala, MD Assistant Professor-Clinical Department of Internal Medicine Division of Hospital Medicine The Ohio State University Wexner Medical Center Objectives Define
A Symptom not a Diagnosis Vijay Duggirala, MD Assistant Professor-Clinical Department of Internal Medicine Division of Hospital Medicine The Ohio State University Wexner Medical Center Objectives Define
Welcome! To submit questions during the presentation: or Text:
 Welcome! To participate in the interactive Q & A please do the following: 1. Download the Socrative Student App 2. Enter Teacher s Room Code: ZD0F3X5Q 3. Select Quiz: Intermountain Cardiac Stress Testing
Welcome! To participate in the interactive Q & A please do the following: 1. Download the Socrative Student App 2. Enter Teacher s Room Code: ZD0F3X5Q 3. Select Quiz: Intermountain Cardiac Stress Testing
Death after Syncope: Can we predict it? Daniel Zamarripa, MD Senior Medical Director December 2013
 Death after Syncope: Can we predict it? Daniel Zamarripa, MD Senior Medical Director December 2013 Death after Syncope: Can we predict it? Those who suffer from frequent and severe fainting often die suddenly
Death after Syncope: Can we predict it? Daniel Zamarripa, MD Senior Medical Director December 2013 Death after Syncope: Can we predict it? Those who suffer from frequent and severe fainting often die suddenly
Syncope. A Symptom not a Diagnosis. Vijay Duggirala, MD
 Syncope A Symptom not a Diagnosis Vijay Duggirala, MD Assistant Professor-Clinical Department of Internal Medicine Division of Hospital Medicine The Ohio State University Wexner Medical Center Objectives
Syncope A Symptom not a Diagnosis Vijay Duggirala, MD Assistant Professor-Clinical Department of Internal Medicine Division of Hospital Medicine The Ohio State University Wexner Medical Center Objectives
Antony French Consultant Cardiologist & Electrophysiologist
 Antony French Consultant Cardiologist & Electrophysiologist Palpitations Unpleasant awareness of rapid or forceful heart beat Not all tachycardias cause palpitations, and not all palpitations are due to
Antony French Consultant Cardiologist & Electrophysiologist Palpitations Unpleasant awareness of rapid or forceful heart beat Not all tachycardias cause palpitations, and not all palpitations are due to
Diagnosis of CAD S Richard Underwood
 Diagnosis of CAD S Richard Underwood Professor of Cardiac Imaging Royal Brompton Hospital & Imperial College Faculty of Medicine London, UK The history and diagnosis 89% Non-cardiac chest pain 50% Atypical
Diagnosis of CAD S Richard Underwood Professor of Cardiac Imaging Royal Brompton Hospital & Imperial College Faculty of Medicine London, UK The history and diagnosis 89% Non-cardiac chest pain 50% Atypical
Improving Patient Outcomes with a Syncope Center. Suneet Mittal, MD
 Improving Patient Outcomes with a Syncope Center Suneet Mittal, MD Improving Patient Outcomes with a Syncope Center: Early Risk Stratification of Patients who Require Device Therapy Suneet Mittal, MD Director,
Improving Patient Outcomes with a Syncope Center Suneet Mittal, MD Improving Patient Outcomes with a Syncope Center: Early Risk Stratification of Patients who Require Device Therapy Suneet Mittal, MD Director,
Which Test When? Avoid the Stress of Stress Testing. Marc Newell, MD, FACC, FSCCT Minneapolis Heart Institute
 Which Test When? Avoid the Stress of Stress Testing Marc Newell, MD, FACC, FSCCT Minneapolis Heart Institute Outline Understand the importance of coronary artery disease assessment Understand the basics
Which Test When? Avoid the Stress of Stress Testing Marc Newell, MD, FACC, FSCCT Minneapolis Heart Institute Outline Understand the importance of coronary artery disease assessment Understand the basics
Conflict Disclosures. Vermont Cardiac Network. Outline. Series Learning Objectives 4/27/2016. Scott E. Friedman April 28, 2016
 Conflict Disclosures Vermont Cardiac Network The Speaker has reported no significant financial relationship with any companies whose product may be germane to the content of their presentations or who
Conflict Disclosures Vermont Cardiac Network The Speaker has reported no significant financial relationship with any companies whose product may be germane to the content of their presentations or who
2018 ESC Guidelines for the diagnosis and management of syncope
 2018 ESC Guidelines for the diagnosis and management of syncope Michele Brignole (Chairperson) (Italy); Angel Moya (Co-chairperson) (Spain); Jean-Claude Deharo (France); Frederik de Lange (The Netherlands);
2018 ESC Guidelines for the diagnosis and management of syncope Michele Brignole (Chairperson) (Italy); Angel Moya (Co-chairperson) (Spain); Jean-Claude Deharo (France); Frederik de Lange (The Netherlands);
CONFUSION IN CARDIAC TESTING. Bilal Aijaz M.D FACC FSCAI
 CONFUSION IN CARDIAC TESTING Bilal Aijaz M.D FACC FSCAI WHY DOES CARDIOLOGY HAVE SO MANY TESTS? to create confusion (of course) to generate more business (maybe?) to accommodate the ever expanding patient
CONFUSION IN CARDIAC TESTING Bilal Aijaz M.D FACC FSCAI WHY DOES CARDIOLOGY HAVE SO MANY TESTS? to create confusion (of course) to generate more business (maybe?) to accommodate the ever expanding patient
There are 3 principle types of stress tests which do not involve the measurement of radiolabelled distribution within the body.
 National Imaging Associates, Inc. Clinical guidelines MYOCARDIAL PERFUSION IMAGING HEART (CARDIAC) PET SCAN STRESS ECHOCARDIOGRAM (Non-emergent outpatient testing) CPT4 Codes: Refer to pages 11-12 LCD
National Imaging Associates, Inc. Clinical guidelines MYOCARDIAL PERFUSION IMAGING HEART (CARDIAC) PET SCAN STRESS ECHOCARDIOGRAM (Non-emergent outpatient testing) CPT4 Codes: Refer to pages 11-12 LCD
CHEST PAIN CDU INCLUSION CRITERIA
 CHEST PAIN CDU INCLUSION CRITERIA No clinical criteria for ACS Stable vital signs Initial ECG and cardiac biomarkers not consistent with ACS Low to intermediate ACS risk (HEART score 0-6) [Ref 1, 2] Plan
CHEST PAIN CDU INCLUSION CRITERIA No clinical criteria for ACS Stable vital signs Initial ECG and cardiac biomarkers not consistent with ACS Low to intermediate ACS risk (HEART score 0-6) [Ref 1, 2] Plan
When Should I Order a Stress Test or an Echocardiogram
 When Should I Order a Stress Test or an Echocardiogram Updates in Cardiology 2015 March 7, 2015 Donald L. Lappé, MD, FAHA, FACC Chairman, Cardiovascular Department Medical Director, Intermountain Cardiovascular
When Should I Order a Stress Test or an Echocardiogram Updates in Cardiology 2015 March 7, 2015 Donald L. Lappé, MD, FAHA, FACC Chairman, Cardiovascular Department Medical Director, Intermountain Cardiovascular
Chapter 21: Clinical Exercise Testing Procedures
 Publisher link: thepoint http://thepoint.lww.com/book/show/2930 Chapter 21: Clinical Exercise Testing Procedures American College of Sports Medicine. (2010). ACSM's resource manual for guidelines for exercise
Publisher link: thepoint http://thepoint.lww.com/book/show/2930 Chapter 21: Clinical Exercise Testing Procedures American College of Sports Medicine. (2010). ACSM's resource manual for guidelines for exercise
Ve V rmont rmon Card Car iac d Netw Ne ork tw Scott E. Friedman April 28, 2016
 Vermont Cardiac Network Scott E. Friedman April 28, 2016 Conflict Disclosures Th S k h d i ifi fi i l l i hi ih The Speaker has reported no significant financial relationship with any companies whose product
Vermont Cardiac Network Scott E. Friedman April 28, 2016 Conflict Disclosures Th S k h d i ifi fi i l l i hi ih The Speaker has reported no significant financial relationship with any companies whose product
Invasive Risk Stratification: When is it needed?
 Inherited Cardiomyopathies and Channelopathies: Who is at risk for Sudden Cardiac Death? Invasive Risk Stratification: When is it needed? Hung-Fat Tse, MD, PhD Department of Medicine The University of
Inherited Cardiomyopathies and Channelopathies: Who is at risk for Sudden Cardiac Death? Invasive Risk Stratification: When is it needed? Hung-Fat Tse, MD, PhD Department of Medicine The University of
Syncope: The Pediatric Patient
 Syncope: The Pediatric Patient Lindsey Malloy-Walton, DO, MPH, FAAP Division of Pediatric Cardiology Children s Mercy Hospital 2401 Gillham Road Kansas City, MO 64108 Phone (office): 816-234-3255 Email:
Syncope: The Pediatric Patient Lindsey Malloy-Walton, DO, MPH, FAAP Division of Pediatric Cardiology Children s Mercy Hospital 2401 Gillham Road Kansas City, MO 64108 Phone (office): 816-234-3255 Email:
Evaluation and Management of the Patient with Cardiac Disease for Non-Cardiac Surgery WINTER CONFRENCE 2016 RONY GORGES, MD
 Evaluation and Management of the Patient with Cardiac Disease for Non-Cardiac Surgery WINTER CONFRENCE 2016 RONY GORGES, MD 67 yo man Asymptomatic carotid stenosis, CEA planned Golfs regularly, walks and
Evaluation and Management of the Patient with Cardiac Disease for Non-Cardiac Surgery WINTER CONFRENCE 2016 RONY GORGES, MD 67 yo man Asymptomatic carotid stenosis, CEA planned Golfs regularly, walks and
Current and Future Imaging Trends in Risk Stratification for CAD
 Current and Future Imaging Trends in Risk Stratification for CAD Brian P. Griffin, MD FACC Department of Cardiovascular Medicine, Heart and Vascular Institute, Cleveland Clinic Disclosures: None Introduction
Current and Future Imaging Trends in Risk Stratification for CAD Brian P. Griffin, MD FACC Department of Cardiovascular Medicine, Heart and Vascular Institute, Cleveland Clinic Disclosures: None Introduction
C1: Medical Standards for Safety Critical Workers with Cardiovascular Disorders
 C1: Medical Standards for Safety Critical Workers with Cardiovascular Disorders GENERAL ISSUES REGARDING MEDICAL FITNESS-FOR-DUTY 1. These medical standards apply to Union Pacific Railroad (UPRR) employees
C1: Medical Standards for Safety Critical Workers with Cardiovascular Disorders GENERAL ISSUES REGARDING MEDICAL FITNESS-FOR-DUTY 1. These medical standards apply to Union Pacific Railroad (UPRR) employees
Stress echo workshop STRESSORS
 Stress echo workshop STRESSORS Adham Ahmed, MD Lecturer of Cardiology, Ain Shams Indications of Stress Echo CAD Diagnosis Prognosticat ion 1 Physiologic Basis 1930s: Tennant and Wiggers Relationship between
Stress echo workshop STRESSORS Adham Ahmed, MD Lecturer of Cardiology, Ain Shams Indications of Stress Echo CAD Diagnosis Prognosticat ion 1 Physiologic Basis 1930s: Tennant and Wiggers Relationship between
Diagnostic and therapeutic management of the patient with syncope M. Brignole Arrhythmologic Centre and Syncope Unit Lavagna, Italy
 Diagnostic and therapeutic management of the patient with syncope M. Brignole Arrhythmologic Centre and Syncope Unit Lavagna, Italy Eur Heart J. 2009 Nov;30(21):2631-71 Available on www.escardio.org/guidelines
Diagnostic and therapeutic management of the patient with syncope M. Brignole Arrhythmologic Centre and Syncope Unit Lavagna, Italy Eur Heart J. 2009 Nov;30(21):2631-71 Available on www.escardio.org/guidelines
CURRENT STATUS OF STRESS TESTING JOHN HAMATY D.O.
 CURRENT STATUS OF STRESS TESTING JOHN HAMATY D.O. INTRODUCTION Form of imprisonment in 1818 Edward Smith s observations TECHNIQUE Heart rate Blood pressure ECG parameters Physical appearance INDICATIONS
CURRENT STATUS OF STRESS TESTING JOHN HAMATY D.O. INTRODUCTION Form of imprisonment in 1818 Edward Smith s observations TECHNIQUE Heart rate Blood pressure ECG parameters Physical appearance INDICATIONS
David A. Orsinelli, MD, FACC, FASE Professor, Internal Medicine The Ohio State University Division of Cardiovascular Medicine Columbus, Ohio
 1 STABLE ISCHEMIC HEART DISEASE: A NON-INVASIVE CARDIOLOGIST S PERSECTIVE 2018 Cardiovascular Course for Trainees and Early Career Physicians APRIL 20, 2018 David A. Orsinelli, MD, FACC, FASE Professor,
1 STABLE ISCHEMIC HEART DISEASE: A NON-INVASIVE CARDIOLOGIST S PERSECTIVE 2018 Cardiovascular Course for Trainees and Early Career Physicians APRIL 20, 2018 David A. Orsinelli, MD, FACC, FASE Professor,
Slide 1. Slide 2. Slide 3. Sudden Cardiac Death In Athletes. Epidemiology. Epidemiology. Shaun McMurtry, MD Primary Care Sports Medicine
 Slide 1 Sudden Cardiac Death In Athletes Shaun McMurtry, MD Primary Care Sports Medicine Slide 2 Epidemiology College and Professional Athletes 500,000 participants each year Competitive Athletics Estimated
Slide 1 Sudden Cardiac Death In Athletes Shaun McMurtry, MD Primary Care Sports Medicine Slide 2 Epidemiology College and Professional Athletes 500,000 participants each year Competitive Athletics Estimated
Sudden Cardiac Death in Sports: Causes and Current Screening Recommendations
 Sports Cardiology Sudden Cardiac Death in Sports: Causes and Current Screening Recommendations Domenico Corrado, MD, PhD Inherited Arrhytmogenic Cardiomyopathy Unit Department of Cardiac, Thoracic and
Sports Cardiology Sudden Cardiac Death in Sports: Causes and Current Screening Recommendations Domenico Corrado, MD, PhD Inherited Arrhytmogenic Cardiomyopathy Unit Department of Cardiac, Thoracic and
Sudden Cardiac Death What an electrophysiologist thinks a cardiologist should know
 Sudden Cardiac Death What an electrophysiologist thinks a cardiologist should know Steven J. Kalbfleisch, M.D. Medical Director Electrophysiology Laboratory Ross Heart Hospital Wexner Medical Center Sudden
Sudden Cardiac Death What an electrophysiologist thinks a cardiologist should know Steven J. Kalbfleisch, M.D. Medical Director Electrophysiology Laboratory Ross Heart Hospital Wexner Medical Center Sudden
Cardiac Viability Testing A Clinical Perspective Annual Cardiac Imaging Symposium. Lisa M Mielniczuk MD FRCPC University of Ottawa Heart Institute
 Cardiac Viability Testing A Clinical Perspective Annual Cardiac Imaging Symposium Lisa M Mielniczuk MD FRCPC University of Ottawa Heart Institute 62 year old male Anterior STEMI late presentation, occluded
Cardiac Viability Testing A Clinical Perspective Annual Cardiac Imaging Symposium Lisa M Mielniczuk MD FRCPC University of Ottawa Heart Institute 62 year old male Anterior STEMI late presentation, occluded
Syncope. Charles DeBerardinis, DO Iredell Health Systems
 Syncope Charles DeBerardinis, DO Iredell Health Systems Syncope Syncope loss of consciousness Vertigo sensation of motion Drop attacks fall without loss of consciousness seizure Syncope Constatino n=670
Syncope Charles DeBerardinis, DO Iredell Health Systems Syncope Syncope loss of consciousness Vertigo sensation of motion Drop attacks fall without loss of consciousness seizure Syncope Constatino n=670
Syncope evaluation: the role of syncope clinics Michele Brignole Arrhythmologic Centre, Lavagna, Italy
 Syncope evaluation: the role of syncope clinics Michele Brignole Arrhythmologic Centre, Lavagna, Italy Why should we need a Syncope Management Unit? We are not happy with current strategies: - not standardized
Syncope evaluation: the role of syncope clinics Michele Brignole Arrhythmologic Centre, Lavagna, Italy Why should we need a Syncope Management Unit? We are not happy with current strategies: - not standardized
Indications of Coronary Angiography Dr. Shaheer K. George, M.D Faculty of Medicine, Mansoura University 2014
 Indications of Coronary Angiography Dr. Shaheer K. George, M.D Faculty of Medicine, Mansoura University 2014 Indications for cardiac catheterization Before a decision to perform an invasive procedure such
Indications of Coronary Angiography Dr. Shaheer K. George, M.D Faculty of Medicine, Mansoura University 2014 Indications for cardiac catheterization Before a decision to perform an invasive procedure such
Review of Cardiac Imaging Modalities in the Renal Patient. George Youssef
 Review of Cardiac Imaging Modalities in the Renal Patient George Youssef ECHO Left ventricular hypertrophy (LVH) assessment Diastolic dysfunction Stress ECHO Cardiac CT angiography Echocardiography - positives
Review of Cardiac Imaging Modalities in the Renal Patient George Youssef ECHO Left ventricular hypertrophy (LVH) assessment Diastolic dysfunction Stress ECHO Cardiac CT angiography Echocardiography - positives
Approach to Syncope in the ED
 Approach to Syncope in the ED Vukiet Tran, CCFP(EM), FCFP, MHSc, MBA Staff, Emergency Physician University Health Network Case 1 v 75 yo female presents with syncope Multiple previous episodes PMH: CAD,
Approach to Syncope in the ED Vukiet Tran, CCFP(EM), FCFP, MHSc, MBA Staff, Emergency Physician University Health Network Case 1 v 75 yo female presents with syncope Multiple previous episodes PMH: CAD,
Stress Echo Cases Sunday, October 8, :10 3:30 PM 20 min
 2017 ASE Echo Florida, Orlando, FL Stress Echo Cases Sunday, October 8, 2016 3:10 3:30 PM 20 min 1 M U H A M E D S A R I Ć, M D, P H D D i r e c t o r o f E c h o c a r d i o g r a p h y L a b A s s o
2017 ASE Echo Florida, Orlando, FL Stress Echo Cases Sunday, October 8, 2016 3:10 3:30 PM 20 min 1 M U H A M E D S A R I Ć, M D, P H D D i r e c t o r o f E c h o c a r d i o g r a p h y L a b A s s o
The new Guidelines: Focus on Chronic Heart Failure
 The new Guidelines: Focus on Chronic Heart Failure Petros Nihoyannopoulos MD, FRCP, FESC Professor of Cardiology Imperial College London and National & Kapodistrian University of Athens 2 3 4 The principal
The new Guidelines: Focus on Chronic Heart Failure Petros Nihoyannopoulos MD, FRCP, FESC Professor of Cardiology Imperial College London and National & Kapodistrian University of Athens 2 3 4 The principal
Tachycardia Devices Indications and Basic Trouble Shooting
 Tachycardia Devices Indications and Basic Trouble Shooting Peter A. Brady, MD., FRCP Cardiology Review Course London, March 6 th, 2014 2011 MFMER 3134946-1 Tachycardia Devices ICD Indications Primary and
Tachycardia Devices Indications and Basic Trouble Shooting Peter A. Brady, MD., FRCP Cardiology Review Course London, March 6 th, 2014 2011 MFMER 3134946-1 Tachycardia Devices ICD Indications Primary and
Management of Arrhythmias The General Practitioners role
 Management of Arrhythmias The General Practitioners role Rohan Gunawardena MD, FRCP, FCCP, FACC Consultant Cardiac Electrophysiologist National Hospital of Sri Lanka Arrhythmias not common Palpitations
Management of Arrhythmias The General Practitioners role Rohan Gunawardena MD, FRCP, FCCP, FACC Consultant Cardiac Electrophysiologist National Hospital of Sri Lanka Arrhythmias not common Palpitations
Presentation of transient loss of consciousness
 Presentation of transient loss of consciousness Definition of transient loss of consciousness Transient loss of consciousness: sudden onset, complete loss of consciousness of brief duration with relatively
Presentation of transient loss of consciousness Definition of transient loss of consciousness Transient loss of consciousness: sudden onset, complete loss of consciousness of brief duration with relatively
Tilt Table Testing MM /01/2015. HMO; PPO; QUEST Integration 09/22/2017 Section: Medicine Place(s) of Service: Office, Outpatient
 of Service: Office, Outpatient") Tilt Table Testing Policy Number: Original Effective Date: MM.02.024 01/01/2015 Line(s) of Business: Current Effective Date: HMO; PPO; QUEST Integration 09/22/2017 Section: Medicine Place(s) of Service:
Tilt Table Testing Policy Number: Original Effective Date: MM.02.024 01/01/2015 Line(s) of Business: Current Effective Date: HMO; PPO; QUEST Integration 09/22/2017 Section: Medicine Place(s) of Service:
La valutazione dell atleta: è una strategia salva-vita e costo-efficace?
 La valutazione dell atleta: è una strategia salva-vita e costo-efficace? Primo trattato di Medicina Wilson and Jungner s criteria In the 1960s the World Health Organization adopted the Wilson and Jungner
La valutazione dell atleta: è una strategia salva-vita e costo-efficace? Primo trattato di Medicina Wilson and Jungner s criteria In the 1960s the World Health Organization adopted the Wilson and Jungner
Tachycardias II. Štěpán Havránek
 Tachycardias II Štěpán Havránek Summary 1) Supraventricular (supraventricular rhythms) Atrial fibrillation and flutter Atrial ectopic tachycardia / extrabeats AV nodal reentrant a AV reentrant tachycardia
Tachycardias II Štěpán Havránek Summary 1) Supraventricular (supraventricular rhythms) Atrial fibrillation and flutter Atrial ectopic tachycardia / extrabeats AV nodal reentrant a AV reentrant tachycardia
Contra-indications, Risks, and Safety Precautions for Stress Testing. ACSM guidelines, pg 20 7 ACSM RISK FACTORS. Risk Classifications pg 27
 Contra-indications, Risks, and Safety Precautions for Stress Testing Data to Support Stress Testing How safe is stress testing? Contra-indications Termination Criteria Ellstad Chapt 5 ACSM Chapts 3-6 Seattle
Contra-indications, Risks, and Safety Precautions for Stress Testing Data to Support Stress Testing How safe is stress testing? Contra-indications Termination Criteria Ellstad Chapt 5 ACSM Chapts 3-6 Seattle
Dysrhythmias 11/7/2017. Disclosures. 3 reasons to evaluate and treat dysrhythmias. None. Eliminate symptoms and improve hemodynamics
 Dysrhythmias CYDNEY STEWART MD, FACC NOVEMBER 3, 2017 Disclosures None 3 reasons to evaluate and treat dysrhythmias Eliminate symptoms and improve hemodynamics Prevent imminent death/hemodynamic compromise
Dysrhythmias CYDNEY STEWART MD, FACC NOVEMBER 3, 2017 Disclosures None 3 reasons to evaluate and treat dysrhythmias Eliminate symptoms and improve hemodynamics Prevent imminent death/hemodynamic compromise