Le sindromi cardio renali G. VESCOVO
|
|
|
- Augustine Barton
- 5 years ago
- Views:
Transcription

1 Le sindromi cardio renali G. VESCOVO



2 G. VESCOVO MD, PhD, FESC Dip. Medicina Interna VICENZA Le sindromi cardio renali


3 Consensus Conference

4 Prevalence of CVD Any CVD: 80 million (1 in 3) Htn: 73 million CAD: 16 million AMI: 8.1 million CHF: 5.3 million Stroke: 5.8 million Congenital: million Prevalence of CVD and CKD AHA/ACC Circulation 2008 N Engl J Med 2010
5 Prevalence of CVD and CKD CKD in CVD 28.2%! AHA/ACC Circulation 2008
6 CKD and CVD 60 Patients With CKD (%) % 33% 46% 0 CAD FG 60 ml/min AMI FG <60 ml/min CHF FG 60 ml/min Coresh, et al., 2007
7 Hearth and Kidney: a liaison dangereuse Regulation of volume and BP (Na + and H 2 O) Electrolyte and acid-base balance Hormonal function (Erythropoiesis Vascular tone Ca/P) Blood Purification from metabolic waste products Regulation of perfusion pressure and flows to periphery Electrical activity dependent on electrolytes and acid-base Contractility depending on O 2, volume, electrolytes, toxin Hormonal function (ANP - BNP)
8 The Cardiorenal Syndrome There is no commonly accepted definition Term borrowed from other areas (e.g. Hepatorenal Syndrome, the same kidney in another individual would perform normally). Fix the heart, and get the kidney back to normal! General term used to define heart kidney pathological interactions It is a pathophysiological entity that describes the initiation and progression of renal insufficiency (RI) secondary to heart failure(hf); however it also includes the negative effects of reduced renal function on heart function. It should include the damage/dysfunction induced to one of the two organs by an acute or chronic dysfunction of the other organ. Cardiorenal or renocardiac syndrome? Acute or chronic?
9 Chronic Acute C R R C The need for a consensus classification and definition that describes all the clinical conditions together with the bidirectional nature of the organ cross talk emerges clearly. Bidirectionality and time window Cardiorenal syndromes: to indicate the presence of multiple syndromes Subtypes: to recognize primary organ dysfunction (cardiac vs. renal) and the time frame of the insult (acute vs. chronic)
10 What is cardiorenal syndrome? What is it cardiorenal syndrome? How can we define it? What are the types? How do they impact the clinical outcomes? Why is early diagnosis important? What is the role of new biomarkers?

11 Definitions of the 5 subtypes of cardio-renal syndrome





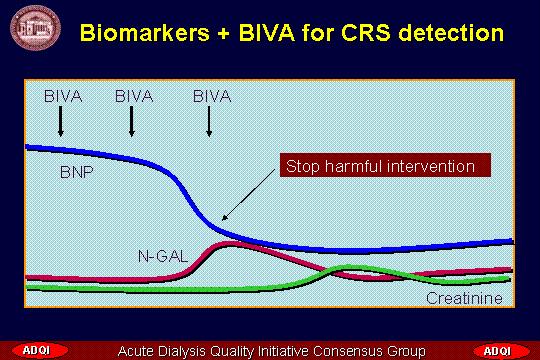
12 ACUTE CARDIO RENAL SYNDROME: TYPE % of patiets hospitalized for acute de-compensated HF develop acute kidney injury Hemodynamically mediated damage Drop in CO Arterial underfilling Incr. venous pressure Acute Heart Disease or Procedures Acute decompensation Ischemic insult Coronary angiography Cardiac Surgery Caspase activation Apoptosis Humoral Signalling BNP Exogenous Factors Contrast media ACE inhibitors Diuretics Sympathetic Activation Humorally mediated damage RAA activation, Na + H2O retention, vasoconstriction Imbalance between ET and EDNO Hormonal Factors Immuno mediated damage Monocyte Activation Endothelial activation Toxicity Vascocostr. ltx, ET, Tx Cytokine secretion Caspase activation Apoptosis Renal hypotperfusion Red. Oxigen delivery Necrosis / apoptosis Drop in GFR Resistance to ANP/BNP BIOMARKERS Creatinine Cystatin C N GAL KIM 1 Acute Kidney Injury
13 CHRONIC CARDIO RENAL SYNDROME: TYPE 2 60% of patients hospitalized with congestive HF have chronic kidney disease Anemia Sodium and H2O retention Uremic solute retention Ca and P abnormalities Hypertension Increased susceptibility to insults Genetic risk factors Acquired Risk factors Low cardiac output (CO) Chronic hypoperfusion Necrosis apoptosis Chronic Heart Disease Low cardiac output (CO) Subclinical inflammation Endothelial dysfunction Accelerate atherosclerosis Insult and Initiation of kidney damage Anemia, hypoxia RAA and sympathetic act. Na and H2O retention Ca and P abnormalities Hypertension, LVH Anemia Sodium and H2O retention Uremic solute retention Ca and P abnormalities Hypertension Chronic hypoperfusion Increased renal vasc. resist. Increased venous pressure Embolism Sclerosis Fibrosis Progression of CKD

14 ACUTE RENO CARDIAC SYNDROME: TYPE 3 Drop in GFR Na + H 2 O retention Volume expansion Increased pre load Hypertension Acute Kidney Injury Sympathetic Activation RAA activation,, vasoconstriction Acute Heart Dysfunction Glomerular diseases Interstitial diseases Acute tubular necrosis Acute pyelonephritis Acute urinary obstruction Humoral Signalling Electrolyte, acid base & coagulation imbalances Cytokine secretion Acute decompensation Acute heart failure Hischemic insult Arrythmias Drop in CO Caspase activation Apoptosis Monocyte Activation Endothelial activation Caspase activation Apoptosis BIOMARKERS Troponin Myoglobin MPO BNP





15 CKD Stage 1 2 Glomerular/interstitial damage CKD Stage 3 4 CHRONIC RENO CARDIAC SYNDROME: TYPE 4 Genetic risk factors Acquired Risk factors Primary nephropathy Diabetes mellitus Anemia Uremic toxins Ca/P abnormalities Nutritional status, BMI Salt and water overload Chronic Inflammation Smoke Obesity Hypertension Dyslipidemia Homocystein levels Chronic inflammation Cardiac remodelling Neurohormonal abnormalities Increased hischemic risk Left ventricular hypertrophy Left diastolic dysfunction Decreased coronary perfusion Stunning Myocardium Hemodynamic worsening Inflammation Coronary and tissue calcification Sclerosis Fibrosis CKD Stage 5 Dialysis Endothelial dysfunction Smooth muscle proliferation LDL oxidation Vascular calcification Oxidant stress Accelerated atherosclerosis Bone remodeling Artificial surfaces Contaminated fluids Muscle catabolism Anemia & malnutrition Ca/P abnormalities Soft tissue calcification Na H2O overload EPO resistance Uremic toxins Unfriendly milieu Appetite monocyte stimulation Acute phase reactants Chronic Inflammation Cytokine production Adipocytokine production Insulin resistance BIOMARKERS Cardiac troponin Natriuretic peptides Asymmetric dimethylarginine Ischemia modified albumin Acute phase proteins Serum amyloid protein A C reactive protein
16 SECONDARY CARDIO RENAL SYNDROME: TYPE 5 Heart failure Sympathetic system activation Neurohumoral stress Inflammation Systemic diseases Diabetes Amyloidosis Vasculitis SEPSIS Hemodynamic changes Hypoperfusion perfusion pressure, RVR Hischemia/ reperfusion hypoxia ox stress toxemia Exogenous toxins heme proteins antibiotics, contrast media, vasopressors Organ damage/dysfunction LPS / endotoxin Monocyte activation cytokines Renal Insufficiency
17 The Cardiorenal Syndrome Assessment and Diagnosis A new definition of cardiorenal syndrome with a comprehensive classification into five different subtypes is available We need to use the new definition/classification to have a standard terminology in clinical settings and new clinical trials. We need to evaluate the impact of early biomarkers on diagnosis and various therapeutic approaches. We need to focus on biomarker profiles to identify patients at risk for any negative cardiorenal interaction. We need to appraise current evidence and generate wise recommendations for practice and when evidence is missing, we need to create a research agenda to fill the gaps and generate the missing evidence





18 A biomarker is a biological compound, objectively measurable, evaluated as an indicator of normal/pathological biological processes, or pharmacologic response to therapeutic intervention. Urine Plasma

19



20 Biomarkers IL 18 Cystatin C NGAL Neutrophil gelatinase associated lipocalin Plasma Urine Using cdna microarray as a screening technique, a subset of genes whose expression is up regulated within the first few hours after renal injury can be discovered. (Or early GFR)

21
22 Pharmacologic therapy in patients with CRS: a complex issue Coexistence of kidney with heart disease has major implications: renal function alters the pharmacochinetics and pharmacodinamics of several cardio-active medications requiring drug dosage adjusments certain CV drugs can interfere with renal function and must admistered with caution to patients with underlying kidney disease patients with kidney disease have been underrepresented in CVD clinical trials


![to ESC guidelines [1] No](/docs-images/94/120043357/images/23-2.jpg "consensus on timing for")









23 ACE inhibitors and ARBS Indication Acute CRS Chronic CRS Intended action and effects No compelling indication according to ESC guidelines [1] No consensus on timing for initiation. Treatment should be continued whenever possible in those already treated Treatment to be initiated before hospital discharge Life savings, reduce morbidity Prevent cardiac remodelling ARBS as an alternative only in patients intolerant to ACEIs Side effects and problems Deterioration of kidney function if already on board Hypotension Monitor kidney function and electrolytes Hypotension Acute RCS - Contraindicated in renal artery stenosis Chronic RCS Nephroprotection RAAS antagonism Decrease proteinuria Mild transient deterioration of kidney function Careful monitoring in dialysis patients (hypotension)









24 Beta-blockers Indication Intended action and effects Acute CRS Chronic CRS Chronic RCS Dose may need to be reduced temporarily, in general should not be withdrawn unless signs of low output Life savings Reduce morbidity Prevent remodelling Cardioprotection and prevention of tachyarrhythmias Side effects and problems Hypotension, bradyarrhythmias Hypotension, bradyarrhythmias Deterioration in heart failure symptoms (transient) Asthma As above


















25 Diuretics Indication Intended action and effects Acute CRS Chronic CRS Acute RCS Chronic RCS Secondary CRS Natriuresis, reduction of fluid overload, Na and H2O elimination Frusemide preferred control of diuresis and extracellular fluid volume Symptoms relief Maintenance of non oliguric AKI Frusemide preferred Maintenance of diuresis in CKD 4 and 5. Control of hypertension and fluid balance Maintenance of diuresis and fluid balance Side effects and problems Potential hypovolemia and worsening of renal failure Volume depletion Hypotension Worsening renal failure, hyperuricemia, K imbalance. Diuretic resistance No evidence for renal protection nor reduction of need for RRT Potential toxic effects Direct and cumulative toxicity with other drugs (antibiotics- anti inflammatory)









26 Digoxin Indication Intended action and effects Side effects and problems Chronic CRS and Chronic RCS Reduce HF Hospitalisation Improve symptoms Mortality unchanged Toxicity if reduced GFR Adjust dosage Acute CRS If high heart rate AF is present As above
27
28 CONCLUSIONS Cardiologists and nephrologists and internists need to talk each other The way they should do that is by a systematic and common approach The classification of cardiorenal syndromes is an attempt to bring this view into the clinical setting G. VESCOVO Medicina Interna VICENZA
29

30 G. VESCOVO Medicina Interna VICENZA


31 G. VESCOVO Medicina Interna VICENZA
32
 Between 30% and 50% of patients with congestive heart failure present a impaired renal function. (Obialo Am J Cardiol 2007).")
.")
33 Cardiologist point of view 18% of pts admitted to 115 hospitals in the EuroHeart Failure Survey Program, had renal dysfunction. (Cleland JGF,Eur Heart J 2003;24: ) Between 30% and 50% of patients with congestive heart failure present a impaired renal function. (Obialo Am J Cardiol 2007). 30% of hospitalized pts for heart failure had a history of chronic renal insufficiency and 20% a serum creatinine level > 2 mh/dl in an evaluation of hospitalizations episodes o at 274 hospitals from the Acute Decompensated Heart Failure National registry (ADHERE). (Adams KF,Am Heart J 2005;149: ) The prevalence of patients who develop during hospitalization for decompensated heart failure a worsening renal function is about 25%,according to a systematic review and meta analysis.
34 Nephrologist point of view In the general population, about one person in 20 has a serum creatinine level above normal, signifying mild kidney disease (Zoccali Nephrol Dial Transplant 2002) Mortality in end stage renal disease and chronic kidney disease patients is due for about 50% to cardiovascular comorbidity (Zoccali Nephrol Dial Transplant 2002). In the year age group cardiovascular mortality rate in dialysis patients is about 65 times higher than in the general population. In younger cohorts cardiovascular mortality rate is 500 times higher than in the general population. (Levey Am J Kidey disease 1998)
35 Heart Kidney Pathologic Interactions CKD secondary to HF AKI secondary to contrast induced nephropathy (CIN) AKI secondary to cardiopulmonary bypass (CPB) AKI secondary to heart valve replacement AKI secondary to HF Cardiovascular mortality increased by end stage renal dysfunction (ESRD) Cardiovascular risk increased by kidney dysfunction Chronic HF progression due to kidney dysfunction Uremia related HF Volume related HF HF due to acute kidney dysfunction Volume/uremia induced HF Renal ischemia induced HF Sepsis/cytokine induced HF










36 The syndrome of Heart Failure Dyspnoea Fatigue Left Ventricular Dysfunction CHF Congestion Lungs Limbs Guts Arrhythmias

37 ACUTE CHRONIC
38 Renal dysfunction is common in patients with acute decompensated HF 50 80% of patients have at least stage CKD 3 Patients (%) < >90 Estimated GFR, ml/min Heywood et al. Heart Failure Reviews 2004;9:











39 ADQI RIFLE Criteria for Acute Renal Dysfunction ADQI GFR Criteria* Urine Output Criteria Risk Increased creatinine x1.5 or GFR decrease > 50% UO <.5ml/kg/h x 6 hr High Sensitivity Injury Increased creatinine x 2 or GFR decrease > 50% UO <.5ml/kg/h x 12 hr Failure Increase creatinine x 3 or GFR dec >75% or creatinine 4mg/dl (Acute rise of 0.5 mg/dl) UO <.3ml/kg/h x 24 hr or Anuria x 12 hrs High Specificity Loss ESRD Persistent ARF** = complete loss of renal function > 4 weeks End Stage Renal Disease
) Increase creatinine x3 or creatinine 4mg/dl (Acute rise of 0.5 mg/dl) RRT Started UO <.")
40 Modifications proposed by AKIN R (I) Increased creatinine x1.5 OR > 0.3mg/dl UO <.5ml/kg/h x 6 hr High Sensitivity I (II) Increased creatinine x2 UO <.5ml/kg/h x 12 hr F (III)) Increase creatinine x3 or creatinine 4mg/dl (Acute rise of 0.5 mg/dl) RRT Started UO <.3ml/kg/h x 24 hr or Anuria x 12 hrs High Specificity
41 RIFLE max Cumulative Survival 1,0,8,6,4 Non ARD Risk Injury Failure,2 0,0 0 P<0.001 (Log Rank) Days after hospital Length admission of hospital stay (d) Hoste et al. Crit Care. 2006;10(3):R73




42 Acute Interactions % Mortality Kidney K + 1 K + 2 K + 3 Number of failing organs
43 Prevalence/Incidence Estimates 2007 Any CVD: 80 million (1 in 3) Htn: 73 million CAD: 16 million AMI: 8.1 million CHF: 5.3 million Stroke: 5.8 million Congenital: million 2007 Any CKD ( Stage I) 16.8% CKD Stage I ~ 5.7% CKD Stage II ~ 5.4% CKD III ~ 5.4% Stage IV-V ~ 0.4% ESKD 2x increase in 10 years (261/million to 348/million) Projected to increase 16% Pts with Heart Failure :recurrent and frequent hospitalization for symptoms and treatment; over 1 million of hospitalizations annually which generate 6.5 million inpatient hospital days per yr Approximately 20% to 40% of patients admitted to a hospital for acute heart failure have comorbid renal insufficency, based on clinical history and serum creatinine levels(1.681 pts admitted at 18 hospitals in Connecticut:21% had baseline renal failure and 41% had a baseline serum creatinine level 1.5 mg/dl ) AHA/ACC Circulation 2008










44 Inotropic Agents Dopamine Dobutamine Levoximendan Milrinone Enoximone Acute CRS To increase cardiac output in low output if proven or to maintain blood pressure Some inotropic agents may decrease peripheral resistances Arrhythmias; Receptor desensitization with prolonged use; Some may adversely affect outcome Vasopressors Epinephrine Norepinephrine Acute CRS Norepinephrine indicated only in cardiogenic shock when other inotropic therapies fail Epinephrine indicated only as rescue therapy for cardiac arrest, not as an inotrope




45 Vasodilators Nitroprusside Nitrates Acute CRS Indicated if organ congestion is present Increase renal and peripheral blood flow Hypotension especially in hypovolemic patients; Cyanide intoxication for nitroprusside Nesiritide Vasopressin Antagonists Acute CRS BNP analogue Vasodilator Data on mortality Uncertain Hypotension Can worsen kidney function, but data uncertain Acute CRS symptoms relief, promote water elimination and weight loss in the short term No changes in mortality and morbidity at one year with tolvaptan




46 Endothelin Antagonists Adenosine A1- receptor antagonists Chronic CRS and Chronic RCS Acute and chronic CRS Aimed to block endothelin II mediated vasoconstriction Block adenosine glomerular vasoconstriction May improve symptoms and prevent deterioration in renal function No changes in mortality Currently licensed only for Pulmonary hypertension with RV failure to improve EC Weight loss?
47 Cardio-Renal Syndromes (CRS) General Definition: Disorders of the heart and kidneys whereby acute or chronic dysfunction in one organ may induce acute or chronic dysfunction of the other Acute Cardio-Renal Syndrome (Type 1) Acute worsening of cardiac function leading to renal dysfunction Chronic Cardio-Renal Syndrome (Type 2) Chronic abnormalities in cardiac function leading to renal dysfunction Acute Reno-Cardiac Syndrome (Type 3) Acute worsening of renal function causing cardiac dysfunction Chronic Reno-Cardiac Syndrome (Type 4) Chronic abnormalities in renal function leading to cardiac disease Secondary Cardio-Renal Syndromes (Type 5) Systemic conditions causing simultaneous dysfunction of the heart and kidney




48 Morphine Acute CRS Relief of dyspnoea, chest pain, helps NIV Respiratory depression

49
50 Syndromes Type 1 Acute Cardiorenal Type 2 Chronic Cardiorenal Type 3 Acute Renocardiac Type 4 Chronic Renocardiac Type 5 Secondary Organ failure sequence Systemic Disease Possible Definition Abrupt worsening of cardiac function leading to acute kidney injury Chronic abnormalities in cardiac function causing progressive and permanent chronic kidney disease Abrupt worsening of renal function causing acute cardiac disorders CKD contributing to decreased cardiac function, cardiac hypertrophy and/or increased risk of cardiovascular events Systemic condition (e.g. diabetes mellitus, sepsis) causing both cardiac and renal dysfunction Primary events Acute decompensated heart failure, ischemic insult, coronary angio, cardiac surgery LV remodeling and dysfunction Diastolic dysfunction Chronic abnormalities in cardiac function AKI (e.g. acute kidney ischaemia or glomerulonephritis) CKD(e.g. chronic glomerular disease) Sepsis Possible Criteria for primary events Severe arrythmia Troponin/ ST elevation ECHO: dilatation Decreased EF Increased CVP NYHF class 3-4 RIFLE R.I.F. or AKIN stage or AKI requiring RRT CKD stage 1-5 or CKD requiring RRT APACHE 2 > SOFA SCORE > N. of failing organs Sequelae Inadequate renal perfusion Reduced diuretic responsiveness Worsening renal function Nephroangiosclerosis, chronic intesrt. Nephr. ADHF, severe arrythmias, shock LVH, Dilatative myocardiopathy, CHF ADHF - AKI Possible Criteria for sequelae RIFLE R,I,F by creatinine or urine output. CKD stage 1-5 Pulmonary edema, electrolyte imbalance arrythmias, cardiac arrest, reduced myocardiac contractility ADHF, AHF, pericarditis CHF Decreased EF Increased CVP NYHF class 3-4 RIFLE R,I,F or RRT Cardiac markers Troponin, BNP, MPO BNP, CRP BNP, CRP CRP CRP, procalcitonin, Renal Markers Serum Cystatine, Creatinine, NGAL. Urinary KIM-1, IL-18, NGAL, NAG Creatinine, Cystatic C, Urea, Uric Acid, CRP Decreased GFR Serum Cystatine, Creatinine, NGAL. Urinary KIM-1, IL-18, NGAL, NAG Creatinine, Cystatic C, Urea, Uric Acid CRP Decreased GFR Creatinine, NGAL, IL-18, KIM-1, NAG

 Biomarkers (prevention protection) Biomarkers")
51 Conceptual Model for AKI Kidney Injury Continuum Vaidya VS, Ferguson MA, Bonventre JV. Biomarkers of Acute Kidney Injury. Annu Rev Pharmacol Toxicol 2008;48: Biomarkers (predictors) Biomarkers (prevention protection) Biomarkers (therapy)



52 Analyze Biology by Time Zones with Adequate and Precision Clocks Multiple Timezone Organ Damage Clock Display MOLECULAR CELLULAR BIOMARKER CLINICAL we can identify different milestones along the timeline of AKI. Injury begins inducing molecular modifications subsequently evolving into cellular damage. Cells start to produce biomarkers of injury and only later does the clinical picture of the syndrome develop with the typical sign and symptoms.
Pathophysiology of Cardio-Renal Interactions
 Pathophysiology of Cardio-Renal Interactions Claudio Ronco, MD Department of Nephrology St. Bortolo Hospital International Renal Research Institute Vicenza - Italy Pathophysiology of Cardio-Renal Interactions
Pathophysiology of Cardio-Renal Interactions Claudio Ronco, MD Department of Nephrology St. Bortolo Hospital International Renal Research Institute Vicenza - Italy Pathophysiology of Cardio-Renal Interactions
Cardiorenal Syndrome
 Cardiorenal Syndrome Peenida Skulratanasak, M.D. Division of Nephrology, Department of Medicine, Faculty of Medicine, Siriraj Hospital, Mahidol University Definition of Cardiorenal syndrome (CRS) Structural
Cardiorenal Syndrome Peenida Skulratanasak, M.D. Division of Nephrology, Department of Medicine, Faculty of Medicine, Siriraj Hospital, Mahidol University Definition of Cardiorenal syndrome (CRS) Structural
Pathophysiology of Cardio-Renal Interactions
 European Society of Cardiology 2011 Paris-France Pathophysiology of Cardio-Renal Interactions Claudio Ronco, MD Department of Nephrology St. Bortolo Hospital International Renal Research Institute Vicenza
European Society of Cardiology 2011 Paris-France Pathophysiology of Cardio-Renal Interactions Claudio Ronco, MD Department of Nephrology St. Bortolo Hospital International Renal Research Institute Vicenza
Heart Failure and Renal Failure. Gerasimos Filippatos, MD, FESC, FHFA President HFA
 Heart Failure and Renal Failure Gerasimos Filippatos, MD, FESC, FHFA President HFA Definition Epidemiology Pathophysiology Management (?) Recommendations for NHLBI in cardiorenal interactions related to
Heart Failure and Renal Failure Gerasimos Filippatos, MD, FESC, FHFA President HFA Definition Epidemiology Pathophysiology Management (?) Recommendations for NHLBI in cardiorenal interactions related to
Heart Failure and Cardio-Renal Syndrome 1: Pathophysiology. Biomarkers of Renal Injury and Dysfunction
 CRRT 2011 San Diego, CA 22-25 February 2011 Heart Failure and Cardio-Renal Syndrome 1: Pathophysiology Biomarkers of Renal Injury and Dysfunction Dinna Cruz, M.D., M.P.H. Department of Nephrology San Bortolo
CRRT 2011 San Diego, CA 22-25 February 2011 Heart Failure and Cardio-Renal Syndrome 1: Pathophysiology Biomarkers of Renal Injury and Dysfunction Dinna Cruz, M.D., M.P.H. Department of Nephrology San Bortolo
Pivotal Role of Renal Function in Acute Heart failure
 Pivotal Role of Renal Function in Acute Heart failure Doron Aronson MD, FESC Department of Cardiology RAMBAM Health Care Campus Haifa, Israel Classification and definitions of cardiorenal syndromes CRS
Pivotal Role of Renal Function in Acute Heart failure Doron Aronson MD, FESC Department of Cardiology RAMBAM Health Care Campus Haifa, Israel Classification and definitions of cardiorenal syndromes CRS
Medical Treatment for acute Decompensated Heart Failure. Vlasis Ninios Cardiologist St. Luke s s Hospital Thessaloniki 2011
 Medical Treatment for acute Decompensated Heart Failure Vlasis Ninios Cardiologist St. Luke s s Hospital Thessaloniki 2011 2010 HFSA guidelines for ADHF 2009 focused update of the 2005 American College
Medical Treatment for acute Decompensated Heart Failure Vlasis Ninios Cardiologist St. Luke s s Hospital Thessaloniki 2011 2010 HFSA guidelines for ADHF 2009 focused update of the 2005 American College
Novel Approaches for Recognition and Management of Life Threatening Complications of AKI and CKD: Focus on Acute Cardiorenal Syndromes
 Novel Approaches for Recognition and Management of Life Threatening Complications of AKI and CKD: Focus on Acute Cardiorenal Syndromes Peter A. McCullough, MD, MPH Baylor University Medical Center, Dallas
Novel Approaches for Recognition and Management of Life Threatening Complications of AKI and CKD: Focus on Acute Cardiorenal Syndromes Peter A. McCullough, MD, MPH Baylor University Medical Center, Dallas
Cardiorenal and Renocardiac Syndrome
 And Renocardiac Syndrome A Vicious Cycle Cardiorenal and Renocardiac Syndrome Type 1 (acute) Acute HF results in acute kidney injury Type 2 Chronic cardiac dysfunction (eg, chronic HF) causes progressive
And Renocardiac Syndrome A Vicious Cycle Cardiorenal and Renocardiac Syndrome Type 1 (acute) Acute HF results in acute kidney injury Type 2 Chronic cardiac dysfunction (eg, chronic HF) causes progressive
The Triple Threat. Cardiac Care in the NT Annual Workshop 2017 is proudly supported by:
 The Triple Threat DR KELUM PRIYADARSHANA FRACP CONSULTANT NEPHROLOGIST ROYAL DARWIN HOSPITAL Cardiac Care in the NT Annual Workshop 2017 is proudly supported by: Pathogenesis Diabetes CKD CVD Diabetic
The Triple Threat DR KELUM PRIYADARSHANA FRACP CONSULTANT NEPHROLOGIST ROYAL DARWIN HOSPITAL Cardiac Care in the NT Annual Workshop 2017 is proudly supported by: Pathogenesis Diabetes CKD CVD Diabetic
Cardiorenal Syndrome
 SOCIEDAD ARGENTINA DE CARDIOLOGIA Cardiorenal Syndrome Joint session ESC-SAC ESC Congress 2012, Munich César A. Belziti Hospital Italiano de Buenos Aires I have no conflicts of interest to declare Cardiorenal
SOCIEDAD ARGENTINA DE CARDIOLOGIA Cardiorenal Syndrome Joint session ESC-SAC ESC Congress 2012, Munich César A. Belziti Hospital Italiano de Buenos Aires I have no conflicts of interest to declare Cardiorenal
Heart Failure and Renal Disease Cardiorenal Syndrome
 Advanced Heart Failure: Clinical Challenges Heart Failure and Renal Disease Cardiorenal Syndrome 17 th Apr 2015 Ju-Hee Lee, M.D Cardiovascular Center, Chungbuk National University Hospital Chungbuk National
Advanced Heart Failure: Clinical Challenges Heart Failure and Renal Disease Cardiorenal Syndrome 17 th Apr 2015 Ju-Hee Lee, M.D Cardiovascular Center, Chungbuk National University Hospital Chungbuk National
Doppler ultrasound, see Ultrasonography. Magnetic resonance imaging (MRI), kidney oxygenation assessment 75
, kidney oxygenation assessment 75") Subject Index Acidemia, cardiorenal syndrome type 3 146 Acute Dialysis Quality Initiative (ADQI) acute kidney injury biomarkers, see Acute kidney injury; specific biomarkers cardiorenal syndrome, see specific
Subject Index Acidemia, cardiorenal syndrome type 3 146 Acute Dialysis Quality Initiative (ADQI) acute kidney injury biomarkers, see Acute kidney injury; specific biomarkers cardiorenal syndrome, see specific
THE KIDNEY IN HYPOTENSIVE STATES. Benita S. Padilla, M.D.
 THE KIDNEY IN HYPOTENSIVE STATES Benita S. Padilla, M.D. Objectives To discuss what happens when the kidney encounters low perfusion To discuss new developments and clinical application points in two scenarios
THE KIDNEY IN HYPOTENSIVE STATES Benita S. Padilla, M.D. Objectives To discuss what happens when the kidney encounters low perfusion To discuss new developments and clinical application points in two scenarios
The Cardiorenal Syndrome in Heart Failure
 The Cardiorenal Syndrome in Heart Failure Van N Selby, MD Assistant Professor of Medicine Advanced Heart Failure Program, UCSF October 9, 2015 Disclosures None 1 Cardiorenal Syndrome (CRS) A pathophysiologic
The Cardiorenal Syndrome in Heart Failure Van N Selby, MD Assistant Professor of Medicine Advanced Heart Failure Program, UCSF October 9, 2015 Disclosures None 1 Cardiorenal Syndrome (CRS) A pathophysiologic
Medical Management of Acute Heart Failure
 Critical Care Medicine and Trauma Medical Management of Acute Heart Failure Mary O. Gray, MD, FAHA Associate Professor of Medicine University of California, San Francisco Staff Cardiologist and Training
Critical Care Medicine and Trauma Medical Management of Acute Heart Failure Mary O. Gray, MD, FAHA Associate Professor of Medicine University of California, San Francisco Staff Cardiologist and Training
Fluid Resuscitation in Critically Ill Patients with Acute Kidney Injury (AKI)
") Fluid Resuscitation in Critically Ill Patients with Acute Kidney Injury (AKI) Robert W. Schrier, MD University of Colorado School of Medicine Denver, Colorado USA Prevalence of acute renal failure in Intensive
Fluid Resuscitation in Critically Ill Patients with Acute Kidney Injury (AKI) Robert W. Schrier, MD University of Colorado School of Medicine Denver, Colorado USA Prevalence of acute renal failure in Intensive
Editorial Staying in the Pink of Health for Patients with Cardiorenal Anemia Requires a Multidisciplinary Approach
 Editorial Staying in the Pink of Health for Patients with Cardiorenal Anemia Requires a Multidisciplinary Approach Anemia and Heart Failure Ragavendra R. Baliga, MD, MBA James B. Young, MD Consulting Editors
Editorial Staying in the Pink of Health for Patients with Cardiorenal Anemia Requires a Multidisciplinary Approach Anemia and Heart Failure Ragavendra R. Baliga, MD, MBA James B. Young, MD Consulting Editors
State of the Art: acute heart failure Is it just congestion?
 ESC CONGRESS 2017 Barcelona, 26. 30. August 2017 State of the Art: acute heart failure Is it just congestion? S.B. Felix, FESC Klinik für Innere Medizin B Ernst-Moritz-Arndt-Universität Greifswald 1456
ESC CONGRESS 2017 Barcelona, 26. 30. August 2017 State of the Art: acute heart failure Is it just congestion? S.B. Felix, FESC Klinik für Innere Medizin B Ernst-Moritz-Arndt-Universität Greifswald 1456
DIAGNOSIS AND MANAGEMENT OF ACUTE HEART FAILURE
 DIAGNOSIS AND MANAGEMENT OF ACUTE HEART FAILURE Mefri Yanni, MD Bagian Kardiologi dan Kedokteran Vaskular RS.DR.M.Djamil Padang The 3rd Symcard Padang, Mei 2013 Outline Diagnosis Diagnosis Treatment options
DIAGNOSIS AND MANAGEMENT OF ACUTE HEART FAILURE Mefri Yanni, MD Bagian Kardiologi dan Kedokteran Vaskular RS.DR.M.Djamil Padang The 3rd Symcard Padang, Mei 2013 Outline Diagnosis Diagnosis Treatment options
Cardiorenal syndrome. Sofie Gevaert. Ghent University Hospital, Belgium
 Cardiorenal syndrome Sofie Gevaert Ghent University Hospital, Belgium Disclosures Consultancy Astra Zeneca Boegringer MSD Novartis 68 y old man, ADHF ICMP, ejection fraction 35 %: progressive dyspnea,
Cardiorenal syndrome Sofie Gevaert Ghent University Hospital, Belgium Disclosures Consultancy Astra Zeneca Boegringer MSD Novartis 68 y old man, ADHF ICMP, ejection fraction 35 %: progressive dyspnea,
Understanding the Cardio-Renal Syndromes
 Understanding the Cardio-Renal Syndromes The Cardio-Renal axis: an underestimated player in cardiovascular diseases ESC Congress Munich 27/08/2012 Alberto Palazzuoli Department of Internal Medicine Cardiology
Understanding the Cardio-Renal Syndromes The Cardio-Renal axis: an underestimated player in cardiovascular diseases ESC Congress Munich 27/08/2012 Alberto Palazzuoli Department of Internal Medicine Cardiology
Acute Kidney Injury for the General Surgeon
 Acute Kidney Injury for the General Surgeon UCSF Postgraduate Course in General Surgery Maui, HI March 20, 2011 Epidemiology & Definition Pathophysiology Clinical Studies Management Summary Hobart W. Harris,
Acute Kidney Injury for the General Surgeon UCSF Postgraduate Course in General Surgery Maui, HI March 20, 2011 Epidemiology & Definition Pathophysiology Clinical Studies Management Summary Hobart W. Harris,
ACUTE HEART FAILURE. Julie Gorchynski MD, MSc, FACEP, FAAEM. Department of Emergency Medicine Emergency Residency Program UTHSC, San Antonio TCEP 2014
 ACUTE HEART FAILURE Julie Gorchynski MD, MSc, FACEP, FAAEM Department of Emergency Medicine Emergency Residency Program UTHSC, San Antonio TCEP 2014 No disclosures Objectives Overview Cases Current Therapy
ACUTE HEART FAILURE Julie Gorchynski MD, MSc, FACEP, FAAEM Department of Emergency Medicine Emergency Residency Program UTHSC, San Antonio TCEP 2014 No disclosures Objectives Overview Cases Current Therapy
Cardiorenal Syndrome Prof. Dr. Bülent ALTUN Hacettepe University Faculty of Medicine Department of Internal Medicine Division of Nephrology
 Cardiorenal Syndrome Prof. Dr. Bülent ALTUN Hacettepe University Faculty of Medicine Department of Internal Medicine Division of Nephrology Heart and Kidney The kidney yin dominates water, The heart yang
Cardiorenal Syndrome Prof. Dr. Bülent ALTUN Hacettepe University Faculty of Medicine Department of Internal Medicine Division of Nephrology Heart and Kidney The kidney yin dominates water, The heart yang
Medical Management of Acutely Decompensated Heart Failure. William T. Abraham, MD Director, Division of Cardiovascular Medicine
 Medical Management of Acutely Decompensated Heart Failure William T. Abraham, MD Director, Division of Cardiovascular Medicine Orlando, Florida October 7-9, 2011 Goals of Acute Heart Failure Therapy Alleviate
Medical Management of Acutely Decompensated Heart Failure William T. Abraham, MD Director, Division of Cardiovascular Medicine Orlando, Florida October 7-9, 2011 Goals of Acute Heart Failure Therapy Alleviate
The Art and Science of Diuretic therapy
 The Art and Science of Diuretic therapy Dr. Fayez EL Shaer Associate Professour of cardiology Consultant cardiologist MD, MSc, PhD, CBNC, NBE FESC, ACCP, FASNC,HFA KKUH, KFCC Heart failure: fluid overload
The Art and Science of Diuretic therapy Dr. Fayez EL Shaer Associate Professour of cardiology Consultant cardiologist MD, MSc, PhD, CBNC, NBE FESC, ACCP, FASNC,HFA KKUH, KFCC Heart failure: fluid overload
M2 TEACHING UNDERSTANDING PHARMACOLOGY
 M2 TEACHING UNDERSTANDING PHARMACOLOGY USING CVS SYSTEM AS AN EXAMPLE NIGEL FONG 2 JAN 2014 TODAY S OBJECTIVE Pharmacology often seems like an endless list of mechanisms and side effects to memorize. To
M2 TEACHING UNDERSTANDING PHARMACOLOGY USING CVS SYSTEM AS AN EXAMPLE NIGEL FONG 2 JAN 2014 TODAY S OBJECTIVE Pharmacology often seems like an endless list of mechanisms and side effects to memorize. To
LXIV: DRUGS: 4. RAS BLOCKADE
 LXIV: DRUGS: 4. RAS BLOCKADE ACE Inhibitors Components of RAS Actions of Angiotensin i II Indications for ACEIs Contraindications RAS blockade in hypertension RAS blockade in CAD RAS blockade in HF Limitations
LXIV: DRUGS: 4. RAS BLOCKADE ACE Inhibitors Components of RAS Actions of Angiotensin i II Indications for ACEIs Contraindications RAS blockade in hypertension RAS blockade in CAD RAS blockade in HF Limitations
HEART FAILURE PHARMACOLOGY. University of Hawai i Hilo Pre- Nursing Program NURS 203 General Pharmacology Danita Narciso Pharm D
 HEART FAILURE PHARMACOLOGY University of Hawai i Hilo Pre- Nursing Program NURS 203 General Pharmacology Danita Narciso Pharm D 1 LEARNING OBJECTIVES Understand the effects of heart failure in the body
HEART FAILURE PHARMACOLOGY University of Hawai i Hilo Pre- Nursing Program NURS 203 General Pharmacology Danita Narciso Pharm D 1 LEARNING OBJECTIVES Understand the effects of heart failure in the body
Acute Kidney Injury. Amandeep Khurana, MD Southwest Kidney Institute
 Acute Kidney Injury Amandeep Khurana, MD Southwest Kidney Institute 66 yr white male w/ DM, HTN, CAD admitted to an OSH w/ E Coli UTI on 7/24/16, developed E Coli bacteremia and Shock (on vaso + levo)
Acute Kidney Injury Amandeep Khurana, MD Southwest Kidney Institute 66 yr white male w/ DM, HTN, CAD admitted to an OSH w/ E Coli UTI on 7/24/16, developed E Coli bacteremia and Shock (on vaso + levo)
Cardiovascular Disease in CKD. Parham Eftekhari, D.O., M.Sc. Assistant Clinical Professor Medicine NSUCOM / Broward General Medical Center
 Cardiovascular Disease in CKD Parham Eftekhari, D.O., M.Sc. Assistant Clinical Professor Medicine NSUCOM / Broward General Medical Center Objectives Describe prevalence for cardiovascular disease in CKD
Cardiovascular Disease in CKD Parham Eftekhari, D.O., M.Sc. Assistant Clinical Professor Medicine NSUCOM / Broward General Medical Center Objectives Describe prevalence for cardiovascular disease in CKD
Definition of Congestive Heart Failure
 Heart Failure Definition of Congestive Heart Failure A clinical syndrome of signs & symptoms resulting from the heart s inability to supply adequate tissue perfusion. CHF Epidemiology Affects 4.7 million
Heart Failure Definition of Congestive Heart Failure A clinical syndrome of signs & symptoms resulting from the heart s inability to supply adequate tissue perfusion. CHF Epidemiology Affects 4.7 million
Metabolic Syndrome and Chronic Kidney Disease
 Metabolic Syndrome and Chronic Kidney Disease Definition of Metabolic Syndrome National Cholesterol Education Program (NCEP) Adult Treatment Panel (ATP) III Abdominal obesity, defined as a waist circumference
Metabolic Syndrome and Chronic Kidney Disease Definition of Metabolic Syndrome National Cholesterol Education Program (NCEP) Adult Treatment Panel (ATP) III Abdominal obesity, defined as a waist circumference
Advanced Care for Decompensated Heart Failure
 Advanced Care for Decompensated Heart Failure Sara Kalantari MD Assistant Professor of Medicine, University of Chicago Advanced Heart Failure, Mechanical Circulatory Support and Cardiac Transplantation
Advanced Care for Decompensated Heart Failure Sara Kalantari MD Assistant Professor of Medicine, University of Chicago Advanced Heart Failure, Mechanical Circulatory Support and Cardiac Transplantation
Objectives 6/14/2016. Cardiorenal Syndrome: Critical Link Between Heart and Kidney
 Cardiorenal Syndrome: Critical Link Between Heart and Kidney Chris M. Bell, ACNP Cardiology Associates of North Mississippi Objectives Review the 5 Subtypes of the Cardiorenal Syndrome (CRS) Discuss the
Cardiorenal Syndrome: Critical Link Between Heart and Kidney Chris M. Bell, ACNP Cardiology Associates of North Mississippi Objectives Review the 5 Subtypes of the Cardiorenal Syndrome (CRS) Discuss the
ENDPOINTS FOR AKI STUDIES
 ENDPOINTS FOR AKI STUDIES Raymond Vanholder, University Hospital, Ghent, Belgium SUMMARY! AKI as an endpoint! Endpoints for studies in AKI 2 AKI AS AN ENDPOINT BEFORE RIFLE THE LIST OF DEFINITIONS WAS
ENDPOINTS FOR AKI STUDIES Raymond Vanholder, University Hospital, Ghent, Belgium SUMMARY! AKI as an endpoint! Endpoints for studies in AKI 2 AKI AS AN ENDPOINT BEFORE RIFLE THE LIST OF DEFINITIONS WAS
Acute heart failure syndromes: clinical challenges. Pathophysiology. ESC Congress August. Paris, France. Marco Metra
 ESC Congress 2011 27-31 August. Paris, France. Acute heart failure syndromes: clinical challenges. Pathophysiology Marco Metra Cardiology, Dept. Of experimental and applied medicine. University of Brescia.
ESC Congress 2011 27-31 August. Paris, France. Acute heart failure syndromes: clinical challenges. Pathophysiology Marco Metra Cardiology, Dept. Of experimental and applied medicine. University of Brescia.
RRT in Advanced Heart Failure and Liver Failure When to start and when to stop?
 Critical Care Medicine Apollo Hospitals RRT in Advanced Heart Failure and Liver Failure When to start and when to stop? Ramesh Venkataraman, AB (Int. Med), AB (CCM) Senior Consultant, Critical Care Medicine
Critical Care Medicine Apollo Hospitals RRT in Advanced Heart Failure and Liver Failure When to start and when to stop? Ramesh Venkataraman, AB (Int. Med), AB (CCM) Senior Consultant, Critical Care Medicine
Overcoming the Cardiorenal Syndrome
 Overcoming the Cardiorenal Syndrome October 29, 2016 Randall C Starling MD MPH FACC FESC FHFSA FHFA Professor of Medicine Heart & Vascular Institute Cleveland Clinic Lerner College of Medicine Cleveland
Overcoming the Cardiorenal Syndrome October 29, 2016 Randall C Starling MD MPH FACC FESC FHFSA FHFA Professor of Medicine Heart & Vascular Institute Cleveland Clinic Lerner College of Medicine Cleveland
Cardio-Renal Syndrome in Acute Heart Failure:
 Cardio-Renal Syndrome in Acute Heart Failure: Target for Therapy Marvin A. Konstam, M.D. Research support and/or consulting relevant to this lecture: Merck, Otsuka, Johnson & Johnson; Amgen; Cardiokine
Cardio-Renal Syndrome in Acute Heart Failure: Target for Therapy Marvin A. Konstam, M.D. Research support and/or consulting relevant to this lecture: Merck, Otsuka, Johnson & Johnson; Amgen; Cardiokine
Heart-failure or Kidney Failure?
 Heart-failure or Kidney Failure? Dr Ajith James Consultant Nephrologist Barts Health and BHRUT Mr AR 65 yrs Case Type 2 DM, IHD-MI 1998, 2003. PCI x 3. CABG 2008, HT CCF with LVEF 30% 2014. NYHA Class
Heart-failure or Kidney Failure? Dr Ajith James Consultant Nephrologist Barts Health and BHRUT Mr AR 65 yrs Case Type 2 DM, IHD-MI 1998, 2003. PCI x 3. CABG 2008, HT CCF with LVEF 30% 2014. NYHA Class
Treating the patient with acute heart failure. What do we really know? Principles of acute heart failure treatment
 ESC 2012 27Aug - 3Sep, 2012, Munich, Germany Treating the patient with acute heart failure. What do we really know? Principles of acute heart failure treatment Marco Metra, MD, FESC Cardiology University
ESC 2012 27Aug - 3Sep, 2012, Munich, Germany Treating the patient with acute heart failure. What do we really know? Principles of acute heart failure treatment Marco Metra, MD, FESC Cardiology University
Update on Cardiorenal Syndrome: A Clinical Conundrum
 Advances in Peritoneal Dialysis, Vol. 27, 2011 Eric J. Chan, 1 Kevin C. Dellsperger 1 3 Update on Cardiorenal Syndrome: A Clinical Conundrum Our understanding of the cardiorenal syndrome continues to progress.
Advances in Peritoneal Dialysis, Vol. 27, 2011 Eric J. Chan, 1 Kevin C. Dellsperger 1 3 Update on Cardiorenal Syndrome: A Clinical Conundrum Our understanding of the cardiorenal syndrome continues to progress.
Summary/Key Points Introduction
 Summary/Key Points Introduction Scope of Heart Failure (HF) o 6.5 million Americans 20 years of age have HF o 960,000 new cases of HF diagnosed annually o 5-year survival rate for HF is ~50% Classification
Summary/Key Points Introduction Scope of Heart Failure (HF) o 6.5 million Americans 20 years of age have HF o 960,000 new cases of HF diagnosed annually o 5-year survival rate for HF is ~50% Classification
Pearls in Acute Heart Failure Management
 Pearls in Acute Heart Failure Management Best Practices Juan M. Aranda Jr., M.D. Professor of Medicine Medical Director of Heart Failure/ Transplant Program University of Florida College of Medicine Disclosures:
Pearls in Acute Heart Failure Management Best Practices Juan M. Aranda Jr., M.D. Professor of Medicine Medical Director of Heart Failure/ Transplant Program University of Florida College of Medicine Disclosures:
Ruolo dei Marcatori Bioumorali nello scompenso cardiaco
 Ruolo dei Marcatori Bioumorali nello scompenso cardiaco Head Emergency Medicine Sant Andrea Hospital Director Postgraduate School of Emergency Medicine Faculty od Medicine and Psycology Sapienza University
Ruolo dei Marcatori Bioumorali nello scompenso cardiaco Head Emergency Medicine Sant Andrea Hospital Director Postgraduate School of Emergency Medicine Faculty od Medicine and Psycology Sapienza University
Biomarkers for optimal management of heart failure. Cardiorenal syndrome. Veli-Pekka Harjola Helsinki University Central Hospital Helsinki, Finland
 Biomarkers for optimal management of heart failure Cardiorenal syndrome Veli-Pekka Harjola Helsinki University Central Hospital Helsinki, Finland Presenter Disclosure Information V-P Harjola The following
Biomarkers for optimal management of heart failure Cardiorenal syndrome Veli-Pekka Harjola Helsinki University Central Hospital Helsinki, Finland Presenter Disclosure Information V-P Harjola The following
Effects of Kidney Disease on Cardiovascular Morbidity and Mortality
 Effects of Kidney Disease on Cardiovascular Morbidity and Mortality Joachim H. Ix, MD, MAS Assistant Professor in Residence Division of Nephrology University of California San Diego, and Veterans Affairs
Effects of Kidney Disease on Cardiovascular Morbidity and Mortality Joachim H. Ix, MD, MAS Assistant Professor in Residence Division of Nephrology University of California San Diego, and Veterans Affairs
Management of acute decompensated heart failure and cardiogenic shock. Arintaya Phrommintikul Department of Medicine CMU
 Management of acute decompensated heart failure and cardiogenic shock Arintaya Phrommintikul Department of Medicine CMU Acute heart failure: spectrum Case 64 y/o M with Hx of non-ischemic DCM (LVEF=25-30%)
Management of acute decompensated heart failure and cardiogenic shock Arintaya Phrommintikul Department of Medicine CMU Acute heart failure: spectrum Case 64 y/o M with Hx of non-ischemic DCM (LVEF=25-30%)
Cardiorenal Biomarkers and Heart Failure. Nicholas Wettersten, MD April 7 th, 2017
 Cardiorenal Biomarkers and Heart Failure Nicholas Wettersten, MD April 7 th, 2017 Disclosures Still none, but looking for some Acute Kidney Injury Biomarkers 547 in 2015 4112 as of March 2017 Case 1 60
Cardiorenal Biomarkers and Heart Failure Nicholas Wettersten, MD April 7 th, 2017 Disclosures Still none, but looking for some Acute Kidney Injury Biomarkers 547 in 2015 4112 as of March 2017 Case 1 60
Cardiovascular Complications Of Chronic Kidney Disease. Dr Atir Khan Consultant Physician Diabetes & Endocrinology West Wales Hospital, Carmarthen
 Cardiovascular Complications Of Chronic Kidney Disease Dr Atir Khan Consultant Physician Diabetes & Endocrinology West Wales Hospital, Carmarthen Markers of kidney dysfunction Raised Albumin / Creatinine
Cardiovascular Complications Of Chronic Kidney Disease Dr Atir Khan Consultant Physician Diabetes & Endocrinology West Wales Hospital, Carmarthen Markers of kidney dysfunction Raised Albumin / Creatinine
Management of Advanced Systolic Heart Failure. Robert W. Hull MD FACC Associate Professor of Medicine West Virginia University
 Management of Advanced Systolic Heart Failure Robert W. Hull MD FACC Associate Professor of Medicine West Virginia University American College of Cardiology Foundation (ACCF) American Heart Association
Management of Advanced Systolic Heart Failure Robert W. Hull MD FACC Associate Professor of Medicine West Virginia University American College of Cardiology Foundation (ACCF) American Heart Association
Akash Ghai MD, FACC February 27, No Disclosures
 Akash Ghai MD, FACC February 27, 2015 No Disclosures Epidemiology Lifetime risk is > 20% for American s older than 40 years old. > 650,000 new cases diagnosed each year. Incidence increases with age: 2%
Akash Ghai MD, FACC February 27, 2015 No Disclosures Epidemiology Lifetime risk is > 20% for American s older than 40 years old. > 650,000 new cases diagnosed each year. Incidence increases with age: 2%
Pathophysiology: Heart Failure
 Pathophysiology: Heart Failure Mat Maurer, MD Irving Assistant Professor of Medicine Outline Definitions and Classifications Epidemiology Muscle and Chamber Function Pathophysiology Heart Failure: Definitions
Pathophysiology: Heart Failure Mat Maurer, MD Irving Assistant Professor of Medicine Outline Definitions and Classifications Epidemiology Muscle and Chamber Function Pathophysiology Heart Failure: Definitions
Contrast Induced Nephropathy
 Contrast Induced Nephropathy O CIAKI refers to an abrupt deterioration in renal function associated with the administration of iodinated contrast media O CIAKI is characterized by an acute (within 48 hours)
Contrast Induced Nephropathy O CIAKI refers to an abrupt deterioration in renal function associated with the administration of iodinated contrast media O CIAKI is characterized by an acute (within 48 hours)
Antialdosterone treatment in heart failure
 Update on the Treatment of Chronic Heart Failure 2012 Antialdosterone treatment in heart failure 전남의대윤현주 Chronic Heart Failure Prognosis of Heart failure Cecil, Text book of Internal Medicine, 22 th edition
Update on the Treatment of Chronic Heart Failure 2012 Antialdosterone treatment in heart failure 전남의대윤현주 Chronic Heart Failure Prognosis of Heart failure Cecil, Text book of Internal Medicine, 22 th edition
Outline. Pathophysiology: Heart Failure. Heart Failure. Heart Failure: Definitions. Etiologies. Etiologies
 Outline Pathophysiology: Mat Maurer, MD Irving Assistant Professor of Medicine Definitions and Classifications Epidemiology Muscle and Chamber Function Pathophysiology : Definitions An inability of the
Outline Pathophysiology: Mat Maurer, MD Irving Assistant Professor of Medicine Definitions and Classifications Epidemiology Muscle and Chamber Function Pathophysiology : Definitions An inability of the
Heart Failure (HF) Treatment
 Treatment") Heart Failure (HF) Treatment Heart Failure (HF) Complex, progressive disorder. The heart is unable to pump sufficient blood to meet the needs of the body. Its cardinal symptoms are dyspnea, fatigue, and
Heart Failure (HF) Treatment Heart Failure (HF) Complex, progressive disorder. The heart is unable to pump sufficient blood to meet the needs of the body. Its cardinal symptoms are dyspnea, fatigue, and
Management of Acute Heart Failure
 Management of Acute Heart Failure Uri Elkayam, MD Professor of Medicine University of Southern California School of Medicine Los Angeles, California elkayam@usc.edu ADHF Treatments Goals.2 Improve symptoms.
Management of Acute Heart Failure Uri Elkayam, MD Professor of Medicine University of Southern California School of Medicine Los Angeles, California elkayam@usc.edu ADHF Treatments Goals.2 Improve symptoms.
Dr.Nahid Osman Ahmed 1
 1 ILOS By the end of the lecture you should be able to Identify : Functions of the kidney and nephrons Signs and symptoms of AKI Risk factors to AKI Treatment alternatives 2 Acute kidney injury (AKI),
1 ILOS By the end of the lecture you should be able to Identify : Functions of the kidney and nephrons Signs and symptoms of AKI Risk factors to AKI Treatment alternatives 2 Acute kidney injury (AKI),
Biomarkers, the Kidney and the Heart: Acute Kidney Injury
 Biomarkers, the Kidney and the Heart: Acute Kidney Injury 12th Annual Conference on Biomarkers in Heart Failure and Acute Coronary Syndromes: Diagnosis, Treatment and Devices San Diego May 13, 2016 Ravindra
Biomarkers, the Kidney and the Heart: Acute Kidney Injury 12th Annual Conference on Biomarkers in Heart Failure and Acute Coronary Syndromes: Diagnosis, Treatment and Devices San Diego May 13, 2016 Ravindra
NGAL Connect to the kidneys
 NGAL Connect to the kidneys Acute kidney injury (AKI) An imposing medical and diagnostic challenge >13 million AKI patients each year ~ 30% with fatal outcome Cardiac surgery > 1 million patients/year
NGAL Connect to the kidneys Acute kidney injury (AKI) An imposing medical and diagnostic challenge >13 million AKI patients each year ~ 30% with fatal outcome Cardiac surgery > 1 million patients/year
Acute Liver Failure: Supporting Other Organs
 Acute Liver Failure: Supporting Other Organs Michael A. Gropper, MD, PhD Professor of Anesthesia and Physiology Director, Critical Care Medicine University of California San Francisco Acute Liver Failure
Acute Liver Failure: Supporting Other Organs Michael A. Gropper, MD, PhD Professor of Anesthesia and Physiology Director, Critical Care Medicine University of California San Francisco Acute Liver Failure
Pre-discussion questions
 Amanda Bartlett, PA-C Dustin Bartlett, PA-C Andrea Applegate, PA-C Leslie Yearta Brown, NP CHF Round Table Discussion Objectives ANDREA- Discuss the definition and different categories of CHF DUSTIN- Define
Amanda Bartlett, PA-C Dustin Bartlett, PA-C Andrea Applegate, PA-C Leslie Yearta Brown, NP CHF Round Table Discussion Objectives ANDREA- Discuss the definition and different categories of CHF DUSTIN- Define
ESC Guidelines for the Diagnosis and Treatment of Acute and Chronic Heart Failure
 Patients t with acute heart failure frequently develop chronic heart failure Patients with chronic heart failure frequently decompensate acutely ESC Guidelines for the Diagnosis and A clinical response
Patients t with acute heart failure frequently develop chronic heart failure Patients with chronic heart failure frequently decompensate acutely ESC Guidelines for the Diagnosis and A clinical response
Management of Hypertension. M Misra MD MRCP (UK) Division of Nephrology University of Missouri School of Medicine
 Division of Nephrology University of Missouri School of Medicine") Management of Hypertension M Misra MD MRCP (UK) Division of Nephrology University of Missouri School of Medicine Disturbing Trends in Hypertension HTN awareness, treatment and control rates are decreasing
Management of Hypertension M Misra MD MRCP (UK) Division of Nephrology University of Missouri School of Medicine Disturbing Trends in Hypertension HTN awareness, treatment and control rates are decreasing
2016 Update to Heart Failure Clinical Practice Guidelines
 2016 Update to Heart Failure Clinical Practice Guidelines Mitchell T. Saltzberg, MD, FACC, FAHA, FHFSA Medical Director of Advanced Heart Failure Froedtert & Medical College of Wisconsin Stages, Phenotypes
2016 Update to Heart Failure Clinical Practice Guidelines Mitchell T. Saltzberg, MD, FACC, FAHA, FHFSA Medical Director of Advanced Heart Failure Froedtert & Medical College of Wisconsin Stages, Phenotypes
Case year old female nursing home resident with a hx CAD, PUD, recent hip fracture Transferred to ED with decreased mental status BP in ED 80/50
 Case 1 65 year old female nursing home resident with a hx CAD, PUD, recent hip fracture Transferred to ED with decreased mental status BP in ED 80/50 Case 1 65 year old female nursing home resident with
Case 1 65 year old female nursing home resident with a hx CAD, PUD, recent hip fracture Transferred to ED with decreased mental status BP in ED 80/50 Case 1 65 year old female nursing home resident with
Οξεία καρδιακή ανεπάρκεια: Ποιες παράμετροι συμβάλλουν στη διαστρωμάτωση κινδύνου των ασθενών;
 Οξεία καρδιακή ανεπάρκεια: Ποιες παράμετροι συμβάλλουν στη διαστρωμάτωση κινδύνου των ασθενών; Γ. Φιλιππάτος, MD, FACC, FESC, FCCP Επ. Καθηγητής Καρδιολογίας Πανεπ. Αθηνών Clinical Outcomes in Patients
Οξεία καρδιακή ανεπάρκεια: Ποιες παράμετροι συμβάλλουν στη διαστρωμάτωση κινδύνου των ασθενών; Γ. Φιλιππάτος, MD, FACC, FESC, FCCP Επ. Καθηγητής Καρδιολογίας Πανεπ. Αθηνών Clinical Outcomes in Patients
CKD and risk management : NICE guideline
 CKD and risk management : NICE guideline 2008-2014 Shahed Ahmed Consultant Nephrologist shahed.ahmed@rlbuht.nhs.uk Key points : Changing parameters of CKD and NICE guidance CKD and age related change of
CKD and risk management : NICE guideline 2008-2014 Shahed Ahmed Consultant Nephrologist shahed.ahmed@rlbuht.nhs.uk Key points : Changing parameters of CKD and NICE guidance CKD and age related change of
The Failing Heart in Primary Care
 The Failing Heart in Primary Care Hamid Ikram How fares the Heart Failure Epidemic? 4357 patients, 57% women, mean age 74 years HFSA 2010 Practice Guideline (3.1) Heart Failure Prevention A careful and
The Failing Heart in Primary Care Hamid Ikram How fares the Heart Failure Epidemic? 4357 patients, 57% women, mean age 74 years HFSA 2010 Practice Guideline (3.1) Heart Failure Prevention A careful and
Acute Kidney Injury in the Hospitalized Patient
 Acute Kidney Injury in the Hospitalized Patient Biff F. Palmer, M.D. Professor of Internal Medicine University of Texas Southwestern Medical Center, Dallas Texas Classification of Acute Kidney Injury 1
Acute Kidney Injury in the Hospitalized Patient Biff F. Palmer, M.D. Professor of Internal Medicine University of Texas Southwestern Medical Center, Dallas Texas Classification of Acute Kidney Injury 1
Practical Points in Cardiorenal Syndrome
 Practical Points in Cardiorenal Syndrome Vichai Senthong, MD. Cardiovascular Unit, Faculty of Medicine Khon Kaen university HFCT Annual Scientific Meeting June 16, 2017, Eastin Grand Sathorn Hotel, Bangkok
Practical Points in Cardiorenal Syndrome Vichai Senthong, MD. Cardiovascular Unit, Faculty of Medicine Khon Kaen university HFCT Annual Scientific Meeting June 16, 2017, Eastin Grand Sathorn Hotel, Bangkok
Heart Failure. Cardiac Anatomy. Functions of the Heart. Cardiac Cycle/Hemodynamics. Determinants of Cardiac Output. Cardiac Output
 Cardiac Anatomy Heart Failure Professor Qing ZHANG Department of Cardiology, West China Hospital www.blaufuss.org Cardiac Cycle/Hemodynamics Functions of the Heart Essential functions of the heart to cover
Cardiac Anatomy Heart Failure Professor Qing ZHANG Department of Cardiology, West China Hospital www.blaufuss.org Cardiac Cycle/Hemodynamics Functions of the Heart Essential functions of the heart to cover
WORSENING OF RENAL FUNCTION AFTER RAS INHIBITION IN DECOMPENSATED HEART FAILURE: CLINICAL IMPLICATIONS
 WORSENING OF RENAL FUNCTION AFTER RAS INHIBITION IN DECOMPENSATED HEART FAILURE: CLINICAL IMPLICATIONS George Bakris, MD, FASH, FAHA, FASN Professor of Medicine Director, Comprehensive Hypertension Center
WORSENING OF RENAL FUNCTION AFTER RAS INHIBITION IN DECOMPENSATED HEART FAILURE: CLINICAL IMPLICATIONS George Bakris, MD, FASH, FAHA, FASN Professor of Medicine Director, Comprehensive Hypertension Center
Innovation therapy in Heart Failure
 Innovation therapy in Heart Failure P. Laothavorn September 2015 Topics of discussion Basic Knowledge about heart failure Standard therapy New emerging therapy References: standard Therapy in Heart Failure
Innovation therapy in Heart Failure P. Laothavorn September 2015 Topics of discussion Basic Knowledge about heart failure Standard therapy New emerging therapy References: standard Therapy in Heart Failure
Vasoactive Medications. Matthew J. Korobey Pharm.D., BCCCP Critical Care Clinical Specialist Mercy St. Louis
 Vasoactive Medications Matthew J. Korobey Pharm.D., BCCCP Critical Care Clinical Specialist Mercy St. Louis Objectives List components of physiology involved in blood pressure Review terminology related
Vasoactive Medications Matthew J. Korobey Pharm.D., BCCCP Critical Care Clinical Specialist Mercy St. Louis Objectives List components of physiology involved in blood pressure Review terminology related
Angiotensin Converting Enzyme inhibitor (ACEi) / Angiotensin Receptor Blocker (ARB) To STOP OR Not in Advanced Renal Disease
 / Angiotensin Receptor Blocker (ARB) To STOP OR Not in Advanced Renal Disease") Angiotensin Converting Enzyme inhibitor (ACEi) / Angiotensin Receptor Blocker (ARB) To STOP OR Not in Advanced Renal Disease Investigator Meeting 12 th September 2017 - Sheffield Prof Sunil Bhandari Consultant
Angiotensin Converting Enzyme inhibitor (ACEi) / Angiotensin Receptor Blocker (ARB) To STOP OR Not in Advanced Renal Disease Investigator Meeting 12 th September 2017 - Sheffield Prof Sunil Bhandari Consultant
Heart Failure: Combination Treatment Strategies
 Heart Failure: Combination Treatment Strategies M. McDonald MD, FRCP State of the Heart Symposium May 28, 2011 None Disclosures Case 69 F, prior MIs (LV ejection fraction 25%), HTN No demonstrable ischemia
Heart Failure: Combination Treatment Strategies M. McDonald MD, FRCP State of the Heart Symposium May 28, 2011 None Disclosures Case 69 F, prior MIs (LV ejection fraction 25%), HTN No demonstrable ischemia
Trial to Reduce. Aranesp* Therapy. Cardiovascular Events with
 Trial to Reduce Cardiovascular Events with Aranesp* Therapy John J.V. McMurray, Hajime Uno, Petr Jarolim, Akshay S. Desai, Dick de Zeeuw, Kai-Uwe Eckardt, Peter Ivanovich, Andrew S. Levey, Eldrin F. Lewis,
Trial to Reduce Cardiovascular Events with Aranesp* Therapy John J.V. McMurray, Hajime Uno, Petr Jarolim, Akshay S. Desai, Dick de Zeeuw, Kai-Uwe Eckardt, Peter Ivanovich, Andrew S. Levey, Eldrin F. Lewis,
Optimal blockade of the Renin- Angiotensin-Aldosterone. in chronic heart failure
 Optimal blockade of the Renin- Angiotensin-Aldosterone Aldosterone- (RAA)-System in chronic heart failure Jan Östergren Department of Medicine Karolinska University Hospital Stockholm, Sweden Key Issues
Optimal blockade of the Renin- Angiotensin-Aldosterone Aldosterone- (RAA)-System in chronic heart failure Jan Östergren Department of Medicine Karolinska University Hospital Stockholm, Sweden Key Issues
Biomarkers in cardiovascular disease. Felix J. Rogers, DO, FACOI April 29, 2018
 Biomarkers in cardiovascular disease Felix J. Rogers, DO, FACOI April 29, 2018 Biomarkers NIH: A biomarker is a characteristic that is objectively measured and evaluated as an indicator of normal biological
Biomarkers in cardiovascular disease Felix J. Rogers, DO, FACOI April 29, 2018 Biomarkers NIH: A biomarker is a characteristic that is objectively measured and evaluated as an indicator of normal biological
The Who, How and When of Advanced Heart Failure Therapies. Disclosures. What is Advanced Heart Failure?
 The Who, How and When of Advanced Heart Failure Therapies 9 th Annual Dartmouth Conference on Advances in Heart Failure Therapies Dartmouth-Hitchcock Medical Center Lebanon, NH May 20, 2013 Joseph G. Rogers,
The Who, How and When of Advanced Heart Failure Therapies 9 th Annual Dartmouth Conference on Advances in Heart Failure Therapies Dartmouth-Hitchcock Medical Center Lebanon, NH May 20, 2013 Joseph G. Rogers,
Cardiovascular Protection and the RAS
 Cardiovascular Protection and the RAS Katalin Kauser, MD, PhD, DSc Senior Associate Director, Boehringer Ingelheim Pharmaceutical Inc. Micardis Product Pipeline Scientific Support Ridgefield, CT, USA Cardiovascular
Cardiovascular Protection and the RAS Katalin Kauser, MD, PhD, DSc Senior Associate Director, Boehringer Ingelheim Pharmaceutical Inc. Micardis Product Pipeline Scientific Support Ridgefield, CT, USA Cardiovascular
Cardio-renal syndrome.
 Review Article Cardio-renal syndrome. http://www.alliedacademies.org/archives-of-general-internal-medicine/ ISSN: 2591-7951 Dhiraj Kumar*, Abhijeet Yelale, Girish Sabnis, Hetan Shah, Charan Lanjewar, Prafulla
Review Article Cardio-renal syndrome. http://www.alliedacademies.org/archives-of-general-internal-medicine/ ISSN: 2591-7951 Dhiraj Kumar*, Abhijeet Yelale, Girish Sabnis, Hetan Shah, Charan Lanjewar, Prafulla
WHY ADMINISTER CARDIOTONIC AGENTS?
 Cardiac Pharmacology: Ideas For Advancing Your Clinical Practice The image cannot be displayed. Your computer may not have enough memory to open the image, or Roberta L. Hines, M.D. Nicholas M. Greene
Cardiac Pharmacology: Ideas For Advancing Your Clinical Practice The image cannot be displayed. Your computer may not have enough memory to open the image, or Roberta L. Hines, M.D. Nicholas M. Greene
Nora Goldschlager, M.D. SFGH Division of Cardiology UCSF
 CLASSIFICATION OF HEART FAILURE Nora Goldschlager, M.D. SFGH Division of Cardiology UCSF DISCLOSURES: NONE CLASSIFICATION C OF HEART FAILURE NYHA I IV New paradigm Stage A: Pts at high risk of developing
CLASSIFICATION OF HEART FAILURE Nora Goldschlager, M.D. SFGH Division of Cardiology UCSF DISCLOSURES: NONE CLASSIFICATION C OF HEART FAILURE NYHA I IV New paradigm Stage A: Pts at high risk of developing
HFpEF. April 26, 2018
 HFpEF April 26, 2018 (J Am Coll Cardiol 2017;70:2476 86) HFpEF 50% or more (40-71%) of patients with CHF have preserved LV systolic function. HFpEF is an increasingly frequent hospital discharge. Outcomes
HFpEF April 26, 2018 (J Am Coll Cardiol 2017;70:2476 86) HFpEF 50% or more (40-71%) of patients with CHF have preserved LV systolic function. HFpEF is an increasingly frequent hospital discharge. Outcomes
Tips & tricks on how to treat an acute heart failure patient with low cardiac output and diuretic resistance
 Tips & tricks on how to treat an acute heart failure patient with low cardiac output and diuretic resistance J. Parissis Attikon University Hospital, Athens, Greece Disclosures ALARM investigator received
Tips & tricks on how to treat an acute heart failure patient with low cardiac output and diuretic resistance J. Parissis Attikon University Hospital, Athens, Greece Disclosures ALARM investigator received
Heart Failure. Subjective SOB (shortness of breath) Peripheral edema. Orthopnea (2-3 pillows) PND (paroxysmal nocturnal dyspnea)
 Peripheral edema. Orthopnea (2-3 pillows) PND (paroxysmal nocturnal dyspnea)") Pharmacology I. Definitions A. Heart Failure (HF) Heart Failure Ezra Levy, Pharm.D. HF Results when one or both ventricles are unable to pump sufficient blood to meet the body s needs There are 2 types
Pharmacology I. Definitions A. Heart Failure (HF) Heart Failure Ezra Levy, Pharm.D. HF Results when one or both ventricles are unable to pump sufficient blood to meet the body s needs There are 2 types
Cardiovascular Pharmacotherapy
 Cardiovascular Pharmacotherapy Overview Mechanism of cardiovascular drugs Indications and clinical use in cardiology Renin-Angiotensin Inhibitors: Angiotensin-Converting Enzyme Inhibitors, Angiotensin
Cardiovascular Pharmacotherapy Overview Mechanism of cardiovascular drugs Indications and clinical use in cardiology Renin-Angiotensin Inhibitors: Angiotensin-Converting Enzyme Inhibitors, Angiotensin
Prevalence of anemia and cardiovascular diseases in chronic kidney disease patients: a single tertiary care centre study
 International Journal of Advances in Medicine Sathyan S et al. Int J Adv Med. 2017 Feb;4(1):247-251 http://www.ijmedicine.com pissn 2349-3925 eissn 2349-3933 Original Research Article DOI: http://dx.doi.org/10.18203/2349-3933.ijam20170120
International Journal of Advances in Medicine Sathyan S et al. Int J Adv Med. 2017 Feb;4(1):247-251 http://www.ijmedicine.com pissn 2349-3925 eissn 2349-3933 Original Research Article DOI: http://dx.doi.org/10.18203/2349-3933.ijam20170120
Recognizing and Treating Patients with the Cardio-Renal Syndrome
 Recognizing and Treating Patients with the Cardio-Renal Syndrome Joachim H. Ix, MD, MAS, FASN Professor of Medicine Chief; Division of Nephrology-Hypertension University of California San Diego 1 Conflicts
Recognizing and Treating Patients with the Cardio-Renal Syndrome Joachim H. Ix, MD, MAS, FASN Professor of Medicine Chief; Division of Nephrology-Hypertension University of California San Diego 1 Conflicts
Heart Failure. Jay Shavadia
 Heart Failure Jay Shavadia Definition Clinical syndrome characterized by: Symptoms: breathlessness at rest or on exercise, fatigue, tiredness or ankle swelling AND Signs: tachycardia, tachypnea, pulmonary
Heart Failure Jay Shavadia Definition Clinical syndrome characterized by: Symptoms: breathlessness at rest or on exercise, fatigue, tiredness or ankle swelling AND Signs: tachycardia, tachypnea, pulmonary
MEDICAL MANAGEMENT OF PATIENTS WITH HEART FAILURE AND REDUCED EJECTION FRACTION
 MEDICAL MANAGEMENT OF PATIENTS WITH HEART FAILURE AND REDUCED EJECTION FRACTION FRANCIS X. CELIS, D.O. OPSO FALL CONFERENCE PORTLAND, OR 16 SEPTEMBER 2017 OVERVIEW What are the ACC/AHA Stages of HF? What
MEDICAL MANAGEMENT OF PATIENTS WITH HEART FAILURE AND REDUCED EJECTION FRACTION FRANCIS X. CELIS, D.O. OPSO FALL CONFERENCE PORTLAND, OR 16 SEPTEMBER 2017 OVERVIEW What are the ACC/AHA Stages of HF? What
Acute heart Failure. Critical cardiac care: update Markku S. Nieminen Helsinki, Finland. M S Nieminen, AHF ,ESC Stockholm
 Acute heart Failure Critical cardiac care: update 2010 Markku S. Nieminen Helsinki, Finland M S Nieminen, AHF 300810,ESC Stockholm Acute heart Failure Critical cardiac care: update 2010 Markku S. Nieminen
Acute heart Failure Critical cardiac care: update 2010 Markku S. Nieminen Helsinki, Finland M S Nieminen, AHF 300810,ESC Stockholm Acute heart Failure Critical cardiac care: update 2010 Markku S. Nieminen
Atrial fibrillation in the ICU
 Atrial fibrillation in the ICU Atrial fibrillation Preexisting or incident (new onset) among nearly one in three critically ill patients Formation of arrhythogenic substrate usually fibrosis (CHF, hypertension,
Atrial fibrillation in the ICU Atrial fibrillation Preexisting or incident (new onset) among nearly one in three critically ill patients Formation of arrhythogenic substrate usually fibrosis (CHF, hypertension,
University of Groningen. Acute kidney injury after cardiac surgery Loef, Berthus Gerard
 University of Groningen Acute kidney injury after cardiac surgery Loef, Berthus Gerard IMPORTANT NOTE: You are advised to consult the publisher's version (publisher's PDF) if you wish to cite from it.
University of Groningen Acute kidney injury after cardiac surgery Loef, Berthus Gerard IMPORTANT NOTE: You are advised to consult the publisher's version (publisher's PDF) if you wish to cite from it.
Heart Failure CTSHP Fall Seminar
 Heart Failure CTSHP Fall Seminar Laurajo Ryan, PharmD, MSc, BCPS, CDE Pharmacist Learning Objectives Outline the pathophysiology of heart failure List triggers for decompensated heart failure Describe
Heart Failure CTSHP Fall Seminar Laurajo Ryan, PharmD, MSc, BCPS, CDE Pharmacist Learning Objectives Outline the pathophysiology of heart failure List triggers for decompensated heart failure Describe