Dronedarone in the Post-Pallas Era. Jorge E. Schliamser, MD Carmel Medical Center Haifa
|
|
|
- Willis Farmer
- 5 years ago
- Views:
Transcription
1 Dronedarone in the Post-Pallas Era Jorge E. Schliamser, MD Carmel Medical Center Haifa
2 Disclosures None
3 Dronedarone is a multichannel blocker Dronedarone possesses electrophysiologic characteristics of all Four Vaughan Williams Classes as shown in animal models Outward currents Ikr: rapidly activating delayed rectifier potassium current Iks: slowly activating delayed rectifier potassium current Ito: transient outward current Ik(Ach): muscarinic receptor-operated K+ current (atria) Inward currents Fast sodium currents Calcium channel antagonist Dronedarone has anti-fibrillatory effects in the ventricles and atria Gautier P, et al. J Cardiovasc Pharmacol. 2003;41(2): Doggrell SA, Hancox JC, Expert Opin Investig Drugs 2004;13:
4 Dronedarone possesses a different electrophysiological profile than amiodarone Guinea-pig (IC 50 ; µm) 1 Dronedarone Amiodarone I Kr (ventricle) 3 10 Outward currents I Ks (ventricle) I K1 (ventricle) >30 30 I K(Ach) (atrium)* *I Ks, I Kr, I to, I K1, I KUR Dronedarone Amiodarone Inward currents I Na (human; 3 µm) 2-97% -41% I Ca(L) (guinea pig; CI 50, µm) Adapted from: 1. Lalevée N, et al. J Cardiovasc Electrophysiol. 2003;14: Gautier P, et al. J Cardiovasc Pharmacol. 2003;41:
5 Dronedarone has structural differences compared to amiodarone Dronedarone O (CH 2 ) 3 CH 3 CH 3 SO 2 HN O(CH 2 ) 3 N (CH 2 ) 3 CH 3 O (CH 2 ) 3 CH 3 O (CH 2 ) 3 CH 3 I O(CH 2 ) 2 N CH 2 CH 3 Amiodarone O I CH 2 CH 3 Adapted from Kathofer et al. Cardiovasc Drug Rev. 2005;23(3):
6 Dronedarone and amiodarone-important pharmacological differences Dronedarone Amiodarone Inhibit multiple K + channels Inhibit Na + and Ca 2+ channels Exert anti-adrenergic effects Low proarrhythmic profile No significant effect on LV function No iodine Iodine Short half-life (25-30 hours) and no tissue accumulation High lipophilicity with long half life ( days) and tissue accumulation Coronary vasodilation refractory to Coronary vasodilation highly inhibition of NO synthase pathway dependent on NO Dronedarone has a greater anti-hypertensive effect than amiodarone Adapted from: Gautier P, et al. J Cardiovasc Pharmacol. 2003;41(2): Doggrell SA, Hancox JC, Expert Opin Investig Drugs 2004;13: Kathofer et al. Cardiovasc Drug Rev 2005;23(3): Wegener F et al. J Cardiovasc Electrophysiol. 2006;17(S2):S17-S20 Guiraudou P, et al. European Journal of Pharmacology 2004;496: Le Heuzey JY et al. J Cardiovasc Electrophysiol. 2010;21(6): NO=Nitric oxide 6LV=Left ventricular BP=Blood pressure
7 Dronedarone-CV Properties Antiarrhythmic efficacy at atrial level Rate controlling effects Vasodilatory effects Anti-adrenergic effects Blood pressure lowering properties 7
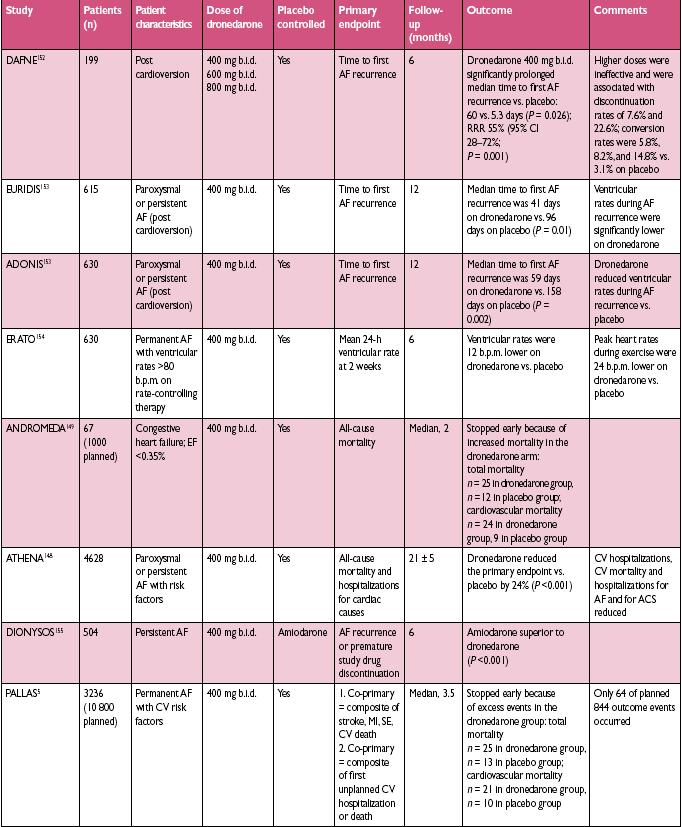
8 Dronedarone Trials I DAFNE 1 EURIDIS/ ADONIS 2 ERATO 3 Trial objective Dose finding study Effect of dronedarone on maintenance of sinus rhythm Effect of dronedarone in the control of mean 24-hour ventricular rate Patient population Persistent AF Paroxysmal/ Persistent AF Permanent AF Patient AF status at baseline In AF but eligible for AAD treatment and cardioversion In sinus rhythm In permanent AF Number of patients 102 1, Dronedarone Versus Placebo Placebo Both arms received standard therapy* Placebo Both arms received standard therapy* Primary endpoint Time to first AF recurrence Time to first AF/AFL recurrence Change in mean ventricular rate measured by 24-hour Holter ECG on Day 14 compared to baseline *Standard therapy may have included rate control agents (beta-blockers, and/or Ca-antagonist and/or digoxin) and/or anti-thrombotic therapy (Vit. K antagonists and/or aspirin and other antiplatelet therapy) and/or other CV agents such as ACEIs/ARBs and statins Adapted from: 1. Touboul P, et al. Eur Heart J. 2003;24: Singh BN, et al. N Engl J Med. 2007;357: Davy et al. Am Heart J. 2008;156:527.e1-527.e9. 8
9 Dronedarone Trials II ATHENA 1 DIONYSOS 2 ANDROMEDA 3 PALLAS 4 Trial objective Evaluate the efficacy and safety of dronedarone in the prevention of CV hospitalisation or allcause death Investigate efficacy and safety of dronedarone versus amiodarone for the maintenance of sinus rhythm Evaluate the potential benefit of dronedarone on all cause death or hospitalisation for worsening heart failure Evaluate the benefit of dronedarone in high risk permanent AF patients in reducing major CV events Patient population Paroxysmal/ Persistent AF Persistent AF Unstable recently decompensated CHF patients Permanent AF Patient AF status at baseline In sinus rhythm or AF but eligible for cardioversion In AF but eligible for AAD treatment and cardioversion N/A In permanent AF Number of patients 4, ,236 (10,800 planned) Dronedarone Versus Placebo Both arms received standard therapy* Amiodarone Placebo Placebo Both arms received standard therapy* Primary endpoint CV hospitalisation or all-cause mortality Treatment failure defined as recurrence of AF OR premature study drug discontinuation for intolerance or lack of efficacy Death from any cause or hospitalisation for worsening heart failure Trial stopped early for safety reasons Stroke, myocardial infarction, systemic embolism or CV death Trial stopped early for safety reasons *Standard therapy may have included rate control agents (beta-blockers, and/or Ca-antagonist and/or digoxin) and/or anti-thrombotic therapy (Vit. K antagonists and/or aspirin and other antiplatelet therapy) and/or other CV agents such as ACEIs/ARBs and statins Adapted from: 1. Hohnloser SH, et al. N Engl J Med 2009;360: Le Heuzey JY et al. J Cardiovasc Electrophysiol. 2010;21(6): Køber L, et al. N Engl J Med. 2008;358: Connolly SJ et al. N Engl J Med 2011; 365:
10 Dronedarone: The most extensively studied antiarrhythmic drug in AF 10,676 patients, including 5,553 receiving dronedarone Studies N Population Objectives DAFNE¹ 270 Persistent AF Dose ranging - cardioversion and maintenance of sinus rhythm EURIDIS/ADONIS 2 612/625 Paroxysmal/Persistent AF/AFL Maintenance of sinus rhythm ERATO Permanent AF Ventricular rate control DIONYSOS Persistent AF Comparative trial vs amiodarone ANDROMEDA / 1,000* ATHENA PALLAS / 10,800* Unstable CHF and LV dysfunction (25% in AF) Paroxysmal/ Persistent AF/AFL Permanent AF Morbidity-mortality study Prevention of CV hospitalization or death Prevention of major CV events/ hospitalization or death Heart failure study *Planned patient enrolment Touboul P, et al. Eur Heart J. 2003;24: Singh BN, et al. N Engl J Med. 2007;357: Davy et al. Am Heart J. 2008;156:527.e1-527.e9..3 Le Heuzey JY et al. J Cardiovasc Electrophysiol Apr 6 Epub Køber L, et al. N Engl J Med. 2008;358: Hohnloser SH, et al. N Engl J Med 2009;360: Connolly SJ, et al. N Engl J Med
11 In patients initiated prior to cardioversion, dronedarone 400 mg bid significantly reduced the risk of AF recurrence by 55% Persistent AF patients: Primary endpoint Proportion of patients in sinus rhythm Placebo DR 800mg DR 1200mg DR 1600mg 55% Reduction in Relative Risk (p=0.001) for 800mg 0.1 Patients at risk: Days Placebo DR 800mg DR 1200mg DR 1600mg Adapted from Touboul P, et al. Eur Heart J. 2003;24:
12 Dronedarone: The most extensively studied antiarrhythmic drug in AF 10,676 patients, including 5,553 receiving dronedarone Studies N Population Objectives DAFNE¹ 270 Persistent AF Dose ranging - cardioversion and maintenance of sinus rhythm EURIDIS/ADONIS 2 612/625 Paroxysmal/Persistent AF/AFL Maintenance of sinus rhythm ERATO Permanent AF Ventricular rate control DIONYSOS Persistent AF Comparative trial vs amiodarone ANDROMEDA / 1,000* ATHENA PALLAS / 10,800* Unstable CHF and LV dysfunction (25% in AF) Paroxysmal/ Persistent AF/AFL Permanent AF Morbidity-mortality study Prevention of CV hospitalization or death Prevention of major CV events/ hospitalization or death Heart failure study *Planned patient enrolment Touboul P, et al. Eur Heart J. 2003;24: Singh BN, et al. N Engl J Med. 2007;357: Davy et al. Am Heart J. 2008;156:527.e1-527.e9..3 Le Heuzey JY et al. J Cardiovasc Electrophysiol Apr 6 Epub Køber L, et al. N Engl J Med. 2008;358: Hohnloser SH, et al. N Engl J Med 2009;360: Connolly SJ, et al. N Engl J Med

 and/or antithrombotic therapy (oral anticoagulation and/or long-term antiplatelet therapy) and/or other CV therapy such as ACE inhibitors and statins 13")
13 Dronedarone more than doubled time to first AF/AFL recurrence Paroxysmal/persistent AF patients: Primary endpoint Median days x p= x Placebo on top of standard therapy* DR 400mg bid on top of standard therapy* p= x p< n=208 n=417 n=201 n=411 ADONIS EURIDIS n=409 n=828 Combined *Standard therapy may have included rate control agents (beta-blockers, and/or Ca-antagonists and/or digoxin) and/or antithrombotic therapy (oral anticoagulation and/or long-term antiplatelet therapy) and/or other CV therapy such as ACE inhibitors and statins 13 Adapted from Singh BN, et al. N Engl J Med. 2007;357:
14 Dronedarone: The most extensively studied antiarrhythmic drug in AF 10,676 patients, including 5,553 receiving dronedarone Studies N Population Objectives DAFNE¹ 270 Persistent AF Dose ranging - cardioversion and maintenance of sinus rhythm EURIDIS/ADONIS 2 612/625 Paroxysmal/Persistent AF/AFL Maintenance of sinus rhythm ERATO Permanent AF Ventricular rate control DIONYSOS Persistent AF Comparative trial vs amiodarone ANDROMEDA / 1,000* ATHENA PALLAS / 10,800* Unstable CHF and LV dysfunction (25% in AF) Paroxysmal/ Persistent AF/AFL Permanent AF Morbidity-mortality study Prevention of CV hospitalization or death Prevention of major CV events/ hospitalization or death Heart failure study *Planned patient enrolment Touboul P, et al. Eur Heart J. 2003;24: Singh BN, et al. N Engl J Med. 2007;357: Davy et al. Am Heart J. 2008;156:527.e1-527.e9..3 Le Heuzey JY et al. J Cardiovasc Electrophysiol Apr 6 Epub Køber L, et al. N Engl J Med. 2008;358: Hohnloser SH, et al. N Engl J Med 2009;360: Connolly SJ, et al. N Engl J Med
15 ANDROMEDA (ANtiarrhythmic trial with DROnedarone in Moderate to severe CHF Evaluating morbidity DecreAse) was: Conducted in high-risk congestive heart failure (CHF) patients with left ventricular dysfunction and a recent acute decompensation Aimed to evaluate the potential benefit of dronedarone on all cause death or hospitalisation for worsening heart failure Patients were not selected based on AF / AFL history Adapted from Køber L, et al. N Engl J Med. 2008;358:
16 Study endpoints Primary endpoint Death from any cause or hospitalisation for worsening heart failure Secondary endpoints Death from all causes Hospitalisation for cardiovascular causes Hospitalisation for worsening heart failure Occurrence of atrial fibrillation or flutter Death from arrhythmia Sudden death Adapted from Køber L, et al. N Engl J Med. 2008;358:
17 In ANDROMEDA, patients were not selected based on history of AF/AFL Placebo n=317 Dronedarone 400mg bid n=310 Age (years) Median (range) 72 (27-96) 71 (33-90) Weight (kg) Gender [n (%)] Male 242 (76.3%) 230 (74.2%) Wall motion index (WMI) Median (range) 0.9 ( ) 0.9 ( ) NYHA class [n (%)] Class II 121 (38.2%) 131 (42.3%) Class III 183 (57.7%) 173 (55.8%) Class IV 13 (4.1%) 6 (1.9%) Mean duration of heart failure (mo) Estimated GFR (ml/min) Mean (range) 52.8 (6-99) 50 (16-104) Atrial fibrillation or flutter mean (%) 85 (26.8) 72 (23.2) WMI=Wall-Motion Index. Adapted from Køber L, et al. N Engl J Med. 2008;358:
18 Increase in all-cause mortality in unstable Cumulative incidence (%) Patients at risk: Secondary endpoint CHF patients Placebo n=317 Number of patients who died Hazard Ratio % CI 1.07; 4.25 Log rank p value 0.03 Placebo Dronedarone 400mg bid Dronedarone 800mg n= Placebo DR 400mg bid Time (days) Adapted from Køber L, et al. N Engl J Med. 2008;358:
19 ANDROMEDA Key points ANDROMEDA was conducted in unstable CHF patients most of whom did not even have AF Dronedarone did not reduce mortality or decrease CV hospitalisations vs. placebo There was an increase in non-sudden cardiac deaths related to worsening heart failure No significant difference between placebo and dronedarone patients was seen for arrhythmic events and sudden deaths Køber L, et al. N Engl J Med. 2008;358:
20 Dronedarone: The most extensively studied antiarrhythmic drug in AF 10,676 patients, including 5,553 receiving dronedarone Studies N Population Objectives DAFNE¹ 270 Persistent AF Dose ranging - cardioversion and maintenance of sinus rhythm EURIDIS/ADONIS 2 612/625 Paroxysmal/Persistent AF/AFL Maintenance of sinus rhythm ERATO Permanent AF Ventricular rate control DIONYSOS Persistent AF Comparative trial vs amiodarone ANDROMEDA / 1,000* ATHENA PALLAS / 10,800* Unstable CHF and LV dysfunction (25% in AF) Paroxysmal/ Persistent AF/AFL Permanent AF Morbidity-mortality study Prevention of CV hospitalization or death Prevention of major CV events/ hospitalization or death Heart failure study *Planned patient enrolment Touboul P, et al. Eur Heart J. 2003;24: Singh BN, et al. N Engl J Med. 2007;357: Davy et al. Am Heart J. 2008;156:527.e1-527.e9..3 Le Heuzey JY et al. J Cardiovasc Electrophysiol Apr 6 Epub Køber L, et al. N Engl J Med. 2008;358: Hohnloser SH, et al. N Engl J Med 2009;360: Connolly SJ, et al. N Engl J Med
21 ATHENA Trial ATHENA Trial (A placebo-controlled, double-blind, parallel arm Trial to assess the efficacy of dronedarone 400 mg bid for the prevention of cardiovascular Hospitalization or death from any cause in patients with Atrial fibrillation/atrial flutter) Copyleft Clinical Trial Results. You Must Redistribute Slides
22 ATHENA Trial: Study Design 4,628 patients >75 years with atrial fibrillation or years with atrial fibrillation and at least one additional cardiovascular risk factor prior to randomization. Double blind. Randomized. Placebo controlled. International multicenter. Mean follow-up 21 months. R Dronedarone 400 mg BID Placebo mos. follow-up Primary Endpoint: composite of all-cause mortality combined with cardiovascular hospitalization Secondary Endpoint: death from any cause, cardiovascular death, hospitalization for cardiovascular reasons Copyleft Clinical Trial Results. You Must Redistribute Slides JCE 2008; 19.1/Heart Rhythm 2008
23 ATHENA Trial: Inclusion Criteria 75 yrs with or without additional risk factors 70 yrs with at least one of the following risk factors: arterial hypertension (ongoing therapy with at least two antihypertensive drugs of different classes), diabetes mellitus, prior stroke or transient ischemic attack or systemic embolism, left atrium diameter 50 mm by M-mode echocardiography, LVEF < 0.40 by 2Dechocardiography. Copyleft Clinical Trial Results. You Must Redistribute Slides JCE 2008; 19.1/Heart Rhythm 2008
24 ATHENA Trial: Exclusion Criteria Presence of one of the following cardiac conditions: Permanent AF Unstable hemodynamic situation (i.e., recently decompensated heart failure) Congestive heart failure NYHA class IV Planned major non-cardiac or cardiac surgery Acute myocarditis Bradycardia < 50 bpm and/or a PR interval > 0.28 seconds Significant sinus node disease in the past, if not treated with a pacemaker Copyleft Clinical Trial Results. You Must Redistribute Slides JCE 2008; 19.1/Heart Rhythm 2008
25 Athena-Baseline Characteristics Placebo n=2,327 Adapted from Hohnloser SH, et al. J Cardiovasc Electrophysiol 2008;19: Dronedarone n=2,301 All patients n=4,628 Age (mean ±SD, years) 71.7 ± ± ±9.0 <65yr 442 (19.0%) 431 (18.7%) 873 (18.9%) 65 to 75yr 907 (39.0%) 923 (40.1%) 1,830 (39.5%) 75yr 978 (42.0%) 947 (41.2%) 1,925 (41.6%) Female gender 1,038 (44.6%) 1,131 (49.2%) 2,169 (46.9%) AF/AFL at baseline 586 (25.2%) 569 (24.7%) 1,155 (25.0%) Structural heart disease 1,402 (60.9%) 1,330 (58.3%) 2,732 (59.6%) Hypertension 1,996 (85.8%) 1,999 (86.9%) 3,995 (86.3%) Coronary heart disease 737 (31.7%) 668 (29.0%) 1,405 (30.4%) Valvular heart disease 380 (16.3%) 379 (16.5%) 759 (16.4%) Non-ischemic cardiomyopathy 131 (5.6%) 123 (5.3%) 254 (5.5%) History of CHF NYHA II/III 515 (22.1%) 464 (20.2%) 979 (21.2%) LVEF < /2,281 (12.5%) 255/2,263 (11.3%) 540/4,544 (11.9%) LVEF < /2,281 (3.8%) 92/2,263 (4.1%) 179/4,544 (3.9%) Lone atrial fibrillation 139 (6.0%) 140 (6.1%) 279 (6.0%) Pacemaker 243 (10.4%) 214 (9.3%) 457 (9.9%) 25



26 In ATHENA, dronedarone decreased significantly the risk of unplanned CV hospitalisation or death by 24% significantly the risk of unplanned hospitalisation by 26% the risk of all-cause death by 16% significantly the risk of CV death by 29% Mean follow-up 21 ±5 months. Adapted from Hohnloser SH, et al. N Engl J Med 2009;360:
27 Athena Trial Results 24% significant risk reduction in the combined endpoint of CV hospitalisation or death 29% significant risk reduction in CV death 16% trend to lower risk of death from any cause 45% significant risk reduction for arrhythmic death (sudden death) 34% significant risk reduction for stroke (sub analysis) 26% significant risk reduction in CV hospitalisation
28 Dronedarone: The most extensively studied antiarrhythmic drug in AF 10,676 patients, including 5,553 receiving dronedarone Studies N Population Objectives DAFNE¹ 270 Persistent AF Dose ranging - cardioversion and maintenance of sinus rhythm EURIDIS/ADONIS 2 612/625 Paroxysmal/Persistent AF/AFL Maintenance of sinus rhythm ERATO Permanent AF Ventricular rate control DIONYSOS Persistent AF Comparative trial vs amiodarone ANDROMEDA / 1,000* ATHENA PALLAS / 10,800* Unstable CHF and LV dysfunction (25% in AF) Paroxysmal/ Persistent AF/AFL Permanent AF Morbidity-mortality study Prevention of CV hospitalization or death Prevention of major CV events/ hospitalization or death Heart failure study *Planned patient enrolment Dronedarone is contraindicated in permanent AF and should not be used for rate control Touboul P, et al. Eur Heart J. 2003;24: Singh BN, et al. N Engl J Med. 2007;357: Davy et al. Am Heart J. 2008;156:527.e1-527.e9..3 Le Heuzey JY et al. J Cardiovasc Electrophysiol Apr 6 Epub Køber L, et al. N Engl J Med. 2008;358: Hohnloser SH, et al. N Engl J Med 2009;360: Connolly SJ, et al. N Engl J Med
29 29
30 PALLAS Permanent Atrial FibriLLAtion Outcome Study using Dronedarone on Top of Standard Therapy Number: NCT
31 Background In paroxysmal and persistent AF, dronedarone reduced AF recurrence; and reduced the combined outcome of cardiovascular hospitalization or death in ATHENA It also reduced cardiovascular death, stroke and arrhythmic death Dronedarone has other potentially beneficial effects Heart rate slowing in AF BP lowering Anti-adrenergic effects Anti-ventricular arrhythmia effects Hypothesis: dronedarone would reduce major vascular events in permanent AF 31
32 PALLAS Patient Inclusion / Exclusion Inclusion criteria Permanent AF Atrial fibrillation or flutter, present for at least 6 months Age 65 years Major Risk factor (at least one) History of either coronary artery or peripheral arterial disease History of stroke or TIA Heart failure hospitalization in past year, or LVEF 40% Age 75 years, with both hypertension and diabetes mellitus Major exclusion criteria Severe heart failure symptoms (NYHA class IV) or recent unstable NYHA class III Bradycardia < 50 bpm or QTc interval > 500 ms without pacemaker Implantable cardioverter-defibrillator 32

33 PALLAS Design Dronedarone 400 mg BID N=5400 Eligible Patients R Placebo N=5400 Two Co-Primary Outcomes 1. Stroke, myocardial infarction, systemic embolism or cardiovascular death 2. Unplanned cardiovascular hospitalization or death Planned study enrolment of 10,800 patients Two years of recruitment and one final year of follow up 844 first co-primary outcome events 33
34 Baseline Characteristics Dronedarone N=1619 Placebo N=1617 Age years mean (SD) 75.0 (5.9) 75.0 (5.9) Duration of permanent AF > 2 years 1119 (69.1%) 1124 (69.5%) Coronary artery disease 661 (40.8%) 666 (41.2%) Peripheral arterial disease 187 (11.6%) 213 (13.2%) Prior Stroke or TIA 436 (26.9%) 458 (28.3%) History of heart failure 1139 (70.4% ) 1117 (69.1%) Left ventricular ejection fraction 40% 345 (21.3%) 335 (20.7%) Baseline use of a Beta-blocker 1201 (74%) 1201 (74%) Baseline use of Vitamin K antagonist 1359 (84%) 1363 (84%) 34
35 Early Termination of PALLAS First patient enrolled on July 19, 2010 Data monitoring Committee recommended study termination for safety on July 5, ,236 Patients randomized from 489 sites in 37 countries 3.5 months median follow-up 35
36 Cumulative Incidence Stroke, systemic embolism, myocardial infarction or cardiovascular death First Co-primary Outcome Dronedarone Placebo Dronedarone vs placebo HR and 95% CI (2.7%) 19 (1.2%) 2.29 ( ) p= Dronedarone Placebo Number at risk : Days Dronedarone Placebo
37 Cumulative Incidence Unplanned cardiovascular hospitalization or death Second Co-primary Outcome Dronedarone Placebo Dronedarone vs placebo HR and 95% CI Number at risk : (7.8%) 67 (4.1%) 1.95 ( ) p<0.001 Dronedarone Placebo Days Dronedarone Placebo
38 Components of the Primary Outcomes Dronedarone N=1619 Placebo N=1617 HR 95% CI, p-value Death [ ] p=0.049 Cardiovascular Death [ ], p=0.046 Arrhythmic Death [ ], p=0.03 Stroke [ ], p=0.02 Myocardial Infarction [ ], p=0.63 Unplanned CV Hospitalization [ ], p<0.001 Heart Failure Hospitalization [ ], p=
39 Cumulative Incidence Heart Failure Hospitalization Heart Failure Hospitalization Dronedarone Dronedarone Placebo Placebo Dronedarone vs placebo HR and 95% CI 43 (2.7%) 24 (1.5%) 1.81 ( ) p= Number at risk : Days Dronedarone Placebo
40 Sub-groups: First Co-primary Outcome Charateristics N HR [95% CI] Hazard Ration (95% CI) P value b Overall 2.29 [1.34;3.94] Age 0.61 < [0.98;4.15] [1.20;6.12] Duration of perm. AF months to 2 years [0.89;6.03] >2 years [1.18;4.37] Baseline LVEF 0.41 LVEF 40% [1.14;10.50] LVEF>40% [1.06;3.70] NYHA 0.72 No class II/III [0.81;4.97] Class II/III [1.26;4.86] CHADS 0.57 CHADS [1.16;6.57] CHADS > [1.01;4.03] Stroke or TIA history 0.49 N [1.36;4.87] Y [0.60;4.73] Coronary artery disease 0.38 N [1.35;6.22] Y [0.82;3.84] Baseline HR 0.20 HR <65 bpm [1.22;24.26] HR 65 bpm [1.05;3.44] Baseline SBP 0.61 SBP <130 mmhg [0.95;4.33] SBP 130 mmhg [1.19;6.07] Digoxin 0.82 N [1.05;4.41] Y [1.07;5.50] Beta blocking agents 0.41 N [1.10;10.36] Y [1.08;3.73] Vitamin K antagonist or Dabigatran 0.12 N [0.51;3.48] Y [1.57;6.12] Regions 0.93 North America/Western Europe [0.85;6.86] Other regions [1.21;4.27] Dronedarone Better Placebo Better
41 Adverse Events and Laboratory Abnormalities High Level Term (preferred term) Dronedarone N=1614 Placebo N=1609 p-value Any Adverse Event 49.4% 37.3% <0.001 Adverse Event; medication discontinuation 13.1% 5.0% <0.001 Any Serious Adverse Event 7.0% 4.8% Asthenic conditions (asthenia, fatigue) 5.5% 2.9% <0.001 Diarrhea 6.3% 2.4% <0.001 Gastrointestinal or abdominal pain 2.0% 0.9% Nausea and vomiting symptoms (nausea) 4.7% 1.7% <0.001 Breathing abnormalities (dyspnea) 4.6% 2.2% <0.001 Edema (peripheral edema) 3.7% 1.8% <0.001 Neurological signs and symptoms (dizziness) 4.7% 2.4% <0.001 Rate and rhythm disorders (bradycardia) 4.2% 1.2% <0.001 Renal failure and impairment 2.2% 0.7% Alanine aminotransferase >3 times ULN 1.5% 0.4%
42 PALLAS Conclusions In patients with permanent AF and major risk factors for vascular events, dronedarone increased both PALLAS primary outcomes This was due to increases in death, heart failure and stroke There was an increased rate of discontinuation of dronedarone due to adverse events Dronedarone should not be used in this patient population 42
43 There is no single explanation for the increase in stroke, CV death and HF observed in PALLAS The possible hypotheses for the increase in the individual outcomes are: Stroke: The time in therapeutic range in the PALLAS trial was significantly lower on dronedarone compared to placebo, but this effect appears to be too small to explain the large increase of stroke. CV death: The increase is driven by arrhythmic death. This may be due to dronedarone-induced digoxin toxicity. Heart Failure: There is no clear explanation for the increase in HF. Permanent AF patients with greater CV risk may be more sensitive to the potential negative-inotropic effect of dronedarone.


44 The Dronedarone Journey
45 Dronedarone-Where to from here?
46 Antiarrhythmic drug therapy - safety and efficacy comparison based on a mixed treatment analysis* Efficacy (AF recurrence) All-cause mortality Dronedarone n= ( , p=0.0002) Dronedarone 0.85 ( ) p=0.165 Propafenone n= ( , p<0.0001) Amiodarone n= ( , p<0.0001) Amiodarone 2.73 ( ) p=0.049 Sotalol n= ( , p<0.0001) Flecainide n= ( , p<0.0001) Sotalol 4.32 ( ) p= Serious adverse events Proarrhythmic events Dronedarone 0.95 ( ) p=0.699 Dronedarone 1.45 ( ) p=0.043 Propafenone 1.56 ( ) p=0.429 Propafenone 4.06 ( ) p=0.035 Amiodarone 2.41 ( ) p=0.060 Amiodarone 5.45 ( ) p=0.095 Sotalol 1.28 ( ) p=0.338 Sotalol 6.44 ( ) p=0.047 Flecainide 2.02 ( ) p=0.450 Flecainide 6.77 ( ) p= Data are odds ratios and 95% confidence intervals *For each individual antiarrhythmic drug versus placebo Freemantle N, et al. Europace 2011;13: For further study information including safety data, please refer to the full Multaq SmPC
47
48
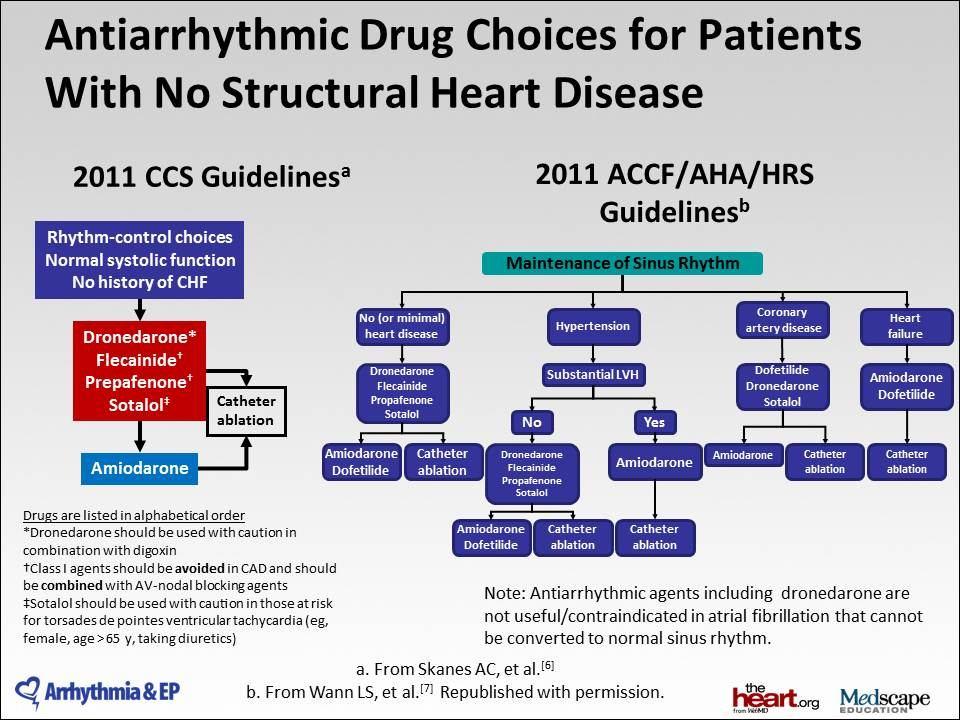
49 LVH American vs European guidelines Canadian guidelines IC and Sotalol
50 Toxicity Hepatic Pulmonary
51 Interactions CYP4503A4 subtrates/inhibitors NOAC Warfarin QT prolonging drugs Digoxin Grapefruit juice CCB BB Statins
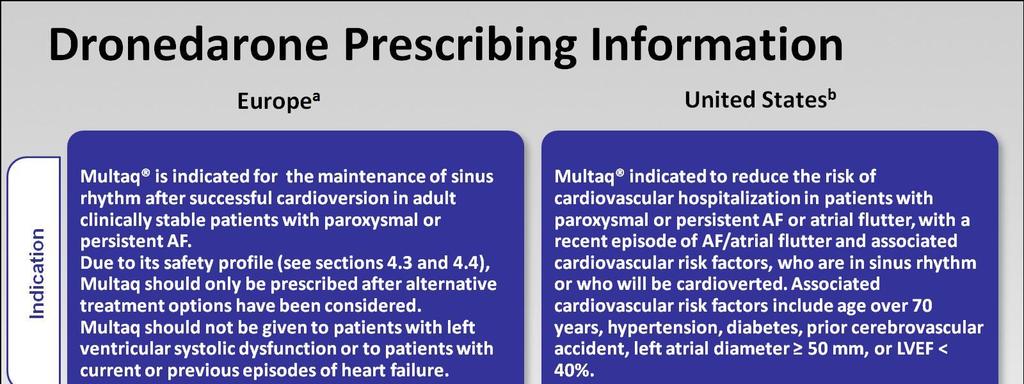
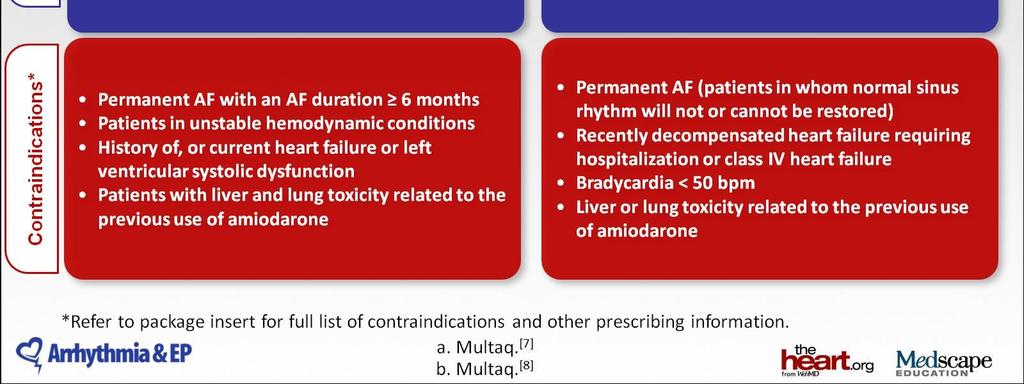
52 Recommendations for Dronedarone Treatment Discontinuation of treatment with dronedarone should be considered in the event of: Recurrence of AF Occurrence of adverse reactions Dronedarone is contraindicated in patients with the following: Permanent AF Unstable haemodynamic conditions History of, or current heart failure or left ventricular systolic dysfunction Liver and lung toxicity related to the previous use of amiodarone Treatment with dronedarone should be stopped during the course of treatment, in case the patient develops any of the conditions which would lead to a contraindication MULTAQ (Dronedarone) SmPC Europe September Refer to full MULTAQ SmPC before prescribing
53 Updated Indication Dronedarone is indicated for the maintenance of sinus rhythm after successful cardioversion in adult clinically stable patients with paroxysmal or persistent atrial fibrillation (AF). Dronedarone should not be given to patients with left ventricular systolic dysfunction or to patients with current or previous episodes of heart failure
54
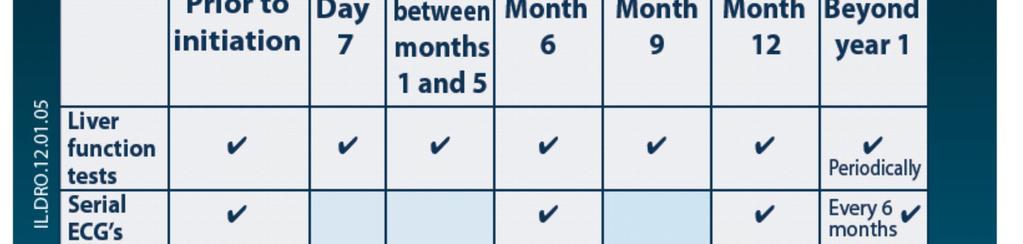
55 Treatment with dronedarone should be initiated and monitored under specialist supervision Patient selection Patient monitoring Paroxysmal or persistent AF (after successful cardioversion) AF status: Serial ECGs and at least every 6 months No CHF, no LVSD No previous liver or lung toxicity with amiodarone Routine clinical assessment with special attention to heart failure and left ventricular systolic dysfunction (LVSD) Baseline LFTs and creatinine, appropriate anti-coagulation LFTs and creatinine at 1 week*, monthly LFTs 1 6 months, 9 and 12 months and regularly thereafter CHF: Congestive heart failure, LVSD: Left ventricular systolic dysfunction, LFTs: Liver function tests *At 2 weeks if there is a rise in accordance with label Adapted from MULTAQ SmPC Europe September Refer to full MULTAQ SmPC for full prescribing information.

56


57 Greek Mythology for Cardiologists I

58 Greek Mythology for Cardiologists II PALLAS ATHENA
59 Thank you
60 Treatment with dronedarone should be initiated and monitored under specialist supervision Patient selection Patient monitoring Paroxysmal or persistent AF (after successful cardioversion) AF status: Serial ECGs and at least every 6 months No CHF, no LVSD No previous liver or lung toxicity with amiodarone Routine clinical assessment with special attention to heart failure and left ventricular systolic dysfunction (LVSD) Baseline LFTs and creatinine, appropriate anti-coagulation LFTs and creatinine at 1 week*, monthly LFTs 1 6 months, 9 and 12 months and regularly thereafter CHF: Congestive heart failure, LVSD: Left ventricular systolic dysfunction, LFTs: Liver function tests *At 2 weeks if there is a rise in accordance with label Adapted from MULTAQ SmPC Europe September Refer to full MULTAQ SmPC for full prescribing information.
61 There are 5 key descriptors of AF patients that impact treatment choice Paroxysmal AF Type Persistent Permanent Degree of symptoms Asymptomatic Mild Moderate Severe Lone AF CHD Co-morbid conditions CHF Other CV co-morbidities HTN, with/without LVH Age < >75 Potential Drug-Drug-Interactions 4 CYP3A4 CYP2D6 P-glycoprotein substrates
62

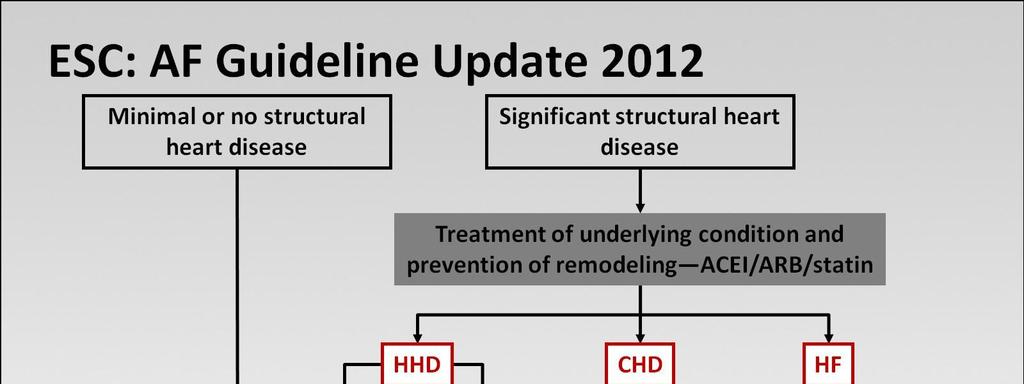
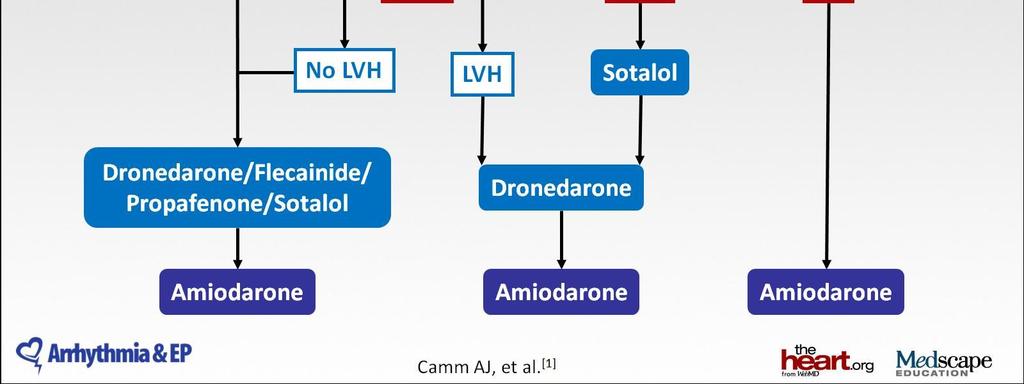
63 2012 focused update of ESC Guidelines for AF Antiarrhythmic drugs and/or left atrial ablation for rhythm control of AF סל: קו CAD I גיידליינס: קו LVH I מושלם: מכבי, כללית, לאומית סל: אחרי ת. לוואי לאמיודרון 2012 focused update of the ESC Guidelines for the management of atrial fibrillation: An update of the 2010 ESC Guidelines for the management of atrial fibrillation * Developed with the special contribution of the European Heart Rhythm Association.Eur Heart J Aug 24.
64 Meta-analysis of cardiovascular outcomes with dronedarone in patients with atrial fibrillation or heart failure. Dronedarone use was associated with a trend toward worse all-cause and cardiovascular mortalities and increased heart failure exacerbations Chatterjee S et al. Am J Cardiol 2012


65 Monitoring
» A new drug s trial
 » A new drug s trial A placebo-controlled, double-blind, parallel arm Trial to assess the efficacy of dronedarone 400 mg bid for the prevention of cardiovascular Hospitalization or death from any cause
» A new drug s trial A placebo-controlled, double-blind, parallel arm Trial to assess the efficacy of dronedarone 400 mg bid for the prevention of cardiovascular Hospitalization or death from any cause
Dronedarone: Need to Perform a CV Outcome Safety Study
 Dronedarone: Need to Perform a CV Outcome Safety Study Gerald V. Naccarelli M.D. Consultant: Glaxo-Smith-Kline, Pfizer, Sanofi, Boehringer-Ingelheim, Daiichi-Sankyo, Bristol Myers Squibb, Otsuka, Janssen
Dronedarone: Need to Perform a CV Outcome Safety Study Gerald V. Naccarelli M.D. Consultant: Glaxo-Smith-Kline, Pfizer, Sanofi, Boehringer-Ingelheim, Daiichi-Sankyo, Bristol Myers Squibb, Otsuka, Janssen
Polypharmacy - arrhythmic risks in patients with heart failure
 Influencing sudden cardiac death by pharmacotherapy Polypharmacy - arrhythmic risks in patients with heart failure Professor Dan Atar Head, Dept. of Cardiology Oslo University Hospital Ullevål Norway 27.8.2012
Influencing sudden cardiac death by pharmacotherapy Polypharmacy - arrhythmic risks in patients with heart failure Professor Dan Atar Head, Dept. of Cardiology Oslo University Hospital Ullevål Norway 27.8.2012
Update on Dronedarone and Cardiovascular Outcomes
 Update on and Cardiovascular Outcomes Dr. Stuart Connolly MD McMaster University Hamilton Ontario Disclosure: Research grants, speaker fees and consulting honoraria from sanofi aventis has key structural
Update on and Cardiovascular Outcomes Dr. Stuart Connolly MD McMaster University Hamilton Ontario Disclosure: Research grants, speaker fees and consulting honoraria from sanofi aventis has key structural
AF#in#pa(ents#with#CAD# Is#dronedarone#a#good#choice?!
 AF#in#pa(ents#with#CAD# Is#dronedarone#a#good#choice?! DRUG#PROPHYLAXIS#OF#AF:# FOCUS#ON#DRONEDARONE# Friday#16C10C2015# Harry%JGM%Crijns% Maastricht,%The%Netherlands% Disclosures Harry Crijns - research
AF#in#pa(ents#with#CAD# Is#dronedarone#a#good#choice?! DRUG#PROPHYLAXIS#OF#AF:# FOCUS#ON#DRONEDARONE# Friday#16C10C2015# Harry%JGM%Crijns% Maastricht,%The%Netherlands% Disclosures Harry Crijns - research
ATHENA - A placebo-controlled, double-blind, parallel arm Trial to assess the efficacy of dronedarone 400 mg bid for the prevention of cardiovascular
 1 ATHENA - A placebo-controlled, double-blind, parallel arm Trial to assess the efficacy of dronedarone 400 mg bid for the prevention of cardiovascular Hospitalization or death from any cause in patients
1 ATHENA - A placebo-controlled, double-blind, parallel arm Trial to assess the efficacy of dronedarone 400 mg bid for the prevention of cardiovascular Hospitalization or death from any cause in patients
PALLAS. Dronedarone on Top of Standard Therapy. Stuart J. Connolly MD. on behalf of the PALLAS investigators
 PALLAS Permanent Atrial FibriLLAtion Outcome Study using on Top of Standard Therapy Stuart J. Connolly MD on behalf of the PALLAS investigators http://clinicaltrials.gov Number: NCT01151137 1 Disclosure
PALLAS Permanent Atrial FibriLLAtion Outcome Study using on Top of Standard Therapy Stuart J. Connolly MD on behalf of the PALLAS investigators http://clinicaltrials.gov Number: NCT01151137 1 Disclosure
Dronedarone for the treatment of non-permanent atrial fibrillation
 Dronedarone for the treatment of non-permanent atrial Issued: August 2010 last modified: December 2012 guidance.nice.org.uk/ta197 NICE has accredited the process used by the Centre for Health Technology
Dronedarone for the treatment of non-permanent atrial Issued: August 2010 last modified: December 2012 guidance.nice.org.uk/ta197 NICE has accredited the process used by the Centre for Health Technology
dronedarone, 400mg, film-coated tablets (Multaq ) SMC No. (636/10) Sanofi-aventis Ltd
 SMC No. (636/10) Sanofi-aventis Ltd") dronedarone, 400mg, film-coated tablets (Multaq ) SMC No. (636/10) Sanofi-aventis Ltd 6 August 2010 The Scottish Medicines Consortium (SMC) has completed its assessment of the above product and advises
dronedarone, 400mg, film-coated tablets (Multaq ) SMC No. (636/10) Sanofi-aventis Ltd 6 August 2010 The Scottish Medicines Consortium (SMC) has completed its assessment of the above product and advises
National Horizon Scanning Centre. Dronedarone (Multaq) for atrial fibrillation and atrial flutter. December 2007
 for atrial fibrillation and atrial flutter. December 2007") Dronedarone (Multaq) for atrial fibrillation and atrial flutter December 2007 This technology summary is based on information available at the time of research and a limited literature search. It is not
Dronedarone (Multaq) for atrial fibrillation and atrial flutter December 2007 This technology summary is based on information available at the time of research and a limited literature search. It is not
PRESCRIBING ALERT
 www.empr.com PRESCRIBING ALERT Dear Healthcare Professional, At MPR we strive to bring you important drug information in a concise and timely fashion. In keeping with this goal, we are pleased to bring
www.empr.com PRESCRIBING ALERT Dear Healthcare Professional, At MPR we strive to bring you important drug information in a concise and timely fashion. In keeping with this goal, we are pleased to bring
Dronedarone For Atrial Fibrillation: Unbridled Enthusiasm Or Just Another Small Step Forward?
 Dronedarone For Atrial Fibrillation: Unbridled Enthusiasm Or Just Another Small Step Forward? James A. Reiffel, M.D. Introduction In July 2009, the federal Food and Drug Administration (FDA) approved the
Dronedarone For Atrial Fibrillation: Unbridled Enthusiasm Or Just Another Small Step Forward? James A. Reiffel, M.D. Introduction In July 2009, the federal Food and Drug Administration (FDA) approved the
Atrial Fibrillation 2009
 Atrial Fibrillation 2009 Michael Glikson, MD Director of Pacing & Electrophysiology Leviev Heart Center Sheba medical Center Sheba Medical Center Tel Hashomer The Leviev Heart Center Rhythm vs rate control
Atrial Fibrillation 2009 Michael Glikson, MD Director of Pacing & Electrophysiology Leviev Heart Center Sheba medical Center Sheba Medical Center Tel Hashomer The Leviev Heart Center Rhythm vs rate control
Geriatric Grand Rounds
 Geriatric Grand Rounds Tuesday, April 13, 21 12: noon Dr. Bill Black Auditorium Glenrose Rehabilitation Hospital In keeping with Glenrose Rehabilitation Hospital policy, speakers participating in this
Geriatric Grand Rounds Tuesday, April 13, 21 12: noon Dr. Bill Black Auditorium Glenrose Rehabilitation Hospital In keeping with Glenrose Rehabilitation Hospital policy, speakers participating in this
Debate PRO. Dronedarone is an important drug in the management of paroxysmal atrial fibrillation. John Camm
 ESC ICM - Internationales Congress Center München 2012 Atrial Fibrillation Controversies in Medical Treatment Debate Dronedarone is an important drug in the management of paroxysmal atrial fibrillation
ESC ICM - Internationales Congress Center München 2012 Atrial Fibrillation Controversies in Medical Treatment Debate Dronedarone is an important drug in the management of paroxysmal atrial fibrillation
Treatment of Atrial Fibrillation in Heart Failure
 Stockholm, September 1st 2010 Treatment of Atrial Fibrillation in Heart Failure Rhythm control: Which drugs? Stefan H. Hohnloser J.W. Goethe University Frankfurt, Germany Presenter disclosure information:
Stockholm, September 1st 2010 Treatment of Atrial Fibrillation in Heart Failure Rhythm control: Which drugs? Stefan H. Hohnloser J.W. Goethe University Frankfurt, Germany Presenter disclosure information:
Dronedarone( What%is%the%future?!
 Dronedarone( What%is%the%future?! DRUG(PROPHYLAXIS(OF(AF:( FOCUS(ON(DRONEDARONE( Friday(16>10>2015( Harry%JGM%Crijns% Maastricht,%The%Netherlands% Disclosures Harry Crijns - research grants, consulting
Dronedarone( What%is%the%future?! DRUG(PROPHYLAXIS(OF(AF:( FOCUS(ON(DRONEDARONE( Friday(16>10>2015( Harry%JGM%Crijns% Maastricht,%The%Netherlands% Disclosures Harry Crijns - research grants, consulting
Saudi Heart Association February 22, 2011
 Pharmacological Therapy of Atrial Fibrillation: Recent Advances Dr Martin Green Professor of Medicine (Cardiology) University of Ottawa Saudi Heart Association February 22, 2011 Atrial Fibrillation Drugs
Pharmacological Therapy of Atrial Fibrillation: Recent Advances Dr Martin Green Professor of Medicine (Cardiology) University of Ottawa Saudi Heart Association February 22, 2011 Atrial Fibrillation Drugs
Samer Nasr, M.D. Mount Lebanon Hospital.
 Samer Nasr, M.D. Mount Lebanon Hospital. Lone atrial fibrillation: Younger than 60 years old. No clinical or echo evidence of cardiopulmonary disease. Favorable prognosis. Thromboembolism usually not
Samer Nasr, M.D. Mount Lebanon Hospital. Lone atrial fibrillation: Younger than 60 years old. No clinical or echo evidence of cardiopulmonary disease. Favorable prognosis. Thromboembolism usually not
Basics of Atrial Fibrillation. By Mini Thannikal NP-BC Mount Sinai St Luke s Hospital New York, NY
 Basics of Atrial Fibrillation By Mini Thannikal NP-BC Mount Sinai St Luke s Hospital New York, NY Atrial Fibrillation(AF) is a supraventricular tachyarrhythmia characterized by uncoordinated atrial activation
Basics of Atrial Fibrillation By Mini Thannikal NP-BC Mount Sinai St Luke s Hospital New York, NY Atrial Fibrillation(AF) is a supraventricular tachyarrhythmia characterized by uncoordinated atrial activation
Dronedarone: Where Does it Fit in the AF Therapeutic Armamentarium?
 Dronedarone: Where Does it Fit in the AF Therapeutic Armamentarium? Abstract James A. Reiffel, M.D. Department of Medicine, Division of Cardiology, Columbia University Medical Center Dronedarone is a derivative
Dronedarone: Where Does it Fit in the AF Therapeutic Armamentarium? Abstract James A. Reiffel, M.D. Department of Medicine, Division of Cardiology, Columbia University Medical Center Dronedarone is a derivative
What s New in the AF Guidelines
 Impact on New AF Guidelines on Heart Failure Management Gothenburg - May 22 nd 2011 Europace (2010) 12, 1360-420 http://europace.oxfordjournals.org JACC (2011) 57, 223-42 http://www.cardiosource.org What
Impact on New AF Guidelines on Heart Failure Management Gothenburg - May 22 nd 2011 Europace (2010) 12, 1360-420 http://europace.oxfordjournals.org JACC (2011) 57, 223-42 http://www.cardiosource.org What
Rate or Rhythm Control? Epidemiology. Relevant Advances in Atrial Fibrillation 6/20/2011. Stroke Prophylaxis
 Relevant Advances in Atrial Fibrillation Stroke Prophylaxis Managing Atrial Fibrillation: Tips for the Generalist Antiarrhythmic Drug Therapy Ablation Gregory M Marcus, MD, MAS Assistant Professor of Medicine
Relevant Advances in Atrial Fibrillation Stroke Prophylaxis Managing Atrial Fibrillation: Tips for the Generalist Antiarrhythmic Drug Therapy Ablation Gregory M Marcus, MD, MAS Assistant Professor of Medicine
Use of Antiarrhythmic Drugs for AF Who, What and How? Dr. Marc Cheng Queen Elizabeth Hospital
 Use of Antiarrhythmic Drugs for AF Who, What and How? Dr. Marc Cheng Queen Elizabeth Hospital Content i. Rhythm versus Rate control ii. Anti-arrhythmic for Rhythm Control iii. Anti-arrhythmic for Rate
Use of Antiarrhythmic Drugs for AF Who, What and How? Dr. Marc Cheng Queen Elizabeth Hospital Content i. Rhythm versus Rate control ii. Anti-arrhythmic for Rhythm Control iii. Anti-arrhythmic for Rate
The pill-in-the-pocket strategy for paroxysmal atrial fibrillation
 The pill-in-the-pocket strategy for paroxysmal atrial fibrillation KONSTANTINOS P. LETSAS, MD, FEHRA LABORATORY OF CARDIAC ELECTROPHYSIOLOGY EVANGELISMOS GENERAL HOSPITAL OF ATHENS ARRHYTHMIAS UPDATE,
The pill-in-the-pocket strategy for paroxysmal atrial fibrillation KONSTANTINOS P. LETSAS, MD, FEHRA LABORATORY OF CARDIAC ELECTROPHYSIOLOGY EVANGELISMOS GENERAL HOSPITAL OF ATHENS ARRHYTHMIAS UPDATE,
Treatment strategy decision tree
 strategy decision tree strategy decision tree Confirmed diagnosis of AF Further investigations and clinical assessment including risk stratification for stroke/thromboembolism Paroxysmal AF Persistent
strategy decision tree strategy decision tree Confirmed diagnosis of AF Further investigations and clinical assessment including risk stratification for stroke/thromboembolism Paroxysmal AF Persistent
Safety and Efficacy of Dronedarone in the Treatment of Atrial Fibrillation/Flutter
 Clinical Medicine Insights: Cardiology Expert Review Open Access Full open access to this and thousands of other papers at http://www.la-press.com. Safety and Efficacy of Dronedarone in the Treatment of
Clinical Medicine Insights: Cardiology Expert Review Open Access Full open access to this and thousands of other papers at http://www.la-press.com. Safety and Efficacy of Dronedarone in the Treatment of
Cost and Prevalence of A fib. Atrial Fibrillation: Guideline Directed Treatment. Prevalence of A Fib. Risk Factors for A Fib. Risk Factors for A Fib
 Atrial Fibrillation: Guideline Directed Treatment Melissa Wendell, FNP-C, MSN Heart Failure - Lead Nurse Practitioner, Aspirus Wausau Hospital and Aspirus Cardiology Cost and Prevalence of A fib 33.5 million
Atrial Fibrillation: Guideline Directed Treatment Melissa Wendell, FNP-C, MSN Heart Failure - Lead Nurse Practitioner, Aspirus Wausau Hospital and Aspirus Cardiology Cost and Prevalence of A fib 33.5 million
Stuart Beldner, MD, FHRS Assistant Professor NSLIJ Hofstra School of Med
 Stuart Beldner, MD, FHRS Assistant Professor NSLIJ Hofstra School of Med None There s no reason to panic. While it is true that one of the crew members is ill, slightly. Absence of discrete P waves Chaotic
Stuart Beldner, MD, FHRS Assistant Professor NSLIJ Hofstra School of Med None There s no reason to panic. While it is true that one of the crew members is ill, slightly. Absence of discrete P waves Chaotic
AF and arrhythmia management. Dr Rhys Beynon Consultant Cardiologist and Electrophysiologist University Hospital of North Staffordshire
 AF and arrhythmia management Dr Rhys Beynon Consultant Cardiologist and Electrophysiologist University Hospital of North Staffordshire Atrial fibrillation Paroxysmal AF recurrent AF (>2 episodes) that
AF and arrhythmia management Dr Rhys Beynon Consultant Cardiologist and Electrophysiologist University Hospital of North Staffordshire Atrial fibrillation Paroxysmal AF recurrent AF (>2 episodes) that
Update in the Management of Atrial Fibrillation
 Update in the Management of Atrial Fibrillation Gregory M Marcus, MD, MAS Associate Professor of Medicine Division of Cardiology University of California, San Francisco Disclosures Research: Gilead, Medtronic,
Update in the Management of Atrial Fibrillation Gregory M Marcus, MD, MAS Associate Professor of Medicine Division of Cardiology University of California, San Francisco Disclosures Research: Gilead, Medtronic,
EFFECTIVE SHARED CARE AGREEMENT. Dronedarone - For the treatment and management of atrial fibrillation
 EFFECTIVE SHARED CARE AGREEMENT Dronedarone - For the treatment and management of atrial fibrillation Specialist details Patient identifier Name INTRODUCTION This shared care agreement outlines how the
EFFECTIVE SHARED CARE AGREEMENT Dronedarone - For the treatment and management of atrial fibrillation Specialist details Patient identifier Name INTRODUCTION This shared care agreement outlines how the
Rate and Rhythm Control of Atrial Fibrillation
 Rate and Rhythm Control of Atrial Fibrillation April 21, 2017 춘계심혈관통합학술대회 Jaemin Shim, MD, PhD Arrhythmia Center Korea University Anam Hospital Treatment of AF Goal Reducing symptoms Preventing complication
Rate and Rhythm Control of Atrial Fibrillation April 21, 2017 춘계심혈관통합학술대회 Jaemin Shim, MD, PhD Arrhythmia Center Korea University Anam Hospital Treatment of AF Goal Reducing symptoms Preventing complication
NHS Kent and Medway Medicines Management. Dronedarone (Multaq ) Shared Care Guideline For Prescribing
 Shared Care Guideline For Prescribing") NHS Kent and Medway Medicines Management Dronedarone (Multaq ) Shared Care Guideline For Prescribing Issue No: 2 Review Date (If Applicable): Accountable Officer: Heather Lucas Contact Details: 01233 618158
NHS Kent and Medway Medicines Management Dronedarone (Multaq ) Shared Care Guideline For Prescribing Issue No: 2 Review Date (If Applicable): Accountable Officer: Heather Lucas Contact Details: 01233 618158
Current Guideline for AF Treatment. Young Keun On, MD, PhD, FHRS Samsung Medical Center Sungkyunkwan University School of Medicine
 Current Guideline for AF Treatment Young Keun On, MD, PhD, FHRS Samsung Medical Center Sungkyunkwan University School of Medicine Case 1 59 year-old lady Sudden palpitation and breathlessness for 12 hours
Current Guideline for AF Treatment Young Keun On, MD, PhD, FHRS Samsung Medical Center Sungkyunkwan University School of Medicine Case 1 59 year-old lady Sudden palpitation and breathlessness for 12 hours
Amiodarone Prescribing and Monitoring: Back to the Future
 Amiodarone Prescribing and Monitoring: Back to the Future Subha L. Varahan, MD, FHRS, CCDS Electrophysiologist Oklahoma Heart Hospital Oklahoma City, OK Friday, February, 8 th, 2019 Iodinated benzofuran
Amiodarone Prescribing and Monitoring: Back to the Future Subha L. Varahan, MD, FHRS, CCDS Electrophysiologist Oklahoma Heart Hospital Oklahoma City, OK Friday, February, 8 th, 2019 Iodinated benzofuran
Management of ATRIAL FIBRILLATION. in general practice. 22 BPJ Issue 39
 Management of ATRIAL FIBRILLATION in general practice 22 BPJ Issue 39 What is atrial fibrillation? Atrial fibrillation (AF) is the most common cardiac arrhythmia encountered in primary care. It is often
Management of ATRIAL FIBRILLATION in general practice 22 BPJ Issue 39 What is atrial fibrillation? Atrial fibrillation (AF) is the most common cardiac arrhythmia encountered in primary care. It is often
Who Gets Atrial Fibrilla9on..?
 Birmingham October 20 th 2013 AFA Pa9ents Day Symptoma9c Atrial Fibrilla9on What therapies are available? GENERAL BACKGROUND Andrew Grace Papworth Hospital and University of Cambridge Consultant: Medtronic
Birmingham October 20 th 2013 AFA Pa9ents Day Symptoma9c Atrial Fibrilla9on What therapies are available? GENERAL BACKGROUND Andrew Grace Papworth Hospital and University of Cambridge Consultant: Medtronic
AF Today: W. For the majority of patients with atrial. are the Options? Chris Case
 AF Today: W hat are the Options? Management strategies for patients with atrial fibrillation should depend on the individual patient. Treatment with medications seems adequate for most patients with atrial
AF Today: W hat are the Options? Management strategies for patients with atrial fibrillation should depend on the individual patient. Treatment with medications seems adequate for most patients with atrial
Supplementary Online Content
 Supplementary Online Content Morillo CA, Verma A, Connolly SJ, et al. Radiofrequency ablation vs antiarrhythmic drugs as first-line Treatment of Paroxysmal Atrial Fibrillation (RAAFT-2): a randomzied clinical
Supplementary Online Content Morillo CA, Verma A, Connolly SJ, et al. Radiofrequency ablation vs antiarrhythmic drugs as first-line Treatment of Paroxysmal Atrial Fibrillation (RAAFT-2): a randomzied clinical
ATRIAL FIBRILLATION: REVISITING CONTROVERSIES IN AN ERA OF INNOVATION
 ATRIAL FIBRILLATION: REVISITING CONTROVERSIES IN AN ERA OF INNOVATION Frederick Schaller, DO, MACOI,FACP Adjunct Clinical Professor Touro University Nevada DISCLOSURES I have no financial relationships
ATRIAL FIBRILLATION: REVISITING CONTROVERSIES IN AN ERA OF INNOVATION Frederick Schaller, DO, MACOI,FACP Adjunct Clinical Professor Touro University Nevada DISCLOSURES I have no financial relationships
Atrial fibrillation and advanced age
 Atrial fibrillation and advanced age Prof. Fiorenzo Gaita Director of the Cardiology School University of Turin, Italy Prevalence of AF in the general population Prevalence and age distribution in patients
Atrial fibrillation and advanced age Prof. Fiorenzo Gaita Director of the Cardiology School University of Turin, Italy Prevalence of AF in the general population Prevalence and age distribution in patients
ESC Stockholm Arrhythmias & pacing
 ESC Stockholm 2010 Take Home Messages for Practitioners Arrhythmias & pacing Prof. Panos E. Vardas Professor of Cardiology Heraklion University Hospital Crete, Greece Disclosures Small teaching fees from
ESC Stockholm 2010 Take Home Messages for Practitioners Arrhythmias & pacing Prof. Panos E. Vardas Professor of Cardiology Heraklion University Hospital Crete, Greece Disclosures Small teaching fees from
Are Drugs Better? Dr Mauro Lencioni. Drugs or ablation as first line treatment for AF? Consultant Cardiologist & Electrophysiologist
 Are Drugs Better? Drugs or ablation as first line treatment for AF? Dr Mauro Lencioni Consultant Cardiologist & Electrophysiologist The Philosophical Issue What do we mean by Better? Outcome measures Measurement
Are Drugs Better? Drugs or ablation as first line treatment for AF? Dr Mauro Lencioni Consultant Cardiologist & Electrophysiologist The Philosophical Issue What do we mean by Better? Outcome measures Measurement
5/5/2010. World incidence 720, 000 new cases / year. World prevalence 5.55 million AF prevalence increasing with aging of population
 Atrial Fibrillation: Guidelines through clinical cases and 2010 updates Samy Claude ELAYI Cardiac Clinical Pacing and Electrophysiology UK World incidence 720, 000 new cases / year World prevalence 5.55
Atrial Fibrillation: Guidelines through clinical cases and 2010 updates Samy Claude ELAYI Cardiac Clinical Pacing and Electrophysiology UK World incidence 720, 000 new cases / year World prevalence 5.55
Primary Care Update in Medicine January 31 February 1, 2013 New Management Options for Patients with Atrial Fibrillation
 Primary Care Update in Medicine January 31 February 1, 2013 New Management Options for Patients with Atrial Fibrillation Anne B. Curtis, MD, FACC, FHRS, FACP, FAHA Charles and Mary Bauer Professor, Chair,
Primary Care Update in Medicine January 31 February 1, 2013 New Management Options for Patients with Atrial Fibrillation Anne B. Curtis, MD, FACC, FHRS, FACP, FAHA Charles and Mary Bauer Professor, Chair,
DECLARATION OF CONFLICT OF INTEREST. Consultant Sanofi Biosense Webster Honorarium Boehringer Ingelheim St Jude Medical
 DECLARATION OF CONFLICT OF INTEREST Consultant Sanofi Biosense Webster Honorarium Boehringer Ingelheim St Jude Medical ESC Congress Paris, France August 27-31, 2011 Risk & Complications of AADs for Rhythm
DECLARATION OF CONFLICT OF INTEREST Consultant Sanofi Biosense Webster Honorarium Boehringer Ingelheim St Jude Medical ESC Congress Paris, France August 27-31, 2011 Risk & Complications of AADs for Rhythm
Rhythm Control: Is There a Role for the PCP? Blake Norris, MD, FACC BHHI Primary Care Symposium February 28, 2014
 Rhythm Control: Is There a Role for the PCP? Blake Norris, MD, FACC BHHI Primary Care Symposium February 28, 2014 Financial disclosures Consultant Medtronic 3 reasons to evaluate and treat arrhythmias
Rhythm Control: Is There a Role for the PCP? Blake Norris, MD, FACC BHHI Primary Care Symposium February 28, 2014 Financial disclosures Consultant Medtronic 3 reasons to evaluate and treat arrhythmias
Relevant Advances in Atrial Fibrillation
 Gregory M Marcus, MD, MAS Assistant Professor of Medicine Division of Cardiology University of California, San Francisco Relevant Advances in Atrial Fibrillation Stroke Prophylaxis Antiarrhythmic Drug
Gregory M Marcus, MD, MAS Assistant Professor of Medicine Division of Cardiology University of California, San Francisco Relevant Advances in Atrial Fibrillation Stroke Prophylaxis Antiarrhythmic Drug
Understanding Atrial Fibrillation Management. Roy Lin, MD
 Understanding Atrial Fibrillation Management Roy Lin, MD Disclosure None Definition of atrial fibrillation Atrial fibrillation is a supraventricular tachyarrhythmia characterized by uncoordinated atrial
Understanding Atrial Fibrillation Management Roy Lin, MD Disclosure None Definition of atrial fibrillation Atrial fibrillation is a supraventricular tachyarrhythmia characterized by uncoordinated atrial
Medical management of AF: drugs for rate and rhythm control
 Medical management of AF: drugs for rate and rhythm control Adel Khalifa Sultan Hamad, BMS, MD, FGHRS, FRCP(Canada) Consultant Cardiologist & Interventional Cardiac Electrophysiologist Head of Electrophysiology
Medical management of AF: drugs for rate and rhythm control Adel Khalifa Sultan Hamad, BMS, MD, FGHRS, FRCP(Canada) Consultant Cardiologist & Interventional Cardiac Electrophysiologist Head of Electrophysiology
AF in the ER: Common Scenarios CASE 1. Fast facts. Diagnosis. Management
 AF in the ER: Common Scenarios Atrial fibrillation is a common problem with a wide spectrum of presentations. Below are five common emergency room scenarios and the management strategies for each. Evan
AF in the ER: Common Scenarios Atrial fibrillation is a common problem with a wide spectrum of presentations. Below are five common emergency room scenarios and the management strategies for each. Evan
The RealiseAF registry:
 The RealiseAF registry: An International, observational, cross-sectional survey evaluating atrial fibrillation management and the cardiovascular risk profile of AF patients initial results PG.Steg on behalf
The RealiseAF registry: An International, observational, cross-sectional survey evaluating atrial fibrillation management and the cardiovascular risk profile of AF patients initial results PG.Steg on behalf
Out with the old, in with The 2010 Atrial Fibrillation Guidelines
 Out with the old, in with The 2010 Atrial Fibrillation Guidelines Kseniya Chernushkin B.Sc.(Pharm.), VCH/PHC Pharmacy Resident Mary Elliot B.Sc.(Pharm.), VCH/PHC Pharmacy Resident March 22, 2011 Outline
Out with the old, in with The 2010 Atrial Fibrillation Guidelines Kseniya Chernushkin B.Sc.(Pharm.), VCH/PHC Pharmacy Resident Mary Elliot B.Sc.(Pharm.), VCH/PHC Pharmacy Resident March 22, 2011 Outline
Dronedarone in patients with congestive heart failure: insights from ATHENA
 European Heart Journal (2010) 31, 1717 1721 doi:10.1093/eurheartj/ehq113 CLINICAL RESEARCH Heart failure/cardiomyopathy Dronedarone in patients with congestive heart failure: insights from ATHENA Stefan
European Heart Journal (2010) 31, 1717 1721 doi:10.1093/eurheartj/ehq113 CLINICAL RESEARCH Heart failure/cardiomyopathy Dronedarone in patients with congestive heart failure: insights from ATHENA Stefan
Half Moon Bay Treatment of Atrial Fibrillation. Dr. Roger A. Winkle MD. Silicon Valley Cardiology, PAMF, Sutter Health Sequoia Hospital
 Half Moon Bay 2018 Treatment of Atrial Fibrillation Dr. Roger A. Winkle MD Silicon Valley Cardiology, PAMF, Sutter Health Sequoia Hospital Disclosures: Investor Farapulse Things a Primary Care Doctor Should
Half Moon Bay 2018 Treatment of Atrial Fibrillation Dr. Roger A. Winkle MD Silicon Valley Cardiology, PAMF, Sutter Health Sequoia Hospital Disclosures: Investor Farapulse Things a Primary Care Doctor Should
Arrhythmias and Heart Failure Dr Chris Lang Consultant Cardiologist and Electrophysiologist Royal Infirmary of Edinburgh
 Arrhythmias and Heart Failure Dr Chris Lang Consultant Cardiologist and Electrophysiologist Royal Infirmary of Edinburgh Arrhythmias and Heart Failure Ventricular Supraventricular VT/VF Primary prevention
Arrhythmias and Heart Failure Dr Chris Lang Consultant Cardiologist and Electrophysiologist Royal Infirmary of Edinburgh Arrhythmias and Heart Failure Ventricular Supraventricular VT/VF Primary prevention
Atrial Fibrillation: Guidelines through clinical cases and 2010 updates
 Atrial Fibrillation: Guidelines through clinical cases and 2010 updates Samy Claude ELAYI Cardiac Clinical Pacing and Electrophysiology World incidence 720, 000 new cases / year World prevalence 5.5 million
Atrial Fibrillation: Guidelines through clinical cases and 2010 updates Samy Claude ELAYI Cardiac Clinical Pacing and Electrophysiology World incidence 720, 000 new cases / year World prevalence 5.5 million
Role of Dronedarone in Atrial Fibrillation: More Questions Than Answers
 Role of Dronedarone in Atrial Fibrillation: More Questions Than Answers Daniel E. Hilleman, Pharm.D., FCCP, and Aryan N. Mooss, M.D. Key Words: dronedarone, atrial fibrillation, sinus rhythm, hypertension,
Role of Dronedarone in Atrial Fibrillation: More Questions Than Answers Daniel E. Hilleman, Pharm.D., FCCP, and Aryan N. Mooss, M.D. Key Words: dronedarone, atrial fibrillation, sinus rhythm, hypertension,
Clinical Investigations
 Clinical Investigations Effects of Dronedarone Started Rapidly After Amiodarone Discontinuation Address for correspondence: Laura Immordino, MD 100 E. Lancaster Avenue Wynnewood, PA 19096 laura.immordino@gmail.com
Clinical Investigations Effects of Dronedarone Started Rapidly After Amiodarone Discontinuation Address for correspondence: Laura Immordino, MD 100 E. Lancaster Avenue Wynnewood, PA 19096 laura.immordino@gmail.com
Reviews. Benefit-Risk Assessment of Current Antiarrhythmic Drug Therapy of Atrial Fibrillation
 Reviews Benefit-Risk Assessment of Current Antiarrhythmic Drug Therapy of Atrial Fibrillation Address for correspondence: Stefan H. Hohnloser, MD Department of Cardiology J.W. Goethe University Hospital
Reviews Benefit-Risk Assessment of Current Antiarrhythmic Drug Therapy of Atrial Fibrillation Address for correspondence: Stefan H. Hohnloser, MD Department of Cardiology J.W. Goethe University Hospital
Management of atrial fibrillation in heart failure
 Nationale hartfalendag 2017 Zeist Management of atrial fibrillation in heart failure Isabelle C Van Gelder University of Groningen University Medical Center Groningen The Netherlands Disclosures Grant
Nationale hartfalendag 2017 Zeist Management of atrial fibrillation in heart failure Isabelle C Van Gelder University of Groningen University Medical Center Groningen The Netherlands Disclosures Grant
Rome Cardiology Forum
 Rome Cardiology Forum Update on Atrial Fibrillation Rome, January 29 th -31 st 214 Pharmacological Prevention of Atrial Fibrillation John Camm St. George s University of London, UK Conflicts of Interest:
Rome Cardiology Forum Update on Atrial Fibrillation Rome, January 29 th -31 st 214 Pharmacological Prevention of Atrial Fibrillation John Camm St. George s University of London, UK Conflicts of Interest:
Antiarrhythmic agents in 2014
 7 AP-HRS Scientific Session, New Dehli, India - Oct 29 to Nov 1, 2014 Antiarrhythmic agents in 2014 Antonio Raviele, MD, FESC, FHRS President ALFA Alliance to Fight Atrial fibrillation - Venice, Italy
7 AP-HRS Scientific Session, New Dehli, India - Oct 29 to Nov 1, 2014 Antiarrhythmic agents in 2014 Antonio Raviele, MD, FESC, FHRS President ALFA Alliance to Fight Atrial fibrillation - Venice, Italy
Practical Rate and Rhythm Management of Atrial Fibrillation
 Practical Rate and Rhythm Management of Atrial Fibrillation pocket guide UPDATED FEBRUARY 2013 Adapted from the ACCF/AHA/HRS 2011 Focused Updates Incorporated into the ACC/AHA/ESC Guidelines for the Management
Practical Rate and Rhythm Management of Atrial Fibrillation pocket guide UPDATED FEBRUARY 2013 Adapted from the ACCF/AHA/HRS 2011 Focused Updates Incorporated into the ACC/AHA/ESC Guidelines for the Management
Transient Atrial Fibrillation and Risk of Stroke after Acute Myocardial Infarction
 Transient Atrial Fibrillation and Risk of Stroke after Acute Myocardial Infarction Doron Aronson MD, Gregory Telman MD, Fadel BahouthMD, Jonathan Lessick MD, DSc and Rema Bishara MD Department of Cardiology
Transient Atrial Fibrillation and Risk of Stroke after Acute Myocardial Infarction Doron Aronson MD, Gregory Telman MD, Fadel BahouthMD, Jonathan Lessick MD, DSc and Rema Bishara MD Department of Cardiology
ABLATION OF CHRONIC AF
 ABLATION OF CHRONIC AF A PISAPIA ST JOSEPH HOSPITAL MARSEILLE MEET 2008 Atrial Fibrillation The most common significant heart rhythm disturbance Incidence increases with age and the development of structural
ABLATION OF CHRONIC AF A PISAPIA ST JOSEPH HOSPITAL MARSEILLE MEET 2008 Atrial Fibrillation The most common significant heart rhythm disturbance Incidence increases with age and the development of structural
Rebuttal. Jerónimo Farré MD 2010
 Rebuttal 1.We do not know what are the types of AF in which ablation is worthless or most effective 2.Waiting implies to consider the ablation at an older age and when the duration of the history of AF
Rebuttal 1.We do not know what are the types of AF in which ablation is worthless or most effective 2.Waiting implies to consider the ablation at an older age and when the duration of the history of AF
Conflict of interest statement
 Risk of stroke, systemic embolism or death according to heart failure and left ventricular function status in patients with atrial fibrillation: results of the ARISTOTLE trial J.J.V. McMurray 1, B. Lewis
Risk of stroke, systemic embolism or death according to heart failure and left ventricular function status in patients with atrial fibrillation: results of the ARISTOTLE trial J.J.V. McMurray 1, B. Lewis
Dysrhythmias 11/7/2017. Disclosures. 3 reasons to evaluate and treat dysrhythmias. None. Eliminate symptoms and improve hemodynamics
 Dysrhythmias CYDNEY STEWART MD, FACC NOVEMBER 3, 2017 Disclosures None 3 reasons to evaluate and treat dysrhythmias Eliminate symptoms and improve hemodynamics Prevent imminent death/hemodynamic compromise
Dysrhythmias CYDNEY STEWART MD, FACC NOVEMBER 3, 2017 Disclosures None 3 reasons to evaluate and treat dysrhythmias Eliminate symptoms and improve hemodynamics Prevent imminent death/hemodynamic compromise
Atrial Fibrillation and the NOAC s. John Raymond MS, PA-C, MHP February 10, 2018
 Atrial Fibrillation and the NOAC s John Raymond MS, PA-C, MHP February 10, 2018 Pathogenesis EPIDEMIOLOGY Arrhythmia-related hospitalisations in the US Ventricular fibrillation 2% Atrial fibrillation 34%
Atrial Fibrillation and the NOAC s John Raymond MS, PA-C, MHP February 10, 2018 Pathogenesis EPIDEMIOLOGY Arrhythmia-related hospitalisations in the US Ventricular fibrillation 2% Atrial fibrillation 34%
Subclinical AF: Implications of device based episodes
 Subclinical AF: Implications of device based episodes Michael R Gold, MD, PhD Medical University of South Carolina Charleston, SC Disclosures: Clinical Trials and Consulting: Medtronic, Boston Scientific
Subclinical AF: Implications of device based episodes Michael R Gold, MD, PhD Medical University of South Carolina Charleston, SC Disclosures: Clinical Trials and Consulting: Medtronic, Boston Scientific
Digoxin And Mortality in Patients With Atrial Fibrillation With and Without Heart Failure: Does Serum Digoxin Concentration Matter?
 Digoxin And Mortality in Patients With Atrial Fibrillation With and Without Heart Failure: Does Serum Digoxin Concentration Matter? Renato D. Lopes, MD, PhD, FACC on behalf of the ARISTOTLE Investigators
Digoxin And Mortality in Patients With Atrial Fibrillation With and Without Heart Failure: Does Serum Digoxin Concentration Matter? Renato D. Lopes, MD, PhD, FACC on behalf of the ARISTOTLE Investigators
Dronedarone for the management of atrial fibrillation
 Published 2 March 2011, doi:10.4414/smw.2011.13158 Cite this as: Dronedarone for the management of atrial fibrillation Roman Brenner, Etienne Delacrétaz Department of Cardiovascular Medicine, University
Published 2 March 2011, doi:10.4414/smw.2011.13158 Cite this as: Dronedarone for the management of atrial fibrillation Roman Brenner, Etienne Delacrétaz Department of Cardiovascular Medicine, University
How atrial fibrillation should be treated in the heart failure patient?
 Advances in Cardiac Arrhhythmias and Great Innovations in Cardiology Torino, 13/15 Ottobre 2016 How atrial fibrillation should be treated in the heart failure patient? Matteo Anselmino Dipartimento Scienze
Advances in Cardiac Arrhhythmias and Great Innovations in Cardiology Torino, 13/15 Ottobre 2016 How atrial fibrillation should be treated in the heart failure patient? Matteo Anselmino Dipartimento Scienze
New Agents for Heart Failure: Ivabradine Jeffrey S. Borer, MD
 New Agents for Heart Failure: Ivabradine Jeffrey S. Borer, MD Professor of Medicine, Cell Biology, Radiology and Surgery Director, The Howard Gilman Institute for Heart Valve Disease and the Schiavone
New Agents for Heart Failure: Ivabradine Jeffrey S. Borer, MD Professor of Medicine, Cell Biology, Radiology and Surgery Director, The Howard Gilman Institute for Heart Valve Disease and the Schiavone
Atrial Fibrillation Cases. Dr Paul Broadhurst Consultant Cardiologist
 Atrial Fibrillation Cases Dr Paul Broadhurst Consultant Cardiologist November 2011 Mr TH age 72 Routine medical for hypertension check Denies any symptoms despite close questioning PMH: hypertension, MI,
Atrial Fibrillation Cases Dr Paul Broadhurst Consultant Cardiologist November 2011 Mr TH age 72 Routine medical for hypertension check Denies any symptoms despite close questioning PMH: hypertension, MI,
Invasive and Medical Treatments for Atrial Fibrillation. Thomas J Dresing, MD Section of Electrophysiology and Pacing Cleveland Clinic
 Invasive and Medical Treatments for Thomas J Dresing, MD Section of Electrophysiology and Pacing Cleveland Clinic Disclosures Fellow s advisory panel for St Jude Medical Speaking honoraria from: Boston
Invasive and Medical Treatments for Thomas J Dresing, MD Section of Electrophysiology and Pacing Cleveland Clinic Disclosures Fellow s advisory panel for St Jude Medical Speaking honoraria from: Boston
Ablation Should Not Be Used as Primary Therapy for Treatment of Patients with Atrial Fibrillation
 Ablation Should Not Be Used as Primary Therapy for Treatment of Patients with Atrial Fibrillation 25 October 2008 Update in Electrocardiography and Arrhythmias Zian H. Tseng, M.D., M.A.S. Assistant Professor
Ablation Should Not Be Used as Primary Therapy for Treatment of Patients with Atrial Fibrillation 25 October 2008 Update in Electrocardiography and Arrhythmias Zian H. Tseng, M.D., M.A.S. Assistant Professor
Atrial Fibrillaiton and Heart Failure: Anticoagulation therapy in all cases?
 Atrial Fibrillaiton and Heart Failure: Anticoagulation therapy in all cases? Nicolas Lellouche Fédération de Cardiologie Hôpital Henri Mondor Créteil Disclosure Statement of Financial Interest I currently
Atrial Fibrillaiton and Heart Failure: Anticoagulation therapy in all cases? Nicolas Lellouche Fédération de Cardiologie Hôpital Henri Mondor Créteil Disclosure Statement of Financial Interest I currently
Etienne Aliot. University of Nancy - France
 Etienne Aliot University of Nancy - France Disclosures Consulting fees : - Bayer, Boehringer Ingelheim,GSK, MedaPharma, Pfizer/BMS,Sanofi Aventis. - Biotronik,Medtronic,St Jude Medical. Electrical vs Pharmacological
Etienne Aliot University of Nancy - France Disclosures Consulting fees : - Bayer, Boehringer Ingelheim,GSK, MedaPharma, Pfizer/BMS,Sanofi Aventis. - Biotronik,Medtronic,St Jude Medical. Electrical vs Pharmacological
ESC. Update of the ESC Guidelines on Medical Therapy. John Camm. ICM Internationales Congress Center München
 ESC 2012 ICM Internationales Congress Center München Update on Consensus Statements on Management of Atrial Fibrillation European Heart Rhythm Association Update of the ESC Guidelines on Medical Therapy
ESC 2012 ICM Internationales Congress Center München Update on Consensus Statements on Management of Atrial Fibrillation European Heart Rhythm Association Update of the ESC Guidelines on Medical Therapy
קוים מנחים לפרפור פרוזדורים - עדכון משה סויסה מרכז רפואי קפלן
 קוים מנחים לפרפור פרוזדורים - עדכון משה סויסה מרכז רפואי קפלן INTRODUCTION The prevalence of atrial fibrillation (AF) is approximately 1.5 2% of the general population The arrhythmia is associated: with
קוים מנחים לפרפור פרוזדורים - עדכון משה סויסה מרכז רפואי קפלן INTRODUCTION The prevalence of atrial fibrillation (AF) is approximately 1.5 2% of the general population The arrhythmia is associated: with
Atrial Fibrillation Management in the ED. J Fisher May 2014"
 Atrial Fibrillation Management in the ED J Fisher May 2014" A 48 yr old man presents with palpitations. He had a big night last night with old mates. ECG How will you manage him? Why important? Common
Atrial Fibrillation Management in the ED J Fisher May 2014" A 48 yr old man presents with palpitations. He had a big night last night with old mates. ECG How will you manage him? Why important? Common
Mehta Hiren R et al. IRJP 2 (3) DRONEDARONE: A NEW MOLECULE FOR ATRIAL FIBRILLATION Patel Paresh B 1, Patel Kamlesh C 1, Mehta Hiren R 2 *
 DRONEDARONE: A NEW MOLECULE FOR ATRIAL FIBRILLATION Patel Paresh B 1, Patel Kamlesh C 1, Mehta Hiren R 2 *") INTERNATIONAL RESEARCH JOURNAL OF PHARMACY ISSN 2230 8407 Available online http://www.irjponline.com Review Article DRONEDARONE: A NEW MOLECULE FOR ATRIAL FIBRILLATION Patel Paresh B 1, Patel Kamlesh C
INTERNATIONAL RESEARCH JOURNAL OF PHARMACY ISSN 2230 8407 Available online http://www.irjponline.com Review Article DRONEDARONE: A NEW MOLECULE FOR ATRIAL FIBRILLATION Patel Paresh B 1, Patel Kamlesh C
EFFECTIVE SHARED CARE AGREEMENT. July Dronedarone (Multaq ) For the treatment and management of atrial fibrillation
 For the treatment and management of atrial fibrillation") Whipps Cross University Hospital NHS Trust EFFECTIVE SHARED CARE AGREEMENT July 2011 Dronedarone (Multaq ) For the treatment and management of atrial fibrillation INTRODUCTION The Whipps Cross University
Whipps Cross University Hospital NHS Trust EFFECTIVE SHARED CARE AGREEMENT July 2011 Dronedarone (Multaq ) For the treatment and management of atrial fibrillation INTRODUCTION The Whipps Cross University
Atrial Fibrillation and Common Supraventricular Tachycardias. Sunil Kapur MD
 Atrial Fibrillation and Common Supraventricular Tachycardias Sunil Kapur MD Cardiac Electrophysiology Brigham and Women s Hospital Instructor, Harvard Medical School No disclosures Cardiac Conduction:
Atrial Fibrillation and Common Supraventricular Tachycardias Sunil Kapur MD Cardiac Electrophysiology Brigham and Women s Hospital Instructor, Harvard Medical School No disclosures Cardiac Conduction:
Hypertension and Atrial Fibrillation in 2017
 Boma Inn, Eldoret, 24th 25thFebruary 2017 Hypertension and Atrial Fibrillation in 2017 Dr Mzee Ngunga Consultant Cardiologist Aga Khan University Hospital, Nairobi Objectives 1. Understand the relationship
Boma Inn, Eldoret, 24th 25thFebruary 2017 Hypertension and Atrial Fibrillation in 2017 Dr Mzee Ngunga Consultant Cardiologist Aga Khan University Hospital, Nairobi Objectives 1. Understand the relationship
Recent observations have focused attention on the PVs as a source of ectopic activity i determining i AF
 Atrial Fibrillation in 2010 Panos Vardas Professor of Cardiology President of EHRA Atrial Fibrillation Pathophysiology of AF Triggers Recent observations have focused attention on the PVs as a source of
Atrial Fibrillation in 2010 Panos Vardas Professor of Cardiology President of EHRA Atrial Fibrillation Pathophysiology of AF Triggers Recent observations have focused attention on the PVs as a source of
Aldosterone Antagonism in Heart Failure: Now for all Patients?
 Aldosterone Antagonism in Heart Failure: Now for all Patients? Inder Anand, MD, FRCP, D Phil (Oxon.) Professor of Medicine, University of Minnesota, Director Heart Failure Program, VA Medical Center 111C
Aldosterone Antagonism in Heart Failure: Now for all Patients? Inder Anand, MD, FRCP, D Phil (Oxon.) Professor of Medicine, University of Minnesota, Director Heart Failure Program, VA Medical Center 111C
Atrial fibrillation (AF) is a disorder seen
 is a disorder seen") This Just In... An Update on Arrhythmia What do recent studies reveal about arrhythmia? In this article, the authors provide an update on atrial fibrillation and ventricular arrhythmia. Beth L. Abramson,
This Just In... An Update on Arrhythmia What do recent studies reveal about arrhythmia? In this article, the authors provide an update on atrial fibrillation and ventricular arrhythmia. Beth L. Abramson,
Atrial Fibrillation 10/2/2018. Depolarization & ECG. Atrial Fibrillation. Hemodynamic Consequences
 Depolarization & ECG Atrial Fibrillation How to make ORDER out of CHAOS Julia Shih, VMD, DACVIM (Cardiology) October 27, 2018 Depolarization & ECG Depolarization & ECG Atrial Fibrillation Hemodynamic Consequences
Depolarization & ECG Atrial Fibrillation How to make ORDER out of CHAOS Julia Shih, VMD, DACVIM (Cardiology) October 27, 2018 Depolarization & ECG Depolarization & ECG Atrial Fibrillation Hemodynamic Consequences
Dronedarone for the treatment of atrial fibrillation and atrial flutter
 National Institute for Health and Clinical Excellence Dronedarone for the treatment of atrial fibrillation and atrial flutter Comment 1: the draft remit Appropriateness Sanofi-aventis Sanofi-aventis believe
National Institute for Health and Clinical Excellence Dronedarone for the treatment of atrial fibrillation and atrial flutter Comment 1: the draft remit Appropriateness Sanofi-aventis Sanofi-aventis believe
Arrhythmias (I) Supraventricular Tachycardias. Disclosures
 Supraventricular Tachycardias. Disclosures") Arrhythmias (I) Supraventricular Tachycardias Amy Leigh Miller, MD, PhD Cardiovascular Electrophysiology, Brigham & Women s Hospital Disclosures None Short R-P Tachycardia REGULAR with 1:1 P/R relationship
Arrhythmias (I) Supraventricular Tachycardias Amy Leigh Miller, MD, PhD Cardiovascular Electrophysiology, Brigham & Women s Hospital Disclosures None Short R-P Tachycardia REGULAR with 1:1 P/R relationship
La terapia non anticoagulante nel paziente con FA secondo le Linee Guida F. CONROTTO
 La terapia non anticoagulante nel paziente con FA secondo le Linee Guida F. CONROTTO Rhythm or rate control strategy? N Engl J Med 2002;347:1834 40 Rate Control versus Electrical Cardioversion for Persistent
La terapia non anticoagulante nel paziente con FA secondo le Linee Guida F. CONROTTO Rhythm or rate control strategy? N Engl J Med 2002;347:1834 40 Rate Control versus Electrical Cardioversion for Persistent
Atrial Fibrillation Ablation in Patients with Heart Failure
 Atrial Fibrillation Ablation in Patients with Heart Failure Eleftherios M. Kallergis, MD, PhD, FESC Cardiology Department, Heraklion University Hospital Since auricular fibrillation so often complicates
Atrial Fibrillation Ablation in Patients with Heart Failure Eleftherios M. Kallergis, MD, PhD, FESC Cardiology Department, Heraklion University Hospital Since auricular fibrillation so often complicates
Dronedarone and Atrial Fibrillation: A Critical Review
 Clinical Medicine Reviews in Vascular Health Review Dronedarone and Atrial Fibrillation: A Critical Review David Singh 1, Eugenio Cingolani 2, Sanjay Kaul 2 and Steven Singh 3 1 University of California
Clinical Medicine Reviews in Vascular Health Review Dronedarone and Atrial Fibrillation: A Critical Review David Singh 1, Eugenio Cingolani 2, Sanjay Kaul 2 and Steven Singh 3 1 University of California
Heart Failure Clinician Guide JANUARY 2016
 Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Heart Failure Clinician Guide JANUARY 2016 Introduction This evidence-based guideline summary is based on the 2016 National Heart Failure Guideline.
Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Heart Failure Clinician Guide JANUARY 2016 Introduction This evidence-based guideline summary is based on the 2016 National Heart Failure Guideline.
Antiarrhythmic Drugs
 Antiarrhythmic Drugs DR ATIF ALQUBBANY A S S I S T A N T P R O F E S S O R O F M E D I C I N E / C A R D I O L O G Y C O N S U L T A N T C A R D I O L O G Y & I N T E R V E N T I O N A L E P A C H D /
Antiarrhythmic Drugs DR ATIF ALQUBBANY A S S I S T A N T P R O F E S S O R O F M E D I C I N E / C A R D I O L O G Y C O N S U L T A N T C A R D I O L O G Y & I N T E R V E N T I O N A L E P A C H D /
Mohammad Zubaid, MB, ChB, FRCPC, FACC
 Management and one year outcome of atrial fibrillation in Middle Eastern cohort enrolled in the observational Gulf Survey of Atrial Fibrillation Events (Gulf SAFE) Mohammad Zubaid, MB, ChB, FRCPC, FACC
Management and one year outcome of atrial fibrillation in Middle Eastern cohort enrolled in the observational Gulf Survey of Atrial Fibrillation Events (Gulf SAFE) Mohammad Zubaid, MB, ChB, FRCPC, FACC