Atrial Fibrillation: Guidelines through clinical cases and 2010 updates
|
|
|
- Lionel Charles
- 6 years ago
- Views:
Transcription

1 Atrial Fibrillation: Guidelines through clinical cases and 2010 updates Samy Claude ELAYI Cardiac Clinical Pacing and Electrophysiology
2 World incidence 720, 000 new cases / year World prevalence 5.5 million AF prevalence increasing with aging of population AF: PUBLIC HEALTH PERSPECTIVE Feinberg WM: Arch Intern Med 1995/ Murgatroyd F and Camm AJ: Lancet 1993
3 When talking about atrial fibrillation treatment, two separate issues: 1/ Prevent thrombo-embolic stroke Coumadin/ASA/plavix/none/Dabigatran 2/ Manage the AF rhythm Rate control/rhythm contol
4 Clinical case 1 65 yo male PMH: HTN Meds: metoprolol 50 mg BID Comes for regular f/u visit, no symptoms with a normal daily activity. Clinically: irregular heart beat.

5
6 You discussed with the patient the potential risk of stroke. What medication would you consider daily regarding this risk? No medication Start Aspirin 81 mg Start Aspirin 325 mg Start Plavix Start Coumadin
7 STROKE RISK/ ANTITHROMBOTIC THERAPY AND AF Moderate-Risk Factors High-Risk Factors Heart failure Hypertension Previous stroke, TIA or embolism Mitral stenosis Age greater than or equal to 75 y LV ejection fraction 35% or less Diabetes mellitus Risk Category Recommended Therapy_ No risk factors One moderate-risk factor Aspirin 81 to 325mg/day or none* Aspirin 81 to 325 mg daily, or warfarin (INR 2.0 to 3.0, target 2.5) Any high risk factor or >1 moderate risk factor warfarin (INR 2.0 to 3.0, target 2.5) * Age less than 60 y, no heart disease (lone AF) 2006 guidelines for the management of patients with AF
8 Stroke risk and CHADS2 score For non valvular AF n Congestive Heart Failure +1 n Hypertension +1 n Age > 75 yo +1 n Diabetes +1 n Prior Stroke/TIA +2 Then classification as: Low-risk = 0 High-risk >2
9 STROKE RISK/ ANTITHROMBOTIC THERAPY AND AF Moderate-Risk Factors High-Risk Factors Heart failure C Previous stroke, TIA or embolism S2 Hypertension H Mitral stenosis Age greater than or equal to 75 y A LV ejection fraction 35% or less Diabetes mellitus D Risk Category Recommended Therapy_ No risk factors One moderate-risk factor Aspirin 81 to 325mg/day or none* Aspirin 81 to 325 mg daily, or warfarin (INR 2.0 to 3.0, target 2.5) Any high risk factor or >1 moderate risk factor warfarin (INR 2.0 to 3.0, target 2.5) * Age less than 60 y, no heart disease (lone AF) 2006 guidelines for the management of patients with AF
10 You discussed with the patient the potential risk of stroke. What would you do next regarding this risk? Not start anything Start Aspirin 81 mg Start Aspirin 325 mg Start Plavix Start Coumadin
11 You decided to start Aspirin 325 mg and determine during the f/u that your patient is always in AF (=persistent AF).
12 AF CLASSIFICATION PAROXYSMAL AF PERSISTENT AF PERMANENT AF Terminates spontaneously AF can be converted to SR (shock or drug) Yes No No N/A Yes No Gallagher MM, Camm AJ. Classification of atrial fibrillation. PACE. 1992;20:
13 What would you do next for this patient with HTN and asymptomatic persistent AF? Restore sinus rhythm with cardioversion (RHYTHM CONTROL) Keep the patient in AF but adjust the metoprolol dose to prevent fast ventricular heart rate to avoid potential tachycardia induced cardiomyopathy with heart failure (RATE CONTROL) Send the patient for an ablation
14 2006 guidelines for the management of patients with AF
15 Rate control Rhythm control 2006 guidelines for the management of patients with AF
16 What would you do next for this patient with HTN and asymptomatic persistent AF? Restore sinus rhythm with cardioversion (RHYTHM CONTROL) Keep the patient in atrial fibrillation but adjust the metoprolol dose to prevent fast ventricular heart rate to avoid potential tachycardia induced cardiomyopathy and heart failure (RATE CONTROL) Send the patient for an ablation
17 Rate vs. Rhythm control The AFFIRM Trial Design in the mid 1990 to help manage AF Potential benefit of maintaining SR: better survival lower risk of stroke better quality of life Hypothesis: maintenance of SR with AAdrugs would improve mortality compared to rate control of AF with AV nodal blockers AFFIRM NEJM 2002;347:
18 Rate vs. Rhythm control The AFFIRM Trial Inclusion criteria One or more recent episodes of AF of > 6 hours (excluded permanent AF). Patients with at least one clinical risk factor for stroke: age> 65 HTN DM CHF LVEF < 40% prior stroke AFFIRM NEJM 2002;347:
19 AFFIRM limitation Patients with frequent or severe symptoms were largely excluded Although this subgroup would benefit the most from SR Constitutes >1/3 of all AF patients
20 Rate vs. Rhythm control The AFFIRM Trial 4060 patients were randomized to: 1. Rhythm control (maintain SR as much as possible using cardioversions and AAdrugs). 2. Rate control (with AV nodal blockers). AFFIRM NEJM 2002;347:
21 It does not mean SR=AF in term of mortality. Primary endpoint: overall mortality Management of AF with the rhythm-control strategy offers no survival advantage over the rate-control strategy > Current guidelines
22 Sinus Rhythm vs. AF AFFIRM study did not compare SR vs AF, but: an ineffective and toxic tool to maintain SR (AAdrugs) versus maintaining AF with rate control drugs. AFFIRM study can not be extrapolated to Sinus rhythm and AF are equivalent in term of mortality. SR is better than AF mortality wise.
23 Clinical impact of AF on mortality AF has a 1.5- to 1.9-fold increased risk of mortality in the general population * compared to sinus rhythm 4.2-fold increased risk for CV mortality in lone AF; 2.5-fold increased risk for mortality in HF; 4.5-fold increased risk for mortality in acute coronary syndromes. Benjamin et al Circulation 1998;98:946-52
24 AFFIRM conclusion: Trying to maintain sinus rhythm with an aggressive strategy using currently available drugs (relatively ineffective to maintain SR or with major side effects) is not better in term of mortality than keeping AF rate controlled in patients with moderately, minimally or not symptomatic AF. The impact of maintaining SR on mortality with ablation or potential new drugs (less toxic, more effective to maintain SR) is unknown.
25 65 yo male HTN metoprolol asymptomatic persistent AF You decided to cardiovert the patient and this restored normal sinus rhythm. However, 4 months latter, he is back in AF and still asymptomatic. What would you do next? Start cardioversion again rate control the AF
26 2006 guidelines for the management of patients with AF
27 65 yo male HTN metoprolol asymptomatic recurrent persistent AF You decided to cardiovert the patient and this restored normal sinus rhythm. However, 4 months latter, he is back in AF and still asymptomatic. What would you do next? Start cardioversion again Rate control the AF
28 61 year old male Clinical case 2 PMH: HTN treated with amlodipine (Norvasc) Complaining of episodes of palpitations for the last year: several episodes/month, from few minutes to 1 hour spontaneous termination. Feels dizzy, SOB and exhausted. He went to the local ED 6 weeks ago and was told he has "A-fib." Had heart echo (EF 65%)/TSH normal. Was started on ASA and metoprolol 150 mg BID and asked to f/u with his PCP. Clinical exam: unremarkable with regular heart beat
29 The patient still has frequent palpitations despite 150 mg BID of metoprolol. His heart rate is around 50 bpm. What would you do next? Consider increasing metoprolol Consider starting antiarrhythmic drugs Consider sending the patient for an AF ablation Consider sending the patient for a pacemaker and AV node junction ablation
30 2006 guidelines for the management of patients with AF
31 The patient still have frequent arrhythmia symptoms despite 300 mg of metoprolol. What would you do next? Consider increasing metoprolol Consider starting antiarrhythmic drugs Consider sending the patient for an AF ablation Consider sending the patient for a pacemaker and AV node junction ablation
32 Drugs used in 2010 for AF FOR RHYTHM CONTROL (maintain SR) Class IC Flecainide (Tambocor*) Propafenone (Rythmol*) Class III Amiodarone (Cordarone*;Pacerone*) Sotalol (Betapace*) Dofetilide (Tikosyn*) Dronedarone (Multaq*) FOR RATE CONTROL (control AF) Betablockers/ calcium blockers (diltiazem/verapamil)/ digoxin
33 61 yo male HTN normal heart echo no CAD nor heart failure very symptomatic AF failed rate control. Which antiarrhythmic could be started?
34 61 yo male HTN normal heart echo no CAD nor heart failure very symptomatic AF failed rate control. Which antiarrhythmic could be started? Depends on the heart condition
35 2006 guidelines for the management of patients with AF
36 The patient was started on flecainide (IC) 50 mg BID, well tolerated. At his 2 months f/u, he reports a few episodes of AF<5 min still symptomatic. What would you consider? Continue same medications and f/u Increase the dose of flecainide to the standard dose of 100 mg BID Change antiarrhythmic drug Consider sending the patient for an AF ablation
37 The patient was started on flecainide 50 mg BID, well tolerated. At his 2 months f/u, he reports a few episodes of AF<5 min still symptomatic. What would you consider? Continue same medications and f/u Increase the dose of flecainide to the standard dose of 100 mg BID Change antiarrhythmic drug Consider sending the patient for an AF ablation
38 You increased the flecainide to 100 mg BID. The patient did well and did not came back to see you for seven months. One day, he calls and wants to been seen quickly because he is short of breath and has bilateral pedal edema for the last few days. Clinically, he is tachycardic around 160 bpm irregular and is in congestive heart failure with bilateral crackles and a systolic BP of 90 mmhg.

39
40 You send him to the ER where he was admitted. His left ventricular EF is now 30% on echo. What do you expect them to do? Keep the patient on aspirin Initiate coumadin Cardiovert the patient to sinus rhythm after TEE Initiate long term amiodarone Initiate immediately dronedarone (Multaq*)
41 STROKE RISK/ ANTITHROMBOTIC THERAPY AND AF Moderate-Risk Factors High-Risk Factors Age greater than or equal to 75 y Hypertension Previous stroke, TIA or embolism Mitral stenosis Heart failure LV ejection fraction 35% or less Diabetes mellitus Risk Category Recommended Therapy_ No risk factors One moderate-risk factor Aspirin 81 to 325mg/day or none* Aspirin 81 to 325 mg daily, or warfarin (INR 2.0 to 3.0, target 2.5) Any high risk factor or >1 moderate risk factor warfarin (INR 2.0 to 3.0, target 2.5) * Age less than 60 y, no heart disease (lone AF) 2006 guidelines for the management of patients with AF
42 You send him to the ER where he was admitted. His left ventricular EF is 30% on echo. What do you expect them to do? Keep the patient on aspirin Initiate coumadin Cardiovert the patient to sinus rhythm after TEE Initiate long term amiodarone Initiate immediately dronedarone (Multaq*)
43 Amiodarone the most effective but side effects +++: -life threatening pulmonary fibrosis -thyroid (hyper or hypo) -QT prolongation (ventricular arrhythmias) -ocular, neurologic, dermatologic, liver
44 You send him to the ER where he was admitted. His left ventricular EF is 30% on echo. What do you expect them to do? Keep the patient on aspirin Initiate coumadin Cardiovert the patient to sinus rhythm after TEE Initiate long term amiodarone Initiate immediately dronedarone (Multaq*)

45 Dronedarone (Multaq*) Class III K blockers Available in the US since august 2009 Wei Sun et al Circ 1999;100:
46 Dronedarone (Multaq*) Advantages -no lung or thyroid toxicity (with a half life <24h) -reduces hospitalization for AF (ATHENA trial NEJM 2009) -no hospital admission for initiation/ no special certification Limits -Contra-indication in unstable heart failure (IV) or class II III< 1 month -efficacy less than amiodarone (-12%) -cost
47 Dronedarone Dronedarone Dronedarone Dronedarone? 2006 guidelines for the management of patients with AF
48 You send him to the ER where he was admitted. His left ventricular EF is 30% on echo. What do you expect them to do? Keep the patient on aspirin Initiate coumadin Cardiovert the patient to sinus rhythm after TEE Initiate long term amiodarone Initiate immediately dronedarone (Multaq*)
49 The patient has been cardioverted. Patient has been discharged on coumadin and Tikosyn 500 mcg BID (maximal dose). He comes at his 2 months f/u after repeating a new heart echo: EF 70% (arrhythmia induced cardiomyopathy). He still reports palpitations and dizziness which are impairing his quality of life.
50 So 61 yo male HTN very symptomatic AF failed two AADS at maximal doses. What would you do next? Stop the tikosyn and start sotalol Send the patient for AF ablation
51 So 61 yo male HTN very symptomatic AF failed two AADS at maximal doses. What would you do next? Stop the tikosyn and start sotalol Send the patient for AF ablation

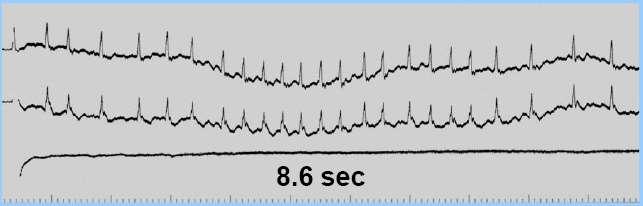
52 I II III avr avl avf V1 V2 V3 V4 V5 V6

53 Posterior Basal View R. pulmonary artery Left Atrium L. pulmonary artery L. auricle L. superior pulmonary vein L. atrium L. inferior pulmonary vein R. superior pulmonary vein R. inferior pulmonary vein Coronary sinus Netter F. Atlas of Human Anatomy. 1989;Plate 202.

54 Myocardial sleeve Veno-atrial junction LA Left atrium LSPV Lung hilum


55

 and right anterior oblique (RAO)")
56 Atrial Fibrillation: Catheter ablation of PV focus The fluoroscopy images show the ablation catheter (ABL) in the left anterior oblique (LAO) and right anterior oblique (RAO) projections.




57 Complex procedure Esophagus temperature monitoring probe LA CT to define the anatomy more precisely Ablation catheter Circular mapping catheter Straight mapping catheter Mapping system during ablation Intracardiac echo probe
58 Paroxysmal AF Targets mainly the trigger by disconnecting the pulmonary veins from the rest of the left atrium

59 Ablation in paroxysmal AF Elayi et al. Heart rhythm 2006
60 Persistent AF May need to target -the trigger (isolation of the pulmonary veins) -the rest of the left atrium and sometimes right atrium (to modify the atrial substrate capable of sustaining persistent AF)

61 Ablation in persistent AF Elayi et al. Heart rhythm 2008
62 Main complications of AF ablation Stroke (0.5 to 1%)+++ like left heart cath Pericardial effusion/tamponnade Others: hematomas; PV stenosis; fistula with esophagus, phrenic nerve paralysis
63 Ablation versus Drugs Advantages -Relative efficacy with a success rate around 70-90% in paroxysmal AF and 50-75% in persistent AF (less successful in enlarged atrium). -Potential cure (no life long treatment) -Potentially stop coumadin Disadvantages -Immediate procedure risk -Operator dependant (long learning curve) -Lack on very long term data
64 2006 guidelines for the management of patients with AF
65 Maintenance of sinus rhythm Catheter ablation is a reasonable alternative to pharmacological therapy to prevent recurrent AF in symptomatic patients with little or no LA enlargement (Class IIA; level of evidence C) 2006 guidelines for the management of patients with AF
66 AF Ablation summary GOAL=Alleviate AF symptoms Relatively effective procedure especially in paroxysmal patients For symptomatic AF After failure of at least one antiarrhythmic drug With potential significant complications long term survival and data unknown (>10 years)
67 Dabigatran Oral direct thrombin inhibitor Advantages over coumadin/enoxaparin: -oral -no routine anticoagutation checks (INR) -few drugs interaction Disavantages: -BID with short half life (compliance) -Liver toxicity RE-LY trial NEJM 2009
68 Dabigatran Was compared to coumadin at two doses (RE-LY trial): -110 mg BID: same embolic stroke rate but less hemorrhagic stroke than coumadin mg BID: less embolic stroke but same hemorrhagic stroke than coumadin FDA approval last week RE-LY trial NEJM 2009
 Symptomatic patients: -AADrugs are always the first option -Failure of AADrugs :")
69 Conclusion In AF, first evaluate thrombo-embolic risk and decide aspirin versus coumadin Several Rx options are available for the rhythm Asymptomatic patients: -Make sure patient really asymptomatic -Rate control is an acceptable option (try cardioversion once reasonable) Symptomatic patients: -AADrugs are always the first option -Failure of AADrugs : ablation
70 Thank you very much If further questions: Phone:(859)
71
72 * RA LA RV LV

73 1 PAC *
74 AF wavelets 400 to 600 bpm AV node filters 1 the atrial 1 1 activity and 1 determines the ventricular rate
75 RHYTHM CONTROL (antiarrhythmic drugs, Ablation) * 1 1 1
 * 1 1")
76 RATE CONTROL (AV nodal blockers filter AF waves) * 1 1 1
77 What would you do next for this patient with HTN and asymptomatic persistent AF? Restore sinus rhythm with cardioversion (RHYTHM CONTROL) Keep the patient in atrial fibrillation but adjust the metoprolol dose to prevent fast ventricular heart rate to avoid potential tachycardia induced cardiomyopathy and heart failure (RATE CONTROL) Send the patient for an ablation
78 Clinical case 3 87 yo female PMH: HTN DM several surgeries COPD AF: permanent with several hospitalizations over the last 2 years for CHF and ventricular heart rate in the despite digoxin and metoprolol which alternates with episodes of heart rate in the 30 s very tired and dizzy Clinically systolic BP in the 90 s
79 What would you do next? Add another AV nodal blockers (diltiazem) Send the patient for a pacemaker Send the patient for a pacemaker and AV node ablation
80 AVN ABLATION AND PACEMAKER Rationale: AVN ablation prevent the fast atria rate (500 bpm) to conduct rapidly and irregularly to the ventricle by disconnecting atria and ventricles The ventricle can be paced regularly.
81 AV Node Ablation

82 AV Node Ablation


83
84 AVN ablation and pacing Only for selected patients with: symptomatic AF failed AADs (rhythm or rate control) not good candidate for ablation
85 Clinical case 4 64 yo male h/o GERD Comes to see you in regular f/u visit. used to be very active but now cannot do any significant effort because of fatigue so limit his activity and doing OK Clinically irregular heart beat 85 bpm

86
87 You do a general workup (CBC ) than is negative. What would you do next? f/u in a few months Do a 24 hours holter to make sure he is correctly rate controlled Try to cardiovert him
88 Hemodynamics Symptoms Assess symptoms is critical because it is going to guide your treatment
89 Hemodynamics Symptoms Reduced cardiac output -Hypotension -Pulmonary and/or systemic CHF Fast/slow/irregular ventricular rate is symptomatic for many patients, resulting in: Palpitations Dyspnea Dizziness Post conversion pauses/ syncope


90 Hemodynamics Symptoms Inappropriate increases in heart rate with exercise may cause -exercise intolerance +++ -fatigue +++ If chronic cardiomyopathy with low EF Increase myocardial oxygen demand may precipitate coronary ischemia.



91
92 (ACC/AHA/ESC 2006 guidelines for the management of patients with atrial fibrillation)
93 CONCLUSION Several AF treatment options available AADs always 1 st option to rhythm control before ablation Rate control is an acceptable primary therapy: -if reach target (80 bpm at rest and 110 bpm exercise) -consider DCV for the 1 st documented AF, even if not symptomatic -no data to compare mortality with ablation and rate control Patient stays symptomatic despite rate/rhythm control consider ablation AVN ablation+ pacemaker last resort
94 Symptoms and AF (2) Atrial fibrillation conducting quickly to the ventricles can lead to tachycardia induced dilated cardiomyopathy with low ventricle ejection fraction. If rate control strategy is chosen, rate control should be efficient.
95 Dronedarone jeff Multaq is contraindicated in patients with NYHA Class IV heart failure, or NYHA Class II-III heart failure with a recent decompensation requiring hospitalization or referral to a specialized heart failure clinic. The Athena trial characterized recent decompensation as occurring in the previous 4 weeks. No criteria were used for ejection fraction however Athena had 1165 patients with Class 1 or 2 CHF and 200 patients with Class 3. There were 179 patients with a LVEF <35% and 4365 patients with LVEF >35%. If a patient has CHF Class 1, 2, or 3, has a normal EF, and is Clinically stable. Multaq may be used just as it was in Athena. If they are becoming unstable they should not be started or the medication should be stopped.
96 dronedarone Pros: -no hospital admission/ drug certification -no renal excretion -should replace IC drugs -multi channel, also AV nodal blocade (per rep, dim HR in AF by bpm) Cons: -longer study f/u 1.5 year -efficacy -12% compared to amiodarone (dionysos) QT -indicated in parox AF -CI in class IV and class 2 to 3 recent within one month= unstable CHF
97 His main concern is the risk of stroke (father had a massive stroke). What would you do regarding his treatment: Keep on ASA Stop ASA and start clopidogrel (Plavix) Stop ASA and start coumadin
98 ACC/AHA/ESC guidelines 2006
99 Rx options for recurrent AF Rhythm control [keep the patient in SR] with antiarrhythmics drugs (AADs) with ablation - Catheter ablation - Surgery (Maze) With hybrid approach: combining AADs and/or ablation and/or pacemakers Rate control [keep patient in AF but control ventricular rate] with AV nodal blockers with AV nodal ablation and pacemaker
5/5/2010. World incidence 720, 000 new cases / year. World prevalence 5.55 million AF prevalence increasing with aging of population
 Atrial Fibrillation: Guidelines through clinical cases and 2010 updates Samy Claude ELAYI Cardiac Clinical Pacing and Electrophysiology UK World incidence 720, 000 new cases / year World prevalence 5.55
Atrial Fibrillation: Guidelines through clinical cases and 2010 updates Samy Claude ELAYI Cardiac Clinical Pacing and Electrophysiology UK World incidence 720, 000 new cases / year World prevalence 5.55
Basics of Atrial Fibrillation. By Mini Thannikal NP-BC Mount Sinai St Luke s Hospital New York, NY
 Basics of Atrial Fibrillation By Mini Thannikal NP-BC Mount Sinai St Luke s Hospital New York, NY Atrial Fibrillation(AF) is a supraventricular tachyarrhythmia characterized by uncoordinated atrial activation
Basics of Atrial Fibrillation By Mini Thannikal NP-BC Mount Sinai St Luke s Hospital New York, NY Atrial Fibrillation(AF) is a supraventricular tachyarrhythmia characterized by uncoordinated atrial activation
ATRIAL FIBRILLATION: REVISITING CONTROVERSIES IN AN ERA OF INNOVATION
 ATRIAL FIBRILLATION: REVISITING CONTROVERSIES IN AN ERA OF INNOVATION Frederick Schaller, DO, MACOI,FACP Adjunct Clinical Professor Touro University Nevada DISCLOSURES I have no financial relationships
ATRIAL FIBRILLATION: REVISITING CONTROVERSIES IN AN ERA OF INNOVATION Frederick Schaller, DO, MACOI,FACP Adjunct Clinical Professor Touro University Nevada DISCLOSURES I have no financial relationships
Jay Simonson, MD, FACC, FHRS Medical Director, Cardiac Electrophysiology Park Nicollet Heart and Vascular Center
 Jay Simonson, MD, FACC, FHRS Medical Director, Cardiac Electrophysiology Park Nicollet Heart and Vascular Center A-Fib Facts Yes, you may be able to blame your parents It is more of a nuisance than a
Jay Simonson, MD, FACC, FHRS Medical Director, Cardiac Electrophysiology Park Nicollet Heart and Vascular Center A-Fib Facts Yes, you may be able to blame your parents It is more of a nuisance than a
2015 Atrial Fibrillation Therapy Meds, Shock, or Ablate? D. Scott Kirby MD, FACC Cardiac Electrophysiologist
 2015 Atrial Fibrillation Therapy Meds, Shock, or Ablate? D. Scott Kirby MD, FACC Cardiac Electrophysiologist Todays Objectives Atrial Fibrillation evaluation and treatment from an EP perspective Multimodal
2015 Atrial Fibrillation Therapy Meds, Shock, or Ablate? D. Scott Kirby MD, FACC Cardiac Electrophysiologist Todays Objectives Atrial Fibrillation evaluation and treatment from an EP perspective Multimodal
Understanding Atrial Fibrillation Management. Roy Lin, MD
 Understanding Atrial Fibrillation Management Roy Lin, MD Disclosure None Definition of atrial fibrillation Atrial fibrillation is a supraventricular tachyarrhythmia characterized by uncoordinated atrial
Understanding Atrial Fibrillation Management Roy Lin, MD Disclosure None Definition of atrial fibrillation Atrial fibrillation is a supraventricular tachyarrhythmia characterized by uncoordinated atrial
Dysrhythmias 11/7/2017. Disclosures. 3 reasons to evaluate and treat dysrhythmias. None. Eliminate symptoms and improve hemodynamics
 Dysrhythmias CYDNEY STEWART MD, FACC NOVEMBER 3, 2017 Disclosures None 3 reasons to evaluate and treat dysrhythmias Eliminate symptoms and improve hemodynamics Prevent imminent death/hemodynamic compromise
Dysrhythmias CYDNEY STEWART MD, FACC NOVEMBER 3, 2017 Disclosures None 3 reasons to evaluate and treat dysrhythmias Eliminate symptoms and improve hemodynamics Prevent imminent death/hemodynamic compromise
Controversies in Atrial Fibrillation and HF
 Controversies in Atrial Fibrillation and HF Dr.Yahya Al Hebaishi Cardiac electrophysiology division, PSCC, Riyadh Atrial Fibrillation: Rate or Rhythm? HF and AF: the twin epidemic of cardiovascular disease.
Controversies in Atrial Fibrillation and HF Dr.Yahya Al Hebaishi Cardiac electrophysiology division, PSCC, Riyadh Atrial Fibrillation: Rate or Rhythm? HF and AF: the twin epidemic of cardiovascular disease.
Cost and Prevalence of A fib. Atrial Fibrillation: Guideline Directed Treatment. Prevalence of A Fib. Risk Factors for A Fib. Risk Factors for A Fib
 Atrial Fibrillation: Guideline Directed Treatment Melissa Wendell, FNP-C, MSN Heart Failure - Lead Nurse Practitioner, Aspirus Wausau Hospital and Aspirus Cardiology Cost and Prevalence of A fib 33.5 million
Atrial Fibrillation: Guideline Directed Treatment Melissa Wendell, FNP-C, MSN Heart Failure - Lead Nurse Practitioner, Aspirus Wausau Hospital and Aspirus Cardiology Cost and Prevalence of A fib 33.5 million
Rate and Rhythm Control of Atrial Fibrillation
 Rate and Rhythm Control of Atrial Fibrillation April 21, 2017 춘계심혈관통합학술대회 Jaemin Shim, MD, PhD Arrhythmia Center Korea University Anam Hospital Treatment of AF Goal Reducing symptoms Preventing complication
Rate and Rhythm Control of Atrial Fibrillation April 21, 2017 춘계심혈관통합학술대회 Jaemin Shim, MD, PhD Arrhythmia Center Korea University Anam Hospital Treatment of AF Goal Reducing symptoms Preventing complication
Treatment strategy decision tree
 strategy decision tree strategy decision tree Confirmed diagnosis of AF Further investigations and clinical assessment including risk stratification for stroke/thromboembolism Paroxysmal AF Persistent
strategy decision tree strategy decision tree Confirmed diagnosis of AF Further investigations and clinical assessment including risk stratification for stroke/thromboembolism Paroxysmal AF Persistent
Invasive and Medical Treatments for Atrial Fibrillation. Thomas J Dresing, MD Section of Electrophysiology and Pacing Cleveland Clinic
 Invasive and Medical Treatments for Thomas J Dresing, MD Section of Electrophysiology and Pacing Cleveland Clinic Disclosures Fellow s advisory panel for St Jude Medical Speaking honoraria from: Boston
Invasive and Medical Treatments for Thomas J Dresing, MD Section of Electrophysiology and Pacing Cleveland Clinic Disclosures Fellow s advisory panel for St Jude Medical Speaking honoraria from: Boston
AF in the ER: Common Scenarios CASE 1. Fast facts. Diagnosis. Management
 AF in the ER: Common Scenarios Atrial fibrillation is a common problem with a wide spectrum of presentations. Below are five common emergency room scenarios and the management strategies for each. Evan
AF in the ER: Common Scenarios Atrial fibrillation is a common problem with a wide spectrum of presentations. Below are five common emergency room scenarios and the management strategies for each. Evan
Fibs and Flutters: The Heart of the Matter
 Fibs and Flutters: The Heart of the Matter Anita Ralstin, CNP By the Numbers Atrial Fibrillation Hospital Discharges /quarter for 2012 -- 116,500 Average Length of Stay 4 days Projected that 20% of those
Fibs and Flutters: The Heart of the Matter Anita Ralstin, CNP By the Numbers Atrial Fibrillation Hospital Discharges /quarter for 2012 -- 116,500 Average Length of Stay 4 days Projected that 20% of those
Current Guideline for AF Treatment. Young Keun On, MD, PhD, FHRS Samsung Medical Center Sungkyunkwan University School of Medicine
 Current Guideline for AF Treatment Young Keun On, MD, PhD, FHRS Samsung Medical Center Sungkyunkwan University School of Medicine Case 1 59 year-old lady Sudden palpitation and breathlessness for 12 hours
Current Guideline for AF Treatment Young Keun On, MD, PhD, FHRS Samsung Medical Center Sungkyunkwan University School of Medicine Case 1 59 year-old lady Sudden palpitation and breathlessness for 12 hours
Geriatric Grand Rounds
 Geriatric Grand Rounds Tuesday, April 13, 21 12: noon Dr. Bill Black Auditorium Glenrose Rehabilitation Hospital In keeping with Glenrose Rehabilitation Hospital policy, speakers participating in this
Geriatric Grand Rounds Tuesday, April 13, 21 12: noon Dr. Bill Black Auditorium Glenrose Rehabilitation Hospital In keeping with Glenrose Rehabilitation Hospital policy, speakers participating in this
AF Today: W. For the majority of patients with atrial. are the Options? Chris Case
 AF Today: W hat are the Options? Management strategies for patients with atrial fibrillation should depend on the individual patient. Treatment with medications seems adequate for most patients with atrial
AF Today: W hat are the Options? Management strategies for patients with atrial fibrillation should depend on the individual patient. Treatment with medications seems adequate for most patients with atrial
How does the heart work? The heart is muscle whose main function is a pump; to push blood the rest of your body.
 1 You have a condition called atrial fibrillation. I would like you to learn more about this condition. You should read about it below, and can also watch an Internet program about it. After reading about
1 You have a condition called atrial fibrillation. I would like you to learn more about this condition. You should read about it below, and can also watch an Internet program about it. After reading about
Atrial Fibrillation Etiologies and Treatment. Shawn Liu Learner Centered Learning Goal
 Atrial Fibrillation Etiologies and Treatment Shawn Liu Learner Centered Learning Goal Pathophysiology Defined by the absence of coordinated atrial systole Results from multiple reentrant electrical waves
Atrial Fibrillation Etiologies and Treatment Shawn Liu Learner Centered Learning Goal Pathophysiology Defined by the absence of coordinated atrial systole Results from multiple reentrant electrical waves
Atrial Fibrillation. Epidemiology. Goals 11/12/2012. Faithful marker for age and underlying cardiopulmonary disease
 Atrial Fibrillation Goals the emerging epidemic Rate Control Thromboembolism and anticoagulation Cardioversion: When, How, and Why 1st time AF < 48hr 1st time AF > 48hr PAF < 48 hr. PAF > 48 hr. Eric R.
Atrial Fibrillation Goals the emerging epidemic Rate Control Thromboembolism and anticoagulation Cardioversion: When, How, and Why 1st time AF < 48hr 1st time AF > 48hr PAF < 48 hr. PAF > 48 hr. Eric R.
Atrial Fibrillation and the NOAC s. John Raymond MS, PA-C, MHP February 10, 2018
 Atrial Fibrillation and the NOAC s John Raymond MS, PA-C, MHP February 10, 2018 Pathogenesis EPIDEMIOLOGY Arrhythmia-related hospitalisations in the US Ventricular fibrillation 2% Atrial fibrillation 34%
Atrial Fibrillation and the NOAC s John Raymond MS, PA-C, MHP February 10, 2018 Pathogenesis EPIDEMIOLOGY Arrhythmia-related hospitalisations in the US Ventricular fibrillation 2% Atrial fibrillation 34%
Atrial Fibrillation: Beyond the AFFIRM trial
 Atrial Fibrillation: Beyond the AFFIRM trial Daniel J. Cantillon MD FACC FHRS Cardiac Electrophysiology and Pacing Assistant Professor, Lerner College of Medicine Cleveland Clinic, Heart & Vascular Institute
Atrial Fibrillation: Beyond the AFFIRM trial Daniel J. Cantillon MD FACC FHRS Cardiac Electrophysiology and Pacing Assistant Professor, Lerner College of Medicine Cleveland Clinic, Heart & Vascular Institute
Treatment of Atrial Fibrillation in Heart Failure
 Stockholm, September 1st 2010 Treatment of Atrial Fibrillation in Heart Failure Rhythm control: Which drugs? Stefan H. Hohnloser J.W. Goethe University Frankfurt, Germany Presenter disclosure information:
Stockholm, September 1st 2010 Treatment of Atrial Fibrillation in Heart Failure Rhythm control: Which drugs? Stefan H. Hohnloser J.W. Goethe University Frankfurt, Germany Presenter disclosure information:
Atrial Fibrillation Management in the ED. J Fisher May 2014"
 Atrial Fibrillation Management in the ED J Fisher May 2014" A 48 yr old man presents with palpitations. He had a big night last night with old mates. ECG How will you manage him? Why important? Common
Atrial Fibrillation Management in the ED J Fisher May 2014" A 48 yr old man presents with palpitations. He had a big night last night with old mates. ECG How will you manage him? Why important? Common
Ablation Update and Case Studies. Lawrence Nair, MD, FACC Director of Electrophysiology Presbyterian Heart Group
 Ablation Update and Case Studies Lawrence Nair, MD, FACC Director of Electrophysiology Presbyterian Heart Group Disclosures No financial relationships to disclose Objectives At the conclusion of this activity,
Ablation Update and Case Studies Lawrence Nair, MD, FACC Director of Electrophysiology Presbyterian Heart Group Disclosures No financial relationships to disclose Objectives At the conclusion of this activity,
Management of ATRIAL FIBRILLATION. in general practice. 22 BPJ Issue 39
 Management of ATRIAL FIBRILLATION in general practice 22 BPJ Issue 39 What is atrial fibrillation? Atrial fibrillation (AF) is the most common cardiac arrhythmia encountered in primary care. It is often
Management of ATRIAL FIBRILLATION in general practice 22 BPJ Issue 39 What is atrial fibrillation? Atrial fibrillation (AF) is the most common cardiac arrhythmia encountered in primary care. It is often
3/25/2017. Program Outline. Classification of Atrial Fibrillation
 Alternate Strategies to Antiarrhythmic Therapy: The Role of Ablation Jennifer El Aile, MS, AGPCNP-BC Electrophysiology Nurse Practitioner Clinical Lecturer at the University of Michigan Program Outline
Alternate Strategies to Antiarrhythmic Therapy: The Role of Ablation Jennifer El Aile, MS, AGPCNP-BC Electrophysiology Nurse Practitioner Clinical Lecturer at the University of Michigan Program Outline
» A new drug s trial
 » A new drug s trial A placebo-controlled, double-blind, parallel arm Trial to assess the efficacy of dronedarone 400 mg bid for the prevention of cardiovascular Hospitalization or death from any cause
» A new drug s trial A placebo-controlled, double-blind, parallel arm Trial to assess the efficacy of dronedarone 400 mg bid for the prevention of cardiovascular Hospitalization or death from any cause
Atrial Fibrillation Topics for Today. Clinical Controversies Management of Atrial Fibrillation. Atrial Fibrillation in the ER Topics for Today
 Clinical Controversies Management of Atrial Fibrillation Yerem Yeghiazarians, M.D. Associate Professor of Medicine Leone-Perkins Family Endowed Chair in Cardiology Atrial Fibrillation Topics for Today
Clinical Controversies Management of Atrial Fibrillation Yerem Yeghiazarians, M.D. Associate Professor of Medicine Leone-Perkins Family Endowed Chair in Cardiology Atrial Fibrillation Topics for Today
Polypharmacy - arrhythmic risks in patients with heart failure
 Influencing sudden cardiac death by pharmacotherapy Polypharmacy - arrhythmic risks in patients with heart failure Professor Dan Atar Head, Dept. of Cardiology Oslo University Hospital Ullevål Norway 27.8.2012
Influencing sudden cardiac death by pharmacotherapy Polypharmacy - arrhythmic risks in patients with heart failure Professor Dan Atar Head, Dept. of Cardiology Oslo University Hospital Ullevål Norway 27.8.2012
Disclosures. Managing Atrial Fibrillation in Atrial Fibrillation: A Growing Problem. Objectives. Atrial Fibrillation: Prevalence Estimates
 Managing Atrial Fibrillation in 2010 Jennifer Cummings, MD FACC Director, Cardiac Electrophysiology Akron General Medical Center Disclosures Company Boston Scientific St. Jude Medical Medtronic Sanofi-Aventis
Managing Atrial Fibrillation in 2010 Jennifer Cummings, MD FACC Director, Cardiac Electrophysiology Akron General Medical Center Disclosures Company Boston Scientific St. Jude Medical Medtronic Sanofi-Aventis
What s New in the AF Guidelines
 Impact on New AF Guidelines on Heart Failure Management Gothenburg - May 22 nd 2011 Europace (2010) 12, 1360-420 http://europace.oxfordjournals.org JACC (2011) 57, 223-42 http://www.cardiosource.org What
Impact on New AF Guidelines on Heart Failure Management Gothenburg - May 22 nd 2011 Europace (2010) 12, 1360-420 http://europace.oxfordjournals.org JACC (2011) 57, 223-42 http://www.cardiosource.org What
Who Needs Admission and Who can go home?
 Who Needs Admission and Who can go home? Where is the presentation (clinic or ER)? Time of onset/duration Can symptoms be relieved? Stroke risk reduction Can adequate heart rate control be achieved? Is
Who Needs Admission and Who can go home? Where is the presentation (clinic or ER)? Time of onset/duration Can symptoms be relieved? Stroke risk reduction Can adequate heart rate control be achieved? Is
Are Drugs Better? Dr Mauro Lencioni. Drugs or ablation as first line treatment for AF? Consultant Cardiologist & Electrophysiologist
 Are Drugs Better? Drugs or ablation as first line treatment for AF? Dr Mauro Lencioni Consultant Cardiologist & Electrophysiologist The Philosophical Issue What do we mean by Better? Outcome measures Measurement
Are Drugs Better? Drugs or ablation as first line treatment for AF? Dr Mauro Lencioni Consultant Cardiologist & Electrophysiologist The Philosophical Issue What do we mean by Better? Outcome measures Measurement
Out with the old, in with The 2010 Atrial Fibrillation Guidelines
 Out with the old, in with The 2010 Atrial Fibrillation Guidelines Kseniya Chernushkin B.Sc.(Pharm.), VCH/PHC Pharmacy Resident Mary Elliot B.Sc.(Pharm.), VCH/PHC Pharmacy Resident March 22, 2011 Outline
Out with the old, in with The 2010 Atrial Fibrillation Guidelines Kseniya Chernushkin B.Sc.(Pharm.), VCH/PHC Pharmacy Resident Mary Elliot B.Sc.(Pharm.), VCH/PHC Pharmacy Resident March 22, 2011 Outline
Catheter Ablation for Treatment of Atrial Fibrillation 2010 and Beyond
 Catheter Ablation for Treatment of Atrial Fibrillation 2010 and Beyond John M. Miller, MD Professor of Medicine Indiana University School of Medicine Director, Clinical Cardiac Electrophysiology Krannert
Catheter Ablation for Treatment of Atrial Fibrillation 2010 and Beyond John M. Miller, MD Professor of Medicine Indiana University School of Medicine Director, Clinical Cardiac Electrophysiology Krannert
Recent observations have focused attention on the PVs as a source of ectopic activity i determining i AF
 Atrial Fibrillation in 2010 Panos Vardas Professor of Cardiology President of EHRA Atrial Fibrillation Pathophysiology of AF Triggers Recent observations have focused attention on the PVs as a source of
Atrial Fibrillation in 2010 Panos Vardas Professor of Cardiology President of EHRA Atrial Fibrillation Pathophysiology of AF Triggers Recent observations have focused attention on the PVs as a source of
Atrial Fibrillation Cases. Dr Paul Broadhurst Consultant Cardiologist
 Atrial Fibrillation Cases Dr Paul Broadhurst Consultant Cardiologist November 2011 Mr TH age 72 Routine medical for hypertension check Denies any symptoms despite close questioning PMH: hypertension, MI,
Atrial Fibrillation Cases Dr Paul Broadhurst Consultant Cardiologist November 2011 Mr TH age 72 Routine medical for hypertension check Denies any symptoms despite close questioning PMH: hypertension, MI,
ABLATION OF CHRONIC AF
 ABLATION OF CHRONIC AF A PISAPIA ST JOSEPH HOSPITAL MARSEILLE MEET 2008 Atrial Fibrillation The most common significant heart rhythm disturbance Incidence increases with age and the development of structural
ABLATION OF CHRONIC AF A PISAPIA ST JOSEPH HOSPITAL MARSEILLE MEET 2008 Atrial Fibrillation The most common significant heart rhythm disturbance Incidence increases with age and the development of structural
What s new in my specialty?
 What s new in my specialty? Jon Melman, MD Heart Rhythm Specialists McKay-Dee Hospital some would say some would say my specialty 1 some would say my specialty First pacemaker 1958 some would say my specialty
What s new in my specialty? Jon Melman, MD Heart Rhythm Specialists McKay-Dee Hospital some would say some would say my specialty 1 some would say my specialty First pacemaker 1958 some would say my specialty
Atrial fibrillation and advanced age
 Atrial fibrillation and advanced age Prof. Fiorenzo Gaita Director of the Cardiology School University of Turin, Italy Prevalence of AF in the general population Prevalence and age distribution in patients
Atrial fibrillation and advanced age Prof. Fiorenzo Gaita Director of the Cardiology School University of Turin, Italy Prevalence of AF in the general population Prevalence and age distribution in patients
Current Management Strategies for Atrial Fibrillation
 Transcript Details This is a transcript of an educational program accessible on the ReachMD network. Details about the program and additional media formats for the program are accessible by visiting: https://reachmd.com/programs/medical-breakthroughs-from-penn-medicine/current-managementstrategies-for-atrial-fibrillation/3502/
Transcript Details This is a transcript of an educational program accessible on the ReachMD network. Details about the program and additional media formats for the program are accessible by visiting: https://reachmd.com/programs/medical-breakthroughs-from-penn-medicine/current-managementstrategies-for-atrial-fibrillation/3502/
Who Gets Atrial Fibrilla9on..?
 Birmingham October 20 th 2013 AFA Pa9ents Day Symptoma9c Atrial Fibrilla9on What therapies are available? GENERAL BACKGROUND Andrew Grace Papworth Hospital and University of Cambridge Consultant: Medtronic
Birmingham October 20 th 2013 AFA Pa9ents Day Symptoma9c Atrial Fibrilla9on What therapies are available? GENERAL BACKGROUND Andrew Grace Papworth Hospital and University of Cambridge Consultant: Medtronic
Atrial Fibrillation: It s More than a Rhythm
 Atrial Fibrillation: It s More than a Rhythm Relax and Learn at the Farm 2013 DNP, RN, CCNS, CCRN-CMC, CHFN Cardiovascular Nursing Education Associates 1 The Quality of a Person s Life is Directly Proportional
Atrial Fibrillation: It s More than a Rhythm Relax and Learn at the Farm 2013 DNP, RN, CCNS, CCRN-CMC, CHFN Cardiovascular Nursing Education Associates 1 The Quality of a Person s Life is Directly Proportional
Ruolo della ablazione della fibrillazione atriale nello scompenso cardiaco
 Ruolo della ablazione della fibrillazione atriale nello scompenso cardiaco Matteo Anselmino Division of Cardiology Città della Salute e della Scienza Hospital University of Turin, Italy Disclosure: Honoraria
Ruolo della ablazione della fibrillazione atriale nello scompenso cardiaco Matteo Anselmino Division of Cardiology Città della Salute e della Scienza Hospital University of Turin, Italy Disclosure: Honoraria
Atrial fibrillation (AF) is a disorder seen
 is a disorder seen") This Just In... An Update on Arrhythmia What do recent studies reveal about arrhythmia? In this article, the authors provide an update on atrial fibrillation and ventricular arrhythmia. Beth L. Abramson,
This Just In... An Update on Arrhythmia What do recent studies reveal about arrhythmia? In this article, the authors provide an update on atrial fibrillation and ventricular arrhythmia. Beth L. Abramson,
NEWLY DETECTED ATRIAL FIBRILLATION. Edgar S. Carell, M.D. Director, Vascular Medicine Clinic West Suburban Cardiology
 NEWLY DETECTED ATRIAL FIBRILLATION Edgar S. Carell, M.D. Director, Vascular Medicine Clinic West Suburban Cardiology 68 y/o woman complains of - generalized fatigue - mild DOE - never eats but keeps gaining
NEWLY DETECTED ATRIAL FIBRILLATION Edgar S. Carell, M.D. Director, Vascular Medicine Clinic West Suburban Cardiology 68 y/o woman complains of - generalized fatigue - mild DOE - never eats but keeps gaining
AF :RHYTHM CONTROL BY DR-MOHAMMED SALAH ASSISSTANT LECTURER CARDIOLOGY DEPARTMENT
 AF :RHYTHM CONTROL BY DR-MOHAMMED SALAH ASSISSTANT LECTURER CARDIOLOGY DEPARTMENT 5-2014 Atrial Fibrillation therapeutic Approach Rhythm Control Thromboembolism Prevention: Recommendations Direct-Current
AF :RHYTHM CONTROL BY DR-MOHAMMED SALAH ASSISSTANT LECTURER CARDIOLOGY DEPARTMENT 5-2014 Atrial Fibrillation therapeutic Approach Rhythm Control Thromboembolism Prevention: Recommendations Direct-Current
Supplementary Online Content
 Supplementary Online Content Morillo CA, Verma A, Connolly SJ, et al. Radiofrequency ablation vs antiarrhythmic drugs as first-line Treatment of Paroxysmal Atrial Fibrillation (RAAFT-2): a randomzied clinical
Supplementary Online Content Morillo CA, Verma A, Connolly SJ, et al. Radiofrequency ablation vs antiarrhythmic drugs as first-line Treatment of Paroxysmal Atrial Fibrillation (RAAFT-2): a randomzied clinical
Catheter Ablation for AF: Patients, Procedures, Outcomes
 Catheter Ablation for AF: Patients, Procedures, Outcomes John Sapp Director Heart Rhythm, QEII Health Sciences Centre Professor of Medicine, Dalhousie University Atrial Fibrillation Atrial Fibrillation
Catheter Ablation for AF: Patients, Procedures, Outcomes John Sapp Director Heart Rhythm, QEII Health Sciences Centre Professor of Medicine, Dalhousie University Atrial Fibrillation Atrial Fibrillation
Arrhythmias and Heart Failure Dr Chris Lang Consultant Cardiologist and Electrophysiologist Royal Infirmary of Edinburgh
 Arrhythmias and Heart Failure Dr Chris Lang Consultant Cardiologist and Electrophysiologist Royal Infirmary of Edinburgh Arrhythmias and Heart Failure Ventricular Supraventricular VT/VF Primary prevention
Arrhythmias and Heart Failure Dr Chris Lang Consultant Cardiologist and Electrophysiologist Royal Infirmary of Edinburgh Arrhythmias and Heart Failure Ventricular Supraventricular VT/VF Primary prevention
Atrial Fibrillation 2009
 Atrial Fibrillation 2009 Michael Glikson, MD Director of Pacing & Electrophysiology Leviev Heart Center Sheba medical Center Sheba Medical Center Tel Hashomer The Leviev Heart Center Rhythm vs rate control
Atrial Fibrillation 2009 Michael Glikson, MD Director of Pacing & Electrophysiology Leviev Heart Center Sheba medical Center Sheba Medical Center Tel Hashomer The Leviev Heart Center Rhythm vs rate control
Ablation Should Not Be Used as Primary Therapy for Treatment of Patients with Atrial Fibrillation
 Ablation Should Not Be Used as Primary Therapy for Treatment of Patients with Atrial Fibrillation 25 October 2008 Update in Electrocardiography and Arrhythmias Zian H. Tseng, M.D., M.A.S. Assistant Professor
Ablation Should Not Be Used as Primary Therapy for Treatment of Patients with Atrial Fibrillation 25 October 2008 Update in Electrocardiography and Arrhythmias Zian H. Tseng, M.D., M.A.S. Assistant Professor
Management strategies for atrial fibrillation Thursday, 20 October :27
 ALTHOUGH anyone who has had to run up a flight of steps or has had a frightening experience is quite familiar with a racing heartbeat, for the more than 2 million Americans who suffer from atrial fibrillation
ALTHOUGH anyone who has had to run up a flight of steps or has had a frightening experience is quite familiar with a racing heartbeat, for the more than 2 million Americans who suffer from atrial fibrillation
Practical Rate and Rhythm Management of Atrial Fibrillation
 Practical Rate and Rhythm Management of Atrial Fibrillation pocket guide UPDATED FEBRUARY 2013 Adapted from the ACCF/AHA/HRS 2011 Focused Updates Incorporated into the ACC/AHA/ESC Guidelines for the Management
Practical Rate and Rhythm Management of Atrial Fibrillation pocket guide UPDATED FEBRUARY 2013 Adapted from the ACCF/AHA/HRS 2011 Focused Updates Incorporated into the ACC/AHA/ESC Guidelines for the Management
Atrial Fibrillation Information for patients
 be informed about... Atrial Fibrillation Information for patients Atrial fibrillation (AF) is an abnormal heart rhythm. This pamphlet answers some questions you may have about AF, and gives an overview
be informed about... Atrial Fibrillation Information for patients Atrial fibrillation (AF) is an abnormal heart rhythm. This pamphlet answers some questions you may have about AF, and gives an overview
AF and arrhythmia management. Dr Rhys Beynon Consultant Cardiologist and Electrophysiologist University Hospital of North Staffordshire
 AF and arrhythmia management Dr Rhys Beynon Consultant Cardiologist and Electrophysiologist University Hospital of North Staffordshire Atrial fibrillation Paroxysmal AF recurrent AF (>2 episodes) that
AF and arrhythmia management Dr Rhys Beynon Consultant Cardiologist and Electrophysiologist University Hospital of North Staffordshire Atrial fibrillation Paroxysmal AF recurrent AF (>2 episodes) that
Atrial Fibrillation: Rate vs. Rhythm. Michael Curley, MD Cardiac Electrophysiology
 Atrial Fibrillation: Rate vs. Rhythm Michael Curley, MD Cardiac Electrophysiology I have no relevant financial disclosures pertaining to this topic. A Fib Epidemiology #1 Most common heart rhythm disturbance
Atrial Fibrillation: Rate vs. Rhythm Michael Curley, MD Cardiac Electrophysiology I have no relevant financial disclosures pertaining to this topic. A Fib Epidemiology #1 Most common heart rhythm disturbance
Atrial Fibrillation and Heart Failure: A Cause or a Consequence
 Atrial Fibrillation and Heart Failure: A Cause or a Consequence Rajat Deo, MD, MTR Assistant Professor of Medicine Division of Cardiology, Electrophysiology Section University of Pennsylvania November
Atrial Fibrillation and Heart Failure: A Cause or a Consequence Rajat Deo, MD, MTR Assistant Professor of Medicine Division of Cardiology, Electrophysiology Section University of Pennsylvania November
Innovations in AF Management
 Innovations in AF Management Barry Boilson MD PhD FRCPI boilson.barry@mayo.edu Disclosures Relevant None financial relationship(s) with industry None Off Label Usage None Overview Mechanisms of AF AF as
Innovations in AF Management Barry Boilson MD PhD FRCPI boilson.barry@mayo.edu Disclosures Relevant None financial relationship(s) with industry None Off Label Usage None Overview Mechanisms of AF AF as
ESC Stockholm Arrhythmias & pacing
 ESC Stockholm 2010 Take Home Messages for Practitioners Arrhythmias & pacing Prof. Panos E. Vardas Professor of Cardiology Heraklion University Hospital Crete, Greece Disclosures Small teaching fees from
ESC Stockholm 2010 Take Home Messages for Practitioners Arrhythmias & pacing Prof. Panos E. Vardas Professor of Cardiology Heraklion University Hospital Crete, Greece Disclosures Small teaching fees from
ECGs and Arrhythmias: Family Medicine Board Review 2012
 Overview ECGs and Arrhythmias: Family Medicine Board Review 2012 Jess Waldura, MD University of California, San Francisco walduraj@nccc.ucsf.edu Bundle branch blocks Quick review of ischemia Arrhythmias
Overview ECGs and Arrhythmias: Family Medicine Board Review 2012 Jess Waldura, MD University of California, San Francisco walduraj@nccc.ucsf.edu Bundle branch blocks Quick review of ischemia Arrhythmias
Practical Approaches to Atrial Fibrillation Management Answers to Your Everyday Questions
 Practical Approaches to Atrial Fibrillation Management Answers to Your Everyday Questions H. Mark Guo, MD, FACC, FHRS Clinical Cardiac Electrophysiology Oregon Heart & Vascular Institute hguo@peacehealth.org
Practical Approaches to Atrial Fibrillation Management Answers to Your Everyday Questions H. Mark Guo, MD, FACC, FHRS Clinical Cardiac Electrophysiology Oregon Heart & Vascular Institute hguo@peacehealth.org
Cardiac Arrhythmias. Cathy Percival, RN, FALU, FLMI VP, Medical Director AIG Life and Retirement Company
 Cardiac Arrhythmias Cathy Percival, RN, FALU, FLMI VP, Medical Director AIG Life and Retirement Company The Cardiovascular System Three primary functions Transport of oxygen, nutrients, and hormones to
Cardiac Arrhythmias Cathy Percival, RN, FALU, FLMI VP, Medical Director AIG Life and Retirement Company The Cardiovascular System Three primary functions Transport of oxygen, nutrients, and hormones to
Dr Chris Ellis. Consultant Cardiologist Auckland City Hospital Auckland
 Dr Chris Ellis Consultant Cardiologist Auckland City Hospital Auckland 8:30-9:25 WS #189: Anticoagulation in AF 9:35-10:30 WS #201: Anticoagulation in AF (Repeated) Anticoagulation in Atrial Fibrillation
Dr Chris Ellis Consultant Cardiologist Auckland City Hospital Auckland 8:30-9:25 WS #189: Anticoagulation in AF 9:35-10:30 WS #201: Anticoagulation in AF (Repeated) Anticoagulation in Atrial Fibrillation
Long-Term Outcome and Risks of Catheter Ablation for Atrial Fibrillation
 Long-Term Outcome and Risks of Catheter Ablation for Atrial Fibrillation Carlo Pappone, MD, PhD, FACC EP Director, Villa Maria Hospital Group How many times AF can increase mortality DO MORTALITY REALLY
Long-Term Outcome and Risks of Catheter Ablation for Atrial Fibrillation Carlo Pappone, MD, PhD, FACC EP Director, Villa Maria Hospital Group How many times AF can increase mortality DO MORTALITY REALLY
Rate or Rhythm Control? Epidemiology. Relevant Advances in Atrial Fibrillation 6/20/2011. Stroke Prophylaxis
 Relevant Advances in Atrial Fibrillation Stroke Prophylaxis Managing Atrial Fibrillation: Tips for the Generalist Antiarrhythmic Drug Therapy Ablation Gregory M Marcus, MD, MAS Assistant Professor of Medicine
Relevant Advances in Atrial Fibrillation Stroke Prophylaxis Managing Atrial Fibrillation: Tips for the Generalist Antiarrhythmic Drug Therapy Ablation Gregory M Marcus, MD, MAS Assistant Professor of Medicine
Case #1. 73 y/o man with h/o HTN and CHF admitted with dizziness and SOB Treated for CHF exacerbation with Lasix Now HR 136
 Tachycardias Case #1 73 y/o man with h/o HTN and CHF admitted with dizziness and SOB Treated for CHF exacerbation with Lasix Now HR 136 Initial Assessment Check Telemetry screen if pt on tele Telemetry
Tachycardias Case #1 73 y/o man with h/o HTN and CHF admitted with dizziness and SOB Treated for CHF exacerbation with Lasix Now HR 136 Initial Assessment Check Telemetry screen if pt on tele Telemetry
Rhythm Control: Is There a Role for the PCP? Blake Norris, MD, FACC BHHI Primary Care Symposium February 28, 2014
 Rhythm Control: Is There a Role for the PCP? Blake Norris, MD, FACC BHHI Primary Care Symposium February 28, 2014 Financial disclosures Consultant Medtronic 3 reasons to evaluate and treat arrhythmias
Rhythm Control: Is There a Role for the PCP? Blake Norris, MD, FACC BHHI Primary Care Symposium February 28, 2014 Financial disclosures Consultant Medtronic 3 reasons to evaluate and treat arrhythmias
Dronedarone: Need to Perform a CV Outcome Safety Study
 Dronedarone: Need to Perform a CV Outcome Safety Study Gerald V. Naccarelli M.D. Consultant: Glaxo-Smith-Kline, Pfizer, Sanofi, Boehringer-Ingelheim, Daiichi-Sankyo, Bristol Myers Squibb, Otsuka, Janssen
Dronedarone: Need to Perform a CV Outcome Safety Study Gerald V. Naccarelli M.D. Consultant: Glaxo-Smith-Kline, Pfizer, Sanofi, Boehringer-Ingelheim, Daiichi-Sankyo, Bristol Myers Squibb, Otsuka, Janssen
Arrhythmia 341. Ahmad Hersi Professor of Cardiology KSU
 Arrhythmia 341 Ahmad Hersi Professor of Cardiology KSU Objectives Epidemiology and Mechanisms of AF Evaluation of AF patients Classification of AF Treatment and Risk stratification of AF Identify other
Arrhythmia 341 Ahmad Hersi Professor of Cardiology KSU Objectives Epidemiology and Mechanisms of AF Evaluation of AF patients Classification of AF Treatment and Risk stratification of AF Identify other
Samer Nasr, M.D. Mount Lebanon Hospital.
 Samer Nasr, M.D. Mount Lebanon Hospital. Lone atrial fibrillation: Younger than 60 years old. No clinical or echo evidence of cardiopulmonary disease. Favorable prognosis. Thromboembolism usually not
Samer Nasr, M.D. Mount Lebanon Hospital. Lone atrial fibrillation: Younger than 60 years old. No clinical or echo evidence of cardiopulmonary disease. Favorable prognosis. Thromboembolism usually not
Medical management of AF: drugs for rate and rhythm control
 Medical management of AF: drugs for rate and rhythm control Adel Khalifa Sultan Hamad, BMS, MD, FGHRS, FRCP(Canada) Consultant Cardiologist & Interventional Cardiac Electrophysiologist Head of Electrophysiology
Medical management of AF: drugs for rate and rhythm control Adel Khalifa Sultan Hamad, BMS, MD, FGHRS, FRCP(Canada) Consultant Cardiologist & Interventional Cardiac Electrophysiologist Head of Electrophysiology
Scompenso cardiaco e F A : ruolo della ablazione transcatetere. Prof. Fiorenzo Gaita
 Scompenso cardiaco e F A : ruolo della ablazione transcatetere Prof. Fiorenzo Gaita Patients with atrial fibrillation (%) Prevalence of AF in HF Trials 60 50 30% NYHA III-IV NYHA IV 40 NYHA II-III 30 20
Scompenso cardiaco e F A : ruolo della ablazione transcatetere Prof. Fiorenzo Gaita Patients with atrial fibrillation (%) Prevalence of AF in HF Trials 60 50 30% NYHA III-IV NYHA IV 40 NYHA II-III 30 20
Atrial Fibrillation. Ivan Anderson, MD RIHVH Cardiology
 Atrial Fibrillation Ivan Anderson, MD RIHVH Cardiology Outline Definition and Pathophysiology Rate versus rhythm control Rate control thresholds (how much is enough) Anti-coagulation CHADS2VASc score HASBLED
Atrial Fibrillation Ivan Anderson, MD RIHVH Cardiology Outline Definition and Pathophysiology Rate versus rhythm control Rate control thresholds (how much is enough) Anti-coagulation CHADS2VASc score HASBLED
Dos and Don t in Cardiac Arrhythmia. Case 1 -ECG. Case 1. Management. Emergency Admissions. Reduction of TE risk -CHADS 2 score. Hospital Admissions
 Emergency Admissions Dos and Don t in Cardiac Arrhythmia Tom Wong, MD, FESC Consultant Cardiologist, Honorary Senior Lecturer Royal Brompton & Harefield Hospitals National Heart and Lung Institute, Imperial
Emergency Admissions Dos and Don t in Cardiac Arrhythmia Tom Wong, MD, FESC Consultant Cardiologist, Honorary Senior Lecturer Royal Brompton & Harefield Hospitals National Heart and Lung Institute, Imperial
Anti arrhythmic drugs. Hilal Al Saffar College of medicine Baghdad University
 Anti arrhythmic drugs Hilal Al Saffar College of medicine Baghdad University Mechanism of Arrhythmia Abnormal heart pulse formation Abnormal heart pulse conduction Classification of Arrhythmia Abnormal
Anti arrhythmic drugs Hilal Al Saffar College of medicine Baghdad University Mechanism of Arrhythmia Abnormal heart pulse formation Abnormal heart pulse conduction Classification of Arrhythmia Abnormal
Half Moon Bay Treatment of Atrial Fibrillation. Dr. Roger A. Winkle MD. Silicon Valley Cardiology, PAMF, Sutter Health Sequoia Hospital
 Half Moon Bay 2018 Treatment of Atrial Fibrillation Dr. Roger A. Winkle MD Silicon Valley Cardiology, PAMF, Sutter Health Sequoia Hospital Disclosures: Investor Farapulse Things a Primary Care Doctor Should
Half Moon Bay 2018 Treatment of Atrial Fibrillation Dr. Roger A. Winkle MD Silicon Valley Cardiology, PAMF, Sutter Health Sequoia Hospital Disclosures: Investor Farapulse Things a Primary Care Doctor Should
Atrial fibrillation: current approaches to management
 DRUG REVIEW n Atrial fibrillation: current approaches to management Upasana Tayal MA, MRCP and Robert Greenbaum BSc, MD, FRCP, FESC, FACC Atrial fibrillation is the commonest arrhythmia and GPs have an
DRUG REVIEW n Atrial fibrillation: current approaches to management Upasana Tayal MA, MRCP and Robert Greenbaum BSc, MD, FRCP, FESC, FACC Atrial fibrillation is the commonest arrhythmia and GPs have an
Atrial Fibrillation 10/2/2018. Depolarization & ECG. Atrial Fibrillation. Hemodynamic Consequences
 Depolarization & ECG Atrial Fibrillation How to make ORDER out of CHAOS Julia Shih, VMD, DACVIM (Cardiology) October 27, 2018 Depolarization & ECG Depolarization & ECG Atrial Fibrillation Hemodynamic Consequences
Depolarization & ECG Atrial Fibrillation How to make ORDER out of CHAOS Julia Shih, VMD, DACVIM (Cardiology) October 27, 2018 Depolarization & ECG Depolarization & ECG Atrial Fibrillation Hemodynamic Consequences
Conflicts of Interests
 Advances in the Management of Atrial Fibrillation State of the Art in 2013 Overview of AF Stroke risk and anticoagulation Rate control Antiarrhythmic Drug Therapy Catheter ablation Conclusion Hugh Calkins
Advances in the Management of Atrial Fibrillation State of the Art in 2013 Overview of AF Stroke risk and anticoagulation Rate control Antiarrhythmic Drug Therapy Catheter ablation Conclusion Hugh Calkins
Atrial Fibrillation and Common Supraventricular Tachycardias. Sunil Kapur MD
 Atrial Fibrillation and Common Supraventricular Tachycardias Sunil Kapur MD Cardiac Electrophysiology Brigham and Women s Hospital Instructor, Harvard Medical School No disclosures Cardiac Conduction:
Atrial Fibrillation and Common Supraventricular Tachycardias Sunil Kapur MD Cardiac Electrophysiology Brigham and Women s Hospital Instructor, Harvard Medical School No disclosures Cardiac Conduction:
Treating Atrial Fibrillation. Richard Schilling. St Bartholomew's Hospital, Queen Mary s University of London
 Treating Atrial Fibrillation Richard Schilling St Bartholomew's Hospital, Queen Mary s University of London AF burden Framingham Lifetime risk of developing AF = 25% Mortality: SMR =1.9 1.5 NHS audit 1%
Treating Atrial Fibrillation Richard Schilling St Bartholomew's Hospital, Queen Mary s University of London AF burden Framingham Lifetime risk of developing AF = 25% Mortality: SMR =1.9 1.5 NHS audit 1%
Catheter Ablation: Atrial fibrillation (AF) is the most common. Another Option for AF FAQ. Who performs ablation for treatment of AF?
 is the most common. Another Option for AF FAQ. Who performs ablation for treatment of AF?") : Another Option for AF Atrial fibrillation (AF) is a highly common cardiac arrhythmia and a major risk factor for stroke. In this article, Dr. Khan and Dr. Skanes detail how catheter ablation significantly
: Another Option for AF Atrial fibrillation (AF) is a highly common cardiac arrhythmia and a major risk factor for stroke. In this article, Dr. Khan and Dr. Skanes detail how catheter ablation significantly
CVD: Cardiac Arrhythmias. 1. Final Cardiac Arrhythmias_BMP. 1.1 Cardiovascular Disease. Notes:
 CVD: Cardiac Arrhythmias 1. Final Cardiac Arrhythmias_BMP 1.1 Cardiovascular Disease 1.2 Directions for taking this course 1.3 Content Experts 1.4 Disclosures 1.5 Accreditation Information 1.6 Learning
CVD: Cardiac Arrhythmias 1. Final Cardiac Arrhythmias_BMP 1.1 Cardiovascular Disease 1.2 Directions for taking this course 1.3 Content Experts 1.4 Disclosures 1.5 Accreditation Information 1.6 Learning
Catheter Ablation for Atrial Fibrillation: Patient Selection and Outcomes
 Catheter Ablation for Atrial Fibrillation: Patient Selection and Outcomes Francis Marchlinski, MD Richard T and Angela Clark President s Distinguished Professor Director Cardiac Electrophysiolgy University
Catheter Ablation for Atrial Fibrillation: Patient Selection and Outcomes Francis Marchlinski, MD Richard T and Angela Clark President s Distinguished Professor Director Cardiac Electrophysiolgy University
Is cardioversion old hat? What is new in interventional treatment of AF symptoms?
 Is cardioversion old hat? What is new in interventional treatment of AF symptoms? Joseph de Bono Consultant Electrophysiologist University Hospitals Birmingham Atrial Fibrillation (AF) Affects 2% of the
Is cardioversion old hat? What is new in interventional treatment of AF symptoms? Joseph de Bono Consultant Electrophysiologist University Hospitals Birmingham Atrial Fibrillation (AF) Affects 2% of the
Congestive Heart Failure or Heart Failure
 Congestive Heart Failure or Heart Failure Dr Hitesh Patel Ascot Cardiology Group Heart Failure Workshop April, 2014 Question One What is the difference between congestive heart failure and heart failure?
Congestive Heart Failure or Heart Failure Dr Hitesh Patel Ascot Cardiology Group Heart Failure Workshop April, 2014 Question One What is the difference between congestive heart failure and heart failure?
Atrial Fibrillation Ablation Recent Clinical Trials That Changed (or not) My Practice
 My Practice") Atrial Fibrillation Ablation Recent Clinical Trials That Changed (or not) My Practice Walid Saliba, MD, FHRS Director, Atrial Fibrillation Center Director EP laboratory Heart and Vascular Institute Cleveland
Atrial Fibrillation Ablation Recent Clinical Trials That Changed (or not) My Practice Walid Saliba, MD, FHRS Director, Atrial Fibrillation Center Director EP laboratory Heart and Vascular Institute Cleveland
The pill-in-the-pocket strategy for paroxysmal atrial fibrillation
 The pill-in-the-pocket strategy for paroxysmal atrial fibrillation KONSTANTINOS P. LETSAS, MD, FEHRA LABORATORY OF CARDIAC ELECTROPHYSIOLOGY EVANGELISMOS GENERAL HOSPITAL OF ATHENS ARRHYTHMIAS UPDATE,
The pill-in-the-pocket strategy for paroxysmal atrial fibrillation KONSTANTINOS P. LETSAS, MD, FEHRA LABORATORY OF CARDIAC ELECTROPHYSIOLOGY EVANGELISMOS GENERAL HOSPITAL OF ATHENS ARRHYTHMIAS UPDATE,
Use of Antiarrhythmic Drugs for AF Who, What and How? Dr. Marc Cheng Queen Elizabeth Hospital
 Use of Antiarrhythmic Drugs for AF Who, What and How? Dr. Marc Cheng Queen Elizabeth Hospital Content i. Rhythm versus Rate control ii. Anti-arrhythmic for Rhythm Control iii. Anti-arrhythmic for Rate
Use of Antiarrhythmic Drugs for AF Who, What and How? Dr. Marc Cheng Queen Elizabeth Hospital Content i. Rhythm versus Rate control ii. Anti-arrhythmic for Rhythm Control iii. Anti-arrhythmic for Rate
Modest Medtronic. Modest Boehringer Ingelheim
 Adults With AF (millions) Modest Medtronic Modest Boehringer Ingelheim Changing Modalities of Care for Atrial Fibrillation Jill Repoley MSN, CRNP, CCDS, CEPS, FHRS 7 6 5 4 3 2 1 2.08 2.26 2.44 2.66 2.94
Adults With AF (millions) Modest Medtronic Modest Boehringer Ingelheim Changing Modalities of Care for Atrial Fibrillation Jill Repoley MSN, CRNP, CCDS, CEPS, FHRS 7 6 5 4 3 2 1 2.08 2.26 2.44 2.66 2.94
Saudi Heart Association February 22, 2011
 Pharmacological Therapy of Atrial Fibrillation: Recent Advances Dr Martin Green Professor of Medicine (Cardiology) University of Ottawa Saudi Heart Association February 22, 2011 Atrial Fibrillation Drugs
Pharmacological Therapy of Atrial Fibrillation: Recent Advances Dr Martin Green Professor of Medicine (Cardiology) University of Ottawa Saudi Heart Association February 22, 2011 Atrial Fibrillation Drugs
MANAGING ATRIAL FIBRILLATION: BEYOND ANTICOAGULATION December 9, 2017
 MANAGING ATRIAL FIBRILLATION: BEYOND ANTICOAGULATION December 9, 2017 1 Faculty Disclosure Faculty: Peter Leong-Sit MSc, MD, FRCPC, FHRS Associate Professor, Western University Cardiologist, London Heart
MANAGING ATRIAL FIBRILLATION: BEYOND ANTICOAGULATION December 9, 2017 1 Faculty Disclosure Faculty: Peter Leong-Sit MSc, MD, FRCPC, FHRS Associate Professor, Western University Cardiologist, London Heart
Stuart Beldner, MD, FHRS Assistant Professor NSLIJ Hofstra School of Med
 Stuart Beldner, MD, FHRS Assistant Professor NSLIJ Hofstra School of Med None There s no reason to panic. While it is true that one of the crew members is ill, slightly. Absence of discrete P waves Chaotic
Stuart Beldner, MD, FHRS Assistant Professor NSLIJ Hofstra School of Med None There s no reason to panic. While it is true that one of the crew members is ill, slightly. Absence of discrete P waves Chaotic
Update in the Management of Atrial Fibrillation
 Update in the Management of Atrial Fibrillation Gregory M Marcus, MD, MAS Associate Professor of Medicine Division of Cardiology University of California, San Francisco Disclosures Research: Gilead, Medtronic,
Update in the Management of Atrial Fibrillation Gregory M Marcus, MD, MAS Associate Professor of Medicine Division of Cardiology University of California, San Francisco Disclosures Research: Gilead, Medtronic,
Arrhythmias (I) Supraventricular Tachycardias. Disclosures
 Supraventricular Tachycardias. Disclosures") Arrhythmias (I) Supraventricular Tachycardias Amy Leigh Miller, MD, PhD Cardiovascular Electrophysiology, Brigham & Women s Hospital Disclosures None Short R-P Tachycardia REGULAR with 1:1 P/R relationship
Arrhythmias (I) Supraventricular Tachycardias Amy Leigh Miller, MD, PhD Cardiovascular Electrophysiology, Brigham & Women s Hospital Disclosures None Short R-P Tachycardia REGULAR with 1:1 P/R relationship
Atrial Fibrillation New Approaches, Techniques, and Technology
 New Cardiovascular Horizons 2015 May 28, 2015 New Orleans, Louisiana Atrial Fibrillation New Approaches, Techniques, and Technology State of the Art - - 2015 Richard Abben, M D Director, Cardiac Arrhythmia
New Cardiovascular Horizons 2015 May 28, 2015 New Orleans, Louisiana Atrial Fibrillation New Approaches, Techniques, and Technology State of the Art - - 2015 Richard Abben, M D Director, Cardiac Arrhythmia
Ectopic Atrial Tachycardia
 Europace Madrid, 26-29 June 2011 Ectopic Atrial Tachycardia P. Loh, MD, PhD University of Utrecht Division Heart & Lungs Epidemiology Nonsustained atrial tachycardia Frequent finding on holter registrations
Europace Madrid, 26-29 June 2011 Ectopic Atrial Tachycardia P. Loh, MD, PhD University of Utrecht Division Heart & Lungs Epidemiology Nonsustained atrial tachycardia Frequent finding on holter registrations
Pediatrics. Arrhythmias in Children: Bradycardia and Tachycardia Diagnosis and Treatment. Overview
 Pediatrics Arrhythmias in Children: Bradycardia and Tachycardia Diagnosis and Treatment See online here The most common form of cardiac arrhythmia in children is sinus tachycardia which can be caused by
Pediatrics Arrhythmias in Children: Bradycardia and Tachycardia Diagnosis and Treatment See online here The most common form of cardiac arrhythmia in children is sinus tachycardia which can be caused by