Life Threatening EKG s In the Toxicology Patient
|
|
|
- Anastasia Parks
- 5 years ago
- Views:
Transcription

1 Life Threatening EKG s In the Toxicology Patient Dean Olsen, DO Faculty, New York City Poison Control Center Director Emergency Medicine Residency Nassau University Medical Center Assistant Professor Pharmacology, Toxicology New York College of Osteopathic Medicine
2 Disclosure I have no financial or academic conflicts of interest.
3 Objectives Review 5 life threating arrythmias seen in poisoning Learn the characteristics that distinguish these from other common arrythmias encountered in the emergency department Learn the pathophysiology behind these arrythmias Develop a treatment plan based on current literature and/or mechanistic principals 3
4 Disclaimer There is very little literature to guide us RCT- none Case series- few Case reports- many- most bad! Animal studies- Few Much of this is based on theory, extrapolation and opinion 4
5 Concept: Resist the urge to shock these Arrythmias
6 Peri-mortem Gestures Lipid emulsion therapy Used for bupivacaine toxicity Lots of case reports and animal studies for other drugs Mechanism Lipid sink Free fatty acid substrate Increase viscosity Dose: 20% Lipid emulsion: 1.5 ml/kg then 0.25 ml/kg/min (may double) Methylene Blue Nitrate scavenger Causes vasoconstriction May increase blood pressure Dose: 1-2 mg/kg IV 6

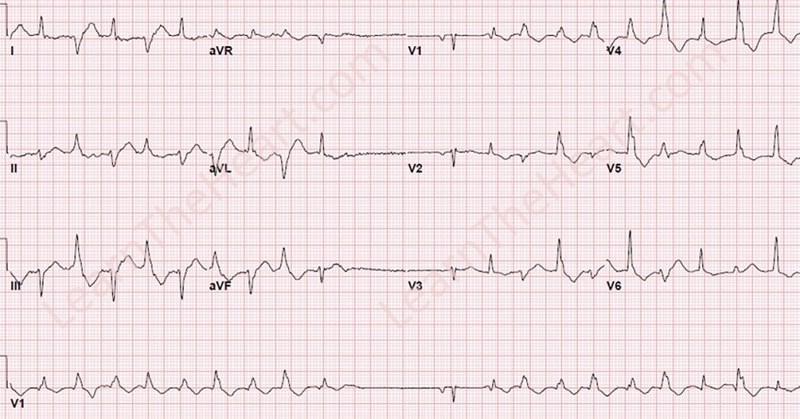
7 Arrythmia 1 7
8 Case 1 27 Year old female BIBEMS agitated diaphoretic found on the street Witnesses report patient acting bizarre and agitated on street 8
9 Vital Signs Blood pressure 180/110 Heart rate 170 Respirations 36 Temperature Extremely agitated and diaphoretic 9
10 Emergency Department Course Cardiac monitor, oxygen, IV access and blood drawn Lorazepam 2mg IV EKG obtained 10
11 What is the cause? Patient admits to cocaine use prior to being picked up by EMS What is the treatment for this patients Arrhythmia? Sodium bicarbonate 1-2meq/kg bolus 11

12 Sodium Channel Blockade 12
13 Cocaine Cocaine induced wide complex tachycardia From sodium channel blockade (similar to TCA) Sinus tachycardia that s aberrantly conducted Usually associated with acidosis Does not respond to electricity 13
14 Cocaine Sodium Channel Blockade Treatment: 1. Sedation with benzodiazepines 2. Sodium bicarbonate 3. Lidocaine 4. Amiodarone? 5. Intralipid?? Avoid Type 1A antidysrhythmics Beta blockers Epinephrine

15 15
16 Parker RB et al: Comparative effects of sodium bicarbonate and sodium chloride on reversing cocaine-induced changes in the electrocardiogram J Cardiovasc Pharmacol Dec;34(6):864-9 Dog model used Randomized to treatment of NS vs NaHCO3 HaHCO3 superior in reversal of arrhythmia Reversal of arrhythmia associated with reversal of acidosis 16

17 Literature review Highlights the data on using NaHCO3 above Lidocaine in the treatment of cocaine induced wide complex tachycardia 17

18 18
19 Lange et al: Annals Internal Med, 1990 June 15; 112 (12) Randomized double blind placebo controlled study Patients administered cocaine on cath table Randomized to beta blocker vs placebo Statistically significant decrease in coronary artery diameter 19
20 Sodium Channel Blockade 20
21 Case 47 year old female took an overdose in a suicide attempt Patient arrives in the ED obtunded and has a witnessed generalized tonic-clonic seizure Vitals P 140 BP 90/60 R 12 T 99.3 Skin: dry Pupils: 6mm not reactive; absent bowel sounds 21
22 Case What is the most likely cause of this patients clinical condition? A. Cocaine B. TCA C. Digoxin D. Zoloft E. Anxiety The patients parents bring in an empty bottle of amitriptyline 22
23 Case The best initial treatment for this patent is? A. Procainamide B. Lidocaine C. Beta blocker D. Sodium bicarbonate 23
24 Case The patient receives NaHCO3 and the ECG improves ph 7.6 and ECG QRS widens to 155ms; Management? Lidocaine Procainamide Hypertonic saline Amiodarone
25 Case report of alkalemic patient with wide QRS that improved with hypertonic saline 7.7% NaCl IV bolus
26 Sodium Channel Blockers Common TCA Quinidine Propafenone Mexiletine Disopyramide Chloroquine Not So Common Procainamide Flecanide Uncommon Sedating H1 blockers Carbamazepine Cocaine Cyclobenzaprine 26
27 TCA 27

28 28
29 29

30
31 Tricyclic Antidepressants Treatment Arrhythmia Does not respond to electricity Sodium bicarbonate 1-2 meq/kg IV bolus Hypertonic saline Lidocaine / amiodarone? Seizures Benzodiazepines Paralyze if needed Intubate / Hyperventilate ph
32 Tricyclic Antidepressants What not to do Procainamide Quinidine Dilantin Beta blockers 32

33 Arrythmia 2 33
34 Case 2 35 year old male s/p overdose HR 35 BP 50s systolic Normal mental status Skin cool, diaphoretic No purposeful movement EKG obtained 34
35 Case 2 Patient found in vicinity of open bottles of atenolol and verapamil 35
36 Beta and Calcium Channel Blockers 2 sets of problems that may or may not be inter-related Bradycardia Improved rate may not translate to improved perfusion Many patients tolerate rates in the 30 s Hypotension Is it rate or contractility? 36
37 Beta and Calcium Channel Blockers Hypotension associated with beta and calcium channel blockers Drug induced cardiogenic shock Ultimate problem is decrease in intracellular calcium Switching of metabolism of myocardium from fatty acids to glucose for fuel 37
38 BETA-BLOCKER β1 Agonist 1 receptor 5 AMP ATP Adenylate cyclase G s protein Ca ++ PDE c-amp protein kinase A L-type voltagesensitive calcium channels Ca ++ Ca ++ Actin-myosin complex Myocardial Cell Sarcoplasmic reticulum Ca ++ CALCIUM CHANNEL BLOCKER 38
39 5 AMP ATP glucagon Adenylate cyclase 1 receptor G s protein catecholamines Calcium channel Ca ++ Ca ++ PDE Ca ++ c-amp protein kinase A Ca ++ Ca ++ Sarcoplasmic reticulum Ca ++ Ca ++ amrinone Actin-myosin complex High dose insulin and glucose Ca ++ 39
40 Beta and Calcium Channel Blockers Treatment 1. Vasopressors 2. Calcium 3. Glucagon 4. High dose insulin therapy 5. Amrinone 6. Intralipid Therapy 7. Bypass, ECHMO or IABP 40
41 Euglycemic Insulin Therapy Rational Myocardial cells normally use primarily fatty acids for metabolism Calcium channel blockers cause myocardial cells to become carbohydrate dependent At the same time CCB s also inhibit the ability of myocardial cells to use these carbohydrates by inhibiting insulin release and increasing myocardial resistance to insulin Decrease substrate delivery to myocardium through decreased blood flow further worsens contractility 41


42 42

43 Euglycemic Insulin Therapy Dose 1u/kg bolus Higher doses may be of benefit 43
44 Euglycemic Insulin Therapy 1u/kg/h infusion Dextrose infusion to keep serum glucose normal Titrate drip as high as possible with keeping serum glucose normal 44

45 Arrythmia 3 45
46 Case 3 16 year old male presents with history of taking grandmothers heart medication in suicide attempt Presents with alteration in color perception confusion and vomiting Intubated for agitation and confusion HR 45 regular BP 120/70 ECG 46
47
48 Case 3 Over the next 30 minutes the patient began to have multiform PVCs that degenerate to ventricular fibrillation No response to defib x 3 Diagnosis and treatment? A. Calcium channel blocker OD; give pressors B. ACE inhibitor OD; standard ACLS C. Diuretic OD; give fluids and ACLS D. Digoxin OD; give Digibind 48



49 Cardiac Glycosides Prior to Digibind survival following cardiac arrest was almost 0 (Bismuth) 49
50 In the multi-center study of Digibind survival for cardiac arrest patients was 54% Most other causes result in 10% or less The most treatable cause of arrest?? 50
51 Na-Ca Exchanger Na-K ATPase 3Na + 2K + K + Voltage sensitive potassium channel Ca ++ 3Na + Na + Voltage sensitive sodium channel Ca ++ Ca ++ Sarcoplasmic reticulum Actin-myosin complex Myocardial Repolarization L-type voltagesensitive calcium channel 51
52 Na-Ca Exchanger 3Na + Na-K ATPase 2K + K + Cardiac Glycosides Voltage sensitive potassium channel Ca ++ 3Na + Na + Voltage sensitive sodium channel Ca ++ Ca ++ Sarcoplasmic reticulum Actin-myosin complex Myocardial Repolarization L-type voltagesensitive calcium channel 52
53 Na-Ca Exchanger 3Na + Na-K ATPase 2K + K + Cardiac Glycosides Voltage sensitive potassium channel Ca ++ 3Na + Na + Ca ++ Voltage sensitive sodium channel Ca ++ Sarcoplasmic reticulum Actin-myosin complex Myocardial Repolarization L-type voltagesensitive calcium channel 53
54 Na-Ca Exchanger K+ K+ K+ Na-K ATPase K+ K+ Increased extracellular K+ K+ K+ Ca ++ Actin-myosin complex Ca++ Ca++ Sarcoplasmic Reticulum Ca++ Ca++ Ca++ Ca++ Ca++ K+ More Ca++ Available for contraction 54
55 Cardiac Glycosides Additional Therapeutic Effects Increased vagal tone Decreased SA node firing Decreased AV node conduction 55
56 Toxic Effects Vagal stimulation sinus bradycardia/arrest, PR prolongation, nodal blocks Increased intracellular Ca++ automaticity Increased resting membrane potential Increased delayed after-depolarization's Overall Slowing of normal conduction Increased atrial, AV node, and ventricular ectopy 56
57 Effect Of Digitalis OD On Resting Membrane Potential Phase 1 0mv Phase 2 Depolarization Threshold -65mv Phase 0 Phase 3-90mv Resting Membrane Potential Digitalis OD Myocardial Cell Action Potential Phase 4 57

58
59 Digoxin immune Fab Treatment Digibind Antibody to digitalis DO NOT PACE THESE PATIENTS!!! Recommended dose : 20 vials in cardiac arrest Equimolar neutralization is goal (not based on weight) More may not be better Not enough is bad Case reports of patients responding to Digibind post cardiac arrest 59
60 Electricity Digoxin toxicity decreases fibrillation threshold Normal digoxin levels do not appear to do this Consider Digibind or antidysrhythmic before cardioversion 60
61 Arrythmia 4 ame ent rate e 00 PC 5 urations Acct P OB 3 y ear s Mal e S Othe r ech 5 5 m 00 nterv als Sub ectiv e Sy mptom Other specif ied sy mptoms and P si ns inv olv in the O circulatory P O S AC a Contact Pa er 00 5 Conf irmin M c 0 Order M Med Med d A es P ept C nst u ealt h S 3 ate 0 0 ime Speed 5 mm s imb ead ain 0 0 mm m Chest ead ain 0 0 mm m ilters s otch 0 Artif act 00 Stable Of f a a 5 a 3 CO M 5 3 c od es Pa e of
62 Case A 31-year-old male with a history of opioid abuse was brought to the ED after being unresponsive at home Naloxone was given in route HR 103, R 24, BP 140/101, T 37.1 Pt is diaphoretic in the ED

63
64 Loperamide (Imodium) Devoid of opioid effects at therapeutic doses (<16mg/day) When taken in large does can cause opioid effects Used to treat withdrawal Used as an agent of abuse in absence of opioids Sodium channel blockade Potassium channel blockade
65
66
67 After some a CO3 and M

68
69 Loperamide Treatment Probably will not respond to electricity Naloxone for respiratory depression Sodium bicarbonate Magnesium for qt prolongation

70 Arrythmia 5
71 Case A 55 year old male presents with oral numbness and chest pain after ingesting a plant he thought was ground elder from a private garden about 45 minutes prior The patient goes in to cardiac arrest shortly after arrival and is defibrated

72

73 Case His wife arrives with the plant Aconitum napellus Monkshood Aconite Wolf's bane Devils helmet
74 Aconite Sodium Channel activation Myocardium Nerve Delayed after-depolarization Early after-depolarization Prolonged sodium influx Wide complex dysrhythmias with ectopy
75 Aconite Treatment Does not respond to electricity Amiodarone Flecainide Lidocane Procainamide
76 Summary Wide complex tachycardia without ectopy in poisoned patient Think sodium channel blockade Cocaine TCA Sedating H1 blockers Loperamide (Imodium) Treatment NaHCO3 Hypertonic saline Amiodarone? Wide complex tachycardia with ectopy Sodium channel opener Aconite Treatment Class 1 antidysrhythmics
77 Summary Bradycardia with blocks and hypotension Calcium channel blocker or beta blocker Treatment Insulin Ca+ Glucagon Inotropic agents Bradycardia with or without ectopy with normal or high BP Digoxin Plant cardioactive steroid Treatment Digabind on t pace

78 Questions? 78
Cardiotoxic Medications
 Cardiotoxic Medications Dean Olsen, DO Faculty, New York City Poison Control Center Director Emergency Medicine Residency Nassau University Medical Center Assistant Professor Pharmacology, Toxicology New
Cardiotoxic Medications Dean Olsen, DO Faculty, New York City Poison Control Center Director Emergency Medicine Residency Nassau University Medical Center Assistant Professor Pharmacology, Toxicology New
Chapter 9. Learning Objectives. Learning Objectives 9/11/2012. Cardiac Arrhythmias. Define electrical therapy
 Chapter 9 Cardiac Arrhythmias Learning Objectives Define electrical therapy Explain why electrical therapy is preferred initial therapy over drug administration for cardiac arrest and some arrhythmias
Chapter 9 Cardiac Arrhythmias Learning Objectives Define electrical therapy Explain why electrical therapy is preferred initial therapy over drug administration for cardiac arrest and some arrhythmias
The Hypotensive Poisoned Patient. Robert S. Hoffman, MD Director, NYC PCC
 The Hypotensive Poisoned Patient Robert S. Hoffman, MD Director, NYC PCC Some Definitions Hypotension = Low blood pressure Failure of macrocirculation Shock = Poor tissue perfusion Failure of microcirculation
The Hypotensive Poisoned Patient Robert S. Hoffman, MD Director, NYC PCC Some Definitions Hypotension = Low blood pressure Failure of macrocirculation Shock = Poor tissue perfusion Failure of microcirculation
EM Cases Course 2017 Toxicology Module
 EM Cases Course 2017 Toxicology Module quick IV access and diazepam is administered. The seizure stops. The first set of vitals show: HR 30bpm, BP 70/40. His ECG is shown below. Margaret Thompson & JP
EM Cases Course 2017 Toxicology Module quick IV access and diazepam is administered. The seizure stops. The first set of vitals show: HR 30bpm, BP 70/40. His ECG is shown below. Margaret Thompson & JP
Antiarrhythmic Drugs
 Antiarrhythmic Drugs DR ATIF ALQUBBANY A S S I S T A N T P R O F E S S O R O F M E D I C I N E / C A R D I O L O G Y C O N S U L T A N T C A R D I O L O G Y & I N T E R V E N T I O N A L E P A C H D /
Antiarrhythmic Drugs DR ATIF ALQUBBANY A S S I S T A N T P R O F E S S O R O F M E D I C I N E / C A R D I O L O G Y C O N S U L T A N T C A R D I O L O G Y & I N T E R V E N T I O N A L E P A C H D /
Dysrhythmias. Dysrythmias & Anti-Dysrhythmics. EKG Parameters. Dysrhythmias. Components of an ECG Wave. Dysrhythmias
 Dysrhythmias Dysrythmias & Anti-Dysrhythmics Rhythm bad in the heart: Whitewater rafting Electrical impulses coordinate heart Reduction in Cardiac Output PEA Asystole Components of an ECG Wave EKG Parameters
Dysrhythmias Dysrythmias & Anti-Dysrhythmics Rhythm bad in the heart: Whitewater rafting Electrical impulses coordinate heart Reduction in Cardiac Output PEA Asystole Components of an ECG Wave EKG Parameters
2/1/2013. Poisoning pitfalls. The original pitfall
 The original pitfall Poisoning pitfalls Craig Smollin MD Associate Medical Director, California Poison Control System - SF Division Assistant Professor of Emergency Medicine, UCSF What will we talk about?
The original pitfall Poisoning pitfalls Craig Smollin MD Associate Medical Director, California Poison Control System - SF Division Assistant Professor of Emergency Medicine, UCSF What will we talk about?
Clinical Pathway: Management Of The Life-Threatening Overdose
 Clinical Pathway: Management Of The Life-Threatening Overdose Intravenous access Oxygen Pulse oximetry n-invasive blood pressure monitoring Accu-Check ECG monitoring and ECG Chest x-ray Respiratory depression?
Clinical Pathway: Management Of The Life-Threatening Overdose Intravenous access Oxygen Pulse oximetry n-invasive blood pressure monitoring Accu-Check ECG monitoring and ECG Chest x-ray Respiratory depression?
Episode 90 Low and Slow Poisoning
 Hyperkalemia Myxedema coma Spinal cord injury Hypothermia Episode 90 Low and Slow Poisoning With Drs. Margaret Thompson & Emily Austin Prepared by Dr. Keerat Grewal, edited by Dr. Anton Helman, Jan 2017
Hyperkalemia Myxedema coma Spinal cord injury Hypothermia Episode 90 Low and Slow Poisoning With Drs. Margaret Thompson & Emily Austin Prepared by Dr. Keerat Grewal, edited by Dr. Anton Helman, Jan 2017
WHAT DO YOU SEE WHEN YOU STIMULATE BETA
 CARDIAC DRUG REVIEW WHAT DO YOU SEE WHEN YOU STIMULATE BETA VASODILATE BRONCHODILATE +CHRONOTROPE +INOTROPE EPI S OTHER NAME? ADRENALIN WHAT DOES EPI DO THAT NOREPI AND DOPAMINE DO NOT DO? BETA 2 BRONCHODILATOR
CARDIAC DRUG REVIEW WHAT DO YOU SEE WHEN YOU STIMULATE BETA VASODILATE BRONCHODILATE +CHRONOTROPE +INOTROPE EPI S OTHER NAME? ADRENALIN WHAT DOES EPI DO THAT NOREPI AND DOPAMINE DO NOT DO? BETA 2 BRONCHODILATOR
ADULT DRUG REFERENCE Drug Indication Adult Dosage Precautions / Comments
 ADENOSINE Paroxysmal SVT 1 st Dose 6 mg rapid IV 2 nd & 3 rd Doses 12 mg rapid IV push Follow each dose with rapid bolus of 20 ml NS May cause transient heart block or asystole. Side effects include chest
ADENOSINE Paroxysmal SVT 1 st Dose 6 mg rapid IV 2 nd & 3 rd Doses 12 mg rapid IV push Follow each dose with rapid bolus of 20 ml NS May cause transient heart block or asystole. Side effects include chest
Arrhythmias. Simple-dysfunction cause abnormalities in impulse formation and conduction in the myocardium.
 Arrhythmias Simple-dysfunction cause abnormalities in impulse formation and conduction in the myocardium. However, in clinic it present as a complex family of disorders that show variety of symptoms, for
Arrhythmias Simple-dysfunction cause abnormalities in impulse formation and conduction in the myocardium. However, in clinic it present as a complex family of disorders that show variety of symptoms, for
Prevention and Treatment Patrick Levelle, MD
 Prevention and Treatment Patrick Levelle, MD LOCAL ANESTHETIC TOXICITY 1. PERIPHERAL NERVE BLOCKS 2. ROLE OF THE PERIANESTHESIA RN 3. LOCAL ANESTHETIC TOXICITY Use of Lipid Emulsion Regional and Peripheral
Prevention and Treatment Patrick Levelle, MD LOCAL ANESTHETIC TOXICITY 1. PERIPHERAL NERVE BLOCKS 2. ROLE OF THE PERIANESTHESIA RN 3. LOCAL ANESTHETIC TOXICITY Use of Lipid Emulsion Regional and Peripheral
Adult Drug Reference. Dopamine Drip Chart. Pediatric Drug Reference. Pediatric Drug Dosage Charts DRUG REFERENCES
 Adult Drug Reference Dopamine Drip Chart Pediatric Drug Reference Pediatric Drug Dosage Charts DRUG REFERENCES ADULT DRUG REFERENCE Drug Indication Adult Dosage Precautions / Comments ADENOSINE Paroxysmal
Adult Drug Reference Dopamine Drip Chart Pediatric Drug Reference Pediatric Drug Dosage Charts DRUG REFERENCES ADULT DRUG REFERENCE Drug Indication Adult Dosage Precautions / Comments ADENOSINE Paroxysmal
HTEC 91. Performing ECGs: Procedure. Normal Sinus Rhythm (NSR) Topic for Today: Sinus Rhythms. Characteristics of NSR. Conduction Pathway
 Topic for Today: Sinus Rhythms. Characteristics of NSR. Conduction Pathway") HTEC 91 Medical Office Diagnostic Tests Week 3 Performing ECGs: Procedure o ECG protocol: you may NOT do ECG if you have not signed up! If you are signed up and the room is occupied with people who did
HTEC 91 Medical Office Diagnostic Tests Week 3 Performing ECGs: Procedure o ECG protocol: you may NOT do ECG if you have not signed up! If you are signed up and the room is occupied with people who did
1/29/2014. Objectives. The unstable overdose patient. Unstable overdose case #1. Outline
 Objectives The unstable overdose patient Craig Smollin MD Associate Medical Director California Poison Control Center, SF Division Discuss clinical scenarios unique to the acutely poisoned patient and
Objectives The unstable overdose patient Craig Smollin MD Associate Medical Director California Poison Control Center, SF Division Discuss clinical scenarios unique to the acutely poisoned patient and
Chapter 26. Media Directory. Dysrhythmias. Diagnosis/Treatment of Dysrhythmias. Frequency in Population Difficult to Predict
 Chapter 26 Drugs for Dysrythmias Slide 33 Slide 35 Media Directory Propranolol Animation Amiodarone Animation Upper Saddle River, New Jersey 07458 All rights reserved. Dysrhythmias Abnormalities of electrical
Chapter 26 Drugs for Dysrythmias Slide 33 Slide 35 Media Directory Propranolol Animation Amiodarone Animation Upper Saddle River, New Jersey 07458 All rights reserved. Dysrhythmias Abnormalities of electrical
Adenosine. poison/drug induced. flushing, chest pain, transient asystole. Precautions: tachycardia. fibrillation, atrial flutter. Indications: or VT
 Adenosine Indications: 1. Narrow complex PSVT 2. Does not convert atrial fibrillation, atrial flutter or VT 1. Side effects include flushing, chest pain, transient asystole 2. May deteriorate widecomplex
Adenosine Indications: 1. Narrow complex PSVT 2. Does not convert atrial fibrillation, atrial flutter or VT 1. Side effects include flushing, chest pain, transient asystole 2. May deteriorate widecomplex
Arrhythmias. 1. beat too slowly (sinus bradycardia). Like in heart block
. Like in heart block") Arrhythmias It is a simple-dysfunction caused by abnormalities in impulse formation and conduction in the myocardium. The heart is designed in such a way that allows it to generate from the SA node electrical
Arrhythmias It is a simple-dysfunction caused by abnormalities in impulse formation and conduction in the myocardium. The heart is designed in such a way that allows it to generate from the SA node electrical
Atrial Fibrillation 10/2/2018. Depolarization & ECG. Atrial Fibrillation. Hemodynamic Consequences
 Depolarization & ECG Atrial Fibrillation How to make ORDER out of CHAOS Julia Shih, VMD, DACVIM (Cardiology) October 27, 2018 Depolarization & ECG Depolarization & ECG Atrial Fibrillation Hemodynamic Consequences
Depolarization & ECG Atrial Fibrillation How to make ORDER out of CHAOS Julia Shih, VMD, DACVIM (Cardiology) October 27, 2018 Depolarization & ECG Depolarization & ECG Atrial Fibrillation Hemodynamic Consequences
PEDIATRIC CARDIAC RHYTHM DISTURBANCES. -Jason Haag, CCEMT-P
 PEDIATRIC CARDIAC RHYTHM DISTURBANCES -Jason Haag, CCEMT-P General: CARDIAC RHYTHM DISTURBANCES - More often the result and not the cause of acute cardiovascular emergencies - Typically the end result
PEDIATRIC CARDIAC RHYTHM DISTURBANCES -Jason Haag, CCEMT-P General: CARDIAC RHYTHM DISTURBANCES - More often the result and not the cause of acute cardiovascular emergencies - Typically the end result
Effects of Amiodarone in a Swine Model of Nortryptiline Toxicity
 Toxicology Investigations Effects of Amiodarone in a Swine Model of Nortryptiline Toxicity Fermin Barrueto, Jr., MD a, Indira Murr, MD b, Andrew Meltzer, MD a, Kori Brewer, PhD b, and William Meggs, MD,
Toxicology Investigations Effects of Amiodarone in a Swine Model of Nortryptiline Toxicity Fermin Barrueto, Jr., MD a, Indira Murr, MD b, Andrew Meltzer, MD a, Kori Brewer, PhD b, and William Meggs, MD,
B. 14 Antidysrhythmic drugs. a. Classify antidysrhythmics by their electrophysiological actions. Vaughan-Williams classification
 B. 14 Antidysrhythmic drugs a. Classify antidysrhythmics by their electrophysiological actions. Vaughan-Williams classification I II III IV membrane stabilizers all ERP, ERP/APD, all except c APD classified
B. 14 Antidysrhythmic drugs a. Classify antidysrhythmics by their electrophysiological actions. Vaughan-Williams classification I II III IV membrane stabilizers all ERP, ERP/APD, all except c APD classified
4/14/15 HTEC 91. Topics for Today. Guess That Rhythm. Premature Ventricular Contractions (PVCs) Ventricular Rhythms
 Ventricular Rhythms") 4/14/15 Topics for Today HTEC 91 Medical Office Diagnostic Tests Week 5 Ventricular Rhythms PVCs: Premature Ventricular Contractions VT: Ventricular Tachycardia VF: Ventricular Fibrillation Asystole Study
4/14/15 Topics for Today HTEC 91 Medical Office Diagnostic Tests Week 5 Ventricular Rhythms PVCs: Premature Ventricular Contractions VT: Ventricular Tachycardia VF: Ventricular Fibrillation Asystole Study
ALS MODULE 7 Pharmacology
 ALS MODULE 7 Pharmacology Relates to HLT404C Apply Advanced Resuscitation Techniques Introduction There are no studies that addressed the order of drug administration. There is inadequate evidence to define
ALS MODULE 7 Pharmacology Relates to HLT404C Apply Advanced Resuscitation Techniques Introduction There are no studies that addressed the order of drug administration. There is inadequate evidence to define
The most common. hospitalized patients. hypotension due to. filling time Rate control in ICU patients may be difficult as many drugs cause hypotension
 Arrhythmias in the critically ill ICU patients: Approach for rapid recognition & management Objectives Be able to identify and manage: Atrial fibrillation with a rapid ventricular response Atrial flutter
Arrhythmias in the critically ill ICU patients: Approach for rapid recognition & management Objectives Be able to identify and manage: Atrial fibrillation with a rapid ventricular response Atrial flutter
MWLCEMS SYSTEM Continuing Education Packet Management of the Acute MI Patient
 MWLCEMS SYSTEM Continuing Education Packet Management of the Acute MI Patient In this CE we will discuss the patient presenting with an acute ST-Elevation Myocardial Infarction (STEMI) Definition: Myocardial
MWLCEMS SYSTEM Continuing Education Packet Management of the Acute MI Patient In this CE we will discuss the patient presenting with an acute ST-Elevation Myocardial Infarction (STEMI) Definition: Myocardial
ECMO for treatment of cardiotoxic intoxications
 ECMO for treatment of cardiotoxic intoxications Bruno Mégarbane, MD, PhD Medical and Toxicological Critical Care Department Lariboisiere Hospital, INSERM UMRS-1144, Paris-Diderot University Paris France
ECMO for treatment of cardiotoxic intoxications Bruno Mégarbane, MD, PhD Medical and Toxicological Critical Care Department Lariboisiere Hospital, INSERM UMRS-1144, Paris-Diderot University Paris France
Arrhythmic Complications of MI. Teferi Mitiku, MD Assistant Clinical Professor of Medicine University of California Irvine
 Arrhythmic Complications of MI Teferi Mitiku, MD Assistant Clinical Professor of Medicine University of California Irvine Objectives Brief overview -Pathophysiology of Arrhythmia ECG review of typical
Arrhythmic Complications of MI Teferi Mitiku, MD Assistant Clinical Professor of Medicine University of California Irvine Objectives Brief overview -Pathophysiology of Arrhythmia ECG review of typical
Contra Costa County Emergency Medical Services Drug Reference. Indication Dosing Cautions Comments
 Drug Adenosine Albuterol Indication Dosing Cautions Comments Narrow complex tachycardia Bronchospasm Crush injury - hyperkalemia Initial 6mg rapid IV Repeat 12mg rapid IV Follow each dose with 20ml NS
Drug Adenosine Albuterol Indication Dosing Cautions Comments Narrow complex tachycardia Bronchospasm Crush injury - hyperkalemia Initial 6mg rapid IV Repeat 12mg rapid IV Follow each dose with 20ml NS
Atrial fibrillation in the ICU
 Atrial fibrillation in the ICU Atrial fibrillation Preexisting or incident (new onset) among nearly one in three critically ill patients Formation of arrhythogenic substrate usually fibrosis (CHF, hypertension,
Atrial fibrillation in the ICU Atrial fibrillation Preexisting or incident (new onset) among nearly one in three critically ill patients Formation of arrhythogenic substrate usually fibrosis (CHF, hypertension,
Rhythm Control: Is There a Role for the PCP? Blake Norris, MD, FACC BHHI Primary Care Symposium February 28, 2014
 Rhythm Control: Is There a Role for the PCP? Blake Norris, MD, FACC BHHI Primary Care Symposium February 28, 2014 Financial disclosures Consultant Medtronic 3 reasons to evaluate and treat arrhythmias
Rhythm Control: Is There a Role for the PCP? Blake Norris, MD, FACC BHHI Primary Care Symposium February 28, 2014 Financial disclosures Consultant Medtronic 3 reasons to evaluate and treat arrhythmias
Emergency Cardiovascular Care: EMT-Intermediate Treatment Algorithms. Introduction to the Algorithms
 Emergency Cardiovascular Care: EMT-Intermediate Treatment Algorithms Introduction to the Algorithms Cardiac Arrest Algorithms Prehospital Medication Profiles Perspective regarding the EMT- Intermediate
Emergency Cardiovascular Care: EMT-Intermediate Treatment Algorithms Introduction to the Algorithms Cardiac Arrest Algorithms Prehospital Medication Profiles Perspective regarding the EMT- Intermediate
! YOU NEED TO MONITOR QT INTERVALS IN THESE PATIENTS.
 Antiarrhythmic Pharmacopoeia Powerful drugs, split into 4 major classes, according to the predominant receptor they effect. Some fit into several classes at once, like sotolol. Some don t fit at all, owing
Antiarrhythmic Pharmacopoeia Powerful drugs, split into 4 major classes, according to the predominant receptor they effect. Some fit into several classes at once, like sotolol. Some don t fit at all, owing
Yolo County Health & Human Services Agency
 Yolo County Health & Human Services Agency Kristin Weivoda EMS Administrator John S. Rose, MD, FACEP Medical Director DATE: December 28, 2017 TO: Yolo County Providers and Agencies FROM: Yolo County EMS
Yolo County Health & Human Services Agency Kristin Weivoda EMS Administrator John S. Rose, MD, FACEP Medical Director DATE: December 28, 2017 TO: Yolo County Providers and Agencies FROM: Yolo County EMS
DYSRHYTHMIAS. D. Assess whether or not it is the arrhythmia that is making the patient unstable or symptomatic
 DYSRHYTHMIAS GENERAL CONSIDERATIONS A. The 2015 American Heart Association Guidelines were referred to for this protocol development. Evidence-based science was implemented in those areas where the AHA
DYSRHYTHMIAS GENERAL CONSIDERATIONS A. The 2015 American Heart Association Guidelines were referred to for this protocol development. Evidence-based science was implemented in those areas where the AHA
Cardiac arrhythmias. Janusz Witowski. Department of Pathophysiology Poznan University of Medical Sciences. J. Witowski
 Cardiac arrhythmias Janusz Witowski Department of Pathophysiology Poznan University of Medical Sciences A 68-year old man presents to the emergency department late one evening complaining of increasing
Cardiac arrhythmias Janusz Witowski Department of Pathophysiology Poznan University of Medical Sciences A 68-year old man presents to the emergency department late one evening complaining of increasing
ANTI - ARRHYTHMIC DRUGS
 ANTI - ARRHYTHMIC DRUGS CARDIAC ACTION POTENTIAL K Out Balance Ca in/k out Na in K Out GENERATION OF ARRHYTHMIAS Four mechanisms of arrhythmia generation; Increased normal automaticity Abnormal automaticity
ANTI - ARRHYTHMIC DRUGS CARDIAC ACTION POTENTIAL K Out Balance Ca in/k out Na in K Out GENERATION OF ARRHYTHMIAS Four mechanisms of arrhythmia generation; Increased normal automaticity Abnormal automaticity
Objectives: This presentation will help you to:
 emergency Drugs Objectives: This presentation will help you to: Five rights for medication administration Recognize different cardiac arrhythmias and determine the common drugs used for each one List the
emergency Drugs Objectives: This presentation will help you to: Five rights for medication administration Recognize different cardiac arrhythmias and determine the common drugs used for each one List the
Mr. Eknath Kole M.S. Pharm (NIPER Mohali)
") M.S. Pharm (NIPER Mohali) Drug Class Actions Therapeutic Uses Pharmacokinetics Adverse Effects Other Quinidine IA -Binds to open and inactivated Na+ -Decreases the slope of Phase 4 spontaneous depolarization
M.S. Pharm (NIPER Mohali) Drug Class Actions Therapeutic Uses Pharmacokinetics Adverse Effects Other Quinidine IA -Binds to open and inactivated Na+ -Decreases the slope of Phase 4 spontaneous depolarization
Review Packet EKG Competency This packet is a review of the information you will need to know for the proctored EKG competency test.
 Review Packet EKG Competency 2015 This packet is a review of the information you will need to know for the proctored EKG competency test. Normal Sinus Rhythm Rhythm: Regular Ventricular Rate: 60-100 bpm
Review Packet EKG Competency 2015 This packet is a review of the information you will need to know for the proctored EKG competency test. Normal Sinus Rhythm Rhythm: Regular Ventricular Rate: 60-100 bpm
Pediatrics ECG Monitoring. Pediatric Intensive Care Unit Emergency Division
 Pediatrics ECG Monitoring Pediatric Intensive Care Unit Emergency Division 1 Conditions Leading to Pediatric Cardiology Consultation 12.7% of annual consultation Is arrhythmias problems Geggel. Pediatrics.
Pediatrics ECG Monitoring Pediatric Intensive Care Unit Emergency Division 1 Conditions Leading to Pediatric Cardiology Consultation 12.7% of annual consultation Is arrhythmias problems Geggel. Pediatrics.
CSI Skills Lab #5: Arrhythmia Interpretation and Treatment
 CSI 202 - Skills Lab #5: Arrhythmia Interpretation and Treatment Origins of the ACLS Approach: CSI 202 - Skills Lab 5 Notes ACLS training originated in Nebraska in the early 1970 s. Its purpose was to
CSI 202 - Skills Lab #5: Arrhythmia Interpretation and Treatment Origins of the ACLS Approach: CSI 202 - Skills Lab 5 Notes ACLS training originated in Nebraska in the early 1970 s. Its purpose was to
Treatment of Arrhythmias in the Emergency Setting
 Treatment of Arrhythmias in the Emergency Setting Zian H. Tseng, M.D. Assistant Professor of Medicine Cardiac Electrophysiology Section Cardiology Division University of California, San Francisco There
Treatment of Arrhythmias in the Emergency Setting Zian H. Tseng, M.D. Assistant Professor of Medicine Cardiac Electrophysiology Section Cardiology Division University of California, San Francisco There
Antiarrhythmic Pharmacology. The Electronics
 Antiarrhythmic Pharmacology Linking Pharmacological Treatment to the Patient and the Rhythm Presented By: Karen Marzlin BSN, RN,C, CCRN-CMC CNEA 2009 1 The Electronics Action Potential of Cardiac Cells
Antiarrhythmic Pharmacology Linking Pharmacological Treatment to the Patient and the Rhythm Presented By: Karen Marzlin BSN, RN,C, CCRN-CMC CNEA 2009 1 The Electronics Action Potential of Cardiac Cells
European Resuscitation Council
 European Resuscitation Council Objectives To know basic elements to evaluate patients with rythm disturbance To know advanced treatment of paediatric cardiac arrest To know emergency treatment of most
European Resuscitation Council Objectives To know basic elements to evaluate patients with rythm disturbance To know advanced treatment of paediatric cardiac arrest To know emergency treatment of most
Antiarrhythmic Drugs 1/31/2018 1
 Antiarrhythmic Drugs 1/31/2018 1 Normal conduction pathway: 1- SA node generates action potential and delivers it to the atria and the AV node 2- The AV node delivers the impulse to purkinje fibers Other
Antiarrhythmic Drugs 1/31/2018 1 Normal conduction pathway: 1- SA node generates action potential and delivers it to the atria and the AV node 2- The AV node delivers the impulse to purkinje fibers Other
Full file at
 MULTIPLE CHOICE. Choose the one alternative that best completes the statement or answers the question. 1) What electrical event must occur for atrial kick to occur? 1) A) Atrial repolarization B) Ventricular
MULTIPLE CHOICE. Choose the one alternative that best completes the statement or answers the question. 1) What electrical event must occur for atrial kick to occur? 1) A) Atrial repolarization B) Ventricular
Heart Failure (HF) Treatment
 Treatment") Heart Failure (HF) Treatment Heart Failure (HF) Complex, progressive disorder. The heart is unable to pump sufficient blood to meet the needs of the body. Its cardinal symptoms are dyspnea, fatigue, and
Heart Failure (HF) Treatment Heart Failure (HF) Complex, progressive disorder. The heart is unable to pump sufficient blood to meet the needs of the body. Its cardinal symptoms are dyspnea, fatigue, and
INSTITUTE FOR MEDICAL SIMULATION & EDUCATION ACLS PRACTICAL SCENARIOS
 Practical Teaching for Respiratory Arrest with a Pulse (Case 1) You are a medical officer doing a pre-operative round when 60-year old patient started coughing violently and becomes unconscious. Fortunately
Practical Teaching for Respiratory Arrest with a Pulse (Case 1) You are a medical officer doing a pre-operative round when 60-year old patient started coughing violently and becomes unconscious. Fortunately
Drug Max dose approved for IVP Dilution Rate Monitoring Parameters. Dilution not necessary (Available in prefilled syringe)
") Drug Max dose approved for IVP Dilution Rate Monitoring Parameters Acetazolamide 500 mg Reconstitute with at least 5ml sterile water (max concentration should not exceed 100mg/ml) 100-500 mg/min Hypotension
Drug Max dose approved for IVP Dilution Rate Monitoring Parameters Acetazolamide 500 mg Reconstitute with at least 5ml sterile water (max concentration should not exceed 100mg/ml) 100-500 mg/min Hypotension
ACLS Prep. Preparation is key to a successful ACLS experience. Please complete the ACLS Pretest and Please complete this ACLS Prep.
 November, 2013 ACLS Prep Preparation is key to a successful ACLS experience. Please complete the ACLS Pretest and Please complete this ACLS Prep. ACLS Prep Preparation is key to a successful ACLS experience.
November, 2013 ACLS Prep Preparation is key to a successful ACLS experience. Please complete the ACLS Pretest and Please complete this ACLS Prep. ACLS Prep Preparation is key to a successful ACLS experience.
CHAPTER 150 CHAPTER 161. CV Drug Toxicity Pesticides
 CHAPTER 150 CHAPTER 161 CV Drug Toxicity Pesticides 20 November 2013 1. Which of the following poisoningantidote therapeutic pairings is correct? A.Anticholinergic-atropine A.Beta-blocker- octreotide A.Calcium-channel
CHAPTER 150 CHAPTER 161 CV Drug Toxicity Pesticides 20 November 2013 1. Which of the following poisoningantidote therapeutic pairings is correct? A.Anticholinergic-atropine A.Beta-blocker- octreotide A.Calcium-channel
MICHIGAN. State Protocols. Pediatric Cardiac Table of Contents 6.1 General Pediatric Cardiac Arrest 6.2 Bradycardia 6.
 MICHIGAN State Protocols Protocol Number Protocol Name Pediatric Cardiac Table of Contents 6.1 General Pediatric Cardiac Arrest 6.2 Bradycardia 6.3 Tachycardia PEDIATRIC CARDIAC PEDIATRIC CARDIAC ARREST
MICHIGAN State Protocols Protocol Number Protocol Name Pediatric Cardiac Table of Contents 6.1 General Pediatric Cardiac Arrest 6.2 Bradycardia 6.3 Tachycardia PEDIATRIC CARDIAC PEDIATRIC CARDIAC ARREST
WRITER TRISTAN WALKER TABLE OF CONTENTS. The Basics of cardiac pharmacology 2007
 WRITER TRISTAN WALKER TABLE OF CONTENTS 1. WHAT ARE THE MAJOR CLASSES OF CARDIAC DRUGS?...2 2. HOW DO THEY WORK?...3 3. CONSIDERATIONS FOR THE PEDIATRIC PATIENT...7 4. SUMMARY TABLE...10 REFERENCES...14
WRITER TRISTAN WALKER TABLE OF CONTENTS 1. WHAT ARE THE MAJOR CLASSES OF CARDIAC DRUGS?...2 2. HOW DO THEY WORK?...3 3. CONSIDERATIONS FOR THE PEDIATRIC PATIENT...7 4. SUMMARY TABLE...10 REFERENCES...14
Collin County Community College
 Collin County Community College BIOL. 2402 Anatomy & Physiology WEEK 5 The Heart 1 The Heart Beat and the EKG 2 1 The Heart Beat and the EKG P-wave = Atrial depolarization QRS-wave = Ventricular depolarization
Collin County Community College BIOL. 2402 Anatomy & Physiology WEEK 5 The Heart 1 The Heart Beat and the EKG 2 1 The Heart Beat and the EKG P-wave = Atrial depolarization QRS-wave = Ventricular depolarization
Cardiac Arrhythmias & Drugs used in Advanced Life Support and Cardiac Emergencies
 Cardiac Arrhythmias & Drugs used in Advanced Life Support and Cardiac Emergencies CNHE Ballarat Health Services Valid from 1 st March 2016 to 31 st June 2018 1 Supraventricular Tachycardia (SVT) An atrial
Cardiac Arrhythmias & Drugs used in Advanced Life Support and Cardiac Emergencies CNHE Ballarat Health Services Valid from 1 st March 2016 to 31 st June 2018 1 Supraventricular Tachycardia (SVT) An atrial
*Generating blood pressure *Routing blood: separates. *Ensuring one-way blood. *Regulating blood supply *Changes in contraction
 *Generating blood pressure *Routing blood: separates pulmonary and systemic circulations *Ensuring one-way blood flow: valves *Regulating blood supply *Changes in contraction rate and force match blood
*Generating blood pressure *Routing blood: separates pulmonary and systemic circulations *Ensuring one-way blood flow: valves *Regulating blood supply *Changes in contraction rate and force match blood
Chapter 13. Learning Objectives. Learning Objectives 9/11/2012. Poisonings, Overdoses, and Intoxications
 Chapter 13 Poisonings, Overdoses, and Intoxications Learning Objectives Discuss use of activated charcoal in treatment of poisonings List treatment options for acetaminophen overdose List clinical manifestations
Chapter 13 Poisonings, Overdoses, and Intoxications Learning Objectives Discuss use of activated charcoal in treatment of poisonings List treatment options for acetaminophen overdose List clinical manifestations
Requirements to successfully complete PALS:
 The American Heart Association released new resuscitation science and treatment guidelines on October 19, 2010. The new AHA Handbook of Emergency Cardiac Care (ECC) contains these 2010 Guidelines.The 2010
The American Heart Association released new resuscitation science and treatment guidelines on October 19, 2010. The new AHA Handbook of Emergency Cardiac Care (ECC) contains these 2010 Guidelines.The 2010
CORONARY ARTERIES. LAD Anterior wall of the left vent Lateral wall of left vent Anterior 2/3 of interventricluar septum R & L bundle branches
 CORONARY ARTERIES RCA Right atrium Right ventricle SA node 55% AV node 90% Posterior wall of left ventricle in 90% Posterior third of interventricular septum 90% LAD Anterior wall of the left vent Lateral
CORONARY ARTERIES RCA Right atrium Right ventricle SA node 55% AV node 90% Posterior wall of left ventricle in 90% Posterior third of interventricular septum 90% LAD Anterior wall of the left vent Lateral
PHARMACOLOGY OF ARRHYTHMIAS
 PHARMACOLOGY OF ARRHYTHMIAS Course: Integrated Therapeutics 1 Lecturer: Dr. E. Konorev Date: November 27, 2012 Materials on: Exam #5 Required reading: Katzung, Chapter 14 1 CARDIAC ARRHYTHMIAS Abnormalities
PHARMACOLOGY OF ARRHYTHMIAS Course: Integrated Therapeutics 1 Lecturer: Dr. E. Konorev Date: November 27, 2012 Materials on: Exam #5 Required reading: Katzung, Chapter 14 1 CARDIAC ARRHYTHMIAS Abnormalities
a lecture series by SWESEMJR
 Electrolyte disturbances Hypokalaemia Decreased extracellular potassium increases excitability in the myocardial cells and consequently the effect of very severe hypokalaemia is ventricular arrhythmia.
Electrolyte disturbances Hypokalaemia Decreased extracellular potassium increases excitability in the myocardial cells and consequently the effect of very severe hypokalaemia is ventricular arrhythmia.
VENTRICULAR FIBRILLATION. 1. Safe scene, standard precautions. 2. Establish unresponsiveness, apnea, and pulselessness. 3. Quick look (monitor)
") LUCAS COUNTY EMS SUMMARY PAGES VENTRICULAR FIBRILLATION 2. Establish unresponsiveness, apnea, and pulselessness 3. Quick look (monitor) 4. Identify rhythm 5. Provide 2 minutes CPR if unwitnessed by EMS
LUCAS COUNTY EMS SUMMARY PAGES VENTRICULAR FIBRILLATION 2. Establish unresponsiveness, apnea, and pulselessness 3. Quick look (monitor) 4. Identify rhythm 5. Provide 2 minutes CPR if unwitnessed by EMS
POISON ANTIDOTE DOSE* COMMENTS
 Antidotes Acetaminophen N-acetylcysteine 140 mg/kg initial oral dose, followed Most effective within 16 24 hr; may by 70 mg/kg every 4 hr 17 doses be useful after chronic intoxication or intravenously
Antidotes Acetaminophen N-acetylcysteine 140 mg/kg initial oral dose, followed Most effective within 16 24 hr; may by 70 mg/kg every 4 hr 17 doses be useful after chronic intoxication or intravenously
Chapter 14. Agents used in Cardiac Arrhythmias
 Chapter 14 Agents used in Cardiac Arrhythmias Cardiac arrhythmia Approximately 50% of post-myocardial infarction fatalities result from ventricular tachycarida (VT) or ventricular fibrillation (VF). These
Chapter 14 Agents used in Cardiac Arrhythmias Cardiac arrhythmia Approximately 50% of post-myocardial infarction fatalities result from ventricular tachycarida (VT) or ventricular fibrillation (VF). These
Notes on Antidotes Insulin/Glucose for CCB overdose
 Overview Notes on Antidotes for CCB overdose for cyanide poisoning Rob Gair, BSc (Pharm), CSPI CSHP Spring Therapeutics Update April 23, 2009 Lipid rescue for local anesthetic toxicity BC Drug & Poison
Overview Notes on Antidotes for CCB overdose for cyanide poisoning Rob Gair, BSc (Pharm), CSPI CSHP Spring Therapeutics Update April 23, 2009 Lipid rescue for local anesthetic toxicity BC Drug & Poison
PEDIATRIC TREATMENT GUIDELINES - CARDIAC VENTRICULAR FIBRILLATION - PULSELESS VENTRICULAR TACHYCARDIA (SJ-PO1) effective 05/01/02
 effective 05/01/02") PEDIATRIC TREATMENT GUIDELINES - CARDIAC VENTRICULAR FIBRILLATION - PULSELESS VENTRICULAR TACHYCARDIA (SJ-PO1) effective 05/01/02 Revision #5 04/19/02 Identify Dysrhythmia DEFIBRILLATE: 2 J/kg, 4 J/kg,
PEDIATRIC TREATMENT GUIDELINES - CARDIAC VENTRICULAR FIBRILLATION - PULSELESS VENTRICULAR TACHYCARDIA (SJ-PO1) effective 05/01/02 Revision #5 04/19/02 Identify Dysrhythmia DEFIBRILLATE: 2 J/kg, 4 J/kg,
Instruct patient and caregivers: Need for constant monitoring Potential complications of drug therapy
 Assessment Prior to administration: Assess patient for chest pain, dysrhythmias, and vital signs (initially and throughout therapy) Obtain complete medical history, including allergies, especially heart
Assessment Prior to administration: Assess patient for chest pain, dysrhythmias, and vital signs (initially and throughout therapy) Obtain complete medical history, including allergies, especially heart
Update in Poison Management. Update in Poison Management. Antidote Use. Fomepizole. Pediatric Ingestions 1. No financial disclosures
 Update in Poison Management No financial disclosures Robert J. Hoffman, MD,MS FACMT, FACEP, FAAEM, FAAP Department of Emergency Medicine Albert Einstein College of Medicine New York, New York Update in
Update in Poison Management No financial disclosures Robert J. Hoffman, MD,MS FACMT, FACEP, FAAEM, FAAP Department of Emergency Medicine Albert Einstein College of Medicine New York, New York Update in
Krittin Bunditanukul Pharm.D, BCPS Department of Pharmacy Practice, Faculty of Pharmaceutical Sciences, Chulalongkorn University
 Krittin Bunditanukul Pharm.D, BCPS Department of Pharmacy Practice, Faculty of Pharmaceutical Sciences, Chulalongkorn University Cardiac arrest Cardiac arrest can be caused by 4 rhythms: Ventricular fibrillation
Krittin Bunditanukul Pharm.D, BCPS Department of Pharmacy Practice, Faculty of Pharmaceutical Sciences, Chulalongkorn University Cardiac arrest Cardiac arrest can be caused by 4 rhythms: Ventricular fibrillation
1. Normal sinus rhythm 2. SINUS BRADYCARDIA
 1. Normal sinus rhythm 2. SINUS BRADYCARDIA No signs and symptoms observe There are severe signs or symptoms o What are the signs and symptom Hypotension
1. Normal sinus rhythm 2. SINUS BRADYCARDIA No signs and symptoms observe There are severe signs or symptoms o What are the signs and symptom Hypotension
Fundamentals of Pharmacology for Veterinary Technicians Chapter 8
 Figure 8-1 Figure 8-2 Figure 8-3 Figure 8-4 Figure 8-5 Figure 8-7 Figure 8-8 Figure 8-9 TABLE 8-1 Blood Flow Through the Heart The right atrium receives blood from all tissues, except the lungs, through
Figure 8-1 Figure 8-2 Figure 8-3 Figure 8-4 Figure 8-5 Figure 8-7 Figure 8-8 Figure 8-9 TABLE 8-1 Blood Flow Through the Heart The right atrium receives blood from all tissues, except the lungs, through
Advanced Cardiac Life Support
 Advanced Cardiac Life Support Algorithm Drugs Class I: definitely helpful, excellent Class II: Class II a -probably helpful; good to very good Class II b -possibly helpful; fair to good Class
Advanced Cardiac Life Support Algorithm Drugs Class I: definitely helpful, excellent Class II: Class II a -probably helpful; good to very good Class II b -possibly helpful; fair to good Class
Updated Policies and Procedures # s 606, 607, 610, 611, 612, 613, 625, 628, 630, 631, and 633 (ACLS Protocols and Policies)
") SLO County Emergency Medical Services Agency Bulletin 2012-09 PLEASE POST Updated Policies and Procedures # s 606, 607, 610, 611, 612, 613, 625, 628, 630, 631, and 633 (ACLS Protocols and Policies) July
SLO County Emergency Medical Services Agency Bulletin 2012-09 PLEASE POST Updated Policies and Procedures # s 606, 607, 610, 611, 612, 613, 625, 628, 630, 631, and 633 (ACLS Protocols and Policies) July
99 Problems but hyperglycemia ain t one SHEEREENE HUSSAIN MD, MA RAPID CITY REGIONAL HOSPITAL HOSPITALIST DEPARTMENT SEPT 12, 2018
 99 Problems but hyperglycemia ain t one SHEEREENE HUSSAIN MD, MA RAPID CITY REGIONAL HOSPITAL HOSPITALIST DEPARTMENT SEPT 12, 2018 ER Admit 17 yo F reported intentional overdose handful of her mother s
99 Problems but hyperglycemia ain t one SHEEREENE HUSSAIN MD, MA RAPID CITY REGIONAL HOSPITAL HOSPITALIST DEPARTMENT SEPT 12, 2018 ER Admit 17 yo F reported intentional overdose handful of her mother s
Heart Failure. Dr. Alia Shatanawi
 Heart Failure Dr. Alia Shatanawi Left systolic dysfunction secondary to coronary artery disease is the most common cause, account to 70% of all cases. Heart Failure Heart is unable to pump sufficient blood
Heart Failure Dr. Alia Shatanawi Left systolic dysfunction secondary to coronary artery disease is the most common cause, account to 70% of all cases. Heart Failure Heart is unable to pump sufficient blood
Chapter 13 The Cardiovascular System: Cardiac Function
 Chapter 13 The Cardiovascular System: Cardiac Function Overview of the Cardiovascular System The Path of Blood Flow through the Heart and Vasculature Anatomy of the Heart Electrical Activity of the Heart
Chapter 13 The Cardiovascular System: Cardiac Function Overview of the Cardiovascular System The Path of Blood Flow through the Heart and Vasculature Anatomy of the Heart Electrical Activity of the Heart
Drugs Used in Heart Failure. Assistant Prof. Dr. Najlaa Saadi PhD pharmacology Faculty of Pharmacy University of Philadelphia
 Drugs Used in Heart Failure Assistant Prof. Dr. Najlaa Saadi PhD pharmacology Faculty of Pharmacy University of Philadelphia Heart Failure Heart failure (HF), occurs when cardiac output is inadequate to
Drugs Used in Heart Failure Assistant Prof. Dr. Najlaa Saadi PhD pharmacology Faculty of Pharmacy University of Philadelphia Heart Failure Heart failure (HF), occurs when cardiac output is inadequate to
The ABCs of EKGs/ECGs for HCPs. Al Heuer, PhD, MBA, RRT, RPFT Professor, Rutgers School of Health Related Professions
 The ABCs of EKGs/ECGs for HCPs Al Heuer, PhD, MBA, RRT, RPFT Professor, Rutgers School of Health Related Professions Learning Objectives Review the basic anatomy of the heart Describe the cardiac conducting
The ABCs of EKGs/ECGs for HCPs Al Heuer, PhD, MBA, RRT, RPFT Professor, Rutgers School of Health Related Professions Learning Objectives Review the basic anatomy of the heart Describe the cardiac conducting
Use of Antiarrhythmic Drugs for AF Who, What and How? Dr. Marc Cheng Queen Elizabeth Hospital
 Use of Antiarrhythmic Drugs for AF Who, What and How? Dr. Marc Cheng Queen Elizabeth Hospital Content i. Rhythm versus Rate control ii. Anti-arrhythmic for Rhythm Control iii. Anti-arrhythmic for Rate
Use of Antiarrhythmic Drugs for AF Who, What and How? Dr. Marc Cheng Queen Elizabeth Hospital Content i. Rhythm versus Rate control ii. Anti-arrhythmic for Rhythm Control iii. Anti-arrhythmic for Rate
EKG Competency for Agency
 EKG Competency for Agency Name: Date: Agency: 1. The upper chambers of the heart are known as the: a. Atria b. Ventricles c. Mitral Valve d. Aortic Valve 2. The lower chambers of the heart are known as
EKG Competency for Agency Name: Date: Agency: 1. The upper chambers of the heart are known as the: a. Atria b. Ventricles c. Mitral Valve d. Aortic Valve 2. The lower chambers of the heart are known as
Core Content In Urgent Care Medicine
 Palpitations/Arrhythmias Ebrahim Barkoudah, MD Clinical Instructor in Internal Medicine Harvard Medical School Assistant in Internal Medicine & Pediatrics Massachusetts General Hospital MGH Chelsea Chelsea,
Palpitations/Arrhythmias Ebrahim Barkoudah, MD Clinical Instructor in Internal Medicine Harvard Medical School Assistant in Internal Medicine & Pediatrics Massachusetts General Hospital MGH Chelsea Chelsea,
Chapter 03: Sinus Mechanisms Test Bank MULTIPLE CHOICE
 Instant download and all chapters Tesst Bank ECGs Made Easy 5th Edition Barbara J Aehlert https://testbanklab.com/download/tesst-bank-ecgs-made-easy-5th-edition-barbara-jaehlert/ Chapter 03: Sinus Mechanisms
Instant download and all chapters Tesst Bank ECGs Made Easy 5th Edition Barbara J Aehlert https://testbanklab.com/download/tesst-bank-ecgs-made-easy-5th-edition-barbara-jaehlert/ Chapter 03: Sinus Mechanisms
Intraoperative and Postoperative Arrhythmias: Diagnosis and Treatment
 Intraoperative and Postoperative Arrhythmias: Diagnosis and Treatment Karen L. Booth, MD, Lucile Packard Children s Hospital Arrhythmias are common after congenital heart surgery [1]. Postoperative electrolyte
Intraoperative and Postoperative Arrhythmias: Diagnosis and Treatment Karen L. Booth, MD, Lucile Packard Children s Hospital Arrhythmias are common after congenital heart surgery [1]. Postoperative electrolyte
ANZCOR Guideline 12.4 Medications and Fluids in Paediatric Advanced Life Support
 ANZCOR Guideline 12. Medications and Fluids in Paediatric Advanced Life Support Who does this guideline apply to? This guideline applies to infants and children. Summary Who is the audience for this guideline?
ANZCOR Guideline 12. Medications and Fluids in Paediatric Advanced Life Support Who does this guideline apply to? This guideline applies to infants and children. Summary Who is the audience for this guideline?
Clinical Problem. Management. Discussion
 Optimum management of atrial fibrillation in the Intensive Care Unit Clinical Problem A 61 year old man, PD, presented to the Intensive Care Unit (ICU) after angiography and intra arterial thrombolysis
Optimum management of atrial fibrillation in the Intensive Care Unit Clinical Problem A 61 year old man, PD, presented to the Intensive Care Unit (ICU) after angiography and intra arterial thrombolysis
The Cardiovascular System
 Chapter 18 Part A The Cardiovascular System 1/19/16 1 Annie Leibovitz/Contact Press Images Similarities of Cardiac and Skeletal Muscle RMP Ion concentration Deploarization Action Potential Repolarization
Chapter 18 Part A The Cardiovascular System 1/19/16 1 Annie Leibovitz/Contact Press Images Similarities of Cardiac and Skeletal Muscle RMP Ion concentration Deploarization Action Potential Repolarization
Michigan Pediatric Cardiac Protocols. Date: November 15, 2012 Page 1 of 1 TABLE OF CONTENTS
 Date: November 15, 2012 Page 1 of 1 TABLE OF CONTENTS Pediatric Asystole Section 4-1 Pediatric Bradycardia Section 4-2 Pediatric Cardiac Arrest General Section 4-3 Pediatric Narrow Complex Tachycardia
Date: November 15, 2012 Page 1 of 1 TABLE OF CONTENTS Pediatric Asystole Section 4-1 Pediatric Bradycardia Section 4-2 Pediatric Cardiac Arrest General Section 4-3 Pediatric Narrow Complex Tachycardia
Assistant Professor Dr. Tavga A Baban PhD Pharmacology & Toxicology 1/3/2019 1
 Assistant Professor Dr. Tavga A Baban PhD Pharmacology & Toxicology 1/3/2019 1 Pathophysiology Cardiovascular system (CVS) consist of:- 1. Myocardium. 2. Vascular vessels (arteries, veins and capillaries).
Assistant Professor Dr. Tavga A Baban PhD Pharmacology & Toxicology 1/3/2019 1 Pathophysiology Cardiovascular system (CVS) consist of:- 1. Myocardium. 2. Vascular vessels (arteries, veins and capillaries).
Electrical Conduction
 Sinoatrial (SA) node Electrical Conduction Sets the pace of the heartbeat at 70 bpm AV node (50 bpm) and Purkinje fibers (25 40 bpm) can act as pacemakers under some conditions Internodal pathway from
Sinoatrial (SA) node Electrical Conduction Sets the pace of the heartbeat at 70 bpm AV node (50 bpm) and Purkinje fibers (25 40 bpm) can act as pacemakers under some conditions Internodal pathway from
Cardiac Properties MCQ
 Cardiac Properties MCQ Abdel Moniem Ibrahim Ahmed, MD Professor of Cardiovascular Physiology Cairo University 2007 1- Cardiac Valves: a- Prevent backflow of blood from the ventricles to the atria during
Cardiac Properties MCQ Abdel Moniem Ibrahim Ahmed, MD Professor of Cardiovascular Physiology Cairo University 2007 1- Cardiac Valves: a- Prevent backflow of blood from the ventricles to the atria during
Medical management of AF: drugs for rate and rhythm control
 Medical management of AF: drugs for rate and rhythm control Adel Khalifa Sultan Hamad, BMS, MD, FGHRS, FRCP(Canada) Consultant Cardiologist & Interventional Cardiac Electrophysiologist Head of Electrophysiology
Medical management of AF: drugs for rate and rhythm control Adel Khalifa Sultan Hamad, BMS, MD, FGHRS, FRCP(Canada) Consultant Cardiologist & Interventional Cardiac Electrophysiologist Head of Electrophysiology
Acute Arrhythmias in the Hospitalized Patient
 Acute Arrhythmias in the Hospitalized Patient Gregory M Marcus, MD, MAS Associate Professor of Medicine Division of Cardiology University of California, San Francisc Disclosures Medtronic: Research Support
Acute Arrhythmias in the Hospitalized Patient Gregory M Marcus, MD, MAS Associate Professor of Medicine Division of Cardiology University of California, San Francisc Disclosures Medtronic: Research Support
Where are the normal pacemaker and the backup pacemakers of the heart located?
 CASE 9 A 68-year-old woman presents to the emergency center with shortness of breath, light-headedness, and chest pain described as being like an elephant sitting on her chest. She is diagnosed with a
CASE 9 A 68-year-old woman presents to the emergency center with shortness of breath, light-headedness, and chest pain described as being like an elephant sitting on her chest. She is diagnosed with a
THE CARDIOVASCULAR SYSTEM. Heart 2
 THE CARDIOVASCULAR SYSTEM Heart 2 PROPERTIES OF CARDIAC MUSCLE Cardiac muscle Striated Short Wide Branched Interconnected Skeletal muscle Striated Long Narrow Cylindrical PROPERTIES OF CARDIAC MUSCLE Intercalated
THE CARDIOVASCULAR SYSTEM Heart 2 PROPERTIES OF CARDIAC MUSCLE Cardiac muscle Striated Short Wide Branched Interconnected Skeletal muscle Striated Long Narrow Cylindrical PROPERTIES OF CARDIAC MUSCLE Intercalated
Michigan Pediatric Cardiac Protocols. Date: November 15, 2012 Page 1 of 1 TABLE OF CONTENTS
 Date: November 15, 2012 Page 1 of 1 TABLE OF CONTENTS Pediatric Asystole Section 4-1 Pediatric Bradycardia Section 4-2 Pediatric Cardiac Arrest General Section 4-3 Pediatric Narrow Complex Tachycardia
Date: November 15, 2012 Page 1 of 1 TABLE OF CONTENTS Pediatric Asystole Section 4-1 Pediatric Bradycardia Section 4-2 Pediatric Cardiac Arrest General Section 4-3 Pediatric Narrow Complex Tachycardia
Antiarrhythmic Drugs. Munir Gharaibeh MD, PhD, MHPE School of Medicine, The University of Jordan November 2018
 Antiarrhythmic Drugs Munir Gharaibeh MD, PhD, MHPE School of Medicine, The University of Jordan November 2018 2 Ion Permeability Changes Potential Changes Genes and Proteins 3 Cardiac Na+ channels 5 6
Antiarrhythmic Drugs Munir Gharaibeh MD, PhD, MHPE School of Medicine, The University of Jordan November 2018 2 Ion Permeability Changes Potential Changes Genes and Proteins 3 Cardiac Na+ channels 5 6
Management of acute Cardiac Arrhythmias
 Management of acute Cardiac Arrhythmias Dr. Zulkeflee Muhammad MBChB (New Zealand), MRCP (United Kingdom) Cardiologist Electrophysiology Unit Istitut Jantung Negara Objectives Review the etiology and recognition
Management of acute Cardiac Arrhythmias Dr. Zulkeflee Muhammad MBChB (New Zealand), MRCP (United Kingdom) Cardiologist Electrophysiology Unit Istitut Jantung Negara Objectives Review the etiology and recognition
Refractoriness of drug-induced hypotension: Prediction and management Bruno Mégarbane
 Refractoriness of drug-induced hypotension: Prediction and management Bruno Mégarbane Department of Medical and Toxicological Critical Care, INSERM, U1144, Paris Diderot University Lariboisière Hospital,
Refractoriness of drug-induced hypotension: Prediction and management Bruno Mégarbane Department of Medical and Toxicological Critical Care, INSERM, U1144, Paris Diderot University Lariboisière Hospital,