Assessing Cardiac Risk in Noncardiac Surgery. Murali Sivarajan, M.D. Professor University of Washington Seattle, Washington
|
|
|
- Myron McGee
- 5 years ago
- Views:
Transcription
1 Assessing Cardiac Risk in Noncardiac Surgery Murali Sivarajan, M.D. Professor University of Washington Seattle, Washington
2 Disclosure None. I have no conflicts of interest, financial or otherwise.
3 CME Objectives List the risk factors identified in the Revised Cardiac Risk Index (RCRI) and by the National Surgical Quality Improvement Program (NSQIP) database. Develop risk profiles, i.e., state the probability of developing complications, using hypothetical cases. Using hypothetical cases and the American College of Cardiology-American Heart Association algorithm for Perioperative Cardiac Assessment, develop consultation/treatment plan(s).
4 Cardiac Diseases Approximately 7% of surgical patients have cardiac disease. 66% of Cardiac Patients for Noncardiac Surgery have Coronary Artery Disease. Valvular Heart Disease, Congenital Heart Disease, Cardiomyopathy etc comprise the remainder.
5 Major Adverse Cardiac Events (MACE) Perioperative Myocardial Infarction Cardiogenic Pulmonary Edema Life threatening Arrhythmias Death from Cardiac Causes
6 Mortality after a perioperative MI is high, probably ~ 30%
7 Increased Pulmonary and Cardiac complications with lower (or poorer ) ASA Physical Status Higher incidence of Perioperative Myocardial Infarction and Cardiac Death in patients with previous infarction (Tarhan et al. JAMA 1972;220:1451)
8 Cardiac Risk Index Score (CRIS) S3 Gallop or JVD 11 points MI in the previous 6 months 10 points Rhythm other than sinus 7 points More than 5 PVCs/min 7 points Age > 70 years 5 points Emergency/Major operation 4 points Aortic Stenosis 3 points Poor medical condition 3 points (Goldman et al N Engl J Med 1977;297:845)
9 CRIS underestimates complications in aortic surgery patients and overestimates complications in minor surgery patients (Detsky et al. J Gen Inter Med 1986;1:211) (Leppo et al. J Am Coll Cardiol 1987;9:269) (Schein et al. N Engl J Med 2000;342:168)
10 Revised Cardiac Risk Index (RCRI) Derived from 2893 patients Validated in 1422 patients Thoracic 13% Abdominal 13% AAA 5% Other 69% (Lee et al. Circulation 1999;100:1043)
11 Revised Cardiac Risk Index (RCRI) High Risk Surgery Ischemic Heart Disease History of CHF History Cerebrovascular Disease Insulin Dependent Diabetes Preoperative Serum Creatinine > 2 mg/dl (Lee et al. Circulation 1999;100:1043)
12 Revised Cardiac Risk Index (RCRI) Class I (no risk factors) 0.4 Class II (1 risk factor) 0.9 Class III ( 2 risk factors) 6.6 Class IV ( 3 or more) 11 Complication Rate (%) (Lee et al. Circulation 1999;100:1043)
13 Perioperative Myocardial Infarction or Cardiac Arrest Risk Calculator from NSQIP* 1. Age 2. ASA Class 3. Serum Creatinine > 1.5 mg/dl 4. Functional Status 3 states 5. Surgical Procedure 21 different types (Gupta PK et al. Circulation 2011;124: ) * National Surgical Quality Improvement Program
14 Perioperative Myocardial Infarction or Cardiac Arrest Risk Calculator from NSQIP* < (Gupta PK et al. Circulation 2011;124: ) * National Surgical Quality Improvement Program
15
16 Myocardial Ischemia Postop MI Mortality Stable Angina < 1% < 1% Unstable Angina, Acute MI < 30 days 32% 14% Recent MI 31 to 90 days 18% 11.5% Recent MI 91 to 180 days 5.9% 10% (Shah et al. Anesth Analg 1990;70:240) (Livhits et al. Ann Surg 2011;253:857)
17 Congestive Heart Failure Postoperative Pulmonary Edema 15% in uncompensated CHF 5% in well compensated CHF (Shah et al. Anesth Analg 1990;70:240) In elderly patients with CHF undergoing major surgery, 30 day postop mortality is 10% (Van Diepen et al. Circulation 2011;124:289)
18 Valvular Heart Diseases Symptomatic valvular lesions pose higher risk of postoperative myocardial infarction or heart failure Asymptomatic valvular lesions, even if severe by echocardiographic criteria, pose only minimally increased risk of postoperative cardiac complications. (2014 ACC/AHA Guidelines. J Am Coll Cardiol 2014;64:e77-157)
19 Pulmonary Hypertension In patients with pulmonary arterial hypertension, postoperative mortality is 4 to 26% And postoperative morbidity is 6 to 42% (Ramakrishna et al. J Am Coll Cardiol 2005;45:1691) (Lai et al. Br J Anaesth 2007;99:184)
20 Type of Surgery Complication Rate Low Risk Surgery (cataract, plastic, breast) Intermediate Risk Surgery (thoracic, abdominal, major orthopedic) High Risk Surgery (Aortic, trauma, emergency, sepsis) < 1% < 5% > 5% (2007 ACC/AHA Guidelines. J Am Coll Cardiol 2007;50:e241)
21 History and Physical Examination To determine Functional Status Routine Lab test
22 - Climbing 2 flights of stairs without stopping requires ~ 5 METS - How about walking 2 city blocks?

23 6 Minute Walk Test 1 MET ~ 100 meters
24 6 Minute Walk Test Normal adult males can walk 600 m (range m) in 6 minutes. One Year mortality in patients with heart disease who walk < 300 m is 10% and in those who walk > 600 m is 3%; in the same groups hospitalization for heart failure is 22% vs 2% (Bittner et al. JAMA 1993;270:1702) (Faggiano V. Eur J Heart Fail 2004;6:687)
25 Role of Additional Testing? To identify patients who might benefit from coronary revascularization
26 Echocardiography It is inappropriate to perform echocardiography (for screening purposes) in some one without symptoms or signs of cardiovascular disease (ACC/ASE/ACC Appropriate Use Criteria. J Am Coll Cardiol 2011;57:1126)
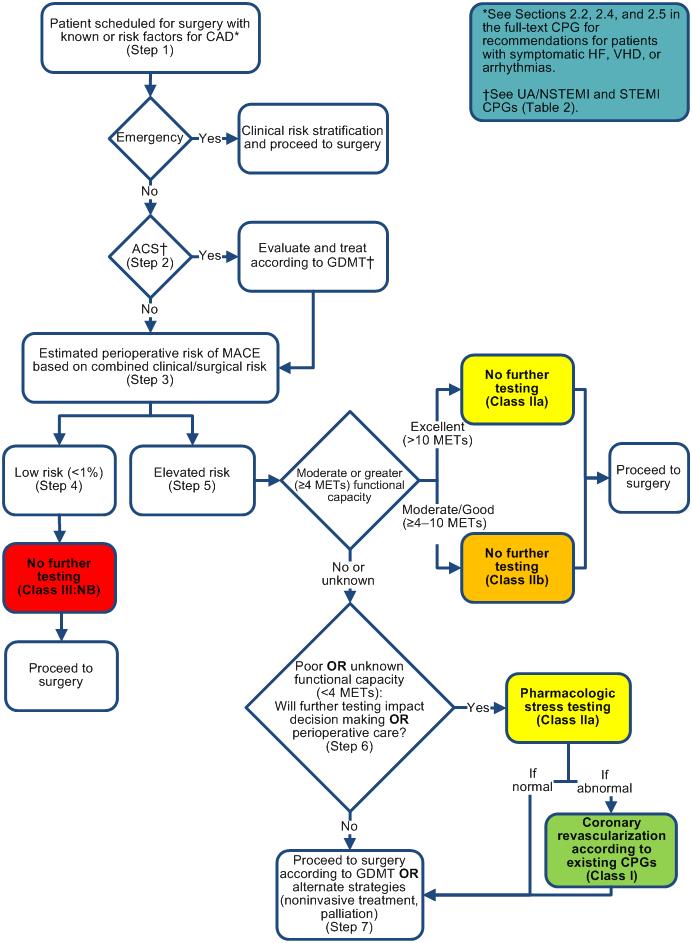
27 2014 ACC/AHA Guideline for Perioperative Cardiovascular Evaluation for Noncardiac Surgery (J Am Coll Cardiol 2014;64:e77)
28
29 Step 1 Scheduled for emergency surgery? If YES, stratify risk and proceed to surgery. Institute intensive monitoring and treatment of complications If NO, go to Step 2 (2014 ACC/AHA Guidelines. J Am Coll Cardiol 2014;64:e77)
30 Step 2 Does the patient have Acute Coronary Syndrome (myocardial infarction, unstable angina)? If YES, treat condition before surgery If NO, go to Step 3 (2014 ACC/AHA Guidelines. J Am Coll Cardiol 2014;64:e77)
31 Step 3 Is it low risk surgery? Complication rate < 1%? If YES, go to Step 4: No further testing needed; proceed to surgery If NO, proceed to Step 5 (2014 ACC/AHA Guidelines. J Am Coll Cardiol 2014;64:e77)
32 Step 5 Elevated risk surgery. Complication rate > 1% Is functional capacity > 4 METS? If YES, No further testing needed; proceed to surgery If NO, go to Step 6 (2014 ACC/AHA Guidelines. J Am Coll Cardiol 2014;64:e77)
33 Step 6 Poor functional capacity (< 4 METS) or unknown functional capacity. Will further testing impact decision making or postoperative care? If NO, proceed with surgery If YES, go to Step 7 (2014 ACC/AHA Guidelines. J Am Coll Cardiol 2014;64:e77)
34 Step 7 Perform Pharmacologic Stress Testing to detect reversible myocardial ischemia If NORMAL (no reversible ischemia), proceed to surgery If ABNORMAL (reversible ischemia present), perform coronary revascularization before surgery (2014 ACC/AHA Guidelines. J Am Coll Cardiol 2014;64:e77)

35 Perfusion Studies Alternative test for patients who can not exercise Identifies regions of reversible ischemia
36 Cardiac catheterization to determine feasibility of Angioplasty or CABG surgery before noncardiac surgery

37 CABG Before Noncardiac Surgery Risk of cardiac complications due to CABG surgery has to be taken into account
38 CABG Before Noncardiac Surgery CABG before vascular surgery reduces overall mortality only when the risk of vascular surgery exceeds the risk of CABG (Mason et al. JAMA 1995;27 3:1919)
39 Coronary Artery Revascularization Prophylaxis (CARP) Study In patients with stable angina and two vessel CAD, CABG or Angioplasty before abdominal aortic surgery compared to medical therapy offered no benefits. (McFall EO et al. N Engl J Med 2004;351: )
40 CABG before Major Vascular Surgery CABG before major vascular surgery may offer benefits only in patients in whom CABG itself offers significant survival benefits: Left main disease 3 vessel CAD with ischemic LV dysfunction Unstable angina or acute coronary syndrome

41 Angioplasty Before Noncardiac Surgery Does not seem to offer immediate protection. May increase near-term complications
42 Angioplasty Before Noncardiac Surgery Eight out of 40 patients who underwent high-risk noncardiac surgery with in 14 days of angioplasty died. Stent thrombosis was the major cause (Kaluza et al. J Am Coll Cardiol 2000;35:1288)
43 Angioplasty Before Noncardiac Surgery Dual platelet inhibition therapy should be continued for: 4-6 weeks after bare metal stents 6 months to 1year after drug eluting stents (2014 ACC/AHA Guidelines. J Am Coll Cardiol 2014;64:e77)
44 Summary History and clinical exam to derive functional capacity and routine labs to determine risk of complications are sufficient in most patients. Low Risk is complication rate < 1% High Risk is complication rate > 1%
45 Summary Revised Cardiac Risk Index (RCRI) High Risk Surgery Ischemic Heart Disease History of CHF History Cerebrovascular Disease Insulin Dependent Diabetes Preoperative Serum Creatinine > 2 mg/dl (Lee et al. Circulation 1999;100:1043)
46 Summary Perioperative Myocardial Infarction or Cardiac Arrest Risk Calculator from NSQIP* < (Gupta PK et al. Circulation 2011;124: ) * National Surgical Quality Improvement Program
47 Summary Additional testing (perfusion and catheterization studies) are needed only in a small subset of patients. Beta blockers and statins should be continued in patients who are already receiving them. Beta blockers should not be started on the day of surgery; if needed, should be started days before surgery to monitor response
48 Summary CABG before major vascular surgery is indicated only if there is survival benefit from CABG. Elective Surgery should be delayed for 4 weeks after bare metal stent and for up to one year after drug eluting stent.
49 Thank You
50 Question 1 From the list of risk factors listed below, circle the six (6) risk factors that are identified in the Revised Cardiac Risk Index (RCRI): Coronary Artery Disease Hypertension Cerebrovascular disease Smoking Chronic Obstructive Pulmonary Disease (FEV1/FVC < 50% predicted) Chronic Kidney Disease with serum creatinine > 2mg/dL Obesity Insulin dependent diabetes mellitus Alcoholic cirrhosis of the liver with ascites and esophageal varices History of congestive heart failure Atrial fibrillation Open abdominal or thoracic surgery or vascular surgery above the inguinal ligament
51 Question 2 The risk or the probability of postoperative cardiac complication in a surgical patient who has 3 or more of the risk factors identified in the Revised Cardiac Risk Index (RCRI) is approximately: A. 5% B. 10% C. 15% D. 20%
52 Question 3 A 68-year-old male was found to have a an abdominal aortic aneurysm (AAA) measuring 6 cm in diameter and he has been advised by a vascular surgeon to have an open resection of the AAA and replacement with an aorto-iliac bifurcation graft. He has stable angina precipitated by climbing 3 flights of stairs relieved by rest or sublingual nitroglycerin. He also has hypertension. He takes metoprolol and hydrochlorthiazide. Echocardiogram shows left ventricular hypertrophy with an ejection fraction = 65%. Cardiac catheterization reveals 90% stenosis of distal left anterior descending coronary artery and 80% stenosis of mid circumflex coronary artery. The best line of treatment is: A. Coronary artery bypass grafting (CABG) and AAA resection and repair at the same sitting B. CABG followed weeks later by AAA resection and repair. C. Percutaneous coronary intervention with stents followed weeks later by AAA resection and repair D. AAA resection and repair within days after medical optimization.
Cardiac evaluation for the noncardiac. Nathaen Weitzel MD University of Colorado Denver Dept of Anesthesiology
 Cardiac evaluation for the noncardiac patient Nathaen Weitzel MD University of Colorado Denver Dept of Anesthesiology Objectives! Review ACC / AHA guidelines as updated for 2009! Discuss new recommendations
Cardiac evaluation for the noncardiac patient Nathaen Weitzel MD University of Colorado Denver Dept of Anesthesiology Objectives! Review ACC / AHA guidelines as updated for 2009! Discuss new recommendations
8/28/2018. Pre-op Evaluation for non cardiac surgery. A quick review from 2007!! Disclosures. John Steuter, MD. None
 Pre-op Evaluation for non cardiac surgery John Steuter, MD Disclosures None A quick review from 2007!! Fliesheret al, ACC/AHA 2007 Guidelines on Perioperative Cardiovascular Evaluation and are for Noncardiac
Pre-op Evaluation for non cardiac surgery John Steuter, MD Disclosures None A quick review from 2007!! Fliesheret al, ACC/AHA 2007 Guidelines on Perioperative Cardiovascular Evaluation and are for Noncardiac
Perioperative Cardiovascular Evaluation and Care for Noncardiac. Dr Mahmoud Ebrahimi Interventional cardiologist 91/9/30
 Perioperative Cardiovascular Evaluation and Care for Noncardiac Surgery Dr Mahmoud Ebrahimi Interventional cardiologist 91/9/30 Active Cardiac Conditions for Which the Patient Should Undergo Evaluation
Perioperative Cardiovascular Evaluation and Care for Noncardiac Surgery Dr Mahmoud Ebrahimi Interventional cardiologist 91/9/30 Active Cardiac Conditions for Which the Patient Should Undergo Evaluation
Preoperative Cardiac Risk Assessment: Approach & Guidelines
 Preoperative Cardiac Risk Assessment: Approach & Guidelines By, Liam Morris, MD., FACC (02/03/18) CPG : Clinical Practice Guidelines GDMT : Guidelines Directed Medical Therapy GWC : Guideline Writing Committee
Preoperative Cardiac Risk Assessment: Approach & Guidelines By, Liam Morris, MD., FACC (02/03/18) CPG : Clinical Practice Guidelines GDMT : Guidelines Directed Medical Therapy GWC : Guideline Writing Committee
PERIOPERATIVE CARDIAC RISK ASSESSMENT. Divya Gollapudi, MD
 PERIOPERATIVE CARDIAC RISK ASSESSMENT Divya Gollapudi, MD Clinical Assistant Professor Hospital Medicine Program Division of General Internal Medicine Harborview Medical Center None Disclosures Objectives
PERIOPERATIVE CARDIAC RISK ASSESSMENT Divya Gollapudi, MD Clinical Assistant Professor Hospital Medicine Program Division of General Internal Medicine Harborview Medical Center None Disclosures Objectives
Perioperative Cardiac Management. Emma Sargsyan, MD, FACP
 Perioperative Cardiac Management Emma Sargsyan, MD, FACP March 22-24, 2018 Outline Evaluation of cardiac risk prior to non-cardiac surgery Management of cardiac risk for non-cardiac surgery 2 Preop medical
Perioperative Cardiac Management Emma Sargsyan, MD, FACP March 22-24, 2018 Outline Evaluation of cardiac risk prior to non-cardiac surgery Management of cardiac risk for non-cardiac surgery 2 Preop medical
PERIOPERATIVE EVALUATION AND ANESTHETIC MANAGEMENT OF PATIENTS WITH CARDIAC DISEASE FOR NON CARDIAC SURGERY
 PERIOPERATIVE EVALUATION AND ANESTHETIC MANAGEMENT OF PATIENTS WITH CARDIAC DISEASE FOR NON CARDIAC SURGERY WHICH PATIENT IS AT HIGHEST RISK? 1. 70 yo asymptomatic patient with history of heart failure
PERIOPERATIVE EVALUATION AND ANESTHETIC MANAGEMENT OF PATIENTS WITH CARDIAC DISEASE FOR NON CARDIAC SURGERY WHICH PATIENT IS AT HIGHEST RISK? 1. 70 yo asymptomatic patient with history of heart failure
Preoperative Cardiac Evaluation:
 Preoperative Cardiac Evaluation: The New Guidelines Hugo Quinny Cheng, MD Division of Hospital Medicine University of California, San Francisco Disclosures No financial relationships with pharmaceutical
Preoperative Cardiac Evaluation: The New Guidelines Hugo Quinny Cheng, MD Division of Hospital Medicine University of California, San Francisco Disclosures No financial relationships with pharmaceutical
Perioperative Cardiology Consultations for Noncardiac Surgery Ischemic Heart Disease
 2012 대한춘계심장학회 Perioperative Cardiology Consultations for Noncardiac Surgery Ischemic Heart Disease 울산의대울산대학병원심장내과이상곤 ECG CLASS IIb 1. Preoperative resting 12-lead ECG may be reasonable in patients with
2012 대한춘계심장학회 Perioperative Cardiology Consultations for Noncardiac Surgery Ischemic Heart Disease 울산의대울산대학병원심장내과이상곤 ECG CLASS IIb 1. Preoperative resting 12-lead ECG may be reasonable in patients with
Preoperative Evaluation Guidelines and Work up
 Preoperative Evaluation Guidelines and Work up Wesley Fiser, MD Disclosures: None 1 Case An 80 year old woman with osteoarthritis of the hip, DM, CKD (Cr 2.1), and HTN is diagnosed with an obstructing
Preoperative Evaluation Guidelines and Work up Wesley Fiser, MD Disclosures: None 1 Case An 80 year old woman with osteoarthritis of the hip, DM, CKD (Cr 2.1), and HTN is diagnosed with an obstructing
Conflicts of Interest. Evaluation of Cardiac and Pulmonary Risk in the Preop Patient. Introduction. Risk Assessment. Risk Assessment: RCRI
 Evaluation of Cardiac and Pulmonary Risk in the Preop Patient Conflicts of Interest I have no conflicts of interest to declare Adam Schaffer, MD Brigham and Women s Hospital July 20, 2012 Introduction
Evaluation of Cardiac and Pulmonary Risk in the Preop Patient Conflicts of Interest I have no conflicts of interest to declare Adam Schaffer, MD Brigham and Women s Hospital July 20, 2012 Introduction
Guidelines PATHOLOGY: FATAL PERIOPERATIVE MI NON-PMI N = 25 PMI N = 42. Prominent Dutch Cardiovascular Researcher Fired for Scientific Misconduct
 PATHOLOGY: FATAL PERIOPERATIVE MI NON-PMI N = 25 PMI N = 42 Preoperative, Intraoperative, and Postoperative Factors Associated with Perioperative Cardiac Complications in Patients Undergoing Major Noncardiac
PATHOLOGY: FATAL PERIOPERATIVE MI NON-PMI N = 25 PMI N = 42 Preoperative, Intraoperative, and Postoperative Factors Associated with Perioperative Cardiac Complications in Patients Undergoing Major Noncardiac
Q: Do cardiac risk stratification indexes
 1-MINUTE CONSULT ROHAN MANDALIYA, MD, FACP Clinical Fellow, Division of Gastroenterology and Hepatology, Department of Medicine, Georgetown University Hospital, Washington, DC GENO MERLI, MD, MACP Professor
1-MINUTE CONSULT ROHAN MANDALIYA, MD, FACP Clinical Fellow, Division of Gastroenterology and Hepatology, Department of Medicine, Georgetown University Hospital, Washington, DC GENO MERLI, MD, MACP Professor
The MAIN-COMPARE Study
 Long-Term Outcomes of Coronary Stent Implantation versus Bypass Surgery for the Treatment of Unprotected Left Main Coronary Artery Disease Revascularization for Unprotected Left MAIN Coronary Artery Stenosis:
Long-Term Outcomes of Coronary Stent Implantation versus Bypass Surgery for the Treatment of Unprotected Left Main Coronary Artery Disease Revascularization for Unprotected Left MAIN Coronary Artery Stenosis:
Indications of Coronary Angiography Dr. Shaheer K. George, M.D Faculty of Medicine, Mansoura University 2014
 Indications of Coronary Angiography Dr. Shaheer K. George, M.D Faculty of Medicine, Mansoura University 2014 Indications for cardiac catheterization Before a decision to perform an invasive procedure such
Indications of Coronary Angiography Dr. Shaheer K. George, M.D Faculty of Medicine, Mansoura University 2014 Indications for cardiac catheterization Before a decision to perform an invasive procedure such
Pre-op Risk Assessment. Hal Blanks MD FACC
 Pre-op Risk Assessment Hal Blanks MD FACC Objectives: Identify and manage patients with known or suspected CAD and other cardiac diseases who are at risk of cardiac complications during noncardiac surgery.
Pre-op Risk Assessment Hal Blanks MD FACC Objectives: Identify and manage patients with known or suspected CAD and other cardiac diseases who are at risk of cardiac complications during noncardiac surgery.
Pre-operative Evaluations. Objectives. General Considerations. FP Consultation Considerations. CV Credits 7/24/2017. Brian Bachelder, MD Akron, Ohio
 Pre-operative Evaluations Brian Bachelder, MD Akron, Ohio Objectives Discuss the perioperative cardiopulmonary evaluation and management of patients undergoing non-cardiac surgery Objectively estimate
Pre-operative Evaluations Brian Bachelder, MD Akron, Ohio Objectives Discuss the perioperative cardiopulmonary evaluation and management of patients undergoing non-cardiac surgery Objectively estimate
SESSION 5 2:20 3:35 pm
 SESSION 2:2 3:3 pm Strategies to Reduce Cardiac Risk for Noncardiac Surgery SPEAKER Lee A. Fleisher, MD Presenter Disclosure Information The following relationships exist related to this presentation:
SESSION 2:2 3:3 pm Strategies to Reduce Cardiac Risk for Noncardiac Surgery SPEAKER Lee A. Fleisher, MD Presenter Disclosure Information The following relationships exist related to this presentation:
Pre-Operative Services Teaching Rounds 3 Jan 2011
 Pre-Operative Services Teaching Rounds 3 Jan 2011 Deborah Richman MBChB FFA(SA) Director Pre-Operative Services Department of Anesthesia Stony Brook University Medical Center, NY drichman@notes.cc.sunysb.edu
Pre-Operative Services Teaching Rounds 3 Jan 2011 Deborah Richman MBChB FFA(SA) Director Pre-Operative Services Department of Anesthesia Stony Brook University Medical Center, NY drichman@notes.cc.sunysb.edu
COMPARISON OF 2014 ACCAHA VS. ESC GUIDELINES EDITORIAL
 COMPARISON OF 2014 ACCAHA VS. ESC GUIDELINES EDITORIAL Guidelines in review: Comparison of the 2014 ACC/AHA guidelines on perioperative cardiovascular evaluation and management of patients undergoing noncardiac
COMPARISON OF 2014 ACCAHA VS. ESC GUIDELINES EDITORIAL Guidelines in review: Comparison of the 2014 ACC/AHA guidelines on perioperative cardiovascular evaluation and management of patients undergoing noncardiac
Perioperative Medicine 2016 Some Answers, Even More Questions
 Learning Objectives Perioperative Medicine 2016 Some Answers, Even More Questions Kurt Pfeifer, MD, FACP, FHM Professor of Medicine Medical College of Wisconsin Outline changes to the ACC/AHA perioperative
Learning Objectives Perioperative Medicine 2016 Some Answers, Even More Questions Kurt Pfeifer, MD, FACP, FHM Professor of Medicine Medical College of Wisconsin Outline changes to the ACC/AHA perioperative
DUKECATHR Dataset Dictionary
 DUKECATHR Dataset Dictionary Version of DUKECATH dataset for educational use that has been modified to be unsuitable for clinical research or publication (Created Date and Time: 28OCT16 14:35) Table of
DUKECATHR Dataset Dictionary Version of DUKECATH dataset for educational use that has been modified to be unsuitable for clinical research or publication (Created Date and Time: 28OCT16 14:35) Table of
Agenda. Perioperative Cardiac Risk Stratification circa Surgical Mortality: What is High Risk? Presenter Disclosure Information
 9:45 1:45 am Perioperative Evaluation and Management of the Cardiac Patient in Noncardiac Surgery SPEAKER Joshua A. Beckman, MD, MS Presenter Disclosure Information The following relationships exist related
9:45 1:45 am Perioperative Evaluation and Management of the Cardiac Patient in Noncardiac Surgery SPEAKER Joshua A. Beckman, MD, MS Presenter Disclosure Information The following relationships exist related
Perioperative Cardiovascular Evaluation and Care for Noncardiac Surgery
 Perioperative Cardiovascular Evaluation and Care for Noncardiac Surgery 2008 Update Plus Overview of the Guidelines Concept John Coyle, M.D. October 16, 2008 The History of Medicine As Mountaineering Feat
Perioperative Cardiovascular Evaluation and Care for Noncardiac Surgery 2008 Update Plus Overview of the Guidelines Concept John Coyle, M.D. October 16, 2008 The History of Medicine As Mountaineering Feat
Cardiac Risk Assessment in the Preoperative period
 Cardiac Risk Assessment in the Preoperative period Catherine Curley, MD May, 2017 Disclosures I am not a cardiologist! 1 Case 1 78 yo man presenting to the ED after mechanical fall on his driveway. Found
Cardiac Risk Assessment in the Preoperative period Catherine Curley, MD May, 2017 Disclosures I am not a cardiologist! 1 Case 1 78 yo man presenting to the ED after mechanical fall on his driveway. Found
Timing of Surgery After Percutaneous Coronary Intervention
 Timing of Surgery After Percutaneous Coronary Intervention Deepak Talreja, MD, FACC Bayview/EVMS/Sentara Outline/Highlights Timing of elective surgery What to do with medications Stopping anti-platelet
Timing of Surgery After Percutaneous Coronary Intervention Deepak Talreja, MD, FACC Bayview/EVMS/Sentara Outline/Highlights Timing of elective surgery What to do with medications Stopping anti-platelet
Detailed Order Request Checklists for Cardiology
 Next Generation Solutions Detailed Order Request Checklists for Cardiology 8600 West Bryn Mawr Avenue South Tower Suite 800 Chicago, IL 60631 www.aimspecialtyhealth.com Appropriate.Safe.Affordable 2018
Next Generation Solutions Detailed Order Request Checklists for Cardiology 8600 West Bryn Mawr Avenue South Tower Suite 800 Chicago, IL 60631 www.aimspecialtyhealth.com Appropriate.Safe.Affordable 2018
Clinical Controversies in Perioperative Medicine
 Clinical Controversies in Perioperative Medicine Hugo Quinny Cheng, MD Division of Hospital Medicine University of California, San Francisco Predicting & Managing Cardiac Risk A 70-y.o. man with progressive
Clinical Controversies in Perioperative Medicine Hugo Quinny Cheng, MD Division of Hospital Medicine University of California, San Francisco Predicting & Managing Cardiac Risk A 70-y.o. man with progressive
Coronary Artery Disease: Revascularization (Teacher s Guide)
") Stephanie Chan, M.D. Updated 3/15/13 2008-2013, SCVMC (40 minutes) I. Objectives Coronary Artery Disease: Revascularization (Teacher s Guide) To review the evidence on whether percutaneous coronary intervention
Stephanie Chan, M.D. Updated 3/15/13 2008-2013, SCVMC (40 minutes) I. Objectives Coronary Artery Disease: Revascularization (Teacher s Guide) To review the evidence on whether percutaneous coronary intervention
Clinical Controversies in Perioperative Medicine
 Clinical Controversies in Perioperative Medicine Hugo Quinny Cheng, MD Division of Hospital Medicine University of California, San Francisco Cardiac Evaluation: New Guidelines A 70-y.o. man with progressive
Clinical Controversies in Perioperative Medicine Hugo Quinny Cheng, MD Division of Hospital Medicine University of California, San Francisco Cardiac Evaluation: New Guidelines A 70-y.o. man with progressive
Perioperative Decision Making The decision has been made to proceed with operative management timing and site of surgery the type of anesthesia preope
 Preoperative Evaluation In Endocrine Disorders Dr Nahid Zirak 2012 Perioperative Decision Making The decision has been made to proceed with operative management timing and site of surgery the type of anesthesia
Preoperative Evaluation In Endocrine Disorders Dr Nahid Zirak 2012 Perioperative Decision Making The decision has been made to proceed with operative management timing and site of surgery the type of anesthesia
Update on Perioperative Medicine. Update on Perioperative Medicine. Question 1: Clinical Risk Prediction. for the Office-based Practitioner
 Update on Perioperative Medicine Update on Perioperative Medicine for the Office-based Practitioner Hugo Quinny Cheng, MD Division of Hospital Medicine University of California, San Francisco Predicting
Update on Perioperative Medicine Update on Perioperative Medicine for the Office-based Practitioner Hugo Quinny Cheng, MD Division of Hospital Medicine University of California, San Francisco Predicting
The MAIN-COMPARE Registry
 Long-Term Outcomes of Coronary Stent Implantation versus Bypass Surgery for the Treatment of Unprotected Left Main Coronary Artery Disease Revascularization for Unprotected Left MAIN Coronary Artery Stenosis:
Long-Term Outcomes of Coronary Stent Implantation versus Bypass Surgery for the Treatment of Unprotected Left Main Coronary Artery Disease Revascularization for Unprotected Left MAIN Coronary Artery Stenosis:
by Brian Wolfe, MD Assistant Professor of Medicine, University of Colorado Denver
 Perioperative Cases by Brian Wolfe, MD Assistant Professor of Medicine, University of Colorado Denver 75 yo for left knee arthroplasty Problem List Social Hx: obesity uses a walker diabetes because of
Perioperative Cases by Brian Wolfe, MD Assistant Professor of Medicine, University of Colorado Denver 75 yo for left knee arthroplasty Problem List Social Hx: obesity uses a walker diabetes because of
Agenda. Disclosures. Surgical Mortality: What is High Risk?
 Pre-Operative Cardiac Evaluation of the Vascular Patient: Updated AHA/ACC Guidelines Choosing Wisely UCSF Vascular Symposium 2015 Joshua A. Beckman, M.D., M.S. Brigham and Women s Hospital Consulting Merck
Pre-Operative Cardiac Evaluation of the Vascular Patient: Updated AHA/ACC Guidelines Choosing Wisely UCSF Vascular Symposium 2015 Joshua A. Beckman, M.D., M.S. Brigham and Women s Hospital Consulting Merck
Perioperative Medical Therapy: Beta Blockers, Statins, ACE-Inhibitors, ARB Effects on Mortality
 Perioperative Medical Therapy: Beta Blockers, Statins, ACE-Inhibitors, ARB Effects on Mortality Art Wallace, MD, PhD SF VAMC Chief of Anethesia and Vice Chair of Anesthesia and Perioperative Care UCSF
Perioperative Medical Therapy: Beta Blockers, Statins, ACE-Inhibitors, ARB Effects on Mortality Art Wallace, MD, PhD SF VAMC Chief of Anethesia and Vice Chair of Anesthesia and Perioperative Care UCSF
AMERICAN SOCIETY OF ANESTHESIOLOGISTS ANESTHESIA PRE OPERATIVE SCREENING ASA PHYSICAL STATUS CLASSIFICATION ANESTHESIOLOGISTS
 ANESTHESIA PRE OPERATIVE SCREENING CAPA S 37 TH ANNUAL CONFERENCE PALM SPRINGS OCTOBER 5, 2013 ROBERT F. KOPEL, MD, FACP, FCCP HOAG HOSPITAL ASSISTANT CLINICAL PROFESSOR UCLA SCHOOL OF MEDICINE AMERICAN
ANESTHESIA PRE OPERATIVE SCREENING CAPA S 37 TH ANNUAL CONFERENCE PALM SPRINGS OCTOBER 5, 2013 ROBERT F. KOPEL, MD, FACP, FCCP HOAG HOSPITAL ASSISTANT CLINICAL PROFESSOR UCLA SCHOOL OF MEDICINE AMERICAN
Preoperative Cardiac Evaluation of Patients With Acute Hip Fracture
 An Original Study Preoperative Cardiac Evaluation of Patients With Acute Hip Fracture Jonathan Cluett, MD, Jill Caplan, MD, and Warren Yu, MD Abstract The goals of the present study were to assess if there
An Original Study Preoperative Cardiac Evaluation of Patients With Acute Hip Fracture Jonathan Cluett, MD, Jill Caplan, MD, and Warren Yu, MD Abstract The goals of the present study were to assess if there
PERIOPERATIVE ANESTHETIC RISK IN THE GERIATRIC PATIENT
 PERIOPERATIVE ANESTHETIC RISK IN THE GERIATRIC PATIENT Susan H. Noorily, M.D. Clinical Professor of Anesthesiology Medical Director University Preoperative Medicine Center IMPORTANCE Half of all currently
PERIOPERATIVE ANESTHETIC RISK IN THE GERIATRIC PATIENT Susan H. Noorily, M.D. Clinical Professor of Anesthesiology Medical Director University Preoperative Medicine Center IMPORTANCE Half of all currently
NIH Public Access Author Manuscript Ann Vasc Surg. Author manuscript; available in PMC 2014 July 01.
 NIH Public Access Author Manuscript Published in final edited form as: Ann Vasc Surg. 2013 July ; 27(5): 646 654. doi:10.1016/j.avsg.2012.07.024. Contemporary outcomes in vascular patients who require
NIH Public Access Author Manuscript Published in final edited form as: Ann Vasc Surg. 2013 July ; 27(5): 646 654. doi:10.1016/j.avsg.2012.07.024. Contemporary outcomes in vascular patients who require
Supplementary Material to Mayer et al. A comparative cohort study on personalised
 Suppl. Table : Baseline characteristics of the patients. Characteristic Modified cohort Non-modified cohort P value (n=00) Age years 68. ±. 69.5 ±. 0. Female sex no. (%) 60 (0.0) 88 (.7) 0.0 Body Mass
Suppl. Table : Baseline characteristics of the patients. Characteristic Modified cohort Non-modified cohort P value (n=00) Age years 68. ±. 69.5 ±. 0. Female sex no. (%) 60 (0.0) 88 (.7) 0.0 Body Mass
Stable Ischemic Heart Disease. Ivan Anderson, MD RIHVH Cardiology
 Stable Ischemic Heart Disease Ivan Anderson, MD RIHVH Cardiology Outline Review of the vascular biology of atherosclerosis Why not just cath everyone with angina? Medical management of ischemic cardiomyopathy
Stable Ischemic Heart Disease Ivan Anderson, MD RIHVH Cardiology Outline Review of the vascular biology of atherosclerosis Why not just cath everyone with angina? Medical management of ischemic cardiomyopathy
Preoperative Management. Presley Regional Trauma Center Department of Surgery University of Tennessee Health Science Center Memphis, Tennessee
 Preoperative Management Presley Regional Trauma Center Department of Surgery University of Tennessee Health Science Center Memphis, Tennessee Perioperative Care Consideration Medical care provided to prepare
Preoperative Management Presley Regional Trauma Center Department of Surgery University of Tennessee Health Science Center Memphis, Tennessee Perioperative Care Consideration Medical care provided to prepare
AAA CAG CAG. ACC / AHA Guidelines for Perioperative Cardiovascular Evaluation for Noncardiac. Group Group AAA AAA.
 13 591 596 2004 AAA CAG CAG 5527 15 CAG ACC / AHA Guidelines for Perioperative Cardiovascular Evaluation for Noncardiac Surgery CAG 55 34 62CAG 75 CAG 73 63 66 ACC / AHA CAGGroup 1 9 8 Group 225 22 Group
13 591 596 2004 AAA CAG CAG 5527 15 CAG ACC / AHA Guidelines for Perioperative Cardiovascular Evaluation for Noncardiac Surgery CAG 55 34 62CAG 75 CAG 73 63 66 ACC / AHA CAGGroup 1 9 8 Group 225 22 Group
2010, Metzler Helfried
 Perioperative Strategies in Patients on Dual Antiplatelet Drug Therapy: Noncardiac Surgery H. Metzler Department of Anaesthesiology and Intensive Care Medicine Medical University of Graz, Austria What
Perioperative Strategies in Patients on Dual Antiplatelet Drug Therapy: Noncardiac Surgery H. Metzler Department of Anaesthesiology and Intensive Care Medicine Medical University of Graz, Austria What
Objectives. Old School. Preoperative Evaluation and Postoperative Complications: Where are the opportunities for risk reduction?
 Preoperative Evaluation and Postoperative Complications: Where are the opportunities for risk reduction? Jeffrey Carter, MD RMHMS October 5, 2010 Objectives Understand the preoperative cardiac evaluation
Preoperative Evaluation and Postoperative Complications: Where are the opportunities for risk reduction? Jeffrey Carter, MD RMHMS October 5, 2010 Objectives Understand the preoperative cardiac evaluation
4/27/2015. Cardiac Events #1 cause of postoperative complications/ mortality- CHF, complete heart block, MI,
 Not intended for medical clearance Identify, document, and evaluate health conditions Medication Management Stratify Risks Optimize conditions within context of surgical illness Recommend measures that
Not intended for medical clearance Identify, document, and evaluate health conditions Medication Management Stratify Risks Optimize conditions within context of surgical illness Recommend measures that
Preoperative Cardiac Risk Calculators
 The Fort Lauderdale, Florida Preoperative Cardiac Risk Calculators Steven L. Cohn, MD, FACP, SFHM Professor Emeritus Director - Medical Consultation Service Jackson Memorial Hospital University of Miami
The Fort Lauderdale, Florida Preoperative Cardiac Risk Calculators Steven L. Cohn, MD, FACP, SFHM Professor Emeritus Director - Medical Consultation Service Jackson Memorial Hospital University of Miami
Quality Measures MIPS CV Specific
 Quality Measures MIPS CV Specific MEASURE NAME Atrial Fibrillation and Atrial Flutter: Chronic Anticoagulation Therapy CAHPS for MIPS Clinician/Group Survey Cardiac Rehabilitation Patient Referral from
Quality Measures MIPS CV Specific MEASURE NAME Atrial Fibrillation and Atrial Flutter: Chronic Anticoagulation Therapy CAHPS for MIPS Clinician/Group Survey Cardiac Rehabilitation Patient Referral from
Safety of Single- Versus Multi-vessel Angioplasty for Patients with AMI and Multi-vessel CAD
 Safety of Single- Versus Multi-vessel Angioplasty for Patients with AMI and Multi-vessel CAD Mun K. Hong, MD Associate Professor of Medicine Director, Cardiovascular Intervention and Research Weill Cornell
Safety of Single- Versus Multi-vessel Angioplasty for Patients with AMI and Multi-vessel CAD Mun K. Hong, MD Associate Professor of Medicine Director, Cardiovascular Intervention and Research Weill Cornell
Perioperative myocardial infarction is a major cause of morbidity and mortality in patients who
 Focused Issue of This Month Anesthesia for Noncardiac Surgery in the Patients with Cardiac Disease Kyung Yeon Yoo, MD Department of Anesthesiology and Pain Medicine, Chonnam National University College
Focused Issue of This Month Anesthesia for Noncardiac Surgery in the Patients with Cardiac Disease Kyung Yeon Yoo, MD Department of Anesthesiology and Pain Medicine, Chonnam National University College
2018 David Stultz. The Consultant s Job
 The Consultant s Job Cardiac Pre-Operative Evaluation ACC 2014 Guidelines David Stultz, MD September 8, 2017 www.drstultz.com KPN Heart & Vascular Objectives of Conference Understand Cardiac Clearance
The Consultant s Job Cardiac Pre-Operative Evaluation ACC 2014 Guidelines David Stultz, MD September 8, 2017 www.drstultz.com KPN Heart & Vascular Objectives of Conference Understand Cardiac Clearance
Asif Serajian DO FACC FSCAI
 Anticoagulation and Antiplatelet update: A case based approach Asif Serajian DO FACC FSCAI No disclosures relevant to this talk Objectives 1. Discuss the indication for antiplatelet therapy for cardiac
Anticoagulation and Antiplatelet update: A case based approach Asif Serajian DO FACC FSCAI No disclosures relevant to this talk Objectives 1. Discuss the indication for antiplatelet therapy for cardiac
IHCP bulletin INDIANA HEALTH COVERAGE PROGRAMS BT JANUARY 24, 2012
 IHCP bulletin INDIANA HEALTH COVERAGE PROGRAMS BT201203 JANUARY 24, 2012 The IHCP to reimburse implantable cardioverter defibrillators separately from outpatient implantation Effective March 1, 2012, the
IHCP bulletin INDIANA HEALTH COVERAGE PROGRAMS BT201203 JANUARY 24, 2012 The IHCP to reimburse implantable cardioverter defibrillators separately from outpatient implantation Effective March 1, 2012, the
Perioperative Medicine 2017 November 3, Disclosures
 Perioperative Medicine 2017 November 3, 2017 Scott Marsal, MD MSc FACP Chief, Medicine Division Medical Director, Quality & Patient Safety Providence St. Vincent Medical Center Disclosures No conflicts
Perioperative Medicine 2017 November 3, 2017 Scott Marsal, MD MSc FACP Chief, Medicine Division Medical Director, Quality & Patient Safety Providence St. Vincent Medical Center Disclosures No conflicts
HEART AND SOUL STUDY OUTCOME EVENT - MORBIDITY REVIEW FORM
 REVIEW DATE REVIEWER'S ID HEART AND SOUL STUDY OUTCOME EVENT - MORBIDITY REVIEW FORM : DISCHARGE DATE: RECORDS FROM: Hospitalization ER Please check all that may apply: Myocardial Infarction Pages 2, 3,
REVIEW DATE REVIEWER'S ID HEART AND SOUL STUDY OUTCOME EVENT - MORBIDITY REVIEW FORM : DISCHARGE DATE: RECORDS FROM: Hospitalization ER Please check all that may apply: Myocardial Infarction Pages 2, 3,
Supplementary Online Content
 Supplementary Online Content Inohara T, Manandhar P, Kosinski A, et al. Association of renin-angiotensin inhibitor treatment with mortality and heart failure readmission in patients with transcatheter
Supplementary Online Content Inohara T, Manandhar P, Kosinski A, et al. Association of renin-angiotensin inhibitor treatment with mortality and heart failure readmission in patients with transcatheter
Cardiovascular Disorders Lecture 3 Coronar Artery Diseases
 Cardiovascular Disorders Lecture 3 Coronar Artery Diseases By Prof. El Sayed Abdel Fattah Eid Lecturer of Internal Medicine Delta University Coronary Heart Diseases It is the leading cause of death in
Cardiovascular Disorders Lecture 3 Coronar Artery Diseases By Prof. El Sayed Abdel Fattah Eid Lecturer of Internal Medicine Delta University Coronary Heart Diseases It is the leading cause of death in
D M Y Y Y Y D D M M Y Y Y Y. Previous MI (apart from acute PCI) 0=no 1=yes 9=unknown
 0=no 1=yes 9=unknown") I Patient details and Preoperative Data Date of Informed Consent dd-mm-yyyy (Please leave blank if waived by Ethics Committee) Please enter Patient ID in this format xxx-xx-xxx 3 digit code for the country,
I Patient details and Preoperative Data Date of Informed Consent dd-mm-yyyy (Please leave blank if waived by Ethics Committee) Please enter Patient ID in this format xxx-xx-xxx 3 digit code for the country,
Update in Perioperative Medicine
 Update in Perioperative Medicine Linda Venner MD FACP March 2018 Agenda 1 2 3 4 5 Optimized not Cleared Identify red flags for cardiac and pulmonary complications Optimize management Prevent delirium Don
Update in Perioperative Medicine Linda Venner MD FACP March 2018 Agenda 1 2 3 4 5 Optimized not Cleared Identify red flags for cardiac and pulmonary complications Optimize management Prevent delirium Don
Common Codes for ICD-10
 Common Codes for ICD-10 Specialty: Cardiology *Always utilize more specific codes first. ABNORMALITIES OF HEART RHYTHM ICD-9-CM Codes: 427.81, 427.89, 785.0, 785.1, 785.3 R00.0 Tachycardia, unspecified
Common Codes for ICD-10 Specialty: Cardiology *Always utilize more specific codes first. ABNORMALITIES OF HEART RHYTHM ICD-9-CM Codes: 427.81, 427.89, 785.0, 785.1, 785.3 R00.0 Tachycardia, unspecified
I have no disclosures
 Preparing patients for out of hospital anesthesia BobbieJean Sweitzer, M.D. Director, Anesthesia Perioperative Medicine Clinic Professor of Anesthesia and Critical Care Professor of Medicine University
Preparing patients for out of hospital anesthesia BobbieJean Sweitzer, M.D. Director, Anesthesia Perioperative Medicine Clinic Professor of Anesthesia and Critical Care Professor of Medicine University
Preoperative Cardiac Evaluation. Preoperative Cardiac Evaluation Prior to Noncardiac Surgery
 Prior to Noncardiac Surgery Carmine D Amico, D.O. Overview Learning objectives Introduction Procedure risk categorization Preoperative estimation of cardiac risk Stepwise approach to preoperative evaluation
Prior to Noncardiac Surgery Carmine D Amico, D.O. Overview Learning objectives Introduction Procedure risk categorization Preoperative estimation of cardiac risk Stepwise approach to preoperative evaluation
Managing Hypertension in the Perioperative Arena
 Managing Hypertension in the Perioperative Arena Optimizing Perioperative Management Strategies for Hypertension in the Cardiac Surgical Patient Objectives: Treatment of hypertensive emergencies. ALBERT
Managing Hypertension in the Perioperative Arena Optimizing Perioperative Management Strategies for Hypertension in the Cardiac Surgical Patient Objectives: Treatment of hypertensive emergencies. ALBERT
Cardiovascular Health Practice Guideline Outpatient Management of Coronary Artery Disease 2003
 Authorized By: Medical Management Guideline Committee Approval Date: 12/13/01 Revision Date: 12/11/03 Beta-Blockers Nitrates Calcium Channel Blockers MEDICATIONS Indicated in post-mi, unstable angina,
Authorized By: Medical Management Guideline Committee Approval Date: 12/13/01 Revision Date: 12/11/03 Beta-Blockers Nitrates Calcium Channel Blockers MEDICATIONS Indicated in post-mi, unstable angina,
Preoperative Evaluation of Patients Undergoing Noncardiac Surgery
 Preoperative Evaluation of Patients Undergoing Noncardiac Surgery Shazia Khan, MD Assistant Professor of Clinical Medicine Keck School of Medicine LAC+USC Medical Center Learning Objectives Use a risk
Preoperative Evaluation of Patients Undergoing Noncardiac Surgery Shazia Khan, MD Assistant Professor of Clinical Medicine Keck School of Medicine LAC+USC Medical Center Learning Objectives Use a risk
SUPPLEMENTAL MATERIAL
 SUPPLEMENTAL MATERIAL Table S1: Number and percentage of patients by age category Distribution of age Age
SUPPLEMENTAL MATERIAL Table S1: Number and percentage of patients by age category Distribution of age Age
LM stenting - Cypher
 LM stenting - Cypher Left main stenting with BMS Since 1995 Issues in BMS era AMC Restenosis and TLR (%) 3 27 TLR P=.282 Restenosis P=.71 28 2 1 15 12 Ostium 5 4 Shaft Bifurcation Left main stenting with
LM stenting - Cypher Left main stenting with BMS Since 1995 Issues in BMS era AMC Restenosis and TLR (%) 3 27 TLR P=.282 Restenosis P=.71 28 2 1 15 12 Ostium 5 4 Shaft Bifurcation Left main stenting with
Controversies in Cardiac Pharmacology
 Controversies in Cardiac Pharmacology Thomas D. Conley, MD FACC FSCAI Disclosures I have no relevant relationships with commercial interests to disclose. 1 Doc, do I really need to take all these medicines?
Controversies in Cardiac Pharmacology Thomas D. Conley, MD FACC FSCAI Disclosures I have no relevant relationships with commercial interests to disclose. 1 Doc, do I really need to take all these medicines?
Managing Cardiac & Pulmonary Risk in the Surgical Patient
 Managing Cardiac & Pulmonary Risk in the Surgical Patient Hugo Quinny Cheng, MD Division of Hospital Medicine University of California, San Francisco Preoperative Evaluation Guidelines Cardiac: Fleisher
Managing Cardiac & Pulmonary Risk in the Surgical Patient Hugo Quinny Cheng, MD Division of Hospital Medicine University of California, San Francisco Preoperative Evaluation Guidelines Cardiac: Fleisher
My Patient Needs a Stress Test
 My Patient Needs a Stress Test Amy S. Burhanna,, MD, FACC Coastal Cardiology Cape May Court House, New Jersey Absolute and relative contraindications to exercise testing Absolute Acute myocardial infarction
My Patient Needs a Stress Test Amy S. Burhanna,, MD, FACC Coastal Cardiology Cape May Court House, New Jersey Absolute and relative contraindications to exercise testing Absolute Acute myocardial infarction
TCTAP Upendra Kaul MD,DM,FACC,FSCAI,FAMS,FCSI
 Indian TUXEDO Trial In Medically Treated Diabetics Upendra Kaul MD,DM,FACC,FSCAI,FAMS,FCSI Executive Director and Dean Escorts Heart Institute & Medical Research Center and Fortis Hospitals, New Delhi
Indian TUXEDO Trial In Medically Treated Diabetics Upendra Kaul MD,DM,FACC,FSCAI,FAMS,FCSI Executive Director and Dean Escorts Heart Institute & Medical Research Center and Fortis Hospitals, New Delhi
Controversies in Perioperative Medicine
 Controversies in Perioperative Medicine Staying Abreast & Ahead of the Guidelines Hugo Quinny Cheng, MD Division of Hospital Medicine University of California, San Francisco Controversies in Perioperative
Controversies in Perioperative Medicine Staying Abreast & Ahead of the Guidelines Hugo Quinny Cheng, MD Division of Hospital Medicine University of California, San Francisco Controversies in Perioperative
Cardiovascular Nursing Practice: A Comprehensive Resource Manual and Study Guide for Clinical Nurses 2 nd Edition
 Cardiovascular Nursing Practice: A Comprehensive Resource Manual and Study Guide for Clinical Nurses 2 nd Edition Table of Contents Volume 1 Chapter 1: Cardiovascular Anatomy and Physiology Basic Cardiac
Cardiovascular Nursing Practice: A Comprehensive Resource Manual and Study Guide for Clinical Nurses 2 nd Edition Table of Contents Volume 1 Chapter 1: Cardiovascular Anatomy and Physiology Basic Cardiac
7. Echocardiography Appropriate Use Criteria (by Indication)
") Criteria for Echocardiography 1133 7. Echocardiography Criteria (by ) Table 1. TTE for General Evaluation of Cardiac Structure and Function Suspected Cardiac Etiology General With TTE 1. Symptoms or conditions
Criteria for Echocardiography 1133 7. Echocardiography Criteria (by ) Table 1. TTE for General Evaluation of Cardiac Structure and Function Suspected Cardiac Etiology General With TTE 1. Symptoms or conditions
Lessons learned From The National PCI Registry
 Lessons learned From The National PCI Registry w a v e On Behalf of The Publication Committee of the National PCI Registry Objectives & Anticipated Achievements To determine the epidemiology of patients
Lessons learned From The National PCI Registry w a v e On Behalf of The Publication Committee of the National PCI Registry Objectives & Anticipated Achievements To determine the epidemiology of patients
Why is co-morbidity important for cancer patients? Di Riley Associate Director Clinical Outcomes Programme
 Why is co-morbidity important for cancer patients? Di Riley Associate Director Clinical Outcomes Programme Co-morbidity in cancer Definition:- Co-morbidity is a disease or illness affecting a cancer patient
Why is co-morbidity important for cancer patients? Di Riley Associate Director Clinical Outcomes Programme Co-morbidity in cancer Definition:- Co-morbidity is a disease or illness affecting a cancer patient
WHI Form Report of Cardiovascular Outcome Ver (For items 1-11, each question specifies mark one or mark all that apply.
 WHI Form - Report of Cardiovascular Outcome Ver. 6. COMMENTS To be completed by Physician Adjudicator Date Completed: - - (M/D/Y) Adjudicator Code: OMB# 095-044 Exp: 4/06 -Affix label here- Clinical Center/ID:
WHI Form - Report of Cardiovascular Outcome Ver. 6. COMMENTS To be completed by Physician Adjudicator Date Completed: - - (M/D/Y) Adjudicator Code: OMB# 095-044 Exp: 4/06 -Affix label here- Clinical Center/ID:
Supplementary Table S1: Proportion of missing values presents in the original dataset
 Supplementary Table S1: Proportion of missing values presents in the original dataset Variable Included (%) Missing (%) Age 89067 (100.0) 0 (0.0) Gender 89067 (100.0) 0 (0.0) Smoking status 80706 (90.6)
Supplementary Table S1: Proportion of missing values presents in the original dataset Variable Included (%) Missing (%) Age 89067 (100.0) 0 (0.0) Gender 89067 (100.0) 0 (0.0) Smoking status 80706 (90.6)
Surgery for patients with diffuse atherosclerotic disease
 Surgery for patients with diffuse atherosclerotic disease Special hospital for surgery Skopje Macedonia September, 2012 Mitrev Z, Anguseva T, E.Stoicovski, Hristov N, E.Idoski Oktomvri, 2008 Atherosclerosis
Surgery for patients with diffuse atherosclerotic disease Special hospital for surgery Skopje Macedonia September, 2012 Mitrev Z, Anguseva T, E.Stoicovski, Hristov N, E.Idoski Oktomvri, 2008 Atherosclerosis
Unprotected LM intervention
 Unprotected LM intervention Guideline for COMBAT Seung-Jung Park, MD, PhD Professor of Internal Medicine, Seoul, Korea Current Recommendation for unprotected LMCA Stenosis Class IIb C in ESC guideline
Unprotected LM intervention Guideline for COMBAT Seung-Jung Park, MD, PhD Professor of Internal Medicine, Seoul, Korea Current Recommendation for unprotected LMCA Stenosis Class IIb C in ESC guideline
Consensus Core Set: Cardiovascular Measures Version 1.0
 Consensus Core Set: Cardiovascular s NQF 0330 Hospital 30-day, all-cause, riskstandardized readmission rate (RSRR) following heart failure hospitalization 0229 Hospital 30-day, all-cause, riskstandardized
Consensus Core Set: Cardiovascular s NQF 0330 Hospital 30-day, all-cause, riskstandardized readmission rate (RSRR) following heart failure hospitalization 0229 Hospital 30-day, all-cause, riskstandardized
Cardiac Risk Factors and Noninvasive Cardiac Diagnosis-ECG, ECHO, et al. Martin C. Burke, DO, FACOI ACOI IM Board Review Course 2018
 Cardiac Risk Factors and Noninvasive Cardiac Diagnosis-ECG, ECHO, et al. Martin C. Burke, DO, FACOI ACOI IM Board Review Course 2018 No Disclosures The American Heart Association Evidence-Based Scoring
Cardiac Risk Factors and Noninvasive Cardiac Diagnosis-ECG, ECHO, et al. Martin C. Burke, DO, FACOI ACOI IM Board Review Course 2018 No Disclosures The American Heart Association Evidence-Based Scoring
Ischemic Heart Disease Interventional Treatment
 Ischemic Heart Disease Interventional Treatment Cardiac Catheterization Laboratory Procedures (N = 89) is a regional and national referral center for percutaneous coronary intervention (PCI). A total of
Ischemic Heart Disease Interventional Treatment Cardiac Catheterization Laboratory Procedures (N = 89) is a regional and national referral center for percutaneous coronary intervention (PCI). A total of
Revascularization in Severe LV Dysfunction: The Role of Inducible Ischemia and Viability Testing
 Revascularization in Severe LV Dysfunction: The Role of Inducible Ischemia and Viability Testing Evidence and Uncertainties Robert O. Bonow, MD, MS, MACC Northwestern University Feinberg School of Medicine
Revascularization in Severe LV Dysfunction: The Role of Inducible Ischemia and Viability Testing Evidence and Uncertainties Robert O. Bonow, MD, MS, MACC Northwestern University Feinberg School of Medicine
Ischemic Heart Disease Interventional Treatment
 Ischemic Heart Disease Interventional Treatment Cardiac Catheterization Laboratory Procedures (N = 11,61) is a regional and national referral center for percutaneous coronary intervention (PCI). A total
Ischemic Heart Disease Interventional Treatment Cardiac Catheterization Laboratory Procedures (N = 11,61) is a regional and national referral center for percutaneous coronary intervention (PCI). A total
Clinical Controversies in Perioperative Medicine
 Update on Perioperative Medicine Clinical Controversies in Perioperative Medicine Hugo Quinny Cheng, MD Division of Hospital Medicine University of California, San Francisco Cardiac Medications & Perioperative
Update on Perioperative Medicine Clinical Controversies in Perioperative Medicine Hugo Quinny Cheng, MD Division of Hospital Medicine University of California, San Francisco Cardiac Medications & Perioperative
Preoperative Risk. Geoffrey C Zarrella DO FACC. Assessment
 Preoperative Risk Geoffrey C Zarrella DO FACC Assessment your late add ons keep calm use your tools stick to your guns PURPOSE OF THE PREOP EVAL ASSESS PERIOP RISK CAN INFORM DECISION TO PROCEED OR
Preoperative Risk Geoffrey C Zarrella DO FACC Assessment your late add ons keep calm use your tools stick to your guns PURPOSE OF THE PREOP EVAL ASSESS PERIOP RISK CAN INFORM DECISION TO PROCEED OR
(For items 1-12, each question specifies mark one or mark all that apply.)
") Form 121 - Report of Cardiovascular Outcome Ver. 9.2 COMMENTS -Affix label here- Member ID: - - To be completed by Physician Adjudicator Date Completed: - - (M/D/Y) Adjudicator Code: - Central Case No.:
Form 121 - Report of Cardiovascular Outcome Ver. 9.2 COMMENTS -Affix label here- Member ID: - - To be completed by Physician Adjudicator Date Completed: - - (M/D/Y) Adjudicator Code: - Central Case No.:
Guideline Number: NIA_CG_024 Last Review Date: January 2011 Responsible Department: Last Revised Date: May 2, 2011 Clinical Operations
 National Imaging Associates, Inc. Clinical guidelines NUCLEAR CARDIAC IMAGING (MYOCARDIAL PERFUSION STUDY) CPT Codes: 78451, 78452, 78453, 78454, 78466, 78468, 78469, 78481, 78483, 78494, 78499 Original
National Imaging Associates, Inc. Clinical guidelines NUCLEAR CARDIAC IMAGING (MYOCARDIAL PERFUSION STUDY) CPT Codes: 78451, 78452, 78453, 78454, 78466, 78468, 78469, 78481, 78483, 78494, 78499 Original
ESC Congress 2011 SIMULTANEOUS HYBRID REVASCULARIZATION OF CAROTID AND CORONARY DISEASE INITIAL RESULTS OF A NEW THERAPEUTIC APPROACH
 ESC Congress 2011 SIMULTANEOUS HYBRID REVASCULARIZATION OF CAROTID AND CORONARY DISEASE IN PATIENTS WITH ACUTE CORONARY SYNDROME: INITIAL RESULTS OF A NEW THERAPEUTIC APPROACH AUTHORS: Marta Ponte 1, RICARDO
ESC Congress 2011 SIMULTANEOUS HYBRID REVASCULARIZATION OF CAROTID AND CORONARY DISEASE IN PATIENTS WITH ACUTE CORONARY SYNDROME: INITIAL RESULTS OF A NEW THERAPEUTIC APPROACH AUTHORS: Marta Ponte 1, RICARDO
ACC/AHA Guideline. Downloaded from by on September 30, 2018
 ACC/AHA Guideline ACC/AHA 2007 Guidelines on Perioperative Cardiovascular Evaluation and Care for Noncardiac Surgery: Executive Summary A Report of the American College of Cardiology/American Heart Association
ACC/AHA Guideline ACC/AHA 2007 Guidelines on Perioperative Cardiovascular Evaluation and Care for Noncardiac Surgery: Executive Summary A Report of the American College of Cardiology/American Heart Association
Heart disease remains the leading cause of morbidity and mortality in industrialized nations. It accounts for nearly 40% of all deaths in the United
 Heart disease remains the leading cause of morbidity and mortality in industrialized nations. It accounts for nearly 40% of all deaths in the United States, totaling about 750,000 individuals annually
Heart disease remains the leading cause of morbidity and mortality in industrialized nations. It accounts for nearly 40% of all deaths in the United States, totaling about 750,000 individuals annually
Heart 101. Objectives. Types of Heart Failure How common is HF? Sign/Symptoms, when to see a doctor? Diagnostic testing
 EXAMING HEART FAILURE: HOW TO RECOGNIZE AND TREAT THE WEAK HEART What is Heart Failure? Treatment of Heart Failure End Stage Heart Failure Munir S. Janmohamed M.D. FACC Assistant Clinical Professor of
EXAMING HEART FAILURE: HOW TO RECOGNIZE AND TREAT THE WEAK HEART What is Heart Failure? Treatment of Heart Failure End Stage Heart Failure Munir S. Janmohamed M.D. FACC Assistant Clinical Professor of
Occurrence of Bleeding and Thrombosis during Antiplatelet therapy In Non-cardiac surgery. A prospective observational study.
 Occurrence of Bleeding and Thrombosis during Antiplatelet therapy In Non-cardiac surgery A prospective observational study OBTAIN Study Statistical Analysis Plan of Final Analysis Final Version: V1.1 from
Occurrence of Bleeding and Thrombosis during Antiplatelet therapy In Non-cardiac surgery A prospective observational study OBTAIN Study Statistical Analysis Plan of Final Analysis Final Version: V1.1 from
PERIOPERATIVE MYOCARDIAL INFARCTION THE ANAESTHESIOLOGIST'S VIEW
 PERIOPERATIVE MYOCARDIAL INFARCTION THE ANAESTHESIOLOGIST'S VIEW Bruce Biccard Perioperative Research Group, Department of Anaesthetics 18 June 2015 Disclosure Research funding received Medical Research
PERIOPERATIVE MYOCARDIAL INFARCTION THE ANAESTHESIOLOGIST'S VIEW Bruce Biccard Perioperative Research Group, Department of Anaesthetics 18 June 2015 Disclosure Research funding received Medical Research
Why is co-morbidity important for cancer patients? Michael Chapman Research Programme Manager
 Why is co-morbidity important for cancer patients? Michael Chapman Research Programme Manager Co-morbidity in cancer Definition:- Co-morbidity is a disease or illness affecting a cancer patient in addition
Why is co-morbidity important for cancer patients? Michael Chapman Research Programme Manager Co-morbidity in cancer Definition:- Co-morbidity is a disease or illness affecting a cancer patient in addition
CORONARY ARTERY BYPASS GRAFT (CABG) MEASURES GROUP OVERVIEW
 MEASURES GROUP OVERVIEW") CONARY ARTERY BYPASS GRAFT (CABG) MEASURES GROUP OVERVIEW 2015 PQRS OPTIONS F MEASURES GROUPS: 2015 PQRS MEASURES IN CONARY ARTERY BYPASS GRAFT (CABG) MEASURES GROUP: #43 Coronary Artery Bypass Graft (CABG):
CONARY ARTERY BYPASS GRAFT (CABG) MEASURES GROUP OVERVIEW 2015 PQRS OPTIONS F MEASURES GROUPS: 2015 PQRS MEASURES IN CONARY ARTERY BYPASS GRAFT (CABG) MEASURES GROUP: #43 Coronary Artery Bypass Graft (CABG):
CCS/CAIC/CSCS Position Statement on Revascularization Multi-vessel CAD. Teo et al, Canadian Journal of Cardiology 2014;30:
 CCS/CAIC/CSCS Position Statement on Revascularization Multi-vessel CAD Teo et al, Canadian Journal of Cardiology 2014;30: 1482-1491 Parallel Paper: Canadian Cardiovascular Society Guidelines for the Diagnosis
CCS/CAIC/CSCS Position Statement on Revascularization Multi-vessel CAD Teo et al, Canadian Journal of Cardiology 2014;30: 1482-1491 Parallel Paper: Canadian Cardiovascular Society Guidelines for the Diagnosis
PREOPERATIVE ASSESSMENT OF THE PATIENT WITH CARDIAC DISEASE
 CHAPTER 7 V O L U M E T H I R T Y - T H R E E PREOPERATIVE ASSESSMENT OF THE PATIENT WITH CARDIAC DISEASE LEE A. FLEISHER, M.D. ROBERT D. DRIPPS PROFESSOR AND CHAIR DEPARTMENT OF ANESTHESIOLOGY AND CRTICAL
CHAPTER 7 V O L U M E T H I R T Y - T H R E E PREOPERATIVE ASSESSMENT OF THE PATIENT WITH CARDIAC DISEASE LEE A. FLEISHER, M.D. ROBERT D. DRIPPS PROFESSOR AND CHAIR DEPARTMENT OF ANESTHESIOLOGY AND CRTICAL