Medical Rx vs PCI vs CABG
|
|
|
- Marjory Hubbard
- 6 years ago
- Views:
Transcription

1 Medical Rx vs PCI vs CABG S. Hinan Ahmed, MD Associate Professor: Cardiology and Cardiothoracic Surgery Program Director: Interventional Fellowship Program Assoc Editor: Cath and Cardiovasc Intervention UTHSC, San Antonio There are no conflicts of interest relevant to this presentation
2 Goals of Treatment Improve symptoms angina, anginal equivalents dyspnea, heart failure Reduce morbidity myocardial infarction, ischemic cardiomyopathy, dysrhythmias hospitalization, repeat revascularization procedures Reduce mortality Cost effective therapy
3 Topics 1. Overview of treatmen strategies 2. Key randomized clinical trials CABG vs. medical rx PCI vs. medical therapy: stable angina Invasive vs. conservative: ACS/NSTEMI CABG vs PCI 3. Guidelines
4 Randomized Strategy Comparisons Invasive vs Cons. (ACS) TIMI IIIB, VANQWISH FRISC II TACTICS-TIMI 18 SWISSI-II RITA-3 ICTUS PCI vs Medicine ACME ACME VA RITA-2 AVERT COURAGE 6 smaller trials CABG vs Balloon BARI CABRI EAST GABI RITA AWESOME, 4 smaller trials CABG vs Medicine CASS VA Cooperative European Cooperative STICH 4 smaller trials CABG vs Stent ARTS (ARTS II) ERACI II SoS SIMA Leipzig FREEDOM SYNTAX and growing
5 CABG vs Medical Rx


6 CABG vs. Medical Therapy Coronary Artery Bypass Surgery Trialists Collaboration Total Mortality All studies Medical rx CABG n=1325 n=1324 Trials VA European CASS Texas Oregon NZ NZ Time from randomization (years) Yusuf S et al, Lancet 1994;344:563

7 CABG vs.medical Therapy Coronary Artery Bypass Surgery Trialists Collaboration (7 randomized trials*) Disease N med mortality at 5y OR single vessel % double vessel % triple vessel % p=.001 left main % p= CABG better Med rx *VA Coop., European Coop., CASS, Texas, Oregon, NZ, NZ Yusuf S et al, Lancet 1994;344:563
8 STICH Revascularization Hypothesis 1212 Randomized MED only Randomized CABG 99 clinical sites in 22 countries Enrollment: July 2002 May 2007 Velazquez et al, NEJM 2011;364:




9 STICH: All-Cause Mortality HR 0.86 (0.72, 1.04) P = Adjusted HR 0.82 (0.68, 0.99) Adjusted P =
10 PCI vs Medical Rx
11 Stable Angina ACME ACME VA RITA-2 AVERT COURAGE 6 smaller trials
 1,018 pts: 504 PTCA, 514")
12 RITA-2: Design Second Randomized Intervention Treatment of Angina Randomized clinical trial early 1990 s PTCA (balloon) versus medical therapy 20 centers in UK & Ireland Cardiologist opinion: either medical rx or PTCA appropriate Stable angina (ACS/NSTEMI, other high risk patients excluded) 1,018 pts: 504 PTCA, 514 medical


13 RITA-2: Seven Year Outcomes Henderson RA et al., J Am Coll Cardiol 2003;42:
14 Atorvastatin Versus Revascularization Treatments (AVERT) Trial Randomized Clinical Trial mid 1990 s PTCA (with usual care) versus aggressive lipidlowering therapy Low risk patients with 1V or 2V CAD High LDL (>115 mg/dl), no ischemia for >4 min (Bruce) 341 patients: 177 PCI, 164 med (80 mg atorvastatin)



15 AVERT Trial: Study Design 341 pts with 1V or 2V CAD (> 50% stenosis) 16% female, mean age 58 years, mean EF 61% High-dose atorvastatin and usual medical therapy n=164 Angioplasty + usual care, including standard lipid lowering n= Months Primary Endpoint: Composite of ischemic events - death, nonfatal MI, CVA, CABG, PCI, or hospitalization due to worsening angina Pitt B et al. N Engl J Med. 1999;341:70-76.
 P=0.03 Time since randomization (months) Pitt B et al. N Engl J Med.")
16 AVERT: Time to First Ischemic Event Angioplasty / usual care (n=177) High-dose atorvastatin (n=164) Cumulative incidence (%) P=0.03 Time since randomization (months) Pitt B et al. N Engl J Med. 1999;341:70-76.
17 PCI vs Medical Rx Katritsis DG et al. Circulation. 2005;111:
18 Stable CAD: PCI vs Conservative Medical Management Meta-analysis of 11 randomized trials; N = 2,950 Favors PCI Favors Medical Management P Death Cardiac death or MI Nonfatal MI CABG PCI Risk ratio (95% Cl) Katritsis DG et al. Circulation. 2005;111:
19 COURAGE Design Clinical Outcomes Utilizing Revascularization And Aggressive DruG Evaluation Randomized Clinical Trial stent era PCI + Optimal Medical Therapy vs Optimal Medical Therapy alone Intensive, guideline-driven medical rx and lifestyle intervention in both groups Stable patients with 1-3V CAD amenable to PCI 2287 pts: 1149 PCI + OMT, 1138 OMT 2.5 to 7 year (mean 4.6 year) follow-up Boden W et al., N Engl J Med 356: , 2007
20 Survival Free of Death from Any Cause and Myocardial Infarction 1.0 Optimal Medical Therapy (OMT) (with pci crossover) PCI + OMT Hazard ratio: % CI ( ) P = Number at Risk Years Medical rx PCI
21 Subsequent Revascularization At a median 4.6 year follow-up, 21.1% of the PCI patients required an additional revascularization; 32.6% of the OMT group required a 1 st revascularization 77 patients in the PCI group and 81 patients in the OMT group required subsequent CABG surgery
22 Freedom from Angina During Long-Term Follow-up PCI + OMT OMT p Clinical Angina free Baseline 12% 13% NS 1 Yr 66% 58% < Yr 72% 67%.02 5 Yr 74% 72% NS
23 PCI versus Medical Therapy Large heterogeneity between studies balloon PTCA era (except COURAGE) No mortality benefit in Stable Angina No difference in need for CABG Trend for increase in non-fatal MI in PCI group ~30% increase, mostly peri-pci More subsequent PCI in medical group Less angina in PCI group
24 PCI vs CABG
25 Clinical Randomized Studies CABG vs PTCA RITA (1011) ERACI (127) Lausanne (134) GABI (359) EAST (392) CABRI (1054) MASS (142) BARI (1829) Toulousse (152) CABG vs Stents SIMA (121) ERACI-II (450) ARTS 1 (1205) ARTS II (606) SoS (988) MASS-II (611) AWSOME (454) SYNTAX (1800) BARI 2D (2368) CARDia (600)

26 CABG vs. PCI Meta-Analysis of Late Outcomes Survival MVD Trials Follow-up Favors PTCA Favors CABG # pts #studies 1 year 3 year year 8 year p=0.025 p= Survival Risk Difference (%) Hoffman et al. JACC. 2003;41:
27 CABG vs. PCI Meta-Analysis of Late Outcomes Repeat Revascularization Follow-up Favors PTCA Favors CABG # pts #studies 1 year 3 year 5 year 8 year 2643 (3) 1559 (3) Stent No Stent Revascularization Risk Difference (%) Hoffman et al. JACC. 2003;41:
")
 (Terminated) COMBAT")
28 Trials of DES vs CABG in Multivessel CAD Patients ARTS 2 FREEDOM (NIH) SYNTAX (BSI) CARDia (UK & Ireland) VA study (US) (Terminated) COMBAT (CORDIS)


29 ARTS II TRIAL Study Design ARTS II CYPHER Sirolimus Eluting stent N=606 ARTS I R Bare metal stent N= 600 CABG N=605 Primary Endpoint: 1 year MACCE event-free survival with Cypher DES versus CABG MACCE in ARTS 1
30 ARTS II: 1 year MACCE P=NS P=NS P=<0.001 P=0.46 P= % 89.5% 73.7% 88.5% 96.9% 90.7% 92.0% 91.5% 78.1% 95.9% 80% 60% 40% 20% 0% MACCE free survival Survival w/o CVE/MI Survival w/o revasc ARTS II: DES ARTS I: BMS ARTSI: CABG
 treatment approach Randomized Arms N=1800 Stratification: Stratification: LM and Diabetes Referring MD or pts.")
31 SYNTAX Trial Design 62 EU Sites + 23 US Sites All Heart Pts Team with (surgeon de novo & Total enrollment 3VD interventionalist) and/or LM N=3075 disease (N=4,337) Amenable for both Amenable for only one treatment options Treatment preference (9.4%) treatment approach Randomized Arms N=1800 Stratification: Stratification: LM and Diabetes Referring MD or pts. refused informed LM and consent Diabetes (7.0%) Inclusion/exclusion (4.7%) Two Registry Arms Withdrew before consent (4.3%) Other (1.8%) N=1275 Randomized Arms Two Registry Arms Medical treatment (1.2%) CABG n=1800 TAXUS * CABG PCI vs 2500 N=897 n=897 N=903 n=903 n=1077 N=1077 N= w/ f/u n=198 follow up Non LMDM vs 3VD DM NonDM 71% LM enrolled 5yr f/u no f/u (N=3,075) n=649 n=428 3VD DM 66.3% 28.5% 33.7% 71.5% 28.2% 65.4% 71.8% 34.6% all captured w/ * TAXUS Express

32 Primary Endpoint: 12 Month MACCE Non-inferiority analysis Pre-specified Margin = 6.6% 5.5% +95% CI = 8.3% 0 5% 10% 15% Difference in MACCE 20% The criteria for non-inferiority comparison was not met for the primary endpoint, further comparisons for the LM and 3VD subgroups are observational only and hypothesis generating

33 Outcomes by Syntax Score: 3 Years Kappetein et al EHJ 2011


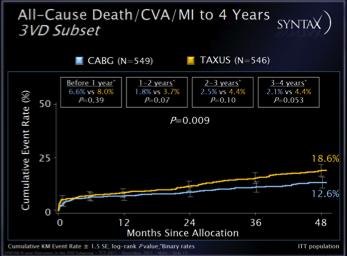

34 Syntax: Outcomes at 4 Years

35 SYNTAX Trial 5-year f/u results (2013)
36
37
38 Conclusions: PCI versus CABG PCI Decreased procedural morbidity Less likely to have complete revascularization with complex/severe CAD More repeat revascularization Treatment of CTO in question CABG Increased procedural/early risk better long-term outcomes in complex CAD LIMA conduit has demonstrated longevity
39 Guidelines
40 Revascularization to Improve Survival: Left Main CAD Revascularization I IIaIIbIII I IIa IIb III CABG to improve survival is recommended for patients with significant ( 50% diameter stenosis) left main CAD. PCI to improve survival is reasonable as an alternative to CABG in selected stable patients with significant ( 50% diameter stenosis) unprotected left main CAD with: 1) anatomic conditions associated with a low risk of PCI procedural complications and a high likelihood of a good long-term outcome (e.g., a low SYNTAX score [ 22], ostial or trunk left main CAD); and 2) clinical characteristics that predict a significantly increased risk of adverse surgical outcomes (e.g., STS-predicted risk of operative mortality 5%).
41 Revascularization to Improve Survival: Left Main CAD Revascularization I IIaIIbIII I IIaIIbIII PCI to improve survival is reasonable in patients with UA/NSTEMI when an unprotected left main coronary artery is the culprit lesion and the patient is not a candidate for CABG. PCI to improve survival is reasonable in patients with acute STEMI when an unprotected left main coronary artery is the culprit lesion, distal coronary flow is TIMI (Thrombolysis In Myocardial Infarction) grade <3, and PCI can be performed more rapidly and safely than CABG.
42 Revascularization to Improve Survival: Non-Left Main CAD Revascularization CABG I IIaIIbIII PCI I IIaIIbIII CABG or PCI to improve survival is beneficial in survivors of sudden cardiac death with presumed ischemia-mediated ventricular tachycardia caused by a significant ( 70% diameter) stenosis in a major coronary artery.
43 Revascularization to Improve Symptoms I IIaIIbIII I IIaIIbIII CABG or PCI to improve symptoms is beneficial in patients with 1 or more significant ( 70% diameter) coronary artery stenoses amenable to revascularization and unacceptable angina despite GDMT. CABG or PCI to improve symptoms is reasonable in patients with 1 or more significant ( 70% diameter) coronary artery stenoses and unacceptable angina for whom GDMT cannot be implemented because of medication contraindications, adverse effects, or patient preferences.
44 Revascularization to Improve Symptoms I IIa IIb III I IIa IIb III PCI to improve symptoms is reasonable in patients with previous CABG, 1 or more significant ( 70% diameter) coronary artery stenoses associated with ischemia, and unacceptable angina despite GDMT. It is reasonable to choose CABG over PCI to improve symptoms in patients with complex 3- vessel CAD (e.g., SYNTAX score >22), with or without involvement of the proximal LAD artery who are good candidates for CABG.
45 Revascularization to Improve Symptoms I IIa IIb III Harm CABG or PCI to improve symptoms should not be performed in patients who do not meet anatomic ( 50% left main or 70% non left main stenosis) or physiologic (e.g., abnormal fractional flow reserve) criteria for revascularization.
46 Risk Prediction
47 Models of Risk for PCI and CABG Clinical Anatomic Observational registries Duke New York Northern New England Mayo Clinic Randomized trials Balloon PTCA vs. CABG Stent PCI vs. CABG Bare Metal Stent Drug Eluting Stents
48 Angiographic Predictors of Mortality Findings 2vd, 95% LAD 2vd, Prox LAD 3vd, 1>95% 3vd, prox LAD 3vc, 95% Prox LAD Left Main Severe Left main Odds Ratio N=11, Adapted from Dvazik Am Heart J 142:


49 Myocardial Jeopardy Scores Modified APPROACH score BARI score Eu Heart J 2007:28;




50 SYNTAX Score


51 SYNTAX Score
52 PCI Risk Models ACC New York State Northern New England Michigan Cleveland Clinic Foundation Mayo Clinic CADILLAC


")
53 NCDR Risk Assessment Peterson et al JACC (18) 2010:
54 STS Database Variables 1. Age 15. Multiple Reoperations 2. Aortic Stenosis 16. Myocardial Infarction 3. Body Surface Area 17. Number of Diseased Vessel 4. Cerebrovascular Accident 18. New York Heart Association Class IV 5. Chronic Lung Disease 19. PTCA (< 6 hours) 6. Diabetes/Insulin or Oral 20. PVD, CVA 7. Ejection Fraction 21. Preoperative IABP 8. First Reoperation 22. Racial Designation 9. Hypercholesterolemia 23. Renal Failure, Dialysis 10. Hypertension 24. Shock 11. Immunosuppressive Treatment 25. Status 12. Left Main Disease 13. Male Gender 14. Mitral Insufficiency variables are listed in alpha order to protect the propriety of the STS national database related to variable-specific data
55 Thank You
Surgery Grand Rounds
 Surgery Grand Rounds Coronary Artery Bypass Grafting versus Coronary Artery Stenting Charles Ted Lord, R1 Coronary Artery Disease Stenosis of epicardial vessels Metabolic & hematologic Statistics 500,000
Surgery Grand Rounds Coronary Artery Bypass Grafting versus Coronary Artery Stenting Charles Ted Lord, R1 Coronary Artery Disease Stenosis of epicardial vessels Metabolic & hematologic Statistics 500,000
VCU Pauley Heart Center: A 2009 US News Top 50 Heart and Heart Surgery Hospital
 VCU Pauley Heart Center: A 2009 US News Top 50 Heart and Heart Surgery Hospital Complex PCI: Multivessel Disease George W. Vetrovec, MD. Kimmerling Chair of Cardiology VCU Pauley Heart Center Virginia
VCU Pauley Heart Center: A 2009 US News Top 50 Heart and Heart Surgery Hospital Complex PCI: Multivessel Disease George W. Vetrovec, MD. Kimmerling Chair of Cardiology VCU Pauley Heart Center Virginia
Unprotected LM intervention
 Unprotected LM intervention Guideline for COMBAT Seung-Jung Park, MD, PhD Professor of Internal Medicine, Seoul, Korea Current Recommendation for unprotected LMCA Stenosis Class IIb C in ESC guideline
Unprotected LM intervention Guideline for COMBAT Seung-Jung Park, MD, PhD Professor of Internal Medicine, Seoul, Korea Current Recommendation for unprotected LMCA Stenosis Class IIb C in ESC guideline
Can Angiographic Complete Revascularization Improve Outcomes for Patients with Decreased LV Function? NO!
 Can Angiographic Complete Revascularization Improve Outcomes for Patients with Decreased LV Function? NO! Young-Hak Kim, MD, PhD Heart Institute, University of Ulsan College of Medicine Asan Medical Center,
Can Angiographic Complete Revascularization Improve Outcomes for Patients with Decreased LV Function? NO! Young-Hak Kim, MD, PhD Heart Institute, University of Ulsan College of Medicine Asan Medical Center,
Advances in Cardiovascular Diagnosis and Therapy. No disclosure or conflicts. Outline
 Advances in Cardiovascular Diagnosis and Therapy Firas Zahr, MD Assistant Professor of Medicine Interventional Cardiology University Of Iowa No disclosure or conflicts Outline What is new with revascularization?
Advances in Cardiovascular Diagnosis and Therapy Firas Zahr, MD Assistant Professor of Medicine Interventional Cardiology University Of Iowa No disclosure or conflicts Outline What is new with revascularization?
PCI vs. CABG From BARI to Syntax, Is The Game Over?
 PCI vs. CABG From BARI to Syntax, Is The Game Over? Seung-Jung Park, MD, PhD Professor of Medicine, University of Ulsan College of Medicine Asan Medical Center, Seoul, Korea PCI vs CABG Multi-Vessel Disease
PCI vs. CABG From BARI to Syntax, Is The Game Over? Seung-Jung Park, MD, PhD Professor of Medicine, University of Ulsan College of Medicine Asan Medical Center, Seoul, Korea PCI vs CABG Multi-Vessel Disease
EXCEL vs. NOBLE: How to Treat Left Main Disease in 2017 AATS International Cardiovascular Symposium December 8-9, 2017
 EXCEL vs. NOBLE: How to Treat Left Main Disease in 2017 AATS International Cardiovascular Symposium December 8-9, 2017 Igor F. Palacios, MD Director of Interventional Cardiology Professor of Medicine Massachusetts
EXCEL vs. NOBLE: How to Treat Left Main Disease in 2017 AATS International Cardiovascular Symposium December 8-9, 2017 Igor F. Palacios, MD Director of Interventional Cardiology Professor of Medicine Massachusetts
The Case for PCI as the Preferred Therapy in Most Patients with Chronic Stable Angina
 The Case for PCI as the Preferred Therapy in Most Patients with Chronic Stable Angina Ajay J. Kirtane,, MD Columbia University Medical Center The Cardiovascular Research Foundation Conflict of Interest
The Case for PCI as the Preferred Therapy in Most Patients with Chronic Stable Angina Ajay J. Kirtane,, MD Columbia University Medical Center The Cardiovascular Research Foundation Conflict of Interest
Diabetic Patients: Current Evidence of Revascularization
 Diabetic Patients: Current Evidence of Revascularization Alexandra J. Lansky, MD Yale University School of Medicine University College of London The Problem with Diabetic Patients Endothelial dysfunction
Diabetic Patients: Current Evidence of Revascularization Alexandra J. Lansky, MD Yale University School of Medicine University College of London The Problem with Diabetic Patients Endothelial dysfunction
Unprotected Left Main Stenting: Patient Selection and Recent Experience. Alaide Chieffo. S. Raffaele Hospital, Milan, Italy
 Unprotected Left Main Stenting: Patient Selection and Recent Experience Alaide Chieffo S. Raffaele Hospital, Milan, Italy Class IIa (Level B) AHA/ACC 2005 Guidelines Left Main CAD The use of PCI for pts
Unprotected Left Main Stenting: Patient Selection and Recent Experience Alaide Chieffo S. Raffaele Hospital, Milan, Italy Class IIa (Level B) AHA/ACC 2005 Guidelines Left Main CAD The use of PCI for pts
Controversies in Coronary Revascularization. Atlanta CCU April 15, 2016
 Controversies in Coronary Revascularization Atlanta CCU April 15, 2016 Habib Samady MD FACC FSCAI Professor of Medicine Director, Interventional Cardiology, Emory University Director, Cardiac Catheterization
Controversies in Coronary Revascularization Atlanta CCU April 15, 2016 Habib Samady MD FACC FSCAI Professor of Medicine Director, Interventional Cardiology, Emory University Director, Cardiac Catheterization
The SYNTAX-LE MANS Study
 The SYNTAX-LE MANS Study Synergy Between PCI with TAXUS Express and Cardiac Surgery: Late (15-month) Left Main Angiographic Substudy A. Pieter Kappetein, MD, PhD Erasmus MC, Rotterdam, NL SYNTAX-LE MANS
The SYNTAX-LE MANS Study Synergy Between PCI with TAXUS Express and Cardiac Surgery: Late (15-month) Left Main Angiographic Substudy A. Pieter Kappetein, MD, PhD Erasmus MC, Rotterdam, NL SYNTAX-LE MANS
COMMENT DEFINIR UN PLURITRONCULAIRE. Didier Carrié CHU Toulouse Rangueil
 COMMENT DEFINIR UN PLURITRONCULAIRE VISION ANGIOGRAHIQUE DU PLURITRONCULAIRE Didier Carrié CHU Toulouse Rangueil Congrès GRCI 03 Décembre 2010 Pôle Cardiovasculaire et Métabolique Avec quel œil je regarde
COMMENT DEFINIR UN PLURITRONCULAIRE VISION ANGIOGRAHIQUE DU PLURITRONCULAIRE Didier Carrié CHU Toulouse Rangueil Congrès GRCI 03 Décembre 2010 Pôle Cardiovasculaire et Métabolique Avec quel œil je regarde
Controversies in Cardiac Surgery
 Controversies in Cardiac Surgery 3 years after SYNTAX : Percutaneous Coronary Intervention for Multivessel / Left main stem Coronary artery disease Pro ESC Congress 2010, 28 August 1 September Stockholm
Controversies in Cardiac Surgery 3 years after SYNTAX : Percutaneous Coronary Intervention for Multivessel / Left main stem Coronary artery disease Pro ESC Congress 2010, 28 August 1 September Stockholm
Reconciling the Results of the Randomized Trials
 Management of Stable Angina in Multivessel Disease: Reconciling the Results of the Randomized Trials Eric A. Cohen MD, FRCPC Schulich Heart Centre Sunnybrook Health Sciences Centre Toronto ON ACC Rockies
Management of Stable Angina in Multivessel Disease: Reconciling the Results of the Randomized Trials Eric A. Cohen MD, FRCPC Schulich Heart Centre Sunnybrook Health Sciences Centre Toronto ON ACC Rockies
Benefit of Performing PCI Based on FFR
 Benefit of Performing PCI Based on FFR William F. Fearon, MD Associate Professor Director, Interventional Cardiology Stanford University Medical Center Benefit of FFR-Guided PCI FFR-Guided PCI vs. Angiography-Guided
Benefit of Performing PCI Based on FFR William F. Fearon, MD Associate Professor Director, Interventional Cardiology Stanford University Medical Center Benefit of FFR-Guided PCI FFR-Guided PCI vs. Angiography-Guided
Clinical Seminar. Which Diabetic Patient is a Candidate for Percutaneous Coronary Intervention - European Perspective
 Clinical Seminar Which Diabetic Patient is a Candidate for Percutaneous Coronary Intervention - European Perspective Stephan Windecker Department of Cardiology Swiss Cardiovascular Center and Clinical
Clinical Seminar Which Diabetic Patient is a Candidate for Percutaneous Coronary Intervention - European Perspective Stephan Windecker Department of Cardiology Swiss Cardiovascular Center and Clinical
How to approach non-infarct related artery disease in patients with STEMI in a limited resource setting
 How to approach non-infarct related artery disease in patients with STEMI in a limited resource setting Ahmed A A Suliman, MBBS, FACP, FESC Associate Professor, University of Khartoum Interventional Cardiologist,
How to approach non-infarct related artery disease in patients with STEMI in a limited resource setting Ahmed A A Suliman, MBBS, FACP, FESC Associate Professor, University of Khartoum Interventional Cardiologist,
LM stenting - Cypher
 LM stenting - Cypher Left main stenting with BMS Since 1995 Issues in BMS era AMC Restenosis and TLR (%) 3 27 TLR P=.282 Restenosis P=.71 28 2 1 15 12 Ostium 5 4 Shaft Bifurcation Left main stenting with
LM stenting - Cypher Left main stenting with BMS Since 1995 Issues in BMS era AMC Restenosis and TLR (%) 3 27 TLR P=.282 Restenosis P=.71 28 2 1 15 12 Ostium 5 4 Shaft Bifurcation Left main stenting with
Left Main Intervention: Where are we in 2015?
 Left Main Intervention: Where are we in 2015? David A. Cox, MD FSCAI Director, Cardiology Research Associate Director, Cardiac Cath Lab Lehigh Valley Health Network Allentown, PA Fall Fellows Course Laa
Left Main Intervention: Where are we in 2015? David A. Cox, MD FSCAI Director, Cardiology Research Associate Director, Cardiac Cath Lab Lehigh Valley Health Network Allentown, PA Fall Fellows Course Laa
Surgical vs. Percutaneous Revascularization in Patients with Diabetes and Acute Coronary Syndrome
 Surgical vs. Percutaneous Revascularization in Patients with Diabetes and Acute Coronary Syndrome Chris C. Cook, MD Associate Professor of Surgery Director, CT Residency Program, WVU ACOI 10/17/18 No Disclosures
Surgical vs. Percutaneous Revascularization in Patients with Diabetes and Acute Coronary Syndrome Chris C. Cook, MD Associate Professor of Surgery Director, CT Residency Program, WVU ACOI 10/17/18 No Disclosures
Coronary Artery Disease: Revascularization (Teacher s Guide)
") Stephanie Chan, M.D. Updated 3/15/13 2008-2013, SCVMC (40 minutes) I. Objectives Coronary Artery Disease: Revascularization (Teacher s Guide) To review the evidence on whether percutaneous coronary intervention
Stephanie Chan, M.D. Updated 3/15/13 2008-2013, SCVMC (40 minutes) I. Objectives Coronary Artery Disease: Revascularization (Teacher s Guide) To review the evidence on whether percutaneous coronary intervention
COURAGE to Leave Diseased Arteries Alone
 COURAGE to Leave Diseased Arteries Alone Spencer King MD MACC, FSCAI St. Joseph s s Heart and Vascular Institute Professor of Medicine Emeritus Emory Univ. Atlanta, USA Conflict: I am an Interventionalist
COURAGE to Leave Diseased Arteries Alone Spencer King MD MACC, FSCAI St. Joseph s s Heart and Vascular Institute Professor of Medicine Emeritus Emory Univ. Atlanta, USA Conflict: I am an Interventionalist
Management of cardiovascular disease - coronary interventions -
 Master Classes in Preventive Cardiology I Management of diabetes in patients with CVD European Heart House Management of cardiovascular disease - coronary interventions - Francesco Cosentino MD, PhD, FESC
Master Classes in Preventive Cardiology I Management of diabetes in patients with CVD European Heart House Management of cardiovascular disease - coronary interventions - Francesco Cosentino MD, PhD, FESC
Trial. International Study of Comparative Health Effectiveness with Medical and Invasive Approaches
 Trial International Study of Comparative Health Effectiveness with Medical and Invasive Approaches Stable Ischemic Heart Disease What is the best initial management strategy for patients with SIHD? What
Trial International Study of Comparative Health Effectiveness with Medical and Invasive Approaches Stable Ischemic Heart Disease What is the best initial management strategy for patients with SIHD? What
What do the guidelines say?
 Percutaneous coronary intervention in 3-vessel disease and main stem What do the guidelines say? Nothing to disclose Dariusz Dudek Institute of Cardiology, Jagiellonian University Krakow, Poland The European
Percutaneous coronary intervention in 3-vessel disease and main stem What do the guidelines say? Nothing to disclose Dariusz Dudek Institute of Cardiology, Jagiellonian University Krakow, Poland The European
Left Main Intervention: Will it become standard of care?
 Left Main Intervention: Will it become standard of care? David Cox, MD FSCAI, FACC Director, Interventional Cardiology Research Associate Director, Cardiac Cath Lab Lehigh Valley Health Network Allentown,
Left Main Intervention: Will it become standard of care? David Cox, MD FSCAI, FACC Director, Interventional Cardiology Research Associate Director, Cardiac Cath Lab Lehigh Valley Health Network Allentown,
Management of High-Risk CAD : Surgeons Perspective
 Management of High-Risk CAD : Surgeons Perspective Steven F. Bolling, M.D. Professor of Cardiac Surgery University of Michigan Conflict : Cardiac Surgeon! High Risk CABG 77 year old with prior large anterior
Management of High-Risk CAD : Surgeons Perspective Steven F. Bolling, M.D. Professor of Cardiac Surgery University of Michigan Conflict : Cardiac Surgeon! High Risk CABG 77 year old with prior large anterior
Count Down to COMBAT
 Count Down to COMBAT Randomized COMparison of Bypass Surgery versus AngioplasTy using Sirolimus-Eluting Stent in Patients with Left Main Coronary Artery Disease Roxana Mehran, MD Associate Professor of
Count Down to COMBAT Randomized COMparison of Bypass Surgery versus AngioplasTy using Sirolimus-Eluting Stent in Patients with Left Main Coronary Artery Disease Roxana Mehran, MD Associate Professor of
Culprit PCI vs MultiVessel PCI for Acute Myocardial Infarction
 Culprit PCI vs MultiVessel PCI for Acute Myocardial Infarction Dipti Itchhaporia, MD, FACC, FESC Trustee, American College of Cardiology Director of Disease Management, Hoag Hospital Robert and Georgia
Culprit PCI vs MultiVessel PCI for Acute Myocardial Infarction Dipti Itchhaporia, MD, FACC, FESC Trustee, American College of Cardiology Director of Disease Management, Hoag Hospital Robert and Georgia
Assessing Myocardium at Risk: Applying SYNTAX
 Assessing Myocardium at Risk: Applying SYNTAX Farouc Jaffer MD PhD FSCAI FACC FAHA Associate Professor of Medicine, Harvard Medical School Director, CAD Program and Chronic Total Occlusion PCI Program
Assessing Myocardium at Risk: Applying SYNTAX Farouc Jaffer MD PhD FSCAI FACC FAHA Associate Professor of Medicine, Harvard Medical School Director, CAD Program and Chronic Total Occlusion PCI Program
Δημήτριος Αγγοσράς, FETCS
 ΣΕΜΙΝΑΡΙΟ ΟΜΑΔΩΝ ΕΡΓΑΣΙΑΣ Δημήτριος Αγγοσράς, FETCS Επίκοσρος Καθηγηηής Καρδιοτειροσργικής Ιαηρική Πανεπιζηημίοσ Αθηνών Πανεπιζηημιακό Γενικό Νοζοκομείο Αηηικόν Randomized Controlled Trials (RCTs) Why
ΣΕΜΙΝΑΡΙΟ ΟΜΑΔΩΝ ΕΡΓΑΣΙΑΣ Δημήτριος Αγγοσράς, FETCS Επίκοσρος Καθηγηηής Καρδιοτειροσργικής Ιαηρική Πανεπιζηημίοσ Αθηνών Πανεπιζηημιακό Γενικό Νοζοκομείο Αηηικόν Randomized Controlled Trials (RCTs) Why
Adults With Diagnosed Diabetes
 Adults With Diagnosed Diabetes 1990 No data available Less than 4% 4%-6% Above 6% Mokdad AH, et al. Diabetes Care. 2000;23(9):1278-1283. Adults With Diagnosed Diabetes 2000 4%-6% Above 6% Mokdad AH, et
Adults With Diagnosed Diabetes 1990 No data available Less than 4% 4%-6% Above 6% Mokdad AH, et al. Diabetes Care. 2000;23(9):1278-1283. Adults With Diagnosed Diabetes 2000 4%-6% Above 6% Mokdad AH, et
Chest Pain: To Cath or Not? Part I
 Chest Pain: To Cath or Not? Part I Georgios Papaioannou, MD Ioannis Karavas, MD Newton-Wellesley Hospital 5/3/2000 1 A Typical Scenario... 57 year old female, Mrs. X., presents to your office with a 2
Chest Pain: To Cath or Not? Part I Georgios Papaioannou, MD Ioannis Karavas, MD Newton-Wellesley Hospital 5/3/2000 1 A Typical Scenario... 57 year old female, Mrs. X., presents to your office with a 2
2/17/2010. Grace Lin, MD Assistant Professor of Medicine University of California, San Francisco
 Modern Management of Patients with Stable Coronary Artery Disease Grace Lin, MD Assistant Professor of Medicine University of California, San Francisco Scope of the Problem Prevalence of CAD: 17.6 million
Modern Management of Patients with Stable Coronary Artery Disease Grace Lin, MD Assistant Professor of Medicine University of California, San Francisco Scope of the Problem Prevalence of CAD: 17.6 million
Management of High-Risk Coronary Artery Disease
 Management of High-Risk Coronary Artery Disease Jeffrey J. Popma, MD Director, Interventional Cardiology Clinical Services Beth Israel Deaconess Medical Center Associate Professor of Medicine Harvard Medical
Management of High-Risk Coronary Artery Disease Jeffrey J. Popma, MD Director, Interventional Cardiology Clinical Services Beth Israel Deaconess Medical Center Associate Professor of Medicine Harvard Medical
Revascularization in Severe LV Dysfunction: The Role of Inducible Ischemia and Viability Testing
 Revascularization in Severe LV Dysfunction: The Role of Inducible Ischemia and Viability Testing Evidence and Uncertainties Robert O. Bonow, MD, MS, MACC Northwestern University Feinberg School of Medicine
Revascularization in Severe LV Dysfunction: The Role of Inducible Ischemia and Viability Testing Evidence and Uncertainties Robert O. Bonow, MD, MS, MACC Northwestern University Feinberg School of Medicine
Michael Mack, M.D. Baylor Healthcare System Heart Hospital Baylor Plano Dallas, TX
 Michael Mack, M.D. Baylor Healthcare System Heart Hospital Baylor Plano Dallas, TX Boston Scientific, Inc.- Syntax Trial Steering Committee Member- travel expenses paid by trial sponsor Maquet, Inc.- unpaid
Michael Mack, M.D. Baylor Healthcare System Heart Hospital Baylor Plano Dallas, TX Boston Scientific, Inc.- Syntax Trial Steering Committee Member- travel expenses paid by trial sponsor Maquet, Inc.- unpaid
high SYNTAX Score? I Sheiban Division of Cardiology Interventional Card. University of Turin Turin / Italy
 What to do with patients with high SYNTAX Score? I Sheiban Division of Cardiology Interventional Card. University of Turin San Giovanni Battista Hospital Turin / Italy Who are the patients with high SYNTAX
What to do with patients with high SYNTAX Score? I Sheiban Division of Cardiology Interventional Card. University of Turin San Giovanni Battista Hospital Turin / Italy Who are the patients with high SYNTAX
Management of ST-elevation myocardial infarction Update 2009 Late comers: which options?
 European Society of Cardiology Annual Session 2009 Management of ST-elevation myocardial infarction Update 2009 Late comers: which options? Antonio Abbate, MD Assistant Professor of Medicine Virginia Commonwealth
European Society of Cardiology Annual Session 2009 Management of ST-elevation myocardial infarction Update 2009 Late comers: which options? Antonio Abbate, MD Assistant Professor of Medicine Virginia Commonwealth
Revascularization In HFrEF: Are We Close To The Truth. Ali Almasood
 Revascularization In HFrEF: Are We Close To The Truth Ali Almasood HF epidemic 1-2% of the population have HF At least one-half have heart failure with reduced ejection fraction (HF- REF) The most common
Revascularization In HFrEF: Are We Close To The Truth Ali Almasood HF epidemic 1-2% of the population have HF At least one-half have heart failure with reduced ejection fraction (HF- REF) The most common
Rationale for Percutaneous Revascularization ESC 2011
 Rationale for Percutaneous Revascularization Marie Claude Morice, Massy FR MD, FESC, FACC ESC 2011 Paris Villepinte - 27-31 August, 2011 Massy, France Potential conflicts of interest I have the following
Rationale for Percutaneous Revascularization Marie Claude Morice, Massy FR MD, FESC, FACC ESC 2011 Paris Villepinte - 27-31 August, 2011 Massy, France Potential conflicts of interest I have the following
Approach to Multi Vessel disease with STEMI
 Approach to Multi Vessel disease with STEMI MANAGEMENT OF ST-ELEVATION MYOCARDIAL INFARCTION Dr. Thomas Alexander, M.D; D.M; F.A.C.C. Senior Consultant and Interventional Cardiologist Kovai Medical Centre
Approach to Multi Vessel disease with STEMI MANAGEMENT OF ST-ELEVATION MYOCARDIAL INFARCTION Dr. Thomas Alexander, M.D; D.M; F.A.C.C. Senior Consultant and Interventional Cardiologist Kovai Medical Centre
COMBAT- Revised Protocol
 COMBAT- Revised Protocol Randomized COMparison of Bypass Surgery versus AngioplasTy using Sirolimus-Eluting Stent in Patients with Left Main Coronary Artery Disease Roxana Mehran, MD Associate Professor
COMBAT- Revised Protocol Randomized COMparison of Bypass Surgery versus AngioplasTy using Sirolimus-Eluting Stent in Patients with Left Main Coronary Artery Disease Roxana Mehran, MD Associate Professor
Cindy L. Grines MD FACC FSCAI
 Cindy L. Grines MD FACC FSCAI Hofstra Northwell School of Medicine Chair, Cardiology Academic Chief of Cardiology, Northwell Health North Shore University Hospital, Manhasset NY Multivessel Disease in
Cindy L. Grines MD FACC FSCAI Hofstra Northwell School of Medicine Chair, Cardiology Academic Chief of Cardiology, Northwell Health North Shore University Hospital, Manhasset NY Multivessel Disease in
ISAR-LEFT MAIN: A Randomized Clinical Trial on Drug-Eluting Stents for Unprotected Left Main Lesions
 Julinda Mehilli, MD Deutsches Herzzentrum Technische Universität Munich Germany ISAR-LEFT MAIN: A Randomized Clinical Trial on Drug-Eluting Stents for Unprotected Left Main Lesions Background Left main
Julinda Mehilli, MD Deutsches Herzzentrum Technische Universität Munich Germany ISAR-LEFT MAIN: A Randomized Clinical Trial on Drug-Eluting Stents for Unprotected Left Main Lesions Background Left main
Michael Mack, M.D. Baylor Healthcare System Heart Hospital Baylor Plano Dallas, TX
 Michael Mack, M.D. Baylor Healthcare System Heart Hospital Baylor Plano Dallas, TX Maquet, Inc.,- unpaid consultant Cordis, Inc.,- unpaid consultant Boston Scientific, Inc.,- travel expenses paid for Syntax
Michael Mack, M.D. Baylor Healthcare System Heart Hospital Baylor Plano Dallas, TX Maquet, Inc.,- unpaid consultant Cordis, Inc.,- unpaid consultant Boston Scientific, Inc.,- travel expenses paid for Syntax
Revascularization after Drug-Eluting Stent Implantation or Coronary Artery Bypass Surgery for Multivessel Coronary Disease
 Impact of Angiographic Complete Revascularization after Drug-Eluting Stent Implantation or Coronary Artery Bypass Surgery for Multivessel Coronary Disease Young-Hak Kim, Duk-Woo Park, Jong-Young Lee, Won-Jang
Impact of Angiographic Complete Revascularization after Drug-Eluting Stent Implantation or Coronary Artery Bypass Surgery for Multivessel Coronary Disease Young-Hak Kim, Duk-Woo Park, Jong-Young Lee, Won-Jang
The MAIN-COMPARE Study
 Long-Term Outcomes of Coronary Stent Implantation versus Bypass Surgery for the Treatment of Unprotected Left Main Coronary Artery Disease Revascularization for Unprotected Left MAIN Coronary Artery Stenosis:
Long-Term Outcomes of Coronary Stent Implantation versus Bypass Surgery for the Treatment of Unprotected Left Main Coronary Artery Disease Revascularization for Unprotected Left MAIN Coronary Artery Stenosis:
James M. Kirshenbaum, MD, FACC
 James M. Kirshenbaum, MD, FACC Associate Professor of Medicine Harvard Medical School Co-Director, Clinical Cardiology Director, Acute Interventional Cardiology Brigham and Women s Hospital Boston, MA
James M. Kirshenbaum, MD, FACC Associate Professor of Medicine Harvard Medical School Co-Director, Clinical Cardiology Director, Acute Interventional Cardiology Brigham and Women s Hospital Boston, MA
New Generation Drug- Eluting Stent in Korea
 New Generation Drug- Eluting Stent in Korea Young-Hak Kim, MD, PhD Department of Cardiology, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea Purpose To briefly introduce the
New Generation Drug- Eluting Stent in Korea Young-Hak Kim, MD, PhD Department of Cardiology, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea Purpose To briefly introduce the
Evaluating Clinical Risk and Guiding management with SPECT Imaging
 Evaluating Clinical Risk and Guiding management with SPECT Imaging Raffaele Giubbini Chair and Nuclear Medicine Unit University & Spedali Civili Brescia- Italy U.S. Congressional Budget Office. Technological
Evaluating Clinical Risk and Guiding management with SPECT Imaging Raffaele Giubbini Chair and Nuclear Medicine Unit University & Spedali Civili Brescia- Italy U.S. Congressional Budget Office. Technological
Treatment Options for Angina
 Treatment Options for Angina Interventional Cardiology Perspective Michael A. Robertson, M.D. 10/30/10 Prevalence of CAD in USA 15 million Americans with CAD 2 million diagnostic catheterizations 1 million
Treatment Options for Angina Interventional Cardiology Perspective Michael A. Robertson, M.D. 10/30/10 Prevalence of CAD in USA 15 million Americans with CAD 2 million diagnostic catheterizations 1 million
Journal of the American College of Cardiology Vol. 35, No. 5, by the American College of Cardiology ISSN /00/$20.
 Journal of the American College of Cardiology Vol. 35, No. 5, 2000 2000 by the American College of Cardiology ISSN 0735-1097/00/$20.00 Published by Elsevier Science Inc. PII S0735-1097(00)00546-5 CLINICAL
Journal of the American College of Cardiology Vol. 35, No. 5, 2000 2000 by the American College of Cardiology ISSN 0735-1097/00/$20.00 Published by Elsevier Science Inc. PII S0735-1097(00)00546-5 CLINICAL
Implications of the New ESC/EACTS Guidelines for Myocardial Revascularization in 2011
 Implications of the New ESC/EACTS Guidelines for Myocardial Revascularization in 2011 Prof. Dr. Volkmar Falk Klinik für Herz- und Gefäßchirurgie, Universitätsspital Zürich, Schweiz In 2004 headlines were
Implications of the New ESC/EACTS Guidelines for Myocardial Revascularization in 2011 Prof. Dr. Volkmar Falk Klinik für Herz- und Gefäßchirurgie, Universitätsspital Zürich, Schweiz In 2004 headlines were
Coronary interventions
 Controversial issues in the management of ischemic heart failure Coronary interventions Maciej Lesiak Department of Cardiology, University Hospital in Poznan none DECLARATION OF CONFLICT OF INTEREST CHF
Controversial issues in the management of ischemic heart failure Coronary interventions Maciej Lesiak Department of Cardiology, University Hospital in Poznan none DECLARATION OF CONFLICT OF INTEREST CHF
Left Main Disease: what is left to surgery? Prof. Jacques Monségu CardioVascular Institute Grenoble, France
 Left Main Disease: what is left to surgery? Prof. Jacques Monségu CardioVascular Institute Grenoble, France Background on LM stenosis 5% of patients undergoing angiography Of the myocardium 80% Bifurcation
Left Main Disease: what is left to surgery? Prof. Jacques Monségu CardioVascular Institute Grenoble, France Background on LM stenosis 5% of patients undergoing angiography Of the myocardium 80% Bifurcation
Perspective of LM stenting with Current registry and Randomized Clinical Data
 Asian Pacific TCT Perspective of LM stenting with Current registry and Randomized Clinical Data Patrick W. Serruys MD PhD Yoshinobu Onuma MD Seung-Jung Park MD, PhD 14:48-15:00, 2009 Symposium Arena, Level
Asian Pacific TCT Perspective of LM stenting with Current registry and Randomized Clinical Data Patrick W. Serruys MD PhD Yoshinobu Onuma MD Seung-Jung Park MD, PhD 14:48-15:00, 2009 Symposium Arena, Level
Revascularization for Patients with HFrEF: CABG and PCI and the Concept of Myocardial Viability
 Revascularization for Patients with HFrEF: CABG and PCI and the Concept of Myocardial Viability 22nd Annual Heart Failure 2018: an Update on Therapy April 2018 Eric J. Velazquez, MD, FACP, FACC, FASE,
Revascularization for Patients with HFrEF: CABG and PCI and the Concept of Myocardial Viability 22nd Annual Heart Failure 2018: an Update on Therapy April 2018 Eric J. Velazquez, MD, FACP, FACC, FASE,
Lessons learned From The National PCI Registry
 Lessons learned From The National PCI Registry w a v e On Behalf of The Publication Committee of the National PCI Registry Objectives & Anticipated Achievements To determine the epidemiology of patients
Lessons learned From The National PCI Registry w a v e On Behalf of The Publication Committee of the National PCI Registry Objectives & Anticipated Achievements To determine the epidemiology of patients
When should we indisputably perform CABG? Quand faut-il indiscutablement opérer? Dr Hakim BENAMER
 When should we indisputably perform CABG? Quand faut-il indiscutablement opérer? Dr Hakim BENAMER ICPS, Massy ICV-GVM La Roseraie, Aubervilliers Hôpital FOCH, Suresnes Disclosure Statement of Financial
When should we indisputably perform CABG? Quand faut-il indiscutablement opérer? Dr Hakim BENAMER ICPS, Massy ICV-GVM La Roseraie, Aubervilliers Hôpital FOCH, Suresnes Disclosure Statement of Financial
Better CABGs vs Better PCI Devices
 CABG vs PCI 2017 Multivessel Coronary Disease Better CABGs vs Better PCI Devices ACC New York, Dec 8, 2017 No Disclosures CABG vs PCI 2017 Stable Multivessel Coronary Disease 1. Are These The two Critical
CABG vs PCI 2017 Multivessel Coronary Disease Better CABGs vs Better PCI Devices ACC New York, Dec 8, 2017 No Disclosures CABG vs PCI 2017 Stable Multivessel Coronary Disease 1. Are These The two Critical
CPORT E Trial. Atlantic C PORT
 CPORT E Trial Randomized trial comparing medical, economic and quality of life outcomes of non primary PCI at hospitals with and without on site cardiac surgery Mo#va#on for Trial Sustain primary PCI program
CPORT E Trial Randomized trial comparing medical, economic and quality of life outcomes of non primary PCI at hospitals with and without on site cardiac surgery Mo#va#on for Trial Sustain primary PCI program
Master Class in Preventive Cardiology Focus on Diabetes and Cardiovascular Disease Geneva April
 Master Class in Preventive Cardiology Focus on Diabetes and Cardiovascular Disease Geneva April 14 2011 Coronary interventions in patients with diabetes Lars Rydén Karolinska Institutet Stockholm, Sweden
Master Class in Preventive Cardiology Focus on Diabetes and Cardiovascular Disease Geneva April 14 2011 Coronary interventions in patients with diabetes Lars Rydén Karolinska Institutet Stockholm, Sweden
Complex CAD (5) PVD-P Valv. CM. Sub-Clinical Arterial (2) DBD/Frailty (2) Health Political (1) Personal (3)
 PVD-P Valv. CM. Sub-Clinical Arterial (2) DBD/Frailty (2) Health Political (1) Personal (3)") 1. A Transition From Disease to Health 2. Heart Brain Integration 3. Imaging / Omics / Regeneration / Life Style Complex CAD (5) PVD-P Valv. CM AF Sub-Clinical Arterial (2) DBD/Frailty (2) Health Political
1. A Transition From Disease to Health 2. Heart Brain Integration 3. Imaging / Omics / Regeneration / Life Style Complex CAD (5) PVD-P Valv. CM AF Sub-Clinical Arterial (2) DBD/Frailty (2) Health Political
PROMUS Element Experience In AMC
 Promus Element Luncheon Symposium: PROMUS Element Experience In AMC Jung-Min Ahn, MD. University of Ulsan College of Medicine, Heart Institute, Asan Medical Center, Seoul, Korea PROMUS Element Clinical
Promus Element Luncheon Symposium: PROMUS Element Experience In AMC Jung-Min Ahn, MD. University of Ulsan College of Medicine, Heart Institute, Asan Medical Center, Seoul, Korea PROMUS Element Clinical
Southern Thoracic Surgical Association CABG in 2012: Implications of the New ESC/EACTS Guidelines
 Southern Thoracic Surgical Association 2011 CABG in 2012: Implications of the New ESC/EACTS Guidelines David P Taggart MD PhD FRCS Professor of Cardiovascular Surgery, University of Oxford Conflicts of
Southern Thoracic Surgical Association 2011 CABG in 2012: Implications of the New ESC/EACTS Guidelines David P Taggart MD PhD FRCS Professor of Cardiovascular Surgery, University of Oxford Conflicts of
Komplexe Koronarintervention heute: Von Syntax zu bioresorbierbaren Stents
 Komplexe Koronarintervention heute: Von Syntax zu bioresorbierbaren Stents Prof. Dr. med. Julinda Mehilli Medizinische Klinik und Poliklinik I Klinikum der Universität München Campus Großhadern Key Factors
Komplexe Koronarintervention heute: Von Syntax zu bioresorbierbaren Stents Prof. Dr. med. Julinda Mehilli Medizinische Klinik und Poliklinik I Klinikum der Universität München Campus Großhadern Key Factors
(ClinicalTrials.gov ID: NCT ) Title: The Italian Elderly ACS Study Author: Stefano Savonitto. Date: 29 August 2011 Meeting: ESC congress, Paris
 Title: The Italian Elderly ACS Study Author: Stefano Savonitto. Date: 29 August 2011 Meeting: ESC congress, Paris") Early aggressive versus initially conservative strategy in elderly patients with non-st- elevation acute coronary syndrome: the Italian randomised trial (ClinicalTrials.gov ID: NCT00510185) Stefano Savonitto,
Early aggressive versus initially conservative strategy in elderly patients with non-st- elevation acute coronary syndrome: the Italian randomised trial (ClinicalTrials.gov ID: NCT00510185) Stefano Savonitto,
Safety of Single- Versus Multi-vessel Angioplasty for Patients with AMI and Multi-vessel CAD
 Safety of Single- Versus Multi-vessel Angioplasty for Patients with AMI and Multi-vessel CAD Mun K. Hong, MD Associate Professor of Medicine Director, Cardiovascular Intervention and Research Weill Cornell
Safety of Single- Versus Multi-vessel Angioplasty for Patients with AMI and Multi-vessel CAD Mun K. Hong, MD Associate Professor of Medicine Director, Cardiovascular Intervention and Research Weill Cornell
FFR in Multivessel Disease
 FFR in Multivessel Disease April, 26 2013 Coronary Physiology in the Catheterization Laboratory Location: European Heart House, Nice, France Pim A.L. Tonino, MD, PhD Hartcentrum, Eindhoven, the Netherlands
FFR in Multivessel Disease April, 26 2013 Coronary Physiology in the Catheterization Laboratory Location: European Heart House, Nice, France Pim A.L. Tonino, MD, PhD Hartcentrum, Eindhoven, the Netherlands
PCI for Left Main Coronary Artery Stenosis. Jean Fajadet Clinique Pasteur, Toulouse, France
 PCI for Left Main Coronary Artery Stenosis Jean Fajadet Clinique Pasteur, Toulouse, France Athens, October 19, 2018 Left Main Coronary Artery Disease Significant unprotected left main coronary artery disease
PCI for Left Main Coronary Artery Stenosis Jean Fajadet Clinique Pasteur, Toulouse, France Athens, October 19, 2018 Left Main Coronary Artery Disease Significant unprotected left main coronary artery disease
Guidelines/Appropriateness ARCH 2015 St Louis, Missouri April 9-11, 2015 Manish A. Parikh, MD, FACC,FSCAI
 Guidelines/Appropriateness ARCH 2015 St Louis, Missouri April 9-11, 2015 Manish A. Parikh, MD, FACC,FSCAI Center for Interventional Vascular Therapy Columbia University Medical Center / New York Presbyterian
Guidelines/Appropriateness ARCH 2015 St Louis, Missouri April 9-11, 2015 Manish A. Parikh, MD, FACC,FSCAI Center for Interventional Vascular Therapy Columbia University Medical Center / New York Presbyterian
Le# Main Interven-on: When Is It Appropriate. Femi Philip, MD Assistant Professor Of Medicine UC Davis
 Le# Main Interven-on: When Is It Appropriate Femi Philip, MD Assistant Professor Of Medicine UC Davis Nil Disclosures Outline What is the LMCA? Should we revascularize severe LMCA disease? What revascularizacon
Le# Main Interven-on: When Is It Appropriate Femi Philip, MD Assistant Professor Of Medicine UC Davis Nil Disclosures Outline What is the LMCA? Should we revascularize severe LMCA disease? What revascularizacon
STEMI AND MULTIVESSEL CORONARY DISEASE
 STEMI AND MULTIVESSEL CORONARY DISEASE ΤΣΙΑΦΟΥΤΗΣ Ν. ΙΩΑΝΝΗΣ ΕΠΕΜΒΑΤΙΚΟΣ ΚΑΡΔΙΟΛΟΓΟΣ Α ΚΑΡΔΙΟΛΟΓΙΚΗ ΝΟΣ ΕΡΥΘΡΟΥ ΣΤΑΥΡΟΥ IRA 30-50% of STEMI patients have additional stenoses other than the infarct related
STEMI AND MULTIVESSEL CORONARY DISEASE ΤΣΙΑΦΟΥΤΗΣ Ν. ΙΩΑΝΝΗΣ ΕΠΕΜΒΑΤΙΚΟΣ ΚΑΡΔΙΟΛΟΓΟΣ Α ΚΑΡΔΙΟΛΟΓΙΚΗ ΝΟΣ ΕΡΥΘΡΟΥ ΣΤΑΥΡΟΥ IRA 30-50% of STEMI patients have additional stenoses other than the infarct related
What oral antiplatelet therapy would you choose? a) ASA alone b) ASA + Clopidogrel c) ASA + Prasugrel d) ASA + Ticagrelor
 ASA alone b) ASA + Clopidogrel c) ASA + Prasugrel d) ASA + Ticagrelor") 76 year old female Prior Hypertension, Hyperlipidemia, Smoking On Hydrochlorothiazide, Atorvastatin New onset chest discomfort; 2 episodes in past 24 hours Heart rate 122/min; BP 170/92 mm Hg, Killip Class
76 year old female Prior Hypertension, Hyperlipidemia, Smoking On Hydrochlorothiazide, Atorvastatin New onset chest discomfort; 2 episodes in past 24 hours Heart rate 122/min; BP 170/92 mm Hg, Killip Class
Coronary stenting: the appropriate use of FFR
 Coronary stenting: the appropriate use of FFR Morton J. Kern, MD Professor of Medicine Chief of Cardiology LBVA Associate Chief Cardiology University California Irvine Orange, California To treat or not
Coronary stenting: the appropriate use of FFR Morton J. Kern, MD Professor of Medicine Chief of Cardiology LBVA Associate Chief Cardiology University California Irvine Orange, California To treat or not
Risk of Stroke With Coronary Artery Bypass Graft Surgery Compared With Percutaneous Coronary Intervention
 Journal of the American College of Cardiology Vol. 60, No. 9, 2012 2012 by the American College of Cardiology Foundation ISSN 0735-1097/$36.00 Published by Elsevier Inc. http://dx.doi.org/10.1016/j.jacc.2011.10.912
Journal of the American College of Cardiology Vol. 60, No. 9, 2012 2012 by the American College of Cardiology Foundation ISSN 0735-1097/$36.00 Published by Elsevier Inc. http://dx.doi.org/10.1016/j.jacc.2011.10.912
Perioperative Cardiology Consultations for Noncardiac Surgery Ischemic Heart Disease
 2012 대한춘계심장학회 Perioperative Cardiology Consultations for Noncardiac Surgery Ischemic Heart Disease 울산의대울산대학병원심장내과이상곤 ECG CLASS IIb 1. Preoperative resting 12-lead ECG may be reasonable in patients with
2012 대한춘계심장학회 Perioperative Cardiology Consultations for Noncardiac Surgery Ischemic Heart Disease 울산의대울산대학병원심장내과이상곤 ECG CLASS IIb 1. Preoperative resting 12-lead ECG may be reasonable in patients with
PCI for Stable Ischemic Heart Disease: What Happened in the Last Week?
 PCI for Stable Ischemic Heart Disease: What Happened in the Last Week? Ajay J. Kirtane, MD, SM Center for Interventional Vascular Therapy Columbia University Medical Center / NewYork Presbyterian Hospital
PCI for Stable Ischemic Heart Disease: What Happened in the Last Week? Ajay J. Kirtane, MD, SM Center for Interventional Vascular Therapy Columbia University Medical Center / NewYork Presbyterian Hospital
ESC GUIDELINES ON DIABETES AND CARDIOVASCULAR DISEASES
 ESC GUIDELINES ON DIABETES AND CARDIOVASCULAR DISEASES Pr. Michel KOMAJDA Institute of Cardiology - IHU ICAN Pitie Salpetriere Hospital - University Pierre and Marie Curie, Paris (France) DEFINITION A
ESC GUIDELINES ON DIABETES AND CARDIOVASCULAR DISEASES Pr. Michel KOMAJDA Institute of Cardiology - IHU ICAN Pitie Salpetriere Hospital - University Pierre and Marie Curie, Paris (France) DEFINITION A
Supplementary Material to Mayer et al. A comparative cohort study on personalised
 Suppl. Table : Baseline characteristics of the patients. Characteristic Modified cohort Non-modified cohort P value (n=00) Age years 68. ±. 69.5 ±. 0. Female sex no. (%) 60 (0.0) 88 (.7) 0.0 Body Mass
Suppl. Table : Baseline characteristics of the patients. Characteristic Modified cohort Non-modified cohort P value (n=00) Age years 68. ±. 69.5 ±. 0. Female sex no. (%) 60 (0.0) 88 (.7) 0.0 Body Mass
Mise à Jour sur le traitement du Pluritronculaire Philippe Généreux, MD
 Mise à Jour sur le traitement du Pluritronculaire Philippe Généreux, MD Columbia University Medical Center and The Cardiovascular Research Foundation, New York, USA Hôpital du Sacré-Coeur de Montréal,
Mise à Jour sur le traitement du Pluritronculaire Philippe Généreux, MD Columbia University Medical Center and The Cardiovascular Research Foundation, New York, USA Hôpital du Sacré-Coeur de Montréal,
Coronary Heart Disease in Patients With Diabetes
 Journal of the American College of Cardiology Vol. 49, No. 6, 2007 2007 by the American College of Cardiology Foundation ISSN 0735-1097/07/$32.00 Published by Elsevier Inc. doi:10.1016/j.jacc.2006.09.045
Journal of the American College of Cardiology Vol. 49, No. 6, 2007 2007 by the American College of Cardiology Foundation ISSN 0735-1097/07/$32.00 Published by Elsevier Inc. doi:10.1016/j.jacc.2006.09.045
FAME STUDY: 2-year Follow-Up & CLINICAL SUBGROUP ANALYSIS
 Coronary Physiology In The Cathlab FAME STUDY: 2-year Follow-Up & CLINICAL SUBGROUP ANALYSIS Educational Training Program ESC European Heart House april 7th 9th 2011 Nico H.J.Pijls, MD, PhD Catharina Hospital,
Coronary Physiology In The Cathlab FAME STUDY: 2-year Follow-Up & CLINICAL SUBGROUP ANALYSIS Educational Training Program ESC European Heart House april 7th 9th 2011 Nico H.J.Pijls, MD, PhD Catharina Hospital,
Patients in whom PCI is preferred over CABG _ Aleksander Ernst Clinical Hospital Center Zagreb University of Zagreb School of Medicine Zagreb, CROATIA
 3rd Dubrovnik Cardiology Highlights An ESC Update Programme in Cardiology 26.09.-29.09.2013, Hotel Excelsior, Dubrovnik, Croatia Patients in whom PCI is preferred over CABG _ Aleksander Ernst Clinical
3rd Dubrovnik Cardiology Highlights An ESC Update Programme in Cardiology 26.09.-29.09.2013, Hotel Excelsior, Dubrovnik, Croatia Patients in whom PCI is preferred over CABG _ Aleksander Ernst Clinical
Drug Eluting Stents: Bifurcation and Left Main Approach
 TCT Asia 2006 Drug Eluting Stents: Bifurcation and Left Main Approach Eberhard Grube MD FACC, FSCAI Heart Center,, Germany Stanford University, School of Medicine, CA, USA DES in High Risk Lesions TAXUS
TCT Asia 2006 Drug Eluting Stents: Bifurcation and Left Main Approach Eberhard Grube MD FACC, FSCAI Heart Center,, Germany Stanford University, School of Medicine, CA, USA DES in High Risk Lesions TAXUS
The MAIN-COMPARE Registry
 Long-Term Outcomes of Coronary Stent Implantation versus Bypass Surgery for the Treatment of Unprotected Left Main Coronary Artery Disease Revascularization for Unprotected Left MAIN Coronary Artery Stenosis:
Long-Term Outcomes of Coronary Stent Implantation versus Bypass Surgery for the Treatment of Unprotected Left Main Coronary Artery Disease Revascularization for Unprotected Left MAIN Coronary Artery Stenosis:
CLINICAL CONSEQUENCES OF THE
 CLINICAL CONSEQUENCES OF THE FAME STUDY TCT ASIA Seoul, Korea, april 26 th, 2012 Nico H. J. Pijls, MD, PhD Catharina Hospital, Eindhoven, The Netherlands GUIDELINES ESC SEPTEMBER 2010 FFR UPGRADED TO LEVEL
CLINICAL CONSEQUENCES OF THE FAME STUDY TCT ASIA Seoul, Korea, april 26 th, 2012 Nico H. J. Pijls, MD, PhD Catharina Hospital, Eindhoven, The Netherlands GUIDELINES ESC SEPTEMBER 2010 FFR UPGRADED TO LEVEL
Cardiogenic Shock. Carlos Cafri,, MD
 Cardiogenic Shock Carlos Cafri,, MD SHOCK= Inadequate Tissue Mechanisms: Perfusion Inadequate oxygen delivery Release of inflammatory mediators Further microvascular changes, compromised blood flow and
Cardiogenic Shock Carlos Cafri,, MD SHOCK= Inadequate Tissue Mechanisms: Perfusion Inadequate oxygen delivery Release of inflammatory mediators Further microvascular changes, compromised blood flow and
ACUTE CORONARY SYNDROME PCI IN THE ELDERLY
 ACUTE CORONARY SYNDROME PCI IN THE ELDERLY G.KARABELA MD.PhD ATHENS NAVAL HOSPITAL INTERVENTIONAL CARDIOLOGY DEPARTMENT NO CONFLICT OF INTEREST TO DECLAIRE Risk stratification in Αcute Coronary Syndrome.
ACUTE CORONARY SYNDROME PCI IN THE ELDERLY G.KARABELA MD.PhD ATHENS NAVAL HOSPITAL INTERVENTIONAL CARDIOLOGY DEPARTMENT NO CONFLICT OF INTEREST TO DECLAIRE Risk stratification in Αcute Coronary Syndrome.
Unprotected Left Main Coronary Artery Disease in Patients With Low Predictive Risk of Mortality
 Unprotected Left Main Coronary Artery Disease in Patients With Low Predictive Risk of Mortality Shun Watanabe, MD, Tatsuhiko Komiya, MD, Genichi Sakaguchi, MD, PhD, and Takeshi Shimamoto, MD, PhD Department
Unprotected Left Main Coronary Artery Disease in Patients With Low Predictive Risk of Mortality Shun Watanabe, MD, Tatsuhiko Komiya, MD, Genichi Sakaguchi, MD, PhD, and Takeshi Shimamoto, MD, PhD Department
Management of stable CAD FFR guided therapy: the new gold standard
 Management of stable CAD FFR guided therapy: the new gold standard Suleiman Kharabsheh, MD Director; CCU, Telemetry and CHU Associate professor of Cardiology, Alfaisal Univ. KFHI - KFSHRC Should patients
Management of stable CAD FFR guided therapy: the new gold standard Suleiman Kharabsheh, MD Director; CCU, Telemetry and CHU Associate professor of Cardiology, Alfaisal Univ. KFHI - KFSHRC Should patients
Management of Stable Ischemic Heart Disease. Vinay Madan MD February 10, 2018
 Management of Stable Ischemic Heart Disease Vinay Madan MD February 10, 2018 1 Disclosure No financial disclosure. 2 Overview of SIHD Diagnosis Outline of talk Functional vs. Anatomic assessment Management
Management of Stable Ischemic Heart Disease Vinay Madan MD February 10, 2018 1 Disclosure No financial disclosure. 2 Overview of SIHD Diagnosis Outline of talk Functional vs. Anatomic assessment Management
The synergy between percutaneous coronary intervention with TAXUS and cardiac surgery study: A surgical perspective
 SYNTAX STUDY The synergy between percutaneous coronary intervention with TAXUS and cardiac surgery study: A surgical perspective Jacques van Wyk ABSTRACT Panorama Medi-Clinic and Department of Cardiothoracic
SYNTAX STUDY The synergy between percutaneous coronary intervention with TAXUS and cardiac surgery study: A surgical perspective Jacques van Wyk ABSTRACT Panorama Medi-Clinic and Department of Cardiothoracic
Left Main PCI vs. CABG: Real World
 Management of Patients with Stable CAD Left Main PCI vs. CABG: Real World Marco Roffi, MD, FESC University Hospital Geneva, Switzerland SYNTAX-LMT The SYNTAX trial included a pre-specified subgroup of
Management of Patients with Stable CAD Left Main PCI vs. CABG: Real World Marco Roffi, MD, FESC University Hospital Geneva, Switzerland SYNTAX-LMT The SYNTAX trial included a pre-specified subgroup of
By 2000, more than percutaneous and
 Review: Current Perspective Indications for Coronary Artery Bypass Surgery and Percutaneous Coronary Intervention in Chronic Stable Angina Review of the Evidence and Methodological Considerations Charanjit
Review: Current Perspective Indications for Coronary Artery Bypass Surgery and Percutaneous Coronary Intervention in Chronic Stable Angina Review of the Evidence and Methodological Considerations Charanjit
Emergency surgery in acute coronary syndrome
 Emergency surgery in acute coronary syndrome Teerawoot Jantarawan Division of Cardiothoracic Surgery, Department of Surgery, Faculty of Medicine Siriraj Hospital, Mahidol University, Bangkok, Thailand
Emergency surgery in acute coronary syndrome Teerawoot Jantarawan Division of Cardiothoracic Surgery, Department of Surgery, Faculty of Medicine Siriraj Hospital, Mahidol University, Bangkok, Thailand
Fractional Flow Reserve: Review of the latest data
 Fractional Flow Reserve: Review of the latest data Michalis Hamilos, MD, PhD, FESC University Hospital of Heraklion Fractional Flow Reserve (FFR) Coronary angiography does not always tell the truth Most
Fractional Flow Reserve: Review of the latest data Michalis Hamilos, MD, PhD, FESC University Hospital of Heraklion Fractional Flow Reserve (FFR) Coronary angiography does not always tell the truth Most
ΑΓΓΕΙΟΠΛΑΣΤΙΚΗ ΣΤΟ ΔΙΑΒΗΤΙΚΟ ΑΣΘΕΝΗ
 ΑΓΓΕΙΟΠΛΑΣΤΙΚΗ ΣΤΟ ΔΙΑΒΗΤΙΚΟ ΑΣΘΕΝΗ Νίκος Μεζίλης MD, FESC Κλινική Άγιος Λουκάς Why diabetes is associated with restenosis endothelial dysfunction metabolic alterations accelerated platelet deposition
ΑΓΓΕΙΟΠΛΑΣΤΙΚΗ ΣΤΟ ΔΙΑΒΗΤΙΚΟ ΑΣΘΕΝΗ Νίκος Μεζίλης MD, FESC Κλινική Άγιος Λουκάς Why diabetes is associated with restenosis endothelial dysfunction metabolic alterations accelerated platelet deposition