Inhaled nitric oxide: clinical evidence for use in adults
|
|
|
- Brianne Cameron
- 6 years ago
- Views:
Transcription



1 Inhaled nitric oxide: clinical evidence for use in adults Neill Adhikari Critical Care Medicine Sunnybrook Health Sciences Centre and University of Toronto 31 October 2014
2 Conflict of interest Ikaria provided data for 3 trials included in a metaanalysis No other support
3 Objectives Review data from randomized trials of inhaled NO, primarily in ARDS Consider whether our practice should change



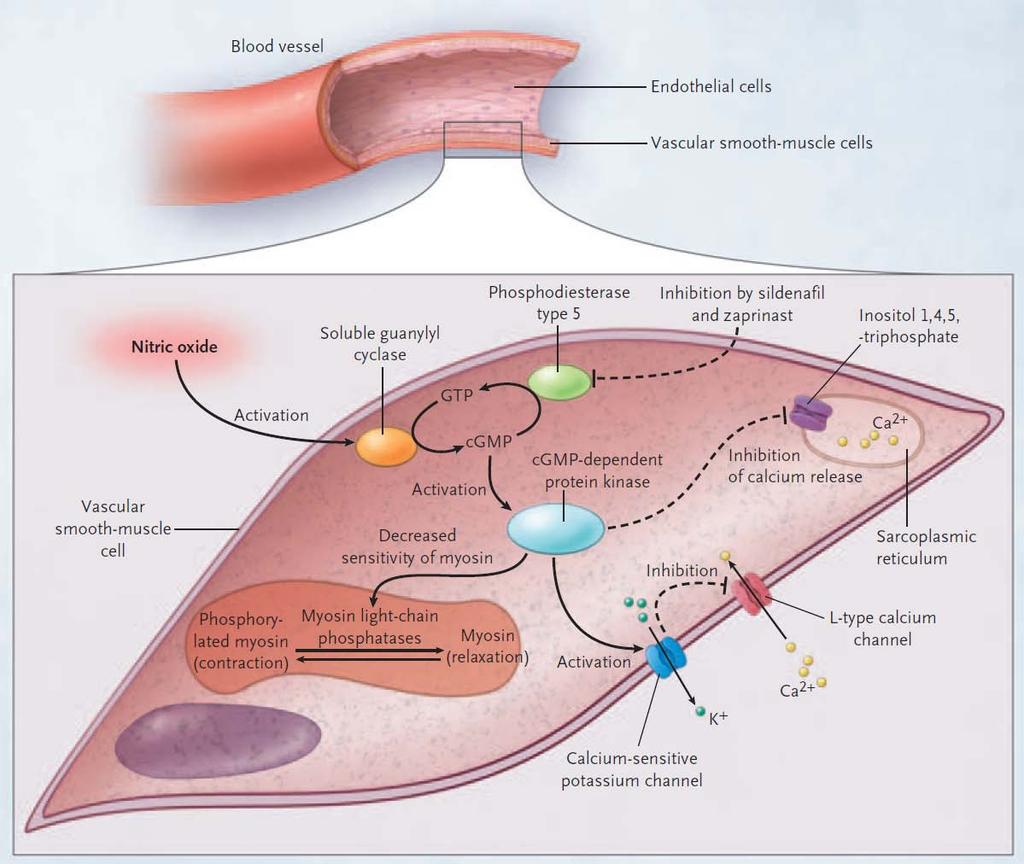
4 1998 Nobel Prize in Physiology or Medicine Robert Furchgott Louis Ignarro Ferid Murad
5 N Engl J Med 1993;328: N=9
6 N Engl J Med 1993;328: N=9
7 N Engl J Med 1993;328: N=9
8 N Engl J Med 1993;328: N=7
9 Rapid clinical uptake Survey of ESICM members, % (196/310) used NO (95% reported ARDS as an indication) Survey of Ontario intensivists, % used NO sometimes or always 15% rarely 47% never Intensive Care Med 24:864-77, Crit Care Med 32:946-54



10 It s 2014 why is anyone still talking about NO?
11 This is one reason 250, ,000 total cost total patient-hours 2,500 2, ,000 1, ,000 1,000 50, /8 2008/9 2009/ / / / /14 Sunnybrook HSC, NO utilisation data Protocol 0
12 We re not the only ones who use NO Mayo Clinic: 7% of ARDS patients 10% of patients with LIS 3 H1N1 pandemic South Korea, 8% Europe, 12% Canada, 14% Crit Care Med 2010; 38(12 Suppl):377; Am J Respir Crit Care Med 2011; 183:A1643; Am J Respir Crit Care Med 2011; 183:A1698; Intensive Care Med 2010; 36(Suppl 2):S370 JAMA 2009; 302:
13 Arguments from the bedside Mayo Clinic: 7% of ARDS patients 10% of patients with LIS 3 H1N1 pandemic South Korea, 8% Europe, 12% Canada, 14% Absence of evidence Evidence of absence Don t talk to me about trials, my patient is very sick Crit Care Med 2010; 38(12 Suppl):377; Am J Respir Crit Care Med 2011; 183:A1643; Am J Respir Crit Care Med 2011; 183:A1698; Intensive Care Med 2010; 36(Suppl 2):S370 JAMA 2009; 302:
14 NO does not belong in this category Intubation or tracheostomy for airway obstruction Vasopressors for shock Early antibiotics for septic shock Insulin for DKA Epinephrine for anaphylaxis General anaesthesia for surgery Thus, using GRADE s definition of quality of evidence, the underlying quality of evidence to support these clinical interventions would be considered high although the evidence comes from observational studies or from unsystematic clinical observations. Journal of Clinical Epidemiology 64 (2011)
15 The data: meta-analysis of ARDS trials Old data! Mortality analysis: 9 trials, 1142 patients 2 other eligible trials (lost data; no contact) AECC criteria for ARDS (1 trial, ALI) Dose Fixed, 4 trials Lowest dose to improve oxygenation, 4 trials Randomized to different doses, 1 trial Duration Median 6.5 d (3.5-9)
16 P/F ratio: short term effect BMJ 2007;334:779
17 PA mean : short term effect BMJ 2007;334:779
18 No effect on mortality Crit Care Med 2014; 42:
19 Crit Care Med 2014; 42: No effect on mortality regardless of P/F ratio
20 Intensive Care Med 2010;36: Unlike proning
 mechanism?")
21 More AKI these trials represent 72% of randomized patients variable definitions (new RRT in Lundin, Payen) mechanism? BMJ 2007;334:779
22 Why was NO ineffective? (1) Oxygenation may be the wrong target ARDS network trial OSCILLATE Only 13-19% die from respiratory failure Benefit overwhelmed by injurious MV NO does not decrease VILI Chest 2005;128:525 32; ARRD 1985;132:485-9
23 Why was NO ineffective? (2) Accumulated toxicity over time Am J Respir Crit Care Med 2003;167:
24 84 patients undergoing lung transplantation Randomised to NO 20 ppm or nitrogen Started 10 mins after start of reperfusion, for 6 hours Median duration 10.5 hr (NO) vs. 9.6 hr (N 2 ) Criteria for unblinded NO Criteria for weaning Am J Respir Crit Care Med 2003;167:1483

25 Am J Respir Crit Care Med 2003;167:1483
26 Mitral valve surgery 28 patients with MS and pulmonary HTN for MV repair or replacement PA sys >60 mmhg and NYHA 2 Randomised, unblinded NO 10 ppm vs oxygen from end of CPB to up to 48 hours Via ETT and sealed mask after extubation Am J Cardiol 2011;107:
27 Mitral valve surgery NO Oxygen Am J Cardiol 2011;107:

28 LVAD implantation: physiology 20 ppm 20 ppm 11 patients with LVAD with PA mean >25 mmhg and CI <2.5 L/min/m 2 at end of CPB Ann Thorac Surg 1998;65:340 5
29 LVAD implantation: clinical 150 patients undergoing LVAD, with PVR 200 dyne/s/cm -5 Excluded: current or planned BiVAD or ECLS Randomised to NO 40 ppm or placebo starrting 5 mins before CPB wean, continued for up to 48 hrs Main outcome RV dysfunction J Heart Lung Transplant 2011;30:870 8
30 LVAD implantation: clinical NO Placebo p-value Open-label NO 21% 26% RV dysfunction 9.6% 15.6% day mortality 11.3% 11.4% day RVAD 5.6% 10.0% 0.47 RRT 14.1% 11.4% /35 crossovers BEFORE study defined criteria 15/18 from 1 centre J Heart Lung Transplant 2011;30:870 8
31 Possible responses to the data I don t believe the results Wrong patients Not enough patients Wrong design Wrong outcome Wrong treatment specifics I may still use NO sometimes, with appropriate humility about my convictions We need a total crackdown on NO prescription
32 Conclusions Physiologic mechanism of NO makes it an attractive therapy for several conditions RCTs support time-limited modest physiological effects RCTs in ARDS No effect on mortality regardless of hypoxemia Increased AKI mechanism unclear
33 Conclusions Use of NO is highly likely to continue In short term: limited harm and modest benefit more dramatic benefit in some Rule of rescue (clinicians thresholds differ) Temporising strategy Easy to administer Clinicians insensitive to costs at point of care Protocols may force early reassessment and stopping when physiologic goals not met

34 Conclusion: In summary, the discovery of and research on the many positive effects of ino has improved care of critically ill patients worldwide. It is a noble effort to continue on this path. Conflicts of interest: None.
35 thank you
36 What is NO? Atmospheric gas, 10 ppb to 1.5 ppm Rapidly inactivated when inhaled Airway epithelium: NO 2 reactive oxygen and nitrogen species Blood: Methemoglobin S-nitrosothiols vasodilation, platelet inhibitor
37 N Engl J Med 2005;353:



38 N Engl J Med 2005;353:
39 Effects of NO from RCTs Several multicentre RCTs found no mortality benefit Lundin, 1999, n=180 Payen, 1999, n=203 Taylor, 2004, n=385 Meta-analysis (2003) pooled data from 2 trials: RR 0.98 ( ) Additional data since previous review
40 Lundin et al, 1999 Intensive Care Med 25: centres in Europe Concealed, not blinded, 10/87 crossovers, ITT, complete f/u Stopped early (planned n=600) N=180 (responders randomized) Unilateral or bilateral infiltrates, P/F 165, PEEP 5, Paw 10 Lowest effective dose (mean 9 ppm, SD 8) Up to 30d (mean 9, SD 6)
41 Lundin et al, 1999 Intensive Care Med 25:911-9 NO n=93 control n=87 30d mortality 44.1% 40.2% 90d mortality Reversal ALI Severe resp fail p=0.04 New RRT or p=0.01 creat >300
42 Payen et al, 1999 Intensive Care Med 25(Suppl. 1):S centres in France Concealed, blinded, 19/105 crossovers to NO, ITT, complete f/u N=203 AECC criteria and LIS 2-3 after 24h optimisation 10 ppm Up to 28d (median 5d)
43 Payen et al, 1999 Intensive Care Med 25(Suppl. 1):S166 NO n=98 control n=105 28d mortality 49.0% 43.8% Hosp DC 90d New RRT
44 Taylor et al, 2004 JAMA 291: centres in USA Concealed, blinded, no crossovers, ITT, complete f/u Stopped early, planned N=516 N=385 AECC (ALI), P/F 250, PEEP 8 5 ppm Max 28 d (mean?)
45 Taylor et al, 2004 JAMA 291: NO n=192 control n=193 28d mortality 22.9% 20.2% VFD (28d) 10.7d 10.6d creat 6.2% 4.1%
46 Observations from these RCTs Slightly higher mortality in NO arm Slightly more renal dysfunction in NO arm The trial restricted to responders (Lundin) did not show benefit either
47 Objective: current meta-analysis evaluate the effects of NO in patients with established ALI and ARDS on pulmonary physiology (P a O 2 /F i O 2, OI, mean PA pressure) clinical outcomes (mortality and duration of ventilation) Adverse events
48 Methods Search of MEDLINE, EMBASE, CINAHL, CENTRAL (to Oct 2006) Proceedings ATS, SCCM, ESICM, Chest ( ) Bibliographies Contact with trial authors / experts
49 Methods Inclusion Parallel group RCTs NO used for treatment 80% ALI/ARDS or separately reported subgroup ALI/ARDS using authors definitions Adults and children (not neonates) Duplicate data abstraction
50 Methods Outcomes Mortality Duration MV, VFD Pulmonary physiology (days 1, 2, 3, 4) Adverse events
51 Methods Analysis Random-effects RCTs with <50% crossovers included in clinical outcomes analyses Data from multiple-dose groups combined Binary outcomes: RR Continuous outcomes: ratio of means, weighted mean difference Heterogeneity considered: dose, duration, ALI vs ARDS
52 OI: short term effect BMJ 2007;334:779
ARDS and Lung Protection
 ARDS and Lung Protection Kristina Sullivan, MD Associate Professor University of California, San Francisco Department of Anesthesia and Perioperative Care Division of Critical Care Medicine Overview Low
ARDS and Lung Protection Kristina Sullivan, MD Associate Professor University of California, San Francisco Department of Anesthesia and Perioperative Care Division of Critical Care Medicine Overview Low
Year in Review Intensive Care Training Program Radboud University Medical Centre Nijmegen
 Year in Review 2013 Intensive Care Training Program Radboud University Medical Centre Nijmegen Contents ARDS Ventilator associated pneumonia Tracheostomy and endotracheal intubation Enteral feeding Fluid
Year in Review 2013 Intensive Care Training Program Radboud University Medical Centre Nijmegen Contents ARDS Ventilator associated pneumonia Tracheostomy and endotracheal intubation Enteral feeding Fluid
ARDS Assisted ventilation and prone position. ICU Fellowship Training Radboudumc
 ARDS Assisted ventilation and prone position ICU Fellowship Training Radboudumc Fig. 1 Physiological mechanisms controlling respiratory drive and clinical consequences of inappropriate respiratory drive
ARDS Assisted ventilation and prone position ICU Fellowship Training Radboudumc Fig. 1 Physiological mechanisms controlling respiratory drive and clinical consequences of inappropriate respiratory drive
SCVMC RESPIRATORY CARE PROCEDURE
 Page 1 of 7 New: 12/08 R: 4/11 R NC: 7/11, 7/12 B7180-63 Definitions: Inhaled nitric oxide (i) is a medical gas with selective pulmonary vasodilator properties. Vaso-reactivity is the evidence of acute
Page 1 of 7 New: 12/08 R: 4/11 R NC: 7/11, 7/12 B7180-63 Definitions: Inhaled nitric oxide (i) is a medical gas with selective pulmonary vasodilator properties. Vaso-reactivity is the evidence of acute
Pro: Early use of VV ECMO for ARDS
 Pro: Early use of VV ECMO for ARDS Kyle J. Rehder, MD, FCCP Associate Professor Division of Pediatric Critical Care Medicine Department of Pediatrics Duke Children s Hospital The ventilator is slowly killing
Pro: Early use of VV ECMO for ARDS Kyle J. Rehder, MD, FCCP Associate Professor Division of Pediatric Critical Care Medicine Department of Pediatrics Duke Children s Hospital The ventilator is slowly killing
Wet Lungs Dry lungs Impact on Outcome in ARDS. Charlie Phillips MD Division of PCCM OHSU 2009
 Wet Lungs Dry lungs Impact on Outcome in ARDS Charlie Phillips MD Division of PCCM OHSU 2009 Today s talk Pathophysiology of ARDS The case for dry Targeting EVLW Disclosures Advisor for Pulsion Medical
Wet Lungs Dry lungs Impact on Outcome in ARDS Charlie Phillips MD Division of PCCM OHSU 2009 Today s talk Pathophysiology of ARDS The case for dry Targeting EVLW Disclosures Advisor for Pulsion Medical
Outcomes From Severe ARDS Managed Without ECMO. Roy Brower, MD Johns Hopkins University Critical Care Canada Forum Toronto November 1, 2016
 Outcomes From Severe ARDS Managed Without ECMO Roy Brower, MD Johns Hopkins University Critical Care Canada Forum Toronto November 1, 2016 Severe ARDS Berlin Definition 2012 P:F ratio 100 mm Hg Prevalence:
Outcomes From Severe ARDS Managed Without ECMO Roy Brower, MD Johns Hopkins University Critical Care Canada Forum Toronto November 1, 2016 Severe ARDS Berlin Definition 2012 P:F ratio 100 mm Hg Prevalence:
Application of Lung Protective Ventilation MUST Begin Immediately After Intubation
 Conflict of Interest Disclosure Robert M Kacmarek Managing Severe Hypoxemia!" 9-28-17 FOCUS Bob Kacmarek PhD, RRT Massachusetts General Hospital, Harvard Medical School, Boston, Massachusetts I disclose
Conflict of Interest Disclosure Robert M Kacmarek Managing Severe Hypoxemia!" 9-28-17 FOCUS Bob Kacmarek PhD, RRT Massachusetts General Hospital, Harvard Medical School, Boston, Massachusetts I disclose
Adjunct Therapies for Pediatric ARDS: Where are the Data?
 Adjunct Therapies for Pediatric ARDS: Where are the Data? Alexandre T. Rotta, MD, FCCM Professor of Pediatrics, Linsalata Family Endowed Chair in Pediatric Critical Care and Emergency Medicine Rainbow
Adjunct Therapies for Pediatric ARDS: Where are the Data? Alexandre T. Rotta, MD, FCCM Professor of Pediatrics, Linsalata Family Endowed Chair in Pediatric Critical Care and Emergency Medicine Rainbow
USE OF INHALED NITRIC OXIDE IN THE NICU East Bay Newborn Specialists Guideline Prepared by P Joe, G Dudell, A D Harlingue Revised 7/9/2014
 USE OF INHALED NITRIC OXIDE IN THE NICU East Bay Newborn Specialists Guideline Prepared by P Joe, G Dudell, A D Harlingue Revised 7/9/2014 ino for Late Preterm and Term Infants with Severe PPHN Background:
USE OF INHALED NITRIC OXIDE IN THE NICU East Bay Newborn Specialists Guideline Prepared by P Joe, G Dudell, A D Harlingue Revised 7/9/2014 ino for Late Preterm and Term Infants with Severe PPHN Background:
Back to the Future: Updated Guidelines for Evaluation and Management of Adrenal Insufficiency in the Critically Ill
 Back to the Future: Updated Guidelines for Evaluation and Management of Adrenal Insufficiency in the Critically Ill Joe Palumbo PGY-2 Critical Care Pharmacy Resident Buffalo General Medical Center Disclosures
Back to the Future: Updated Guidelines for Evaluation and Management of Adrenal Insufficiency in the Critically Ill Joe Palumbo PGY-2 Critical Care Pharmacy Resident Buffalo General Medical Center Disclosures
The new ARDS definitions: what does it mean?
 The new ARDS definitions: what does it mean? Richard Beale 7 th September 2012 METHODS ESICM convened an international panel of experts, with representation of ATS and SCCM The objectives were to update
The new ARDS definitions: what does it mean? Richard Beale 7 th September 2012 METHODS ESICM convened an international panel of experts, with representation of ATS and SCCM The objectives were to update
ACUTE RESPIRATORY DISTRESS SYNDROME
 ACUTE RESPIRATORY DISTRESS SYNDROME Angel Coz MD, FCCP, DCE Assistant Professor of Medicine UCSF Fresno November 4, 2017 No disclosures OBJECTIVES Identify current trends and risk factors of ARDS Describe
ACUTE RESPIRATORY DISTRESS SYNDROME Angel Coz MD, FCCP, DCE Assistant Professor of Medicine UCSF Fresno November 4, 2017 No disclosures OBJECTIVES Identify current trends and risk factors of ARDS Describe
Sub-category: Intensive Care for Respiratory Distress
 Course n : Course 3 Title: RESPIRATORY PHYSIOLOGY, PHYSICS AND PATHOLOGY IN RELATION TO ANAESTHESIA AND INTENSIVE CARE Sub-category: Intensive Care for Respiratory Distress Topic: Acute Respiratory Distress
Course n : Course 3 Title: RESPIRATORY PHYSIOLOGY, PHYSICS AND PATHOLOGY IN RELATION TO ANAESTHESIA AND INTENSIVE CARE Sub-category: Intensive Care for Respiratory Distress Topic: Acute Respiratory Distress
ECMO: a breakthrough in care for respiratory failure. PD Dr. Thomas Müller Regensburg no conflict of interest
 ECMO: a breakthrough in care for respiratory failure? PD Dr. Thomas Müller Regensburg no conflict of interest 1 Overview Mortality of severe ARDS Indication for ECMO PaO 2 /FiO 2 Efficiency of ECMO: gas
ECMO: a breakthrough in care for respiratory failure? PD Dr. Thomas Müller Regensburg no conflict of interest 1 Overview Mortality of severe ARDS Indication for ECMO PaO 2 /FiO 2 Efficiency of ECMO: gas
Acute Lung Injury/ARDS. Disclosures. Overview. Acute Respiratory Failure 5/30/2014. Research funding: NIH, UCSF CTSI, Glaxo Smith Kline
 Disclosures Acute Respiratory Failure Carolyn S. Calfee, MD MAS UCSF Critical Care Medicine and Trauma CME May 30, 2014 Research funding: NIH, UCSF CTSI, Glaxo Smith Kline Medical advisory boards: Cerus
Disclosures Acute Respiratory Failure Carolyn S. Calfee, MD MAS UCSF Critical Care Medicine and Trauma CME May 30, 2014 Research funding: NIH, UCSF CTSI, Glaxo Smith Kline Medical advisory boards: Cerus
PAEDIATRIC RESPIRATORY FAILURE. Tang Swee Fong Department of Paediatrics University Kebangsaan Malaysia Medical Centre
 PAEDIATRIC RESPIRATORY FAILURE Tang Swee Fong Department of Paediatrics University Kebangsaan Malaysia Medical Centre Outline of lecture Bronchiolitis Bronchopulmonary dysplasia Asthma ARDS Bronchiolitis
PAEDIATRIC RESPIRATORY FAILURE Tang Swee Fong Department of Paediatrics University Kebangsaan Malaysia Medical Centre Outline of lecture Bronchiolitis Bronchopulmonary dysplasia Asthma ARDS Bronchiolitis
Ventilation update Anaesthesia departmental PGME. Tuesday 10 th December Dr Alastair Glossop Consultant Anaesthesia and Critical Care
 Ventilation update Anaesthesia departmental PGME Tuesday 10 th December Dr Alastair Glossop Consultant Anaesthesia and Critical Care What s fashionable in ICU ventilation? Acute respiratory distress syndrome
Ventilation update Anaesthesia departmental PGME Tuesday 10 th December Dr Alastair Glossop Consultant Anaesthesia and Critical Care What s fashionable in ICU ventilation? Acute respiratory distress syndrome
Oxygenation Failure. Increase FiO2. Titrate end-expiratory pressure. Adjust duty cycle to increase MAP. Patient Positioning. Inhaled Vasodilators
 Oxygenation Failure Increase FiO2 Titrate end-expiratory pressure Adjust duty cycle to increase MAP Patient Positioning Inhaled Vasodilators Extracorporeal Circulation ARDS Radiology Increasing Intensity
Oxygenation Failure Increase FiO2 Titrate end-expiratory pressure Adjust duty cycle to increase MAP Patient Positioning Inhaled Vasodilators Extracorporeal Circulation ARDS Radiology Increasing Intensity
Landmark articles on ventilation
 Landmark articles on ventilation Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity ARDS AECC DEFINITION-1994 ALI Acute onset Bilateral chest infiltrates PCWP
Landmark articles on ventilation Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity ARDS AECC DEFINITION-1994 ALI Acute onset Bilateral chest infiltrates PCWP
ino in neonates with cardiac disorders
 ino in neonates with cardiac disorders Duncan Macrae Paediatric Critical Care Terminology PAP Pulmonary artery pressure PVR Pulmonary vascular resistance PHT Pulmonary hypertension - PAP > 25, PVR >3,
ino in neonates with cardiac disorders Duncan Macrae Paediatric Critical Care Terminology PAP Pulmonary artery pressure PVR Pulmonary vascular resistance PHT Pulmonary hypertension - PAP > 25, PVR >3,
ECMO for Severe Hypoxemic Respiratory Failure: Pro-Con Debate. Carolyn Calfee, MD MAS Mark Eisner, MD MPH
 ECMO for Severe Hypoxemic Respiratory Failure: Pro-Con Debate Carolyn Calfee, MD MAS Mark Eisner, MD MPH June 3, 2010 Case Presentation Setting: Community hospital, November 2009 29 year old woman with
ECMO for Severe Hypoxemic Respiratory Failure: Pro-Con Debate Carolyn Calfee, MD MAS Mark Eisner, MD MPH June 3, 2010 Case Presentation Setting: Community hospital, November 2009 29 year old woman with
Prone Position in ARDS
 Prone Position in ARDS Rich Kallet MS RRT FAARC, FCCM Respiratory Care Services San Francisco General Hospital University of California, San Francisco, Case Study A 39 yo F admitted to SFGH TICU s/p hanging,
Prone Position in ARDS Rich Kallet MS RRT FAARC, FCCM Respiratory Care Services San Francisco General Hospital University of California, San Francisco, Case Study A 39 yo F admitted to SFGH TICU s/p hanging,
Steroids for ARDS. Clinical Problem. Management
 Steroids for ARDS James Beck Clinical Problem A 60 year old lady re-presented to ICU with respiratory failure. She had previously been admitted for fluid management and electrolyte correction having presented
Steroids for ARDS James Beck Clinical Problem A 60 year old lady re-presented to ICU with respiratory failure. She had previously been admitted for fluid management and electrolyte correction having presented
THE USE OF HYPERINFLATION IN THE MANAGEMENT OF INTUBATED AND VENTILATED ADULT PATIENTS RECOMMENDATIONS
 THE USE OF HYPERINFLATION IN THE MANAGEMENT OF INTUBATED AND VENTILATED ADULT PATIENTS RECOMMENDATIONS Recommendation 1 on website Hyperinflation (Ventilator or manual) might be included in the management
THE USE OF HYPERINFLATION IN THE MANAGEMENT OF INTUBATED AND VENTILATED ADULT PATIENTS RECOMMENDATIONS Recommendation 1 on website Hyperinflation (Ventilator or manual) might be included in the management
Ventilatory Management of ARDS. Alexei Ortiz Milan; MD, MSc
 Ventilatory Management of ARDS Alexei Ortiz Milan; MD, MSc 2017 Outline Ventilatory management of ARDS Protected Ventilatory Strategy Use of NMB Selection of PEEP Driving pressure Lung Recruitment Prone
Ventilatory Management of ARDS Alexei Ortiz Milan; MD, MSc 2017 Outline Ventilatory management of ARDS Protected Ventilatory Strategy Use of NMB Selection of PEEP Driving pressure Lung Recruitment Prone
ARDS: an update 6 th March A. Hakeem Al Hashim, MD, FRCP SQUH
 ARDS: an update 6 th March 2017 A. Hakeem Al Hashim, MD, FRCP SQUH 30M, previously healthy Hx: 1 week dry cough Gradually worsening SOB No travel Hx Case BP 130/70, HR 100/min ph 7.29 pco2 35 po2 50 HCO3
ARDS: an update 6 th March 2017 A. Hakeem Al Hashim, MD, FRCP SQUH 30M, previously healthy Hx: 1 week dry cough Gradually worsening SOB No travel Hx Case BP 130/70, HR 100/min ph 7.29 pco2 35 po2 50 HCO3
Prone Position in ARDS
 Prone Position in ARDS Rich Kallet MS RRT FAARC, FCCM Respiratory Care Services Department of Anesthesia & Perioperative Care University of California, San Francisco, San Francisco General Hospital Case
Prone Position in ARDS Rich Kallet MS RRT FAARC, FCCM Respiratory Care Services Department of Anesthesia & Perioperative Care University of California, San Francisco, San Francisco General Hospital Case
Continuous vs Intermittent Dosing of Antibiotics in Critically-Ill Patients
 Continuous vs Intermittent Dosing of Antibiotics in Critically-Ill Patients Jan O Friedrich, MD DPhil Associate Professor of Medicine, University of Toronto Medical Director, MSICU St. Michael s Hospital,
Continuous vs Intermittent Dosing of Antibiotics in Critically-Ill Patients Jan O Friedrich, MD DPhil Associate Professor of Medicine, University of Toronto Medical Director, MSICU St. Michael s Hospital,
The use of proning in the management of Acute Respiratory Distress Syndrome
 Case 3 The use of proning in the management of Acute Respiratory Distress Syndrome Clinical Problem This expanded case summary has been chosen to explore the rationale and evidence behind the use of proning
Case 3 The use of proning in the management of Acute Respiratory Distress Syndrome Clinical Problem This expanded case summary has been chosen to explore the rationale and evidence behind the use of proning
Management of Severe ARDS: Current Canadian Practice
 Management of Severe ARDS: Current Canadian Practice Erick Duan MD FRCPC Clinical Scholar, Department of Medicine, Division of Critical Care, McMaster University Intensivist, St. Joseph's Healthcare Hamilton
Management of Severe ARDS: Current Canadian Practice Erick Duan MD FRCPC Clinical Scholar, Department of Medicine, Division of Critical Care, McMaster University Intensivist, St. Joseph's Healthcare Hamilton
ARDS and Ventilators PG26 Update in Surgical Critical Care October 9, 2013
 ARDS and Ventilators PG26 Update in Surgical Critical Care October 9, 2013 Pauline K. Park MD, FACS, FCCM University of Michigan School of Medicine Ann Arbor, MI OVERVIEW New Berlin definition of ARDS
ARDS and Ventilators PG26 Update in Surgical Critical Care October 9, 2013 Pauline K. Park MD, FACS, FCCM University of Michigan School of Medicine Ann Arbor, MI OVERVIEW New Berlin definition of ARDS
ARDS: The Evidence. Topics. New definition Breaths: Little or Big? Wet or Dry? Moving or Still? Upside down or Right side up?
 ARDS: The Evidence Todd M Bull MD Professor of Medicine Division of Pulmonary Sciences and Critical Care Division of Cardiology Director Pulmonary Vascular Disease Center Director Center for Lungs and
ARDS: The Evidence Todd M Bull MD Professor of Medicine Division of Pulmonary Sciences and Critical Care Division of Cardiology Director Pulmonary Vascular Disease Center Director Center for Lungs and
The Berlin Definition: Does it fix anything?
 The Berlin Definition: Does it fix anything? Gordon D. Rubenfeld, MD MSc Professor of Medicine, University of Toronto Chief, Program in Trauma, Emergency, and Critical Care Sunnybrook Health Sciences Centre
The Berlin Definition: Does it fix anything? Gordon D. Rubenfeld, MD MSc Professor of Medicine, University of Toronto Chief, Program in Trauma, Emergency, and Critical Care Sunnybrook Health Sciences Centre
Outline. Basic principles of lung protective ventilation. The challenging areas. Small tidal volumes Recruitment
 ARDS beyond 6/kg Gordon D. Rubenfeld, MD MSc Professor of Medicine, University of Toronto Chief, Program in Trauma, Emergency, and Critical Care Sunnybrook Health Sciences Centre Outline Basic principles
ARDS beyond 6/kg Gordon D. Rubenfeld, MD MSc Professor of Medicine, University of Toronto Chief, Program in Trauma, Emergency, and Critical Care Sunnybrook Health Sciences Centre Outline Basic principles
Tailored Volume Resuscitation in the Critically Ill is Achievable. Objectives. Clinical Case 2/16/2018
 Tailored Volume Resuscitation in the Critically Ill is Achievable Heath E Latham, MD Associate Professor Fellowship Program Director Pulmonary and Critical Care Objectives Describe the goal of resuscitation
Tailored Volume Resuscitation in the Critically Ill is Achievable Heath E Latham, MD Associate Professor Fellowship Program Director Pulmonary and Critical Care Objectives Describe the goal of resuscitation
Difficult Ventilation in ARDS Patients
 Thank you for viewing this presentation. We would like to remind you that this material is the property of the author. It is provided to you by the ERS for your personal use only, as submitted by the author.
Thank you for viewing this presentation. We would like to remind you that this material is the property of the author. It is provided to you by the ERS for your personal use only, as submitted by the author.
ARDS and treatment strategies
 ARDS and treatment strategies Geoff Bellingan Medical Director University College Hospital ARDS: Definitions History of predisposing condition Refractory hypoxaemia of acute onset PaO 2 /FiO 2 ratio:
ARDS and treatment strategies Geoff Bellingan Medical Director University College Hospital ARDS: Definitions History of predisposing condition Refractory hypoxaemia of acute onset PaO 2 /FiO 2 ratio:
Year in Review: Critical Care Medicine
 Year in Review: Critical Care Medicine No disclosures Eric J. Seeley, M.D. Assistant Professor of Medicine Division of Pulmonary and Critical Care Medicine Why I Selected These Studies High quality studies
Year in Review: Critical Care Medicine No disclosures Eric J. Seeley, M.D. Assistant Professor of Medicine Division of Pulmonary and Critical Care Medicine Why I Selected These Studies High quality studies
Acute Kidney Injury (AKI) How Wise is Early Dialysis in Critically Ill Patients? Modalities of Dialysis
 How Wise is Early Dialysis in Critically Ill Patients? Modalities of Dialysis") Acute Kidney Injury (AKI) How Wise is Early Dialysis in Critically Ill Patients? A common condition in ICU patients Associated with high mortality and morbidity Renal Replacement Therapy (RRT) is the cornerstone
Acute Kidney Injury (AKI) How Wise is Early Dialysis in Critically Ill Patients? A common condition in ICU patients Associated with high mortality and morbidity Renal Replacement Therapy (RRT) is the cornerstone
1. Screening to identify SBT candidates
 Karen E. A. Burns MD, FRCPC, MSc (Epid) Associate Professor, Clinician Scientist St. Michael s Hospital, Toronto, Canada burnsk@smh.ca Review evidence supporting: 1. Screening to identify SBT candidates
Karen E. A. Burns MD, FRCPC, MSc (Epid) Associate Professor, Clinician Scientist St. Michael s Hospital, Toronto, Canada burnsk@smh.ca Review evidence supporting: 1. Screening to identify SBT candidates
OSCAR & OSCILLATE. & the Future of High Frequency Oscillatory Ventilation (HFOV)
") & & the Future of High Frequency Oscillatory Ventilation (HFOV) www.philippelefevre.com What do we know already? Sud S et al. BMJ 2010 & Multi-centre randomised controlled trials of HFOV verses current
& & the Future of High Frequency Oscillatory Ventilation (HFOV) www.philippelefevre.com What do we know already? Sud S et al. BMJ 2010 & Multi-centre randomised controlled trials of HFOV verses current
NIV in hypoxemic patients
 NIV in hypoxemic patients Massimo Antonelli, MD Dept. of Intensive Care & Anesthesiology Università Cattolica del Sacro Cuore Rome - Italy Conflict of interest (research grants and consultations): Maquet
NIV in hypoxemic patients Massimo Antonelli, MD Dept. of Intensive Care & Anesthesiology Università Cattolica del Sacro Cuore Rome - Italy Conflict of interest (research grants and consultations): Maquet
Policy #: 440 Latest Review Date: May 2016
 Name of Policy: Inhaled Nitric Oxide Policy #: 440 Latest Review Date: May 2016 Category: Therapy Policy Grade: B Background/Definitions: As a general rule, benefits are payable under Blue Cross and Blue
Name of Policy: Inhaled Nitric Oxide Policy #: 440 Latest Review Date: May 2016 Category: Therapy Policy Grade: B Background/Definitions: As a general rule, benefits are payable under Blue Cross and Blue
10/16/2017. Review the indications for ECMO in patients with. Respiratory failure Cardiac failure Cardiorespiratory failure
 Review the indications for ECMO in patients with Respiratory failure Cardiac failure Cardiorespiratory failure 1 Extracorporeal membrane lung and/or cardiac support. A support therapy, in no way definitive.
Review the indications for ECMO in patients with Respiratory failure Cardiac failure Cardiorespiratory failure 1 Extracorporeal membrane lung and/or cardiac support. A support therapy, in no way definitive.
Effects of mechanical ventilation on organ function. Masterclass ICU nurses
 Effects of mechanical ventilation on organ function Masterclass ICU nurses Case Male, 60 - No PMH - L 1.74 m and W 85 kg Pneumococcal pneumonia Stable hemodynamics - No AKI MV in prone position (PEEP 16
Effects of mechanical ventilation on organ function Masterclass ICU nurses Case Male, 60 - No PMH - L 1.74 m and W 85 kg Pneumococcal pneumonia Stable hemodynamics - No AKI MV in prone position (PEEP 16
Best of Pulmonary Jennifer R. Hucks, MD University of South Carolina School of Medicine
 Best of Pulmonary 2012-2013 Jennifer R. Hucks, MD University of South Carolina School of Medicine Topics ARDS- Berlin Definition Prone Positioning For ARDS Lung Protective Ventilation In Patients Without
Best of Pulmonary 2012-2013 Jennifer R. Hucks, MD University of South Carolina School of Medicine Topics ARDS- Berlin Definition Prone Positioning For ARDS Lung Protective Ventilation In Patients Without
Update in Critical Care Medicine
 Update in Critical Care Medicine Michael A. Gropper, MD, PhD Professor and Executive Vice Chair Department of Anesthesia and Perioperative Care Director, Critical Care Medicine UCSF Disclosure None Update
Update in Critical Care Medicine Michael A. Gropper, MD, PhD Professor and Executive Vice Chair Department of Anesthesia and Perioperative Care Director, Critical Care Medicine UCSF Disclosure None Update
Cardiorespiratory Interactions:
 Cardiorespiratory Interactions: The Heart - Lung Connection Jon N. Meliones, MD, MS, FCCM Professor of Pediatrics Duke University Medical Director PCVICU Optimizing CRI Cardiorespiratory Economics O2:
Cardiorespiratory Interactions: The Heart - Lung Connection Jon N. Meliones, MD, MS, FCCM Professor of Pediatrics Duke University Medical Director PCVICU Optimizing CRI Cardiorespiratory Economics O2:
Steroids in ARDS: if, when, how much? John Fowler, MD, FACEP Dept. of Emergency Medicine Kent Hospital, İzmir, Türkiye
 Steroids in ARDS: if, when, how much? John Fowler, MD, FACEP Dept. of Emergency Medicine Kent Hospital, İzmir, Türkiye Steroids in ARDS: conclusion Give low-dose steroids if indicated for another problem
Steroids in ARDS: if, when, how much? John Fowler, MD, FACEP Dept. of Emergency Medicine Kent Hospital, İzmir, Türkiye Steroids in ARDS: conclusion Give low-dose steroids if indicated for another problem
Ventilation in Paediatric ARDS: extrapolate from adult studies?
 Ventilation in Paediatric ARDS: extrapolate from adult studies? ASMIC 2014 Dr Adrian Plunkett Consultant Paediatric Intensivist Birmingham Children s Hospital, UK Aims of the presentation Ventilation
Ventilation in Paediatric ARDS: extrapolate from adult studies? ASMIC 2014 Dr Adrian Plunkett Consultant Paediatric Intensivist Birmingham Children s Hospital, UK Aims of the presentation Ventilation
Noninvasive Ventilation: Non-COPD Applications
 Noninvasive Ventilation: Non-COPD Applications NONINVASIVE MECHANICAL VENTILATION Why Noninvasive Ventilation? Avoids upper A respiratory airway trauma system lacerations, protective hemorrhage strategy
Noninvasive Ventilation: Non-COPD Applications NONINVASIVE MECHANICAL VENTILATION Why Noninvasive Ventilation? Avoids upper A respiratory airway trauma system lacerations, protective hemorrhage strategy
Guideline for the Use of inhaled Nitric Oxide (NO) Catarina Silvestre Prof. Harish Vyas
 Catarina Silvestre Prof. Harish Vyas") Inhaled Nitric Oxide Title of Guideline Guideline for the Use of inhaled Nitric Oxide (NO) 1a 2a 2b Contact Name and Job Title (author) Directorate & Speciality Date of submission October 2015 Date when
Inhaled Nitric Oxide Title of Guideline Guideline for the Use of inhaled Nitric Oxide (NO) 1a 2a 2b Contact Name and Job Title (author) Directorate & Speciality Date of submission October 2015 Date when
Impact of Fluids in Children with Acute Lung Injury
 Impact of Fluids in Children with Acute Lung Injury Canadian Critical Care Forum Toronto, Canada October 27 th, 2015 Adrienne G. Randolph, MD, MSc Critical Care Division, Department of Anesthesia, Perioperative
Impact of Fluids in Children with Acute Lung Injury Canadian Critical Care Forum Toronto, Canada October 27 th, 2015 Adrienne G. Randolph, MD, MSc Critical Care Division, Department of Anesthesia, Perioperative
Pulmonary Vasodilator Treatments in the ICU Setting
 Pulmonary Vasodilator Treatments in the ICU Setting Lara Shekerdemian Circulation 1979 Ann Thorac Surg 27 Anesth Analg 211 1 Factors in the ICU Management of Pulmonary Hypertension After Cardiopulmonary
Pulmonary Vasodilator Treatments in the ICU Setting Lara Shekerdemian Circulation 1979 Ann Thorac Surg 27 Anesth Analg 211 1 Factors in the ICU Management of Pulmonary Hypertension After Cardiopulmonary
MEDICAL POLICY I. POLICY POLICY TITLE POLICY NUMBER INHALED NITRIC OXIDE MP-4.021
 Original Issue Date (Created): August 23, 2002 Most Recent Review Date (Revised): January 28, 2014 Effective Date: April 1, 2014 I. POLICY Inhaled nitric oxide may be considered medically necessary as
Original Issue Date (Created): August 23, 2002 Most Recent Review Date (Revised): January 28, 2014 Effective Date: April 1, 2014 I. POLICY Inhaled nitric oxide may be considered medically necessary as
The Association Between Oxygenation Thresholds and Mortality During Extracorporeal Life Support
 The Association Between Oxygenation Thresholds and Mortality During Extracorporeal Life Support Laveena Munshi, MD, MSc November 1, 2016 Critical Care Canada Forum Interdepartmental Division of Critical
The Association Between Oxygenation Thresholds and Mortality During Extracorporeal Life Support Laveena Munshi, MD, MSc November 1, 2016 Critical Care Canada Forum Interdepartmental Division of Critical
Surgery Grand Rounds. Non-invasive Ventilation: A valuable tool. James Cromie, PGY 3 8/24/09
 Surgery Grand Rounds Non-invasive Ventilation: A valuable tool James Cromie, PGY 3 8/24/09 History of mechanical ventilation 1930 s: use of iron lung 1940 s: First NIV system (Bellevue Hospital) 1950 s:
Surgery Grand Rounds Non-invasive Ventilation: A valuable tool James Cromie, PGY 3 8/24/09 History of mechanical ventilation 1930 s: use of iron lung 1940 s: First NIV system (Bellevue Hospital) 1950 s:
Management of refractory ARDS. Saurabh maji
 Management of refractory ARDS Saurabh maji Refractory hypoxemia as PaO2/FIO2 is less than 100 mm Hg, inability to keep plateau pressure below 30 cm H2O despite a VT of 4 ml/kg development of barotrauma
Management of refractory ARDS Saurabh maji Refractory hypoxemia as PaO2/FIO2 is less than 100 mm Hg, inability to keep plateau pressure below 30 cm H2O despite a VT of 4 ml/kg development of barotrauma
Prone ventilation revisited in H1N1 patients
 International Journal of Advanced Multidisciplinary Research ISSN: 2393-8870 www.ijarm.com DOI: 10.22192/ijamr Volume 5, Issue 10-2018 Case Report DOI: http://dx.doi.org/10.22192/ijamr.2018.05.10.005 Prone
International Journal of Advanced Multidisciplinary Research ISSN: 2393-8870 www.ijarm.com DOI: 10.22192/ijamr Volume 5, Issue 10-2018 Case Report DOI: http://dx.doi.org/10.22192/ijamr.2018.05.10.005 Prone
Early Rehabilitation in the ICU: Do We Still Need Chest Physiotherapy?
 Early Rehabilitation in the ICU: Do We Still Need Chest Physiotherapy? Michelle Kho, PT, PhD Assistant Professor, School of Rehabilitation Science, McMaster University Adjunct Assistant Professor, Department
Early Rehabilitation in the ICU: Do We Still Need Chest Physiotherapy? Michelle Kho, PT, PhD Assistant Professor, School of Rehabilitation Science, McMaster University Adjunct Assistant Professor, Department
Inhaled epoprostenol vs inhaled nitric oxide for refractory hypoxemia in critically ill patients
 Journal of Critical Care (2013) 28, 844 848 Inhaled epoprostenol vs inhaled nitric oxide for refractory hypoxemia in critically ill patients Heather Torbic PharmD, BCPS a,, Paul M. Szumita PharmD, BCPS
Journal of Critical Care (2013) 28, 844 848 Inhaled epoprostenol vs inhaled nitric oxide for refractory hypoxemia in critically ill patients Heather Torbic PharmD, BCPS a,, Paul M. Szumita PharmD, BCPS
Phenotyping of ARDS and non ARDS Patients
 Critical Care Canada Forum 2018 Sheraton Toronto, Toronto, Canada November 8, 2018; 11:05h 11:25h Phenotyping of and non Patients Berlin & Kigali, RALE score, Reclassification, Driving Pressure and Mechanical
Critical Care Canada Forum 2018 Sheraton Toronto, Toronto, Canada November 8, 2018; 11:05h 11:25h Phenotyping of and non Patients Berlin & Kigali, RALE score, Reclassification, Driving Pressure and Mechanical
Disclosures Paul Walker MD PhD FRCSC
 1 ` Disclosures Paul Walker MD PhD FRCSC CEO Spectral Medical 2001-present Inaugural Critical Care Program Director - University of Toronto Chief of Surgery - University Health Network 1991-1999 COO Toronto
1 ` Disclosures Paul Walker MD PhD FRCSC CEO Spectral Medical 2001-present Inaugural Critical Care Program Director - University of Toronto Chief of Surgery - University Health Network 1991-1999 COO Toronto
Original Policy Date
 MP 8.01.17 Inhaled Nitric Oxide Medical Policy Section Therapy Issue 12/2013 Original Policy Date 12/2013 Last Review Status/Date Reviewed with literature search/12/2013 Return to Medical Policy Index
MP 8.01.17 Inhaled Nitric Oxide Medical Policy Section Therapy Issue 12/2013 Original Policy Date 12/2013 Last Review Status/Date Reviewed with literature search/12/2013 Return to Medical Policy Index
Part 2 of park s Ventilator and ARDS slides for syllabus
 Part 2 of park s Ventilator and ARDS slides for syllabus Early Neuromuscular Blockade Question 4 The early use of cis-atracurium in severe ARDS is: A. Contraindicated in patients with diabetes B. Associated
Part 2 of park s Ventilator and ARDS slides for syllabus Early Neuromuscular Blockade Question 4 The early use of cis-atracurium in severe ARDS is: A. Contraindicated in patients with diabetes B. Associated
15 Years Of Clinical Trials In ARDS: What Progress Have We Made?
 15 Years Of Clinical Trials In ARDS: What Progress Have We Made? Niall D. Ferguson, MD, FRCPC, MSc Head of Critical Care Medicine University Health Network & Mount Sinai Hospital Senior Scientist, Toronto
15 Years Of Clinical Trials In ARDS: What Progress Have We Made? Niall D. Ferguson, MD, FRCPC, MSc Head of Critical Care Medicine University Health Network & Mount Sinai Hospital Senior Scientist, Toronto
Marcelo Cypel MD MSc
 Ex vivo Organ Repair Marcelo Cypel MD MSc Canada Research Chair in Lung Transplantation Surgical Director ECLS Program UHN Assistant Professor of Surgery Division of Thoracic Surgery University Health
Ex vivo Organ Repair Marcelo Cypel MD MSc Canada Research Chair in Lung Transplantation Surgical Director ECLS Program UHN Assistant Professor of Surgery Division of Thoracic Surgery University Health
Subject: Inhaled Nitric Oxide
 07-00007-12 Original Effective Date: 04/15/01 Reviewed: 09/27/18 Revised: 10/15/18 Subject: Inhaled Nitric Oxide THIS MEDICAL COVERAGE GUIDELINE IS NOT AN AUTHORIZATION, CERTIFICATION, EXPLANATION OF BENEFITS,
07-00007-12 Original Effective Date: 04/15/01 Reviewed: 09/27/18 Revised: 10/15/18 Subject: Inhaled Nitric Oxide THIS MEDICAL COVERAGE GUIDELINE IS NOT AN AUTHORIZATION, CERTIFICATION, EXPLANATION OF BENEFITS,
Surviving Sepsis Campaign. Guidelines for Management of Severe Sepsis/Septic Shock. An Overview
 Surviving Sepsis Campaign Guidelines for Management of Severe Sepsis/Septic Shock An Overview Mechanical Ventilation of Sepsis-Induced ALI/ARDS ARDSnet Mechanical Ventilation Protocol Results: Mortality
Surviving Sepsis Campaign Guidelines for Management of Severe Sepsis/Septic Shock An Overview Mechanical Ventilation of Sepsis-Induced ALI/ARDS ARDSnet Mechanical Ventilation Protocol Results: Mortality
Inhaled Nitric Oxide or Prostacyclin in Acute Respiratory Failure: Efficacy, Safety, and Cost
 Inhaled Nitric Oxide or Prostacyclin in Acute Respiratory Failure: Efficacy, Safety, and Cost Richard H Kallet MS RRT FAARC, FCCM Respiratory Care Services Dept of Anesthesia & Perioperative Care University
Inhaled Nitric Oxide or Prostacyclin in Acute Respiratory Failure: Efficacy, Safety, and Cost Richard H Kallet MS RRT FAARC, FCCM Respiratory Care Services Dept of Anesthesia & Perioperative Care University
Mechanical ventilation induced or exacerbated right ventricular failure
 Mechanical ventilation induced or exacerbated right ventricular failure Toronto 2016 Jesse Hall MD Professor of Medicine, Anesthesia & Critical Care University of Chicago Faculty Disclosures Dr. Hall
Mechanical ventilation induced or exacerbated right ventricular failure Toronto 2016 Jesse Hall MD Professor of Medicine, Anesthesia & Critical Care University of Chicago Faculty Disclosures Dr. Hall
A Validated Practical Risk Score to Predict the Need for RVAD after Continuous-flow LVAD
 A Validated Practical Risk Score to Predict the Need for RVAD after Continuous-flow LVAD SK Singh MD MSc, DK Pujara MBBS, J Anand MD, WE Cohn MD, OH Frazier MD, HR Mallidi MD Division of Transplant & Assist
A Validated Practical Risk Score to Predict the Need for RVAD after Continuous-flow LVAD SK Singh MD MSc, DK Pujara MBBS, J Anand MD, WE Cohn MD, OH Frazier MD, HR Mallidi MD Division of Transplant & Assist
Patient characteristics Intervention Comparison Length of followup
 ORAL MUCOLYTICS Ref ID: 2511 Bachh AA, Shah NN, Bhargava R et al. Effect oral N- in COPD - A randomised controlled trial. JK Practitioner. 2007; 14(1):12-16. Ref ID: 2511 RCT Single blind; unclear allocation
ORAL MUCOLYTICS Ref ID: 2511 Bachh AA, Shah NN, Bhargava R et al. Effect oral N- in COPD - A randomised controlled trial. JK Practitioner. 2007; 14(1):12-16. Ref ID: 2511 RCT Single blind; unclear allocation
Pediatric Acute Respiratory Distress Syndrome (PARDS): Do we have consensus? Doug Willson, MD Children s Hospital of Richmond at VCU April 20, 2015
: Do we have consensus? Doug Willson, MD Children s Hospital of Richmond at VCU April 20, 2015") Pediatric Acute Respiratory Distress Syndrome (PARDS): Do we have consensus? Doug Willson, MD Children s Hospital of Richmond at VCU April 20, 2015 Conflicts to Disclose! I am a consultant for Discovery
Pediatric Acute Respiratory Distress Syndrome (PARDS): Do we have consensus? Doug Willson, MD Children s Hospital of Richmond at VCU April 20, 2015 Conflicts to Disclose! I am a consultant for Discovery
RESEARCH. High frequency oscillation in patients with acute lung injury andacuterespiratorydistresssyndrome(ards):systematic review and meta-analysis
:systematic review and meta-analysis") High frequency oscillation in patients with acute lung injury andacuterespiratorydistresssyndrome(ards):systematic review and meta-analysis Sachin Sud, fellow, 1 Maneesh Sud, medical student, 2 Jan O Friedrich,
High frequency oscillation in patients with acute lung injury andacuterespiratorydistresssyndrome(ards):systematic review and meta-analysis Sachin Sud, fellow, 1 Maneesh Sud, medical student, 2 Jan O Friedrich,
Critical Care: Role of MV, ECMO, and other critical infrastructure
 Critical Care: Role of MV, ECMO, and other critical infrastructure Christian Sandrock, MD, MPH UC Davis School of Medicine The Next 30 Minutes Why the ICU? Why are some critical care issues, particularly
Critical Care: Role of MV, ECMO, and other critical infrastructure Christian Sandrock, MD, MPH UC Davis School of Medicine The Next 30 Minutes Why the ICU? Why are some critical care issues, particularly
Neuromuscular Blockade in ARDS
 Neuromuscular Blockade in ARDS Maureen O. Meade, MD, FRCPC Critical care consultant, Hamilton Health Sciences Professor of Medicine, McMaster University www.oscillatetrial.com Disclosures None Possible
Neuromuscular Blockade in ARDS Maureen O. Meade, MD, FRCPC Critical care consultant, Hamilton Health Sciences Professor of Medicine, McMaster University www.oscillatetrial.com Disclosures None Possible
What is sepsis? RECOGNITION. Sepsis I Know It When I See It 9/21/2017
 Sepsis I Know It When I See It September 15, 2017 Matthew Exline, MD MPH Medical Director, Medical ICU What is sepsis? I shall not today attempt further to define the kinds of material [b]ut I know it
Sepsis I Know It When I See It September 15, 2017 Matthew Exline, MD MPH Medical Director, Medical ICU What is sepsis? I shall not today attempt further to define the kinds of material [b]ut I know it
Right Ventricular Failure: Prediction, Prevention and Treatment
 Right Ventricular Failure: Prediction, Prevention and Treatment 3 rd European Training Symposium for Heart Failure Cardiologists and Cardiac Surgeons University Hospital Bern June 24-25, 2016 Disclosures:
Right Ventricular Failure: Prediction, Prevention and Treatment 3 rd European Training Symposium for Heart Failure Cardiologists and Cardiac Surgeons University Hospital Bern June 24-25, 2016 Disclosures:
Targeting depression after ARDS. Neill Adhikari Sunnybrook Health Sciences and University of Toronto 29 October 2012
 Targeting depression after ARDS Neill Adhikari Sunnybrook Health Sciences and University of Toronto 29 October 2012 None Conflicts of interest Objectives Review epidemiology of depression after ARDS Review
Targeting depression after ARDS Neill Adhikari Sunnybrook Health Sciences and University of Toronto 29 October 2012 None Conflicts of interest Objectives Review epidemiology of depression after ARDS Review
Lies, damn lies, & clinical trials. Paul Young
 Lies, damn lies, & clinical trials Paul Young Base rate neglect statistical power probability of detecting a difference if one exists P of
Lies, damn lies, & clinical trials Paul Young Base rate neglect statistical power probability of detecting a difference if one exists P of
Nutrition and Sepsis
 Nutrition and Sepsis Todd W. Rice, MD, MSc Associate Professor of Medicine Vanderbilt University 2017 DNS Symposium June 2, 2017 Case 55 y.o. male COPD, DM, HTN, presents with pneumonia and septic shock.
Nutrition and Sepsis Todd W. Rice, MD, MSc Associate Professor of Medicine Vanderbilt University 2017 DNS Symposium June 2, 2017 Case 55 y.o. male COPD, DM, HTN, presents with pneumonia and septic shock.
Clinical syndrome of severe dyspnea of rapid onset, hypoxemia, and diffuse pulmonary infiltrates leading to respiratory failure.
 Yuanlin Song, M.D. Clinical syndrome of severe dyspnea of rapid onset, hypoxemia, and diffuse pulmonary infiltrates leading to respiratory failure. Pneumonia Trauma SARS PaO2/fiO2
Yuanlin Song, M.D. Clinical syndrome of severe dyspnea of rapid onset, hypoxemia, and diffuse pulmonary infiltrates leading to respiratory failure. Pneumonia Trauma SARS PaO2/fiO2
ECLS Bridge to Lung Transplantation Optimizing and Ambulating the Recipient
 ECLS Bridge to Lung Transplantation Optimizing and Ambulating the Recipient Shaf Keshavjee MD MSc FRCSC FACS Surgeon-in-Chief, University Health Network James Wallace McCutcheon Chair in Surgery Director,
ECLS Bridge to Lung Transplantation Optimizing and Ambulating the Recipient Shaf Keshavjee MD MSc FRCSC FACS Surgeon-in-Chief, University Health Network James Wallace McCutcheon Chair in Surgery Director,
Fluids in Sepsis Less is more. Dr Anand Senthi Joondalup Health Campus ED MBBS, MAppFin, GradCertPubHlth,
 Fluids in Sepsis Less is more Dr Anand Senthi Joondalup Health Campus ED MBBS, MAppFin, GradCertPubHlth, FRACGP @drsenthi Summary Discussion of the evidence for/against fluid resuscitation in septic shock
Fluids in Sepsis Less is more Dr Anand Senthi Joondalup Health Campus ED MBBS, MAppFin, GradCertPubHlth, FRACGP @drsenthi Summary Discussion of the evidence for/against fluid resuscitation in septic shock
What is Acute Respiratory Distress Syndrome? Acute Respiratory Distress Syndrome (ARDS)
") Acute Respiratory Distress Syndrome (ARDS) Sonal Pannu, MD Clinical Assistant Professor Department of Internal Medicine Division of Pulmonary, Allergy, Critical Care and Sleep Medicine The Ohio State University
Acute Respiratory Distress Syndrome (ARDS) Sonal Pannu, MD Clinical Assistant Professor Department of Internal Medicine Division of Pulmonary, Allergy, Critical Care and Sleep Medicine The Ohio State University
Acute Respiratory Distress Syndrome (ARDS) What is Acute Respiratory Distress Syndrome?
 What is Acute Respiratory Distress Syndrome?") Acute Respiratory Distress Syndrome (ARDS) Sonal Pannu, MD Clinical Assistant Professor Department of Internal Medicine Division of Pulmonary, Allergy, Critical Care and Sleep Medicine The Ohio State University
Acute Respiratory Distress Syndrome (ARDS) Sonal Pannu, MD Clinical Assistant Professor Department of Internal Medicine Division of Pulmonary, Allergy, Critical Care and Sleep Medicine The Ohio State University
Protective ventilation for ALL patients
 Protective ventilation for ALL patients PAOLO PELOSI, MD, FERS Department of Surgical Sciences and Integrated Diagnostics (DISC), San Martino Policlinico Hospital IRCCS for Oncology, University of Genoa,
Protective ventilation for ALL patients PAOLO PELOSI, MD, FERS Department of Surgical Sciences and Integrated Diagnostics (DISC), San Martino Policlinico Hospital IRCCS for Oncology, University of Genoa,
Optimize vent weaning and SBT outcomes. Identify underlying causes for SBT failures. Role SBT and weaning protocol have in respiratory care
 Optimize vent weaning and SBT outcomes Identify underlying causes for SBT failures Role SBT and weaning protocol have in respiratory care Lower risk of developing complications Lower risk of VAP, other
Optimize vent weaning and SBT outcomes Identify underlying causes for SBT failures Role SBT and weaning protocol have in respiratory care Lower risk of developing complications Lower risk of VAP, other
Keep. with life MEDICATION TECHNOLOGY SERVICES INSPIRED BY YOUR NEEDS
 Keep with life MEDICATION TECHNOLOGY SERVICES INSPIRED BY YOUR NEEDS 2 KINOX MEDICATION KINOX, inhaled nitric oxide, is a selective pulmonary vasodilator developed by Air Liquide Healthcare and characterized
Keep with life MEDICATION TECHNOLOGY SERVICES INSPIRED BY YOUR NEEDS 2 KINOX MEDICATION KINOX, inhaled nitric oxide, is a selective pulmonary vasodilator developed by Air Liquide Healthcare and characterized
Optimizing the Donor Lung with EVLP
 Optimizing the Donor Lung with EVLP Marcelo Cypel MD MSc FRCSC Canada Research Chair in Lung Transplantation Surgical Director ECLS Lung Program UHN Associate Professor of Surgery Division of Thoracic
Optimizing the Donor Lung with EVLP Marcelo Cypel MD MSc FRCSC Canada Research Chair in Lung Transplantation Surgical Director ECLS Lung Program UHN Associate Professor of Surgery Division of Thoracic
Analyzing Lung protective ventilation F Javier Belda MD, PhD Sº de Anestesiología y Reanimación. Hospital Clinico Universitario Valencia (Spain)
") Analyzing Lung protective ventilation F Javier Belda MD, PhD Sº de Anestesiología y Reanimación Hospital Clinico Universitario Valencia (Spain) ALI/ARDS Report of the American-European consensus conference
Analyzing Lung protective ventilation F Javier Belda MD, PhD Sº de Anestesiología y Reanimación Hospital Clinico Universitario Valencia (Spain) ALI/ARDS Report of the American-European consensus conference
CSIM annual meeting Acute respiratory failure. Dr. John Ronald, FRCPC Int Med, Resp, CCM. October 10, 2018
 CSIM annual meeting - 2018 Acute respiratory failure Dr. John Ronald, FRCPC Int Med, Resp, CCM. October 10, 2018 NRGH affiliated with UBC medicine Disclosures None relevant to this presentation. Also no
CSIM annual meeting - 2018 Acute respiratory failure Dr. John Ronald, FRCPC Int Med, Resp, CCM. October 10, 2018 NRGH affiliated with UBC medicine Disclosures None relevant to this presentation. Also no
Canadian Society of Internal Medicine Annual Meeting 2018 Banff, AB
 Canadian Society of Internal Medicine Annual Meeting 2018 Banff, AB Mortality and morbidity in acutely ill adults treated with liberal vs. conservative oxygen therapy: systematic review and meta-analysis
Canadian Society of Internal Medicine Annual Meeting 2018 Banff, AB Mortality and morbidity in acutely ill adults treated with liberal vs. conservative oxygen therapy: systematic review and meta-analysis
Keeping Patients Off the Vent: Bilevel, HFNC, Neither?
 Keeping Patients Off the Vent: Bilevel, HFNC, Neither? Robert Kempainen, MD Pulmonary and Critical Care Medicine Hennepin County Medical Center University of Minnesota School of Medicine Objectives Summarize
Keeping Patients Off the Vent: Bilevel, HFNC, Neither? Robert Kempainen, MD Pulmonary and Critical Care Medicine Hennepin County Medical Center University of Minnesota School of Medicine Objectives Summarize
9/5/2018. Conflicts of Interests. Pediatric Acute Respiratory Distress Syndrome. Objectives ARDS ARDS. Definitions. None
 Pediatric Acute Respiratory Distress Syndrome Conflicts of Interests Diane C Lipscomb, MD Director Inpatient Pediatric Medical Director Mercy Springfield Associate Clerkship Clinical Director University
Pediatric Acute Respiratory Distress Syndrome Conflicts of Interests Diane C Lipscomb, MD Director Inpatient Pediatric Medical Director Mercy Springfield Associate Clerkship Clinical Director University
Veno-Venous ECMO Support. Chris Cropsey, MD Sept. 21, 2015
 Veno-Venous ECMO Support Chris Cropsey, MD Sept. 21, 2015 Objectives List indications and contraindications for ECMO Describe hemodynamics and oxygenation on ECMO Discuss evidence for ECMO outcomes Identify
Veno-Venous ECMO Support Chris Cropsey, MD Sept. 21, 2015 Objectives List indications and contraindications for ECMO Describe hemodynamics and oxygenation on ECMO Discuss evidence for ECMO outcomes Identify
Supplementary appendix
 Supplementary appendix This appendix formed part of the original submission and has been peer reviewed. We post it as supplied by the authors. Supplement to: Blum CA, Nigro N, Briel M, et al. Adjunct prednisone
Supplementary appendix This appendix formed part of the original submission and has been peer reviewed. We post it as supplied by the authors. Supplement to: Blum CA, Nigro N, Briel M, et al. Adjunct prednisone